Embed Size (px)
Citation preview

A
a
>tt
s(
d©
K
1
pmteec[
f
g
CT
1d
Available online at www.sciencedirect.com
Digestive and Liver Disease 41 (2009) 364–369
Liver, Pancreas and Biliary Tract
How do we interpret an elevated carbohydrate antigen 19-9 level inasymptomatic subjects?�
B.J. Kim, K.T. Lee ∗, T.G. Moon, P. Kang, J.K. Lee, J.J. Kim, J.C. RheeDepartment of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Republic of Korea
Received 24 July 2008; accepted 3 December 2008Available online 21 January 2009
bstract
Aim. This prospective cohort study aimed to evaluate the etiology of elevated CA 19-9 levels and to present appropriate guidelines for thesymptomatic patients.
Methods. Between January 2004 and March 2007, we enrolled consecutive asymptomatic patients who had elevated CA 19-9 levels37 U/mL. To evaluate the etiology, the CA 19-9 level was rechecked and further studies were carried out. If the CA 19-9 level decreased to
he normal range, or if it showed a decreasing trend, then it was monitored annually. Yet, if the CA 19-9 level showed an increasing trend,hen the level was monitored at intervals of 1, 3, and 6 months until no evidence of malignancy was proven.
Results. Of the 62,976 patients, 501 (0.8%) subjects showed an elevated CA 19-9 level. This prospective analysis was conducted on 353ubjects (70.5%) who were followed up for at least 6 months. Ten patients (2.8%) were diagnosed with malignancies. There were 97 patients
27.5%) with benign diseases and 246 patients (69.7%) were deemed non-specific.Conclusions. CA 19-9 should not be used as a screening tool. In the case of a persistently elevated CA 19-9 level, further work-up foretermining the etiology should be done.
2009 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
ker
itcvpgmifb
eywords: Asymptomatic patient; CA 19-9; Pancreatic cancer; Tumor mar
. Introduction
Routine examination of asymptomatic people for healthromotion has recently been expanded, and several tumorarkers are being examined for their potential to diagnose
he early stages of cancers [1]. Among various tumor mark-rs, the serum carbohydrate antigen, CA 19-9, level has beenstablished as a useful tumor marker for gastrointestinal can-ers, and especially for biliary tract and pancreas cancers2,3].
CA 19-9 is a high molecular weight glycolipid derivedrom a monoclonal antibody isolated from mice that were
� This work was supported by Samsung Biomedical Research Instituterant #SBRI C-A7-419-1.∗ Corresponding author at: Department of Medicine, Samsung Medicalenter, #50 Irwon-dong, Gangnam-gu, Seoul 135-710, Republic of Korea.el.: +82 2 3410 3409; fax: +82 2 3410 6983.
E-mail address: [email protected] (K.T. Lee).
vtaa
tpn[
590-8658/$30 © 2009 Editrice Gastroenterologica Italiana S.r.l. Published by Elseoi:10.1016/j.dld.2008.12.094
mmunized with a human colon cell line [1,3–6]. It is syn-hesized by normal human pancreatic and biliary ductularells, as well as by gastric, colonic, endometrial, and sali-ary epithelia [1]. Although CA 19-9 can be detected inatients with biliary, hepatocellular, gastric, colonic, and non-astrointestinal cancers, it is still considered the best serumarker for pancreatic cancer because of its high sensitiv-
ty and specificity [1]. CA 19-9 may be a valuable markeror differentiating pancreatic and biliary cancers from otherenign diseases if it is utilized in conjunction with the indi-idual clinical settings [3]. Previous studies have reportedhat CA 19-9 has a sensitivity of 70–90%, a specificity ofpproximately 90%, a positive predictive value of 69%, andnegative predictive value of 90% [1,6–9].
CA 19-9 usefulness has recently been demonstrated in
he staging, evaluation of resectability, assessment of therognosis and recurrence, as well as in the initial diag-osis of malignant disorders, especially pancreatic cancer1,4,7,8,10–12]. It can, however, be difficult to interpret ele-vier Ltd. All rights reserved.

