-
8/6/2019 Hepatic Adenoma and Focal Nodular Hyperplasia
1/6
Hepatic Adenoma and Focal NodularHyperplasia: Diagnosis and
Criteriafor Treatment
Luciano De Carlis,* Vincenzo Pirotta,* GianFranco
Rondinara,*
Cosimo V. Sansalone,* Giovanni Colella,* Giuseppe
Maione,*Abdallah O. Slim,* Antonio Rampoldi, Alberto Cazzulani,Luca
Belli, and Domenico Forti*
Focal nodular hyperplasia (FNH) and adenomaare rare benign
hepatic tumors, and the standardsfor diagnosis and treatment still
remain controver-sial. Usually adenoma is an indication for
resec-tion, due to its tendency to bleed and to degener-ate; FNH,
on the contrary, may be treatedconservatively. Preoperation
differential diagno-sis is, however, difficult, often impossible.
Materi-als and methods. Thirty-eight patients with pre-
sumed hepatic adenoma and/or FNH were studiedat our department
from 1984 to 1996. Preoperativeassessment included clinical
evaluation andsymptoms, laboratory tests, liver biopsy, ultra-sound
scan, computed tomography scan, mag-netic resonance imaging,
scintigraphy, and angi-ography. Thirteen patients had a
presumeddiagnosis of FNH, 16 of adenoma, and 9 of unde-termined
benign lesions; 27 had hepatic resec-tions (3 with laparoscopic
technique), and 11 werenot operated on and are actually under a
strictfollow-up observation. Results. The final diagno-sis was 19
FNH and 19 adenomas (2 of which
contained areas of hepatocarcinoma). Presumeddiagnosis was
confirmed in 71% of cases. Use oforal contraceptives, abdominal
symptoms, andpathologic liver test results were more frequent
inpatients with adenomas. There were no deathsafter surgery. All
resected patients were tumorfree during the follow-up, and in 10 of
the 11nonoperated cases, the size of the nodules re-mained
unchanged. We conclude that precise
diagnosis of these benign liver tumors remainsdifficult and
sometimes impossible, despite newimaging techniques. Hepatic
resections can beperformed under very safe conditions;
laparo-scopic surgery may play a role in selected cases.Adenomas
and uncertain cases are clear indica-tions for surgery. Only when a
diagnosis of FNHcan be firmly confirmed in asymptomatic patientsis
strict observation without surgery recom-mended.Copyrightr 1997 by
theAmericanAssociation forthe Study of Liver Diseases
I n contrast with hemangioma,1 focal nodular
hyperplasia (FNH) and hepatic adenoma are
very uncommon benign lesions affecting the liver,
and their diagnosis and differentiation may be
difficult. Moreover, their natural history is not well
defined. Because of all these considerations, their
surgical indication and treatment remain controver-
sial. As a consequence of the widespread use of
improved imaging modalities, these tumors are
now recognized more frequently, and more informa-
tion is available on their behavior.2 In particular, a
strict correlation exists between these tumors and
the use of oral contraceptives.3,4 Hepatic adenomas
have the tendency to grow to conspicuous sizes,
and spontan eous ruptu res or bleeding are relatively
frequent. Malignant degeneration has been re-
ported in some cases, and resection is therefore
advisable.5 On the contrary, FNH is often an
incidental finding, and to date there is no convinc-
ing report showing that these tumors can bleed or
degenerate. Because of this, resection may be
avoided when the diagnostic assessment evidences
FNH.2 In clinical practice, computed tomography
(CT), magnetic resonance imaging (MRI), ultra-
sound (US), and angiography are used in an
attempt to determine the nature of the solitary
masses of t he liver, but accurate distinction be-
tween adenoma and FNH before surgery is often
difficult.6-10 Furthermore, percutaneous needle bi-
opsy cannot differentiate these tumors with accu-
racy.11,12
From the *Department of Surgery and Abdominal Transplanta-
tion, the Department of Radiology, and the Department of
Hepatology, Niguarda Hospital, Milan, Italy.
