Embed Size (px)
Citation preview

gett
yim
ages
/Kat
arzy
naBi
alas
iew
icz
34 VOLUME 36 • ISSUE 2 2018
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES
HOW CAN AUSTRALIA’S MEDICARE SYSTEM BE REFORMED SO THATEXERCISE-BASED
THERAPIES ARE PROPERLY
FUNDED?

VOLUME 36 • ISSUE 2 2018 35
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES
IN THIS SPECIAL GUEST EDITORIAL, SPORT AND EXERCISE PHYSICIAN, DR JOHN ORCHARD PRESENTS A COMPELLING CASE ON HOW TO INCREASE FUNDING AND RECOGNITION FOR EXERCISE-BASED TREATMENTS.
The question posed by the title of this article is of the utmost importance, because exercise-based therapies should be front
and centre in our health system. Even though I think this topic is of critical importance, I’ll o� er some caveats to start with. The con� ict of interest is the � rst declaration, as I’m a sport & exercise medicine (SEM) physician, so I stand to bene� t if exercise-based therapies are better funded (as will the other primary exercise-based groups, physiotherapists and exercise physiologists, EPs). However, if anyone reading has been living in an evidence-free cave for the last decade and not fully aware that exercise-based therapies are e� ective for preventing and treating cancer, cardiovascular disease, osteoarthritis, back pain, diabetes, osteoporosis and depression, amongst other medical conditions, then spend some time reading the systematic reviews in these areas before you pass go. I’m assuming knowledge of the � eld, with the discussion moving on to why one of the most e� ective forms of management is poorly funded. There also isn’t space to detail that exercise-based management isn’t as easy as specialists in non-exercise-based medical specialties may think it is (refer Dunning-Kruger E� ect). I acknowledge that disease-modifying anti-rheumatic drugs, chemotherapy
and surgical techniques all require great expertise to master, but please acknowledge in return that exercise prescription actually does require expertise as well. Just because you read how important exercise-prescription is recently, doesn’t mean you can do it as well as someone who’s been specialising in it for 20 years. If you want to read more from medical specialists who are non-experts in exercise prescription, Google the article “Your doctor does not give a crap about your � tness tracker data”. SEM physicians, who are doctors, and who do care very much about your � tness tracker data, know how to interpret it more than doctors who “don’t give a crap” and physios and EPs who also care about your � tness tracker data, might be o� ering you the best available treatment for your condition, even though they aren’t medical doctors.
A further warning is to those who subscribe to the view that “all specialties and practitioners in di� erent � elds should stick to their � eld and refrain from criticising others”. I’d love to be in a position to follow this advice, but may seem to break this edict in the sections that follow. The reason why is that “others” have lobbying to rig the Medicare Bene� ts Schedule (MBS) in order to stop exercise-based therapies from being properly funded. The onus should actually be on the non-exercise-based therapies (especially doctors who prescribe drugs and surgery) to prove superiority to exercise-based therapies in order to justify far more generous MBS funding. My motivation is to promote exercise-based therapies, but some of it may come across as arguing against doctors who use drugs and surgery as primary treatment.
If everyone was funded fairly – and by fairly, I mean according to the evidence of which treatments work and which don’t – then there’d be no need to draw any comparisons between exercise-based practitioners and drug/surgery-based doctors. But if you don’t want to read any criticism of other doctors and their treatment options, please stop reading now, and perhaps pick up a copy of my recent MJA Perspective “How exercise medicine has evolved from sports medicine” [208(6):244-245] which is the nicer, politically-correct peer-reviewed version.
I will elaborate later, but the exercise-based practitioners (SEM physicians, physios and EPs) need to form a lobbying block with the help of an ally (to be revealed across the course of this article). SEM physicians need physios and exercise physiologists, because SEM physicians are too small a group to be able to provide the (required) mass delivery of exercise-based therapy to the greater population. SEM physicians currently provide great services to the higher socioeconomic segment that can a� ord the out-of-pocket expenses, given the lack of meaningful government funding (either state through public hospitals, or Federal through MBS). If SEM physicians were funded so that lower socioeconomic groups could access services, there would be a di� erent problem: an enormous shortage of SEM physicians. Physios and EPs however, are more plentiful and have the workforce numbers to be able to provide services to the entire community, but again, with respect to lower socioeconomic groups, only if the funding follows.