d Liver
vocssap
cutcTaa
2
2
a>MacoipisatOtUa
s
2
cCnV
21
ipfi
wao(ptwa3
ttcl
2
teTcltttde
fmndpt
3
3l
1lreHlyu
B.J. Kim et al. / Digestive an
ated concentrations of CA 19-9 because the concentrationf CA 19-9 used for the differentiation of pancreaticobiliaryancer can also be high in benign conditions, such as cholesta-is, acute cholangitis, or pancreatitis [3]. Moreover, severaltudies have revealed that CA 19-9 measurement is not usefuls a screening test for pancreatic cancer in an asymptomaticopulation [1].
Most previous studies have involved patients with clini-al symptoms, including weight loss or abdominal pain ofnknown origin, or suspicious radiologic findings. However,here have been few reports regarding the clinical signifi-ance of an elevated CA 19-9 level in asymptomatic subjects.herefore, the aim of this study was to prospectively evalu-te the etiology of an elevated CA 19-9 level and to presentppropriate guidelines for its use in asymptomatic patients.
. Materials and methods
.1. Subjects
Between January 2004 and March 2007, we enrolledsymptomatic patients who had an elevated CA 19-9 level37 U/mL at the Health Promotion Center of Samsungedical Center. An asymptomatic patient was defined asperson who did not have abdominal pain or signifi-
ant weight loss. Patients who had a history of cancer,r who were being treated for severe diseases or acutenfections requiring admission were excluded. All of theatients underwent extensive health examinations, includ-ng full physical examinations, routine blood tests (includingerum CA 19-9 and thyroid function tests), chest X-ray,bdominal ultrasonography (USG; LOGIQ 700; GE, USA),hyroid USG, esophagogastroduodenoscopy (GIF XQ 240;lympus, Japan), and colonoscopy (CF 240I; Olympus). For
he female patients, pelvic USG (HDI 5000 SonoCT; Philips,SA) and breast USG (HDI 5000 SonoCT; Philips) were
dded to the above examinations.Informed consent was obtained from all patients, and this
tudy was approved by the Local Ethics Committee.
.2. Assay of CA 19-9
Carbohydrate antigen was assayed by means of a mono-lonal antibody immunoradiometric kit (CA 19-9 RIA kit;entocore, New York City, NY, USA). The upper limit of theormal range was defined as 37 U/mL, as suggested by Delillano et al. [13].
.3. Assessment of the subjects with an increased CA9-9 level
To evaluate the etiology of elevated CA 19-9 levels, wenitially rechecked the CA 19-9 levels and we reviewed theatients’ medical records and the laboratory and radiologicndings.
9al(
Disease 41 (2009) 364–369 365
Further studies were performed when the CA 19-9 levelas above the cut-off value, and these tests included pancre-
tic computed tomography (CT) (Briliance 40; Philips) withr without endoscopic retrograde cholangiopancreatographyERCP; TJF-240; Olympus) or positron emission tomogra-hy (ADVANCE-TM; GE). In these additional CT studies,he late arterial and portal venous phase dynamic CT scansere obtained beginning 45 and 70 s, respectively, after
dministering an IV injection of 100 mL of non-iodinated00 mg I/mL iohexel at the rate of 3 mL/s.
If the subjects had abnormal findings on the examination,hen they were referred to a special clinic for determininghe differential diagnosis. Appropriate management at eachlinic was followed by regular determinations of the CA 19-9evels until they were normalized or stabilized.
.4. Follow-up of patients with an elevated CA 19-9 level
The patients with persistent elevation of CA 19-9 abovehe cut-off value (37 U/mL) at the recheck without definitevidence of the etiology were followed for at least 6 months.he CA 19-9 level was monitored at regular intervals in thease of a normal finding on abdominal CT. If the CA 19-9evel decreased to the normal range or exhibited a decreasingrend during follow-up, then the CA 19-9 level was moni-ored annually. Yet, if the CA 19-9 level had an increasingrend, it was then monitored at intervals of 1, 3, and 6 monthsuring the first 6 months, and then every 3–6 months until novidence of malignancy was demonstrated (Fig. 1).
