Embed Size (px)
Citation preview

Kidney International (Vol. 13), 1978, pp. 324 —328
Hepatitis B surface antigen in urine of hemodialysis patients
MICHAEL R. HOURANI, GILBERT H. MAYOR, DAVID 5. GREENBAUM, DAVID 0. HUGGETand MARIA J. PATTERSON
Department of Medicine and Microbiology, Michigan State University, East Lansing, Michigan, and Michigan Departmentof Public Health, Lansing, Michigan
Hepatitis B surface antigen in urine of hemodialysis patients. Aspart of an extensive epidemiological survey of chronic hemodialy-sis patients in Michigan, hepatitis B surface antigen (HB,Ag) wasidentified in the sera of 79 of 701 (11%) patients. Of these patients,59 were carriers of HBAg for three or more months. Urinesamples were collected from 36 of 39 HBAg carriers havingurinary output. Of these samples, 19 (52%) were positive forHB,Ag by radioimmunoassay; this was confirmed by specificantibody neutralization. The HBAg was not identified in the urineof seven hemodialysis patients who were lacking serum HB,Ag orin urine samples from three HB,Ag sero-carriers who had normalrenal function. Patients undergoing maintenance hemodialysis ap-pear to constitute a large reservoir of HBAg chronic carriers. Thisstudy indicates that a minimum of 50% ofpersistent HB,Ag car-riers who are producing urine have detectable HBAg in single,randomly timed, unconcentrated urine specimen. These data sug-gest that urine may represent a potential vehicle for transmissionin nonparenterally acquired hepatitis B.
Antigéne de surface de I'hépatite B dans l'urine de malades enhémodialyse. Dans le cadre d'une large enquête épidémiologique apropos des malades en hémodialyse chronique dans le Michigan,l'antigene de surface de l'hépatite B (HBAg) a été identiflé dans leserum de 79 parmi 701 malades (11%). Parmi ces malades, 59étaient des porteurs de HB,Ag depuis 3 mois ou plus. L'urine de 36des 39 porteurs de HBAg, qui avaient une diurése, a éte recueillie.Parmi ces 36 urines, 19 (52%) sont positives pour HB5Ag parradio-immunologie, cc qui est confirmé par Ia neutralisation aumoyen d'anticorps spécifique. Le HB,Ag n'a pas été identiflé dansl'urine de 7 malades en hémodialyse qui n'avaient pas Ic HB,Agsérique et dans l'urine de 3 porteurs de HB,Ag dont les fonctionsrdnales étaient normales. Les malades soumis a l'hémodialyseiterative paraissent constituer un grand reservoir de porteurs chro-niques de HB,Ag. Cette étude indique qu'au minimum 5Wo desporteurs chroniques de HB,Ag qui ont une diurése, ont un HB,Agdetectable dans un echantilion unique d'urine, preleve au hasard,non concentré. Ces resultats suggérent quc l'urinc peut étre unvéhicule de transmission de l'hépatitc B acquise par voic nonparcntéralc.
Hepatitis B is an important cause of morbidity andmortality among patients with end-stage renal dis-ease. Of additional importance is the risk of infectionfor persons having intimate contact with thesepatients and/or their secretions. Previous studies [1—
8] have estimated that the prevalence of hepatitis Binfection varies from 0 to 100% among dialysispatients and up to 40% among hospital personneldealing with these patients. Furthermore, up to 61%of the family members of dialysis patients with ahistory of hepatitis B were found to have hepatitis Bsurface antigen (HB5Ag) or hepatitis B surface anti-body (anti-HB) in their sera [2]. Previous studieshave demonstrated HBAg in saliva [9—li], semen[9], and breast milk [12], suggesting transmission bythese secretions. Other studies have documentedthat HB,Ag is present in menstrual blood [13] and invaginal secretions [14] of female antigen carriers.While the exact mode(s) of transmission of hepatitisB in hemodialysis units remains unclear, previousepidemiologic studies [2, 3, 15] have neglected thepossible role of urine as a vehicle for the spread ofhepatitis B. Studies [11, 16—22] that have examinedurine as a transmission vehicle involved subjectswith virtually intact glomeruli and no proteinuria.Presence of hepatitis antigen in the urine of each ofseven renal transplant recipients has been reported[23]. Because of the impaired glomerular permeabili-ty of patients who have end-stage renal disease, andsince many of these patients produce significantamounts of urine, this study was undertaken toexamine a large population of these patients to deter-mine the incidence of HB,Ag-positive urine.
