Embed Size (px)
Citation preview

HIV im Überblick – ART mit 2DR im Fokus
Dr. med. Dr. phil. Celia Jonsson-Oldenbüttel, Ärztliche Leitung

Financial Disclosure
Der Autor erklärt Berater-, Gutachter-, Vortragstätigkeit oder Teilnahme an Studien oder die Zuwendung für die Durchführung von Forschungsprojekten von folgenden
Unternehmen:
Abbvie, Gilead, Glaxo Smith Kline, Janssen-Cilag, ViiV Healthcare

Überblick
• Epidemiologie• Essentials HIV• Therapie HIV • 2 Drug Regimen• Outlook

Epidemiologie
https://www.who.int/docs/default-source/hiv-hq/2019-global-summary-web-v6fc86781480f44a439713a6f53b1aeb57.pptx

Epidemiologie Deutschland - ca. 90.700 Menschen mit HIV/AIDS
Geschätzte Zahl von Neuinfektionen in Deutschland im Jahr 20191
Gesamtzahl 2.600(2.400 – 2.900)
Männer 2.200(2.000-2.400)
Frauen 480(400-450)
Geschätzte Zahl von Erstdiagnosen in Deutschland im Jahr 20192
Gesamtzahl 3.300(3.100 – 3.400)
Fortgeschrittener Immundefekt3 1.100 (1.000-1.200)
Mit AIDS 510 (470-540)
Geschätzte Zahl von Todesfällen in Deutschland im Jahr 2019
Gesamtzahl 380(370-400)
1) HIV-Infektionen, die von Menschen mit Herkunft außerhalb Deutschlands im Ausland erworben wurden und spater in Deutschland diagnostiziert wurden („Auslandsinfektionen“), sind hier nicht enthalten. 2) Diese Schatzung wurde berechnet aus den gemeldeten Erstdiagnosen und einem Teil der unklaren Meldungen (nicht eindeutig als Erst- oder Doppelmeldung erkennbar). Im Unterschied zu der Zahl der HIV-Neuinfektionen enthalt die Zahl der HIV-Erstdiagnosen auch die in Deutschland diagnostizierten Auslandsinfektionen.
RKI Epi Bulletin 26. November2020/ Nr. 48, S. 487

Epidemiologie HIV-Neudiagnosen nach Transmissionsrisiko seit Beginn der HIV-Epidemie (1975 – 2019)
Epid Bull 2020; 48:3–16 | DOI 10.25646/7213

Überblick
• Epidemiologie• Essentials HIV• Therapie HIV • 2 Drug Regimen• Outlook

HIV Basics - Verlauf der unbehandelten HIV-Infektion
Akute HIV Infektion Asymptomatische Periode AIDS
CD4+ Zellzahl
6–12 Wochen 1–15+ Jahre 2–3 Jahre
Plasmaviruslast
Modifiziert nach Rowland-Jones, NatRevImmun 2003

Klinische Warnhinweise auf HIV – Akute HIV-Infektion
• Tage bis wenige Wochen nach Infektion
• 40–80% aller Fälle symptomatisch
Dauer der Symptomatik: 7-10 Tage
• Unspezifische Mononukleose-ähnliche Erkrankung
Fieber (38-40°C) ca. 80%
Abgeschlagenheit ca. 70%
Makulopapulöses Exanthem ca. 50%
schmerzhafte orale Ulzerationen ca. 40%
Pharyngitis ca. 40%
Lymphadenopathie k.A.
• Symptomatische Infektion: schlechtere Prognose
• Ursache für ca. 50% aller Neuinfektionen
• Wichtig: daran denken (Differentialdiagnose)!
• Bei Verdacht: Test veranlassen (Einwilligung Patient obligat)
Exanthem
Orale Ulzerationen
Lymphadenopathie
HIV 2014/2015. Hoffmann und Rockstroh. www.hivbuch.de

Klinische Warnhinweise auf HIV – Chronische HIV-Infektion (Indikatorerkrankungen)
• B – Symptomatik, Fatigue• Chronische Diarrhoe• Fieber unklarer Genese • Herpes zoster• Kaposi Sarkom• Orale Haarleukoplakie (OHL)• Oropharyngeale Candidose• Seborrhoische Dermatitis
• Sexuell übertragbare Erkrankungen
• Tuberkulose• Thrombozytopenie• Virushepatitiden
Herpes Zoster
Orale Haarleukoplakie (OHL)
Oropharyngeale CandidoseHIV 2014/2015. Hoffmann und Rockstroh. www.hivbuch.de

Überblick
• Epidemiologie• Essentials HIV• Therapie HIV • 2 Drug Regimen• Outlook

