Embed Size (px)
Citation preview
Journal of Surgical Oncology 41:256-262 (1989)
Hepatocellular Carcinoma: Some Aspects to Improve Long-Term Survival
XIN-DA ZHOU, MD, ZHAO-YOU TANG, MD, YE-QIN YU, MD, ZENG-CHEN MA, MD,
BING-HUI YANG, MD, JI-ZHEN LU, MD, AND ZHI-YING LIN, MD
From the Liver Cancer Institute, Shanghai Medical University, Shanghai, People’s Republic of China
Sixty-six patients surviving over 5 years after resection of hepatocellular carcinoma (HCC) are investigated. Of them, subclinical stage amounted to 56.1% (37/66) and moderate stage to 43.9% (29/66). There were 35 cases with small HCC (5 5 cm). Cirrhosis was present in 81.1% (54/66). Radical resection was performed in 98.5% (65/66) and palliative resection in 1.5% (1/66). Reoperation for subclinical recurrence and solitary pul- monary metastasis was done in 14 patients, and sequential resection of huge tumors, in three patients. By the end of June 1988, follow-up varied from 60 to 319 months (mean, 115 months); 80.3% of the patients (53/66) are still alive and free of disease; 19.7% (13/66) died with disease. The majority of long-term survivors have returned to their original work; some young patients got married after resection of small HCC 10 years ago, and some can even play football again. Some aspects to improve long-term survival are discussed.
KEY WORDS: limited resection, recurrence, reoperation
INTRODUCTION
Hepatocellular carcinoma (HCC) is seen frequently in China and other Asian countries. Since most patients in these areas have associated liver cirrhosis or a related liver disease [ 1 1, the long-term results of surgical treat- ment have been far from satisfactory compared with those reported from Western series dealing mostly with noncirrhotic patients [2]. However, the remarkable ad- vances in early diagnosis using alpha-fetoprotein (AFP) serosurvey and imaging techniques in the last decade have made it possible to discover relatively small HCC more frequently in China [3,4]. Although major hepatic resection is usually contraindicated in cirrhotic patients [5-81, most patients with small tumors can be success- fully treated by nonanatomical minor hepatectomy [9- 111, which has yielded higher resectability, lower oper- ative mortality, and encouraging 5 year survival [12]. Furthermore, reoperation for subclinical liver recurrence or solitary pulmonary metastasis after a radical resection seems acceptable with further prolongation of survival [ 131. Moreover, multimodality palliative surgery and new modality treatment have provided an opportunity to
0 1989 Alan R. Liss, Inc.
convert nonresectable to resectable HCC [ 14,151. Thus, overall HCC prognosis has progressed.
In this article, we report 66 cases surviving over 5 years after resection of HCC. Some aspects to improve long-term survival are discussed.
MATERIALS AND METHODS A total of 566 cases with pathologically proven pri-
mary liver cancer (PLC) were collected from the Zhong Shan Hospital of Shanghai Medical University in the past 25 years, from July 1958 to June 1983. Of these, 43.6% (247/566) resected and 26.7% (66/247) survivors consti- tute the material of this study. The diagnosis was con- firmed by light microscopic examination, all being HCC. The patients ages ranged from 20 to 60 years (median, 45 years), and the male: female ratio was 5: l .
Accepted for publication January 27, 1989. Address reprint requests to Xin-da Zhou, MD, Liver Cancer Institute, Zhong Shan Hospital, Shanghai Medical University, Shanghai 200032, People’s Republic of China.
HCC: Improve Long-Term Survival 257
patients received four operations for HCC recurrence or metastasis.
Routine preoperative medication was given for 2 days [20]. An uneventful postoperative course was observed in patients undergoing local resection, left lateral seg- mentectomy , and left hemihepatectomy in a noncirrhotic liver. Intensive care with albumin or plasma, fresh blood, and coagulants was, however, necessary in pa- tients receiving right hemihepatectomy in cirrhotic liver. Postoperative adjuvant therapy with Chinese traditional medicine in combination with chemotherapy and/or im- munotherapy was given in 58 cases (87.9%). Serum AFP level and ultrasonography were measured every 2-3 months after resection to discover subclinical recurrence or metastasis.
Criteria for clinical staging was defined as follows: stage 1 (subclinical), without obvious HCC symptoms or signs; and stage 2 (moderate), with obvious HCC symp- toms or signs, but without obvious jaundice, ascites, or distant metastases. In this series, subclinical stage was 56.1% (37/66), and moderate stage, 43.9% (29/66). There were 35 cases with small HCC (I 5 cm).
