Embed Size (px)
Citation preview

Hepatitis C Virus
Resistance Testing
Mark Douglas

About 170 Million People Worldwide Have Chronic HCV Infection
Blatt LM, et al. J Viral Hepat 2000;7:196-202; Yu M, et al. J Gastroenterol Hepatol 2009;24:336-45; Narahari S, et al. Infect Genet Evol 2009;9:643-5;Higuchi M, et al. Jpn J Infect Dis 2002;55:69-77; Dore GJ, et al. J Clin Virol 2003;26:171-84; Wkly Epidemiol Rec 2002;77:45-7;
Centers for Disease Control and Prevention. 2009. http://www.cdc.gov/hepatitis/statistics.htm; Di Bisceglie AM. Essentials of Hepatitis C Infection. 2009;Chen CH, et al. J Formos Med Assoc 2007;106:148-55; Negro F & Alberti A. Liver Int 2011;31(s2):1-3; Shin HR, et al. J Korean Med Sci 2005;20:985-8.M, million
SoutheastAsia
30–35 M
Western Europe
5 M
United States3–4 M
South America12–15 M
Africa30–40 M
Eastern Europe10 M
Japan2 M
China40 M
Australia0.2 M
Taiwan0.4 M
India12–13 M
Korea0.2 M
1.0–1.9%2.0–10%
Prevalence of infection>10%
<1.0%
China40 M
Korea0.2 M
Taiwan0.4 M
India12–13 M
Japan2 M
Asia-Pacific Region~90 M
Australia0.2 M
SoutheastAsia
30–35 M
• 27% of cirrhosis and 25% of HCC worldwide
• Main cause of cirrhosis, liver transplant and HCC in
Australia, USA, UK
• Causes more deaths than HIV in Australia and USA

SVR (%)
80
60
40
20
024 48 78 Peg-
IFN
IFN +
RBV
PEG +
RBVweeks
IFN
monotherapy
G2/3
6-22
18-39
35-
43
61-79
33-
36
76-82
42-46
*Range of values reported;
lower bar represents lower value
G2/3G1
ALL
ALL
Evolution of SVR rates
Adapted from Manns, Foster et
al., Nature Reviews Drug
Discovery 2007
100
G1
1989 1995 1998 2001

Potential New Drug Targets
Pockros, PJ (2010, Therap Adv Gastro, 3:191–202)

Direct Acting Antivirals (DAAs)
NS3/4A protease inhibitors
– telaprevir, boceprevir, simeprevir, paretaprevir
NS5B polymerase inhibitors
– Nucleos(t)ide analogues (sofosbuvir)
– Non-nucleoside analogues (dasabuvir)
NS5A inhib. (daclatasvir, ledipasvir, ombitasvir)
Rosen, H. R. (2011, NEJM, 364:2429–2438)

SVR (%)
80
60
40
20
024 48 78 Peg-
IFN
IFN +
RBV
PEG +
RBVweeks
IFN
monotherapy
G2/3
6-22
18-39
35-
43
61-79
33-
36
76-82
42-46
*Range of values reported;
lower bar represents lower value
G2/3G1
ALL
ALL
Evolution of SVR rates
Adapted from Manns, Foster et
al., Nature Reviews Drug
Discovery 2007
100
G1
1989 1995 1998 2001 2011
PEG +
RBV +
TPV
or BOC
63-75
G1
IFN free DAA therapy
SOF +
LDV
or DCV
(8-12w)
97-99
G1N96-99
(86)
G1R
2014
PTV/r +
OTV+
DBV+
RBV
(12w)
92-96
G1N
PEG +
RBV +
SMV
80-81
G1
PEG +
RBV +
SOF
(12w)
82-92
G1
2012
SOF +
RBV
(12w)
2013
93-97
G2
56-68
G3
79-89
G3
SOF +
RBV
(24w)
GPV +
EBV
(8-12w)
94-99
G1
SOF+
VPV
(12w)
97-99
G1
90-95
G3
But what about resistance?
Resistance associated variants
(RAVs)

