Embed Size (px)
Citation preview

CALIFORNIA STATE UNIVERSITY, FRESNO AUXILIARY CORPORATIONS
Association Agricultural Foundation Foundation Fresno State Programs for Children
Hiring Checklist
Name:________________________ SSN:_____________________ Date of Hire:__________________ Dept/Project:_______________ Cost Center:__________________ To be returned to Human Resources: . . . . . . Application – Completed and signed. . . . . . . I-9 Completed and Copies of Identification Attached. . . . . . . W-4 & DE 4 Forms Attached. . . . . . . IIPP Safety Signoff Sheet. . . . . . . Student/Part-time Employee Information Sheet completed. . . . . . . Nature of Employment Acknowledgment (signed). . . . . . . Payroll Agreement completed for all University Employees . . . . . . Copy of Driver’s License (if new hire required to drive). . . . . . . Proof of Insurance (if new hire required to drive on duty). Given to Employee at Original Date of Hire: . . . . . . Sexual Harassment Brochure. . . . . . . Nature of Employment Policy. . . . . . . Employee Assistance & Development Brochure (EAP). . . . . . . Workers’ Compensation Informational Brochures. . . . . . . Workplace Violence Guide. . . . . . . State Disability Insurance Brochure. . . . . . . Paid Family Leave Insurance Brochure. . . . . . . IIPP Manual. _________________________________ ________________ Employee Signature Date _________________________________ ________________ Supervisor’s Signature Date

CALIFORNIA STATE UNIVERSITY, FRESNO FOUNDATION
STUDENT/PART-TIME/TEMPORARY EMPLOYEE INFORMATION SHEET
PLEASE CHECK ALL THAT APPLY: NEW HIRE PART-TIME STUDENT at Fresno State CHANGE
RE-HIRE
Fresno State Faculty _________ #of units enrolled for:
Fresno State Staff Fall Spring Summer Non-Fresno State Employee
Address Emergency Info Pay Increase
(complete below)
TO BE COMPLETED BY EMPLOYEE
Name:
Social Security Number:
/ / Local Address: _____________________________________________________________________________________________ No. Street City State Zip Code Permanent Address: _____________________________________________________________________________________________
Home Phone Number:
( ) ____________ Work Phone Number:
( ) ____________ No. Street City State Zip Code CSU Fresno Email Address: ______________________________________________________
Married Single
Male Female
Date of Birth: Check Route: Foundation Bookstore U.S. Mail
Have you worked or are you currently working for the Foundation, Ag Foundation, or Fresno State Programs for Children?
Yes No
If Yes, Last Day Worked: ______________________________________ Location: ___________________________________________________________________
EMERGENCY CONTACT INFORMATION (Employee must update each semester) In case of emergency, notify:
Name: _________________________________________________________
Relationship:
__________________________________
Phone Number:
( ) ________________
Address: _____________________________________________________________________________________________________________________ No. Street City State Zip Code
ACKNOWLEDGEMENTS I have completed the attached forms: (please check) I have received the following:
I-9 (Form and Instructions attached) 1. Sexual harassment information and brochure
W-4 & DE 4 forms 2. Workers’ Compensation brochure
Application for Employment 3. State Disability Insurance brochure
Nature of Employment Acknowledgement 4. Nature of Employment Policy
Dated: _____________________________________ _____________________________________________
Employee Signature
TO BE COMPLETED BY SUPERVISOR Cost Center:
Date of Hire or Re-hire:
Work Location and Mail Stop:
Hourly rate of Pay: $
Position Title and brief description of duties: Confidential Data Access? Yes No
Is driving a requirement for this position? Yes No
Nepotism: “Related employees are not permitted to work in job positions in which a conflict of interest could arise or in a direct supervisory relationship.” To my knowledge, this hire will not violate the Foundation Nepotism policy. Yes No http://www.auxiliary.com/Foundation/documents/FoundationNepotismPolicy.doc
PAY INCREASE Reason for increase: Current Hourly Rate: New Hourly Rate: Effective Date:
AUTHORIZATION REQUIRED Signature of Employee Date
Signature of Supervisor
Date
Signature of Project Director Date
Signature of Grant Accountant Date
OFFICE USE ONLY HR Setup
Entered by (Initial) Date
PR Input (Initial) Date



CALIFORNIA STATE UNIVERSITY, FRESNO AUXILIARY CORPORATIONS
M:\HR\Forms\Forms - New Hire\Emergency Information Sheet-Auxiliaries.doc Revised: 1/31/2008
EMPLOYEE EMERGENCY INFORMATION
Please complete the following emergency information (please print): Employee Name _____________________________________ Phone _______________________ Address _______________________________________________Cell__________________________ City _____________________________________________ Zip __________________________ In case of emergency, notify the following:
Name ______________________________________ Relationship __________________ Address ____________________________________ Phone: Home _________________ City ________________________ Zip ___________ Work__________________ -------------------------------------------------------------------------------------------------------------------------------------------------
PRE-DESIGNATE PHYSICIAN FOR WORK RELATED INJURY Please read carefully: This information pertains to work-related injury or illness: You are entitled to be treated by your own personal physician if the pre-designation form is completed and returned to the Auxiliaries Human Resources Office prior to any work-related injury. If you do not designate a physician and need medical treatment for a work-related injury or illness, you will be referred to the organization’s approved physician. If you do not pre-designate a physician before the injury, you will be treated by the organization’s approved physician. Please complete below:
I elect to be treated by the organizations’s approved work physician
I elect to be treated by my own physician (Please list physician information below) __________________________________ ___________________
Physician Name Phone ___________________________________________________________________ Address City Zip Code Employee Signature ______________________________________ Date ________________________








DRUG-FREE WORKPLACE POLICY
Purpose and Goal California State University, Fresno Foundation (“Foundation”) is committed to protecting the safety, health and well being of all employees and other individuals in our workplace. We recognize that alcohol abuse and drug use pose a significant threat to our goals. We have established a drug-free workplace program that balances our respect for individuals with the need to maintain an alcohol and drug-free environment. The organization encourages employees to voluntarily seek help with drug and alcohol problems. Covered Workers Any individual who conducts business for the organization, is applying for a position or is conducting business on the organization's property is covered by our drug-free workplace policy. Our policy includes, but is not limited to executive management, managers, supervisors, full-time employees, part-time employees, contractors, volunteers, interns and applicants. Applicability Our drug-free workplace policy is intended to apply whenever anyone is representing or conducting business for the organization. Employees are expected and required to report to work on time and in appropriate mental and physical condition for work. It is our intent and obligation to provide a drug free, healthful, safe, and secure work environment. Prohibited Behavior • The unlawful manufacture, distribution, dispensation, possession, or use of a controlled substance at a
Foundation worksite or on the campus or while elsewhere conducting Foundation or university business is absolutely prohibited and subject to sanctions noted below.
• On campus or Foundation worksite use of alcohol is limited to certain approved events and locations covered by the guidelines of Fresno State’s official Policy on Alcohol and Other Drugs. Workplace abuse of alcohol will not be tolerated.
California State University, Fresno Foundation encourages employees to voluntarily seek help with drug and alcohol problems through use of the Employee Assistance Program at (559)278-4357. Notification of Convictions Foundation employees must, as a condition of employment, abide by the terms of the Policy and report any conviction under a criminal drug statute for violations occurring at the Foundation worksite or university or while elsewhere conducting Foundation or university business. A conviction must be reported to Human Resources within 5 (five) days. Violation of the Policy may result in disciplinary action up to and including suspension or termination of employment and referral for prosecution where laws have been broken. Federal/state contracting agencies will be notified when appropriate. As a condition of continued institutional grant or contract eligibility, and as a condition of employment under any federal/state contract or grant, employees must comply not only with this policy, but also with the requirement of notifying the Human Resources Department within five (5) days of any conviction

