Embed Size (px)
Citation preview

Hybrid Closed Loop Status &
Practical Challenges in Implementation
Bruce Buckingham, MD
Professor of Pediatric Endocrinology
Stanford School of Medicine

Company Nature of RelationshipNovo-Nordisk ConsultingSanofi ConsultingBD ConsultingConvatec ConsultingMedtronic Research FundingInsulet Research FundingDexcom Research SupportBigfoot Research FundingTandem Research Funding, Consulting
Conflict of Interests

Current State of Type 1 Diabetes
Updated T1D Exchange - 2015K. Miller , Diabetes Care 38: 971

58%50%
58% 57% 56%61% 60% 56%
61% 62% 66% 60%56%
65%62% 58%
0%
20%
40%
60%
80%
100%
Overall <6 6-12 13-17 18-25 26-49 50-64 ≥65Age (years)
Enrolled 9/1/2010 - 8/1/2012Current 4/1/2014 - 4/1/2015
Insulin Pump Use Is Increasing

CGM Use Is Increasing - 2016
17%
10%6% 8%
25%21%
14%
32%
17%
10% 12%
27% 27%
18%
0%
10%
20%
30%
40%
50%
<6 6-12 13-17 18-25 26-49 50-64 ≥ 65
Enrolled 2014-2015 (8% use CGMoverall)

24% 24%22% 17%
31% 28%36%
20% 22% 18% 15%
31% 28%36%
0%
20%
40%
60%
80%
100%
<6 6-12 13-17 18-25 26-49 50-64 ≥65
Age (years)
Enrolled 2010 - 2012 Current 2014 - 2015
ADA HbA1c Targets Not Met by Most
A1c Goal = <7.0%A1c Goal = <7.5%

6% 7% 8% 6% 7% 8% 9%6%
0%
10%
20%
30%
40%
<6.0% 6.0%-<6.5%
6.5%-<7.0%
7.0%-<8.0%
8.0%-<9.0%
9.0%-<10.0%
10.0%-<11.0%
≥11.0%
HbA1c %
3-month Frequency of Severe Hypoglycemia* According to HbA1c
*Seizure or Loss of Consciousness: 1 or more events in 3 mo from subset who completed insulin and device questionnaire

Closed-Loop AdvancesInsulin pump
advocated for children
1990s 2004-2008
RT Glucose Sensors
2008
Weinzimer et. al. DCPediatric n=17
34h
2013
Phillip et. al. NEJMPediatric n=56
1 night
2014
Russell et. al. NEJMAdults + adolescents n=52
5 days
2015
Thabit et. al. NEJMAdults n=32
3 months
O’Grady, Ly et. al. DC n=8, 2 nights
2016
670G Pivotal - JAMAAdults + adolescents, n=124
3 months
2017
First commercial CL system- Released July 2017
Ly, Buckingham et. al. DCn=21, 6 days
Steil, DCN=10,
30 hours

Dr. Arnold KadishAm J Med Electronics 3:82-86, 1964
• 1964
• Measured Venous blood every 15 seconds with 7 min lag time
• Delivered insulin at 0.1 U/min if >150 mg/dl (8.3 mmol/L)
• Delivered glucagon at 0.05 mg/min if < 50 mg/dl (2.8 mmol/L)

Medtronic Inpatient Studies - 2009
• 0.025 unit basal increments
• 0.025 bolus increments
• 1 unit in 30 sec

2013 - 2014

Medtronic 670G – 2014

JDRF Modular Closed-Loop Control 2008

DiAs (UVA) System - 2014

Type Zero
InControl

International Diabetes Closed-Loop Trial
(iDCL)
• 7 centers
• 3 month study
• Ages 14-75
• 140 subjects
• Followed by 3 month study with Algorithm on Tandem
Pump
• 84 subjects

FlorenceD2A closed-loop system
Children and adolescents
Nexus 4 LG smartphone
Nav 2 CGM receiver and translator
DANA-R pump
DANA-R pump
Dell Latitude tablet
Thabit, Tauschmann, Hovorka et. al. on behalf of APCam consortium and AP@home consortium, NEJM Sep 2015
Adults

Automated Closed-Loop System for Hovorka Studies

Multicenter Closed-loop Hovorka Study
• 7 centers
• 130 subjects
• 6 to 18 years old
• 1 Year day and night
• At home
• No remote monitoring

