Embed Size (px)
Citation preview

HIT-MED Guidance for Patients
with newly diagnosed
Medulloblastoma
Ependymoma
CNS Embryonal Tumour* and
Pineoblastoma
Version 4.0
Attention: The guidance given here describes current treatment strategies used in Austria and Germany for patients with
medulloblastoma, ependymoma, non-rhabdoid embryonal tumour of the CNS and pineoblastoma. The described
principals are based on the treatment used in the previous HIT studies and this guidance does not represent a systematic
review of available treatment options. All therapeutic decisions need to be adapted to the individual patient and to the
local experiences.
All treatment regimens have been developed for primary (first-line) treatment of newly diagnosed patients without
additional risk-factors. Therefore even selected elements from these regimens should not be applied at tumour
progression or relapse, or in pretreated patients. All guidelines for application and dose-modifications given in chapters
7 and 8 must be carefully considered. The medical therapy must be conducted only by individuals with the appropriate
training and qualifications and in appropriate paediatric oncology centres.
Although the guidance has been written and checked carefully, the authors cannot guarantee correctness and do not
assume any liability for the content. If you detect a mistake or if you have any doubts, please contact the HIT-MED study
centre.
The guidance does not substitute individual responsibility of the treating physicians for the entire treatment, selection of
drugs, doses, timing, application, and management of side-effects and adverse reactions. It also does not replace the
need of any other required medical assessment of every patient, nor the requirement of fully informing the patient about
the treatment, and obtaining written consent. The sole responsibility for the treatment lies with the treating physicians.
All rights reserved. The guidance is the property of the authors and protected by copyright.
Universitätsklinikum Hamburg-Eppendorf © Stand 06/2017
* meaning all non-rhabdoid embryonal CNS tumours other than medulloblastoma in this whole guidance

HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 1
Treatment Stratification Medulloblastoma (2.1) Not all possible constellations are described
Age Histological
subtype
Molecular
subgroup
Metas-
tasis
Therapy recommendation Page
< 3 y CMB Group 3/4 M0 Intensified Induction chemotherapy
with response-adjusted consolidation
(b)
or SKK chemotherapy without i.vtr.
MTX (a)
20 or
19
< 4 y LCA Group 3/4
(SHH)
M0/M+ Intensified Induction chemotherapy with
response-adjusted consolidation (b)
– genetic counselling in case of SHH –
20
CMB M+ ± R >
1.5 cm²
< 5 y DMB/MBEN SHH M0/M+ SKK chemotherapy with i.vtr. MTX (a)
– genetic counselling in case of SHH –
19
> 3 y
to
21 y
CMB
(DMB > 5 y)
WNT, SHH,
Group 3/4
M0R0 (R+) – eligible for PNET 5 MB –
Conventional RT (23.4 Gy CSI + boost)
with Maintenance chemotherapy (c)
– genetic counselling in case of SHH –
21
> 4 y
to
21 y
any
(DMB > 5 y)
WNT, SHH,
Group 3/4
M2/3 Two cycles SKK chemotherapy with
HFRT (40 Gy CSI + boost) and
Maintenance chemotherapy (e)
– genetic counselling in case of SHH –
23
no M2/3, but any of the following
features:
LCA, MYC/N amplification, M1
(R > 1.5 cm²)
Conventional RT, enhanced dose (35.2 Gy
CSI + boost) with Maintenance
chemotherapy (d)
– genetic counselling in case of SHH –
22
Ependymoma (2.2) Age Metastasis Residual
tumour
Therapy recommendation
– check eligilibity for EPENDYMOMA II –
Page
< 1.5 y M0 R0 Five cycles SKK chemotherapy with local RT (54 Gy) (h) 24
> 1.5 y to
21 y
M0 R0 Local 59.4 Gy conventional or 68 Gy HFRT (local 59.4 Gy
conventional RT for children < 4 years) (i)
26
all until
21 y
M0 R > 0.5 cm²
Two cycles Modified SKK chemotherapy and re-surgery with
local RT (f)
– only if a 2nd surgery would become feasible –
24
all until
21 y
M+ all individual (j)
CNS embryonal tumour (2.3) Age Histology Metastasis Therapy recommendation Page
< 4 y ETMR M0/M+ CARBO/ETO-96h induction with response-adjusted
consolidation (k)
27
≥ 4 y to
21 y
Pineoblastoma M0 Conventional RT, enhanced dose (35.2 Gy CSI + boost) with
Maintenance chemotherapy (l)
22
Pineoblastoma M+ Two cycles SKK chemotherapy with HFRT (40 Gy CSI +
boost) and Maintenance chemotherapy (m)
23

HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 2
Authors: B.-Ole Juhnke
Martin Mynarek
Katja von Hoff
Sabine Klagges (radiotherapy)
Rolf-D. Kortmann (radiotherapy) and
Stefan Rutkowski
for the HIT-MED study committee
The HIT-MED study centre is supported by
Deutsche Kinderkrebsstiftung
Damp Stiftung
Fördergemeinschaft Kinderkrebs-Zentrum Hamburg e. V.

Preface
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 3
Preface This document is provided by the HIT-MED study centre in Hamburg, Germany. The guidance given
here describes current treatment strategies used in Austria and Germany for patients with
medulloblastoma, ependymoma, non-rhabdoid embryonal tumour of the CNS and pineoblastoma. The
described principals are based on the treatment used in the previous HIT studies and this guidance
does not represent a systematic review of available treatment options. The HIT-MED study centre does
not guarantee correctness of all doses or timing and does not assume any liability for the content of
this guidance. All treatment regimens have been developed for primary (first-line) treatment of newly
diagnosed patients without additional risk-factors. Therefore even selected elements from these
regimens should not be applied at tumour progression or relapse, or in pretreated patients. All
guidelines for application and dose-modifications given in chapters 7 and 8 must be carefully considered. The medical therapy must be conducted only by individuals with the appropriate training
and qualifications and in appropriate paediatric oncology centres.
Treatment recommendations in paediatric oncology are subject to constant change and update
frequently. Please register at [email protected] in order to make sure you will receive all updates of
this document.
The administration of the therapies described in this document requires expert experience in
paediatric oncology in order to prevent the patient from an unjustified risk of complications. Improper
patient management or application errors may result in the patients’ death. Moreover, serious
complications may occur even if the therapy is correctly administered. Therefore, sufficient measures have to be undertaken by the treating institution to prevent, recognize and treat these complications.
By using these treatment recommendations, the user accepts full responsibility for the consequences
of the treatment and declares that he/she has sufficient knowledge and sufficient institutional
support to manage this therapy and its complications. All therapeutic decisions need to be adapted to
the individual patient and to the local experiences. The guidance does not substitute individual
responsibility of the treating physicians for the entire treatment, selection of drugs, doses, timing,
application, and management of side-effects and adverse reactions. It also does not replace the need
of any other required medical assessment of every patient, nor the requirement of fully informing the
patient about the treatment, and obtaining written consent. The sole responsibility for the treatment
lies with the treating physicians.
This document focuses on the description of postoperative chemotherapy and radiotherapy.
Supportive therapy (including fluid management, antiemetic treatment and infection prophylaxis) has
to be defined by the responsible physician.
All described therapeutic schedules and therapeutic elements are based on the German multicentre
experience with the HIT2000, HIT’91 and HIT-SKK therapy studies. They may serve as a guidance for
the treatment of patients, who cannot be treated within a prospective trial. They are described for
informative reasons only. Selection and application of the appropriate treatment can only be made by
the responsibility of the treating paediatric oncologist. For many of the drugs described here, formal approval by the drug regulatory affairs is not available for children with brain tumour.
Surveillance of toxicity and efficacy is an important task in rare diseases. Physicians are encouraged
to use available systems for the documentation of these effects, e.g. national cancer registries or
drug safety committees (e. g. Drug Commission of the German Medical Association in Germany).
Although the guidance has been written and checked carefully, the authors cannot guarantee
correctness and do not assume any liability for the content. If you detect a mistake or if you have any
doubts, please contact the HIT-MED study centre.

Preface
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 4
Contact details HIT-MED study centre:
Prof. Dr. Stefan Rutkowski, Dr. Katja von Hoff
Dr. Martin Mynarek, B.-Ole Juhnke Clinical Trial Manager: Regine Riechers
Data Manager: Susanne Becker
Antje Stiegmann
Address: Clinic for Paediatric Haematology and Oncology
University Medical Centre Hamburg-Eppendorf
Martinistraße 52
D-20246 Hamburg
Phone: +49-40/7410-58200
Fax: +49-40/7410-58300
Email: [email protected]
Contact details Radiotherapy reference centre:
Prof. Dr. Rolf-D. Kortmann, Dr. Sabine Klagges
Address: Clinic for Radiotherapy and Radiooncology
University Clinical Centre Leipzig
Stephanstraße 9a
D-04103 Leipzig

Table of contents
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 5
Table of Contents 1. Introduction ..................................................................................................................................... 9
2. Stratification and standard Treatment Recommendations .......................................................... 10
2.1. Medulloblastoma ................................................................................................................. 10
2.2. Ependymoma (intracranial) ................................................................................................. 12
2.3. CNS Embryonal Tumour NOS, ETMR (both formerly CNS-PNET) and Pineoblastoma......... 14
3. Results of other prospective clinical Trials and planned international Studies (SIOP-E) .............. 15
3.1. Medulloblastoma ................................................................................................................. 15
3.2. Ependymoma ....................................................................................................................... 16
3.3. CNS Embryonal Tumour and Pineoblastoma ....................................................................... 17
4. Therapy Flowcharts ....................................................................................................................... 18
4.1. SKK chemotherapy ............................................................................................................... 19
4.2. Intensified Induction chemotherapy with response-adjusted consolidation ...................... 20
4.3. Conventional RT (23.4 Gy CSI + boost) with Maintenance chemotherapy .......................... 21
4.4. Conventional RT, enhanced dose (35.2 Gy CSI + boost) with Maintenance chemotherapy 22
4.5. Two cycles SKK chemotherapy with HFRT (40 Gy CSI + boost) and Maintenance
chemotherapy ................................................................................................................................... 23
4.6. Two cycles Modified SKK chemotherapy and re-surgery with local RT ............................... 24
4.7. Five cycles SKK chemotherapy with local RT (54 Gy) ........................................................... 25
4.8. Local 59.4 Gy conventional or 68 Gy HFRT (local 59.4 Gy conventional RT for children < 4
years) 26
4.9. CARBO/ETO-96h induction with response-adjusted consolidation ..................................... 27
5. Chemotherapy Documentation Sheets ......................................................................................... 28
5.1. Documentation sheet SKK chemotherapy ........................................................................... 29
5.2. Documentation sheet Modified SKK chemotherapy ........................................................... 30
5.3. Documentation sheet Maintenance chemotherapy ........................................................... 31
5.4. Documentation sheet Intensified Induction chemotherapy ............................................... 32
5.5. Documentation sheet CARBO/ETO-96h chemotherapy ...................................................... 33
5.6. Documentation sheet Tandem high-dose chemotherapy (1st HDCT and 2nd HDCT) ........... 34
6. Surgery recommendations ............................................................................................................ 35
6.1. Interventions for elevated intracranial pressure ................................................................. 35
6.2. Tumour resection ................................................................................................................. 35
6.3. Further surgery/surgery for residual tumours ..................................................................... 36
6.4. Implantation of Rickham or Ommaya reservoir .................................................................. 36
7. Description of radiotherapy elements .......................................................................................... 38
7.1. Medulloblastoma, CNS Embryonal Tumour and Pineoblastoma ........................................ 39

Table of contents
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 6
7.2. Ependymoma ....................................................................................................................... 46
7.3. Dose Constraints and Organs at Risk for Medulloblastoma, Ependymoma, CNS Embryonal
Tumour and Pineoblastoma .............................................................................................................. 51
8. Description of chemotherapy elements ........................................................................................ 53
8.1. Maintenance chemotherapy Cisplatin/Lomustine/Vincristine ............................................ 53
8.2. SKK chemotherapy ............................................................................................................... 56
8.3. Intensified Induction chemotherapy ................................................................................... 64
8.4. Carboplatin/Etoposide-96h chemotherapy ......................................................................... 67
8.5. Tandem high-dose chemotherapy ....................................................................................... 69
8.6. Intraventricular Methotrexate ............................................................................................. 73
8.7. Leucovorin rescue after intravenous high-dose Methotrexate ........................................... 77
9. Members of the HIT-MED study committee ................................................................................. 81
10. History of changes ..................................................................................................................... 82
10.1. Version 1.0 ........................................................................................................................... 82
10.2. Version 2.0 ........................................................................................................................... 82
10.3. Version 3.0 ........................................................................................................................... 82
10.4. Version 4.0 ........................................................................................................................... 83
Publication bibliography ........................................................................................................................ 85

Abbreviations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 7
Abbreviations
AMB Anaplastic Medulloblastoma
CARBO Carboplatin
CDDP Cisplatin
CMB Classic Medulloblastoma
CNS Central Nervous System
CNS-PNET Central Nervous System Primitive Neuroectodermal Tumour
CRF Case Record Form
CSF Cerebrospinal Fluid
CT Computed Tomography
CR Complete Response
CSI Craniospinal Irradiation
CSRT Craniospinal Radiation Therapy
CTV Clinical Target Volume
CYCLO Cyclophosphamide
DMB Desmoplastic Medulloblastoma
DRBE Direct Radiobiological Effectiveness
DTI Diffusion Tensor Imaging
DTPA Diethylene Triamine Pentaacetic Acid
DVH Dose Volume Histogram
e. g. exempli gratia (Latin for the sake of example)
EC European Committee
EDC Electronic Data Capture
EFS Event-Free Survival
ETO Etoposide
FDA Food and Drug Administration
FLAIR Fluid Attenuated Inversion Recovery
FSD Focus to Surface Distance
GCP Good Clinical Practice
GPOH Gesellschaft für Pädiatrische Onkologie und Hämatologie
GTR Gross Total Resection
GTV Gross Tumour Volume
Gy Gray
HART Hyperfractionated Accelerated Radiation Therapy
HFRT Hyperfractionated Radiation Therapy
HIT Hirntumoren (German brain tumours)
i. e. id est (Latin that is)
i. v. intra-venous
i. vtr. intra-ventricular
ICH International Conference on Harmonisation
ICRU International Commission on Radiation Units and Measurements
IMP Improvement
IMRT Intensity Modulated Radiation Therapy
LCA Large-Cell/Anaplastic Medulloblastoma
LCMB Large-Cell Medulloblastoma
M0 no metastasis
M+ metastasis

Abbreviations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 8
M1 CSF metastasis
M2 cranial metastasis
M3 spinal metastasis
M4 metastasis outside the central nervous system
MB Medulloblastoma
MBEN Medulloblastoma with Extensive Nodularity
MED Medulloblastoma, Ependymoma, Diverse
MeV Mega-electron Volt
MRI Magnetic Resonance Imaging
MRS Magnetic Resonance Spectroscopy
MTX Methotrexat
MYC human regulator gene for transcription factor c-myc
MYCN human regulator gene for transcription factor n-myc
NTR Near-Total Resection
OAR Organs At Risk
PD Progressive Disease
Pineo Pineoblastoma
PNET Primitive Neuroectodermal Tumour
PR Partial Response
PTV Planning Target Volume
QA Quality Assurance
R0 without residual disease
R+ with residual disease
RBE Radiobiological Effectiveness
RDE Remote Data Entry
RT Radiation Therapy
SAD Source-to-Axis Distance
SD Stable Disease
SIOP-E Société Internationale d’Oncologie Pédiatrique – Europe
SKK Säuglinge und Kleinkinder (German babies and infants)
STR Sub-Total Resection
TMZ Temozolomide
TSE Turbo Spin Echo
TT Thiotepa
VCR Vincristine
VMAT Volumetric intensity Modulated Arc Therapy
VP Ventriculoperitoneal
WBC White Blood Cells
WHO World Health Organisation
WNT WNT signalling

Introduction
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 9
1. Introduction The therapy recommendations given here are based on the experience obtained during the HIT2000
trial, which was open for recruitment between 01.01.2001 and 31.12.2011 in Austria, Germany and
Switzerland. Feasibility of these treatment concepts has been shown in a multi-institutional setting
with far more than 50 experienced contributing centres.
After the end of the inclusion period of HIT2000, the HIT-MED study group committee agreed on these
therapy recommendations with the aim to give an update on current treatment strategies to the
participating centres of HIT2000. The recommendations were originally written to guide physicians in
Austria, Germany and Switzerland and were most recently reviewed in 2016. These recommendations
for historical reasons base on the therapy elements described and used in HIT2000 (and the preceding
trials HIT’91 and HIT-SKK’92) and have been modified according to published results of HIT2000 and
other brain tumour trials and according to unpublished preliminary results of HIT2000. Evidence for
most recommendations is limited, as well-designed, randomised controlled trials are lacking. Results
of case series and sometimes personal opinion of the members of the HIT-MED study committee were
also considered, where no better evidence was available.
The HIT2000 trial included central review for histopathology, neuroradiology and CSF cytology as well
as central quality control for radiotherapy. These measures also have proven their feasibility in this
setting and are considered standard of care by the brain tumour network (HIT) of the German Society
of Paediatric Oncology and Haematology (GPOH). Therefore, a central review of these critical results
by independent experienced specialists is strongly recommended for all patients with brain tumours.

Stratification and standard Treatment Recommendations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 10
2. Stratification and standard Treatment Recommendations
2.1. Medulloblastoma
Please note: Eligibility for the PNET 5 Medulloblastoma trial should be carefully evaluated according
to national policy in all national groups, in which PNET 5 Medulloblastoma is open for recruitment.
Please consider genetic counselling in case of SHH-pathway activation (Fanconi anaemia, Gorlin-Goltz
syndrome, Li-Fraumeni syndrome etc.) before radiotherapy, according to national laws. As possible,
PTCH/SUFU and TP53 germline mutations should be excluded prior to the start of radiotherapy. You
may contact the HIT-MED study centre for discussion of therapy alternatives for patients with
predisposition syndromes.
Age Histological
subtype
Molecular
subgroup
Metas-
tasis
Therapy recommendation Page
< 3 y CMB Group 3/4 M0 Intensified Induction chemotherapy
with response-adjusted
consolidation (b)
or SKK chemotherapy without i.vtr.
MTX (a)
20 or
19
< 4 y LCA Group 3/4
(SHH)
M0/M+ Intensified Induction chemotherapy
with response-adjusted
consolidation (b)
– genetic counselling in case of SHH
–
20
CMB M+ ± R >
1.5 cm²
< 5 y DMB/MBEN SHH M0/M+ SKK chemotherapy with i.vtr. MTX (a)
– genetic counselling in case of SHH
–
19
> 3 y
to
21 y
CMB
(DMB > 5 y)
WNT, SHH,
Group 3/4
M0R0
(R+)
– eligible for PNET 5 MB –
Conventional RT (23.4 Gy CSI +
boost) with Maintenance
chemotherapy (c)
– genetic counselling in case of SHH
–
21
> 4 y
to
21 y
any
(DMB > 5 y)
WNT, SHH,
Group 3/4
M2/3 Two cycles SKK chemotherapy with
HFRT (40 Gy CSI + boost) and
Maintenance chemotherapy (e)
– genetic counselling in case of SHH
–
23
no M2/3, but any of the following
features:
LCA, MYC/N amplification, M1
(R > 1.5 cm²)
Conventional RT, enhanced dose
(35.2 Gy CSI + boost) with
Maintenance chemotherapy (d)
– genetic counselling in case of SHH
–
22
Not all possible constellations are described

Stratification and standard Treatment Recommendations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 11
a. SKK chemotherapy
(infants with low- and standard-risk medulloblastoma)
This therapy was first introduced in the SKK’92 study with the intention to avoid radiotherapy for young
children (Rutkowski et al. 2005). The HIT2000 trial was designed to validate the positive results of the
SKK’92 study. High efficiency of this regimen was confirmed for patients with desmoplastic/nodular
histology (Bueren et al. 2011). The finding that the histological subtype is an independent predictor of
outcomes in young children with medulloblastoma in a meta-analysis of several European studies
(Rutkowski et al. 2010b) resulted in a subtype-specific stratification of therapy recommendation for
medulloblastoma. An attempt to improve the prognosis of young patients with classic (or
anaplastic/large-cell) medulloblastoma by addition of local radiotherapy to SKK chemotherapy was not
successful (Ashley et al. 2012 and HIT2000 unpublished results), but complicated relapse treatment
because of the difficulty to administer craniospinal radiotherapy after local radiotherapy.
b. Intensified Induction chemotherapy with response-adjusted consolidation
(infants with high-risk medulloblastoma)
In the first years of the HIT2000 study, continuous 96h infusions of Cisplatin and Etoposide were
evaluated as induction regimen for young children with metastatic medulloblastoma.
The response rate with this regimen was relatively low. Due to the poor outcome of this patient group
(Rutkowski et al. 2010b) and the promising results obtained by the HeadStart group (Chi et al. 2004),
the HIT2000 protocol was amended in 2005. An intensified induction regimen based on the Head Start
regimen was introduced for all patients younger than 4 years at diagnosis with initially disseminated
disease. Preliminary analyses show enhanced response rates, as well as enhanced EFS rates. However,
this treatment regimen was associated with toxic events, and may only be applied by experienced
teams in paediatric oncology centres.
Patients between 3 and 4 years with high-risk features such as large residual tumour, anaplastic or
large-cell histology or MYC/N-amplification might have insufficient outcomes with both SKK-
chemotherapy (with or without intraventricular Methotrexate) and PNET 4 like therapy (Conventional
RT with 23.4 Gy CSI + Boost + maintenance chemotherapy). In these patients, this regimen might be
alternative to avoid high-dose craniospinal radiotherapy (35.2 Gy).
c. Conventional RT (23.4 Gy CSI + boost) with Maintenance chemotherapy
(PNET 4 standard regimen)
The multinational European trial PNET 4 demonstrated that in children older than 4 years with
standard-risk medulloblastoma (classical or desmoplastic histology, no dissemination),
hyperfractionated radiotherapy (HFRT) did not have a benefit compared to conventional radiotherapy,
in combination with 8 cycles of maintenance chemotherapy. EFS rates were satisfactory even after
lowering the dose of craniospinal irradiation from 35.2 Gy to 23.4 Gy in the standard radiotherapy arm
(Lannering et al. 2012).
The prospective study PNET 5 MB is open for recruitment in Germany, France, Italy, Switzerland,
Finland, Sweden, Belgium, Spain and Austria for patients with standard-risk and low-risk
medulloblastoma. Please check eligibility for PNET 5 MB.
d. Conventional RT, enhanced dose (35.2 Gy CSI + boost) with Maintenance chemotherapy
(HIT’91 Maintenance regimen)
The HIT’91 trial compared outcomes of postoperative radiotherapy (35.2 Gy CSI + boost) followed by
maintenance chemotherapy versus “sandwich” chemotherapy (i. e. postoperative chemotherapy
followed by radiotherapy followed by chemotherapy). Radiotherapy followed by maintenance
chemotherapy was superior, especially in patients older than 6 years at diagnosis and in patients with
M1-disease (Hoff et al. 2009; Kortmann et al. 2000), while in M2/M3 disease a difference was not

Stratification and standard Treatment Recommendations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 12
detected (Kortmann et al. 2000). Due to the inferior outcome of patients with large-cell or anaplastic
histology, the reduced CSI dose used in the PNET 4 trial (23.4 Gy) was not regarded sufficient for the
treatment of these patients (Lannering et al. 2010). Therefore, patients with large-cell or anaplastic
histology receive the higher CSI dose. The same was true for patients with M1 disease and MYC-
amplified AMB/LCMB (Hoff et al. 2010). Due to the inferior outcome compared to M0 CMB/DMB
patients, M1 patients were considered at higher risk for relapse (Hoff et al. 2009) and a reduction of
the CSI dose was not regarded justifiable so far.
Patients with a residual tumour > 1.5 cm² (R2–4) had a higher relapse-risk in some series. However, it
remains unclear whether a higher CSI dose is actually necessary to prevent distant relapse. Therefore,
in individual cases, a RT concept as described in (c) might be an adequate alternative treatment.
e. Two cycles SKK chemotherapy with HFRT (40 Gy CSI + boost) and Maintenance chemotherapy
(MET-HIT-AB4 regimen)
The HIT2000 trial evaluated the effectivity of a combination of induction chemotherapy with SKK,
hyperfractionated radiotherapy and maintenance chemotherapy in patients with disseminated
medulloblastoma. The observed survival rates were in the range of the rates observed by other groups
(Rutkowski et al. 2010a; Bueren et al. 2016). Unlike treatment strategies for localized
medulloblastoma, strategies for disseminated medulloblastoma are very diverse between the
different groups worldwide. Currently, attempts are being made to harmonise treatment between the
European groups. If hyperfractionated radiotherapy is impossible, conventional fractionated
radiotherapy should be applied (CSI 35.2 Gy + boost, see d.).
2.2. Ependymoma (intracranial)
Please note: The SIOP Ependymoma II trial is open for recruitment in several European countries.
Please note that all patients of participating national groups should be registered and treated within
SIOP Ependymoma II after national start of recruitment.
The following treatment is standard in use in Austria and Germany until the opening of SIOP
Ependymoma II.
Age Metastasis Residual
tumour
Therapy recommendation
– check eligilibity for EPENDYMOMA II –
Page
< 1.5 y M0 R0 Five cycles SKK chemotherapy with local RT (54 Gy)
(h)
24
> 1.5 y
to 21 y
M0 R0 Local 59.4 Gy conventional or 68 Gy HFRT (local
59.4 Gy conventional RT for children < 4 years) (i)
26
all until
21 y
M0 R > 0.5 cm²
Two cycles Modified SKK chemotherapy and re-
surgery with local RT (f)
– only if a 2nd surgery would become feasible –
24
all until
21 y
M+ all individual (j)
f.

