Embed Size (px)
Citation preview
COPYRIGHT HIMAA 2021
D R E D A H E A R D
HIMAA PROFESSIONAL DEVELOPMENT WEBINARS CDI SERIES /2
COPYRIGHT HIMAA 2021 Health Information Management Association of AustraliaSlide No. 2
CDI Supporting Engagement & Quality through Standards AlignmentNSQHS, Good Medical Practice, Nursing & Allied Health Professional Practice Guidelines

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia
Clinicians practice good documentation within all record types
Slide No. 3
Dimensions of good documentation
• Compliant & CompleteC• Accessible & AccurateA• ReadableR•EnduringE
CARE developed by Bucknall & Hutchinson 2017, recommended by the NSQHS at https://www.safetyandquality.gov.au/standards/nsqhs-standards/communicating-safety-standard/documentation-information

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 4
Standards, policies ,
procedures or guidelines
Standards, policies and procedures
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 5
Interaction & Unit or
Specialty
Standards, policies ,
procedures or guidelines
So why do documentation practice vary?

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 6
Interaction & Unit or
Specialty
Documenters Responsibility
Standards, policies ,
procedures or guidelines
So why do documentation practice vary?

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 7
Interaction & Unit or
Specialty
Type of Record
Documenters Responsibility
Standards, policies ,
procedures or guidelines
So why do documentation practice vary?
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 8
Interaction & Unit or
Specialty
Type of Record
Documenters Responsibility
Standards, policies ,
procedures or guidelines
the nature & use of the document
So why do documentation practice vary?

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 9
Interaction & Unit or
Specialty
Type of Record
Documenters Responsibility
Standards, policies ,
procedures or guidelines
the nature & use of the document
State Reporting
So why do documentation practice vary?
COPYRIGHT HIMAA 2021
Great! But what has that got to do with CDI?
10
EDUCATION
Ongoing Education Schedule – MO, CC, CDS Webinars, Workshops,
Team Collaboration, Education Delivery to Complement Clinician workflow
HIMAA Articles & Hospital News & Service Linkedin Page
Supports Program Maturity
Operational Strategy:Embedding Change
COPYRIGHT HIMAA 2021
Great! But what has that got to do with CDI?
11
EDUCATION
Orientation
COPYRIGHT HIMAA 2021
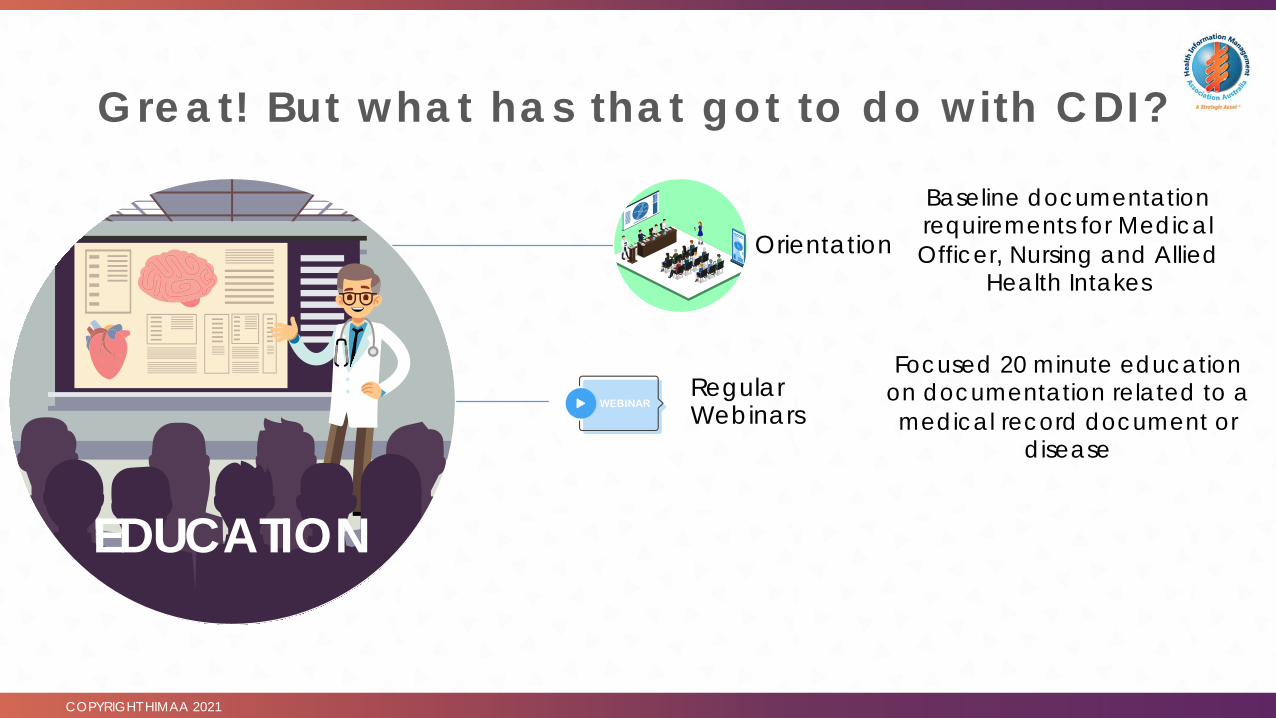
Great! But what has that got to do with CDI?
12
EDUCATION
Orientation
Regular Webinars
Baseline documentation requirements for Medical Officer, Nursing and Allied
Health Intakes
Focused 20 minute education on documentation related to a medical record document or
disease
COPYRIGHT HIMAA 2021
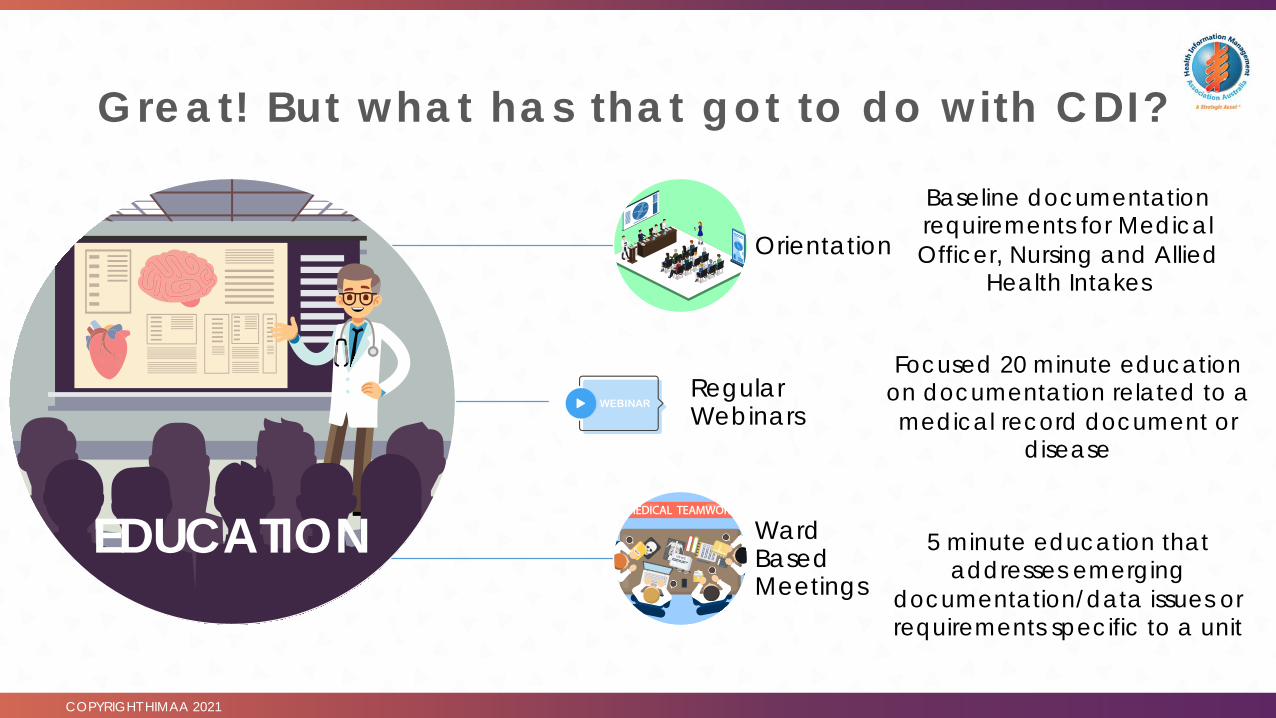
Great! But what has that got to do with CDI?
13
EDUCATION
Orientation
Regular Webinars
Ward Based Meetings
Baseline documentation requirements for Medical Officer, Nursing and Allied
Health Intakes
Focused 20 minute education on documentation related to a medical record document or
disease
5 minute education that addresses emerging
documentation/data issues or requirements specific to a unit

