Embed Size (px)
Citation preview

HIV/AIDS REPORT FROM MAJURO, RMI
HIV/AIDS REPORT FROM MAJURO, RMI
Dr. Zachraias Zachraias
Public Health Clinician
HIV Clinical Manager

Total: Pop 11,396
Total: Pop 29,488

Basic DemographyBasic Demography
Health Indicators 1999 (census) 2004Population 50,840 61,215
Age 0-14 21,837(42%)
Age 15-29 14,198 (27%)
Age 65+ 1113 (2%)
Crude Birth Rate 41.21/1000 pop
49.2 in 1988
26.45/1000
Crude Death Rate 4.47/1000 pop. 4.31/1000
Life Expectancy Life expectancy at birth:
Female (67) Male (64)
Female (69.4)
Male (65.7)

HIV Report 2001HIV Report 2001Quarterly Male Tested Female Tested Total Tested
First Quart 90 459 549
Second 107 569 676
Third Quart 326 802 1128
Fourth 82 535 617
Total 605 (20%) 2365 2970

HIV/AIDS Screening from 01/01/2002 to 12/31/2002HIV/AIDS Screening from 01/01/2002 to 12/31/2002
AGE Group Male Female Total
< 15 age 114 159 279
15-19 age 290 559 849
20-24 age 178 660 839
25-29 age 91 462 554
30-34 age 87 328 415
35-39 age 58 249 307
40-44 age 37 189 227
45-49 age 23 136 159
50+ age 43 153 197
Total 921(24%) 2895(76%) 3,826

Reason For Test (Screen) for 2002
Reason For Test (Screen) for 2002
STD 106 (2.70%)
PRENATAL 1,212 (30.9%)
PREEMPLOYMENT 1,577 (40.2%)
STUDENTS 891(22.75%)
OTHER (VOLUNTARY) 129 (4%)
TOTAL 3,915

Number of HIV Tests 2001-2004
Number of HIV Tests 2001-2004
Years 2001 2002 2003 2004
HIV Tests Performed
2970 3826 2387

Comparison between Majuro and Ebeye HIV Program
Comparison between Majuro and Ebeye HIV Program
NAME MAJURO EBEYE
POPULATION (+)35,000 (+)11,000
HIV (POSITIVE) CUMULATIVE (10) Only one case residing in Ebeye
SUBPOPULATION PREGNANT/STUDENT/ALIEN/
STD/F.HANDLERS/VOLUNTARY/
Taxi Driver
Same but not include taxi drivers
CME/OUTREACH PROGRAMS
Ongoing Activities On going Activities
DIAGNOSTIC TEST RAPID TESTS (SERODIA TEST)
CONFIRMATION (OFF ISLAND)
SAME
BARRIERS +++++ +++++
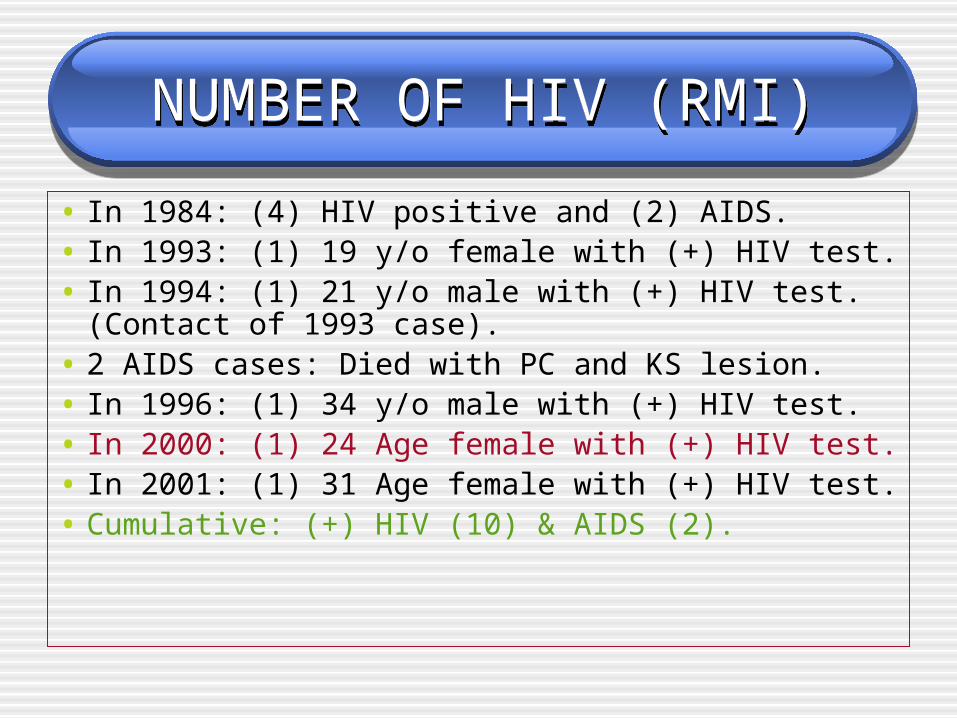
NUMBER OF HIV (RMI)NUMBER OF HIV (RMI)
• In 1984: (4) HIV positive and (2) AIDS.• In 1993: (1) 19 y/o female with (+) HIV test. • In 1994: (1) 21 y/o male with (+) HIV test.
(Contact of 1993 case).• 2 AIDS cases: Died with PC and KS lesion.• In 1996: (1) 34 y/o male with (+) HIV test.• In 2000: (1) 24 Age female with (+) HIV test.• In 2001: (1) 31 Age female with (+) HIV test. • Cumulative: (+) HIV (10) & AIDS (2).

