-
ORIGINAL ARTICLE Reproductive epidemiology
Prevalence and risk factors forobstetric haemorrhage in
6730singleton births after assistedreproductive technology
inVictoria AustraliaD.L. Healy1,2,8, S. Breheny2, J. Halliday6,7,
A. Jaques6, D. Rushford3,C. Garrett3, J.M. Talbot5, and H.W.G.
Baker3,41Department of Obstetrics and Gynaecology, Monash
University, Level 5, Monash Medical Centre, 246 Clayton Road,
Clayton, VIC 3168Australia 2Monash IVF, Richmond, Australia
3Department of Obstetrics and Gynaecology, University of Melbourne,
Melbourne, Australia4Melbourne IVF Reproductive Services, The Royal
Womens Hospital, Parkville, Australia 5Melbourne Assisted
Conception Centre,Heidelberg, Australia 6Murdoch Childrens Research
Institute, Melbourne, Australia 7Department of Paediatrics,
University of Melbourne,Melbourne, Australia
8Correspondence address. Tel: 61-03-9594-5374; Fax:
61-03-9594-6389; E-mail: [email protected]
background: Obstetric haemorrhages have been reported to be
increased after assisted reproduction technologies (ART) but
themechanisms involved are unclear.
methods: This retrospective cohort study compared the prevalence
of antepartum haemorrhage (APH), placenta praevia (PP),
placentalabruption (PA) and primary post-partum haemorrhage (PPH)
in women with singleton births between 1991 and 2004 in Victoria
Australia:6730 after IVF/ICSI, 24 619 from the general population,
779 after gamete intrafallopian transfer (GIFT) and 2167 non-ART
conceptions ininfertile patients. Risk factors for haemorrhages in
the IVF/ICSI group were examined by logistic regression.
results: The IVF/ICSI group had more APH: 6.7 versus 3.6%
(adjusted OR 2.0; 95% CI 1.82.3), PP: 2.6 versus 1.1% (2.3;
1.92.9),PA: 0.9 versus 0.4% (2.1; 1.43.0) and PPH: 11.1 versus 7.9%
(1.3; 1.21.4) than the general population. APH, PP and PA were as
frequentin the GIFT group as in the IVF/ICSI group, but were less
frequent in the non-ART group. Within the IVF/ICSI group, fresh
compared withfrozen thawed embryo transfers (FET) was associated
with more frequent APH (1.5; 1.21.8) and PA (2.1; 1.23.7) and the
oddsratio increased with number of oocytes collected (1.02;
1.001.04). Endometriosis patients had more PP (1.7; 1.22.4) and PPH
(1.3;1.11.6) than those without endometriosis. FET in articial
cycles was associated with increased PPH (1.8; 1.32.6) compared
with FETin natural cycles.
conclusions: Obstetric haemorrhages are more frequent with
singleton births after IVF, ICSI and GIFT. The exploratory analysis
offactors in the IVF/ICSI group, showing associations with fresh
embryo transfers in stimulated cycles, endometriosis and hormone
treatments,suggests that events around the time of implantation may
be responsible and that suboptimal endometrial function is the
critical mechanism.
Key words: IVF / obstetrics / antepartum haemorrhage /
post-partum haemorrhage / assisted reproductive technology
IntroductionObstetric haemorrhage and primary post-partum
haemorrhage (PPH)are important causes of maternal mortality
worldwide (World HealthOrganisation, 2007). Antepartum haemorrhage
(APH), placentapraevia (PP) and placental abruption (PA) are major
obstetric compli-cations in all countries. Increased frequencies of
these complications
with births after assisted reproduction technology (ART) have
beenreported by several groups (Daniel et al., 2000; Perri et al.,
2001;Smithers et al., 2003; Jackson et al., 2004; Kallen et al.,
2005b;Shevell et al., 2005; Romundstad et al., 2006; Schieve et
al., 2007).Although increased multiple births after ART were an
importantfactor increasing obstetric haemorrhages, PP and PA are
also knownto be more frequent with singleton deliveries after ART
than after
& The Author 2009. Published by Oxford University Press on
behalf of the European Society of Human Reproduction and
Embryology. All rights reserved.For Permissions, please email:
[email protected]
Human Reproduction, Vol.25, No.1 pp. 265274, 2010
Advanced Access publication on November 7, 2009
doi:10.1093/humrep/dep376
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
natural conceptions in matched controls but the mechanisms
involvedare not clear and deserve further study (Schieve et al.,
2007).
We have previously reported a high frequency of APH and PP in
IVFtwin pregnancies (Smithers et al., 2003). We speculated this was
aconsequence of embryo transfer through the vagina and cervix,
com-pared with in-vivo conception and implantation via the uterine
tube.More recently, Romundstad et al. (2006) conrmed an
increasedrisk of PP [adjusted OR 5.6, 95% condence interval (CI)
4.47.0]in 5581 singleton ART births. They also compared results of
twobirths in the same woman who had both an ART and a natural
con-ception and found that the risk of PP was also higher (OR 2.9)
inthe ART pregnancy. These authors suggested the higher risk of
PPwas largely attributed to factors related to the ART and that
APHand PP may occur as a consequence of embryo transfer through
thevagina and cervix.
Studying factors affecting obstetric haemorrhage after ART
isimportant because ART accounts for 35% of all births in
developedcountries and is increasing in use. Understanding the
mechanismsmight lead to prevention not only of these haemorrhages
in ART preg-nancies but also those in the general community. PPH
has not pre-viously been reported in detail in ART patients (Kallen
et al.,2005b), yet PPH is a leading cause of maternal death.
Studying single-ton births is appropriate with the general move to
elective singleembryo transfer to minimize the multiple pregnancy
rate with ART.
Here we report a multi-centre study of obstetric haemorrhage
andPPH in singleton births of patients who conceived with IVF or
ICSI andcomparison groups from the general community, women who
con-ceived with gamete intrafallopian transfer (GIFT), and
infertilewomen who became pregnant without ART. Our strategy was
asfollows: rstly, to replicate the ndings that the risks of these
haemor-rhages are greater after IVF/ICSI than in the general
population afteradjusting for confounding factors; secondly, to
compare the frequen-cies of the haemorrhages after IVF/ICSI and
GIFT to assess theeffect of manipulation and culture of the embryos
in the embryologylaboratory as this does not occur with GIFT;
thirdly, to compare thefrequencies of the haemorrhages after
IVF/ICSI and non-ART con-ception in infertile women to examine the
effect of infertility; andfourthly, to examine factors within the
IVF/ICSI group that might berelated to haemorrhages.