COPYRIGHT HIMAA 2021
Connected Conversations
14
Connected Conversations• CR - Conversation Relevance• CO – Clarity of Offer• CA – Commitment and Ask

COPYRIGHT HIMAA 2021
Standards, Guidel ines: Connected Conversat ions
15
CONVERSATION RELEVANCE Relevance to their role/position

COPYRIGHT HIMAA 2021
Standards, Guidel ines: Connected Conversat ions
16
CLARITY OFFERWhat’s in it for them? What are you giving them in exchange
for support?

COPYRIGHT HIMAA 2021
Standards, Guidel ines: Connected Conversat ions
17
COMMITMENT ASKBe specific about
what you are asking. The ask must be role
related and achievable
.

COPYRIGHT HIMAA 2021
The message in your conversat ion needs to be meaningful - don’t just R inse & Repeat!
18
‘Its not written down, it didn’t
happen…’
Legal record of care and clinician
protection

COPYRIGHT HIMAA 2021
Rinse, Repeat: R isk los ing your audience
19
Legal Record of CareClinician Protection
Beware of losing your audience by
regurgitating the message in the same
way every time!

COPYRIGHT HIMAA 2021
Keep your audience with you – Pivot the message on the Standard or Guidel ine!
20
Beware of losing your audience by
regurgitating the message in the same
way every time!
Understanding the documentation elements of Standards, Procedures and Professional Practice Guidelines gives context.
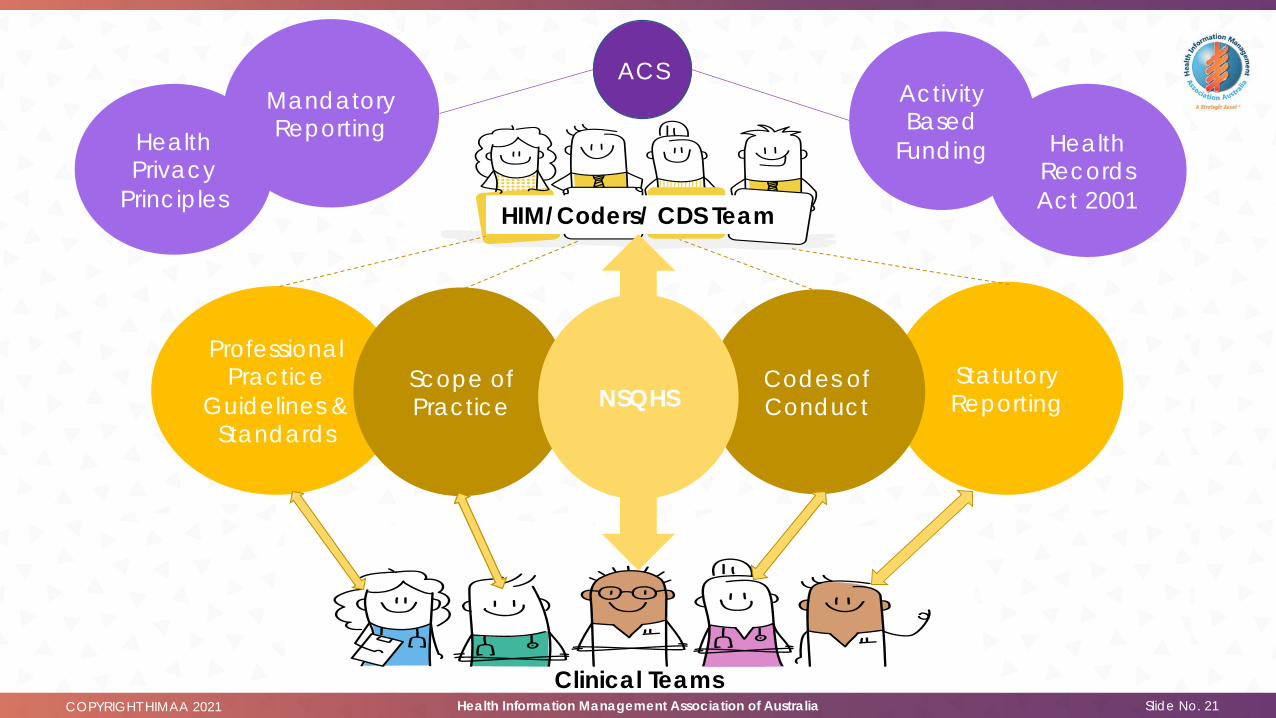
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 21
Health Records Act 2001
Health Privacy
Principles
Professional Practice
Guidelines & Standards
Statutory Reporting
Codes of Conduct
Scope of Practice
Clinical Teams
HIM/Coders/ CDS Team
ACS
NSQHS
Mandatory Reporting
Activity Based
Funding

