Embed Size (px)
Citation preview
‘‘How I do’ CMR in valvular heart How I do’ CMR in valvular heart diseasedisease
Dr. Saul MyersonClinical Lecturer in Cardiovascular Medicine
For www.scmr.org 02/2007
This presentation posted for members of scmr as an educational guide – it represents the views and practices of the author, and not necessarily those of SCMR.
University of Oxford Centre for Clinical Magnetic Resonance Research
(OCMR)
© Saul Myerson 2007
Advantages of CMRAdvantages of CMR
• All areas of the body accessible - free choice of imaging planes with no ‘hidden’ sections
• Range of imaging techniques – anatomical, cine, angiography, flow
• Quantification of flow and thus valve lesion severity
• 3D imaging with angiography
• No ionising radiation
• Other techniques (Echo) do have strengths, esp. in the acute setting
© Saul Myerson 2007
Standard imaging for all studiesStandard imaging for all studies
• Long axis planes – HLA, VLA, LVOT, LVOT coronal, (RVOT +/- RV inflow if right-sided lesions)
• Need two perpendicular views of the valve(s) in question
• LV & RV function

© Saul Myerson 2007
LV and RV functionLV and RV function
Gold standard accuracy for
volumes, mass & function
This is important for assessing the impact of the valve lesion on the LV / RV and should be performed in all cases
See How I do a CMR volume study by James Moon, here

© Saul Myerson 2007
Specific valve lesions - overviewSpecific valve lesions - overview
• Aortic valve disease
• Mitral valve disease
• Pulmonary stenosis & regurgitation
• Tricuspid regurgitation
• Complex lesions
– Mixed stenosis/regurgitation
– Multiple valves

© Saul Myerson 2007
Aortic stenosis (1)Aortic stenosis (1)
• Plan initial LVOT view from short axis pilot scan, with the plane through the
aortic root/valve
• The second LVOT (coronal) plane is planned through this, aligned with the
stenotic jet. There is often a central core in the jet comprising laminar flow,
with turbulent flow (black/low intensity on gradient echo) surrounding this
• Align planes with AS jet rather than Ao root
SA pilot LVOT view Coronal LVOT view

© Saul Myerson 2007
Aortic stenosis (2)Aortic stenosis (2)
Choose the best LVOT view for in-plane flow assessment (the one with
the best view of the core jet)

© Saul Myerson 2007
Aortic stenosis (3)Aortic stenosis (3)
• Measure the peak velocity, either from the in-plane flow itself, or using the in-plane flow to identify the point of peak velocity and acquire a through-plane flow sequence at this point:
Position for through-plane flow acquisition
© Saul Myerson 2007
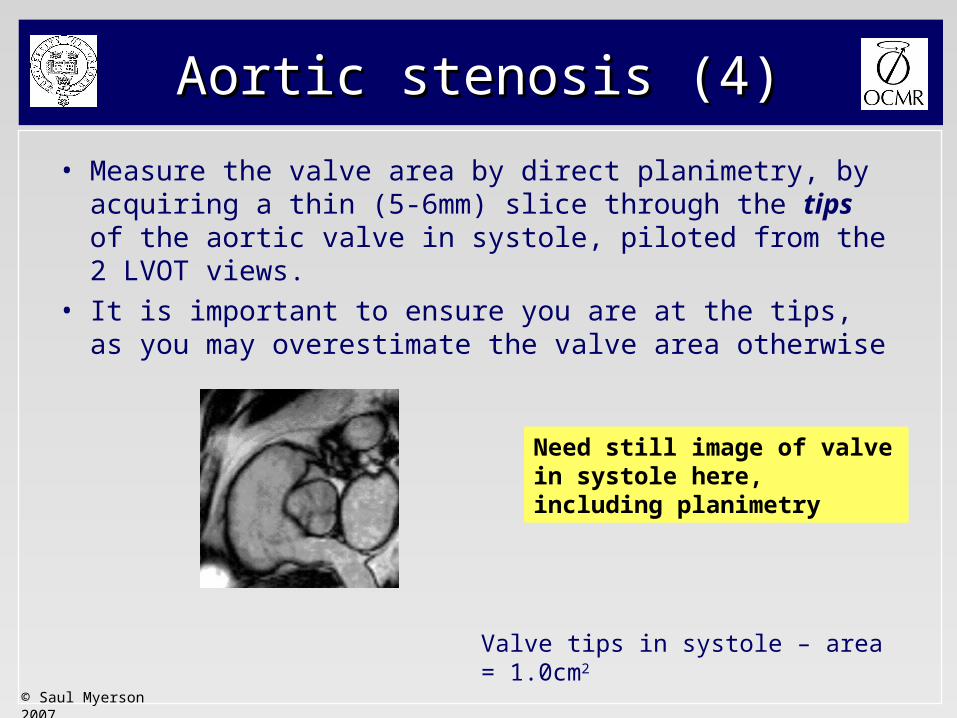
Aortic stenosis (4)Aortic stenosis (4)
• Measure the valve area by direct planimetry, by acquiring a thin (5-6mm) slice through the tips of the aortic valve in systole, piloted from the 2 LVOT views.
• It is important to ensure you are at the tips, as you may overestimate the valve area otherwise
Valve tips in systole – area = 1.0cm2
Need still image of valve in systole here, including planimetry