under a criminal drug statute where the criminal act upon which the conviction is based occurred while at a Foundation worksite or while elsewhere conducting Foundation or university business, or upon property owned, operated or controlled by the University. Within ten (10) days after receiving such notice, the Foundation must notify the federal/state grant or contract authority. Within thirty (30) days after receiving such notice, the Foundation may initiate appropriate disciplinary action, including discharge, against the employee or require the employee to participate in an approved rehabilitation program. A copy of this policy statement will be provided each Foundation employee whether employed under a federal/state contract or grant or otherwise. In addition, the Foundation will make drug education programs available utilizing the University’s Employment Assistance Program. Consequences One of the goals of our drug-free workplace program is to encourage employees to voluntarily seek help with alcohol and/or drug problems. If, however, an individual violates the policy, the consequences are serious. In the case of applicants, if he or she violates the drug-free workplace policy, the offer of employment can be withdrawn. The applicant may not reapply. If an employee violates the policy, he or she will be subject to disciplinary action (which may include termination) and may be required to enter rehabilitation. An employee required to enter rehabilitation that fails to successfully complete it and/or repeatedly violates the policy will be terminated from employment. Nothing in this policy prohibits the employee from being disciplined or discharged for other violations and/or performance problems. Penalties for Workplace Drug Use WARNING • State and Federal penalties apply to anyone convicted of the manufacture, distribution, possession
or use of controlled substances. • Misdemeanor convictions for workplace drug use can result in a fine and incarceration of up to a
year in a county jail. Relatively few drug-related infractions may be considered misdemeanor offenses, however. Most drug use convictions are defined as felony acts.
• Felony convictions for workplace drug use can result in a substantial fine and a lengthy sentence in state prison. Convictions for manufacture, possession for sale or use of substances such as the following examples are felony offenses: amphetamines (whites, uppers), barbiturates, codeine, cocaine/crack, heroin, L.S.D., Methamphetamines (crank, crystal), marijuana, and P.C.P
• The Foundation is required by federal law to take disciplinary action up to and including suspension or termination of employment for staff convicted of a workplace drug offense.
The bottom line? The price for drug use is high…let’s keep a drug-free workplace!! Assistance
The Foundation recognizes drug and alcohol dependency as treatable conditions and offers the Employee Assistance and Wellness (EA&W) office for employees with substance abuse or dependency problems. Employees are encouraged to seek assistance for drug- and alcohol-related problems and may request leaves of absence for this purpose, in addition to using approved vacation or sick leave. Information obtained regarding an employee during participation in EA&W will be treated as confidential. • Foundation employees may contact the Employee Assistance and Wellness Office (278-4357) for
confidential consultation regarding substance abuse or other personal problems at no cost to the employee or member of their immediate family. A careful assessment of the situation will be made and alternatives will be offered which are both appropriate and affordable.
• Community agencies are also available to address drug and alcohol problems. Most of the various local drug treatment programs offer no-cost assessment. They can be located in the Yellow Pages of the phone book or on the Internet under “Drug Abuse & Addiction Information & Treatment Centers”
Treatment for alcoholism and/or other drug use disorders may be covered by the employee benefit plan. However, the ultimate financial responsibility for recommended treatment belongs to the employee. Confidentiality All information received by the organization through the drug-free workplace program is confidential communication. Access to this information is limited to those who have a legitimate need to know in compliance with relevant laws and management policies. Drug Free Workplace Awareness workshops and seminars sponsored by the Fresno State Human Resources and EA&D offices are another source of information and assistance. Shared Responsibility A safe and productive drug-free workplace is achieved through cooperation and shared responsibility. Both employees and management have important roles to play. All employees are required to not report to work or be subject to duty while their ability to perform job duties is impaired due to on- or off-duty use of alcohol or other drugs. It is the supervisor's responsibility to: * Inform employees of the drug-free workplace policy. * Document negative changes and problems in performance. Communication Communicating our drug-free workplace policy to both supervisors and employees is critical to our success. To ensure all employees are aware of their role in supporting our drug-free workplace program: * All employees will receive a written copy of the policy. * All employees will receive an update of the policy annually with their paychecks. * Employee education about the dangers of alcohol and drug use and the availability of help will be provided to all employees. Impact of Substance Abuse in the Workplace

Employee Health • Higher use of health benefits • Increased use of sick time • Higher absenteeism and tardiness Productivity: • Reduced output • Increased errors • Lower quality of work • Reduced customer satisfaction Decision Making • Reduced innovation • Reduced creativity • Less competitiveness • Poor decisions, both daily and strategic Safety/Danger • Increased accidents • Increased health and safety risks for others • More workers’ compensation claims Employee Morale • Higher turnover • Lower quality • Reduced team effort Security • Theft • Law enforcement involvement Organizational Image and Community Relations • Reduced trust and confidence • Reduced ability to attract high-quality employees Specific Drugs of Abuse Alcohol - signs and symptoms of abuse: • Dulled mental processes • Lack of coordination • Slowed reaction time • Poor judgment • Reduced inhibitions Marijuana - Signs and symptoms of use: • Bloodshot eyes • Impaired or reduced short-term memory and comprehension • Altered sense of time • Reduced ability to perform tasks requiring concentration and coordination, such as driving a car

Inhalants – signs and symptoms of abuse: • Nausea • Nosebleeds • Muscle fatigue • Permanent damage to the nervous system • Severely impaired judgment and driving ability. • Severe disorientation, visual distortion and confusion. Cocaine - signs and symptoms of abuse: • Dilated pupils • Insomnia • Paranoia • Anxiety, agitation • Periods of increased activity followed by fatigue and depression • Wide mood swings • Difficulty in concentration