Bionic Pancreas - 2014

Outpatient bionic pancreas
Russell SJ et al. N Engl J Med 2014;371(4):313–25.
157(8.7)
138(7.7)
154
138
157(8.7)
138(7.7)
154
138
Mean glucose levels in adolescentsMean glucose levels in adults

The iLet -2015

The iLet

Gen 4 iLet – 201757% smaller than Gen 3

Beta Bionics Planned Studies
• Insulin-Only – Bridging Study Late 2017, Early 2018
• Bihormonal Bridging Study – Early 2018

Bigfoot Biomedical

Bigfoot Clinical Studies
• Tested for 36 hours in research center
• Tested for extremes
– Missed meal bolus
– Meal overbolus
– Exercise
• Will use Abbott “Libre” Real Time Sensor
• Additional Clinical Trials Planned soon

Insulet Commercial System

Insulet Studies
• In research center for 36 hours
– Adults
– Adolescents
– 6-12 year olds
• In AirBnB 54 hours
– Adults
– Testing Exercise, Missed Meal Bolus, High Fat Meal, and Overbolus
• Starting AirBnB 5 days
– Free range during the day
– 6-12 year olds on Sunday

Tandem

Tandem Pipeline
• Using G5
• Predictive Low Glucose Suspend
– Studies starting next month
• Once FDA approved – immediately internet downloaded to current Tandem t:slim X2
• Type Zero (UVA) algorithm on Pump
Closing the Loop
• Meters
• Sensors
• Pumps
• Algorithm

Dexcom G4P Sensor PerformanceLy, Diabetes Care 37:2310-2316,2014
• Inpatient Studies (YSI) = Day 1 of sensor wear
– n=201
– Mean ARD 10.4 ± 9.1%
• Camp Studies (Contour Next)
– n=740
– Mean ARD 17.5%

What happens in reality
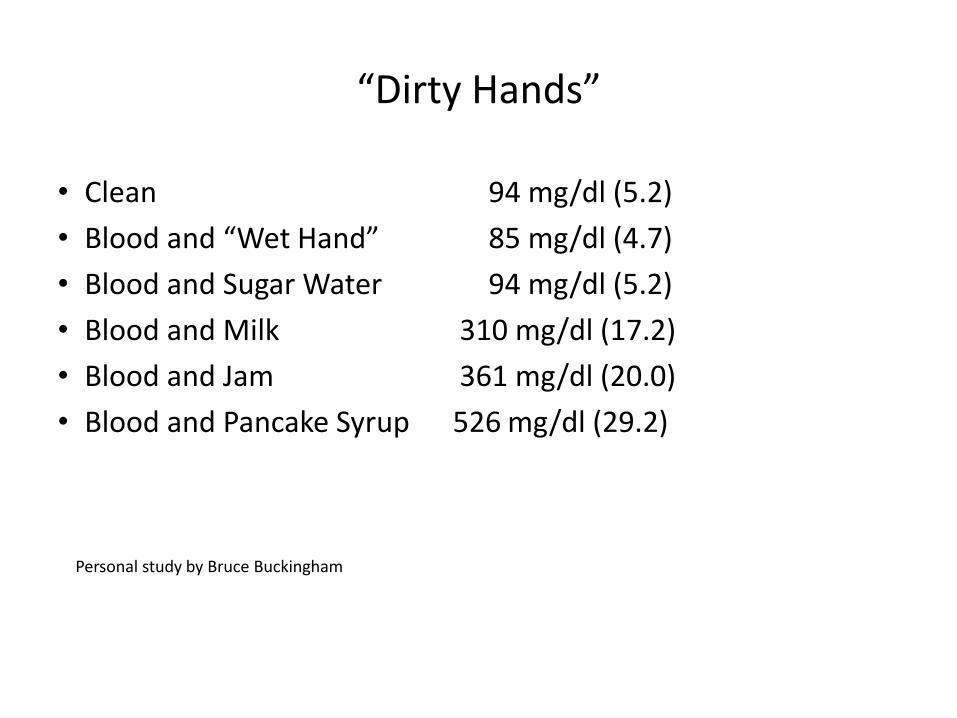
“Dirty Hands”
• Clean 94 mg/dl (5.2)
• Blood and “Wet Hand” 85 mg/dl (4.7)
• Blood and Sugar Water 94 mg/dl (5.2)
• Blood and Milk 310 mg/dl (17.2)
• Blood and Jam 361 mg/dl (20.0)
• Blood and Pancake Syrup 526 mg/dl (29.2)
Personal study by Bruce Buckingham