AFP diagnosis criteria for subclinical HCC was as follows: AFP 2 500 ng/ml (radioimmunoassay) persist- ing over 1 month or AFP L 200 ng/ml for more than 2 months, provided alanine aminotransferase (ALT) is nor- mal and pregnancy and gonadal teratoma can be ex- cluded. In this series, preoperative serum AFP study in- dicated that 84.7% of the patients (50/59) had AFP levels 2 200 ng/ml; of these, 82.0% (41/50) had AFP levels P 500 ng/ml.
Liver disease background was noted as follows: with hepatitis history: 54.5% (36/66); of these, 88.9% (32/36) had a hepatitis history of over 5 years. Cirrhosis was present in 81.8% (54/66). Serum hepatitis B surface an- tigen (HBsAg) by reverse passive hemagglutination (RPHA) was observed in 82.7% (43/52).
The positive findings in different measures for local- ization were as follows: radionuclide scan 60.0% (36/60), ultrasonography 64.5% (40/62), and hepatic an- giography 93.8% ( 1 5/16). The tumor was located in the right lobe in 53.0% (35/66), in the left lobe in 39.4% (26/66), in the middle lobe in 3.0% (2/66), and in bilat- eral lobes in 4.5% (3/66).
Types of resection in 66 patients included right hemi- hepatectomy in five cases (7.6%), left hemihepatectomy in 14 cases (21.2%), left lateral segmentectomy in nine cases (1 3.6%), and local resection (any sublobar, how- ever large) in 38 cases (57.6%) of whom 37 had radical resection and one had palliative resection. The radical resection refers to complete removal of the tumor with a resection margin at least 2 cm from the tumor capsule, without grossly identified tumor emboli in portal vein and no tumor residue in the remaining liver tissue or cut surface. In this series, 98.5% (65/66) had radical resec- tion, including one patient who underwent tumor resec- tion by the ne0dymium:yttrium-aluminum-garnet (Nd: YAG) laser [16,17] and two patients who underwent tumor resection by bloodless hepatectomy with organ isolation hypothermic perfusion [ 18,191. One patient (1.5%) underwent palliative resection for HCC in the caudal lobe plus cryosurgery on the cut surface.
Reoperation was done in 25.8% of the patients ( 17/66), including reoperation for subclinical recurrence after an initial radical resection in ten patients and for solitary pulmonary metastasis in four patients, and reop- eration for sequential resection of huge tumor after mul- timodality palliative surgery in three patients. In this se- ries, three patients received three operations and two
RESULTS By the end of June 1988, follow-up varied from 60 to
319 months, with a mean follow-up of 115 months; of them, 80.3% (53/66) are still alive, free of disease; 19.7% (13/66) died from tumor recurrence or metastasis. The majority of long-term survivors have returned to their original work, some young patients got married after resection of small HCC 10 years ago, and some can even play football again.
During the follow-up period, subclinical HCC recur- rence in the remaining liver was detected in ten patients (Table I, nos. 5-14); of them, all but one had reappear- ance of AFP. Among the ten patients with recurrent HCC, eight patients underwent a second hepatic resec- tion and two patients received cryosurgery with liquid nitrogen [21-231. The time span between the first oper- ation and reoperation was from 11 to 106 months (mean, 5 1.1 months). Site of recurrent HCC was in the same lobe of the liver as the first resection in four cases, and in the opposite lobe, in six cases. Survival varied from 60 to 154 months (mean, 89.5 months); six patients are still alive, free of disease, and four patients died from tumor recurrence or metastasis.
Subclinical solitary pulmonary metastasis after resec- tion of HCC was detected in four patients (Table I, nos. 1-4) because of a secondary rise in AFP level. All four patients underwent lobectomy for metastatic tumors. The time span between the first operation and reoperation was from 31 to 64 months (mean, 43.0 months). Sur- vival varied from 91 to 158 months (mean, 125.3 months); two patients are still alive, free of disease, and two patients died from tumor recurrence.
Sequential resection was carried out in three patients (Table I , nos. 15-17). Initially, these patients had huge tumors in the right lobe of the liver and could not tolerate a right hemihepatectomy owing to coexisting cirrhosis. For the first-step operation, hepatic artery ligation (HAL) plus hepatic artery cannulation (HAC) was performed,
