Embed Size (px)
Citation preview

876
Hemorrhagic Infarct of the Brain Withouta Reopening of the Occluded Arteries
in Cardioembolic StrokeJun Ogata, MD, Chikao Yutani, MD, Masami Imakita, MD,
Hatsue Ishibashi-Ueda, MD, Yoshisuke Saku, MD, Kazuo Minematsu, MD,
Tohru Sawada, MD, and Takenori Yamaguchi, MD
We examined the brains of 14 patients (four men and 10 women, mean age 68.9 years) who diedfrom brain herniation after cardioembolic stroke with persistent occlusion of the internalcarotid-middle cerebral arterial axis. Our examination showed hemorrhagic infarct in sevenpatients and pale infarct in the other seven, contradicting the commonly proposed pathophys-iologic mechanism for the development of hemorrhagic infarct that the opening of previouslyoccluded vessels makes an infarct hemorrhagic. Analysis of blood pressure after stroke revealedone or more surges of arterial hypertension or rapid rise of blood pressure in patients withhemorrhagic infarct without a reopening of the occluded artery. Such arterial hypertension wasnot always present in patients with pale infarct. Hemorrhage into an infarct with persistingocclusion of the proximal artery is assumed to occur when the involved blood vessels are exposedto the force of arterial blood pressure from the leptomeningeal collaterals. This occurs whenarterial blood pressure rises after stroke in the presence of efficient leptomeningeal collateralsand before occlusion of these collaterals by a swollen cerebral hemisphere containing a largeinfarct. (Stroke 1989;20:876-883)
Fisher and Adams1 reported a high incidenceof hemorrhagic infarct (HI) in their autopsystudy of cerebral embolism. They usually
found an embolus occluding the proximal artery inpatients with pale infarct. In patients with HI, therewas no embolus occluding the proximal artery, butfragments of the embolus in distal arterial brancheswere found. From these observations, Fisher andAdams proposed that the area of infarct becomeshemorrhagic when an embolus fragments andmigrates distally, thereby opening the previouslyoccluded vessel and exposing necrotic brain to thefull force of arterial blood pressure. This concepthas been further validated by autopsy2-3 andangiographic4'5 studies.
While pathologic examination of brains with HIin our hospital showed a reopening of the occludedartery in most cases, there were some cases in whichHI occurred and the artery remained occluded. This
From the Research Institute (J.O., Y.S.), Division of Pathol-ogy (C.Y., M.I., H.I.), Cerebrovascular Division, Department ofInternal Medicine (K.M., T.S., T.Y.), National CardiovascularCenter, Osaka, Japan.
Address for reprints: Jun Ogata, MD, National CardiovascularCenter, Research Institute, 5-7-1 Fujishiro-dai, Suita, Osaka, 565Japan.
Received August 12, 1988; accepted January 9, 1989.
observation seems to be compatible with that madeby Jorgensen and Torvik,3 who found the entire areaof HI lying distal to the embolus in seven cases. Theysuggested that some blood could have passed beyondthe plug during its migration or pulsation and thatblood flow could also have been established viacollaterals. Mohr and Barnett6 also found in a fewcases that HI occurred distal to the site of thepersisting occlusion in the arterial bed exposed atbest only to retrograde collaterals. Yamaguchi et al7
observed a few cases of massive HI in whichcomplete embolic occlusion was confirmed atautopsy. The importance of retrograde collateralsas unobstructed arterial channels thus has not beenemphasized as has been the importance of thereopening of the occluded artery as the mechanismcausing HI to develop. The role of reperfusion vialeptomeningeal collaterals in hemorrhagic transfor-mation has been validated only in experimentalmodels.8-9 Therefore, we analyzed clinical and patho-logic findings to assess the mechanism that allowshemorrhagic transformation of an infarct with per-sistent occlusion in cardioembolic stroke.