MAJURO HIV PROGRAMMAJURO HIV PROGRAM
• In early 2004, encountered 2 HIV positive tests (one pregnant and one foodhandler).
• Two series of blood sample from both clients were taken in two different occasion and all HIV serodia tests were still positive.
• Samples were sent off island to Aloha Lab for confirmation. Result for the pregnant was negative for ELISA and the male client was indetermined.
• In two, four and six months period, male client was retest and serodia test turn negative.
• Pregnant client delivered a healthy baby girl and retest two weeks later and result was negative.

MAJURO HIV PROGRAMMAJURO HIV PROGRAM
• There was no positive test until early 2005, 17 y/o pregnant girl with two partners was reported to the program due to positive HIV test.
• Second blood sample was drawn for retest. Second sample was positive.
• Two partners were located and advise for HIV test. Both were negative.
• Multiple counseling sessions were conducted with the client with guidance and consultation with Dr. Amy Kindrick. (Thanks you, Dr. Kindrick)

MAJURO HIV PROGRAMMAJURO HIV PROGRAM
• Around that time, two positive HIV tests were detected. (couple).
• There were referred to my office for counseling and retest. They were seen at separate time. The male were complaining of diarrhea and weight lost but female partner was only experiencing weight lost 5-7 bounds.
• Both clients denies having other outside affair other than their previous partner many years ago.

MAJURO HIV PROGRAMMAJURO HIV PROGRAM• Blood samples for three clients(pregnant girl and
the couple) were sent off island (aloha lab) for confirmation.
• Confirmation was received on email on (date) with result positive for ELISA test and western blot.
• Post test counseling were conducted to all three client. Pregnant client was immediately called for post counseling and immediate family members were involved in the counseling session.

MAJURO HIV PROGRAMMAJURO HIV PROGRAM
• Plan for elective C-section was introduce and successfully agree with the pt and family members.
• On (date) patient underwent c-section without complication. Baby was tested for HIV and result was negative. Baby was on bottle feeding and remain to be on bottle until now.
• Follow up for mother and baby was conducted on two, four and six weeks postpartum.
• Mother was retest at four weeks postpartum and result was negative.

MAJURO HIV PROGRAMMAJURO HIV PROGRAM
• Meeting was conducted with the chief of laboratory and two other senior lab technicians.
• Recommendations to retest all positive HIV in one month period and any positive tests will be send off island for re-confirmation.
• Couple are still anxious on when to start the ARV. AVR procurement is still going with the new pharmacist on island working on it.
• Pregnant client doing fine and baby was taken to outer island by grandparent.