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 22
yourself with clinician standards/guidelinesFamiliarise
to your clinical interactions, clinical workflows, unit documentation needs, document type, condition specificity
Map
to ACS documentation requirements where appropriateRelate
standard references in education – this evidences embedding quality & safetyEmbed
engagement over time!Support

COPYRIGHT HIMAA 2021 Health Information Management Association of AustraliaSlide No. 23
Professional Practice Standards, Codes & Guidelines

COPYRIGHT HIMAA 2021
Guidelines & Standards
24
Standard Who does it apply toGood Medical Practice: A code of conduct All doctors registered in Australia by APHRARegistered Nursing Standards for PracticeMidwife Standards for Practice Nurse Practitioner Standards
All registered nurses registered in Australia by APHRA and practicing within these specialties
APHRA Allied Health Codes of Conduct All ATSI Health Practitioners, Occupational, Medical Radiation Practitioners, Therapists, Pharmacists, PodiatristsPsychologists
Social Workers Practice Standards All Social Workers registered to practice in Australian*Australian Orthotics & Prosthetics Practice Standards
All Orthotists & Prosthetists registered to practice in Australian*
Speech Pathology Australian Professional Standards
All Social Workers registered to practice in Australian*
National Mental Health Care Standards All gazette Mental Health Service ProvidersNational Quality & Safety Health Care Standards All public & private hospitals, day procedure services
and public dental practices*not currently require to be registered with APHRA**Mental Health is subject to NSQHS also

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 25
Good Medical Practice – A Code of Conduct
Source: https://www.medicalboard.gov.au/codes-guidelines-policies/code-of-conduct.aspx
1. Describes expectations of all doctors registered to practice in Australia
2. Sets out the principles that characterise good medical practice
3. Explicitly states the standards of ethical practice and professional conduct
4. Provides a framework to guide professional judgement
5. Has 13 Standards to inform professional conduct
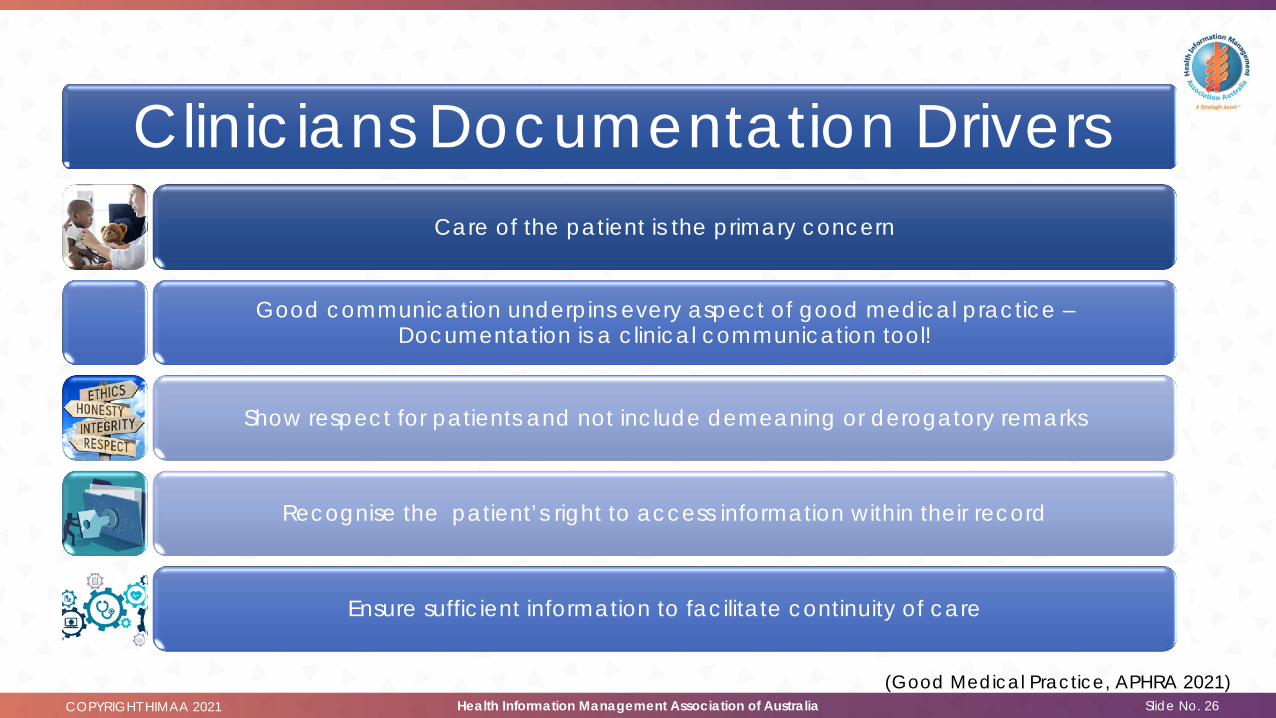
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 26(Good Medical Practice, APHRA 2021)
Clinicians Documentation DriversCare of the patient is the primary concern
Good communication underpins every aspect of good medical practice –Documentation is a clinical communication tool!
Show respect for patients and not include demeaning or derogatory remarks
Recognise the patient’s right to access information within their record
Ensure sufficient information to facilitate continuity of care

COPYRIGHT HIMAA 2021
Good Medical Practice: Standard 10.510.5 Medical records – Medical Practitioners
• Maintaining clear and accurate medical records is essential for the continuing good care of patients. Good medical practice involves:
10.5.1 Keeping accurate, up to date and legible records that report relevant details of clinical history, clinical findings, investigations, diagnosis, information given to patients, medication, referral and other management in a form that can be understood by other health practitioners.
10.5.2 Ensuring that your medical records are held securely and are protected against unauthorised access.
10.5.3 Ensuring that your medical records show respect for your patients and do not include demeaning or derogatory remarks.
10.5.4 Ensuring that the records are sufficient to facilitate continuity of patient care.
10.5.5 Making records at the time of the events, or as soon as possible afterwards.
10.5.6 Dating any changes and additions to medical records, including when the record is electronic.
10.5.7 Recognising patients’ right to access information contained in their medical records and facilitating that access.
10.5.8 Promptly facilitating the transfer of health information when requested by the patient or third party with requisite authority.
10.5.9 Retaining records for the period required by law and ensuring they are destroyed securely when they are no longer required.
27Source: https://www.medicalboard.gov.au/codes-guidelines-policies/code-of-conduct.aspx