Subjects and MethodsWe evaluated clinical and autopsy findings of 14
patients who died from brain herniation after car-
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

Ogata et al Hemorrhagic Infarct in Embolic Stroke 877
TABLE 1. Clinical Findings of Patients With Hemorrhagic or Pale Brain Infarct
Case Age/sexUnderlying
heart diseasePatients with hemorrhagic infarct of the brain
1
2
3
4
5
6
7
80/M62/F76/F77/F72/F52/F68/F
NVAF with PMIRHD with MR, AfRHD with MR, AfRHD with MSR, AR, AfMVP with PMI for A-V blockRHD with MSRHD with MSR, Af
Patients with pale infarct of the brain8
9
10
11
12
13
14
67/M42/M78/F67/F75/F91/F57/M
MVP
DCM
RHD with MS, AS, AfSSS with PMIRHD with MS, AfOMI, AMI with AfDCM with Af
Duration ofstroke (days)
4.9
2.1
2.6
1.1
3.1
2.7
5.3
6.7
2.2
4.5
2.3
5.2
5.1
10.8
Cerebral arteryexamined byangiography
R CAG, L CAG, R VAGR CAG, L CAGND
ND
L CAG, L VAGRCAGL CAG, L VAG
L CAG, R VAGL CAG, R CAG, L VAGND
R CAG, R VAGL CAG, R CAG, L VAGND
L CAG, L VAG
Interval betweenstroke and
angiography
<6 hours<6 hours
<6 hours<6 hours<8 hours
<6 hours<6 hours
30 hours<6 hours
36 hours
Occlusion of cerebralartery demonstrated
by angiography
R ICA-MCAR ICA, L ACA
L MCA, L ACAR MCA, R ACAL MCA, L PCA
LICAL ICA-MCA-ACA
RICAL ICA-MCA, L ECA
LMCA
M, male; NVAF, nonvalvular atrial fibrillation; PMI, pacemaker implantation; R, right; CAG, carotid angiography; L, left; VAG,vertebral angiography; ICA, internal carotid artery; MCA, middle cerebral artery; F, female; RHD, rheumatic heart disease; MR, mitralregurgitation; Af, atrial fibrillation; ACA, anterior cerebral artery; ND, not done; MSR, mitral stenosis and regurgitation; AR, aorticregurgitation; MVP, mitral valve prolapse; MS, mitral stenosis; DCM, dilated type of idiopathic cardiomyopathy; SSS; sick sinussyndrome; ECA, external carotid artery; OMI, old myocardial infarction; AMI, acute myocardial infarction.
diogenic thromboembolism with persistent occlu-sion of the internal carotid-middle cerebral arterial(ICA-MCA) axis. These patients included four menand 10 women, aged 42-91 years, with a mean ageof 68.9 years. Patients were admitted a few hoursafter stroke and died within 2 weeks in the StrokeCare Unit of the National Cardiovascular Centerfrom 1977 to 1988. We did not include in our studypatients with the following clinical and pathologicfindings: 1) cardiogenic thromboembolism showinga reopening of the occluded artery or migration ofthe embolus, 2) cerebral embolism whose embolicsources were the vegetations of nonbacterial throm-botic endocarditis or bacterial endocarditis,3) treatment with anticoagulants or thrombolyticagents after stroke, 4) previous major strokes in thecarotid system, 5) simultaneous development of
significant embolism to the vertebral or basilarartery, and 6) macerated brain due to prolongedperiod of brain death. Treatment consisted of intra-venous fluid replacement with dehydrating agentssuch as mannitol or glycerol. All patients wereexamined with computed tomography of the brain,and in 10 of 14, angiography of the brain wasperformed after stroke.
The neurologic status, vital signs, and bloodpressure (BP) were examined and recorded every 2hours. BP was measured with a standard mercurysphygmomanometer and an appropriately sized armcuff. Because BP was analyzed in our study toassess the dynamic process of intracranial bloodflow, BP values during the period of brain death,10
when intracranial blood flow can be absent orsignificantly reduced, were not used.
