Embed Size (px)
Citation preview
How We Can Make Health Care as Safe as Air Travel
Mark R. Chassin, MD, FACP, MPP, MPHPresident, The Joint Commission
SCHA/SCMA 32nd Annual TAP ConferenceSCHA/SCMA 32 Annual TAP ConferenceHilton Head, SC
September 14 2012September 14, 2012





Current State of QualityRoutine safety processes fail routinely
• Hand hygiene• Hand hygiene• Medication administration• Patient identification• Communication in transitions of care
Uncommon, preventable adverse events• Surgery on wrong patient or body part• Surgery on wrong patient or body part• Fires in ORs, retained foreign objects• Infant abductions, inpatient suicides

How Have Others Done It?“High reliability organizations” manage
very serious hazards extremely wellvery serious hazards extremely well• Commercial aviation, nuclear power
What do they all have in common?Highl effecti e process impro ement• Highly effective process improvement
• Fully functional safety culturey yDiscover and fix unsafe conditions early“C ll ti i df l ”“Collective mindfulness”

How Safe are US Airlines?How Safe are US Airlines? 1990-2001
• 129 deaths per year• 9 3 million flights per year9.3 million flights per year• Rate = 13.9 deaths per million flights
2002 20102002-2010• 18 deaths per year = 87% • 10.6 million flights per year• Rate = 1.74 deaths per million flightsRate 1.74 deaths per million flights

Safety: Airlines vs. Health CareyIOM “To Err is Human” estimate
44 000 98 000 d h i h i l• 44,000-98,000 deaths in hospitals due to errors in care
• 34.4 million hospitalizations per year• Rate = 1300-2800 deaths per million p
hospitalizationsUS Airlines: 2002-2010US Airlines: 2002 2010
• Rate = 1.74 deaths per million flightsH it l i 750 1600 ti l fHospital care is 750-1600 times less safe

Reframing the Mission of The Joint Commission
Mission: refocused in 2009Mission: refocused in 2009“To improve health care for the public by
l ti h lth i ti devaluating health care organizations and inspiring them to excel…”
Enhancing value dramatically in core businessWe are no longer only an accreditorg yMany programs today to move all of health
care toward consistent excellencecare toward consistent excellence

Growth in Joint Commission US CustomersUS Customers
20000 Q2
18000
19000
17000
18000
16000
14000
15000
140002005 2006 2007 2008 2009 2010 2011 2012

High Reliability ScienceHigh Reliability ScienceResearch has defined how HROs
produce sustained excellence over timeNo health care organizations functionNo health care organizations function
at this high level of sustained safetyN id h t t fNo guidance on how to transform
organizations from low to high reliabilityHow do we create blueprints for health
care to build high reliability?care to build high reliability?