The etiologies of increased CA 19-9 were categorized asollows: (1) a normal or decreased CA 19-9 level after treat-ent for the causative condition (including surgery), (2) a
ormal or decreased CA 19-9 level with management wheneterioration of the underlying disease was suspected, and (3)ersistent elevation of the CA 19-9 level, but not an increasingrend without evidence of malignancy.
. Results
.1. Characteristics of the patients in whom the CA 19-9evel was increased (Table 1)
Of the 62,976 asymptomatic patients who underwent CA9-9 measurement, 825 (1.3%) patients had a CA 19-9evel >37 U/mL. All the patients had their CA 19-9 levelsechecked, and the 501 (0.8%) patients who had persistentlylevated CA 19-9 levels >37 U/mL at recheck were enrolled.owever, among the 501 enrolled patients, 148 (29.5%) were
ost to follow-up after diagnosis. Thus, this prospective anal-sis involved the 353 patients (70.5%) who were followedp for at least 6 months. The study group was composed of
9 men and 254 women, with a mean (±standard deviation)ge of 51.7 (±12.6) years. Of these patients, 52 had under-ying diseases that were under control, such as hypertensionn = 27) and diabetes mellitus (n = 10). But these patients had
366 B.J. Kim et al. / Digestive and Liver Disease 41 (2009) 364–369
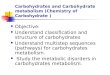
Fig. 1. Diagnostic work-up protocol for asymptomatic patients with elevated CA 19-9 levels. To evaluate the etiology of elevated CA 19-9 levels, recheckCA 19-9 levels initially. If the CA 19-9 level is above the cut-off value, abdominal computed tomography (CT) is performed. If the CT finding is normal,t If the CA19-9 level decreases to the normal range or if it shows a decreasingt CA 19-9 level has an increasing trend, additional studies, including endoscopicr opancreatography (MRCP), or positron emission tomography are performed to ruleo
nt
3e
1i9ti
iawlohs
TDv
MF
TC
Table 2Follow-up results of the subjects with an elevated serum carbohydrate anti-gen 19-9 level >37 IU/mL.
Follow-up result No. (%)
Malignancy 10 (2.8)Pancreatic cancer 4 (1.1)Thyroid cancer 4 (1.1)Duodenal cancer 1 (0.3)Colon cancer 1 (0.3)
Benign disease 97 (27.5)Non-specific 246 (69.7)
T
9(p
hen the CA 19-9 level is monitored at intervals of 1, 3, and 6 months.rend, then it is monitored regularly. If the CT finding is abnormal or theetrograde cholangiopancreatography (ERCP)/magnetic resonance cholangiut malignancy.
o subjective symptoms that suggested any aggravation ofhose diseases.
.2. Follow-up results of the patients who had anlevated serum CA 19-9 level (Table 2)
Most patients revealed a similar or decreased serum CA9-9 level when they were followed up during a short-termnterval (1–3 months). The etiology of the elevated CA 19-
level was evaluated and then classified into the followinghree categories: malignant, benign, and non-specific find-ngs.
Ten patients (2.8%) were diagnosed with malignancies,ncluding pancreatic (n = 4), thyroid (n = 4), duodenal (n = 1),nd colon cancers (n = 1). There were 97 patients (27.5%)ith benign diseases that could explain the elevated CA 19-9
evels. The serum CA 19-9 levels returned to a normal range
r decreased when the underlying causes were corrected. Twoundred forty-six patients (69.7%) were shown to be non-pecific after an extensive evaluation.able 1istribution of the asymptomatic patients with elevated serum CA 19-9alues.
Age (years)
≤29 30–39 40–49 50–59 60–69 ≥70 Total (%)
ale 1 9 16 32 26 15 99 28.0emale 12 37 81 68 40 16 254 72.0
otal 13 46 97 100 66 31 353 100.0olumn (%) 3.7 13.0 27.5 28.3 18.7 8.8 100.0
a
3m
3pMbidwP
otal 353 (100.0)
Ninety-nine patients had a persistent elevation of CA 19-levels for >6 months. When we followed these patients
median, 12 months; range, 6–36 months), we identified 1atient with thyroid cancer, 39 patients with benign diseases,nd 59 patients with a non-specific etiology.