Ziele der HIV Therapie
Normalisierung der Lebenserwartung bei minimaler
Toxizität und Belastung
Infektionsbedingte
Symptome
unterdrücken
Krankheitsprogression
verringern
Rekonstitution der
zellulären Immunität
Chronische
Immunaktivierung
reduzieren
Dauerhafte
Suppression
der Viruslast
Deutsch-Österreichische Leitlinien zur antiretroviralen Behandlung der HIV-Infektion

Meilensteine der HIV Therapie
Zweifach
NRTI
CCR5 In
1987 1991 1993 1994 1995 1996 1997 1998 1999 200019881989 1990
NRTI
PI
NNRTI
2001 2002 2003
FI
2004
Mono
NRTI
Dreifach (HAART)
2 NRTI+PI 3 NRTI
2 NRTI + NNRTI
2005 2006
InI
20072008 2009 2010 … 2017 2018
2 NRTI + InI
NRTI = Nukleosidale Reverse Transkriptase Inhibitoren
NNRTI = Nicht-Nukleosidale Reverse Transkriptase Inhibitoren
PI = Protease Inhibitoren
InI = Integrase Inhibitoren
CCR5 In = CCR5 Inhibitoren
DTG basierte
2DR
2019
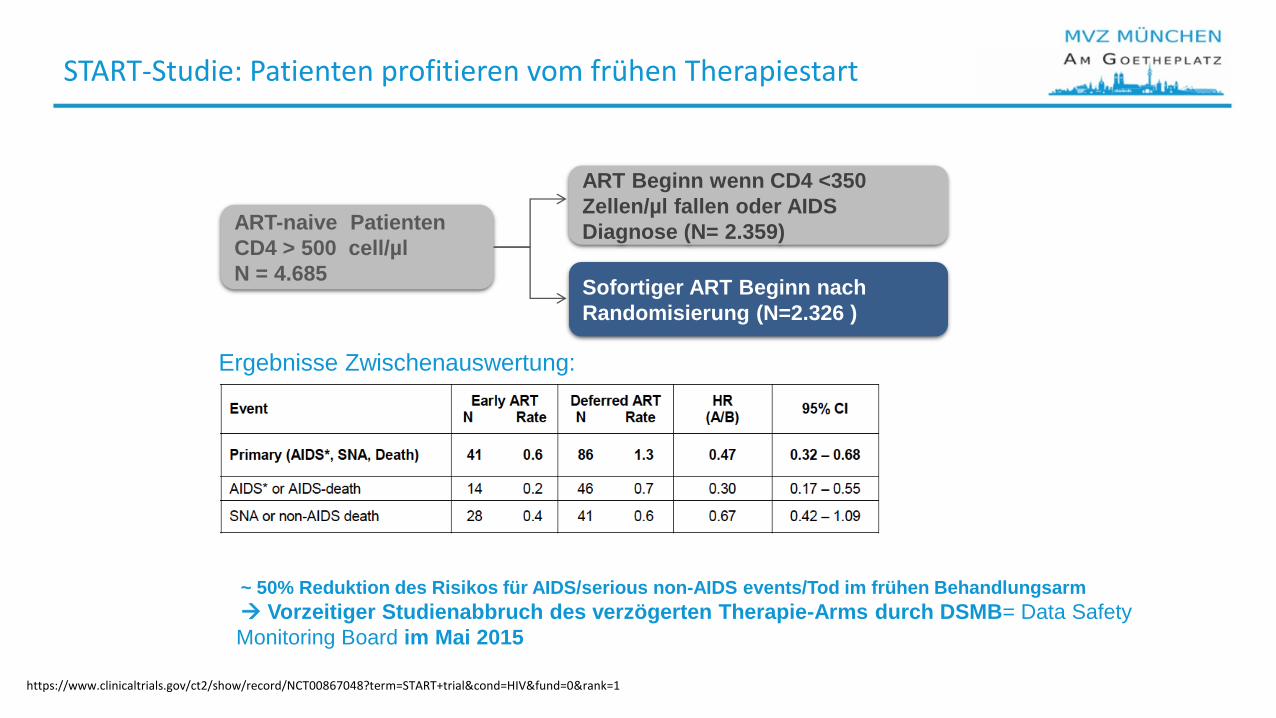
START-Studie: Patienten profitieren vom frühen Therapiestart
Sofortiger ART Beginn nach
Randomisierung (N=2.326 )
ART Beginn wenn CD4 <350
Zellen/µl fallen oder AIDS
Diagnose (N= 2.359)ART-naive Patienten
CD4 > 500 cell/µl
N = 4.685
Ergebnisse Zwischenauswertung:
~ 50% Reduktion des Risikos für AIDS/serious non-AIDS events/Tod im frühen Behandlungsarm
Vorzeitiger Studienabbruch des verzögerten Therapie-Arms durch DSMB= Data Safety
Monitoring Board im Mai 2015
https://www.clinicaltrials.gov/ct2/show/record/NCT00867048?term=START+trial&cond=HIV&fund=0&rank=1