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 28
Good Medical Practice – A Code of Conduct
The code of conduct is used to assist the Medical Board of Australia to evaluate a doctors’ professional conduct.
Where significant variation in professional practice occurs doctors need to be able to explain and justify their
decisions and actions against the requirements of the Good Medical Practice Standards
Source: https://www.medicalboard.gov.au/codes-guidelines-policies/code-of-conduct.aspx
COPYRIGHT HIMAA 2021
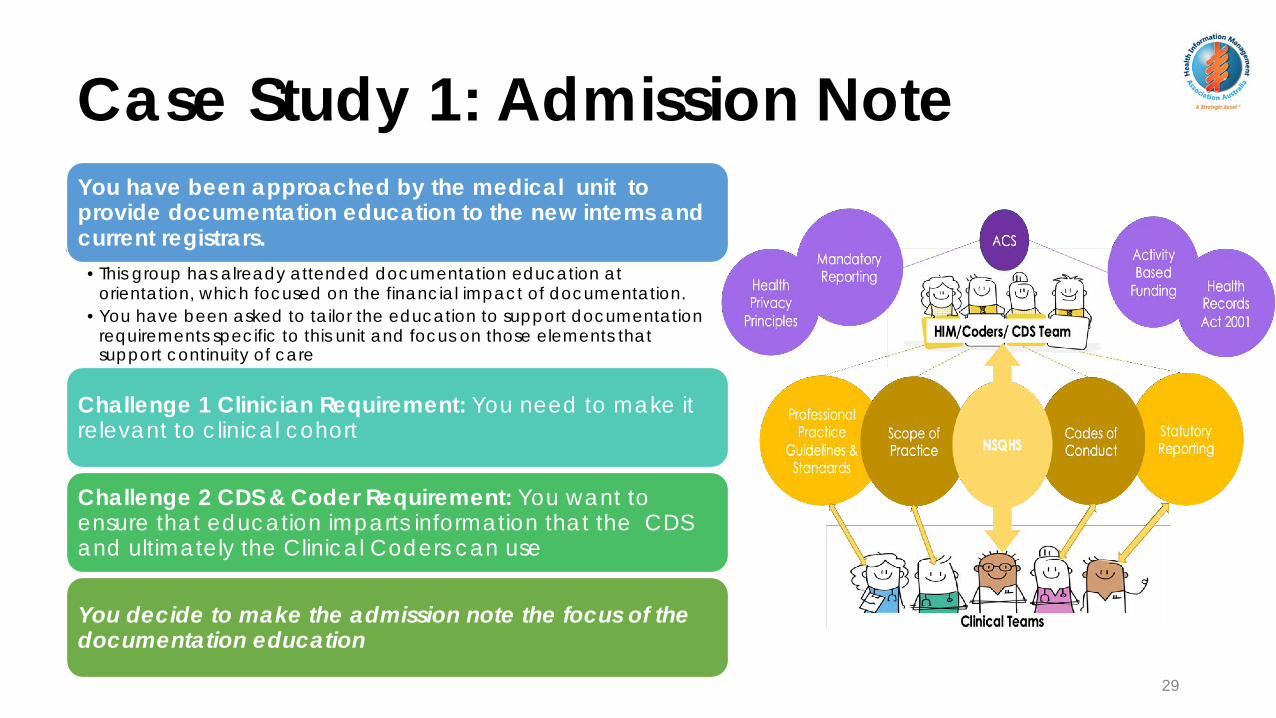
Case Study 1: Admission Note
29
You have been approached by the medical unit to provide documentation education to the new interns and current registrars. •This group has already attended documentation education at
orientation, which focused on the financial impact of documentation. •You have been asked to tailor the education to support documentation
requirements specific to this unit and focus on those elements that support continuity of care
Challenge 1 Clinician Requirement: You need to make it relevant to clinical cohort
Challenge 2 CDS & Coder Requirement: You want to ensure that education imparts information that the CDS and ultimately the Clinical Coders can use
You decide to make the admission note the focus of the documentation education

COPYRIGHT HIMAA 2021
Q: Why use the admission note?A: It is a formative clinical document
30
Upon admission to ward a 4-hour management plan must be agreed between ED doctor and Admitting doctor
The plan may evolve in response to new information from results, the patient or from improvement or deterioration
The admission note records transfer of care, history of presenting complaint and management plan
Its primary function is as a clinical communication tool, and it forms the basis of subsequent medical officer progress notes
It establishes the base from which members of the care team provide care in the initial stage of the admission
Comprehensive admission notes form the basis of good discharge summaries!
Well written admission note provides information required to evidence the code assignment, supports coding practice and is a key document for CDS conducting concurrent documentation reviews
CLI
NIC
IAN
SC
C/C
DS

COPYRIGHT HIMAA 2021
31
Standards AlignmentGMP Standards: 10.5.4 Ensuring records are sufficient to
facilitate continuity of care NSQHS 6.09: Communication at clinical handover -
consider minimum requirements at all transitions of care to support continuity of care
ASK: Is it achievable and related to the clinical role? We ask you to follow the documentation steps outlined in the Admission Note cheat sheet
This will support capture of the patients’ clinical status and communication of critical information to inform care
OFFER: What is in it for me? (Doctor)This will help streamline the documentation process as a clinical communication tool and to accurately reflect patients’
current status
RELEVANCE: How is this relevant to me? (Doctor)
You are responsible for writing a timely, comprehensive admission note for continuity of care

COPYRIGHT HIMAA 2021
Admission Note Documentation Requirements
32
Specify kind, frequency, duration, current status
Identifies factors that may impact on care/ management
Name of prescribing doctor, last medication review, changes, dispensing pharmacy
Check the UR, Name, Age, Gender,confirm you are writing in the correct record Right Patient
Who is the patient, state their name and age, chronic conditions impacting on presentation, relevant social factors, cognition, external referrals/reason for admission, preferred name and gender identity
Brief Patient Introduction
What has happened in the last 24hrs: presenting complaint, symptoms, medications, treatment, response – improvement or response
Why is the patient here?
Onset, severity, degree, duration, aggravating factors, include clinical markers that are typical to the presentation and whether present or not present, clinical indicators, results, mechanism of injury?
HOPC
Provisional Diagnosis, differential diagnoses and additional diagnoses present on admission, relevant results Diagnoses
What is the current plan for treating patient, what are the goals of care, who is responsible for care, referrals, discharge planningManagement Plan
Chronic Illnesses and comorbidities, resolved, medications used to manage, overdose, self harm or suicide attempts, mental health history
Past Medical History
Procedures, hospitalisations, reason, complicationsSurgical History
All medications, over the counter, herbal remedies, type, frequency, compliance, changes, allergies, abuse of prescription, multi-resistance?Medications
Current and past history of alcohol, non-prescription steroids, street drugs, Drug Use
Work, activity, family, relationships, support, accommodation, cultural/religious issues, income (in general terms), housing, current and pre-morbid level of function
Social History
What else do I need to capture to inform care plan?
All aspects that help identify the severity of illness, potential points of clinical variation or increased risk
Confirmed diagnoses, results, source of confirmation, comorbidities impacting on care or being treated
Include timeframes, confirmed referrals/speciality consults or who is responsible for making them
Type, severity, active, well controlled, type and dosage of medications to treat, compliance, impact on life
Date, outcome, number, where performed & by whom
Last used, number, type and frequency, previous rehab, duration of cessation, setting of use, overdose, psychosis
Any social history issues or factors that have the potential to impact on patient care, readmission or compliance