258 Zhou et al.
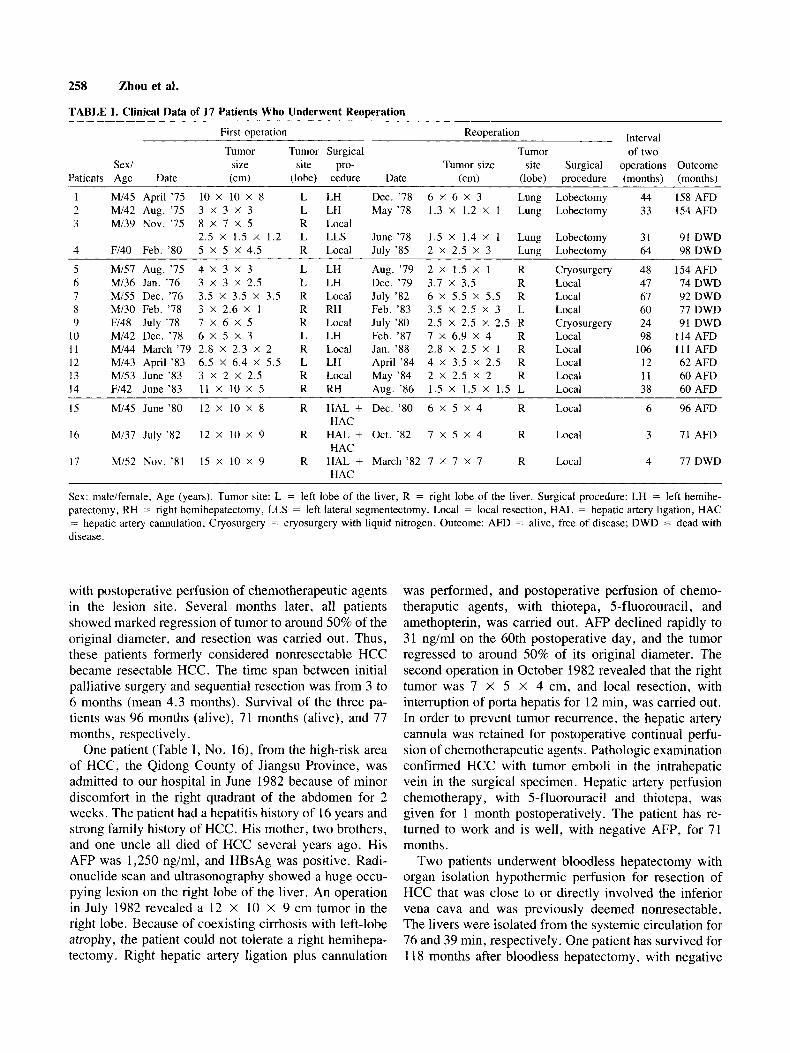
TABLE I. Clinical Data of 17 Patients Who Underwent Reoperation
Interval First operation Reoperation
Tumor Tumor Surgical Tumor of two Sex/ size site pro- Tumor size site Surgical operations Outcome
Patients Age Date (cm) (lobe) cedure Date (cm) (lobe) procedure (months) (months)
I Mi45 April '75 10 X 10 X 8 L LH Dec. '78 6 x 6 x 3 Lung Lobectomy 44 I58 AFD 2 MI42 Aug. '75 3 X 3 X 3 L LH May '78 1.3 X 1.2 X 1 Lung Lobectomy 33 154 AFD 3 Mi39 Nov. '75 8 X 7 X 5 R Local
2.5 x 1.5 x 1.2 L LLS June '78 1.5 x 1.4 X 1 Lung Lobectomy 31 91 DWD 4 Fl40 Feb. '80 5 X 5 X 4.5 R Local July '85 2 X 2.5 X 3 Lung Lobectomy 64 98 DWD
5 M/57 Aug. '75 4 X 3 X 3 L LH Aug. '79 2 X 1.5 X 1 R Cryosurgery 48 154 AFD 6 MI36 Jan. '76 3 X 3 X 2.5 L LH Dec. '79 3.7 x 3.5 R Local 47 74 DWD 7 MI55 Dec. '76 3.5 X 3.5 X 3.5 R Local July '82 6 X 5.5 X 5.5 R Local 67 92 DWD 8 MI30 Feb. '78 3 x 2.6 x 1 R RH Feb. '83 3.5 X 2.5 X 3 L Local 60 77 DWD 9 F/48 July '78 7 X 6 X 5 R Local July '80 2.5 X 2.5 X 2.5 R Cryosurgery 24 91 DWD
10 Mi42 Dec. '78 6 X 5 X 3 L LH Feb. '87 7 X 6.9 X 4 R Local 98 114 AFD 11 M/44 March '79 2.8 X 2.3 X 2 R Local Jan. '88 2.8 X 2.5 X 1 R Local 106 111 AFD 12 Mi43 April '83 6.5 X 6.4 X 5.5 L LH April '84 4 X 3.5 X 2.5 R Local 12 62AFD 13 Mi53 June '83 3 X 2 X 2.5 R Local May '84 2 X 2.5 X 2 R Local 11 60 AFD 14 Fl42 June '83 11 X 10 X 5 R RH Aug. '86 1.5 X 1.5 X 1.5 L Local 38 60AFD
15 MI45 June '80 12 X 10 X 8 R HAL + Dec. '80 6 x 5 x 4 R Local 6 96AFD
16 MI37 July '82 12 X 10 X 9 R HAL + Oct. '82 7 x 5 x 4 R Local 3 71 AFD
17 Mi52 Nov. '81 15 X 10 X 9 R HAL + March '82 7 X 7 X 7 R Local 4 77DWD
HAC
HAC
HAC
Sex: maleifemale, Age (years). Tumor site: L = left lobe of the liver, R = right lobe of the liver. Surgical procedure: LH = left hemihe- patectomy, RH = right hemihepatectomy, LLS = left lateral segmentectomy, Local = local resection, HAL = hepatic artery ligation, HAC == hepatic artery cannulation, Cryosurgery = cryosurgery with liquid nitrogen. Outcome: AFD = alive, free of disease; DWD = dead with disease.
