Embed Size (px)
Citation preview

American Journal of Emergency Medicine xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
American Journal of Emergency Medicine
j ourna l homepage: www.e lsev ie r .com/ locate /a jem
Case Report
Hookworm infestation as unexpected cause of recurrent pancreatitis
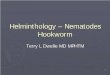
Fig. Image from endoscopic retrograde cholangiopancreatography shows A duodenalehookworms attached to the duodenum (arrows).
Abstract
Parasite infestation is still associated with significant morbidityand mortality. Hookworm infestation is a very rare cause ofpancreatitis. This parasitic infestation might be asymptomatic. Acutepancreatitis as a result of the hookworms migrating into the ampullaof Vater with chronic inflammation was a very rare complication. Wereport a case of hookworm infestation that was associated withsignificant complication of recurrent pancreatitis. The patient wastreated with mebendazole. He was asymptomatic and had gainedweight at the 3-month follow-up. Our case demonstrates thatpancreatitis secondary to hookworm infection can occur and mayresolve after anthelmintic treatment.
An 86-year-old man who had recently been treated for irondeficiency anemia presented to our emergency department (ED)because of general weakness, edema, dyspnea, diarrhea, abdominalpain, and dyspepsia for 5 days. He had no history of diabetes mellitus,hypertension, alcohol consumption, or malignancy. He did not haveheadaches, nasal discharge, productive cough, sore throat, chest pain,dysuria, or trauma. He was initially diagnosed and treated forrecurrent pancreatitis and iron deficiency anemia at a local clinic for6 months prior to his ED presentation.
On physical examination, he appeared malnourished. His bloodpressure was 110/80 mmHg, with a heart rate of 112 beats/min and arespiratory rate of 30 breaths/min. He was afebrile. The physicalexamination was otherwise unremarkable, except for pale conjunc-tiva, abdominal distention, and tenderness more marked over theumbilicus with no guarding or rebound tenderness. Bowel soundswere decreased. A complete blood cell count showed the following:leukocyte count, 6900/mm3; segmented neutrophils, 90%; no eosin-ophil, anemia with a hemoglobin level of 4.0 g/dL; hematocrit, 15.6%;and platelet, 110000/μL. Other laboratory studies included the following:glucose, 96 mg/dL; serum urea nitrogen, 50 mg/dL; serum creatinine, 1.6mg/dL; sodium, 148 mEq/L; potassium, 2.5 mEq/L; glutamic oxaloacetictransaminase (GOT), 265U/L; albumin,3.4 g/dL; total bilirubin, 1.1mg/dL;C-reactive protein, 2.73mg/L; lipase, 988U/L; and prothrombin timewithan international normalized ratio of 1.89. Stool examination was positivefor occult blood and ova. His chest x-ray showed a right lower lunginfiltration and pleural effusion. He was transfused with 6 U packed redblood cells. With a working diagnosis of recurrent pancreatitis, anendoscopic retrograde cholangiopancreatography was performed on theday of admission with extraction of multiple worms (Fig.). Endoscopicretrograde cholangiopancreatography examination showed erythemaand edema of the ampulla of Vater and duodenal ulceration withduodenitis. The worms were identified as Ancylostoma duodenale. Basedon these findings, oral mebendazole 100 mg twice a day for 3 days wasprescribed. Iron supplements were used to treat iron deficiency anemia.After initiation of the therapy, the patient showed signs of improvement
Please cite this article as: Tseng L-M, et al, Hookworm infestation as unhttp://dx.doi.org/10.1016/j.ajem.2014.03.046
0735-6757/© 2014 Elsevier Inc. All rights reserved.
and recovered uneventfully after 7 days treatment. Hewas asymptomaticwith recovery of appetite and weight, and no further abdominal painoccurred and no stool ova was found at subsequent outpatient visits.
