Embed Size (px)
Citation preview

How to Create A Culture of Continuous, Sustainable Improvement Christopher Kodama, MD, MBA
President, MultiCare Connected Care March 24, 2017
Objectives
• To outline governance and structure to support your physicians and staff
• To describe how to efficiently develop evidence-based guidelines & pathways
• Explain how to implement data analytics to engage your teams in performance improvement
2

Agenda
1.Who
2.Why
3.How
4.Case Studies
3

4
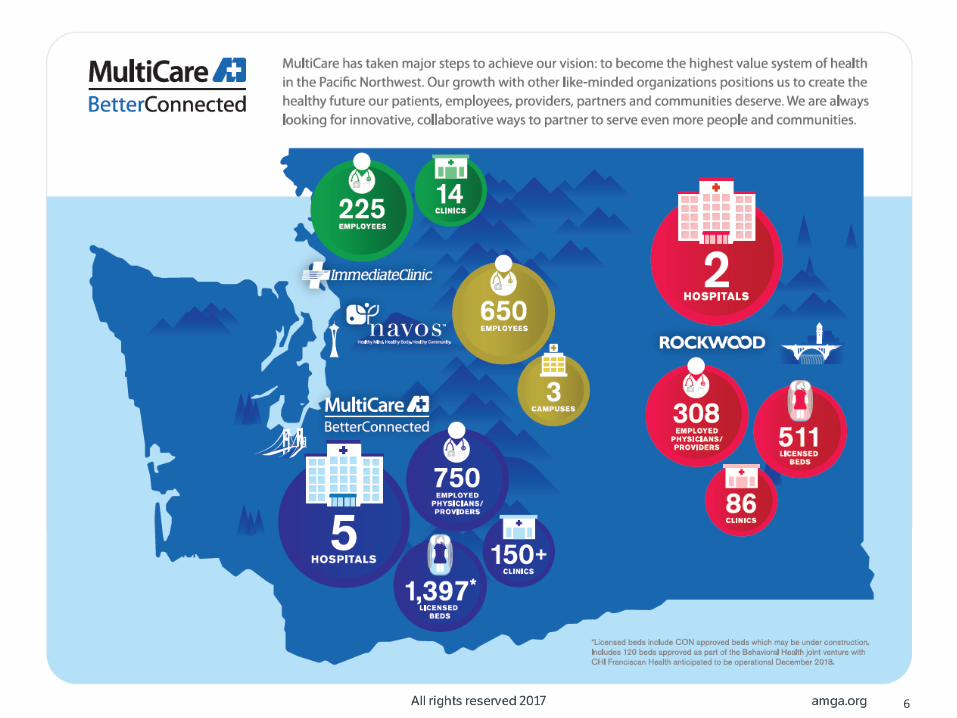
WHO MultiCare Health System

Key Attributes
• Washington State Footprint
• Integrated Healthcare Delivery System
• Tertiary Children’s Health Network
• Employed Provider Group of 800+
• Clinically Integrated Network of >2400 providers
5
6

MultiCare Connected Care
• Separate entity from MultiCare Health System
• Wholly owned by MultiCare Health System
• Commercial
• Physician-led
• Houses the CIN (MCC Network)
7

MCC Network
• Primary Care + Multispecialty
• Pediatric to Adult
• MultiCare-employed (MMA) & Independent
• Continuum of Care
• 2400+ physicians, AP’s, and ancillaries
• 80K+ covered lives
8

9
WHY A Case for Change

10
eco system (ee·koh·sis·tuh·m) n.
any system or network of interconnecting and interacting parts
Why Now?

Our Ecosystem
11
CONSTITUENTS COLLEAGUES
CONSUMER
POPULATIONS
CORPORATE COLLABORATORS

9.4%
9.1%
10.2%
www.worldbank.gov April 25, 2016
Comparisons

Current Value
• Life Expectancy
• Infant Mortality
• 2+ Chronic Conditions
• Obesity
14
www.commonwealthfund.com october 2015

Focus
QUALITY
S E R V I C E COST
15

Value Proposition
Q U A L I T Y S E R V I C E
COST
x = VALUE
16

Accountable Care
838
28.3M
http://healthaffairs.org/blog/2016/04/21/accountable-care-organizations-in-2016-private-and-public-sector-growth-and-dispersion/
17

