Embed Size (px)
Citation preview

HJÄRTFUNKTION OCH DIALYS
Jan MalikPrague, CZ

Patients with chronic kidney disease (CKD)
• Very high mortality – mostly cardiovascular
• Very high morbidity – frequently cardiovascular
Tonelli M. et al. JASN 2006
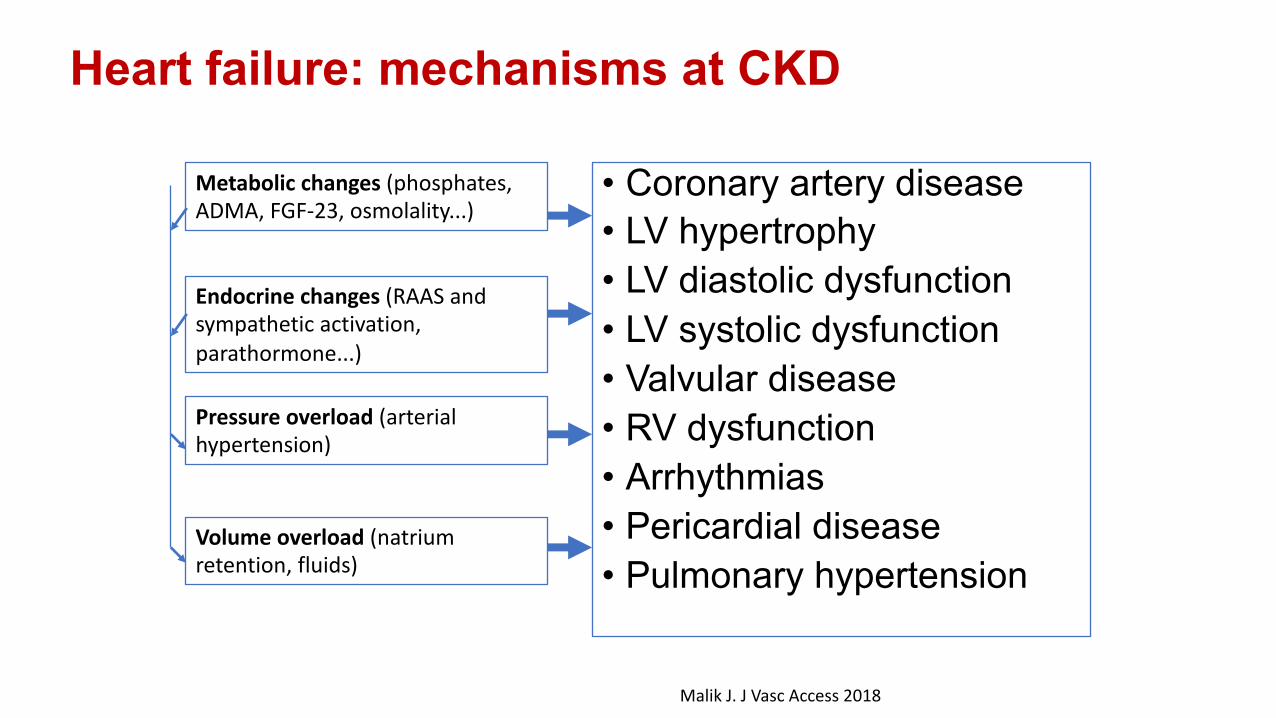
Heart failure: mechanisms at CKD
• Coronary artery disease• LV hypertrophy• LV diastolic dysfunction• LV systolic dysfunction• Valvular disease• RV dysfunction• Arrhythmias• Pericardial disease• Pulmonary hypertension
Metabolic changes (phosphates, ADMA, FGF-23, osmolality...)
Endocrine changes (RAAS and sympathetic activation, parathormone...)
Pressure overload (arterial hypertension)
Volume overload (natrium retention, fluids)
Malik J. J Vasc Access 2018

Heart failure: mechanisms at CKD
• Coronary artery disease• LV hypertrophy• LV diastolic dysfunction• LV systolic dysfunction• Valvular disease• RV dysfunction• Arrhythmias• Pericardial disease• Pulmonary hypertension
Metabolic changes (phosphates, ADMA, FGF-23, osmolality...)
Endocrine changes (RAAS and sympathetic activation, parathormone...)
Pressure overload (arterial hypertension)
Volume overload (natrium retention, fluids)
Malik J. J Vasc Access 2018