Drug-Free Workplace Policy California State University, Fresno Foundation
Acknowledgment
I understand that the Foundation is committed to protecting the safety, health and well being of all employees and other individuals in the workplace. It is also my understanding that the drug-free workplace policy is intended to apply whenever anyone is representing or conducting business for the organization. Therefore, I understand that I am expected and required to report to work on time and in an appropriate mental and physical condition for work. Furthermore, I acknowledge that if I am convicted of a criminal drug violation in the workplace I must notify the organization in writing within five calendar days of the conviction. Employee Acknowledgement: I certify that I have read and understand the contents contained in the Drug-Free Workplace Policy for California State University, Fresno Foundation. I understand a copy of this agreement will be placed in my personnel file in Human Resources. _____________________________ ________________________ Employee Signature Date _____________________________ ________________________ Manager Signature Date

Page 1 of 2
CALIFORNIA STATE UNIVERSITY, FRESNO FOUNDATION
Effective May 1, 2008
Criteria for Driving On Foundation Business Driver must be a Foundation employee who is:
Paid directly by the Foundation at full-time or part-time salaried status, or at part-time hourly status.
Driver may be a California State University, Fresno state employee who is: Authorized by the Foundation to drive in order to conduct directly related business on an awarded Foundation sponsored program (grant or contract). The state employee is to have an authorized Released Reimbursed Time Contract or a Foundation Payroll Overload Agreement on file at the Foundation for conducting work specific to a Foundation sponsored program. Please note: State employees must be conducting state business in order to be covered by State insurance as provided by university/State guidelines.
Driver must possess valid California Drivers License Non-occasional drivers must complete a CSU approved defensive driving course. Non-occasional drivers are employees who drive more than once a week in order to conduct Foundation sponsored program business or whose primary duty is driving-related. Refer to the Defensive Driving Course registration which includes the DMV Employee Pull Notice Program located on the website at: http://www.csufresno.edu/ehs/. Drivers must have a good driving record:
No more than 3 DMV points within last four years No failures to appear No unpaid fines No convictions within last four years for offenses that are assigned two (2) points by the DMV.
Use of privately owned vehicles to conduct official Foundation business is authorized, but damages incurred to the individual or to the automobile is the vehicle owner’s responsibility. Vehicles temporarily owned by a Foundation sponsored project and authorized to be the responsibility of the Foundation as outlined in a Foundation sponsored project shall only be used in the conduct of Foundation business specific to the awarding sponsored project:
This means only when driven in the performance of, or necessary to, or in the course of, the duties of the Foundation sponsored project associated with the vehicle.

Page 2 of 2
Foundation employees misusing vehicles owned by a sponsored project are liable for the costs of misuse incurred by them or consented to by them.
Motor vehicle accidents:
Make no comment or statement regarding the accident to any one except police, other approved Foundation officials or employees, or an identified representative of the Foundation’s contract adjuster, Alliant Insurance. Report all communication within 48 hours after occurrence regarding vehicle accidents, claims, including summons or complaints, to the Foundation Staff Counsel (559) 278-0818 and Financial Services Office (559) 278-0850 at Mail stop #OF 123. Please ask for your Grant Accountant. The driver’s immediate supervisor will be required to report acknowledgement of the accident to the Foundation.
Motor vehicle liability insurance: Foundation Staff Counsel will respond to claims of bodily injury and/or property damage of third party individuals that occur during official Foundation business. Evaluation and payments of claims will be handled in conjunction with the Foundation’s insurers. Foundation employees renting a vehicle to conduct Foundation business are covered while conducting that business, by an insurance policy provided by the Foundation insurance agency as a provision of the Foundation contract with the insurance company. Prior to renting a vehicle employees should contact the Foundation to verify the appropriate vehicle rental agency that Foundation may have a negotiated contract accounts that include certain insurance coverage with their negotiated rates. State employees who are not compensated directly by the Foundation (no payroll overload agreement on file at the Foundation) are not covered by the Foundation’s insurance policy for damage to a rented vehicle. State employees not directly compensated by the Foundation must purchase the additional insurance from the vehicle rental agency in the name of the California State University, Fresno Foundation if the state employee is conducting Foundation business. State employees can consult the university Environmental Health and Safety Department for questions regarding university insurance coverage while driving to conduct State business.
The Foundation’s insurance does not provide for loss or damage to privately owned vehicles, CSU, or State vehicles used on Foundation business. It is designed to provide reimbursements to third parties only (when an accident is the fault of the Foundation driver conducting Foundation business) and not Foundation, State, or University employees or their vehicles.







California State University, Fresno Foundation Payroll Agreement
Completed by the Employee Agreement #_________________
(Foundation Use) Section 1: Employee Information
Employee Social Security # University Status: � 10 month � 12 month � Academic Year (AY) �Faculty or � Staff University College/Department Section 2: Complete this Section Only if Requesting Academic Year Overload and/or Summer Pay that was budgeted/approved
Project Title Cost Center # Project Director Sponsoring Agency Period Covered / / to / /
Original/Current approved budget:
AY Overload : # Hours ________ Salary $ ___________ Fringe Benefits $ ____________ Total $ Summer Pay: # Hours ________ Salary $ ___________ Fringe Benefits $ ____________ Total $______________ Section 3: Complete this Section Only if Requesting Change from approved Reimbursed Release Time (RRT) to AY Overload Pay (A proposed change from reimbursed released time to academic year overload must be for the same time period within the academic year as was originally approved.) NOTE: Changing RRT to summer pay cannot be accomplished by completing this form. This type of request would change the Scope of Work and timeline for project activities. If you wish to request such a change in effort, you must submit a revised Scope of Work and timeline to the funding agency and provide their written approval to your Grant Accountant prior to changing the effort. Project Title Cost Center # ______________ Project Director Sponsoring Agency Period Covered / / to / / Original/Current approved budget: Released Reimbursed Time: # WTU’s___________ Percent (%) time ________ Salary $ ___________ Fringe Benefits $ ____________ Total $ ____________ Proposed effort change: AY Overload : # Hours ________ Salary $ ___________ Fringe Benefits $ ____________ Total $
Reason for proposed change:______________________________________________________________ __________________________________________________________________________________ The following documents must be obtained/attached: • Written approval from your Department Chair and Dean to change from Released Reimbursed Time to Academic Year
Overload pay (approval signature below is sufficient) • Written approval from the funding agency to change effort from Released Reimbursed Time to Academic Year
Overload pay. (In some cases e-mail documentation may be sufficient). • Copy of the original/current approved budget. • Summary of all AY overload commitments for the same time period. [Foundation Use Only: Verified By:__________ Date:___________]
Section 4: Required Signatures for Approval Employee Date Project Director (Foundation) Date
Dept. Chair/Supervisor (University) Date College/School Dean or Vice President (University) Date
_____________________________________________________________ Grant Accountant (Foundation) Date This is not an employment contract, but is required in accordance with Additional Employment Policy G-02.1. October 2008

