-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
1/12
FEATURE REVIEW
How psychotherapy changes the brain the contributionof
functional neuroimagingDEJ Linden1,2
1School of Psychology, University of Wales Bangor, Bangor, UK
and 2North West Wales NHS Trust, Bangor, UK
A thorough investigation of the neural effects of psychotherapy
is needed in order to provide aneurobiological foundation for
widely used treatment protocols. This paper reviews
functionalneuroimaging studies on psychotherapy effects and their
methodological background,including the development of symptom
provocation techniques. Studies of cognitivebehavioural therapy
(CBT) effects in obsessive-compulsive disorder (OCD) were
consistentin showing decreased metabolism in the right caudate
nucleus. Cognitive behavioural therapyin phobia resulted in
decreased activity in limbic and paralimbic areas. Interestingly,
similareffects were observed after successful intervention with
selective serotonin reuptakeinhibitors (SSRI) in both diseases,
indicating commonalities in the biological mechanisms of
psycho- and pharmacotherapy. These findings are discussed in the
context of currentneurobiological models of anxiety disorders.
Findings in depression, where both decreasesand increases in
prefrontal metabolism after treatment and considerable differences
betweenpharmacological and psychological interventions were
reported, seem still too heterogeneousto allow for an integrative
account, but point to important differences between the
mechanismsthrough which these interventions attain their clinical
effects. Further studies with largerpatient numbers, use of
standardised imaging protocols across studies, and
ideallyintegration with molecular imaging are needed to clarify the
remaining contradictions. Thiseffort is worthwhile because
functional imaging can then be potentially used to monitortreatment
effects and aid in the choice of the optimal therapy. Finally,
recent advances in thefunctional imaging of hypnosis and the
application of neurofeedback are evaluated for theirpotential use
in the development of psychotherapy protocols that use the direct
modulation ofbrain activity as a way of improving
symptoms.Molecular Psychiatry(2006)11, 528538.
doi:10.1038/sj.mp.4001816; published online 7 March 2006
Keywords: psychotherapy; anxiety disorders; depression;
functional magnetic resonanceimaging; positron emission tomography;
selective serotonin reuptake inhibitors
Introduction
It has long been recognised by clinicians thatpsychological
interventions can profoundly alterpatients sets of beliefs, ways of
thinking, affectivestates and patterns of behaviour. Yet the
putativemechanisms and underlying changes in the brainhave only
recently attracted the attention theydeserve.1 This enterprise is
important for two mainreasons. First, psychotherapy needs to be
based on asound understanding of the biological processesinvolved.
There is no reason why this generalstandard of contemporary
medicine, which is, forexample, needed in order to detect and fight
potentialside effects, should not apply here as well. Second, a
better understanding of these biological mechanismsmight aid in
the improvement of therapeutic inter-
ventions or even in the utilisation of these verymechanisms, as
in the case of neurofeedback.
One reason for the sluggish development of re-search into the
neural side of psychotherapy might bethat here plastic changes in
the human brain have to
be detected with noninvasive techniques, whileconventionally
plasticity research has been con-ducted at the cellular level. Yet
the tools of non-invasive functional brain imaging can now
reliably
detect training- and learning-related changes in brainactivation
patterns in healthy volunteers,2 and thereis no reason why this
should not be possible in thoseaffected by mental disorders as
well. Potentially,functional imaging can detect
psychotherapy-relatedchanges at the level of brain areas and
circuits, andthus contribute to an elucidation at least of the
mostglobal neural mechanisms (Figure 1a). Such anapproach would not
only benefit basic research intothe mechanisms of action of
psychotherapy, but alsoaid our understanding of differences and
commonal-ities between psycho- and pharmacotherapy, providea
further tool for the evaluation of therapy effects and,might
ultimately help clinicians to select optimal
Received 30 August 2005; revised 24 January 2006; accepted
30January 2006; published online 7 March 2006
Correspondence: Dr DEJ Linden, School of Psychology,
Universityof Wales Bangor, Brigantia Building, Penrallt Road,
Bangor LL572AS, UK.E-mail: [email protected]
Molecular Psychiatry (2006) 11, 528538&2006 Nature
Publishing Group All rights reserved 1359-4184/06$30.00
www.nature.com/mp
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
2/12
treatment for individual patients on the basis ofbaseline
functional activation patterns3,4 (Figure 1b).
Most functional imaging studies into psychother-
apy effects have been conducted with nuclearmedicine methods
like positron emission tomography(PET) or single photon emission
computed tomogra-phy (SPECT), and assessed changes in brain
metabo-lism or blood flow between a pre- and post-treatmentscan.
The use of functional magnetic resonanceimaging (fMRI), which does
not expose the patientto radiation, would potentially confer the
advantageof more measurement points, including measures of
brain activation during treatment or at follow-up. YetfMRI has
traditionally been used to probe the brainactivation patterns
during perceptual or cognitivetasks, rather than to measure
baseline brain metabo-lism. The use of fMRI for the detection of
psychother-
apy-related changes thus presupposed twomethodological
developments, the measurement ofthe neural correlates of
psychopathology5 and tech-niques for symptom provocation in the MRI
environ-ment.6
In this article, I shall first review functional imagingstudies
that used symptom provocation techniques tomimic psychopathological
states in a laboratorysetting. This avenue of research has been
particularlysuccessful in obsessive-compulsive disorder (OCD)and
simple phobias, and is also being pursued forsocial phobia,
depression, and post-traumatic stressdisorder (PTSD). I shall go on
to review the reports oftreatment trials that monitored the effects
of psy-chotherapy with one of the functional imagingtechniques,
sometimes comparing it with a groupreceiving standard
pharmacotherapy. Subheadings forthe review of these studies will be
according todisease (phobia, OCD, depression), rather than ima-ging
modality. The selection of the material reviewed
in this section was based on a Pubmed search for theconjunctions
of the term psychotherapy with func-tional imaging, functional
magnetic resonance,positron emission, and single photon emission,on
the reference sections of the retrieved originalreports, and on a
textbook to which the authorcontributed.7 Studies on patients under
the age of 18or on single cases were not included, nor were
studiesemploying other biological markers or looking
atpsychological interventions for substance abusedisorders. A
search of The Cochrane Database ofSystematic Reviews
(http://www.mrw.interscience.wiley.com/cochrane/cochrane_clsysrev_arti-cles_fs.html,
accessed on 14 December 2005) did not
yield existing systematic reviews of this topic. In thefinal
sections, I shall discuss potential molecularmechanisms of
psychological interventions, reviewfindings on neurobiological
effects of specific psy-chological interventions and suggest topics
for furtherresearch.
