Embed Size (px)
Citation preview

HP
H(2ocumtabM
*
†
A
1
ereditary Nonpolyposis Colorectal Canceraul E. Wise, MD,* and Matthew G. Mutch, MD†
Hereditary nonpolyposis colorectal cancer (HNPCC) is the most common form of heredi-tary colorectal cancer (CRC). The disease carries a >80% lifetime risk of CRC (mean ageat diagnosis being 46 years). The CRCs that arise in HNPCC are usually right-sided andassociated with synchronous and metachronous tumors. HNPCC is also associated with ahigh risk of extracolonic cancers, predominantly endometrial cancer. Predisposition tocancer in HNPCC has been attributed to mutations in mismatch repair (MMR) genes, over95% of the identified mutations in HNPCC being in hMSH2, hMLH1, and hMSH6. Theabnormal MMR genes lead to instabilities in nucleotide repeat sequences (microsatellites)within the genome (MSI, microsatellite instability) that may lead to tumorigenesis andconcerning pathologic features but improved clinical outcomes when compared withsporadic CRCs without MSI. Mutations in MMR genes are also associated with a host ofother extraintestinal cancers. Each individual MMR gene has its own genotype–phenotypepattern of expression that can vary from individual to individual. As a result, this geneticinformation can be used to direct surveillance of affected and at-risk family members. Oncethe clinical criteria for HNPCC have been met and/or a gene mutation confirmed, affectedpatients show improved survival with cancer screenings every 1 to 2 years starting beforeage 25 years. Prophylactic colectomy for asymptomatic gene mutation carriers and theextent of colectomy when polyps or cancer arise in HNPCC remain the subject of debate.This issue will discuss our current understanding of the genetics of HNPCC, the variousphenotypic expressions, genetic testing, surveillance, and current recommendations ofmanagement of this familial cancer syndrome.Semin Colon Rectal Surg 15:136-146 © 2004 Elsevier Inc. All rights reserved.
KEYWORDS hereditary nonpolyposis colorectal cancer, HNPCC, hereditary cancer, prophy-lactic colectomy, microsatellite instability, mismatch repair genes
implcHrqifmitetacaf
ereditary nonpolyposis colorectal cancer (HNPCC) isthe most common form of hereditary colorectal cancer
CRC), accounting for 2 to 7% of all CRCs and approximately0 to 35% of all inherited CRC.1-3 Overall it is believed toccur in 1 in 400 to 1 in 3100 individuals with a lifetimelinical penetrance of greater than 80%.4-6 Affected individ-als have a germline mutation in a class of genes called mis-atch repair genes (MMR). Over 90% of the known muta-
ions have been identified in three genes (hMSH2, hMLH1,nd hMSH6), but there are several other MMR genes that haveeen implicated in HNPCC. Identification of a mutation in anMR gene confirms the diagnosis and allows genetic screen-
Section of Surgical Sciences, Division of General Surgery, Vanderbilt Uni-versity Medical Center, Nashville, TN.
Division of General Surgery, Section of Colon and Rectal Surgery, Wash-ington University School of Medicine, St. Louis, MO.
ddress reprint requests to: Paul E. Wise, MD, Assistant Professor of Sur-gery, Section of Surgical Sciences, Division of General Surgery, Vander-bilt University Medical Center, D-5220 MCN, Nashville, TN 37232.
uE-mail: [email protected].
36 1043-1489/04/$-see front matter © 2004 Elsevier Inc. All rights reserved.doi:10.1053/j.scrs.2005.02.008
ng of at-risk individuals within the family. Unfortunately, autation is not identified for all families that demonstrate aattern of inherited cancers. Therefore identification, surveil-
ance, and management of these patients must proceed onlinical grounds. The mean age at diagnosis of CRC inNPCC is approximately 46 years.5,7 The CRCs that arise in
elation to HNPCC usually arise in adenomas (albeit moreuickly than the “usual” 8- to 10-year transformation noted
n sporadic CRC3), are usually right-sided (60 to 70%), andrequently are associated with synchronous (5 to 10%) andetachronous (10 to 50%) tumors.4,5 This autosomal-dom-
nantly inherited hereditary cancer syndrome is also relatedo extracolonic cancers that include endometrial (60% risk ofndometrial cancer in women with HNPCC), ovarian, gas-ric, urinary tract, renal, bile duct, central nervous system,nd small bowel.5,7 Unfortunately, the statistics on HNPCCome from studies in previously identified at-risk familiesnd registries, not from the population at large, and there-ore, the true incidence of this condition and its cancers is
nknown. As more is understood about the genetics of
Ha
HTwMtftc(HialiitcToppcwwlt
Nsatlaiotsgtav
CTtbtaCssiw
oCpuCtuti
pHlIvafimsntdfiT3rcbms
eipnDccsddHdCpmHyttr5aatfn
Hereditary nonpolyposis colorectal cancer 137
NPCC, the ability to provide comprehensive clinical man-gement to these families will improve.
istoryhe history of the identification of HNPCC began in 1913hen Dr. Aldred Warthin, a pathologist at the University ofichigan at the time, published an account of Family G and
heir cancer syndrome. His description of his seamstress’amily (she died from metastatic endometrial cancer) andheir predilection for gastric, colonic, and endometrial can-ers with a notably autosomal-dominant inheritance patternlater identified as having an hMLH2 mutation3) inspired Dr.enry T. Lynch to publish on the “cancer family syndrome”
n 1971. In 1966, Dr. Lynch described two extended familiesnd their propensity for gastrointestinal and gynecologic ma-ignancies despite no predisposing colonic polyps (one fam-ly later identified as having an hMSH2 mutation3). Interest-ngly enough, he and his collaborators first postulated thathere might be an oncogenic virus interacting with geneti-ally susceptible humans to cause these cancer pedigrees.hey later discounted this theory for a primarily genetic eti-logy as they toured the United States in a customized vehicleerforming interviews and obtaining tissue and blood sam-les from affected family members.3 In 1984 the family can-er syndrome was renamed Lynch syndrome I for familiesith early onset CRC and Lynch syndrome II for familiesith early onset CRC and extracolonic cancers. These were
ater consolidated under the name of HNPCC to differentiatehem from other hereditary CRCs.1,5,8
The International Collaborative Group on Hereditaryonpolyposis Colorectal Cancer (ICG-HNPCC) developed
tandardized criteria for HNPCC in 1991 in Amsterdam in anttempt to recruit patients for prospective studies. These cri-eria became known as the Amsterdam I criteria that wereater supplanted by the Bethesda guidelines in 1996 in anttempt to improve sensitivity of the criteria and establishndicators for need for microsatellite instability (MSI) testingf tumors (described below). Because of the improved sensi-ivity but decreased specificity of these guidelines, the Am-terdam II criteria were released in 1999 to find a middleround.5 These were further revised and released in 2004 ashe revised Bethesda guidelines for the diagnosis of HNPCCs well as testing recommendations.5 Table 1 gives an over-iew of these various guidelines.
