Embed Size (px)
Citation preview

How Good a Doctor…?Physical Health Care in a Forensic Setting
Dr. Alan Cohen FRCGP
Director of Primary Care, West London Mental Health TrustRetired Grumpy Old Git

Take Diabetes
More common in people with severe mental illness (SMI)
One of the major causes of premature death in this group
But no information on the quality of care provided to people with a SMI
There is a National Diabetes Audit that could address this omission

• Commissioned by HCIP and funded by NHSE, since 2004
• Takes data from inpatient care, and primary care
• Addresses four specific questions• Is everyone with diabetes diagnosed and recorded on a practice
register?
• What percentage receive the 9 key interventions recommended by NICE?
• What percentage achieved the 7 treatment targets recommended by NICE?
• What are the acute and long term complication rates?
The National Diabetes Audit
9 Key Interventions –process measures
HbA1c (mmol/mol)
Smoking
BMI
Blood Pressure (mmHg)
Serum Cholesterol (mmol/l)
Serum Creatinine
Urine Albumen
Foot Surveillance
Retinal screening*
7 Treatment Targets – outcome measures
HbA1c <58 mmol/mol
HbA1c <= 64 mmol/mol
HbA1c <= 75 mmol/mol
Blood Pressure (Systolic) <150mmHg
Blood Pressure (Systolic) <140 mmHg
Blood Pressure <=140/80
Serum Cholesterol < 5mmol/l

West London Mental Health Trust
0 – 9 years
10 – 19 years
20 – 29 years
30 – 39 years
40 – 49 years
50 – 59 years
60 – 69 years
70 – 79 years
80 – 89 years
90 – 99 years
Age Distribution at Broadmoor and at WLFS
Broadmoor Male (%) Broadmoor Female (%)
WLFS Male (%) WLFS Female (%)
Aim: to compare the standard of care delivered at Broadmoor and WLFS with the standards of the National Diabetic Audit
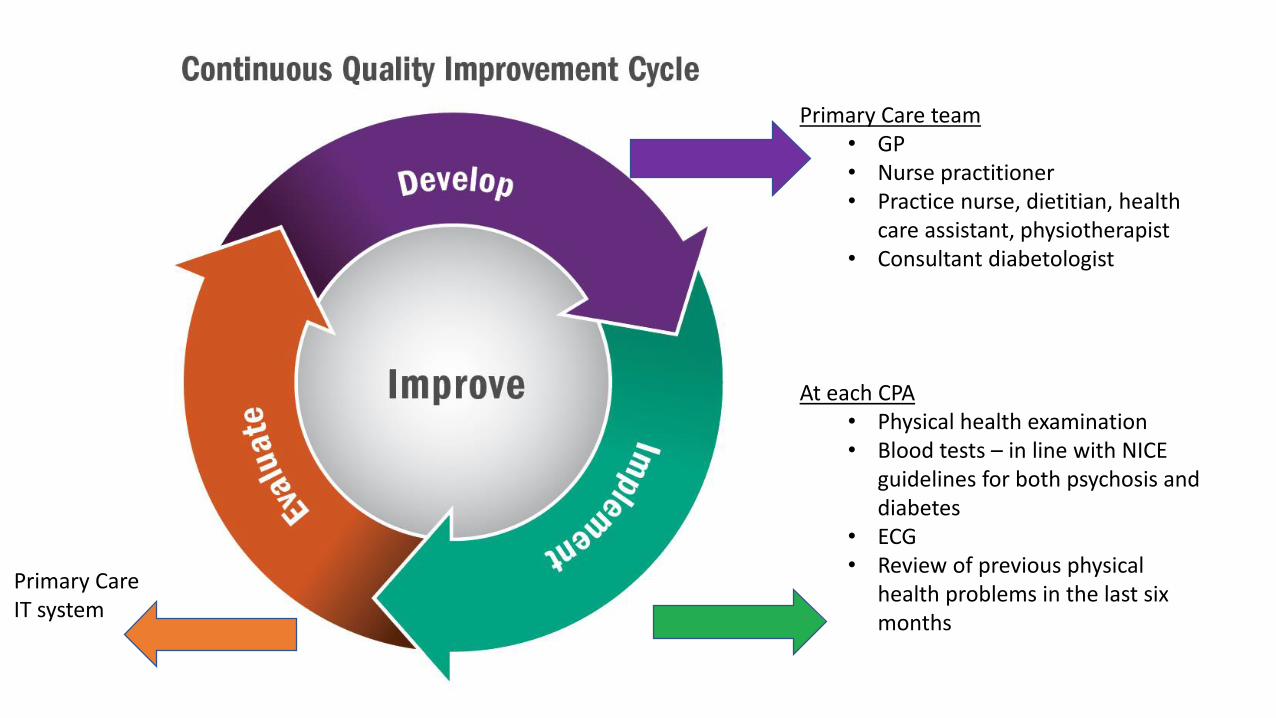
Primary Care team• GP• Nurse practitioner• Practice nurse, dietitian, health
care assistant, physiotherapist• Consultant diabetologist
Primary Care IT system
At each CPA• Physical health examination• Blood tests – in line with NICE
guidelines for both psychosis and diabetes
• ECG• Review of previous physical
health problems in the last six months
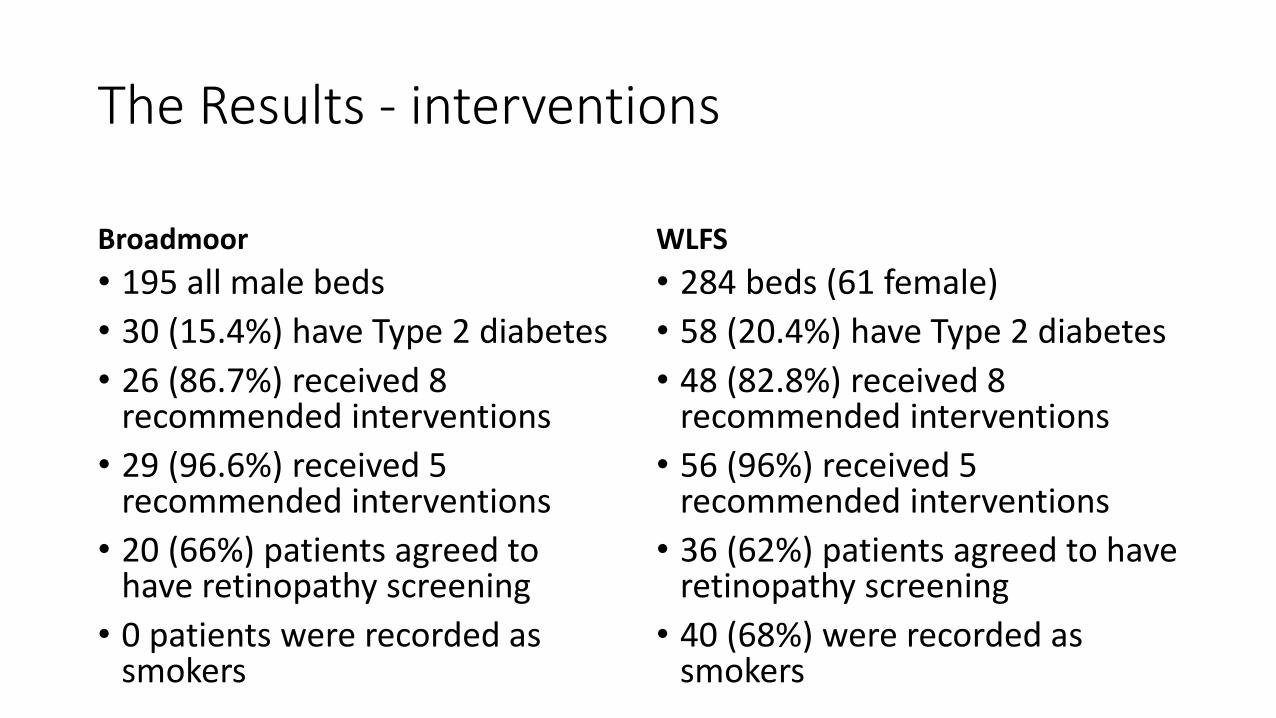
The Results - interventions
Broadmoor
• 195 all male beds
• 30 (15.4%) have Type 2 diabetes
• 26 (86.7%) received 8 recommended interventions
• 29 (96.6%) received 5 recommended interventions
• 20 (66%) patients agreed to have retinopathy screening