Effect of Handling Fruit on Meter BG
First Drop Second Drop
Washed Hands 153 mg/dl 157 mg/dl
Finger Exposed To Fruit, No Washing
270 mg/dl 160 mg/dl
After Washing Fruit-exposed Finger
151 mg/dl 150 mg/dl
Hortensius, (2011)

Effect of Handling Fruit on Meter BG
Hortensius, (2011)


Accuracy (MARD) of Sensors When Used in Pediatric Outpatient Studies
AccuracyInpatient Reference
Outpatient Accuracy with
Adults
Outpatient accuracy in Pediatrics
Outpatient Using secondDrop of blood
Russell – Dexcom G4
10.8%* 16.7%** 19.2%***
Ly –Dexcom G4 10.4% 17.5%†
Ly – Enlite 14.1% (first day)
19.2%††
Ly – Enlite 3 10.8% (first day)
12.6%†††
* Damiano, JDST 2014** Russell, NEJM 2014
*** Russell, Lancet 2016
† Ly, Diabetes Care 2014†† Ly, DTT 2016
††† Ly Diabetes Care 2015

Closing the Loop
• Meters
• Sensors
• Pumps
• Algorithm

Infusion Sets
• The weak link in insulin pump delivery

Integrated Sensor and Infusion Set

Summary of 353 Weeks of Testing Summary of 353 Weeks of Testing for 7 days of Infusion Set Wear
Mean Duration of Wear 5.0 ± 1.8 days
Percent Lasting 7 days 40%
Removal for unexplained hyperglycemia 26%
Removal for pain, infection or erythema 17%
Removal for other – eg. pulled out adhesive failure, unknown 20%

Nocturnal Hypoglycemia
• In DCCT, 55% of severe hypoglycemia occurred during sleep
• In children, 75% of severe hypoglycemia occurred during sleep
• Real-time CGM provides nocturnal alarms
– But 71% of alarms are not responded to
DCCT, Diabetes Care 18:1415, 1995
Davis, Diabetes Care 20:22, 1997
Buckingham, DTT 7:440, 2005

Overnight Glucose Control
• Preventing low
– Threshold suspend on low
– Predictive low glucose suspend
– Full Closed-loop at night

Duration of Nocturnal Hypoglycemia Prior to a Seizure - 16 year old
Buckingham, Diabetes Care 31:2110, 2008
Seizure2 hr 15 min

Duration of Nocturnal Hypoglycemia Prior to a Seizure - 16 year old
Buckingham, Diabetes Care 31:2110, 2008Australian patient courtesy of Fergus Cameron
4 hrs 45 min

Off Duty

Low Glucose Suspend with Exercise Induced Hypoglycemia (50 subjects)DTT (2012) 14:205
Threshold of 80 mg/dl
30 Minute Horizon

