Embed Size (px)
Citation preview

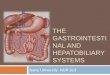
Hepatobiliary Anatomy and Pathology
By Zach Krahn MS4

Anatomy Review
The liver is one of two organs in the body with a dual blood supply; the portal vein supplies ~2/3 of the total blood with the hepatic artery supplying the rest.
The major function of the liver is to filter the blood of toxins although it is also very important in protein synthesis and metabolism.
The gallbladder is the storage unit for bile, a substance that aids in fat metabolism

CT Basics
CT images are constructed based upon the differing density of substances in the body.
Dense substances (e.g. bone or metal) appear bright {hyperdense}
Low density substances (e.g. organ tissue or fat) appear less bright {hypodense}
Hounsfield units are used to describe the relative brightness of a substance on CT
Contrast, either oral or IV, can be given to better delineate anatomic structures

50 Shades of Gray
White
Shades
of gray
Black
Hounsfield units

Hepatobiliary CT
IVC
R Kidney
R renal artery
Aorta
L Kidney
Desc Colon
SMA
SMVGallbladder
Liver

Case #1Which is normal? What is abnormal?
Hyperdense material in gallbladder (biliary sludge, blood or contrast) with thickened wall
Without contrast, the bowel appears black (air)
The white “stuff” is contrast in the bowel

Case #1: CholecystitisPresentation: colicky pain (comes and goes), nausea,
and fever.
Risks: Obesity, gallstones, prolonged fasting
Treatment is usually surgical plus antibiotics

Case #2
Where is the abnormality?
What structure is it in? Common Bile Duct
Irregular soft tissue within the duct suggests malignancy. Dilation due to cystic common bile duct

Case #2: CholangiocarcinomaCholangiocarcinoma is a
cancer of the bile duct system
Symptoms include RUQ pain and intermittent jaundice
Risk factors: Clonorchis sinensis infection, toluene/benzene exposure, cysts within bile duct
Treatment: Surgical +/- adjuvant chemotherapy; poor prognosis

Case #3Where is the abnormality?
What structure is it in?
Note calcifications
Liver

Case #3: Hepatocellular Carcinoma Imaging demonstrates large
hypodense area within liver parenchyma, calcifications are present.
Common presentation: male between ages of 40-60, often vague symptoms including jaundice, RUQ pain, fever, weight loss
Risk factors: Cirrhosis, Hepatitis B (more so than Hepatitis C), hemochromatosis
Treatment: Resection, liver transplant, radiofrequency ablation.

Case #4What is abnormal?
What could it be? Blood (hemorrhage), pus (abscess), water (cyst)
Fluid around liver could also be blood, pus, or water

Case #4: Hepatic AbscessCT imaging shows an area
of necrosis surrounded by inflammation (heterogeneous density)
Common presentation: May be subtle. RUQ pain and fever may be present
Risk factors: Biliary tract disease, pancreatic disease, can be idiopathic
Treatment: Drainage and antibiotics

Case #5
What is abnormal? How do you know?
Spleen is normally about the same density as liver
Liver is less dense than spleen, suggests problem

Case #5: SteatohepatitisFat deposition in liver
parenchyma
Presentation: Often asymptomatic. May have RUQ pain, muscle pain, jaundice, liver enzyme elevations
Risk Factors: Obesity, excessive alcohol, extensive weight loss (bariatric surgery)
Treatment: Lifestyle interventions

Case #6
Abnormality? Describe the difference.
The edges of the liver should be smooth in appearance
This liver has a rough surface with many nodules

Case #6: Cirrhosis
Scarring of liver parenchyma due to chronic inflammation
Presentation: Fatigue, weight loss, jaundice, spider angioma, gynecomastia
Risk Factors: Alcoholism, Hepatitis C or B, history of blood transfusion before 1992 (before Hep C routinely tested), hemochromatosis
Treatment: Liver transplant, cease alcohol use, vaccinate against Hepatitis A, treat underlying condition

Take Home Points
Learning the anatomy now will help you better understand pathology and radiology in the future.
When looking at imaging studies, it is useful to know what “normal” looks like
CT imaging relies on the differing density of tissues whatever surrounds those tissues (air, water, fat)

References
Case in Point. American College of Radiology. Multiple topics: cholangiocarcinoma, cholecystitis, hepatocellular carcinoma
Dynamed. Topics: Cirrhosis, steatohepatitis, hepatic abscess
Images obtained from Case in Point at American College of Radiology, Imaging Consult, Radiopaedia