Materials and MethodsThe project was approved by each Human
Research and Ethics committeeof the hospitals involved and the
Victorian Department of Human Services.
Data sourcesArt clinic databasesThe infertility clinics are
required to keep comprehensive records of allprocedures that result
in birth by Victorian State regulations and forreporting to the
Fertility Society of Australias Reproductive
TechnologyAccreditation Committee and all patients sign consent
forms acknowled-ging this. The databases include information on
clinical features, diagnosis,treatments and the embryos. Additional
information about investigationsand lifestyle factors was added
from the patients records.
Victorian birth dataIn the Victorian Department of Human
Services, the Perinatal Data Collec-tion Unit (PDCU) oversees
mandatory registration of all births of 20weeks gestation and over.
There were approximately 862 000 singletonbirths in the study
period (19912004). Miscarriages and terminationsof pregnancy at ,20
weeks gestation are not registered as births in Vic-toria unless a
birth defect is recorded. Data on the existing maternalmedical
conditions, previous pregnancies, gestation at birth,
maternalcomplications of pregnancy and mode of delivery are
provided on formsby midwives involved with the births and entered
on computer centrally.Over 99.6% of all births in Victoria were
reported to the PDCU in 1996(Riley and Grifn, 1997).
SubjectsThe ART data relate to women treated in the state of
Victoria by any ofthree infertility services: Melbourne IVF, Monash
IVF and the MelbourneAssisted Conception Centre (MACC) between
January 1991 andDecember 2004. Only the subjects rst singleton
birth during the studyperiod were included. This is a retrospective
cohort study using recordlinkage to obtain the information on
obstetric haemorrhages in infertilewomen conceiving after IVF or
ICSI and three comparison groups:women conceiving in the general
community and infertile womenconceiving by GIFT or without ART.
In vitro fertilization/intracytoplasmic sperm injectionFor this
group, oocytes were collected by transvaginal ultrasound
guidedoocyte collections under neurolept or general anaesthesia.
ICSI was intro-duced in 1993. Treatment of male infertility was
attempted with standardIVF before the introduction of ICSI.
Stimulation regimens involved clomi-phene, human menopausal
gonadotrophin and human chorionic gonado-trophin up to 1993. The
oral contraceptive pill was used increasinglyafter 1995 to regulate
the starting time of gonadotrophin treatment.Long down-regulation
with gonadotrophin releasing hormone agonistswas used after 2001.
Recombinant FSH was used after 1994. Gonado-trophin releasing
hormone antagonists were used in increasing numbersof patients
after 2000.
Culture media changed from human tubal uid to multi-stage media
in2000. The protein supplement was human serum albumin until 2000
andhighly puried albumin thereafter. Embryo cryopreservation
involved pro-panediol with embryo freezing on day 2, 3 or 5.
Cryopreserved embryoswere thawed and transferred on the same day as
their age after ovulationin natural or articial cycles until 1996.
After September 1997, all cryopre-served embryos were thawed the
day before transfer and cultured over-night so they would be on
average 18 h more advanced than embryostransferred fresh.
Frozen-thawed ET (FET) was usually performed innatural menstrual
cycles but women with oligomenorrhoea or amenor-rhoea had articial
cycles induced with cyclical estradiol and progesteronetreatment.
Some other patients had luteal phase support with hCG
orprogesterone. During the time of the study relatively low numbers
ofembryos were transferred and the multiple pregnancy rate was
,20%.Embryo cryopreservation was common and approximately one third
ofthe singleton births were from FET.
National health funding of ART covered about half of the
patients costs.Patients without private health insurance or their
own specialist gynaecol-ogist were classied as semiprivate and this
is an indicator of socio-economic status.
General populationFor each IVF/ICSI subject, three records of
singleton births were randomlyselected from the PDCU data matching
on year of maternal age and yearof birth of the baby to balance the
exposed and unexposed groups on
266 Healy et al.
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
maternal age and possible temporal changes in ascertainment of
the obste-tric haemorrhages.
Gamete intrafallopian transferThe results of singleton births
from GIFT were analysed to determine if thein-vitro fertilization
and embryology laboratory procedures contributed tothe outcome, as
these do not occur with GIFT. GIFT was performedunder general
anaesthesia and involved laparoscopic placement of theoocytes and
spermatozoa into the ampulla of a uterine tube via the m-brial end
of the tube. Most of the GIFT was performed between 1990and 1998.
Except at one centre (MACC), extra oocytes not transferredwere
inseminated and embryos resulting were cryopreserved.
Non-ARTInfertile women who conceived without ART (non-ART group)
were ana-lysed to determine the contribution of infertility itself
to the outcomes.The women were classied as infertile because they
were seen in theMelbourne or Monash clinics between 1991 and 2000
but were knownnot to have given birth after IVF, ICSI, GIFT or
donor insemination atthe three Melbourne clinics. They were found
in the Victorian PDCUbirth data to have given birth to a singleton
baby within 5 years of regis-tration at the clinics. They may or
may not have had ART treatment butany ART treatments did not result
in a birth after 20 or more weeks ges-tation. Some patients may
have been treated by ovulation induction orarticial insemination
but most would have naturally conceived. The possi-bility that they
had conceived by ART at other clinics interstate or overseaswas
checked by inspection of the patient records. The three
Melbourneclinics performed most of the ART procedures in the State
during thetime of the study (.98% of clinical pregnancies,
www.ita.org.au) andreproductive tourism was infrequent.
ExclusionsDonor oocyte and embryo recipients (n 339) were
excluded. Bychance, some women in the IVF/ICSI, GIFT and non-ART
groups whoalso had naturally conceived children were matched with
other IVF/ICSIgroup subjects. Similarly some women with more than
one birth werein the general population group. All these second and
subsequent preg-nancies in the study groups were excluded so that
each woman wasonly analysed once thus avoiding correlations between
outcomes thatmight otherwise occur.
Primary outcome: haemorrhagesThe obstetric haemorrhages were
dened using the Victorian PDCU elec-tronic user manual. APH was
coded when bleeding of 15 ml or moreoccurred from the birth canal
after 20 weeks gestation and before thebirth of the baby. This
overarching category includes PP, PA and APHfor other reasons. PP
was coded where the placenta was located overor very close to the
cervical os as veried by independent ultrasoundexamination and
conrmed at birth. APH may or may not have occurred.The standardized
form sent to the PDCU does not differentiate betweenmarginal PP
(grade I) from more major PP (grade II III) to grade IV PPwhich
cover the internal cervical os. PA was coded where there was
pre-mature separation of the placenta. There was evidence of
retroplacentalbleeding and the amount of blood lost was always
moderate or severewhether out of the vagina or internally. PPH was
coded when there wasblood loss greater than 500 ml within 24 h of
vaginal delivery or childbirthor greater than 750 ml after
Caesarean section. The PDCU denitions areconsistent with the
International Classication of Diseases (ICD10) codingsystem. In
this study, six women had both PP and PA. Also 70 women withPP had
no bleeding and were not classied as having APH.