Stratification and standard Treatment Recommendations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 13
g. Two cycles Modified SKK chemotherapy and re-surgery with local RT
(only if a 2nd surgery would become feasible after possible response to chemotherapy)
This treatment strategy may be used to possibly render the residual tumour more amenable for second
surgery before the start of radiotherapy. Experiences in HIT2000 and other series showed (Garvin, Jr.
et al. 2012; Massimino et al. 2010; Merchant et al. 2009), that diligent evaluation of second surgery is
very important for the success of this approach.
A re-surgery should be aimed whenever feasible in patients with residual tumour, administration of
window chemotherapy without re-surgery has not improved EFS in HIT2000.
h. Five cycles SKK chemotherapy with local RT (54 Gy)
(infants with localised and GTR or NTR)
Within HIT2000, young children with ependymoma were treated with primary SKK chemotherapy
(without i. vtr. MTX) and delayed local radiotherapy, if they were younger than 4 years at primary
diagnosis. The preliminary results for R0 patients treated with this strategy compared favourably with
the results of older patients, who received primary radiotherapy. However, international data as well
as own unpublished data show that local radiotherapy is well tolerated also in younger patients
(Merchant et al. 2005; Fouladi et al. 2005) and the SKK chemotherapy represents a high burden for the
patients and their families. Therefore we would recommend this strategy only for very young patients
(younger than 1.5 years at diagnosis).
i. Local 59.4 Gy conventional or 68 Gy HFRT (local 59.4 Gy conventional RT for children < 4 years)
Primary local radiotherapy can be considered as standard treatment for patients with ependymoma.
In HIT2000, the age limit for the application of primary local radiotherapy was 4 years at first diagnosis.
We recommend lowering this age limit to 1.5 years for treatment outside of prospective studies (see
4.8). Regarding hyperfractionation, the impact cannot be defined yet. It is only recommended for
patients, where application of hyperfractionation is practicable. Also the role of adjuvant
chemotherapy has yet to be defined. It is currently evaluated within a COG trial (ACNS0831) and the
upcoming SIOP Ependymoma II trial. In HIT2000, adjuvant chemotherapy was applied to all patients
with WHO grade III ependymomas. Stratification of treatment regimens according to tumour grading
cannot be further recommended, as the prognostic significance of the ependymoma grading could not
be confirmed (Ellison et al. 2011). The evidence for effectivity of chemotherapy after radiotherapy is
limited in ependymoma and chemotherapy is not used by most international groups (Merchant et al.
2009; Pajtler et al. 2017).
j. Individual
(primary metastatic ependymoma)
Disseminated ependymoma is rare at initial presentation, although it is more frequently seen at
relapse. Due to the low number of patients with heterogeneous manifestation, standardised therapy
recommendations cannot be given. A high rate of false positive results has been encountered in the
HIT studies. Please verify any diagnostic result of metastases at presentation before starting an
intensified treatment approach. You may contact the HIT-MED study centre if you wish to discuss
individual treatment options.

Stratification and standard Treatment Recommendations
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 14
2.3. CNS Embryonal Tumour NOS, ETMR (both formerly CNS-PNET) and Pineoblastoma
Age Histology Metastasis Therapy recommendation Page
< 4 y ETMR M0/M+ CARBO/ETO-96h induction with response-adjusted
consolidation (k)
27
≥ 4 y to
21 y
Pineoblastoma M0 Conventional RT, enhanced dose (35.2 Gy CSI +
boost) with Maintenance chemotherapy (l)
22
Pineoblastoma M+ Two cycles SKK chemotherapy with HFRT (40 Gy
CSI + boost) and Maintenance chemotherapy (m)
23
k. CARBO/ETO-96h induction with response-adjusted consolidation
(infant non-cerebellar non-rhabdoid CNS embryonal tumours)
Due to the low number of CNS embryonal tumour/ETMR & pineoblastoma with heterogenous
manifestation and limited entity-specific treatment experiences, no standard treatment
recommendations are included in this guidance. Please contact the HIT-MED study centre if you wish
to discuss individual treatment options.
l. Conventional RT, enhanced dose (35.2 Gy CSI + boost) with Maintenance chemotherapy
(HIT’91 regimen)
In HIT’91 radiotherapy dose has been shown to have a relevant influence on the outcome of patients
with CNS-PNET (Timmermann et al. 2002). In HIT2000 primary hyperfractionated RT (HFRT) followed
by Packer’s maintenance chemotherapy was introduced for all older patients with M0 CNS embryonal
tumour/ETMR and pineoblastoma, but showed no superior outcome. In the second phase of the
HIT2000 trial, the evaluation of an alternative treatment with primary postoperative SKK
chemotherapy, followed by HFRT and maintenance chemotherapy (as used for treatment of metastatic
medulloblastoma patients) did not show a superior effectivity (preliminary analysis, unpublished).
m. Two cycles SKK chemotherapy with HFRT (40 Gy CSI + boost) and Maintenance chemotherapy
(MET-HIT-AB4 regimen)
For older patients with metastatic CNS embryonal tumour/ETMR or pineoblastoma, the same
treatment strategy as for patients with metastatic medulloblastoma was used in HIT2000: primary
postoperative SKK chemotherapy followed by HFRT and Maintenance chemotherapy. The preliminary
results of this strategy were in the same range as published results from other series.

Results of other prospective clinical Trials and planned international Studies (SIOP-E)
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 15
3. Results of other prospective clinical Trials and planned
international Studies (SIOP-E) Please note that the scope of this chapter is to give a shortcut of relevant information. The mentioned
literature is just a selection and cannot give an encompassing overview on the topic.
3.1. Medulloblastoma
Much progress has recently been made on elucidation of the tumour biology of medulloblastoma,
supporting that subgroups of medulloblastoma have distinct cellular origins (Wang et al. 2015). Results
also show prominent molecular and clinical differences between SHH- and WNT-subgroup
medulloblastomas (Gibson et al. 2010). According to current consensus, at least 4 different biological
groups can be differentiated (Northcott et al. 2011; Taylor et al. 2012). A meta-analysis assessed
molecular and clinical data of medulloblastomas brought together from seven independent studies,
which showed mostly congruent results of molecular subgroups with respect to transcriptome profile,
DNA copy number aberrations, demographics and survival (Kool et al. 2012). Despite the stratification
of young medulloblastoma patients according to histology (which overlaps with the biological group),
the application of biological subgrouping or prognostic markers for therapy stratification currently
cannot be recommended outside of clinical trials (Shih et al. 2014; Pietsch et al. 2014). In the
upcoming studies, as in PNET 5, the on-time evaluation of the biological prognostic markers MYC and
MYCN will be evaluated, and diagnosis of WNT-pathway activation will be integrated for therapy
stratification.
In 2015, a consensus conference was convened in Heidelberg with the objective to further refine the
risk stratification in the context of subgroups and agree on a definition of risk groups of non-infant
paediatric medulloblastoma (Ramaswamy et al. 2016).
3.1.1. Standard-Risk Medulloblastoma
According to current understanding, medulloblastoma can be considered clinically standard risk in the
absence of metastases, and the absence of significant residual tumour. Clinical trials, which have
evaluated therapy strategies for treatment of standard risk medulloblastoma are:
- PNET 4, evaluation of hyperfractionated vs. conventionally fractionated radiotherapy followed
by maintenance chemotherapy (Lannering et al. 2010)
- COG 9961, evaluation of 2 different postradiotherapy chemotherapies (Packer et al. 2006)
- SJMB96, risk adapted craniospinal radiotherapy followed by high dose chemotherapy (Gajjar
et al. 2006)
- SFOP HFRT, online quality control, hyperfractionated radiotherapy alone, and reduced boost
volume for standard risk medulloblastoma (Carrie et al. 2009)
- PNET 3, pre-irradiation chemotherapy versus radiotherapy alone (Taylor et al. 2003)
These trials have shown good survival rates (3-y EFS about 80%) with CSI doses of 23.4 Gy combined
with post-irradiation chemotherapy. The application of hyperfractionated radiotherapy was not
associated with improved survival rates in PNET 4.
The SIOP-E trial PNET 5 MB will include clinically standard risk patients, and stratify treatment due to
the biological profile.
3.1.2. High-Risk Medulloblastoma
According to current understanding, non-WNT medulloblastoma can be considered clinically high-risk
in case of metastatic presentation (Ramaswamy et al. 2016). The prognostic impact of a large residual

Results of other prospective clinical Trials and planned international Studies (SIOP-E)
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 16
tumour is controversial. Clinical trials, which have evaluated therapy strategies for treatment of high
risk medulloblastoma are:
- MET-HIT2000-AB4, intensified sandwich-chemotherapy (Bueren et al. 2016)
- POG 9031, chemotherapy before or after radiotherapy (Tarbell et al. 2013)
- HART, hyperfractionated, accelerated radiotherapy (Gandola et al. 2009)
- SJMB96, risk adapted craniospinal radiotherapy followed by high dose chemotherapy (Gajjar
et al. 2006)
- SFOP, 8in1 and CARBO/ETO chemotherapy and radiotherapy (Verlooy et al. 2006)
- PNET 3, pre-irradiation chemotherapy and radiotherapy (Taylor et al. 2005b)
Improved survival rates have been achieved with intensified treatment.
A SIOP-E multinational trial for high risk medulloblastoma patients is currently in the phase of
conceptualization.
3.1.3. Medulloblastoma of young children and infants
The prognostic influence of desmoplastic histology (and extensive nodularity as the extreme end of
nodular desmoplastic differentiation) and SHH subgroup was demonstrated in several young children
brain tumour studies and an international meta-analysis:
- SKK’92, postoperative chemotherapy alone: SKK + i. vtr. MTX (Rutkowski et al. 2005)
- HIT2000, postoperative chemotherapy alone: SKK + i. vtr. MTX (Bueren et al. 2011)
- COG 9934, induction chemotherapy and conformal irradiation (Ashley et al. 2012)
- CCG 9921, multiagent chemotherapy and deferred radiotherapy (Leary et al. 2011)
- Head Start, induction chemotherapy and myeloablative chemotherapy (Dhall et al. 2008)
- international meta-analysis (Rutkowski et al. 2010b)
For most young children with SHH-MB, primary treatment with chemotherapy and avoidance of
radiotherapy is effective.
For young patients with CMB, AMB, LC MB none of the above mentioned strategies have shown clear
superiority, and the effectivity of these standard treatments was limited. As a high percentage of young
patients with CMB, AMB or LCMB relapse after a treatment which avoids craniospinal irradiation, the
ability and toxicity of relapse treatment must be taken into account for planning of treatment.
A SIOP-E multinational trial on young children with medulloblastoma is currently in the phase of
conceptualization.
3.2. Ependymoma
Progress has also been achieved on the understanding of biology of ependymoma. After it has become
evident that the biological characteristics differ between ependymoma with different primary location,
distinct subgroups have been defined (Taylor et al. 2005a; Witt et al. 2011). DNA methylation patterns
identify nine distinct molecular subgroups, three within each CNS compartment (Pajtler et al. 2015;
Pajtler 2016; Pajtler et al. 2017). The impact of the tumour location and the biological group on therapy
stratification has not been prospectively evaluated yet.
Standard treatment for children with ependymoma is primary local radiotherapy. For young patients
and patients with postoperative residual tumour, primary chemotherapy strategies have been
evaluated. Recent clinical trials, which have evaluated treatment strategies for treatment of
ependymoma are:
- primary proton radiotherapy (Macdonald et al. 2013)

Results of other prospective clinical Trials and planned international Studies (SIOP-E)
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 17
- St Jude, conformal radiotherapy after surgery for children (Merchant et al. 2009)
- SFOP, postoperative hyperfractionated radiotherapy (Conter et al. 2009)
- AIEOP, hyperfractionated radiotherapy and chemotherapy (Massimino et al. 2004)
- CCG 9942, primary chemotherapy for R+ patients (Garvin, Jr. et al. 2012)
- Head Start, induction chemotherapy and myeloablative chemotherapy (Zacharoulis et al.
2007; Venkatramani et al. 2013)
- AIEOP, second look surgery for ependymoma (Massimino et al. 2011)
- AIEOP, omitted or deferred radiotherapy for infant ependymoma (Massimino et al. 2010)
- UKCCSG, primary postoperative chemotherapy without RT (Grundy et al. 2007)
- BBSFOP, postoperative chemotherapy without irradiation (Grill et al. 2001)
These trials have shown good survival rates with primary local radiotherapy. The role of
hyperfractionation remains unclear. Application of conformal local radiotherapy is tolerable at a young
age. Chemotherapy has been used for deferral of radiotherapy for young children with different
success. The role of chemotherapy in the treatment of patients with residual tumour also remains to
be clarified. Second surgery was effective for improvement of survival of patients with residual tumour
after first surgery.
In the upcoming multinational SIOP Ependymoma II trial, different therapy strategies will be
evaluated: the role of chemotherapy after irradiation for R0 patients, postoperative chemotherapy
window for R+ patients, and primary baby type chemotherapy for very young patients.
3.3. CNS Embryonal Tumour and Pineoblastoma
There are only few studies on the rare diseases CNS embryonal tumour and pineoblastoma. For the
interpretation of these results, one has to regard that CNS embryonal tumours are a heterogeneous
group of tumours, and the histological diagnosis has been refined in the meantime.
For pineoblastoma, combined radio- and chemotherapy regimens were evaluated. Young children
have been treated with primary baby type chemotherapy, and also with intensified regimens:
Ø Meta-analysis of European and US pineoblastoma treatment strategies (Mynarek et al. 2016)

Therapy Flowcharts
HIT-MED Therapy Guidance Version 4.0 – 02. May 2017 18
4. Therapy Flowcharts
4.1. SKK chemotherapy
4.2. Intensified Induction chemotherapy with response-adjusted consolidation
4.3. Conventional RT (23.4 Gy CSI + boost) with Maintenance chemotherapy
4.4. Conventional RT, enhanced dose (35.2 Gy CSI + boost) with Maintenance chemotherapy
4.5. Two cycles SKK chemotherapy with HFRT (40 Gy CSI + boost) and Maintenance chemotherapy
4.6 Two cycles Modified SKK chemotherapy and re-surgery with local RT
4.7 Five cycles SKK chemotherapy with local RT (54 Gy)
4.8 Local 59.4 Gy conventional or 68 Gy HFRT (local 59.4 Gy conventional RT for children < 4 years)
4.9 CARBO/ETO-96h induction with response-adjusted consolidation

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
1
9
4.1
. S
KK
ch
em
oth
era
py
Intr
ave
ntr
icu
lar
Me
tho
tre
xate
is in
ten
de
d o
nly
fo
r p
rim
ary
tre
atm
en
t, n
ot
in a
re
lap
se s
itu
atio
n.
Intr
ave
ntr
icu
lar
or
syst
em
ic M
eth
otr
exa
te m
ust
ne
ver
be
giv
en
du
rin
g o
r af
ter
rad
ioth
era
py!
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly.N
eit
he
r w
ho
le r
egi
me
ns
no
r p
arts
of
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
No
tes
-
Co
nsi
de
r sp
eci
al s
urg
ery
re
com
me
nd
atio
ns
for
“gra
pe
-lik
e”
MB
EN
(ch
apte
r 6
).
-
I. v
tr.
MT
X s
ho
uld
on
ly b
e g
ive
n i
n D
MB
or
MB
EN
pa
tie
nts
, si
nce
th
e l
ike
lih
oo
d o
f
ne
cess
ity
of
cra
nio
spin
al i
rra
dia
tio
n a
nd
su
bse
qu
en
t to
xici
tie
s a
nd
late
eff
ect
s is
hig
he
r
in L
CA
/CM
B p
ati
en
ts.
-
In c
ase
of
pro
gre
ssio
n/r
ela
pse
in D
MB
or
MB
EN
pat
ien
ts,
ple
ase
co
nta
ct H
IT-M
ED
stu
dy
cen
tre
.
-
In c
ase
of
ear
ly p
rogr
ess
ion
/re
lap
se i
n C
MB
pat
ien
ts,
rad
ioth
era
py
sho
uld
be
in
itia
ted
imm
ed
iate
ly;
in c
ase
of
late
re
lap
se i
n C
MB
pat
ien
ts r
e-i
nd
uct
ion
ch
em
oth
era
py
an
d
rad
ioth
era
py
mig
ht
be
co
nsi
de
red
.
-
I. v
tr.
Me
tho
tre
xate
mu
st o
nly
be
use
d i
n c
en
tre
s w
ith
re
spe
ctiv
e e
xpe
rie
nce
(se
e
gu
ide
lin
es
cha
pte
r 8
.6).
-
Ple
ase
co
nsi
de
r g
en
eti
c co
un
sell
ing
in
ca
se
of
SH
H-p
ath
wa
y-a
ctiv
ati
on
b
efo
re
rad
ioth
era
py
, a
cco
rdin
g t
o n
ati
on
al
law
s (f
or
Go
rlin
-Go
ltz
an
d L
i-Fr
au
me
ni
syn
dro
me
).
Ind
ica
tio
ns
Ag
e
His
tolo
gic
al
sub
typ
e
Mo
lecu
lar
sub
gro
up
M
eta
sta
sis
0–
5 y
ea
rs
DM
B, M
BE
N
SHH
M
0 a
nd
M+
0–
3 y
ea
rs
LCA
MB
, CM
B
Gro
up
3/4
(SH
H)
M0
DM
B:
de
smo
pla
stic
me
du
llob
last
om
a, M
BE
N:
me
du
llob
last
om
a w
ith
ext
en
sive
no
du
lari
ty,
th
is s
ub
typ
e s
ho
ws
typ
ical
ly a
SH
H-p
ath
way
act
ivat
ion
CM
B:
clas
sica
l me
du
llob
last
om
a, A
MB
: an
apla
stic
me
du
llob
last
om
a
SK
K (
5.1
)
Cyc
lop
ho
sph
amid
e/V
incr
isti
ne
2
× h
igh
-do
se M
eth
otr
exa
te/V
incr
isti
ne
C
arb
op
lati
n/E
top
osi
de
i.
vtr.
MT
X (
on
ly f
or
pat
ien
ts w
ith
DM
B/M
BE
N)
Mo
dif
ied
SK
K (
5.2
)Cyc
lop
ho
sph
am
ide
/Vin
cris
tin
e
C
arb
op
lati
n/E
top
osi
de
*
no
i. v
tr. M
TX
Ma
inte
na
nce
(5
.3)C
isp
lati
n/L
om
ust
ine
/Vin
cris
tin
e
Ra
dio
the
rap
y (
7.1
)CSI
24
.0 G
y
p
ost
eri
or
foss
a b
oo
st 3
0.6
Gy
(to
tal 5
4.6
Gy)
m
eta
stas
is b
oo
st 2
5.2
Gy
n
o V
incr
isti
ne

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
0
4.2
. In
ten
sifi
ed
In
du
ctio
n c
he
mo
the
rap
y w
ith
re
spo
nse
-ad
just
ed
co
nso
lida
tio
n
Intr
ave
ntr
icu
lar
Me
tho
tre
xate
is in
ten
de
d o
nly
fo
r p
rim
ary
tre
atm
en
t, n
ot
in a
re
lap
se s
itu
atio
n.
Intr
ave
ntr
icu
lar
or
syst
em
ic M
eth
otr
exa
te m
ust
ne
ver
be
giv
en
du
rin
g o
r af
ter
rad
ioth
era
py!
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly. N
eit
he
r w
ho
le r
egi
me
ns
no
r p
arts
of
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
Ind
ica
tio
ns
Ag
e
His
tolo
gic
al
sub
typ
e
Mo
lecu
lar
sub
gro
up
M
eta
sta
sis
0–
4 y
ea
rs
CM
B, L
CA
MB
Gro
up
3/4
(SH
H)
M0
/M+
CM
B:
clas
sica
l me
du
llob
last
om
a, A
MB
: an
apla
stic
me
du
llob
last
om
a, L
CM
B:
larg
e c
ell
me
du
llob
last
om
a
Inte
nsi
fie
d I
nd
uct
ion
(5
.4)
Cis
pla
tin
/Vin
cris
tin
e/E
top
osi
de
/
Cyc
lop
ho
sph
amid
e/h
igh
-do
se M
eth
otr
exa
te
i.vtr
. MT
X (
on
ly f
or
pat
ien
ts w
ith
M+
)
1.
HD
CT
(5
.6)
C
arb
op
lati
n/E
top
osi
de
/i.v
tr. M
TX
/ASC
T
2.
HD
CT
T
hio
tep
a/C
yclo
ph
osp
ham
ide
/i.v
tr. M
TX
/ASC
T
Ma
inte
na
nce
(5
.3)
Cis
pla
tin
/Lo
mu
stin
e/V
incr
isti
ne
Ra
dio
the
rap
y
CSI
24
.0 G
y
po
ste
rio
r fo
ssa
bo
ost
30
.6 G
y (t
ota
l 54
.6 G
y)
me
tast
asis
bo
ost
25
.2 G
y
no
Vin
cris
tin
e
No
tes
-
In c
ase
of
WN
T-p
ath
way
-act
ivat
ion
, ple
ase
ch
eck
elig
ibili
ty f
or
tria
ls (
e. g
. PN
ET
5 M
B)!
-
Hig
h t
ox
icit
y -
> o
nly
exp
eri
en
ced
, sp
eci
ali
zed
on
colo
gic
ce
ntr
es!
-
For
pat
ien
ts w
ith
ou
t m
eas
ura
ble
po
sto
pe
rati
ve d
ise
ase
, th
ere
are
tw
o o
pti
on
s fo
r tr
eat
me
nt:
-
Ind
uct
ion
wit
ho
ut
i. vt
r. M
TX
fo
llow
ed
by
CSI
or
-
Ind
uct
ion
wit
h i.
vtr
. MT
X f
ollo
we
d b
y H
DC
T;
CSI
in c
ase
of
no
n-C
R/r
ela
pse
.
-
Pat
ien
ts w
ith
po
siti
ve C
SF-c
yto
logy
aft
er
ind
uct
ion
are
de
fin
ed
as
no
n-r
esp
on
de
rs.
-
Th
era
py
regi
me
ns
wit
h p
rim
ary
CSI
(se
e c
hap
ter
4.4
or
4.5
) m
igh
t b
e m
ore
eff
icie
nt
and
p
oss
ibly
to
lera
ble
in p
ati
en
ts >
3 y
ear
s b
ut
may
be
ass
oci
ate
d w
ith
po
ore
r n
eu
rop
sych
olo
gica
l o
utc
om
e.
-
I. v
tr.
MT
X m
ust
on
ly b
e u
sed
in
ce
ntr
es
wit
h r
esp
ect
ive
exp
eri
en
ce (
see
gu
ide
lin
es
cha
pte
r
8.6
).
-
Ple
ase
co
nsi
de
r g
en
eti
c co
un
sell
ing
in c
ase
of
SH
H-p
ath
wa
y-a
ctiv
ati
on
be
fore
ra
dio
the
rap
y,
acc
ord
ing
to
na
tio
na
l la
ws
(fo
r G
orl
in-G
olt
z a
nd
Li-
Fra
um
en
i sy
nd
rom
e).
-
Th
era
py
acco
rdin
g SK
K c
he
mo
the
rap
y (4
.1)
may
be
co
nsi
de
red
fo
r M
0 g
rou
p 3
/4 M
B (
LCA
, C
MB
).
-
Mai
nte
nan
ce c
he
mo
the
rap
y m
ay b
e n
ot
we
ll to
lera
ted
. M
on
ito
rin
g o
f to
xici
ty i
s cr
uci
al a
nd
d
ose
mo
dif
icat
ion
s ar
e f
req
ue
ntl
y re
qu
ire
d (
see
gu
ide
line
s).