linicopathologic Featureshrough the dedicated work of Dr. Lynch and other scien-
ists, the clinical and pathologic features of HNPCC haveeen clarified. The primary clinical features, as outlined inhe Bethesda guidelines and Amsterdam criteria, are early-ge onset of familial clustering cancers, including primarilyRC and extracolonic cancers of the endometrium, ovary,
tomach, urinary tract, bile duct, central nervous system, andmall bowel. The disease has an autosomal-dominant inher-tance pattern related to an 80 to 92% lifetime risk of CRC,
ith the mean age of diagnosis being approximately 46 years fild (between 44 and 48 years old).5,7 This is unlike sporadicRC with a mean onset at age 65 years old and a left-sidedredilection.1 The CRC associated with HNPCC does notsually arise before age 30, but there are isolated cases ofRC developing before age 20.5 Approximately one-third of
he HNPCC-related CRC arise proximal to the splenic flex-re, and there is up to a 10% rate of synchronous CRC and upo a 50% rate of metachronous CRC within 10 years of thenitial diagnosis.4,5
Although the name of the disease suggests that there are noolyps related to the formation of these early-onset cancers,NPCC-related CRC occur in adenomas that form earlier in
ife and with an elevated rate of progression to cancer.1,3,5
nterestingly, the rate of polyp formation is only slightly ele-ated in these patients relative to sporadic adenomas (newdenomas after a previous adenoma was removed are identi-ed at a mean of 16 months1), but the underlying MMR geneutations appear to influence the increased rate of progres-
ion through the adenoma–carcinoma pathway.5,9 The ade-omas that form in HNPCC are usually villous, have dysplas-ic features,1 and have the same underlying molecularerangements (MSI) as the CRC identified in HNPCC, con-rming that most of these cancers do progress from polyps.5
ypically, CRC in HNPCC, progress from polyp to cancer into 4 years.1,3 However, this cancer formation can occur so
apidly that patients who have had negative-screeningolonoscopies or even segmental colectomies for cancer haveeen found to have new cancers develop in less than 12onths in some cases.10,11 This is much quicker than the
poradic adenoma to cancer formation time of 8 to 10 years.3
Histologically, these HNPCC tumors are associated withvidence of a host immune response including lymphocyticnfiltrates and a Crohn’s-like reaction. They also are oftenoorly differentiated with cribriforming associated with sig-et-ring cells, medullary-type, and mucinous features.5,3,12
espite these aggressive pathologic features of HNPCC can-ers, numerous retrospective analyses have shown better out-omes for these patients stage-for-stage when compared withporadic CRC. There is evidence that these patients haveecreased likelihood for lymph node metastases and thatisease-free and overall survival is improved in patients withNPCC-related CRC versus most sporadic CRC (those thato not show MSI, which shows an improved prognosis in allRC13,14). Even if there are lymph node metastases, theseatients have improved survival. This survival advantage re-ains even without adjuvant chemotherapy.1,15 Patients withNPCC (all stages) had an improved overall survival at 5ears of 76% versus 54% for sporadic cancers, and at 10 yearshe survival was 68% versus 48%, respectively.3,5 Althoughhis improved survival is not seen in all studies (including aeview by Bertario and coworkers of 2340 patients showing-year overall survivals to be equivalent for HNPCC, familialdenomatous polyposis (FAP), and sporadic CRC patientsfter adjusting for demographics and tumor stage and loca-ion12), the majority of studies have shown improved survivalor patients with CRC in the setting of HNPCC. The expla-ation for this improvement in survival has not been identi-
ed, but is thought to be due to an earlier stage identification
oh
EsmEHaaogcwticbat
Uqtetfdfwbt
ocbhwfs
T
A
B
A
R
138 P.E. Wise and M.G. Mutch
f the cancers, improved surveillance, and possibly the en-anced immune response in the HNPCC tumors.1,5
Extracolonic cancers are frequently identified in HNPCC.ndometrial cancer is the most common extracolonic cancer,o much so that it has been at times characterized as being aore frequent cancer in HNPCC women than even CRC.ndometrial cancer occurs in 20 to 60% of women withNPCC5,16 with an average age at diagnosis of between 46
nd 48 years old1 (in comparison to a sporadic rate of 2 to 3%t an average age in the mid 60s). These cancers are moreften associated with mutations in the hMSH2 and hMSH6enes than in the hMLH1 gene. Although it is a frequentancer, it has only been the cause of death in 12% of HNPCComen.5 This may be due to earlier diagnosis from symp-
oms, more frequent screening with HNPCC patients, or anncreased rate of prophylactic hysterectomy at the time ofolectomy or other operation, but these reasons have noteen proven. It should be noted that a study by Weinbergnd coworkers showed that a primary diagnosis of endome-
able 1 Criteria and Guidelines for Hereditary Nonpolyposis
msterdam I criteria (must fit all criteria):1. One family member with colorectal cancer before age2. Two generations affected3. Three relatives affected, one of them a first-degree rela4. Familial adenomatous polyposis excluded5. Pathologic verification of tumors
ethesda guidelines (can fit any of the criteria):1. Individuals with cancer in families that meet the Amste2. Individuals with two HNPCC-related cancers, including
extracolonic cancers (endometrial, ovarian, gastric, heppelvis or ureter)
3. Individuals with colorectal cancer and a first-degree recancer and/or colorectal adenoma; one of the cancers
4. Individuals with colorectal cancer or endometrial cance5. Individuals with right-sided colon cancer with an undif
undifferentiated) diagnosed before age 456. Individuals with signet-ring cell type colorectal cancer7. Individuals with colorectal adenomas diagnosed before
msterdam II criteria (must fit all criteria):1. At least three relatives with an HNPCC-related cancer2. One should be the first-degree relative of the other tw3. At least two successive generations affected4. At least one diagnosed before age 505. Familial adenomatous polyposis excluded6. Pathologic verification of tumors
evised Bethesda guidelines for testing colorectal tumors fo1. Colorectal cancer diagnosed before age 502. Presence of synchronous or metachronous colorectal o
pancreas, ureter, and renal pelvis, biliary tract, small band sebaceous gland adenomas and keratoacanthomas
3. Colorectal cancer with the microsatellite instability-higlymphocytic reaction, mucinous/signet-ring differentiatbelow age 60
4. Colorectal cancer diagnosed in one or more first-degrecancers being diagnosed before age 50
5. Colorectal cancer diagnosed in two or more first- or seof age
rial (or ovarian) cancer before age 50 years in the general m
.S. population is an independent risk factor for a subse-uent diagnosis of CRC (incidence ratio of 3.39 for endome-rial and 3.67 for ovarian cancer).17 They were unable tostablish from this retrospective cohort of over 50,000 pa-ients whether this was due to genetic factors, environmentalactors, or both, but there is a clear association between theseiseases. When HNPCC families with a known predilectionor endometrial cancer are studied, however, MSI is not al-ays identified.4 Therefore the etiology of these tumors maye through a pathway different from that identified as leadingo the formation of HNPCC-related CRC.
