-
8/13/2019 Human Sigmoid Colon
1/12
Effect of otilonium bromide on contractile patterns in the
human sigmoid colon
D. GALLEGO,* M. AULI,, J. ALEU, E. MARTINEZ ,, L. ROFES,* J.
MARTI-RAGUE, M. JIMENEZ *, & P. CLAVE*,,
*Centro de Investigacion Biomedica en Red de Enfermedades
Hepaticas y Digestivas (Ciberehd), Instituto de Salud Carlos
III,
Barcelona, Spain
Department of Surgery, Hospital de Mataro, Mataro, Spain
Fundacio de Gastroenterologia Dr. F. Vilardell, Barcelona,
Spain
Department of Cell Biology, Physiology and Immunology,
Universitat Autonoma de Barcelona, Barcelona, Spain
Abstract
BackgroundThe mechanism of action of the spas-molytic compound
otilonium bromide (OB) on human
colonic motility is not understood. The aim of our
study was to characterize the pharmacological effects
of OB on contractile patterns in the human sigmoid
colon. Methods Circular sigmoid strips were studied
in organ baths. Isolated smooth muscle cells from
human sigmoid colon were examined using the cal-
cium imaging technique. Key Results Otilonium bro-
mide inhibited by 85% spontaneous non-neural
rhythmic phasic contractions (RPCs), (IC50 = 49.9 n-
mol L)1) and stretch-induced tone (IC50 = 10.7 n-
mol L)1) with maximum effects at micromolar range.
OB also inhibited by 50% both on- (IC50 = 38.0 n-
mol L)1) and off-contractions induced by electrical
stimulation of excitatory motor neurons. In contrast,
the inhibitory latency period prior to off-contractions
was unaffected by OB. OB inhibited acetylcholine-,
substance P-, and neurokinin A-induced contractions.
The L-type Ca2+ channel agonist BayK8644 reversed
the effects of OB on RPCs, on- and off-contractions.
Hexamethonium, atropine, the NK2 antagonist, or
depletion of intracellular Ca2+ stores by thapsigargin
did not prevent the inhibitory effect of OB on RPCs
and electrical contractions. KCl-induced calcium
transients in isolated smooth muscle cells were also
inhibited by OB (IC50= 0.2 lmol L)1
).Conclusions &Inferences Otilonium bromide strongly
inhibited the
main patterns of human sigmoid motility in vitro by
blocking calcium influx through L-type calcium
channels on smooth muscle cells. This pharmacolog-
ical profile may mediate the clinically observed effects
of the drug in patients with irritable bowel syndrome.
Keywordsgastrointestinal motility, sigmoid colon,
smooth muscle, spasmolytic drugs.
INTRODUCTION
Irritable bowel syndrome (IBS) is a chronic
functionalgastrointestinal disorder affecting up to 11.5% of
the
general population1 and is characterized by abdominal
pain or discomfort associated with a change in bowel
habit. Altered motility in the small bowel and colon
may contribute to a change in bowel behavior, and a
combination of increased motility and spasm, visceral
hypersensitivity, and abnormalities in central pain
processing may explain the origin of the abdominal
pain.2 Recent in vivo studies showed that pain hyper-
sensitivity and colon hypermotility including
increased phasic motility and enhanced smooth mus-
cle tone are independent factors contributing to
symptoms in patients with IBS.3 Antispasmodics and
muscle relaxants are widely used as first-line treat-
ment in these patients. However, the biological ratio-
nale for the efficacy of antispasmodics is unclear, and
their pharmacological effects may vary among com-
pounds. Recent studies found that antispasmodics may
act by reducing colonic contraction and increasing
transit time and therefore reducing pain and stool
frequency in patients with IBS.2 Among antispasmo-
dics, otilonium bromide (OB), a quaternary ammonium
Address for correspondence
Pere Clave, MD, PhD, Associate Professor of Surgery,Department
of Surgery, Hospital de Mataro, UniversitatAutonoma de Barcelona,
C/Cirera s/n. 08304, Mataro, Spain.Tel: +34 93 741 77 00; fax: +34
93 741 77 33;e-mail: [email protected] study was presented in
part at the 21st InternationalSymposium on Neurogastroenterology
and Motility, Jeju,Korea, August 2007.Received: 15 October 2009
Accepted for publication:22 February 2010
Neurogastroenterol Motil (2010) 22, e180e191 doi:
10.1111/j.1365-2982.2010.01495.x
2010 Blackwell Publishing Ltde180
-
8/13/2019 Human Sigmoid Colon
2/12
derivative compound, has shown consistent evidence
of efficacy on IBS patients.2,4,5 Clinically, the main
effects of OB include a global improvement of IBS
symptoms, a reduction in the frequency and severity of
abdominal pain, and an increase in the distension pain
threshold with the use of a sigmoid balloon.69
How-ever, the effects and the mechanism of action of OB on
human colonic motility are not fully understood, and
the few studies that have investigated the mechanisms
of action of OB in animal models described a hetero-
geneous pharmacological profile.5,10
Most studies on the pharmacodynamics of OB have
been conducted on rodents and suggest several mecha-
nisms of inhibition of OB on spontaneous and stimu-
lated intestinal motility. Animal studies found that OB
inhibited contractions induced by acetylcholine (ACh),
serotonin, substance P (SP), histamine, barium chloride
(BaCl2) a n d K+ and described how OB exerted its
spasmolytic action by a combination of antagonistic
actions at muscarinic receptors, by blocking L-type Ca
channels, by antagonizing tachykinin NK1 and NK2receptors and by
blocking nicotinic-mediated
responses;5,1012 however this has not been fully char-
acterized in humans. We haverecently characterized the
different types of contractions in human sigmoid colon
in vitro. Circular strips of human sigmoid colonin vitro
developed spontaneous rhythmic phasic contractions
(RPCs) of non-neural origin and responded to electrical
stimulation (EFS) of enteric motor neurons (EMNs) with
twodistinctpatterns of strongcontractile responses: (i)a
phasiccontractionduring EFS on-contractions or (b)aphasic
contraction after EFS off-contraction caused
by stimulation of excitatory EMNs following a period of
latency caused by stimulation of inhibitory EMNs
releasingNOandATPactingatP2Y1 receptors.13Ampli-
tude of electrical-induced contractions depended on
stimulation of excitatory EMNs releasing ACh and
tachykinins acting on muscarinic and NK2 receptors
located on smooth muscle cells.13
The aim of this study was to assess the pharmaco-
dynamics and effects of the spasmolytic agent OB on
the main types of in vitro contractions in human
sigmoid colon and to pharmacologically characterize
OBs mechanism of action.