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
1
4.3
. C
on
ven
tio
na
l R
T (
23
.4 G
y C
SI
+ b
oo
st)
wit
h M
ain
ten
an
ce c
he
mo
the
rap
y
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly. N
eit
he
r w
ho
le r
egi
me
ns
no
r p
arts
of
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
Ind
ica
tio
ns
Ag
e
His
tolo
gic
al
sub
typ
e
Mo
lecu
lar
sub
gro
up
S
tag
ing
3–
21
y
CM
B, M
YC
/N n
eg,
or
no
t e
val.
WN
T, S
HH
, Gro
up
3/4
M
0R
0
5–
21
y
DM
B, M
YC
/N n
eg,
or
no
t e
val.
SH
H, G
rou
p 3
/4
M0
R0
CM
B:
clas
sica
l me
du
llob
last
om
a , D
MB
: d
esm
op
last
ic m
ed
ullo
bla
sto
ma
W
NT-
pat
hw
ay a
ctiv
ate
d t
um
ou
rs m
igh
t h
ave
be
tte
r p
rogn
osi
s an
d s
ho
uld
be
incl
ud
ed
in P
NE
T5
Ma
inte
na
nce
(5
.3)
Cis
pla
tin
/Lo
mu
stin
e/V
incr
isti
ne
Ra
dio
the
rap
y
CSI
23
.4 G
y
po
ste
rio
r fo
ssa
(on
ly P
NE
T 5
: tu
mo
ur
site
): 3
0.6
Gy
(to
tal 5
4.0
Gy)
Vin
cris
tin
e
No
tes
-
Ple
ase
ch
eck
elig
ibili
ty f
or
PN
ET
5 M
B!
-
Exp
eri
me
nta
l tr
eat
me
nt
red
uct
ion
s fo
r p
atie
nts
wit
h l
ow
-ris
k d
ise
ase
sh
ou
ld o
nly
be
pe
rfo
rme
d w
ith
in c
linic
al t
rial
s (e
. g.
WN
T in
PN
ET
5).
-
Mai
nte
nan
ce c
he
mo
the
rap
y m
ay
be
to
xic.
Mo
nit
ori
ng
of
toxi
city
is
cru
cial
an
d d
ose
mo
dif
icat
ion
s ar
e
fre
qu
en
tly
req
uir
ed
(s
ee
gu
ide
line
s).
Do
se
red
uct
ion
w
as
no
t
asso
ciat
ed
wit
h i
nfe
rio
r p
rogn
osi
s in
HIT
’91
(vo
n H
off
Eu
r J
Can
cer
20
09
). A
lte
rnat
ive
mai
nte
na
nce
ch
em
oth
era
py
cou
rse
s ac
cord
ing
to P
OG
90
31
(T
arb
ell
JCO
20
13
) o
r P
acke
r
JCO
20
06
may
be
alt
ern
ativ
es
in c
ase
of
pro
lon
ged
/ s
eve
re t
oxi
city
.
-
Evi
de
nce
fo
r e
ffic
acy
of
vin
cris
tin
e d
uri
ng
RT
is li
mit
ed
.
-
Ple
ase
co
nsi
de
r g
en
eti
c co
un
sell
ing
in
ca
se
of
SH
H-p
ath
wa
y-a
ctiv
ati
on
b
efo
re
rad
ioth
era
py
, a
cco
rdin
g t
o n
ati
on
al
law
s (f
or
Go
rlin
-Go
ltz
an
d L
i-Fr
au
me
ni
syn
dro
me
).
-
Th
is c
on
cep
t m
ay a
lso
be
eff
ect
ive
fo
r p
atie
nts
wit
h la
rge
re
sid
ual
tu
mo
urs
. P
rese
nce
of
larg
e r
esi
du
al t
um
ou
r is
ass
oci
ate
d w
ith
hig
he
r ri
sk o
f re
lap
se.
Evi
de
nce
fo
r h
igh
er
eff
icac
y o
f a
hig
he
r C
SI d
ose
in t
his
co
nd
itio
n is
lim
ite
d.

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
2
4.4
. C
on
ven
tio
na
l R
T,
en
ha
nce
d d
ose
(3
5.2
Gy
CS
I +
bo
ost
) w
ith
Ma
inte
na
nce
ch
em
oth
era
py
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly.
Ne
ith
er
wh
ole
re
gim
en
s n
or
par
ts o
f th
em
sh
ou
ld b
e u
sed
fo
r sa
lvag
e t
he
rap
y.
No
tes
-
In c
ase
of
WN
T-p
ath
way
-act
ivat
ion
, ple
ase
ch
eck
elig
ibili
ty f
or
tria
ls (
e.
g. P
NE
T 5
MB
)!
-
Mai
nte
nan
ce c
he
mo
the
rap
y m
ay
be
to
xic.
Mo
nit
ori
ng
of
toxi
city
is
cru
cial
an
d d
ose
mo
dif
icat
ion
s ar
e
fre
qu
en
tly
req
uir
ed
(s
ee
gu
ide
line
s).
Do
se
red
uct
ion
w
as
no
t
asso
ciat
ed
wit
h i
nfe
rio
r p
rogn
osi
s in
HIT
’91
(vo
n H
off
Eu
r J
Can
cer
20
09
). M
ain
ten
ance
che
mo
the
rap
y ac
cord
ing
to P
OG
90
31
(T
arb
ell
JCO
20
13
) o
r P
acke
r JC
O 2
00
6 m
ay b
e
alte
rnat
ive
s.
-
Evi
de
nce
fo
r e
ffic
acy
of
vin
cris
tin
e d
uri
ng
RT
is li
mit
ed
.
-
Ple
ase
co
nsi
de
r g
en
eti
c co
un
sell
ing
in
ca
se
of
SH
H-p
ath
wa
y-a
ctiv
ati
on
b
efo
re
rad
ioth
era
py
, a
cco
rdin
g t
o n
ati
on
al
law
s (f
or
Go
rlin
-Go
ltz
an
d L
i-Fr
au
me
ni
syn
dro
me
).
-
Pre
sen
ce o
f la
rge
re
sid
ual
tu
mo
ur
is a
sso
ciat
ed
wit
h h
igh
er
risk
of
rela
pse
. E
vid
en
ce f
or
hig
he
r e
ffic
acy
of
a h
igh
er
CSI
do
se i
n t
his
co
nd
itio
n i
s lim
ite
d.
Alt
ern
ativ
ely
, a
red
uce
d
CSI
do
se a
s in
4.3
mig
ht
be
co
nsi
de
red
as
we
ll.
-
For
pin
eo
bla
sto
ma
pat
ien
ts,
36
Gy
HFR
T w
as e
valu
ate
d i
n P
-HIT
20
00
-AB
4 a
nd
may
be
use
d a
lte
rnat
ive
ly..
Ma
inte
na
nce
(5
.3)
Cis
pla
tin
/Lo
mu
stin
e/V
incr
isti
ne
Ra
dio
the
rap
y
CSI
35
.2 G
y
po
ste
rio
r fo
ssa
bo
ost
19
.8 G
y (t
ota
l 55
.0 G
y)
Vin
cris
tin
e
Ind
ica
tio
ns
Ag
e
His
tolo
gic
al
sub
typ
e
Mo
lecu
lar
sub
gro
up
M
eta
sta
sis
5–
21
ye
ars
D
MB
SHH
(G
rou
p 3
/4)
M0
R+
(>
1.5
cm²)
or
M1
D
MB
MY
C/N
am
plif
icat
ion
SH
H (
Gro
up
3/4
) M
0R
0
4–
21
ye
ars
P
ine
ob
last
om
a
M
0
Ag
e
an
y o
f th
e f
oll
ow
ing
fe
atu
res
Me
tast
asi
s
4–
21
ye
ars
LC
A
MY
C/N
am
plif
icat
ion
SHH
, Gro
up
3/4
M
1, n
o M
2/3
(R >
1.5
cm
²)
DM
B:
de
smo
pla
stic
me
du
llob
last
om
a, C
MB
: cl
assi
cal m
ed
ullo
bla
sto
ma,
AM
B:
anap
last
ic
me
du
llob
last
om
a, L
CM
B:
larg
e c
ell
me
du
llob
last
om
a

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
3
4.5
. T
wo
cyc
les
SK
K c
he
mo
the
rap
y w
ith
HF
RT
(4
0 G
y C
SI
+ b
oo
st)
an
d M
ain
ten
an
ce c
he
mo
the
rap
y
In
trav
en
tric
ula
r M
eth
otr
exa
te is
inte
nd
ed
on
ly f
or
pri
mar
y tr
eat
me
nt,
no
t in
a r
ela
pse
sit
uat
ion
. In
trav
en
tric
ula
r o
r sy
ste
mic
Me
tho
tre
xate
mu
st n
eve
r b
e g
ive
n d
uri
ng
or
afte
r
rad
ioth
era
py!
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly. N
eit
he
r w
ho
le r
egi
me
ns
no
r p
arts
of
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
No
tes
Ø
I. v
tr.
MT
X m
ust
on
ly b
e u
sed
by
ce
ntr
es
wit
h r
esp
ect
ive
exp
eri
en
ce (
see
8.6
).
Ø
Mai
nte
nan
ce c
he
mo
the
rap
y m
ay
be
to
xic.
Mo
nit
ori
ng
of
toxi
city
is
cru
cial
an
d
do
se
mo
dif
icat
ion
s ar
e
fre
qu
en
tly
req
uir
ed
(s
ee
8
.1).
M
ain
ten
ance
che
mo
the
rap
y ac
cord
ing
to P
acke
r e
t al
. 2
00
6 o
r T
arb
ell
et
al.
20
13
may
be
alte
rnat
ive
s in
MB
pat
ien
ts.
Ø
If h
yp
erf
ract
ion
ate
d r
ad
ioth
era
py
is
no
t p
oss
ible
, co
nv
en
tio
na
l fr
act
ion
ate
d
rad
ioth
era
py
sh
ou
ld b
e a
pp
lie
d (
CS
I 3
5.2
Gy
+ b
oo
st,
see
7.1
.14
.4).
Ø
Evi
de
nce
fo
r e
ffic
acy
of
Vin
cris
tin
e d
uri
ng
RT
is li
mit
ed
.
Ø
Ple
ase
co
nsi
de
r g
en
eti
c co
un
sell
ing
in
ca
se o
f S
HH
-pa
thw
ay
act
iva
tio
n b
efo
re
RT
, a
cco
rdin
g t
o n
ati
on
al
law
s (f
or
Go
rlin
-Go
ltz
an
d L
i-Fr
au
me
ni
syn
dro
me
).
SK
K (
5.1
)
Cyc
lop
ho
sph
amid
e/V
incr
isti
ne
2
× h
igh
-do
se M
eth
otr
exa
te/V
incr
isti
ne
C
arb
op
lati
n/E
top
osi
de
i.
vtr.
MT
X
Ma
inte
na
nce
(5
.3)
Cis
pla
tin
/Lo
mu
stin
e/V
incr
isti
ne
Ra
dio
the
rap
y (
7.1
) h
ype
rfra
ctio
nat
ed
40
.0 G
y C
SI (
see
no
tes
for
alte
rnat
ive
)
po
ste
rio
r fo
ssa
bo
ost
20
.0 G
y (t
ota
l 60
.0 G
y)
tum
ou
r b
oo
st 2
8.0
Gy
(to
tal 6
8.0
Gy)
sup
rate
nto
rial
me
tast
asis
bo
ost
20
.0 G
y
spin
al m
eta
stas
is b
oo
st 1
0.0
Gy
Vin
cris
tin
e
Ind
ica
tio
ns
Ag
e
His
tolo
gic
al
sub
typ
e
Mo
lecu
lar
sub
gro
up
M
eta
sta
sis
5–
21
ye
ars
D
MB
SHH
, Gro
up
3/4
M
2/M
3
4–
21
ye
ars
C
MB
, AM
B, L
CM
B
WN
T, G
rou
p 3
/4
M2
/M3
4–
21
ye
ars
P
ine
ob
last
om
a
M
+
DM
B:
de
smo
pla
stic
me
du
llob
last
om
a, C
MB
: cl
assi
cal m
ed
ullo
bla
sto
ma,
AM
B:
anap
last
ic
me
du
llob
last
om
a, L
CM
B:
larg
e c
ell
me
du
llob
last
om
a, E
TM
R:
emb
ryo
nal
tu
mo
ur
wit
h m
ult
i-la
yere
d
rose
tte
s

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
4
4.6
. T
wo
cyc
les
Mo
dif
ied
SK
K c
he
mo
the
rap
y a
nd
re
-su
rge
ry w
ith
loca
l R
T
Me
tho
tre
xate
mu
st n
eve
r b
e g
ive
n d
uri
ng
or
afte
r ra
dio
the
rap
y! A
ll tr
eat
me
nt
regi
me
ns
hav
e b
ee
n d
eve
lop
ed
fo
r p
rim
ary
tre
atm
en
t o
nly
. Ne
ith
er
wh
ole
re
gim
en
s n
or
par
ts o
f
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
Ind
ica
tio
ns
Ag
e
His
tolo
gy
Me
tast
asi
s 0
–2
1 y
ea
rs
intr
acra
nia
l
Ep
en
dym
om
a
(WH
O g
rad
e II
+ I
II)
M0
R+
Me
asu
rab
le (
no
du
lar)
re
sid
ua
l tu
mo
ur
No
tes
-
Ch
eck
po
ssib
ility
fo
r in
clu
sio
n in
SIO
P E
pe
nd
ymo
ma
II!
-
Pat
ien
ts w
ith
re
sid
ual
tu
mo
ur
sho
uld
un
de
rgo
co
nse
qu
en
t e
valu
ati
on
fo
r se
con
d s
urg
ery
.
-
Pat
ien
ts w
ith
sm
all,
no
t m
eas
ura
ble
re
sid
ual
tu
mo
ur
may
be
tre
ate
d a
cco
rdin
g to
th
e
pro
toco
l fo
r R
0 p
atie
nts
.
-
Th
e a
im o
f th
e w
ind
ow
ch
em
oth
era
py
is r
e-s
urg
ery
be
fore
ra
dio
the
rap
y,
ad
min
istr
ati
on
of
win
do
w c
he
mo
the
rap
y w
ith
ou
t re
-su
rge
ry h
as
no
t im
pro
ve
d E
FS i
n H
IT2
00
0.
-
Th
e e
vid
en
ce f
or
sup
eri
ori
ty o
f H
FRT
is
lim
ite
d.
Mo
dif
ied
SK
K (
5.2
) C
yclo
ph
osp
ham
ide
/Vin
cris
tin
e
Car
bo
pla
tin
/Eto
po
sid
e
* n
o i.
vtr
. MT
X
SK
K (
5.1
)
Cyc
lop
ho
sph
amid
e/V
incr
isti
ne
2 ×
hig
h-d
ose
Me
tho
tre
xate
/Vin
cris
tin
e
Car
bo
pla
tin
/Eto
po
sid
e
* n
o i.
vtr
. MT
X
Ra
dio
the
rap
y (
7.2
) 5
9.4
Gy
con
ven
tio
nal
fra
ctio
nat
ed
loca
l RT
(68
.0 G
y h
ype
rfra
ctio
nat
ed
loca
l RT
)
(+ s
tere
ota
ctic
bo
ost
in c
ase
of
pe
rsis
tin
g re
sid
ual
tu
mo
ur)
no
Vin
cris
tin
e

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
5
4.7
. F
ive
cyc
les
SK
K c
he
mo
the
rap
y w
ith
loca
l R
T (
54
Gy)
Me
tho
tre
xate
mu
st n
eve
r b
e g
ive
n d
uri
ng
or
afte
r ra
dio
the
rap
y!
Me
tho
tre
xate
mu
st n
eve
r b
e g
ive
n d
uri
ng
or
afte
r ra
dio
the
rap
y! A
ll tr
eat
me
nt
regi
me
ns
hav
e b
ee
n d
eve
lop
ed
fo
r p
rim
ary
tre
atm
en
t o
nly
. Ne
ith
er
wh
ole
re
gim
en
s n
or
par
ts o
f
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
SK
K (
5.1
) C
yclo
ph
osp
ham
ide
/Vin
cris
tin
e
2 ×
hig
h-d
ose
Me
tho
tre
xate
/Vin
cris
tin
e
Car
bo
pla
tin
/Eto
po
sid
e
* n
o i.
vtr
. MT
X
Mo
dif
ied
SK
K (
5.2
) C
yclo
ph
osp
ham
ide
/Vin
cris
tin
e
C
arb
op
lati
n/E
top
osi
de
*
no
i. v
tr. M
TX
Ra
dio
the
rap
y (
7.2
) 5
4.0
Gy
loca
l RT
no
Vin
cris
tin
e
(lo
we
r ag
e li
mit
fo
r ra
dio
the
rap
y: 1
8 m
on
ths)
Ind
ica
tio
ns
Ag
e
His
tolo
gy
M
eta
sta
sis
0–
18
mo
nth
s in
trac
ran
ial
Ep
en
dym
om
a
(WH
O g
rad
e II
+ II
I)
M0
R0
(no
or
smal
l, n
ot
me
asu
rab
le r
esi
du
al
tum
ou
r )
No
tes
-
Incl
ud
es
pat
ien
ts t
hat
re
ach
R0
aft
er
seco
nd
(th
ird
) su
rge
ry.
-
Pat
ien
ts w
ith
sm
all,
no
t m
eas
ura
ble
re
sid
ual
tu
mo
ur
may
be
tre
ate
d a
cco
rdin
g to
th
is
pro
toco
l.
-
Ch
eck
po
ssib
ility
fo
r in
clu
sio
n in
SIO
P-E
pe
nd
ymo
ma
II!
-
Wit
hin
pro
spe
ctiv
e s
tud
ies,
rad
ioth
era
py
was
als
o a
pp
lied
in y
ou
nge
r ch
ildre
n (
> 1
ye
ar).

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
6
4.8
. Lo
cal 5
9.4
Gy
con
ven
tio
na
l o
r 6
8 G
y H
FR
T (
loca
l 5
9.4
Gy c
on
ven
tio
na
l R
T f
or
child
ren
< 4
ye
ars
)
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly. N
eit
he
r w
ho
le r
egi
me
ns
no
r p
arts
of
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
Ra
dio
the
rap
y (
7.2
)
59
.4 G
y co
nve
nti
on
al f
ract
ion
ate
d lo
cal R
T
(68
.0 G
y h
ype
rfra
ctio
nat
ed
loca
l RT
)
(+ s
tere
ota
ctic
bo
ost
in c
ase
of
pe
rsis
tin
g re
sid
ual
tum
ou
r)
no
Vin
cris
tin
e
Ind
ica
tio
ns
Ag
e
His
tolo
gy
M
eta
sta
sis
18
mo
nth
s -
21
ye
ars
in
trac
ran
ial
Ep
en
dym
om
a
(WH
O g
rad
e II
+ II
I)
M0
R0
(no
or
smal
l, n
ot
me
asu
rab
le, r
esi
du
al
tum
ou
r )
No
tes
-
Ch
eck
po
ssib
ility
fo
r in
clu
sio
n in
SIO
P E
pe
nd
ymo
ma
II!
-
Incl
ud
es
pat
ien
ts t
hat
re
ach
R0
aft
er
seco
nd
(th
ird
) su
rge
ry.
-
Pat
ien
ts w
ith
sm
all,
no
t m
eas
ura
ble
re
sid
ual
tu
mo
ur
may
be
tre
ate
d a
cco
rdin
g to
th
is
pro
toco
l.
-
Evi
de
nce
fo
r ad
min
istr
atio
n o
f ch
em
oth
era
py
is l
imit
ed
an
d c
urr
en
t co
nse
nsu
s o
n
tre
atm
en
t re
com
me
nd
s ir
rad
iati
on
on
ly (
Paj
tle
r e
t al
. 20
17
).

The
rap
y Fl
ow
char
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
7
4.9
. C
AR
BO
/ET
O-9
6h
ind
uct
ion
wit
h r
esp
on
se-a
dju
ste
d c
on
solid
ati
on
Intr
ave
ntr
icu
lar
Me
tho
tre
xate
is in
ten
de
d o
nly
fo
r p
rim
ary
tre
atm
en
t, n
ot
in a
re
lap
se s
itu
atio
n.
Intr
ave
ntr
icu
lar
or
syst
em
ic M
eth
otr
exa
te m
ust
ne
ver
be
giv
en
du
rin
g o
r af
ter
rad
ioth
era
py!
All
tre
atm
en
t re
gim
en
s h
ave
be
en
de
velo
pe
d f
or
pri
mar
y tr
eat
me
nt
on
ly. N
eit
he
r w
ho
le r
egi
me
ns
no
r p
arts
of
the
m s
ho
uld
be
use
d f
or
salv
age
th
era
py.
Ind
ica
tio
ns
Ag
e
His
tolo
gy
M
eta
sta
sis
0–
4 y
ea
rs
ETM
R
M0
/M+
No
tes
Ø
Mai
nte
nan
ce c
he
mo
the
rap
y m
ay
be
to
xic;
mo
nit
ori
ng
of
toxi
city
is
cru
cial
an
d
do
se m
od
ific
atio
ns
are
fre
qu
en
tly
req
uir
ed
(8
.1).
In p
atie
nts
wit
h M
2/M
3 d
ise
ase
,
CR
/PR
is d
efi
ne
d o
f p
ost
op
era
tive
tu
mo
ur/
me
tast
asis
AN
D n
ega
tive
CSF
cyt
olo
gy
for
tum
ou
r ce
llsP
atie
nts
, w
ho
are
no
t in
CR
be
fore
HD
CT
, b
ut
reac
h C
R a
fte
r
HD
CT
, may
op
tio
nal
ly r
ece
ive
CSI
(d
ata
un
cle
ar).
Ø
Pa
tie
nts
wit
h i
sola
ted
M1
dis
ea
se a
re t
rea
ted
lik
e “
po
or
resp
on
de
rs”
be
cau
se
resp
on
se t
o in
du
ctio
n c
he
mo
the
rap
y ca
nn
ot
be
eva
luat
ed
.
Ø
Pat
ien
ts w
ith
po
siti
ve C
SF c
yto
logy
aft
er
ind
uct
ion
are
de
fin
ed
po
or
resp
on
de
rs.
CA
RB
O/E
TO
(5.5
)
Car
bo
pla
tin
/Eto
po
sid
e-9
6h
infu
sio
n
i. v
tr.
Me
tho
tre
xa
te o
nly
fo
r M
+ p
ati
en
ts
Ma
inte
na
nce
(5.3
)
Cis
pla
tin
/Lo
mu
stin
e/V
incr
isti
ne
1st
HD
CT
(5
.6)
Car
bo
pla
tin
/Eto
po
sid
e/A
SCT
i. v
tr.
Me
tho
tre
xa
te o
nly
fo
r M
+ p
ati
en
ts
2n
d H
DC
T
Thio
tep
a/C
yclo
ph
osp
ham
ide
/ASC
T
i. v
tr.
Me
tho
tre
xa
te o
nly
fo
r M
+ p
ati
en
ts
Ra
dio
the
rap
y
(no
Vin
cris
tin
e)
CSI
24
.0 G
y
tum
ou
r b
oo
st 3
0.6
Gy
(to
tal 5
4.6
Gy)
# E
vid
en
ce f
or
ne
cess
ity
of
RT
afte
r H
DC
T fo
r
pat
ien
ts, w
ho
we
re in
CR
be
fore
, is
limit
ed
.