COPYRIGHT HIMAA 2021
Why does this approach connect with clinicians?
33
The focus is on the documentation components required for a good admission note, clinical decisions, clinical communication and safe care!
ü does not direct the clinician to document in a way maximise funding gainsü facilitates documentation practice to optimize the value for the documentation for
communication of criticalü Clearly describes minimum documentation requirements for admission note
ü Allows for documentation of the patients’ presentation & information based on information currently available and according to the clinical judgement
ü supports ongoing documentation improvementü complements clinician workflowü following this approach will capture detail and specificity to support code assignment
and reduce need for documentation queries
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia
Professional Practice Guidelines: Nurses
Slide No. 34
COPYRIGHT HIMAA 2021
35
Nurses at the heart of
careNursing Documentation: How important is it?
Very important to evidence • Continuity of care• Communication of critical information• Consent• Actioned Treatment Plans• Identifying existing and emerging risks• Keeping all members of the care team
informed of patient progress
For the CDS and Coders• A signpost to identify emerging conditions
or support coding queries

COPYRIGHT HIMAA 2021
Professional Practice Guidelines: Nurses1.6 Maintains accurate, comprehensive and timely documentation of assessments, planning, decision-making, actions and evaluations
1.7 contributes to quality improvement and relevant research
2.2 communicates effectively, and is respectful of a person’s dignity culture, values, beliefs and rights
2.4 provides support and directs people to resources to optimise health-related decisions
2.5 advocates on behalf of people in a manner that respects the persons autonomy and legal capacity
4.2 uses a range of assessment techniques to systematically collect relevant and accurate information and data to inform practice
4.3 works in partnership to determine factors that affect, or potentially affect, the health and wellbeing of people and populations to determine priorities for action and/or for referral5.1 uses assessment data and best available evidence to develop a plan
5.2 collaboratively constructs nursing practice plans until contingencies, option priorities, goals, actions, outcomes and timeframes are agreed with the relevant persons
5.3 documents, evaluates and modifies plans accordingly to facilitate the agreed outcomes
7.1 evaluates and monitors progress towards the expected goals and outcomes
7.3 determines, documents and communicates further priorities, goals and outcomes with the relevant persons.
36Source: https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/Professional-standards/registered-nurse-standards-for-practice.aspx

COPYRIGHT HIMAA 2021
Professional Practice Guidelines: Nurses1.6 Maintains accurate, comprehensive and timely documentation of assessments, planning, decision-making, actions and evaluations
1.7 contributes to quality improvement and relevant research
2.2 communicates effectively, and is respectful of a person’s dignity culture, values, beliefs and rights
2.4 provides support and directs people to resources to optimise health-related decisions
2.5 advocates on behalf of people in a manner that respects the persons autonomy and legal capacity
4.2 uses a range of assessment techniques to systematically collect relevant and accurate information and data to inform practice
4.3 works in partnership to determine factors that affect, or potentially affect, the health and wellbeing of people and populations to determine priorities for action and/or for referral
5.1 uses assessment data and best available evidence to develop a plan
5.2 collaboratively constructs nursing practice plans until contingencies, option priorities, goals, actions, outcomes and timeframes are agreed with the relevant persons5.3 documents, evaluates and modifies plans accordingly to facilitate the agreed outcomes
7.1 evaluates and monitors progress towards the expected goals and outcomes
7.3 determines, documents and communicates further priorities, goals and outcomes with the relevant persons.
37Source: https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/Professional-standards/registered-nurse-standards-for-practice.aspx
COPYRIGHT HIMAA 2021
Evidencing Collaboration & Continuity of Care
38
Admission
During the Shift
HandoverCase Conferences
Discharge
Inform the clinical picture of the patient and communicate critical information about• the patient, their family • goals of care• create care plans• administer prescribed & nursing initiated• Changes in patient’s physical & psychological condition,• Deterioration,• New conditions• Risk factors• Follow up care• Results review• Discharge planning
COPYRIGHT HIMAA 2021
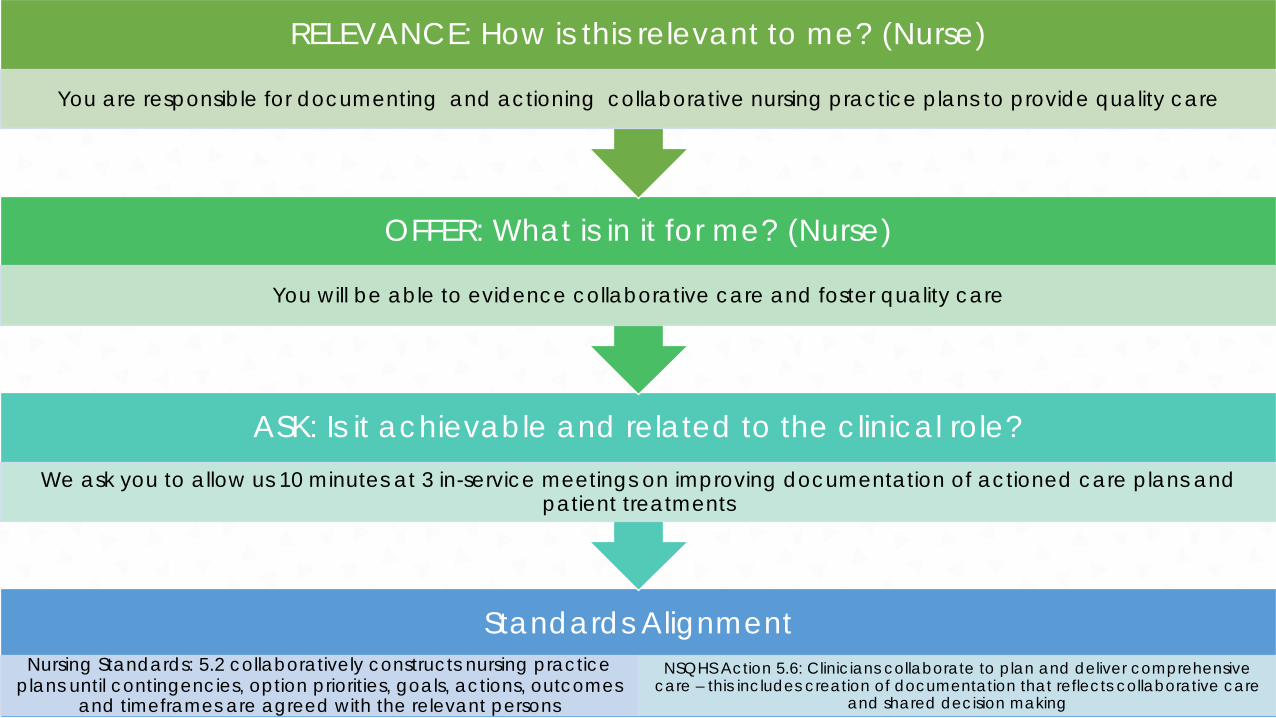
39
Standards AlignmentNursing Standards: 5.2 collaboratively constructs nursing practice
plans until contingencies, option priorities, goals, actions, outcomes and timeframes are agreed with the relevant persons
NSQHS Action 5.6: Clinicians collaborate to plan and deliver comprehensive care – this includes creation of documentation that reflects collaborative care
and shared decision making
ASK: Is it achievable and related to the clinical role? We ask you to allow us 10 minutes at 3 in-service meetings on improving documentation of actioned care plans and
patient treatments
OFFER: What is in it for me? (Nurse)
You will be able to evidence collaborative care and foster quality care
RELEVANCE: How is this relevant to me? (Nurse)
You are responsible for documenting and actioning collaborative nursing practice plans to provide quality care