METHODS
Tissue specimens
Tissue specimens of human sigmoid colon were obtained from
70
patients without symptoms of major clinical motility
disorders
who underwent surgery for rectal cancer (T2/T3 stages, age
range3285 years, 44% women). All strips were obtained from
macro-
scopically non-invaded regions. The experimental protocols
were
approved by the Institutional Review Board of the Hospital
de
Mataro, Barcelona, Spain.
Preparation of circular muscle strips andisometric tension
recording
The colonic segment was cut open longitudinally along the
mesenteric border, the mucosal layer was removed and trans-
mural muscle strips (3 mm wide by 10 mm long) were cut inthe
direction of the circular muscular fibers. Weight of the
strips was 0.21 0.01 g, N = 31. A silk thread was attached
to
either end of the strips and they were placed in 10 mL organ
baths filled with Krebs solution (37 C, bubbled with a mixtureof
5% CO2/95% O2, pH 7.4) as described in previous stud-
ies.13,14 Strips were positioned between two parallel
platinum
wire electrodes 10 mm apart and changes in tension weremeasured
using isometric force transducers, recorded on a chart
recorder (model 03 Force Transducer and model 7 Series
Polygraph; Grass Instruments Co, Quincy, MA, USA) anddigitized
(Acqknowledge, MP100; Biopac Systems, Inc, Goleta,
CA, USA). In each experiment, up to six strips from the same
specimen were simultaneously studied. Strips were
initiallystretched to 4 g of force and equilibrated for 1 h and
then the
following patterns of colonic motility were assessed.
Spontaneous RPCs After the equilibration period, strips
devel-
oped spontaneous RPCs. Origin of RPCs was characterized by
the ganglionic blocker hexamethonium 100 lmol L)1, the neu-ral
blocker tetrodotoxin (TTX) 1 lmol L)1 that interrupts Na+
action potentials along the axon of EMNs, withdrawal
ofextracellular Ca2+ from the medium (by using a Ca2+-free
Krebs solution with EGTA 1 mmol L)1), and depletion of
intracellular Ca2+ stores by 20-min incubation with
thapsigargin
10 lmol L)1, a blocker of sarco/endoplasmic reticulum Ca2+
ATPase.15
Stretch-induced responses After the period of
equilibration,stretch was applied to strips from 0 to 7 g in steps
of 1 g each
30 min. Baseline tone and amplitude of RPCs was measuredduring
the last 10 min of each stretch. To avoid neural mediated
responses, this study was performed in the presence of the
neuralblocker TTX (1 lmol L)1).
Contractions induced by EFS of EMNsElectrical stimulation
was
applied by an electrical stimulator (Model S88; Grass
Instru-
ments Co) and a power booster (Stimu-Splitter II; Med-Lab
Instruments, Loveland, CO, USA).13 Ten-second trains of pulsesof
0.4 ms duration at 140 Hz and 26 V were delivered to the
electrodes and simultaneously recorded on tension tracings
through a synchronized TransistorTransistor logic signal
be-tween the electrical stimulator Grass S88 and the
computerized
Biopac System. In a previous study, we found sigmoid
stripsresponded to EFS with two distinct patterns of contractile
re-sponses of neural origin (a) a phasic contraction which
began
during EFS on-contractions or (b) a phasic contraction which
began after EFS off-contractions.13 In the present study,
theseEFS responses were further characterized by hexamethonium
100 lmol L)1, and depletion of extracellular and
intracellular
Ca2+ stores.
Direct contractions induced by excitatory neurotransmittersIn
a
previous study, we found that sigmoid contractions induced
bystimulation of excitatory EMNs were mediated by released ACh
and tachykinins mainly acting on muscarinic and NK2
receptors
Volume 22, Number 6, June 2010 Otilonium bromide inhibits human
sigmoid motility
2010 Blackwell Publishing Ltd e181
-
8/13/2019 Human Sigmoid Colon
3/12
located on smooth muscle cells.13 In this study, we assessed
the
direct effect of ACh (0.01100 lmol L)1), SP (0.00110 lmol
L)1),and neurokinin A (NKA) (1 nmol L)1 to 1 mmol L)1) on
sigmoid
strips.
Calcium image technique
Smooth muscle cells were isolated by a mechanical and enzy-
matic process. Briefly, the circular muscular layer was
dissected
and cut into small pieces (12 mm). The muscle pieces were
placed in Ca2+-free Hanks solution (NaCl 115 mmol L)1, KCl5.4
mmol L)1, MgCl26H2O 0.5 mmol L
)1, NaHCO34.2 mmol L)1,
Na2HPO4 0.3 mmol L)1, KH2PO4 0.4 mmol L
)1, MgSO47H2O
0.4 mmol L)1, glucose 5 mmol L)1). They were incubated with1.5
mg mL)1 papain (Sigma, St Louis, MO, USA), 1 mg mL)1
bovine serum albumin (BSA) and 2 mg mL)1 soy bean trypsin
inhibitor (SBTI) for 3 min at 32 C and stirred at 108 g.16,17
Aftercentrifugation, the muscle pieces were incubated in 1 mg
mL)1
BSA, 0.75 mg mL)1 collagenase type II (Worthington,
Lakewood,
NJ, USA) at 32 C and stirred again at 27 g until isolated
cellsappeared. Isolated smooth muscle cells were placed in a
recording
medium (NaCl 145 mmol L)1, KCl 4.8 mmol L)1, MgCl26H2O 1
mmol L)1, CaCl2 1.8 mmol L)1, glucose 10 mmol L)1, HEPES
10 mmol L)1, pH 7.4). Fluo-4/AM (Teflabs, Inc., Austin, TX,
USA)was used to monitor changes in the calcium level in cytosol.