Record linkageWith the aid of a computer programme, LinkageWiz,
probabilistic recordlinkage was used to match the ART data to the
PDCU common identifyingvariables: name, date of birth and postcode
(Tayor, 1998). Once recordlinkage was complete, IVF clinical data
were used to ensure matches to sin-gleton births were correct.
Cross-checking between the Victorian ARTclinics was done to ensure
the birth was not the result of ART atanother clinic. Data were
extracted for rst singleton births within thestudy period of
greater than 19 weeks gestation for the groups: IVF/ICSI (6730),
population control (24 619), GIFT (779) and non-ART(2167).
Stillbirths, late terminations and neonatal deaths (within 28
daysof birth) were included.
Data analysisThe background characteristics of the births in
each of the four compari-son groups were described using means and
ranges for quantitative vari-ables and percentages for categorical
variables. The proportions ofAPH, PP, PA and PPH in each group were
compared between the IVF/ICSI group and each of the general
population, GIFT and non-ARTgroups using the x2 test. Logistic
regression was performed usingGenStat 11th Edition (McCullagh and
Nelder, 1989) to compare theodds of each complication between the
IVF/ICSI and general populationgroups in unadjusted analyses and
analyses adjusted for potential confoun-ders: age, year of birth of
baby, marital status, parity, previous miscarriageor termination of
pregnancy, country of birth and vertex presentation(Model 1). Also
giving birth in tertiary, private or other maternity hospitalswas
also included with the other factors in model (Model 2). For PPH,
theeffect of adjusting for other complications of pregnancy:
pre-eclampsia,APH, PP, PA, premature rupture of membranes and
induced labour,were added to Models 1 and 2. Also, because of the
different denitionsof post-partum haemorrhage for vaginal and
Caesarean section deliveries,these were examined separately.
To determine which factors within the IVF/ICSI group were
indepen-dently related to obstetric haemorrhages, causes of
infertility, ovarianstimulation, fertilization procedure (IVF or
ICSI), transfer of fresh orfrozen embryos, number of embryos
transferred, average embryoquality, average cell number, luteal
phase support and number of fetalhearts were examined by logistic
regression to adjust for the potential con-founders listed above.
Graphs were plotted to check the linearity andnature of the
relationships between the data and the t of the models.Additional
analyses were performed omitting factors which might be aneffect of
the obstetric complication being studied, such as birth in a
tertiarymaternity hospital, to determine if these affected the
relationship betweenthe ART or infertility factor and the
end-point. To study the possibleeffects of ovarian stimulation,
oocyte numbers, fertilization rate andembryo numbers, and births
resulting from fresh embryo transfer wereanalysed separately.
Similarly, FET was analysed separately to examinefactors specic to
this group such as the effects of natural and articialcycles and
overnight culture of embryos after thawing.
Results
IVF/ICSI group compared with the controlgroupsThe main
differences in characteristics in the subjects in the groups
aresummarized in Table I. Compared with the IVF/ICSI group,
thegeneral population group were more likely to be born in Asia or
theMiddle East and migrated to Australia, to have previous
pregnanciesand to have a vertex presentation, and less likely to be
married,
Increased obstetric haemorrhage after ART 267
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
give birth in a private hospital, have an induced labour or have
an Cae-sarean section. Compared with the IVF/ICSI group, the GIFT
patientswere slightly younger, more often married, treated earlier
in the studyperiod and less likely to have Caesarean sections. The
non-ART groupwere younger, more often born in Asia or the Middle
East, more likelyto have previous pregnancies, miscarriages and
termination of preg-nancy, and less likely to use a private
hospital and have a Caesareansection than the IVF/ICSI group. The
IVF/ICSI group had higherrates of all the haemorrhagic
complications than the general popu-lation (Table II). For GIFT,
APH was more frequent than in the IVF/ICSI group, whereas
frequencies of PP and PA were similar and post-partum haemorrhage
was less frequent than in the IVF/ICSI group.The non-ART group had
frequencies of these complications inter-mediate between those in
the general population and the IVF/ICSIgroup (Table II).
The IVF/ICSI group had more of the obstetric haemorrhage
com-plications than the general population group. The ORs changed
littlefor APH, PP, PA and other APHs after the adjustments for
confoun-ders were made (Table III). For post-partum haemorrhage,
adjustingfor covariates reduced the OR. The factors producing the
greatestchange in the OR were parity and Caesarean section.
Analysing
vaginal deliveries and Caesarean section births separately
producedsimilar results. Thus there is some evidence for an
additional effectof IVF/ICSI on post-partum haemorrhage independent
of theincreases in other maternal complications of pregnancy. The
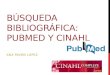
differencein the frequencies of the haemorrhages in Primiparous
women in theIVF/ICSI group and in the general population group, by
age, is shownin Fig. 1.
Factors within the IVF/ICSI group affectingthe risk of the
haemorrhagic complicationsFresh versus frozen-thawed embryo
transfersAPH was more frequent with fresh embryo transfer than with
FET(Tables IV and V). Adjusting for other covariates made little
differenceto the OR for fresh embryo transfer versus FET. The weak
evidence(P 0.10.01) for effects of female infertility, tubal
disease, threeor more embryos transferred and luteal phase support
with hCGwas lost when fresh embryo transfer versus FET was included
in theregression models. The data for PA were sparse (not shown)
butthere was moderately strong evidence (P 0.01) that PA was
morefrequent with fresh embryo transfer (49/422, 1.2%) than with
FET
.............................................................................................................................................................................................
Table II Obstetric haemorrhages: APH, PP, PA and PPH in IVF/ICSI
and general population, GIFT and Non-ART groups
Complication IVF/ICSI (6730) General Population (24 619) GIFT
(779) Non-ART (2167)
APH 454 (6.7) 881 (3.6), P, 0.001 78 (10.0), P 0.001 98 (4.5),
P, 0.001PP 174 (2.6) 273 (1.1), P, 0.001 21 (2.7), P 0.85 26 (1.2),
P, 0.001PA 63 (0.9) 107 (0.4), P, 0.001 11 (1.4), P 0.20 13 (0.6),
P 0.14PPH 746 (11.1) 1954 (7.9), P, 0.001 54 (6.9), P, 0.001 192
(8.9), P 0.003
APH, antepartum haemorrhage; PA, placental abruption; PP,
placenta praevia; PPH, primary post-partum haemorrhage; GIFT,
gamete intro-fallopian transfer.The number and (%) in each group is
shown with the P-value for the comparison with the IVF/ICSI
group.