.3. Follow-up results for the patients diagnosed with aalignancy (Table 3)
The median value of CA 19-9 was 115.5 U/mL (range,7.6–538.8 U/mL). With respect to malignancy, one of fourancreatic cancers was stage IV at the time of diagnosis.oreover, another case of pancreatic cancer was diagnosed
y abdominal CT 1 month later due to a sudden increase
n the CA 19-9 level. One of the four thyroid cancers wasiagnosed by PET 2 months later, although the initial studyas normal. A case of duodenal cancer was diagnosed byET 3 months later in spite of the normal abdominal CT.
B.J. Kim et al. / Digestive and Liver Disease 41 (2009) 364–369 367
Table 3Clinical courses of the patients with malignancies.
No. Age Gender Organ Initial CA 19-9 level (IU/mL) TNM Stage Treatment
1 70 F Pancreas 43.3 T3N1M0 II Op2 68 M Pancreas 37.6 T1N1M1 IV CTx3 55 M Pancreas 52.9 T3NOM0 II Op4 44 F Pancreas 131.0 T3N0M0 II Op5 35 M Thyroid 103.4 T2N1M0 III Op6 55 F Thyroid 42.7 T1N0M0 I No7 49 F Thyroid 421.0 T2N0M0 II Op8 50 F Thyroid 127.7 T1N0M0 III Op
1
O py.
Ad
3b
3kga
d((uuanLm
ag
eolpl
tita
dp1s
3fi
TF
O
P
BLGL
E
R
O
T
Ip
9 47 M Duodenum 187.30 41 F Colon 49.6
p, operation; CTx, chemotherapy; CCRT, concurrent chemoradiation thera
n advanced case of colon cancer involving the rectum wasetected by colonoscopy.
.4. Follow-up results for the patients diagnosed withenign diseases (Table 4)
The median value of CA 19-9 was 56.7 U/mL (range,7.6–5860 U/mL). As shown in Table 4, there were variousinds of benign diseases: 10 pancreatic, 7 biliary, 3 liver, 1astrointestinal, 26 lung, 28 endocrinologic, 20 gynecologic,nd 2 other diseases.
In our study, the following common benign diseases wereiagnosed: chronic pancreatitis (n = 7), choledocholithiasisn = 7), thyroid nodular hyperplasia (n = 8), hypothyroidismn = 8), non-tuberculous mycobacterial lung disease (n = 13),terine myomas (n = 7), ovarian teratomas (n = 6), andncontrolled diabetes mellitus (n = 7). Other benign pancre-tobiliary diseases included intraductal papillary mucinouseoplasms, biliary cystic adenomas, and pancreatic lipomas.ung, endocrinologic, and gynecologic diseases were com-
on among the benign extrapancreatobiliary diseases.Interstitial pulmonary fibrosis, mesothelioma, andspergillosis were detected as pulmonary causes. Nontoxicoiter, as well as lymphocytic thyroiditis, was found as
ntwe
able 4ollow-up results of the patients with benign diseases.
rgan Distribution Disease
ancreas n = 10 (10.3%) Chroniccystic ad
iliary tract n = 7 (7.2%) Chroniciver n = 3 (3.1%) Chronicastrointestinal tract n = 1 (1.0%) Papillitiung n = 26 (26.8%) NTM in
(1) PneuMesothe
ndocrine system n = 28 (28.9%) ThyroidLympho
eproductive organ n = 20 (20.7%) Uterinecyst (2),
thers n = 2 (2.0%) Renal T
otal n = 97 (100.0%)
HD, Intrahepatic duct; CBD, Common bile duct; NTM, Nontuberculosis mycobulmonary fibrosis; RML, Right middle lobe; DM, Diabetes mellitus; Tbc, Tubercu
T3N1M1 IV Op → CCRTT3N2M0 III Op
ndocrinologic causes. For the women, endometriosis andvarian cystic lesions caused an elevation of the CA 19-9evels. Elevation of the CA 19-9 level was also noticed inatients diagnosed with renal tuberculosis and tuberculousymphadenitis.