FIGURE 1. Diagrammatic representation of location ofemboli in cerebral arteries in seven cases with hemor-rhagic brain infarct.
Lt.
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

878 Stroke Vol 20, No 7, July 1989
FIGURE 2. Diagrammatic representation of loca-tion of emboli in cerebral arteries in seven caseswith pale brain infarct.
Lt.
At autopsy, the brains were removed and fixed in10% formalin for 2-3 weeks. After fixation, arteriesat the base of the brain were separated from the brainand histologically examined at approximately 3-mmintervals. The extracranial carotid and vertebral arter-ies were examined at approximately 5-mm intervals.The cerebrum was horizontally sectioned every 1cm. Representative sections were taken from thebrain for embedding and histologic examination withhematoxylin and eosin and other methods as needed.Special attention was paid to the source of theembolus to the brain in examining the heart, ascend-ing aorta, and carotid and vertebral arteries.
Both hemorrhagic and pale infarcts of the brainwere determined by gross examination as defined byAdams and Vander Eecken.2 The HI consists of anordinary softening of tissue, the major portion ofwhich is speckled by congested blood vessels andinnumerable small hemorrhages. With pale infarct,the tissue is soft and swollen, with poorly demarcated
anatomic structures. There are no hemorrhages, exceptoccasionally at the margins of the infarct.
ResultsTable 1 shows the clinical findings of the 14
patients with hemorrhagic or pale infarct of thebrain. All 14 cases showed embolic occlusion of thecerebral artery proximal to the infarct.
Eleven patients showed a sudden onset of strokewhile awake with a maximal deficit at the verybeginning of the event. Three patients (Cases 5, 7,and 13) suffered neurologic deficits while in bed, 12patients developed stroke at home, and two patients(Cases 2 and 14) developed stroke during hospitaladmission. In each patient, prothrombin time, activepartial thromboplastin time, and platelet countswere normal. None of the patients showed severeanemia, suggesting that a bleeding disorder was nota factor.
FIGURE 3. Origin of right middle cerebralartery of Case 2 with hemorrhagic braininfarct. Lumen is occluded with fibrin plateletembolus. Bar=0.5 mm.
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

Ogata et al Hemorrhagic Infarct in Embolic Stroke 879
| | Area of pale infarct
^ ^ H Area of hemorrhagic infarct
hematoma (arrows)
FIGURE 4. Diagrammatic representation oflocation of hemorrhagic and pale brain in-farcts in 14 cases. Hemorrhagic infarct ofoccipital lobe associated with descending ten-toral hemiation in absence of embolic occlu-sion of posterior cerebral artery is not shown.Infarct of right cerebral hemisphere in Case11 is shown on left side of diagram and notedwith *.
FIGURE 5. Transverse section through basal gan-glia of Case 3. Hemorrhagic infarct of territorysupplied by right middle cerebral artery (MCA) dueto occlusion of ipsilateral internal carotid arteryand MCA can be seen. Petechiae are confined tocortical ribbon. Bar=2 cm.
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

880 Stroke Vol 20, No 7, July 1989
FIGURE 6. Transverse section through basal ganglia ofCase 4. Hemorrhagic infarct of territory supplied bybilateral middle cerebral arteries can be seen. Petechiaeare confined to cortical ribbon. Bar=2 cm.
The duration between the onset of stroke andcardiac arrest (or brain death if a period of braindeath was present) was 3.1±1.4 days (mean±SD)(range 1.1-5.3 days) in patients with HI and 5.2±2.9days (range 2.2-10.8 days) in patients with paleinfarct.