.............................................................................................................................................................................................
Table I Characteristics of the subjects
Characteristic IVF/ICSI General population GIFT Non-ART
Number 6730 24 619 779 2167
Age 34 (2045) 34 (2050) 33 (2346) 33 (1947)
COB Asia or ME* 641 (9.5) 3100 (12.6) 54 (6.9) 273 (12.6)
Married 6326 (94.0) 20 345 (82.6) 766 (98.3) 2048 (94.5)
Gravidity 0.8 (016) 1.8 (022) 0.7 (06) 1.1 (013)
Parity 23 1345 (20.0) 13 880 (56.4) 174 (22.3) 530 (24.4)
.3 122 (1.8) 3204 (13.0) 8 (1.0) 39 (1.8)
Any abortions** 2013 (29.9) 8790 (35.7) 197 (25.3) 898
(41.4)
Tertiary hospital 1566 (23.3) 5381 (21.8) 207 (26.6) 488
(22.5)
Private hospital 3941 (58.6) 8528 (34.6) 437 (56.1) 1184
(54.6)
Year of birth 1999 (19912004) 1999 (19912004) 1995 (19912004)
1997 (19912004)
Vertex presentation 6143 (91.3) 23 126 (93.9) 703 (90.2) 1995
(92.1)
Induced labour 2138 (31.8) 6383 (25.9) 214 (27.5) 644 (29.7)
Caesarean section 2681 (39.8) 6689 (27.2) 236 (30.3) 763
(35.2)
The number and (%) or mean and (range) is shown.*COB: country of
birth; ME: middle East **Abortions include miscarriages and
terminations of pregnancy before 20 weeks gestation.
268 Healy et al.
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
(14/2503, 0.6%), OR 2.1 (1.23.7), Model 2 adjusted OR 2.1
(1.23.9). There was also some evidence that fresh transfers were
associ-ated with increased PP, but with less post-partum
haemorrhage, indi-cating increased rates of post-partum haemorrhage
with FET(Table IV).
The results for fresh embryo transfer in FSH stimulated cycles
(freshtransfers in natural cycles excluded) and for FET in natural
cycles (arti-cial cycles excluded) are compared in Table V. There
were more
APH and PA after fresh embryo transfer. There was also a trend
tohigher PP with the fresh transfers but no evidence of a
difference inthe frequency of post-partum haemorrhage with fresh
embryo transferor FET.
Number of oocytes collected before fresh embryo
transfersAnalysing the results of fresh embryo transfer alone
produced moder-ate evidence for an increase in frequency of APH
with the number of
.............................................................................................................................................................................................
Table III Odds ratios of obstetric haemorrhages: APH, PP, PA and
PPH in the IVF/ICSI group compared with the generalpopulation group
unadjusted and adjusted for possible confounding
OR (95% CI), P-value Model 1 Ad OR (95% CI), P-value Model 2 Ad
OR (95% CI), P-value
APH 1.95 (1.732.19), ,0.001 1.98 (1.732.26)*, ,0.001 2.04
(1.782.33)*, ,0.001
PP 2.37 (1.952.87), ,0.001 2.27 (1.822.83)*, ,0.001 2.34
(1.872.92)*, ,0.001
PA 2.16 (1.582.96), ,0.001 2.02 (1.412.88)*, ,0.001 2.07
(1.442.98)*, ,0.001
Other APH 1.59 (1.361.85), ,0.001 1.67 (1.401.99)*, ,0.001 1.74
(1.462.07)*, ,0.001
PPH 1.45 (1.321.58), ,0.001 1.19 (1.071.32)$, ,0.001 1.28
(1.161.42)$, ,0.001
Vaginal PPH 1.46 (1.291.65), ,0.001 1.18 (1.031.35)#, 0.02 1.24
(1.081.42)#, 0.002
Caesarean PPH 1.23 (1.071.40), 0.002 1.18 (1.011.38)#, 0.03 1.31
(1.121.54)#, ,0.001
APH, antepartum haemorrhage; PA, placental abruption; PP,
placenta praevia; PPH, primary post-partum haemorrhage.*Model 1
adjusted for age, year of birth, marital status, parity, any
miscarriages or terminations of pregnancy and vertex presentation.
Model 2 adjusted in addition for tertiary and privatehospital
status.$Model 1 adjusted for age, year of birth, marital status,
parity, any miscarriages or terminations of pregnancy, vertex
presentation, pre-eclampsia, APH, PP, PA, premature rupture
ofmembranes, induced labour, Caesarean section. Model 2 adjusted in
addition for tertiary and private hospital status.#Model 1 adjusted
for age, year of birth, marital status, parity, any miscarriages or
terminations of pregnancy, vertex presentation, pre-eclampsia, APH,
PP, PA, premature rupture ofmembranes, induced labour. Model 2
adjusted in addition for tertiary and private hospital status.
Figure 1 The effect of maternal age on the frequency of
obstetric haemorrhage: APH, PP, PA and PPH in Primiparous women in
the IVF/ICSI andgeneral population groups (error bars indicate the
95% CI). APH, antepartum haemorrhage; PA, placental abruption; PP,
placenta praevia; PPH,primary post-partum haemorrhage.
Increased obstetric haemorrhage after ART 269
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
.................................................................
................................................................
.................................................................
..........................................................................................................................................................................................................................................................
