Embed Size (px)
Citation preview

Hip Fracture and the Orthogeriatrician
Antony Johansen
The geriatric orthopaedic unit Irvine and Devas. J Bone Joint Surgery 1963; 49-B:186-7
Management of the fractured neck of femur in the
elderly female: a joint approach Clarke and Wainwright. Gerontology Clinics 1966; 8:321-6
“the surgical procedure must never be
considered to be the whole treatment
but merely an incident in the general
rehabilitation of the patient”
BMJ 1974; 1:190-2

Effectiveness of geriatric rehabilitation after proximal
femur fracture in the elderly
Kennie et al. BMJ 1988; 297:1083-6
GP run, geriatrician led orthopaedic rehab. ward
- earlier discharge, better mortality and independence
Prospective randomised study of an orthopaedic geriatric in-
patient service
Gilchrist et al. BMJ 1988; 297:1116-1118
Surgeon run rehab. ward, with weekly combined OG round
- better care of medical conditions, but no effect on outcome

Geriatric rehabilitation following fractures in
older people: a systematic review Cameron et al. NHS HTA 2000;4:2
Specific therapy, nursing, medical input
Miscellaneous hospital programmes
Clinical pathways
Early supported discharge
Prospective payment systems
Geriatric orthopaedic rehabilitation unit
Hip fracture programme

Gateway reference: 15618 1
Payment by Results Guidance for 2011-12

Orthogeriatric Rehabilitation – Hospital-based coordinated MDT care for hip fracture patients 7 Randomised controlled trials Gilchrist 1988 (Scotland) Post-surgical – Off-site orthopaedic vs. off-site orthogeriatric ward Huusko 2002 (Finland) Post-surgical – Acute hospital geriatric rehab. (MARU) vs. off-site local health centre hospital Kennie 1988 (Scotland) Post-surgical – acute orthopaedic ward vs. move to off-site geriatrician-led GP-run orthop. ward Naglie 2002 (Canada) Post-surgical – Acute site routine post-op. care vs. acute site intensive multidisciplinary rehab. Stenvall 2007 (Sweden) Post-op. – care in conventional orthop. ward vs. specific intervention programme in geriatric ward Fordham 1986 OG rehab vs. controls Galvard 1995 (Sweden) OG rehabilitation trial Cohort studies Hempsall 1990, Fox 1993, Fordham 1995 Hip Fracture Programme – Orthogeriatrician-led peri-op. care leading into MDT rehabilitation 5 Randomised controlled trials Swanson 1998 (Australia) Early intervention – standard orthopaedic care vs. HFP Vidan 2005 (Spain)
Acute phase HFP vs. standard care Shyu 2008 (Taiwan) MDT intervention programme for hip fracture vs. usual care Marcantonio 2001 (USA) Acute setting HFP vs. controls (this is definitely an HFP, even though outcome focuses on delirium) Cameron 1993/4 (Australia) Acute accelerated hip fracture rehabilitation programme Case controlled trial Jette 1987 Cohort studies Zuckerman 1992, Elliot 1996, Miura 2009, Fisher 2006 Farnworth 1994 (Antonia's economic analysis, an Australian observational study)
Orthogeriatric Rehabilitation – Hospital-based coordinated MDT care for hip fracture patients 7 Randomised controlled trials Gilchrist 1988 (Scotland) Post-surgical – Off-site orthopaedic vs. off-site orthogeriatric ward Huusko 2002 (Finland) Post-surgical – Acute hospital geriatric rehab. (MARU) vs. off-site local health centre hospital Kennie 1988 (Scotland) Post-surgical – acute orthopaedic ward vs. move to off-site geriatrician-led GP-run orthop. ward Naglie 2002 (Canada) Post-surgical – Acute site routine post-op. care vs. acute site intensive multidisciplinary rehab. Stenvall 2007 (Sweden) Post-op. – care in conventional orthop. ward vs. specific intervention programme in geriatric ward Fordham 1986 OG rehab vs. controls Galvard 1995 (Sweden) OG rehabilitation trial Cohort studies Hempsall 1990, Fox 1993, Fordham 1995 Hip Fracture Programme – Orthogeriatrician-led peri-op. care leading into MDT rehabilitation 5 Randomised controlled trials Swanson 1998 (Australia) Early intervention – standard orthopaedic care vs. HFP Vidan 2005 (Spain)
Acute phase HFP vs. standard care Shyu 2008 (Taiwan) MDT intervention programme for hip fracture vs. usual care Marcantonio 2001 (USA) Acute setting HFP vs. controls (this is definitely an HFP, even though outcome focuses on delirium) Cameron 1993/4 (Australia) Acute accelerated hip fracture rehabilitation programme Case controlled trial Jette 1987 Cohort studies Zuckerman 1992, Elliot 1996, Miura 2009, Fisher 2006 Farnworth 1994 (Antonia's economic analysis, an Australian observational study)



