Embed Size (px)
DESCRIPTION
Hemodynamic Disorders, Thromboembolic Diseases,
Citation preview
Hemodynamic Disorders,
Thromboembolic Diseases, and Shock
DE PEDROPALERBSPHIII

ContentsEdemaThrombosisHemostasisEmbolismInfarctionHemorrhageShock
Edema

•abnormal increase in interstitial fluid within tissues • caused by either increased capillary pressure or
diminished colloid osmotic pressure•mostly seen in subcutaneous tissues, lungs and brain.•Type of edema: exudate in inflammatory and
transudate in non inflammatory conditions

Edema - Pathogenesis
PATHOPHYSIOLOGIC CATEGORIES OF EDEMA

I. Increased Hydrostatic Pressure
• results to focal impairment in venous return.•Most common cause - Congestive heart failure,
others – DVT
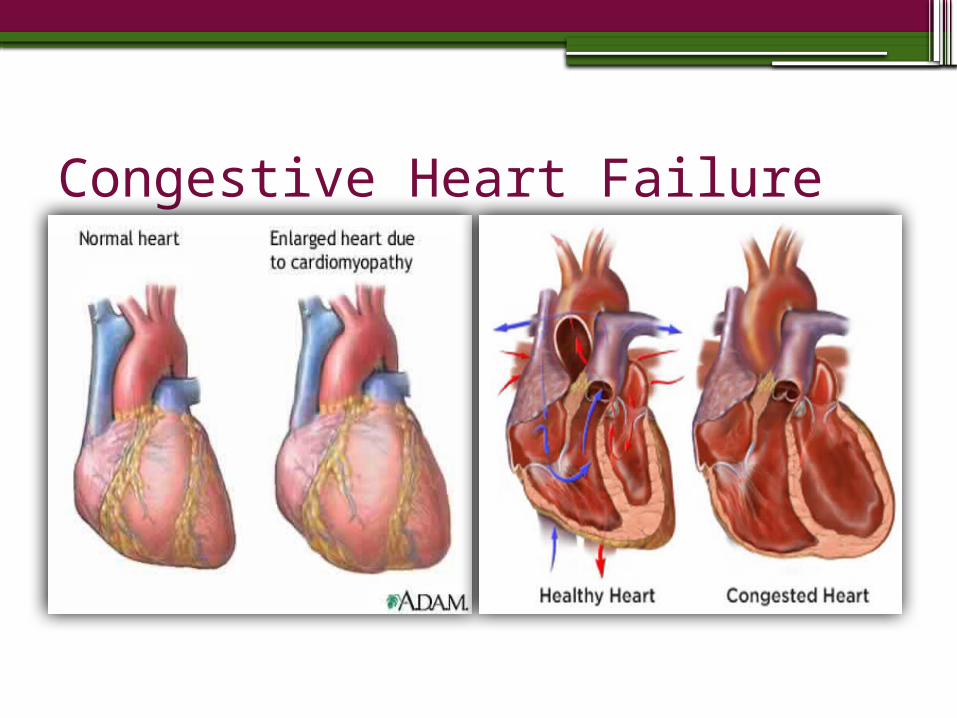
Congestive Heart Failure
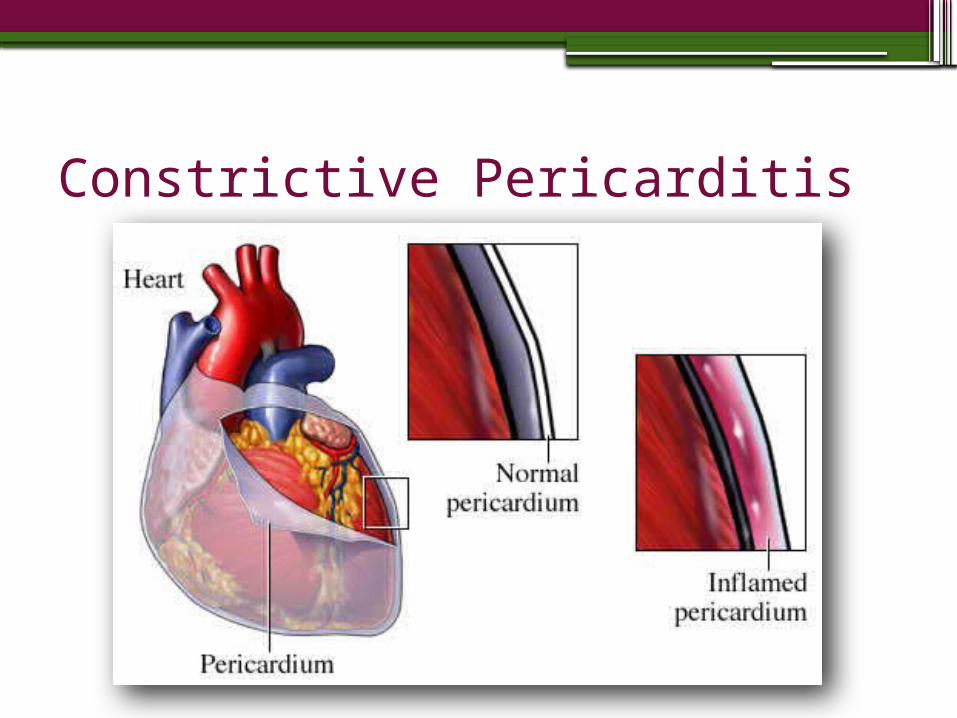
Constrictive Pericarditis
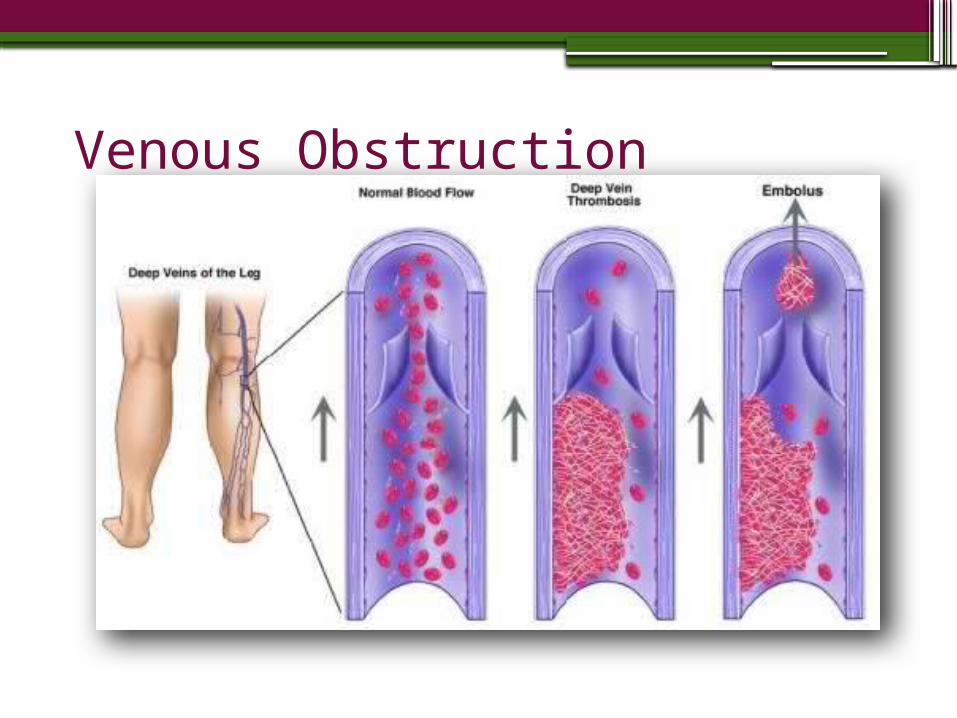
Venous Obstruction