Address reprints request to Luciano De Carlis, MD, Divisione
di
Chirurgia Generale e dei Trapianti Addominali, Pizzamiglio
27,
Ospedale Niguarda, 20162 Milano, Italy.
Copyrightr 1997 by the American Association for the Study of
Liver Diseases
1074-3022/97/0302-0009$3.00/0
Liver Transplantation andSurgery, Vol 3, No 2 (March), 1997:pp
160-165160
-
8/6/2019 Hepatic Adenoma and Focal Nodular Hyperplasia
2/6
The authors report herein their experience in
the treatment of these benign lesions of the liver.
Preoperative findings were matched with definite
diagnoses and with th e results of surgery; when
surgery was unadvisable, the clinical courses of
these patients were closely followed up throughtime. The aim of
this study was both to define the
diagnostic criteria and establish in which cases
surgical treatment of these tumors is indicated.
Materials and Methods
From January 1984 to May 1996, 38 patients with either
hepatic
adenoma or FNH were observed in our surgical department.
Nine patients were observed in the first 6 years, whereas
the
remaining 29 were referred to u s between 1990 and 1996.
The patient population included 37 women and 1 man,
ranging in age from 21 to 57 years (average age, 32.6). No
chronic liver diseases nor abnormalities in serum alpha-
fetoprotein levels were detected in any patients. Thirty
women
(78.9%) had a history of oral contraceptive consumption for
an
average time of 5.8 years (range, 7 months to 12 years)
before
diagnosis.
Ten (26.3%) patients were completely asymptomatic, and
the lesions were discovered during periodic routine examina-
tions (8 cases) or laparotomies (2 cases) performed for
different
medical reasons; 23 (60.5%) complained of abdominal pain,
which was acute in 9 (23.6%); 11 (28.9%) had a palpable
mass,
and 15 ( 39.4%) suffered from vague digestive troubles with
fatigue and sense of heaviness in the right abdomen.
All patients were evaluated with routine laboratory
analyses,
including liver tests. Only alkaline phosphatase, gamma-
glutamyl transpeptidase, and red blood cell count showed
some
abnormalities in 14 cases (36.8%). US scan, liver
scintigraphy,
CT, and selective hepatic angiography were performed in all
cases. MRI, available to u s since 1990, was employed in th e
last
28 patients (Figs. 1, 2). The diagnosis was made by adopting
predefined criteria, slightly modified by the authors.
(Table
1).10,11,12
Percutaneous fine-needle liver biopsies were performed in
all except 3 patients, where fresh frozen section specimens
were
obtained during laparotomy.
FNH was preoperatively diagnosed in 13 cases and adenom a
in 16. In 9 patients, a differential diagnosis could not be
obtained. Two symptomatic patients with diagnosis of FNH, 16
with diagnosis of adenoma, and 9 with uncertain diagnosis
underwent liver resection. Eleven patients were not operated
on
because preoperative stud y, including h istology, showed
the
typical features of FNH; in 8 of these cases no clinical
symptoms
were evident, and in 7, moreover, the lesions were not
easily
resectable because of their central location in the liver
paren-
chyma. All 11 of these lesions were the only lesion in each
patient, with an average size at CT of 4.2 cm (range 2.5 to
5.5).
Right hepatectomy was performed in 3 cases, left hepatec-
tomy in 2, left lateral lobectomy in 4, and segmentectomy or
enucleation in 18. An intraoperative USscan was used rout
inely
to determine the location of the tumor and its relationship
with
the vascular system.
Three superficial nodules, two located in the third and one
in the sixth liver segment were excised by laparoscopic
tech-
nique. Nodules were solitary in 35 of 38 patients ( 92.1%),
whereas 3 patients had multiple tumors: Two had two FNH and
1 had three adenomas. The size of the different nodules
ranged
from 2.5 to 22 cm (mean, 8.7 cm). Intratumor hemorrhage was
noted in five nodules. All the lesions were submitted to
extensive evaluation by a trained path ologist. Follow-up
was
completed in 100% of cases and ranged from 2 months to 12
years (average, 46 months). Patients underwent an annual
check-up with clinical examination, US scan, and biochemical
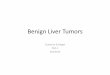
Figure 1. Typical CT appearance of an adenomaof the left liver
lobe. (A) A hypodense area on theleft lateral hepatic segments is
present beforecontrast administration. (B) A typical marked
con-trast enhancement is evident in the early arterialphase.