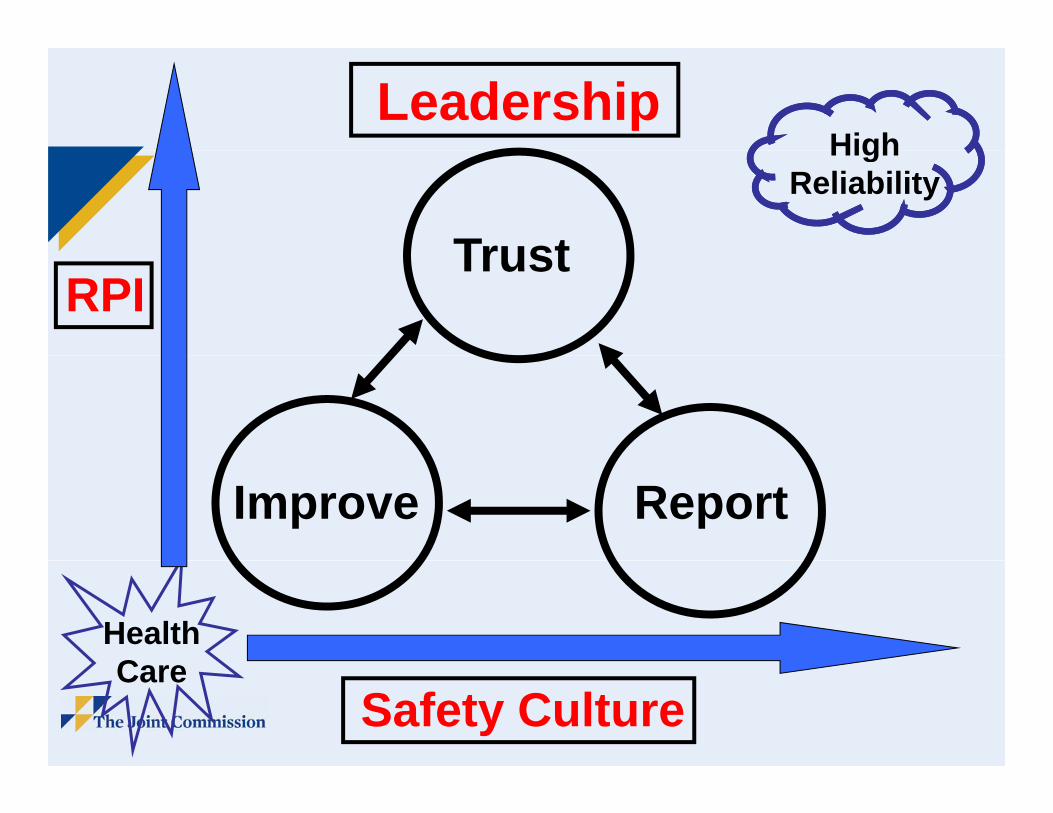
HighLeadership
HighReliability
TrustRPI
Trust
Improve Report
HealthCCare
Safety Culture

From Health Affairs
Health Affairs 2011;30:559-68

High Reliability S lf A t T l (HRST)Self-Assessment Tool (HRST)
Leadership: Board, CEO, physiciansLeadership: Board, CEO, physicians• Quality strategy, quality measures, IT
Safety cultureSafety culture• Trust and accountability• Identifying unsafe conditions or practices• Strengthening systems, measurementS e g e g sys e s, easu e e
Robust process improvement• Methods training spread• Methods, training, spread

Stages of Maturity in Moving g y gToward High Reliability
4 t f h f 14 t4 stages for each of 14 components: beginning, developing, advancing, approaching
Question: Overall focus of quality programs?1. Meeting requirements of regulatorsg q g2. Beginning to set our own goals3 Primarily on achieving our own goals3. Primarily on achieving our own goals
Has the board committed to reaching the l t l f j lit f il ?long-term goal of zero major quality failures?

Robust Process ImprovementRobust Process ImprovementSystematic approach to problem solving:
(RPI l i i h t)(RPI = lean, six sigma, change management)The Joint Commission has adopted RPIp
• Improve processes and transform culture• Focus on our customers increase value• Focus on our customers, increase value
The Joint Commission is adopting all t f f t ltcomponents of safety culture
We measure RPI and safety culture and report on strategic metrics to Board

Training and Deploymentg p yWe have a large group of experts in lean,
six sigma and change management (RPI)six sigma, and change management (RPI)• Extensive experience with 27 hospitals
d t l i RPI t land systems applying RPI tools• Studied experience of major corporations
(for example, GE, Lilly, BD, Cardinal)We offer training in the full suite of RPI g
tools or in its component partsWe offer assistance in program designWe offer assistance in program design


Center for Transforming Healthcare
www.centerfortransforminghealthcare.org

Center for Transforming HealthcareDelivering products at no added cost
• TJC: $20M; 9 other major donors• AHA, BCBSA, BD, Cardinal Health
Ecolab, GE, GSK, J&J, Medlineco ab, G , GS , J&J, ed e2009: hand hygiene, wrong site surgery
and hand-off communicationsand hand-off communications2010: colorectal surgery SSIs 2011 f l bl HF2011: safety culture, preventable HF
hospitalizations, and falls with injury2012: sepsis, medication safety

