Embed Size (px)
Citation preview

High-quality BreastUltrasonography
Janice S. Sung, MDKEYWORDS
� Breast � Ultrasonography � Imaging � Image quality
KEY POINTS
� Ultrasonography is an important modality that is frequently used in all aspects of breast imaging,including breast cancer screening, the evaluation of palpable abnormalities, further characteriza-tion of lesions seen mammographically, and for determining the method of percutaneous biopsy.
� Understanding the basic technical aspects of ultrasonography equipment is critical to ensure highbreast ultrasonography image quality.
ics.com
INTRODUCTION
Ultrasonography is an important imaging modalityfor the detection and characterization of lesions inthe breast. Appropriate indications for breast ultra-sonography as recommended by the AmericanCollege of Radiology Practice Guidelines includethe following:
� Evaluation and characterization of palpablemasses and other breast-related signs and/or symptoms
� Evaluation of abnormalities detected onmammography or breast magnetic resonance(MR) imaging
� Determining the method of guidance forpercutaneous biopsy
� Supplemental screening to mammography incertain populations
Advantages of breast ultrasonography includethat it is a rapid, widely available, and inexpensivemodality that does not involve breast compressionor ionizing radiation. As with all imaging modal-ities, ultrasonography’s value in the detectionand characterization of breast lesions largely de-pends on the quality of the images. Ultrasonogra-phy is highly operator dependent, and erroneousconclusions may be caused by technique or theapplication or misapplication of image processingalgorithms. Although there have been advances in
Department of Radiology, Memorial Sloan-Kettering CanE-mail address: [email protected]
Radiol Clin N Am 52 (2014) 519–526http://dx.doi.org/10.1016/j.rcl.2014.02.0120033-8389/14/$ – see front matter � 2014 Elsevier Inc. All
ultrasonography, including the development ofthree-dimensional transducers and automatedwhole-breast systems, breast ultrasonographystill requires real-time imaging in many situationsfor accurate interpretation.
In recent years, multiple states have passedlegislation mandating that women with densebreasts be notified of their breast density and thatthey may benefit from supplemental screening.This development has led to the proliferation ofwhole-breast screening ultrasonography as a sup-plemental screening modality to mammography inwomenwith dense breasts. Particularly when ultra-sonography is used in the screening setting, it isimperative to understand the various technicalfactors affecting image optimization in order tomaximize sensitivity while reducing the numberof unnecessary biopsies and recommendationsfor short term follow-up studies. This article re-views the technical factors that should be con-sidered in order to perform high-quality breastultrasonography.
PATIENT POSITIONING
The optimal position of the patient should minimizethe thickness of the portion of the breast beingimaged. During breast ultrasonography, the pa-tient should be positioned with the ipsilateral armover the head. In general, medial lesions should
cer Center, New York, NY 10065, USA
rights reserved. radiologic.th
eclin

Sung520
be scanned with the patient in the supine position,whereas lateral lesions should be scanned withthe patient in a supine oblique position in orderto reduce the thickness of the breast.
TRANSDUCER SELECTION
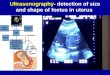
High-quality breast ultrasonography begins withselection of an appropriate transducer. The trans-ducers used in breast imaging must have a highfrequency (between 10 and 15 MHz) because ofthe superficial nature of the breast and the needto resolve small structures (Fig. 1). However,higher frequency sound waves are more stronglyattenuated by tissue than lower frequency waves.Therefore there is a trade-off between higher reso-lution and reduced penetration. With proper posi-tioning and the patient in the supine or supineoblique position, most breasts are only a few cen-timeters thick and high-frequency transducersprovide optimum image quality for all of the breasttissue. When evaluating deep tissue in patientswith particularly large breasts, it may be helpfulto have lower frequency transducers available tobe used only in this specific situation.Bandwidth is another consideration in trans-
ducer selection. The bandwidth is the spread offrequency around the central frequency of thetransducer, and transducers with a broader band-width have improved resolution. Transducers usedin breast imaging may either be linear or matrixarray, which affects image resolution.