Hepatic Adenoma and FNH 161
-
8/6/2019 Hepatic Adenoma and Focal Nodular Hyperplasia
3/6
data; CT and/or MRI were performed only when indicated.
Statistical analysis was based on the Students t-test,
assuming
significance when P , .05. The therapeutic protocol wasapproved
by the ethical committee of the hospital, and an
informed consent was obtained from each patient included in
the study.
Results
The final diagnosis in the resected cases was FNH
in 8 patients and hepatic adenoma in 19. These
results appear in Table 2. In 2 patients, an accurate
pathological examination revealed areas of well-
differentiated hepatocarcinoma within the adeno-
matous n odules. Two presumed adenomas were
determined to be FNH, whereas in the nine undeter-
mined cases, four were diagnosed as FNH and five
as adenomas. All presumed FNH were confirmed
both by pathological examinations and by fol-
low-up data. The 11 patients with unresected FNH
are regularly followed in our outpatient clinic, as
mentioned earlier (average follow-up, 23.7 month s;
range, 5 to 39), and the clinical courses were
uneventful except for 1. All 11 patients presented
typical CT, MRI, angiographic, and/or histological
features of FNH. In one case the nodule size
increased from 4.5 to 5.5 cm and is now under
strict evaluation. Preoperative biopsy and postop-
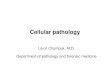
Figure 2. Focal nodular hyperplasia of the leftliver lobe. (A)
MRI shows an isointense mass witha little hyperintense central scar
on T2-weightedimages. (B) At selective angiography a
markedhypervascular lesion appears; the feeding arteryis evident
with rapid contrast filling from thecenter to the periphery of the
node.
Table 1. Diagnostic Criteria for Adenoma and FNH
Adenoma FNH
Enlarging nodules
At CT, ipodensity followed
by a marked contrast
enhancement, calcifica-
tions, capsule, and fat
infiltration
At angiography, vascular
supply from the
periphery to the center
of the node
At biopsy, sheets of
normal hepatocytes
without bile ducts and
Kupffer cells
At CT, isodensity with an
iperdense central scar
(50% of cases)
At angiography, a central
feeding artery with
rapid visualization of
the suprahepatic vein
At MRI, isointense lesion
on T1T2 with hyperin-
tense central scar on
T2
At scintigrams, normal or
increased uptake
At biopsy, normal hepato-
cytes separated by
fibrous septa, prolifer-
ating vessels, bile
ducts, and inflamma-tory cells
Table 2. Comparison Between Presumed and
Definitive Diagnosis in the 38 Considered Patients
FNH Adenoma Uncertain
Presumed diagnosis 13 16 9
Final diagnosis
FNH 13* 2 4
Adenoma 0 14 5
*Including the 11 nonresected patients.Including the 2 cases
with areas of HCC.
De Carlis et al162
-
8/6/2019 Hepatic Adenoma and Focal Nodular Hyperplasia
4/6
erative surgical pathologic evaluation or follow-up
data (in the nonoperated cases) were in agreement,
thus allowing a definite diagnosis in 19 of 35 cases
(54.2%). All preoperative studies showed a diagnos-
tic accuracy of 71% (27/38 patients).
Oral contraceptive use was more frequent in thepatients with
adenoma (17/19 or 89.4%) than in
those with FNH (13/19 or 68.4%; P5 ns). Acute
pain (possibly related to intranodular bleeding)
and pathologic liver test results were significantly
more frequently associated with the presence of an
adenoma or an hepatocarcinoma (P, .05). All
hemorrhagic nodules were adenomas. Other clini-
cal features of our patient population are shown in
Table 3.