Physios and EPs need SEM physicians for a di� erent reason, or more speci� cally, they need SEM physicians to be taken seriously in the specialist medical world. If the status quo of “other” medical specialists not taking SEM physicians seriously (both in reputation and funding) continues, then there is little hope of physios and EPs being taken seriously

36 VOLUME 36 • ISSUE 2 2018
by mainstream medical specialists. We have to break the perception of “real/hard/proper” medicine being drugs and surgery and that therefore exercise prescription is “soft/easy/basic.” But even though I think physios and SEM physicians should be part of a lobbying block, I don’t see a future of major cross-referral between these two groups that cuts out the GP. In fact, and I’ll eventually work my argument towards this, GPs may actually be the key health practitioner to drive the change of exercise-based practitioners being taken seriously by the health system.
How badly has the MBS been hacked by the non-exercise based practitioners who have traditionally had greater pull with the health bureaucrats? Let’s consider a hypothetical patient: ‘Patient X’ who is a 55-year-old sedentary female with breast cancer. There is very good evidence that successfully implementing an exercise program in this patient will
decrease her mortality by 30%; in lay terms, “save her life” or “cure her cancer”. But let’s make her a typical real-life patient and give her a right knee medial meniscal tear with early osteoarthritis and bilateral tennis elbow pain, so that when her oncologist or GP ask her to “do some exercise,” she says, “I can’t exercise my legs because my right knee hurts and I can’t do anything with my arms because my elbows hurt.” We’ll also put her on a Health Care Card and having her breast cancer treated in the Public Hospital System because she struggles to a� ord out of pocket expenses. I won’t touch on her chemotherapy, radiotherapy and breast surgery management, because I don’t know much about how these are funded (although I presume good quality treatment is available in the Public Hospitals). I’m keen to discuss how a practitioner might get this patient to be able to do more exercise, which we need to remember, is a very important factor in whether she survives her cancer.
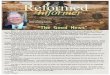
Let’s see what the MBS has to o� er her in terms of rebates for exercise-based therapies compared to other options to allow her to get exercising and reduce her mortality from breast cancer (Table 1).
Table 1 shows that the most generous rebate o� ered (for a 40-minute service) is for a discredited procedure for her condition – a knee arthroscopy and chondroplasty. This has been subjected to multiple randomised control trials (RCTs) and has never been able to signi� cantly beat a comparator treatment or placebo surgery. Yet it is by far, the most generously funded item by Medicare (remembering that the surgeon also has the bene� t that the hospital funding is paid separately so rent does not need to be paid out of the MBS rebate as it does for the consultation items). Although the number of knee arthroscopies have dropped in recent years as patients become more aware of evidence, item 49561 was still claimed 32,429 times in Australia in the most recent � nancial year July 2017 – July 2018. Menisectomy plus chrondroplasty, as a discredited operation, should have lost most of its funding, but it has been indexed over the years even as the RCTs mount up showing that it is an ine� ective operation.
Table 1 – Rebates available for various practitioners to treat Patient X
Practitioner MBS Item number – 2018
Best MBS rebate for a 40-minute service in 2018
Service Evidence-based?