Chemotherapy Documentation Sheets
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 28
5. Chemotherapy Documentation Sheets
5.1 Documentation sheet SKK chemotherapy
5.2 Documentation sheet modified SKK chemotherapy
5.3 Documentation sheet Maintenance chemotherapy
5.4 Documentation sheet Intensified Induction chemotherapy
5.5 Documentation sheet CARBO/ETO-96h
5.6 Documentation sheet Tandem high-dose chemotherapy (1st HDCT and 2nd HDCT)

Ch
em
oth
era
py
Do
cum
en
tati
on
Sh
ee
ts
HIT
-MED
Th
era
py
Gu
idan
ce
Ve
rsio
n 4
.0 –
02
May
20
17
2
9
5.1
. D
ocu
me
nta
tio
n s
he
et
SK
K c
he
mo
the
rap
y
Pre
vio
us
the
rap
y e
lem
en
t:_
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
_ E
nd
da
te:_
__
__
__
__
__
__
__
__
__
C
ycl
op
ho
sph
am
ide
(1x
800
mg/
m²/
d x
3d)
Me
sna
Vin
cris
tin
e
(1x
1.5
mg/
m²/
d x
1d, m
ax
2 . 0
mg)
i. v
tr.
Me
tho
tre
xa
te*
(� 1
x (1
-) 2
mg/
d x
4d
� n
ot in
dica
ted)
Me
tho
tre
xa
te i
. v
.
(1x
5g/m
² x 1
d)
Leu
cov
ori
n r
esc
ue
Vin
cris
tin
e
(1x
1.5
mg/
m²/
d x
1d, m
ax
2 . 0
mg)
i. v
tr.
Me
tho
tre
xa
te*
(� 1
x (1
-) 2
mg/
d x
2d
� n
ot in
dica
ted)
Me
tho
tre
xa
te i
. v
.
(1x
5g/m
² x1d
)
Leu
cov
ori
n r
esc
ue
Vin
cris
tin
e
(1x
1.5
mg/
m²/
d x
1d, m
ax
2 . 0
mg)
i. v
tr.
Me
tho
tre
xa
te*
(� 1
x (1
-) 2
mg/
d x
2d
� n
ot in
dica
ted)
Ca
rbo
pla
tin
(1x
200
mg/
m²/
d x
3d)
Eto
po
sid
e
(1x
150
mg/
m²/
d x
3d)
i. v
tr.
Me
tho
tre
xa
te*
(� 1
x (1
-) 2
mg/
d x
4d
� n
ot in
dica
ted)
MR
I O
utc
om
e
Cy
cle
1
we
igh
t: _
__
.__
kg
he
igh
t: _
__
__
cm
bo
dy
surf
ace
__
_._
__
__
_m
²
Dat
e:
__
_._
__
.__
__
_
CY
C:
__
x__
.__
mg/
d
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
MT
X:
__
.__
g
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
MT
X:
__
.__
g
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
CA
RB
O:
__
x__
.__
mg/
d
ET
O:
__
x__
.__
mg/
d
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
__
_._
__
.__
__
_
�C
R
�P
R
�SD
�P
D
Cy
cle
2
we
igh
t: _
__
.__
kg
he
igh
t: _
__
__
cm
bo
dy
surf
ace
__
_._
__
__
_m
²
Dat
e:
__
_._
__
.__
__
_
CY
C:
__
x__
.__
mg/
d
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
MT
X:
__
.__
g
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
MT
X:
__
.__
g
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
CA
RB
O:
__
x__
.__
mg/
d
ET
O:
__
x__
.__
mg/
d
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
__
_._
__
.__
__
_
�C
R
�P
R
�SD
�P
D
Cy
cle
3*
*
we
igh
t: _
__
.__
kg
he
igh
t: _
__
__
cm
bo
dy
surf
ace
__
_._
__
__
_m
²
Dat
e:
__
_._
__
.__
__
_
CY
C:
__
x__
.__
mg/
d
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
MT
X:
__
.__
g
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
MT
X:
__
.__
g
VC
R:
__
.__
mg
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
Dat
e:
__
_._
__
.__
__
_
CA
RB
O:
__
x__
.__
mg/
d
ET
O:
__
x__
.__
mg/
d
i. v
tr.
MT
X:
__
x__
mg
� f
ull
/ �
re
du
ced
do
se
__
_._
__
.__
__
_
�C
R
�P
R
�SD
�P
D
Re
-Su
rge
ry:
Dat
e:
__
_._
__
_._
__
__
__
Pro
ced
ure
:
__
_._
__
.__
__
_
�C
R
�P
R
�SD
�P
D
Co
nti
nu
e t
he
rap
y w
ith
:__
__
__
__
__
__
__
__
__
__
__
__
__
_
*i.
vtr.
MTX
mu
st o
nly
be
use
d b
y ce
ntr
es
wit
h r
esp
ect
ive
exp
eri
en
ce (
see
gu
ide
line
s ch
apte
r 8
.6)
**
Cyc
le 3
is n
ot
ind
icat
ed
in a
ll sc
he
du
les,
cro
ss o
ut
if n
ot
ind
icat
ed

Chemotherapy Documentation Sheets
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 30
5.2. Documentation sheet Modified SKK chemotherapy
Previous therapy element:________________________________ End date:___________________
Cyclophosphamide (1x 800 mg/m²/d x 3d) Mesna Vincristine (1x 1 . 5 mg/m²/d x
1d, max 2 . 0 mg)
No HD-MTX in
modified SKK
chemotherapy!
Carboplatin (1x 200 mg/m²/d x 3d)
Etoposide (1x 150 mg/m²/d x 3d)
MRI Outcome
Cycle 1
Weight:
___.___kg
Height:
_____cm
Body surface
___.______m²
Date: ___.___._____
CPM: __x__.__ mg/d
VCR: __.__ mg
� Full / � reduced dose
Date: ___.___._____
Carbo: __x__.__ mg/d
Eto: __x__.__ mg/d
� Full / � reduced dose
___.___._____
�CR
�PR
�SD
�PD
Cycle 2
Weight:
___.___kg
Height:
_____cm
Body surface
___.______m²
Date: ___.___._____
CPM: __x__.__ mg/d
VCR: __.__ mg
� Full / � reduced dose
Date: ___.___._____
Carbo: __x__.__ mg/d
Eto: __x__.__ mg/d
� Full / � reduced dose
___.___._____
�CR
�PR
�SD
�PD
Cycle 3*
Weight:
___.___kg
Height:
_____cm
Body surface
___.______m²
Date: ___.___._____
CPM: __x__.__ mg/d
VCR: __.__ mg
� Full / � reduced dose
Date: ___.___._____
Carbo: __x__.__ mg/d
Eto: __x__.__ mg/d
� Full / � reduced dose
___.___._____
�CR
�PR
�SD
�PD
Cycle 4*
Weight:
___.___kg
Height:
_____cm
Body surface
___.______m²
Date: ___.___._____
CPM: __x__.__ mg/d
VCR: __.__ mg
� Full / � reduced dose
Date: ___.___._____
Carbo: __x__.__ mg/d
Eto: __x__.__ mg/d
� Full / � reduced dose
___.___._____
�CR
�PR
�SD
�PD
Cycle 5*
Weight:
___.___kg
Height:
_____cm
Body surface
___.______m²
Date: ___.___._____
CPM: __x__.__ mg/d
VCR: __.__ mg
� Full / � reduced dose
Date: ___.___._____
Carbo: __x__.__ mg/d
Eto: __x__.__ mg/d
� Full / � reduced dose
___.___._____
�CR
�PR
�SD
�PD
Re-Surgery:
Date:
___.____._______
Procedure:
___.___._____
�CR
�PR
�SD
�PD
Continue therapy with:___________________________
* Cycles 3–5 are not indicated in all schedules, cross out if not indicated

Chemotherapy Documentation Sheets
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 31
5.3. Documentation sheet Maintenance chemotherapy
Previous therapy element:________________________________ End date:___________________
Cisplatin (1 x 70 mg/m²/d x
1d)
Lomustine (1 x 75 mg/m²/d x
1d)
VCR (1 x 1 . 5 mg/m²/d x 1d, max
2 . 0 mg)
VCR (1 x 1 . 5 mg/m²/d x 1d, max 2 . 0 mg)
VCR (1 x 1 . 5 mg/m²/d x 1d, max 2 . 0 mg)
MRI Outcome
Cycle 1
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
Cycle 2
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose:: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
___.___._____ �CR
�PR
�SD
�PD
Cycle 3
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose:: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
Cycle 4
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
___.___._____ �CR
�PR
�SD
�PD
Cycle 5*
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
Cycle 6*
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
___.___._____ �CR
�PR
�SD
�PD
Cycle 7*
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
Cycle 8*
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Date:___.___._____ Date:___.___._____
� Full / � reduced dose:: Cisplatin: _____.___mg
CCNU: _____.___mg
VCR: ___x ___.___mg
___.___._____ �CR
�PR
�SD
�PD
Continue therapy with:___________________________
* Cycle 5-8 is not indicated in all schedules, cross out if not indicated

Chemotherapy Documentation Sheets
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 32
5.4. Documentation sheet Intensified Induction chemotherapy
Previous therapy element:________________________________ End date:___________________
Cisplatin (1 x 3 . 5 mg/kg/d x 1d)
VCR (1x 0 . 05 mg/kg/d x 1d, max. 2 . 0 mg)
Etoposide (1x 4 mg/kg/d x 2d)
Cyclophosphamide (1x 65 mg/kg/d x 2d)
Mesna
i. vtr. MTX (1 x (1-) 2 mg/d x 4d)*
Methotrexate (1x 5g/m²/d x 1d)
Leucovorin rescue
Vincristine (1x 0 . 05 mg/kg/d x 1 d, max.
2 . 0 mg)
i. vtr. MTX (1 x (1-) 2 mg/d x 2d) )*
MRI Outcome
Cycle 1
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____
Cisplatin: ___ x ___.___mg
VCR: ___ x ___.___mg
Eto: ___ x ______mg
Cyclo: ___ x ______mg
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
Date:___.___._____
Methotrexate: ____.___g
VCR: ____.___mg
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
___.___._____ �CR
�PR
�SD
�PD
Autologous stem cell collection: ___.____.________ ____x108 nucleated cells /kg
____x106 CD34+ cells /kg
Cycle 2
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____
Cisplatin: ___ x ___.___mg
VCR: ___ x ___.___mg
Eto: ___ x ______mg
Cyclo: ___ x ______mg
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
Date:___.___._____
Methotrexate: ____.___g
VCR: ____.___mg
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
Cycle 3
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____
Cisplatin: ___ x ___.___mg
VCR: ___ x ___.___mg
Eto: ___ x ______mg
Cyclo: ___ x ______mg
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
Date:___.___._____
Methotrexate: ____.___g
VCR: ____.___mg/kg
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
___.___._____ �CR
�PR
�SD
�PD
Continue with high-dose chemotherapy only if good response!
Continue therapy with:___________________________
*i. vtr. MTX must only be used by centres with respective experience (see guidelines chapter 8.6)

Chemotherapy Documentation Sheets
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 33
5.5. Documentation sheet CARBO/ETO-96h chemotherapy
Previous therapy element:________________________________ End date:___________________
Carboplatin (1 x 200 mg/m²/d x 4d continuous)
Etoposide (1 x 100 mg/m²/d x 4d continuous)
i. vtr. MTX (1 x (1-) 2 mg/d x 4d continuous)*
MRI Outcome
Cycle 1
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____ Carboplatin: ___ x ______mg/d
Eto: ___ x ______mg/d
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
Cycle 2
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____
Carboplatin: ___ x ______mg/d
Eto: ___ x ______mg/d
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
___.___._____ �CR
�PR
�SD
�PD
Autologous stem cell collection: ___.____.________ ____x108 nucleated cells /kg
____x106 CD34+ cells /kg Cycle 3
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Date:___.___._____
Carboplatin: ___ x ______mg/d
Eto: ___ x ______mg/d
i. vtr. MTX: ___ x ______mg
� Full / � reduced dose
___.___._____ �CR
�PR
�SD
�PD
Continue with high-dose chemotherapy only if good response!
Continue therapy with:___________________________
*i. vtr. MTX must only be used by centres with respective experience (see guidelines chapter 8.6)

Chemotherapy Documentation Sheets
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 34
5.6. Documentation sheet Tandem high-dose chemotherapy (1st HDCT and 2nd HDCT)
Previous therapy element:________________________________ End date:___________________
1. HDCT:
Carboplatin (1 x 500 mg/m²/d x 4d) Etoposide (1 x 250 mg/m²/d x 4d)
i. vtr. MTX (1 x (1-) 2 mg/d x 4d) )* ASCT
G-CSF
MRI Outcome
1. HDCT
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Start date: ___.___._____
Carboplatin ___ x _______mg/d
Etoposide ___ x _______mg/d
i. vtr. MTX: ___ x _______mg
� Full dose / � reduced dose:
ASCT date: ___.___._____
2. HDCT:
Thiotepa (1 x 300 mg/m²/d x 3d)
Cyclophosphamide (1 x 1500 mg/m²/d x 3d)
Mesna i. vtr. MTX: (1 x (1-) 2 mg/d x 4d) )* ASCT
G-CSF
2. HDCT
Weight: ___.___kg
Height: _____cm
Body surface
___.______m²
Start date: ___.___._____
Thiotepa ___ x _______mg/d
Cyclophosphamide ___ x _______mg/d
i. vtr. MTX: ___ x _______mg
� Full dose / � reduced dose:
ASCT date: ___.___._____
___.___._____ �CR
�PR
�SD
�PD
Continue therapy with:___________________________
*i. vtr. MTX must only be used by centres with respective experience (see guidelines chapter 8.6)

Surgery recommendations
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 35
6. Surgery recommendations
6.1. Interventions for elevated intracranial pressure
In case of hydrocephalus at presentation, a preoperative third ventriculostomy might be helpful to
normalise CSF flow and to allow tumour surgery with normalised CSF pressure. An transient alternative
way to treat this condition would be the external ventricular drain.
The implantation of a permanent VP-shunt should be avoided whenever possible.
6.2. Tumour resection
Maximal safe surgery is recommended at diagnosis. The tumour resection must not incur any excessive
risk of postoperative neurological deficits. Preservation of function should be deemed more important
than complete resection.
Tumour resection in patients with medulloblastoma, ependymoma, CNS embryonal tumour or
pineoblastoma should only be conducted in centres with respective experience in this field. As
postoperative adjuvant treatment modalities are always required in these histologies, the availability
or referral to an appropriate paediatric oncology section must be timely considered.
Fresh frozen tissue for further pathological and molecular biological evaluations should be gathered
for all patients.
Although maximum safe surgical resection should remain the standard of care, surgical removal of
small portions of medulloblastoma is not recommended when the likelihood of neurological morbidity
is high because there is no definitive benefit to gross total resection compared with near-total
resection.
A neurosurgical second opinion might be helpful in doubtful cases.
Note:
MBEN are very sensitive to chemotherapy and typically present with a “grape like” appearance on the
MRI in young children (mostly <3 years) with posterior fossa tumour. In this case surgery should
consider good prognosis even in incompletely resected tumours.

Surgery recommendations
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 36
MRI with typical “grape like” appearance of MBEN. Note the typical frontal bossing, which can typically
also be observed clinically. Courtesy of M. Warmuth-Metz, Department of Neuroradiology, University
of Wuerzburg.
6.3. Further surgery/surgery for residual tumours
In case of residual postoperative tumour or nodular metastatic disease, the feasibility of a resection
should be evaluated regularly during the course of the treatment. Re-surgery should be considered if
a significant reduction of tumour mass is deemed realistic with adequate risks. If possible, gross total
resection should be aimed at, but subtotal resection may be acceptable in large tumours.
Second surgery planned before the onset of postoperative adjuvant treatment (either radiotherapy or
chemotherapy) should be performed early after first surgery. Moreover, further surgery should be
considered during the treatment course. The time points given in the description of therapy regimens
should be considered as suggestions. Surgery is possible at any time during the treatment.
Please note that re-surgery is a very effective treatment for patients with ependymoma and residual
tumour. As prognosis for patients with persistent residual tumour is impaired, the possibility of re-
surgery should diligently be evaluated for patients with ependymoma.
6.4. Implantation of Rickham or Ommaya reservoir
Please note, that i. vtr. MTX treatment should only be considered in centres with respective experience
with this treatment.
Patients with scheduled i. vtr. treatment need a Rickham or Ommaya reservoir. The reservoir should
be implanted postoperatively as soon as the patients’ condition allows the operation, which
sometimes may be after initiation of postoperative adjuvant therapy.
A perioperative single shot antibiotic treatment with e. g. cefuroxime should be considered. Small
reservoir sizes should be preferred for implantation to avoid dead space in the system. Ample incisions
and placement of the suture besides the reservoir may help to prevent wound dehiscence. The

Surgery recommendations
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 37
perforated area at the end of the used catheters should be as short as possible. It occurs that the
reservoir catheter is misplaced, even if cerebrospinal fluid can be aspirated. Therefore, a radiological
control of the catheter placement by CT or MRI is recommended.
In case of questionable CSF flow functionality (diffuse and widespread metastases, high CSF pressure,
high CSF protein, and clinical signs of hydrocephalus are known risk factors), a CSF flow scintigraphy
can be performed (Chamberlain 1998). If there is access to the ventricular system prior to reservoir
implantation, due to e. g. an external ventricular drain, also the administration of a contrast agent and
subsequent imaging is possible to examine the CSF circulation. Given clinical or neuroradiological signs
of a compartmentalised or otherwise obstructive hydrocephalus, the reservoir implantation should
not be performed. Non-metastatic patients with permanent shunts should not receive i. vtr. MTX.
The presence of a permanent shunt does not exclude i. vtr. MTX application as such, and is therefore
no contraindication for reservoir implantation. If a permanent shunt is needed, the free circulation of
CSF should be assessed either by scintigraphy or contrast agent administration. If allowed by national
regulations, devices with on-off-valves should be preferred and may assure higher Methotrexate CSF-
levels. Programmable shunts do not guarantee that no Methotrexate is distributed into the
peritoneum and tend to break down after several adjustments. On-off-valve reservoirs should only be
implanted frontally as an occipital implanted device might be unintentionally deactivated. Either way,
the families should be informed about the possibility of accidental closure of this kind of reservoir
system which might lead to increased intracranial pressure.
Another strategy to handle intraventricular administration of Methotrexate in patients with a
permanent shunt is to withdraw 10 ml CSF prior to the injection of Methotrexate. This is only possible
if the ventricles are wide enough to allow the removal of this amount CSF, but will prevent an opening
of the shunt valve until the withdrawn CSF is reproduced.
After therapy the reservoir may maintain in the patient or be explanted according to the guidelines of
the treatment centre. If an explantation is planned, it should take place within one year after
treatment, as the possibility of complications as a result of explantation may increase after a longer
time span.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 38
7. Description of radiotherapy elements 7.1. Medulloblastoma, CNS Embryonal Tumour and Pineoblastoma ........................................ 39
7.1.1. Timing of Radiotherapy (RT) .......................................................................................... 39
7.1.2. Equipment ..................................................................................................................... 39
7.1.3. Energy (craniospinal/local RT) ....................................................................................... 39
7.1.4. Treatment Position ........................................................................................................ 39
7.1.5. RT Planning .................................................................................................................... 40
7.1.6. Treatment volume, anatomical description and dose .................................................. 40
7.1.7. Organs at Risk (OAR)...................................................................................................... 42
7.1.8. Dose Specification ......................................................................................................... 42
7.1.9. Reference Points ........................................................................................................... 42
7.1.10. Treatment Verifications ................................................................................................. 43
7.1.11. Rests .............................................................................................................................. 43
7.1.12. Treatment Technique and Volumes .............................................................................. 43
7.1.13. Treatment Modifications due to haematological Toxicity ............................................ 44
7.1.14. Dose prescriptions ......................................................................................................... 44
7.1.15. Fractionation ................................................................................................................. 46
7.2. Ependymoma ....................................................................................................................... 46
7.2.1. Timing of radiotherapy .................................................................................................. 46
7.2.2. Equipment ..................................................................................................................... 46
7.2.3. Conformal/ 3D Radiotherapy ........................................................................................ 46
7.2.4. Target Volumes ............................................................................................................. 47
7.2.5. Metastatic Deposits (Ependymoma) ............................................................................. 48
7.2.6. Organs at Risk (OAR)...................................................................................................... 48
7.2.7. Dosimetry ...................................................................................................................... 48
7.2.8. Treatment technique ..................................................................................................... 48
7.2.9. Dose prescriptions ......................................................................................................... 49
7.2.10. Dose to Organs at Risk ................................................................................................... 51
7.3. Dose Constraints and Organs at Risk for Medulloblastoma, Ependymoma, CNS Embryonal
Tumour and Pineoblastoma .............................................................................................................. 51
7.3.1. Dose constraints ............................................................................................................ 51
7.3.2. Organs at Risk (OAR)...................................................................................................... 52