Fluo-
4 (50 lg) was dissolved in DMSO (25 lL) and 2 lL of this
stock
solution was added to each culture plate in 1 mL recording
medium for 45 min. After washing out the remaining dye,
cellswere incubated in the recording medium. The cells were
imaged
with IX-FLA equipment (Olympus Biosystems, Heidelberg,
Germany) connected to an Olympus IX70 microscope with an20 lens.
The cells were scanned using CellR software (Olympus
Biosystems). Cells were exposed briefly (5 s) to high
potassium
solution (75 mmol L)1 KCl) causing a sudden increase in
transient
intracellular calcium [Ca2 + ]i in the smooth muscle
cells(control), and the effect of 10 min incubation of
cumulative
concentrations of OB (10 nmol L)1 to 100 lmol L)1) was
assessed.
Experimental design
We assessed the effect of OB (10 pmol L)1 to 100 lmol L)1) on
the
main human sigmoid motility patterns: (i) spontaneous RPCs;
(ii)
stretch-induced tone; (iii) contractions induced by EFS of
EMNs
EFS on and off contractions ; (iv) direct contractions inducedby
ACh, SP and NKA, and (v) calcium transients induced by KCl
in isolated muscle cells. We compared the effects of OB with
those
caused with the specific L-type channel antagonist nifedipine(10
pmol L)1 to 10 lmol L)1), atropine (1 pmol L)1 to 1 lmol L)1),
and the NK2 receptor antagonist GR 94800 (1 pmol L)1 to
1 lmol L)1). We also characterized the mechanism of action ofOB
by pharmacological studies using the specific L-type channel
agonist BayK8644 (1 nmol L)1 to 10 lmol L)1), and by
assessing
the effect of OB on RPCs and EFS contractions following
blockadeof nAChRs by hexamethonium 100 lmol L)1, blockade of
mus-
carinic receptors by atropine 1 lmol L)1, blockade of NK2
recep-
tors by the NK2 receptor antagonist GR 94800 (1 lmol L)1)
and
following depletion of intracellular calcium stores by
thapsigargin10 lmol L)1.
Drugs
Otilonium bromide was obtained from Laboratorios Menarini
SA,
(Badalona, Spain). Acetylcholine chloride (ACh), SP,
BayK8644,nifedipine, hexamethonium, BSA, SBTI from Sigma; TTX,
atropine sulphate, from Research Biochemicals International
(Natick, MA, USA); NKA, thapsigargin, NK2 receptor antagonistGR
94800 from Tocris, (Bristol, UK); Fluo-4 AM from Teflabs Inc.
Thapsigargin, n-butyl-hyoscine 20 mg per 1 mL from
BoehringerIngelhemim Espana SA, (Barcelona, Spain). Stock solutions
were
made by dissolving drugs in distilled water except for
thapsigargin
and Fluo-4 AM which were dissolved in DMSO (0.01%) and
BayK8644 which was dissolved in ethanol (0.01%).
Data analysis and statistical procedures
Spontaneous RPCs were measured as the area under the curve
(AUC), in g min)1 and paired Students t-test was used to
assess
the effect of antagonists and agonists on the proposed
putativeneurotransmitters. The effect of antagonists on RPCs
was
assessed following 20 min incubation, the last 10-min period
being analyzed. Data were normalized with respect to a
controlperiod (10 min before addition of the antagonist) and
concen-
tration response curves analyzed by two-way repeated
measureANOVA analysis. The effect of agonists was measured as
theAUC of the 2-min period following their addition to the
bath.
The concentrationresponse curve for each agonist was com-
puter fitted using nonlinear regression, and the IC50 was
calculated (GRAPHPAD PRISM, version 4.01; GraphPad Prism
Soft-ware, San Diego, CA, USA). Latency of EFS contractions was
defined as the period of time from the beginning of EFS to
the
onset of contraction; and maximal amplitude of EFS contrac-
tions (in g) was also measured. The effect of OB and the
otherdrugs on latency and amplitude of on- and off-contractions
was
analyzed by two-way ANOVA for repeated measures. When the
two-way ANOVA was significant, the Bonferroni test was
carriedout to determine the frequencies or doses of
statistically
different responses. Data are expressed as mean SEM. Changes
in the Fluo4 fluorescence were recorded for 30 s at 2.5 Hz
with a spatial resolution of 512 480 pixels. At the end ofthe
experiments, the images were analyzed over time by
CellR software (Olympus Optical Co., Ltd, Tokyo, Japan)
using
regions of interest (ROIs). Fluorescence intensity was
normal-ized to the basal fluorescence at the onset of the recording
for
each ROI, and peaks were analyzed as previously described.
Paired Students t-test or ANOVA test was used before and
afterdrug addition. A P < 0.05 was considered statistically
signifi-
cant. N values indicate the number of samples from different
patients.
RESULTS
Effects of OB on spontaneous RPCs
Human circular sigmoid strips developed spontaneous
RPCs after 1 h equilibration. The AUC, amplitude, and
frequency of RPCs were 72.85 10.87 g min)
1, 3.53 0.52 g, and 2.48 0.24 contractions min)1 (N= 20)
respectively. The activity of RPCs(AUC) was unaffected
by 30-min exposure to the neural blocker TTX
1 lmol L)1 (+6.16 1.5%. ns, N = 11) or hexametho-
nium (100 lmol L)1) ()3.1 23.57%, ns,N= 5). Block-
ade of muscarinic receptors by atropine (1 pmol L)1 to
1 lmol L)1) or hyoscine (4.5 pmol L)1 to 4.5 lmol L)1)
and blockade of NK2 receptors by the NK2 receptor
antagonist GR 94800 (1 pmol L)11 lmol L)1) caused a
D. Gallegoet al. Neurogastroenterology and Motility
2010 Blackwell Publishing Ltde182
-
8/13/2019 Human Sigmoid Colon
4/12
significant reduction of RPCs, an effect dependent on
theirconcentration,the design of the experiment (cumu-
lative vs single concentrations)and the timeof exposure,
but did not block them (Fig. 1). All these results suggest
that RPCs have a non-neural originbut aremodulated by
EMNs. RPCs were greatly reduced ()
62.54 18.89%,P < 0.01;N= 6), following 30 s removal of
extracellular
calcium and in contrast were only slightly reduced by
depletion of intracellular calcium stores by 30-min
incubation with thapsigargin 10 lmol L)1 ()26.47
16.76%, ns; N= 5) indicating the importance of extra-
cellular calcium in the origin of this pattern of contrac-
tions. RPCs were almost abolished by OB ()84.17
16.87% at 100 lmol L)1) in a concentration-dependent
manner (IC50of 49.9 nmol L)1,N= 8). RPCs were also
abolished ()96 1.75% at 10 lmol L)1) by the L-type
calcium channel blocker, nifedipine, with an IC50 of
1.00 nmol L)1 (N= 7) (Fig. 1, Table 1).