Earlier CKD mechanisms
• Metabolic syndrome: DM and hypertension as rising causes of CKD• coronary artery disease statins, gliflozides, ACEi.....
• Phosphate retention
• Salt + water retention

Earlier CKD mechanisms: phosphate retention
increase of FGF-23 and parathormone

FGF-23 and the heart
• Heart (arteries+veins) calcification
• Left ventricular hypertrophy
Mall G. Nephrol Dial Transplant 1990
Normal heart
LV hypertrophy at hypertension
LV hypertrophy at ESRD

Left ventricular hypertrophy
Incidence• Ca 20% of CKD 1-3 patients• Up to 80% of patients beginning HD therapy)
Risks• Cardiovascular diseases including sudden death• Faster progression of CKD)
1) Park M et al. J Am Soc Nephrol 20122) Mostovaya IM et al. PloS One 2014
Salt and water retention

www.nefrol.czNa + H2O excretion within 8 hours after i.v. normal saline 20ml/kgHealthy subjects vs. mild CKD

• CKD®impared Na+H2O excretion• ESRD significant Na+H2O retention between
hemodialysis sessions (accompanied by blood pressure increase)
® VOLUMEXPANSION
Increase of cardiac output„Luxurious“ tissue perfusion
Brod J. Ulster Med J. 1975
Salt and water retention ®volume overload

Some natrium is not excreted...where is it?
Brod J. Ulster Med J. 1985
Non-osmotic natrium storage
CKD/ESRD patiens:
synthesis of glykosaminoglykans
(muccopolysaccharides)
Tissue concentrations:
Skin: 1.0-14.0 g/kg
Muscles: 0.6-7.1 g/kg
Arterial wall: 0.9-9.8 g/kg
Fischereder M et al. Am J Physiol Renal Physiol 2017;319(2):F319-F325
Increased production of
glykosaminoglykans leads to
excessive calcification of aorta
in micePumomo E. J Am Heart Assoc 2013
Na® Ca
2+
?

Volume overload:consequences
Pulmonary and systemic venous congestion
Dyspnoea, edema, impaired organ perfusion
Development of LV systolic dysfunction
Increased mortality

Hemodynamic consequences of volumexpansion Central venous pressure, left atrial pressure® PRELOAD¯ systemic vascular resistance ®¯ AFTERLOAD
Cardiac output
Pulmonary artery pressure
Pulmonary congestion
Pulmonary hypertension

Anemia
J. Scultet: Armamentarium chirurgicum, Leiden 1693

Hemodynamic impact of acute anemia*):
Blood loss up to 2 liters
No change in plasma lactate
*)Weiskopf: JAMA. 1998;279:217-221.

Anemia therapy
¯ stroke volume, CO*)
*)Fellner SK et al. Kidney Int 1993;44:1309-1315
**) Moecks J Nephron 2000;86(4):455-462
***)Druecke TB et al. NEJM 2006;355:2071-2084
¯ morbidity
¯ mortality ??**) – CREATE, CHOIR
„Optimal“ values***) Hgb 110-120g/l

Arteriovenous access

AV access creation
Decrease of peripheral vascular resistance
Flow increase
Increase of wall shear stress
NO
Feeding artery dilatation
Endothelium
WSS(τ) = (velocity*viscosity)/dia
meter
Hemodynamic changes after AV access creation

Usual flow volume via an AV-access (Qa): forearm 600-1200 ml/minbrachial 800-1500 ml/min
Normal resting cardiac output (CO): 4-6 l/min
Normal brachial artery flow volume: 80-150ml/minBrachial artery flow volume:ESRD pts. 60-120 ml/min

A-V access creation
¯ Systemic vascular resistance
¯Afterload Preload
Cardiac output
Volume retention
Venous return

3 factors leading to hyperkinetic circulation
Na + H2O retention
Anemia A-V dialysis access

Flow competition
• The flow is driven by:• perfusion pressure (mean arterial-central venous pressure)• vascular resistance¯
www.matrix.co.nz
Peripheral vascular resistance:
ability of arteries to dilate (endothelial function)
arterial stenosis (athero- and arteriosclerosis)

Flow competition
• Hand ischemia
• Ipsilateral CABG
• Vertebral artery??
• Far tissues and organs??????

