Embed Size (px)
Citation preview

Human fetal bilirubin levels and fetal hemolytic disease
Carl P. Weiner, MD
Iowa City, Iowa
The development of secondary fetal anemia in association with maternal red blood cell alloimmunization
requires hemolysis. In specimens obtained at the time of a clinically indicated cordocentesis, total and
direct umbilical venous bilirubin was measured and the indirect umbilical venous bilirubin calculated in 43antigen-positive and 30 control fetuses. Twenty-two (51%) of the antigen-positive fetuses had or
SUbsequently developed severe anemia (hematocrit <30%). Umbilical venous total bilirubin (r = 0.47,P = 0.0008) and direct bilirubin (r = 0.520, P = 0.04) levels each rose with gestation. Indirect bilirubin did
not vary significantly with gestation. Bilirubin was unrelated to hemoglobin. In contrast to the controlfetuses, umbilical venous total bilirubin for antigen-positive fetuses was inversely related to hemoglobin
(r = -0.57, P < 0.0001) independent of gestational age (r = 0.53, P < 0.0001) (multiple R of hemoglobinand gestational age for umbilical venous total bilirubin = 0.76, P < 0.0001). Eighteen of 22 (82%) fetuses
in whom anemia developed had an umbilical venous total bilirubin ;0,97.5 percentile compared with only
eight of 21 (38%) fetuses in whom anemia did not develop (p = 0.009). In longitudinal study the umbilicalvenous total bilirubin frequently rose above normal weeks before the development of anemia. An umbilicalvenous total bilirubin >3 mgldl represented the warning line. Fifteen of 16 (94%) fetuses in whom either
severe antenatal anemia or significant postnatal hyperbilirubinemia developed had an umbilical venoustotal bilirubin >3 mg/dl. We conclude that the normal placental capacity for the transport of fetal bilirubin is
exceeded in the face of enhanced fetal hemolysis. An elevated fetal bilirubin often precedes the
development of antenatal anemia. The antigen-positive fetus with an elevated bilirubin is at high risk todevelop anemia antenatally. (AMJ DasTET GVNECOL 1992;166:1449-54.)
Key words: Fetus, bilirubin, hemolytic anemia, alloimmunization, cordocentesis
Although the fetal response to maternal red bloodcell alloimmunization depends on several factors, including the quantity of antibody bound to the fetal redblood cell and the rate of red blood cell production,'the development of fetal anemia ultimately requireshemolysis. In a preliminary study our unit observedthat the normal fetal concentration of bilirubin exceeded that of the neonate." This suggested that theplacental capacity for fetal bilirubin clearance was limited. The purposes of this investigation were to determine (l) the concentration of fetal bilirubin across gestation, (2) whether antigen-positive fetuses of alloimmunized women have higher bilirubin concentrationsthan control fetuses, and (3) whether a high bilirubin concentration preceded the development of fetalanemia.
From the Fetal Diagnosis and Treatment Unit, Division ofMaternalFetal Medicine, Department of Obstetricsand Gynecology, Universityof Iowa College of Medicine.Supported in part by grant 24494 from the National Institutes ofHealth, National Institute of Child Health and Development.Received for publication May 7, 1991; revised September 6, 1991;accepted November 26, 1991.Reprint requests:Carl P. Weiner, M D, Department of ObstetricsandGynecology, University of Iowa College of Medicine, Iowa City, IA52242.611135284
Material and methods
Cordocentesis was performed in 73 pregnancies withreferral to the University of Iowa Fetal Diagnosis andTreatment Unit. Forty-three antigen-positive fetuses atrisk for hemolytic anemia were sampled (95 specimens)to determine the severity of their disease as describedpreviously.' The remaining 30 fetuses were sampledonce for a variety of indications (most commonly maternal red cell or platelet alloimmunization) and shownto be free of disease.
Laboratory measurements performed in the centralhospital laboratory included total bilirubin, direct bilirubin, and a complete blood cell count. The indirectbilirubin was calculated. Total and direct bilirubin(mg/dl) were measured in serum by a commerciallyavailable colorimetric assay (Boehringer-Mannheim)on an autoanalyzer (Hitachi 737). Hemolyzed sampleswere excluded. The complete blood cell count was performed with an autoanalyzer (Technicon H-l) on bloodanticoagulated with ethylenediaminetetraacetic acid.Because of the limited sample volume, not alI tests couldbe performed on each occasion.