Therapie der HIV Infektion Deutsch-österreichische Leitlinien 2020
Leitlinien — Deutsche AIDS Gesellschaft e.V. (daignet.de)

Überblick
• Epidemiologie• Essentials HIV• Therapie HIV • 2 Drug Regimen• Outlook

Kriterien der Deutsch-Österreichischen Leitlinien
• Hohe virologische Wirksamkeit und niedrige Rate an virologischem Versagen ...
• Wirksamkeit CD4-Zellzahl <200/μl und/oder HIV-RNA >100.000 Kopien/ml vor Beginn der Therapie
• Wirksamkeit im ZNS
• Rasches virologisches Ansprechen (HIV-RNA < Nachweisgrenze)
• Kein oder sehr seltenes Therapieversagen mit Resistenz in Studien
• Gute Verträglichkeit, insbesondere keine potenziell schwerwiegenden unerwünschten Arzneimittelwirkungen der eingesetzten Substanzen wie
• Geringe Einnahmefrequenz, niedrige Tablettenzahl, wenig pharmakokinetische Interaktionen und diätetische Restriktionen
• Anwendbarkeit, auch bei Komorbitäten oder Risikofaktoren für das Auftreten von KomorbiditätenDeutsch-Österreichische Leitlinien zur antiretroviralen Therapie der HIV-1-Infektion, AWMF 055-001, Version 9 vom 01.09.2020

Therapie
• 2 Drug Regimen
DTG + 3TCDTG + RPV

DTG/3TC Studienüberblick
DTG+3TC vs
TAF-based CAR
PADDLE1
n=20
ACTG53532,8
n=120
GEMINI-13,7
n=714
GEMINI-23,7
n=719
TANGO6
n=741
DTG+3TC
VL <100.000c/ml
Woche 48:
90%VL <50 c/ml
DTG+3TC
VL<500.000c/ml
Woche 24:
90%VL <50 c/ml
DTG+3TC vs
DTG+TDF/FTC
VL<500.000c/ml
Woche 48:
91%VL <50 c/ml
SUPPRESSED SWITCHTREATMENT-NAÏVE
non-inferior
Woche 48:
93%VL <50 c/ml
non-inferior
Woche 96:
86%VL <50 c/ml
Woche 96:
90%VL <50 c/ml
Woche 48:
85%VL <50 c/ml
LAMIDOL4
n=104
ASPIRE5
n=89
DTG+3TC
Woche 48:
97%VL <50 c/ml
DTG+3TC
vs CAR
Woche 48:
91%VL <50 c/ml
LAMIDOL ASPIRE
non-inferior
DOLAM9
n=131
DTG+3TC
vs CAR
Woche 48:
93%VL <50 c/ml
DOLAM
non-inferior
Phase III Phase IIIISS ISS ISS ISS ISS
1. Cahn P et al. J. of the Int. AIDS Society 2017, 20:21678; 2. Taiwo et al. CID 2018;66(11):1689–97; 3. Cahn et al. Lancet 2018; 4. Joly et al. Lamidol CROI 2017, Poster 458; 5. Taiwo et al. CID 2018;66(11):1794–7; 6. van Wyk et al. IAS 2019; Mexico City, Mexico. Slides WEAB0403LB 7. Cahn et al. IAS 2019; Mexico City, Mexico. Slides WEAB0404LB; 8. Nyako et al. J Antimicrob Chemother 2019; Rojas et al. AIDS 2020; Virtual. Poster PDB0105

GEMINI-1 and GEMINI-2 Study Design - Naive Patienten
.
DTG + 3TC (N=716)
Day 1
Screening (28 days)
DTG + TDF/FTC (N=717)
DTG + 3TC
Week48
Double-blind phase
Open-labelphase
Continuation phase
Week144
Week 24
Week96
• ART-naive adults
1:1
Primary endpoint
at Week 48:
participants with
HIV-1 RNA <50 c/mL
(ITT-E Snapshot)a
CountriesArgentina Australia Belgium
Canada France Germany
Italy Republic of Korea Mexico
Netherlands Peru Poland
Portugal Romania Russian Federation
South Africa Spain Switzerland
Taiwan United Kingdom United States
Eligibility criteria
• VL 1000-500,000 c/mL at screening
• ≤10 days of prior ART
• No major RT or PI resistance mutations
• No HBV infection or need for HCV therapy
Cahn et al. HIV Glasgow 2020; Virtual. Poster P018

Hohe Wirksamkeit - GEMINI-1 and GEMINI-2
Snapshot Analysis of the Proportion of Participants With Plasma HIV-1 RNA <50 c/mL through Week 144 by Visit in the Pooled ITT-E Population
DTG + 3TC was non-inferior to DTG + TDF/FTC in Snapshot HIV-1 RNA <50 c/mL for GEMINI-1, GEMINI-2, and the pooled population at Week 144
Cahn et al. HIV Glasgow 2020; Virtual. Poster P018.

