Embed Size (px)
Citation preview

How, Who, What Happens Next?
Betty C. Tong, MD, MHS Division of Cardiovascular and Thoracic Surgery Co-Director, Lung Cancer Screening Program Duke University Medical Center

Disclosures
• Member, NCCN Lung Cancer Screening Guidelines panel (no compensation)
• Consultant, W.L. Gore (fees donated to Women in Thoracic Surgery)

Outline
• Background and rationale for lung cancer screening– Current guidelines and recommendations– Insurance coverage and reimbursement
• Components of a successful lung cancer screening program– Fundamentals and logistics– Challenges
• The future

15%
22%
56%
7%
Lung Cancer Stage at Diagnosis
I (Localized)II and III (Regional)IV (Distant)Unknown
http://seer.cancer.gov/statfacts/html/lungb.html

NLSTLung Cancer Cases
Lung Cancer Diagnoses: CT (n = 1060)
649 from positive screens44 after negative screens367 in those who missed
screens or after trial completed
Lung Cancer Diagnoses: CXR (n = 941)
279 from positive screens137 after negative screens535 in those who missed
screens or after trial completed
61.8% 29.6%

N Engl J Med 2011;365:395-409
50%
49%
NLST: Stage Groupings

20% reduction in lung-cancer specific mortality with LDCT6.7% reduction in overall mortality with LDCT
N Engl J Med 2011;365:395-409

Insurance Coverage Circa 2014Covered Not Covered
April 2015
Current Recommendations for Lung Cancer Screening


Summary of Current GuidelinesCMS
Primary Criteria
• 55 – 79 years• > 30 pack-yrs
• 55 – 74 years• > 30 pack-yrs• Current
smoker or quit < 15 yrs
• Asymptomatic
• 55 – 80 years• > 30 pack-yrs• Current
smoker or quit < 15 yrs
• Asymptomatic
• 55 – 77 years• > 30 pack-yrs• Current
smoker or quit < 15 yrs
• Asymptomatic
Secondary Criteria
• Lung cancer survivor
• > 50 years• > 20 pack-yrs
ANDAdded >5% risk of lung CA within 5
years
• > 50 years• > 20 pack-yrs• At least one
other risk factor (not second-hand smoke)
None None
Grade BRecommendation

CMS: Additional Requirements
• Must be performed at specialized centers– Radiology imaging center with appropriate
expertise, equipment– Must collect and submit data to a CMS-approved
national registry• Registries
??APPROVED Application In Progress

• Initial LDCT must be ordered during a lung cancer screening counseling and shared decision making visit
• Documentation
1. Eligibility Criteria are all met and documented
2. One or more decision aids to discuss benefits, harms, follow-up diagnostic testing, over-diagnosis, false positive rate, total radiation exposure
3. Counseling on importance of adherence to annual LDCT screening, impact of comorbidities, willingness to undergo diagnosis and/or treatment
4. Counseling on smoking cessation (or continued abstinence), including offering additional tobacco cessation counseling services if appropriate
CMS: Additional Requirements

Lung Cancer Screening in Practice

• Multidisciplinary program– Communication is key– Include PMDs
• “Real time” scan and consultation– Shared decision making– NCCN Guidelines– Smoking cessation counseling
• Referral for incidental findings
Lung Cancer Screening Program

Patient/PMD call for or order lung cancer
screening
Chest Radiology Thoracic SurgeonNP/CTTS
Workflow
Eligibility confirmed
Screening clinic appointment made

Check in at Radiology
Day of Screening
LDCT Done
Screening clinicfor results
CT read by Chest Radiologist (< 1 hr)
Pre-screen discussion (clinic)

Pre-screen Discussion (Screening Clinic)
Low-dose CT
Negative screen
• Discussion of findings• Schedule appt for next annual screen• Letter to referring/PMD with report
Smoking Cessation Counseling as appropriate
Duke Thoracic Oncology Program
Screening Algorithm
Screening Clinic
Radiology
Screening Clinic