CABG: Coronary Artery Bypass Graft

Risk of flow competition –coronary artery bypass

Flow competition between AVF and vertebral artery?

Brain atrophy and cognitive dysfunction
Cerebral oxymetryHD pts. vs. controls:51.5±10.9% vs. 68±7%, p<0.0001
Malik J et al. J Vasc Access 2017Kovarova L. et al. Nephron Clin Practice 2018
RELATION TO HEART FAILURE?

The heart at CKD patients

Hyperkinetic circulation
Na + H2O retention
Anemia A-V dialysis access

Heart function depends on:
• LV contractility• LV compliance (diastolic function)• Heart rate• Preload• Afterload• Valvular disease• Arrhythmias• Pericardial disease• .....
Cardiac output
Malik J. J Vasc Access 2018

Cardiac output (CO)Calculation: ECHO, dialysis dilution techniques (Transonic...), Swan-Ganz catheter
Normal values 4-6 l/min
Cardiac index: CI = CO/BSA (body surface area)

Cardiac output and access flow volume (Qa)
• Effective CO: COef. = CO-Qa
• Effective cardiac index (CIef. )
• High-flow AVF:• >1500-2000 ml/min• Qa > 1/3 of CO
Basile C, Lomonte C. Semin Dial 2018

How does the heart react to the hyperkinetic circulation ???
Normal (effective) CO
AVF
CKD stage.........

Hyperkinetic circulation consequences
• Left ventricular dilatation ® mitral regurgitation• Left atrial dilatation® risk of atrial fibrillation• Left ventricular hypertrophy• Accelerated degeneration of cardiac valves• Accelerated stiffening of aorta and arteries?• Pulmonary hypertension• Right ventricular dilatation ® tricuspid regurgitation
Malik J. J Vasc Access 2018

Heart failure

Heart failure
• very frequent in ESRD patients• is associated with significantly higher mortality• many mechanisms are involved• AVF may play a role

Heart failure: mechanisms at CKD
• Coronary artery disease• LV hypertrophy• LV diastolic dysfunction• LV systolic dysfunction• Valvular disease• RV dysfunction• Arrhythmias• Pericardial disease• Pulmonary hypertension
Metabolic changes (phosphates, ADMA, FGF-23, osmolality...)
Endocrine changes (RAAS and sympathetic activation, parathormone...)
Pressure overload (arterial hypertension)
Volume overload (natrium retention, fluids)
Malik J. J Vasc Access 2018

Heart failure: diagnostic tools
BNP

Heart failure types
• Classic, congestive HF• Relatively or absolutely low CO (COef.) at reast or excercise• Very frequent
• High-output HF• Very high CO• Rare
High-output heart failure
• Symptoms of heart failure (dyspnoe, fatique)• Signs: BNP, congestion on X-ray, left atrial pressure • High cardiac output indexed to body surface area (CI)
• Cut-off values: CI >3.5-3.9 l/min/m2
• Qa usually > 2000 ml/min

Hyperkinetic heart failure series• E. Chemla et al.*• n=17, symptomatic heart failure• surgical banding of the A-V access
• Qa 3135 ± 692 Þ1025 ± 551 ml/min!!!
• CO 8.0 ± 3.1 Þ 5.6 ± 1.7 l/min symptoms disappeared
*)Semin Dial. 2007;20(1):68-72
change 2.1 l/min
change 2.4 l/min

Hyperkinetic heart failure(CI > 3.5 l/min)invasive hemodynamic ex.
Mayo clinic: right-sided catheterization during 2000-2014 (n = 16,462)• High CI: 525 pac.• of them with heart failure without anemia or thyreotoxicosis: 120 pts
(0.7%)
• A-V shunt as the cause in 22%
Reddy YNV et al. J Am Coll Cardiol 2016;68(5): 473-482