The CA 19-9 level showed a normal or decreasingrend along with improvement of the chest X-ray findingsn patients with bronchiectasis. For patients with non-uberculous mycobacterium, the CA 19-9 levels fluctuatedlong with the treatment response during follow-up.
In uncontrolled diabetic patients, the CA 19-9 levelsecreased with improvement of the blood glucose status. Inatients with ovarian teratomas or uterine myomas, the CA9-9 levels returned to a normal range or decreased afterurgery.
.5. Follow-up results for the patients with non-specificndings
Non-specific findings were defined as a condition in which
o causative disease was found in spite of a thorough diagnos-ic work-up. The median value of CA 19-9 for these patientsas 50.9 U/mL (range, 37.0–1526 U/mL). The CA 19-9 lev-ls in the group with non-specific findings were monitored
s (number)
pancreatitis (7), Intraductal papillary mucinous neoplasm (1), Biliaryenoma (1), Pancreatic lipoma (1)calculous cholecystitis (4), IHD stone (2), CBD stone (1)viral hepatitis (2), Alcoholic liver cirrhosis (1)
s (1)fection (13), Bronchiectasis (4), IPF (3), Tuberculosis (1), Aspergillosismonia (1), RML syndrome (1), Inflammatory granuloma (1),lioma (1)nodular hyperplasia (8), Hypothyroidism (8), Hyperthyroidism (3),cytic thryoiditis (1), Nontoxic goiter (1), Uncontrolled DM (7)myoma (7), Ovarian teratoma (6), Endometriosis (4), Ovarian dermoidovarian mucinous cyst (1)
bc (1), Tbc lymphadenitis (1)
acterium; MOTT, Mycobacteria other than tuberculosis; IPF, Interstitiallosis.

3 d Liver
usam
4
mafottsac
scta[ssesibwdcea[c[
bcmiocp
pmic
isdap
wlb1eph[
iietttb
t[tctrf
Cptoaswdctwoil
srsmsttmb
i
68 B.J. Kim et al. / Digestive an
ntil the CA 19-9 levels normalized or decreased. However,ome patients had persistent elevation of CA 19-9 withoutny further increase, even though there was no evidence ofalignant or benign diseases.
. Discussion
The routine use of CA 19-9 level along with USG forass screening to detect pancreatic cancer is ineffective in
n asymptomatic population since such screening does notacilitate the early identification of subjects with cancer orther diseases [1]. In addition, it is not possible to reliably dis-inguish benign disease from malignant disease processes onhe basis of this tumor marker [14]. Therefore, the diagnosticignificance of an elevated CA 19-9 level must be evalu-ted cautiously, while giving consideration to an individual’slinical situation [3].
This study focused on the diagnostic value of an elevatederum CA19-9 level and the appropriate interpretation in alinical setting. The elevation of CA 19-9 is well knowno be associated not only with cancer of the pancreas, butlso with cancer of the liver, lung, stomach, colon, and ovary10,14–16]. Thus, an elevated value should trigger an exten-ive search for an underlying malignancy [15]. In the presenttudy, the authors revealed the etiology and prevalence oflevated CA 19-9 levels in asymptomatic patients. Our datahowed a substantially small proportion of cancer (2.8%)n the asymptomatic patients. Benign conditions, includingenign diseases (27.5%) and non-specific causes (69.7%),ere the main cause of an elevated CA 19-9 level. Our dataemonstrated that pancreatic cancer was the most prevalentancer along with thyroid cancer. Elevated CA 19-9 lev-ls are commonly associated with an underlying neoplasm,nd these frequently originate from the gastrointestinal tract17–19]. The serum CA19-9 levels are also elevated in gyne-ology patients with malignant and benign ovarian tumors16].