Best MBS rebate for a 20-minute non-initial service
Best 40 min rebate 2008
Best 20 min rebate in 2008
General practitioner 743 $151.25 Coordinating multidisciplinary
case conference Yes $72.80 $131.35 $63.75
Physiotherapist 10960 $52.95Chronic care consult based on exercise & load management
Yes $52.95 $48.95 $48.95
Exercise physiologist 10953 $52.95
Chronic care consult based on exercise & load management
Yes $52.95 $48.95 $48.95
Anti-vaccine Chiropractor 10964 $52.95 Chronic care consult based
on ??? No $52.95 $48.95 $48.95
Orthopaedic surgeon 49561 $505.50 Arthroscopic menisectomy/
chondroplasty No $37.15 $467.10 $33.75
Rheumatologist 132 $227.70Chronic care consultation including cortisone injections*
Yes?/No* $114.00 $207.25 $103.75
All other Physicians (not SEM) 132 $227.70 Chronic care consultation ? $114.00 $207.25 $103.75
Sport & Exercise Medicine Physician 104 $73.85 Consultation based on
exercise & load management Yes $37.15 $93.80 $63.75
HOW CAN AUSTRALIA’S MEDICARE SYSTEM BE REFORMED SO THATEXERCISE-BASED
THERAPIES ARE PROPERLY
FUNDED?
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES
* According to the 2017 Therapeutic Guidelines: Rheumatology, a rheumatologist should treat both knee osteoarthritis and tennis elbow with multiple cortisone injections. Randomised controlled trials against placebo injections has found that cortisone injections are harmful for both of these conditions when compared to placebo injections.

gett
yim
ages
/Kat
arzy
naBi
alas
iew
icz
VOLUME 36 • ISSUE 2 2018 37
The next most generous category of rebate is granted to almost all medical specialist physicians, with the glaring exception of SEM physicians (who are not deemed to qualify as “physicians” under the MBS). Consultant physicians can generally be relied upon to provide high-quality service, but in the musculoskeletal world, you can’t be sure. Therapeutic Guidelines: Rheumatology (2017 version, sadly) states that both the knee osteoarthritis and tennis elbow of Patient X should be treated with “multiple” cortisone injections (multiple being required as the patient often gets worse after the initial one(s) wear o� , so you need to repeat them). The 2017 version, I kid you not, written from a cave where you don’t have to read RCT results. TG:R isn’t picky about which joint or which tendon you have pain in, by the way, it o� ers a blanket recommendation for cortisone injection for every joint and every tendon listed. It states that the most important factor in considering a cortisone injection is the expertise of the practitioner (not whether there is RCT evidence that it beats placebo).
On the third tier of MBS rebates for Patient X is the general practitioner, who is awarded a mid-range rebate for a longer consultation which gets upgraded (fairly) in the event of organising team care arrangements, which in the scenario I painted for Patient X, seems highly justi� ed. Like any practitioner, there is the capacity for GPs to be delivering harmful treatment options, and the biggest failing of GPs in recent years is not “inappropriate antibiotics” but instead
“inappropriate painkillers.” Patient X can get sensibly prescribed opiate painkillers if she has entered palliative care for advanced cancer, but if she gets incorrectly prescribed opiates for her knee pain or tennis elbow, it is a disaster.
Basically at the bottom tier for MBS practitioner rebates is a collective of all Allied Health practitioners and SEM Physicians, meaning that all of the Exercise-based practitioners are part of a group of practitioners that receive relatively paltry patient rebates from Medicare. SEM Physicians have the unique distinction of being the only practitioners in the entire MBS whose patients’ rebates are lower in absolute terms than they were 10 years ago. The SEM rebates are actually 20-35% lower, even o� a low base, whereas the other MBS rebates have generally been minimally indexed (10% higher in 10 years, obviously well below CPI). As can be seen from Table 1, even though the Australian Medical Council (AMC) assessed SEM as being a fully-� edged medical specialty ten years ago, patient rebates are up to 66% lower than for Rheumatology & Rehab Medicine, which would be the closest specialties to SEM. It is not simply a matter of being penalised for being a “newer” specialty. Sexual Health and Addiction Medicine were recognised at exactly the same time as SEM yet have subsequently been granted equity with the other physician specialties. It is hard not to reach the conclusion that SEM is penalised under the MBS simply for the fact that SEM is an exercise-based medical specialty and not a drug-based or procedure-based
specialty. It is important to interpret Table 1 as a “patient payment” not “practitioner payment.” SEM physicians being specialists who are slightly undersupplied in the market can and do typically charge similarly to the fees that are the Medicare rebate amounts for other physicians, meaning that most of the fee has to be paid out of the patient’s pocket. E� ectively, this might mean our hypothetical Patient X can’t a� ord to see a SEM physician, and since there aren’t SEM physicians in public hospitals either, it is an important service that may not be available for Patient X due to lack
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES

gett
yim
ages
/Hal
fpoi
ntge
ttyi
mag
es/H
alfp
oint
38 VOLUME 36 • ISSUE 2 2018
of government support. Physiotherapy and EP charges may be slightly lower compared to SEM physicians and there is somewhat of a presence in public hospitals, but similar logic applies. The highest quality (longer consultations one-on-one focused on exercise programs) physios and EPs are not fully subsidised by MBS and hence, are services that higher socioeconomic patients can fully access, but poorer patients can’t. And for Patient X – we need to keep repeating it – these are services that will increase her survival from breast cancer which the government is not fully funding.