564! APPENDIX!H!
Table!98:!Incremental!resource!use!for!GORU/MARU!programme!versus!usual!care!
Staff!resources!! Incremental!resources!
used,!based!on!a!LOS!of!
32.88!days!!
Source! Unit!cost!(source:!
PSSRU!2008/09),!
£!per!hour!
Incremental!
cost!
Orthogeriatrician!! Two!consultant!ward!
rounds!(0.25/hour!per!
patient!each)!and!one!
weekly!conference!
(0.25/hour!=!0.75!hour!
per!week!per!patient!!
0.75*4.6!weeks!=!3.45!
hours!per!patients!!
Kennie!et!al!
(1988)176!
£108! £372.6!
Physiotherapist!! 8.5!hours!per!patient!!! Naglie!2002222! £23! £195.5!
Occupational!
therapist!!
5!hr/patient!!!! GDG!adjustment!
from!the!7.5!
hr/pt!reported!in!
Naglie222!!
£23! £115!
Nurse!! Initial!assessment!
within!72!hours!(0.5!
hour!per!patient)!and!
twice!weekly!
assessment!afterwards!
(0.25*2)/hour!per!
patient!!!
0.5+0.5*4.6!weeks=!2.8!
hours!per!patient!
Naglie!2002222! Nurse!team!
leader:!£27!
Nurse!day!ward:!
£21!
£75.6!
£58.8!
Social!worker! b0.4!hour!per!patient!!! Naglie!2002222! £29!(from!
community!data)!
b£11.6!
Dietician! b0.4!hour!per!patient!!! Naglie!2002222! £23/! b£9.2!
Total!incremental!cost!for!GORU/MARU!over!usual!care:!!
!
£721!(with!
generic!
nurse,!Band!
5);!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
£738!(with!
team!leader!
nurse,!Band!
6)!
!
!
!