Auxiliary Additional Employment California State University, Fresno
October 2008 Policy No. G-02.1
Written Employment Agreements To provide adequate internal control over auxiliary resources, written employment agreements are required for employment of University employees at all auxiliaries. Grants and Contracts Current CSU and campus policies – Executive order 890 and the Policy on the Administration of Grant and Contract Activity (Academic Policy Manual, Section 501) – prevent the hiring of project directors, consultants and other project staff until the terms and conditions of employment, particularly salary, have been documented in a written agreement between the individual and the employing auxiliary. Guidance on the development and implementation of written employment agreements is provided below. Other Auxiliary Activities Written employment agreements will also be required for University employees involved in auxiliary projects other than grants and contracts (e.g. summer programs, Programs for Children, etc.). University employees must negotiate written employment agreements prior to commencing work on any auxiliary project, regardless of the type of employment or the amount of compensation. Written Employment Agreements 1. Employment agreements will exist between the compensating auxiliary and the University employee, but
must be approved by the employee’s supervisor and the appropriate Dean or Vice President. 2. Written employment agreements must indicate the number of hours contracted during the applicable time
period, the calendar year for 12-month employees and the academic year for 10-month and academic year employees. Written employment agreements must be obtained for each applicable period.
3. It is the responsibility of the employee and appropriate Dean or Vice President to negotiate compensation
and complete the written employment agreement prior to commencement of work. The requirement for written employment agreements as outlined herein apply to compensation earned after October 2008.
4. It is the responsibility of the employee to file the written employment agreement with the auxiliary prior to
requesting payment of compensation. 5. Auxiliaries will not compensate a University employee until such time as a properly approved written
employment agreement is filed with the auxiliary. 6. To ensure proper University oversight, Auxiliaries will prepare annual reports of compensation paid and
hours worked for all University employees.



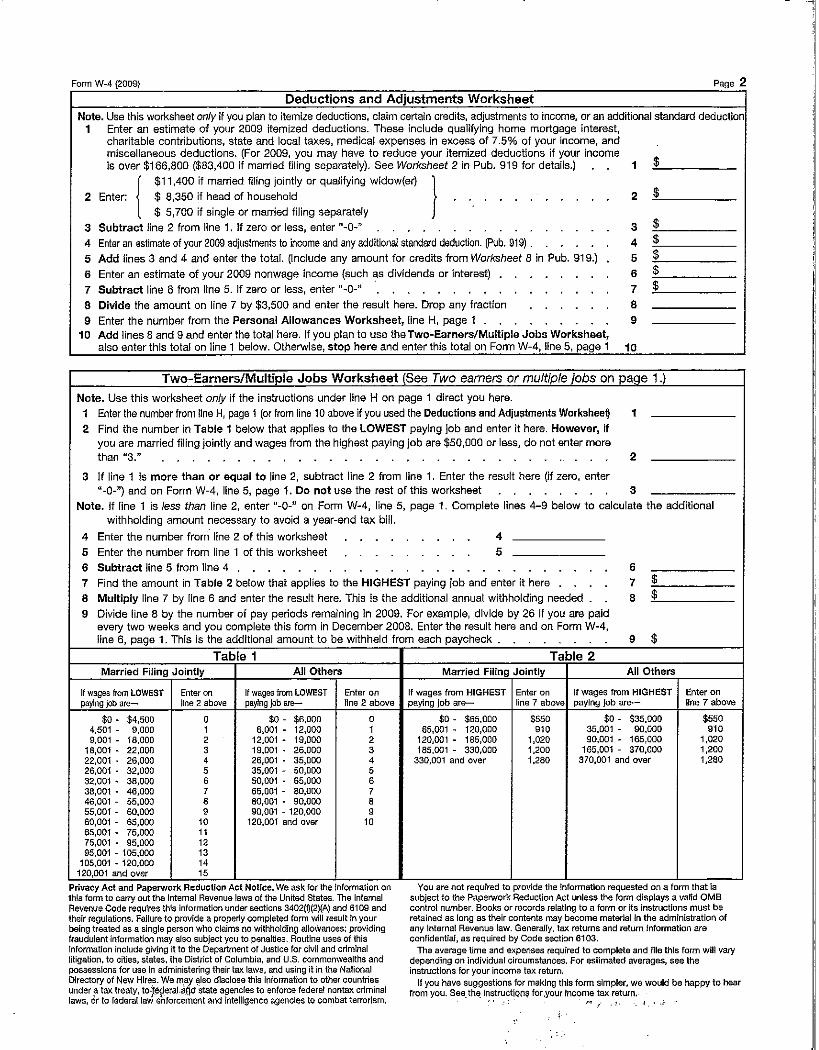

EMPLOYEE’S WITHHOLDING ALLOWANCE CERTIFICATE
1. Number of allowances for Regular Withholding Allowances, Worksheet A
Number of allowances from the Estimated Deductions, Worksheet B Total Number of Allowances (A + B) when using the California Withholding Schedules for 2007
OR
2. Additional amount of state income tax to be withheld each pay period (if employer agrees), Worksheet C
Under the penalties of perjury, I certify that the number of withholding allowances claimed on this certifi cate does not exceed the number to which I am entitled or, if claiming exemption from withholding, that I am entitled to claim the exempt status.
Signature Date
Employer’s Name and Address California Employer Account Number
cut here
Give the top portion of this page to your employer and keep the remainder for your records.
YOUR CALIFORNIA PERSONAL INCOME TAX MAY BE UNDERWITHHELD IF YOU DO NOT FILE THIS DE 4 FORM
IF YOU RELY ON THE FEDERAL W-4 FOR YOUR CALIFORNIA WITHHOLDING ALLOWANCES, YOUR CALIFORNIA STATE PERSONAL INCOME TAX MAY BE UNDERWITHHELD AND YOU MAY OWE MONEY AT THE END OF THE YEAR.
PURPOSE: This certifi cate, DE 4, is for California personal income tax withholding purposes only. The DE 4 is used to compute the amount of taxes to be withheld from your wages, by your employer, to accurately refl ect your state tax withholding obligation.
You should complete this form if either:
(1) You claim a different marital status, number of regular allowances, or different additional dollar amount to be withheld for California personal income tax withholding than you claim for federal income tax withholding or,
(2) You claim additional allowances for estimated deductions.
THIS FORM WILL NOT CHANGE YOUR FEDERAL WITHHOLDING ALLOWANCES.
The federal Form W-4 is applicable for California withholding purposes if you wish to claim the same marital status, number of regular allowances, and/or the same additional dollar amount to be withheld for state and federal purposes. However, federal tax brackets and withholding methods do not refl ect state personal income tax withholding tables. If you rely
City, State, and ZIP Code
Home Address (Number and Street or Rural Route)
Type or Print Your Full Name Your Social Security Number
Filing Status Withholding Allowances
SINGLE or MARRIED (with two or more incomes)
MARRIED (one income)
HEAD OF HOUSEHOLD
on the number of withholding allowances you claim on your Form W-4 withholding allowance certifi cate for your state income tax withholding, you may be signifi cantly underwithheld. This is particularly true if your household income is derived from more than one source.
CHECK YOUR WITHHOLDING: After your W-4 and/orDE 4 takes effect, compare the state income tax withheld with your estimated total annual tax. For state withholding, use the worksheets on this form, and for federal withholding use the Internal Revenue Service (IRS) Publication 919 or federal withholding calculations.
EXEMPTION FROM WITHHOLDING: If you wish to claim exempt, complete the federal Form W-4. You may only claim exempt from withholding California income tax if you did not owe any federal income tax last year and you do not expect to owe any federal income tax this year. The exemption automatically expires on February 15 of the next year. If you continue to qualify for the exempt fi ling status, a new Form W-4 designating EXEMPT must be submitted before February 15. If you are not having federal income tax withheld this year but expect to have a tax liability next year, the law requires you to give your employer a new Form W-4 by December 1.
This form can be used to manually compute your withholding allowances, or you can electronically compute them at www.taxes.ca.gov/de4.xls (Microsoft
Excel required).
DE 4 Rev. 33 (1-07) (INTERNET) Page 1 of 4 CU

