Upload
others
View
3
Download
0
Embed Size (px)
Citation preview
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Sharon Kimble(S.E.N.,R.G.N.)
Hormones 2016
Build - 2016.3576
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Contents
List of Tables 8
List of Figures 9
1 Preface 10Disclaimer . . . . . . . . . . 10Introduction . . . . . . . . . 10This document . . . . . . . . 11Please note . . . . . . . . . . 11Acknowledgements . . . . . 12Creative Commons . . . . . 12About the author . . . . . . 12Changes . . . . . . . . . . . 13
2 README FIRST 15Ametop . . . . . . . . . . . . 15Bicalutamide . . . . . . . . . 16Cyproterone Acetate . . . . 17Dutasteride . . . . . . . . . . 18Dydrogesterone . . . . . . . 18Emla Cream . . . . . . . . . 19Estradiol Valerate . . . . . . 19Finasteride . . . . . . . . . . 21Flutamide . . . . . . . . . . 21Goserelin . . . . . . . . . . . 22Leuprorelin Acetate . . . . . 23Minoxidil . . . . . . . . . . . 23Oestrogel . . . . . . . . . . . 23Progesterone . . . . . . . . . 24Sandrena . . . . . . . . . . . 25Testosterone . . . . . . . . . 26Triptorelin . . . . . . . . . . 26Vaniqa . . . . . . . . . . . . 28
3 Preamble 29What are hormones? . . . . 29Possible Health Risks . . . . 29Side effects . . . . . . . . . . 30Where do hormones come
from? . . . . . . . . . . 31
Long-term treatment . . . . 32What will hormones do to
me? . . . . . . . . . . . 32What changes will I see? . . 33Common therapies . . . . . 42Drugs used in Male to Fe-
male transitioning . . . 44Drugs used in Female to
Male transitioning . . . 44How oestrogen works . . . 44Hormone effects in
male→female . . . . . 47Hormone effects in
female→male . . . . . 54
4 Endocrinology 63An overview of the en-
docrine system . . . . . 63The major endocrine glands 65The Biochemistry of Sex
Hormones . . . . . . . 67
5 Human anatomy 71Male Genital Anatomy . . . 71Female Genital Anatomy . . 72
6 Hormones 76Estradiol Valerate . . . . . . 76Oestrogel . . . . . . . . . . . 88Sandrena . . . . . . . . . . . 93Testosterone . . . . . . . . . 98
7 DHT-blockers 109Dutasteride . . . . . . . . . . 109Finasteride . . . . . . . . . . 114
8 Anti-androgens 118Bicalutamide . . . . . . . . . 118Cyproterone Acetate . . . . 124Flutamide . . . . . . . . . . 132Goserelin . . . . . . . . . . . 138
2
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Contents
Leuprorelin Acetate . . . . . 149Triptorelin . . . . . . . . . . 160
9 Progestogens 172Dydrogesterone . . . . . . . 172Progesterone . . . . . . . . . 176
10 Other useful drugs 185Ametop . . . . . . . . . . . . 185Emla Cream . . . . . . . . . 187Minoxidil . . . . . . . . . . . 190Vaniqa . . . . . . . . . . . . 192
11 Deprecated Drugs 194Ethinylestradiol . . . . . . . 194Medroxyprogesterone
Acetate . . . . . . . . . 202Oestrogens, conjugated . . . 211Spironolactone . . . . . . . . 216
12 Potential problems 226Allergic reactions . . . . . . 226Breast Self Examination . . . 226Deep Vein Thrombosis . . . 229Osteoporosis . . . . . . . . . 233Prostate cancer . . . . . . . . 236Pulmonary Embolism . . . . 237Testicular Self Examination . 237Thrombophlebitis . . . . . . 240Urinary Tract Infections -
UTI’s . . . . . . . . . . 241
13 Blood tests and their results 245What To Expect With Blood
Tests . . . . . . . . . . . 245Blood testing . . . . . . . . . 246Blood groups . . . . . . . . . 251Reference ranges . . . . . . . 252Alkaline phosphate - ALP . 253Bilirubin . . . . . . . . . . . 255Blood Glucose . . . . . . . . 255Cholesterol . . . . . . . . . . 256Dehydroepiandrosterone
sulphate - DHEAS . . . 260Dihydrotestosterone - DHT 263Follicle stimulating hor-
mone - FSH . . . . . . . 264High-density lipoprotein -
HDL . . . . . . . . . . . 266
Low-density lipoprotein -LDL . . . . . . . . . . . 268
Liver function tests . . . . . 270Luteinizing hormone - LH . 272Oestrogen . . . . . . . . . . 273Prolactin - PRL . . . . . . . . 276Prothrombin - PT . . . . . . 277Sex hormone binding glob-
ulin - SHBG . . . . . . 278Testosterone . . . . . . . . . 279Thyroxine, free - T4 . . . . . 282Further blood tests . . . . . 282Blood, urea and nitrogen -
BUN . . . . . . . . . . . 283Full Blood Count - FBC . . . 284Erythrocyte sedimentation
rate - ESR . . . . . . . . 291International Normalised
Ratio - INR . . . . . . . 292Prostate specific antigen -
PSA . . . . . . . . . . . 293Thyroid function test - TFT . 296
14 Urine tests and their results 299How should I collect and
store a urine sample? . 299Urine and electrolytes . . . . 300Albumin . . . . . . . . . . . 307Urinary tract infections -
UTI’s . . . . . . . . . . 307
15 Sexually transmitted infec-tions - STI’s 308Chlamydia . . . . . . . . . . 309Genital herpes . . . . . . . . 313Genital warts . . . . . . . . . 319Gonorrhoea . . . . . . . . . 323Hepatitis . . . . . . . . . . . 328HIV . . . . . . . . . . . . . . 336Molluscum contagiosum . . 346Pubic lice . . . . . . . . . . . 353Scabies . . . . . . . . . . . . 356Shigella . . . . . . . . . . . . 358Syphilis . . . . . . . . . . . . 360Trichomoniasis . . . . . . . . 365How to avoid sexually
transmitted infections- STI’s? . . . . . . . . . 368
Condoms . . . . . . . . . . . 3703
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Contents
16 Other infections that canbe caused by an STI 385Bacterial vaginosis - BV . . . 385Proctitis . . . . . . . . . . . . 390Thrush . . . . . . . . . . . . 392Urethritis . . . . . . . . . . . 397Vaginal Thrush . . . . . . . 405Vaginitis . . . . . . . . . . . 409
17 Discussion 411Accessing your health records411Adrenal Fatigue . . . . . . . 415Adrenal Insufficiency . . . . 417Bio-equivalence . . . . . . . 418Blood levels . . . . . . . . . 423Blood tests . . . . . . . . . . 426Body fat . . . . . . . . . . . . 435Breast Development . . . . . 436Breast disorders . . . . . . . 439Breast Implants . . . . . . . 455Breast Screening . . . . . . . 456Coming out . . . . . . . . . 461Consent and Informed Con-
sent . . . . . . . . . . . 462Contact lenses and drug
treatment . . . . . . . . 463Cranberry Juice . . . . . . . 464Cycling Hormones? . . . . . 464Depression . . . . . . . . . . 465Drug names . . . . . . . . . 466E-numbers . . . . . . . . . . 466Ethinylestradiol . . . . . . . 467Exercise . . . . . . . . . . . . 468Expiry dates . . . . . . . . . 468From Amazon . . . . . . . . 469Further discussion of Vita-
min D . . . . . . . . . . 469Gender . . . . . . . . . . . . 472Getting a urine sample . . . 474Getting older . . . . . . . . . 475Grapefruit Juice . . . . . . . 476Heamatological Reference
Values . . . . . . . . . . 479Hormones and dementia . . 481Hospital Records . . . . . . 481How to Take Your Tablets. . 482Renewed Confidence in HRT 483
Implants, Testosterone andEstradiol . . . . . . . . 483
Importation of prescribedmedication . . . . . . . 484
Infection? . . . . . . . . . . . 485Injections . . . . . . . . . . . 486Kegel exercises . . . . . . . . 494Lactation . . . . . . . . . . . 497Leg Cramps . . . . . . . . . 497Liver damage . . . . . . . . 497Male pattern baldness . . . 500Male pregnancy . . . . . . . 500Measuring Your Transition . 501Medroxyprogesterone Ac-
etate and osteoporosis 503Memory enhancing effects
of oestrogen . . . . . . 503Menopause . . . . . . . . . . 504Menopausal symptoms . . . 509Methods of Delivery or Ad-
ministration . . . . . . 511Mood swings and depression 511Oestrogen and Alzheimer’s
Disease . . . . . . . . . 513Online Pharmacies . . . . . 514Pelvic examination . . . . . 515Permanent sterility and sex-
ual dysfunction . . . . 516Pharmacodynamics . . . . . 517Pharmacokinetics . . . . . . 517Photosensitivity of the skin . 517PMS - Pre-menstrual syn-
drome . . . . . . . . . . 518Premarin . . . . . . . . . . . 519Prescriptions . . . . . . . . . 519Prevalence of Transsexual-
ism in the UK . . . . . 521Prostate cancer . . . . . . . . 522Regimes . . . . . . . . . . . . 523Safety of HRT . . . . . . . . 530Sexual Health . . . . . . . . 532Shared Care . . . . . . . . . 534Shrinking Testicles! . . . . . 534Sitting down? . . . . . . . . 535Skin care . . . . . . . . . . . 535Sleep . . . . . . . . . . . . . 542Smoking and taking hor-
mones . . . . . . . . . . 5494
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Contents
Sperm banking . . . . . . . . 549Stopping hormones prior to
surgery . . . . . . . . . 550Stress management . . . . . 551Stretch marks . . . . . . . . 566Sunshine protection . . . . . 567Supplies . . . . . . . . . . . 568Testosterone . . . . . . . . . 568Testosterone replacement
therapy, menopauseand libido: the facts . . 569
The real side effects oftestosterone replace-ment therapy for men . 572
The risks of breast cancer . . 575The risks of smoking . . . . 576The usage of Aspirin . . . . 577Thrush . . . . . . . . . . . . 578Transdermal medication. . . 578Transgender Definitions . . 580Transphobia . . . . . . . . . 584Treatment aims . . . . . . . 588Understanding "Enteric
Coating" . . . . . . . . 589Units of measurement . . . 590Urinary Tract Infections . . . 590Vaginal Itching and Discharge591Vitality . . . . . . . . . . . . 592Vitamins . . . . . . . . . . . 593Water . . . . . . . . . . . . . 600What is a hormone? . . . . . 601What is a ’vitamin’? . . . . . 601Why we forget and how to
remember . . . . . . . . 602
Zoff . . . . . . . . . . . . . . 603
18 Other resources 605Books . . . . . . . . . . . . . 605Email . . . . . . . . . . . . . 606Films . . . . . . . . . . . . . 608Some web sites . . . . . . . . 609Surgeons . . . . . . . . . . . 610
19 Appendix 1 611American vs British Drug
names . . . . . . . . . . 611American vs British Lab
values . . . . . . . . . . 612Conversion table . . . . . . . 612Metric weights and Liquid
measures . . . . . . . . 613How to evaluate health in-
formation on the inter-net . . . . . . . . . . . . 613
Glossary 618
Acronyms 628
Bibliography 631
Index of Hormones 677
Index of Hormones Side-Effects681
Index of Interactions 691
