Embed Size (px)
Citation preview

How to meet protein requirements
in the ICU?
Kate Fetterplace APD Senior Dietitian PhD Candidate

Supervisors and collaborators – A/Prof Adam Deane
– A/Prof Christopher MacIsaac
– A/Prof Jeffery Presneill
– Dr Audrey Tierney
– Dr Marina Mourtzakis
– Dr Adrienne Forsyth
– A/Prof Linda Dehehy
– Mrs Lisa Beach
– Ms Laura Knight
– Dr Thomas Rechnitzer
• Conflicts of interest: received honorarium / sponsorship support from Baxter, Fresenius Karbi, Nestle and Nutricia
Acknowledgments & Conflicts

• In healthy adults – balance between synthesis and breakdown
• During metabolic stress (major surgery, trauma) – imbalance occurs leading to net loss of body protein
• Regulated by pro-inflammatory modulators such as TNF-alpha and IL-6
Protein Metabolism
Muscle Protein
Muscle Breakdown
Muscle Synthesis
Amino Acids
Blood
Muscle
Amino Acids
Muscle loss occurs when
Muscle Breakdown > Muscle Synthesis

Protein Recommendations
McClave et al JPEN 2017, Singer et al Clin Nut 2009, CCPG Crit Care Nut 2015
SCCM & ASPEN 2016 ESPEN PN 2009 Canadian 2015
1.2-2.0g/kg actual body weight Likely higher in burn or multitrauma patients Quality: Low
1.3–1.5 g/kg ideal body weight Quality: Level B
Insufficient data to make a recommendation on the use of high protein diets in critically ill patients
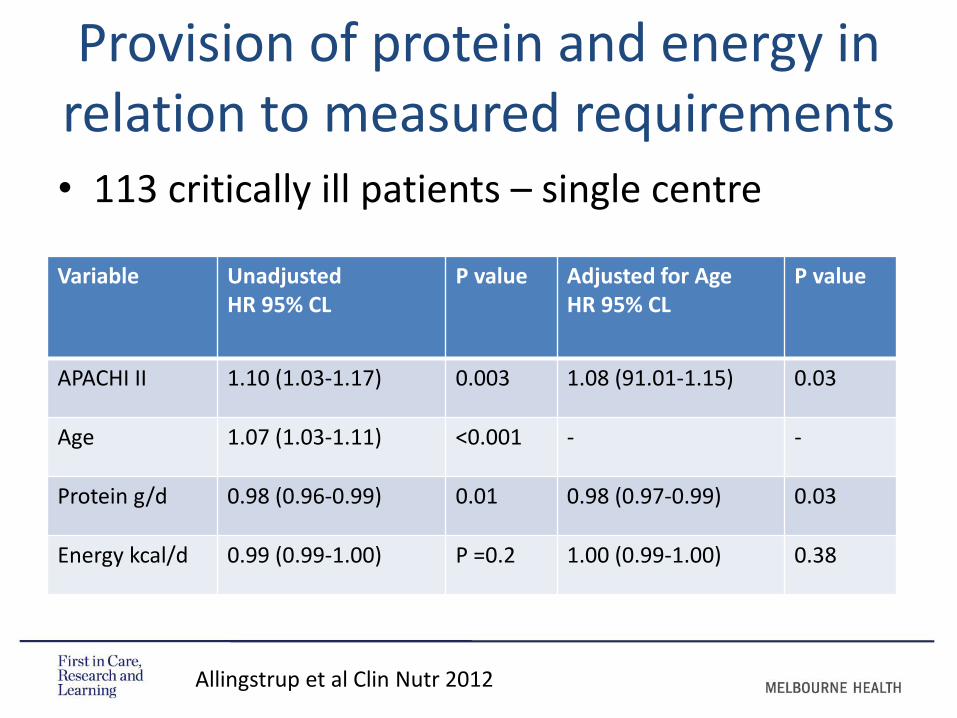
• 113 critically ill patients – single centre
Provision of protein and energy in relation to measured requirements
Variable Unadjusted HR 95% CL
P value Adjusted for Age HR 95% CL
P value
APACHI II 1.10 (1.03-1.17) 0.003 1.08 (91.01-1.15) 0.03
Age 1.07 (1.03-1.11) <0.001 - -
Protein g/d 0.98 (0.96-0.99) 0.01 0.98 (0.97-0.99) 0.03
Energy kcal/d 0.99 (0.99-1.00) P =0.2 1.00 (0.99-1.00) 0.38
Allingstrup et al Clin Nutr 2012