IMAGE RESOLUTION
The goal of equipment selection is to maximize im-age resolution, which is the ability to distinguishstructures that are close together as separate le-sions. Image resolution is composed of contrastand spatial resolution (Fig. 2). Optimal contrastresolution is necessary to differentiate subtle le-sions from the surrounding breast tissue, andthese lesions may have subtle variations of gray
Fig. 1. Transducer frequency. High-quality breast ultrasoducers. The same mass (arrows) is imaged using 9-MHz (A(12 MHz) transducer results in better detail of the mass an
scale. Transducers with higher frequencies haveimproved contrast resolution.Spatial resolution is composed of both axial
and lateral resolution. Axial resolution is the abilityto resolve structures along the axis of the ul-trasound beam or the Z plane (the depth). Axialresolution depends on pulse length, which isdetermined by the frequency and the bandwidthof the transducer. A transducer with a higher fre-quency and a broader bandwidth has a shorterwavelength and pulse length relative to a lowerfrequency transducer, which improves axialresolution.Lateral resolution is the ability to resolve struc-
tures in the X and Y planes that are at the samedepth. Lateral resolution is related to the trans-ducer beam width, and lateral resolution is notadequate when lesions positioned side by sideare within the same beam width. Because a higherfrequency transducer has a narrower beam widthrelative to a lower frequency transducer, lateralresolution is improved.
FOCAL ZONE
As discussed earlier, lateral resolution is relatedto the beam width. In addition to selecting ahigh-frequency transducer to maintain a narrowbeam width, the beam width can be furtherreduced by adjusting the focal zone.Linear array transducers have multiple piezo-
electric crystals or elements arranged side byside. If a single element is used to both transmitand receive the signal, the beam diverges quicklyafter traveling a few millimeters, resulting in poorlateral resolution because of beam divergence.Linear array transducers pulse adjacent elementssimultaneously as a single element group to over-come beam divergence and then in succession toform the image. Delaying the timing of firing of el-ements within a single element group adjusts thefocal zone so that the beam is narrowed alongthe long-axis plane. The specific time delay
nography requires the use of high-frequency trans-) and 12-MHz (B) transducers. The higher frequencyd the surrounding breast parenchyma.

Fig. 2. Image resolution. Static ultrasonography im-age shows a subtle 2-mm invasive cancer (arrow)that would easily have been missed if image qualitywas not optimized.
High-quality Breast Ultrasonography 521
determines the depth of focus for the transmittedbeam. Matrix array transducers, which have multi-ple rows of elements, allow focusing in both theshort and long axes. The focal zone representsthe narrowest part of the beam and is the areawhere lateral resolution is optimized. Thereforethe focal zone should be placed at or slightly belowthe area of interest (Fig. 3). Because of transducerlimitations, even the shallowest focal zone settingmay not achieve the narrowest beam widthpossible for lesions near the skin. Therefore astandoff pad may be required to improve resolu-tion (Fig. 4).
DEPTH
During an initial survey, the depth on the ultraso-nography image should be set so that the breastparenchyma is imaged to the pectoralis muscle,which should be along the far field of view(Fig. 5). Once a finding is identified, the depthmay be adjusted.
GAIN AND TIME GAIN COMPENSATION
The overall gain control provides uniform amp-lification of all echo signals returning to the
Fig. 3. Focal zone. Images of the same mass with the focadepth (B, arrow). When the focal zone is at the level of thecharacterized.
transducer, compensating for increased attenua-tion of the ultrasound beam as it penetratesdeeper into the tissues. Increasing the gain am-plifies the intensity of all signals returning to thetransducer so that the image is brighter andmore visible on the display screen.
The initial gain setting should be adjusted so thatthe subcutaneous fat is a medium level of gray. Le-sions may be mischaracterized if the gain is inap-propriately set. For example, a subcentimeterhypoechoic solid mass or a complicated cystcan mimic a simple anechoic cyst if the gain isset too low (Fig. 6). In contrast, by inappropriatelysetting the gain too high, a simple or complicatedcyst may appear solid.
Unlike the gain, which adjusts all signals return-ing to the transducer, the time gain compensation(TGC) function allows selective amplification ofweaker signals from areas deeper in the breast.The TGC should be set so that all echoes fromsimilar structures are displayed with the samebrightness from the near to far field. For example,the subcutaneous fat should be the same shade ofmedium gray as the retromammary fat.