Other extracolonic cancers include gastric (13 to 19%),varian (9 to 12%), small bowel (1 to 4%), bladder (4%),entral nervous system (4%), upper urinary tract (3%), andiliary tract (2 to 18%).5,16 The gastric cancer risk may be asigh as 20% in endemic areas such as Asia and is often higherith the hMSH2 gene mutation. Urinary tract cancers are
requently also related to this gene mutation. Muir-Torre’syndrome refers to HNPCC patients with sebaceous skin tu-
ctal Cancer5,7
f the other two
I criteriahronous and metachronous colorectal cancers orliary, small bowel, or transitional cell cancer of the renal
with colorectal cancer and/or HNPCC-related extracolonicage 45 and the adenoma diagnosed before age 40
nosed before age 45ated pattern on histopathology (solid/cribriform, poorly or
osed before age 45 (composed of >50% signet-ring cells)0
ectal, endometrial, small bowel, ureter, or renal pelvis)
rosatellite instability (MSI) (can fit any criteria):
r HNPCC-related cancer (endometrial, gastric, ovarian,brain (usually glioblastoma as seen in Turcot syndrome),uir–Torre syndrome), regardless of ageI-H) histology (tumor infiltrating lymphocytes, Crohn’s-liker medullary growth pattern) diagnosed in a patient who is
tives with an HNPCC-related tumor, with one of the
degree relatives with HNPCC-related tumors, regardless
Colore
50
tive o
rdamsyncatobi
lativebeforer diag
ferenti
diagnage 4
(coloro
r mic
r otheowel,
in Mh (MSion, o
e rela
cond-
ors usually related to hMSH2, and Turcot’s syndrome, an-

om
GTdlhcHttkaHetgsmeHott5mm7aecgTHrt
cctHtliftopCcthelcf
psq
ccpipioDppmffihaslfacseb
mtlDtdnpaffboseottrTitmaigEs
Hereditary nonpolyposis colorectal cancer 139
ther HNPCC-related syndrome, is associated with the for-ation of glioblastoma multiforme.5
eneticshe molecular genetic etiology of HNPCC was first eluci-ated in the early 1990s when linkage analysis identified two
oci on chromosomes 2p and 3p.3 Later, within these loci,MSH2 and hMLH1 were identified, respectively, which ac-ount for over 90% of the identified gene mutations inNPCC.1,5 It was around this same time that tumors in pa-
ients who fit the early clinical criteria for HNPCC were notedo have recurrent replication error phenotypes that are nownown as MSI. Putting this data together allowed scientistsnd geneticists to conclude that the genes involved inNPCC were those that performed the function of repairing
rrors in DNA replication (MMR) that, when mutated, led tohe increased cancer risks seen in HNPCC. This is opposed toenetic disorders where the cancer-causing genes are them-elves mutated, such as the tumor-suppressor APC (adeno-atous polyposis coli) gene in FAP. Since the initial discov-
ry of the primary genes hMSH2 and hMLH1 involved inNPCC, they have been linked to approximately 35 and 60%f the genetically characterized HNPCC families, respec-ively.16 Other genes have also been shown to play a role ashe primary gene mutation in some families.3 Approximatelyto 10% of HNPCC families with a known mutation have autation in hMSH6,4 which was identified in 1997 on chro-osome 2p16.5 Other genes include hPMS1 (chromosome
p22), hPMS2 (7p22), hMLH3 (14q24.3), TGF�R2 (3p22),nd possibly EXO1 (1q42.32).5,16,18,19 Still, with these discov-ries, there are approximately 50% of families who meet thelinical criteria for HNPCC but do not have an identifiableene mutation based on our current diagnostic technologies.3
his suggests that other gene mutations exist that lead to theNPCC phenotype and have yet to be identified, or the cur-
ent technology is not sensitive enough to detect other mu-ations in the previously identified genes.
There have been few conclusive genotype-to-phenotypeorrelations with the genes involved in HNPCC, the types ofancers, and their prevalence, except for those families withhe hMSH6 mutation.16 A recent report from a GermanNPCC registry containing 706 families demonstrated a dis-
inctly different pattern of expression of CRC and extraco-onic cancers in families with hMSH6 mutations than in fam-lies with hMSH2 and hMLH1 mutations.20 Twenty-sevenamilies had hMSH6 mutations, and the authors found thathe frequency of CRC cancer was less with a median age ofnset that was 10 years later in these patients compared withatients with hMSH2 and hMLH1 mutations. In contrast toRC, the presence of an hMSH6 mutation carried an in-reased risk of non-HNPCC-associated tumors such as pros-ate, lung, and renal cancers. It has also been recognized thatMSH6 mutations are associated with increased incidence ofndometrial cancer and there is an increased risk of extraco-onic cancers with the hMSH2 mutation.1,5 The genetic andlinical heterogeneity among families with HNPCC makes
ocused genetic mutational identifications based on familial shenotype a difficult endeavor, and therefore, a better under-tanding of MSI and its genetic testing implications is re-uired.MSI usually occurs due to abnormalities in the MMR pro-
ess that is crucial to proper cell division during DNA repli-ation. Replication is the process whereby DNA is copied toroceed to cell division or mitosis. Errors of incorrectly pair-
ng DNA base-pairs during this process are known to occur,ossibly as frequently as once in every 103 or 104 base-pair-
ngs.16 Other errors include accidental insertions or deletionsf base-pairs due to failure to correct problems caused byNA-polymerase.5 When any of these errors occur, MMRroteins, a complex and specialized set of proteins that act asroofreaders and repairers, identify and correct any mis-atched or incorrect DNA base-pairs to prevent the error
rom propagating through the cell lines. The genes that codeor these MMR proteins are the autosomal-dominantly inher-ted MMR genes (hMLH1, hMSH2, hMSH6, hPMS1, hPMS2,MLH3, EXO1, and TGF�R2). A germline mutation in onellele of these genes is not manifested until the inactivation oromatic loss of the remaining wild-type allele, which theneads to abnormalities in the MMR system.1,16 Over 400 dif-erent known familial mutations of the MMR genes, includingnumber of known hMSH2 and hMLH1 founder mutations,
an be found on the ICG-HNPCC’s web site: http://www.in-ight-group.org. Based on the data to date, it appears thatach family has its own unique germline mutation (addressedelow).The effect of MMR loss is an accumulation of mutations inicrosatellite regions of the DNA. Microsatellites are short,
andemly repeated sequences of mono-, di-, or trinucleotidesocated primarily in the introns or noncoding regions of theNA and are spread throughout the genome.1,5,15 When
here is variability in the lengths of these regions of the DNAue to insertions or deletions of the repeated segments ofucleotides, it is termed MSI. This phenotype is identified byerforming polymerase chain reaction (PCR) amplificationnd separation by electrophoresis of the particular genesrom the tissue in question. Instead of having two bands, oneor each allele, there may be anywhere from 4 to 10 or moreands. Each band corresponds to an allele that has evidencef MMR that was then passed along to daughter cells, whichubsequently allowed further errors in replication and thusxpanded nucleotide repeats (referred to as MSI). When MSIccurs in exons (coding regions of DNA), it is believed to leado abnormalities in the function of multiple genes includingumor suppressor genes, oncogenes, and other cell growthegulators that can lead to neoplastic transformation. TheGF-� type II receptor (TGF�R2) important for cell growth
nhibition was one of the first MSI-affected genes to be iden-ified in the mid-1990s when a correlation between MMRutations and tumor formation was shown.4 Other MSI-
ffected genes that may lead to tumorigenesis in HNPCCnclude the BAX gene important in apoptosis, insulin-likerowth factor II receptor important in cell growth regulation,2F4 key to cell-cycle regulation, and the MMR genes them-elves including hMSH6 and hMLH3.1,16 Despite clarifying
ome of the genes involved in HNPCC, the reason for only
pH
coIetMsiidtfjsshidMdiHpwmtMowfc(wmcitht
GGtawiwmitfdw
rp
cuhttbiw8bHBgogonsH
gpiHaphelaamoH(HatMDtitttswImcibm
140 P.E. Wise and M.G. Mutch
articular organ systems being affected by cancer in mostNPCC patients remains unknown.16
The degree of microsatellite instability in a tumor or tissuean be characterized as MSI high (MSI-H), MSI low (MSI-L),r MSI stable (MSS) based on the use of the National Cancernstitute microsatellite testing panel that includes five differ-nt markers. If two or more of the microsatellite markers onhe panel show allelic instability, the tumor is considered