Symptom provocation and functional imaging
Symptom reduction is one of the main aims ofpsychotherapy in
general, and can be regarded asthe benchmark against which the
success of beha-
vioural and cognitive therapies is to be measured.Elucidation of
the neural correlates of symptomreduction is therefore a primary
goal of any investiga-tion into the biological mechanisms of
psychotherapy.The reliable induction of the symptoms in question
inthe imaging environment has been an important toolfor this
enterprise. Such a symptom provocation willpermit the comparison of
brain responses to triggerscenarios (e.g. for social phobia or
PTSD) or stimuli(e.g. for simple phobias) before and after
treatment,and thus the assessment of therapy effects on
neuralactivation. It furthermore has the benefit of allowingthe
comparison of response patterns to trigger stimuliin patients and
healthy controls,810 elucidating
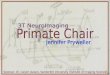
Figure 1 Three possibilities of integrating psychotherapyand
functional neuroimaging with potential clinical im-plications. (a)
Baseline imaging measures (with any of thetechnique discussed in
the review) are obtained (1) before a
course of psychotherapy (2), after which patients areclassified
as responders or nonresponders based on symp-tom improvement or
other clinical outcome measures (3)and re-examined with the imaging
protocol (4). Thistechnique allows for the assessment of
psychotherapy-related changes in brain activation and their
specificity forsuccessful outcome. With some modifications, this
ap-proach has been used in all studies cited in Tables 13.(b)
Baseline imaging measures are obtained (1) before acourse of either
psycho- or pharmacotherapy (2), afterwhich patients are classified
as responders or nonrespon-ders (3). This outcome information is
entered into ananalysis of the pretreatment imaging data (4) with
the aimof deriving activation patterns that are predictive
oftreatment response (5). (c) Imaging identifies abnormalactivity
in a particular brain area or network in a patient (1).This
abnormal brain activity is targeted by psychotherapy(based on
information derived from studies of type (a),neurofeedback, or a
combination of both (2). Patients arethen classified as responders
and nonresponders (3). Theoutcome data can then be compared with
standardtreatment protocols. Post-treatment imaging (4) will
beinformative but not mandatory.
Functional neuroimaging and psychotherapyDEJ Linden
Molecular Psych
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
3/12
commonalities and differences in the processing ofaversive
material.
A paradigm for the provocation of OCD symptomsduring PET
scanning was developed by Rauch et al.11
They demonstrated increased regional cerebral bloodflow (rCBF)
in the right caudate, left anteriorcingulate cortex (ACC) and
bilateral orbitofrontalcortex (OFC) when patients were exposed to
indivi-dually tailored provocative stimuli compared toneutral
stimuli. Orbitofrontalstriatalthalamic acti-vation was also
reported by McGuire et al.,12 whoadditionally found activity in the
left hippocampusand posterior cingulate gyrus to correlate with
theintensity of OCD symptoms. They suggested that theformer network
might reflect urges to performcompulsive movements, while the
latter might bemore related to the accompanying anxiety. Breiter
etal.8 used a similar approach with fMRI, showingincreased blood
oxygenation level-dependent (BOLD)signal in the right caudate,
bilateral OFC, prefrontal
cortex (PFC) and temporal lobes. Thus, the conver-ging evidence
from these studies points to increasedneural activity in the right
caudate and bilateral OFCduring the experience of symptoms of OCD.
Addi-tionally, the insula seems to be activated whencontamination
fear is prominent.10 OFC and insulawere activated during the
provocation of phobicsymptoms as well,13 as was the left
amygdala.14
Symptom provocation studies of PTSD were basedeither on the
presentation of trauma-related visual oracoustic stimuli or on
script-driven imagery. Thelatter technique induces traumatic
imageries and thusmimics flashbacks of the aversive events (as
evi-denced by both subjective ratings and psychophysio-
logical parameters) by reading accounts of theirindividual
traumatic experiences to patients duringfunctional imaging.15
Increased activation of the rightamygdala was found across
provocation techniquesand imaging modalities,1517 while medial
prefrontalareas were consistently reported to be less active inPTSD
patients than controls when traumatic eventshad to be
recalled.18,19 In regions of the medialtemporal cortex commonly
associated with memoryretrieval and visual association areas
involved inmental imagery both higher and lower activation have
been reported for PTSD patients, possibly reflectingthe
heterogeneity of patient samples across studies.
Both autobiographical scripts and visual materialhave been used
to induce sadness in patients withdepression and healthy
volunteers. Beauregardet al.20
found higher activation in ACC and left medial PFCin patients
than controls. Mayberg et al.21 foundactivity in the subgenual
cingulate cortex to be high
both when sadness was induced in healthy indivi-duals and when
dysphoric symptoms were present inpatients with MDD. One consistent
finding seems to
be that the amygdala (particularly on the left) showshigher
and/or longer responses to sadness-inducingstimuli in depressed
patients than controls.22,23 Anormalisation of this induced
amygdala hyperactivityhas been observed after treatment with
antidepres-
sants,22 but functional imaging studies of psychother-apy
effects in depression have so far exclusivelyrelied on resting
state metabolic patterns. The same istrue for most studies on OCD,
while studies on phobiahave utilised the symptom provocation
techniquesdescribed above to assess the physiological effects
ofpsychotherapy.
Functional imaging studies of psychotherapyeffects
Obsessive-compulsive disorderIncreased activity in the right
caudate was thecommon finding of symptom provocation studies inOCD
across imaging modalities.8,11 Correspondingly,all studies of the
effects of cognitive behaviouraltherapy (CBT) in OCD on resting
state glucosemetabolism or blood flow (Table 1) so far reported
adecrease in right caudate activity in treatmentresponders.2426
This decrease of caudate activity
correlated with clinical improvement in one of thestudies, and
showed no difference between CBT andtreatment with the selective
serotonin reuptakeinhibitor (SSRI) fluoxetine.24
Two studies24,25 reported a correlation betweencaudate, OFC and
thalamus activity before treatment,which would conform to current
pathophysiologicalmodels of OCD.27,28 This correlation disappeared
aftertreatment with either CBT24,25 or fluoxetine,24 againpointing
to common or converging mechanisms
between psycho- and pharmacotherapy. The confir-mation of such
converging effects would not only beclinically relevant but also
help elucidate themechanisms of psychotherapy at the cellular
andneurotransmitter level.
The only fMRI study of CBT effects in OCD29
assessed both effects on symptom provocation andon activation
during a cognitive task (the Stroop task).Unfortunately, in this
study, data from the CBT andthe SSRI group had to be pooled because
of otherwiseinsufficient power, which made a comparison be-tween
pharmaco- and psychotherapy impossible.
PhobiasSimple phobias are particularly suited to the
inves-tigation of treatment effects with fMRI becausesymptom
provocation is relatively straightforward
(Table 2). Whereas in most studies of OCD, PTSDand depression,
the inducing triggers had to betailored individually, the symptoms
of spider phobiacould be mimicked by standardised images14 or
filmsequences30 of spiders, contrasted with innocuousanimals or
natural objects. This use of identicalstimulus material across
participants removes asource of variance that is especially
undesirable instudies with small sample sizes.
Paquette et al.30 used this symptom provocationtechnique in
order to assess the effect of symptomreduction by CBT directly.
Before the intervention,patients showed increased activity of right
dorsolat-eral PFC and parahippocampal gyrus to the aversive
Functional neuroimaging and psychotherapyDEJ Linden
530
Molecular Psychiatry
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
4/12
Table 1 Psychotherapy effects in OCD
Authors Trial size/interventions andprepost interval
Functional imaging technique Post-treatment decre
Baxteret al.24 N= 9 CBT,N= 9 fluoxetine,N= 4 healthy controlsa,
all 1072 weeks
FDG (fluoro-deoxyglucose)-PET,resting state, normalised data,no
PVCb
Responders: right caucorrelation between caudate and thalamu
Schwartzet al.25 N= 9 CBT, 1072 weeks FDG-PET, resting
state,normalised data, no PVC
Responders: caudatecorrelation between
caudate and thalamuNakataniet al.26 N=22 CBT
(some also received clomipramine),duration based on clinical
improvement
Xenon-enhanced CT(measures rCBF),resting state
Right head of caudat
Nakaoet al.29 N= 6 CBT,N= 4 fluvoxamine,12 weeks
fMRI during Stroop task andsymptom provocation
Bilateral OFC, DLPFACC (symptom prov
aControl groups are only listed where a second measurement after
an interval comparable to the treatment period was
obtainedpretreatment effects (as, e.g., in Nakatani et al.26).bPVC:
partial volume correction.cFor some parts of the PET data analysis,
data were pooled with those from Baxter et al.24.dBecause of the
small N, data for the CBT and fluvoxamine groups were not analysed
separately.