Methods
This study is part of an epidemiologic survey ofdialysis patients which involves 27 of 29 hemodialy-sis units in Michigan. In this survey, 701 patients of apossible 800 on center chronic hemodialysis werestudied. There were 59 patients identified as persis-
Received for publication September 13, 1977;and in revised form October 27, 1977.
324
0085—2538/78/001 3-0324 $01.00
© 1978, by the International Society of Nephrology.

HB5Ag in urine of hemodialysis patients 325
tent carriers of HBAg for a period ranging betweenthree months and three years. An additional 20patients were discovered to be antigenemic duringthe initial survey sampling and are not included inthis study.
Urine specimens were obtained from 36 of the 59persistent HB5Ag carriers. Of the remaining 23 per-sistent carriers, 13 were anephric, 7 had no urinaryoutput, and in 3 cases cooperation in obtaining speci-mens was lacking. In addition, 7 urine specimenswere obtained from hemodialysis patients who wereHBAg-negative, and 3 urine specimens wereobtained from healthy carriers of serum HB5Ag. Allurine samples were coded and stored at —20°C. Sam-ple volumes ranged from 5 to 200 ml, and they werenot concentrated prior to testing.
All urine specimens were tested for HBAg byradioimmunoassay (Ausria 11-125, Abbott Laborato-ries). Two-tenths of a milliliter of unconcentratedurine was incubated in wells for 16 hr at 20 to 23°C(room temperature) with anti-HB-coated beads.After incubation, the beads were washed three timeswith 5 ml of glass distified water, and '251-labeledanti-HB, was added to each well. The samples werethen incubated for 60 mm in a 45°C water bath, andthe beads were rinsed, as described above. Theresidual radioactivity on each bead was countedimmediately in a gamma-counter for 60 sec. The netnegative control mean value was calculated fromdata obtained from seven beads that reacted with asingle-source urine sample from an HB5Ag negativeindividual. The urine samples with 2.1 times the netnegative control value were considered as presump-tive positives for HB5Ag.
Urine specimens positive for HB5Ag by the abovemethod were confirmed using the specific antibodyConfirmatory Neutralization Test (Ausria 11-125, Ab-bott Laboratories) rather than other licensed but lesssensitive HBAg test systems. Initial incubation andwashing of antibody-coated beads with unconcen-trated urine was performed as above. Human anti-HB. was added then to the wells for neutralization ofbound patient HBAg during an incubation at 45°Cfor one hour. '25I-anti-HB was subsequently addedto the wells without washing. After incubation at45°C for three hours, the contents of the wells wereaspirated, washed, and transferred to tubes forgamma scintillation spectrometry. The net negativecontrol mean was calculated from data obtained fromseven beads incubated with urine from an HB5Agnon-reactive individual. A presumptive positive sam-ple was considered a confirmed positive for HB5Ag if50% or more of the radioactivity was inhibited byspecific antibody.
All urine samples were tested for the presence ofprotein and occult blood by Bili-Labstix (AmesCompany).
Results
Of the 36 urine samples collected from persistentserum HBAg carriers, 20 (55%) were positive forHB5Ag by radioimmunoassay. Nineteen of thesepositive urines were confirmed by specific neutrali-zation, and suppression of radioactivity by neutraliz-ing antibody was usually much greater than 50%.Only one initially reactive urine specimen could notbe confirmed.
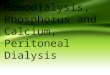
Figure 1 shows the distribution of corrected countsper minute from urine samples of both HBAg sero-positive and sero-negative end-stage renal diseasepatients. In addition, the counts per minute from
x0o 2000000
40
30
C D
Urine sample
Fig. 1. Corrected counts per minute of'25I-anti-HB bound in urinesamples from: A, persistent HB,Ag sero-positive, end-stage renaldisease patients with HB,Ag in urine (mean of 19 patients); B,persistent HBg sero-positive end-stage renal disease patientswithout HB)Ag in urine (mean of 17 patients); C, HBAg sero-negative end-stage renal disease patients (mean of7 patients); anaD, healthy sero-carriers of HB,Ag without renal disease (mean of3 patients). The bracketed lines indicate 1 SEM.