SI-H; if only one marker has instability, the tumor is con-idered MSI-L, and if no markers have instability, the tumors considered MSS. Microsatellite instability has been used todentify patients who are likely to have HNPCC and to pre-ict the prognosis of both sporadic and HNPCC-related CRCumors. Mutations in the MMR genes normally lead to theormation of MSI-H tumors that are characteristic of the ma-ority of HNPCC CRC as well as approximately 5 to 20% ofporadic CRC. Microsatellite instability-high CRC oftenhow a proclivity for formation of proximal colon cancer withigh differentiation, mucin production, and tumor-infiltrat-
ng lymphocytes. They also appear to have a decreased inci-ence of lymph node and liver metastasis compared withSI-L and MSS tumors. In addition, MSI-H tumors have
ifferent responses to chemotherapy and show an overallmproved prognosis,15,18,21 whether the tumor is related toNPCC or not.13-15 The majority of MSI-H tumors (85%) inopulation testing do not come from patients with HNPCC,hich is thought to be due to hypermethylation of the pro-oter region of hMLH1 (rather than a germline mutation)
hat leads to positivity on the MSI testing panel.15 MSI-L andSS cancers do not appear to show any differences in terms
f their pathologic or prognostic characteristics, both doingorse than MSI-H cancers.15 The testing for MSI is the basis
or the Bethesda criteria that sets forth recommendations forlinical scenarios in which MSI testing should be performedTable 1).18 Based on the results of MSI testing of the tumor asell as immunohistochemistry (IHC) testing for gene abnor-alities in the tumor tissue in affected patients who fit the
linical HNPCC criteria, the decision to perform genetic test-ng for the disease can be facilitated. If the tumor is MSI-H,he likelihood of identifying a gene mutation of hMLH1 andMSH2 is 60%,7 whereas only 3 to 8% of MSI-L or MSSumors show germline mutations.16
enetic Testingenetic testing to define the underlying MMR gene muta-
ions leading to HNPCC has become more universally avail-ble in the past decade since the above-mentioned genesere first identified. A resource for genetics clinics and test-
ng sites is available through the GeneTests web site: http://ww.genetests.org. In general, genetic testing is recom-ended if the test can be interpreted, the results will
nfluence the care of the family members involved, and theesting methods have been validated.5 If the clinical criteriaor HNPCC have been met, the patient and their family un-erstand the risks and benefits of the testing, and they are
illing to follow surveillance recommendations based on the iesults of the testing, it is felt that gene testing should beerformed.Because of the difficulties with genotype-to-phenotype
orrelations in HNPCC (unlike FAP) and the high cost ofniversal genetic testing on all patients with CRC, researchersave tried to focus on identification of clinicopathologic cri-eria in HNPCC to guide focused genetic testing. As men-ioned previously, the Amsterdam and Bethesda criteria (Ta-le 1) have variable sensitivity and specificity when trying to
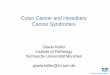
dentify patients with HNPCC gene mutations. For example,hen all five Amsterdam I criteria are met, there is a 25 to6% chance of identifying an hMSH2 or hMLH1 mutation,ut this drops to 16 to 30% if all of the criteria are not met butNPCC is still suspected. Similarly, meeting the first threeethesda criteria showed a 30% likelihood of identifying aene mutation5 (Bethesda criteria being 96% sensitive butnly 27% specific for identifying MSI-H tumors7). Overall,ene mutation testing will be confirmatory in only 45 to 64%f patients who meet the clinical criteria for HNPCC.19 Aumber of algorithms have therefore been constructed totreamline and economize the genetic testing process forNPCC, an example of which is in Figure 1.Most of the available algorithms for testing for HNPCC
ermline mutations involve either direct gene testing of theatient or testing of the patient’s tumor for MSI or gene stain-
ng with IHC. Functional assays of the genes involved inNPCC have not been developed due to the fact that, as an
utosomal-dominant condition, a normal gene allele isresent that may mask the abnormal allele function. Also, itas been shown that tumors with hMSH6 mutations do notxpress the MSH6 protein, so the utility of functional assays isimited. Conversion technology (a process to force a cell intohemizygous state), however, may make useful functional
ssays a reality in the future. Additionally, this technologyay improve the accuracy of gene mutation identification
ver current recognition rates.5,16 The direct gene testing forNPCC is available for hMLH1 and hMSH2 fairly universally
since they are the genes most frequently mutated inNPCC), while hMSH6 testing is only selectively available
nd best performed if the first two genes are normal. Unfor-unately, due to the heterogeneity in the mutations of the
MR genes for each HNPCC family, direct sequencing of theNA is necessary to identify the mutation.5 This is a very
ime-consuming and costly process. Once the defect has beendentified, however, the remaining family members to beested can undergo a more specific and cheaper gene muta-ion evaluation. As a result, MSI and/or IHC evaluations ofhe patient’s tumor have become the most widely acceptedcreening method to create a cost-effective means to identifyho would best benefit from direct gene testing. The use of
HC testing on the tumor tissue (actual staining for the threeain genes mutated in HNPCC) has been additive when
ombined with tumor testing for MSI and may offer insightnto the MMR gene that is mutated.1,5,7,16 MSI testing itself isased on sequence testing for the National Cancer Instituteicrosatellite panel. The cost-effectiveness of using MSI test-
ng to identify HNPCC gene mutations and potentially offer a

se
twheticbMft(bpatipftsmn
limeiwHofph
GAidtmbffctH
. Gastr
Hereditary nonpolyposis colorectal cancer 141
urvival advantage has been well-established in various mod-ls.7,22-24
Therefore, as outlined in Fig 1, it is recommended to starthe evaluation for the underlying gene mutation in a patientho is at risk for a germline mutation based on their familyistory and clinical criteria (the most important aspect of thevaluation24). Direct DNA sequencing can be performed ifhere are sufficient clinical criteria for the patient being stud-ed (Bethesda criteria) or if tumor tissue is not available. If theriteria are not as impressive, MSI testing of the tumor shoulde performed to show whether it is MSI-L or MSS versusSI-H. Because only 3 to 8% of MSI-L or MSS tumors in
amilies with clinical criteria for HNPCC have germline mu-ations,16 further testing can usually be avoided for this groupbut potentially still leave the patient in a high-risk groupased on clinical criteria). In combination with IHC for theossible genes involved, however, gene mutation analysis forpatient with an MSI-H tumor should then be performed
hrough direct DNA sequencing.24 If an MMR gene mutations identified in the initial at-risk patient, it is recommended toroceed with focused gene testing on the remaining at-riskamily members. If they are negative for the gene mutation,hey may be screened for cancers in a fashion similar to thecreening for high-risk individuals. If they have the geneutation identified, this is diagnostic of HNPCC, and they
Figure 1 Algorithm for gene mutation identification in HWM: Genetic testing for high-risk colon cancer patients
eed to follow the intensive screening recommendations out- i
ined below. If an MMR gene mutation is not identified in thenitial at-risk patient, further testing of other at-risk family
embers is not warranted. It should be remembered, how-ver, that based on the sensitivity of current DNA tests (rang-ng from 50 to 95%), the possibility of a sporadic cancerithin an HNPCC family, or the possibility that a phenotypicNPCC family may not have an identifiable genotypic etiol-gy, a negative mutational analysis does not mean that theamily does not have a predisposition to form cancers.5 Theseatients should undergo surveillance as if they have a familyistory and clinical criteria concerning for HNPCC.
enetic Counselingn important aspect of genetic testing is the genetic counsel-
ng that should be performed with it. Counseling is crucial toeal with the complex issues that arise when patients andheir family members are informed that they have a geneutation that may lead to cancer formation. It is therefore
elieved that extensive counseling should be given and in-ormed consent obtained before any genetic testing is per-ormed as well as after the results are given.1,5,25 Lynch andoworkers identified a number of psychosocial issues relatedo genetic testing when 199 members of seven knownNPCC families were surveyed.25 These included the follow-
(used with permission from W.B. Saunders from Gradyoenterology 124: 1583, 2003).