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 39
7.1. Medulloblastoma, CNS Embryonal Tumour and Pineoblastoma
7.1.1. Timing of Radiotherapy (RT)
For all patients older than 3 years with CMB, AMB and LCMB (older than 5 years for DMB) without
metastases (M0), radiotherapy should start less than 4 weeks after surgery. Patients to adjuvant PNET
5 radiotherapy treatment should start as soon as possible. If there is a progress under chemotherapy,
radiotherapy should start immediately.
For all patients with CNS embryonal tumour older 4 years without metastases (M0), radiotherapy
should start in less than 40 days after surgery. Patients younger than 3 years (AMB, CMB, LCMB),
younger than 5 years (DMB, MBEN) without metastases (M0) and patients with metastases (M+)
should start with chemotherapy first, followed by radiotherapy.
7.1.2. Equipment
Patients should be treated using conformal radiation therapy treatment planning and delivery
techniques. IMRT techniques will be allowed assuming that appropriate departmental QA procedures
are available and prospectively approved by the national co-ordinator. A primary IMRT approach
(including arcing techniques e.g. tomotherapy, VMAT, RapidArc) should ensure adequate irradiation
of the target volume allowing for tissue heterogeneity and the junction between the cranial fields and
spinal field can be precisely calculated and implemented and a sufficient dose gradient is employed
over the vertebral bodies to ensure symmetrical bone growth arrest. All patients should be treated on
isocentric linear accelerators with a minimum source-to-axis distance (SAD) of 80 cm. Megavoltage
photons with a nominal energy ≥ 4 MV should be used. Treatment with ⁶⁰Co should be avoided.
The use of electron spinal fields may be acceptable, provided a beam of sufficient energy is available
to ensure adequate irradiation of the target volume allowing for tissue heterogeneity and the junction
between the photon cranial fields and spinal electron field can be precisely calculated and
implemented.
Equally, primary proton therapy is acceptable. If proton beams are delivered using passive scattering
technology: appropriate beam energy, range of spread out Bragg peak, collimators and compensators
are individualised for each beam.
If spot scanning technology is used, conformality will be achieved by treatment planning, software
steering and control systems. Hardware accessories will not necessarily need to be used. However,
attention should be paid to achieve sharp penumbra and appropriate energy (reducing of air gap, slim
range shifter, avoiding neutron production etc.).
7.1.3. Energy (craniospinal/local RT)
Cranial (whole brain) fields shall be treated with megavoltage photons with energies in the range of 4–
6 MeV. Energies higher than 6 MeV should be avoided due to the risk of under-dosing the lateral
meninges. Tumour bed RT can be given with a higher energy if deemed dosimetrically beneficial.
Photons of 4–6 MeV will generally be used for spinal irradiation but electrons of suitable energy or
protons can be used as an alternative.
7.1.4. Treatment Position
Patients should be immobilised using an immobilisation device according to departmental policies. The
patient should be maintained in the same position for the cranial and spinal components of
craniospinal radiotherapy (CSRT) for the duration of this treatment phase. For local radiotherapy
patients should be treated in the supine position. Use of immobilization devices is mandatory. In
selected cases a boost to the posterior fossa can also be applied in prone position provided that an
adequate head fixation can be achieved.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 40
For young children, deep sedation or general anaesthesia is strongly recommended.
7.1.5. RT Planning
A planning CT should be done for the definition of the target volumes of both craniospinal axis and
posterior fossa (tumour bed SIOP PNET 5). It is strongly recommended that the CT slice thickness
should be no greater than 4.8 mm in the region of the cribriform fossa, base of skull, posterior fossa
and cranio-cervical field junction (ideally 2.4 mm or smaller), and no greater than 8 mm elsewhere
within the craniospinal axis.
If the spinal field is treated with electron beams the dose along the entire spinal axis should be
calculated with an appropriate correction for tissue heterogeneity.
7.1.5.1. Treatment Planning Images for Boost
A treatment planning CT (or MRI) with the patient in the treatment position is required. CT slices
thickness should be no greater than 2.4 mm. Planning CT images should be registered with diagnostic
MR images obtained at the same time point (last week of conformal radiotherapy phase).
7.1.6. Treatment volume, anatomical description and dose
7.1.6.1. Target Volume
Target volumes should be defined according to ICRU 50/62 guidelines. Delineation of all target volumes
is based on a planning CT with i. v. contrast and or CT/MR image fusion and will be outlined on each
slice of the planning scan.
7.1.6.2. Craniospinal Axis
The clinical target volume (CTV) for CSRT comprises the whole brain as well as the spinal cord and
thecal sac.
7.1.6.3. Whole Brain Volume
The whole brain CTV should extend anteriorly to include the entire frontal lobe and cribriform plate
region. In order to include the cribriform fossa within the CTV and allowing an additional appropriate
margin for PTV, the edge of the field (i. e. the geometric edge of the shielding block) would in many
cases include the lenses.
If a conventional technique is applied, the geometric edge of the shielding should extend at least
0.5 cm inferiorly below the cribriform plate and at least 1 cm elsewhere below the base of the skull.
The margin between the shielding and the anterior border of the upper cervical vertebrae should be
0.5 cm. The lower border of the cranial fields should form a precise match with the upper border of
the spinal field.
The CTV should include any herniation of the meninges through the craniotomy scar.
No consensus is existing concerning the inclusion of the optic nerves especially in IMRT technologies
and proton therapy.
7.1.6.4. Posterior Fossa
The posterior fossa CTV is defined as:
Ø meninges/superiorly – the tentorium cerebelli
Ø meninges/inferiorly – the extension of the spinal meninges should include the first
upper cervical segment
Ø meninges/anteriorly – the anterior edge of the brain stem
Ø meninges/posteriorly – the posterior extension of the meninges to the inner table of the
skull
The CTV should include all herniations of the meninges through the craniotomy defect.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 41
Ø laterally – the lateral extension of the meninges around the cerebellum
7.1.6.5. Cervical spinal Volume
The spinal field should extend superiorly to form an accurate match with the border with the lower
borders of the cranial fields.
7.1.6.6. Dorso-lumbar Spine Volume
The inferior limit of the spinal CTV should be determined by imaging the lower limit of the thecal sac
on a spinal MRI performed as part of the staging process. The treatment field edge should be set 8 mm
below the lowest point of the thecal sac as visualised on MRI.
7.1.6.7. Width of the spinal Volume
The aim is to include the entire subarachnoid space including the extensions along the nerve roots as
far as the intervertebral foramina. Thus the spinal CTV should extend laterally to cover the
intervertebral foramina. An additional margin, generally 1.0 cm on either side should be added for PTV,
and an appropriate field width chosen to allow for this, depending on the geometric precision of the
technology applied. The use of a ‘spade’ shaped field to treat the lumbo-sacral spine is not
recommended.
7.1.6.8. Tumour Bed Volume (e. g. SIOP PNET 5, CNS Embryonal Tumour/Pineoblastoma)
In the SIOP PNET 5 study, the local boost (tumour site only) will be investigated. Patients with
medulloblastoma (CMB, DMB only), which are not included in clinical trials, should also receive
irradiation of the tumour site (COG ACNS 0331, ISPNO/ASTRO 2016). This is only available for patients
with clinically low risk (without metastatic disease and without residual tumour). For details see 4.3.
For patients with other subtypes of a medulloblastoma (LCA, MBEN) and clinically high-risk
medulloblastoma (with metastatic disease), irradiation of the posterior fossa is mandatory (for details
see 4.4 and 4.5).
The definition of the tumour bed is also valid for CNS embryonal tumours and pineoblastoma.
The GTV includes all gross residual tumour and/or the walls of the resection cavity at the primary site,
based on the initial imaging examination that defines the tissue initially involved with disease
anatomically and the post-operative and pre-irradiation neuro-imaging examinations. The GTV will
have to take into account any anatomical shift or changes after surgery.
The CTV includes the GTV with an added margin that is meant to treat sub-clinical microscopic disease
and is anatomically confined (i. e. the CTV is limited to the confines of the bony calvarium and
tentorium where applicable). The CTV is defined as the GTV plus a 1.0 cm margin except at bone or
tentorial interface where it remains within the confines of the posterior fossa.
The PTV is defined as the CTV plus an additional 0.3–0.5 cm margin depending on geometric precision
of the technology applied. The size of the required margin will depend on the quality of the
immobilisation device chosen and the departmental reproducibility records for the patient position
and chosen device. If the treating oncologist feels that a 0.5 cm margin is insufficient as a CTV/PTV
margin, the national reference centre should be informed and the case should be discussed. CAVE: The
final PTV should not extending beyond the boundaries of a “classical” PTV when the entire posterior
fossa is defined as CTV unless clinically indicated.
A field arrangement using 3D conformal planning is a useful requirement. At least the use of posterior
oblique fields is strongly recommended. The purpose of this is to minimise the RT dose to the middle
ears and temporal lobes. A beam arrangement of a parallel opposed pair is not permitted.
By using a reproducible head fixation system the safety margins between CTV and PTV for the posterior
fossa irradiation can be reduced down to 2–3 mm.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 42
7.1.6.9. Metastatic Deposits (Embryonal Tumour/MB/Pineoblastoma):
For intracranial metastasis: It is strongly recommended that the CTV for metastatic deposits should be
determined on a planning CT including CT/MR image fusion. The safety margin for CTV circulating sites
is 0.5 cm considering anatomical borders. Definition of CTV is based on post-chemotherapeutical or
postoperative imaging. For PTV, an additional margin should be allowed according to departmental
policy depending on the geometric precision. The field arrangement will be chosen to provide a high
conformity index, avoiding OAR where possible.
For spinal sites the safety margins to visible tumour in cranio-caudal direction should be the length of
one vertebral body. Postoperative imaging should be used in case of surgical resection. Laterally the
field border should encompass the pedicles.
7.1.7. Organs at Risk (OAR)
For organs at risk and dose constraints see 7.3.
The supratentorial volume for the OAR definition is defined as whole brain volume (down to the
foramen magnum) minus the posterior fossa volume.
7.1.8. Dose Specification
Dose Definition: All doses will be specified according to ICRU 50/62.
7.1.9. Reference Points
7.1.9.1. Brain
If the brain is treated by a pair of parallel opposed fields, the dose should be defined at the midpoint
of the central axis.
7.1.9.2. Spine
The dose to the spine should be prescribed along the central axis at a depth representing the posterior
margin of the vertebral bodies.
In the case of electron RT to the spine, the anterior border of the target volume (posterior aspect of
the vertebral bodies) must be encompassed within the 85 % isodose (ICRU 71 report).
In general, in electron therapy, the beam energy and the beam delivery system are adjusted so that
the maximum of the depth-dose curve on the beam axis (peak dose) is reached at the centre (or in the
central part) of the PTV. This point is selected as the ICRU Reference Point for reporting.
No strict recommendations can be given in this setting. In general, details with 85–90 % should be
considered and individually be adapted (ICRU 71 report).
7.1.9.3. Tumour Bed Boost
The primary tumour bed should be treated using a suitable technique, that allows for the least amount
of normal brain tissue and organs to be at risk from exposure to high dose irradiation. The prescription
point should be the isocentre unless an IMRT technique is used.
7.1.9.4. Dose Uniformity
Dose variations across the target volume should be within +7 % and –5 % of the prescription point
referring to ICRU 50/62/83 recommendations. If technically achievable, the dose variation should
preferentially be kept within ±5 %. An effort should be made to spare the cochlea and middle ear,
especially in combination with subsequent platinum based consolidation chemotherapy.
7.1.9.5. Field Shaping
The use of customised divergent beam blocks or multi-leaf collimators using beam’s eye view facilities
is strongly recommended.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 43
7.1.9.6. Metastatic Deposit
The prescription point is at or near the isocentre unless an IMRT technique is adopted.
7.1.10. Treatment Verifications
Regular treatment verification according to institutional policies is required. As a minimum standard,
weekly portal images should be performed and the set-up variations recorded.
7.1.11. Rests
There should be no planned rests. Delays due to machine services and bank holidays should be avoided
whenever possible.
7.1.12. Treatment Technique and Volumes
No detailed recommendations can be made regarding specific treatment technologies. IMRT
technologies and proton therapy are increasingly used providing a conformal 3D approach.
For craniospinal irradiation, a homogenous dose distribution should be provided throughout the whole
brain including meninges and spinal canal. If a classical treatment technique is given, the following
recommendations should be followed.
7.1.12.1. Volumes
Cranial RT: The cranial fields will be treated with lateral opposed fields.
Spine Irradiation: If possible, the spinal volume should be treated with a single posterior field. If necessary the spinal
field can be treated at an extended FSD. The exit from the spinal field should not include the teeth and
jaw.
Junctions: Junctions of abutting fields should be moved on a regular basis either intra-fractionally, daily or by
other predefined time points (moving junction technique).
Posterior Fossa/primary Tumour Bed Volume: It is strongly recommended, that this volume is treated conformal. The field arrangement should be
chosen to provide a high conformity index and to minimise the RT dose to the OAR.
7.1.12.2. Technologies
Intensity Modulated Radiotherapy (IMRT)/Proton: Today, different technologies are available (Conformal, ARC-Technologies). These may individually be
used to reduce the total dose to the cochlea and other organs at risk. If centres employ IMRT-
technologies/proton therapy, then it will be essential to observe strict criteria for immobilisation and
departmental quality assurance.
Proton Beam Therapy: Proton beam therapy will be done according to the ICRU 78 report. Dosimetry, geometric and dose-
volume terms, treatment planning, uncertainties in dose delivery, motion management, quality
assurance, prescribing, recording and reporting treatment will be done according to the ICRU 78 report
for proton beam therapy. Proton beam therapy is attractive to reduce dose to normal tissues i. e.
cochlea, lenses, non-involved brain or pituitary gland. Due to smaller volume receiving a low or
medium dose, theoretically also the risk for secondary malignancies may decrease. As there is some
uncertainty about increased RBE (relative biological effectiveness) as the distal Bragg peak, weighting
of spots and Bragg peaks need to be carefully evaluated. The use of multiple field techniques might be
preferable if high weighted spots cumulate in critical areas. As with conventional treatment, organ
tolerances as well as target coverage are to be respected.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 44
An adequate coverage of the entire vertebral body to minimise the risk for asymmetric bone growth
arrest should be provided depending on the age of the patient. No consensus is existing concerning
dose constraints.
In case of proton therapy, the definition of CTV is identical to that with photon therapy.
7.1.13. Treatment Modifications due to haematological Toxicity
Whenever tolerable for the patient, treatment should not be interrupted for anaemia, leukopenia or
thrombocytopenia, unless life-threatening. Blood product or growth factor support should be
instituted according to institutional guidelines (e. g. SIOP PNET 5). Irradiated blood products should be
used at all times. Transfusions are recommended when the haemoglobin levels fall below 6 mmol/l
(10 g/l). Thrombocytes should be transfused as clinically indicated when counts are ≤ 25 ×10⁹/l. In case
of low absolute neutrophil count (≤ 0.5 ×10⁹/l), growth factors should be considered and given
preferably during the weekends. Any treatment interruption should be compensated according to
national or institutional policies.
7.1.14. Dose prescriptions
7.1.14.1. Radiotherapy in therapy flowchart 4.1 (SKK chemotherapy)
a) < 5 years, DMB, MBEN, with or without metastasis (M0/M+) and < 3 years, CMB, AMB, LCMB
without metastasis (M0) if not in CR after 3 cycles of SKK chemotherapy
< 3 years CMB, AMB, LCMB without metastasis (M0) in case of relapse or progressive disease
during chemotherapy, no Vincristine
Number fractions Dose per
fraction
Schedule Dose Duration
[weeks; days]
CSI 15 1.6 Gy 1x daily 24.0 Gy 3; 0
Posterior fossa 17 1.8 Gy 1x daily +30.6 Gy +3; 2
Metastasis 14 1.8 Gy 1x daily +25.2 Gy +2; 4
Total: 32 54.6 Gy 6; 2
b) < 5 years, DMB/MBEN, with or without metastasis (M0/M+), radiotherapy in case of relapse or
progressive disease during chemotherapy: Please contact the HIT-MED study centre.
7.1.14.2. Radiotherapy in therapy flowchart 4.2 (Intensified Induction chemotherapy with response-
adjusted consolidation)
< 4 years, AMB/CMB/LCMB with metastasis (M+)* and less than good response after induction
chemotherapy
3–4 years, AMB/LCMB, CMB with residual tumour (R2–4) or MYC/N+, no Vincristine
Number fractions Dose per
fraction
Schedule Dose Duration
[weeks; days]
CSI 15 1.6 Gy 1x daily 24.0 Gy 3; 0
Posterior fossa +17 1.8 Gy 1x daily + 30.6 Gy +3; 2
Metastasis* +14 1.8 Gy 1x daily + 25.2 Gy + 2; 4
Total 32 54.6 Gy 6; 2 * In case of diffuse spinal metastasis, please contact the HIT-MED study centre

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 45
7.1.14.3. Radiotherapy in therapy flowchart 4.3 (Conventional RT 23.4 Gy + boost with Maintenance
chemotherapy)
> 3 years CMB, > 5 years DMB without metastasis (M0), with no or small (< 1.5 cm²) postoperative
residual tumour (R0); in individual cases, this concept may be considered for R+ patients as well
Please check eligibility for PNET 5 MB in this cohort!
Number fractions Dose per
fraction
Schedule Dose Duration
[weeks; days]
CSI 13 1.8 Gy 1x daily 23.4 Gy 2; 3
Posterior fossa
(PNET 5 patients:
tumour site)
+17 1.8 Gy 1x daily + 30.6 Gy +3; 2
Total 30 54.0 Gy 6; 0
7.1.14.4. Radiotherapy in therapy flowchart 4.4 (Conventional RT 35.2 Gy + boost with Maintenance
chemotherapy)
> 4 years AMB/LCMB with or without isolated CSF metastasis (M0/M1) or MYC/N+
> 4 years CMB and > 5 years DMB with isolated CSF metastasis (M1) or residual tumour (> 1.5 cm²)
> 4 years Pineo without metastasis (M0)
In individual cases, a reduced CSI dose as in flowchart 4.3 may be considered for R+ patients as well.
Number fractions Dose per
fraction
Schedule Dose Duration
[weeks; days]
CSI 22 1.6 Gy 1x daily 35.2 Gy 4; 2
Posterior fossa +11 1.8 Gy 1x daily + 19.8 Gy +2; 1
Total 33 55.0 Gy 6; 3
7.1.14.5. Radiotherapy in therapy flowchart 4.5 (Two cycles of SKK chemotherapy with
hyperfractionated RT and Maintenance chemotherapy)
> 5 years, DMB with M2–M4
> 4 years, AMB/CMB/LCMB with M2-M4
> 4 years, CNS embryonal tumour and pineoblastoma with metastasis (M+)
Number
fractions
Dose
per
fraction
Schedule Dose Duration
[weeks;
days]
CSI 40 1.0 Gy 2x daily 40.0 Gy 4; 0
Tumour site +28 (cum. 68 Gy)
1.0 Gy 2x daily +28 Gy +2; 4
Posterior fossa +20 (cum. 60 Gy)
1.0 Gy 2x daily +20 Gy + 2;0
Supratentorial
metastasis +20 1.0 Gy 2x daily +20 Gy +2; 0
Spinal metastasis +10 1.0 Gy 2x daily +10 Gy +1; 0
Total 68 68 Gy (residual tumour:
72 Gy)
6; 4 (7; 1)

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 46
7.1.14.6. Radiotherapy in therapy flowchart 4.9 (CARBO/ETO induction with response-adjusted
consolidation)
< 4 years, CNS embryonal tumour and pineoblastoma, with or without metastasis (M0/M+) in case
of partial response or progressive disease during chemotherapy, no Vincristine during RT
Number
fractions
Dose
per
fraction
Schedule Dose Duration
[weeks;
days]
CSI 15 1.6 Gy 1×daily 24.0 Gy 3; 0
Metastases +14 1.8 Gy 1× daily +25.2 Gy +2; 4
Tumour
site +17 1.8 Gy 1× daily +30.6 Gy +3; 2
Total 32 54.6 Gy
(metastasis: 49.2 Gy)
6; 2
7.1.14.7. Radiotherapy alternative to therapy flowchart 4.4 (Conventional RT, enhanced dose (35.2 Gy
CSI + boost) with Maintenance chemotherapy) for pineoblastoma
> 4 years, CNS embryonal tumour and pineoblastoma without metastasis (M0)
Number
fractions
Dose
per
fraction
Schedule Dose Duration
[weeks;
days]
CSI 36
22
1.0 Gy
1.6 Gy
2× daily
1× daily
36.0 Gy
35.2 Gy
3; 3
4; 2
Residual
tumour +36 +14
1.0 Gy 1.8 Gy
2× daily 1× daily
+36.0 Gy +25.2 Gy
+3; 3 +2; 4
Tumour
site
+32
+11
1.0 Gy
1.8 Gy
2× daily
1× daily
+32.0 Gy
+19.8 Gy
+3; 1
+2; 1
Total 68 (72)
33 (36)
68.0 Gy (72.0 Gy)
55.0 Gy (60.4 Gy)
6; 4 (7; 1)
6; 3 (7; 1)
7.1.15. Fractionation
All fields should be treated daily 5 days per week.
7.2. Ependymoma
7.2.1. Timing of radiotherapy
The interval between surgery and radiotherapy should be less than 6 weeks.
7.2.2. Equipment
Ø Use of megavoltage photons with a nominal energy ≥ 6MV are strongly encouraged and
obligatory in the SIOP-Ependymoma II Protocol.
Ø Treatment with 60 Co is discouraged and not permitted in the SIOP-Ependymoma II Protocol
Ø IMRT techniques are allowed.
Ø Proton beams may be used.
7.2.3. Conformal/ 3D Radiotherapy
Radiotherapy should be delivered using 3D-conformal treatment planning and delivery techniques that
require:
a. 3-D imaging data (CT and/or MR) acquisition with the patient in the treatment position.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 47
b. Imaging data are utilized to delineate and reconstruct in three dimensions the gross tumour
volume (GTV), the clinical target volume (CTV), the planning target volume (PTV), critical
structures, and patient anatomy.
c. Beam geometry in three dimensions is defined on an individual base taking into account
structures traversed by each single beam as visualised by the beam’s eye view.
d. Dose distribution to the target and organs at risk is calculated on a point-by-point basis in the
three dimensions.
7.2.4. Target Volumes
Target volumes are defined according to the ICRU 50/62/78/83 reports.
MRI obtained immediately before radiotherapy should be used for treatment planning. To properly
delineate target volumes, complete information defining the extent of disease before and after surgery
are needed. Pre- and post-operative MRI, in particular pre- and post-gadolinium contrast T1, T2, and
FLAIR sequences, should be reviewed. Sequences that best define post-operative tumour bed and
residual disease at each time point should be utilised to define the GTV and registered to planning CT.
Photon definition for GTV, CTV, and PTV
Gross Tumour Volume (GTV): the GTV includes the tumour bed at the primary site and macroscopic
residual tumour after surgery. The pre-operative imaging defines all the tissues and anatomical areas
initially involved with disease. The post-operative and pre-irradiation MRI define the residual disease
and the possibly collapsed post-surgical tumour bed which is the edge of the resection cavity. It is
strongly suggested to register the best pre-operative MRI sequence showing tumour extension and to
contour a structure denominated GTV pre-operatively to better identify relations between tumour and
surrounding normal tissue anatomically involved. Tissue defects from surgical procedures should not
be included in GTV if not involved by tumour. In case of discrepancies between intra-operative finding
and imaging, the larger volume will define the GTV
Clinical Target Volume (CTV): the CTV includes the GTV with an added margin to treat subclinical
microscopic disease and is anatomically confined (i.e. the CTV is limited to the confines of the bony
calvarium, falx and tentorium or extend up to but not beyond neuroanatomic structures surely not
invaded by tumour). The CTV margin will be 0.5 cm for all patients.
CTV for the stereotactic boost, if persistent macroscopic disease (2x 4.0 Gy) is CTV = GTV i.e. no
additional margin to be applied to GTV for CTV. This is to restrict the boost volume as far as possible.
The stereotactic boost, however, should only be given within the SIOP Ependymoma II protocol.
Planning Target Volume (PTV): the PTV is a geometric expansion of the CTV to take into account for
uncertainties in immobilisation, daily patient positioning and image registration. The PTV margin will
be 0.3 cm - 0.5 cm in all directions. The size of the required margins will depend on the quality of the
immobilisation device chosen and the departmental reproducibility records for the patient position
and chosen device.
Proton definition for GTV, CTV and PTV
Gross Tumour Volume (GTV): is the same for photons and protons
Clinical Target Volume (CTV): is the same for photons and protons
Planning Target Volume (PTV): for protons both lateral margins and the margin in depth (relative to
proximal and distal tumour surface) have to be considered. Consequently for each beam orientation
one would need a separate PTV with different margins laterally and along the beam direction, that will
take into account range uncertainties and tissue inhomogeneities. Any individual adaptation is at the
discretion of the local team (radiotherapist and physicist).
Metastatic ependymoma (M1–M3)

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 48
Ø Individual case management is required.
Ø Craniospinal irradiation followed by a boost to the primary tumour site and metastatic
deposits should be considered. The application of treatment technologies and the definition
of CTV and PTV is identical to chapter 7.1.12.
Ø The treatment concept for the boost of the primary tumour site is identical to the approach in
non-metastatic disease (see above).
7.2.5. Metastatic Deposits (Ependymoma)
For intracranial metastasis: It is strongly recommended, that the CTV for metastatic deposits should
be determined on a planning CT including MR imaging/image fusion. The safety margin for CTV
circulating sites is 0.5 cm considering anatomical borders. Definition of CTV is based on post-
chemotherapeutical or postoperative imaging. For PTV, an additional margin should be allowed
according to departmental policy depending on the geometric precision. The field arrangement will be
chosen to provide a high conformity index, avoiding OAR, where possible.
For spinal sites the safety margins to visible tumour in cranio-caudal direction should be the length of
one vertebral body. Postoperative imaging should be used in case of surgical resection. Laterally the
field border should encompass the pedicles.
7.2.6. Organs at Risk (OAR)
For organs at risk and dose constraints, see 7.3.
7.2.7. Dosimetry
Photon dose is specified in dose-to-water (Gy).
Proton dose is prescribed in cobalt Gray equivalent (Gy1.1) using a recommended value of
radiobiological effectiveness (RBE) of 1.1 (Paganetti et al. 2002). For simplicity all proton doses referred
to in this protocol are the RBE-weighted proton absorbed dose (DRBE) and are the dose of photons
that would produce the same therapeutic effect as a proton absorbed-dose, given under identical
circumstances (ICRU 78).
Prescription point: for photon beams the prescription point is at or near the isocentre unless an IMRT
technique is adopted.
Children younger than 18 months (and older than 12 months) at irradiation without post-surgical
residual disease or children with risk factors, namely multiple surgeries (more than 2) or poor
neurological status should receive 54 Gy
Dose uniformity: at least 95% of the protocol specified dose should encompass 100% of the PTV and
no more than 10% of the PTV should receive 110% of the protocol dose as evaluated by DVH.
N. B.: Attention should be paid to avoid 110% isodose involving normal tissue outside the PTV.
110 % isodose distribution should be confined to the PTV
Metastatic deposits
The prescription point is at or near the isocentre unless an IMRT technique is adopted.
7.2.8. Treatment technique
Patient position: patients may be treated in the supine or prone position. Use of immobilisation devices
is mandatory. Deep sedation or general anaesthesia is strongly recommended for younger children.
Treatment planning images: a treatment planning CT with the patient in the treatment position is
required. CT slices thickness should be ≤4 mm, preferably 2 mm, and the study should be obtained as
close as possible to the start of radiotherapy.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 49
MRI registration: registration of MRI to treatment planning CT is strongly recommended for all
patients.
Treatment planning: computerized treatment planning systems for 3D conformal radiotherapy should
be utilised (DVH, BEV, DRR). Beam geometries and treatment techniques must be selected to minimise
dose to critical organs without compromising dose homogeneity to PTV.
Proton beams: for posterior fossa treatment, rotating gantries seem to be advisable as compared to
horizontal beam lines only capable of achieving lateral beam arrangements. As there is some
uncertainty about increased RBE at the distal Bragg peak, weighting of spots and Bragg peaks need to
be carefully evaluated. The use of multiple field techniques might be preferred if high weighted spots
cumulate in critical areas. As with conventional treatment, organ tolerances as well as target coverage
are to be respected.
Beam shaping: all photon beams should be individually shaped with shielding at least 5HVL thick or
multi-leaf collimation.
If proton beams are delivered using passive scattering technology: appropriate beam energy, range of
spread out Bragg peak, collimators and compensators are individualised for each beam.
If spot scanning technology is used, conformality will be achieved by treatment planning, software
steering and control systems. Hardware accessories will not necessarily need to be used. However,
attention should be paid to achieve sharp penumbra and appropriate energy (reducing of air gap, slim
range shifter, avoiding neutron production etc.).
Treatment verification: regular treatment verification according to institutional policies is required. As
a minimum standard, weekly portal images should be performed and the set-up variations recorded.
Rest: There will be no planned rest or breaks of treatment.
7.2.9. Dose prescriptions
7.2.9.1. Radiotherapy in therapy flowchart 0 (Two cycles Modified SKK chemotherapy with local RT
and response-adjusted maintenance)
All ages, ependymoma without metastasis (M0) with residual disease (R2–4), children 12–18 months
with risk factors (namely multiple surgeries or poor neurological status) will receive 54.0 Gy.
Number
fractions
Dose
per
fraction
Schedule Dose Duration
[weeks;
days]
12–18 months
Tumour site 30 1.8 Gy 1× daily 54.0 Gy 6; 0
Stereotactic boost 2 4.0 Gy* 1× daily 8.0 Gy 0; 2
1.5–4 years
Tumour site 33 1.8 Gy 1× daily 59.4 Gy 6; 3
Stereotactic boost 2 4.0 Gy* 1× daily 8.0 Gy 0; 2
4–21 years
Tumour site 68
33
1.0 Gy
1.8 Gy
2× daily
1× daily
68.0 Gy
59.4 Gy
6; 4
6; 3
Stereotactic boost 4
2
1.0 Gy
4.0 Gy*
2× daily
1× daily
4.0 Gy
8.0 Gy
0; 2
0; 2
* A stereotactic boost according to the SIOP Ependymoma II protocol should be discussed with the
HIT-MED study centre and/or Radiotherapy Reference Centre (2× 4.0 Gy).

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 50
7.2.9.2. Radiotherapy in therapy flowchart 4.7 (Five cycles SKK chemotherapy with local RT)
12–18 months, ependymoma without metastasis (M0), without residual disease (R0), no Vincristine
Number fractions Dose per
fraction
Schedule Dose Duration
[weeks; days]
12–18 months
Tumour site 30 1.8 Gy 1x daily 54.0 Gy 6; 0
7.2.9.3. Radiotherapy in therapy flowchart 4.8 (Local 59.4 Gy conventional or 68 Gy HFRT (local 59.4
Gy conventional RT for children < 4 years))
> 18 months, ependymoma without metastasis (M0) without residual disease (R0)
Number fractions Dose per
fraction
Schedule Dose Duration
[weeks; days]
1.5–4 years
Tumour site 30 1.8 Gy 1× daily 54.0 Gy 6; 0
≥ 4 years
Tumour site 68
33
1.0 Gy
1.8 Gy
2× daily
1× daily
68.0 Gy
59.4 Gy
6; 4
6; 3
7.2.9.4. Radiotherapy in ependymoma, all ages, with metastasis (M+), with/or without residual
disease (R0/R+)
Individual therapy discussion is recommended. Please contact the HIT-MED study centre.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 51
7.2.10. Dose to Organs at Risk
Ø Spinal cord: the spinal cord should be contoured from the inferior border of the foramen
magnum to a length of at least 6 cm caudally. For infratentorial tumours extending beyond the
foramen magnum, the corresponding spinal cord will be excluded at a cumulative physical
dose of 54 Gy. In all other cases, the cervical spinal cord possibly included in the PTV will be
excluded at a cumulative physical dose of 50 Gy.
Ø Brain Stem: the brain stem should be contoured from the superior border of the foramen
magnum to the upper aspect of the mesencencephalon as detected on the most cranial
planning CT slice. For patients receiving prescriptions in excess of 68 Gy an IMRT approach is
in the attempt to spare as much as possible portion of the brain stem at least from the highest
dose levels. No dose constraints at the brainstem at hyperfractionation.
Ø Optic chiasm: should be contoured on at least 2 successive planning CT slices. Optic chiasm
should be excluded at a cumulative treatment dose of 54 Gy or 60 Gy at hyperfractionation.
Ø Cochlea: each cochlea should be contoured on at least 2 successive slices of planning CT as a
circular structure within the petrous portion of the temporal bone. The mean dose to at least
one cochlea should be limited to 30 Gy.
7.3. Dose Constraints and Organs at Risk for Medulloblastoma, Ependymoma, CNS
Embryonal Tumour and Pineoblastoma
7.3.1. Dose constraints
7.3.1.1. Dose constraints for conventional fractionated (SD 1.8 Gy) radiotherapy
Brain stem, if tumour arises inside the posterior fossa/PTV respectively:
Ø Upper limit for delineation: junction 3rd–4th ventricle
Ø Lower limit for delineation: inferior border of foramen magnum
Ø Dose constraints: Boost of the tumour bed according to COG 59,4 Gy
Ø Aim: D90% ≤ 44 Gy; D50% ≤ 61 Gy, D10% ≤ 63 Gy
Ø Max: D90% ≤ 59 Gy; D50% ≤ 62 Gy, D10% ≤ 64 Gy
Spinal cord – CV1 level:
Ø Upper limit for delineation: from inferior border of foramen magnum
Ø Lower limit for delineation: to CV1/CV2
Ø Dose constraints: D near Max (2%) < 50 Gy
Spinal cord – CV2/CV3 level:
Ø Upper limit for delineation: from CV1/CV2
Ø Lower limit for delineation: to CV3/CV4
Ø Dose constraints: D near Max (2%) < 45 Gy
Spinal cord – CV4 level:
Ø Upper limit for delineation: down to CV3/CV4
Ø Dose constraints: D near Max (2%) < 45 Gy
Inner ear:
For protection of the inner ear, the median dose should not exceed 30 Gy (Hua et al. 2008). The dose
maximum to the optic chiasma should not exceed 54 Gy.