The extensive overlap of the CA19-9 values from theenign and malignant cases indicates that confident dis-rimination can rarely be made on the basis of a singleeasurement [14]. While the usual causes are pancreatobil-
ary malignant tumors, benign diseases can cause elevationf CA 19-9 [2,3,7,11,14,20,21]. In the present study, theseauses ranged from chronic pancreatitis to tuberculous lym-hadenitis, and they are listed in Table 4.
The common underlying mechanism for each disease isrobably inflammatory hypersecretion of CA19-9 by nor-al epithelial cells [22]. However, the increase of CA19-9
n benign diseases is usually not significant, and finding aoncentration of CA19-9 exceeding 1000 U/mL is rare.
Elevated serum levels of CA19-9 can also be observedn various non-malignant gastrointestinal diseases, as was
hown in this study. In the present study, the CA 19-9 levelecreased with improvement of the alleged chronic viral hep-titis and alcoholic liver cirrhosis, which is in agreement withrevious studies [16,23].clMc
Disease 41 (2009) 364–369
It has been reported that the serum levels of CA19-9ere elevated in some patients with non-malignant diffuse
ung diseases, such as idiopathic pulmonary fibrosis (IPF),ronchiectasis, and cystic fibrosis [2]. In this study, the CA9-9 level was elevated in patients with benign lung dis-ases. This indicates that the higher serum CA 19-9 wasrobably due to hypersecretion of mucus glycoprotein fromypertrophic glands and/or epithelial cells in the bronchioles24].
It has been shown that an increase in the CA 19-9 leveln patients suffering from hypothyroidism and the gradualmprovement of thyroid function resulted in resolution of thelevated CA 19-9 levels [25]. Recent reports have suggestedhat diabetes mellitus may be, in part, responsible for eleva-ion of CA 19-9 [26,27]. In this study, the CA 19-9 levels ofhe uncontrolled diabetes mellitus patients were normalizedy strict control of their blood glucose levels.
It has been reported that CA 19-9 may be an impor-ant marker for the diagnosis of mature cystic teratoma28]. This can be explained by the routes for transferringumor-produced CA 19-9 into the circulation [29]. We shouldonsider the underlying diseases when generating a differen-ial diagnosis for an elevated CA 19-9 level, and we shouldeview and exclude the presence of all possible benign causesor the evaluated CA 19-9 levels of these patients.
In our study, in 210 of 246 non-specific cases (85.3%), theA 19-9 levels normalized within 6 months of the follow-uperiod. Yet, in 36 cases (14.7%), no further decrease belowhe normal range was found. Knowledge of the various causesf elevated CA 19-9 enables the clinician to make moreccurate evaluations and earlier diagnoses. Although elevatederum CA19-9 levels are found in various benign conditionsithout malignancy in any site, an extensive work-up foriagnosis may be necessary. As mentioned above, in mostases of benign diseases, CA 19-9 levels increased at first,hen showed a similar or decreasing trend during follow-up,hereas in the case of malignancy, it showed a continu-usly increasing trend in the short-term. Therefore, it is moremportant to observe the trend of the tumor marker than theevel itself as a single test.
If the CA 19-9 level decreases to a normal range or if ithows a decreasing trend after an extensive work-up, thenegular follow-up may be helpful. In addition, if there wereuspected benign causes, close follow-up with proper treat-ent would be necessary. However, if the CA 19-9 level
hows an increasing trend, especially if it more than doubled,hen further evaluation for malignancy may be warranted. Ifhe CA 19-9 level is normalized or decreases during the 6
onths of follow-up, then regular follow-up afterwards maye helpful.