No perioperative deaths occurred in the patients
who underwent liver resection. Three p atients had
subdiaphragmatic fluid collections: One was reop-
erated and a small biliary fistula was sealed; theother 2
maintained percutaneous drainages for a
few days. Minor complications occurred in 5 other
patients including pleural effusion in 2, pneumon ia
in 1, and wound suppuration in 2: All were treated
conservatively. The average hospitalization time
was 10.9 days (range, 625). The 3 patients oper-
ated with the laparoscopic technique showed no
postoperative problems and were discharged from
hospital on the 4th postoperative day. During t he
follow-up, one patient died in a traffic accident 3
years after the resection. All the others are alive
with no evidence of tumor recurrence. All patients
had discontinued oral contraceptive use.
Discussion
Our experience seems to confirm that FNH, whencorrectly
diagnosed, may be managed conserva-
tively and monitored with repeated US scans.13,14,15
Problems may exist in obtaining a certain differen-
tial diagnosis between FNH and adenoma and, in
some cases, between benign and malignant tumors.
From our data, only 15/19 (78.9%) of FNH had a
correct preoperative diagnosis with accurate imag-
ing techniques. US scan is nonspecific in the
differentiation of these lesions but h as a great value
as a noninvasive method in the follow-up of both
resected and nonresected patients. CT permits
diagnosis in typical cases when a central scar
within the nodule or a feeding vessel can beobserved, but these
characteristic pictures are pres-
ent only in 50% of patients. Moreover, fibrolamel-
lar carcinoma may present an important fibrotic
component, similar to the central scar described as
typical for FNH. MRI has an accuracy comparable
to CT, and when used together, th ey may add 10%
to 15% to specificity. Selective hepatic angiography
was performed routinely in this series of patients,
giving excellent diagnostic confirmation without
any related complications. Concern exists about its
extensive utilization for benign hepatic lesions
because it has the disadvantage of being an invasive
procedure. The preference for angiography results
from our extensive experience in the treatment of
portal hypertension, in which it proved to be
extremely safe and exhaustive. Furthermore, th e
importance of angiography is incomparable for
technical reasons when planning a liver resection.
The procedure has diagnostic value for FNH when
a feeding artery to the mass is demonstrable: This
was the case in 11 of 19 (57.8%) of our patients
with FNH, and in all, this diagnosis was confirmed
either by postoperative pathologic evaluation or by
follow-up data. In our experience, in t he typical
cases, a suprahepatic vein selectively draining themass was
usually rapidly seen along with the
feeding artery (Fig. 3). To our knowledge, this
observation is n ot reported in the literature and
seems to be a pathognomonic picture of FNH; no
patient with adenoma or other hepatic masses
evidenced such angiographic features. Scintigra-
phy shows normal uptake in all cases of FNH due
to the presence of Kupffer cells, but recent data
Table 3. Clinical Features of the Patients
FNH
(n 5 19)
Adenoma
(n 5 19*)
P
Value
Age (mean 1
range) 33.4 (23-57) 31.8 (21-43) ns
Oral contraceptive
use 13 (68.4%) 17 (89.4%) ns
Symptoms
None 8 (42.1%) 2 (10.5%) ns
Abdominal pain 8 (42.1%) 15 (78.9%) ns
Acute pain 0 (0%) 9 (47.3%) ,.05Palpable mass 5 (26.3%) 6
(31.5%) ns
Vague 5 (26.3%) 10 (52.6%) ns
Biochemical
alterations 2 (10.5%) 12 (63.4%) ,.05
Single lesion 19 (100%) 16 (84.2%) ns
Size (mean) 9.2 7.9 ns
*Including two cases with areas of HCC.
Hepatic Adenoma and FNH 163
-
8/6/2019 Hepatic Adenoma and Focal Nodular Hyperplasia
5/6
demonstrate normal uptake also in 25% of cases of
adenoma; four of our cases confirmed this find-
ing.6,8,13 Laboratory tests and symptoms are not
diagnostic. In case of FNH, however, there is a
tendency to observe asymptomatic masses, inciden-
tally seen, without any biochemical abnormalities.