IF YOU NEED MORE DETAILED INFORMATION, SEE THE INSTRUCTIONS THAT CAME WITH YOUR LAST CALIFORNIA INCOME TAX RETURN OR CALL THE FRANCHISE TAX BOARD.
IF YOU ARE CALLING FROM WITHIN THE UNITED STATES 1-800-852-5711 (voice) 1-800-822-6268 (TTY)
IF YOU ARE CALLING FROM OUTSIDE THE UNITED STATES (Not Toll Free) (916) 845-6500
The California Employer’s Guide (DE 44) provides the income tax withholding tables. This publication may be found on EDD’s Web site at www.edd.ca.gov/taxrep/taxform.htm. To assist you in calculating your tax liability, please visit the Franchise Tax Board’s Web site at: www.ftb.ca.gov/individuals/tax_table/index.asp.
NOTIFICATION: Your employer is required to send a copy of your DE 4 to the Franchise Tax Board (FTB) if it meets any of the following conditions:• You claim more than 10 withholding allowances• You claim exemption from state or federal income tax• You make major changes to DE 4, such as crossing out words or writing more than is asked• You admit that the DE 4 is false
IF THE IRS INSTRUCTS YOUR EMPLOYER TO WITHHOLD FEDERAL INCOME TAX BASED ON A CERTAIN WITHHOLDING STATUS, YOUR EMPLOYER IS REQUIRED TO USE THE SAME WITHHOLDING STATUS FOR STATE INCOME TAX WITHHOLDING IF YOUR WITHHOLDING ALLOWANCES FOR STATE PURPOSES MEET THE REQUIREMENTS LISTED UNDER “NOTIFICATION.” IF YOU FEEL THAT THE FEDERAL DETERMINATION IS NOT CORRECT FOR STATE WITHHOLDING PURPOSES, YOU MAY REQUEST A REVIEW.
To do so, write to: Franchise Tax Board W-4 Unit MS F-180 P.O. Box 2952 Sacramento CA 95812-2952
Your letter should contain the basis of your request for review. You will have the burden of showing the federal determination incorrect for state withholding purposes. The Franchise Tax Board (FTB) will limit its review to that issue. FTB will notify both you and your employer of its fi ndings. Your employer is then required to withhold state income tax as instructed by FTB. In the event FTB or IRS fi nds there is no reasonable basis for the number of withholding exemptions that you claimed on your W-4/DE 4, you may be subject to a penalty.
PENALTY: You may be fi ned $500 if you fi le, with no reasonable basis, a DE 4 that results in less tax being withheld than is properly allowable. In addition, criminal penalties apply for willfully supplying false or fraudulent information or failing to supply information requiring an increase in withholding. This is provided for by Section 19176 of the California Revenue and Taxation Code.
DE 4 Rev. 33 (1-07) (INTERNET) Page 2 of 4 CU