Participating HospitalsAtlantic Health Memorial Hermann Barnes-JewishBaylor
Nebraska Medical CenterNew York-Presbyterian
Cedars-SinaiCleveland ClinicE l
North Shore-LIJNorthwesternOSFExempla
FairviewFloyd Medical Center
OSF Partners HealthCareSharp HealthcareFloyd Medical Center
FroedtertIntermountain
Sharp HealthcareStanford HospitalTexas Health ResourcesIntermountain
Johns HopkinsKaiser-Permanente
Texas Health ResourcesTrinity HealthVirtua
Mayo Clinic Wake Forest BaptistWentworth-Douglass

Current State of QualityRoutine safety processes fail routinely
• Hand hygiene• Hand hygiene• Medication administration• Patient identification• Communication in transitions of care
Uncommon, preventable adverse events• Surgery on wrong patient or body part• Surgery on wrong patient or body part• Fires in ORs, retained foreign objects• Infant abductions, inpatient suicides

Current State of ImprovementpUsual approaches: best practices, toolkits,
protocols checklists “bundles”protocols, checklists, bundles• Describe a specific set of process steps
th t t b f ll d t l blthat must be followed to solve a problem• ICU central line protocol, VAP bundle
The “one-size-fits-all” best practice produces good results only in limited circumstancesg y• Process varies little from place to place• Causes of failure are few and common• Causes of failure are few and common

A New Way is Delivering ResultsComplex processes require more
sophisticated problem-solving methodssophisticated problem solving methodsThree crucial and consistent findings:
M f th bl• Many causes of the same problem• Each cause requires a different strategy• Key causes differ from place to place
Next generation of best practices will useNext generation of best practices will use RPI to produce solutions---customized to an organization’s most important causesan organization s most important causes

Semmelweis’ Original DatagMonthly Death Rates
Handwashing ProgramProgram
1841 1842 1843 1844 1845 1846 1847 1848

Some Important Causes of Hand Hygiene FailuresHand Hygiene Failures
1. Faulty data on performance2. Inconvenient location of sinks or
hand gel dispensershand gel dispensers3. Hands full4. Ineffective education of caregivers5 Lack of accountability5. Lack of accountability
Each requires a very different q ystrategy to eliminate

Causes Differ by HospitalEach letter = one hospitalEach letter = one hospital

Some Important Causes of Hand Off Communication Failures
1 “Sender” and “receiver” have1. Sender and receiver have different expectations
2. Lack of teamwork and respect3. Inaccurate or incomplete information3. Inaccurate or incomplete information4. Receiver has competing priorities5. Interruptions during hand-off6 Ineffective communication method6. Ineffective communication method

Causes Differ by HospitalE h l tt h it lEach letter = one hospital

Improving TransitionsImproving TransitionsHand-off communication failed to includeHand off communication failed to include
adequate information 41% of the time Interventions reduced this rate to 17%Interventions reduced this rate to 17%One hospital focused on the transition
from its inpatient units to a nursing homefrom its inpatient units to a nursing homeBaseline Improve
Inadequate hand-offs 29% <1%30-day readmissions 21% 10% y % %

