Embed Size (px)
Citation preview

Histo-Meeting 22-10-2015
2
- Seit 2 Monate persistierende abdominale Beschwerden:
Schmerzen, Diarrhö ohne Melena, ohne frischer Blut
- Beschwerdensanfang: 1 Monat nach einer Reise im Thailand
- St.nach Dekompressionskrankheit beim Tauchen dort behandelt
- Calprotectin positv, Stuhlprobe: positiv für Giardia lamblia
- Behandlung: Metronidazol über 6d, Umstellung auf Zentel über 5d
bei fehlendem Ansprechen, Planung einer Koloskopie
Erneute notfallmäßige Vostellung am 28.09.15
- Keine Besserung,Schwäche und anamnestisch Gewichtsverlust
von 15 kg/3 Monate und täglicher Cannabiskonsum
30-jähriger Mann

3
Untersuchungen
• Ileo-Kolonoskopie vom 29.09.2015:
bei mässiger Darmvorbereitung unauffällig
• Ösophago-Gastro-Duodenoskopie vom 29.09.15:
6 kraterförmige bis 4cm große Ulcera im Korpus und Fundus,
fibrin- und hämatinbelegt, mit erhabenem Randwall bis zum
gastroösophagealen Übergang

4
Oesophago-Gastro-Duodenoskopie 29.09.2015

5
Histologie: nur wenige Drüsen, Lamina propria
expandiert

6
Starke Proliferation, Rasen
mittelgroßer Blasten mit 3-6
Nukleolen,
Kerntrümmermakrophagen
“Sternenhimmel“
Immunhistochemie:
CD79a als B-Zell-Marker v.a. im
Rahmen von Lymphomen

7
CT Thorax Abdomen vom 30.09.2015:
Vermehrte Magenwandfältelung im Bereich des Fundus,
zudem Wandverdickung im Bereich des Antrums
Ödematöse zirkuläre Wandverdickung des Colon ascendens,
der rechten Colonflexur und der rechtsseitigen Hälfte des
Colon transversums, keine Zeichen einer Perforation
prominente Lymphknoten kaudal des Magens sowie links
lateral der Nebenniere und pulmonal links
20 x 17 mm grosse pulmonale Raumforderung am
Interlobium links

8
Diagnose: Burkitt-Lymphom
– Infiltrate in gastrisch-glandulärer Schleimhaut des Korpus und
Fundus
– Translokation des c-Myc-Genlokus, keine Hinweise für einen
Chromosomenbruch am BCL2 oder BCL6-Genlokus
–Serologien 01.10.2015: EBV IgG positiv, IgM negativ; HCV
negativ, HIV negativ, Treponemen negativ, H. pylori negativ
PET-CT vom 07.10.15:
Multiple Stoffwechselaktive Lymphommanifestationen im
Nasopharynx , pulmonal, Magen, peritoneal, Haut
KMP vom 08.10.15: unauffällig
Therapie: 6 Zyklen Chemotherapie, z.T. intrathekal

9
29yo male• Morbus Crohn (diagnose 11/2014: terminal ileum, 05/2015: sigma)
– Currently treated with Methotrexat 25 mg per week, folic acid 3x/day
and budenofalc 9 mg
• St. post. abscess perianal at 5 o’clock in lithomy position 05/2015
• St. post. acute pancreatitis 05/2015, most likely drug induced
(Puri-Nethol)
• Adiposity
• Chronic nicotine abuse 1 packet per day (15 py)
• 15/09/15: epigastric pain, radiating to the back and belly button,
beginn in the morning, vomiting suspicion of gastritis
• 22/09/2015: consultation appointment and control by diarrhea
with blood admixture and anal pruritus since 3 weeks

10
Colonoscopy 22/09/2015
Discrete aphtoid lesions in the
rectum
Terminal ileum with fibrin-
coated ulcerations
11
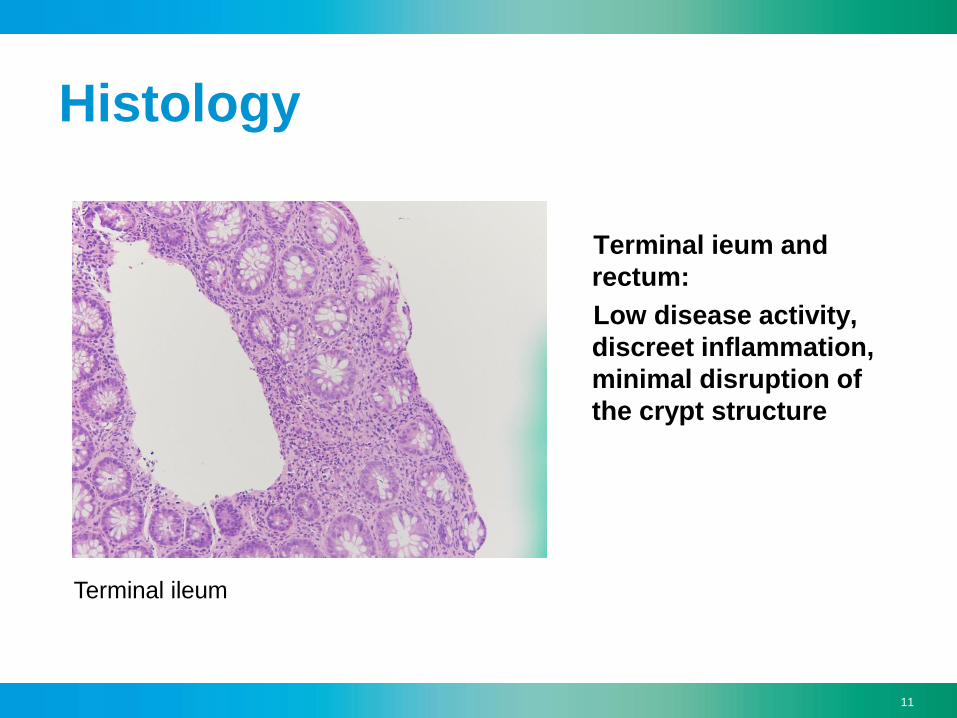
Histology
Terminal ieum and
rectum:
Low disease activity,
discreet inflammation,
minimal disruption of
the crypt structure
Terminal ileum