INSTRUCTIONS — 1 — ALLOWANCES*
When determining your withholding allowances, you must consider your personal situation:— Do you claim allowances for dependents or blindness?— Are you going to itemize your deductions?— Do you have more than one income coming into the household?
TWO-EARNER/TWO-JOBS: When earnings are derived from more than one source, underwithholding may occur. If you have a working spouse or more than one job, it is best to check the box “SINGLE or MARRIED (with two or more incomes).” Figure the total number of allowances you are entitled to claim on all jobs using only one DE 4 form. Claim allowances with one employer. Do not claim the same allowances with more than one employer. Your withholding will usually be most accurate when all allowances are claimed on the DE 4 or W-4 fi led for the highest paying job and zero allowances are claimed for the others.
MARRIED BUT NOT LIVING WITH YOUR SPOUSE: You may check the “Head of Household” marital status box if you meet all of the following tests:(1) Your spouse will not live with you at any time during the year;(2) You will furnish over half of the cost of maintaining a home
for the entire year for yourself and your child or stepchild who qualifi es as your dependent; and
(3) You will fi le a separate return for the year.
HEAD OF HOUSEHOLD: To qualify, you must be unmarried or legally separated from your spouse and pay more than 50% of the costs of maintaining a home for the entire year for yourself and your dependent(s) or other qualifying individuals. Cost of maintaining the home includes such items as rent, property insurance, property taxes, mortgage interest, repairs, utilities, and cost of food. It does not include the individual’s personal expenses or any amount which represents value of services performed by a member of the household of the taxpayer.
(A) Allowance for yourself — enter 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (A)
(B) Allowance for your spouse (if not separately claimed by your spouse) — enter 1 . . . . . . . . . . . . . . (B)
(C) Allowance for blindness — yourself — enter 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (C)
(D) Allowance for blindness — your spouse (if not separately claimed by your spouse) — enter 1 . . . . . . . (D)
(E) Allowance(s) for dependent(s) — do not include yourself or your spouse . . . . . . . . . . . . . . . . . . (E) E-1. Please enter the number of dependents for which you are claiming allowances: E-2. Please multiply the number entered in E-1 by 3 and enter on line E
(F) Total — add lines (A) through (E) above . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (F)
INSTRUCTIONS — 2 — ADDITIONAL WITHHOLDING ALLOWANCES
If you expect to itemize deductions on your California income tax return, you can claim additional withholding allowances. Use Worksheet B to determine whether your expected estimated deductions may entitle you to claim one or more additional withholding allowances. Use last year’s FTB 540 form as a model to calculate this year’s withholding amounts.
Do not include deferred compensation, qualifi ed pension payments or fl exible benefi ts, etc., that are deducted from your gross pay but are not taxed on this worksheet.
You may reduce the amount of tax withheld from your wages by claiming one additional withholding allowance for each $1,000, or fraction of $1,000, by which you expect your estimated deductions for the year to exceed your allowable standard deduction.
WORKSHEET B ESTIMATED DEDUCTIONS
WORKSHEET A REGULAR WITHHOLDING ALLOWANCES
1. Enter an estimate of your itemized deductions for California taxes for this tax year as listed in the schedules in the FTB 540 form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1. _______________________
2. Enter $6,820 if married fi ling joint, head of household, or qualifying widow(er) with dependent(s) or $3,410 if single or married fi ling separately . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . - 2. _______________________
3. Subtract line 2 from line 1, enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . = 3. _______________________
4. Enter an estimate of your adjustments to income (alimony payments, IRA deposits) . . . . . . . . . . . + 4. _______________________
5. Add line 4 to line 3, enter sum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . = 5. _______________________
6. Enter an estimate of your nonwage income (dividends, interest income, alimony receipts) . . . . . . . . - 6. _______________________ 7. If line 5 is greater than line 6 (if less, see below); Subtract line 6 from line 5, enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . = 7. _______________________
8. Divide the amount on line 7 by $1,000, round any fraction to the nearest whole number . . . . . . . . . 8. _______________________ Enter this number on line 1 of the DE 4. Complete Worksheet C, if needed.
9. If line 6 is greater than line 5; Enter amount from line 6 (nonwage income) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9. _______________________
10. Enter amount from line 5 (deductions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10. _______________________
11. Subtract line 10 from line 9, enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11. _______________________ Complete Worksheet C
*Due to recent legislation, beginning January 1, 2007, wages paid to registered domestic partners will be treated the same for state income tax pur-poses as wages paid to spouses for California personal income tax (PIT) withholding and PIT wages. This new law does not impact federal income tax law. A registered domestic partner means an individual partner in a domestic partner relationship within the meaning of Section 297 of the Family Code. For more information, please call our Taxpayer Assistance Center at 1-888-745-3886.
x 3 =
DE 4 Rev. 33 (1-07) (INTERNET) Page 3 of 4 CU
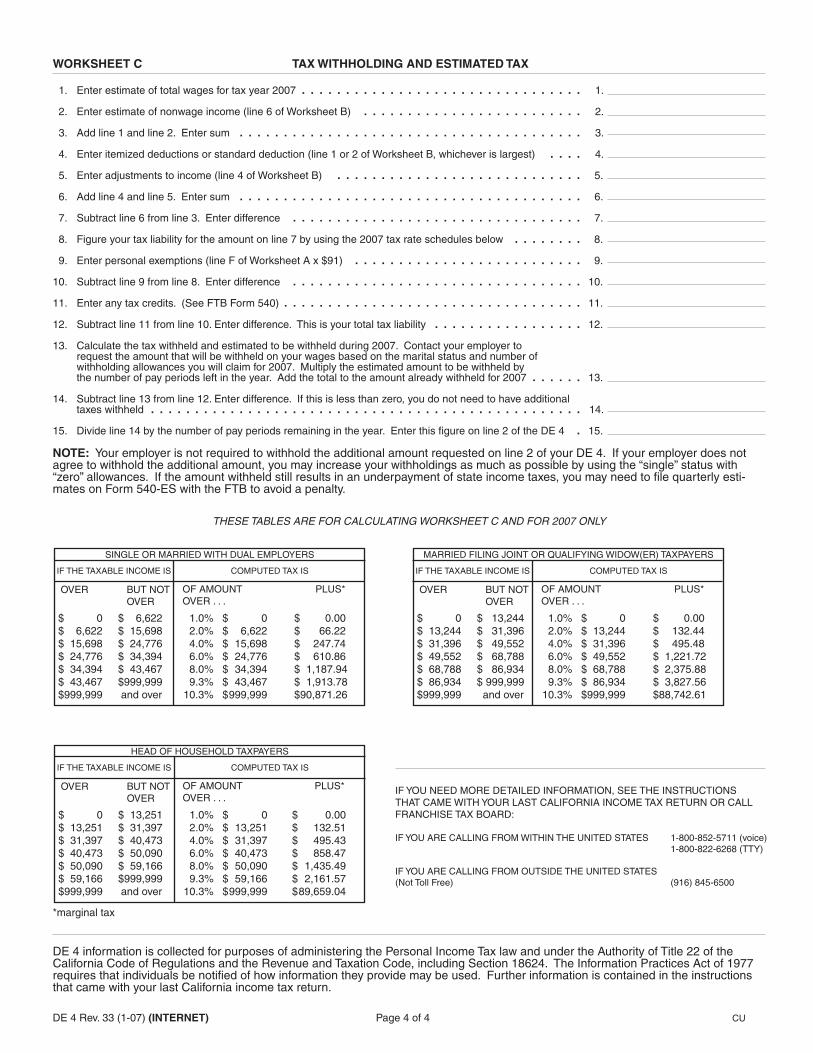
WORKSHEET C TAX WITHHOLDING AND ESTIMATED TAX
1. Enter estimate of total wages for tax year 2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1. 2. Enter estimate of nonwage income (line 6 of Worksheet B) . . . . . . . . . . . . . . . . . . . . . . . . . 2.
3. Add line 1 and line 2. Enter sum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.
4. Enter itemized deductions or standard deduction (line 1 or 2 of Worksheet B, whichever is largest) . . . . 4. 5. Enter adjustments to income (line 4 of Worksheet B) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. 6. Add line 4 and line 5. Enter sum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.
7. Subtract line 6 from line 3. Enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7. 8. Figure your tax liability for the amount on line 7 by using the 2007 tax rate schedules below . . . . . . . . 8.
9. Enter personal exemptions (line F of Worksheet A x $91) . . . . . . . . . . . . . . . . . . . . . . . . . . 9.
10. Subtract line 9 from line 8. Enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10.
11. Enter any tax credits. (See FTB Form 540) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.
12. Subtract line 11 from line 10. Enter difference. This is your total tax liability . . . . . . . . . . . . . . . . . 12.
13. Calculate the tax withheld and estimated to be withheld during 2007. Contact your employer to request the amount that will be withheld on your wages based on the marital status and number of withholding allowances you will claim for 2007. Multiply the estimated amount to be withheld by the number of pay periods left in the year. Add the total to the amount already withheld for 2007 . . . . . . 13.
14. Subtract line 13 from line 12. Enter difference. If this is less than zero, you do not need to have additional taxes withheld . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.
15. Divide line 14 by the number of pay periods remaining in the year. Enter this fi gure on line 2 of the DE 4 . 15.
NOTE: Your employer is not required to withhold the additional amount requested on line 2 of your DE 4. If your employer does not agree to withhold the additional amount, you may increase your withholdings as much as possible by using the “single” status with “zero” allowances. If the amount withheld still results in an underpayment of state income taxes, you may need to fi le quarterly esti-mates on Form 540-ES with the FTB to avoid a penalty.
THESE TABLES ARE FOR CALCULATING WORKSHEET C AND FOR 2007 ONLY
IF YOU NEED MORE DETAILED INFORMATION, SEE THE INSTRUCTIONS THAT CAME WITH YOUR LAST CALIFORNIA INCOME TAX RETURN OR CALL FRANCHISE TAX BOARD:
IF YOU ARE CALLING FROM WITHIN THE UNITED STATES 1-800-852-5711 (voice) 1-800-822-6268 (TTY)
IF YOU ARE CALLING FROM OUTSIDE THE UNITED STATES (Not Toll Free) (916) 845-6500
*marginal tax
DE 4 information is collected for purposes of administering the Personal Income Tax law and under the Authority of Title 22 of theCalifornia Code of Regulations and the Revenue and Taxation Code, including Section 18624. The Information Practices Act of 1977 requires that individuals be notifi ed of how information they provide may be used. Further information is contained in the instructionsthat came with your last California income tax return.
SINGLE OR MARRIED WITH DUAL EMPLOYERS
IF THE TAXABLE INCOME IS COMPUTED TAX IS
OVER BUT NOT OVER
OF AMOUNT PLUS* OVER . . . $ 0 $ 6,622
$ 6,622 $ 15,698$ 15,698 $ 24,776$ 24,776 $ 34,394$ 34,394 $ 43,467$ 43,467 $999,999$999,999 and over
1.0% $ 0 $ 0.00 2.0% $ 6,622 $ 66.22 4.0% $ 15,698 $ 247.74 6.0% $ 24,776 $ 610.86 8.0% $ 34,394 $ 1,187.94 9.3% $ 43,467 $ 1,913.78 10.3% $ 999,999 $90,871.26
MARRIED FILING JOINT OR QUALIFYING WIDOW(ER) TAXPAYERS
IF THE TAXABLE INCOME IS COMPUTED TAX IS
OVER BUT NOT OVER
OF AMOUNT PLUS* OVER . . . $ 0 $ 13,244
$ 13,244 $ 31,396$ 31,396 $ 49,552$ 49,552 $ 68,788$ 68,788 $ 86,934$ 86,934 $ 999,999$999,999 and over
1.0% $ 0 $ 0.00 2.0% $ 13,244 $ 132.44 4.0% $ 31,396 $ 495.48 6.0% $ 49,552 $ 1,221.72 8.0% $ 68,788 $ 2,375.88 9.3% $ 86,934 $ 3,827.56 10.3% $999,999 $ 88,742.61
HEAD OF HOUSEHOLD TAXPAYERS
IF THE TAXABLE INCOME IS COMPUTED TAX IS
OVER BUT NOT OVER
OF AMOUNT PLUS* OVER . . . $ 0 $ 13,251
$ 13,251 $ 31,397$ 31,397 $ 40,473$ 40,473 $ 50,090$ 50,090 $ 59,166$ 59,166 $999,999$999,999 and over
1.0% $ 0 $ 0.00 2.0% $ 13,251 $ 132.51 4.0% $ 31,397 $ 495.43 6.0% $ 40,473 $ 858.47 8.0% $ 50,090 $ 1,435.49 9.3% $ 59,166 $ 2,161.57 10.3% $ 999,999 $ 89,659.04
DE 4 Rev. 33 (1-07) (INTERNET) Page 4 of 4 CU

