Embed Size (px)
Citation preview

How Can We, and Why Should We, Treat and
Prevent Burnout?
Charles Meredith, MDInterim Medical Director
Washington Physicians Health ProgramAssistant Clinical Professor
Psychiatry and Behavioral SciencesUniversity of Washington School of Medicine
February 4, 2011

What is Burnout?
Burnout is a syndrome of
depersonalization, emotional
exhaustion, and low personal
accomplishment leading to
decreased effectiveness at work.

Maslach Burnout Inventory Developed in 1980, validated over the
last 30 years. 22 item survey evaluates the 3 domains
of burnout. Respondents rate frequency on 7 point
Likert scale. 3 Sub-Scales: Depersonalization,
Emotional Exhaustion and Low Personal Accomplishment
Normative national samples of like professionals

Identification of Burnout
Overwhelming physical and emotional exhaustion
Feelings of cynicism and detachment from the job
A sense of ineffectiveness and lack of accomplishment
Over identification Irritability and hypervigilance
Adapted from Kearney MK. Self-Care of Physicians Caring for Patients at the End Of Life. JAMA. 2009;301:1155-1164

Identification of Burnout
Sleep problems, including nightmares
Social withdrawal Professional and personal
boundary violations Poor judgment Perfectionism and rigidity Questioning the meaning of life
Adapted from Kearney MK. Self-Care of Physicians Caring for Patients at the End Of Life. JAMA. 2009;301:1155-1164

Identification of Burnout Questioning prior religious beliefs Interpersonal conflicts Avoidance of emotionally difficult
clinical situations Numbness and detachment Difficulty in concentrating Frequent illness—headaches,
gastrointestinal disturbances
Adapted from Kearney MK. Self-Care of Physicians Caring for Patients at the End Of Life. JAMA. 2009;301:1155-1164

Have you Seen the Following in Someone
You Know? physical exhaustion repetitive cynicism guilt ineffectiveness a sense of depersonalization in
relationships with coworkers or patients

The “Physician Personality”Adaptive
Diagnostic rigor Thoroughness Commitment to
patients Desire to stay
current Recognize
responsibility of patients trust
Maladaptive Difficulty relaxing Problem allocating
time for family Sense responsibility
beyond what you control
Sense “not doing enough”
Difficulty setting limits Confusion of
selfishness vs. healthy self-interest
Difficulty taking time off
-Gabbard JAMA 254:2926

What we typically do when we feel stress:
Intellectualize the stress: “I need to understand what is going on”
Minimize or deny: “I should not be feeling this way” or “I don’t feel this way”
Intensify our effort: “I just need to hunker down”

Physician characteristics associated with increased risk
for burnout Studies suggest high association with the following:
a hectic schedule a strong achievement orientation an inability to say “no”
One study suggested that the very traits that define a good physician—also place them at greater risk for burnout: commitment to patients attention to detail recognizing the responsibility associated with
patients’ trust

Why Should We Care?
Impact on Team (potential impairment!)
Disrupts collaboration, consultation, collegialism, and morale
High job turnover Impaired job performance
(decreased empathy, increased absenteeism)
Staff splitting and conflicting

What’s happening to physicians and surgeons?


Canadian National Physician Survey
Sullivan, CMAJ 159:525 (1998) >3500 physicians responding
(RR 44%)
62% Workload too heavy
55% Family & personal life suffers because physician
65% Opportunities to change career limited

Burnout Among Surgeons
Campbell, Surgery 130:696 (2001) Surgeons in Michigan (RR= 44%;
n=582) Among practicing responders ~ 32%
burned out BO > among younger surgeons
(p<0.01) Sense of imbalance
work/family/personal growth correlated with BO

2008 ACS Survey Anonymous, cross-sectional
survey ACS members current e-mail
(n=24,922) 61 item survey including
standard tools assess:BurnoutMental and physical QOLSymptoms of depression
Response rate 32% (n=7905)