with postoperative perfusion of chemotherapeutic agents in the lesion site. Several months later, all patients showed marked regression of tumor to around 50% of the original diameter, and resection was carried out. Thus, these patients formerly considered nonresectable HCC became resectable HCC. The time span between initial palliative surgery and sequential resection was from 3 to 6 months (mean 4.3 months). Survival of the three pa- tients was 96 months (alive), 71 months (alive), and 77 months, respectively.
One patient (Table I, No. 16), from the high-risk area of HCC, the Qidong County of Jiangsu Province, was admitted to our hospital in June 1982 because of minor discomfort in the right quadrant of the abdomen for 2 weeks. The patient had a hepatitis history of 16 years and strong family history of HCC. His mother, two brothers, and one uncle all died of HCC several years ago. His AFP was 1,250 ng/ml, and HBsAg was positive. Radi- onuclide scan and ultrasonography showed a huge occu- pying lesion on the right lobe of the liver. An operation in July 1982 revealed a 12 X 10 X 9 cm tumor in the right lobe. Because of coexisting cirrhosis with left-lobe atrophy, the patient could not tolerate a right hemihepa- tectomy . Right hepatic artery ligation plus cannulation
was performed, and postoperative perfusion of chemo- theraputic agents, with thiotepa, 5-fluorouracil, and amethopterin, was carried out. AFP declined rapidly to 31 ng/ml on the 60th postoperative day, and the tumor regressed to around 50% of its original diameter. The second operation in October 1982 revealed that the right tumor was 7 X 5 X 4 cm, and local resection, with interruption of porta hepatis for 12 min, was carried out. In order to prevent tumor recurrence, the hepatic artery cannula was retained for postoperative continual perfu- sion of chemotherapeutic agents. Pathologic examination confirmed HCC with tumor emboli in the intrahepatic vein in the surgical specimen. Hepatic artery perfusion chemotherapy, with 5-fluorouracil and thiotepa, was given for 1 month postoperatively. The patient has re- turned to work and is well, with negative AFP, for 71 months.
Two patients underwent bloodless hepatectomy with organ isolation hypothermic perfusion for resection of HCC that was close to or directly involved the inferior vena cava and was previously deemed nonresectable. The livers were isolated from the systemic circulation for 76 and 39 min, respectively. One patient has survived for 1 18 months after bloodless hepatectomy, with negative

HCC: Improve Long-Term Survival 259
present in 8 1.8% (54/66); micronodular cirrhosis amounted to 44.4% (24/54), and macronodular, to 55.6% (30/54) of the patients with cirrhosis.
On admission, serum AFP was detected in 59 patients. Of these, 50 patients (84.7%) had serum AFP levels 2
200 ng/ml. The normalization rate (to < 20 ng/ml) of AFP after radical resection of the tumor was 100% (50/50) in this series, including the patient with palliative resection plus cryosurgery with liquid nitrogen on the cut surface. AFP returned to normal within 2 months in sub- clinical HCC.
AFP, and has returned to work. The other patient (Table I, no. 4) had solitary pulmonary metastatic lesion. She had survived for 98 months and died of tumor metastasis to bone.
One asymptomatic patient was picked up by AFP se- rosurvey. A selective hepatic arteriogram showed a small tumor measuring 2 X 2 X 1.9 cm in the right lobe. An operation was performed in May 1980, and the tumor was resected by Nd:YAG laser, and the basis of the cut surface, was vaporized by laser. Pathologic examination confirmed HCC with micronodular cirrhosis. The patient has been well for 97 months, with negative AFP, and has resumed his original work.
Three young patients, two female and one male, have survived for 183, 153, and 115 months, respectively, after resection of HCC. They are all now still well, have gotton married, and have had babies.