More Positive Impacts ofMore Positive Impacts of Improving Transitions
33% reduction in time spent in Emergency Department after decision to admitDepartment after decision to admit
Reduced readmissions (“bounce backs”) to ICU after discharge to medical inpatient unitICU after discharge to medical inpatient unit
Improved patient and family satisfactionImproved staff satisfactionImproved teamworkp
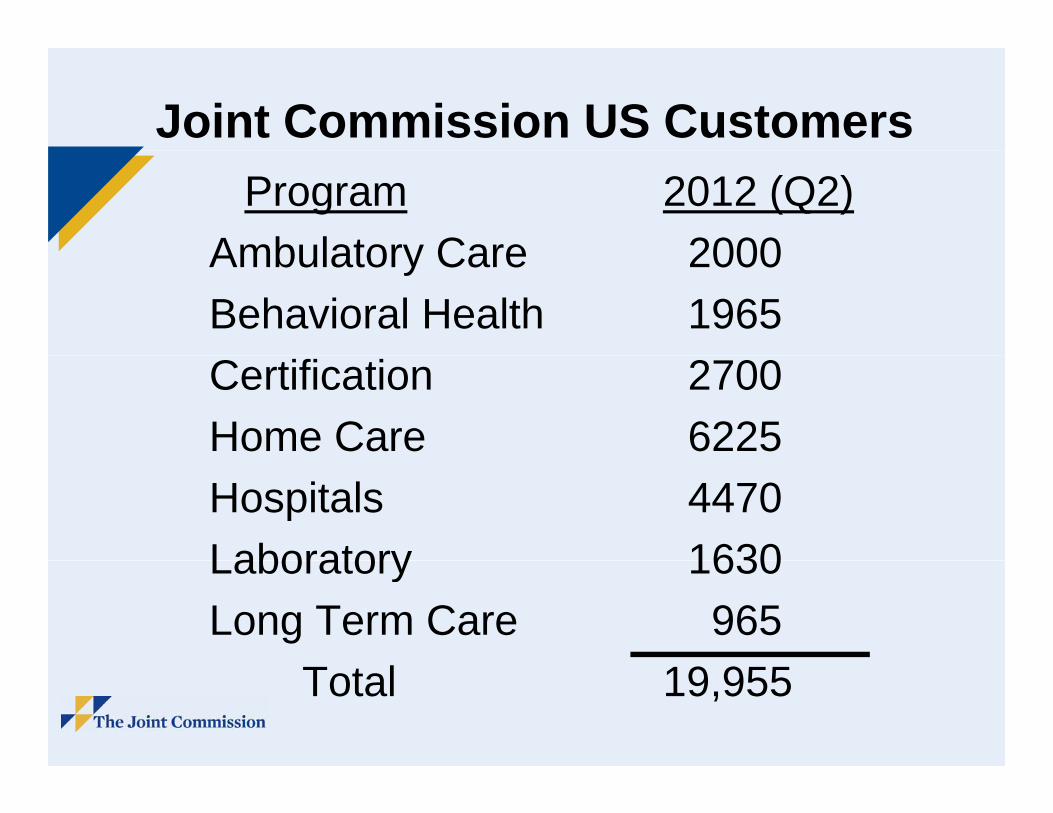
Joint Commission US CustomersProgram 2012 (Q2)
Ambulatory Care 2000Ambulatory Care 2000Behavioral Health 1965Certification 2700Home Care 6225Hospitals 4470Laboratory 1630Laboratory 1630Long Term Care 965
Total 19,955

Wrong Site Surgeryg g yJoint Commission Universal Protocol 2003:
a simple one size fits all best practicea simple, one-size-fits-all best practiceToday: 40 per week in USCenter project found many more risks:
• Scheduling: 39% of cases had risksg• Pre-op area: 52% of cases had risks• OR: 59% of cases had risks• OR: 59% of cases had risks
Risks varied by hospital, ASCTargeted interventions reduced risk by 50%

Results are ConsistentMore sophisticated improvement methods
(RPI) required for complex problems(RPI) required for complex problems• Measure and discover specific causes• Identify how causes vary among
different organizations and settings• Target interventions to specific causes
to maximize effectiveness• Avoid wasting resources by targeting
This is the Center’s unique capabilityThis is the Center s unique capability

Targeted Solutions Tool (TST)g ( )Uses secure, established extranet channels
N dd d l fid i l• No added cost, voluntary, confidential• Simplified, RPI-driven problem solving
Educational, no jargon, no special trainingGuides users to customized proven solutionsGuides users to customized, proven solutionsTargeting only your causes means you don’t
use resources where they aren’t neededuse resources where they aren t neededHand hygiene (2010), WSS (Feb 2012);
h d ff i ti (J 2012)hand-off communication (June 2012)

Hand Hygiene Results: July 2012715 projects are using interventions
• Baseline = 52 9% (n = 79 844)*• Baseline = 52.9% (n = 79,844)• Improve = 77.0% (n = 263,707)*
*p<0.0001
Unit Baseline Improve• Adult critical care 52% 73%• Emergency dept. 47% 76%• Adult med surg 48% 75%• Adult med-surg 48% 75%• Long term care 55% 74%
20% have improved to 90% or greater