NPCC
ng: concerns regarding insurability, family pressure for seek-

isugpcftccaksvHf(hipc
tsrrmmpjakHcauoaHac
CCRhopnttHiavs
Ncbotlfintfotsffascamps2lcc
otHwntatssinceatkaci3Cctoarmcc
142 P.E. Wise and M.G. Mutch
ng testing (either from or on the identified proband), unre-olved grief (due to multiple family members havingntimely cancer or deaths), family solidarity, and survivoruilt (seen in those with a negative gene test). These sameatients also helped to identify barriers to screening that in-luded lack of insurance, denial and other psychological de-ense mechanisms, and physical discomfort with screeningests.25 While counseling can alleviate or avoid many of theseoncerns and issues, some are outside the realm of the clini-ian to resolve. This is often the case with patient concernsbout affects of genetic testing on insurability, despite fewnown cases of discrimination based on genetic testing re-ults. This discrimination remains the greatest concernoiced by patients in studies on genetic counseling forNPCC.25-27 One limited survey demonstrated that these
eelings may in fact be well-founded. Despite the majority98%) of insurance providers showing willingness to insureypothetical HNPCC patients and their relatives (often with
ncreased premiums), 45% stated they would not cover pro-hylactic colectomy and 33% would not cover more frequentolonoscopies.26
In order for genetic counseling to be effective, it must leado acceptance of genetic testing followed by appropriatecreening in those who test positive for gene mutations. Ineality, the acceptance of gene testing by at-risk patientsanges from 43 to 75%2,27,28 and the compliance with recom-ended increased surveillance for those shown to have geneutations is at best 75%.2 Clearly this counseling should beerformed by well-educated practitioners given that the ma-
ority of physicians in one survey did not know about thevailability of genetic testing for HNPCC and fewer actuallynew the recommended surveillance or screening forNPCC patients who had gene mutations.2 Having dedi-
ated genetic counselors available also ensures that appropri-te family pedigrees are obtained to identify at-risk individ-als, that appropriate testing is done, and that the tests areptimally interpreted and utilized.5 Furthermore, physiciannd patient education must be a future priority both forNPCC as well as for other hereditary cancer syndromes to
ttempt to improve the morbidity and mortality from theseonditions.
ancer Surveillanceolorectal Cancer Screening
ecommendations about colonic surveillance for HNPCCave changed only slightly in the past decade, partly becausef retrospective data supporting the original protocols andartly because of a lack of improvement in diagnostic tech-iques. Full colonic evaluation with sigmoidoscopic evalua-ion and barium enema or full colonoscopy is necessary dueo the predominance of right-sided colonic lesions inNPCC.4,5 Most of the initial protocols for CRC surveillance
n HNPCC have been based on retrospective cohort analyses,nd few have shown evidence of survival benefit from sur-eillance despite showing earlier CRC identification. Initial
tudies by Renkonen-Sinisalo and coworkers11 and de Vos tot sederveen Cappel and coworkers10 supported that CRCould be identified at earlier stages (thus potentially havingetter prognosis) with surveillance versus none. However,verall survival was not significantly impacted, and six pa-ients in each author’s surveillance cohort developed cancersess than 24 months after a negative colonoscopy (as well asve and nine cancers identified between 2 and 3 years afteregative surveillance, respectively). This prompted both ofhese groups to conclude that increasing the colonoscopicrequency to 1 to 2 years might increase the earlier detectionf CRC.10,11 The recognition of cancers so early after a nega-ive-screening colonoscopy underlies two concerns aboutcreening for CRC. The first is the established acceleratedormation of adenomas in HNPCC and their quicker trans-ormation to cancer, especially in comparison to sporadicdenomas.1,29 Studies on adenoma formation in HNPCChowed new (or previously missed) adenomas after a “clean”olonoscopy being found at a mean of 48 months and newdenomas after previous polypectomy were identified at aean of 16 months.1 A second concern is the rate of missedolyps due to inadequate prep, inadequate colonoscopickills, or difficult accessibility that was noted to be as high as7% for 3-mm adenomas in one study5 and 29% for polyps
ess than 5 mm in another.3 The impact of newer measures ofolonic evaluation such as computed tomographic (CT)olonography (virtual colonoscopy) is unclear.30
Jarvinen and coworkers were the first to show an impactn CRC survival with colonoscopy in a 15-year follow-up ofheir HNPCC patients (133 subjects and 119 controls in 22NPCC families) by comparing those patients who under-ent routine colonoscopy and those who chose not to.9 Theyoted a 62% decrease in CRC incidence, a likelihood of iden-ifying the cancers at an earlier stage, and an overall mortalitydvantage of 65% with colon surveillance every 3 years. Al-hough they did not conclude that the screening frequencyhould be shortened, they did note that adequate colonicurveillance and CRC prevention may lead to a greater man-festation of extracolonic malignancies, thus increasing theeed for adequate screening for these tumors. Overall, theurrent consensus recommendations are for full colonoscopyvery 1 to 2 years (some recommend yearly8) beginning atge 25 (or 5 years earlier than the earliest cancer developed inhe HNPCC family, whichever is first) in patients with anown MMR gene mutation, and increasing to every year atge 35 to 40.6 This is altered only slightly for individuals withlinical criteria for HNPCC without genotypic confirmationn that the biennial exams should start between ages 20 and0 years (or 5 years before the earliest diagnosed familialRC) and convert to yearly at age 40.1,5 Based on the lowomplication rate of colonoscopic evaluation and polypec-omy (even with the slightly increased risk due to the numberf studies required over a 25-year time span5) and the limiteddverse effects on quality of life (QOL),31 there should be feweal impediments to compliance with these screening recom-endations beyond concern for the preparation and fear of
ancer discovery. To the contrary, Syngal and coworkersoncluded from their Markov model that colonoscopy
howed the greatest improvement in QOL and improved
oHbep
sipicfpdimswit
EBtibcaccrmtmmphrAeHrthpdamt
eiautit
todoocvosa
OCrplvctalptsb
TTttatrHiwdwsfseacmta
tpBc(Hr
Hereditary nonpolyposis colorectal cancer 143
verall survival in comparison to no surveillance forNPCC.31 In addition, colonic screening has been shown toe more cost-effective than no surveillance.5 Unfortunately,ven in HNPCC patients with proven gene mutations, com-liance with screening recommendations is not 100%.2
In patients who have undergone colectomy, yearly endo-copic or radiologic evaluation of the remaining large bowels necessary due to the high rate of metachronous CRCs inatients with HNPCC (see below). The colonoscopic screen-
ng should be continued in all patients with any remainingolon or rectum until at least age 75 and can be adjusted inrequency or terminated based on patient comorbidities andersonal preference.5,6 For those patients who cannot un-ergo regular surveillance due to anatomic or compliance
ssues, prophylactic colectomy can be considered.1,5,30 Thisay also be an option for patients with undue psychological
tress due to the fear of cancer development, but difficultiesith fecal incontinence, irritable bowel syndrome, or signif-
cant comorbidities might preclude prophylactic colec-omy.1,30
xtracolonic Cancer Screeningecause gynecologic malignancies (uterine and ovarian) arehe second most common in HNPCC, and the most commonn women with the disease, screening recommendations haveeen made for these malignancies. Unfortunately, as witholonic screening, these are based on retrospective case seriesnd anecdotes due to the lack of prospective data. Unlikeolon screening, however, these malignancies are more diffi-ult to diagnose due to a lack of effective screening tools. Theecommendations may be altered based on the patterns ofalignancy in each particular HNPCC family to focus on
hose malignancies most likely to occur, but all potentialalignancies should be screened. Particular gene mutationsay also have an impact on the type of malignancies to ex-ect in each family (eg, hMSH6 mutation carriers may be atigher risk for endometrial cancer and hMSH2 mutation car-iers may be at high risk for extracolonic cancers in general).5
nnual surveillance including transvaginal ultrasound andndometrial biopsy (�80% sensitivity and specificity in non-NPCC postmenopausal women), and measurement of se-
um CA-125 should begin at age 25 to 35 (or 5 years beforehe youngest affected family member), depending on familyistory.1,5,29 Although prophylactic hysterectomy and oo-herectomy have not been recommended based on availableata (no evidence of improvement in cancer-related or over-ll survival), performing this at the time of CRC resectionay be advocated for some women, especially after comple-
ion of child-bearing.1,5,29
Screening for other extracolonic malignancies includessophagogastroduodenoscopy (EGD) for gastric cancer start-ng between ages 30 and 50 (or 5 years before the earliestffected family member) and continuing every 2 to 3 yearsntil age 75. This is especially important in areas where gas-ric cancer is endemic or in HNPCC kindreds with a highncidence of gastric cancer.1,5 With a family history of transi-
ional cell cancer of the ureter or renal pelvis, recommenda- aions include yearly urine cytology and renal ultrasound withr without cystoscopy. Small bowel cancer surveillance isifficult and requires contrasted small bowel follow-throughr capsule endoscopy when symptoms arise as there are nother surveillance recommendations available. Bile duct can-er, much like small bowel cancer, does not have stated sur-eillance recommendations beyond yearly liver function lab-ratory assessment. Dermatologic assessment for basal orquamous cell cancer is also recommended when appropri-te.