• 0 patients were recorded as smokers
WLFS
• 284 beds (61 female)
• 58 (20.4%) have Type 2 diabetes
• 48 (82.8%) received 8 recommended interventions
• 56 (96%) received 5 recommended interventions
• 36 (62%) patients agreed to have retinopathy screening
• 40 (68%) were recorded as smokers

The Results - outcomes
Broadmoor
• Mean HbA1c was 63.9mmol/mol
• 14 (46.7%) achieved good control of diabetes
• 5 (16%) achieved the composite of good diabetic control, ideal blood pressure and ideal cholesterol
• Insulin needed in 8 (27%) of patients
WLFS
• Mean HbA1c was 52.4mmol/mol
• 43 (74.1%) achieved good control of diabetes
• 27 (46.5%) achieved the composite of good diabetic control, ideal blood pressure and ideal cholesterol
• Insulin needed in 5 (8.6%) of patients
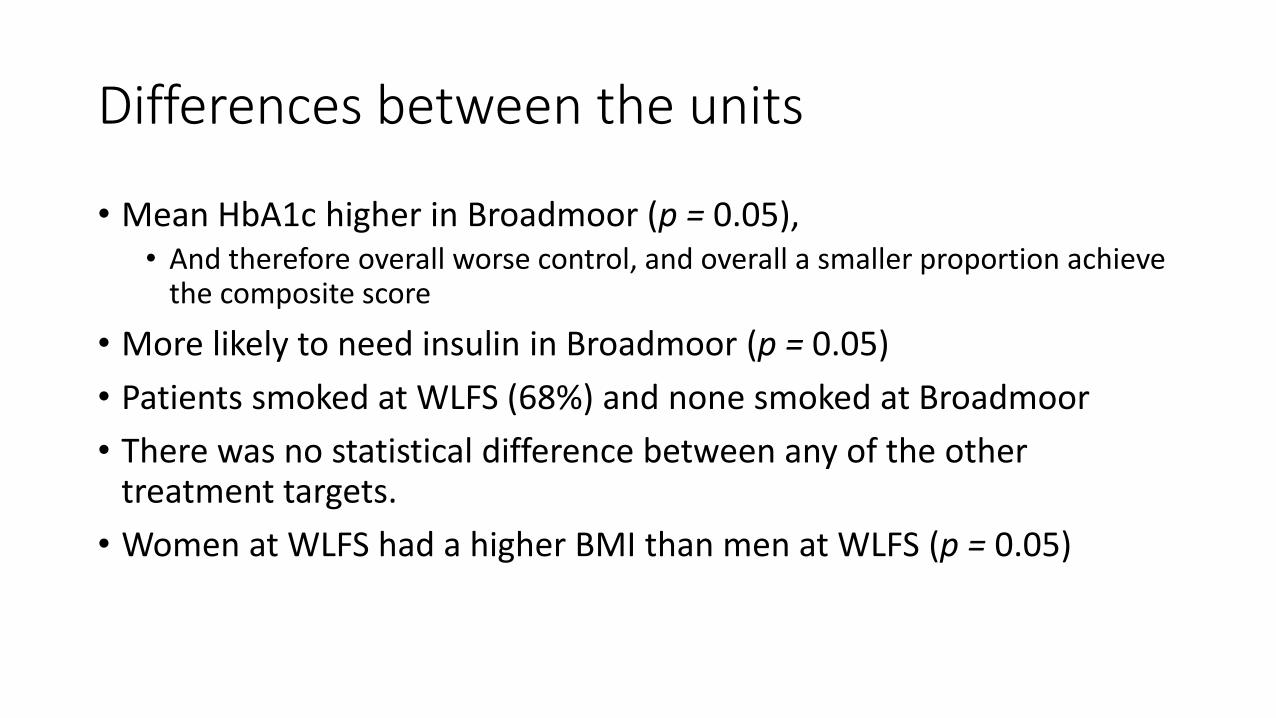
Differences between the units
• Mean HbA1c higher in Broadmoor (p = 0.05),• And therefore overall worse control, and overall a smaller proportion achieve
the composite score
• More likely to need insulin in Broadmoor (p = 0.05)
• Patients smoked at WLFS (68%) and none smoked at Broadmoor
• There was no statistical difference between any of the other treatment targets.