In this series, palliative resection was carried out in only one asymptomatic patient who was detected by AFP serosurvey. An operation in March 1975 revealed a 2.5 x 2 x 2 cm tumor in the caudal lobe. Palliative resec- tion was performed. Cryosurgery with liquid nitrogen was also employed on the cut surface because the resec- tion was inadequate, and immediately after the opera- tion, external local radiation therapy was given. Patho- logic examination confirmed HCC with tumor residue in the cut surface, with micronodular cirrhosis. AFP dropped to normal after the operation, increased some- what by the end of the first postoperative year, and per- sisted at a low level. During the ensuing years, the patient received long-term conservative treatment con- sisting of chemotherapy, immunotherapy , and Chinese medicinal herbs. Despite slowly increasing AFP, the pa- tient was apparently in good health without any symp- toms 100 months after the operation. The patient finally died of upper gastrointestinal hemorrhage 102 months after the operation.
Operative and histological findings were as follows: The sizes of tumor ranged from 1 X 1 X 1.5 to 12 X 15 x 15 cm. Of the patients, 53.0% (35/66) had small tumors (5 5 cm), 31.8% (21/66) had large tumors (> 5 to > 10 cm), and 15.2% (10/66) had very large tumors (> 10 cm). single-nodule tumors amounted to 87.9% (58/66); grossly well-encapsulated tumors were found in 84.8% (56/66). Tumor emboli presented in the intrahe- patic veins in 6.1% (4/66). There was one patient (1.5%) with tumor residue in the cut surface. Histologic findings revealed that all 66 patients were HCC. The differentia- tion of HCC cells was as follows: 3.4% (2159) were grade I; 3.4% (2/59), grades 1-11; 79.7% (47/59), grade 11; 1.7% (1/59), grades 11-111; and 11.9% (7/59), grade 111, according to the classification of Edmondson [24]. Cell differentiation was not recorded in seven patients in this series. In the noncancerous portion, cirrhosis was
DISCUSSION In recent years, it has been universally accepted that
early detection and early treatment of subclinical cancer may be an important approach to rescuing the patient until breakthroughs are made in the research on basic as well as etiological aspects [25]. In China, advances in early detection of subclinical HCC have been made since the application of AFP serosurvey in high-risk areas and monitoring in the population with a hepatitis or cirrhosis background [26]. It has been reported that in operated cases of subclinical HCC, up to 81.6% (40/49) of the tumor nodules measured smaller than 5 cm [27]. On the other hand, up to 76.7% (23/30) of patients with surgi- cally proven small HCC were asymptomatic [28].
The discovery of patients with subclinical or small HCC was realized principally by AFP serosurvey in China, by AFP monitoring of chronic liver disease in Japan [29], and by accidental findings during surgery in the United States [2]. Recently, Heyward et al. [30] demonstrated that AFP screening proved to be an effec- tive approach in persons infected with hepatitis B virus (HBV) in detecting HCC at a potentially curable stage. They reported that during a 26 month screening period, AFP tests were performed on 1,394 persons infected with HBV in Alaskan natives. Of 125 persons with ele- vated levels of AFP (> 25 ng/ml), nine were found to have HCC (all with AFP > 350 ng/ml). Six of these nine were asymptomatic, and four had small tumors (< 6 cm) that were surgically resected. Curutchet et al. [31], col- lecting the data of 45 authors over 65 years (1905- 1970), found that only forty-five 5 year survivors were obtained worldwide. However, 66 cases were collected in our series during the past 25 years (1958-1983) and 84.8% (56/66) were collected during the later 8 years (1975-1983); 37 of them were subclinical HCC, and 35 of them were small HCC (5 5 cm). Our previous results demonstrated that a much higher 5 year survival rate was obtained after subclinical HCC resection as compared with clinical HCC resection (72.9 vs. 16.1%) [26]. Thus, the discovery of subclinical or small HCC may play an important approach in improving overall HCC prognosis.

260 Zhou et al.
It has long been emphasized that the presence of cir- rhosis is generally a contraindication to major hepatic resection because the possibility of postoperative liver failure is higher [5-81. This may be not a great problem in the West because of the relatively low rate of coexis- tent cirrhosis, which was 20.5% (26/127) in the United States during the period 1960-1974 [2]. However, it is of great importance in Asian patients. The rate of coex- istent cirrhosis was 81.8% (54/66) in this series. In fact, microscopically, over 90% of the patients with PLC in our area have underlying cirrhosis [1]. Thus, major re- section is severely limited.