Hohe virologische Wirksamkeit bei ART-naiven Patienten bei CD4-Zellzahl <200/μlund/oder HIV-RNA >100.000 Kopien/ml vor Beginn der Therapie
• At Week 144, in participants with baseline HIV-1 RNA >100,000 c/mL, 82% and 84% in the DTG + 3TC and DTG + TDF/FTC groups, respectively, achieved HIV-1 RNA <50 c/mL; among participants with baseline CD4+ cell count ≤200 cells/mm3, 67% in the DTG + 3TC group and 76% in the DTG + TDF/FTC group achieved HIV-1 RNA <50 c/mL
• The corresponding proportions were 81% and 84%, respectively, for those with baseline HIV-1 RNA ≤100,000 c/mL and 83% and 84%, respectively, for those with baseline CD4+ cell count >200 cells/mm3
.
Cahn et al. HIV Glasgow 2020; Virtual. Poster P018

Hohe Wirksamkeit in der TRDF Analyse
87 8890 9097 9797 96
84
68
86 8794 9395 96
0
20
40
60
80
100
• At Week 96, there were 3 confirmed virologic withdrawals in the DTG + 3TC group and 2 in the DTG + TDF/FTC group in the CD4 <200 cells/mm3 stratum
• TRDF, treatment-related discontinuation equals failure. aTRDF was a pre-planned analysis at Week 96. Percentages estimated from the TRDF Kaplan–Meier analysis.
>100,000≤100,000
Baseline HIV-1 RNA, c/mL
>200 ≤200
Baseline CD4+ cell count, cells/mm3
HIV
-1 R
NA
<5
0 c
/mL
or
wit
ho
ut
TRD
F, %
560/576
499/576
510/564
117/140
132/153
132/140
146/153
573/653
594/662
633/653
43/63
48/55
59/63
53/55
545/564
638/662 n/N
SnapshotDTG + 3TCDTG + TDF/FTC
TRDFDTG + 3TCDTG + TDF/FTC
van Wyk et al. IDWeek 2019; Washington, DC. Slides 2842

Reasons for Snapshot Nonresponse in the CD4+ ≤200 cells/mm3 (Wk 96)
• aOne other participant met the criteria for confirmed virologic withdrawal at Week 12 but was not reported at the Week 48 analysis because of a laboratory reporting error identified after the Week 48 analysis. This participant was not withdrawn as per protocol at the time and has been allowed to continue in the study (the participant has maintained virologic suppression from Week 24 and at the Week 96 Snapshot analysis).
DTG + 3TC (n=20/63) DTG + TDF/FTC (n=7/55)
Reason n Notes n Notes
Confirmed virologic withdrawala 3 1a
HIV-1 RNA ≥50 c/mL in window 2 1 resuppressed 0
Discontinued due to AEs related to treatment
1 Worsening of fatigue, anxiety, and irritability
0
Discontinued due to non-treatment related AEs
2 Tuberculosis, Chagas disease 0
Protocol violation 3 1 pregnancy and 2 incorrectly randomized
0
Lost to follow-upb 3 3
Withdrew consent 4 3 relocated and 1 due to non–treatment-related AE
2 1 relocated
Change in ARTb 1 Incarcerated 0
Investigator discretion 1 Started HCV treatment 1 Incarcerated
van Wyk et al. IDWeek 2019; Washington, DC. Slides 2842

GEMINI 1&2: Proportion of Participants With Plasma HIV-1 RNA <50 c/mL at Week 48(Snapshot Analysis) by Baseline Plasma HIV-1 RNA: Pooled ITT-E Population
80
83
89
90
94
85
89
88
92
91
0 20 40 60 80 100
>500,000 c/mL
>400,000 c/mL
>250,000 c/mL
>100,000 c/mL
≤100,000 c/mL
HIV-1 RNA <50 c/mL, %
Ba
se
line
vira
l lo
ad
str
ata
4,6
5,6
-0,9
1,9
-2,8
-30 -20 -10 0 10 20 30 40
Difference in proportion, % (95% CI)
DTG + 3TC (N=716) DTG + TDF/FTC (N=717)
138/153
41/46
20/24
12/15
531/564
DTG + TDF/FTC DTG + 3TC
129/140
45/51
16/18
11/13
526/576
Eron et al. HIV DART and Emerging Viruses 2018; Miami, FL. Oral Presentation #7.

Summary of AEs in the Pooled Safety Population (GEMINI-1 and GEMINI-2)
4 deaths occurred (3 in the DTG + 3TC group and 1 in the DTG + TDF/FTC group), all considered unrelated to the study drug regimen
Cahn et al. HIV Glasgow 2020; Virtual. Poster P018.