August 24 2012August 24, 2012
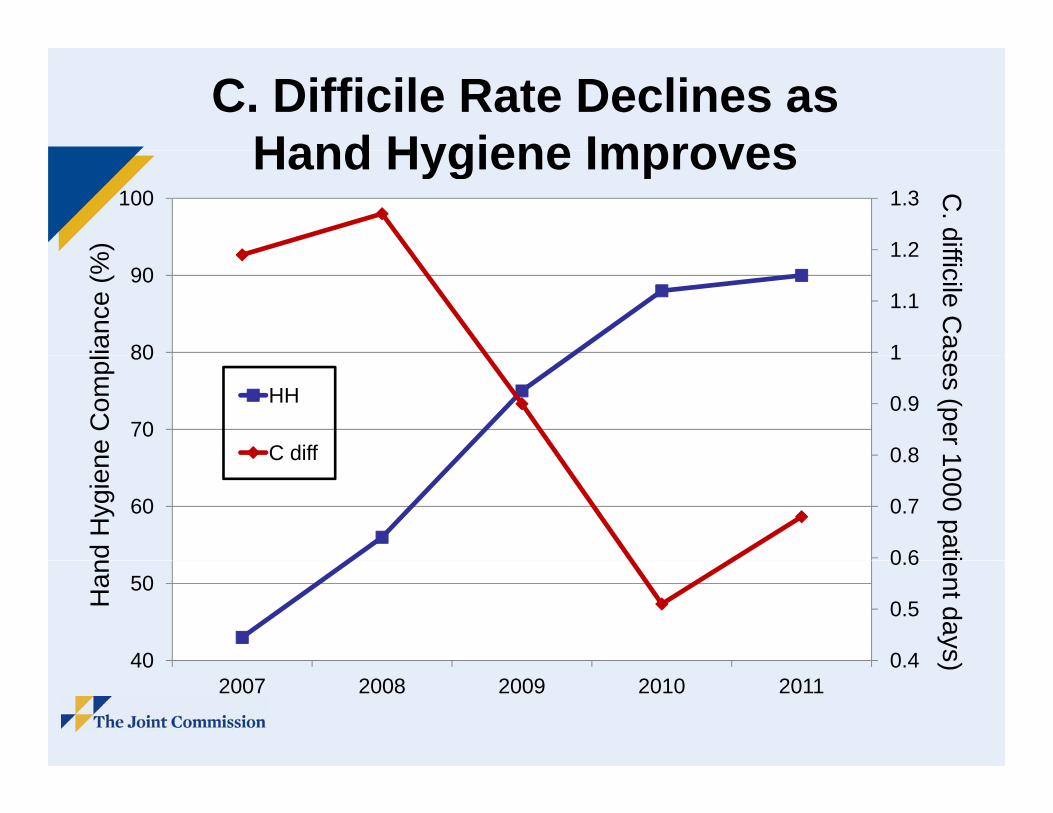
C. Difficile Rate Declines as Hand Hygiene ImprovesHand Hygiene Improves
1 2
1.3100
%)
C. dif
1
1.1
1.2
80
90
ianc
e (%
fficile Cas
0 8
0.9
1
70
80
HH
C diffne C
ompl
ses (per 1
0 6
0.7
0.8
60
C diff
d H
ygie
n 1000 pati
0 4
0.5
0.6
40
50Han
ent days
0.4402007 2008 2009 2010 2011
)

MRSA Rate Decreases as Hand Hygiene Improves
100 2.5
Hand Hygiene Improves%
)M
RS
80
902.0
lianc
e (%
SA C
ases
70 1.5HH
MRSA
ne C
omp s (per 10
50
60
0 5
1.0
nd H
ygie
n 00 patien
30
40
0.0
0.5
Han
nt days)
2008 2009 2010
Memorial Hermann’s Story: G tti t ZGetting to Zero
Leadership commitment to zeropRecognized need for culture changeMH Woodlands Hospital was among the 8MH Woodlands Hospital was among the 8
Center hospitals in first hand hygiene project 2010 MH itt d t TST t i2010: MH committed to use TST to improve
hand hygiene system-wide (12 hospitals)Baseline (150 inpatient units) = 44%
• Range (12 hospitals): from 21% to 65%g ( )• Aim: to exceed 90%