Adenoma was correctly diagnosed in 12 of 19
cases (63.1%); patients had symptoms present in a
higher percentage of cases, especially when bleed-
ing or sudden growth occurred13,14 (Fig. 4). Labora-
tory tests in most cases show alterations in stasis
indexes. In our series, these signs had statisticalsignificance
in the differentiation between ad-
enoma and FNH. CT and MRI frequently demon-
strate the presence of necrosis or hemorrhage
within the nodules (five cases in our series; Fig. 4);
these findings, however, may be encountered also
in malignant lesions, such as large hepatomas.7,9,10
Either an enlarging lesion or anemia on subsequent
controls may indicate the presence of an adenoma.
On scintigram a reduced uptake is usually evident,
but not always.
Percutaneous liver biopsy alone is reported to be
of little value in the diagnosis of these benign
tumors due to the frequent lack of specific featuresin a small
specimen; moreover, th e material is often
inadequate, and typical signs were p resent in only
54.2% of our cases.11,12 Other problems are related
to the fact that biopsy may be contraindicated in
hemorrhagic lesions, and the distinction between
adenoma and well-differentiated h epatocellular car-
cinoma remains difficult.11 Our study confirms the
strict correlation between adenoma and the use of
oral contraceptives; less evident is the correlation
in cases of FNH, but it un doubtedly seems that the
incidence in patients u sing sex hormones who
manifested FNH is higher than the percentage of
Figure 3. Typical angiographic images of focalnodular
hyperplasia of the right liver lobe. (A)Early arterial phase
showing a hypervascularmass with a central feeding artery: The
contrastdye rapidly fills the node from the center to theperiphery.
(B) In late phases the node is com-pletely opacified, and a
suprahepatic vein, selec-tively draining the node, is well
evidenced.
Figure 4. A 27-year-old female with double he-patic adenoma. CT
scan showed an enormoushemorrhagic and necrotic mass arising from
theleft liver lobe and occupying the whole left hypo-condrium.
Another nonhemorrhagic, contrast-enhanced lesion is evident on the
fourth liversegment.
De Carlis et al164
-
8/6/2019 Hepatic Adenoma and Focal Nodular Hyperplasia
6/6
women in the general population in Italy using
these drugs (68.4% v. 30%). This fact may reflect a
selection bias in the study but is, in our opinion, an
interesting finding.
In the last 10 years, hepatic surgeons have
largely improved their results, and hepatic resec-tions are now
performed safely, with low morbidity
and very low mortality rates. In specialized surgical
units these operations are done without any need
of transfusions and with reduced hospitalization
time.5,13-16 Laparoscopic surgery may, in very se-
lected cases (superficial plongeantlesions), be an
operative option.17 The prolonged duration of
laparoscopic procedures compared with lapa-
rotomic techniques is still a major concern; never-
theless the duration of the operation usually does
not affect the recovery of patients in overall good
condition, and hospitalization time is reduced (4 v.
10.9 days in our series).An important area on which to focus
when
studying these lesions is the risk of not identifying
malignant tumors. Two patients in our series had
adenomas containing degenerated areas of hepato-
carcinoma. Malignant transformation of adenoma
is a rare event, but recent reports point out this
possibility in an increasing percentage of cases.18
In conclusion, all the diagnostic preoperative
studies in our series led to the right diagnosis in
71% of cases, with more than one quarter being
misdiagnosed. It is our opinion that this is the
actual limit in the treatment of these tumors. Our
philosophy, therefore, is to resect all lesions preop-eratively
classified as adenoma, independent of
their location and size. In cases of undetermined
diagnosis, we usually resect all easily resectable
lesions and keep under close observation those in
which the risks of resection seem high; any in-
crease in size or in imaging characteristics should
be signal for excision. Asymptomatic patients who
have a diagnosis of FNH based on the aforemen-
tioned typical signs are also under repeated clinical
and ecographic controls.19
The extensive use of hepatic resection in such
cases can be justified by offering patients the
guarantee of a higher recovery rate, as well as fewer
complications, which specialized liver centers offer
today.