The specific L-type channel agonist, BayK8644
(1 nmol L)1 to 10 lmol L)1), increased the amplitude
of RPCs in a concentration-dependent manner
(1 nmol L)1 to 1 lmol L)1, EC50= 0.07 lmol L)1); and
at10 lmol L)1 this excitatory effect was reduced (N= 3)
(Fig. 2). BayK concentration dependently reversed the
inhibitory effects of nifedipine and OB (10 lmol L)1) on
RPCs (Fig. 2). In addition, OB 100 lmol L)1 strongly
inhibited RPCs following blockade of muscarinic recep-
tors by atropine 1 lmol L)1 ()64.12% 11.62, P < 0.05,
N= 5), blockade of NK2receptors by the antagonist GR
94800 ()70.49 10.32%, P < 0.0001, N= 7), depletion
of intracellular calcium by thapsigargin 10 lmol L)1
()75.16 7.12%P < 0.05,N= 5), and blockade of nico-
tinic receptors by hexamethonium 100 lmol L)1
()86.49 9.23%P < 0.05,N= 4) (Fig. 3).
Effect of OB on stretch-induced contractions
Stretch of strips did not modify the frequency of sponta-
neous RPCs. On the contrary, basal tone of strips and
amplitude of RPCs were progressively increased by
stretch (N= 15, ANOVAP < 0.001). OB was tested at six
differentconcentrations from1 nmol L)1 to 1 lmol L)1,
N = 5. Amplitude of stretch-induced contractions was
decreasedby OB, significant differences wereobservedat
the concentration of 1 lmol L)1 ()64.21%). (From
36.08 7.5% in control conditions to 12.9 8.1 after
incubationwithOB1 lmol L)1,at7 gofinducedstretch,
N= 5 P < 0.001.) Stretch-induced tone was also reduced
by OB, with significant differences observed at 0.1
lmol L)1 ()52.76%) and 1 lmol L)1 ()55.37%; Fig. 4).
(From3.07 0.23 gincontrolconditionsto1.45 0.18 g
with OB 0.1 lmol L)1,N= 5 and to 1.37 0.29 g with
OB 1 lmol L)1, N= 5, P < 0.001 each.)
Effect of OB on sigmoid contractions induced byelectrical
stimulation of EMNs
In a recent study, we found EFS produced two distinct
patterns of contractile responses in the human sigmoid
colon: (i) contractions which began during EFS, definedas
on-contractions caused by selective stimulation of
excitatory EMNs and (ii) contractions which began after
EFS, defined asoff-contractions also caused by stimula-
tion of excitatory EMNs following a period of latency
caused by stimulation of inhibitory EMNs.13 In the
present study, OB induced a significant concentration-
dependent inhibition in the amplitude of EFS-induced
on-contractions (IC50= 0.38 nmol L)1, )49.39
13.75% at 40 HzP < 0.05,N= 6) (Table 1). Incubation
with the L-type calcium channel blocker nifedipine
abolished on-contractions (IC50= 0.13 nmol L)1,
)96.28 3.71% at 40 Hz P < 0.05, N= 6, Fig. 5). EFS
on-contractions were fully abolished following incuba-
tion with free calcium Krebs solution for 30 s (N= 6),
and were reduced by atropine (1 lmol L)1, 40 Hz,
)69.58 3.49%, N= 9, P < 0.001), n-butyl-hyoscine
100 lmol L)1 40 Hz, )49.81 8.49%,N= 6,P < 0.05),
GR94800 (1 lmol L)1) (40 Hz: )26.07 6.71% N= 6,
P < 0.001), and unaffected by hexamethonium
(100 lmol L)1) (40 Hz, )9.69 7.82%, N= 5, ns) and
thapsigargin (10 lmol L)1, 40 Hz, )10.35 14.56%,
N= 5, ns). OB 100 lmol L)1 significantly inhibited the
amplitude of EFSon-contractions following blockade of
muscarinic receptors by atropine 1 lmol L)1 ()40.47
9.28%, N= 9, P < 0.01), blockade of NK2 receptors byGR4800 1
lmol L)1 ()58.61 9.08%) blockade of nico-
tinic receptor by hexamethonium 100 lmol L)1
()47.33 9.04%) and depletion of intracellular calcium
stores by thapsigargin 10 lmol L)1 ()47.19 9.92%).
OB also induced a concentration-dependent inhibition
in the amplitude of electrical off-contractions at high
frequencies of stimulation (2040 Hz) ()58.69 15.61%
at 40 Hz, P < 0.05, N = 6). In contrast, latency of off-
contractions was unaffected by OB ()5.18 2.26%, at
40 Hz, ns, N = 6). Nifedipine 1 lmol L)1 strongly re-
duced off-contractions at 140 Hz ()67.86 12.4%, at
40 Hz, P 0.001, N= 5), an effectthat wasfully reversed
by BayK8644 (1 lmol L)1). The inhibition of the ampli-
tude of EFS on- and off-contractions caused by OB
10 lmol L)1 was also fully reversed by the calcium
channel activator BayK8644 (1 lmol L)1) (Fig. 6).