Table 2 Psychotherapy effects in phobias and panic disorder
Authors Trial size/interventions andprepost interval
Functional imaging technique Post-treatment decreases
Furmarket al.34 Patients with social phobia,N= 6: CBT,N= 6:
citalopram,N= 6: waiting list, all 9 weeks
PET with oxygen15-labeled water,symptom provocation,normalised
data, no PVC
Both treatment groups:bilateral amygdala,
hippocampus,parahippocampal gyrus,further paralimbic areas
Paquetteet al.30 Patients with spider phobia,N= 12: CBT, 5
weeks
fMRI, symptom provocation Right dorsolateral PFC,parahippocampal
gyrus
Straubeet al.
31
Patients with spider phobia,N= 14: CBT, 2 sessions,N= 14:
waiting list
fMRI, symptom provocation Bilateral insula, thalamus,ACC in
treatment but notwaiting list group
Praskoet al.75 Patients with panic disorder,N= 6: CBT,N= 6:
different antidepressants,
both groups 3 months
FDG-PET, resting state,normalised data
Both treatment groups:mainly right frontal andtemporal
regions,with partial overlapacross groups
MolecularPsychiatry
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
5/12
sequences. This difference disappeared after fourintensive
exposure sessions in a group setting.Instead, patients showed a
higher activity in visualassociation areas for aversive than
neutral sequences,similar to the pattern observed in the
healthycontrols. Thus, CBT seems to have led to a restitutionof
normal cortical processing of the spider sequencesin these
patients. A recent study by Straube et al.31
employed a similar design, but added a waiting listpatient
group. Patients showed higher activation inthe ACC and insula
bilaterally when pretreatmentfMRI was compared to healthy controls.
This hyper-activation remained at the second measurement in
thewaiting list group, but disappeared in the grouptreated with
CBT. Thus, again, CBT of spider phobiawas accompanied by a
normalisation of brain activityin specific areas. This reduction of
ACC and insulaactivity might reflect (or underlie) the attenuation
ofthe affective response to spiders after
successfultreatment.31
Yet these studies30,31
probably do not present thefull pattern of pathological
activation in simplephobias. For example, no hyperactivity was
observed
before treatment in the amygdala in the study byPaquetteet
al.,30 and neither study reported reductionof amygdala activity
after treatment. This is at oddswith most studies of affective
stimulus processingand aversive conditioning, and indeed with
currentmodels of the pathophysiological network of simplephobias,
and might be explained by habituationeffects in the block
design.14
Several studies of patients with social phobia havealso shown
hyperactivity of the amygdala, even witha weak form of symptom
provocation, presentation of
human faces.32,33 After successful treatment, eitherwith CBT or
citalopram, activation of amygdala andhippocampus was reduced in
the symptom provoca-tion study by Furmark et al.,34 who utilised a
publicspeaking task. Again, it is interesting to observe thatthe
pharmacological and psychological interventionseem to have
modulated the same brain areas, in thiscase parts of the limbic
system. In the studies on OCD(see preceding section), CBT and SSRI
had similareffects on metabolic patterns as well, presumablyleading
to a reduction of the activity of fronto-striato-thalamic
circuits.
Depression
While symptom provocation and resting state studiesproduced
fairly consistent signatures of pathologicalmetabolism for OCD
(right caudate hyperactivity) andphobias (limbic and paralimbic
hyperactivity), thesituation is more complicated for major
depressivedisorder (MDD). Most studies of resting state bloodflow
or metabolism reported an anterior prefrontalhypoperfusion that
normalised after the remission ofsymptoms of depression.35,36
Conversely, the inter-vention study by Brody et al.37 started from
an initialprefrontal hypermetabolism that normalised in boththe
IPT- and the SSRI-treated group (Table 3). T
able
3
Psychotherapyeffectsinm
ajordepressivedisorder(MDD)
Authors
Trialsize/interv
entions
andprepostin
terval
Functionalimaging
technique
Post-treatmentd
ecreases
Post-treatmentincre
ases
Brodyetal.37
N=14:IPT,
N=10:paroxeti
ne,
N=16:healthy
controls,
all12weeks
FDG-PET,restingstate,
globalnorm
aliseddata,
imagefusionwithMRI
Bothtreatmentg
roups:
bilateralPFC;IP
T:
leftventralACC;
paroxetine:leftmiddleACC
Bothtreatmentgrou
ps:
lefttemporallobe
Martinetal.39
N=13:IPT,
N=15:
venlafaxine,all
6weeks
HMPAO-SP
ECT,restingstate,
normalised
data,noPVC
None
IPT:Rightbasalgan
glia,posteriorCC;
Venlafaxine:rightbasalganglia,
posteriortemporalcortexa
Goldappleetal.38
N=14:CBT,
2677weeks
(standarddevia
tion),
N=13:paroxeti
ne,
6weeks(sampl
efrom
differentstudy)
FDG-PET,restingstate,
normalised
data,noPVC
CBT:bilateralPF
C;
Paroxetine:righthippocampus
CBT:bilateralhippo
campus,
dorsalCC;Paroxetine:
leftdorsolateralPFC
aTheposteriortemporalcortexactiv
ationwaseliminatedwithonepatie
ntsexclusion.
Functional neuroimaging and psychotherapyDEJ Linden
532
Molecular Psychiatry
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
6/12
Decreases in lateral prefrontal metabolism were alsoobserved
after successful treatment with CBT.38
In this study by Goldapple et al.,38 the group thatunderwent
pharmacological treatment differed fromthe CBT group in that it
showed an increasedmetabolism in left dorsolateral PFC after the
trial.Although this finding does not directly contradictthat of
Brody et al.,37 because in that study thedecrease of PFC metabolism
in the SSRI group wasmore ventral and lateral, it indicates that
mechanismsof pharmaco- and psychotherapy might be moredivergent in
MDD than in the disorders discussedabove. Yet one region of
convergence of the twoapproaches seems to be in the right basal
ganglia,where another recent study39 found increased activityafter
successful treatment with either IPT or venlafax-ine, a combined
serotonin and norephinephrinereuptake inhibitor.
The functional imaging studies of therapy effects inMDD thus
yielded partly heterogeneous results across
studies and also across treatment approaches. Theheterogeneity
across studies might be an effect of themany different symptoms
that can contribute to adiagnosis of MDD according to the DSM IV,40
the useof resting state (rather than symptom provocation)paradigms
and the absence of well-characterised andreplicable abnormalities
prior to treatment.41 It is alsoimportant to consider that all of
the PET or SPECTstudies on treatment effects in depression
reportednormalised, rather than absolute or quantitativeregional
blood flow or glucose metabolism (Table 3)(the same applies to
studies on phobia and OCD,Tables 1 and 2). The normalisation
approach yieldsratios of activity for each region of interest
(ROI)
compared to the global mean of the whole brain or theipsilateral
hemisphere. Thus, changes in global brainmetabolism or blood flow
between pre- and post-treatment scan can influence the outcome in a
ROI.An absolute increase in rCBF or regional glucosemetabolism
might still result in a lower ratio to globalactivity, if the
latter increases more, and would thus
be reported as post-treatment decrease of normalisedactivity.