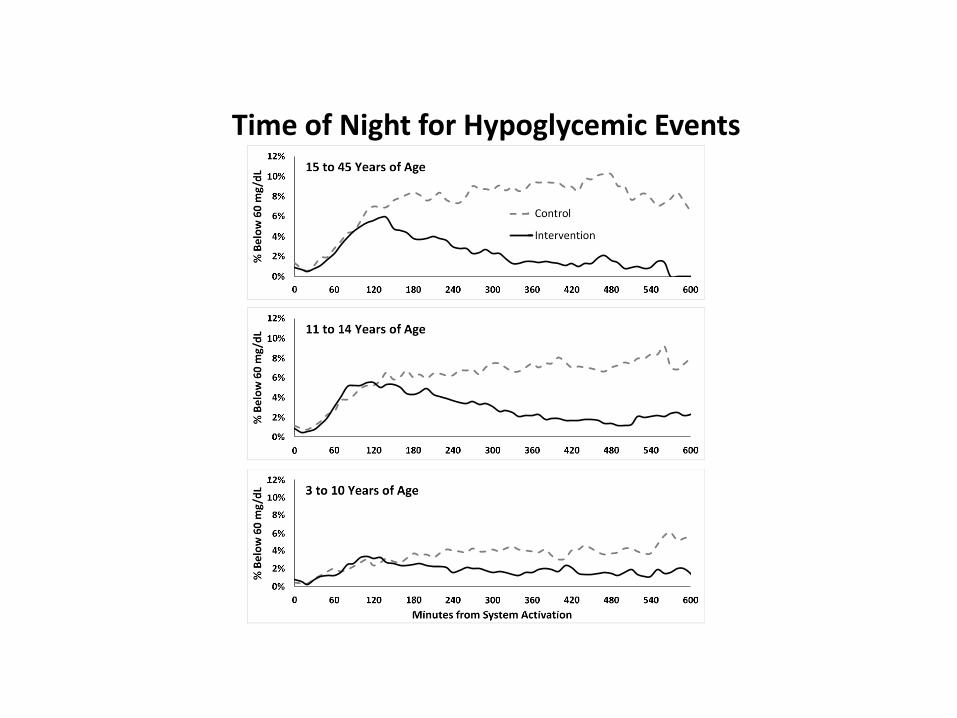
Time of Night for Hypoglycemic Events

Overnight closed-loop control
Phillip M et al. N Engl J Med 2013;368(9):824–33.
Artificial-pancreas nights Control nights

Overnight closed-loop: home studies
• 16 adolescents, 12–18 years of age
• 3 weeks of overnight closed-loop at home
• Crossed over to 3 weeks SAP
• No remote monitoring
SAP, sensor-augmented pump.Hovorka R et al. Diabetes Care 2014;37(5):1204–11.

Glucose profiles
• 33 adults
• 3 months SAP
• 3 months 24/7 hybrid-closed
• 25 children and adolescents
• 3 months SAP
• 3 months overnight closed-loop
Adults Children and adolescents
SAP, sensor-augmented pump.Thabit H et al. N Engl J Med 2015;373(22):2129–40.

Three weeks of closed-loop in adolescents
• 12 adolescents
• Initial A1c = 8.5%
• Crossover study
• Compared to21-day SAP
• Hybrid closed-loop
A1c, haemoglobin A1c; SAP, sensor-augmented pump.Tauschmann M et al. Diabetes Care 2016;39(11):2019–25.

DiAs System

Remote Monitoring


Three Day Tracing
DiAs Hotel

Camp Activities

Median ± 90%tile Envelope
Blue = Sensor Augmented PumpRed = Closed-loop
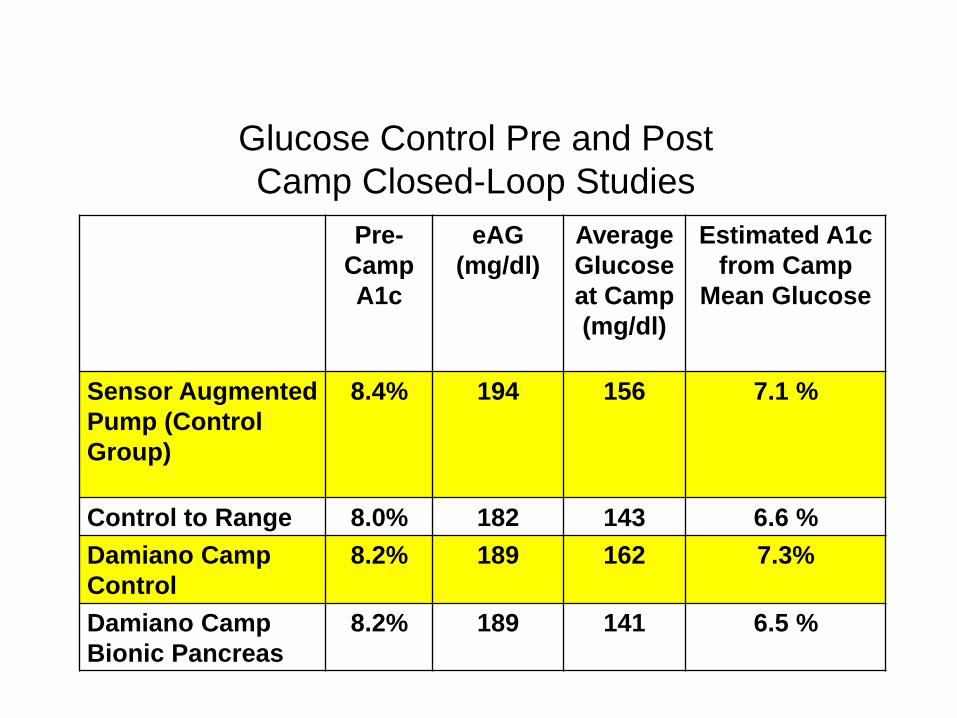
Glucose Control Pre and Post
Camp Closed-Loop Studies
Pre-CampA1c
eAG(mg/dl)
Average Glucoseat Camp(mg/dl)
Estimated A1c from Camp
Mean Glucose
Sensor Augmented Pump (Control Group)
8.4% 194 156 7.1 %
Control to Range 8.0% 182 143 6.6 %Damiano Camp Control
8.2% 189 162 7.3%
Damiano Camp Bionic Pancreas
8.2% 189 141 6.5 %