In conclusion, CA 19-9 should not be assessed as a screen-ng tool in asymptomatic subjects because the incidence of
arcinoma in asymptomatic subjects with elevated CA 19-9evels was very low (2.8% [10/353]), as seen in our study.any benign diseases, as well as malignancy, should beonsidered as possible causes of elevated CA 19-9 levels in

d Liver
apfi
CN
A
fdfdccKddlaitc
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
B.J. Kim et al. / Digestive an
symptomatic subjects. Therefore, more attention should beaid to these causative diseases in asymptomatic patients andurther work-up for determining the etiology should be donen cases of persistently elevated CA 19-9 levels.
onflict of interestone declared.
cknowledgements
Author contributions: Beom Jin Kim, M.D. contributedor conception and design; analysis and interpretation of theata; and drafting the article. Kyu Taek Lee, M.D. contributedor conception and design; analysis and interpretation of theata; drafting the article; and critical revision of the arti-le for important intellectual content. Tae Gun Moon, M.D.ontributed for analysis and interpretation of the data. Pungang, M.D. contributed for analysis and interpretation of theata. Jong Kyun Lee, M.D. contributed for conception andesign; and critical revision of the article for important intel-ectual content. Jae J. Kim, M.D. contributed for conceptionnd design and critical revision of the article for importantntellectual content. Jong Chul Rhee, M.D. contributed forhe critical revision of the article for important intellectualontent.
eferences
[1] Kim JE, Lee KT, Lee JK, Paik SW, Rhee JC, Choi KW. Clinicalusefulness of carbohydrate antigen 19-9 as a screening test for pan-creatic cancer in an asymptomatic population. J Gastroenterol Hepatol2004;19:182–6.
[2] Kodama T, Satoh H, Ishikawa H, Ohtsuka M. Serum levels of CA19-9 in patients with nonmalignant respiratory diseases. J Clin Lab Anal2007;21:103–6.
[3] Kim HJ, Kim MH, Myung SJ, Lim BC, Park ET, Yoo KS, et al. A newstrategy for the application of CA19-9 in the differentiation of pancre-aticobiliary cancer: analysis using a receiver operating characteristiccurve. Am J Gastroenterol 1999;94:1941–6.
[4] Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, Fernandez-delCastillo C, Warshaw AL. Perioperative CA19-9 levels can predictstage and survival in patients with resectable pancreatic adenocarci-noma. J Clin Oncol 2006;24:2897–902.
[5] Goonetilleke KS, Siriwardena AK. Systematic review of carbohydrateantigen (CA 19-9) as a biochemical marker in the diagnosis of pancre-atic cancer. Eur J Surg Oncol 2007;33:266–70.
[6] Boeck S, Stieber P, Holdenrieder S, Wilkowski R, Heinemann V.Prognostic and therapeutic significance of carbohydrate antigen 19-9 as tumor marker in patients with pancreatic cancer. Oncology2006;70:255–64.
[7] Kilic M, Gocmen E, Tez M, Ertan T, Keskek M, Koc M. Value of preop-erative serum CA 19-9 levels in predicting resectability for pancreatic
cancer. Can J Surg 2006;49:241–4.[8] Tian F, Appert HE, Myles J, Howard JM. Prognostic value of serum CA19-9 levels in pancreatic adenocarcinoma. Ann Surg 1992;215:350–5.
[9] Safi F, Roscher R, Bittner R, Schenkluhn B, Dopfer HP, Beger HG. Highsensitivity and specificity of CA 19-9 for pancreatic carcinoma in com-
[
Disease 41 (2009) 364–369 369
parison to chronic pancreatitis. Serological and immunohistochemicalfindings. Pancreas 1987;2:398–403.
10] Tsao KC, Hong JH, Wu TL, Chang PY, Sun CF, Wu JT. Elevation ofCA 19-9 and chromogranin A, in addition to CA 125, are detectablein benign tumors in leiomyomas and endometriosis. J Clin Lab Anal2007;21:193–6.
11] Kang CM, Kim JY, Choi GH, Kim KS, Choi JS, Lee WJ, et al. The useof adjusted preoperative CA 19-9 to predict the recurrence of resectablepancreatic cancer. J Surg Res 2007;140:31–5.
12] Safi F, Beger HG, Bittner R, Buchler M, Krautzberger W. CA 19-9 andpancreatic adenocarcinoma. Cancer 1986;57:779–83.