The technique for cordocentesis has previously beendetailed.' Briefly, a 22-gauge spinal needle was held inthe ultrasonographic plane of a 5 MHz sector transducer with a fixed-needle guide (CIVCO, Kalona, la.).
1449

1450 Weiner
TB(mg/dL)
3.0
2.0
1.0
n =30 r =0.473 p =O.0008
TB = 2.53-21.8 /Weeks
May 1992Am J Obstet Gynecol
o18 20 22 24 26 28 30 32 34 36 38
Weeks
Fig. 1. Prediction interval (95%) for umbilical venous serum total bilirubin (TH) in healthy, antigennegative fetuses (n = 30). There was no relationship between bilirubin and hemoglobin in this group.
The umbilical vein was preferred over the umbilicalartery to minimize the risk of a procedure-relatedbradycardia." Pancuronium (0.3 mg/kg estimated fetalweight) was administered intravenously whenever fetalmovement was felt to pose a risk.
All records were maintained prospectively in a computerized data base whose veracity was confirmed ona regular basis. The results are presented as themean ± SD unless otherwise stated. One hundredeleven of 125 (90.2%) specimens were from the umbilical vein. Only the first measurement from each antigen-positive fetus was included in the search for arelationship between bilirubin and both hemoglobinand gestational age. Because the small number of arterial specimens precluded an accurate comparison ofarterial and venous samples controlling for gestationalage, the statistical analyses presented here were limitedto specimens from the umbilical vein. The 95% prediction interval of bilirubin for control fetuses wasbased on the regression obtained using bilirubin as thedependent variable and gestational age as the independent variable. Subsequent bilirubin measurementsfrom antigen-positive, not transfused, fetuses weregraphed to reveal the natural history. An analysis ofcovariance was used to compare the bilirubin slopes ofantigen-positive and control fetuses. Receptor-operated curves were applied to determine the umbilicalvenous total bilirubin concentration most predictive ofa fetal or neonatal hemolytic complication. Other analyses included independent t test, stepwise multipleregression, and cross tabulation. A p value ~0.05 wasconsidered to indicate a significant difference.
ResultsThe mean gestational age of fetuses at risk for hemo
lytic anemia was 24.9 ± 3 weeks and ranged from 20to 36 weeks. Twenty-two (51%) developed a hematocrit<30% and were considered candidates for transfusiontherapy.' The mean gestational age of the controlgroup was 27 ± 5 weeks and ranged from 20 to 38weeks.
Umbilical venous total bilirubin (r = 0.47, P<0.0008, n = 30) (Fig. 1) and direct bilirubin (r = 0.52,P = 0.04, n = 15) for the control group rose progressively with advancing gestation and were unrelated tothe fetal hemoglobin. Indirect bilirubin did not changesignificantly with gestation (mean 1.4 ± 0.3 mg/dl,n = 15).
In contrast to the control fetuses, umbilical venoustotal bilirubin from antigen-positive fetuses was inversely related to hemoglobin (r = - 0.57, P< 0.0001)(Fig. 2) independent of gestational age (r = 0.53,P< 0.0001) (multiple R of hemoglobin and gestationalage for umbilical venous total bilirubin = 0.76,P< 0.0001). There was no relationship between hemoglobin and gestational age in the antigen-positivefetuses (r = 0.05, P = 0.75). Although there was a significant relationship between umbilical venous total bilirubin and gestational age in both groups, they weredifferent (Fig. 3). Umbilical venous total bilirubin inantigen-positive fetuses rose at a rate significantlygreater (p < 0.01) than that expected for the normalgestational increment. A similar association was alsoobserved for both the direct and indirect bilirubin concentrations and hemoglobin and gestational age (Table

Volume 166Number 5
Fetal bilirubin 1451
uvTB = 4.932 - 0.249 * Hb (n= 41)
uvTBmg/dL
7.57
6.56
5.55
4.54
3.53
2.52
1.51
.5o
o
.~ .::.:v ..