© Saul Myerson 2007
Aortic stenosis (5)Aortic stenosis (5)
• Correct alignment with AS jet – Accurate trans-valvular velocity (in-plane / through
plane) – avoids underestimation with angulated roots
• Valve orifice area (direct planimetry)
• LV mass & volumes to assess impact on LV
Advantages of CMR:
© Saul Myerson 2007
• Through-plane flow measurement
• Allows quantification of regurgitation
Aortic regurgitationAortic regurgitation
© Saul Myerson 2007
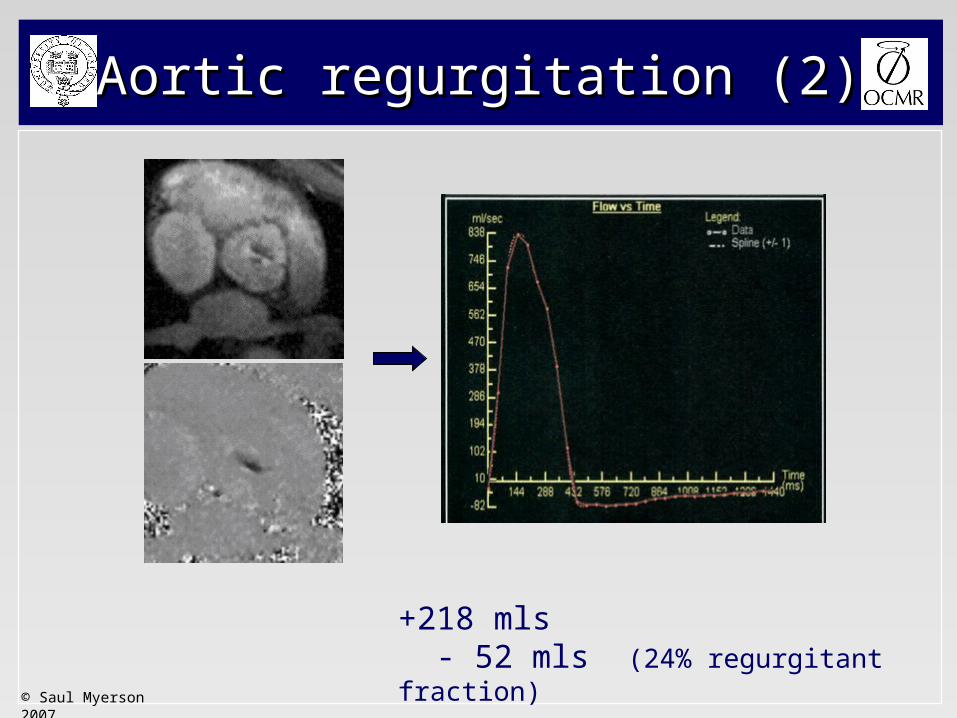
Aortic regurgitation (2)Aortic regurgitation (2)
+218 mls - 52 mls (24% regurgitant fraction)

© Saul Myerson 2007
Aortic regurgitation (3)Aortic regurgitation (3)
• Quantification allows more accurate assessment of severity
(echo parameters less precise)
• More detail required on how quantification fits into clinical practice