Fully quantitative studies42 would be a wayto resolve this issue,
but are considerably moredifficult and invasive.
Another important feature of the methodologyemployed in the
reviewed studies is the absence of
corrections for differences in tissue volume. De-creased
regional blood flow or glucose metabolism,as measured by PET or
SPECT, does not necessarilyreflect reduced neural activity, but
might be an effectof locally reduced grey matter volume. This
partialvolume effect is due to the low spatial resolution ofthese
techniques. It has been shown to explain, atleast partly, reduced
blood flow and metabolism insubgenual cingulate cortex in patients
with depres-sion.43 In this data set, full correction for
corticalvolume differences even resulted in a reversal of
theeffect, with patients showing higher metabolic activ-ity than
controls.44 Thus, any local hypometabolismin a patient group can be
an effect of cortical volume
loss in that area, although volume loss in areasoutside the
limbiccorticostriatopallidothalamicloop has rarely been reported in
MDD.45
Whether loss of brain tissue might have thusexplained some of
the metabolic decreases aftertreatment cannot be determined based
on the presentstate of the literature. While some studies on
childrensuffering from OCD found grey matter decreases
aftertreatment with the SSRI paroxetine,46,47 volumetricmeasures
were stable in a group of adult patients withunipolar depression
over a 3-month period of treat-ment with antidepressants.43 It
would certainly behelpful if future functional imaging studies
alsoincluded high-resolution MRI before and after treat-ment to
determine potential structural changes andenable partial volume
correction.
At present, the available evidence suggests that anymodel that
relies on global frontal hypometabolism toexplain symptoms of
depression and its reversal toaccount for treatment effects would
be oversimplify-
ing the complex nature of cortico-cortical andsubcortical
interactions in affective disorders. Thedifference between the
neural correlates of clinicalimprovement after pharmacological and
psychologi-cal interventions37,38 is a case in point.
Thesedifferences were particularly pronounced in the study
by Goldapple et al.,38 where opposite changes wereobserved in
PFC (decrease after CBT, increase afterparoxetine) and limbic areas
(increase after CBT,decrease after paroxetine). The authors
interpretedthe specific CBT-related changes in brain activation
ascorrelates of the learned reduction of ruminations andmaladaptive
associative memories (frontal decreases)and increased attention to
emotional stimuli (limbic
increases). The differences between CBT and pharma-cotherapy
were explained in the framework of top-down versus bottom-up
effects, with CBT operatingmore through the former and
pharmacotherapy morethrough the latter (e.g. limbic and subcortical
areas).
The theoretical framework proposed by Goldappleet al.38 to
account for the observed differences in theneural effects of
psycho- and pharmacotherapy isattractive because it recognises that
any therapeuticimprovement of a complex disorder like depression
islikely to be mediated through altered interactions
between several brain areas rather than unidirectionalchanges in
a single region. It also allows for predic-
tions about changes in specific networks based on thecontent and
behavioural targets of a particularpsychological intervention.
However, it will ulti-mately have to be tested in prospective
trialscomparing pharmaco- and psychotherapy effects indepression,
ideally with the inclusion of molecularmarkers of their respective
effects at the synapticlevel.
Molecular mechanisms of psychotherapy
What, then, can we infer from the functional imagingliterature
on the molecular mechanisms that underlieor modulate responses to
psychotherapy? In the
Functional neuroimaging and psychotherapyDEJ Linden
Molecular Psych
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
7/12
absence of molecular imaging studies (e.g. PET
withneurotransmitter receptor ligands) of psychotherapyeffects,
these inferences will have to be indirect. Wecan evaluate the
extant functional imaging studies ofpsychotherapeutic interventions
as to their compat-ibility with and impact on current
neurobiologicaland neurochemical models of psychological
disor-ders, and we can adduce parallels from pharmacolo-gical or
alternative interventions, where molecularimaging studies have
indeed been performed.
With the development of specific radiotracers of theserotonin
transporter (SERT) for SPECT and PET,48,49
in vivo molecular imaging studies of the effects ofSSRIs have
become feasible. The main consistentfinding across these studies
has been that radiotracer
binding to SERT decreases with SSRI treatment,reflecting the
expected blockade of binding sites bythe SSRI. Blockade of SERT by
SSRI has beendocumented for midbrain, striatum, amygdala andfurther
subcortical areas. It has been shown to occur
in healthy individuals50
and in patients with depres-sion,5052 social phobia53 and
OCD.50,54 SERT occu-pancy was around 80% at therapeutic doses of
theSSRIs fluoxetine, citalopram, sertraline and parox-etine and the
serotonin and norephinephrine reup-take inhibitor velafaxine.50
How can these findings be related to the changesobserved in the
functional imaging studies discussedin this paper? The molecular
imaging studies indi-cated SSRI binding to SERT in areas, where
thefunctional imaging studies showed reduced bloodflow34 or glucose
metabolism24 in SSRI responders,for example, the amygdala for
social phobia53 and thestriatum for OCD.50 SERT-mediated reuptake
of
serotonin into the presynaptic cell, which is partlyblocked by
administering an SSRI, is an ATP-dependent and thus metabolically
very demandingprocess. The reduced metabolic activity in these
areasafter treatment with an SSRI might thus reflect thedecreased
activity of SERT. Reduced striatal glucosemetabolism in OCD and
reduced limbic blood flow insocial phobia were also observed after
CBT.24,34
The similarity of the functional imaging findingsindicates a
convergence of the neural pathways thatmediate pharmacotherapy and
psychotherapy effects,at least for phobia and OCD. This convergence
and thecommonalities in the clinical effects might suggest
that psychotherapy effects in anxiety disorders canalso be
mediated through the serotonin system.55
However, this claim is at present not supported bybiochemical or
molecular imaging evidence forchanges in the serotonin system after
psychologicalinterventions. Future studies of psychotherapy
inanxiety disorders should therefore assess potentialchanges in
neurotransmitter metabolites to determinewhich system is likely to
be involved. Concurrently,molecular imaging will be needed to
determine thelevel at which these changes take place. This
wouldhave to involve radiotracers that probe the presynap-tic (e.g.
transporter proteins), postsynaptic (e.g.receptors) and
postreceptor (e.g. proteins involved
in signal transduction) levels of synaptic transmis-sion.49
Functional imaging studies as discussed inthis paper cannot resolve
the molecular pathwaysmediating the therapy effects, but may play
animportant role in defining the target areas to beprobed with the
molecular techniques.
The molecular underpinnings of psychotherapyeffects in
depression likewise still wait to be ex-plored. Molecular imaging
studies of nonpharmaco-logical interventions have only been
performed fortotal sleep deprivation.56 The therapeutic success
ofsleep deprivation was associated with lower bindingof a dopamine
D2 receptor ligand and thus higherdopamine release, and with
reduction in cingulateperfusion. Reduced ACC glucose metabolism was
alsoobserved in patients with MDD who responded toIPT.37 This might
implicate the dopamine system inthe therapeutic effects of IPT, but
the other mono-amine neurotransmitters have been shown to
influ-ence the activity of the cingulate as well.37,57 The
reduced activity in lateral PFC, as evidenced byreduced glucose
metabolism, after both IPT37 andCBT38 has been suggested to be an
effect of increasedsynaptic serotonin, either through GABAergic
inhibi-tory interneurons or direct suppression of glutama-tergic
activity.37 Yet, multiple neuromodulatorsystems could be
responsible. Direct molecularimaging of psychotherapy effects in
depression willtherefore be paramount. Again, functional imaginghas
identified key nodes in the pathophysiologicalnetwork of
depression, such as the cingulate, basalganglia, lateral PFC and
hippocampus, that will beworthwhile targets for these molecular
studies.