NICE economic model – HFP vs. usual care

Guideline
Summary
Hip Fracture
CG124
NICE 2011

Yes – but what does an orthogeriatrician actually do?
Patients with suspected hip fracture
Assessment
Proforma
Hip Fracture Service
University Hospital of Wales
Medical history
□ MI/angina
□ Heart failure
□ Pacemaker
□ Defibrillator
□ HT
□ DM
□ Asthma/COPD
□ DVT/PE
□ Anticoagulated
□ Jaundice
□ Stroke/TIA
□ Epilepsy
□ Smoking
□ Alcohol/addiction
□ Previous cancer
Details:
Trauma consultant : Date: Time:
Admitting doctor: Bleep number:
Presenting complaint
Events leading to any fall:
□ Clear story of trip, slip or accident
□ Palpitations, chest pain, SOB
□ Aura, fit, tongue biting, incontinence
□ Dizzy, light headed, pale, sweaty
□ Other associated medical symptoms
□ Unexplained loss of consciousness
Details:
Social circumstances
Admitted from: Home support: Usual mobility: Usual walking aids:
□ house □ living alone □ able to do own shopping □ none
□ bungalow □ living with someone □ able to get out of home □ one aid (stick, crutch)
□ downstairs flat □ living with carer -but unable to shop □ two aids
□ upstairs flat □ home care package □ home bound □ frame
□ residential home □ institutional care □ wheel-chair/bed-bound
□ nursing home □ no fixed abode
□ hospital
Medication
Drug allergies:
Examination
Temperature Pulse
BP Respiratory rate Oxygen saturation BM
Mental state assessment
□ Known dementia
□ Recent memory decline
□ Previous confusion in hospital
Details:
Mental test scores are the most powerful predictors of outcome following hip fracture, and the early assessment of a patient’s
cognitive state is key to anticipating and preventing the onset of delirium.
Abbreviated Mental Test Score Result ………/ 10
Correct Incorrect 8-10 is normal
□ □ What is your age? 0-7 is abnormal
□ □ What is the time (to the nearest hour)
Can you repeat this address “42 West Street”, and I will ask you to remember it at the end of the test
□ □ What year is it?
□ □ What is the name of the place we are in now?
□ □ Recognition of two people (doctor, nurse etc.)
□ □ What is your date of birth (day and month)
□ □ Give the year in which the First World War began
□ □ Give the name of the present monarch
□ □ Count back from 20 to 0
□ □ Can you remember the address I gave you earlier?
Clock Face Drawing (see back page of assessment form) is an alternative
This is a quick, simple test - highly sensitive in identifying cognitive problems, and a validated predictor of hip fracture outcome
Systematic scoring is not needed - 'if it looks right, it is right', and abnormalities speak for themselves
Diagnosis and management plan
Fracture: Underlying cause: Planned procedure:
□ undisplaced intracapsular □ none / osteoporosis □ screws
□ displaced intracapsular □ malignant 20
□ DHS
□ basocervical □ malignant 10 □ nail
□ 2-part trochanteric □ bone-cyst □ hemiarthroplasty
□ multi-part trochanteric □ Paget’s disease □ THR
□ sub-trochanteric □ Atypical/bisphosphonate □ other ...…..................………..
□ peri-prosthetic □ other ........................…..
Hip Fracture Service - Patient assessment document - Johansen, 2012
Clock Face Drawing
Ask the patient to: "Fill in the numbers of this clock face, and draw in the hands of the clock pointing to 3 o’clock”
Pre-operative investigations
All patients If indicated
Result Sent Result
Hb
WCC
Platelets
INR □ If taking warfarin
Clotting screen □
If liver disease or
clinical concern
Na+
K+
Urea
Creatinine
Liver function tests □
Arterial gases
pH □
pO2 □
pCO2 □ BE □
If severe chronic
airways disease, or
clinical pointer to
respiratory failure
Ca2+
Albumin
Sent
Group & save □
X-match …..... units (see following pages) □
Blood culture □
Sputum culture □
MSU □
MRSA screen □
If concern over
possible infection Pelvis and lateral hip X-ray □
Chest X-ray (if aged >65) □
ECG □ Glucose □ If possible diabetes
Senior review or post-take ward round

Hip Fracture Assessment pro forma – initial management protocols – 2012

Hip Fracture Assessment pro forma – initial management protocols – 2012

Hip Fracture Assessment pro forma – initial management protocols – 2012

Hip Fracture Assessment pro forma – initial management protocols – 2012

Yes – but what does an orthogeriatrician actually do?

R=0.59, p<0.0001
Frailty Index – integrating the results of Comprehensive Geriatric
Assessment to predict hip fracture outcome
Krishnan, Johansen et al. Age and Ageing (in press)

Reducing delirium after hip fracture: a randomised trial
Marcantonio et al. JAGS 2001; 49:516–522
126 consenting patients with hip
fracture aged >65 (mean 79) years
Randomized to ‘usual care’, or
Geriatrics consultation
- pre-op. or <24 hours post-op.
- plus daily geriatrician visits
Offered a mean of 10 management
suggestions per patient
- 77% adherence achieved