Table IV Factors in IVF/ICSI group related to APH, PP and
PPH
Factors Total APH PP PPH
n (%) OR (95% CI) Ad OR (95% CI)* n (%) OR (95% CI) Ad OR (95%
CI)* n (%) OR (95% CI) Ad OR (95% CI)$
Not female infertility 3274 195 (6.0) 1 1 67 (2.0) 1 1 332
(10.1) 1 1
Female infertility 3456 259 (7.5) 1.28 (1.061.55) 1.27
(1.051.55) 107 (3.1) 1.53 (1.122.08) 1.55 (1.132.12) 414 (12.0)
1.21 (1.041.40) 1.14 (0.971.33)
Not endometriosis 5465 356 (6.5) 1 1 126 (2.3) 1 1 581 (10.6) 1
1
Endometriosis 1265 98 (7.7) 1.20 (0.951.52) 1.21 (0.951.53) 48
(3.8) 1.67 (1.192.34) 1.65 (1.182.32) 165 (13.0) 1.26 (1.051.52)
1.28 (1.061.56)
Not ovulatory 5742 380 (7.7) 1 1 145 (2.5) 1 1 610 (10.6) 1
1
Ovulatory disorder 988 74 (6.5) 1.14 (0.881.48) 1.14 (0.871.48)
29 (2.9) 1.17 (0.781.75) 1.14 (0.751.74) 136 (13.8) 1.34 (1.101.64)
1.27 (1.031.57)
Not tubal 5076 320 (6.3) 1 1 122 (2.4) 1 1 564 (11.1) 1 1
Tubal disease 1654 134 (8.1) 1.31 (1.0621.62) 1.34 (1.0821.67)
52 (3.1) 1.32 (0.951.83) 1.41 (1.001.98) 182 (11.0) 0.99 (0.831.18)
0.94 (0.781.13)
IVF 3340 232 (6.9) 1 1 95 (2.8) 1 1 376 (11.3) 1 1
ICSI 3390 222 (6.5) 0.94 (0.781.14) 0.89 (0.721.09) 79 (2.3)
0.82 (0.601.10) 0.72 (0.521.00) 370 (10.9) 0.96 (0.831.12) 0.94
(0.801.12)
Fresh transfer 4227 321 (7.6) 1.46 (1.1921.80) 1.46 (1.181.80)
123 (2.9) 1.44 (1.042.00) 1.40(1.001.95) 432 (10.2) 0.79 (0.680.92)
0.81(0.690.95)
FET 2503 133 (5.3) 1 1 51 (2.0) 1 1 314 (12.5) 1 1
Number transferred 1 1024 73 (7.1) 1.11 (0.861.45) 1.06
(0.811.38) 29 (2.8) 1.16 (0.771.75) 1.08 (0.711.65) 118 (11.5) 1.02
(0.831.27) 1.00 (0.801.25)
Number transferred 2 4807 310 (6.4) 1 1 118 (2.4) 1 1 542 (11.3)
1 1
Number transferred .2 899 71 (7.9) 1.24 (0.951.63) 1.37
(1.031.80) 27 (3.0) 1.23 (0.801.88) 1.42 (0.912.22) 86 (9.6) 0.83
(0.661.06) 0.88 (0.691.14)
Average cell number ,4 887 66 (7.4) 1.12 (0.841.50) 1.16
(0.861.56) 26 (2.9) 1.23 (0.781.95) 1.30 (0.822.08) 94 (10.6) 0.95
(0.741.21) 0.94 (0.731.21)
Average cell number 4 2804 188 (6.7) 1 1 67 (2.4) 1 1 312 (11.1)
1 1
Average cell number .4 2050 139 (6.8) 1.01 (0.811.27) 1.04
(0.821.30) 61 (3.0) 1.25 (0.881.78) 1.26 (0.881.79) 232 (11.3)
1.02(0.851.22) 1.07(0.891.29)
Unknown 989 61 (6.2) 0.91 (0.681.23) 1.01 (0.711.43) 20 (2.0)
0.84 (0.511.39) 1.02 (0.571.82) 108 (10.9) 0.98(0.781.23)
1.01(0.761.34)
Luteal phase hCG 1345 104 (7.7) 1.28 (1.011.62) 1.31 (1.031.67)
41 (3.0) 1.20 (0.831.72) 1.26 (0.871.82) 115 (8.6) 0.70 (0.570.86)
0.72 (0.580.90)
Progesterone 1200 93 (7.8) 1.28 (1.001.64) 1.26 (0.981.61) 26
(2.2) 0.84 (0.551.30) 0.82 (0.531.27) 138 (11.5) 1 1
None 4185 257 (6.1) 1 1 107 (2.6) 1 1 493 (11.8) 0.97(0.801.19)
0.93(0.761.15)
Fetal heart 1 6456 439 (6.8) 1 1 169 (2.6) 1 1 719 (11.1) 1
1
Fetal heart .1 274 15 (5.5) 0.79 (0.471.35) 0.79 (0.461.34) 5
(1.8) 0.69 (0.281.68) 0.69 (0.281.70) 27 (9.8) 0.87 (0.581.31) 0.86
(0.571.30)
APH, antepartum haemorrhage; PA, placental abruption; PP,
placenta praevia.*Adjusted for age, year of birth, country of birth
Asia and Middle East, marital status, parity, any miscarriages or
terminations of pregnancy, vertex presentation, tertiary and
private hospital status (Model 2).$Adjusted for age, year of birth,
country of birth Asia and Middle East, marital status, parity, any
miscarriages or terminations of pregnancy, vertex presentation,
tertiary and private hospital status, pre-eclampsia, APH, PP, PA,
premature rupture ofmembranes, induced labour, Caesarean section
(Model 2).
270Healy
etal.
by guest on February 24, 2014 http://humrep.oxfordjournals.org/
Downloaded from
-
oocytes collected (,6 oocytes 51/897, 5.7%; 69 oocytes
93/1220,7.6%; 1013 oocytes 77/947, 8.1%; .13 oocytes 100/1163,
8.6%,P 0.009).
Infertility diagnosis: endometriosis and ovulatory disordersPP
and post-partum haemorrhage were increased with
endometriosis.Adding the other IVF/ICSI factors to the models did
not change theOR greatly: PP 1.7 (1.22.4) and post-partum
haemorrhage 1.3(1.11.6). Post-partum haemorrhage was also
moderately stronglyassociated with ovulatory disorders and this
continued after addingthe other IVF/ICSI factors to the model [OR
1.3 (1.11.6)].
Hormone treatmentPost-partum haemorrhage was less frequent when
hCG was used forluteal phase support. Adding the other IVF/ICSI
covariates did notchange the OR greatly [0.7 (0.60.9)].
Analysing only the frozen embryo transfer results showed
strongevidence (P, 0.001) for an increase in post-partum
haemorrhagewith FET in articial cycles compared with natural cycles
[OR 2.2(95% CI 1.62.9), Adjusted OR 1.8 (1.32.6)]. There were 93
post-partum haemorrhages following 458 FET in articial cycles
(20.3%) and221 post-partum haemorrhages in 2045 FET in natural
cycles (10.8%).
Factors within the IVF/ICSI group without strong evidence of
anassociation with the haemorrhagic complicationsOther factors
analysed, including number of previous oocyte collec-tions or ETs,
types of ovarian stimulation and drugs used, source ofsperm,
overnight culture of embryos, maternal height, smoking andobesity
(for which data were incomplete), showed no evidence ofassociation
with APH, PP or post-partum haemorrhage (P . 0.1).