Effect of OB on the responses induced by directstimulation of
sigmoid smooth muscle cells
Otilonium bromide 100 lmol L)1 significantly inhibi-
ted the direct contraction produced by ACh
Volume 22, Number 6, June 2010 Otilonium bromide inhibits human
sigmoid motility
2010 Blackwell Publishing Ltd e183
-
8/13/2019 Human Sigmoid Colon
5/12
(10 lmol L)1, )74.63 8.69%; P < 0.001, N= 10) and
SP (10 lmol L)1, )78.8 6.66%; P < 0.05, N= 7) in this
preparation. Nifedipine 100 lmol L)1 also inhibited the
direct contractions induced by ACh, and SP. Contrac-
tion induced by 10 lmol L)1 NKA was also significantly
reduced by 100lmol L)1OB)61.61 4.12%; P < 0.001,
N= 4) and almost abolished by 100 lmol L)1 nifedipine
further suggesting L-type Ca2+ channels contribute to
cholinergic and tachykinergic responses. During exper-
iments with calcium image technique, application of
high extracellular potassium (75 mmol L)1) induced an
intracellular calcium increase in smooth muscle cells.
This increase was concentration dependently reduced
by OB (0.01100 lmol L)1). OB inhibited the calcium
transients with an IC50of 0.2 lmol L)1, 15 cells,N= 5)
(Fig. 7).
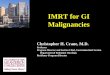
Figure 1 Mechanical recordings showing inhibition of spontaneous
motility (RPCs) by increasing concentrations of otilonium bromide
(A),nifedipine (B), atropine (C), n-butyl-hyoscine (D) and the NK2
antagonist GR94800 (E). Cumulative concentrationresponse curves of
(F) L-type
calcium channel blockers, otilonium bromide and nifedipine, (G)
muscarinic receptor blockers, atropine and n-butyl-hyoscine and (H)
the NK2
antagonist GR94800.
D. Gallegoet al. Neurogastroenterology and Motility
2010 Blackwell Publishing Ltde184
-
8/13/2019 Human Sigmoid Colon
6/12
DISCUSSION AND CONCLUSIONS
In the present study, we have assessed the strong
inhibitory effect OB has on the main patterns of human
sigmoid motility in vitro (RPCs, smooth muscle tone,
contractions induced by stimulation of excitatoryEMNs,
contractions induced by direct effect of excit-
atory neurotransmitters and calcium transients in
isolated colonic smooth muscle cells). In contrast, OB
did not affect inhibitory neuromuscular transmission.
OB inhibited calcium transients induced by KCl in
isolated sigmoid smooth muscle cells in a similar way
to the inhibition of inward currents driven by L-type
calcium channels in rat colonic smooth muscle cells17
and human small intestine.18 Moreover, binding stud-
A
B
C
Figure 2 (A) Mechanical recording and histograms showing the
increase in the activity of spontaneous rhythmic phasic
contractions (RPCs) induced
by the L-type Ca2+ channel agonist BayK8644. Incubation of
strips with (B) the L-type Ca2+ channel antagonist nifedipine (10
lmol L)1) or (C)
otilonium bromide (10 lmol L)1) concentration-dependently
antagonized and prevented the effect of BayK8644. AUC, area under
the curve of RPCs.
Data are expressed as mean SEM (*P < 0.05, **P < 0.01,
***P < 0.001).
Table 1 Pharmacodynamics of otilonium bromide and nifedipine
on
in vitro motor patterns in the human sigmoid colon
Pattern
IC50+ SEM
(mol L)1)
Emax(% inhibition)
Otilonium
bromide
RPCs 4.99 10)8 0.14 84.17 16.87
Stretch-induced
tone (7 g)
1.07 10)8 0.69 54.92 8.21
Stretch-induced
amplitude (7 g)
7.76 10)6 0.25 64.21 4.03
EFS-on 3.80 10)8 0.20 49.39 13.75ACh contraction 2.52 10)2 0.58
74.63 8.69
SP contraction 3.16 10)4 0.45 78.8 6.66
Nifedipine RPCs 1.00 10)8 0.69 95.35 6.37
EFS-on 1.32 10)10 0.45 96.28 3.71
ACh contraction 6.92 10)8 0.31 73.56 12.51
SP contraction 5.13 10)9 0.25 89.59 7.15
Volume 22, Number 6, June 2010 Otilonium bromide inhibits human
sigmoid motility
2010 Blackwell Publishing Ltd e185
-
8/13/2019 Human Sigmoid Colon
7/12
A
B
C
D
Figure 3 Representative tracings and graph bars showing how
single concentrations of OB (100 lmol L)1) strongly inhibit
rhythmic phasic con-
tractions following: (A) blockade of muscarinic receptors by
atropine 1 lmol L)1, (B) depletion of intracellular Ca by
thapsigargin 10 lmol L)1, (C)
blockade of nicotinic receptors by hexamethonium 100 lmol L)1,
and (D) blockade of NK2 receptors by GR 94800. Data are expressed
as mean SEM
(*P < 0.05, **P < 0.01).
D. Gallegoet al. Neurogastroenterology and Motility
2010 Blackwell Publishing Ltde186
-
8/13/2019 Human Sigmoid Colon
8/12
ies also found that OB showed competitive interaction
and nmol L)1 affinity for the L-type calcium channel.12
The pharmacological profile of OB in our studysuggests that OB
might exert its spasmolytic effect
mainly by reducing calcium influx through L-type
calcium channels on human colonic smooth muscle
cells.
After oral administration, OB is not absorbed sys-
temically and pharmacokinetic studies in humans
have found that OB is mainly eliminated by feces
(97.8%) and minimally excreted by urine (0.71%).5,19,20
Animal studies using oral doses similar to those used
in humans show maximal and specific accumulation of
OB in the colonic circular muscle,21 and peak levels in
colonic tissues reaching the micromolar range 8 h after
oral drug administration.22 Accordingly, OB might actat the
level of the gastrointestinal tract without
systemic absorption. The pharmacological profile of
the effect of OB in our study shows that OB strongly
inhibits spontaneous RPCs (IC50 = 49.9 nmol L)1 for
OB and 1.00 nmol L)1 for nifedipine) but with lesser
potency than the specific L-type calcium channel
blocker nifedipine (Emax= 84.17% and Emax= 95.35%
respectively). These results suggest similar affinity but
lesser intrinsic activity of OB on L-type channels
compared with nifedipine and agree with our previous
studies on the rat colon.17 The effects of OB and
nifedipine on RPCs in our study are reversed by thespecific
L-type Ca2+-channel agonist, BayK8644, con-
firming the involvement of L-type calcium channels in
the effect of OB on RPCs. Stretch is an important
stimulus in the gastrointestinal tract and L-type
calcium channels are gated by voltage, several chem-
ical mediators and stretch.23 We found that stretch
increased the amplitude of spontaneous contractions
and baseline tone in the human sigmoid colon through
non-neural mechanisms, and stretch-induced contrac-
tions and tone were also strongly inhibited by OB.