1. Adequate CNS oxygen delivery:
Supplemental oxygen to keep saturation >90%, preferably >95%
Treatment to raise systolic BP >2/3 baseline or >90 mmHg
Transfusion to keep haematocrit >30%
2. Fluid/electrolyte balance:
Treatment to restore normal Na+, K+, Glucose
Treat fluid overload or dehydration detected by examination or blood tests
3. Treatment of severe pain:
Regular paracetamol (1g qds)
Early-stage break-through pain: low-dose subcutaneous morphine
Late-stage break-through pain: oxycodone as needed
4. Elimination of unnecessary medications:
Discontinue/minimize benzodiazepines, anticholinergics, antihistamines
Eliminate drug interactions, adverse effects, modify drugs accordingly
Eliminate medication redundancies

5. Regulation of bowel/bladder function:
Bowel movement by post-op. day 2 and every 48 hours
Urinary catheter out by post-op. day 2, screen for retention/incontinence
Skin care program for patients with established incontinence
6. Adequate nutritional intake:
Dentures used properly, proper positioning for meals, assist as needed
Supplements: 1 can Ensure (3 cans Ensure for poor oral intake)
If unable to take food orally, feed via temporary NGT
7. Early mobilization and rehabilitation:
Out of bed on post-op. day 1, and for several hours daily
Mobilise with nursing staff as tolerated, such as to bathroom
Daily physiotherapy, with OT if needed

8. Prevention, early detection, and treatment of major complications:
MI/ischemia - ECG, cardiac enzymes if needed
SVT/AF - rate control, U&E adjustments, anticoagulation
Pneumonia/COPD - screening, treatment, including chest therapy
PE - appropriate anticoagulation
Screening for and treat UTI
9. Appropriate environmental stimuli:
Appropriate use of glasses and hearing aids
Provision of clock and calendar
If available, use of radio, tape recorder, and soft lighting
10. Treatment of agitated delirium:
Appropriate diagnostic workup/management
Relieve agitation - calm reassurance, family presence, and/or sitter
- if absolutely necessary, low-dose haloperidol/lorazepam

Controls CGA
n Delirium
64
50%
62
32%
*
Severe delirium 29% 12% *
Duration (days) 3.1 2.9
LOS (days) 5 5
Discharge home 12% 8%
Reducing delirium after hip fracture: a randomized trial
Marcantonio et al. JAGS 2001; 49:516–522

OK – so how are orthogeriatricians actually doing?

Wales
Performance data for individual hospitals
compared with Wales and Overall figures

Surgery in 48 hours Excludes patients who were: - in hospital pre-fracture - died before 48 hours - managed conservatively - medically unfit at 48 hours

Received operation before 48 hours (%)
0 10 20 30 40 50 60 70 80 90 100
Aberystwyth
Rhyl
Bangor
Swansea
Abergavenny
Llantrisant
Cardiff
Wrexham
Carmarthen
Haverford West
Wales
UK

Web-site data on time to theatre – UHW
0
10
20
30
40
50
60
70
80
90
100
Monthly admissions
Mean hours to operation
Linear (Mean hours to operation)

Pre-operative assessment Best Practice Tariff requires assessment by: - geriatrician or physician - grade ST3 or above

Pre-operative geriatrician assessment (%)
0 20 40 60 80 100
Aberystwyth
Rhyl
Bangor
Swansea
Abergave…
Llantrisant
Cardiff
Wrexham
Carmarthen
Haverford…
Wales
UK
Orthogeriatrician
Other assessment

Network of Orthogeriatrics in Wales (NOW)
Survey of existing hip fracture services – December 2012
Orthogeriatrician Majority of hip fracture patients will be offered: NHFD
Consultant in post Pre-op. OG assessment OG-led rehabilitation Secondary prevention 2012 data reported
Abergavenny
Aberystwyth
Bangor
Bridgend
Cardiff
Carmarthen
Haverford West
Llantrisant
Merthyr
Newport
Rhyl
Swansea
Wrexham