Variable Low Protein (54g) (n= 37)
Medium Protein (84g) (n=38)
High protein (115g) (n=38)
Protein/kg/day mean (SD)
0.79 (0.29) 1.06 (0.23) 1.46 (0.29)
N balance g/kg per day mean (SD)
0.59 (0.48) -0.35 (0.41) -0.2 (0.58)
ICU Mortality n (%) 10 (27) 9 (24) 6(16)
Higher Protein Provision May Influence Survival
Allingstrup et al Clin Nutr 2012
• Morality between the high and low group was significantly different (p = 0.011)
• Survival probability: Low 49%, Medium 79%, High 88%

Protein delivery & clinical outcomes in the critically ill:
A systematic review and meta-analysis
Literature between 1966 and 2015
Inclusion criteria:
– RCTs comparing two different nutrition strategies for > 48hrs
– Reported a statistically significant difference in protein delivery (p <0.05)
– MV critically ill patients
– Outcome of mortality
Davies et al Criti Care & resus June 2017

• 14 studies including 3238 patients
• Mean protein delivered:
– Low mean (SD): 42.95 g/day (20.45) or 0.67g/kg/day (0.38)
– High mean (SD): 67.15 g/day (28.47) or 1.02g/kg/day (0.42)
• Lower protein had no influence on mortality OR 0.935 (Cl 0.72-1.22 p = 0.618)
Protein delivery & clinical outcomes in the critically ill:
A systematic review and meta-analysis
Davies et al Criti Care & Resus 2017

Professor Olav Rooijackers, Stockholm, Sweden
• Stable-isotope–labelled phenylalanine and tyrosine tracers
• Used to measure protein synthesis, breakdown and oxidation
• Critically ill patients are able to utilise extra enteral and parenteral amino acid to build new body protein
• Protein feeding yielded a detectable, although small, improvement in whole body protein balance
Amino Acid Tracers
Liebau F et al CC 2015, Liebau F et al. Am J Clin Nut 2015

Positive Protein Balance
Protein Balance Phe oxidation
• Conclusion: Protein intakes of
> 1.2 g/kg/day result in a positive protein balance
Synthesis WB Breakdown
Liebau et al. Critical Care (2015) 19:106

Protein Requirements in the Critically Ill: A RCT Using PN
• N = 120 Critically ill
• Aim: to deliver 1.2g/kg/day V. 0.8g/kg/day protein via PN – Delivered: 1.1g/kg Vs 0.9g/kg per day protein
– No difference in mortality (20% vs. 15%) p = 0.47
– Greater forearm muscle thickness:
• mean (SD): 3.2cm (0.4) vs 2.8 cm (0.4), p <0.0001
– Improved handgrip strength:
• mean (SD): 22 kg (10) vs 18.6 kg (12), p = 0.025
Ferrie et al JPEN 2016

Targeted Full Energy and Protein Delivery in Critically Ill Patients : A Pilot RCT
Fetterplace et al Unpublished data
60 MV critically ill enterally fed patients
Standard Care Intervention
Energy Target 25kcal/kg 25kcal
Protein Target 1.0g/kg 1.5g/kg
Formula 1.0kcal/ml standard 1.25kcal/ml high protein + Protein powder (6g bolus)
Delivery Method Hourly rate prescription
Volume prescription