326 Hourani et a!
Table 1. Urine HBAg and occult blood in persistentsero-positive HBAg in patients with end-stage renal
disease
Urine occultblood
Urine HBAgPositive Negative
Positive 5 2 3Negative 31 17 14
Total 36 19 17
urine samples of three sero-positive persons withoutrenal disease are included. HBAg was not found inany of the seven urine specimens from dialysispatients without detectable serum HBAg, nor inthree urine specimens from healthy individuals whoare carriers of HBAg in their sera.
As shown in Table 1, occult blood was found infive urine specimens of the 36 samples obtained fromdialysis patient carriers of HBAg, but only two ofthese were found to contain HBAg. None of theurine samples from seven sero-negative end-stagerenal disease patients or three healthy carriersshowed the presence of occult blood. All 36 speci-mens collected from patients having end-stage renaldisease exhibited proteinuria, but none of the urinesamples from three healthy carriers exhibitedproteinuria.
Among sero-positive hemodialysis patients, serumtransaminase activities, bilirubin levels, age, sex,duration of hemodialysis, duration of HB8Ag carrierstate, volume of urinary output and the originalnature of end-stage renal disease were not signifi-cantly different by analysis of variance (P > 0.05) inpatients with or without HBAg in their urine.
Discussion
Using a solid-phase radioimmunoassay to detectHBAg in unconcentrated urine samples, we havedemonstrated HBAg in 52% of the urine specimensfrom hemodialysis patients who are persistent car-riers of HBAg in their sera. This finding is notrelated to the presence of gross or occult blood in theurine. Verification of presumptive HBAg positiveurine samples was accomplished using a specifichuman anti-HB, neutralization assay.
There are conflicting reports regarding the pres-ence of HBAg in urine. Ogra [18] has shown thatviruria is detectable in a small number of hepatitispatients for a short time in comparison to fecal shed-ding of virus. In their study of seven renal transplantrecipients who had become chronic serum carriers ofhepatitis antigen, Blainey et al [23], using a comple-ment fixation test, detected low levels of antigen inthe unconcentrated urine of each patient. The pres-
ence of hepatitis antigen in the urine samples fromthese patients may be linked to residual output fromtheir original kidney(s). Apostolov et al [19] havereported Australia antigen in the urine from 8 of 13sero-positive patients with acute viral hepatitis, andin 4 of 13 sero-positive patients with chronic liverdisease; however, they also reported Australia anti-gen in the urine in 4 of 13 sero-negative patients withchronic liver disease, and in 2 of 7 healthy volunteerswho were not carriers of Australia antigen in theirserum. In addition, all their HB5Ag positive urineswere detected by the counterimmunoelectrophoresisassay after 70- to 80-fold concentration of the urinesamples. Also, the antibody used in their study wasobtained from one of the HB8Ag sero-negativepatients who had biliary cirrhosis and who was notfully characterized.
Heathcote, Tsianides, and Sherlock [17] havereported that 10% of urine samples collected from 52patients with acute viral hepatitis were positive forhepatitis B antigen by the complement fixation tech-nique. Of the total urines, 62% were positive on atleast one occasion during six months of continuedfollow-up study. These authors, however, found that48% of the household contacts of these patients haddetectable antigen in their urine without being car-riers of hepatitis B antigen in their serum.
In contrast to the results of Blainey et al [23],Apostolov et al [19], and Heathcote et al [17], otherreports [11, 21] have shown that only 3 of 130 urinesamples from sero-positive carriers (each of the 3having occult blood in the urine at the time of testing)and 1 of 13 urine specimens from HBAg sero-posi-tive blood donors were positive for HBAg byradioimmunoassay. Furthermore, no HB5Ag wasdetected in the urine of patients with acute or chronichepatitis [21] or of blood donor volunteers with ser-um HB8Ag [22]. Finally, Irwin et al [16], using aradioimmunoassay, did not detect HBAg in uncon-centrated urine samples of 43 HBAg sero-carriers. A100-fold concentration of urine samples from thesepatients, however, resulted in seven patients (16%)showing detectable HBAg.