„Hyperkinetic heart failure is characterized by the activation of natriuretic peptides, expansionof plasma volume, increased ventricular fillingpressure and by pulmonary hypertension“
Reddy YNV et al. J Am Coll Cardiol 2016;68(5): 473-482

Wohlfart P. et al. Hypertension Res 2016
The effect of Qa reduction on the heartdepending on cardiac index
® Indication to flow reduction
Pts. with symptoms of HF, larger LV and CI>3.9l/min/m2

Congestive heart failure
• Very individual tolerance of Qa
• Qa effects similar to anemia, volume overload
• BNP rises after access creation with „normal“ Qa*)
*)Malik J.et al. Int Urol Nephrol. 2009 Dec;41(4):997-1002

Diagnosis of congestive HF at ESRD patients
Difficult: overhydration vs. heart failure
Heart failure criteria at ESRD pts.:• Shortness of breath in the absence of pulmonary
disease• Congestion withdrawal with ultrafiltration• Structural heart disease
Chawla LS et al. JACC 2014Acute Dialysis Quality Initiative XI workgroup
Structural heart disease according to Acute Dialysis Quality Initiative XI workgroup
• The largest trial investigating the influence of heart disease on mortality at ESRD pts. (Mayo clinic, n= 654)
• Included patients had echo before/shortly after hemodialysis initiation; dialysis lasted for ³ 30 days
• During the median of 2.4 years 26% of pts. died
Hickson LJ et al. JACC 2016

Included patients: n= 1187
No ECHO: n= 533
415 died during follow-up
ECHO: n=654age 66±16 let
Less comorbidities, more often AVF
Sudden cardiac death 29%
Hemodialysis withdrawal leading to death25%
Sepsis 7%
Other causes, unknown 38%
3-year mortality 46%38%

Structural heart diseaseAcute Dialysis Quality Initiative XI workgroup
Criterion³ 1 must be present
Definition
LV hypertrophy LVMi > 110g/m2 for ♀and > 130 g/m2 for ♂or LVMI > 47 g/m2.7 in♀> 50 g/m2.7 for ♂
Increased LV volume LVEDVi > 86 ml/m2
LVESVi > 37 ml/m2
LV systolic dysfunction/RWMA
EF £ 45% and/or RWMA
RV systolic dysfunction Lateral tricuspid annular systolic velocity (s´)<9.5cm/s
Or semiquantitatively abnormal systolic functionLeft atrial dilatation LAVi > 34 ml/m2
Diastolic dysfunction ³ grade 2
Mitral valve disease Moderate to severe stenosis or regurgitation
Aortic valve disease Moderate to severe stenosis or regurgitationHickson LJ et al. JACC 2016

Structural heart diseasePercentage of pathol. findings
Criterionprior to HD th.
Frequency
LV hypertrophy 49% u g/m2 resp. 71% g/m2.7
Increased LV volume 72%
LV RWMA/dysfunction 50%RV systolic dysfunction 34%
Left atrial dilatation 81%LV diastolic dysfunction 78%Mitral valve disease 13%Aortic valve disease 3%
Hickson LJ et al. JACC 2016At least one at 87% pac.
Stro
nges
t pr
edict
ors o
f de
ath

(My) Criticism of the trialby Acute Dialysis Quality Initiative XI workgroup
Not determined• Pulmonary hypertension!!!• Coronary artery disease!!!• Calcium score• Pericardial disease• Arrhythmias
Echo changes significantly after hemodialysis initiation (de-congestion)Many of the patiens did not have echo at all!Cardiac output was not measured
Other

Qa and congestive heart failure
• Paucity of data
• AVF decreases blood pressure – does it help in patients with very stiff arteries by lowering BP?
• AVF could be the last drop in patients with failing heart
• The role of high Qa is often overestimated – too high dry weight is not so rare condition
Come tommorrow to the workshop!

Conclusions
• The interaction between kidneys and heart is very complex
• Hyperkinetic circulation (volume retention, anemia, Qa) contributes to the morbidity of CKD patients
• However, we still do not know the safe values of Qa

General University Hospital in Prague
Thank you for your attention
UNIVERSITAS CAROLINA PRAGENSISEst. 1348





