Glucose Control Pre and Post
Camp Closed-Loop Studies
Pre-CampA1c
eAG(mg/dl)
Average Glucoseat Camp(mg/dl)
Estimated A1c from
Camp Mean Glucose
Sensor Augmented Pump (Control Group)
8.4% 194 156 7.1 %
Control to Range 8.0% 182 143 6.6 %Damiano Camp Control
8.2% 189 162 7.3%
Damiano Camp Bionic Pancreas
8.2% 189 141 6.5 %

Ski camps done safely for 20 years at BDC
Early ‘90’s Dr. Chase

Ski Camp Study: UVA/BDC2017

The Present Medtronic 670G
Enlite 3 sensor

Min – Max YSI, mg/dL % In-Range, Tighter (70 – 150, mg/dL)
% In-Range (70 – 180, mg/dL)
Avg. YSI, mg/dL Sensor MARD, %
95 – 140 100 100 114.9 5.3
Admission Date: 6/29/2013 – 6/30/2013 (Subject 11RJ) CGM
YSI
Manual
Bolus
Setpoint
Fault
Infusion
Rate
Insulin
Limits
Meter BG*
Training
Err.
Corr. Bolus
Missed Tx
Start CL
Stop CL
Umin
TimeoutSafe Basal
22 23 24 25 26 27 28 29 30 31 320
40
80
120
160
200
240
280
320
Glu
cose (
mg/d
L)
Sbj #11
22 23 24 25 26 27 28 29 30 31 320
1
2
3
4
5
6
Infu
sio
n R
ate
(U
/h)
Time (h)

Open Loop Compared to Closed-Loop

Open Loop Compared to Closed-Loop

Important to Understand what it can and cannot do
• This is a basal rate modulator
• Works well overnight
• Still requires meal boluses, correction bolus, and many fingersticks
• Diabetes tasks during the day are not decreased
• There are more alarms

670G Safety Features
• If at minimal insulin deliver for 2 ½ hours,
defaults to safe basal
–To detect sensor failure
• If at >300 for 1 hour, or >250 for 2 hours,
requires glucose entry
–To detect infusion set failure
• Sensor performance is checked with impedance
spectroscopy

Enlite 3 Sensor
• Accuracy is 10.6% with two fingersticks/d
• Accuracy is 9.6% with four fingersticks/d
• Has “impedance spectroscopy” as a built in second measure of sensor function

Impedance Spectroscopy

Initialization
• Requires a minimum of 2 days of sensor and pump data to be initialized the first time it is used or not used for 2 weeks
• If pump is suspended or turned off for more than 4 hours, then aa 5 hour warm-up is required to recalculate active insulin (insulin-on-board)

Controller Adaptability and Settings
• Blood glucose target of 120
• Can temporarily change to 150 for a set duration
– For activities such as sports or driving
• The controller gain (how aggressive it is), maximum basal insulin delivery limit, insulin sensitivity factor, and “safe basal” rates are adapted daily
– Based on glucose levels overnight and total daily insulin dose

Tunable parameters
• Carbohydrate to insulin ratios
– Can have multiple ratios throughout the day
• Duration of insulin action
• Insulin Bolus Speed

Different bolus speeds
• 20 subjects, studied twice
• 15-unit bolus
– Animas pump over 30 seconds
– Minimed 512 over 10 minutes
Regittnig W et al. Diabetes 2013;62(Suppl. 1):Abstract 966-P.