DAA Resistance - sequencing
Drug-susceptible quasispecies
Drug-resistant quasispecies
Treatment begins
Vir
al L
oad
Selection of resistantquasispecies
Incomplete suppressionInadequate potencyInadequate drug levelsInadequate adherencePreexisting resistance
Zeuzem S. http://www.clinicaloptions.com/Hepatitis/TreatmentUpdates/Future Generations.aspx Accessed 6/2011.
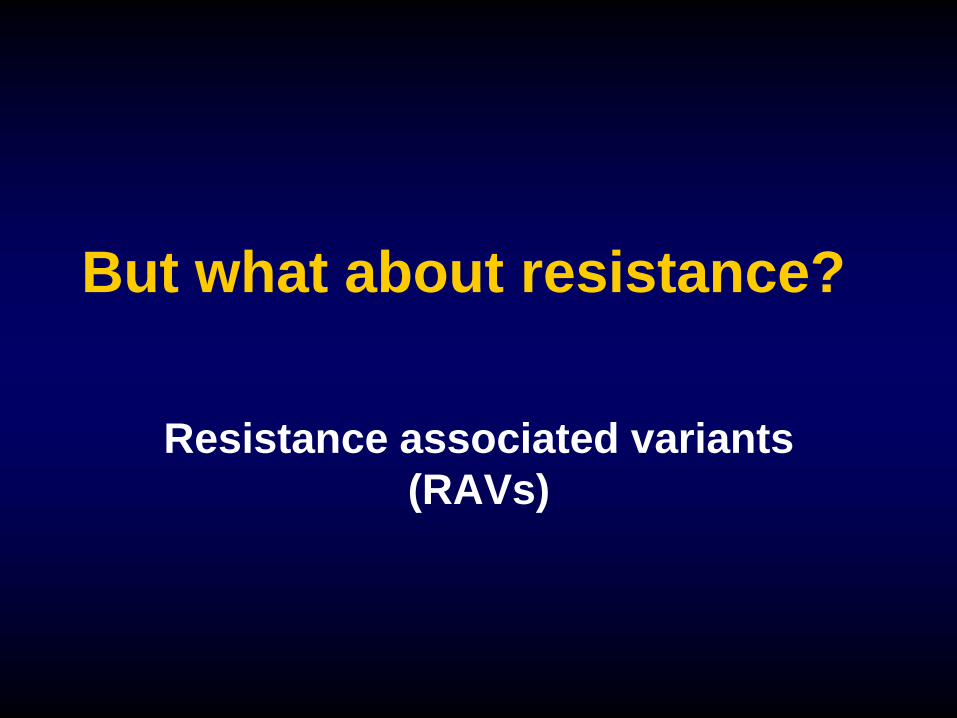
Market Introduction and Emergence of
Resistance (Selected Drugs)
The Race Against Drug Resistance: A Report of the Center for Global Development’s
Drug Resistance Working Group. Nugent R, Back E, Beith A. 2010

NS3
Boceprevir, telaprevir - genotype 1
Simeprevir - genotype 1, 4
Paritaprevir - genotype 1
Grazoprevir - pan genotypic
RAV prevalence 0.1 - 3.1% (likely due to fitness cost)
except Q80K (5-48%)
RAV persistence wk48 post treatment 9%

NS5A
Daclatasvir (BMS) - pan genotypic
Ombitasvir (AbbVie) - pan genotypic
Ledipasvir (Gilead) - Genotype 1
Elbasvir (MSD) - genotypes 1, 3, 4, 6
Velpatasvir (Gilead) - pan genotypic
RAV prevalence 0.3-3.5%
RAV persistence high– up to 85% 48 wks post treatment)

NS5B
Nucleos(t)ide analogue
– Sofosbuvir (Pan genotypic)
– RAV prevalence 0.0%
– RAV persistence 0.0% by Wk 4 post treatment
Non nucleoside analogue
– Dasabuvir (genotype 1)
– RAV prevalence 0.2-3.1%
– RAV persistence at wk48 post treatment 57%

HCV Resistance:
Does it matter?
0
10
20
30
40
50
60
70
80
90
100
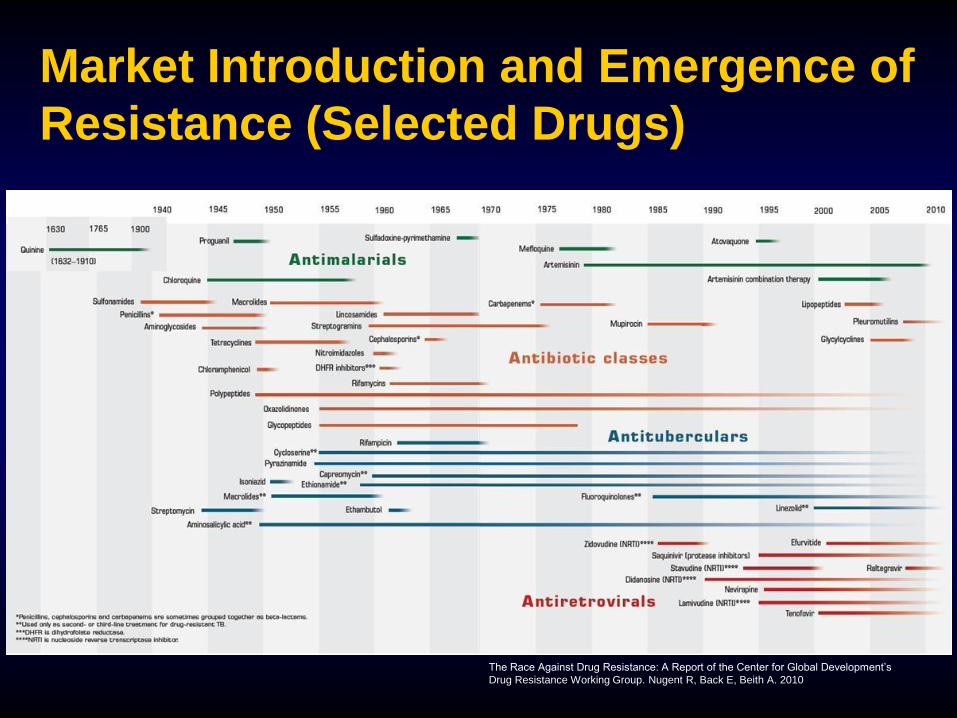
PEG/RBV (n=44) PEG/RBV/SMV (n=84) PEG/RBV (n=83) PEG/RBV/SMV (n=165)
SVR12
%
QUEST-1/2: PEG-IFN/RBV/Simeprevir (24-48 weeks)
Genotype 1 treatment naïve
Jacobson I et al. AASLD 2013
GT1a + Q80K GT1a – Q80K