Description of radiotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 52
7.3.1.2. Dose constraints for hyperfractionated (SD 1.0 Gy) radiotherapy according to PNET 4
For protection of the inner ear, the median dose should not exceed 30 Gy (Hua et al. 2008). The total
dose in the upper spinal cord should not exceed 50 Gy (below CV1), the dose maximum at the optic
chiasma, the optic nerves and the brain stem should not exceed 60 Gy.
7.3.2. Organs at Risk (OAR)
The following minimum number of OAR should be defined for 3D conformal radiation therapy or IMRT
planning:
Ø pituitary gland
Ø hypothalamus, left and right
Ø cochlea, left and right
Ø lens, left and right
Ø optic chiasma
Ø optic nerves, left and right
Ø whole brain
o supratentorial brain
o posterior fossa (infratentorial brain)
o temporal lobes, left and right
o hippocampus, left and right
o brain stem
Ø spinal cord
Ø thyroid gland

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 53
8. Description of chemotherapy elements
8.1. Maintenance chemotherapy Cisplatin/Lomustine/Vincristine
Timing:
Start approximately 6 weeks after end of radiotherapy
Recommended examinations and entry criteria (dose modifications see below):
Physical examination Good clinical conditions
No organ dysfunction
Blood count
Haematological regeneration:
Ø WBC >2000/µl
Ø Neutrophils >500/µl
Ø Thrombocytes >100 000/µl
Creatinine
(additional renal function parameters if
indicated)
Normal renal function
Audiometry No major hearing loss
Transaminases No organ dysfunction
Additional examinations upon local policy and patient’s requirements
Dosing:
Day Drug Dose Route
Day 1 Cisplatin 70 mg/m² Continuous infusion
over 6h
Lomustine 75 mg/m² Oral
Vincristine 1.5 mg/m²
(max: 2 mg)
i.v./short infusion*
Day 8 Vincristine 1.5 mg/m²
(max: 2 mg)
i.v./short infusion*
Day 15 Vincristine 1.5 mg/m²
(max: 2 mg)
i.v./short infusion*
Day 43 = Day 1
Minimum supportive care:
· Hyperhydration 3000ml/m²/d during Cisplatin treatment
· Use mannit during Cisplatin treatment to regulate diuresis
· Antiemesis
· Infection prophylaxis
* Please consider WHO-recommendation to deliver Vinca alkaloids only in minibags in order to avoid accidental
intrathecal administration [either in the same or in another patient!] (WHO Information Exchange System Alert
No. 115, 2007)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 54
Dose modifications:
Haematological
toxicity
Before initiation of the cycle:
WBC <2000/µl or
Neutrophils <500/µl or Thrombocytes <100 000/µl
Postpone cycle for at least one
week or until haematological regeneration
After the cycle:
In case of first sepsis AND
WBC < 500/µl OR
Neutrophils <50/µl
Reduce Lomustine to 50 mg/m²
and give G-CSF support
In case of second sepsis AND
WBC < 500/µl OR
Neutrophils <50/µl
Reduce Cisplatin to 50 mg/m²
Thrombocytopenia < 30 000/µl AND
substitution required
Reduce Lomustine to 50 mg/m²
Thrombocytopenia < 30 000/µl AND
substitution required despite reduction of
Lomustine to 50 mg/m²
Discontinue Lomustine
Delayed haematological regeneration
results in delay of chemotherapy >2
weeks for the first time
Do not give Lomustine in this
cycle
Reduce Lomustine to 50 mg/m² in
subsequent cycle
Delayed haematological regeneration
results in delay of chemotherapy >2
weeks for the second time
Discontinue Lomustine
Neurotoxicity Seizure after VCR Omit VCR in this cycle Reduce VCR in the subsequent
cycle to 1 mg/m²
Give full dose thereafter if
completely recovered
Ileus Omit VCR in this cycle
Reduce VCR in the subsequent
cycle to 1 mg/m²
Give full dose thereafter if
completely recovered
Dysesthesia
Muscular weakness
Severe abdominal pain
Reduce total dose of VCR by
reducing the number of doses in
each cycle
(give only 1st and 2nd, only the 1st or even no VCR according to
severity of symptoms)
Increase number of doses per
cycle upon recovery

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 55
Renal toxicity Creatinine >1.2 mg/dl [>105 µmol/l] OR
Creatinine >1.5 x baseline / normal OR
Creatinine-Clearance
<80 ml/min/1.73 m²
if no regeneration:
GFR > 60 ml/min/1.73 m²
GFR <60 ml/min/1.73 m²
Postpone chemotherapy for 1
week
nephrological diagnostics
Replace Cisplatin by Carboplatin
(400 mg/m²)
Discontinue platinum-based
chemotherapy
Ototoxicity Hearing loss
16-30db @ 1-3 kHz OR
>40db @ >4kHz
Replace Cisplatin by Carboplatin
(400 mg/m²)
Hearing loss
>30db @ 1-3kHz
Discontinue platinum-based
chemotherapy
Weight loss Weight loss >20% during maintenance
chemotherapy
Reduce Lomustine to 50 mg/m²
Further weight loss with reduced
Lomustine
Discontinue Lomustine

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 56
8.2. SKK chemotherapy
8.2.1. Overview
SKK chemotherapy and Modified SKK chemotherapy are modular chemotherapy cycles consisting of
four or two blocks, respectively.
One regular SKK chemotherapy cycle consists of four subsequent blocks. SKK chemotherapy is only
to be used as induction chemotherapy and is not intended as salvage treatment after radiotherapy.
a) SKK Cyclophosphamide/Vincristine
b) SKK high-dose Methotrexate/Vincristine (1)
c) SKK high-dose Methotrexate/Vincristine (2)
d) SKK Carboplatin/Etoposide (conventional dose)
These four blocks may be given WITH or WITHOUT intraventricular Methotrexate via an
intraventricular access device (Ommaya/Rickham), depending on the stratification and depending on
the centre’s expertise with this treatment.
Please note, that intraventricular Methotrexate treatment should only be considered in centres with
respective experience with this treatment.
During SKK chemotherapy, intraventricular Methotrexate is recommended only in the induction
chemotherapy and only for patients with:
è non-metastatic and metastatic DMB/MBEN, who are younger than 5 years at diagnosis,
during the first three cycles of SKK chemotherapy
è metastatic DMBMBEN, who are older than 5 years at diagnosis during the first two cycles of
SKK chemotherapy
è metastatic CMB, LCMB or AMB, who are older than 3 years at diagnosis, during the first two
cycles of SKK chemotherapy
è metastatic CNS embryonal tumour older than 4 years at diagnosis during the first two cycles
of SKK chemotherapy
One Modified SKK chemotherapy cycle consists of two subsequent blocks:
a) SKK Cyclophosphamide/Vincristine
d) SKK Carboplatin/Etoposide (conventional dose)
These two blocks are always given WITHOUT intraventricular Methotrexate.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 57
8.2.2. Block SKK – Cyclophosphamide/Vincristine
Timing:
SKK chemotherapy is only to be used as induction chemotherapy and is not intended as salvage
treatment after radiotherapy.
if used prior to radiotherapy start as early after operation as appropriate, ideally within 2–4
weeks if used after previous cycle SKK
chemotherapy start approximately 3 weeks after initiation of the previous
block
Recommended examinations and entry criteria (for dose modifications see below):
physical examination good clinical conditions, no organ dysfunction
blood count
haematological regeneration:
v WBC: > 2000/µl
v Neutrophils: > 500/µl
v Thrombocytes: > 80 000/µl
creatinine (additional renal function parameters, if indicated)
normal renal function
transaminases no organ dysfunction
aditional examinations according to local policy and patients requirements
Dosing:
Day Drug Dose Route
1 Cyclophosphamide 800 mg/m2/day 1 h i.v.
Mesna 250 mg/m² i.v. (directly before 1st
Cyclophosphamide)
Mesna 750 mg/m2/day 24 h i.v.
Vincristine 1,5 mg/m2 (max. 2 mg) i.v./short infusion*
Optional intraventricular therapy (depending on stratification):
Methotrexate† 2 mg/day i. vtr.
2 Cyclophosphamide 800 mg/m2/day 1 h i.v.
Mesna 750 mg/m2/day 24 h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate† 2 mg/day i. vtr.
3 Cyclophosphamide 800 mg/m2/day 1 h i.v.
Mesna 750 mg/m2/day 24 h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate† 2 mg/day i. vtr.
4 Mesna 750 mg/m2/day 24 h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate† 2 mg/day i. vtr.
15 Continue with next block
* Please consider WHO-recommendation to deliver Vinca alkaloids only in minibags in order to avoid accidental
intrathecal administration [either in the same or in another patient!] (WHO Information Exchange System Alert
No. 115, 2007). † See the separate application guidelines for i. vtr. MTX (chapter 8.6). Please note, that i. vtr. MTX treatment
should only be considered in centres with respective experience with this treatment and that i. vtr. MTX is only
scheduled during max. 3 cycles SKK chemotherapy within the treatment course.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 58
Minimum supportive care:
· Hyperhydration 3000ml/m²/d
· Antiemesis (e. g. Dolasetron 50 mg/m² before Cyclophosphamide)
· Infection prophylaxis
Indications for intraventricular Methotrexate
Intraventricular Methotrexate during SKK chemotherapy is recommended only in the induction
chemotherapy and only for patients with:
è non-metastatic and metastatic DMB/MBEN, who are younger than 5 years at diagnosis,
during the first three cycles of SKK chemotherapy
è metastatic DMB/MBEN, who are older than 5 years at diagnosis during the first two cycles
of SKK chemotherapy
è metastatic CMB, LCMB or AMB, who are older than 3 years at diagnosis, during the first two
cycles of SKK chemotherapy
è metastatic CNS embryonal tumour older than 4 years at diagnosis during the first two cycles
of SKK chemotherapy
CAUTION
Age specific dose reductions are required for Cyclophosphamide and Vincristine.
< 6 month : ⅔ of the m² dosage
7 to 12 month age: ⅘ of the m² dosage
>12 month: full m² dosage.
Intraventricular Methotrexate dose is 1 mg/day in children < 6 months.
Dose modifications:
Haematological
toxicity
Before initiation of the block:
WBC <2000/µl or
Neutrophils <500/µl or
Thrombocytes <80 000/µl
Postpone block for at least one
week or until haematological
regeneration
After the block:
In case of first sepsis AND WBC < 500/µl OR
Neutrophils <50/µl
Give G-CSF support in the next block
In case of second sepsis AND
WBC < 500/µl OR
Neutrophils <50/µl
Omit day 3 of the block

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 59
8.2.3. Block SKK - high-dose Methotrexate /Vincristine
Timing:
Start 2 weeks after initiation of the previous block. Complete haematological regeneration is not
essential to start high-dose Methotrexate.
Recommended examinations and entry criteria (dose modifications see below):
Physical examination Good clinical conditions No organ dysfunction No mucositis
Blood count
Haematological regeneration:
· Thrombocytes: >30 000/µl
Creatinine (additional renal function parameters if indicated)
Normal renal function
Transaminases No organ dysfunction
Additional examinations upon local policy and patient’s requirements
Dosing:
Day Drug Dose Route
1
Methotrexate 5 g/m²
Divide in 2 doses:
0.5 g/m² (= 10%)
4.5 g/m² (= 90%)
0.5 h i.v.
23.5 h i.v.
Vincristine 1,5 mg/m2 (max. 2 mg) i.v./short infusion*
Optional intraventricular therapy (depending on stratification):
Methotrexate§ 2 mg/day i. vtr.
2 Leukovorin rescue† 15 mg/m2 x6q6h i.v., Start h42
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg/day i. vtr.
15 Continue with next block †for details of Leucovorin rescue see chapter 8.7 Leucovorin rescue after intravenous high-dose . §See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX treatment
should only be considered in centres with respective experience with this treatment and that i. vtr.
MTX is only scheduled during max. 3 SKK-chemotherapy-cycles within the treatment course.
Minimum supportive care:
· Hyperhydration 3000ml/m²/d (or higher if Methotrexate underexcretion, see chapter 8.7)
· Consider urine alkalysation
· For detailed description of Leucovorin-rescue see chapter 8.7.
· Antiemesis
· Infection prophylaxis
* Please consider WHO-recommendation to deliver Vinca alkaloids only in minibags in order to avoid accidental
intrathecal administration [either in the same or in another patient!] (WHO Information Exchange System Alert
No. 115, 2007)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 60
Indications for intraventricular MTX
Intraventricular Methotrexate during SKK chemotherapy is recommended only in the induction
chemotherapy and only in patients with:
è non-metastatic and metastatic DMB/MBEN, who are younger than 5 years at diagnosis,
during the first three cycles of SKK chemotherapy
è metastatic DMB/MBEN, who are older than 5 years at diagnosis during the first two cycles
of SKK chemotherapy
è metastatic CMB, LCMB or AMB, who are older than 3 years at diagnosis, during the first two
cycles of SKK chemotherapy
è metastatic CNS embryonal tumour older than 4 years at diagnosis during the first two cycles
of SKK chemotherapy
CAUTION
Age specific dose reduction is required for Vincristine.
< 6 month : 2/3 of the m² dosage
7 to 12 month age: 4/5 of the m² dosage
>12 month: full m² dosage
Intraventricular Methotrexate dose is 1 mg/day in children < 6 months.
Dose modifications:
Haematological
toxicity
Before initiation of the block
Thrombocytes <30 000 /µl
Postpone block until
thrombocytes > 30 000 /µl
Liver toxicity Before initiation of the block
ASAT [AST/GOT] > 500 U/l or
ALAT [ALT/GPT] > 500 U/l
Postpone block until values
below the limit

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 61
8.2.4. Block SKK - Carboplatin/Etoposide (conventional dose)
Timing:
if used as 4th block in SKK cycles start approximately 2 weeks after day 1 of the previous block
if used as 2nd block in Modified SKK cycles start approximately 3 weeks after day 1 of the previous block
Recommended examinations and entry criteria (dose modifications see below):
Physical examination Good clinical conditions
No organ dysfunction
No mucositis
Blood count
Haematological regeneration:
Ø WBC: >2000/µl
Ø Neutrophils: >500/µl
Ø Thrombocytes: >80 000/µl
Creatinine (additional renal function
parameters if indicated)
Normal renal function
Transaminases No organ dysfunction
Audiometry No hearing disability
Additional examinations upon local policy and patient’s requirements
Dosing:
Day Drug Dose Route
1 Carboplatin 200 mg/m2/day 1 h i.v.
Etoposide 150 mg/m2/day ½ h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg/day i. vtr.
2 Carboplatin 200 mg/m2/day 1 h i.v.
Etoposide 150 mg/m2/day ½ h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg/day i. vtr.
3 Carboplatin 200 mg/m2/day 1 h i.v.
Etoposide 150 mg/m2/day ½ h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg/day i. vtr.
4 Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg/day i. vtr.
§See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX
treatment should only be considered in centres with respective experience with this treatment and
that i. vtr. MTX is only scheduled during max. 3 SKK-chemotherapy-cycles within the treatment course.
Minimum supportive care:
· Hyperhydration 3000ml/m²/d
· Use mannit during Carboplatin treatment to regulate diuresis
· Antiemesis
· Infection prophylaxis

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 62
Indications for intraventricular Methotrexate
Intraventricular Methotrexate during SKK chemotherapy is recommended only in the induction
chemotherapy and only in patients with
è non-metastatic and metastatic DMB/MBEN, who are younger than 5 years at diagnosis,
during the first three cycles of SKK chemotherapy
è metastatic DMB/MBEN, who are older than 5 years at diagnosis during the first two cycles
of SKK chemotherapy
è metastatic CMB, LCMB or AMB, who are older than 3 years at diagnosis, during the first two
cycles of SKK chemotherapy
è metastatic CNS embryonal tumour older than 4 years at diagnosis during the first two cycles
of SKK chemotherapy
CAUTION
Age specific dose reduction is required for Carboplatin, and may be considered for Etoposide.
<6 month: 2/3 of the m² dosage
7 to 12 month: 4/5 of the m² dosage
>12 month: full m² dosage
Intraventricular Methotrexate dose is 1 mg/day in children < 6 months.
Dose modifications:
Haematological
toxicity
Before initiation of the block:
WBC <2000/µl or
Neutrophils <500/µl or Thrombocytes <80 000/µl
Postpone block for at least
one week or until haematological regeneration
After the block:
In case of first sepsis AND
WBC <500/µl OR
Neutrophils <50/µl
Give G-CSF support in the
next block
In case of second sepsis AND
WBC <500/µl OR
Neutrophils <50/µl
Give only day 1 and 2 of the
block
Renal toxicity Creatinine >1.2 mg/dl [>105 µmol/l] OR
Creatinine >1.5 x baseline / norm OR
Creatinine-Clearance
<80 ml/min/1.73m²
if no improvement of renal impairment
after 1 week GFR >60 ml/min/1.73m²
GFR <60 ml/min/1.73m²
Postpone chemotherapy for
1 week
Nephrological diagnostics
Reduce Carboplatin to 3 x
125 mg/m²
Replace Carboplatin by
Cyclophosphamide (1 x 800
mg/m²/d day 1-3 + mesna)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 63
Ototoxicity Hearing loss
16-30db @ 1-3kHz OR
>40db @ 4-8kHz
Reduce Carboplatin to
3 x 125 mg/m²
Hearing loss >30db @ 1-3kHz
Replace Carboplatin by Cyclophosphamide
(1 x 800 mg/m²/d day 1-3 +
mesna)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 64
8.3. Intensified Induction chemotherapy
Timing:
Start with the first cycle upon recovery from the surgery, ideally 2–4 weeks postoperatively. The
interval between the cycles should be at least 4 weeks (day 29 = day 1).
This cycle is associated with relevant toxicity (in particular liver toxicity).
Therapy should be performed only in experienced centres.
Intensified Induction chemotherapy is not intended as salvage treatment after radiotherapy.
Recommended examinations and entry criteria (dose modifications see below):
Physical examination Good clinical conditions
No organ dysfunction
No mucositis
Blood count
Haematological regeneration:
· WBC: >2000/µl
· Neutrophils: >500/µl
· Thrombocytes: >80
000/µl
Creatinine
(additional renal function parameters if indicated)
Normal renal function
Transaminases No organ dysfunction
Audiometry No hearing disability
Additional examinations upon local policy and patient’s requirements
Dosing:
Day Drug Dose Route
1 Cisplatin 3,5 mg/kg 6 h i.v.
Vincristine* 0.05 mg/kg i.v. / short infusion*
Intraventricular therapy
Methotrexate§ 2 mg i. vtr.
2 Etoposide 4 mg/kg 1 h i.v.
Cyclophosphamide 65 mg/kg 3 h i.v.
Mesna
Mesna
25 mg/kg
65 mg/kg
i.v. (directly before 1st Cyclophosphamide)
24 h i.v.
Intraventricular therapy
Methotrexate§ 2 mg i. vtr.
3 Etoposide 4 mg/kg 1 h i.v.
Cyclophosphamide 65 mg/kg/d 3 h i.v.
Mesna 25 mg/kg
65 mg/kg/d
i.v. bolus
24 h i.v.
Intraventricular therapy
Methotrexate§ 2 mg i. vtr.
4 Intraventricular therapy
Methotrexate§ 2 mg i. vtr.
6-13 G-CSF 5 µg/kg i.v. / s.c.
* Please consider WHO-recommendation to deliver Vinca alkaloids only in minibags in order to avoid accidental
intrathecal administration [either in the same or in another patient!] (WHO Information Exchange System Alert
No. 115, 2007)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 65
§ See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX
treatment should only be considered in centres with respective experience with this treatment.
Proceed with day 15 only if
· Neutrophils > 500/µl
· Transaminases < 1.5x upper limit of normal (ULN)
· Normal renal function
· Good clinical conditions/no infection
Interval between last dose of G-CSF and start of intravenous Methotrexate should be at least 48 hours.
G-CSF treatment can be continued 3 days after start of Methotrexate, if Methotrexate level is < 0.25
µmol / l at this time.
Day Drug Dose Route
15 Methotrexate 5 g/m²
Divide in 2 doses:
0.5 g/m² (=10 %)
4.5 g/m² (=90 %)
0.5 h i.v.
23.5 h i.v.
Vincristine* 0,05 mg/kg (max. 2 mg) i.v. / short infusion Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
16 Leukovorin rescue† 15 mg/m2 x6q6h i.v. q6h, start h42
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
18
if Methotrexate
levels
<0.25 µmol/l
G-CSF 5 µg/kg i.v. / s.c.
29 = Day 1
Minimum interval since first day of Methotrexate = 14 days
§ See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX
treatment should only be considered in centres with respective experience with this treatment. †for details of Leucovorin rescue see chapter 8.7 Leucovorin rescue after intravenous high-dose .
Continue G-CSF until neutrophils >500 /µl or until stem cell collection (after the first cycle; consider
increased dose of 10 µg/kg upon neutrophil regeneration in order to accelerate stem cell collection).
Minimum supportive care:
· Hyperhydration 3000 ml/m²/d (or higher if Methotrexate underexcretion, see chapter 8.7)
· Consider urine alkalinisation during Methotrexate administration
· For detailed description of Leucovorin-rescue see chapter 8.7.
· Antiemesis
· Infection prophylaxis
CAUTION
NO age specific dose reductions are required in this cycle for intravenous drugs!
Intraventricular Methotrexate dose is 1 mg/day in children < 6 months.
* Please consider WHO-recommendation to deliver Vinca alkaloids only in minibags in order to avoid accidental
intrathecal administration [either in the same or in another patient!] (WHO Information Exchange System Alert
No. 115, 2007)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 66
Dose modifications:
Haematological
toxicity
Before initiation of the cycle:
WBC <2000/µl or
Neutrophils <500/µl or Thrombocytes <80 000/µl
Postpone cycle for at least one
week or until haematological regeneration
At day 15:
WBC <500/µl Postpone day 15 up to 7 days (until day 22)
Renal toxicity Creatinine >1.2 mg/dl [>105µmol/l] OR
Creatinine >1.5 x baseline / norm OR
Creatinine-Clearance <80 ml/min/1.73m²
if no improvement or renal impairment after 1
week:
GFR > 60 ml/min/1.73m²
GFR <60 ml/min/1.73m²
Postpone chemotherapy
Nephrological diagnostics
Replace Cisplatin by Carboplatin
[12 mg/kg]
Omit all platinum-containing agents
Ototoxicity Hearing loss 16-30db @ 1-3kHz OR
>40db @ 4-8kHz
Replace Cisplatin by Carboplatin
[12 mg/kg]
Hearing loss
>30db @ 1-3kHz
Omit all platinum-containing
agents
Liver toxicity Transaminases > 1.5 ULN Postpone chemotherapy until
regeneration; consider
defibrotide in case of suspicion of hepatic veno-occlusive disease
(VOD)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 67
8.4. Carboplatin/Etoposide-96h chemotherapy
Timing:
Start with the first cycle upon recovery from the surgery, ideally 2-4 weeks postoperatively. The
interval between the cycles should be at least 4 weeks (day 29 = day 1).
Recommended examinations and entry criteria (dose modifications see below):
Physical examination Good clinical conditions
No organ dysfunction
No mucositis
Blood count
Haematological regeneration: Ø WBC: >2000/µl
Ø Neutrophils: >500/µl
Ø Thrombocytes: >80
000/µl
Creatinine
(additional renal function parameters if indicated)
Creatinine Clearance
>60 ml/min/1.73m²
Transaminases No organ dysfunction
Audiometry Hearing loss
>30db @ 2-4 kHz
Additional examinations upon local policy and patient’s requirements
Dosing:
Day Drug Dose Route
1 Carboplatin 200 mg/m² 24h i.v.
Etoposide 100 mg/m² 24h i.v. (start 6h after
Start of Carboplatin)
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg i. vtr.
2 Carboplatin 200 mg/m² 24h i.v.
Etoposide 100 mg/m² 24h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg i. vtr.
3 Carboplatin 200 mg/m² 24h i.v.
Etoposide 100 mg/m² 24h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg i. vtr.
4 Carboplatin 200 mg/m² 24h i.v.
Etoposide 100 mg/m² 24h i.v.
Optional intraventriular therapy (depending on stratification):
Methotrexate§ 2 mg i. vtr.
Day 22-29 = Day 1
§ See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX
treatment should only be considered in centres with respective experience with this treatment.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 68
Minimum supportive care:
· Hyperhydration 3000 ml/m²/d
· Antiemesis
· Infection prophylaxis
Dose modifications:
Haematological
toxicity
Before initiation of the cycle:
WBC <2000/µl or
Neutrophils <500/µl or
Thrombocytes <80 000/µl
Postpone cycle until
haematological regeneration
Nephrotoxicity Creatinine-Clearance
<60 ml/min/1.73m²
Dose modifications for renal
toxicity have not been
established for this cycle and
should be done upon individual
consideration
Ototoxicity Hearing loss
>16db @ 1-3 kHz >40db @ 4-8 kHz
Dose modifications for
ototoxicity have not been established for this cycle and
should be done upon individual
consideration