Our findings indicate that the prevalence of HBAgin urine of end-stage renal disease patients withHB5Ag positive serum is substantial. Physiologicalmechanisms that might account for this finding, how-ever, remain unclear. We speculate that altered gb-merular premeability could account for the substan-tial number of patients with detectable urine HBAg.This hypothesis is supported by the finding of quali-tative proteinuria in all end-stage renal diseasepatients in our study and those of Irwin [16] demon-strating urine HBAg concentrations 100-fold greatet

HBAg in urine of hemodialysis patients 327
than serum in patients with abnormal renal functionand proteinuria. In addition, none of our threehealthy carriers (without proteinuria) have HBAg-positive urine, and only a small percentage ofpatients from previous studies in whom renal func-tion was presumably not compromised have HBAg-positive urine.
No significant difference (P > 0.05) in urine outputof the group having HBAg in their urine, vs. thosewithout, rules out the possibility that HBAg-nega-tive urine patients had a large volume of dilute urineresulting in levels of HBAg below the limits of de-tection by the radioimmunoassay. In fact, severalpatients with urine which was positive for HBAghad a urinary output in excess of 1,000 ml per day. Itwould be of interest, however, to monitor thosepatients who are negative for HBAg in their urine,following concentration of the urine specimens andrepeated urine sampling to maximize detection ofviruria.
Hepatitis B infection among hemodialysis patientsis an endemic problem of relatively high frequency.At the time of this survey, 90% of the 27 hemodialy-sis units studied reported hepatitis B infections.Approximately 25,000 patients are being dialyzedthroughout the United States. From the carrier datain our study, at least 2,750 patients might be expect-ed to be HBAg carriers at any given time, 1,900would have significant urine output, and 1,000patients would have detectable HBAg in the urine.
HBAg in the urine may not correlate with itsinfectivity. Further evidence is needed to confirm theinfectivity of urine and to define the characteristics ofinfectious urine, particularly to determine if all mor-phological forms of HBAg, including the wholevirions (Dane particles), cross the glomerulus.Recent studies [24—261 have suggested that the pres-ence of DNA polymerase and e antigen in serum ofHBAg-positive patients appear to be indicators ofthe relative infectivity of this serum. This is particu-larly true in non-percutaneous transmitted hepatitisafter small-volume exposure. To our knowledge,there is no available evidence regarding the presenceof e antigen or DNA polymerase in urine that ispositive for HBAg. There is, however, some evi-dence suggesting that these two apparent indices ofinfectivity are not found in the absence of HBAg inthe serum [261. Thus, it is probable that all urinespositive for HB5Ag are not equally infectious andthat some are not infectious at all. The ability of eantigen and DNA polymerase to define the relativeinfectivity of HB5Ag-positive blood may also applyto HBAg-positive urine. Until it is certain that allbody fluids, including urine, negative for e antigen
and polymerase are non-infectious, and also untilinfectivity tests are available to all dialysis centers,urine from antigenemic hemodialysis patients shouldbe considered a potential vehicle for the transmissionof hepatitis B virus.
Acknowledgments
A portion of this work was presented at the annualmeeting of the Kidney Foundation of Michigan, Lan-sing, Michigan, June 10, 1977. This research is sup-ported by a grant from the Michigan Department ofPublic Health, "Can hepatitis in patients with end-stage renal disease and their contacts be detected orprevented?" We acknowledge the physicians andstaff of the hemodialy sis units who cooperated in thisstudy, Bruce Schreiman for his critical review of themanuscript, and Sanford Izensen, Renal DiseaseControl, Michigan Department of Public Health.
Reprint request to Dr. Gilbert H. Mayor, Department of Medi-cine, Michigan State University, B220 Lfe Sciences, East Lan-sing, Michigan 48824, U.S.A.