TJC Hand Hygiene ComplianceCenter for Transforming Healthcare
Baseline
g
85%
90%14,000
Compliance44% 80%
85%
10,000
12,000
70%
75%
6,000
8,000
60%
65%
4,000
,
50%
55%
0
2,000
Oct‐10 Dec‐10 Feb‐11 Apr‐11 Jun‐11 Aug‐11 Oct‐11 Dec‐11 Feb‐12 Apr‐12 Jun‐12
Secret Observations Compliance Rate

NICU Central Line Associated Blood Stream Infections (CLABSI)
Mean = 1.85
Mean = 1.07

Ventilator Associated Pneumonias (VAP)( )
Mean = 0.95
Mean = 0.5

Woodlands: Zero Hospital Central Line Blood Stream Infections

Memorial Hermann: Summary ySystem-wide HAI reductions using TST
Baseline Control(pre-TST) (post TST) RelativeOct 2010- Jan-June Decrease May 2011 2012 (%)
Adult ICU CLABSI1 0.79 0.45 43NICU CLABSI1 1 85 1 07 42NICU CLABSI1 1.85 1.07 42VAP2 0.95 0.5 47
1 BSI per 1000 line days 2 VAP per 1000 ventilator days
Michael Shabot, MDMemorial Hermann System CMO
“We fully attribute to the Center forWe fully attribute to the Center for Transforming Healthcare’s hand hygiene [tools] the final drop in HAI rates to zero or[tools] the final drop in HAI rates to zero or near-zero system-wide. After implementing CTH hand hygiene our hospitals began toCTH hand hygiene, our hospitals began to report zeros as their most common monthly CLABSI and VAP result Our mothers wereCLABSI and VAP result. Our mothers were right after all! Feel free to quote me. This actually saves lives ”actually saves lives.
The Joint Commission and High ReliabilitHigh Reliability
Consistent excellence is the visionLeadership + safety culture + RPIAll Joint Commission programs and activitiesAll Joint Commission programs and activities
are aligning around this aim:A dit ti f t• Accreditation, performance measurement
• JCR education, publication, consulting• Center-developed improvement solutions
Help customers improve no matter whereHelp customers improve no matter where they are on the journey to high reliability

Launching a New InitiativegHigh reliability is achievableStri ing for high reliabilit is not a projectStriving for high reliability is not a project
• Leadership commitment to goal of zero• Highly effective improvement capacity• Fully functioning culture of safetyFully functioning culture of safety
Enhances your hospital’s ability to produce better outcomes in many different areasbetter outcomes in many different areas, including CMS Partnership goals
South Carolina High Reliability InitiativeSouth Carolina High Reliability Initiative

South Carolina Hi h R li bilit I iti tiHigh Reliability Initiative
TJC, SCHA partnering to help SC hospitalsTJC, SCHA partnering to help SC hospitals accelerate progress toward high reliability
Outline of activities over 3 years:Outline of activities over 3 years:• Core group (8-10 hospitals) to complete
in depth self assessment using HRSTin-depth self assessment using HRST• Identify, address most pressing barriers • Learn together, share what works• Learnings communicated regularly and g g y
widely to all other interested SC hospitals

Not Another ProjectNot Another ProjectStage set by your past and current projects:
DTB f j t lt l i iDTB, safe surgery, just culture, lean six sigmaCreates platform for consistent excellenceAmong first to test CTH safety culture solutionsPlanning will continue for next several monthsPlanning will continue for next several months,
so sign up now to join core group of hospitals:• CEO and team: time and effort required• CEO and team: time and effort required• Financial commitment: TBD
First meeting expected early in 2013






