© Saul Myerson 2007
Aortic diseaseAortic disease
Don’t forget the aorta in your valve assessment !
Residual root dissection in a patient with a previous type A dissection repair (inter-positional graft)
© Saul Myerson 2007
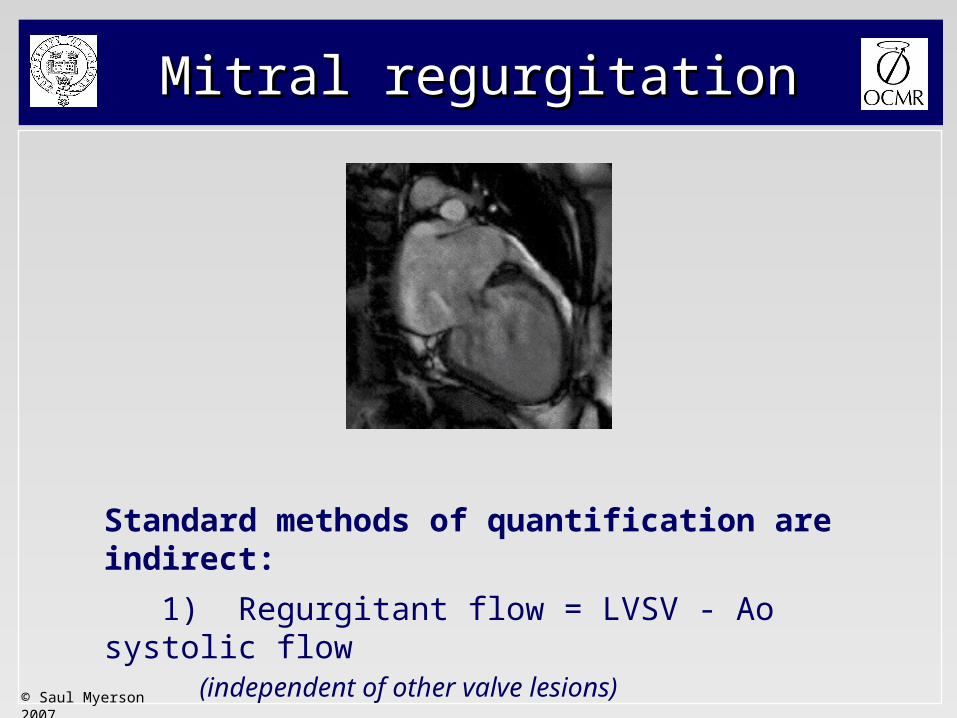
Mitral regurgitationMitral regurgitation
Standard methods of quantification are indirect:
1) Regurgitant flow = LVSV - Ao systolic flow(independent of other valve lesions)
2) Regurgitant flow = LVSV - RVSV
© Saul Myerson 2007
Mitral stenosisMitral stenosis
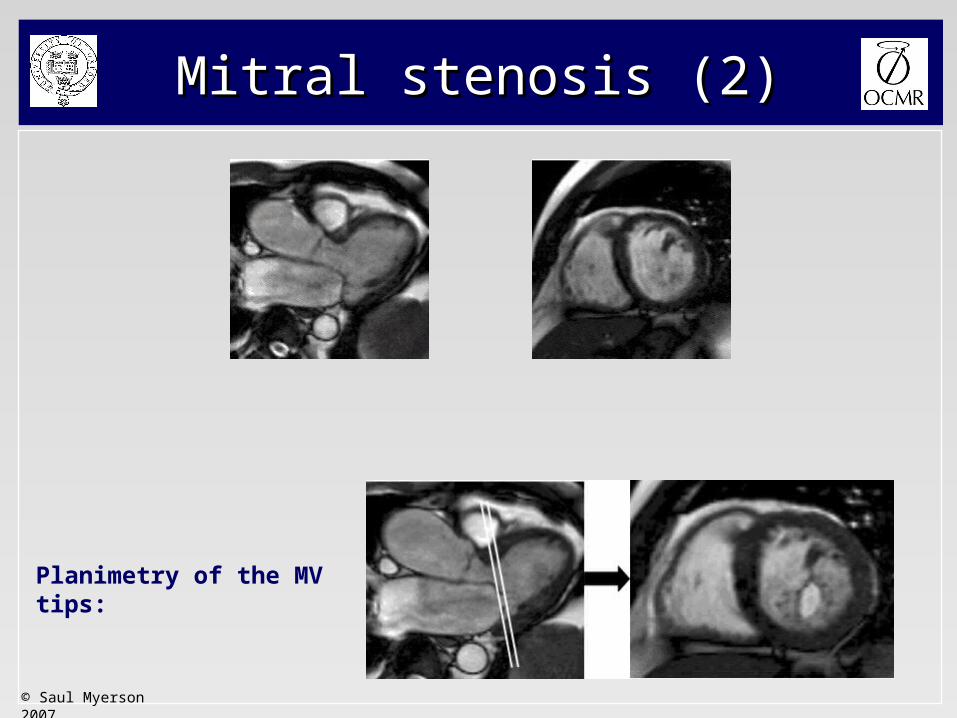