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 69
8.5. Tandem high-dose chemotherapy
8.5.1. 1. High-dose chemotherapy (1. HDCT)
High dose chemotherapy requires autologous stem cell support!
Severe, life-threatening complications must be expected. Therefore high-dose chemotherapy
may only be performed in centres with experience in autologous stem cell transplantation.
Centres need to make sure that toxicity rates do not exceed potential benefits of HDCT!
Tandem high-dose chemotherapy is not intended as salvage treatment after radiotherapy.
Recommended examinations and entry criteria (see below for dose modifications):
Physical examination Good clinical conditions, no organ dysfunction,
no mucositis
Blood count
Haematological regeneration:
Ø WBC: >2000/µl
Ø Neutrophils: >500/µl
Ø Thrombocytes: >50 000/µl
Creatinine (additional renal function
parameters if indicated)
Creatinine Clearance >50ml/min/1.73m²
Liver function parameters No liver dysfunction
Chest X-ray, Spirometry No severe lung disorder
Echokardiography and electrocardiography No severe cardiac disorder
No severe neurological dysfunction
No therapy resistant seizure disorder
Additional examinations upon local policy and patient’s requirements
Dosing:
Day Drug Dose Route
-8 Carboplatin 500 mg/m² 24 h i.v.
Etoposide 250 mg/m² 24 h i.v. (start 6h after start Carboplatin)
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
-7 Carboplatin 500 mg/m² 24 h i.v.
Etoposide 250 mg/m² 24 h i.v.
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
-6 Carboplatin 500 mg/m² 24 h i.v.
Etoposide 250 mg/m² 24 h i.v.
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
-5 Carboplatin 500 mg/m² 24 h i.v.
Etoposide 250 mg/m² 24 h i.v.
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
0 Autologous stem cell transplantation
+5 Start G-CSF 5 µg/kg i.v. or s.c.
§ See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX treatment should only be considered in centres with respective experience with this treatment.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 70
Minimum supportive care:
· Sufficient autologous stem cell support available
· Hyperhydration 3000 ml/m²/d
· Antiemesis
· Infection prophylaxis
· Do high-dose chemotherapy with stem cell rescue only in centres with sufficient experience in
stem cell transplantation
Dose modifications:
Experience with HDCT in children younger than 1 is very limited. Dose-reduction of chemotherapy
should be considered according to local standards and to the tolerance to previous chemotherapy of
the individual patient.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 71
8.5.2. 2. High-dose chemotherapy (2. HDCT)
High dose chemotherapy requires autologous stem cell support!
Severe, life threatening complications must be expected. Therefore high dose chemotherapy
may only be performed in centres with experience in autologous stem cell transplantation!
Centres must make sure that toxicity rates do not exceed potential benefits of HDCT!
Tandem high-dose chemotherapy is not intended as salvage treatment after radiotherapy.
Timing:
Start with the second cycle high-dose chemotherapy only after the patient has recovered completely
from first cycle. Do not start earlier than day +28 after ASCT.
Recommended examinations and entry criteria (see below for dose modifications):
Physical examination Good clinical conditions No organ dysfunction
No mucositis
Blood count
Haematological regeneration:
Ø WBC: >2000/µl
Ø Neutrophils: >500/µl
Ø Thrombocytes: >50 000/µl
Creatinine (additional renal function parameters
if indicated)
Creatinine Clearance >50ml/min/1.73m²
No evidence of fanconi syndrome
Liver function parameters No liver dysfunction
Chest X-ray, Spirometry No severe lung disorder
Echokardiography and electrocardiography No severe cardiac disorder
No severe neurological dysfunction
No therapy resistant seizure disorder
Additional examinations upon local policy and patient’s requirements

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 72
Dosing:
Day Drug Dose Route
-4 Thiotepa 300 mg/m² i.v. (1 hour)
Cyclophosphamide 1500 mg/m² i.v. (1 hour)
Mesna 500 mg/m² i.v. (directly before 1st Cyclophosphamide)
Mesna 1500 mg/m² Continuously i.v.(24 h) Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
-3 Thiotepa 300 mg/m² i.v. (1 hour)
Cyclophosphamide 1500 mg/m² i.v. (1 hour)
Mesna 1500 mg/m² Continuously i.v.(24 h)
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
-2 Thiotepa 300 mg/m² i.v. (1 hour)
Cyclophosphamide 1500 mg/m² i.v. (1 hour)
Mesna 1500 mg/m² Continuously i.v.(24 h)
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
-1 Mesna 1500 mg/m² Continuously i.v.(24 h)
Intraventricular therapy:
Methotrexate§ 2 mg i. vtr.
0 Autologous stem cell transplantation
+5 G-CSF 5 µg/kg i.v. or s.c.
§ See separate application guidelines for i. vtr. MTX (chapter 8.6)! Please note, that i. vtr. MTX
treatment should only be considered in centres with respective experience with this treatment.
Minimum supportive care:
· Sufficient autologous stem cell support available
· Hyperhydration 3000 ml/m²/d
· Antiemesis
· Infection prophylaxis
· Do high-dose chemotherapy with stem cell rescue only in centres with sufficient experience in
stem cell transplantation
Dose modifications:
Experience with HDCT in children younger than 1 is very limited. Dose-reduction of chemotherapy should be considered according to local standards and to the tolerance to previous chemotherapy of
the individual patient.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 73
8.6. Intraventricular Methotrexate
Intraventricular Methotrexate must only be used in experienced centres by trained physicians.
Despite good outcomes and acceptable toxicity in published clinical trials using intraventricular
Methotrexate in combination therapy, there are no formal phase I/II trials and it must still be considered
experimental.
Intraventricular Methotrexate is not recommended during or after radiotherapy.
Timing:
Intraventricular Methotrexate is part of different treatment regimens and depends on stratification.
See corresponding guidelines for timing.
When used in patients after radiotherapy, i. vtr. MTX is associated with reduced neuropsychological
outcomes. Taking into account the lack of randomized evidence for a survival benefit, its use requires
good explanation and consent of parents and/or their legal representatives.
Intraventricular Methotrexate requires implantation of an intraventricular access device (e.g.
Ommaya, Rickham). Repeated lumbar punctions are not equivalent!
Recommended examinations and entry criteria:
Please note that administration of intraventricular Methotrexate has only been evaluated within
combination therapies within the clinical trials (HIT2000 and preceeding HIT-SKK’92 trials). Formal
phase I/II trials have not been performed. Effectiveness is not proven and specific toxicity associated
with intraventricular Methotrexate cannot be determined. Therefore, a general recommendation
outside clinical trials is difficult. However, in centres with long-lasting experience we encourage to
consider intraventricular Methotrexate in
a) patients with favourable risk profile, who are likely not to require radiotherapy during their
treatment course
b) patients with very poor risk profile, for whom high treatment intensity is desired to maximise
survival.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 74
The HIT-MED trial commission suggests to consider intraventricular Methotrexate for first-line
chemotherapy in patients with:
è non-metastatic and metastatic DMB/MBEN, who are younger than 5 years at diagnosis,
during the first three cycles of SKK chemotherapy
è metastatic DMB/MBEN, who are older than 5 years at diagnosis during the first two cycles
of SKK chemotherapy
è metastatic CMB, LCMB or AMB younger than 3 years at diagnosis during intensified
induction chemotherapy
è metastatic CMB, LCMB or AMB, who are older than 3 years at diagnosis, during the first two
cycles of SKK chemotherapy
è metastatic CNS embryonal tumour or pineoblastoma younger than 4 years at diagnosis
during induction chemotherapy
è metastatic CNS embryonal tumour or pineoblastoma older than 4 years at diagnosis during
the first two cycles of SKK chemotherapy
Ø Improved stratification will likely lead to identification of more precisely defined risk groups
within the next years. In good prognosis patients, a combination of intraventricular
Methotrexate and radiotherapy should be avoided.
Recommended examinations and entry criteria:
I. vtr. therapy must only be administered if there is no evidence for dislocation of the
reservoir/ventricular catheter. Correct placement may be checked routinely before 1st use by native
CT scan or other imaging.
Preventive measures have to be established to strictly exclude i. vtr. application of any other drug
than Methotrexate.
Contraindications for i. vtr. applications are:
· Clinical or laboratory signs for CNS infection
· Thrombocytes < 30 000 /µl
· Clinical or neuroradiological signs for disturbed CSF flow (including CSF malabsorption) – be
careful in case of malabsorption associated with meningeosis carcinomatosa! Careful initiation
of intraventricular treatment might be justified (reduced dose, frequent measurements of CSF-
MTX concentrations), but data is very limited.
· Hygroma in connection to the ventricular system
· Elevated MTX CSF level of ≥ 5 µmol/l (measurement required on day 2 before i. vtr. MTX
application)
· CSF protein > 800 mg/l (measurement required on day 1 and day 2 before i. vtr. MTX
application)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 75
Dosing:
Children < 6 months MTX i. vtr. 1 mg/day
Children > 6 months MTX i. vtr. 2 mg/day
Please note:
· Methotrexate for intraventricular use must not be dissolved in an alcohol containing
compound.
· Preventive measures have to be established to assure that the intraventricular
Methotrexate dose is correct.
· Accidental administration of Vinca-alkaloids is lethal. Measures should be established to
prevent accidental installation.*
· Confirmation of regular Methotrexate CSF levels on day 2 of every treatment block/cycle is
strictly required before the application of intraventricular Methotrexate.
In case of suspected Methotrexate-related toxicity discuss further intraventricular treatment!
The HIT-MED study centre will be happy to assist you with your decision.
The following detailed guidelines for the intraventricular application of MTX need to be followed!
* Please consider WHO-recommendation to deliver Vinca alkaloids only in minibags in order to avoid accidental
intrathecal administration [either in the same or in another patient!] (WHO Information Exchange System Alert
No. 115, 2007)

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 76
8.6.1. Guidelines for the intraventricular application of Methotrexate
Injection of i. vtr. MTX should be performed by an experienced physician under sterile conditions using
a mask, sterile gloves and a sterile cloth. The patient should lay down (upper body raised to 45
degrees), and should wear a mask. Skin disinfection should be done thoroughly (e.g. 3 times with 0,1%
Octenidin/2%g Phenoxyethanol [e.g. Octenisept ®]) and let it dry. Injection can be done with a 27-G
Butterfly. (If you use an older Ommaya device, check if it is necessary to rinse repeatedly before and
after injection using a sterile swab). After the puncture use a sterile patch with or without a Providon-
Jod salve.
Methotrexate must not be administered if CSF aspiration is disturbed (check dislocation)!
Make sure not to administer any other drug than Methotrexate intraventricularly! Establish
preventive measures (e. g. color-codes/different injection systems) to prevent accidental
injection of Vincristine!
Do not use intraventricular Methotrexate during or after radiotherapy.
Day 1:
1) Aspirate 2 ml CSF (4 ml in case of Ommaya)
Store syringe with CSF in a sterile place to be able to use it to flush after Methotrexate
injection 2) Aspirate 2 ml CSF for Methotrexate and protein CSF concentration
Aspirate 4 ml CSF for cytology
3) Dilute Methotrexate with CSF to a total volume of 2 ml (2 mg Methotrexate = 0.8ml)
4) Inject Methotrexate under sterile conditions
5) Inject the 2 ml CSF (4 ml in case of Ommaya) you have aspirated and stored in step 1
Day 2: 2 punctures!
Puncture 1 (approx. 20-24 hours after first injection)
1) Aspirate 2 ml CSF (ca. 4 ml in case of Ommaya)
Store syringe with CSF in a sterile place
2) Aspirate 2 ml CSF for Methotrexate and protein CSF concentration
3) Inject the 2 ml CSF (4 ml in case of Ommaya) you have aspirated and stored in step 1
Only proceed if Methotrexate CSF levels are below 5 µmol/l!
If > 5 µmol/l: see guidelines for elevated Methotrexate CSF levels.
Puncture 2
1) Aspirate 2 ml CSF (ca. 4 ml in case of Ommaya)
Store syringe with CSF in a sterile place to be able to use it to flush after Methotrexate
injection 2) Dilute Methotrexate with CSF to a total volume of 2 ml (2 mg Methotrexate = 0.8ml)
3) Inject Methotrexate under sterile conditions
4) Inject the 2 ml CSF (4 ml in case of Ommaya) you have aspirated and stored in step 1
Days 3 and 4 (the same as day 1, but without cytology!):
1) Aspirate 2 ml CSF (ca. 4 ml in case of Ommaya)
Store syringe with CSF in a sterile place to be able to use it to flush after Methotrexate
injection
2) Aspirate 2 ml CSF for Methotrexate and protein CSF concentration 3) Dilute Methotrexate with CSF to a total volume of 2 ml (2 mg Methotrexate = 0.8ml)
4) Inject Methotrexate under sterile conditions
5) Inject the 2 ml CSF (4 ml in case of Ommaya) you have aspirated and stored in step 1

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 77
8.6.2. Guidelines for elevated MTX CSF levels after intraventricular application
Elevated CSF MTX levels after intraventricular application of Methotrexate are an emergency
situation and require urgent intervention!
The most common reason for MTX CSF levels ≥ 5 μmol/l are sampling errors, especially if there is no
evidence of disturbed circulation of the CSF and the child is in good clinical condition without any
neurological symptoms. Please recheck CSF level.The amount of CSF used to flush after the
Methotrexate injection may have been too low, leaving some Methotrexate in the device. Therefore
please aspirate first 2–4 ml CSF, store the syringe sterilely and aspirate again 2 ml for detection of the
MTX CSF level.
If rechecked CSF concentrations remain elevated, the patient has neurological symptoms compatible
with CNS toxicity, or MTX CSF concentrations continue to be elevated after 24 hours > 5 μmol/L, please
consider emergency measures as follows:
1) Aspirate at least 20-30 ml CSF (may be substituted by sterile NaCl)
2) As next step please consider:
- Leucovorin intravenously, caution: do not inject Leucovorin into the CSF!
- Dexamethasone intravenously/orally
3) Contact the HIT-MED study centre for advice
4) As further steps consider (experimental!):
- Ventriculolumbar CSF lavage
- Carboxypeptidase intrathecally [There are case reports on the intrathecal administration of
carboxypeptidase. (Widemann et al. 2004)]
8.7. Leucovorin rescue after intravenous high-dose Methotrexate
Expected Methotrexate-levels and standard leukovorin-rescue after high-dose Methotrexate 5g/m²:
Time after start of
Methotrexate
[hours]
Routine creatinine
measurements
Methotrexate serum
concentration [µmol/l]
Leucovorin dose
[mg/m²]
24 X < 150 -
36* < 3* -
42 X ≤ 1 15
48 X ≤ 0,4 15
54 ≤ 0,25 15
60 ** 15
66 ** 15
72 ** 15
* Methotrexate serum concentration 36 h after start of Methotrexate only needs to be determined if
the level 24 h after start of Methotrexate is >150 µmol/l. For improved security, consider measurement
of Methotrexate serum concentration 36h after start in all patients treated with intensified induction.
** if the serum concentration of Methotrexate is below the upper expected limit at 42, 48, and 54
hours after start of Methotrexate infusion, further evaluations of Methotrexate serum levels are not
necessary. Leukovorin-rescue has to be continued until hour 72.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 78
In case of excessively increased Methotrexate levels, consider additional individual interventions
(e. g. higher dose of Leucovorin, application of Carboxypeptidase-G2, dialysis).
See chapter “Methotrexate underexcretion” for more information.
Monitoring of serum Methotrexate concentrations and consequences of elevated Methotrexate
levels
1.) Measure Methotrexate serum concentrations at 24 hours after start of i.v. MTX
Ø If the Methotrexate serum concentration is > 150 µmol/l please
a) Raise fluid intake to 4500 ml/m²/24 h with consequent urine alkalinisation (urine pH ≥ 7.0) and
tight fluid equilibration upon receipt of the result
If the urine pH drops < 7.0, give sodium bicarbonate (1 mmol/kg) [e.g. sodium bicarbonate
8.4% 1 ml/kg [= 1 mmol/kg] mixed together with aqua ad iniectabilia
1 ml/kg as short infusion in 30-60 minutes]
b) Determine Methotrexate serum concentration additionally at hour 36.
c) If the Methotrexate serum concentration is > 3 µmol/l at 36 hours after start of Methotrexate
· Continue increased fluid intake (4500 ml/m²/24 h) with consequent urine
alkalinisation (urine pH ≥ 7.0) and tight fluid equilibration (if not already done before)
If the urine pH drops < 7.0, give sodium bicarbonate (1 mmol/kg) [e.g. sodium bicarbonate 8.4% 1ml/kg [= 1 mmol/kg] mixed together with aqua ad iniectabilia 1
ml/kg as short infusion in 30-60 minutes]
· Give Leucovorin upon receipt of the result according to the diagram depicted below,
i.e. 60 mg/m² if serum Methotrexate concentration is between 3 and 4µmol/l and
75 mg/m² of serum Methotrexate concentration is between 4 and 5µmol/l. If above
5µmol/l see calculation below. Remember to give very high doses of Leucovorin only
as short infusion and to check serum calcium concentrations (for details see below).
· Consider repeating Leucovorin 42 hours after start of Methotrexate: either repeat the
same dose as given before, or adapt dose to result of Methotrexate serum
concentration measurement at 42 hours (depending on time to receipt of the result,
Methotrexate serum level and local policy)
2.) Measure Methotrexate serum concentration at 42 hours, 48 hours and 54 hours after start of
i.v. MTX. If the Methotrexate- serum concentration is above the upper expected limits
a) Adjust the Leucovorin dose for the subsequent time point to the following:
- If the Methotrexate serum concentration is < 5 µmol/l, upon receipt of the result, the
leukovorin dose should be determined according to the diagram
Ø Methotrexate
mmol/l

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 79
5 75 mg/m2
4 60 mg/m2
3 45 mg/m2
2 30 mg/m2
1 15 mg/m2
0,25 NO RESCUE
0 24 36 42 48 54 60 66 72 78 84
Hours after Start of the Methotrexate-Infusion
- If the Methotrexate serum concentration is > 5 µmol/l, upon receipt of the result, the leukovorin dose can be calculated by the formula:
Leukovorin [mg] = Methotrexate level in serum [µmol/l] x Body weight [kg]
Caution: Leukovorin doses > 20 mg/kg should be administered as short infusion (1 h). Shorter
infusion times cannot be recommended because of the high content of Calcium. Repeated
determination of serum Calcium levels may be necessary. Oral administration is not
recommended because of saturable enteral resorption.
b) Raise fluid intake to 4500 ml/m²/24 h with consequent urine alkalinisation (urine pH ≥ 7.0) and
tight fluid equilibration.
If the urine pH drops < 7.0, give sodium bicarbonate (1 mmol/kg; e.g. sodium bicarbonate 8.4%
1ml/kg [= 1mmol/kg] mixed together with aqua ad iniectabilia 1ml/kg as short infusion in 30-
60 minutes).
c) Continue Methotrexate level determination and Leucovorin rescue every 6 h until the
Methotrexate level is below 0.25 µmol/l.

Description of chemotherapy elements
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 80
Renal Methotrexate underexcretion
A Methotrexate induced renal dysfunction with prolonged Methotrexate clearance is a medical
emergency. Potential signs of renal Methotrexate underexcretion are one or more of the following
symptoms that occur during the first day of Methotrexate therapy:
- Drop of urine pH < 6.0
- Rise of the creatinine (serum) > 50% of the basic level
- Dropping diuresis despite adequate therapy with furosemide
- 24 h Methotrexate level above the target level
Typical clinical signs of acute Methotrexate intoxication are severe, therapy resistant vomiting during
the first 24-48 h after exposition to Methotrexate, yellow diarrhoea (the same colour as Methotrexate)
and neurological symptoms (disorientation, impaired vision, seizures).
In case of a severe disruption of the Methotrexate excretion it is possible to decrease the Methotrexate
serum level by application of carboxypeptidase-G2 (CPD-G2) very rapidly. Methotrexate will be
hydrolysed by the bacterial enzyme (CPD-G2) to the inactive metabolite 2,4-diamino-N10-
methylpteroinacid (DAMPA). CPD-G2 does not cross the blood-brain barrier. In the event of a severe
disruption of the Methotrexate excretion, please contact the HIT-MED office in order to discuss the
next safety measures.
Carboxypeptidase is expensive and may not be available without pre-organized contacts to
hospitals/pharmacies who store this drug for emergency use. Physicians using this treatment
schedule have to make sure in advance that supply of caboxypeptidase is available in case of an
emergency

Members of the HIT-MED study committee
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 81
9. Members of the HIT-MED study committee Neuro-Oncology Radiotherapy
Dr. med. Frank Deinlein Dr. med. Stephanie Combs
Prof. Dr. med. Gudrun Fleischhack Prof. Dr. med. Anca Grosu
Prof. Dr. Dr. med. Michael Frühwald Dr. med. Dagmar Hornung
Prof. Dr. med. Norbert Graf Prof. Dr. med. R.-D. Kortmann
Dr. med. Astrid Gnekow Prof. Dr. med. Beate Timmermann
Prof. Dr. med. Peter Hau Dr. med. Jutta Welzel
Dr. med. Katja von Hoff
B.-Ole Juhnke
Dr. med. Martin Mynarek Prof. Dr. med. Stefan Rutkowski
Prof. Dr. med. Wolfram Scheurlen
Prof. Dr. med. Paul-Gerhardt Schlegel
Neuroradiology Neuropathology
Dr. med. Ulrike Löbel Prof. Dr. med. Christian Hagel
Prof. Dr. med. Monika Warmuth-Metz Prof. Dr. med. Torsten Pietsch
Dr. med. Brigitte Bison Prof. Dr. med. Ulrich Schüller
Neurosurgery Neuropaediatrics:
Dr. med. Gertrud Kammler Dr. med. Jonas Denecke
Dr. med. Jürgen Krauß Dr. med. Pablo Hernáiz-Driever
Prof. Dr. med. Martin Schuhmann Dr. med. Ronald Sträter
Dr. med. Ulrich Thomale
Biology Human genetics:
Prof. Dr. med. Stefan Pfister Prof. Dr. med. Stefan Aretz
Dr. med. Hendrik Witt
Prof. Dr. med. Olaf Witt
Late effects Quality of Survival
Prof. Dr. med. Thorsten Langer Prof. Dr. med. Gabriele Calaminus
Neuropsychology International Collaborations
Dr. rer. nat. Holger Ottensmeier Prof. Dr. med. Martin Benesch /Österreich
Dipl.-Psych. Tanja Tischler Prof. Dr. med. Karin Dieckmann /Österreich
Dr. med. Nicolas Gerber /Schweiz
Biometry
Prof. Dr. rer. nat. et med. habil. Andreas Faldum

History of changes
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 82
10. History of changes Substantial changes marked in bold
10.1. Version 1.0
HIT-MED guidance established and published
10.2. Version 2.0
Chapter Change
2.1, 2.2, 2.3 “until 21” deleted where not indicated
2.1, 4.2, 4,4 Change in stratification algorithm: Patients 3 to 4 years with MYC-pos. CMB, CMB
M0R+, AMB, LCMB, that before were stratified into treatment with conventional RT
with 35.2Gy CSI + boost + maintenance chemotherapy should receive intensified
induction chemotherapy followed by response-adapted high-dose chemotherapy +/-
radiotherapy
(Decision made by HIT-MED trial committee 23 Jan 2015)
4.3 Information on differences to PNET 5 chemotherapy added
Appendix A
(Germany)
Added information for 2 cycles SKK-chemotherapy
Replaced “Hickman” by “Rickham” where misspelled.
10.3. Version 3.0
Chapter Change
2.2 replaced “59.4 Gy” by “54.0 Gy”, where mistyped
4.2 changed decision algorithm for treatment options: patients up to 4 years with
CMB, AMB, LCMB, that present isolated M1-dissemination can be treated either by
high-dose-chemotherapy or CSI after the intensified induction chemotherapy but
should not receive i. vtr. Methotrexate during induction in case a CSI is planned
4.1, 4.2, 4.3,
4.4, 4.5
note on genetic counselling in case of SHH-pathway-activation added
removed notes on diagnosis-verification and DICER1/RB1 mutations added
5.2 another two cycles on documentation sheet modified SKK added
6.1, 6.2, 6.4 surgery recommendations revised
8.1 information on dose modifications of Lomustine added
8.2 information on timing of 1st block SKK chemotherapy added
8.3 start of G-CSF in the interval between Cisplatin/Vincristine/Etoposide/
Cyclophosphamide and high-dose Methotrexate changed from day 5 to day 6
(transcription error)

History of changes
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 83
10.4. Version 4.0
Chapter Change
flyleaf clarified attention note
added a stratification overview for faster finding of information
new title due to the changed WHO classification of tumours of the CNS
preface added contact details Radiotherapy reference centre
2.1 changed and simplified stratification tableau,
added information on genetic counselling for SHH medulloblastoma +
comment on molecular subgroups
2.2 clarification of therapeutic approaches for ependymoma with residual
tumour
2.3 exclusion of general recommendations for infants with embryonal tumors
NOS and pineoblastoma (see comment k)
3.1 added current information on MB subgroups
4 overworked most of the flowcharts completely
added note, that all regimens were developed for primary treatment only
4.1 greyed out indication for infant AMB + CMB, added information on
subgroups
4.2 added infant M0 AMB, CMB + LCMB to indications, added information on
subgroups
added information on toxicity of Maintenance chemotherapy into “notes”
4.3 highlighted note on genetic counselling for SHH MB before RT, added
information on subgroups
simplified indication table
4.4 highlighted note on genetic counselling for SHH MB before RT, added
information on subgroups
simplified indication table
included Pineo > 4 years into this scheme
4.5 added information on subgroups
4.6 the old diagram 4.6 has been removed
emphasised role of re-surgery for ependymoma with residual tumour,
clarified the rationale for pre-RT chemotherapy in incompletely resected
ependymoma
4.7 The old diagram 4.7 has been removed (Pineo > 4 years now in 4.4)
4.8 Removed recommendation for chemotherapy after radiotherapy in
completely resected ependymoma
4.6, 4.7, 4.8 added “WHO grade II + III” to clarify the term “ependymoma”