Paradigm Shifts
FROM TO
Sick care WELLNESS and disease management
Episodic Care SEAMLESS comprehensive care across the
continuum
Silos & Fragmented Care PERSON-CENTERED & Integrated
Exclusively Fee-For-Service TOTAL COST of Care
Duplication COORDINATED Providers
Bricks & Mortar Care VIRTUAL Care
Acute Care CONTINUUM of Care
Single EHR Single Source of INFORMATION
Patients POPULATIONS
18

A Transformational Mindset
19

20
HOW Approaching Performance Improvement
• Physician-led
• Reduce Clinical Variation & Standardize Care
• Improve and Sustain Clinical Outcomes
• Improve Patient Experience
• Reduce Costs
Clinical Collaboratives
21
• Evidence-based Care Pathways
• Order Sets
• Staff and Patient Education Tools
• Leading and Lagging Indicators
• Implementation Plan
• Communication Plan
Objectives
22

SYST
EM P
AR
TNER
SHIP
S Pe
rfo
rma
nce
Exc
elle
nce
Sta
nd
ard
s
CULTURE PROCESS TECHNOLOGY
Safety Team Learning
TRUST
HIGH RELIABILITY ORGANIZATION
STRUCTURE
Collaboratives Focused Interventions
5 Principles of HRO’s 1. Sensitivity to operations (Situational awareness) 2. Preoccupation with failure (Proactive instead of reactive 3. Reluctance to simplify (Multiple viewpoints) 4. Deference to expertise (Shared decision making) 5. Commitment to resilience (Containment capabilities)
Partners • Quality • Finance • Service Excellence • Colleagues (clinicians) • Business Operations • Corporate • Constituents • Consumers • Support Services (e.g. Carelines, Service Lines) • Human Potential (e.g. ILD, change management) • Information Technology • Business Intelligence
NO
YES
NO
Prioritization
YES
Collaborative Criteria?
Operational Priority?
23

What Qualifies As A Collaborative?
INCLUSION CRITERIA (Draft) • Addresses clinical variation
• Pareto analysis for high cost
• Risk contract requirement
• Continuum of care
• Purchaser potential priority (future contract requirement)
EXCLUSION CRITERIA (Draft) • Business Unit specific
• Department specific
24

Clinical Integration
25
MCC Board of Managers
Clinical Leadership Committee
Network Development Committee
Collaboratives
Standard Pathways
Guidelines
Core Performance Measures

Alignment
contract focus
multicare focus
What purchasers &
payors are telling us
is important to them
Our
interpretation of
what we think
matters most
Partnering for healing &
a healthy future
CO
LL
AB
OR
AT
IVE
S
26

Key Considerations
• PEOPLE
– right skills
– right temperament
– role clarity
• FOCUS & ALIGNMENT
– prioritization
– discipline
• INFORMATION-DRIVEN INSIGHT
– credible
– actionable
– real-time
• MEASURABLE
– deployment
– adoption
– favorable results
27

1 People
Executive Oversight
Quality Safety Steering Council
Physician Lead Operations Lead Clinical Lead
Lead
ers
hip
&
Dir
ect
ion
Co
ord
inat
ion
, A
lign
men
t &
A
cco
un
tab
ility
Critical Resources Operations Clinical Subject Matter Experts
Exe
cuti
on
28

1 People
Executive Oversight
Quality Safety Steering Council
Physician Lead Operations Lead Clinical Lead
Lead
ers
hip
&
Dir
ect
ion
Co
ord
inat
ion
, A
lign
men
t &
A
cco
un
tab
ility
Critical Resources
Operations Clinical Subject Matter Experts
Exe
cuti
on
29

2 Focus & Alignment
• Performance improvement framework
• Market differentiator for our CIN
• Staying relevant
• Aligned with strategic objectives (LEM)
Internal Opportunity
Existing Risk-Based
Contract Measures*
Anticipated Purchaser Priorities
Collaboratives
30

Alignment
31
Primary
Care
Critical
Care
Emergency
Services
Medicine Pediatrics Surgery Women’s
Services
Readmissions
LOS
Service Excellence
Mortality
*Cardiac is managed separately via the Pulse Heart Institute
50 40 55 40 50 70 30
>300