5
Hb (g/dL)10 15
Fig. 2. Relationship between total umbili cal veno us bilirubin (uvTB) and hem oglobin (H b) in ant igenpositive fetuses. The higher the bilirubin concentration, the lower the fetal hemoglobin. Note thattotal bilirubin of 3 mg/d l approximates hemoglobin of 8 gm /d l (two missing values).
4.0 r-----------------....,
T.B.mg/dL
3.5
3.0
2.5
2.0
1.5
1.0
.5
-Control
- - Antigen positive
o20 22 24 26 28
Weeks30 32 34
Fig. 3. Regression lines for umbilical venous total bilirubin (T.8 .) and gestati onal age in contro l andantigen-positive groups. Antigen-positive fetuses have steeper slope. This demonstrates that severi tyof fetal hemolytic d isease was progressive.
I). Because the relationships between indirect and direct bilirubin for hemoglobin in antigen-positive fetu seswere similar to tha t for umbilical venous total bilirubin,we ha ve focused on the latter because of the largersample size.
The umbilical veno us total bilirubin exceeded the97.5 per centile in 18 of 22 (82%) of ant igen-positivefetuses who de velop ed a hematocrit <30%. In eight of10 fetus es with two or more samples, the elevation preceded the development of anemia by several weeks(Fig. 4). In contrast, only eight of 21 (38%) of fetus eswho did not develop severe anemia had an umbili cal
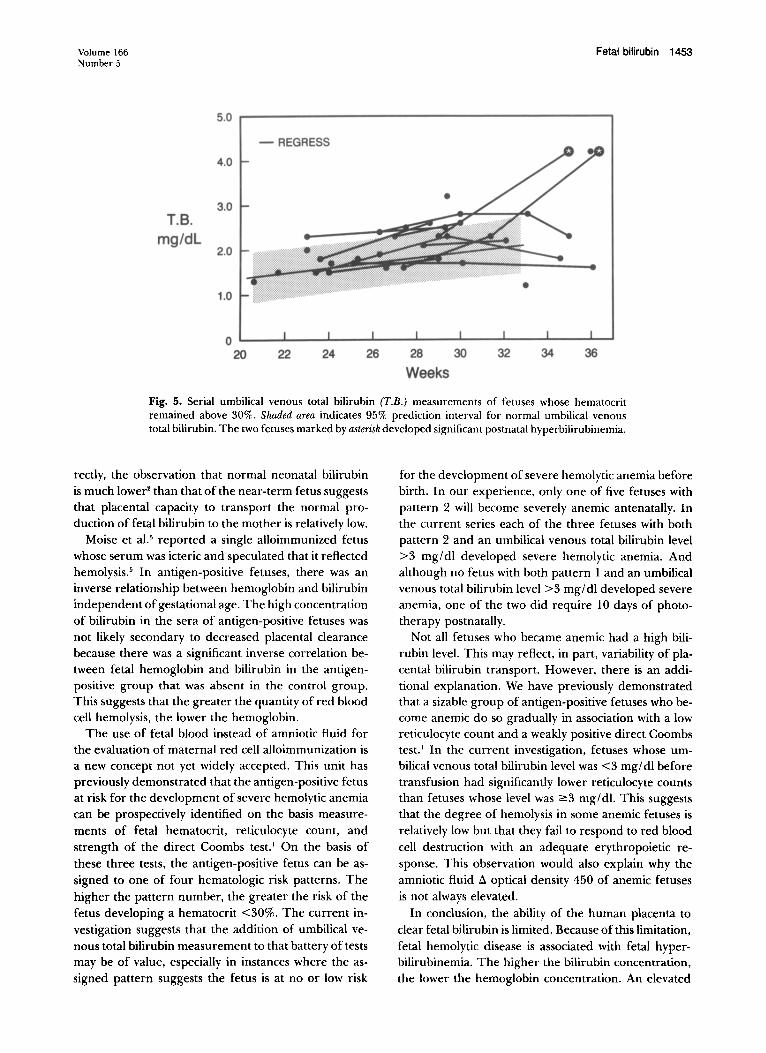
venous total bilirubin above the 97.5 percentile at anytime before delivery (p = 0.009 from fetu ses who requ ired tra nsfusion) (Fig. 5). Overall, the positive predictive value of a high umbilical veno us total bilirubinfor the development of severe fetal hemolytic anemiawas 69% (18 of 26), and the negative predictive valueof a low umbili cal veno us total bilirubin for the development of severe anemia was 76% (13 of 17).