Table 1 shows the time interval between onset ofneurologic symptoms and angiography. The angio-graphic findings were proper for the site of thearterial occlusion, which was confirmed at autopsy.The internal carotid artery (ICA) was occluded atthe carotid bifurcation in Cases 2, 11, and 12; a fewcentimeters above the carotid bifurcation in Case 9;and at its most distal portion in Cases 1 and 8. Themiddle cerebral artery (MCA) was occluded at itsdivision of the cortical branches in four otherpatients. Separated from the ICA-MCA axis occlu-sion, the distal cortical branch of the anterior cere-bral artery (ACA) was occluded in three and theposterior cerebral artery (PCA) in one patient.Branches of the left external carotid artery wereoccluded in one patient. Cross-filling of the leftACA as demonstrated by right carotid angiographywas delayed in Cases 8 and 12, while cross-filling ofthe right ACA as demonstrated by left carotidangiography was sufficient in Case 1. There wassome retrograde collateral filling to the leptomenin-geal branches of the occluded MCA as demon-strated by carotid or vertebral angiography in Cases
5, 7, and 14. Leptomeningeal collaterals to the areaof infarct were poor in the other patients. Capillaryblush or early venous filling was not found in any ofthe patients.
Five of 14 patients had cerebral ischemic eventsbefore the last stroke. Three patients experienced asingle episode of hemiparesis with minimal residu-als 2 months (Case 1), 2 years (Case 2), and 19 years(Case 8) before death. Occlusion of the proximalportion of the left ACA was found in angiography inCase 2. Case 10 experienced a transient ischemicattack 7 years before death, at which time angiog-raphy showed transient occlusion of the right MCA.Case 11 developed right-sided quadrantanopsia 15months and right hemiparesis 13 months beforedeath, with some residuals.
Of the 14 patients, seven had rheumatic heartdisease with valvular deformities. Of those seven,all except one showed atrial fibrillation. Two patientshad a dilated type of idiopathic cardiomyopathy,and one of them showed atrial fibrillation. Twopatients had mitral valve prolapse. A permanentpacemaker had been implanted in three patients.One patient showed old and acute myocardial infarc-tion with atrial fibrillation and mitral ring calcifica-tion. Six patients (Cases 2, 3, 4, 6, 13, and 14) hadcongestive heart failure before stroke. There wasmural thrombus in the auricle of the left atrium infour (Cases 4, 5, 12, and 13) and in the left ventriclein two (Cases 8 and 10).
Atherosclerotic changes of the arteries at thebase of the brain were severe in one patient (Case5), moderate in eight patients (Cases 1, 2, 3, 4, 7, 8,12, and 13), and slight in five patients (Cases 6, 9,10, 11, and 14). The atherosclerotic changes of thecerebral artery caused no occlusion or significantstenosis of the lumen that could have influenced thedevelopment of the infarct. The ascending aorta,aortic arch, and extracranial carotid and vertebralarteries contained no occlusive lesion or atheroscle-rotic plaques that would give rise to emboli.
The ICA-MCA axis was occluded with thrombo-embolic material in all cases (Figures 1 and 2). Thearteries proximal to the infarct were macroscopi-cally stuffed with emboli colored gray or brown.These emboli were microscopically composed offibrin with some white blood cells and variablenumbers of entrapped red blood cells (Figure 3).The arteries lodged with emboli showed no endo-thelial lesions, such as rupture of atheroma, thatwould produce local thrombus. Occasionally, earlycellular reactions were found at the proximal ordistal margin of the emboli. These emboli wereassociated with various lengths of retrograde andantegrade red thrombi.
Figures 1 and 2 show the site of occlusion withthromboembolic material in 14 cases. Besides theocclusion of the ICA-MCA axis, there was occlusionof the ipsilateral PCA, which branched off directlyfrom the ICA in Cases 7 and 10. In Case 2, theproximal portion of the ACA contralateral to the last
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

Ogata et al Hemorrhagic Infarct in Embolic Stroke 881
FIGURE 7. Transverse section through basal gangliaof Case 14. Pale infarct of territory supplied by leftmiddle cerebral artery and hemorrhagic infarct ofterritory supplied by ipsilateralposterior cerebral arterycan be seen. Bar=2 cm.
embolic event was hypoplastic. Four cases exhibitedembolus occluding the distal cortical branch of theACA, 1-2.5 cm distal to the anterior communicatingartery. Branches of the left external carotid arterywere occluded with emboli in Case 12.