Index of STI’s 722
General Index 726
5
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
List of Tables
1.1 Previous versions of this document . . . . . . . . . . . . . . . . 11
3.1 Taking anti-androgens alone (without oestrogen) which mayvary from person to person . . . . . . . . . . . . . . . . . . . . 33
3.2 Typical changes from using oestrogen (which may vary fromperson to person) . . . . . . . . . . . . . . . . . . . . . . . . . . 34
3.3 Things that might, or might not, change . . . . . . . . . . . . . 343.4 Expected effects of feminizing hormone therapies . . . . . . . 363.5 Risks associated with feminizing hormone therapies . . . . . . 363.6 Typical changes from using testosterone (which may vary
from person to person) . . . . . . . . . . . . . . . . . . . . . . . 373.7 Effects and expected time course of masculinizing hormones . 383.8 Things that will, and won’t, change . . . . . . . . . . . . . . . . 383.9 Common masculinizing therapies . . . . . . . . . . . . . . . . . 393.10 Popular androgens . . . . . . . . . . . . . . . . . . . . . . . . . 393.11 Anti-hormones . . . . . . . . . . . . . . . . . . . . . . . . . . . 393.12 The expected effects of masculinizing hormone therapy . . . . 413.13 The risks associated with masculinizing hormone therapy . . 413.15 Popular Oestrogens . . . . . . . . . . . . . . . . . . . . . . . . . 423.17 Popular anti-androgens . . . . . . . . . . . . . . . . . . . . . . 433.19 Popular progesteronic drugs . . . . . . . . . . . . . . . . . . . 433.20 Popular GnRH agonists . . . . . . . . . . . . . . . . . . . . . . 443.21 The effects of female hormone treatment begun after male
puberty has completed (i.e. after about age 17) . . . . . . . . . 62
4.1 The major hormones synthesized and secreted by thepituitary gland . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
6.1 Normal range & dose of Estradiol, for oral tablets only . . . . 77
8.1 Dosages of Triptorelin . . . . . . . . . . . . . . . . . . . . . . . 161
13.1 Reference ranges for Alkaline Phosphate - ALP . . . . . . . . . 25313.2 Reference ranges for Bilirubin . . . . . . . . . . . . . . . . . . . 25513.3 Glucose reference ranges . . . . . . . . . . . . . . . . . . . . . . 25613.4 Reference ranges for cholesterol . . . . . . . . . . . . . . . . . . 25713.5 Reference ranges of dehydroepiandrosterone sulphate - DHEAS26113.6 Reference ranges for dihydrotestosterone - DHT . . . . . . . . 26413.7 Reference ranges of follicle stimulating hormone . . . . . . . . 26613.8 Reference ranges for high-density lipoprotein . . . . . . . . . . 26613.9 Reference ranges for low-density lipoprotein . . . . . . . . . . 269
6
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
List of Tables
13.10Reference ranges of luteinizing hormone - LH . . . . . . . . . . 27313.11Reference ranges of estradiol . . . . . . . . . . . . . . . . . . . . 27413.12 Reference ranges of prolactin - PRL . . . . . . . . . . . . . . . 27613.13Reference ranges of SHBG . . . . . . . . . . . . . . . . . . . . . 27813.14Reference ranges of testosterone - T . . . . . . . . . . . . . . . . 28013.15Reference ranges of thyroxine, free - T4 . . . . . . . . . . . . . . 28213.16Normal Range of ESR . . . . . . . . . . . . . . . . . . . . . . . . 29213.17A summary of test results and their meaning . . . . . . . . . . 297
17.1 Bio-equivalent doses of Oestrogen . . . . . . . . . . . . . . . . 41917.2 Bio-equivalent doses of Oestrogen used in menopause
treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42017.3 Hormone Replacement Therapies . . . . . . . . . . . . . . . . . 42117.4 Oral oestrogens vs transdermal oestrogens - 1 . . . . . . . . . . 42217.5 Oral And Transdermal Estrogen Dose Equivalents - 2 . . . . . 42317.6 Reference ranges for various blood tests . . . . . . . . . . . . . 42417.7 Estradiol reference ranges of adults . . . . . . . . . . . . . . . . 42417.8 Reference values for hormone therapy of transsexuals . . . . . 42517.9 Normal reference values for adults . . . . . . . . . . . . . . . . 42617.10Adult normal ranges of the full blood count . . . . . . . . . . . 42817.11Reference Values for Commonly Ordered Tests . . . . . . . . . 43517.12Common breast symptoms . . . . . . . . . . . . . . . . . . . . . 44117.13Some causes of nipple discharge . . . . . . . . . . . . . . . . . 45017.14The e-numbers used in some tablets . . . . . . . . . . . . . . . 46717.15The primary factors that can potentially determine an
individual’s vitamin D blood level from A to Z . . . . . . . . . 47117.16Pharmacological effects of grapefruit juice with medications . 47917.17Heamatological Reference Values . . . . . . . . . . . . . . . . . 48017.18The difference between fungal and bacterial infections . . . . . 48517.19The rise and fall of women’s sex hormones . . . . . . . . . . . 50517.20Additional therapies for transwoman in the UK . . . . . . . . . 52517.21Hormone therapy for UK transwoman . . . . . . . . . . . . . . 52517.22Regime commonly used by transwomen in British Columbia,
Canada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52617.23Transwomen hormone regime from the Amsterdam Gender
Clinic, Holland . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52617.24Some self-medding regimes . . . . . . . . . . . . . . . . . . . . 52817.25Hormone regime commonly used by transmen in British
Columbia, Canada . . . . . . . . . . . . . . . . . . . . . . . . . . 52917.26Hormone therapy for transmen in the UK . . . . . . . . . . . . 52917.27Transmen hormone regime from the Amsterdam Gender
Clinic, Holland . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52917.28Equivalents of 1 IU . . . . . . . . . . . . . . . . . . . . . . . . . 59017.29Recommended Daily Intakes for Vitamins . . . . . . . . . . . . 59417.30Recommended Dietary Allowance (RDA) in micrograms
(mcg) of Retinol Activity Equivalents (RAE) . . . . . . . . . . . 59417.31Recommended Dietary Allowance (RDA) of Vitamin C . . . . 595
7
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
List of Tables
17.32Recommended Dietary Allowance (RDA) or Adequate Intake(AI) of Vitamin D . . . . . . . . . . . . . . . . . . . . . . . . . . 595
17.33Recommended Dietary Allowance (RDA) in milligrams (mg)and International Units (IU) of Vitamin E . . . . . . . . . . . . 596
17.34Recommended Dietary Allowance (RDA) or Adequate Intake(AI) of Vitamin K . . . . . . . . . . . . . . . . . . . . . . . . . . 596
17.35Recommended Dietary Allowance (RDA) of Vitamin B1 . . . . 59717.36Recommended Dietary Allowance (RDA) or Adequate Intake
(AI) of Vitamin B3 . . . . . . . . . . . . . . . . . . . . . . . . . . 59817.37Recommended Dietary Allowance (RDA) of Vitamin B5 . . . . 59817.38Recommended Dietary Allowance (RDA) of Vitamin H . . . . 59917.39Recommended Dietary Allowance (RDA) of Vitamin B6 . . . . 59917.40Recommended Dietary Allowance (RDA) in micrograms
(mcg) of Vitamin B12 . . . . . . . . . . . . . . . . . . . . . . . . 59917.41Recommended Dietary Allowance (RDA) of Vitamin B9 . . . . 600
19.1 American vs British Drug names . . . . . . . . . . . . . . . . . 61219.2 American vs British Lab values . . . . . . . . . . . . . . . . . . 61219.4 Conversion factors between the US and European SI units . . 61319.5 Metric weights and Liquid measures . . . . . . . . . . . . . . . 613
8
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
List of Figures
3.1 Positive and negative effects of oestrogen . . . . . . . . . . . . 47
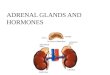
4.1 The human body, showing all the endocrine sites . . . . . . . . 634.2 The cholesterol degradation . . . . . . . . . . . . . . . . . . . . 684.3 The overall process of hormonal biosynthesis . . . . . . . . . . 70
12.1 Feel your breasts whilst lying down . . . . . . . . . . . . . . . 22712.2 Lines examination . . . . . . . . . . . . . . . . . . . . . . . . . . 22712.3 Circle examination . . . . . . . . . . . . . . . . . . . . . . . . . 22812.4 Wedges examination . . . . . . . . . . . . . . . . . . . . . . . . 22812.5 Examine your breasts while standing . . . . . . . . . . . . . . . 22812.6 Examine your breasts whilst turning . . . . . . . . . . . . . . . 22812.7 Look for dimples or bulges . . . . . . . . . . . . . . . . . . . . . 22812.8 Flex your chest muscles . . . . . . . . . . . . . . . . . . . . . . . 22812.9 How to do testicular self examination . . . . . . . . . . . . . . 238
17.1 Anatomy of the breast . . . . . . . . . . . . . . . . . . . . . . . 43617.2 The growing breast . . . . . . . . . . . . . . . . . . . . . . . . . 43717.3 Various positions for breast examination . . . . . . . . . . . . . 44217.4 17β-Estradiol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46917.5 X marks the injection site . . . . . . . . . . . . . . . . . . . . . . 49017.6 This shows how to insert the needle . . . . . . . . . . . . . . . 49117.7 This shows how the "Z-tracking" technique works . . . . . . . 49117.8 A MRI scan of an IM injection . . . . . . . . . . . . . . . . . . . 49217.9 This shows the site of the "Double Cross" . . . . . . . . . . . . 49217.10The underlying anatomy of the "Double Cross" . . . . . . . . . 49317.11Female pelvic floor muscles . . . . . . . . . . . . . . . . . . . . 494
9
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Chapter 1Preface
Disclaimer
The author of this book has used her best efforts in preparing this bookand the information contained in it. This book is distributed as is, withoutwarranty of any kind, either express or implied, respecting the contents ofthis ebook, including but not limited to implied warranties for the ebook’squality, performance, or fitness for any purpose. The author and any dealersand distributors shall not be liable to the purchaser or any other person orentity with respect to liability, loss, or damages caused or alleged to havebeen caused directly or indirectly by this ebook. This document is providedas is.