• Pulse protein feeding patterns may enhance protein synthesis
• 25-30g protein per meal (containing 2.5-2.8g leucine)
• ‘Fast’ protein may have benefit over ‘slow’ proteins
• Proteins or amino acids are recommended in close proximity to exercise or activity
Optimise Muscle Protein Synthesis
Deutz et al Clin nut 2014, Bauer et al JAMDA 2013
• Leucine is an essential amino acid and has been shown to promote muscle protein synthesis
• Many amino acid preparations have been studied including BCAA (Valine, Leucine: isoleucine)
– Systematic review: 22 studies (4 in ICU & 18 muscle wasting condition)
• Leucine enriched EAA, HMB and creatine have shown some promising results in decreasing muscle loss in the critically ill
Optimal amino acids to maintain muscle mass
Wandrag et al J Human Nut & Diet 2014

Nutrition Interventions to Optimise Protein Provision
1
• High protein formula
• Enteral or Parenteral
2
• Protein Supplementation
• Enteral or Parenteral
3
• Volume based protocols
• Supplemental PN
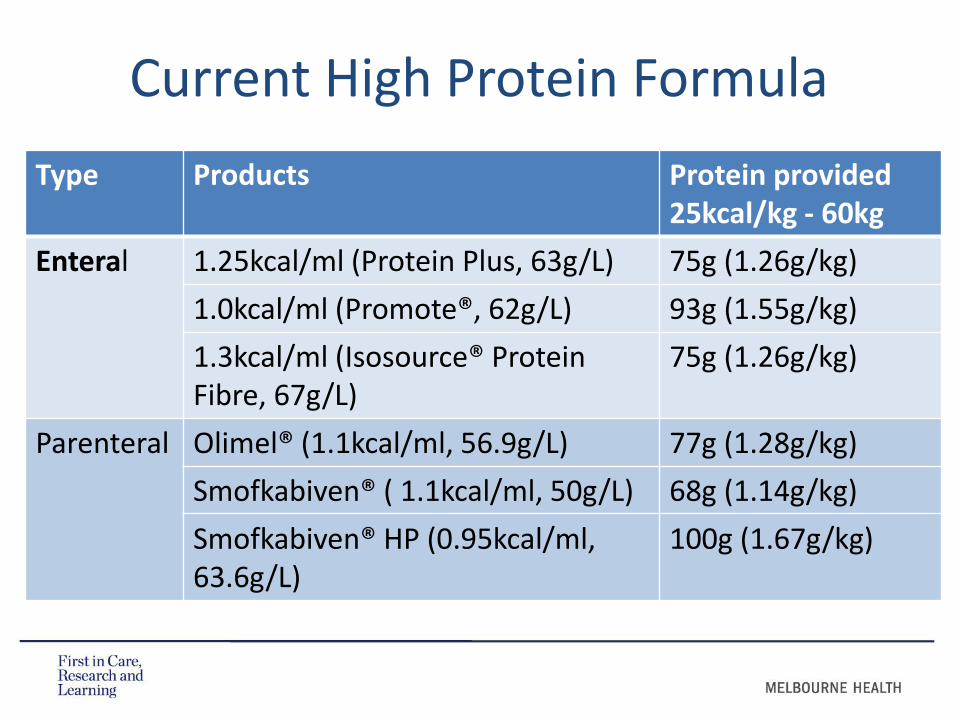
Current High Protein Formula
Type Products Protein provided 25kcal/kg - 60kg
Enteral 1.25kcal/ml (Protein Plus, 63g/L) 75g (1.26g/kg)
1.0kcal/ml (Promote®, 62g/L) 93g (1.55g/kg)
1.3kcal/ml (Isosource® Protein Fibre, 67g/L)
75g (1.26g/kg)
Parenteral Olimel® (1.1kcal/ml, 56.9g/L) 77g (1.28g/kg)
Smofkabiven® ( 1.1kcal/ml, 50g/L) 68g (1.14g/kg)
Smofkabiven® HP (0.95kcal/ml, 63.6g/L)
100g (1.67g/kg)