Department of Homeland Security U.S. Citizenship and Immigration Services
Form I-9, Employment Eligibility Verification
Anti-Discrimination Notice. It is illegal to discriminate against any individual (other than an alien not authorized to work in the U.S.) in hiring, discharging, or recruiting or referring for a fee because of that individual's national origin or citizenship status. It is illegal to discriminate against work eligible individuals. Employers CANNOT specify which document(s) they will accept from an employee. The refusal to hire an individual because the documents presented have a future expiration date may also constitute illegal discrimination.
All employees, citizens and noncitizens, hired after November 6, 1986 and working in the United States must complete a Form I-9.
OMB No. 1615-0047; Expires 06/30/09
Preparer/Translator Certification. The Preparer/Translator Certification must be completed if Section 1 is prepared by a person other than the employee. A preparer/translator may be used only when the employee is unable to complete Section 1 on his/her own. However, the employee must still sign Section 1 personally.
Form I-9 (Rev. 06/05/07) N
Please read all instructions carefully before completing this form. Instructions
When Should the Form I-9 Be Used?
What Is the Purpose of This Form?
The purpose of this form is to document that each new employee (both citizen and non-citizen) hired after November 6, 1986 is authorized to work in the United States.
Section 2, Employer: For the purpose of completing this form, the term "employer" means all employers including those recruiters and referrers for a fee who are agricultural associations, agricultural employers or farm labor contractors.
Filling Out the Form I-9
document(s) within three business days, they must present a receipt for the application of the document(s) within three business days and the actual document(s) within ninety (90) days. However, if employers hire individuals for a duration of less than three business days, Section 2 must be completed at the time employment begins. Employers must record:
Section 1, Employee: This part of the form must be completed at the time of hire, which is the actual beginning of employment. Providing the Social Security number is voluntary, except for employees hired by employers participating in the USCIS Electronic Employment Eligibility Verification Program (E-Verify). The employer is responsible for ensuring that Section 1 is timely and properly completed.
1. Document title;2. Issuing authority;3. Document number;4. Expiration date, if any; and 5. The date employment begins.
Employers must sign and date the certification. Employees must present original documents. Employers may, but are not required to, photocopy the document(s) presented. These photocopies may only be used for the verification process and must be retained with the Form I-9. However, employers are still responsible for completing and retaining the Form I-9.
Employers must complete Section 2 by examining evidence of identity and employment eligibility within three (3) business days of the date employment begins. If employees are authorized to work, but are unable to present the required
Section 3, Updating and Reverification: Employers must complete Section 3 when updating and/or reverifying the Form I-9. Employers must reverify employment eligibility of their employees on or before the expiration date recorded in Section 1. Employers CANNOT specify which document(s) they will accept from an employee.
B. If an employee is rehired within three (3) years of the date this form was originally completed and the employee is still eligible to be employed on the same basis as previously indicated on this form (updating), complete Block B and the signature block.
C. If an employee is rehired within three (3) years of the date this form was originally completed and the employee's work authorization has expired or if a current employee's work authorization is about to expire (reverification), complete Block B and:
A. If an employee's name has changed at the time this form is being updated/reverified, complete Block A.
1. Examine any document that reflects that the employee is authorized to work in the U.S. (see List A or C);
2. Record the document title, document number and expiration date (if any) in Block C, and
3. Complete the signature block.