The author takes no responsibilities for any problems, damages, orloss of sanity resulting from improper usage of hormones. If youare in any doubt, do NOT take the tablets, or whatever but post aquestion to your relevant newsgroup or refer to a competent medicaldoctor or endocrinologist. Messing about with something you do notunderstand may seriously damage your health. YOU HAVE BEENWARNED.
Introduction
Very little information, if any, is given to us when we are prescribed thesedrugs, or when they are dispensed at the pharmacy. We are not told thebenefits that we should expect from these drugs or of what to be aware ofwith regard to any side effects. I am concerned about the scarcity of reliableinformation for transsexuals in any public forum, or in any easily read,
10
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
This document
understandable format. This then, is the primary reason for the existenceof this ebook - to hopefully help to remedy that situation. Also, thesemedications are licensed for use in specific circumstances, which generallydo not include usage on or for transsexuals.
All of the drugs mentioned are ones that I have heard about. I make norecommendations as to which is best, it is up to the individual prescriberand their knowledge of the drugs action and also their knowledge oftheir patient. It is inadvisable also, to take any medication that has beenprescribed for someone else.
This document
This document has a long history, having had several previous incarnations,first in December 1999, then in December 2001, and next in August 2005,and then a long gap until March 2015. On each occasion it seemed to bewell received, but it was just for transsexuals within the United Kingdomutilising the National Health Service and the private medical sector. Sincethen things have moved on and more information is available on theinternet, so its time for a revision and update. As I now have moreinformation available, I’ve decided to use information which is applicable tofolk all over the world. And I’ve found that as people seem to be confusedover the title, its now just called "Hormones 2016".
This is written to be read online, or offline with your favourite PDF reader.If you were to print it out you would lose access to all the cross-references,and other stuff too.
Previous versions
Title Version Whenpublished
UK Hormone FAQ v3.6 December 1999UK Hormones FAQ v4.0 December 2001UK Hormones 2005 August 2005Universal Hormones2015
v1.0 March 2015
Table 1.1 – Previous versions of this document
11
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Please note
Please note
In some places you may see on a word or two, these show that they are acommon side-effect.
You may also see this which shows a moderately common side-effect.
This a warning that something is amiss and needs attending to.
Shows a dangerous side-effect which should be notified extremely soon, ifnot now, to your local General Practitioner, a community-based doctor (GP),Doctor, Endocrinologist, or Hospital.
Shows an overdose. Speak to your local GP, Doctor, Endocrinologist, orHospital As Soon As Possible, if not sooner!
Possible other side-effects are shown like this one.
I have placed various sections in what I consider to be a logical order, butalso in alphabetical order within the chapters.
Acknowledgements
Thanks to all the people, too many to list individually, who contributed tomy research for this book. Any errors or omissions are nobodies fault exceptmy own, but I would also refer you back to the disclaimer.
Creative Commons
This work is licensed under a Creative Commons “Attribution-ShareAlike 4.0 International” license.
You are free to Share (to copy, distribute and transmit the work) and toRemix (to adapt the work) provided you follow the Share Alike guidelinesof the licence.
The only restriction is -
Attribution You must attribute the work in the manner specified by theauthor or licensor (but not in any way that suggests that they endorse youor your use of the work).
(For the full licence text, please visit:http://creativecommons.org/licenses/by-sa/4.0/legalcode)
12
Version 2016.3576– – Document LATEXed – 1st May 2016
https://creativecommons.org/licenses/by-sa/4.0/deed.enhttps://creativecommons.org/licenses/by-sa/4.0/deed.enhttp://creativecommons.org/licenses/by-sa/4.0/legalcode
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
About the author
About the author
My name is Sharon Kimble, and I am a former Registered General Nurseand a State Enrolled Nurse, living and working in the United Kingdom.
I have approached this subject with the idea and question of - “Whatinformation would I want to know about this drug if I were going to starttaking it?”
Some people have wondered why I have used such old documents andreferences? My reasoning is that yes, some are old, like Richard Dollwith his ground-breaking research into smoking sixty years ago. But, justbecause they are old does not diminish from the strength of their message,which is still vibrant and worth listening to. So the first time that someonesays something that is important and relevant, and it is published in someformat, is the time that I record it.
Sharon Kimblek My email address1st May 2016
Changes
These are the changes between version 1.0, and this version 2.0.
Removed
• Chapter 5 - Herbal Hormones - now superseded by its own document.• Individual prices in the individual drugs, as the prices are out of date
by the time that its published.• Blood donating,• the legal situation in the UK.
Added
• Sleep at page 542,• Stretch marks at page 566,• Infection? at page 485,• Sitting down? at page 535,• Pelvic examination at page 515,• Sexually transmitted infections - STI’s at page 308,• Getting a urine sample at page 474,• Getting older at page 475,• Grapefruit Juice at page 476,• Depression at page 465,
13
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Changes
• Free prescriptions at page 520,• Blood tests and their results at page 245,• Urine tests and their results at page 299,• Other infections that can be caused by an STI at page 385,• Skin care at page 535,• Deprecated Drugs at page 194,• README FIRST at page 15,• Stress management at page 551,• Renewed Confidence in HRT at page 483,• Accessing your health records at page 411,• Treatment aims at page 588,• Breast Screening at page 456,• Expiry dates at page 468,• Removed all coloured boxes and replaced them with coloured text,
hopefully it will be easier to read?
14
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Chapter 2README FIRST
This chapter gives a quick introduction to the most important parts of"Hormones". The rest of the book is basically a verbose version of thischapter. You should start by reading this chapter, as it summarises all thehormones, giving their name, uses, and common side-effects. For moredetailed information you can read their main entries. It’s arranged inalphabetical order to make it easier to find things.
If you want to know more about endocrinology, you can read Preambleand also Endocrinology. Or you can jump right in and read your favouritehormone in this chapter and then click on the hormones name at the end ofits section to jump straight to its main entry.
If you want to know more about the different colour of the side-effects, thenjump to Please note.
Whatever, I hope you read it and enjoy what you’re learning. If you haveany questions you can email me on my email address at the end of Chapter1, and I’ll endeavour to help.
Ametop
Used as a topical anaesthetic for skin anaesthesia.
Also known as
Tetracaine, Amethocaine.
15
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Bicalutamide
Common side-effects
Skin
• Erythema, (skyscape, 2014).
Further information
This can be found at Ametop.
Bicalutamide
What is it?
Anti-androgen.
Also known as
Casodex, Bicalutamid (German), Bicalutamida (Spanish)
Common side-effects
General
• Back pain,• pelvic pain,• general body pain,
• headache,• weakness,• asthenia.
Gastrointestinal
• constipation,• diarrhoea,
• flatulence,• nausea, (Abramovitz, 2016).