COPYRIGHT HIMAA 2021
Allied Health &Scope of Practice
40
COPYRIGHT HIMAA 2021
Allied Health
41
Allied Health registered with APHRA follow the same documentation principles in the
Good Medical Practice (this is captured under Standard 8.4 of
Allied Health Code of Conduct)
COPYRIGHT HIMAA 2021
Allied Health
42
Formulate, document and implement management plans – including treatments, investigations and
collaborative care

COPYRIGHT HIMAA 2021
Allied Health
43
Other Allied Health have their own industry standards which include
documenting the clinical justification for treatment provided or prescribed device

COPYRIGHT HIMAA 2021
Allied Health
44
Allied Health Professions Australian requires that all clinicians document all
aspects of care, maintain legible, consiseand accurate documentation

COPYRIGHT HIMAA 2021
Examples of Allied Health Documentation Standards
45
1.3.1 Providing clinical justification for prescribed orthotics
2.3 Documents all aspects of care
2.5.2 Maintains legible, concise and accurate documentation using contemporary methods
a. assessing patient or client taking into account their history, views, and appropriate physical examination where relevant; the history includes social and cultural aspects
b. formulating and implementing a suitable management plan (including providing treatment and advice and, where relevant, arranging investigations and liaising with other treating practitioners)
7.1 Record and manage information appropriately.
a. Informs people of social work records and the purpose for which a record is made.
b. Informs people of who will/may have access to their record and why.
c. Advises people of how to access their records.
d. Writes information in an accurate, objective and contemporaneous manner, acknowledging the basis of any subjective opinions.
7.2 Keep and maintain information in accordance with ethical principles and relevant legislation.
4.2 adapts written, verbal and non-verbal communication appropriate to the client and practice context
4.5. Complies with legal and procedural requirements for the responsible and accurate documentation, sharing and storage of professional information and records of practice
4.6 Maintains contemporaneous accurate and complete records of practices
4.7 Obtains and documents informed consent for interventions
4.11 Articulates the rational for practice to clients and relevant others
Being aware of the requirements of the privacy and/or health records legislation that operates in relevant states and territories and applying these requirements to information held in all formats, including electronic information
From discussing patients or clients in a non-professional context complying with relevant legislation, policies and procedures relating to consent using consent processes, including formal documentation if required, for the release and exchange of health and medical information, and
Orthotists Social Workers OTs
Verbal discussions & decisions to be documented in the clinical record
ATSI, Pharmacy, PT, Podiatry (Summary)
documenting consent appropriately, including considering the need for written consent for procedures which may result in serious injury or deathc. facilitating coordination and
continuity of care
https://ahpa.com.au/allied-health-accreditation/https://www.ahpra.gov.au/
COPYRIGHT HIMAA 2021
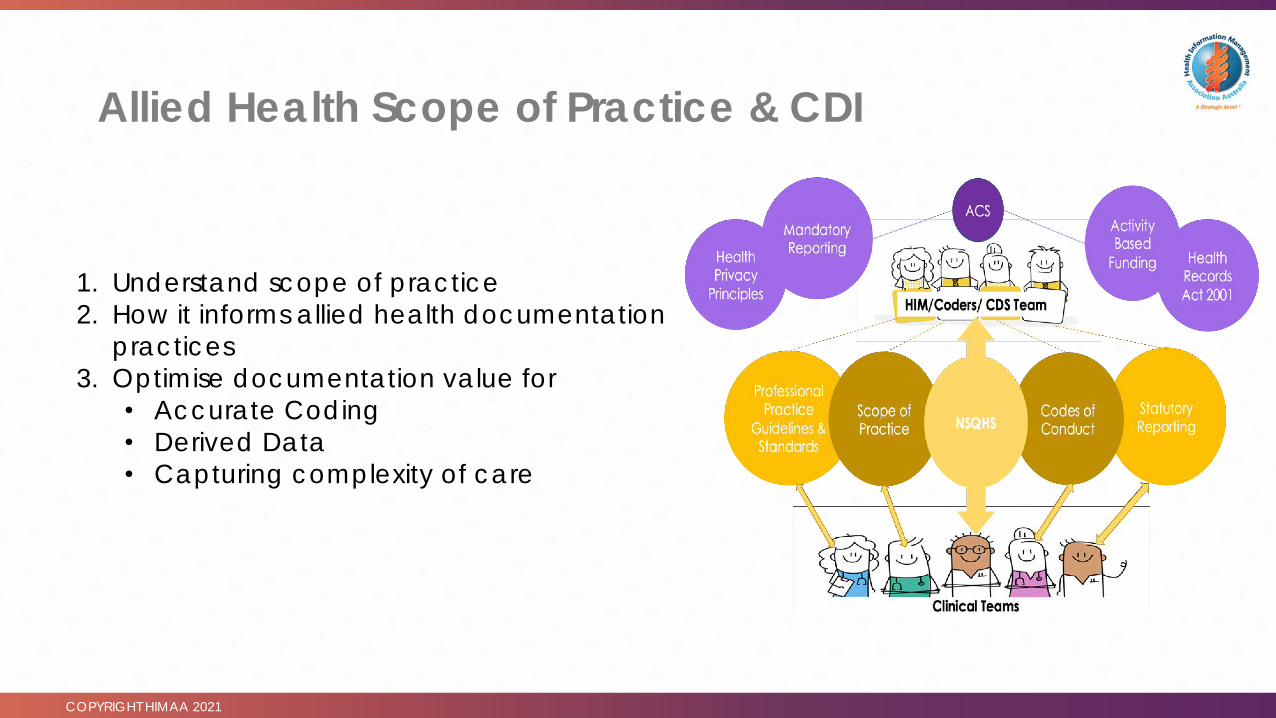
Allied Health Scope of Practice & CDI
46
1. Understand scope of practice2. How it informs allied health documentation
practices3. Optimise documentation value for
• Accurate Coding• Derived Data• Capturing complexity of care