12
90 year old female
• Choledocholithiasis
– ERCP: stone extraction, stent
• Gastroscopy: 1.5 cm lesion Bulbus duodeni, biopsy
• Coronary artery disease
• Valvular aortic stenosis
• Chronic renal insufficiency
• COPD Gold I
• PAVK

13
Gastroscopy 09/2015
12-15 mm lesion with central cavity

14
HistologyRunde monomorphe Zellen in Nestern &
Trabekeln, dd NET vom trabekulären
Wachstum, dd GIST
Immunhistochemie auf Chromogranin A:
Positiv somit NET, hier G1

15
72yo male• NSCLC right Stadium IB,pT2apN0(0/24) L0V0Pn0G2R0 ED 06.2015
- Thoracoscopic uniportal lung resection with radical mediastinal
lymphadenopathy
• Obtructive pulmonary disease
• Dilatative arteriopathy
- St.n. ruptured infrarenal abdominal aortic aneurysm with ruptur in vena cava
inferioir 10/2006
- Aortobiliakal Y Graft
- St n Cavotomie, ilio-caval thrombectomy, patch vena cava inf 11.2006
- Poplitealaneursyma resection and reconstruction with VSM interponat 05.2015 by
asymptomatic thrombosed popliteal aneurysma left
• Coronary artery disease 3 vessels
- St n NSTEMI 11/2012
- St n PTA/DES RCX and RCA 2012
- St n PTA/DES RCA and RIVA 01/2013

16
Gastroscopy 09/2015
«Normal» chromoendoscopyBarrett Osophagus C7M10

17
EUS 09/2015
EUS uT1, evtl uN1

18
Gastroscopy 10/2015
Suspicious lesionChromoendoscopy

19
Gastroscopy 10/2015
ESD with hybrid knife 28-34cm EMR 37cm

20
EMR Resectat
Kryptenempyem, Nekrosen: red flags
signs
Intramukosale Neoplasie, «never
ending» Drüsen
21
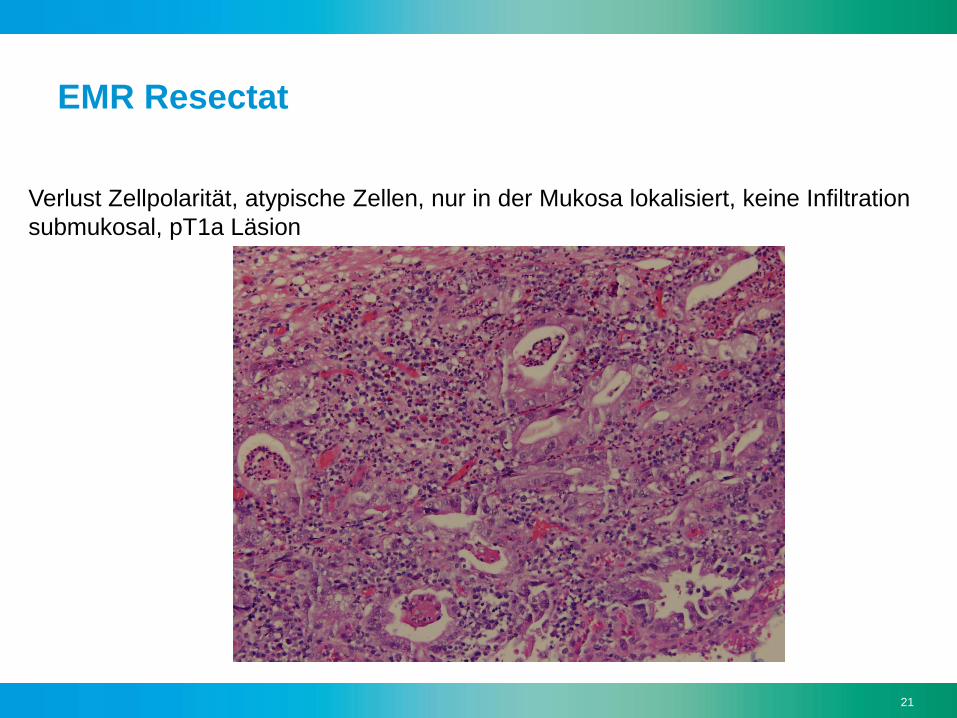
EMR Resectat
Verlust Zellpolarität, atypische Zellen, nur in der Mukosa lokalisiert, keine Infiltration
submukosal, pT1a Läsion

22
- Diarrhea since 14 days before admission
- Haematemesis
- 16.8.15 Gastroscopy :submucosal Tumor in
Corpus/Antrum Adrenalin injektion
- 16.8.15 CT : Tumor in Antrum without Metastasis or
pos. LN
Other Dg:
DM Type 2
Hypertension
64-year old male

23

24
Endoscopy- Stomach

25
Histology - GIST
Principal patterns are spindled 2/3
or epithelioid 1/3
Spindeled: eosinophilic, indistinct cytoplasm
Oval spindled nuclei
Distinct from surrounding stroma
PAS/d positive
Epithelioid: Round/polygonal cells,
Round to oval nuclei, Frequent cytoplasmic
retraction creates clearing artifact





