Intervention-specific effects
The functional imaging studies of psychologicalinterventions in
mental disorders, which were re-viewed in the previous sections,
elucidated some ofthe neural correlates of symptom reduction
andgeneral clinical improvement. In most studies thatcompared
pharmacological and psychological inter-ventions (with the
exception of Goldapple et al.,38)the effects on cerebral metabolism
were rather similar.Thus, they are informative on the
dysfunctionalcircuits generating the symptoms of a specific
diseaseand potentially useful for treatment evaluation, but
reveal little about any specific neural mechanismsthrough which
psychotherapy might operate. In orderto clarify the neural
mechanisms of a psychologicalintervention, it will probably not
suffice to compare itto standard pharmacotherapy in a classic
controlledtrial setting. Rather, investigators will have to
changethe parameters of the treatment protocol, varying thedesired
mental states that they aim to induce, andapply it across different
patient groups. While thiswill be very challenging even with the
most standar-dised CBT protocols, the results obtained
withhypnosis, targeting specific mental states, and
withneurofeedback, explicity targeting specific brainareas, are
encouraging.
Functional neuroimaging and psychotherapyDEJ Linden
534
Molecular Psychiatry
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
8/12
Functional imaging of hypnosisPositron emission tomography
images were acquiredduring hypnosis while participants were exposed
tonociceptive stimuli. Hypnotic suggestions selectivelytargeted the
intensity and the affective component ofthe pain.58 In the latter
case, the painful experiencewas reported as being less aversive,
and ACC (but notsomatosensory cortex) activity was reduced.59
Con-versely, when the intensity of pain was modulated byhypnosis,
activity in the somatosensory cortex con-tralateral to the
stimulated hand was attenuated.60
Similar results were obtained during hypnosis-in-duced
depersonalisation.61
These studies revealed the neural correlates ofdifferent aspects
of hypnotic analgesia. They showedACC or somatosensory cortex to be
suppressed,depending on the content of the hypnotic suggestions.Yet
by what mechanism are these areas suppressed?Studies of hypnotic
induction and suggestion indi-cate that activation of medial PFC
and left dorsolat-
eral PFC62
might be nonspecific features of hypnosisthrough which the
effects on specific symptoms aremediated.
Neurofeedback with functional magnetic resonanceimagingWhile
hypnosis, in this respect similar to some CBTprotocols, aims to
induce certain mental states (andthe accompanying physiological
reaction), the newtechnique of neurofeedback directly targets
theactivity of a specific brain area. This technique,originally
developed with EEG slow cortical poten-tials at low spatial
resolution for binary communica-tion with paralysed patients,63 has
recently been
expanded for fMRI, using techniques for real-timeimage analysis.
Weiskopfet al.64 used such a braincomputer interface to train a
volunteer to modulatethe BOLD signal in his own ACC. The point
about thisapproach is that participants are not supposed tomodulate
activity of a certain brain region by engagingin a specific task
(e.g. increase activity in the fusiformface area by mental imagery
of faces), but learn toevoke a mental state that reliably
corresponds to acertain activation level in that region. For this
reason,noneloquent regions of the brain are ideally targetedto
demonstrate the feasibility of the fMRI-basedneurofeedback
technique.
The initial approach of deCharms et al.65
combinedthe induction of a specific mental state (imagining
ahand movement) with neurofeedback training, whichallowed their
volunteers to enhance activity inprimary motor cortex without
actually performing amovement. Such a self-regulation of cortical
activity
by neurofeedback might play a therapeutic role in itsown right,
and first reports on pain reduction bymodulation of ACC activity66
are encouraging. Thestudies reviewed here might help define target
areasfor the transfer of this technique to symptom reduc-tion in
psychiatric disorders. However, any lastingtherapeutic effect in
psychiatric patients wouldprobably require a modulation of
functional connec-
tivity patterns67 rather than solitary brain regions andthus
presuppose further methodological develop-ments.
Similar considerations apply to the assessment oftherapy effect
with the symptom provocation-basedfunctional imaging. While this
technique provides animportant instrument for the detection of
neuralchanges during psychotherapy, any stable changesin neural
networks or rewiring should becomemanifest in changes in functional
connectivity pat-terns that can be detected in asymptomatic states
aswell.
In sum, studies of hypnosis have revealed theability to
selectively suppress ACC or somatosensorycortex during nociceptive
processing, depending onthe aspect of pain that was to be
influenced. Theregulation of the activity of a particular brain
areamight also be achieved directly by neurofeedback.Combined with
the evidence from symptom provoca-tion techniques, this technique
may eventually result
in the development of neuroimaging-based psy-chotherapies
(Figure 1c). Beyond the interestingclinical possibilities, these
prospects also presentnew ethical challenges and will surely have
an impacton the mind-brain debate in the years to come.
General discussion and conclusions
Functional neuroimaging is a promising tool for theinvestigation
of the brain changes induced by psy-chotherapy. So far, only few
studies have used it toassess the effects of CBT in OCD and phobia,
and ofCBT and IPT in depression. In OCD, psychologicalintervention
led to decreased metabolism in the
caudate and a decreased correlation of right OFCwith ipsilateral
caudate and thalamus. The hyper-activity of the caudate in OCD and
its activitydecrease after intervention conform to its putativerole
in the pathophysiology of this disorder. Dysfunc-tional
striato-thalamic pathways have been impli-cated in inefficient
thalamic gating, leading tohyperactivity in orbitofrontal and other
corticalareas.68 Such a scenario would be compatible withthe
functional neuroimaging findings, especially ifincreased caudate
activity led to disinhibition of thethalamus by means of the direct
pathway, whichwould indeed increase the correlation between
caudate, thalamus and OFC activity. Finer resolutionof
functional imaging studies (e.g. in order to look forevidence of
suppression of activity at the level of theglobus pallidus
internus) would be required to furtherdisentangle the differential
contribution of the basalganglia to the pathophysiology of OCD. The
promi-nent reduction of caudate activity after treatmentmight be
explained in the context of the high level ofstriatal plasticity
that has been shown in numerousstudies of implicit and associative
learning in humanand animal models.69,70
In phobia, the most consistent effect of successfulCBT on brain
activation was a decrease in limbic andparalimbic areas. It is
plausible that decreasing
Functional neuroimaging and psychotherapyDEJ Linden
Molecular Psych
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
9/12
amygdala activation, in particular, should accompanythe
reduction of phobic symptoms because bothmechanical lesions and
chemical suppression of theamygdala have consistently resulted in a
reduction of
both subjective and psychophysiological measures offear.71
However, based on these functional imagingfindings alone, we cannot
determine whether thedecrease in amygdala activity after treatment
was thecause or rather the effect of symptom reduction.Altered
neural processes in other brain areas (whichmight have been
interindividually more variable andtherefore not detected in group
analysis) could haveresulted in the originally offensive stimuli
beingperceived as less aversive with the consequence ofreduced
firing of amygdala neurons. More detailedinvestigations of network
changes during the treat-ment of anxiety disorders, involving
measures offunctional67 or effective72 connectivity, will be
re-quired in order for such questions to be addressed.