COPYRIGHT HIMAA 2021 Health Information Management Association of AustraliaSlide No. 47Source: CDI Program Western Health, 2019
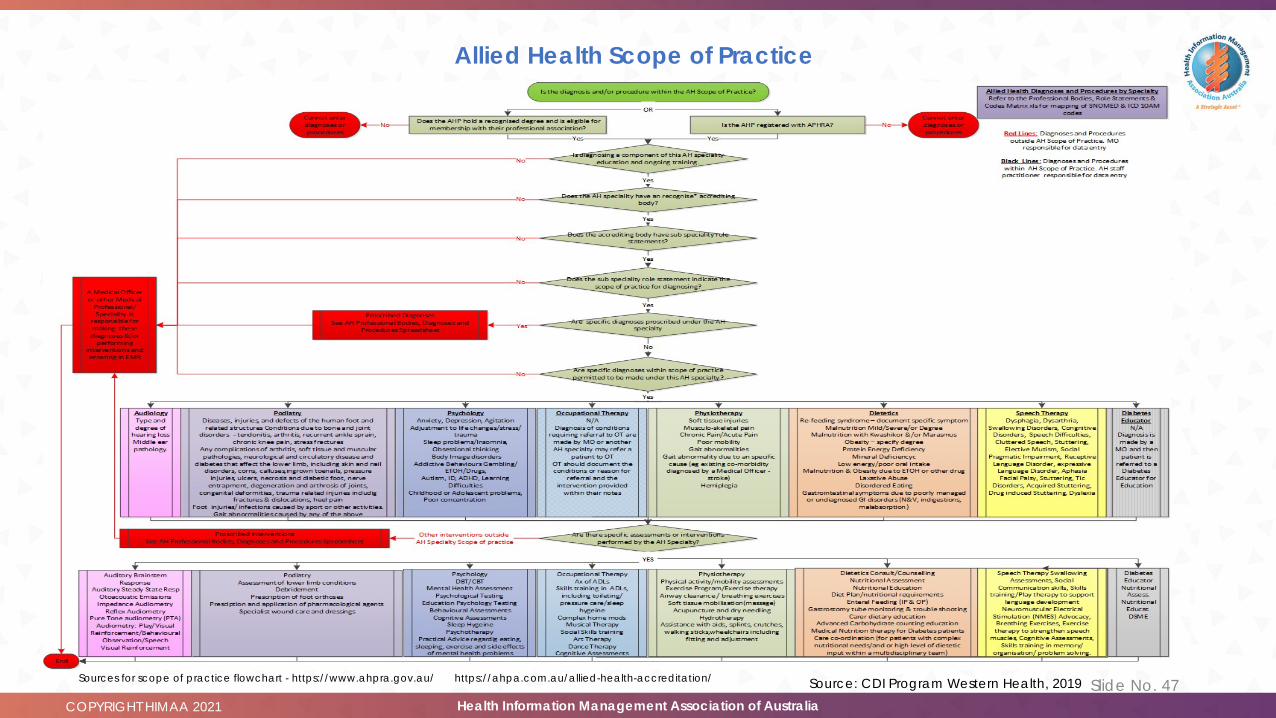
Allied Health Scope of Practice
https://ahpa.com.au/allied-health-accreditation/Sources for scope of practice flowchart - https://www.ahpra.gov.au/

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 48
Aust ra l ian Commiss ion on Safe ty & Qual i ty in Heal th Care
https://www.safetyandquality.gov.au/standards/nsqhs-standards
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 49
Grow your knowledge o f the s tandards
https://www.safetyandquality.gov.au/standards/nsqhs-standards
• Pre-empt the stakeholder question ‘What’s in it for me?’
• Position the work of HIMs, Coders & CDS with clinical and business partners
• Optimise the value of documentation and increase data integrity
• Identify areas where you need to grow your applied knowledge

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 50
Governance Health Care Records
Action 1.16Record is available at point of care, support staff in maintaining accurate and complete records, comply with security and privacy, support systematic audit of clinical information
Action 1.17Work towards implementing systems and supporting documentation that provides clinical information into My Health Record that optimise safety and quality of healthcare, use standard national terminologies
Action 1.18Provide information uploads into the My Health Record system that are accurate and complete, including amendments

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 51
My Health Record & Discharge Summaries
My Health Record requires from Health Care ProviderShared health summary from your GPHospital Discharge SummaryTest and Scan resultsCurrent Medicines and prescriptionsReferral Letters
CDI, GP Liaison & Medical Education Unit Initiative: Best Practice Discharge Summary Training
Standards Alignment: • NSQHS 1.17 & 1.18 • GMP 3.1.3 Facilitating coordination and continuity of careRelevance • Accurate, timely and complete discharge summary for
continuity of careOffer• Ease the burden of writing discharge summaries Ask• Please participate in one 20-minute discharge summary
education session per year, and • refer to the online resource as necessary

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 52
Medication Safety
Action 4.05 & 4.06Medication Reconciliation – document best possible medication history (BPMH) and review current orders against BPMH
Action 4.07 & 4.08Process in place for documenting history of medication allergies and adverse drug reactions (ADRs), document ADRs experienced during the episode of care
Action 4.10Perform medication reviews and document any actions taken as a result of medication reviews, identify and monitoring-related including those that have been prevented
Action 4.11Document in the healthcare records that patients and carers have been informed about the medicine; documentation may occur as a component of the consent process within the patient record or NIMC or MMP

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 53
Medication Safety & the BPMH
Documentation Improvement Education related to Medication Align with Actions 4.05 & 4.06 and supports relevance to clinical practice
A BPMH is essential for:• Ensuring continuity of medication management• Identifying medicine-related problems• Identifying potential medicine-related discrepancies• Informing the decision-making process• Optimising the use of medicines
Further alignment with 4.07 & 4.06 will encourage documentation practices that facilitate complete documentation of adverse events.