Burnout Domains
40
13
32
26
0 10 20 30 40 50
"Burned Out"
Low PersonalAccomplishment
Hi EmotionalExhaustion
Hi Depersonal
% of Surgeons

Hours and Burnout
p<0.001

Factors Independently Associated with Burnout
(ACS Survey; Multivariate Logistic Analysis)
Characteristic and Associated Factors Odds Ratio1 P Value
Sub-specialty choice 1.2-1.6 All <0.013
Youngest child less than 21 years old 1.54 <0.0001
Compensation = incentive pay based entirely on billing 1.37 <0.001
Spouse works as other healthcare professional 1.23 0.004
# nights on call per week 1.05 <0.001
Hours worked per week (each additional hour) 1.02 <0.001
Age (each additional year older) 0.96 <0.001
>50% time non-patient care 0.81 <0.001
1 OR >1 indicate increased risk of burnout; OR<1 indicate lower risk of burnout

Factors Associated with Career Satisfaction (Surgeon)
Odds Ratio
P value
Absence of Burnout 4.12 <0.001Higher academic rank ~1.3 <0.02
Age (each year) 1.03 <0.001Hours/week in OR (each
hour)1.01 0.033
# Nights on call/week (each night)
0.95 <0.001
Private practice 0.71 <0.001

Career Satisfaction
71% responders would become physician again
74% would become surgeon again
51% would recommend their children become physician/surgeon
36% work schedule leaves enough time for personal/family life

Again, Why Should We Care?

Self-reported Major Medical Errors in ACS
Survey
OR Reporting Error
p
Each 1 point increase EE
1.05 <0.0001
Each 1 point increase DP
1.11 <0.0001
Each 1 point decrease PA
0.97 <0.0001
Screen + depression 3.21 <0.0001

4.85%
9.46%
14.69%
0%
5%
10%
15%
20%
25%
Low EE Int EE High EE
Emotional Exaustion
% M
ajor
Med
ical
Err
or in
Las
t 3
Mo
Emotional Exhaustion and Errors

Perceived Errors%
Reported Error last 3 months 9%
Greatest contributing factor
Lapse judgment 32%
A system issue 15%
Degree of stress/burnout 13%
Lapse concentration 13%
Fatigue 7%
Lack of knowledge 5%
Other 16%

JAMA 302:1294 (2006)
JAMA 296:1071 (2009)

Professional consequences of burnout
poor judgment in patient care decision-making
hostility towards patients medical errors adverse patient events diminished commitment and dedication
to productive, safe and optimal patient care
Diminished relations with colleagues Approximately 15% of all physicians will be impaired
at some time in their career and will be unable to meet professional responsibilities because of mental illness, alcoholism or drug dependency
(Boisaubin and Levine: Am J Med Sci 2001;322:31-36.

Professional consequences of burnout
Increased rates of malpractice events Burn out in students is correlated with
lower scores in empathy and professionalism
This is predictive of later trouble with the disciplinary board and significant boundary violations
Data suggests that burnout can precipitate chemical dependency and mood disorders Approximately 15% of all physicians will be impaired
at some time in their career and will be unable to meet professional responsibilities because of mental illness, alcoholism or drug dependency
(Boisaubin and Levine: Am J Med Sci 2001;322:31-36.

Depression
30% of responders in the ACS survey screened positive for depression Suggest ~ 10% would meet
criteria MDD

Suicidal Ideation Among Surgeons
501 (6.4%) surgeons thoughts suicide last 12 months
78% surgeons with SI had symptoms depression
26% surgeons SI sought psychiatric help 60% SI reluctant to seek help for
treatment of depression due repercussions medical license
Only 22% used depression medication last 12 mo
26% self-prescribed or had prescribed by colleague