Cardiovascular
• hot flashes.
Genitourinary
16
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Cyproterone Acetate
• nocturia, • impotence (Abramovitz, 2016).
Metabolic
• Peripheral oedema,• hyperglycaemia, and
• weight loss, (Abramovitz,2016).
Nervous system
• insomnia, • dizziness, (Abramovitz, 2016).
Dermatological
• sweating, (Abramovitz, 2016).
Other
• breast tenderness,• breast swelling,
• hot flashes, (unknown, 2014a).
• breast pain,• gynaecomastia,• generalized pain,• hot flashes,
• pelvic pain,• libido decrease,• impotence, (unknown, 2014a).
Further information
This can be found at Bicalutamide.
Cyproterone Acetate
What is it?
Cyproterone acetate, sometimes abbreviated as CPA, and sold underbrand names such as Androcur and Cyprostat, is a synthetic steroidalantiandrogen drug with additional progestogen and antigonadotropicproperties (Neumann and Topert, 1986).
17
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Dutasteride
Also known as
Androcur, Cyprostat, Dianette, Siterone in USA, Diane-35 in Canada, andDixi-35 in Chile.
Common side-effects
Respiratory
• Breathlessness. (BNF, 2016a), • shortness of breath, (emc,2016).
Gastrointestinal
• Weight changes, (BNF, 2016a).
Genitourinary
• Breast swelling,• decreased sex drive,• impotence,
• reduced sperm count,• reduced volume of ejaculate,
(emc, 2016)
Other
• Tiredness,• lassitude,• Hot flushes,
• sweating,• depressed mood,• restlessness, (emc, 2016).
Further information
This can be found at Cyproterone Acetate.
Dutasteride
What is it?
dihydrotestosterone (DHT)-blocker.
Also known as
Avodart, Dutasterid (German), Dutasterida (Spanish).18
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Dydrogesterone
Common side-effects
• Gynaecomastia, (Abramovitz, 2016).
Further information
This can be found at Dutasteride.
Dydrogesterone
A synthetic progestational hormone with no androgenic or oestrogenicproperties (drugbank, 2014b).
Also known as
Duphaston, Duphaston Hormone Replacement Therapy (HRT).
Common side-effects
Central Nervous System
• Headache,• dizziness,• insomnia,
• drowsiness,• depression, (BNF, 2016a).
Gastrointestinal
• Weight gain, • nausea, (BNF, 2016a).
Skin
• Skin reactions (includingurticaria, pruritis, rash, andacne),
• urticaria,• hirsutism, and• alopecia, (BNF, 2016a).
Metabolism
• Bloating,• fluid retention,
• weight gain,• nausea, (BNF, 2016a).
19
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Emla Cream
Genitourinary
• Breast tenderness, (BNF, 2016a).
Further information
This can be found at Dydrogesterone.
Emla Cream
EMLA stands for ’eutectic mixture of local anaesthetic’.
Common side-effects
None known.
Further information
This can be found at Emla Cream.
Estradiol Valerate
Estradiol Valerate is a naturally occurring oestrogen given in the formof Estradiol Valerate or one of its semisynthetic esters as oestrogenreplacement therapy in menopausal women (TGC, 2015a).
Also known as
Climaval, Estraderm MX, Estraderm TTS, Estradiol implant, Evorel,Progynova, Progynova TS, Zumenon, Estradiol (USA), Estradiol (German),Estradiol (French), Estradiol (Spanish).
Common side-effects
Central Nervous System
• headache, (Abramovitz, 2016).
20
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Estradiol Valerate
Cardiovascular
• oedema, (Abramovitz, 2016).
Eyes
• Myopia/astigmatism worsens, • contact lens intolerance,(Abramovitz, 2016).
Gastrointestinal
• Nausea,• vomiting,
• abdominal cramps,• bloating, (Abramovitz, 2016).
Genito-urinary
• Testicular atrophy, • erectile dysfunction, (Abramovitz,2016).
Metabolic
• Weight changes, (Abramovitz, 2016).
Skin
• Melasma, • hair loss, (Abramovitz, 2016).
Other
• gynaecomastia,• hot flashes,• breast tenderness,
• breast enlargement, (Abramovitz,2016).
Further information
This can be found at Estradiol Valerate.
21
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Finasteride
Finasteride
What is it?
DHT-blocker
Also known as
Proscar, Propecia, Finasterid (German), Finastéride (French), Finasterida(Spanish).
Common side-effects
Central Nervous System
• Dizziness.
Cardiovascular
• orthostatic hypotension.
Other
• Gynaecomastia, (Abramovitz, 2016).
Further information
This can be found at Finasteride.
Flutamide
What is it?
Anti-androgen.
Also known as
Flutamid (German), Flutamida (Spanish).
22
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Goserelin
Common side-effects
Gastrointestinal
• Diarrhoea,• nausea,
• vomiting, (Abramovitz, 2016)
Genitourinary
• Erectile dysfunction, (Abramovitz, 2016).
Further information
This can be found at Flutamide.
Goserelin
Used for the treatment of advanced prostate cancer, endometriosis,advanced breast cancer, endometrial thinning (Abramovitz, 2016).
Also known as
Zoladex, Zoladex LA, Goséréline (French), Goserelina (Spanish).
Common side-effects
Central Nervous System
• headache, (Abramovitz, 2016). • Hot flushes (drugs.com,2014c).
Cardiovascular
• hot flashes, (Abramovitz, 2016)
Genitourinary
• Sexual dysfunction,• vaginitis, (Abramovitz, 2016).• amenorrhoea,
• PSA increased,• decreased libido, (rxisk,
2016d).23
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Leuprorelin Acetate
Other
• Changes in breast size,• changes in libido,
• breast swelling, (Abramovitz,2016).
Further information
This can be found at Goserelin.
Leuprorelin Acetate
Anti-androgen
Also known as
Prostap SR, and Prostap 3.
Common side-effects
Central Nervous system
• Headache, (Macmillan, 2014).
Genitourinary
• Hot flushes,• impotence,• ↓ libido,
• gynaecomastia, (Macmillan,2014).
Further information
This can be found at Leuprorelin Acetate
Minoxidil
Applied to the scalp in the treatment of male-pattern baldness.
24
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Oestrogel
Also known as
Regaine, Rogaine.
Common side-effects
None known.
Further information
This can be found at Minoxidil.
Oestrogel
Applied to the skin as an alternative route for administering oestrogen.
Also known as
Estrodose, divigel, elestrin, EstroGel.
Common side-effects
Skin
• Irritation,• reddening of the skin,
• mild and transient erythemaat the site of application (emc,2016).
Further information
This can be found at Oestrogel.
Progesterone
A pharmaceutical-grade progesterone.
25
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Sandrena
Also known as
Cyclogest, Gestone, Utrogestan, Prometrium (USA and Canada), Crinone.
Common side-effects
Central Nervous System
• headache,• fever, (WebMD, 2014e)• chills,
• cold or flu-like symptoms,(drugs.com, 2014c).
• dizziness, (Medscape, 2014).
Gastrointestinal
• cough, (drugs.com, 2014c).
Genitourinary
• Breast tenderness,• breast discomfort or• enlargement, (WebMD, 2014e).
• problems with urination,(drugs.com, 2014c).
• breast pain, (Medscape, 2014).
Further information
This can be found at Progesterone.
Sandrena
Hormone replacement therapy for oestrogen deficiency symptoms inpostmenopausal women.
Common side-effects
Central Nervous System
• headache, (Abramovitz, 2016).
Cardiovascular
26
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Testosterone
• oedema, (Abramovitz, 2016). • hot flushes, (rxisk, 2016e).
Eyes
• myopia/astigmatism worsens, • contact lens intolerance,(Abramovitz, 2016).
Gastrointestinal
• Nausea,• vomiting,
• abdominal cramps,• bloating, (Abramovitz, 2016).
Genito-urinary
• Testicular atrophy, • erectile dysfunction, (Abramovitz,2016).
Metabolic
• Weight changes, (Abramovitz, 2016)
Skin
• Melasma, • hair loss, (Abramovitz, 2016)
Other
• Gynaecomastia,• breast tenderness,
• breast enlargement, (Abramovitz,2016)
Further information
This can be found at Sandrena.
Testosterone
Administration is by deep muscular injection, in the form of a gel, or as apatch.
27
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Triptorelin
Also known as
Sustanon 100, Sustanon 250, Testogel, Andropatch, Restandol, Testosteron(German), Testostérone (French), Testosterona (Spanish).
Common side-effects
Gastrointestinal
• gum or mouth irritation,• gum pain,• gum tenderness, or
• gum oedema, (Abramovitz,2016).
Haematologic
• haematocrit 1 increased, • polycythaemia 2.
Genitourinary
• decreased libido, • PSA increased, (rxisk, 2016f).
Other
• gynaecomastia, (Abramovitz, 2016).
Further information
This can be found at Testosterone.
Triptorelin
Triptorelin is a synthetic analogue of gonadotropin-releasing hormone(gonadotropin-releasing hormone (GnRH)) agonist. It works by decreasingthe production of certain hormones, which reduces testosterone levels in thebody (drugs.com, 2016).
1a blood test that measures the percentage of the volume of whole blood that is madeup of red blood cells
2having a high concentration of red blood cells in your blood
28
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Triptorelin
Common side-effects
Gastrointestinal disorders
• Nausea (emc, 2009)
General disorders
• asthenia,• hyperhidrosis,• fatigue,• injection site erythema,
• injection site inflammation,• injection site pain,• injection site reaction,• oedema (emc, 2009).