Different bolus speeds
Animas15 units over 30 sec
Medtronic 512 15 units over 10 min
Onset of insulin action 21 ± 2.5 min 34.3 ± 2.7 min
Time to peak effect 98 ± 11 min 125 ± 16 min
Insulin AUC from 0 to 60 min
10307 ± 1291 8192 ± 865
AUC, area under the curve.Regittnig W et al. Diabetes 2013; 62(Suppl. 1):A247.
Fixed parameters
• Correction factor
– Based on total daily dose divided into 1800
– Requires a fingerstick glucose value
– Automatically corrects to a target of 150 mg/dl if glucose is >150 mg/dl

Daily Use
• Need to take a fingerstick glucose before each meal
• Recommended to wait at least 10 minutes after taking bolus before eating
• Need to respond to alarms to keep in Closed-loop

670G Study Subject Download
Average glucose = 153 (eA1c = 7.5%), 1% of readings < 70 mg/dl

Adolescent male, 78 kg
Carbohydrates vary from 160 to 971 grams a day
Insulin varies from 73 to 267 units a dayMean Glucose = 124 ± 52 mg/dl

Day of 971 grams of CHO

670G Pivotal Study
CharacteristicAdolescents
age ≤21
(N=30)
Adults age >21(N=94)
Age – yr 16.5± 2.29 44.6 ± 12.79
Diabetes Duration - years 7.7 ± 4.15 26.4 ±12.43
Total daily insulin dose – U/kg/day 0.8 ±0.24 0.6 ±0.20
HbA1c % at screening 7.7 ±0.84 7.3 ±0.91

All Patients in 670G Pivotal Study
A
B
C

Adults in 670G Pivotal
A
B
C
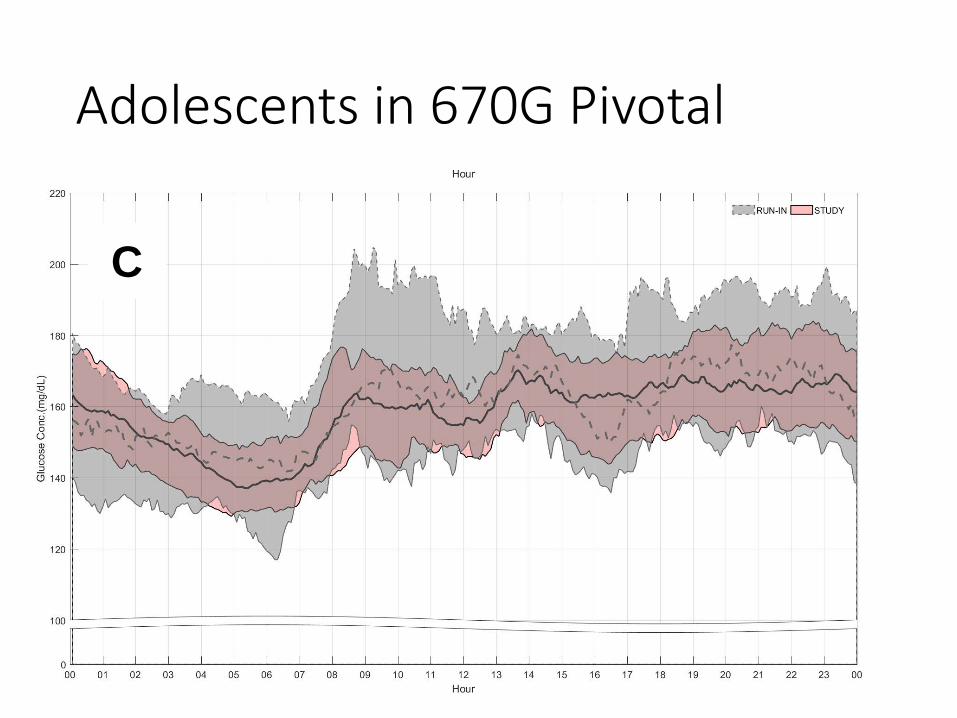
Adolescents in 670G Pivotal
A
B
C
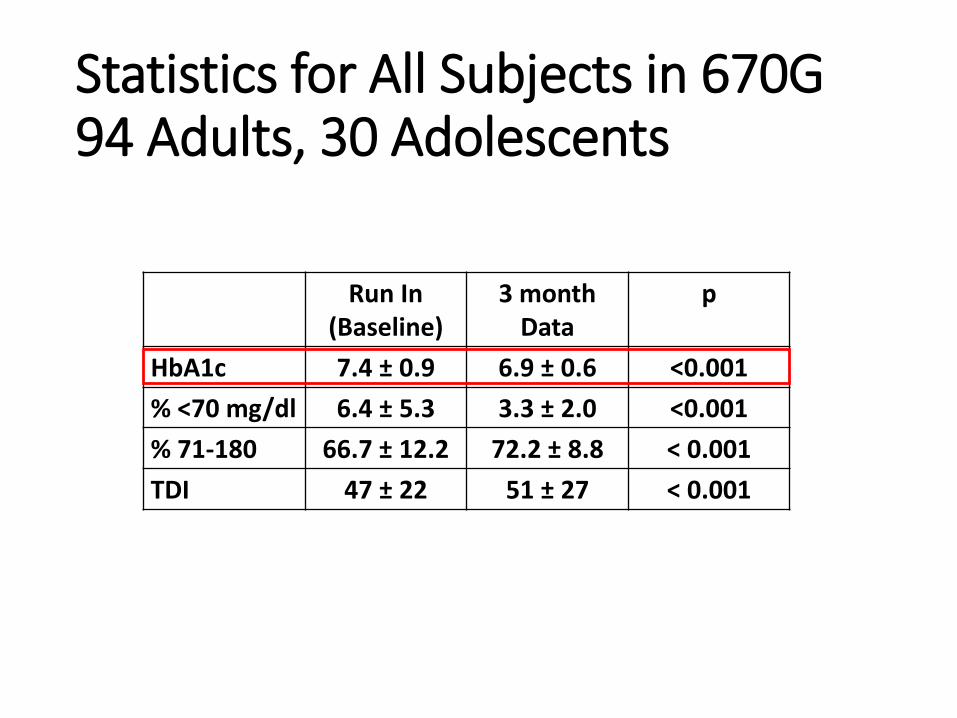
Statistics for All Subjects in 670G94 Adults, 30 Adolescents
Run In (Baseline)
3 month Data
p
HbA1c 7.4 ± 0.9 6.9 ± 0.6 <0.001
% <70 mg/dl 6.4 ± 5.3 3.3 ± 2.0 <0.001
% 71-180 66.7 ± 12.2 72.2 ± 8.8 < 0.001
TDI 47 ± 22 51 ± 27 < 0.001