Inhibitory neurotransmission can be quantified with
the latency observed before the onset of the
off-contraction.13 This latency is caused by stimulationof
inhibitory motor neurons releasing NO and a purine
acting on P2Y1 receptors.13 The latency is well-corre-
lated with electrophysiological data where the fast and
the slow component of the IJP is due to a purine acting
on P2Y1 receptors and NO respectively.14 The present
study shows that OB does not modify the latency
suggesting that inhibitory neurotransmission in the
human colon is unaffected by OB. Similar results were
reported in the rat colon where the fast component of
A B
Figure 4 (A) Mechanical recording showing the effect of induced
tension on spontaneous motility and tone in control conditions (top
trace) and
in the presence of otilonium bromide (OB) (0.1 lmol L)1) (bottom
trace). (B) Plot graph showing (top) the amplitude increase of
spontaneous
contractions induced by tension and (bottom) the increase of
basal tone induced by tension. Data are expressed as mean SEM.
Volume 22, Number 6, June 2010 Otilonium bromide inhibits human
sigmoid motility
2010 Blackwell Publishing Ltd e187
-
8/13/2019 Human Sigmoid Colon
9/12
the IJP was not modified.17 In contrast, we found a
strong inhibitory effect of OB on the amplitude of thetwo main
types (on and off) of sigmoid contractions
induced by EFS of excitatory EMNs. The mechanisms
of action of OB on the inhibition of amplitude of EFS
on- and EFS off-contractions both mediated by
stimulation of excitatory EMNs co-releasing ACh and
tachykinins acting on NK2 receptors13 need careful
discussion. Initial in vitro studies in the guinea pig
ileum found OB counteracted the spasmogenic effect of
ACh with an IC50 in the 20100 nmol L)1 range,
similar to that found for atropine in the same exper-
iments.10 This antimuscarinic activity was confirmedin binding
studies that show that OB binds with sub
lmol L)1 affinity to many types of muscarinic recep-
tors in different tissues.12 Results from these initial
studies described the pharmacological profile of OB as
a non-competitive antimuscarinic compound.10 Other
in vitro studies demonstrated that OB also behaves as a
potent blocker of neuronal nicotinic ACh receptors
blocking Ca2+ uptake induced by nicotinic agonists
with an IC50in the lmol L)1 range, and suggested that
Figure 5 (A) Plot graph showing the effect of
otilonium bromide (OB) (top) and nifedipine
(bottom) on the amplitude of electrical
stimulation (EFS) induced on-contractions.
(B) Concentrationresponse curves reflecting
the inhibitory effect OB and nifedipine on
the amplitude of the EFS inducedon-contractions at the maximum
frequency
of stimulation (40 Hz). Data are expressed
as mean SEM (*P < 0.05 vs previousconcentration).
D. Gallegoet al. Neurogastroenterology and Motility
2010 Blackwell Publishing Ltde188
-
8/13/2019 Human Sigmoid Colon
10/12
blockade of nAChRs at the myenteric plexus might
contribute to the spasmolytic effect of OB.11 In addi-
tion, pharmacological studies on guinea-pig proximal
colon and binding studies on isolated cells transfected
with the human tachykinin NK2receptor demonstrate
that OB acts in the lmol L)1 range as muscarinic and
A B
B
Figure 6 (A) Representative tracings showing electrical
stimulation (EFS)off-contractions and (B) EFSon-contractions. Note
EFSoffresponses occur
after a period of latency (marked in the tracing). Histograms
show the reduction of amplitude of electrical on- and
off-contractions by otilonium
bromide and the reversion of this effect by the L-type Ca 2+
channel agonist, BayK8644 (1 lmol L)1). Data are expressed as mean
SEM (*P < 0.05,
**P < 0.01, ***P< 0.001).
A B C
KCI
OB 0.01 mol L1
OB 0.01 mol L1
A B C
OB 0.1 mol L1
OB 1 mol L1
OB 10 mol L1
OB 0.1 mol L1
OB 10 mol L1
OB 3 mol L1
OB 10 mol L
1
OB 100 mol L1
7
A
C
B
6
5
4
3
2
1
Fluorescence
F/F
0 5 10 15
Time (s)
75
50
25
08 7
Log (otilonium)
Percentage
ofcontrol
6 5 4
20 25 30
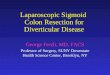
Figure 7 (A) Ca2+ transients induced by KCl. (A) This figure
illustrates the change in relative Fluo4 fluorescence in one cell
in response to an
application of KCl (75 mmol L)1) (showed with a bar) in the
presence of increasing concentrations of otilonium bromide (OB;
from 10 nmol L )1 to
100 lmol L)1). (B) Images taken at specific time points and
corresponding to the dotted lines in different OB concentrations.
(C) Doseresponse data
fitted to a sigmoid curve of relative Fluo4 fluorescence DF/F in
response to an application of KCl in the presence of different OB
concentrations. Data
are expressed as mean SEM.