Interestingly, in both OCD and phobia, similar
effects were obtained in the CBT and SSRI-treatedgroups. These
findings, albeit preliminary, point to acommon final pathway for
the neural changes under-lying the clinical effects of a
biochemical and apsychological intervention. It is remarkable that
thedifference in the effects between drugs with
similarpharmacological effects (fluoxetine and citalopram)across
different disease groups (OCD: decrease ofcaudate activity and
OFC-caudate-thalamus correla-tion;24 phobia: decrease of limbic and
paralimbicactivity34) was much more pronounced that than
between drug and psychotherapy within the samedisease group.
Thus, the brain changes induced byand underlying the effects of
therapy seem to be more
dependent on the original dysfunctional area orneural network
than on the nature of the intervention.This view is supported by
evidence from an FDG-PETstudy by Saxena et al .,73 which reported
majordifferences between OCD and depression in thepretreatment
metabolic patterns that predicted aclinical response to
paroxetine.
Studies of depression yielded a less consistentpattern than
those of OCD and phobia, with reports of
both decreases and increases in prefrontal metabolismafter
successful treatment, and considerable differ-ences between
pharmacological and psychologicalinterventions in some studies.
Some of these incon-
sistencies might be attributable to a lack of replicablebaseline
abnormalities of regional cerebral metabo-lism in depression. In
general, the small number offunctional imaging studies on
psychotherapy effects(24 per disease group) and enrolled patients
(notmore than 30 in any of the studies, considerably lessin some)
warrant replication with larger patientsamples before the clinical
utility can finally beassessed.
Of the reviewed studies, five assessed changes inglucose
metabolism, three measured blood flow andthree measured changes in
task-induced blood oxy-genation (the BOLD signal of fMRI). While
all thesephysiological parameters are considered indirectly to
reflect neuronal activity, they are governed bydifferent
regulatory system and are thus prone toinfluences from different
confounding variables, forexample, changes in neurovascular
coupling inelderly patients in the case of fMRI.74 Thus, it
would
be desirable for future functional imaging studies oftherapy
effects to follow standardised protocols, or atleast include a
standardised component to whichindividual research groups could add
their ownparadigms.
For PET or SPECT studies, future protocols shouldinclude the
comparison of baseline activity with acontrol group, the
acquisition of MR images for partialvolume correction, and,
ideally, quantification ofglucose metabolism or blood flow. For
BOLD fMRI,which is by its very nature a relative measure,
controltasks of basic sensory stimulation (that are notexpected to
lead to different activation patterns inrelation to treatment)
might be useful in order tocorroborate the specificity of the
effects of interest.
Wherever possible, research should also aim atintegrating
functional imaging with molecular tech-niques such as radioligand
imaging or biochemicalanalysis of metabolites in order to elucidate
themolecular mechanisms of psychotherapy and itscommonalities and
differences with pharmacotherapy.
The experience with functional imaging studies ofpsychotherapy
so far has been that in some disorders(e.g. OCD) findings were
rather consistent while forothers (e.g. depression) they differed
across studiesand treatment modalities. Findings in OCD
arecompatible with a model of initial hyperactivity in
astriatothalamicorbitofrontal network, which is nor-malised in a
similar way after treatment with either
psycho- or pharmacotherapy. Conversely, in depres-sion, psycho-
and pharmacotherapy seem to operatethrough different pathways, one
more top-down, theother more bottom-up. We will have to hope that
asmore evidence from functional and metabolic imaging
becomes available, more detailed models of the neuralpathways of
psychotherapy effects can be con-structed.
References
1 Kandel ER. Biology and the future of psychoanalysis: a new
intellectual framework for psychiatry revisited. Am J
Psychiatry1999; 156: 505524.2 Linden DEJ. Cerebral mechanisms of
learning revealed by func-
tional neuroimaging in humans. In: Kuhn R, Menzel R, Menzel
W,Ratsch U, Richter MM, Stamatescu I-O (eds). Adaptivity
andLearning An Interdisciplinary Debate. Springer: Heidelberg,
2003pp 4957.
3 Brody AL, Saxena S, Schwartz JM, Stoessel PW, Maidment
K,Phelps ME et al. FDG-PET predictors of response to
behavioraltherapy and pharmacotherapy in obsessive compulsive
disorder.Psychiatry Res 1998; 84: 16.
4 Hendler T, Goshen E, Tzila Zwas S, Sasson Y, Gal G, Zohar J.
Brainreactivity to specific symptom provocation indicates
prospectivetherapeutic outcome in OCD. Psychiatry Res 2003; 124:
87103.
5 Dierks T, Linden DEJ, Jandl M, Formisano E, Goebel R,
Lanfer-mann H et al. Activation of Heschls Gyrus during
auditoryhallucinations. Neuron1999;22: 615621.
Functional neuroimaging and psychotherapyDEJ Linden
536
Molecular Psychiatry
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
10/12
6 Beutel ME, Stern E, Silbersweig DA. The emerging
dialoguebetween psychoanalysis and neuroscience: neuroimaging
perspec-tives. J Am Psychoanal Assoc2003; 51: 773801.
7 Linden DEJ, Prvulovic D, Stirn A, Maurer K.
FunktionelleBildgebung und Psychotherapie. In Walter H (ed).
FunktionelleBildgebung in Psychiatrie und Psychotherapie.
MethodischeGrundlagen und klinische Anwendungen. Schattauer:
Stuttgart,2005 pp 373382.
8 Breiter HC, Rauch SL, Kwong KK, Baker JR, Weisskoff RM,Kennedy
DN et al. Functional magnetic resonance imaging ofsymptom
provocation in obsessive-compulsive disorder. Arch
GenPsychiatry1996; 53: 595606.
9 Mataix-Cols D, Cullen S, Lange K, Zelaya F, Andrew C, Amaro
Eet al. Neural correlates of anxiety associated with
obsessive-compulsive symptom dimensions in normal volunteers.
BiolPsychiatry2003; 53: 482493.
10 Shapira NA, Liu Y, He AG, Bradley MM, Lessig MC, James GAet
al. Brain activation by disgust-inducing pictures in
obsessive-compulsive disorder. Biol Psychiatry2003; 54: 751756.
11 Rauch SL, Jenike MA, Alpert NM, Baer L, Breiter HC, Savage
CRet al. Regional cerebral blood flow measured during
symptomprovocation in obsessive-compulsive disorder using oxygen
15-labeled carbon dioxide and positron emission tomography. ArchGen
Psychiatry1994; 51: 6270.
12 McGuire PK, Bench CJ, Frith CD, Marks IM, Fackowiak RS,
DolanRJ. Functional anatomy of obsessive-compulsive phenomena.Br J
Psychiatry1994; 164: 459468.
13 Rauch SL, Savage CR, Alpert NM, Miguel EC, Baer L, Breiter
HCetal. A positron emission tomographic study of simple
phobicsymptom provocation. Arch Gen Psychiatry1995; 52: 2028.
14 Dilger S, Straube T, Mentzel HJ, Fitzek C, Reichenbach JR,
Hecht Het al.Brain activation to phobia-related pictures in spider
phobichumans: an event-related functional magnetic resonance
imagingstudy. Neurosci Lett2003; 348: 2932.
15 Rauch SL, van der Kolk BA, Fisler RE, Alpert NM, Orr SP,
SavageCR et al. A symptom provocation study of posttraumatic
stressdisorder using positron emission tomography and
script-drivenimagery.Arch Gen Psychiatry1996; 53: 380387.