Q80K Prevalence

Q80K in Western Sydney?
Samples tested 378 (Gt 1a)
Age: mean 31 yrs
Gender: Male: 270 (71%)
Correctional centre (annonymous):
119 (31%)

Of 378 samples:
Mutation Number %
Q80K 21 5.6
V55A 16 4.2
T54S 10 2.6
Q80L 5 1.3
Q80R 3 0.8
R155K 2 0.5
Q80H 1 0.3

IFN-free therapy?
Combination DAA high cure rates
Failure more likely if baseline RAVs,
particularly multiple NS5A RAVs
Patients failing DAA therapy have
high levels of RAVs

Methods of detecting resistance
Population (Sanger) sequencing
High throughput (Next generation)
sequencing
– Better sensitivity with NGS - down to
<1% (Sanger ~20%)
» clinical relevance not yet determined
– Bioinformatics (big data) with NGS
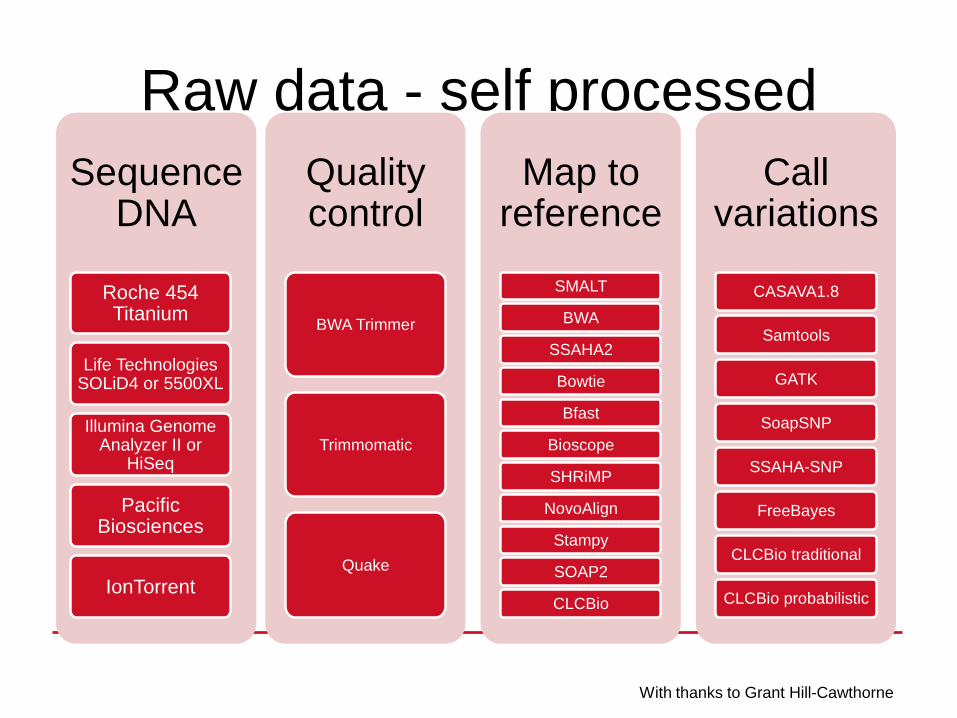
Raw data - self processedThe more complicated stucture for variation detection
Sequence DNA
Roche 454 Titanium
Life Technologies SOLiD4 or 5500XL
Illumina Genome Analyzer II or
HiSeq
Pacific Biosciences
IonTorrent
Quality control
BWA Trimmer
Trimmomatic
Quake
Map to reference
SMALT
BWA
SSAHA2
Bowtie
Bfast
Bioscope
SHRiMP
NovoAlign
Stampy
SOAP2
CLCBio
Call variations
CASAVA1.8
Samtools
GATK
SoapSNP
SSAHA-SNP
FreeBayes
CLCBio traditional
CLCBio probabilistic
With thanks to Grant Hill-Cawthorne
Bioinformatics

Known Resistance Variants

Summary
HCV is curable
High cure rates with DAAs
Resistance can emerge and may
affect (re)-treatment response
Reliable, high-throughput assays
required to detect RAVs
Next Generation Sequencing most
sensitive, becoming feasible





![Hepatitis B virus and hepatitis C virus play different ... · alcoholic cirrhosis, hepatitis viruses, tobacco and metabolic diseases[4]. Hepatitis viruses, including hepatitis B virus](https://img.dokumen.tips/doc/110x75/60e46cab5bd9101a6f539e91/hepatitis-b-virus-and-hepatitis-c-virus-play-different-alcoholic-cirrhosis.jpg)