• Women at WLFS had a higher BMI than men at WLFS (p = 0.05)
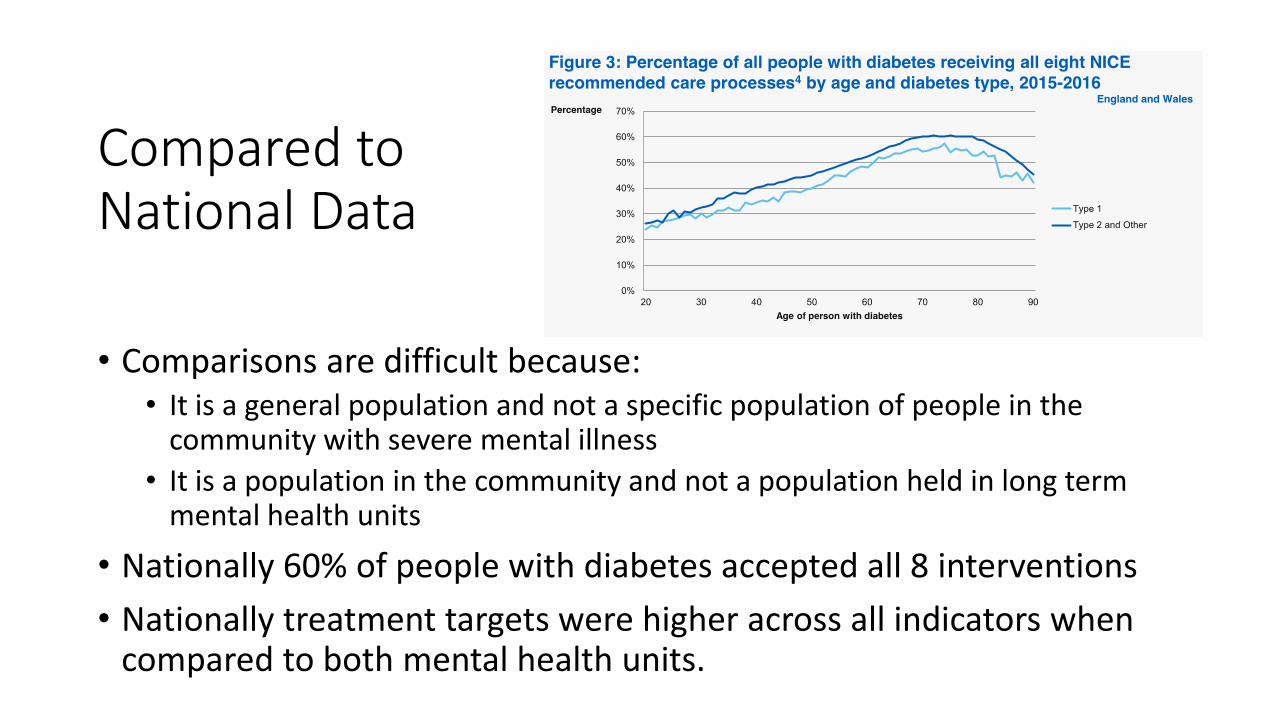
Compared to National Data
• Comparisons are difficult because:• It is a general population and not a specific population of people in the
community with severe mental illness
• It is a population in the community and not a population held in long term mental health units
• Nationally 60% of people with diabetes accepted all 8 interventions
• Nationally treatment targets were higher across all indicators when compared to both mental health units.
So what?
• Both units were good at offering the interventions (84%) compared to the national average (60%)
• But despite offering the interventions, treatment target achievements were worse than the national figures, and worse at Broadmoor than at WLFS
• What could explain this?• Smoking?
• Antipsychotics?
Smoking
Smoking (nicotine) induces liver enzymes
Which increases the metabolism of anti-psychotic medication
So to achieve the same therapeutic effect in a smoker, a higher dose of medication is needed
When a smoker stops smoking, it is recommended that the dose of medication is reduced by about 25%, otherwise the drug level will increase to potentially toxic levels
68% of WLFS patients smoked
But they had better diabetic control…
Antipsychotic medication
No electronic data at WLMHT as to overall comparative use of antipsychotics
No information on relative diabetogenic effects of different antipsychotics, alone or in combination.
Some thoughts…
• Setting up the organisation of care was straightforward
• Getting the data was straightforward
• Interpreting the data was straightforward
But…
• Diabetes is more complex to manage in forensic settings
• The treatment target achievements were poor despite offering all the interventions recommended by NICE
• The role of smoking is ill-understood
• The role of antipsychotic medication is ill-understood
… and some questions
Are psychiatrists (or psychiatrists in training) the best people to offer diabetic care to a group that are more complex to treat than most other diabetics?
If not psychiatrists –then who (and how)?
Why don’t we have better information about medication use?
Why doesn’t the National Diabetic Audit include mental health trusts? Is this what is called “Parity of Esteem”?
In Summary
• We have the tools to deliver high quality physical health care
• When we start to do so, it raises clinical questions that are complex
• We do need some national leadership (politically and administratively) which is effective
But…





![[d], [o] If one doctor doctors another doctor does the doctor who doctors the doctor doctor the doctor the way the doctor he is doctoring doctors? Or](https://img.dokumen.tips/doc/110x75/56649e995503460f94b9c732/d-o-if-one-doctor-doctors-another-doctor-does-the-doctor-who-doctors-the.jpg)