A problem with the funding for the Allied Health group under the MBS is that it represents a vast array of practitioners and provides no quality di� erentiation between them (either between type of practitioner, or within the group). An anti-vaccine chiropractor who claims that all of Patient X’s cancer, tennis elbow and knee pain can be cured by “spinal manipulation” gets the same MBS
rebates as a physiotherapist trying the implement the � rst 5 visits of the GLA:D program before the rebates run out.
The Allied Health option which is perhaps the easiest to reform is exercise physiology. There are particular conditions, such as breast cancer and depression, where treatment bene� t has been shown after a healthy number of EP consultations (often >5 visits). It is a no-brainer to o� er higher rebates and more consultations speci� cally for EP and speci� cally for these conditions.
Physiotherapy may be more suitable for load-base treatment requiring subtlety. For knee and hip osteoarthritis, back pain, chronic tendinopathy etc., the amount of exercise that the patient needs to do must be very carefully dosed by a practitioner who understands the biomechanics of that particular condition. However, a good deal of physiotherapy practice involves passive
treatment that is not evidence-based. Physiotherapy should be able to argue for higher rebates for musculoskeletal conditions that have been shown to respond to load-based management, such as GLA:D for osteoarthritis, but the higher rebates and higher number of visits should relate to delivering high-quality exercise-based treatment, not passive treatment. Other Allied Health groups such as chiropractic and osteopathy also have the capacity to deliver exercise-based treatments, but typically deliver non-evidence-based passive treatments. Groups like COCA may be in a position to break away from traditional chiropractic and eventually use higher rebates for exercise-based treatments, if these are successfully trialled by physiotherapy. The same political issue that is dividing medicine may apply in that the government may only agree to increased rebates for the evidence-based treatments if funding is cut for the non-evidence-based treatment.
This brings me back to SEM itself. I’ve lost count of the number of times I’ve been
told that “SEM is not a real medical specialty,” but let
me recount the most notable occasions
HOW CAN AUSTRALIA’S MEDICARE SYSTEM BE REFORMED SO THATEXERCISE-BASED
THERAPIES ARE PROPERLY
FUNDED?