DiscussionThis large, multi-centre study shows increased rates
of obstetric haem-orrhage in mothers of singleton ART babies. Our
results add to infor-mation in national and international studies
(Dickey, 2007; Halliday,2007; Anderson et al., 2008). It has been
hitherto uncertainwhether the increases in these complications are
caused by factorsintrinsic to the ART procedures or factors related
to the character-istics of the ART-seeking population. We have
interrogated our data
to address this question and examined possible mechanisms
forthese adverse outcomes.
The GIFT women were different because this group was small
innumber, younger, treated earlier and more often married than
theIVF/ICSI group. They also had less Caesarean sections
probablyrelated to the increasing rate of Caesarean section over
the time ofthe study. The GIFT method of treatment has become less
popularover time with improvements in the results of IVF. Although
theyhad less post-partum haemorrhage than the IVF/ICSI group,
theyhad the same or higher rates of APH, PP and PA (Table II). The
sig-nicance of this is that in contrast to IVF and ICSI, embryos
are notformed in vitro with GIFT. The oocytes and sperm are
introducedinto the outer end of the uterine tube and fertilization
and earlyembryo cleavage occurs in vivo. GIFT was also usually used
incouples with unexplained infertility. The fact that APH is not
less fre-quent with GIFT than with IVF and ICSI indicates that it
is not the fer-tilization and embryo manipulation within the
laboratory that isresponsible for the increased frequency of APH in
the IVF/ICSIgroup. Furthermore, the adverse APH results with GIFT
are also evi-dence that it is not the trans-cervical embryo
transfer with low place-ment of embryos into the uterus that
increases the risk of APH andparticularly PP, as previously
suggested (Smithers et al., 2003;Romundstad et al. 2006). In
contrast, as IVF/ICSI and GIFT areboth undertaken during a
stimulated cycle, factors common to bothprocedures such as ovarian
stimulation, or anaesthesia and surgeryfor oocyte collection may be
implicated in the adverse outcomes.
The non-ART group had fewer of the haemorrhages than the
IVF/ICSI group. From these data there is inconclusive evidence
ofincreased rates of obstetric haemorrhages related to
infertility;however, it is likely this group of patients had less
severe infertilitythan did those in the IVF/ICSI group. It is
possible but unlikely thatsome of these patients may have conceived
by ART interstate or over-seas. As this would bias this groups
results towards more haemor-rhages, we conclude there appears to be
adverse effects of IVF/ICSIincreasing the haemorrhagic
complications separate from theinfertility.
Having conrmed higher frequencies of APH and
post-partumhaemorrhage with ART, we were interested to determine if
the differ-ences in characteristics between subjects in the
IVF/ICSI and generalpopulation groups would account for some or all
of the effect.
.............................................................................................................................................................................................
Table V Obstetric complications in IVF/ICSI patients with fresh
embryo transfer (embryo transfer) in a stimulated cycleor FET in a
natural cycle [number (%), unadjusted and adjusted odds ratios and
95% CI with FET as reference]
Group APH PP PA PPH
Stimulated cycle: fresh embryo transfer(N 4058)
314 (7.7) 122 (3.0) 46 (1.1) 417 (10.3)
Unstimulated cycle: FET (N 2045) 105 (5.1) 44 (2.2) 9 (0.4) 221
(10.8)OR (95% CI), P-value 1.55 (1.231.94), ,0.001 1.41 (1.001.99),
0.05 2.59 (1.295.18), 0.007 0.94 (0.801.12), 0.52
Ad OR (95% CI), P-value 1.53 (1.221.93)*, ,0.001 1.37
(0.961.95)*, 0.08 2.56 (1.255.27)* 0.01 0.94 (0.781.22)$, 0.49
APH, antepartum haemorrhage; PA, placental abruption; PP,
placenta praevia; PPH, primary post-partum haemorrhage, FET, frozen
thawed embryo transfer.*Adjusted for age, year of birth, country of
birth Asia and Middle East, marital status, parity, any
miscarriages or terminations of pregnancy, vertex presentation,
tertiary and private hospitalstatus (Model 2).$Adjusted for age,
year of birth, country of birth Asia and Middle East, marital
status, parity, any miscarriages or terminations of pregnancy,
vertex presentation, tertiary and private hospitalstatus,
pre-eclampsia, APH, PP, PA, premature rupture of membranes, induced
labour, Caesarean section (Model 2).
Increased obstetric haemorrhage after ART 271
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
Although we matched the general population group and the
IVF/ICSIsubjects by age of mother and date of birth, this left some
importantdifferences between the two groups particularly in
gravidity and parity.Also the IVF/ICSI group delivered by Caesarean
section more often.Adjusting for confounding left the ORs for APH
either unchanged orincreased (Table III). In contrast, for
post-partum haemorrhage, theORs decreased with adjustments for the
other factors particularlyparity, Caesarean section and other
maternal complications(Table III). Thus some of the higher
frequency of post-partum haem-orrhage after IVF/ICSI is explained
by differences in the characteristicsof women having these
treatments from those in the general commu-nity, particularly their
lower parity and higher use of Caesareansection. However, there
remained some evidence of a small excessof post-partum haemorrhage
related to some other aspect of IVF/ICSI.
Having conrmed an increase in the obstetric haemorrhages
specicto IVF/ICSI, we then analysed the IVF/ICSI group on its own
toexplore which factors were related to the higher frequencies of
thehaemorrhages. We found that APH, PP and PA were higher withfresh
embryo transfer than with FET, and within the fresh embryotransfer
treatments, APH increased with the numbers of oocytes col-lected.
PP and post-partum haemorrhage were increased in subjectswith
endometriosis. Post-partum haemorrhage was also more fre-quent in
women with ovulatory disorders, but less frequent whenhCG had been
used for luteal phase support. Post-partum haemor-rhage was more
frequent with FET treatments in articial cyclesthan with FET in
natural cycles. It is possible that some of thesenew ndings may be
statistically signicant by chance alone and theyneed conrmation by
analysis of separate datasets. Also it is difcultto know if these
signicant associations reect direct mechanisms orresult from a
peripheral relationship. For example the luteal phasehCG and FET in
articial cycle effects maybe more related to thecharacteristics of
the patients having these treatments than to thetreatments
themselves. However, if these ndings are true theremay be important
implications and some speculation on the possiblemechanisms, is
useful for further studies.
Therewas a greater risk of APH after fresh embryo transfer in a
stimu-lated cycle than FET in a natural cycle (Tables IV and V).