We sought to determ ine whether the clinical application of the umbili cal venous total bilirubin measurement could be further simplified by the identificationof a warning line . An umbilical venou s total bilirubin
1452 Weiner May 1992Am J Obstet Gynecol
36343228 30
Weeks262422
o20
10.0
- REGRESS
8.00
6.0T.e.
mg/dL4.0
00
2.0
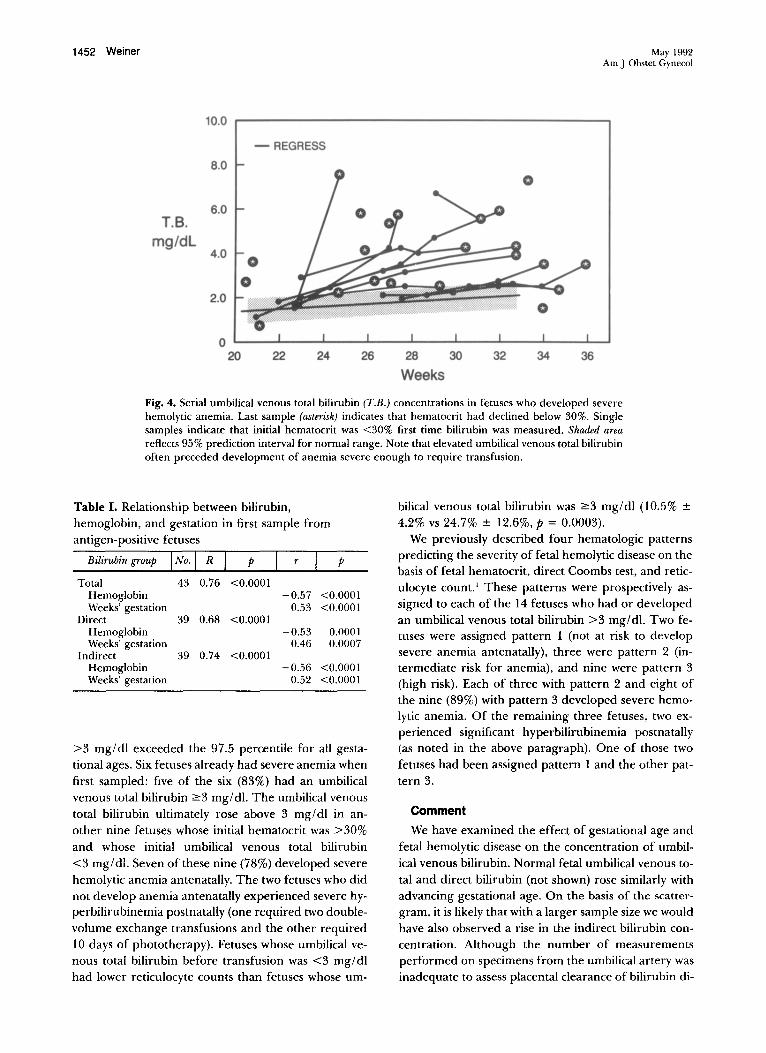
Fig. 4. Serial umbilicalvenous total bilirubin (T.B.) concentrations in fetuses who developed severehemolytic anemia. Last sample (asterisk) indicates that hematocrit had declined below 30%. Singlesamples indicate that initial hematocrit was <30% first time bilirubin was measured. Shaded areareflects95% prediction interval for normal range. Note that elevated umbilical venous total bilirubinoften preceded development of anemia severe enough to require transfusion.