Abdominal pain is themost common chief concern of patients in ED[1]. Pancreatitis should be considered in all patients with unexplainedabdominal pain. The patient presented with multiple episodes ofpancreatitis and anemia for which the etiology was initially unknown.Parasitic agents are rarely identified in ED. The persistent andworseningof abdominal pain and anemia was related to hookworm infestation.Longstanding hookworm infection may result in malabsorption inaffected individual. The major consequence of heavy hookworminfestation is iron deficiency anemia and hypoproteinemia. It maylead to iron deficiency anemia that results from chronic blood loss [2].Mature worms of A duodenale develop in the duodenum and jejunum,bite into mucosa, and suck blood at a rate of 0.25 mL/d per worm,causing a variable degree of anemia. Hookworms in the intestine cancause abdominal pain, nausea, and diarrhea [3]. It commonly causessmall intestinal infections, but pancreatitis induced by A duodenale is anunusual diagnosis. The pancreatitis occurred secondary to chronicinflammation involving the ampulla of Vater.
Most infected individuals are asymptomatic. Hookworm infection isa treatable condition and results in complete recovery. The proteinlosses associated with heavy hookworm infection can result inhypoproteinemia and anasarca. Loss of plasma protein results frommalabsorption and increased intestinal permeability secondary toinflammation. Because large infestation is associated with highmorbidity, it is critical to screen by examining stools under amicroscopefor the presence of worm larvae or eggs. Endoscopic retrograde
expected cause of recurrent pancreatitis, Am J Emerg Med (2014),

2 L-M. Tseng et al. / American Journal of Emergency Medicine xxx (2014) xxx–xxx
cholangiopancreatography may be used for direct diagnosis [4].Hookworm infestation is acquired by contacting soil contaminatedwith human feces and ingesting larvae crawling on contaminated freshvegetables. It should be suspected in patients with a history of exposureon poor sanitation and hygiene and immigrants from endemic areas.
Our case demonstrates that pancreatitis secondary to hookworminfection can occur and may resolve after anthelmintic treatment.Hookworm infection should be considered in malnourished patientswith clinical signs and symptoms of abdominal pain, diarrhea withoccult bleeding, and anemia.
Li-Ming Tseng MDEmergency Department, Shin Kong Wu Ho-Su Memorial Hospital
Taipei, Taiwan
Cheuk-Kay Sun MDDepartment of Gastroenterology
Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
Tzong-Luen Wang MD, PhDEmergency Department, Shin Kong Wu Ho-Su Memorial Hospital
Taipei, TaiwanSchool of Medicine, Fu-Jen Catholic University, New Taipei City, Taiwan
Please cite this article as: Tseng L-M, et al, Hookworm infestation as unhttp://dx.doi.org/10.1016/j.ajem.2014.03.046
Aming Chor-Ming Lin MS, MDEmergency Department
Shin Kong Wu Ho-Su Memorial HospitalTaipei, Taiwan
Department of Intensive Care UnitShin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
School of Medicine, Fu-Jen Catholic UniversityNew Taipei City, Taiwan
E-mail addresses: [email protected]@ms.skh.org.tw
http://dx.doi.org/10.1016/j.ajem.2014.03.046
References
[1] Graff IV Louis G, Robinson Dave. Abdominal pain and emergency departmentevaluation. Emerg Med Clin North Am 2001;19(1):123–36.
[2] Stoltzfus RJ, Dreyfuss ML, Chwaya HM. Hookworm control as a strategy to preventiron deficiency. Nutr Rev Jun 1997;55(6):223–32.
[3] Varghese Thomas, Harish K, Tony J, Sunilkumar R, Ramachandran TM, Anitha PM.Colitis due to Ancylostoma duodenale. Indian J Gastroenterol 2006;25:210–1.
[4] Osman M, Bach Lausten S, El-Sefi T, Boghdadi I, Rashed M-Y, Lindkær Jensen SM.Biliary parasites. Dig Surg 1998;15:287–96.
expected cause of recurrent pancreatitis, Am J Emerg Med (2014),