Network of Orthogeriatrics in Wales (NOW)
Survey of existing hip fracture services – December 2012
0 2 4 6 8 10 12 14
Abergavenny
Aberystwyth
Bangor
Bridgend
Cardiff
Carmarthen
Haverford West
Llantrisant
Merthyr
Newport
Rhyl
Swansea
Wrexham
Orthogeriatrician sessions
Hip # admissions per week
Hours per hip # patient
0 2 4 6 8 10 12 14
Abergavenny
Aberystwyth
Bangor
Bridgend
Cardiff
Carmarthen
Haverford West
Llantrisant
Merthyr
Newport
Rhyl
Swansea
Wrexham
Orthogeriatrician sessions
Hip # admissions per week
Hours per hip # patient
0 2 4 6 8 10 12 14
Abergavenny
Aberystwyth
Bangor
Bridgend
Cardiff
Carmarthen
Haverford West
Llantrisant
Merthyr
Newport
Rhyl
Swansea
Wrexham
Orthogeriatrician sessions
Hip # admissions per week
Hours per hip # patient

Expansion in OG provision – NHFD Facilities Audit 2012-13
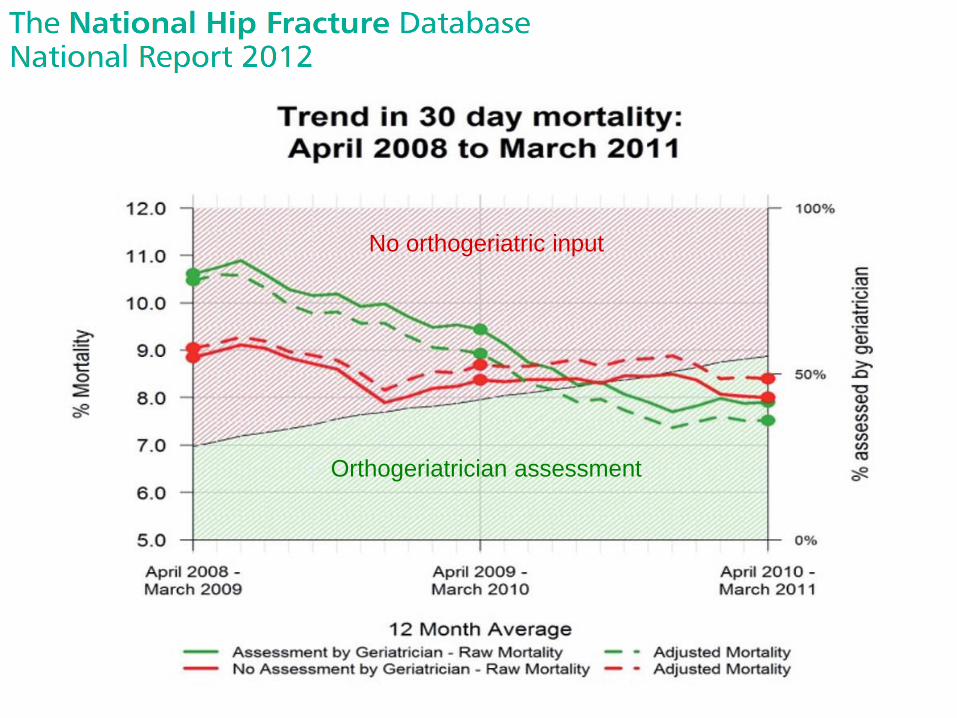
No orthogeriatric input
Orthogeriatrician assessment

NICE Quality Standards – QS16

NICE economic model – room for improvement

QS16 – focus for an NHFD Sprint Audit
- Jointly agreed protocols from admission into EU
- Acute ward with continuity of orthogeriatrician-led MDT care
- Documentation of goals and early discharge planning
- Physio day 1 post-op., then daily mobilisation by physio/nurse
- Named clinician from each speciality leading within the HFP
- Mortality, LOS, and adverse events monitored in HFP meetings
- Follow-up data to show HFP-team influence over IC rehab.






