EACS Guidelines
Skin Digestive Liver CV Musculo-
skeletal
Genito-
urinary
Nervous Body fat Metabolic Other
NRTI
ABC Rash Nausea*
Diarrhoea*
IHD* HSRi
ZDV ii Nail
pigment.
Nausea Steatosis Myopathy
Rhabdo-
myolysis
Lipo-atrophy Dyslipid-aemia,
Hyperlactat-
aemia
Anaemia
3TC
FTC
Plasma
lipids
TDF iii BMD
Osteo-
malacia,
Fractures risk
eGFR,
Fanconi
Syndrome
TAF iii Weight
increase
EACS Guidelines Version 10.0, November 2019

Gute Resistenzbarriere
a1 participant met the criteria for CVW at Week 12 but was not reported at the Week 48 analysis because of a laboratory report ing error identified after the Week 48 analysis.
GEMINI-1 GEMINI-2 Pooled
Week Variable, n (%)
DTG + 3TC
(N=356)
DTG +
TDF/FTC
(N=358)
DTG + 3TC
(N=360)
DTG +
TDF/FTC
(N=359)
DTG + 3TC
(N=716)
DTG +
TDF/FTC
(N=717)
48 CVW 4 (1.1) 2 (0.6) 2 (0.6) 2 (0.6) 6 (0.8) 4 (0.6)
96 CVW 5 (1.4) 4 (1.1)a 6 (1.7) 3 (0.8) 11 (1.5) 7 (1.0)a
Treatment-emergent resistance
0 0 0 0 0 0
144 CVW 1 2Treatment-emergent resistance (CVW)* 0 0
* 1 non-CVW participant with reported non-adherence in the DTG + 3TC group developed M184V at Week 132 (HIV-1 RNA 61,927 c/mL) and R263R/K at Week 144 (HIV-1 RNA 135 c/mL), conferring a 1.8-fold change in susceptibility to DTG
van Wyk et al. IDWeek 2019; Washington, DC. Slides 2842., Cahn et al. HIV Glasgow 2020; Virtual. Poster P018.

Zusammenfassung Gemini Daten
Die Ergebnisse bestätigen, dass der Einsatz von DTG/3TC in der Initialtherpieeine dauerhaft hohe Wirksamkeit beiguter Verträglichkeit kombiniert mit einerhohen Resistenzbarriere bietet