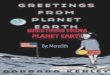
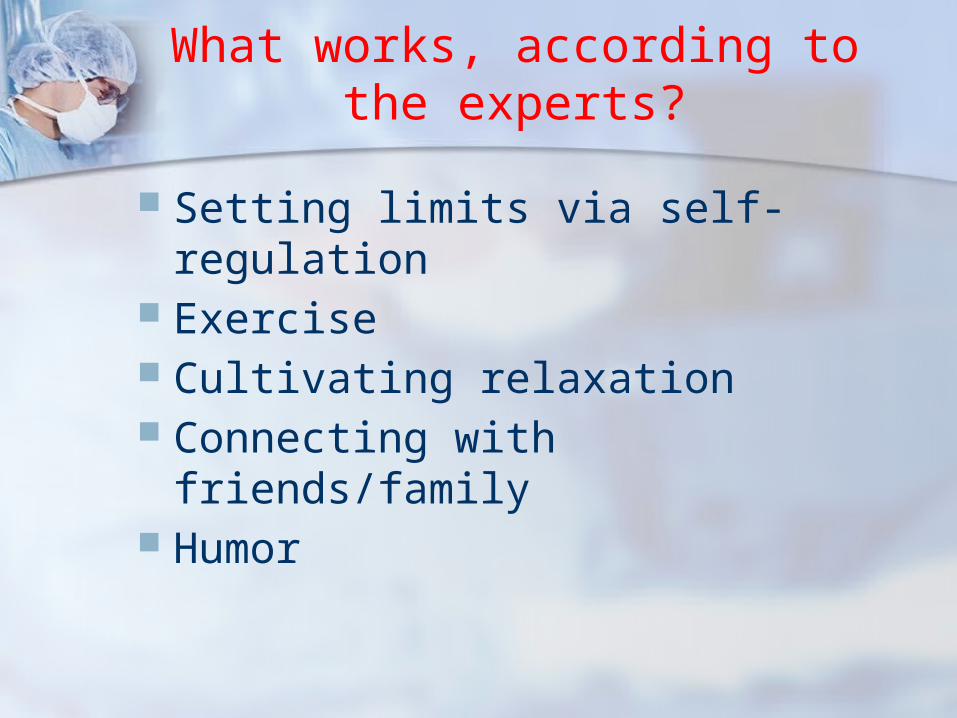
Depersonalization and SI
OR p
+ Depression screen 7.0 <0.001
Burnout 1.9 <0.001
Perceived error last 3 mo 1.9 <0.001
Youngest child age 19-22 1.6 0.004
Incentive pay only 0.8 0.035
Married 0.7 0.002
Practice academic medical center
0.6 <0.001
Factors Associated with Suicidal Ideation on Multi-
variable Analysis
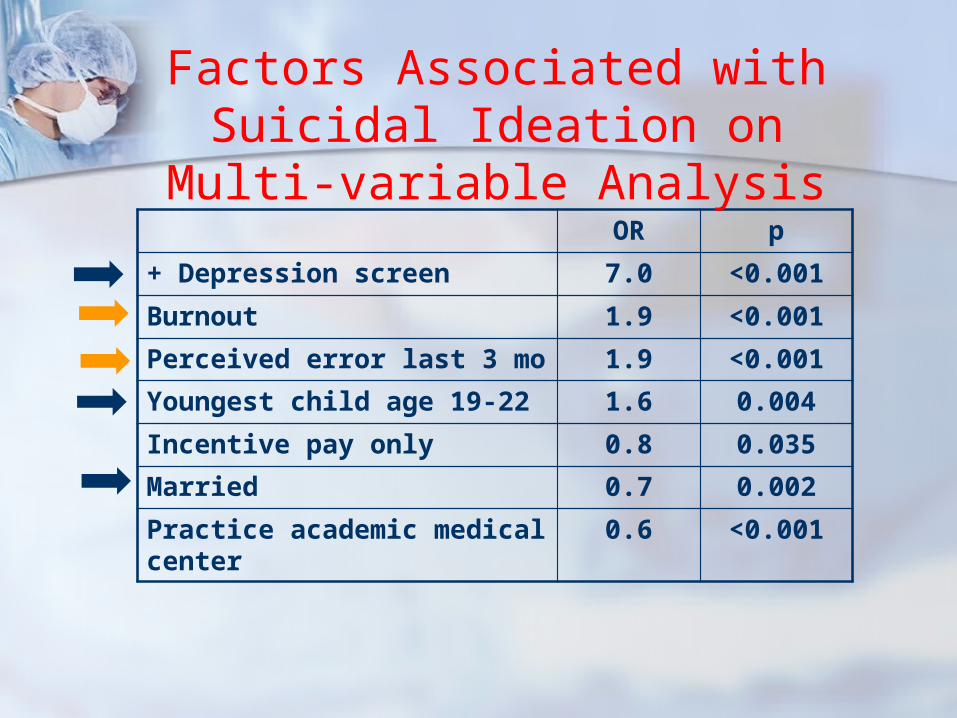
Proportionate Mortality Ratio:Male Physicians vs Male
Professionals
Frank, JAMA.289:3161 (2003)