The pathologic and angiographic findings of thecerebral arteries showed a difference in the effi-ciency of collateral circulation to the area of infarctbetween cases with HI and pale infarct. Six ofseven cases with pale infarct showed embolic occlu-sion of the dista! ICA to MCA, obstructing theproximal portion of the ipsilateral ACA. In suchcases, leptomeningeal collaterals from the ACA tothe area of infarct must receive blood flow from thecontralateral ICA crossing the anterior communi-cating artery. Also, of six cases with pale infarctcaused by embolic occlusion of the distal ICA toMCA, one exhibited occlusion of the distal corticalbranch of the ipsilateral ACA, and the other wasassociated with occlusion of the ipsilateral PCA. Bycontrast, five of seven cases with HI showed em-bolic occlusion at various sites of the MCA, provid-ing efficient leptomeningeal collaterals to the area of
infarct from the proximal portion of the ACA throughthe ipsilateral ICA.
All the cerebral hemispheres containing largeinfarcts were swollen with descending tentorial orsubfalcial herniation. Most of them showed tonsillarherniation and secondary brainstem hemorrhage.
Seven brains contained HI in the area distal to thearterial occlusion (Figures 4, 5, and 6). Case 2showed HI of the area supplied by the right MCAand pale infarcts of the area supplied by the rightACA and the small medial portion of the areasupplied by the left ACA. Although the basal gan-glia were involved in the infarct in Cases 1, 2, and 3,the basal ganglia were hemorrhagic in Cases 1 and 2and pale in Case 3. Case 7 showed a frank hematomameasuring 4.5x2.3x2.3 cm within the HI lateral tothe basal ganglia.
There were innumerable discrete petechiae orconfluent purpura confined principally to the corti-cal gray matter of the area of infarct, whereas thewhite matter involved in the infarct remained pale.The discrete petechiae appeared in the cortical graymatter, commonly more marked within the perisul-
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

882 Stroke Vol 20, No 7, July 1989
C7t
150
140
130
120
110
100Q.
OD 90
80
70
60
50
Patientswith hemorrhagic
infarct
150
140
130
120
70
60
50
Patientswith pale infarct
££ 2 3 4 5gS Days after stroke
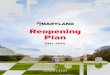
FIGURE 8. Mean blood pressure course after strokefor patients with hemorrhagic and pale brain infarcts.Blood pressure values are expressed as mean of valuesobtained every 4 hours during each 12-hour period.Numbers at left side of curves indicate case number ofpatient.
2 3 4 5 6 7 8 9 10Days after stroke
cal cortex than at the crowns of the gyri. In general,they were evenly distributed in the infarct, andthere was no tendency to appear predominantly atthe margin of the infarct (Figures 5 and 6). Micro-scopically, cortical gray matter showed small hem-orrhages around small vessels and capillaries whoselumina were distended and overflowed with redblood cells. Many hemorrhages were observed tobe confluent, thus making larger hemorrhages. Thesehemorrhages were observed only in the area of theinfarct consisting of ischemic change of the neuronsand glial reactions. Fragments of the embolus in thedistal branches were not encountered in the ordi-nary histologic sections.
Seven brains contained pale infarct in the area ofarterial occlusion (Figures 4 and 7).
Case 6 with HI of the area supplied by the MCAand ACA and three others (Cases 11, 13, and 14)with pale infarct of the area supplied by the MCAshowed HI of the mesial and inferior sides of theipsilateral occipital lobe. This HI was associatedwith descending tentorial herniation of the uncusand hippocampus in the absence of embolic occlu-sion of the PCA (Figure 7).