• Can assess mitral valve area by direct planimetry• Important to ensure correct slice positioning at MV tips
(as for echo)• Diastolic flow (volume and velocity) is feasible though
temporal resolution is lower than echo
© Saul Myerson 2007
Mitral stenosis (2)Mitral stenosis (2)
Planimetry of the MV tips:
© Saul Myerson 2007
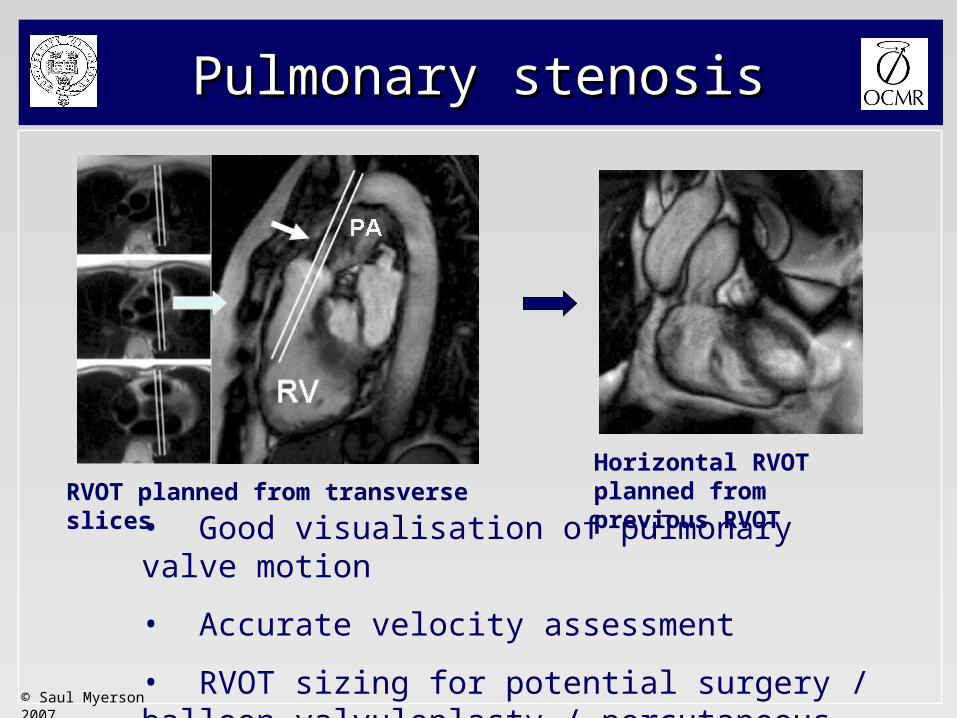
Pulmonary stenosisPulmonary stenosis
• Good visualisation of pulmonary valve motion
• Accurate velocity assessment
• RVOT sizing for potential surgery / balloon valvuloplasty / percutaneous valve replacement
RVOT planned from transverse slicesHorizontal RVOT planned from previous RVOT