References
1. LONDON w'r, DIFIGLIA M, SUTNICK Al, BLUMBERG BS: Anepidemic of hepatitis in a chronic hemodialysis unit. N Engi JMed 281:571—578, 1969
2. SZMUNESS W, PRINCE AM, GRADY GE, MANN MK, LEVINERW, FRIEDMAN EA, JACOBS MJ, JOSEPHSON A, RIBOT S,SHAPIRO FL, STENZEL KH, SuKI WN, VYAS GJ: Hepatitis Binfection: A point-prevalence study in 15 U.S. hemodialysiscenters. JAMA 227:901—906, 1974
3. GARIBALDI RA, FORREST JN, BRYAN JA, HANSON BF, Dis-MUKES WE: Hemodialysis-associated hepatitis. JAMA225:384—389, 1973
4. SNYDMAN DR, BRYAN JA, HANSON BH: Hemodialysis-asso-ciated hepatitis in the United States—1972. J Infect Dis132:109—113, 1975
5. EASTWOOD JB, CURTIS JR, WING AJ, DEWARDENER HE:Hepatitis in a maintenance hemodialysis unit. Ann intern Med69:59—66, 1968
6. WILLIAMS SV, FEINC;LASS EJ, Gs.GG MB, HATCH MH,MATSEN JM: Epidemic viral hepatitis, type B, in hospitalpersonnel. Am J Med 57:904—911, 1974
7. SZMUNESS W: Recent advances in the study of the epidemiol-ogy of hepatitis B. Am J Pathol 81:629—649, 1975
8. PATTISON CP, MAYNARD JE, BERQUIST KR, WEBSTER HM:Serological and epidemiological studies of hepatitis B in heino-dialysis units. Lancet 2:172—176, 1973
9. HEATHCOTE J, CAMERON CH, DANE DS: Hepatitis B antigenin saliva and semen. Lancet 1:71—73, 1974
10. WARD R, BORCHERT P, WRIGHT A, KLINE E: Hepatitis Bantigen in saliva and mouth washings. Lancet 2:726—727, 1972
11. VILLAREJOS VM, VISONA KA, GUTIERREZ A, RODRIQUEZA: Role of saliva, urine and feces in the transmission of type Bhepatitis. N Engi J Med 291:1375—1378, 1974
12. LINNEMANN CC, GOLDBERG S: HBAg in breast milk. Lan-cet 2:155, 1974

328 Hourani et al
13. MAZZUR S: Menstrual blood as a vehicle of Australia antigentransmission. Lancet 2:749, 1973
14. DARANI M, GERBER M: Hepatitis B antigen in vaginal secre-tions. Lancet 2:1008, 1974
15. MARMION BP, TONKIN RW: Control of hepatitis in dialysisunits. Br Med Bull 28:169—179, 1972
16. IRWIN GR, ALLEN AM, BANCROFT WH, KARWACKI ii,BROWN HL, PINKERTON RH, WILLHIGHT M, TOP FH: Hep-atitis B antigen in saliva, urine and stool. Infect Immunol11:142—145, 1975
17. HEATHCOTE J, Tsiis A, SHERLOCK 5: A urinary sub-stance in patients with acute type B hepatitis and their house-hold contacts. Lancet 2:593—595, 1973
18. ORGA PL: Immunologic aspects of hepatitis associated antigenand antibody in human body fluids. J Immunol 110:1197—1205, 1973
19. APOSTOLOV K, BAUER DJ, SELWAY JW, Fox RA, DUDLEYJF, SHERLOCK S: Australia antigen in urine. Lancet 1:1274—1275, 1971
20. TRIPATzI5 I: Australia antigen in urine and feces. Am J DisChild 123:401—404, 1972
21. VITTAL SB, DOURDOUREKAS D, STEIGMAN F: Hepatitis Bantigen in saliva, urine and tears. Am J Gastroenterol 61:133—135, 1974
22. SZMUNESS W, PRINCE AM, BROTMAN B, HIRSCH RL: Hepa-titis B antigen and antibody in blood donors: An epidemiologicstudy. JlnfDis 127:17—25, 1973
23. BLAINEY JD, EARLE A, FLEWETT TH, WILLIAMS LK: Is theurine infective in serum hepatitis? Lancet 1:797, 1971
24. MAGNIUS LO, LINDHOLM A, LUNDIN P, IWAFRON S: A new
antigen-antibody system: Clinical significance in long-termcarriers of hepatitis B surface antigens. JAMA 231:356—359,1975
25. MAYNARD JE, BARRETT DH, MURPHY BL, BRADLEY DW,BERQUIST KR, BENDER TR: Relation of e antigen to hepatitisB virus infection in an area of hyperendemicity. J Infect Dis133:339—342, 1976
26. ALTER HJ, SEEFF LB, KAPLAN PM, MCAULIFFE Ui,WRIGHT EC, GERIN JL, PURCELL RH, HOLLAND PV, ZIM-MERMAN HJ: Type B hepatitis: The infectivity of blood posi-tive for e antigen and DNA polymerase after accidentalneedlestick exposure. N Engl J Med 295:909—913, 1976