SPATIAL COMPOUND IMAGING
With standard imaging, the ultrasound pulses arepropagated perpendicular to the long axis of thetransducer. Spatial compounding uses electronicbeam steering to obtain multiple images atdifferent angles, which are then combined toform a single image in real time.1 Spatial com-pounding enhances returning echoes from realstructures, thereby improving image resolution,so that image features such as lesion marginsmay be better characterized. Artifacts, such asposterior acoustic enhancement characteristic ofsimple cysts and posterior shadowing seen withsome solid masses, tend to be averaged outand reduced. However, some small cancers aredetected primarily because of their posterioracoustic shadowing. When scanning for a subtle
l zone set too deep (A, arrow) and at the appropriatemass, the margins and internal features can be better

Fig. 4. Focal zone of superficial lesion. Because of transducer limitations, even the shallowest focal zone settingmay not achieve the narrowest beam width possible for lesions near the skin. Therefore a standoff pad may berequired to improve resolution. (A) A superficial hypoechoic mass (arrow). With the use of a standoff pad (B) al-lowing optimal resolution at the level of the skin, a skin tract (arrow) is now seen, confirming the diagnosis of abenign sebaceous cyst.
Sung522
lesion, it may be beneficial to use standard ultraso-nography imaging, in which the posterior shadow-ing may help identify the lesion, and then applyspatial compound imaging for analysis once thelesion has been detected.
HARMONIC IMAGING
Harmonic imaging is another signal processingtechnique to improve contrast and lateral resolu-tion and reduce artifacts.1 Harmonic imaging ap-plies a filter to remove image harmonics, whichare multiples of the transmitted frequency. Thistechnique is advantageous because much of theartifact degrading image resolution is containedwithin the lower frequency components of thebeam (Fig. 7).
COLOR DOPPLER AND POWER DOPPLER
Tumor angiogenesis plays a fundamental role inlocal tumor growth, invasion, and progression tometastases.2,3 As tumors outgrow their nativeblood supply, hypoxia ensues, which inducesexpression of multiple angiogenic factors such asvascular endothelial growth factor. These factorsinduce the growth of existing capillaries andthe formation of abnormal vessels that are oftentortuous and disordered, which may be seen on
Fig. 5. Depth. The depth should be set so that the imagelung, which provides no useful information (A). When the(arrows) are better seen.
color Doppler.4 Power Doppler imaging may beused to increased sensitivity compared with colorDoppler in detecting small vessels and low flow.The presence or absence or type of tumor
vascularity alone is not sufficient to characterizea lesion as benign or malignant. Features suggest-ing malignant lesions include hypervascularity,irregular branching central vessels, and morethan one vascular pole.5,6 Demonstrating internalvascularity within a sonographic lesion confirmsthat it is either solid or at least contains a solidcomponent. Doppler imaging is most useful in dis-tinguishing a high-grade invasive cancer or meta-static lymph node, both of which can appearanechoic, from a simple or complicated cyst(Fig. 8). Color Doppler may also be useful in differ-entiating between debris within a duct and an in-traductal mass.When using Doppler imaging, it is important to
apply light transducer pressure to prevent occlu-sion of slow flow within vessels. The position andsize of the color box should also be focused tothe lesion of interest tomaximize sensitivity to flow.
REAL-TIME IMAGING
Real-time imaging may be essential for accurateinterpretation in many situations. In patients withpalpable complaints, real-time ultrasonography by
focuses on the area of interest without including thedepth is set appropriately (B), the features of the mass

Fig. 6. Gain. Lesions can be mischaracterized if the gain is set too low or too high. (A) The gain is set too low andthe lesion appears anechoic (arrow), suggesting a simple cyst. With the gain set correctly (B), low-level internalechoes (arrow) are now seen in this complicated cyst. (C) The gain is set too high, creating artificial internalechoes (arrow) mimicking a solid mass. When the gain is corrected (D), the lesion is seen to be a simple cyst(arrow).