Statistics for All Subjects in 670G94 Adults, 30 Adolescents
Run In (Baseline)
3 month Data
p
HbA1c 7.4 ± 0.9 6.9 ± 0.6 <0.001
% <70 mg/dl 6.4 ± 5.3 3.3 ± 2.0 <0.001
% 71-180 66.7 ± 12.2 72.2 ± 8.8 < 0.001
TDI 47 ± 22 51 ± 27 < 0.001

Statistics for All Subjects in 670G94 Adults, 30 Adolescents
Run In (Baseline)
3 month Data
p
HbA1c 7.4 ± 0.9 6.9 ± 0.6 <0.001
% <70 mg/dl 6.4 ± 5.3 3.3 ± 2.0 <0.001
% 71-180 66.7 ± 12.2 72.2 ± 8.8 < 0.001
TDI 47 ± 22 51 ± 27 < 0.001


Low
Minimal insulin delivery
Alert on High


Does A1c determine who is a good candidate? Does A1c determine who is a good candidate?

670G
• Greatly improves overnight control
• Start the day with a good glucose
• Improved sensor - MARD 10.3%
• Need to optimize meal coverage -insulin:carbohydrate ratio
• Understand the causes of auto-mode exit, and do a little work to stay in closed loop
– Calibrate at least every 12 hours
– Bolus before eating

6% 7% 8% 6% 7% 8% 9%6%
0%
10%
20%
30%
40%
HbA1c %
3-month Frequency of Severe Hypoglycemia* According to HbA1c
*Seizure or Loss of Consciousness: 1 or more events in 3 mo from subset who completed insulin and device questionnaire

670G and Severe Hypoglycemia
• 65,000 days and nights of 670G wear• This represents 178 patient years• From T1D Exchange data there should have been at
least 12 severe hypoglycemic events with seizure or loss of consciousness
• Actual number of severe hypoglycemic events = 0• CDC estimates there are 300,000 ER visits in adults
each year for hypoglycemia–Average cost per visit is about $1,161 (Foos, J Med Econ, 2015)
• The 670G allows for a good, safe nights sleep, without the risk of a severe, costly hypoglycemic event

Insurance Coverage for the 670G
• COVERED
• Aetna
• Cigna
• Humana
• United Health Care
• Sutter Health
• Valley Health Plan
• Tricare West
• Blue Shield of California
• Health Net California
• California Children’s Services (County and Individual Specific) (1 yes)
• Not covered with Anthem Blue Cross Blue Shield
• NOT COVERED
• Anthem Blue Cross Blue Shield
• California Children’s Services (County and Individual specific) (7 no)