Volume 22, Number 6, June 2010 Otilonium bromide inhibits human
sigmoid motility
2010 Blackwell Publishing Ltd e189
-
8/13/2019 Human Sigmoid Colon
11/12
tachykinin NK2receptor antagonist.24 Taken together,
these studies suggest multiple mechanisms of action
for the inhibitory properties of OB to reduce stimulated
motility of intestinal smooth muscle.5,24 In the present
study, we could not distinguish between a putative
effect on muscarinic, nicotinic or tachykinergic recep-tors
because the predominant effect of OB in the
human sigmoid colon was probably the blockade of
L-type calcium channels. In agreement with this
hypothesis, nifedipine inhibited both EFS-induced on-
and off-contractions and the L-type Ca2+ channel
activator BayK8644 reversed the inhibitory action of
OB on both EFS on- and off-contractions. Altogether,
our results suggest that the predominant mechanism of
action of OB on these potent contractions induced by
stimulation of excitatory EMNs is exerted through
blockade of L-type calcium channels, the same mech-
anisms that we found for the effect of OB on non-
neural RPCs. L-type calcium channels have different
binding sides to dihydropyridines (nifedipine), ben-
zothiazepines (diltiazem) and phenylalkilamines
(verapamil).25 Previous studies have demonstrated that
OB binds to the diltiazem binding side of the L-type
calcium channel with a minor binding on the dihydro-
pyridine binding side.12 Our results show that BayK, a
dihydropiyidine derivative, is able to counteract the
effects of OB. This is probably due to the interaction
with the fraction of OB bound to the dihydropyridine
binding side or to interactions between the different
binding sides of the channel.25 The stretch sensor of
the L-type calcium channel is located in the alpha(1C)-subunit26
where the binding of these different antag-
onists is located. Contraction of smooth muscle cells
from the gastrointestinal tract depends on extra cellu-
lar calcium influx mainly through L-type calcium
channels and calcium release from intracellular stores.
Entry of calcium through L-type voltage-dependent
Ca2+ channels provides the major source for the
contractile response to ACh in canine circular colonic
smooth muscle.27 In contrast, contraction of human
sigmoid circular smooth muscle cells in response to
NKA requires release of intracellular calcium.28 In our
study, contractions induced by ACh, NKA and SP were
strongly inhibited by OB as were intracellular calcium
transients caused by direct KCl-depolarization of sig-
moid smooth muscle cells.
It is always difficult to establish a correlation
between colonic motility in vivo and in vitro. In vivo
human colonic motility is complex and involves three
main motor patterns to produce the normal mixing
and propulsive motor functions: RPCs, giant migrat-
ing contractions (GMCs) and tone, each with specific
mechanisms of control.29 Spontaneous RPCs are
caused by direct transmission of electrical slow waves
from interstitial cells of cajal to smooth muscle
cells30 and contribute to the mixing of colonic
contents.29 Colonic tone can modulate the mechan-
ical efficacy of RPCs and GMCs.29 In vitro on-con-
tractions correlate well with in vivo simultaneouscontractions,
the most common pattern of pressure
activity in the human colon, which can slow transit;
and in vitro off-contractions might be equivalent to
sigmoid GMCs, or high-amplitude propagating con-
tractions causing propulsion of stools and initiation of
defecation.31 Latency of in vitro off-contractions
determines the velocity of propagation of in vivo
GMCs,31 suggesting OB might decrease the amplitude
of sigmoid contractions without affecting their prop-
agation. Previous in vivo studies in humans by
sigmoid manometry found OB reduced sigmoid motil-
ity and enhanced the pain threshold following infla-
tion of a endoluminal balloon,69 agreeing with the
present study. We believe the evaluation of an
antispasmodic drug should include the assessment of
its effects on all these specific motor patterns and its
effects on direct excitability of sigmoid smooth
muscle cells.29 In conclusion, we found a predomi-
nant mechanism of action for the strong spasmolytic
properties of OB on the normal human sigmoid
motility patterns based in its properties as a blocker
of L-type calcium channels mediating calcium influx
on smooth muscle cells. We believe these pharmaco-
logical properties might mediate the clinically proven
effects of OB on the spastic motility disturbancesdescribed in
subsets of patients with IBS.
ACKNOWLEDGMENTS
The authors thank Dr Alex Saenz, M. Marti-Gallostra and
J. Cases (Clnica Sagrada Familia) and Dr Xavier Sunol,
Dr Oscar Estrada, Dr Fran Espin, Dr Adolfo Heredia, Dr Eva
Garca, and Dr Lus Antonio Hidalgo (Hospital de Mataro)
forproviding human tissue. We also thank Dr S. Evangelista and
Mrs Jane Lewis for revising the manuscript. This study was
supported by a grant from the Fundacio de Gastroenterologia
Dr Francisco Vilardell, the Fundacio Salut del Consorci
Santaridel Maresme, the Departament dUniversitats, Recerca i
Soci-
etat de la Informacio (2009-SGR-708), the Fondo de
Investigac-
iones Sanitarias del Ministerio de Sanidad y
Consumo(IF063678-1), the CIDEM (Centre dInnovacio i
Desenvolupa-
ment Empresarial) (RDITSIND06-1-0174), BFU2006-05055/BFI
and by Laboratorios Menarini SA. Ciberehd is funded by
theInstituto de Salud Carlos III.
CONFLICT OF INTEREST
P. Clave has served as a speaker for Menarini International
and
has received research funding from Laboratorios Menarini
SA-Menarini Group, Badalona, Spain.
D. Gallegoet al. Neurogastroenterology and Motility
2010 Blackwell Publishing Ltde190
-
8/13/2019 Human Sigmoid Colon
12/12
REFERENCES
1 Hungin AP, Whorwell PJ, Tack J,Mearin F. The prevalence,
patternsand impact of irritable bowel syn-
drome: an international survey of40,000 subjects. Aliment
PharmacolTher2003; 17: 64350.
2 Ford AC, Talley NJ, Spiegel BMet al.Effect of fibre,
antispasmodics, andpeppermint oil in the treatment ofirritable
bowel syndrome: systematicreview and meta-analysis. BMJ2008;337:
a2313.
3 Kanazawa M, Palsson OS, Thiwan SIet al. Contributions of pain
sensitiv-ity and colonic motility to IBSsymptom severity and
predominantbowel habits. Am J Gastroenterol2008; 103: 255061.
4 Jailwala J, Imperiale TF, Kroenke K.Pharmacologic treatment of
the irri-table bowel syndrome: a systematicreview of randomized,
controlled tri-als. Ann Intern Med 2000; 133: 13647.
5 Spinelli A. Irritable bowel syndrome.Clin Drug Investig2007;
27: 1533.