Musculoskeletal disorders
• back pain,• musculoskeletal pain,
• pain in extremity (emc, 2009).
Nervous system
• paraesthesia in lower limbs,• dizziness,
• headache (emc, 2009).
Psychiatric disorders
• depression, • mood changes (emc, 2009).
Reproductive system
• erectile dysfunction, • loss of libido (emc, 2009).
Skin disorders
• hyperhidrosis (emc, 2009).
Vascular disorders
• hot flush (emc, 2009).
Further Information
This can be found at Triptorelin.
29
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Vaniqa
Vaniqa
Eflornithine, an antiprotozoal drug, inhibits the enzyme ornithine decar-boxylase in hair follicles and topical application can reduce the growth ofunwanted facial hair (BNF, 2016a).
Common side-effects
None known.
Further information
This can be found at Vaniqa.
30
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Chapter 3Preamble
What are hormones?
Hormones are the body’s way of carrying messages from organs in aperson’s body through the bloodstream to its cells where homeostasis isachieved. Some of the glands, from about a dozen, in the endocrine systemresponsible for secreting hormones are the pancreas, thyroid, adrenals, andthe pituitary. These glands play a large part in keeping a natural balance inthe body.
Possible Health Risks
Some health risks are involved and should be fully researched andconsidered before beginning HRT. Pre-existing health problems could alsodisqualify a person for HRT.
One of the most troublesome aspects of HRT is that such little researchhas been performed to find out what health risks are involved. Therecould possibly be serious long-term health risks involved that still havenot been uncovered. One serious risk that is definitely correlated withHRT is thromboembolic disease, which is a disease that causes blood clots.The risk for this can be decreased by regular exercise. Transwomen3 canexperience extreme mood swings on oestrogen and severe depression andloss of energy can result. The mortality rate in transwomen is 6 times higherthan the general population. This is primarily due to suicide and unknowncauses. Oestrogen can also cause transwomen to be a higher risk for benignpituitary tumors, gallbladder disease, and hypertension.
3is someone who was labelled male at birth but has a female gender identity, andtherefore transitions to live completely and permanently as a woman (LGBT, 2014b)
31
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Side effects
Transmen4 can develop serious acne problems, and weight gain of greaterthan 10% is fairly common. Transmen face higher risks of breast cancer,diabetes, high cholesterol, hypertension, heart attacks, and liver disease.Smoking tobacco makes these risks even greater, so a person pursuing HRTshould be or become a non-smoker.
The most obvious risk with HRT is that once changes begin to occur, manyof the changes are irreversible. Sterility results in both transwomen andtransmen after prolonged treatment. If an transwoman thinks she wouldeventually like to father a child, she should seriously consider storing spermin a sperm bank prior to starting HRT. (Also see Sperm banking) If antransman would like to have a child, it is sometimes possible to becomepregnant after being on testosterone for a period of time, though pregnancywould require cessation of hormone treatment. It is possible to freeze eggs,but the technology has not sufficiently developed yet for this to be a long-term feasible solution for most people (University, 2014).
Side effects
Most drugs have some side-effects, and it is essential that the side-effectsdo not outweigh the benefits to you, the user. Because, if they do, thencompliance with your regime will be scanty and full benefit will not beobtained. However, as with all medications, some people react differentlyto others. It is important for you to understand that there are side-effects tohormones, some side-effects may be acceptable, after all, you have comethis far and a few slight adverse reactions are not going to slow youdown now! These are the details you need to know however, to makean informed choice and to gain the maximum benefit from your hormoneregime with the safest possible level of self-care. Side-effects are potential,NOT inevitable (unknown, 2005).
Taking Progynova as an example; some people may experience problemswith their "cardiovascular" system (heart and circulation). There may besome evidence of fluid build-up in the body and blood clotting, oedemaor thromboembolism5 - the latter can be quite a serious side-effect so youneed to understand the symptoms of this. (See Deep Vein Thrombosisfor more information). Taking oral medication also carries a slight risk ofliver problems, so watch out for symptoms such as jaundice. You may alsoexperience nausea and vomiting (some women report that this is only inthe early stages), as well as abdominal cramps and bloating. A commonside effect is weight gain, generally through fluid or sodium retentionin the tissues. So attention to diet becomes even more important if you
4is someone who was labelled female at birth but has a male gender identity, andtherefore transitions to live completely and permanently as a man (LGBT, 2014b)
5Blockage of a blood vessel caused by a blood clot carried by the bloodstream from itspoint of origin
32
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Side effects
want to keep your weight down! Your breasts may become tender andenlarge slightly, called gynaecomastia, (so that’s the good news!). Somepeople report headaches, and changes in their vision. If you’re short-sighted it may worsen, and if you use contact lenses you may find themmore uncomfortable. Remember, some side effects are temporary, butsome are a continuing characteristic of the medication. Your GP6 and/orendocrinologist will be able to advise you as to the most effective regimefor you and will monitor your reactions to the hormones. Your ownobservations of the side effects are also very important so that you can takean active part in the medication that assists your transition. It will helpif you keep a "hormone diary" where you record how you feel and whatchanges you see.
This is a considerably simplified overview, but I have tried to list theside effects in terms of increasing risk/discomfort to you, but people’sexperiences do differ.
You may feel more prepared for side effects and symptoms if you knowabout them in advance, which is one of the reasons for writing thisdocument. Discuss the possible side effects of a drug with your doctorbefore starting treatment. Once you start treatment, make sure you talkto your doctor about side effects or symptoms you are experiencing. It’shelpful to take notes so you can describe them accurately to your doctor.Side effects often improve over time. Knowing that can make it easier tostick with a drug until you see whether the side effects really do improve.
Remember that many things could be causing the problem you are having.Get a full diagnosis from your doctor. Yes, it could be a drug side effect- but maybe it’s a problem with what you are eating, or an infection or aresult of Getting older. There are options for dealing with symptoms andside effects.
• If the problem isn’t too serious, wait and see if it improves on its own.• If it’s clear which drug is causing the side effect, your doctor may
decide to switch you to another drug that doesn’t cause this side effect.• Perhaps it is not a drug that is causing the problem. Maybe it is
something else that is causing it. In this case, your doctor will tryto diagnose and treat this problem.
• You and your doctor may be able to find some way to deal with theproblem, so you can live with it.
6General Practitioner, a community-based doctor
33
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Where do hormones come from?
Where do hormones come from?
In both sexes, the adrenal cortex secretes significant amounts of bothoestrogens (female hormones) and androgens7. In the female, the ovariesproduce oestrogens and progesterone; oestrogen from the graafian folliclesand progesterone from a temporary structure known as the corpus luteum.In the male, testosterone is secreted by the testes (TGC, 2015a).
Long-term treatment
Any long-term treatment should only be prescribed on the basis of"informed consent", see also Consent and Informed Consent hence anotherreason for this ebook. You should be aware that you will continue to takeone form or other of hormones for the rest of your natural life.
Research has found that compliance for drug regimes can be increased bykeeping the regime simple (sounds obvious, doesn’t it), which in most casesmeans you take your medication only once or twice a day (Lynn, 1995). Thismeans that you’re less likely to forget to take a dose, and less likely to getmuddled and to take too much dosage.
What will hormones do to me?
The following physiological effects are normally observed -
1 They are not a magic pill. You won’t "become a woman" taking them.2 Hormonal-induced changes are generally quite subtle.3 Do not depend on them alone to make you passable, because they will
not.4 They will have an effect on body hair eventually (especially androgen
blockers, which, strictly speaking, are not hormones but rather"hormone blockers").
5 Androgen blockers can help to reduce the doses of hormones needed,but only if taken concurrently.
6 Androgen blockers may have a use for assisting with and helping tohalt scalp hair loss, but this is debatable.
7 You will see changes in your complexion and fat redistribution.8 They had a wonderful calming effect for me and took the edge off my
sex drive
7a male sex hormone, such as testosterone
34
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
9 You can hide the effects of hormones from others for as long as youwant in virtually every case. Those who say they can’t seem to wantpeople to notice.
10 Hormones are potentially dangerous.11 I do not recommend herbals or care about them, since their potency
and safety are not regulated. Those serious about a safe, successfultransition should be taking prescription hormones under a physician’scare.
12 Getting a prescription and doing it supervised is often cheaper, safer,and more effective than black market options (James, 2014).
What changes will I see?