-0.57 <0.00010.53 <0.0001
39 0.68 <0.0001-0.53 0.0001
0.46 0.000739 0.74 <0.0001
-0.56 <0.00010.52 <0.0001
Table I. Relationship between bilirubin,hemoglobin, and gestation in first sample fromantigen-positive fetuses
Bilirubin group ~ p C=::::=I p
Total 43 0.76 <0.0001HemoglobinWeeks' gestation
DirectHemoglobinWeeks' gestation
IndirectHemoglobinWeeks' gestation
>3 mg/dl exceeded the 97.5 percentile for all gestational ages. Six fetuses already had severe anemia whenfirst sampled: five of the six (83%) had an umbilicalvenous total bilirubin ?3 mg/dl. The umbilical venoustotal bilirubin ultimately rose above 3 mg/dl in another nine fetuses whose initial hematocrit was >30%and whose initial umbilical venous total bilirubin<3 mg/dl. Seven of these nine (78%) developed severehemolytic anemia antenatally. The two fetuses who didnot develop anemia antenatally experienced severe hyperbilirubinemia postnatally (one required two doublevolume exchange transfusions and the other required10 days of phototherapy). Fetuses whose umbilical venous total bilirubin before transfusion was <3 mg/dlhad lower reticulocyte counts than fetuses whose um-
bilical venous total bilirubin was ?3 mg/dl (10.5% ±
4.2% vs 24.7% ± 12.6%, P = 0.0003).We previously described four hematologic patterns
predicting the severity of fetal hemolytic disease on thebasis of fetal hematocrit, direct Coombs test, and reticulocyte count. 1 These patterns were prospectively assigned to each of the 14 fetuses who had or developedan umbilical venous total bilirubin >3 mg/dl. Two fetuses were assigned pattern 1 (not at risk to developsevere anemia antenatally), three were pattern 2 (intermediate risk for anemia), and nine were pattern 3(high risk). Each of three with pattern 2 and eight ofthe nine (89%) with pattern 3 developed severe hemolytic anemia. Of the remaining three fetuses, two experienced significant hyperbilirubinemia postnatally(as noted in the above paragraph). One of those twofetuses had been assigned pattern 1 and the other pattern 3.
Comment
We have examined the effect of gestational age andfetal hemolytic disease on the concentration of umbilical venous bilirubin. Normal fetal umbilical venous total and direct bilirubin (not shown) rose similarly withadvancing gestational age. On the basis of the scattergram, it is likely that with a larger sample size we wouldhave also observed a rise in the indirect bilirubin concentration. Although the number of measurementsperformed on specimens from the umbilical artery wasinadequate to assess placental clearance of bilirubin di-
Volume 166Number 5
Fetal bilirubin 1453
5.0
- REGRESS
4.0
•3.0
T.B.mg/dL
2.0
1.0
020 22 24 26 28 30 32 34 36
Weeks
Fig. 5. Serial umbilical venous total bilirubin (T.R.) measurements of fetuses whose hematocritremained above 30%. Shaded area indicates 95% prediction interval for normal umbilical venoustotal bilirubin. The two fetuses marked by asterisk developed significant postnatal hyperbilirubinemia.
rectly, the observation that normal neonatal bilirubinis much lower" than that of the near-term fetus suggeststhat placental capacity to transport the normal production of fetal bilirubin to the mother is relatively low.
Moise et aJ.5 reported a single alloimmunized fetuswhose serum was icteric and speculated that it reflectedhemolysis." In antigen-positive fetuses, there was aninverse relationship between hemoglobin and bilirubinindependent of gestational age. The high concentrationof bilirubin in the sera of antigen-positive fetuses wasnot likely secondary to decreased placental clearancebecause there was a significant inverse correlation between fetal hemoglobin and bilirubin in the antigenpositive group that was absent in the control group.This suggests that the greater the quantity of red bloodcell hemolysis, the lower the hemoglobin.