16 Pissiota A, Frans O, Fernandez M, von Knorring L, Fischer
H,Fredrikson M. Neurofunctional correlates of posttraumatic
stressdisorder: a PET symptom provocation study. Eur Arch
Psychiatry
Clin Neurosci2002; 252: 6875.17 Driessen M, Beblo T, Mertens M,
Piefke M, Rullkotter N, Silva
Saavedra A et al. Different fMRI activation patterns of
traumaticmemory in borderline personality disorder with and
withoutadditional posttraumatic stress disorder. Biol
Psychiatry2004;55:603611.
18 Bremner JD, Narayan M, Staib LH, Southwick SM, McGlashan
T,Charney DS. Neural correlates of memories of childhood
sexualabuse in women with and without posttraumatic stress
disorder.Am J Psychiatry1999; 156: 17871795.
19 Shin LM, Orr SP, Carson MA, Rauch SL, Macklin ML, Lasko NBet
al. Regional cerebral blood flow in the amygdala and
medialprefrontal cortex during traumatic imagery in male and
femaleVietnam veterans with PTSD. Arch Gen Psychiatry 2004;
61:168176.
20 Beauregard M, Leroux JM, Bergman S, Arzoumanian Y, BeaudoinG,
Bourgouin P et al. The functional neuroanatomy of majordepression:
an fMRI study using an emotional activation para-digm.
NeuroReport1998;9: 32533258.
21 Mayberg HS, Liotti M, Brannan SK, McGinnis S, Mahurin
RK,Jerabek PAet al. Reciprocal limbic-cortical function and
negativemood: converging PET findings in depression and normal
sadness.Am J Psychiatry1999; 156: 675682.
22 Sheline YI, Barch DM, Donnelly JM, Ollinger JM, Snyder
AZ,Mintun MA. Increased amygdala response to masked emotionalfaces
in depressed subjects resolves with antidepressant treat-ment: an
fMRI study. Biol Psychiatry2001;50: 651658.
23 Siegle GJ, Steinhauer SR, Thase ME, Stenger VA, Carter CS.
Cantshake that feeling: event-related fMRI assessment of
sustainedamygdala activity in response to emotional information
indepressed individuals. Biol Psychiatry2002; 51: 693707.
24 Baxter Jr LR, Schwartz JM, Bergman KS, Szuba MP, Guze
BH,Mazziotta JC et al. Caudate glucose metabolic rate changes
with
both drug and behavior therapy for obsessive-compulsive
disorder.Arch Gen Psychiatry1992; 49: 681689.
25 Schwartz JM, Stoessel PW, Baxter Jr LR, Martin KM, Phelps
ME.Systematic changes in cerebral glucose metabolic rate
aftersuccessful behavior modification treatment of
obsessive-compul-sive disorder. Arch Gen Psychiatry1996; 53:
109113.
26 Nakatani E, Nakgawa A, Ohara Y, Goto S, Uozumi N, Iwakiri
Metal. Effects of behavior therapy on regional cerebral blood flow
in
obsessive-compulsive disorder. Psychiatry Res 2003;
124:113120.
27 Schwartz JM. Neuroanatomical aspects of cognitive
behaviouraltherapy response in obsessive-compulsive disorder. An
evolvingperspective on brain and behaviour. Br J Psychiatry
1998;173(Suppl. 35): 3844.
28 Saxena S, Brody AL, Schwartz JM, Baxter LR. Neuroimaging
andfrontal-subcortical circuitry in obsessive-compulsive
disorder.Br J Psychiatry1998;173(Suppl 35): 2637.
29 Nakao T, Nakagawa A, Yoshiura T, Nakatani E, Nabeyama
M,Yoshizato C et al. Brain activation of patients with
obsessive-compulsive disorder during neuropsychological and
symptomprovocation tasks before and after symptom improvement:
afunctional magnetic resonance imaging study. Biol Psychiatry2005;
57: 901910.
30 Paquette V, Levesque J, Mensour B, Leroux JM, Beaudoin
G,Bourgouin P et al. Change the mind and you change the
brain:effects of cognitive-behavioral therapy on the neural
correlates ofspider phobia. Neuroimage 2003; 18: 401409.
31 Straube T, Glauer M, Dilger S, Mentzel HJ, Miltner WHR.
Effects ofcognitive-behavioral therapy on brain activation in
specificphobia. Neuroimage 2006; 29: 125135.
32 Birbaumer N, Grodd W, Diedrich O, Klose U, Erb M, Lotze M et
al.fMRI reveals amygdala activation to human faces in
socialphobics. NeuroReport1998;9: 12231226.
33 Stein MB, Goldin PR, Sareen J, Eyler LT, Brown GG.
Increasedamygdala activation to angry and contemptuous faces in
general-ized social phobia. Arch Gen Psychiatry2002; 59:
10271034.
34 Furmark T, Tillfors M, Marteinsdottir I, Fischer H, Pissiota
A,Langstrom B et al. Common changes in cerebral blood flow
inpatients with social phobia treated with citalopram or
cognitive-
behavioral therapy.Arch Gen Psychiatry2002; 59: 425433.35
Mayberg HS, Silva JA, Brannan SK, Tekell JL, Mahurin RK,
McGinnis S et al. The functional neuroanatomy of the
placeboeffect. Am J Psychiatry2002; 159: 728737.
36 Navarro V, Gasto C, Lomena F, Mateos JJ, Marcos T, Portella
MJ.Normalization of frontal cerebral perfusion in remitted
elderlymajor depression: a 12-month follow-up SPECT study.
Neuro-image 2002; 16: 781787.
37 Brody AL, Saxena S, Stoessel P, Gillies LA, Fairbanks
LA,Alborzian S et al. Regional brain metabolic changes in
patientswith major depression treated with either paroxetine or
inter-personal therapy: preliminary findings.Arch Gen
Psychiatry2001;58: 631640.
38 Goldapple K, Segal Z, Garson C, Lau M, Bieling P, Kennedy Set
al.Modulation of cortical-limbic pathways in major
depression:treatment-specific effects of cognitive behavior
therapy. ArchGen Psychiatry2004; 61: 3441.
39 Martin SD, Martin E, Rai SS, Richardson MA, Royall R.
Brainblood flow changes in depressed patients treated with
interperso-nal psychotherapy or venlafaxine hydrochloride:
preliminaryfindings. Arch Gen Psychiatry2001; 58: 641648.
40 American Psychiatric Association Force or DSM-IV.
Diagnosticand Statistical Manual of Mental Disorders, 4th edn, Text
Revision(DSM-IV-TRs). American Psychiatric Association, 2000.
41 Thase ME. Neuroimaging profiles and the differential
therapies ofdepression. Arch Gen Psychiatry2001; 58: 651653.
42 Cherry SR, Phelps ME. Imaging brain function with
positronemission tomography. In: Toga AW, Mazziotta JC (eds).
BrainMapping. The Methods. Academic Press: San Diego, 1995
pp191221.
43 Drevets WC, Price JL, Simpson Jr JR, Todd RD, Reich T,
Vannier Met al. Subgenual prefrontal cortex abnormalities in mood
dis-orders. Nature 1997; 386: 824827.
44 Drevets WC. Neuroimaging studies of mood disorders.
BiolPsychiatry2000; 48: 813829.