Male-to-Female (MTF) also known as ’transwomen’
Irreversible changes
• breast development,• enlarged nipples and areolae• stretch marks (for some) (unknown, 2015e)
Reversible changes
• decreased libido,• redistribution of body fat,• reduced muscle development,• various skin changes,• significantly reduced body hair• change in body odour and sweat production,• less prominence of veins,• ocular changes,• gonadal size (unknown, 2015e)
Typical changes from anti-androgensAveragetimeline
Effect of blocking testosterone
1–3 months af-ter starting anti-androgens
Testosterone blocking changes, decrease in sexdrive, fewer instances of waking up with anerection or spontaneously having an erection,some M→Fs also have difficulty getting anerection even when they are sexually aroused,decreased ability to make sperm and ejaculatoryfluid
35
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Typical changes from anti-androgensAveragetimeline
Effect of blocking testosterone
Gradualchanges(usually atleast 2 years)
Gradual changes, slower growth of facial andbody hair, slowed or stopped "male"-patternbalding, slight breast growth (reversible in somecases, not in others)(Ashbee and Goldberg,2006b)
Anti-androgens affect the entire bodyIt’s not possible to pick some changes and not others
Table 3.1 – Taking anti-androgens alone (without oestrogen) which may varyfrom person to person
Typical changes from oestrogenAverage time-line
Effect of oestrogen
1–3 months af-ter starting oe-strogen
Oestrogenic changes - softening of skin, decreasein muscle mass and increase in body fat,redistribution of body fat to a more "feminine"pattern, decrease in sex drive, fewer instancesof waking up with an erection or spontaneouslyhaving an erection; some M→Fs also find theirerections are less firm during sex, or can’t geterect at all, decreased ability to make sperm andejaculatory fluid
Gradualchanges(maximumchange after1–2 years onOestrogen)
Gradual changes, nipple and breast growth,slower growth of facial and body hair, slowedor stopped "male"-pattern balding, decrease intesticular size (Ashbee and Goldberg, 2006b)
Oestrogen affects the entire bodyIt’s not possible to pick some changes and not others
Table 3.2 – Typical changes from using oestrogen (which may vary from personto person)
Changes to expect Traits that won’t changeSofter skin and bodyappearance
Voice
Breast growth HeightLessening of body hair Size of hands and feetLoss of strength Presence of facial hair, (may grow
more fine)
36
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Changes to expect Traits that won’t changeIncreased emotionalsensitivity, especiallyto stress - depressionnot uncommon
Hair loss stops, but what has been lostwon’t grow back
Diminished ability toachieve erections andto ejaculate
Adam’s apple
Redistribution of bodyfat from stomach tobreasts, hips, andthighs
(University, 2014)
Table 3.3 – Things that might, or might not, change
Effect Notes
Breast development
Usually starts in 3–6 months,Breasts reach full size in 2–3 years,Size varies. A or B cup-size is typical,This is a permanent change
Body fat redistribu-tion
Usually starts in 3–6 months,Reaches maximum effect in 2–5 years,Less fat on abdomen,More fat on buttocks, hips and thighs,Usually not a permanent change if you stoptaking hormones
Reduced musclemass and strength
Usually starts in 3–6 monthsReaches maximum effect in 1–2 yearsReduced muscle and strength in upper bodyUsually not a permanent change if you stoptaking hormones
Softening of skin
Usually starts in 3–6 monthsSkin will be softer and less oilyUsually not a permanent change if you stoptaking hormones
Less body and facialhair
Usually starts in 6–12 monthsMaximum effect in more than 3 yearsBody hair will appear less noticeableBody hair will grow more slowlyBeard and mustache may grow more slowlyand appear less noticeable, but will not go awayIf you have male pattern baldness, it mayslow downHair that has already been lost likelywill not grow backThis is usually not a permanent change ifyou stop taking hormones
37
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Effect Notes
Reduced sex drive
Usually starts in 1–3 monthsReaches maximum effect in 1–2 yearsFewer morning erectionsFewer spontaneous erectionsUsually not a permanent change if you stoptaking hormones
Fertility
Timeline variesSperm may no longer reach maturityWon’t produce as much semenMay not be able to get hard enough forpenetrative sexMay become permanently unable to makesomeone pregnant (but birth control is stillrecommended)
Smaller testes
Usually starts in 3–6 monthsMaximum effect in 2–3 yearsMay shrink down to half their initial sizeThis may or may not be a permanent changeif you stop taking hormones
Emotional changes
Your overall emotional state may or maynot change; this varies from person to person.You may find that you experience a narrowerrange of emotions or feelings (Transhealth, 2015a).
Table 3.4 – Expected effects of feminizing hormone therapies
Risk level Feminizing hormonesLikely increased risk Serious blood clots (Venous thromboembolic
disease)GallstonesElevated liver enzymesWeight gainHypertriglyceridemia (risk factor for heartdisease and pancreas problems)
Likely increased riskwith presence of addi-tional risk factors
Cardiovascular disease
Possible increased risk High Blood Pressure (Hypertension)Hyperprolactinemia or prolactinoma
Possible increased riskwith presence of addi-tional risk factors
Type 2 Diabetes
No increased risk orinconclusive research
Breast cancer (Transhealth, 2015a)
Table 3.5 – Risks associated with feminizing hormone therapies
38
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Female-to-Male (FTM) also known as ’transmen’
Irreversible changes
• deepening of the voice,• growth of facial and body hair,• male pattern baldness (in some individuals),• an enlargement of the clitoris,• growth spurt and closure of growth plates if given before the end of
puberty, and• possible shrinking and/or softening of breasts, although this is due to
changes in fat tissue (unknown, 2012).
Reversible changes
• increased libido,• redistribution of body fat,• cessation of ovulation and menstruation,• further muscle development (especially upper body),• increased sweat and changes in body odour,• prominence of veins and coarser skin,• acne (especially in the first few years of therapy),• alterations in blood lipids (cholesterol and triglycerides), and• increased red blood cell count (unknown, 2012).
Typical changes from testosteroneAverage timeline Effect of testosterone1–3 monthsafter startingtestosterone
Toestrogenic changes - increased sex drive,vaginal dryness, growth of your cli-toris (typically 1–3 cm), increased growth,coarseness, and thickness of hairs on arms,legs, chest, back, plus abdomen oilier skinand increased acne, increased muscle massand upper body strength, redistributionof body fat to a more "masculine" pattern(more fat around the waist, less around thehips)
1–6 monthsafter startingtestosterone
menstrual periods stop
3–6 monthsafter startingtestosterone
voice starts to crack and drop within first3–6 months, but can take a year to finishchanging
1 year or more af-ter starting testos-terone
gradual growth of facial hair (usually 1–4years to reach full growth), possible "male"-pattern balding (Ashbee and Goldberg,2006a)
Testosterone affects the entire body39
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Typical changes from testosteroneAverage timeline Effect of testosterone
It’s not possible to pick some changes and not others
Table 3.6 – Typical changes from using testosterone (which may vary fromperson to person)
Effect Expectedonset
Expected max-imum effect
Skin oiliness/acne 1–6 months 1–2 yearsFacial/body hair growth 3–6 months 3–5 yearsScalp hair loss >12 months VariableIncreased musclemass/strength
6–12 months 2–5 years
Body fat redistribution 3–6 months 2–5 yearsCessation of menses 2–6 months n/aClitoral enlargement 3–6 months 1–2 yearsVaginal atrophy 3–6 months 1–2 yearsDeepened voice 3–12 months 1–2 years
Table 3.7 – Effects and expected time course of masculinizing hormones
Changes to expect Traits that won’t changeGrowth of facialhair (slow process)
Height (unless starting treatment at a youngage)
A lower voice Size of hands (though feet may grow a fewsizes)
Distribution ofbody fat frombreasts, hips, andthighs to stomach
Breast growth (though they may shrink alittle)
Increased strengthand muscle devel-opmentEnlargement ofthe clitorisIncreased bodyhairMasculinization offacial featuresMale-pattern hair-line and baldnessIncreasedaggression,heightened libidoCessation of men-struation
(University, 2014)
40
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Changes to expect Traits that won’t change
Table 3.8 – Things that will, and won’t, change
Option What is it? Advantages DisadvantagesInjectableTestosterone(e.g.testosteronecypionate ortestosteroneenanthate)
A medication youinject once a weekor once every twoweeks
It’s lower cost.It’s widely avail-able
May create highsand lows in energyand mood in be-tween doses
Testosterone Patch(e.g.Androderm)
A patch you wearevery day on yourback, upper arm,thigh or stomach
It’s administeredat a constant rate,eliminating thehighs and lowsin energy andmood associatedwith injectabletestosterone
It’s relatively ex-pensive. Somepeople have a skinreaction to the ad-hesive
Testosterone Gel(e.g.Androgel,or compoundedtestosteronegel/cream)
A gel or cream ap-plied to your skinat the same timeeach day
It’s administeredat a constant rate,eliminating thehighs and lowsin energy andmood associatedwith injectabletestosterone
Androgel isrelativelyexpensive. Whenyou are in intimatecontact withsomeone, it canbe challenging toavoid exposingthem to the gel
Oral Testosterone(e.g. testosteroneundecanoate)
A pill you takeonce a day
It’s administeredat a constant rate,eliminating thehighs and lowsin energy andmood associatedwith injectabletestosterone
Not commonlyused because itis less effectiveat stoppingmonthly bleeding(Transhealth,2015b).
Table 3.9 – Common masculinizing therapies
Name SafetyTestosterone cypionate GoodTestosterone enanthate goodTestosterone good
Table 3.10 – Popular androgens
41
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Name Safety andEfficacy
Goserelin ExcellentLeuprorelin Acetate Fair
Table 3.11 – Anti-hormones
Effect NotesIncreased sex drive Usually starts in 1–3 monthsMonthly bleedingstops
Usually happens within 2–6 monthsYou may still be able to get pregnant evenwhen your monthly bleeding stops (note: it isnot safe to take testosterone while pregnant)Reversible change, if you stop taking testos-terone
Bigger clitoris Usually starts in 3–6 monthsReaches full size in 1–2 yearsSize typically ranges from 1–3cmLikely permanent, even if you stop takingtestosterone
More facial and bodyhair
Usually starts in 3–6 monthsMaximum effect in 3–5 yearsGradual growth of mustache and beardMore, thicker and coarser hairs on abdomen,arms, chest, back and legsLikely permanent, even if you stop takingtestosterone
Male pattern baldness Usually starts in less than 12 monthsHair loss at temples and along the crown ofheadPossibility of becoming completely baldLikely permanent, even if you stop takingtestosteroneYou can take medications to minimize this
Oily skin and acne Usually starts in 1–6 monthsMaximum effect in 1–2 yearsMore acne. May permanently scarYou can take medications to minimize thisNot a permanent change if you stop takingtestosterone
Increased musclemass and strength
Usually starts in 6–12 monthsMaximum effect in 2–5 yearsThis is not a permanent change if you stoptaking testosterone
42
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
What changes will I see?