Burnout and suicidal ideation in U.S. medical
students
Risk of Suicidal Ideation Odds Ratio
Burnout OR 3.46 P<0.001
High Emotional Exhaustion OR 3.17 P<0.001
High Depersonalization OR 2.10 P<0.001
Low Sense of Personal Accomplishment
OR 2.03 P<0.001
50% of students met criteria for burnout over the past year
11% met criteria for SI in past year
Drybye et al., Annals of Internal Medicine 2008;149:334-341

Burnout and Professionalism in U.S. Medical Students
Dyrbye et al., JAMA 2010;304 (11):1173--1180
What works, according to the experts?
Setting limits via self-regulation Exercise Cultivating relaxation Connecting with friends/family Humor

Individual and Institutional Interventions for Burnout
Increase efficiency, autonomy, and meaning in work
Fostering self-awareness and self-reflection by writing a brief narrative about a personal experience while practicing
Process this “mindfulness” with other participants in small groups (increases attention, awareness, intention, and self-reflection)
Enhancing physicians’ attention to their own experience increases their orientation toward patients but also reduces their distress

*Measures That May Help Prevent Burnout
1. Mindful meditation2. Reflective writing3. Adequate supervision and
mentoring4. Sustainable workload5. Promotion of feelings of choice
and control6. Appropriate recognition and
reward
Adapted from Kearney MK. Self-Care of Physicians Caring for Patients at the End Of Life. JAMA. 2009;301:1155-1164

*Measures That May Help Prevent Burnout
7. Supportive work community8. Promotion of fairness and justice
in the workplace9. Training in communication skills10.Development of self-awareness
skills11.Practice of self-care activities12.Continuing educational activities
Adapted from Kearney MK. Self-Care of Physicians Caring for
Patients at the End Of Life. JAMA. 2009;301:1155-1164

*Measures That May Help Prevent Burnout
13.Mindfulness-based stress reduction for team
14.Meaning-centered intervention for team
*Randomized trials have primarily shown
the effectiveness of mindfulnessmeditation and reflective writing.

*Association of an Educational Program in Mindful Communication with Burnout, Empathy, and Attitudes among Primary
Care Physicians 70 PCPs 8 week intensive course of
mindfulness meditation, self-awareness exercises, narratives of meaningful clinical experiences, appreciative interviews, didactics, discussions
10 month maintenance (2.5 hrs./mo.)
Krasner MS, Epstein RM, et. al. JAMA. 2009; 302:
1284-1293

*Association of an Educational Program in Mindful Communication with Burnout, Empathy, and Attitudes among Primary
Care Physicians Measured mindfulness (2 subscales),
burnout (3), empathy (3), psychosocial orientation, personality (5), mood (6) at 2, 12, 15 mos.
Improvements in mindfulness statistically correlated with improvements in mood, empathy, burnout, conscientiousness, and emotional stability
The improvements were sustained throughout the duration of the study
Krasner MS, Epstein RM, et. al. JAMA. 2009; 302:
1284-1293


How to contact me:
Washington Physicians Health Program
206-583-0127
800-552-7236
Call us to “discuss the situation”!
www.wphp.org