This increase inAPH in general with fresh embryo transfer in
stimulated cycles is particu-larly interesting. Differences in
outcome of singleton births after freshembryo transfer and FET have
been noted for birthweight, pretermbirth, perinatal death and some
birth defects (Sutcliffe et al., 1995;Wen-nerholm et al., 1998;
Aytoz et al., 1999; Kallen et al., 2005a; Olson et al.,2005; Belva
et al., 2008; Shih et al., 2008). These differences are
intri-guing, as they must result from either embryonic effects,
with cryopre-servation improving the outcomes by exerting some
selective effect forbetter embryos, or adverse effects occurring in
the mother in freshembryo transfer cycles that are not present with
FET. The latter maybe related to ovarian stimulation and oocyte
collection.
Anaesthesia or monitored conscious sedation for oocyte
collectionseems unlikely to explain the differences observed
between stimulatedand natural ART cycles. The initial half-life of
anaesthetic medicinessuch as propofol is only 24 min: embryo
transfer is typically 25days after anaesthesia. Moreover,
anaesthetic agents are not thoughtto act on the endometrium.
The increase in APH following fresh embryo transfer with the
numberof oocytes is a particularly important indicator that ovarian
stimulation is
involved. Oocyte number is related to the dose of FSH used and
theovarian responsiveness of the woman. Estradiol and
progesteronelevels at the time of implantation in fresh embryo
transfer cycleswould be expected to be associated with oocyte
number. It may bethat excessive ovarian hormone levels with
multiple follicular develop-ments interfere with the endometrium
during implantation and increasethe risk of APH and PA. We have
recently shown that the endometrialprotein, pregnancy associated
plasma protein A (PAPP-A) is low in preg-nancies after fresh embryo
transfer in stimulated cycles (Amor et al.,2009). PAPP-A is a zinc
binding matrix metalloproteinase. PAPP-Ahelps regulate
extracellular matrix remodelling. This is vital in angiogen-esis
and the establishment of placentation during the early weeks
ofpregnancy. Our nding of increased APH after fresh embryo
transferin stimulated ART cycles suggest that the high estradiol
and progester-one concentrations, as a result of multiple
folliculogenesis, produce sub-optimal angiogenesis and
placentation.
The diagnosis of endometriosis was associated with more PP
andpost-partum haemorrhage. Although PP was also associated
withhigher PPH, there was evidence that the effect of
endometriosisincreased the risk of both complications. We recently
reportedother potential obstetric consequences of endometriosis for
ART:ovarian endometriosis is associated with approximately
doubledrates of preterm birth and small for gestational age babies
(Fernandoet al., 2009).
The less frequent post-partum haemorrhage with luteal phase
hCGalso suggests a disturbance of endometrial function around the
time ofimplantation is involved in increasing PPH. In addition it
suggests thatimproved management of luteal phase support in ART
patients mayhave a benecial effect. With FET there was more PPHs
with the arti-cial cycles. This may be related directly to the
hormone treatmentbeing less effective in preparing the endometrium
for implantationcompared with natural cycles or, alternatively, the
ovulatory disorderin the patients requiring articial cycles may be
responsible. Ovulatorydisorders were also associated with increased
post-partumhaemorrhage.
The strengths of this study are the large study population
anddetailed information available on the treatments from the three
infer-tility services and birth outcomes from the State PCDU
database. Theresults of IVF/ICSI patients were compared with those
of populationcontrols, GIFT and non-ART conceptions in infertile
women. Indepen-dent midwives, not ART clinic staff, recorded all
obstetric data and thisshould minimize ascertainment bias. During
the study period relativelylow numbers of embryos were transferred,
the multiple pregnancyrate was less that 20% and there were few
vanishing twins. The analy-sis of singleton births only and the
high usage of FET is different frommost other data for this time
with higher multiple pregnancy rates. Wecould therefore study the
inuence of ovarian stimulation by compar-ing fresh embryo transfer
with FET in a natural or non-stimulatedcycle. We also assessed the
effects of different methods of stimulationand a marker of the
effect of stimulation: the number of oocytes col-lected before a
fresh embryo transfer. To avoid the problem of analy-sis of
subsequent pregnancies in the same woman and the high withinsubject
correlations with repeated complications in subsequent
preg-nancies, for each woman only the rst birth within the study
periodwas analysed.
There are a number of limitations. The quality of the data is
variable.For example, there were inevitable time-related changes
over the
272 Healy et al.
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
15 years of data collection, with differences in approach to
diagnosisand procedures with the evolution of ART. There were not
manywomen with PA. There was no information on covariates such
asmaternal weight or smoking during pregnancy in the general
popu-lation group and this was also incomplete in the IVF/ICSI
group.Another problem with these data is that we have no
information ofprevious pregnancy complications particularly
previous Caesareansection, which increases the risk of PP in
subsequent pregnancies.We were not able to analyse these factors.
Nevertheless, as 78% ofthe IVF/ICSI patients were primiparous
(Table I), we might haveexpected to see a higher rate of past
Caesarean sections in thegeneral population group thereby producing
more PP cases: weobserved the opposite. Thus it is not possible to
treat the results asif they were from a clinical trial with random
placement of couplesin separate treatment groups or from a
hypothesis based study, andconclusions on cause and effect need to
be guarded.
In conclusion, all the obstetric haemorrhages are more
frequentafter IVF/ICSI than in the general population. For
post-partum haem-orrhage, some of the increase is related to the
IVF/ICSI patientshaving fewer previous pregnancies and using
Caesarean sectionmore. As these complications are less frequent in
non-ART con-ceptions in infertile women, the mechanism of the
increase mustinvolve some aspects of the IVF/ICSI treatment. As APH
is not lessfrequent with GIFT, embryology procedures and embryo
placementthrough the cervix do not appear to be important.
Exploratory analysisof factors in the IVF/ICSI group suggests
events around the time ofimplantation are responsible for the
increase in subsequent obstetrichaemorrhages. The increased APH
with fresh embryo transfer andwith greater numbers of oocytes
collected, and the protective effectof hCG luteal phase support and
the adverse effect of ovulatory dis-orders and articial cycles for
FET on PPH all indicate that suboptimalendometrial function around
the time of implantation is critical.
Authors RolesAll authors have contributed to the conducting of
this study. Themanuscript has been seen and approved by all
authors. D.L.H.,H.W.G.B. and J.H. were the senior investigators
involved in studydesign, method investigations, data analysis and
preparation of themanuscript. S.B., A.J., D.R. and C.G. were
involved in method inves-tigation, data checking and analysis and
review of the manuscript.J.M.T. was involved in data provision.
AcknowledgementsThe authors thank Obi Ukoumunne, Odette Taylor,
Gillian Wheatleyand Associate Professor James King at the Perinatal
Data CollectionUnit for assistance. We acknowledge the nancial
support from theBUPA Foundation and the Fertility Society of
Australia.