Effect NotesBody fat redistribution Usually starts in 3–6 months
Maximum effect in 2–5 yearsMore abdominal fatLess fat around buttocks, hips and thighsNot a permanent change if you stop takingtestosterone
Deepened voice Usually starts in 3–12 monthsMaximum effect in 1–2 yearsWhile your voice may deepen, other aspectsof the way you speak may not sound"manlier". You can work with a speechtherapist to achieve this, if desired.Permanent change
Changes to lining ofthe vagina
Usually starts in 3–6 monthsMaximum effect in 1–2 yearsThinning and drying of the lining of thevaginaMay make penetration uncomfortable (treat-ments are available)
Emotional changes Your overall emotional state may or maynot change; this varies from person toperson. You may find that you have accessto a narrower range of emotions or feelings.You may find that you become irritable,frustrated or angry more easily. (If you areinjecting testosterone every two weeks, youremotional changes may be the result of yourfluctuating testosterone level. You may wantto talk to your doctor about switching toweekly injections) (Transhealth, 2015b).
Table 3.12 – The expected effects of masculinizing hormone therapy
Effect NotesLikely increased risk Polycythemia (blood disorder)
Weight gainAcneAndrogenic alopecia (balding)Sleep apnoea
Possible increased risk Elevated liver enzymesHyperlipidemia
Possible increased riskwith presence of addi-tional risk factors
Destabilization of certain psychiatric disor-ders (bipolar disorder, psychotic disorders)Cardiovascular diseaseHypertension (high blood pressure)Type 2 Diabetes
43
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Common therapies
Effect NotesNo increased risk orinconclusive research
Loss of bone densityBreast cancerCervical cancerOvarian cancerUterine cancer (Transhealth, 2015b).
Table 3.13 – The risks associated with masculinizing hormone therapy
Common therapies
Oestrogens
Option What is it? Advantages DisadvantagesOral Oestrogen(e.g. Estrace)
A pill youswallow ordissolve underyour tongue eachday
Less expensive Highercardiovascularrisk for peopleover 40, orpeople withother risk factors
Oestrogen Patch(e.g. Estradot,Estraderm)
A patch youwear on yourskin that getschanged twice aweek
Lowercardiovascularrisk for peopleover 40, orpeople withother risk factors
More expensive.Some peoplehave a skinreaction to theadhesive in thepatch
Injectable Oestro-gen (e.g. estra-diol valerate)
A substance youinject every twoweeks
Lowercardiovascularrisk for peopleover 40, orpeople withother risk factors
More expensive.Less widelyavailable. Somepeople findinjections tobe painful.Improperinjection canbe dangerous(Transhealth,2015a)
Name Safety &Efficacy
Source
Estradiol Valerate excellent synthetic (plant-based ?)Ethinylestradiol Dep-recated
fair synthetic
44
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Common therapies
Oestrogens,conjugatedDeprecated
fair Live animals or synthetic
Table 3.15 – Popular Oestrogens
Testosterone Blockers
Option What is it? Advantages DisadvantagesCyproterone(e.g.Androcur)
A pill that youswallow once aday
Potenttestosteroneblocker
More expensive.May cause liverinflammationand depression
Finasteride(e.g.Proscar)
A pill thatyou put underyour tongueonce a day orevery otherday. Usuallyused with oneof the aboveanti-androgentherapies
Can help stophereditary hairloss
(Transhealth,2015a)
Name Safety Efficacy ActionSpironolactone Dep-recated
excellent good DHT blocker
Finasteride excellent good Type II 5-androgenreceptor (AR)inhibitor
Dutasteride excellent excellent Type I & II 5-ARinhibitor
Cyproterone Acetate fair excellent testosteroneblocker
Flutamide fair excellent testosteroneblocker
Bicalutamide fair good testosteroneblocker
Table 3.17 – Popular anti-androgens
Progesterone
Option What is it? Advantages Disadvantages
45
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Drugs used in Male to Female transitioning
MicronizedProgesterone(e.g.Prometrium)
A pill you takedaily
Thought to belower risk
Not as widelyavailable(Transhealth,2015a)
Name Safety Efficacy SourceProgesterone excellent highly
variableYams or SoyBeans
Dydrogesterone good variable syntheticMedroxyprogesterone Ac-etate Deprecated
fair variable synthetic
Table 3.19 – Popular progesteronic drugs
GnRH Agonists
Name Safety & EfficacyGoserelin excellentLeuprorelin Acetate fair
Table 3.20 – Popular GnRH agonists
Drugs used in Male to Female transitioning
• Cyproterone Acetate - Androcur, Cyprostat.• Dydrogesterone - Duphaston, Duphaston HRT.• Estradiol Valerate - Climaval, Estraderm MX, Estradiol implant,
Progynova, Progynova TS, Progynova TS forte, Zumenon.• Finasteride - Proscar.• Flutamide - Drogenil.• Goserelin - Zoladex, Zoladex LA.• Leuprorelin Acetate - Prostap SR, Prostap 3.• Minoxidil - Regaine.• Oestrogel - Oestrogel.• Progesterone - Cyclogest, Gestone.
These are listed in alphabetical order. Some are hormones, some are anti-androgens, some are DHT-blockers, and some are progesterones, and sothey are dealt with in separate chapters.
46
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Drugs used in Female to Male transitioning
Drugs used in Female to Male transitioning
Testosterone - Sustanon 100, Sustanon 250.
How oestrogen works
Oestrogen drug products act by regulating the transcription8 of a limitednumber of genes. Oestrogens diffuse through cell membranes, distributethemselves throughout the cell, and bind to and activate the nuclearoestrogen receptor, a deoxyribonucleic acid (DNA)-binding protein whichis found in oestrogen-receptive tissues. The activated oestrogen receptorbinds to specific DNA sequences, or hormone response elements, whichenhances the transcription of adjacent genes and in turn lead to theobserved effects. Oestrogen receptors have been identified in tissuesof the reproductive tract, breast, pituitary, hypothalamus, liver, andbone of women (unknown, 2004a). Oestrogens are important in thedevelopment and maintenance of the female reproductive system andsecondary sex characteristics. With other hormones, such as pituitaryhormones and progesterone, they cause enlargement of the breasts, throughpromotion of ductal growth, stromal development, and the accretion offat. Oestrogens occur naturally in several forms. The primary source ofoestrogen in normally cycling adult women is the ovarian follicle, whichsecretes 70–500 micrograms of estradiol daily, dependant on the phaseof the menstrual cycle. This is converted primarily to estrone, whichcirculates in roughly equal proportion to estradiol, and to small amountsof estriol. After the menopause, most endogenous oestrogen is produced byconversion of androstenedione, secreted by the adrenal cortex, to estroneby peripheral tissues. Thus, estrone - especially in it’s sulphate esterform - is the most abundant circulating oestrogen on postmenopausalwomen. Although circulating oestrogens exist in a dynamic equilibriumof metabolic interconversions, estradiol is the principle intercellular humanoestrogen and is substantially more potent than estrone or estriol at thereceptor. Oestrogens used in therapy are well absorbed through theskin, mucous membranes, and gastrointestinal tract. When applied fora local action, absorption is usually sufficient to cause systemic effects.When conjugated with aryl and alkyl groups for parenteral administration,the rate of absorption of oily preparations is slowed with a prolongedduration of action, such that a singular injection of estradiol valerateor estradiol cypionate is absorbed over several weeks. Administeredoestrogens and their esters are handled within the body essentially thesame as the endogenous hormones. Metabolic conversion of oestrogensoccurs primarily in the liver (first pass effect), but also at local target
8The natural process by which a molecule of RNA is synthsized on the model of a DNAtemplate carrying the necessary genetic information
47
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
How oestrogen works
tissue sites. Complex metabolic processes result in a dynamic equilibriumof circulating conjugated and unconjugated oestrogenic forms whichare continually interconverted, especially between estrone and estradioland between esterified and nonesterified forms. Although naturally-occurring oestrogens circulate in the blood largely bound to sex hormone-binding globulin and albumin, only unbound oestrogens enter targettissue cells. A significant proportion of the circulating oestrogen existsas sulphate conjugates, especially estrone sulphate, which serves as acirculating reservoir for the formation of more active oestrogenic species.A certain proportion of the oestrogen is excreted into the bile and thenreabsorbed from the intestine. During this enterohepatic recirculation,oestrogens are desulphated and resulphated and undergo degradationthrough conversion to less active oestrogens (estriol and other oestrogens),oxidation to nonoestrogenic substances (catecholoestrogens, which interactwith catelcholamine metabolism, especially in the central nervous system),and conjugation with glucoronic acids (which are then rapidly excretedin the urine). When given orally, naturally-occurring oestrogens andtheir esters are extensively metabolised (first pass effect) and circulateprimarily as estrone sulphate, with smaller amounts of conjugated andunconjugated oestrogenic species. This results in limited oral potency. Bycontrast, synthetic oestrogens, such as ethinylestradiol and the nonsteroidaloestrogens, are degraded very slowly in the liver and other tissues,which results in their high intrinsic potency. Oestrogen drug productsadministered by non-oral routes (i.e. transdermally) are not subject to first-pass metabolism, but also undergo significant hepatic9 uptake, metabolism,and enterohepatic10 recycling (unknown, 2004a).