Clinical Collaboratives QI Contractual Deliverables
Quality Improvement Plans Deliverable
Date
Potentially Avoidable Hospital Readmissions 30-Sep-15
Care Coordination for High-Risk Patients 30-Sep-15
Obstetrics and Maternity Care 31-Dec-15
Total Hip and Knee Surgery Bundle 31-Mar-16
Spinal Fusion Bundle 31-Mar-16
Cardiology Improvement 31-Mar-16
End of Life Care Improvement 30-Jun-16
Low Back Pain Improvement 30-Jun-16
Addiction and Dependence Treatment Improvement
30-Jun-16
Spine (Acute BP)
Ortho Joints
Spine (Surgical )
Heart Failure
AMI CAB
Gyn OB
Colon Glycemic Control
Surgery Collaborative
Pneumonia COPD Spirometry
Medicine Collaborative
Sepsis Resp
Failure Early
Mobility ARDS
Critical Care Collaborative
Cardiac Collaborative
Peds Cohort
Pediatric Collaborative
Quality Improvement Plans Deliverable
Date
Potentially Avoidable Hospital Readmissions 30-Sep-15
Care Coordination for High-Risk Patients 30-Sep-15
Obstetrics and Maternity Care 31-Dec-15
Total Hip and Knee Surgery Bundle 31-Mar-16
Spinal Fusion Bundle 31-Mar-16
Cardiology Improvement 31-Mar-16
End of Life Care Improvement 30-Jun-16
Low Back Pain Improvement 30-Jun-16
Addiction and Dependence Treatment Improvement
30-Jun-16
Quality Improvement Plans Deliverable
Date
Potentially Avoidable Hospital Readmissions 30-Sep-15
Care Coordination for High-Risk Patients 30-Sep-15
Obstetrics and Maternity Care 31-Dec-15
Total Hip and Knee Surgery Bundle 31-Mar-16
Spinal Fusion Bundle 31-Mar-16
Cardiology Improvement 31-Mar-16
End of Life Care Improvement 30-Jun-16
Low Back Pain Improvement 30-Jun-16
Addiction and Dependence Treatment Improvement
30-Jun-16
Quality Improvement Plans Deliverable
Date
Potentially Avoidable Hospital Readmissions 30-Sep-15
Care Coordination for High-Risk Patients 30-Sep-15
Obstetrics and Maternity Care 31-Dec-15
Total Hip and Knee Surgery Bundle 31-Mar-16
Spinal Fusion Bundle 31-Mar-16
Cardiology Improvement 31-Mar-16
End of Life Care Improvement 30-Jun-16
Low Back Pain Improvement 30-Jun-16
Addiction and Dependence Treatment Improvement
30-Jun-16
Quality Improvement Plans Deliverable
Date
Potentially Avoidable Hospital Readmissions 30-Sep-15
Care Coordination for High-Risk Patients 30-Sep-15
Obstetrics and Maternity Care 31-Dec-15
Total Hip and Knee Surgery Bundle 31-Mar-16
Spinal Fusion Bundle 31-Mar-16
Cardiology Improvement 31-Mar-16
End of Life Care Improvement 30-Jun-16
Low Back Pain Improvement 30-Jun-16
Addiction and Dependence Treatment Improvement
30-Jun-16
Quality Improvement Plans Deliverable
Date
Potentially Avoidable Hospital Readmissions 30-Sep-15
Care Coordination for High-Risk Patients 30-Sep-15
Obstetrics and Maternity Care 31-Dec-15
Total Hip and Knee Surgery Bundle 31-Mar-16
Spinal Fusion Bundle 31-Mar-16
Cardiology Improvement 31-Mar-16
End of Life Care Improvement 30-Jun-16
Low Back Pain Improvement 30-Jun-16
Addiction and Dependence Treatment Improvement
30-Jun-16
Spine (Acute BP)
OB Gyn
CAB AMI Heart
Failure
Ortho Joints
Spine (Surgical )
Women’s Collaborative
Paying Attention to Your Ecosystem
32

3 • Evidence-Based Best Practice
– Care pathways
– Care guidelines
• Data analytics testing
• Data definitions and standards
• Rapid feedback loops
Information-Driven Insight
Data
Information
Knowledge
33

4 Measureable
• Specific
• Measureable
• Achievable
• Relevant
• Time-bound
34

Consistent Process
Stabilization Deployment /
Implementation Development Investigate
Prioritize / Establish Aims
35
0 month 1-3 months 3-9 months 9-12 months 12+ months
• SMART AIM statement for each collaborative
• Reporting needs identified
• Baseline data and current state process map.
• Prioritization of specific opportunities for improvement related to AIM.
• Draft practice guideline
• Care Guideline/Pathway
• Final order sets
• Training plan & materials
• Performance management plan
• Education materials
• Monthly/quarterly report on outcome metrics
• 3, 6, 9, 12 month follow up reports to assess and mitigate risks
GU
IDEL
INE
AP
PR
OV
AL