High-quality Breast Ultrasonography 523
the interpreting radiologist may be prudent in casesin which initial scanning by the technologist doesnot identify an abnormality. Another situation inwhich real-time imaging may be important is whendifferentiating between mobile debris in a compli-cated cyst versus a complex cystic mass (Fig. 9).
TARGETED ULTRASOUND: LESIONCORRELATION
Targeted ultrasonography is often performed inorder to identify a sonographic correlate to anabnormality identified on mammography orbreast MR imaging before percutaneous biopsy.Ultrasonography-guided biopsy is the method ofchoice to sample any finding that is sonographi-cally evident. Compared with stereotactic or MRimaging–guided biopsy, ultrasonography-guided
Fig. 7. Harmonic imaging. (A) The 12:00 axis of the rightalmost isoechoic to the fat. (B) Harmonic imaging of theand internal features (arrow), which allows the two lesion
biopsy is faster, more comfortable for the patient,and allows greater access to breast tissue, espe-cially for far posterior and medial lesions thatmay not be amenable to either stereotactic orMR imaging–guided biopsy. In addition, adequatesampling is more consistently obtained becausethe needle can be seen traversing the target inreal time.
When targeted ultrasonography is performedto evaluate a mammographic finding, careful trian-gulation of lesion location should be performed.Adjustments should be made when using cranio-caudal and mediolateral-oblique (MLO) views todetermine the clock axis for targeted ultrasonogra-phy. The location of the lesion may be higher orlower than expected based on the MLO view formedial and lateral lesions respectively. In addition,careful attention should bepaid toboth lesiondepth
breast shows 2 subtle structures (arrow) that appearsame area allows better delineation of the marginss to be characterized as complicated cysts.

Fig. 8. Color Doppler. (A) A hypoechoic mass (arrow) in the far field with posterior enhancement, possibly rep-resenting a complicated cyst. With color Doppler (B), vascularity (arrow) is seen within the mass, confirmingthat it is solid and not a complicated cyst. Biopsy yielded invasive ductal carcinoma.
Sung524
and the surrounding anatomic landmarks. The pa-tient is positioned differently during breast ultraso-nography, MR imaging, and mammogram, whichaffects lesion location. A superficial mass at thefat-gland interface on mammography or MR imag-ing should alsobeat that interface on targetedultra-sonography (Fig. 10). Other findings such as anadjacent cyst or dilated duct may also be used asanatomic landmarks.When sampling a potential sonographic corre-
late to a mammographic abnormality, a localizingclip should be placed in the biopsied lesion usingultrasonography guidance. A postbiopsy mammo-gram should be obtained to confirm correlationbetween the biopsied lesion and the mammo-graphic abnormality.Targeted ultrasonography is often performed to
evaluate for a sonographic correlate to an MRimaging finding in order to facilitate biopsy. Apotential correlate is more frequently identifiedfor enhancing masses compared with nonmass
Fig. 9. Real-time imaging. (A) In the right breast at the 6:3(B) When the patient is rolled into the left lateral decubdependent portion of the cyst (arrow), consistent with mo
enhancement.7–11 However, true ultrasonogra-phy–MR imaging correlation can only be con-firmed if follow-up MR imaging is performed,showing the localizing clip placed at the time ofultrasonography-guided biopsy within the area ofenhancement on MR imaging. In one study, thepresumed sonographic correlate biopsied yieldingabenign, concordant diagnosis did not correspondwith the lesion originally detected onMR imaging in12%of cases.10 For this reason, 6-month follow-upMR imaging is recommended following benignconcordant biopsy of a sonographic correlate toan MR imaging–detected lesion.12
AMERICAN COLLEGE OF RADIOLOGYACCREDITATION
The American College of Radiology offers a BreastUltrasound Accreditation Program. Accreditationrequires the application of many of the conceptsdiscussed in this article to obtain high-quality
0 axis is a cyst with a possible intracystic mass (arrow).itus position, the questionable mass moves into thebile debris.