Natural hormones, such as the oestrogen called 17-β-estradiol (pink), travelthrough the bloodstream and enter cells (cyan), where they may findmatching hormone receptors, such as oestrogen receptors (purple). Not allcells have a hormone’s compatible receptor. The ones that do are calledtarget cells.
Once inside a target cell, the hormone (pink) binds to a receptor (purple) -similar to a hand sliding in a glove or mitten - and forms what is known as ahormone-receptor complex between the ligand and receptor. A ligand is anymolecule that binds to a specific site on a protein or other molecule. In thiscase, the oestrogen hormone 17-β-estradiol is the ligand, and the oestrogenreceptor is the protein.
Binding turns on, or activates, a hormone receptor. Activation sets in motioncell signaling systems that trigger gene expression and lead to responsestypical of a particular hormone. First, the activated receptor attaches to aspecific region of the DNA11 in the nucleus where it interacts with otheractivating molecules to turn on a specific gene or suite of genes. Then, the
9Relating to the liver10Circulation of substances which are absorbed from the intestine and carried to the liver
where they are secreted into the bile and again enter the intestine11deoxyribonucleic acid
48
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
How oestrogen works
DNA’s genetic code is copied to make a complimentary messenger RNA(mRNA) through a process called gene transcription. The mRNA movesfrom the nucleus to the cytoplasm, where it is transcribed by ribosomes tomake the proteins (enzymes, other receptors, etc.) that directly guide celland body responses. In the case of oestrogen hormones, these responses caninclude uterine growth to prepare for pregnancy, or to maintaining systemsto prevent bone loss.
Its been found that a more fluid and less structured molecular processallows for related natural hormones, such as the oestrogens 17-β-oestradiol,estrone, and estriol to dock with the same receptor, such as ER-α. Likewise,a single hormone, such as 17-β-oestradiol, can bind with multiple relatedreceptors, such as ER-α and ER-β.
Unexpectedly, other, nonhormone molecules were found to exploit thesystem, too.
Many, vastly different natural compounds and synthetic chemicals do bindto hormone receptors. Nonylphenols, some PolyChlorinated Biphenyls,are industrial products or chemicals (PCB’s)12, some chemicals used tomake plastics (bisphenol-A), and many plant flavonoids, also known asphytoestrogens, are examples.
Generally, these, and other plant and fungal compounds, drugs, pesticides,industrial agents, and metals known to interfere with natural hormones arecollectively called endocrine disrupters endocrine disruptor (ED)13. Moreis understood about how EDs interfere with receptor binding than withthe other ways, or mechanisms, that these foreigners employ to disruptendocrine-related functions. But whether the binding causes any long-term,adverse health conditions in humans is still debated (tulane.edu, 2014).
12PolyChlorinated Biphenyls, are industrial products or chemicals13endocrine disruptor
49
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Hormone effects in male→female
Hormone effects in male→female
Figure 3.1 – Positive and negative effects of oestrogen
Cardiovascular
• The most significant cardiovascular risk for transgender women is thepro-thrombotic effect of oestrogens (Increased blood clotting.) Thismanifests most significantly as an increased risk for thromboembolicdisease: deep venous thrombosis (deep venous thrombosis (DVT)14)and pulmonary embolism (pulmonary embolism (PE)15) which occurswhen DVTs break off and migrate through the venous system tothe lungs. It is important for any person on female hormones toimmediately seek medical care if she develops pain or swelling ofone leg (especially calf) as this is the predominant symptom of a DVT,or if she develops symptoms of PE - chest pain, shortness of breath,fainting, or palpitations (even without leg pain or swelling). See alsoDeep Vein Thrombosis.
14deep venous thrombosis15pulmonary embolism
50
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Hormone effects in male→female
• In practice this becomes very important to transgender womenundergoing surgery. Hormones should be withheld for a week before,and until two weeks after surgery. Also see what your surgeon says.
• DVTs occur more frequently in the first year of treatment withoestrogens. However this may represent a ’screening by treatment’of patients who may have genetic predispositions to thromboembolicdisease, with those who are more likely to develop DVTs doingso early on in therapy. However, if patients have a family historyof thromboembolic disease, screening for known disease may beappropriate.
• DVT risk is greater with oral rather than transdermal or injectableoestrogens.
• DVT risk also increases with age and with smoking, so many cliniciansadvise using the safer transdermal formulations in patients whosmoke or are older than age 40.
• If screening is undertaken for known pro-thrombotic mutations suchas Factor V-Leiden, antithrombin III, and protein C or S deficiency,it should be done so to increase the safety of hormonal therapyand not as a screen for who may undertake hormonal therapy.Given that the risk of warfarin treatment in a relatively young, well-informed, and otherwise healthy population is quite low and thatthe risk of adverse physical and psychological outcome for untreatedtransgender patients is high, a prothrombotic mutation is not anabsolute contraindication for hormonal therapy (Levy, Crown, andReid, 2003).
• The antiandrogen bicalutamide is associated with an increased risk ofheart failure when used as monotherapy (without any other drugs).A study (Iversen et al., 2004) of prostate cancer patients also showedan increased number of deaths unrelated to cancer among patientstaking 150mg/day bicalutamide. This prompted Health Canada towithdraw its approval (Borkowski, 2003) for 150mg bicalutamide asmonotherapy. The increased death rate has not been observed wherebicalutamide was combined with a method of reducing androgenproduction. The exact reasons for the heart failure and deaths havenot been completely determined, however a likely cause is acuteadrenal insufficiency due to the action of DHT (Rossi et al., 1998)during episodes of bicalutamide withdrawal. Because bicalutamideis extremely lipophilic16, it is difficult to avoid periods of lowserum concentration due to the uptake of bicalutamide into fat cells(unknown, 2015e).
16the ability to dissolve or attach to lipids
51
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Hormone effects in male→female
Hair
• Current facial hair is only slightly affected (some reduction in density,coverage, and slower growth) by anti-androgens. Those who are lessthan a decade past puberty and/or whose ethnicity generally lacksa significant amount of facial hair will have better results with anti-androgens. Those taking anti-androgens will have better results withelectrolysis/laser hair removal than those who are not. If one is still intheir teens or early twenties, there will be prevention of new facialhairs from developing if testosterone levels are within the femalerange.
• Body hair (chest, periareolar, shoulders, back, abdomen, rear, thighs,tops of hands, tops of feet) will, over time, turn from terminal hairs17
to vellus hairs18. Hair on the arms, perianal, and perineal will reducebut may not turn to vellus hair on the latter two regions (somenatal females also have some hair in these areas). Underarm hairwill slightly change in texture and length, pubic hair becomes moretypically female in pattern. Lower leg hair becomes less dense inconcentration. All depend upon genetics.
• Head hair may slightly change in texture, curl, and colour (new hairsthat is, not hair that has already formed and reached the surface priorto HRT), this is especially likely with hair growth from previously baldareas.
• Eyebrow hair becomes less "bushy" or scattered (unknown, 2015e).
Urogynaecological effects
• Transgender women report a sometimes significant reduction in libidoall depending upon the dosage of anti-androgens. A small numberof post-operative transsexual women may take small amounts oftestosterone to boost the libido. Many pre-operative transsexualwomen simply wait until after sex-reassignment surgery to begin anactive sex life (due to how they feel towards their genitals and/or, forheterosexual or bisexual transsexual women, an aversion to anal sex)and for post-operative transsexual women how satisfied they are withthe results. Raising oestrogen dosage or adding a progestogen has alsoraised the libido of some transwomen.
• Spontaneous and morning erections decrease in frequency signifi-cantly, however some who have had an orchiectomy still experiencemorning erections. Voluntary erections can be maintained since thebrain is the most important sex organ, a developed repertoire offantasies and good visualization is a must. It also depends on howone views their own genitals (disgust, strong aversion to, tolerable,etc.).
17normal hairs18very tiny, blonde "baby" hairs
52
Version 2016.3576– – Document LATEXed – 1st May 2016
[git] • Branch: 1.5 @ 26b5e6d • Release: 1.5 (2016-05-01)
Hormone effects in male→female
• Testicular volume is reduced by about 25% with typical dosages andas much as 50% in higher dosages, especially after a year of HRT. Thisis in response to the decrease in Leydig cells19, Sertoli cells20, andinterstitial tissue, which produce both sperm and testosterone. Whentestosterone is dramatically reduced spermatogenesis21 is haltedalmost completely, when the cells that are involved in these processesgo unused they atrophy22.
• The prostate shrinks• The bladder shrinks• The line that runs down the underside of the penis and down the
middle of the scrotum, the peno-scrotal raphe (where the urogenitalfolds fused early in the womb), will darken.
• Minor water retention is likely (unknown, 2015e).
Childbearing
• Childbearing, as experienced by cisgender23 women, is impossiblewith today’s technology. Pre-operative sperm banking can be done,however, allowing artificial insemination to be used to producegenetic offspring with someone else at a later date. See also Spermbanking. Medical advances in the near future may one day make thispossible by using a donor uterus long enough to carry a child to termas anti-rejection drugs do not seem to