Six patients (Cases 3, 4, 5, 7, 12, and 13) had ahistory of hypertension. The mean of the meanblood pressure (MBP) obtained every 4 hours dur-ing each 12-hour period after stroke was plotted inFigure 8. In patients with HI, there was a rise ofMBP after stroke except for Cases 3 and 7, whoshowed temporary fall of MBP in the first 24 and 36hours after stroke. Case 1 showed several surges ofhypertension.
Two patients with a dilated type of idiopathiccardiomyopathy (Cases 9 and 14) showed some risein MBP after stroke, but overall BP values were inthe normotensive or hypotensive range. Cases 10and 11 with pale infarct showed progressive fall ofMBP after stroke. Three patients (Cases 8, 12, and13) who lacked collateral pathway from the proxi-mal portion of the ACA through the ipsilateral ICA
to the area of infarct showed a rise of MBP aftertemporary fall of MBP.
DiscussionFor hemorrhagic transformation of a pale infarct
to occur, there must first be ischemic insult ofsufficient degree to induce disruption of the vascu-lar wall followed by restoration of circulation to theinjured vascular bed. Hemorrhagic infarct of thebrain usually appears in patients with reopening ofthe artery occluded by thromboembolus.1-5 How-ever, our study substantiated the existence of HI ofthe brain developing without a reopening of theoccluded artery, implying other routes ofreperfusion.3-6
In cases of HI without a reopening of the occludedarteries, the only possible route of reperfusion ofthe blood to the necrotic area is assumed to be theleptomeningeal arteries. Vander Eecken andAdams11 verified large and important arterial anas-tomoses on the surface of the brain between thethree cerebral arteries. They observed four to eightanastomoses between the ACA and MCA, three tofive anastomoses between the MCA and PCA, andup to two anastomoses between the ACA and PCA,with an average diameter of 311 /xm. It is assumedthat vessels in vasoparalysis within the necroticbrain tissue are exposed to the force of bloodpressure via retrograde leptomeningeal collaterals.
The operation of this mechanism can be sup-ported by the observation of blood pressure afterstroke. Surges of BP into the hypertensive range orrapid rise of BP after stroke are likely to be associ-ated with HI of the brain, with persisting occlusionof the proximal artery. To produce hemorrhagictransformation of an infarct, surges of arterial hyper-tension must occur before swelling of the brainbecomes severe enough to cause herniation, whichwould obstruct all possible collaterals to the necroticarea. Cerebral lesions of patients showing surges ofarterial hypertension after stroke would therefore
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

Ogata et al Hemorrhagic Infarct in Embolic Stroke 883
be pale when arterial hypertension occurred afterthe development of herniation. Because of distor-tion of the rostral brainstem in the case of massivecerebral infarct, BP usually rises because ofincreased sympathetic activity.12-13 The absence ofBP rise in spite of increased sympathetic activitysecondary to the intracranial events in somepatients could be attributed to their decreasedcardiac function.
Although chronic hypertension has no apparentrelation to the development of HI or hematomaformation in patients with cardioembolic stroke inclinical14 or autopsy3 studies, there is a definiterelation between blood pressure and HI using themethod of analysis in our study.
The most feared complication of the early admin-istration of anticoagulants to patients with embolicstroke is hemorrhagic transformation of an infarctor hematoma formation within the infarct.15'16 Thecerebral embolism study group14 has reported that alarge infarct is prone to become hemorrhagic spon-taneously even without anticoagulants, and thatexcessive anticoagulation or acute hypertensioncontributed to hemorrhagic transformation in anti-coagulated patients. These reports are compatiblewith our findings. Therefore, our observationsstrengthen the suggestions made by the CerebralEmbolism Study Group14 that special efforts toavoid excessive anticoagulation and to avoid hyper-tension are needed for patients with large embolicinfarct.