perationsontroversy exists over the surgical treatment of HNPCC-
elated CRCs. This is focused on the choice of colectomy besterformed for HNPCC and the appropriateness of “prophy-
actic” colectomy, a colectomy performed in an at-risk indi-idual despite the lack of gross pathology in the colon. Theseontroversies exist primarily because of the lack of prospec-ive data and randomized trials regarding the surgical man-gement of HNPCC. Further complicating the issues are theack of 100% effective surveillance techniques and variableatient compliance to the ones that are available. Therefore,he debate over these subjects will likely remain until pro-pective, comparative studies with adequate sample size cane performed—a prospect that may not come to fruition.
ype of Resectionhe initial question in relation to the surgical choice for pa-
ients with HNPCC is whether CRC in this setting should bereated differently than in patients with sporadic CRC. Mostuthors agree that, depending on the age and health status ofhe patient involved, due to the high metachronous cancerisk after segmental resection for CRC in a patient withNPCC (especially with genetic confirmation), total abdom-
nal colectomy (TAC) with ileorectal anastomosis for CRCould be advised.29,30,32-37 This metachronous risk has beenetermined to range from 10 to 50% in retrospective studiesith long follow-up, but appears to be 15 to 17% in most
tudies.4,5,30,33,35,37,38 There is more controversy about per-orming TAC for HNPCC patients with endoscopically re-ectable adenomas and extracolonic malignancies withoutvidence of CRCs,30 and therefore, these situations must beddressed with each individual patient based on their age,omorbidities, and pattern of cancers within each family. Itust be underscored that regardless of the surgical approach,
he patient must have lifelong surveillance of their remainingt-risk mucosa in the large intestine.
The choice of TAC must be made with the understandinghat surveillance of the remaining rectum should continueostoperatively. This is based on the data from Rodriguez-igas and coworkers, showing an 11% incidence of rectalancer in 71 patients over a median follow-up of 158 monthsmedian age at rectal cancer diagnosis: 51 years) after TAC forNPCC.39 They therefore estimated the risk of developing
ectal cancer to be 3% every 3 years for the first 12 years. Lee
nd coworkers later reported on an HNPCC registry-based
rhooOnpfs2ydseHct
aThavsqscqswbpfsmectcsslacinvHstrolwet“H
reiapfim
PPtpocgpntctFwtpmmce(rtttQh(ioit
wcstcdiQcolttde
144 P.E. Wise and M.G. Mutch
eview that identified 28% (25 of 89) of HNPCC patients asaving a rectal cancer during their lifetime (overall incidencef 8% metachronous rectal cancer in their registry) and thatne in five developed rectal cancer as their index cancer.32
ne study, however, by Van Dalen and coworkers, showedo metachronous rectal cancers in a cohort of 33 HNPCCatients at the Cleveland Clinic after TAC with proctoscopicollow-up over 14 years.37 Other retrospective reviews havehown metachronous rectal cancer rates ranging from 3.4 to0% after colectomy with a mean follow-up of at least 5ears.10,32 Because of these risks, there have been recommen-ations for proctocolectomy with ileal pouch anal anastomo-is (IPAA) in selected cases of HNPCC with rectal cancer, andven as the elective procedure of choice in some patients withNPCC.29,30,35 It should be noted that the rate of rectal can-
er in HNPCC is similar to that in FAP where elective proc-ocolectomy is the procedure of choice.5,30
The discussion about type of colectomy to perform shouldlso be within the context of the potential QOL impact of aAC versus a segmental resection or proctocolectomy. Thereave been recent reports suggesting that QOL informationnd the inadequacy of at least decade-old colonoscopic sur-eillance data on which many authors’ conclusions are basedhould bring the recommendations for TAC for CRC intouestion.40 Initial attempts to evaluate the impact of colonicurveillance versus types of elective colectomy by Syngal andoworkers, using a Markov model, showed that QOL (inuality-adjusted life years) was better with routine colono-copic surveillance while length of survival was extendedith colectomy (without pathology) at an early age.31 Theseenefits became negligible as the model was tested on olderatients with HNPCC, especially if the colectomy was per-ormed for CRC. These authors concluded that comprehen-ive discussions about risks and benefits and impact on QOLust be held with each patient, as their individual prefer-
nces are crucial to the final decision about the extent ofolectomy to be performed.31 A similar Markov model fromhe Netherlands looking just at life expectancy without QOLonsiderations found that using more specific cancer risk andurvival probabilities for HNPCC than the previous studyhowed a 4.7-year survival advantage for elective proctoco-ectomy and 3.4-year survival advantage for elective totalbdominal colectomy at the time of diagnosis of a Dukes’ Aancer in a 27-year-old patient versus segmental colectomyn the same patient. This life expectancy advantage becameegligible in older patients (67-year-old) with more ad-anced tumors (Dukes’ C).35 They concluded that youngerNPCC patients would benefit from subtotal colectomy over
egmental resection for CRC (and over proctocolectomy dueo the “worse functional results” and the greater morbidityisk of IPAA, but this was not tested in the model), whereaslder patients should undergo segmental resection.35 A fol-ow-up commentary on this study by Olschwang and co-orkers pointed out that the relatively small increase in life
xpectancy after a more extensive resection could not justifyhe decreased QOL during that time and they stated that. . .the conclusions of the French Ad-Hoc Committee [on
NPCC] are that not only are routine extended prophylactic aesections not recommended but, on the contrary, given thefficacy of screening programs, extended surgery is also notndicated.”40 Unfortunately, as mentioned previously, therere no prospective trials comparing surveillance with TAC,roctocolectomy, or segmental colectomy to be able to formrm conclusions. Therefore, the informed consent processust be extensive and involve all of the above considerations.