DTG/3TC Studienüberblick
1. Cahn P et al. J. of the Int. AIDS Society 2017, 20:21678; 2. Taiwo et al. CID 2018;66(11):1689–97; 3. Cahn et al. Lancet 2018; 4. Joly et al. Lamidol CROI 2017, Poster 458; 5. Taiwo et al. CID 2018;66(11):1794–7; 6. van Wyk et al. IAS 2019; Mexico City, Mexico. Slides WEAB0403LB 7. Cahn et al. IAS 2019; Mexico City, Mexico. Slides WEAB0404LB; 8. Nyako et al. J Antimicrob Chemother 2019; Rojas et al. AIDS 2020; Virtual. Poster PDB0105
DTG+3TC vs
TAF-based CAR
PADDLE1
n=20
ACTG53532,8
n=120
GEMINI-13,7
n=714
GEMINI-23,7
n=719
TANGO6
n=741
DTG+3TC
VL <100.000c/ml
Woche 48:
90%VL <50 c/ml
DTG+3TC
VL<500.000c/ml
Woche 24:
90%VL <50 c/ml
DTG+3TC vs
DTG+TDF/FTC
VL<500.000c/ml
Woche 48:
91%VL <50 c/ml
SUPPRESSED SWITCHTREATMENT-NAÏVE
non-inferior
Woche 48:
93%VL <50 c/ml
non-inferior
Woche 96:
86%VL <50 c/ml
Woche 96:
90%VL <50 c/ml
Woche 48:
85%VL <50 c/ml
LAMIDOL4
n=104
ASPIRE5
n=89
DTG+3TC
Woche 48:
97%VL <50 c/ml
DTG+3TC
vs CAR
Woche 48:
91%VL <50 c/ml
LAMIDOL ASPIRE
non-inferior
DOLAM9
n=131
DTG+3TC
vs CAR
Woche 48:
93%VL <50 c/ml
DOLAM
non-inferior
Phase III Phase IIIISS ISS ISS ISS ISS
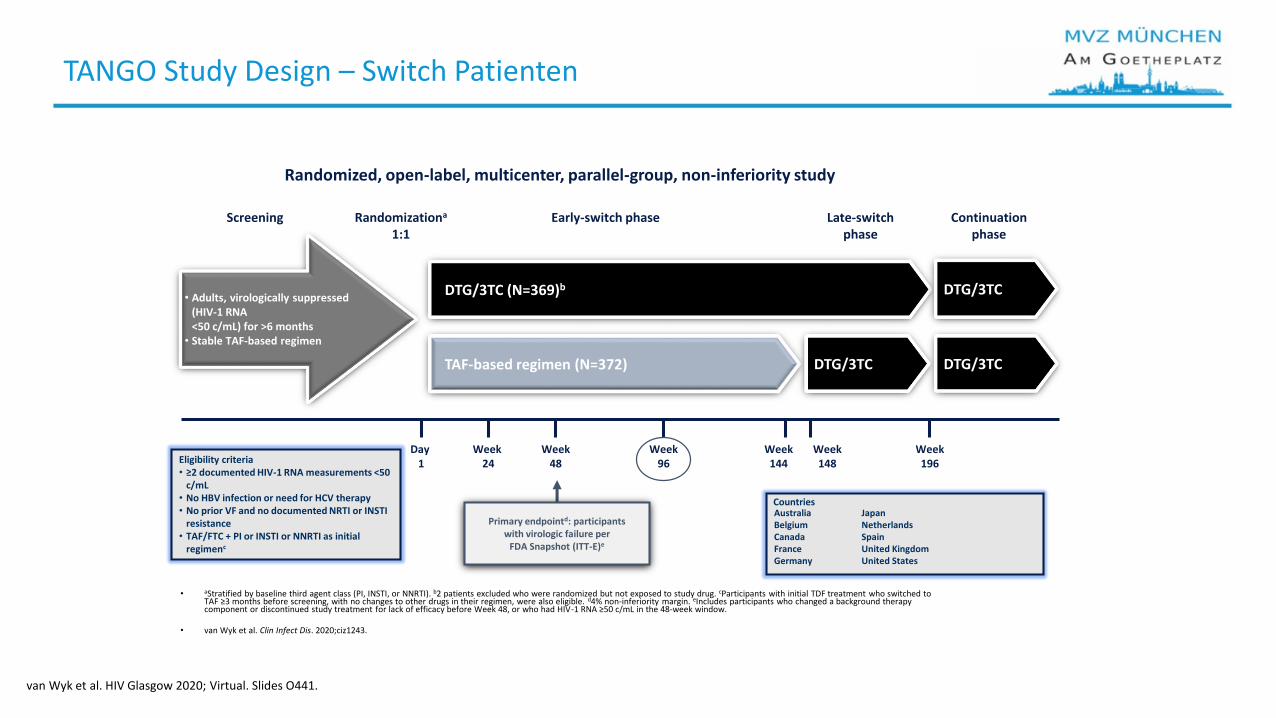
TANGO Study Design – Switch Patienten
• aStratified by baseline third agent class (PI, INSTI, or NNRTI). b2 patients excluded who were randomized but not exposed to study drug. cParticipants with initial TDF treatment who switched to TAF ≥3 months before screening, with no changes to other drugs in their regimen, were also eligible. d4% non-inferiority margin. eIncludes participants who changed a background therapy component or discontinued study treatment for lack of efficacy before Week 48, or who had HIV-1 RNA ≥50 c/mL in the 48-week window.
• van Wyk et al. Clin Infect Dis. 2020;ciz1243.
Randomized, open-label, multicenter, parallel-group, non-inferiority study
DTG/3TC (N=369)b
Day 1
Screening
TAF-based regimen (N=372)
DTG/3TC
Week48
Early-switch phase Late-switch phase
Continuation phase
Week144
Week 24
Week96
• Adults, virologically suppressed (HIV-1 RNA<50 c/mL) for >6 months
• Stable TAF-based regimen
Randomizationa
1:1
Week 148