Low-dose CT
Negative screen
Positive screen
Smoking Cessation Counseling as appropriate
Solid nodule > 6 mmGGO or part-solid nodule > 5 mm
Multi GGO/GGNs >5 mm or dominant
Duke Thoracic Oncology Program
Screening Algorithm
• Discussion of findings• Schedule appt for next annual screen• Letter to referring/PMD with report
Screening Clinic
Radiology
Pre-screen Discussion (Screening Clinic)Screening Clinic

Positive screen
> 6 mm solid> 5 mm GGO
Referral to TSU/IP provider*
Follow-up imaging
PET/CT(> 8 mm solid)
Duke Thoracic Oncology Program
Screening Algorithm
* Can be same day

Positive screen
> 6 mm solid> 5 mm GGO
Advanced Disease
Biopsy (IP/Radiology)
Referral to TSU/IP provider*
Medical Oncology+
Radiation Oncology
PET/CT(> 8 mm solid)
Duke Thoracic Oncology Program
Screening Algorithm
* Can be seen same day
Follow-up imaging

• Developed by leadership of ACCP/ATS• Endorsed by AATS, American Cancer Society, ASCO• Describes 9 essential components / 21 policy statements
– Who is offered screening, and for how long– Technical aspects of LDCT scans– Interpretation of scans / definition of “positive”– Standardized reporting– Management algorithms– Patient and provider education– Data collection– Smoking cessation

Smoking Cessation

Rationale for Including Tobacco Cessation Counseling with LCS
• Decreases risk of lung cancer and other smoking-related conditions
• Increases cost effectiveness of lung cancer screening
• It is the right thing to do• Required by CMS for
reimbursement

• Estimated mean life-years, QALYs, costs per person, ICERs
• Used 3 alternative strategies– Screening with LDCT– Screening with radiography– No screening
• Conclusions– LDCT cost $81,000 / QALY gained– Caveat: “modest changes” in assumptions would greatly
alter results

• Modeling used to estimate QALYs saved by lung cancer screening and treatment
• Included cost of “intensive” cessation programs– Generic NRT vs. buproprion vs. varenicline
• Hypothetical cohort 50-64 yo with > 30 p-y smoking– 2/3 current smokers– 1/3 former smokers


Medical Oncology
Radiation Oncology
Chest Radiology
Thoracic Surgery
Local/Referring
Physicians Smoking Cessation
Lung Cancer Screening Program
Lung Cancer Screening and Management: A Multidisciplinary Effort

Current Challenges• Logistics– Protocoling for scans– Insurers slow to get on point– Standardized reporting
• Access for un- and underinsured
• Referring providers– Appropriate referrals for
screening– Follow-up after initial
screening study

Getting “Buy In” • Multidisciplinary team approach includes
Primary Care, General Medicine and Pulmonary
• Provider Education– Teaching Conferences/Grand Rounds– Community outreach– Electronic alerts and reminders in EMR

Role of the EMR in Screening
• BPAs for primary care providers• Direct access to patients– Electronic reminders (e.g. MyChart)– Reminder letter sent via mail– Pop-up message at check-in kiosk
• “Hard stops” to ensure clinical eligibility during ordering process
• Smoking cessation materials and resources• Decision aid

BPA Example

So What Happens Next?
• Improving existing screening and diagnostic modalities to increase precision and reduce risk– Non-invasive prediction models– Safer practices
• Adjunctive testing– Biomarkers