Product Protein content Ingredients
Beneprotein® 6g protein per scoop
100% Whey protein
Protifar 2.2g protein per scoop
77% Casein 13% whey
Synthamin® 17 (10%) 50g/500ml IV balanced amino acid
Vamin® 18 (11.4%) 57g/ 500ml IV balanced amino acid
Current Protein Modular

What is the Optimal Formula?
• 60 yo male admitted following a MVA
• Head injury and multiple injuries and wounds
• Weight: 75kg BMI: 25
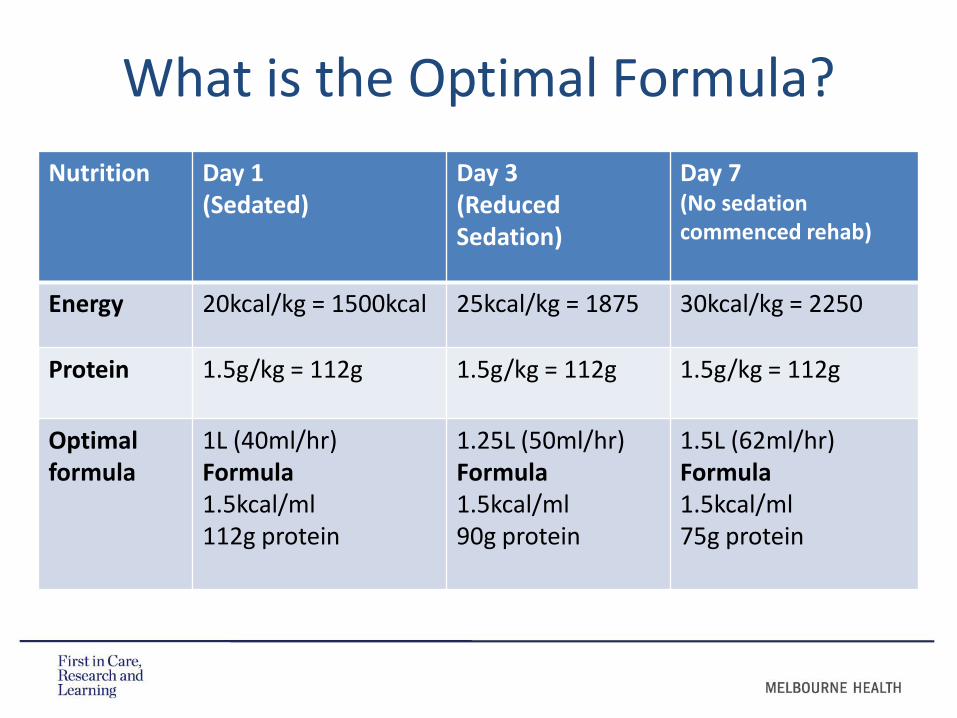
Nutrition Day 1 (Sedated)
Day 3 (Reduced Sedation)
Day 7 (No sedation commenced rehab)
Energy 20kcal/kg = 1500kcal 25kcal/kg = 1875 30kcal/kg = 2250
Protein 1.5g/kg = 112g 1.5g/kg = 112g 1.5g/kg = 112g
Optimal formula
1L (40ml/hr) Formula 1.5kcal/ml 112g protein
1.25L (50ml/hr) Formula 1.5kcal/ml 90g protein
1.5L (62ml/hr) Formula 1.5kcal/ml 75g protein
What is the Optimal Formula?

Optimal Enteral Formula For Critically Ill?
1000ml 1.5kcal/ml
Protein 95-100g/L
High quality protein – including
Whey protein
Osmolality 340-400
mOsmol/kgH20
With and without High quality fibre
Optimise Leucine content
and contain HMB

• What is the optimal protein provision?
–At present: 1.3-1.7g/kg per day
• What is the best type of protein?
• What is the optimal route for protein supplementation?
• How can we monitor protein adequacy ?
• Can these interventions improve functional outcomes and maintain lean body muscle mass?
Future Research

Thank you!





