EMPLOYERS MUST RETAIN COMPLETED FORM I-9 PLEASE DO NOT MAIL COMPLETED FORM I-9 TO ICE OR USCIS
Form I-9 (Rev. 06/05/07) N Page 2
To order USCIS forms, call our toll-free number at 1-800-870- 3676. Individuals can also get USCIS forms and information on immigration laws, regulations and procedures by telephoning our National Customer Service Center at 1-800- 375-5283 or visiting our internet website at www.uscis.gov.
USCIS Forms and Information
What Is the Filing Fee?
There is no associated filing fee for completing the Form I-9. This form is not filed with USCIS or any government agency. The Form I-9 must be retained by the employer and made available for inspection by U.S. Government officials as specified in the Privacy Act Notice below.
The authority for collecting this information is the Immigration Reform and Control Act of 1986, Pub. L. 99-603 (8 USC 1324a).
Privacy Act Notice
This information is for employers to verify the eligibility of individuals for employment to preclude the unlawful hiring, or recruiting or referring for a fee, of aliens who are not authorized to work in the United States.
This information will be used by employers as a record of their basis for determining eligibility of an employee to work in the United States. The form will be kept by the employer and made available for inspection by officials of U.S. Immigration and Customs Enforcement, Department of Labor and Office of Special Counsel for Immigration Related Unfair Employment Practices.
Submission of the information required in this form is voluntary. However, an individual may not begin employment unless this form is completed, since employers are subject to civil or criminal penalties if they do not comply with the Immigration Reform and Control Act of 1986.
We try to create forms and instructions that are accurate, can be easily understood and which impose the least possible burden on you to provide us with information. Often this is difficult because some immigration laws are very complex. Accordingly, the reporting burden for this collection of information is computed as follows: 1) learning about this form, and completing the form, 9 minutes; 2) assembling and filing (recordkeeping) the form, 3 minutes, for an average of 12 minutes per response. If you have comments regarding the accuracy of this burden estimate, or suggestions for making this form simpler, you can write to: U.S. Citizenship and Immigration Services, Regulatory Management Division, 111 Massachusetts Avenue, N.W., 3rd Floor, Suite 3008, Washington, DC 20529. OMB No. 1615-0047.
Paperwork Reduction Act
A blank Form I-9 may be reproduced, provided both sides are copied. The Instructions must be available to all employees completing this form. Employers must retain completed Forms I-9 for three (3) years after the date of hire or one (1) year after the date employment ends, whichever is later.
Photocopying and Retaining the Form I-9
The Form I-9 may be signed and retained electronically, as authorized in Department of Homeland Security regulations at 8 CFR 274a.2.§

Department of Homeland Security U.S. Citizenship and Immigration Services
Form I-9, Employment Eligibility Verification
OMB No. 1615-0047; Expires 06/30/09
Please read instructions carefully before completing this form. The instructions must be available during completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work eligible individuals. Employers CANNOT specify which document(s) they will accept from an employee. The refusal to hire an individual because the documents have a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Verification. To be completed and signed by employee at the time employment begins.Print Name: Last First Middle Initial Maiden Name
Address (Street Name and Number) Apt. # Date of Birth (month/day/year)
StateCity Zip Code Social Security #
A lawful permanent resident (Alien #) AA citizen or national of the United States I am aware that federal law provides for
imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
An alien authorized to work until
(Alien # or Admission #)Employee's Signature Date (month/day/year)
Preparer and/or Translator Certification. (To be completed and signed if Section 1 is prepared by a person other than the employee.) I attest, under penalty of perjury, that I have assisted in the completion of this form and that to the best of my knowledge the information is true and correct.
Address (Street Name and Number, City, State, Zip Code)
Print NamePreparer's/Translator's Signature
Date (month/day/year)
Section 2. Employer Review and Verification. To be completed and signed by employer. Examine one document from List A OR examine one document from List B and one from List C, as listed on the reverse of this form, and record the title, number and expiration date, if any, of the document(s).
ANDList B List CORList ADocument title:
Issuing authority:
Document #:
Expiration Date (if any):Document #:
Expiration Date (if any):
and that to the best of my knowledge the employee is eligible to work in the United States. (State(month/day/year)employment agencies may omit the date the employee began employment.)
CERTIFICATION - I attest, under penalty of perjury, that I have examined the document(s) presented by the above-named employee, that the above-listed document(s) appear to be genuine and to relate to the employee named, that the employee began employment on
Print Name TitleSignature of Employer or Authorized Representative
Date (month/day/year)Business or Organization Name and Address (Street Name and Number, City, State, Zip Code)
B. Date of Rehire (month/day/year) (if applicable)A. New Name (if applicable)
C. If employee's previous grant of work authorization has expired, provide the information below for the document that establishes current employment eligibility.
Document #: Expiration Date (if any):Document Title:
Section 3. Updating and Reverification. To be completed and signed by employer.
l attest, under penalty of perjury, that to the best of my knowledge, this employee is eligible to work in the United States, and if the employee presented document(s), the document(s) l have examined appear to be genuine and to relate to the individual.
Date (month/day/year)Signature of Employer or Authorized Representative
Form I-9 (Rev. 06/05/07) N
I attest, under penalty of perjury, that I am (check one of the following):

For persons under age 18 who are unable to present a document listed above:
LISTS OF ACCEPTABLE DOCUMENTS
LIST A LIST B LIST C
2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551)
7. Unexpired employment authorization document issued by DHS (other than those listed under List A)
1. Driver's license or ID card issued by a state or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color and address
1. U.S. Social Security card issued by the Social Security Administration (other than a card stating it is not valid for employment)
9. Driver's license issued by a Canadian government authority
1. U.S. Passport (unexpired or expired)
2. Certification of Birth Abroad issued by the Department of State (Form FS-545 or Form DS-1350)
3. An unexpired foreign passport with a temporary I-551 stamp
4. An unexpired Employment Authorization Document that contains a photograph
(Form I-766, I-688, I-688A, I-688B)
3. Original or certified copy of a birth certificate issued by a state, county, municipal authority or outlying possession of the United States bearing an official seal
3. School ID card with a photograph
5. An unexpired foreign passport with an unexpired Arrival-Departure Record, Form I-94, bearing the same name as the passport and containing an endorsement of the alien's nonimmigrant status, if that status authorizes the alien to work for the employer
6. Military dependent's ID card
4. Native American tribal document
7. U.S. Coast Guard Merchant Mariner Card
5. U.S. Citizen ID Card (Form I-197)
8. Native American tribal document
6. ID Card for use of Resident Citizen in the United States (Form I-179)
10. School record or report card
11. Clinic, doctor or hospital record
12. Day-care or nursery school record
Illustrations of many of these documents appear in Part 8 of the Handbook for Employers (M-274)
2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color and address
Form I-9 (Rev. 06/05/07) N Page 2
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Both Identity and Employment
Eligibility
Documents that Establish Identity
Documents that Establish Employment Eligibility
OR AND