In principle, excision of a malignant tumor should be wide and extensive enough to eradicate the lesion. How- ever, if this concept is applied in cases of small HCC with a cirrhotic liver, the results are potentially jeopar- dized by the complications that will ensue [9]. There- fore, it has been the policy of our surgical team that 1) for clinical HCC or huge tumor, “classic” lobectomy or extended lobectomy remains the principal type of resec- tion when clinical status and hepatocellular reserve are adequate, which accounted for 28.8% (19/66) in this series; 2) for subclinical HCC or small tumor with a cirrhotic liver, limited hepatic resection, including local resection and segmentectomy with a cut margin at least 2 cm from tumor capsule, became the main resection type, which accounted for 71.2% (47/66) in this series; and 3) furthermore, the limited hepatic resection seems to be the procedure of choice, especially when there is a well- demarcated liver cancer nodule, a wide excision should be done for a noncapsulated mass [9].
Grossly well-encapsulated tumor was found in 84.8% (56/66) in this series. Kanematsu et al. [9] reported that there was no significant difference in the mortality (10.8 vs. 15.4%) and 5 year survival rate (32.6 vs. 22.5%) between limited resection (n = 37, enucleation of the tumor with less than 1 cm of surrounding liver tissue) and standard major hepatic resection (n = 13, formal major hepatic resection with more than 1 cm of surround- ing liver tissue). Careful evaluation of hepatic functional reserve of cirrhotic livers both qualitatively and quanti- tatively are most important in assessing the safe extent of hepatic resection [32,33]. Favorable long-term results of hepatic resection for HCC in cirrhotic patients remain to be confirmed in the Western hemisphere [34].
Reoperation for subclinical recurrence or solitary pul- monary metastasis seems an important approach in pro- longing survival further after radical resection of HCC. As we reported previously, the 1, 3, and 5 year recur- rence rates after radical resection of HCC were 17.1, 32.5, and 61.5%, respectively, and reoperation for sub- clinical recurrence or solitary pulmonary metastasis has resulted in a 20% (from 47.7% to 66.8%) increase of 5 year survival after radical resection of HCC [ 131, which
was difficult to obtain by other approaches. Its basic principles have been reported [4,13,35] and are, briefly, 1) long-term (up to 10 years) monitoring of AFP and ultrasonography after resection of HCC is needed for detecting subclinical HCC recurrence and metastasis; 2) the reappearance of AFP up to 200 ng/ml for 2 months without evidence of active liver disease is a case for thorough investigation, including ultrasonography , com- puted tomography, and selective angiography , if needed; 3) when recurrence or metastasis is diagnosed by these methods, reoperation should be considered; and 4) local resection is the modality of choice in reoperation; cryo- surgery with liquid nitrogen, high-power Nd:YAG laser vaporization, or intrahepatic arterial infusion of chemo- therapeutic agents with or without hepatic arterial liga- tion or embolization can be employed when resection is not indicated.
In this series, subclinical HCC recurrence in the re- maining liver was discovered in 10 patients 11-106 months after the first operation. Eight of them underwent second hepatic resection. The remaining two patients re- ceived cryosurgery. Survival varied from 60 to 154 months (mean, 89.5 months) after the first operation. Six patients are alive, free of disease, and four patients died with disease. Subclinical solitary pulmonary metastasis was detected in four patients 31-64 months after initial operation. All these four patients underwent lobectomy for metastatic lesions. Survival of the four patients was 158 (alive), 154 (alive), 91, and 98 months, respec- tively, after the first operation.
Nagasue et al. [36] reported that during the follow-up period of 91 patients with radical hepatic resection, 31 patients had HCC recurrence in the liver remnant 4-38 months after the first hepatectomy. Nine of them under- went a second hepatic resection. Six patients were alive, four free of HCC and two with disease, for 15-45 months after the first operation. Two patients died of systemic cancer dissemination. The remaining patient had tumor recurrence in the liver and died of hepatic failure after the third laparotomy. The survival rate of these nine patients was significantly better than that of 22 patients who were treated by other palliative methods. Encouraging results have been observed in the literature for reoperation of HCC recurrence and metastasis [37,38]. However, patients with recurrent HCC with multiple nodules and metastases in multiple sites are not good candidates for a second resection.