rophylactic Colectomyerforming a total abdominal colectomy or total proctocolec-omy in an HNPCC patient who has no evidence of colonicathology on endoscopic screening has been another subjectf great controversy. This “prophylactic” procedure has re-eived greater acceptance in those patients with confirmedene mutations.30,33,36 The controversy has related to thehenotypic–genotypic variability of HNPCC. Unlike theear 100% phenotypic penetrance of FAP in which colec-omy is easier to justify in the face of the presence of multipleolonic polyps, HNPCC has an 80 to 90% penetrance, withhe mean age of CRC forming by 46 years.5,7,30 Also unlikeAP, with HNPCC there is no way to tell on a genetic levelhether a mutation carrier will fall into the approximately 10
o 20% who will not form a CRC. Therefore, the decision toerform prophylactic colectomy must be based on familialanifestations of the disease, our knowledge of phenotypicanifestations based on genotypic mutations, and patient
haracteristics (age, psychological status, comorbidities,tc.). Interestingly, in a survey of cancer genetics specialistsprimarily counselors) by Matloff and coworkers, 17.4% ofespondents stated they would have a prophylactic colec-omy if they were positive for an HNPCC gene mutation. Onhe other hand, 61.3% would not have a prophylactic colec-omy due to the believed adequacy of surveillance and theOL issues related to colectomy.41 This same group wouldave or would recommend prophylactic hysterectomy54.1%) and/or oopherectomy (52.4%), primarily due to thenadequacy of surveillance of these organs and lack of impactn body image. It is unclear if these beliefs would have anmpact on these counselors’ recommendations to their pa-ients.41
Many authors will recommend prophylactic colectomyhen there are extenuating circumstances such as a patient’s
ancer fears, poor surveillance compliance, or difficulty withurveillance due to anatomic or other reasons that outweighhe potential risks of the procedure.1,5,30 If the informed de-ision to proceed with prophylactic colectomy is made, theecision as to who will pay for the operation30 and potential
mpact it may have on future employment, insurability, andOL must be discussed preoperatively—much like the dis-
ussion held before genetic testing.38 The best timing of theperation has not been defined,38 but we know that QOL andife expectancy advantages are diminished as patients reachheir late 40s in comparison to their mid to late 20s based onhe aforementioned Markov models.31,35 Timing may best beetermined based on the cancer development patterns ofach respective HNPCC family.30 Prophylactic colectomy is
lso gaining favor now that minimally invasive techniques are
bfchap
wdncetaf(aowtM
CBpmpmommtsasuasa
CsdectaPhlrjHtalH
CHowttsuvstaiFtbpidttHppat
R
1
1
1
Hereditary nonpolyposis colorectal cancer 145
ecoming more ubiquitous,36 although changing indicationsor colectomy based on availability of a particular approachan be fraught with difficulties.30 The laparoscopic approachas not been shown to decrease the potential complicationsssociated with an operation the magnitude of a TAC orroctocolectomy.Concerns about prophylactic colectomy (whether TAC
ith ileorectal anastomosis or proctocolectomy with IPAA)ue to the associated potential morbidity and mortality haveot stopped some authors from recommending prophylacticolectomy for all appropriate young gene mutation carri-rs,30,33 equating the risks with those of prophylactic colec-omy in FAP. Other authors have been reticent to make suchblanket statement and only recommend TAC for HNPCC
or gene mutation carriers with phenotypic manifestationstherefore not truly “prophylactic”),7,34,38 while others believenything beyond segmental colectomy and appropriate post-perative surveillance should be abandoned.40 Dunlop put itell when he stated that “at present there are insufficient data
o recommend for or against primary prophylactic surgery inMR gene carriers.”6
hemopreventionecause of the controversy over the extent of colectomy whenathology becomes apparent with HNPCC and the potentialorbidity with prophylactic colectomy, many patients andhysicians have sought alternative means by which to mini-ize CRC risk and maximize surveillance effectiveness. One
f the tools that has been effective in reducing adenoma for-ation and therefore possibly reduce sporadic CRC is che-oprevention. Although not all of these agents have been
ested in prospective, controlled trials, aspirin and other non-teroidal antiinflammatory drugs (NSAIDs), calcium, folate,nd oral estrogens have all shown promising results.42 Whileome of these agents have shown effectiveness in FAP, theirtility in HNPCC is yet unknown.5,42 In addition, their mech-nisms of action have not been elucidated, and their potentialide effects are not completely understood and must be bal-nced against their apparent protective effects.29,42
Chemoprevention trials for HNPCC have been limited.alcium carbonate has been tested and shown not to have a
ustained response in patients with familial cancer syn-romes.5 There are studies currently ongoing in humans toxamine the utility of NSAIDs in the setting of HNPCC. Spe-ifically, there are randomized, prospective Phase I and IIrials on both celecoxib (a cyclooxygenase-2 inhibitor) andspirin and resistant starch (the CAPP2, Concerted Actionolyp Prevention-2, trial) in HNPCC patients.1,5 NSAIDsave actually shown promise when applied to tumor cell
ines with defects in hMLH1, hMSH2, and hMSH6, but theseesults will obviously require substantiation in human sub-ects.1 The inability to create an effective animal model forNPCC has also limited chemoprevention research.1 Until
he results of the human studies are available or an adequatenimal model is discovered, use of these and the other agentsisted above cannot be widely advocated for patients with
NPCC. 1onclusionNPCC has been crucial to the understanding of the geneticsf CRC. From the infancy of the understanding of the diseasehen linkage analysis combined with MSI testing confirmed
he presence of MMR genes and their potential impact onumorigenesis to the use of the Bethesda criteria and micro-atellite panels to identify patients eligible for gene testing,nderstanding of the patients affected by the disease has re-olved around genetics. This has in turn impacted the under-tanding of sporadic CRC tumorigenesis. The genetic basis ofhe disease has also helped to evolve and impact not only thert of genetic counseling but also the understanding of thempact on cancer surveillance on survival of at-risk patients.urther impact will be made by studying other gene muta-ions linked to the disease, identifying better correlationsetween genotype and phenotype with HNPCC, performingrospective comparative studies of testing algorithms, gain-
ng a better understanding of the import of the extracoloniciseases linked with various gene mutations, and studyinghe use of chemopreventive agents in the disease. Perhapshere will be ways in the future to manipulate the genetics ofNPCC to prevent its phenotypic manifestations. Most im-ortantly though, from a public health standpoint, will berospective studies looking at the impact of genetic testingnd public and physician education on the survival of pa-ients with HNPCC and others at risk for CRC.