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES

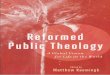
Figure 1 – GP recommended management and referral pathway for knee osteoarthritis, from the Australian Clinical Care Standard, 2017
VOLUME 36 • ISSUE 2 2018 39
when this view has been expressed by a di� erent medical specialist in a representative position. In 1991, I sat and passed the surgical primary exam, as it turned out, the Australasian College of Sport and Exercise Physicians (ACSEP) had some inaugural training positions available just prior to creating their own primary exam, and I thought (correctly) that I could be selected for an ACSEP training position with a surgical primary. One of the surgical training program supervisors, on hearing I had done this, abused me and said it was a disgrace that I had been allowed to sit their exam when I only had intention to train in a specialty “that wasn’t real and didn’t exist”. In 2000, I felt obliged to resign from the Australian Medical Association (AMA), in reply to an enquiry as to whether the AMA could help in having my SEM training recognised as specialist training. My AMA State President wrote to me and said the AMA couldn’t help because “I hadn’t actually done any specialist training.” Various AMA Presidents and Vice-Presidents in the years subsequent to SEM actually being recognised by the Australian Medical Council (AMC) as a medical specialty, when I was considering re-joining, changed their stance to “SEM is in a curious position, not being General Practice, but not really being a specialty,” never stopping to consider for a minute that the curious position existed only because they refused to recognise a specialty that had been completely accepted by the Australian Medical Council (AMC) after a decade-long assessment process. The curious position meant that I wasn’t rejoining the AMA too quickly.
In 2017, I was a panel member to determine the Australian Clinical Care Standard for the management of knee osteoarthritis (OA). I had the temerity to suggest that exercise-based practitioners should be considered priority referral recommendations for GPs treating knee osteoarthritis based on the evidence that exercise was the best available treatment for knee OA. This was rejected by the Chair, who was a leading Rheumatologist representing the Australian Rheumatology Association (who instead, went with Figure 1), based on the following arguments:
(1) That physiotherapists (& EPs) should not be included as the preferred practitioners for GPs to refer to for
knee OA as they were not medical specialists, and the Chair insisted that medical specialists should remain as the preferred referral choices for GPs.
(2) That SEM physicians should not be included as preferred practitioners for GPs to refer to for knee OA as despite being medical specialists, the Chair insisted that their (SEM Physicians’) training and expertise, with respect to managing knee OA, was inferior to rheumatologists and that therefore GPs should be instructed that rheumatologists were preferred.
So, the non-medical specialists who prescribe the correct treatment (exercise) for knee OA, missed out because of the dog whistle that they “weren’t medical specialists”, and I call this a dog whistle as it is an indicator that recommendations are going to be made based on hierarchy of eminence, rather than evidence. However, even the medical specialists (SEM physicians) who prescribe the correct treatment (exercise) missed out also, I presume because of the recurring mantra that “SEM isn’t a real medical specialty.” It absolutely couldn’t be because the cortisone injections, methotrexate, pregabalin and other drugs that rheumatologists are more likely to prescribe, are better for knee OA than the load management that SEM physicians are more likely to prescribe.
Figure 1 is why I refused to sign the � nal Clinical Care Standard, in that it instructs GPs to refer to “Surgeons and Rheumatologists” for knee OA, rather than exercise-based practitioners, which I feel – based on the evidence – is simply a major error.
In 2018, I asked the candidates for the AMA Federal Presidency and Vice-Presidency on Twitter whether they would support equal recognition under the MBS for SEM as a physician specialty. One of the candidates, a hand surgeon, tweeted that the AMA wouldn’t support this as – wait for it – “Sport and Exercise Medicine is not a specialty in Australia”. The AMA has never made any public statement on SEM (for example, not congratulating SEM when it actually did get recognised as a specialty) and it didn’t start by correcting the blatant error of one of its Vice-Presidential candidates.
It’s notable that the last two of these anecdotes involved female medical specialists who have been role models at promoting better access for medical specialty training for women. I’m personally aware that I am a bene� ciary of white privilege, male privilege, doctor privilege, private-school education privilege. It has been an eye-opener for me to have had to face one relatively minor discriminatory handicap of having other doctors tell me I’m not a “real
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES

gett
yim
ages
/Kat
arzy
naBi
alas
iew
icz
40 VOLUME 36 • ISSUE 2 2018
Learn form a range of topics including:• Strength and conditioning• Load management• Injury screening• Injury prevention for Australian football, soccer
and netball• Managing concussion safely• Psychology: handling defeat, celebrating success• Pitch-side assessment for shoulder dislocation, ankle
sprains, hand injuries, and first-aid (bleeding and wound care).