The use of fetal blood instead of amniotic fluid forthe evaluation of maternal red cell alloimmunization isa new concept not yet widely accepted. This unit haspreviously demonstrated that the antigen-positive fetusat risk for the development of severe hemolytic anemiacan be prospectively identified on the basis measurements of fetal hematocrit, reticulocyte count, andstrength of the direct Coombs test. I On the basis ofthese three tests, the antigen-positive fetus can be assigned to one of four hematologic risk patterns. Thehigher the pattern number, the greater the risk of thefetus developing a hematocrit <30%. The current investigation suggests that the addition of umbilical venous total bilirubin measurement to that battery of testsmay be of value, especially in instances where the assigned pattern suggests the fetus is at no or low risk
for the development of severe hemolytic anemia beforebirth. In our experience, only one of five fetuses withpattern 2 will become severely anemic antenatally. Inthe current series each of the three fetuses with bothpattern 2 and an umbilical venous total bilirubin level>3 mg/dl developed severe hemolytic anemia. Andalthough no fetus with both pattern 1 and an umbilicalvenous total bilirubin level >3 mg/dl developed severeanemia, one of the two did require 10 days of phototherapy postnatally.
Not all fetuses who became anemic had a high bilirubin level. This may reflect, in part, variability of placental bilirubin transport. However, there is an additional explanation. We have previously demonstratedthat a sizable group of antigen-positive fetuses who become anemic do so gradually in association with a lowreticulocyte count and a weakly positive direct Coombstest.' In the current investigation, fetuses whose umbilical venous total bilirubin level was <3 mg/dl beforetransfusion had significantly lower reticulocyte countsthan fetuses whose level was :::::3 mg/dl. This suggeststhat the degree of hemolysis in some anemic fetuses isrelatively low but that they fail to respond to red bloodcell destruction with an adequate erythropoietic response. This observation would also explain why theamniotic fluid ~ optical density 450 of anemic fetusesis not always elevated.
In conclusion, the ability of the human placenta toclear fetal bilirubin is limited. Because of this limitation,fetal hemolytic disease is associated with fetal hyperbilirubinemia. The higher the bilirubin concentration,the lower the hemoglobin concentration. An elevated

1454 Weiner
fetal serum bilirubin indicates that the fetus is at highrisk to develop severe hemolytic anemia antenatally. Itmay also provide additional information regarding therisk of postnatal hyperbilirubinemia.
REFERENCES
1. Weiner CP,Williamson RA, Wenstrom KD, Sipes SL, GrantSS, Widness J A. Management of fetal hemolytic disease bycordocentesis: I. Prediction of fetal anemia. AM J OBSTETGYNECOL 1991;165:546-53.
2. Wenstrom KD, Weiner CP, Williamson RA. Effect of gestational age and disease on fetal liver function [Abstract
May 1992Am J Obstet GynecoJ
199]. In : Proceedings of the tenth annual meeting of theSociety of Perinatal Obstetricians, Houston,Texas,January23-27, 1990. Houston: Society of Perinatal Obstetricians,1990.
3. Weiner CPoCordocentesis for diagnostic indications-twoyears' experience. Obstet Gynecol 1987;70:664-8.
4. Weiner CP, Williamson RA, Wenstrom KD, et al. Management of fetal hemolytic disease by cordocentesis. II. Outcome of treatment. AM J OBSTET GYNECOL 1991;165:1302-7.
5. Moise KJ, Kirshon B, Carpenter RJ, Deter RL. Icteric serum as an indicator of fetal vascular access during intravascular transfusion for hemolytic disease. Am J Perinatol1990;7:279-80.
Make researchingeasier with the Ten-Year Cumulative Index (1978-1987) to the AMER
ICAN JOURNAL OFOBSTETRICS AND GYNECOLOGYThe Ten-Year Cumulative Index is a complete guide to more than 30,000 pages of
original articles, case reports, letters, and editorials published in the AMERICAN JOURNALOF OBSTETRICS AND GYNECOLOGY from 1978 through 1987 (volumes 130 to 157). Numbering more than 800 pages, the Cumulative Index includes both a subject and an authorindex. This hard-cover volume is $64.50 ($69.00 international). Prices include shipping.Payment mustaccompany all orders and must be in U.S. funds, drawn on a U.S. bank.
Contact Mosby-Year Book, Inc., Subscription Services, 11830 Westline IndustrialDrive, St. Louis, MO 63146-3318 USA; phone (314) 453-4394. In the U.S., call toll-free:1-800-325-4177, ext. 4394 . Please allow six weeks for delivery.





