History of changes
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 84
added the specification “intracranial” to the indication table
4.9 introduced the general indication of ETMR for this treatment
5.4 corrected count of i. vtr. MTX doses from 3 to 4 times
6.2 rephrased comment on the role of GTR vs. NTR in MB
7.1.2 added comment on proton therapy
7.1.6 added note on controversy concerning optic nerves, rephrased CTV
defintions
7.1.7 added “whole brain” to the OAR
7.1.12 added comment on IMRT and proton therapy
7.1.14 overworked the whole section, added alternative to HFRT 36 CSI in 7.1.14.7
7.2.4 added comment on primary metastatic ependymoma
7.2.6 added “whole brain” to the OAR
7.2.8 added comment on proton therapy
7.2.9 overworked the whole section, added alternative to local HFRT 68 Gy in
7.2.9.1 + 7.2.9.3
8 emphasis on the role of i. vtr. MTX only for primary treatment
8.2.4 included timing recommendations for modified SKK-chemotherapy
8.3 added 4th day of i. vtr. MTX (initially missed)
8.5.1, 8.5.2 added comment on dose modifications for children younger than 1
8.5.2 added timing recommendations
8.6.2 changed “discard” to “store […] sterilely”
9 added T. Tischler to HIT-MED study committee

Publication bibliography
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 85
Publication bibliography Ashley, D. M.; Merchant, T. E.; Strother, D.; Zhou, T.; Duffner, P.; Burger, P. C. et al. (2012): Induction
chemotherapy and conformal radiation therapy for very young children with nonmetastatic
medulloblastoma. Children's Oncology Group study P9934. In J. Clin. Oncol. 30 (26), pp. 3181–3186.
DOI: 10.1200/JCO.2010.34.4341.
Bueren, André Oscar von; Hoff, Katja von; Pietsch, Torsten; Gerber, Nicolas Ulrich; Warmuth-Metz,
Monika; Deinlein, Frank et al. (2011): Treatment of young children with localized medulloblastoma by
chemotherapy alone. results of the prospective, multicenter trial HIT 2000 confirming the prognostic
impact of histology. In Neuro-oncology 13 (6), pp. 669–679.
Bueren, André Oscar von; Kortmann, Rolf D.; Hoff, Katja von; Friedrich, Carsten; Mynarek, Martin;
Müller, Klaus et al. (2016): Treatment of Children and Adolescents With Metastatic Medulloblastoma
and Prognostic Relevance of Clinical and Biologic Parameters. Original Report. In J. Clin. Oncol. 34
(34), pp. 4151–4160. Available online at http://ascopubs.org/doi/pdf/10.1200/JCO.2016.67.2428,
checked on 2/3/2017.
Carrie, C.; Grill, J.; Figarella-Branger, D.; Bernier, V.; Padovani, L.; Habrand, J. L. et al. (2009): Online
quality control, hyperfractionated radiotherapy alone and reduced boost volume for standard risk
medulloblastoma. long-term results of MSFOP 98. In J. Clin. Oncol. 27 (11), pp. 1879–1883.
Chamberlain, M. C. (1998): Radioisotope CSF flow studies in leptomeningeal metastases. In Journal of
neuro-oncology 38 (2-3), pp. 135–140.
Chi, S. N.; Gardner, S. L.; Levy, A. S.; Knopp, E. A.; Miller, D. C.; Wisoff, J. H. et al. (2004): Feasibility
and response to induction chemotherapy intensified with high-dose methotrexate for young children
with newly diagnosed high-risk disseminated medulloblastoma. In J. Clin. Oncol. 22 (24), pp. 4881–
4887.
Cohen, B. H.; Zeltzer, P. M.; Boyett, J. M.; Geyer, J. R.; Allen, J. C.; Finlay, J. L. et al. (1995): Prognostic
factors and treatment results for supratentorial primitive neuroectodermal tumors in children using
radiation and chemotherapy. a Childrens Cancer Group randomized trial. In J. Clin. Oncol. 13 (7),
pp. 1687–1696.
Conter, C.; Carrie, C.; Bernier, V.; Geoffray, A.; Pagnier, A.; Gentet, J. C. et al. (2009): Intracranial
ependymomas in children. society of pediatric oncology experience with postoperative
hyperfractionated local radiotherapy. In International journal of radiation oncology, biology, physics
74 (5), pp. 1536–1542.
Dhall, G.; Grodman, H.; Ji, L.; Sands, S.; Gardner, S.; Dunkel, I. J. et al. (2008): Outcome of children less
than three years old at diagnosis with non-metastatic medulloblastoma treated with chemotherapy
on the "Head Start" I and II protocols. In Pediatric blood & cancer.
Ellison, D. W.; Kocak, M.; Figarella-Branger, D.; Felice, G.; Catherine, G.; Pietsch, Torsten et al. (2011):
Histopathological grading of pediatric ependymoma. reproducibility and clinical relevance in
European trial cohorts. In Journal of negative results in biomedicine 10, p. 7.
Fangusaro, J.; Finlay, J.; Sposto, R.; Ji, L.; Saly, M.; Zacharoulis, S. et al. (2008): Intensive
chemotherapy followed by consolidative myeloablative chemotherapy with autologous
hematopoietic cell rescue (AuHCR) in young children with newly diagnosed supratentorial primitive
neuroectodermal tumors (sPNETs). report of the Head Start I and II experience. In Pediatric blood &
cancer 50 (2), pp. 312–318. DOI: 10.1002/pbc.21307.

Publication bibliography
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 86
Fouladi, M.; Gilger, E.; Kocak, M.; Wallace, D.; Buchanan, G.; Reeves, C. et al. (2005): Intellectual and
functional outcome of children 3 years old or younger who have CNS malignancies. In J. Clin. Oncol.
23 (28), pp. 7152–7160.
Friedrich, Carsten; Bueren, André Oscar von; Hoff, Katja von; Gerber, Nicolas Ulrich; Ottensmeier, H.;
Deinlein, Frank et al. (2013): Treatment of young children with CNS-primitive neuroectodermal
tumors/pineoblastomas in the prospective multicenter trial HIT 2000 using different chemotherapy
regimens and radiotherapy. In Neuro-oncology 15 (2), pp. 224–234. DOI: 10.1093/neuonc/nos292.
Gajjar, A.; Chintagumpala, M.; Ashley, D.; Kellie, S.; Kun, L. E.; Merchant, T. E. et al. (2006): Risk-
adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in
children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96). long-term results
from a prospective, multicentre trial. In The lancet oncology 7 (10), pp. 813–820.
Gandola, L.; Massimino, M.; Cefalo, G.; Solero, C.; Spreafico, F.; Pecori, E. et al. (2009):
Hyperfractionated accelerated radiotherapy in the Milan strategy for metastatic medulloblastoma. In
J. Clin. Oncol. 27 (4), pp. 566–571.
Garvin, James H., Jr.; Selch, Michael T.; Holmes, Emi; Berger, Mitchell S.; Finlay, Jonathan L.; Flannery,
Ann et al. (2012): Phase II study of pre-irradiation chemotherapy for childhood intracranial
ependymoma. Children's Cancer Group protocol 9942. a report from the Children's Oncology Group.
for the Children's Oncology Group. In Pediatric blood & cancer 59 (7), pp. 1183–1189.
Geyer, J. R.; Sposto, R.; Jennings, M.; Boyett, J. M.; Axtell, R. A.; Breiger, D. et al. (2005): Multiagent
chemotherapy and deferred radiotherapy in infants with malignant brain tumors. a report from the
Children's Cancer Group. In J. Clin. Oncol. 23 (30), pp. 7621–7631.
Gibson, Paul; Tong, Yiai; Robinson, Giles; Thompson, Margaret C.; Currle, D. Spencer; Eden,
Christopher et al. (2010): Subtypes of medulloblastoma have distinct developmental origins. In
Nature 468 (7327), pp. 1095–1099. DOI: 10.1038/nature09587.
Grill, J.; Le Deley, M. C.; Gambarelli, D.; Raquin, M. A.; Couanet, D.; Pierre-Kahn, A. et al. (2001):
Postoperative chemotherapy without irradiation for ependymoma in children under 5 years of age. a
multicenter trial of the French Society of Pediatric Oncology. In J. Clin. Oncol. 19 (5), pp. 1288–1296.
Grundy, R. G.; Wilne, S. A.; Weston, C. L.; Robinson, K.; Lashford, L. S.; Ironside, J. et al. (2007):
Primary postoperative chemotherapy without radiotherapy for intracranial ependymoma in children.
the UKCCSG/SIOP prospective study. In The lancet oncology 8 (8), pp. 696–705. DOI: 10.1016/S1470-
2045(07)70208-5.
Hinkes, B. G.; Hoff, Katja von; Deinlein, Frank; Warmuth-Metz, Monika; Sörensen, Niels;
Timmermann, B. et al. (2007): Childhood pineoblastoma. experiences from the prospective
multicenter trials HIT-SKK87, HIT-SKK92 and HIT91. In Journal of neuro-oncology 81 (2), pp. 217–223.
DOI: 10.1007/s11060-006-9221-2.
Hoff, Katja von; Hartmann, Wolfgang; Bueren, André Oscar von; Gerber, Nicolas Ulrich; Grotzer,
Michael Andreas; Pietsch, Torsten; Rutkowski, Stefan (2010): Large cell/anaplastic medulloblastoma.
Outcome according to myc status, histopathological, and clinical risk factors. In Pediatr. Blood Cancer
54 (3), pp. 369–376. DOI: 10.1002/pbc.22339.
Hoff, Katja von; Hinkes, B.; Gerber, Nicolas Ulrich; Deinlein, Frank; Mittler, U.; Urban, C. et al. (2009):
Long-term outcome and clinical prognostic factors in children with medulloblastoma treated in the
prospective randomised multicentre trial HIT'91. In European journal of cancer 45 (7), pp. 1209–
1217. DOI: 10.1016/j.ejca.2009.01.015.

Publication bibliography
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 87
Hua, Chiaho; Bass, Johnnie K.; Khan, Raja; Kun, Larry E.; Merchant, Thomas E. (2008): Hearing loss
after radiotherapy for pediatric brain tumors: effect of cochlear dose. In International journal of
radiation oncology, biology, physics 72 (3), pp. 892–899. DOI: 10.1016/j.ijrobp.2008.01.050.
Jakacki, Regina; Zhou, Tianni; Holmes, Emi; Packer, Roger J.; Goldwein, Joel W.; Mehta, Minesh et al.
(2008): Outcome for Patients with nonpineal supratentorial PNET treated with Carboplatin as a
Radiosensitizer during Radiotherapy followed by adjuvant Cyclophosphamide and Vincristine.
preliminary Results of COG 99701. Abstract from the Thirteenth International Symposium on
Pediatric Neuro-Oncology (ISPNO). In Neuro-oncology 10 (3), p. 485.
Kool, Marcel; Korshunov, Andrey; Remke, Marc; Jones, David T. W.; Schlanstein, Maria; Northcott,
Paul A. et al. (2012): Molecular subgroups of medulloblastoma. An international meta-analysis of
transcriptome, genetic aberrations, and clinical data of WNT, SHH, Group 3, and Group 4
medulloblastomas. In Acta Neuropathol 123 (4), pp. 473–484. DOI: 10.1007/s00401-012-0958-8.
Kortmann, Rolf D.; Kühl, Joachim; Timmermann, B.; Mittler, U.; Urban, C.; Budach, V. et al. (2000):
Postoperative neoadjuvant chemotherapy before radiotherapy as compared to immediate
radiotherapy followed by maintenance chemotherapy in the treatment of medulloblastoma in
childhood. results of the German prospective randomized trial HIT '91. In International journal of
radiation oncology, biology, physics 46 (2), pp. 269–279.
Lannering, B.; Rutkowski, Stefan; Doz, F.; Pizer, B.; Gustafsson, G.; Navajas, A. et al. (2010): HIT-SIOP
PNET 4. A randomised multicentre Study of hyperfractionated versus standard Radiotherapy in
Children with standard Risk Medulloblastoma. In Neuro-Oncology 12 (6), pp. ii1-ii134. DOI:
10.1093/neuonc/noq043.
Lannering, B.; Rutkowski, Stefan; Doz, F.; Pizer, B.; Gustafsson, G.; Navajas, A. et al. (2012):
Hyperfractionated versus conventional radiotherapy followed by chemotherapy in standard-risk
medulloblastoma. results from the randomized multicenter HIT-SIOP PNET 4 trial. In J. Clin. Oncol. 30
(26), pp. 3187–3193. DOI: 10.1200/JCO.2011.39.8719.
Leary, S. E.; Zhou, T.; Holmes, E.; Geyer, J. R.; Miller, D. C. (2011): Histology predicts a favorable
outcome in young children with desmoplastic medulloblastoma. a report from the children's
oncology group. In Cancer 117 (14), pp. 3262–3267.
Macdonald, S. M.; Sethi, R.; Lavally, B.; Yeap, B. Y.; Marcus, K. J.; Caruso, P. et al. (2013): Proton
radiotherapy for pediatric central nervous system ependymoma. clinical outcomes for 70 patients. In
Neuro-oncology 15 (11), pp. 1552–1559.
Massimino, M.; Gandola, L.; Barra, S.; Giangaspero, F.; Casali, C.; Potepan, P. et al. (2010): Infant
Ependymoma in a 10-year AIEOP (Associazione Italiana Ematologia Oncologia Pediatrica) Experience
with Omitted or Deferred Radiotherapy. In International journal of radiation oncology, biology,
physics.
Massimino, M.; Gandola, L.; Giangaspero, F.; Sandri, A.; Valagussa, P.; Perilongo, G. et al. (2004):
Hyperfractionated radiotherapy and chemotherapy for childhood ependymoma. final results of the
first prospective AIEOP (Associazione Italiana di Ematologia-Oncologia Pediatrica) study. In
International journal of radiation oncology, biology, physics 58 (5), pp. 1336–1345.
Massimino, M.; Solero, C. L.; Garre, M. L.; Biassoni, V.; Cama, A.; Genitori, L. et al. (2011): Second-
look surgery for ependymoma. the Italian experience. In Journal of neurosurgery 8 (3), pp. 246–250.
Merchant, T. E.; Kiehna, E. N.; Li, C.; Xiong, X.; Mulhern, R. K. (2005): Radiation dosimetry predicts IQ
after conformal radiation therapy in pediatric patients with localized ependymoma. In International

Publication bibliography
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 88
journal of radiation oncology, biology, physics 63 (5), pp. 1546–1554. DOI:
10.1016/j.ijrobp.2005.05.028.
Merchant, T. E.; Li, C.; Xiong, X.; Kun, L. E.; Boop, F. A.; Sanford, R. A. (2009): Conformal radiotherapy
after surgery for paediatric ependymoma. a prospective study. In The lancet oncology 10 (3),
pp. 258–266.
Mynarek, Martin; Pizer, Barry; Dufour, Christelle; van Vuurden, Dannis; Garami, Miklos; Massimino,
Maura et al. (2016): Evaluation of age-dependent treatment strategies for children and young adults
with pineoblastoma: analysis of pooled European Society for Paediatric Oncology (SIOP-E) and US
Head Start data. In Neuro-Oncology. DOI: 10.1093/neuonc/now234.
Northcott, Paul A.; Korshunov, A.; Witt, H.; Hielscher, T.; Eberhart, C. G.; Mack, S. et al. (2011):
Medulloblastoma Comprises Four Distinct Molecular Variants. In J. Clin. Oncol. 29 (11), pp. 1408–
1414. DOI: 10.1200/JCO.2009.27.4324.
Packer, Roger J.; Gajjar, A.; Vezina, G.; Rorke-Adams, L.; Burger, P. C.; Robertson, P. L. et al. (2006):
Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly
diagnosed average-risk medulloblastoma. In J. Clin. Oncol. 24 (25), pp. 4202–4208.
Paganetti, Harald; Niemierko, Andrzej; Ancukiewicz, Marek; Gerweck, Leo E.; Goitein, Michael;
Loeffler, Jay S.; Suit, Herman D. (2002): Relative biological Effectiveness (RBE) Values for Proton
Beam Therapy. Biology Contribution. In International journal of radiation oncology, biology, physics
53 (2), pp. 407–421. Available online at http://ac.els-cdn.com/S0360301602027542/1-s2.0-
S0360301602027542-main.pdf?_tid=88049ea2-e965-11e6-bc7a-
00000aacb35e&acdnat=1486053476_1887ea7d70d11d53ccf0d661b928daf5, checked on 2/2/2017.
Pajtler, Kristian W. (2016): Toward an integrated histomolecular diagnosis of supratentorial
ependymoma. In Neuro-Oncology 18 (7), pp. 893–894. DOI: 10.1093/neuonc/now054.
Pajtler, Kristian W.; Mack, Stephen C.; Ramaswamy, Vijay; Smith, Christian A.; Witt, Hendrik; Smith,
Amy et al. (2017): The current consensus on the clinical management of intracranial ependymoma
and its distinct molecular variants. In Acta neuropathologica 133 (1), pp. 5–12. DOI: 10.1007/s00401-
016-1643-0.
Pajtler, Kristian W.; Witt, Hendrik; Sill, Martin; Jones, David T. W.; Hovestadt, Volker; Kratochwil,
Fabian et al. (2015): Molecular Classification of Ependymal Tumors across All CNS Compartments,
Histopathological Grades, and Age Groups. In Cancer cell 27 (5), pp. 728–743. DOI:
10.1016/j.ccell.2015.04.002.
Pietsch, Torsten; Schmidt, Rene; Remke, Marc; Korshunov, Andrey; Hovestadt, Volker; Jones, David T.
W. et al. (2014): Prognostic significance of clinical, histopathological, and molecular characteristics of
medulloblastomas in the prospective HIT2000 multicenter clinical trial cohort. In Acta Neuropathol
128 (1), pp. 137–149. DOI: 10.1007/s00401-014-1276-0.
Pizer, B. L.; Weston, C. L.; Robinson, K. J.; Ellison, D. W.; Ironside, J.; Saran, F. et al. (2006): Analysis of
patients with supratentorial primitive neuro-ectodermal tumours entered into the SIOP/UKCCSG
PNET 3 study. In European journal of cancer 42 (8), pp. 1120–1128.
Ramaswamy, Vijay; Remke, Marc; Bouffet, Eric; Bailey, Simon; Clifford, Steven C.; Doz, Francois et al.
(2016): Risk stratification of childhood medulloblastoma in the molecular era: the current consensus.
In Acta neuropathologica 131 (6), pp. 821–831. DOI: 10.1007/s00401-016-1569-6.
Rutkowski, Stefan; Bode, Udo; Deinlein, Frank; Ottensmeier, H.; Warmuth-Metz, Monika; Sörensen,
Niels et al. (2005): Treatment of early childhood medulloblastoma by postoperative chemotherapy
alone. In N Engl J Med 352 (10), pp. 978–986.

Publication bibliography
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 89
Rutkowski, Stefan; Bueren, André Oscar von; Warmuth-Metz, Monika; Sörensen, Niels; Deinlein,
Frank; Schlegel, P. G. et al. (2010a): Treatment of children and adolsecents with metastatic
medulloblastoma by conventional chemotherapy and hyperfractionated radiotherapy. Prelininary
results of the prospective GPOH-trial HIT2000 (MET-HIT 2000 AB4). In Neuro-oncology 12 (6), pp. ii5.
DOI: 10.1093/neuonc/noq043.
Rutkowski, Stefan; Hoff, Katja von; Emser, A.; Zwiener, Isabella; Pietsch, Torsten; Figarella-Branger, D.
et al. (2010b): Survival and prognostic factors of early childhood medulloblastoma. an international
meta-analysis. In J. Clin. Oncol. 28 (33), pp. 4961–4968.
Shih, D. J. H.; Northcott, Paul A.; Remke, M.; Korshunov, A.; Ramaswamy, V.; Kool, Marcel et al.
(2014): Cytogenetic Prognostication Within Medulloblastoma Subgroups. In J. Clin. Oncol. 32 (9),
pp. 886–896. DOI: 10.1200/JCO.2013.50.9539.
Tarbell, N. J.; Friedman, H.; Polkinghorn, W. R.; Yock, T.; Zhou, T.; Chen, Z. et al. (2013): High-risk
medulloblastoma. a pediatric oncology group randomized trial of chemotherapy before or after
radiation therapy (POG 9031). In J. Clin. Oncol. 31 (23), pp. 2936–2941.
Taylor, M. D.; Northcott, Paul A.; Korshunov, A.; Remke, M.; Cho, Y. J.; Clifford, S. C. et al. (2012):
Molecular subgroups of medulloblastoma. the current consensus. In Acta neuropathologica 123 (4),
pp. 465–472. DOI: 10.1007/s00401-011-0922-z.
Taylor, M. D.; Poppleton, H.; Fuller, C.; Su, X.; Liu, Y.; Jensen, P. et al. (2005a): Radial glia cells are
candidate stem cells of ependymoma. In Cancer cell 8 (4), pp. 323–335.
Taylor, R. E.; Bailey, C. C.; Robinson, K.; Weston, C. L.; Ellison, D.; Ironside, J. et al. (2003): Results of a
randomized study of preradiation chemotherapy versus radiotherapy alone for nonmetastatic
medulloblastoma. The International Society of Paediatric Oncology/United Kingdom Children's
Cancer Study Group PNET-3 Study. In J. Clin. Oncol. 21 (8), pp. 1581–1591.
Taylor, R. E.; Bailey, C. C.; Robinson, K. J.; Weston, C. L.; Walker, D. A.; Ellison, D. et al. (2005b):
Outcome for patients with metastatic (M2-3) medulloblastoma treated with SIOP/UKCCSG PNET-3
chemotherapy. In European journal of cancer 41 (5), pp. 727–734.
Timmermann, B.; Kortmann, Rolf D.; Kühl, Joachim; Meisner, C.; Dieckmann, K.; Pietsch, Torsten;
Bamberg, M. (2002): Role of radiotherapy in the treatment of supratentorial primitive
neuroectodermal tumors in childhood. results of the prospective German brain tumor trials HIT
88/89 and 91. In J. Clin. Oncol. 20 (3), pp. 842–849.
Timmermann, B.; Kortmann, Rolf D.; Kühl, Joachim; Rutkowski, Stefan; Meisner, C.; Pietsch, Torsten
et al. (2006): Role of radiotherapy in supratentorial primitive neuroectodermal tumor in young
children. results of the German HIT-SKK87 and HIT-SKK92 trials. In J. Clin. Oncol. 24 (10), pp. 1554–
1560. DOI: 10.1200/jco.2005.04.8074.
Venkatramani, R.; Ji, L.; Lasky, J.; Haley, K.; Judkins, A.; Zhou, S. et al. (2013): Outcome of infants and
young children with newly diagnosed ependymoma treated on the "Head Start" III prospective
clinical trial. In Journal of neuro-oncology 113 (2), pp. 285–291.
Verlooy, J.; Mosseri, V.; Bracard, S.; Tubiana, A. L.; Kalifa, C.; Pichon, F. et al. (2006): Treatment of
high risk medulloblastomas in children above the age of 3 years. a SFOP study. In European journal of
cancer 42 (17), pp. 3004–3014.
Wang, Xin; Dubuc, Adrian M.; Ramaswamy, Vijay; Mack, Stephen; Gendoo, Deena M. A.; Remke,
Marc et al. (2015): Medulloblastoma subgroups remain stable across primary and metastatic
compartments. In Acta Neuropathol 129 (3), pp. 449–457. DOI: 10.1007/s00401-015-1389-0.

Publication bibliography
HIT-MED Therapy Guidance Version 4.0 – 02 May 2017 90
Widemann, B. C.; Balis, F. M.; Shalabi, A.; Boron, M.; O'Brien, M.; Cole, D. E. et al. (2004): Treatment
of accidental intrathecal methotrexate overdose with intrathecal carboxypeptidase G2. In J Natl
Cancer Inst 96 (20), pp. 1557–1559.
Witt, H.; Mack, S. C.; Ryzhova, M.; Bender, S.; Sill, M.; Isserlin, R. et al. (2011): Delineation of two
clinically and molecularly distinct subgroups of posterior fossa ependymoma. In Cancer cell 20 (2),
pp. 143–157.
Zacharoulis, S.; Levy, A.; Chi, S. N.; Gardner, S.; Rosenblum, M.; Miller, D. C. et al. (2007): Outcome for
young children newly diagnosed with ependymoma, treated with intensive induction chemotherapy
followed by myeloablative chemotherapy and autologous stem cell rescue. In Pediatric blood &
cancer 49 (1), pp. 34–40. DOI: 10.1002/pbc.20935.













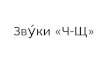











![Shh new fostertraining[1]](https://img.dokumen.tips/doc/110x75/554c94e5b4c905b80b8b4a0b/shh-new-fostertraining1.jpg)