RACI Assessment
• Owns the project/problem
Responsible
• Must approve work before it is effective
Accountable
• Has information/capability necessary to complete the work
Consulted
• Must be notified of results, but need not be consulted
Informed
36

Role Clarity
Prioritize I/C A A I/C R C I
Investigate I A A I R C I
Develop C/R A A C/R R C C
Implement A A A A R C C
Stabilize A A A A R C I
37
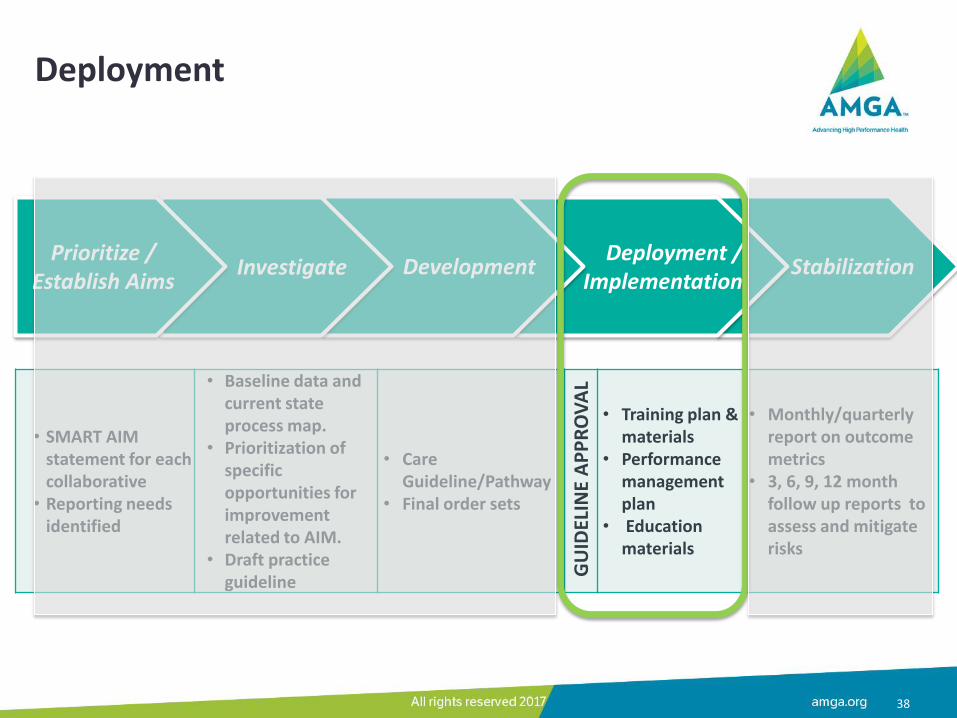
Deployment
Stabilization Deployment /
Implementation Development Investigate
Prioritize / Establish Aims
• SMART AIM statement for each collaborative
• Reporting needs identified
• Baseline data and current state process map.
• Prioritization of specific opportunities for improvement related to AIM.
• Draft practice guideline
• Care Guideline/Pathway
• Final order sets
• Training plan & materials
• Performance management plan
• Education materials
• Monthly/quarterly report on outcome metrics
• 3, 6, 9, 12 month follow up reports to assess and mitigate risks
GU
IDEL
INE
AP
PR
OV
AL
38