Conversion of nonresectable to resectable HCC has gained attention in recent years [14,15,39]. Sitzmann et al. [15] reported that 11 patients with HCC had nonre- sectable lesions and were treated with a variety of new modalities, particularly radiolabeled antiferritin antibod- ies. Following treatment, seven of the 11 patients were considered to have converted their lesions to resectabil-

HCC: Improve Long-Term Survival 261
rhotic and noncirrhotic livers after hepatic lobectomy in men. Ann Surg 162:959-972, 1965. Lin TY, Lee CS, Chen CC, et al.: Regeneration of human liver after hepatic lobectomy studied by repeated liver scanning and repeated needle biopsy. Ann Surg 190:48-53, 1979. Kanematsu T, Takenaka K, Matsumata T, et al.: Limited hepatic resection effective for selected cirrhotic patients with primary liver cancer. Ann Surg 1995-56, 1984. Lee CS, Chao CC, Lin TY: Partial hepatectomy on cirrhotic liver with a right lateral tumor. Surgery 98:942-947, 1985. Tang ZY: Surgical treatment of subclinical cases of hepatocellular carcinoma. In Okuda K, Ishak KG (eds): “Neoplasms of the Liver.” Tokyo: Springer-Verlag. 1987, pp 367-373. Tang ZY, Yu YQ, Zhou XD, et al.: Surgical treatment of sub- clinical hepatocellular carcinoma (HCC) and its ultimate out- come-A comparative study of 74 cases of subclinical HCC and 229 cases of clinical HCC undergone surgery. J Exp Clin Cancer Res 2:261-268, 1983. Tang ZY, Yu YQ, Zhou XD: An important approach to prolong- ing survival further after radical resection of AFP positive hepa- tocellular carcinoma. J Exp Clin Cancer Res 3:359-368, 1984. Yu YQ, Tang ZY, Zhou XD, et al.: Treatment of huge primary liver cancer in stages. Chin J Surg 21:92-93, 1983. Sitzmann JV, Order SE, Klein JL, et al.: Conversion by new treatment modalities of nonresectable to resectable hepatocellular cancer. J Clin Oncol 5:1566-1573, 1987. Zhou XD, Yu YQ, Tang ZY, et al.: Laser surgery of the liver: Experimental study. Acta Acad Med Primae Shanghai 7:216- 221, 1980. Yu YQ, Tang ZY, Zhou XD, et al.: Treatment of primary liver cancer by high power Nd:YAG laser-Experimental and clinical study. Chin J Surg 24:152-155, 1986. Yu YQ, Tang ZY, Zhou XD, et al.: Bloodless hepatectomy. Chin J Surg 18:146-147, 1980. Zhou XD, Tang ZY: Bloodless hepatectomy and hepatic clamp in small hepatocellular carcinoma resection. In Tang ZY (ed): “Sub- clinical Hepatocellular Carcinoma. ’’ Beijing: China Academic Publishers; Berlin: Springer-Verlag, 1985, pp 85-100. Zhou XD, Tang ZY, Yu YQ: Changes in liver function and their management after resection of primary liver cancer. Natl Med J China 60:606-611, 1980. Zhou XD, Tang ZY, Yu YQ, et al.: Cryosurgery for liver cancer- Experimental and clinical study. Chin J Surg 17:480-483, 1979. Zhou XD, Tang ZY, Yu YQ, et al.: Cryosurgery for hepatocel- lular carcinoma. In Tang ZY (ed): ‘‘Subclinical Hepatocellular Carcinoma.” Beijing: China Academic Publishers; Berlin: Springer-Verlag, 1985, pp 107-1 19. Zhou XD, Tang ZY, Yu YQ, et al.: Clinical evaluation of cryo- surgery in the treatment of primary liver cancer: Report of 60 cases. Cancer 61:1889-1892, 1988. Edmondson HA: Tumor of the liver and intrahepatic bile ducts. In: “Atlas of Tumor Pathology,” Sect. 7, Fascicle 25. Washing- ton, DC: Armed Forces Institute of Pathology, 1958. Leffall LD: Subclinical cancer-Concepts and management. In Fox M (ed): “Advances in Medical Oncology, Research and Eduction, Vol. 4.” London: Pergamon, 1979, pp 269-283. Zhou XD, Tang ZY: Factors influencing resectability and resection survival rates of subclinical hepatocellular carcinoma. In Tang ZY (ed): “Subclinical Hepatocellular Carcinoma.” Beijing: China Academic Publishers; Berlin: Springer-Verlag, 1985, pp 78-84. Shanghai Coordinating Group for Research on Liver Cancer: Di- agnosis and treatment of primary hepatocellular carcinoma in early stage-report of 134cases. ChinMed J [Engl] 92:801-806,1979. Tang ZY, Yu YQ, Lin ZY, et al.: Small hepatocellular carci- noma- Clinical analysis of 30 cases. Chin Med J [Engl] 92:455- 462, 1979. Okuda K: Early recognition of hepatocellular carcinoma. Hepa-
Heyward WL, Lanier AP, McMahon BJ, et al.: Early detection of primary hepatocellular carcinoma (PHCC): Screening for PHCC
tology 6:729-738, 1986.