© Saul Myerson 2007
Pulmonary regurgitationPulmonary regurgitation
• Quantification of PR
• Size & shape of RVOT - ?percutaneous stent-valve replacement
• Size & function of RV
Forward flow: 72mls
Regurgitant flow: 27mls (38% regurgitant fraction)

© Saul Myerson 2007
Pulmonary valve disease (3)Pulmonary valve disease (3)
CMR is also important for:
• determining RV mass & volumes
• assessing RVOT morphology
Dilated RV secondary to chronic PR

© Saul Myerson 2007
• Supravalvular stenosis with previous surgical widening
• Now recurrent supravalvular stenosis & valvular regurgitation
• Dilated post-stenotic pulmonary artery
Complex pulmonary diseaseComplex pulmonary disease
© Saul Myerson 2007
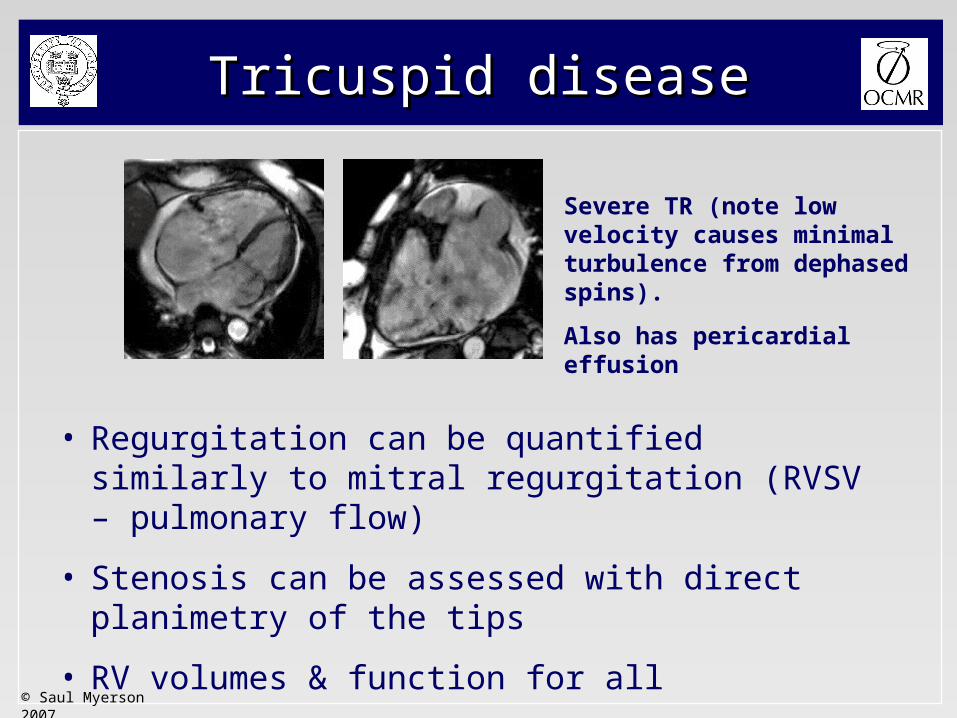
Tricuspid diseaseTricuspid disease
• Regurgitation can be quantified similarly to mitral regurgitation (RVSV – pulmonary flow)
• Stenosis can be assessed with direct planimetry of the tips
• RV volumes & function for all
Severe TR (note low velocity causes minimal turbulence from dephased spins).
Also has pericardial effusion
© Saul Myerson 2007
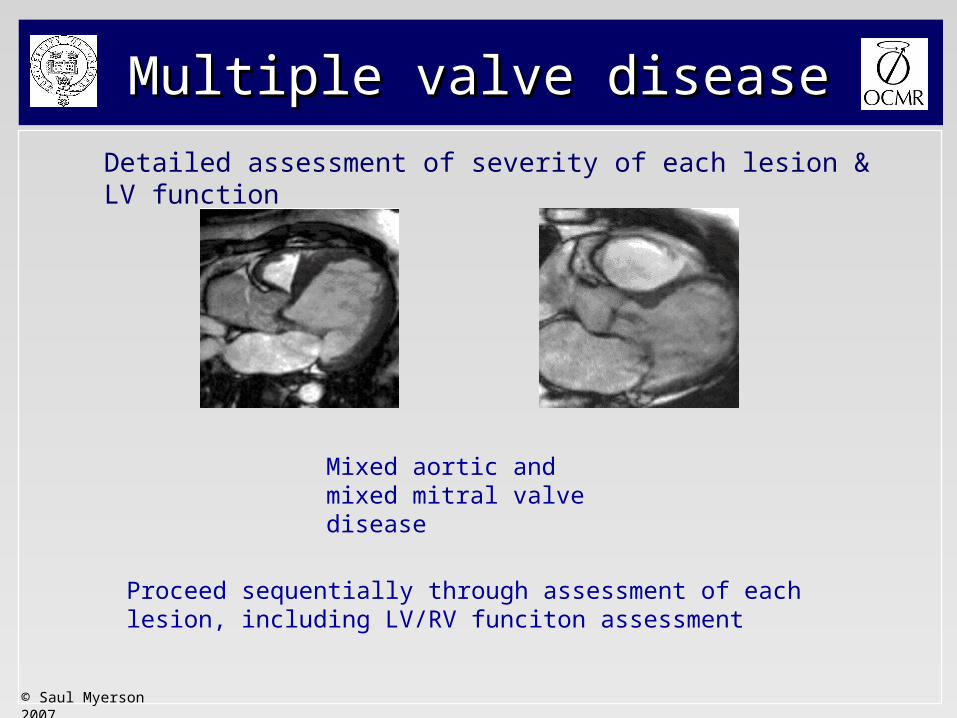
Multiple valve diseaseMultiple valve disease
Detailed assessment of severity of each lesion & LV function
Proceed sequentially through assessment of each lesion, including LV/RV funciton assessment
Mixed aortic and mixed mitral valve disease





