Week196
DTG/3TC DTG/3TC
Primary endpointd: participantswith virologic failure per
FDA Snapshot (ITT-E)e
Eligibility criteria• ≥2 documented HIV-1 RNA measurements <50
c/mL• No HBV infection or need for HCV therapy• No prior VF and no documented NRTI or INSTI
resistance• TAF/FTC + PI or INSTI or NNRTI as initial
regimenc
AustraliaBelgiumCanadaFranceGermany
JapanNetherlandsSpainUnited KingdomUnited States
Countries
van Wyk et al. HIV Glasgow 2020; Virtual. Slides O441.
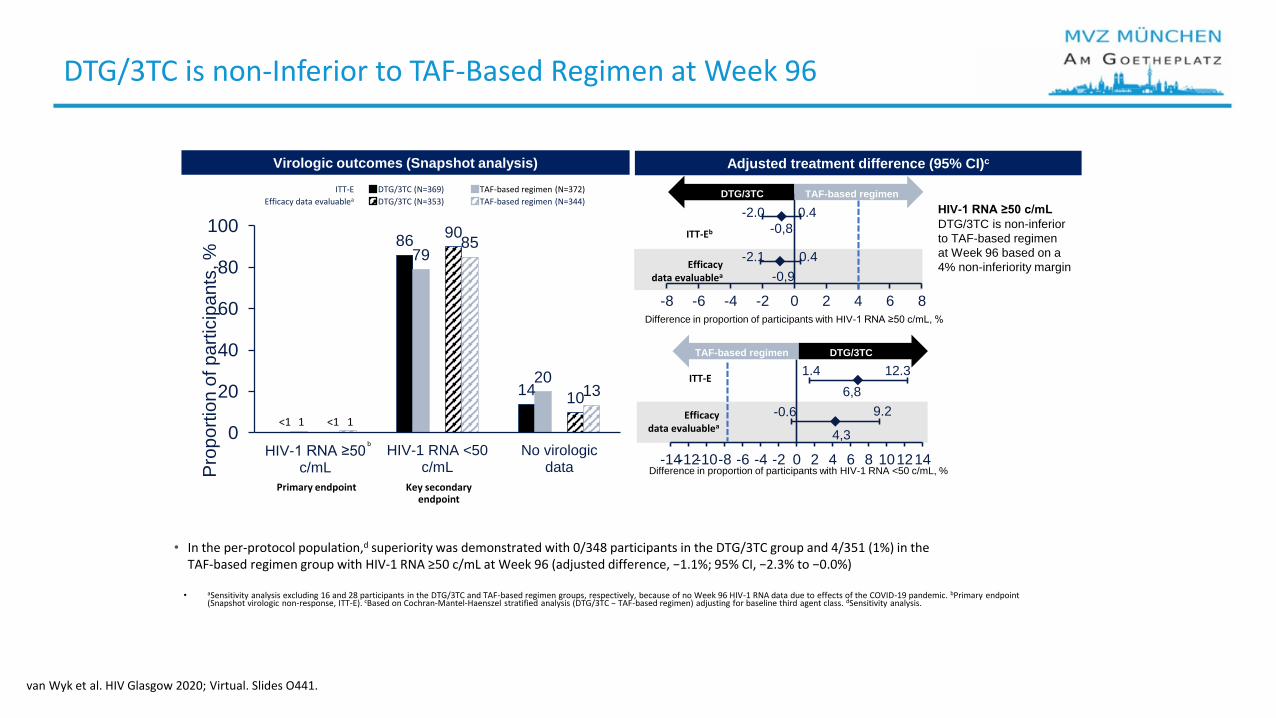
DTG/3TC is non-Inferior to TAF-Based Regimen at Week 96
6,8
4,3
-14-12-10-8 -6 -4 -2 0 2 4 6 8 101214
-0.6 9.2
1.4 12.3
-0,8
-0,9
-8 -6 -4 -2 0 2 4 6 8
-2.1 0.4
-2.0 0.4
86
14
79
20
90
10
85
13
0
20
40
60
80
100
HIV-1 RNA ≥50 c/mL
HIV-1 RNA <50c/mL
No virologicdataP
rop
ort
ion
of p
art
icip
an
ts, %
• aSensitivity analysis excluding 16 and 28 participants in the DTG/3TC and TAF-based regimen groups, respectively, because of no Week 96 HIV-1 RNA data due to effects of the COVID-19 pandemic. bPrimary endpoint (Snapshot virologic non-response, ITT-E). cBased on Cochran-Mantel-Haenszel stratified analysis (DTG/3TC − TAF-based regimen) adjusting for baseline third agent class. dSensitivity analysis.
Virologic outcomes (Snapshot analysis) Adjusted treatment difference (95% CI)c
Difference in proportion of participants with HIV-1 RNA <50 c/mL, %
TAF-based regimen
HIV-1 RNA ≥50 c/mL
DTG/3TC is non-inferior
to TAF-based regimen
at Week 96 based on a
4% non-inferiority margin
DTG/3TC
TAF-based regimen DTG/3TC
ITT-E DTG/3TC (N=369) TAF-based regimen (N=372)
Efficacy data evaluablea DTG/3TC (N=353) TAF-based regimen (N=344)
<1<1 1 1
b
ITT-Eb
Efficacy data evaluablea
ITT-E
Efficacy data evaluablea
Difference in proportion of participants with HIV-1 RNA ≥50 c/mL, %
Primary endpoint Key secondary endpoint
• In the per-protocol population,d superiority was demonstrated with 0/348 participants in the DTG/3TC group and 4/351 (1%) in the TAF-based regimen group with HIV-1 RNA ≥50 c/mL at Week 96 (adjusted difference, −1.1%; 95% CI, −2.3% to −0.0%)
van Wyk et al. HIV Glasgow 2020; Virtual. Slides O441.