References
1. Belli L, De Carlis L, Beati C, Rondinara GF, Sansalone
CV, Brambilla G. Surgical treatment of symptomatic
giant hemangiomas of the liver. Surg Gynecol Obstet
1992;174:474-478.
2. Kerlin P, Davis GL, McGill DB, Weiland LH, Adson MA,
Sheedy PF. Hepatic adenoma and focal nodular hyper-
plasia: Clinical, pathologic and radiologic features. Gas-
troenterology 1983;84:994-1002.
3. Klastin G. Hepatic tumors: Possible relationship to useof
oral contraceptives. Gastroenterology 1977;73:386-
394.
4. Edmonson HA, Henderson B, Benton B. Liver-cell
adenomas associated with use of oral contraceptives. N
Engl J Med 1976;294:470-472.
5. Leese T, Farges O, Bismuth H. Liver cells adenomas: A
12 year surgical experience from a specialist hepatobili-
ary unit. Ann Surg 1988;203:558-564.
6. Welch TJ, Sheedy PF, Johnson TM, Stephens DH,
Charboneau JW, Brown ML, et al. Focal nodular hyper-
plasia and hepatic adenoma: Comparison of angiogra-
phy, CT, US and scintigraphy. Radiology 1985;156:593-
595.
7. Mathieu D, Bruneton JN, Drouillard J, Caron-Pontreau
C, Vasile N. Hepatic adenomas and focal nodularhyperplasia:
Dynamic CT study. Radiology 1986;292:
1355-1357.
8. Vilgrain V, Flejou JF, Arrive L, Belghiti J, Najmark D,
Meny Y, et al. Focal nodular hyperplasia of the liver: MR
imaging and pathologic correlation in 37 patients. Radi-
ology 1992;184:699-703.
9. Coombs RJ, Woldenberg LS, Skeel RT, Bishara HM,
Merrick HW. Magnetic resonance imaging of hepatic
adenoma. Clin Imaging 1990;14:44-47.
10. Bennet WF, Bova JG. Review of hepatic imaging and a
problem oriented approach to liver masses. Hepatology
1990;12:761-775.
11. Anthony PP. Tumors and tumor like lesions of the liver
and biliary tract. In: MacSween RNM, Anthony PP,
Scheuer PJ (eds). Pathology of the liver (ed 2). Edin-burgh,
Churchill Livingstone, 1987:574-645.
12. Casarella WJ, Knowles DM, Wolf M, Johnson PM. FNH
and liver cell adenoma: Radiologic and pathologic
differentiation. Am J Roentgenol 1978;131:393-402.
13. Belghiti J, Pateron D, Panis Y, Vilgrain V, Flejou JF,
Benhamou JP, Fekete F. Resection of presumed benign
liver tumours. Br J Surg 1993;80:380-383.
14. Iwatsuki S, Todo S, Starzl TE. Excisional therapy for
benign hepatic lesions. Surg Gynecol Obstet 1990;171:
240-246.
15. Pain JA, Gimson AES, Williams R, Howard ER. Focal
nodular hyperplasia of the liver: Results of treatment
and options in management. Gut 1991;32:524-527.
16. Habib NA, Koh MK, Zografos G, Awad RW, Bottino G.
Elective hepatic resection for benign and malignant
liverdisease: Early results. Br J Surg 1993;80:1039-1041.
17. Reich H, McGlynn F, De Caprio J, Budin R. Laparo-
scopic excision of benign liver lesions. Obstet Gynecol
1991;78:956-958.
18. Foster JH, Berman MM. The malignant transformation
of liver cell adenomas. Arch Surg 1994;129:712-717.
19. Reddy KR, Shiff ER. Approach to a liver mass. Semin
Liver Dis 1993;13:423-435.
Hepatic Adenoma and FNH 165