• Nutrition for recovery and performance
Sports Medicine Australia invite you to join us for our annual regional event in Gippsland, Victoria. This practical, interactive forum is aimed at equipping participants with practical skills and techniques to help keep athletes injury free and performing at their peak.
Sunday 21st October 2018 9am–4pmLatrobe Performing Arts CentreTraralgon Little TheatreGrey St, Traralgon VIC 3844
@sportsmedicineaustralia@SMA_Events
For more information and to register visitwww.sma.org.au
Elite Care for the Weekend Warrior
This event is a must for any clubs, coaches, athletes and support staff.Learn from and network with leading experts and other clubs in the region.
RegistrationTH
E
EXPERIENCEMATCH-DAY
ABOUT THE AUTHOR
Dr John Orchard is a Sport and Exercise Physician with over 25 years’ experience. He has been published in over 300 scienti� c publications. John has been involved with many elite sports teams including the Sydney Swans, Sydney Roosters, Australian Cricket Team and the Australian NSW State of Origin Team. He is currently the Chief Medical O� cer for Cricket Australia.
Editor’s Note: The views expressed in this editorial piece do not necessarily re� ect those of SMA or SMA’s National Board. Sport Health’s editorial team upholds SMA members’ rights to express themselves in a respectful manner. If you have an editorial you would like to share in the next issue of Sport Health, please contact [email protected]
HOW CAN AUSTRALIA’S MEDICARE SYSTEM BE REFORMED SO THATEXERCISE-BASED
THERAPIES ARE PROPERLY
FUNDED?
specialist” because I’ve chosen SEM as my specialty. It can be noted that facing (unfair) barriers in your medical training for being, say, female, doesn’t necessarily stop you from erecting equally unfair barriers regarding other doctors for other reasons. And although this article seems like a rant against rheumatologists and surgeons, I certainly appreciate that they do great work with many conditions. However, they have their � aws, like all specialists, with one of them being not enough appreciation of practitioners who are primarily exercise-based, rather than being drug or surgery-based.
However, from the depths in 2018 of an AMA Vice Presidential candidate declaring sports medicine as “not a specialty”, an amazing thing happened. One of the AMA Presidential candidates
(who turned out to be the successful candidate) sent me a Twitter message saying he would support SEM getting equitable rebates under the MBS for Chronic Disease Management. I messaged him back and promised that after an 18-year absence, that if he won the Presidency, I would rejoin the AMA, and I did. I’m hoping he’ll get the chance to turn his personal support into actual AMA support of the specialty of SEM, � nally over-ruling the “SEM is not a real specialty” crew, and that I’ll feel comfortable staying on as an AMA Member once his Presidential term ends.
So how is it that a GP can see the value in an exercise-based medical specialty when so many of his medical specialist colleagues haven’t been able to? In retrospect, it’s obvious. GPs are at the centre of the health system and can and do refer to everyone. The good GPs have now had enough contact with SEM physicians, physios and EPs to know that they all provide a good service, that it’s exercise-based, and they keep reading that for knee OA, back pain and tendon problems, that the evidence is moving away from drugs and surgery and towards exercise-based treatment. However, good GPs also know that the patients of SEM Physicians are having to pay a lot out of pocket, and it’s not because of overcharging, it’s because of under-rebating. The same good GPs no doubt think the same about physiotherapy and exercise physiology. They also probably steer patients away from anti-vaccination chiropractors, but they probably know one or two good chiropractors or osteopaths, who are likely to be exercise-based and members of COCA.
Underpinning the need to get proper MBS rebates for exercise-based practitioners is the important science
that exercise is an e� ective treatment – and prevention – for a vast number of chronic diseases. But it is lobbying that is now required for exercise-based practitioners to get fair funding under the MBS, and we must all stick together and work with GPs to get it over the line. The main reason for this is to allow Australians from all socioeconomic backgrounds – not just the rich – be able to access evidence-based exercise-based treatment.
FEATURE: FUNDING FOR EXERCISE-BASED THERAPIES