MAJURO HIV PROGRAMMAJURO HIV PROGRAM
• Around that time, the fourth positive HIV test was referred to my clinic.
• This is ?age taxi driver who is marriage and have multiple sexual partners.
• Two samples was positive for HIV test and both were sent to aloha lab for confirmation.
• In less than two weeks time, result come back negative for ELISA test.
• Until now, result hasn’t disclose to the patient.

Questions for discussion?Questions for discussion?• Why are we encountering too many false positive
confirmation?• How common is to get a false positive result?• How reliable or the effectiveness of the serodia test?
(specificity and sensitivity?)• Is Aloha lab a reference lab?or does CDC play role in
helping the islands to do confirmation tests?• Where are we in term of ARV procurement plan?
What is the role of AETC in this situation?• When do we disclose the result to patient?health
workers?family member?public?

ACCOMPHLISMENTS:ACCOMPHLISMENTS:
• Conduct a Lecture on STD/HIV to Churches Youth Groups. Congregational church on July 15, 2004 BNJ (Assumply of God Church) July 16,2004. Rita Assumply of God Church) July 17,2004 Total participants roughly around 300-350.
• Attend a VTC on HIV case presentation on July 28, 2005 via Peacesat Program.

ACCOMPHLISMENTS:ACCOMPHLISMENTS:
• Present a lecture on STD and HIV to YTYIH program (NGO) participants on July 22, 2005. ( 30 participants).
• SPC HIV surveillance specialist make a site visit on 10/2/2004 and recommends a new HIV database system to installed and BBS and SGS survey.
• Attended a PMTCT workshop in Fiji from October 21-22, 2004.

ACCOMPHLISMENTS:ACCOMPHLISMENTS:• World AIDS day activities on December 4, 2004. • December 4, 2004, approximately 600 to 700 participants
participate in the three site for the walkaton activities. • January 20,2005, conduct a lecture on HIV during the
teacher and principal workshop. (30+ teachers and principals attend the lecture)
• Presentation on the RMI HIV situational analysis by a visiting Medical Student from University of Auckland, New Zealand.
• VTC on HIV case presentation (AETC) on February15, 2005.
•

ACCOMPHLISMENTS.ACCOMPHLISMENTS.
March 3, 2005, gave a HIV lecture to the CMI Nursing Students. (Around 20 students).
Present the HIV positive case (17 y/o pregnant girl) to the medical staffs.
March 7-11 2005, HIV workshop by the Chuuck HIV team conducted. (97 participants from the MOH including medical staffs attended).

GHALLENGES/BARRIERSGHALLENGES/BARRIERS
• LACK OF MANPOWERS.• CLINICAL MANAGER IS WEARING TOO
MANY HATS (OVERWHELMING RESPONSIBILITY)
• OUT DATED PROTOCOL AND GUIDELINE.• NO ARV PROCUREMENT PLAN.• ENCOUNTERING TOO MANY FALSE
POSITIVE TEST.• NO ARV AGENTS FOR THE PMTCT.
ACCOMPHLISMENTS:ACCOMPHLISMENTS:
• LACK OF TRAINING. PRE AND POST COUNSELING. UNIVERSAL PRECAUTION. HIV 101/102 NO GUIDELINE FOR REFERRING CLIENT.
• STIGMA. CULTURAL BELIEF (SENSITIVE ISSUE TO AWARE THE
PUBLIC). SMALL POPULATION CONFIDENTIALITY. DISCLOSURE TO PT/HEALT WORKERS/FAMILY AND
PUBLIC.

RecommendationsRecommendations
• To install a new database system for better recording and surveillance.
• To do a need assessment for the HIV program by conducting a BBS and SGS survey.
• To upgrade and revise the existing HIV guideline and protocol.
• To increase the capacity building by performing more training to the staffs as well as to the medical staffs.
• To implement an accessible and feasible ARV procurement system.

RecommendationsRecommendations
• To expand the community outreach activities to the outer islands and remote villages.
• To link or network with Ebeye HIV program for sharing and collaborating work related activities like training and workshop.
• Increase the manpower and conduct counseling workshop.
• Implement HIV test on all TB clients.• To conduct a week Youth Community Workshop
in Majuro (Capital City).

Conclusion:Conclusion:

THE ENDTHE END
THANK YOU!!
QUESTIONS?
COMMENTS?





