Fig. 10. Lesion miscorrelation. (A) A superficial enhancing mass (arrow) in the superior breast. Targeted ultraso-nography identified a mass (arrow) that was thought to represent a correlate (B). Although the sonographic masswas of a similar size and clock axis to the MR finding, it was deep within the breast, whereas the MR mass was atthe fat-gland interface. Ultrasonography-guided biopsy yielded fibroadenoma. On 6-month follow-up MR imag-ing, the clip (arrow) from ultrasonography-guided biopsy is seen deep to the MR mass (C). Subsequent biopsyyielded invasive ductal carcinoma.
High-quality Breast Ultrasonography 525
images. The center frequency of the transducermust be at least 10 MHz. Unlike breast MR imag-ing accreditation, in which images from each indi-vidual magnet must be submitted, a facility mustonly provide a single example of a cyst and solidmass in the breast for ultrasonography accredita-tion regardless of the number of ultrasonographyunits at that facility. Two orthogonal mammo-graphic views must be submitted with the lesioncircled and visible on both views. Sonographicclinical images include the cyst and solid masson 2 orthogonal views without calibers, and 1 im-age with appropriate measurements. Imagesshould be taken along the longest axis of a lesionand then an orthogonal image. The longest axisof the lesion is not necessarily in the radial or anti-radial plane, but may be in an oblique position.Criteria for a simple cyst include anechoic, circum-scribed margin, and posterior enhancement. Forsubmitted images of cysts, spatial compound im-aging should be avoided if the resulting image failsto show posterior enhancement.
SUMMARY
Ultrasonography is an important modality that isfrequently used in all aspects of breast imaging,
including breast cancer screening, the evaluationof palpable abnormalities, further character-ization of lesions seen mammographically, andfor determining the method of percutaneousbiopsy. Understanding the basic technical as-pects of ultrasonography equipment is criticalto ensure high breast ultrasonography imagequality.
REFERENCES
1. Harvey CJ, Pilcher JM, Eckersley RJ, et al. Ad-
vances in ultrasound. Clin Radiol 2002;57(3):
157–77.
2. Schneider BP, Miller KD. Angiogenesis of breast
cancer. J Clin Oncol 2005;23(8):1782–90.
3. Weidner N, Semple JP, Welch WR, et al. Tumor
angiogenesis and metastasis–correlation in inva-
sive breast carcinoma. N Engl J Med 1991;
324(1):1–8.
4. Less JR, Skalak TC, Sevick EM, et al. Microvascular
architecture in a mammary carcinoma: branching
patterns and vessel dimensions. Cancer Res 1991;
51(1):265–73.
5. Yang W, Dempsey PJ. Diagnostic breast ultrasound:
current status and future directions. Radiol Clin
North Am 2007;45(5):845–61, vii.

Sung526
6. Mehta TS, Raza S, Baum JK. Use of Doppler ultra-
sound in the evaluation of breast carcinoma. Semin
Ultrasound CT MR 2000;21(4):297–307.
7. LaTrenta LR, Menell JH, Morris EA, et al. Breast le-
sions detected with MR imaging: utility and histo-
pathologic importance of identification with US.
Radiology 2003;227(3):856–61.
8. Abe H, Schmidt RA, Shah RN, et al. MR-directed
(“Second-Look”) ultrasound examination for breast
lesions detected initially on MRI: MR and sono-
graphic findings. AJR Am J Roentgenol 2010;
194(2):370–7.
9. Demartini WB, Eby PR, Peacock S, et al. Utility of tar-
geted sonography for breast lesions that were
suspicious on MRI. AJR Am J Roentgenol 2009;
192(4):1128–34.
10. Meissnitzer M, Dershaw DD, Lee CH, et al. Targeted
ultrasound of the breast in women with abnormal
MRI findings for whom biopsy has been recommen-
ded. AJR Am J Roentgenol 2009;193(4):1025–9.
11. Beran L, Liang W, Nims T, et al. Correlation of tar-
geted ultrasound with magnetic resonance imaging
abnormalities of the breast. Am J Surg 2005;190(4):
592–4.
12. Sung JS, Lee CH, Morris EA, et al. Patient follow-up
after concordant histologically benign imaging-
guided biopsy of MRI-detected lesions. AJR Am J
Roentgenol 2012;198(6):1464–9.