13] Del Villano BC, Brennan S, Brock P, Bucher C, Liu V, McClure M, etal. Radioimmunometric assay for a monoclonal antibody-defined tumormarker, CA 19-9. Clin Chem 1983;29:549–52.
14] Mann DV, Edwards R, Ho S, Lau WY, Glazer G. Elevated tumourmarker CA19-9: clinical interpretation and influence of obstructivejaundice. Eur J Surg Oncol 2000;26:474–9.
15] Parra JL, Kaplan S, Barkin JS. Elevated CA 19-9 caused by Hashimoto’sthyroiditis: review of the benign causes of increased CA 19-9 level. DigDis Sci 2005;50:694–5.
16] Kitagawa Y, Iwai M, Muramatsu A, Tanaka S, Mori T, Harada Y, etal. Immunohistochemical localization of CEA, CA19-9 and DU-PAN-2 in hepatitis C virus-infected liver tissues. Histopathology 2002;40:472–9.
17] Reiter W, Stieber P, Reuter C, Nagel D, Lau-Werner U, Pahl H, et al.Preoperative serum levels of CEA and CA 19-9 and their prognosticsignificance in colorectal carcinoma. Anticancer Res 1997;17:2935–8.
18] Reiter W, Stieber P, Reuter C, Nagel D, Lau-Werner U, LamerzR. Multivariate analysis of the prognostic value of CEA and CA19-9 serum levels in colorectal cancer. Anticancer Res 2000;20:5195–8.
19] Reiter W, Stieber P, Reuter C, Nagel D, Cramer C, Pahl H, et al. Prog-nostic value of preoperative serum levels of CEA, CA 19-9 and CA72-4 in gastric carcinoma. Anticancer Res 1997;17:2903–6.
20] Paganuzzi M, Onetto M, Marroni P, Barone D, Conio M, Aste H, etal. CA 19-9 and CA 50 in benign and malignant pancreatic and biliarydiseases. Cancer 1988;61:2100–8.
21] Yamaguchi K, Enjoji M. Adenoma of the ampulla of Vater: putativeprecancerous lesion. Gut 1991;32:1558–61.
22] Howaizi M, Abboura M, Krespine C, Sbai-Idrissi MS, Marty O,Djabbari-Sobhani M. A new cause for CA19.9 elevation: heavy teaconsumption. Gut 2003;52:913–4.
23] Schoniger-Hekele M, Muller C. The combined elevation of tumor mark-ers CA 19-9 and CA 125 in liver disease patients is highly specific forsevere liver fibrosis. Dig Dis Sci 2006;51:338–45.
24] Roberts DD, Monsein DL, Frates Jr RC, Chernick MS, Ginsburg V.A serum test for cystic fibrosis using monoclonal antibody 19-9. ArchBiochem Biophys 1986;245:292–4.
25] Tekin O. Hypothyroidism-related CA 19-9 elevation. Mayo Clin Proc2002;77:398.
26] Petit JM, Vaillant G, Olsson NO, Guignier F, Collignon S, VergesB, et al. Elevated serum CA19-9 levels in poorly controlled diabeticpatients. Relationship with Lewis blood group. Gastroenterol Clin Biol1994;18:17–20.
27] Shimojo N, Naka K, Nakajima C, Ishizaki T, Okuda K, Murai J, et al.The effect of non-insulin-dependent diabetes on serum concentrationsof tumor-associated carbohydrate antigens of CA19-9, CA-50, and sia-lyl SSEA-1 in association with the Lewis blood phenotype. Clin ChimActa 1990;190:283–9.
28] Dede M, Gungor S, Yenen MC, Alanbay I, Duru NK, Hasimi A. CA19-9 may have clinical significance in mature cystic teratomas of the ovary.
Int J Gynecol Cancer 2006;16:189–93.29] Engelen MJ, de Bruijn HW, Hollema H, ten Hoor KA, Willemse PH,Aalders JG, et al. Serum CA 125, carcinoembryonic antigen, and CA19-9 as tumor markers in borderline ovarian tumors. Gynecol Oncol2000;78:16–20.