Reducing Risk in Lung Cancer Screening
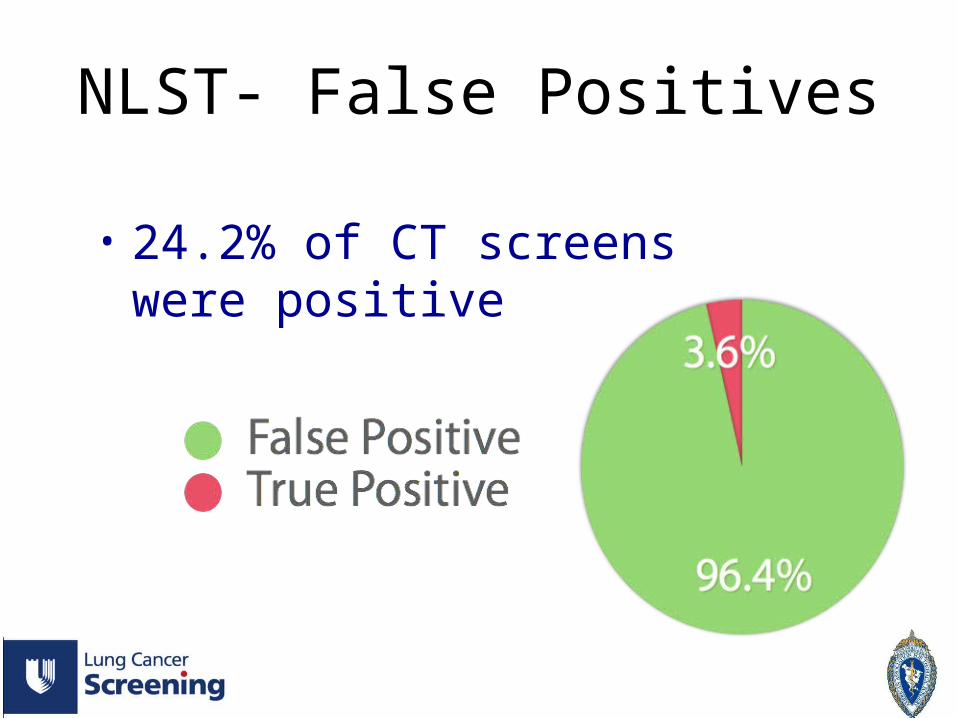
• 24.2% of CT screens were positive
NLST- False Positives

NLST- Positive Studies
• 92% of positive CT screens had a diagnostic evaluation
16 deaths within 60 days 6 of 16 had benign pathology
8.4%

• Overdiagnosis: Detection of disease that does not contribute to death
• Results in unnecessary treatment, morbidity, cost, worry

• Overdiagnosis: Detection of disease that does not contribute to death
• Results in unnecessary treatment, morbidity, cost, worry
Lung Cancer (LDCT)18%
Breast Cancer (Mammo) 30-54%Prostate Cancer (PSA) 29-44%
Etzioni et al. JNCI 2002; 94: 981-990

Risk Reduction
• Increased size threshold for “positive”• Predictive models/algorithms• Improving surgical outcomes– Underutilization of VATS/Robotics?– Use of new technology

• Retrospective analysis of I-ELCAP data• N = 21,136• Measured frequency of positive results and delays in
diagnosis using more restrictive size thresholds• 10.2% positives using 6 mm threshold
Ann Intern Med 2013; 158:248-252.

Frequency of a positive result and cases of lung cancer diagnosed within 12 months of enrollment
Ann Intern Med 2013; 158:248-252.


• NELSON: Dutch trial of LDCT vs. usual care in high risk participants, 7155 in CT group
• Calculation of lung cancer probabilities based on nodule characteristics (diameter, volume, etc.)
• Use of nodule volume and/or volume doubling time improves predictive ability for lung cancer in management algorithms

“…strongly encourages the use of MITS, inclusive of both video-assisted and robotic approaches, whenever available, for the diagnosis and treatment of screen-detected nodules.”
Ann Thorac Surg 2013; 96:357-60

Utilization of VATS for Lobectomy(Under)

New Technology
• Improved precision of TBBx, VATS wedge• In lieu of diagnostic VATS?

Summary
• Screening with LDCT is here, and Thoracic Surgeons are important members of the LCS Team
• Lung cancer screening programs– Multidisciplinary collaboration– Must include smoking cessation
• There is still room for improvement– Better and more tools for accurate prediction – Safer procedures

Thank You