Aemployee, 670
B 3/26/2017 - 4/8/2017 (14 Days)4/9/2017 - 4/22/2017 (14 Days)
Generated: 5/25/2017 12:46:38 PM Data Sources: MiniMed 670G (NG1229760H)
Page 2 of 8Assessment and Progress
77
* Most recent pump settings are displayed
B 9
Hypoglycemic patterns(3)
779Carb Ratio A
1 2 3
A
(g/U) *
Hyperglycemic patterns(0)
Auto Mode Exits Statistics
6.4%Estimated A1C 6.4%137 ± 39 mg/dLAverage SG ± SD 137 ± 34 mg/dL
98% (6d 20hrs)92% (6d 10hrs)Sensor Wear (per week)
17% (1d 05hrs)8% (13hrs)Manual Mode (per week)
83% (5d 19hrs)92% (6d 11hrs)Auto Mode (per week)
10.9 / 3.4
Average BG 145 ± 43 mg/dL
BG / Calibration (per day) 11.6 / 3.5
Total daily dose (per day) 46 units
Bolus amount (per day) 23U (50%)
147 ± 48 mg/dL
4
Set Change 4
Reservoir Change 4
Meal (per day) 7.6
Carbs entered (per day) 154 ± 39g
Active Insulin time 3:00 hrs
4
21U (51%)Auto Basal / Basal amount (per day) 23U (50%)20U (49%)
41 units
123 ± 46g
6.9
3:00 hrs
B BA A
0• • 2Sensor Algorithm
Underread
00BG required for Auto
Mode
00Auto Mode min
delivery
00Auto Mode max
delivery
2 • •0High SG Auto Mode
Exit
00No Calibration
00Unidentified
00Large time/date
change
00Pump Suspend by
user
00Alarms
0• • 2Auto Mode disabled by
user
No SG values 0
Sensor Expired 0 1 •
0
0Sensor Updating 0
1%10%
2%11%
10:42 PM- 11:17 PM
(1 occurrences)
8:48 PM- 9:13 PM
(1 occurrences)
6:46 PM- 7:41 PM
(2 occurrences)
88%
1%
85%
2%
Average A25-75% 0-90%T
ime
inra
ng
e
180 250 400 mg/dL
Percentile comparison
A B
705040
None
Sensor Updating 0

Current State of Type 1 Diabetes
Updated T1D Exchange - 2015K. Miller , Diabetes Care 38: 971
6.5
Bihormonal Closed-Loop
Insulin-only Closed-Loop

What Do Participants Think?
• Great to wake up with a good glucose and no lows
overnight
• Sensors are much better
• Feel liberated from food constraints
• Not perfect during the day
• When can I get one of these?

670G Pivotal Study
• Our daughter “went XC skiing on Sunday noon-3pm. I think she did really well at staying in closed loop. Usually her BG would have been all over the place. We love this system!”
• “I know that I will be able to get a good night's sleep knowing that the pump is taking care of things. If she's high, it will bring her back in range, and if she's low, it will make sure she comes up to a safe range. And all the while both of us will be sleeping soundly in our own beds, with no alarms to disturb us. I've seen the future of diabetes management and it is bright!”

The Future
• Hybrid Closed-Loop During the Day and Full Closed-loop
Overnight
– Premeal bolus
– Remove carbohydrate counting

New Insulin Preparations and
Adjunctive Therapy to Improve Post
Prandial Control
• Fast Aspart
• Biochaperone Lispro
• Afrezza
• GlP-1 agonists to delay gastric emptying and lower
postprandial glucagon

The Future
• Algorithms will continue to improve
• Adapting to individuals
– Modifying set points
– Modifying overnight basal
– Modifying meal responses
• Adapting over time
– Short term for acute changes
– Long term for weekly and monthly patterns

The Future
• Use of Accelerometers and Heart Rate Monitors
– Detect and adjust automatically for activity
– Allows detection of sleep to modify algorithm
• Integration into Consumer Devices
– Apple/Apple Watch
– Google Android

The Future
• Improved infusion sets
– Longer duration of wear
– Combined with sensors
• Improved Sensors
– MARD less than 10%
– Duration of wear 2 weeks
– Factory Calibration

The Future
• Full Closed-Loop
• No CHO counting, no premeal bolus
• Less than perfect, but may be good enough












![Closed loop Urbanism [Autosaved]](https://img.dokumen.tips/doc/110x75/58edac181a28aba90c8b4605/closed-loop-urbanism-autosaved.jpg)



