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 54
Comprehensive Care StandardAction 5.01Include guidance in policies and procedures regarding how to document comprehensive care, screening, assessments, findings, the outcome of shared decision making processes, agreed goal of care and comprehensive care plans
Action 5.04Design systems that support capture of comprehensive care, support clinicians to develop, document and communicate comprehensive care plans, ensure timely referral of patients with specialist health care needs
Action 5.05Apply the governance quality improvement system to monitor, implement and deliver comprehensive care – this includes ongoing data collection about outcomes such as length of stay, alignment of documented patient preferences with actual care, patient experiences and the prevalence of adverse events
Action 5.6Focuses on how clinicians collaborate to plan and deliver comprehensive care – this includes creation of documentation that reflects collaborative care and shared decision making

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 55
Communicating for SafetyAction 6.01Document policies, processes and tools for clinical communication, include details regarding when identification, procedure matching, structured clinical handover and communication of critical information and documentation are required.
Action 6.09Communication at clinical handover – consider minimum handover requirements at all transitions of care to support continuity of care
Action 6.11Ensure that relevant, accurate, complete and up-to-date information about a patients care is documented, and clinicians have access to the right information to make safe clinical decisions and to deliver safe, high-quality care

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 56
Action 6.09
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 57
Standard 6, CDI & Role Relevance
All clinicians need access to the right information for safe clinical
decisions and care
Documentation in the health record is the most important source of information across
time and care settings
Undocumented, poorly documented information or
reliance on memory for details of patient condition increases
risk and potential for misdiagnosis and harm
Participating in documentation education and documentation
improvement initiatives will ensure you understand your
documentation responsibilities
Standard 6 Key Messages for CDI

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 58
Blood Management Standard
Action 7.01As part of the blood governance management structures members of the clinical workforce are trained in documentation requirements relating to transfusion, and receipt, storage, collection and transport of blood and blood products
Action 7.05Documenting blood management requires documentation relating to blood management, transfusion history and transfusion details

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 59
5 Minute Education Aligned to Action 7.01Patient Risk FactorsPrevious history of
haemorrhage, gastrointestinal bleeds, medications,
anticoagulants, compliance with treatment
Document Perioperative Anaemia, type of anaemia, iron deficiency,
current treatments and haemglobin assessments
Where to document the condition requiring the blood
product and consent to receive blood products
On Blood Product form AND progress notes AND include
on discharge summary
Type and frequency of blood product to be administered
Document types and times of blood product administration
and response to treatment
Reason for blood productUnderlying cause,
comorbidity, blood loss, haemorrhage or procedural
complication,
OnsetAcute, acute on chronic,
arising in admission, complication, hospital acquired, or chronic
Linking Terminology Due to, secondary to
SeveritySpecify amount of blood loss,
frequency and symptoms
Outcome Patient Response to treatment
and management plan –deterioration, improvement, ongoing care required post
discharge?

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 60
Responding to Acute DeteriorationAction 8.04 (Detecting Acute Deterioration)Processes for detecting acute physiological deterioration include documentation of individualised care plans, monitoring of patients against individualised monitoring plan, documentation includes graphic representation of vital signs over time
Action 8.05 (Recognising Acute DeteriorationMonitor patients at risk of acute deterioration of mental state, document early warning signs, assess, document and communicate possible causes when changes are observed or reported and document
Action 8.10 – 8.13 (Responding to deterioration)Document details of care provided, emergency assistance, transfer decisions, referral decisions, communication of deterioration and handover

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 61
Deterioration foci for CDI EducationAirway
Obstructions & respiratory
distress
Document if due to neurological event, overdose, adverse
effective of medication or exacerbation of COPD,
fluid overload, sepsis
Document Onset, Severity, Causative Organism,
Treatment and Outcome
Hypotension Document if due to with sepsis, dehydration, post surgical bleeds, maternal haemorrhage, cardiac
failure
Document Onset, Severity, Frequency, Type of surgery,
Causative Organism, Treatment and Outcome
Altered Conscious
States
Document if due to prescription medication interactions, medication allergies drugs, alcohol,
dementia, mental health illness/psychosis, head
injury, falls
Document Onset, Type/Mechanism and location where injury
occurred, type of medication(s) causing altered state, Severity, Causative Organism,
Treatment and Outcome

COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 62
Takeaways!
• Become familiar with professional practice standards (PPS)
• Be aware of Allied Health Scope of Practice
• Understand documentation drivers
• Have Connected Conversations: Tailor Relevance, Offer & Ask• Collaborate with Medical, Nursing & Allied Health Education Teams
• Align CDI and Education to PPS & NSQHS

COPYRIGHT HIMAA 2021 Health Information Management Association of AustraliaSlide No. 63
Build our professional knowledge & industry profile
Don’t forget …What you do matters!
Want to share your expertise or have an idea for a webinar - contact me at https://www.linkedin.com/in/dreda-heard/Or via https://himaa.org.au/
Contact the HIMAA Edi tor ial Board at ht tps://himaa.org.au/committees
Do, Talk, Write, Promote, Share

COPYRIGHT HIMAA 2021
PLEASE JOIN ME FOR THE LIVE CHAT
COPYRIGHT HIMAA 2021 Health Information Management Association of Australia Slide No. 65
https://www.medicalboard.gov.au/Codes-Guidelines-Policies/Code-of-conduct.aspxhttps://www.safetyandquality.gov.au/standards/nsqhs-standardshttps://www.ahpra.gov.au/
https://www.occupationaltherapyboard.gov.au/Codes-Guidelines/Competencies.aspxhttps://ahpa.com.au/our-members/australian-association-of-social-workers/https://www.aopa.org.au/
https://www.speechpathologyaustralia.org.au/SPAweb/Resources_For_Speech_Pathologists/Professional_Standards/Professional_Standards/SPAweb/Resources_for_Speech_Pathologists/CBOS/Professional_Standards.aspx?hkey=583a56af-74e0-4111-95fa-656502269967
https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/Professional-standards/registered-nurse-standards-for-practice.aspx





