ity, six patients had complete resections, and one patient was partially resected. Our previous data demonstrated that by using 1311-antihuman HCC isoferritin antibody, regression of HCC was shown in 58.3% of the patients (7112) [39]. In this series, multimodality palliative sur- gery also provided an opportunity to convert nonresect- able to resectable HCC in three patients (Table I, nos. 15-17) in whom the regression of HCC was around 50% of the original diameter. The time span between initial palliative surgery and subsequent resection was 3 -6 months (mean, 4.3 months). Survival of these three pa- tients was 96 (alive), 71 (alive), and 77 months, respec- tively. Recently, we have treated several patients using I3’I-antiferritin antibodies plus hepatic artery ligation and/or hepatic cannulation. Some of their tumors have converted to being resectable. Our clinical results on this subject will be reported separately.
CONCLUSIONS
In China, advances in early detection of subclinical HCC have been made since the application of AFP se- rosurvey in 1971. For small HCC with a cirrhotic liver, limited hepatic resection is the modality of choice. Re- section of such small HCC has resulted in large-scale prolongation of survival and low operative mortality. Long-term monitoring AFP and ultrasonography after radical resection of HCC is needed for detecting subclin- ical HCC recurrence or metastasis. Reoperation for sub- clinical HCC recurrence or solitary pulmonary metastasis seems to be an important approach to prolong survival further after radical resection of HCC. Conversion of nonresectable to resectable HCC, using multimodality palliative surgery and radiolabeled antibodies, has gained attention in recent years. Problems to be solved in the surgical treatment of HCC include multinodular can- cer and coexistent macronodular cirrhosis with noncom- pensated liver function, in which surgery cannot be tol- erated.
1 .
2.
3.
4.
5
6
7
REFERENCES
Zhou XD, DeTolla L, Custer RP, London WT: Iron, ferritin, hepatitis B surface and core antigens in the livers of Chinese patients with hepatocellular carcinoma. Cancer 59: 1430-1437, 1987. Foster JH, Berman MM: Primary epithelial cancer in adults. In Foster JH, Berman MM (eds): “Solid Liver Tumors.” Philadel- phia: W.B. Saunders Co., 1977, pp 62-104. Yu YQ, Tang ZY, Zhou XD: Experience in resection of small hepatocellular carcinoma. Chin Med J [Engl] 93:491-494, 1980. Tang ZY, Yu YQ, Zhou XD: The changing role of surgery in the treatment of primary liver cancer. Semin Surg Oncol2:103-112, 1986. Ong GB, Lee NW: Hepatic resection. Br J Surg 62:421-430, 1975. Kohno A, Mizumoto R, Honjo I: Changes after major resection of experimental cirrhotic liver. Am J Surg 134:248-252, 1977. Lin TY, Chen CC: Metabolic function and regeneration of cir-
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.

262 Zhou et al.
among persons infected with hepatitis B virus. JAMA 254:3052- 3054, 1985.
31. Curutchet HP, Terz JJ, Kay S, et al.: Primary liver cancer. Sur- gery 70:467-479, 1971.
32. Ozawa K, Yamaoka Y, Kitanura 0, et al.: Clinical application of cytochrome a( + a3) assay of mitochondria from liver specimens: An aid in determining metabolic tolerance of liver remnant for hepatic resection. Ann Surg 180:868-876, 1974.
33. Okanoto E, Kyo A, Yamanaka N, et al.: Prediction of the safe limit of hepatectomy by combined volumetric and functional mea- surements in patients with impaired hepatic function. Surgery
34. Bismuth H, Houssin D, Ornowske J, et al.: Liver resection in cirrhotic patients: A Western experience. World J Surg 10:311- 317, 1986.
951586-591, 1984.
35. Yu YQ, Tang ZY, Zhou XD, et al.: Evaluation of reoperation for recurrence and metastasis after resection of primary liver cancer. Jiangsu Med J 11:4-6, 1980.
36. Nagasue N, Yukaya H, Ogawa Y, et al.: Second hepatic resection for recurrent hepatocellular carcinoma. Br J Surg 73:434-438, 1986.
37. Wilson E: Malignant hepatoma, repeated resection of metastases with survival for 15 years. Med J Aust 2:889-893, 1966.
38. Chen H, Wu MC, Zhang XH: Reoperative primary liver cancer-Report of 28 cases. Chin Med J [Engl] 100:795-799, 1987.
39. Tang ZY, Liu KD, Guo YD, et al.: Tumor imaging and targeting therapy for hepatocellular carcinoma: Preliminary results of ex- perimental and clinical studies. Chin Med J [Engl] 99:855-860, 1986.


