6 Baldi F, Longanesi A, Blasi A et al.Clinical and functional
evaluation ofthe efficacy of otilonium bromide: amulticenter study
in Italy. Ital J Gastroenterol1991; 23: 603.
7 Baldi F, Longanesi A, Blasi A et al.Octylonium bromide in the
treat-ment of the irritable bowel syndrome:a clinical-functional
study 1.Hepatogastroenterology 1992; 39:3925.
8 Battaglia G, Morselli-Labate AM,Camarri E et al. Otilonium
bromidein irritable bowel syndrome: a double-blind,
placebo-controlled, 15-weekstudy 4. Aliment Pharmacol Ther1998; 12:
100310.
9 Tack J, Fried M, Houghton LA, SpicakJ, Fisher G. Systematic
review: theefficacy of treatments for irritablebowel syndrome a
European per-spective 17.Aliment Pharmacol Ther2006; 24:
183205.
10 Evangelista S. Quaternary ammo-nium derivatives as
spasmolytics forirritable bowel syndrome. CurrPharm Des2004; 10:
35618.
11 Gandia L, Villarroya M, Lara B et al.Otilonium: a potent
blocker ofneuronal nicotinic ACh receptors in
bovine chromaffin cells 25. Br JPharmacol 1996; 117: 46370.
12 Evangelista S, Giachetti A, ChapelainB, Neliat G, Maggi CA.
Receptorbinding profile of otilonium bromide
20. Pharmacol Res 1998; 38: 1117.13 Auli M, Martinez E, Gallego
Det al.
Effects of excitatory and inhibitoryneurotransmission on motor
patternsof human sigmoid colon in vitro. Br JPharmacol 2008; 155:
104355.
14 GallegoD, Gil V,Aleu J,AuliM, ClaveP, Jimenez M. Purinergic
and nitrergicjunction potential inthe humancolon.
Am J Physiol Gastrointest Liver
Physiol2008;295: G52233.15 Lindqvist S, Hernon J, Sharp P et
al.
The colon-selective spasmolytic oti-lonium bromide inhibits
muscarinicM(3) receptor-coupled calcium sig-
nals in isolated human colonic crypts1.Br J Pharmacol2002;137:
113442.
16 Farrugia G, Holm AN, Rich A, SarrMG, Szurszewski JH, Rae JL.
A me-chanosensitive calcium channel inhuman intestinal smooth
musclecells 1. Gastroenterology 1999; 117:9005.
17 Martin MT, Hove-Madsen L, JimenezM. Otilonium bromide
inhibits mus-cle contractions via L-type calciumchannels in the rat
colon 5. Neuro-
gastroenterol Motil2004; 16: 17583.18 Strege PR, Evangelista S,
Lyford GL,
Sarr MG, Farrugia G. Otilonium bro-
mide inhibits calcium entry throughL-type calcium channels in
humanintestinal smooth muscle 6. Neuro-
gastroenterol Motil2004; 16: 16773.19 Sutton JA, Kilminster SG,
Mould GP.
The clinical pharmacology of singledoses of otilonium bromide in
heal-thy volunteers. Eur J Clin Pharmacol1997; 52: 3659.
20 Shin BS, Kim JJ, Kim J et al. Oralbioavailability and
enterohepaticrecirculation of otilonium bromide inrats. Arch Pharm
Res 2008; 31: 11724.
21 Amenta F, Baroldi P, Ferrante F,
Napoleone P, Meli A. Autoradio-graphic localization of
octyloniumbromide binding sites in the ratgastrointestinal tract
17. Arch IntPharmacodyn Ther1991; 311: 519.
22 Evangelista S, Cochet P, Bromet N,Criscuoli M, Maggi CA. A
distribu-tion study with (14)C-otilonium
bromide in the rat: evidence forselective tropism for large
intestineafter oral administration.Drug MetabDispos2000; 28:
6437.
23 Malysz J, Richardson D, Farraway L,
Christen MO, Huizinga JD. Genera-tion of slow wave type action
poten-tials in the mouse small intestineinvolves a non-L-type
calcium chan-nel. Can J Physiol Pharmacol 1995;73: 150211.
24 Santicioli P, Zagorodnyuk V, RenzettiAR, Maggi CA.
Antimuscarinic, cal-cium channel blocker and tachykininNK2 receptor
antagonist actions ofotilonium bromide in the circularmuscle of
guinea-pig colon. NaunynSchmiedebergs Arch Pharmacol
1999; 359: 4207.25 Striessnig J, Grabner M, Mitterdorfer
J, Hering S, Sinnegger MJ, GlossmannH. Structural basis of drug
binding toL Ca2 + channels.Trends PharmacolSci1998; 19: 10815.
26 Lyford GL, Strege PR, Shepard Aet al.alpha(1C) (Ca(V)1.2)
L-type calciumchannel mediates mechanosensitivecalcium
regulation.Am J Physiol CellPhysiol 2002;283: C10018.
27 Sato K, Sanders KM, Gerthoffer WT,Publicover NG. Sources of
calciumutilized in cholinergic responses incanine colonic smooth
muscle. Am JPhysiol 1994;267: C166673.
28 Cao W, Pricolo VE, Zhang L, Behar J,
Biancani P, Kirber MT. Gq-linkedNK(2) receptors mediate neurally
in-duced contraction of human sigmoidcircular smooth muscle.
Gastroen-terology2000; 119: 5161.
29 Sarna SK. Molecular, functional, andpharmacological targets
for thedevelopment of gut promotility drugs.
Am J Physiol Gastrointest Liver
Physiol 2006;291: G54555.30 Huizinga JD, Stern HS, Chow E,
Diamant NE, el-Sharkawy TY. Elec-trophysiologic control of
motility inthe human colon. Gastroenterology1985; 88: 50011.
31 Rao SS, Sadeghi P, Beaty J, Kavlock R,Ackerson K. Ambulatory
24-h colonicmanometry in healthy humans. Am JPhysiol Gastrointest
Liver Physiol
2001; 280: G62939.
Volume 22, Number 6, June 2010 Otilonium bromide inhibits human
sigmoid motility
2010 Blackwell Publishing Ltd e191