Buy-in & Approval
18 months 6 months 6 weeks
39

Adoption
Rapid Feedback Loops • Leading (In Process):
– order set utilization
– NOREADMITS
• Lagging (Outcomes):
– Readmissions
– Elective induction rates
– Wound infections
• Public comments
• BI requests
• Physician Engagement
Other Forms of Engagement • Public comments
• BI requests
• Physician Engagement
40
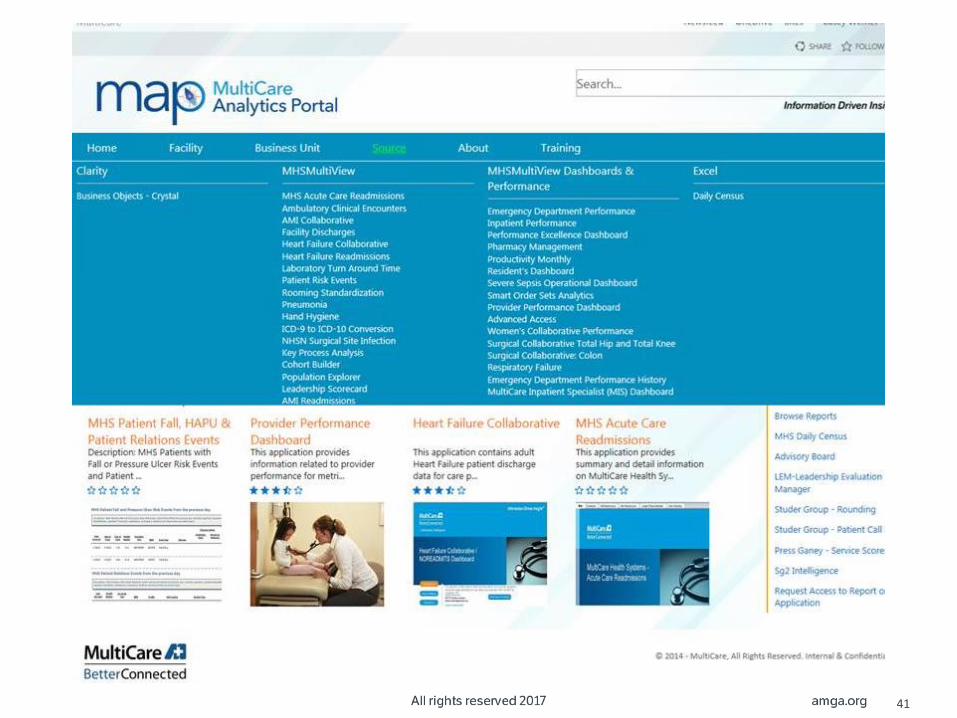
41

by specific physician
name
42

USE CASE COPD
43

1 & 2 People, Focus & Alignment
Prioritize & Investigate
Develop & Implement
Stabilize
• Diverse range of stakeholders
• Patient-centered • System Objective
• Improving quality + lowering the cost
• Engagement and adoption
• Universal solution • Sustained results
44

3 Information-Driven Insight
• Building an enterprise-wide approach:
–Root cause analysis (system/facility/provider group/etc.)
–Order set
–Access to data
– Education & training
–Correlate processes with outcomes
45

4 • Correlate processes with outcomes
– 22% reduction in COPD readmissions from 2015 to YE 2016
– 95% of COPD patients assessed for readmission rate
– 89% increase in COPD Order Set utilization from 2015 to YE 2016
– 42% improvement in PCP notification
Measurable
46

USE CASE Women’s Health
47

1 & 2 People, Focus & Alignment
Prioritize & Investigate
Develop & Implement
Stabilize
• Agreed upon aspiration of standards
• Aligning systems & processes across the enterprise
• Highly engaged physicians and staff
• Channeling efforts and passion to yield results
• Realtime transparency to sustain improvements & results
48

3 Information-Driven Insight
Spark Change
Adoption success
Multiple reimbursement models
Real-time data
Predictable deployment
Marketable outcomes
49

4 • Improved care, efficiency and market share
– 68% reduction in episiotomy rate
– Consistently held Elective Induction rate to 0% for calendar year 2016
– 3-fold increase in the percent of non-invasive hysterectomy techniques
– Rate of exclusive breast feeding increased to 70% at YE 2016
Measureable
50

Wrap Up
51

The journey continues...
Lesson 2014 2015 2016
Top Down Initiated; tied to the ACO Implemented Built into organization-wide objectives
Rapid Sequential Clunky Improved Ongoing optimization
Change Management Ad hoc Implemented practice outreach; public comment periods
Integration into ACO committees
Resource Patchwork Budgeted & Purchased Service Level Agreements
Education Ad hoc Consistent CME events
Don’t Boil the Ocean Anecdotal prioritization Contract alignment Data-driven prioritization
Design + Deploy Strong design, limited deployment
Increased focus on deployment
Ongoing
Good Enough Ongoing Ongoing Ongoing
Approval Process Initial formal process Refinement Simplification
Physician Engagement Silo’d Employed Network
52
Next Steps
• Focused Interventions (HRO)
• Further alignment with operations
• Core measures prioritization
• Ongoing alignment across the organization
• HIE and data reporting
53

Objectives
To outline governance and structure to support your physicians and staff
To describe how to efficiently develop evidence-based guidelines & pathways
Explain how to implement data analytics to engage your teams in performance improvement
54