FundingJ.H. Senior Research Fellowship is funded by the National
Health &Medical Research Council (436904).
ReferencesAmor DJ, Xu JX, Halliday J, Francis L, Healy DL,
Breheny S, Baker HW,Jaques A. Pregnancies conceived using assisted
reproductivetechnologies (ART) have low levels of pregnancy
associated protein-A(Papp-A) leading to a high rate of false
positive results in rsttrimester screening for Down syndrome. Hum
Reprod 2009;24:13301338.
Anderson AN, Goossens V, Ferraretti AP, Bhattacharya S,
Felberbaum R,de Mouzon J, Nygren KG, (ESHRE) EI-mECESoHRaE.
Assistedreproductive technology in Europe, 2004: results generated
fromEuropean registers by ESHRE. Hum Reprod 2008;23:756771.
Aytoz A, Van den Abbeel E, Bonduelle M, Camus M, Joris H,
VanSteirteghem A, Devroey P. Obstetric outcome of pregnancies
afterthe transfer of cryopreserved and fresh embryos obtained
byconventional in-vitro fertilization and intracytoplasmic sperm
injection.Hum Reprod 1999;14:26192624.
Belva F, Henriet S, Van den Abbeel E, Camus M, Devroey P, Van
der Elst J,Liebaers I, Haentjens P, Bonduelle M. Neonatal outcome
of 937 childrenborn after transfer of cryopreserved embryos
obtained by ICSI and IVFand comparison with outcome data of fresh
ICSI and IVF cycles. 2008;23:22272238.
Daniel Y, Ochshorn Y, Fait G, Geva E, Bar-Am A, Lessing JB.
Analysis of104 twin pregnancies conceived with assisted
reproductive technologiesand 193 spontaneously conceived twin
pregnancies. Fertil Steril 2000;74:683689.
Dickey R. The relative contribution of assisted reproductive
technologiesand ovulation induction to multiple births in the
United States 5 yearsafter the Society for Assisted Reproductive
Technology/AmericanSociety for Reproductive Medicine recommendation
to limit thenumber of embryos transferred. Fertil Steril
2007;88:15541561.
Fernando S, Breheny S, Jaques AM, Halliday JL, Baker G, Healy D.
Pretermbirth, ovarian endometriomata, and assisted reproduction
technologies.2009;91:325330.
Halliday J. Outcomes of IVF conceptionsare they different? Best
Pract ResClin Obstet Gynaecol 2007;21:6781.
Jackson RA, Gibson KA, Wu YW, Croughan MS. Perinatal outcomes
insingletons following in vitro fertilization: a meta-analysis.
ObstetGynecol 2004;103:551563.
Kallen B, Finnstrom O, Nygren KG, Olausson PO. In vitro
fertilization(IVF) in Sweden: risk for congenital malformations
after different IVFmethods. Birth Defects Res A Clin Mol Teratol
2005a;73:162169.
Kallen B, Finnstrom O, Nygren KG, Olausson PO, Wennerholm U. In
vitrofertilization (IVF) in Sweden: obstetric characteristics,
maternalmorbidity & mortality. BJOG 2005b;12:15291535.
McCullagh P, Nelder JA. Generalized Linear Models, 2nd edn.
London:Chapman and Hall, 1989.
Olson CK, Keppler-Noreuil KM, Romitti PA, Budelier WT, Ryan
G,Sparks AE, Van Voorhis BJ. In vitro fertilization is associated
with anincrease in major birth defects. Fertil Steril
2005;84:13081315.
Perri T, Chen R, Yoeli R, Merlob P, Orvieto R, Shalev Y,
Ben-Rafael Z,Bar-Hava I. Are singleton assisted reproductive
technologypregnancies at risk of prematurity? J Assist Reprod Genet
2001;18:245249.
Riley M, Grifn O. Validating a statewide data collection:
differences ininformation technology resources between hospitals.
Health Inf Manag1997;27:6768.
Romundstad LB, Romundstad PR, Sunde A, von During V, Skjaerven
R,Vatten LJ. Increased risk of placenta previa in pregnancies
followingIVF/ICSI; a comparison of ART and non-ART pregnancies in
thesame mother. Hum Reprod 2006;21:23532358.
Increased obstetric haemorrhage after ART 273
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from
-
Schieve LA, Cohen B, Nannini A, Ferre C, Reynolds MA, Zhang Z,
Jeng G,Macaluso M, Wright VC, Massachusetts Consortium for
AssistedReproductive Technology Epidemiologic Research (MCARTER).
Apopulation-based study of maternal and perinatal outcomes
associatedwith assisted reproductive technology in Massachusetts.
Matern ChildHealth J 2007;11:517525.
Shevell T, Malone FD, Vidaver J, Porter TF, Luthy DA, Comstock
CH,Hankins GD, Eddleman K, Dolan S, Dugoff L et al.
Assistedreproductive technology and pregnancy outcome. Obstet
Gynecol2005;106:10391045.
Shih W, Rushford DD, Bourne H, Garrett C, McBain JC, Healy
DL,Baker HW. Factors affecting low birthweight after
assistedreproduction technology: difference between transfer of
fresh andcryopreserved embryos suggests an adverse effect of
oocytecollection. Hum Reprod 2008;23:16441653.
Smithers PR, Halliday J, Hale L, Talbot JM, Breheny S, Healy DL.
HighFrequency of Cesarean section, antepartum hemorrhage,
placenta
previa, and preterm delivery in in vitro fertilization twin
pregnancies.Fertil Steril 2003;80:666668.
Sutcliffe AG, DSouza SW, Cadman J, Richards B, McKinlay
IA,Lieberman B. Minor congenital anomalies, major
congenitalmalformations and development in children conceived
fromcryopreserved embryos. Hum Reprod 1995;10:33323337.
Tayor R. Automatic Record Linkage. Sydney: The McGraw-Hill
CompaniesInc., 1998, 184187.
Wennerholm UB, Albertsson-Wikland K, Bergh C, Hamberger
L,Niklasson A, Nilsson L, Thiringer K, Wennergren M, Wikland
M,Borres MP. Post-natal growth and health in children born
aftercryopreservation as embryos. Lancet 1998;351:10851090.
World Health Organisation. WHO Recommendations for the
Prevention ofPostpartum Haemorrhage. Geneva, Switzerland: WHO
Press, 2007.
Submitted on May 20, 2009; resubmitted on September 10, 2009;
accepted onOctober 1, 2009
274 Healy et al.
by guest on February 24, 2014http://hum
rep.oxfordjournals.org/D
ownloaded from