Summary of Adverse Events Between Weeks 48 and 96: Safety Population
Adverse events reported after the end of the Week 48 analysis window are summarized. Participants who discontinued before the end of the Week 48 analysis window were excluded
71
27
2
70
27
10
20
40
60
80
100
All AEs Drug-related AEs Serious AEs AEs leading todiscontinuation
Part
icip
ants
, %
DTG/3TC (n=342) TAF-based regimen (n=342)
Rates of adverse events occurring between Weeks 48 and 96 were similar between treatment groups
van Wyk et al. HIV Glasgow 2020; Virtual. Slides O441.

No Confirmed Virologic Withdrawals With DTG/3TC Through Week 96
• a1 assessment with HIV-1 RNA ≥200 c/mL after Day 1 with an immediately prior HIV-1 RNA ≥50 c/mL.
Confirmed virologic withdrawal (CVW),a n (%)DTG/3TC (N=369)
TAF-based regimen(N=372)
Week 48 0 1 (<1)
Week 96 0 3 (<1)
No resistance mutations observed among participants with confirmed virologic withdrawal in the TAF-based regimen group
van Wyk et al. HIV Glasgow 2020; Virtual. Slides O441.

Change in Serum Lipids From Baseline at Week 96: Safety Population
Changes in total cholesterol, LDL cholesterol, and triglycerides significantly favored the DTG/3TC group; changes in HDL cholesterol favored the TAF-based regimen group
-3,9 -3,3 -4,3-…
-0,5
1,60
1,4
6.5
1,7
-15
-10
-5
0
5
10
15
Totalcholesterol(mmol/L)
HDLcholesterol(mmol/L)
LDL cholesterol(mmol/L)
Triglycerides(mmol/L)
Totalcholesterol/
HDLcholesterol
ratio
Ad
juste
d c
ha
ng
e fro
m
ba
se
line
(9
5%
CI)
, %
b**
** **
DTG/3TC (n=238)a TAF-based regimen (n=213)a
van Wyk et al. HIV Glasgow 2020; Virtual. Slides O441.

Zusammenfassung Tango Daten
Die Ergebnisse bestätigen, dass auch der Wechsel auf DTG/3TC eine dauerhafteWirksamkeit bei guter Verträglichkeitmit einer hohen Resistenzbarriere bietet

Real Life Daten
• 2 Drug Regimen -Real life
URBAN

Dolutegravir + 3TC im Therapiealltag in Deutschland
• Einschluss von therapienaiven und vorbehandelten Patienten, für die entsprechenddem Label eine Therapie mit Dolutegravir + 3TC möglich ist
• N = 366 insgesamt (n = 31 therapienaive Patienten; n = 335 vorbehandelte Patienten)
• Rekrutierungsstart: 11/2018
• Beobachtungsdauer 3 Jahre
• Primärer Endpunkt: Anteil der Patienten mit supprimierter Viruslast <50 Kopien/ml
• Sekundäre Endpunkte (Auswahl): Anteil der Patienten mit Blips, Anteil der Patientenmit Resistenzentwicklung, Nebenwirkungen, Patientenzufriedenheit, Anzahl der Monitoringsmaßnahmen
• Status: Rekrutierung abgeschlossen
Description of Real World Antiviral Effectiveness and Sustainability of the 2-Drug Regimen Dolutegravir + Lamivudine in Untreated and Pre-treated Patients in Routine Clinical Care in Germany
https://clinicaltrials.gov/ct2/show/NCT03754803?term=URBAN&recrs=ab&cond=HIV%2FAIDS&rank=8,Noe et al. KIT 2020, Abstract A-116

Zusammenfassung Urban
• DTG/3TC zeigte mit 95% im ersten halben Jahr eine hoheAkzeptanz in ART-naiven und therapieerfahrenen Patienten
• Eine virale Suppression wurde in 90% bei therapienaivenPatienten und 94% in vorbehandelten Patienten erreicht
• Patienten berichteten von einer signifikanten Verbesserungbezüglich der Therapiezufriedenheit in den ersten Monaten

Überblick
• Epidemiologie• Essentials HIV• Therapie HIV • 2 Drug Regimen• Outlook

Outlook
#AIDS2018 | @AIDS_conference | www.aids2018.org
Technology for Drug Delivery
Long-acting depot injections
Subdermal implant
Vaginal rings
Microneedle drug patch
Wearable infusion pump
Novel oral formulations
New drug delivery systems: The promise of long-acting ART
Kimberly K. Scarsi, PharmD, MSc

Zusammenfassung 2 Drug Regimen
• Epidemiologie: ca. 90.700 Menschen mit HIV/AIDS in Deutschland und 3300 Neuinfektionen in 2019
• Essentials HIV: Indikatorerkrankungen beachten
• Therapie: Früher Therapiestart wichtig
• 2 DR Regimen: Therapien mit hoher Wirksamkeit bei geringem NW Profil und hoher Resistenzbarriere -2 DR besonders geeignet und Leitlinienkonform
• Neue Therapien ante portas

HIV-Therapie im Überblick – ART mit 2DR im Focus
„The less toxic drug is the one that you do not take“
Pérez-Valero, EACS 2017 PS01 Antiretroviral

Transparenzinformation
Diese Fortbildung wird Ihnen auf cme.medlearning.de mit freundlicher Unterstützung von ViiV Healthcare GmbH angeboten (€ 10.650).





