In conclusion, HI, which requires efficient collat-eral pathways of blood flow and surges of arterialhypertension after stroke, was shown to developeven in the absence of the reopening of the arteryoccluded by cardiogenic thromboembolus. An exper-imental study is in progress to analyze the patho-physiologic mechanisms of hemorrhagic transforma-tion of an infarct without a reopening of the occludedproximal artery (Y. Saku, J. Choki, R. Waki, J.Masuda, K. Tamaki, M. Fujishima, J. Ogata, unpub-lished observations).
References1. Fisher CM, Adams RD: Observations on brain embolism
with special reference to the mechanism of hemorrhagicinfarction. J Neuropathol Exp Neurol 1951;10:92-93
2. Adams RD, Vander Eecken HM: Vascular diseases of thebrain. Annu Rev Med 1953;4:213-252
3. Jorgensen L, Torvik A: Ischemic cerebrovascular diseasesin an autopsy series, Part 2. Prevalence, location, pathogen-esis, and clinical course of cerebral infarcts. J Neurol Sci1969;9:285-320
4. Dalai PM, Shah PM, Sheth SC, Deshpande CK: Cerebralembolism, angiographic observations on spontaneous clotlysis. Lancet 1965;l:61-64
5. Irino T, Taneda M, Minami T: Sanguineous cerebrospinalfluid in recanalized cerebral infarction. Stroke 1977;8:22-24
6. Mohr JP, Barnett HJM: Classification of ischemic stroke, inBarnett HJM, Stein BM, Mohr JP, Yatsu FM (eds): Stroke,Pathophysiology, Diagnosis and Management. New York,Churchill Livingstone, Inc, 1986, pp 281-291
7. Yamaguchi T, Minematsu K, Choki J: Arterial embolism, inWood JH (ed): Cerebral Blood Flow, Physiological andClinical Aspects. New York, McGraw-Hill Book Co, 1987,pp 503-517
8. Faris AA, Hardin CA, Poser CM: Pathogenesis of hemor-rhagic infarction of the brain. Arch Neurol 1963;9:468-472
9. Laurent JP, Molinari GF, Oakley JC: Primate model ofcerebreal hematoma. J Neuropathol Exp Neurol 1976;35:560-568
10. Ogata J, Yutani C, Imakita M, Ueda H, Waki R, Ogawa M,Yamaguchi T, Sawada T, Kikuchi H: Autolysis of thegranular layer of the cerebellar cortex in brain death. AdaNeuropathol (Berlin) 1986;70:75-78
11. Vander Eecken HM, Adams RD: The anatomy and func-tional significance of the meningeal arterial anastomoses ofthe human brain. J Neuropath Exp Neurol 1953;12:132-157
12. Myers MG, Norris JW, Hachinski VC, Weingert ME, SoleMJ: Cardiac sequelae of acute stroke. Stroke 1982;13:838-842
13. Thompson RK, Malina S: Dynamic axial brain-stem distor-tion as a mechanism explaining the cardiorespiratory changesin increased intracranial pressure. J Neurosurg 1959;16:664-675
14. Cerebral Embolism Study Group: Immediate anticoagula-tion of embolic stroke: Brain hemorrhage and managementopinions. Stroke 1984;15:779-789
15. Hart RG, Easton JD: Hemorrhagic infarcts. Stroke 1986;17:586-589
16. Yatsu FM, Hart RG, Mohr JP, Grotta JC: Anticoagulation ofembolic strokes of cardiac origin: An update. Neurology1988;38:314-316
KEY WORDS• embolus
cardiovascular diseases • cerebral hemorrhage
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from

YamaguchiJ Ogata, C Yutani, M Imakita, H Ishibashi-Ueda, Y Saku, K Minematsu, T Sawada and T
cardioembolic stroke.Hemorrhagic infarct of the brain without a reopening of the occluded arteries in
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1989 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.20.7.876
1989;20:876-883Stroke.
http://stroke.ahajournals.org/content/20/7/876World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 29, 2018
http://stroke.ahajournals.org/D
ownloaded from