Functional neuroimaging and psychotherapyDEJ Linden
Molecular Psych
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
11/12
45 Sheline Y. Neuroimaging studies of mood disorder effects on
thebrain. Biol Psychiatry2003; 54: 338352.
46 Szeszko PR, MacMillan S, McMeniman M, Lorch E, Madden R,Ivey
J et al. Amygdala volume reductions in pediatric patientswith
obsessive-compulsive disorder treated with paroxetine:preliminary
findings. Neuropsychopharmacology 2004; 29:826832.
47 Gilbert AR, Moore GJ, Keshavan MS, Paulson LA, Narula V,
Mac
Master FPet al.Decrease in thalamic volumes of pediatric
patientswith obsessive-compulsive disorder who are taking
paroxetine.Arch Gen Psychiatry2000; 57: 449456.
48 Laakso A, Hietala J. PET studies of brain monoamine
transporters.Curr Pharmaceut Des 2000;6: 16111623.
49 Talbot PS, Laruelle M. The role ofin vivomolecular imaging
withPET and SPECT in the elucidation of psychiatric drug action
andnew drug development. Eur Neuropsychopharmacol 2002;
12:503511.
50 Meyer JH, Wilson AA, Sagrati S, Hussey D, Carella A, Potter
WZ etal. Serotonin transporter occupancy of five selective
serotoninreuptake inhibitors at different doses: an [11C]DASB
PositronEmission Tomography Study. Am J Psychiatry 2004;
161:826835.
51 Meyer JH, Wilson AA, Ginovart N, Goulding V, Hussey D, Hood
Ket al. Occupancy of serotonin transporters by paroxetineand
citalopram during treatment of depression: a [11C]DASBPET Imaging
Study. Am J Psychiatry 2001; 158: 18431849.
52 Pirker W, Asenbaum S, Kasper S, Walter H, Angelberger P, Koch
Get al. beta-CIT SPECT demonstrates blockade of 5HT-uptake
sites
by citalopram in the human brain in vivo. J Neural Transm
GenSect1995;100: 247256.
53 Kent JM, Coplan JD, Lombardo I, Hwang DR, Huang Y, Mawlawi
Oet al. Occupancy of brain serotonin transporters during
treatmentwith paroxetine in patients with social phobia: a
positronemission tomography study with [11C]McN 5652.
Psychopharma-cology2002; 164: 341348.
54 Pogarell O, Poepperl G, Mulert C, Hamann C, Sadowsky N,
RiedelMet al.SERTand DAT availabilities under citalopram treatment
inobsessive-compulsive disorder (OCD). Eur
Neuropsychopharma-col2005;15: 521524.
55 Baer L. Behavior therapy: endogenous serotonin therapy? J
Clin
Psychiatry1996; 57(Suppl): 3335.56 Ebert D, Feistel H, Kaschka
W, Barocka A, Pirner A. Single photon
emission computerized tomographic assessment of cerebraldopamine
D2 receptor blockade in depression before and aftersleep
deprivation Preliminary results.Biol Psychiatry1994; 35:880885.
57 Ebert D, Ebmeier K. The role of the cingulate gyrus in
depression:from functional anatomy to neurochemistry.Biol
Psychiatry1996;39: 10441050.
58 Rainville P, Carrier B, Hofbauer RK, Bushnell MC, Duncan
GH.Dissociation of sensory and affective dimensions of pain
usinghypnotic modulation.Pain1999;82: 159171.
59 Rainville P, Duncan GH, Price DD, Carrier B, Bushnell MC.
Painaffect encoded in human anterior cingulate but not
somatosensorycortex. Science 1997; 277: 968971.
60 Hofbauer RK, Rainville P, Duncan GH, Bushnell MC.
Corticalrepresentation of the sensory dimension of pain. J
Neurophysiol2001; 86: 402411.
61 Roder CH, Michal M, Overbeck G, van de Ven V, Linden DEJ.
Painresponse in depersonalization a functional imaging study
usinghypnosis in healthy subjects. Psychother Psychosomatics,
inpress.
62 Rainville P, Hofbauer RK, Paus T, Duncan GH, Bushnell MC,
Price
DD. Cerebral mechanisms of hypnotic induction and suggestion.J
Cogn Neurosci1999; 11: 110125.
63 Birbaumer N, Ghanayim N, Hinterberger T, Iversen I,
KotchoubeyB, Kuebler A et al. A spelling device for the paralysed.
Nature1999; 398: 297298.
64 Weiskopf N, Veit R, Erb M, Mathiak K, Grodd W, Goebel R et
al.Physiological self-regulation of regional brain activity using
real-time functional magnetic resonance imaging (fMRI):
methodologyand exemplary data. Neuroimage 2003;19: 577586.
65 deCharms RC, Christoff K, Glover GH, Pauly JM, Whitfield
S,Gabrieli JDE. Learned regulation of spatially localized
brainactivation using real-time fMRI. Neuroimage 2004; 21:
436443.
66 deCharms RC, Maeda F, Glover GH, Ludlow D, Pauly JM, Soneji
Det al. Control over brain activation and pain learned by
usingreal-time functional MRI. Proc Natl Acad Sci USA 2005;
102:1862618631.
67 van de Ven VG, Formisano E, Prvulovic D, Roeder CH, Linden
DEJ.Functional connectivity as revealed by spatial
independentcomponent analysis of fMRI measurements during rest.
HumBrain Mapp 2004; 22: 165178.
68 Kent JM, Rauch SL. Neuroimaging studies of anxiety disorders.
In:Charney DS, Nestler EJ (eds).Neurobiology of Mental Illness,
2ndedn. Oxford University Press: Oxford, UK, 2004 pp 639660.
69 Rauch SL, Whalen PJ, Curran T, Shin LM, Coffey BJ, Savage
CRetal. Probing striato-thalamic function in
obsessive-compulsivedisorder and Tourette syndrome using
neuroimaging methods.Adv Neurol2001; 85: 207224.
70 Pasupathy A, Miller EK. Different time courses of
learning-relatedactivity in the prefrontal cortex and striatum.
Nature 2005; 433:873876.
71 Davis M. Functional neuroanatomy of anxiety and fear.
In:Charney DS, Nestler EJ (eds). Neurobiology of Mental Illness,2nd
edn. Oxford University Press: Oxford, UK, 2004 pp 584604.
72 Goebel R, Roebroeck A, Kim D-S, Formisano E.
Investigatingdirected cortical interactions in time-resolved fMRI
data usingvector autoregressive modeling and Granger causality
mapping.Magn Res Imaging2003; 21: 12511261.
73 Saxena S, Brody AL, Ho ML, Zohrabi N, Maidment KM, Baxter
JrLR. Differential brain metabolic predictors of response to
parox-etine in obsessive-compulsive disorder versus major
depression.Am J Psychiatry2003; 160: 522532.
74 DEsposito M, Deouell LY, Gazzaley A. Alterations in the
BOLDfMRI signal with ageing and disease: a challenge for
neuroimaging.Nat Rev Neurosci2003;4: 863872.
75 Prasko J, Horacek J, Zalesky R, Kopecek M, Novak T, Paskova B
etal.The change of regional brain metabolism (18FDG PET) in
panicdisorder during the treatment with cognitive behavioural
therapyor antidepressants. Neuroendocrinol Lett2004; 25:
340348.
Functional neuroimaging and psychotherapyDEJ Linden
538
Molecular Psychiatry
-
7/27/2019 How Psychotherapy Changes the Brain - The Contribution
of Functional Neuroimaging
12/12