eferences1. Yu HJA, Lin KM, Ota DM, et al: Hereditary nonpolyposis colorectal
cancer: preventive management. Cancer Treat Rev 29:461-470, 20032. Halbert CH, Lynch H, Lynch J, et al: Colon cancer screening practices
following genetic testing for hereditary nonpolyposis colon cancer(HNPCC) mutations. Arch Intern Med 164:1881-1887, 2004
3. Lynch HT, Lynch JF: Lynch syndrome: history and current status. DisMarkers 20:181-198, 2004
4. Nagy R, Sweet K, Eng C: Highly penetrant hereditary cancer syn-dromes. Oncogene 23:6445-6470, 2004
5. DeFrancisco J, Grady WM: Diagnosis and management of hereditarynon-polyposis colon cancer. Gastrointest Endosc 58(3):390-408, 2003
6. Dunlop MG: Guidance on gastrointestinal surveillance for hereditarynon-polyposis colorectal cancer, familial adenomatous polyposis, juve-nile polyposis, and Peutz-Jeghers syndrome. Gut 51:v21-v27, 2002(suppl V)
7. Moslein G, Pistorius S, Saeger HD, et al: Preventive surgery for coloncancer in familial adenomatous polyposis and hereditary nonpolyposiscolorectal cancer syndrome. Langenbecks Arch Surg 388:9-16, 2003
8. Lynch HT, Shaw TG, Lynch JF: Inherited predisposition to cancer: ahistorical overview. Semin Med Genet 129C:5-22, 2004
9. Jarvinen HJ, Aarnio M, Mustonen H, et al: Controlled 15-year trial onscreening for colorectal cancer in families with hereditary nonpolyposiscolorectal cancer. Gastroenterology 118:829-834, 2000
0. Vos tot Nederveen Cappel WH, Nagengast FM, Griffioen G, et al:Surveillance for hereditary nonpolyposis colorectal cancer. Dis ColonRectum 45(12):1588-1594
1. Renkonen-Sinisalo L, Aarnio M, Mecklin JP, et al: Surveillance im-proves survival of colorectal cancer in patients with hereditary nonpol-yposis colorectal cancer. Cancer Detect Prev 24(2):137-142, 2000
2. Bertario L, Russo A, Sala P, et al: Survival of patients with hereditarycolorectal cancer: comparison of HNPCC and colorectal cancer in FAPpatients with sporadic colorectal cancer. Int J Cancer 80:183-187,1999
3. Lim SB, Jeong SY, Lee MR, et al: Prognostic significance of microsatellite

1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
146 P.E. Wise and M.G. Mutch
instability in sporadic colorectal cancer. Int J Colorectal Dis19:533-537, 2004
4. Popat S, Hubner R, Houlston RS: Systematic review of microsatelliteinstability and colorectal cancer prognosis. J Clin Oncol 23:609-618,2005
5. Raut CP, Pawlik TM, Rodriguez-Bigas MA: Clinicopathologic featuresin colorectal cancer patients with microsatellite instability. Mutat Res568:275-282, 2004
6. Chung DC, Rustgi AK: The hereditary nonpolyposis colorectal cancersyndrome: genetics and clinical implications. Ann Intern Med 138(7):560-571, 2003
7. Weinberg DS, Newschaffer CJ, Topham A: Risk for colorectal cancerafter gynecologic cancer. Ann Intern Med 131(3):189-193, 1999
8. Umar A, Boland CR, Terdiman JP, et al: Revised Bethesda guidelines forhereditary nonpolyposis colorectal cancer (Lynch syndrome) and mi-crosatellite instability. J Natl Cancer Inst 96(4):261-268, 2004
9. Giardello FM, Brensinger JD, Petersen GM: AGA technical review onhereditary colorectal cancer and genetic testing. Gastroenterology 121:198-213, 2001
0. Plaschke J, Engel C, Kruger S, et al: Lower incidence of colorectalcancer and later age of disease onset in 27 families with pathogenicMSH6 germline mutations compared with families with MLH1 or MSH2mutations: the German Hereditary Nonpolyposis Colorectal CancerConsortium. J Clin Oncol 22:4486-4494, 2004
1. Umar A: Lynch syndrome (HNPCC) and microsatellite instability. DisMarkers 20:179-180, 2004
2. Kievit W, de Bruin JHFM, Adang EMM, et al: Cost effectiveness of a newstrategy to identify HNPCC patients. Gut 54:97-102, 2005
3. Ramsey SD, Clarke L, Etzioni R, et al: Cost-effectiveness of microsatel-lite instability screening as a method for detecting hereditary nonpol-yposis colorectal cancer. Ann Intern Med 135(8):577-588, 2001
4. Jagadeesh D, Syngal S: Genetic testing for hereditary nonpolyposiscolorectal cancer. Curr Opin Gastroenterol 19:57-63, 2003
5. Lynch HT, Watson P, Shaw TG, et al: Clinical impact of moleculargenetic diagnosis, genetic counseling, and management of hereditarycancer: Part II: hereditary nonpolyposis colorectal carcinoma as amodel. Cancer 86:2457-2463, 1999 (suppl 11)
6. Rodriguez-Bigas MA, Vasen HFA, O’Malley L, et al: Health, life, anddisability insurance and hereditary nonpolyposis colorectal cancer.Am J Hum Genet 62:736-737, 1998
7. Hadley DW, Jenkins J, Dimond E, et al: Genetic counseling and testingin families with hereditary nonpolyposis colorectal cancer. Arch Intern
Med 163:573-582, 20038. Lerman C, Hughes C, Trock BJ, et al: Genetic testing in families withhereditary nonpolyposis colon cancer. JAMA 281(17):1618-1622,1999
9. Burke W, Petersen G, Lynch P, et al: Recommendations for follow-upcare of individuals with an inherited predisposition to cancer. JAMA277(11):915-919, 1997
0. Church JM: Prophylactic colectomy in patients with hereditary non-polyposis colorectal cancer. Ann Med 28:479-482, 1996
1. Syngal S, Weeks JC, Schrag D, et al: Benefits of colonoscopic surveil-lance and prophylactic colectomy in patients with hereditary nonpol-yposis colorectal cancer mutations. Ann Intern Med 129(10):787-796,1998
2. Lee JS, Petrelli NJ, Rodriguez-Bigas M: Rectal cancer in hereditary non-polyposis colorectal cancer. Am J Surg 181:207-210, 2001
3. Lynch HT: Is there a role for prophylactic subtotal colectomy amonghereditary nonpolyposis colorectal cancer germline mutation carriers?Dis Colon Rectum 39:109-110, 1996
4. DeCosse JJ: Surgical prophylaxis of familial colon cancer: prevention ofdeath from familial colorectal cancer. J Natl Cancer Inst Monogr 17:31-32, 1995
5. Vos tot Nederveen Cappel WH, Buskens E, van Duijvendijk P, et al:Decision analysis in the surgical treatment of colorectal cancer due to amismatch repair gene defect. Gut 52:1752-1755, 2003
6. Pocard M, Pomel C, Lasser P: Laparoscopic prophylactic surgery forHNPCC gene mutation carrier: has the time come? Lancet Oncol4:637-638, 2003
7. Van Dalen R, Church J, McGannon E, et al: Patterns of surgery inpatients belonging to Amsterdam-positive families. Dis Colon Rectum46:617-620, 2003
8. Rodriguez-Bigas M: Prophylactic colectomy for gene carriers in hered-itary nonpolyposis colorectal cancer: has the time come? Cancer 78(2):199-201, 1996
9. Rodriguez-Bigas MA, Vasen HFA, Pekka-Mecklin J, et al: Rectal cancerrisk in hereditary nonpolyposis colorectal cancer after abdominal co-lectomy. Ann Surg 225(2):202-207, 1997
0. Olschwang O, Laurent-Puig P, Eisinger F, et al: An alternative to pro-phylactic colectomy for colon cancer prevention in HNPCC syndrome.Gut 54:169-173, 2005
1. Matloff ET, Shappell H, Brierley K, et al: What would you do? Special-ists’ perspectives on cancer genetic testing, prophylactic surgery, andinsurance discrimination. J Clin Oncol 18(12):2484-2492, 2000
2. Janne PA, Mayer RJ: Chemoprevention of colorectal cancer. N Engl
J Med 342(26):1960-1968, 2000