II. Reduced Plasma Osmotic Pressure
•occurs when albumin is not synthesized in adequate amounts or is lost from the circulation
• results to a net movement of fluid into the interstitial tissues with subsequent plasma volume contraction
Nephrotic syndrome, Cirrhosis, Malnutrition

Ascites (Liver Cirrhosis)

III. Sodium and Water Retention
• causes both increased hydrostatic pressure and diminished vascular colloid osmotic pressure.
•occurs whenever renal function is compromised•Renal failure, Renin- Angiotensin - Aldosterone

IV. Lymphatic Obstruction
• causes chronic inflammation with fibrosis, invasive malignant tumors, physical disruption, radiation damage and infectious agents

Hyperemia & Congestion


Hyperemia• Locally increased blood volumes•Active Process
Arteriolar dilation leads to increased blood flow•Redness – due to engorgement with oxygenated
blood• ‘Erythema

Erythema

Congestion• locally increased blood volumes•Passive process ▫resulting from reduced outflow of blood from a tissue.
• can be systemic or local• blue-red color (Cyanosis)• Commonly leads to Edema

Cyanosis


%

Chronic Passive Congestion• Lack of blood flow
Leads to:- chronic hypoxia- ischemic tissue injury and scarring
• Capillary rupture
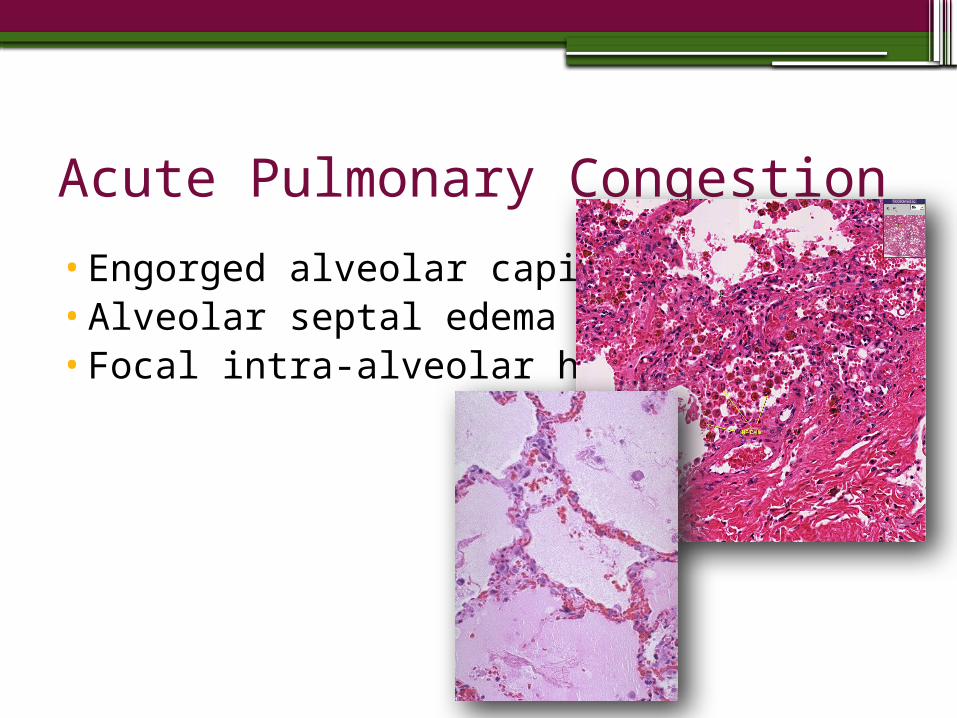
Acute Pulmonary Congestion
•Engorged alveolar capillaries •Alveolar septal edema •Focal intra-alveolar hemorrhage

Chronic Pulmonary Congestion•Thick and fibrotic septa•Heart failure cells ▫Hemosiderin - laden
macrophages in alveoli

Acute Hepatic Congestion•Distended central vein and
sinusoids•Centrilobular hepatocytes
can be ischemic•Periportal hepatocytes may
only develop fatty change.

Chronic Passive Hepatic Congestion
•The centrilobular regions are grossly red - brown and slightly depressed.▫ centrolobular necrosis +
hemorrhage▫periportal fatty change▫ cardiac fibrosis

•Microscopically:▫Central vein is congested as
well as the hepatic sinusoids▫centrilobular hemorrhage▫hemosiderin-laden
macrophages▫degeneration of hepatocytes
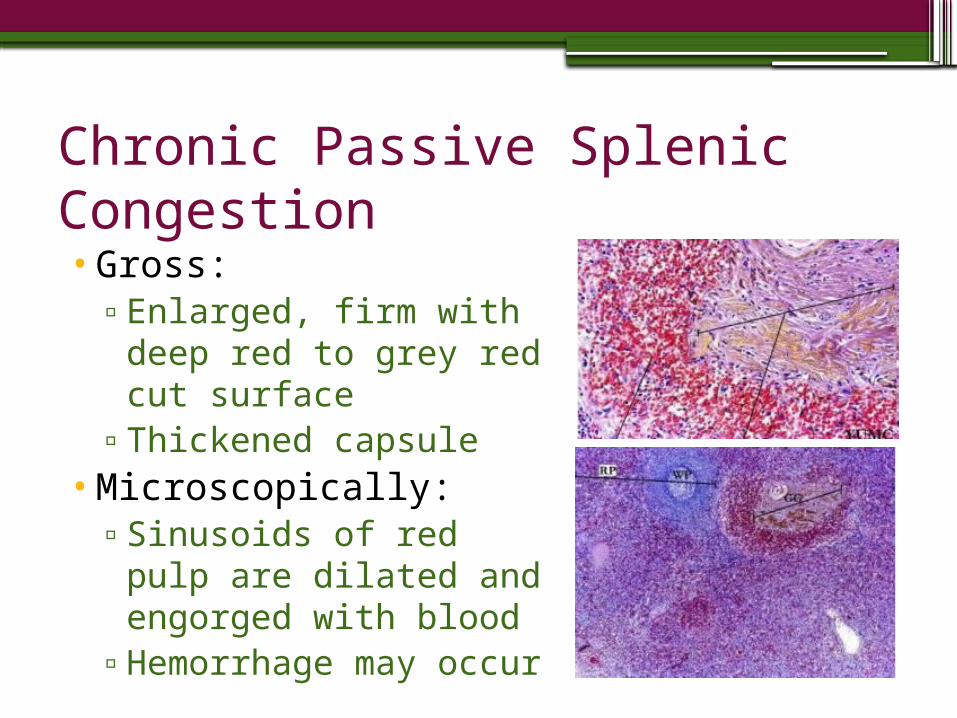
Chronic Passive Splenic Congestion•Gross:▫Enlarged, firm with deep red
to grey red cut surface▫Thickened capsule
•Microscopically:▫Sinusoids of red pulp are
dilated and engorged with blood
▫Hemorrhage may occur
Hemostasis

Hemostasis and Thrombosis
•Three general components:▫Vascular wall (endothelium)▫Platelets▫Coagulation cascade

SEQUENCE of EVENTSfollowing VASCULAR INJURY

•Vasoconstriction▫Reflex neurogenic
mechanism;▫endothelin

•Primary hemostasis▫Platelet adhesion
and aggregation
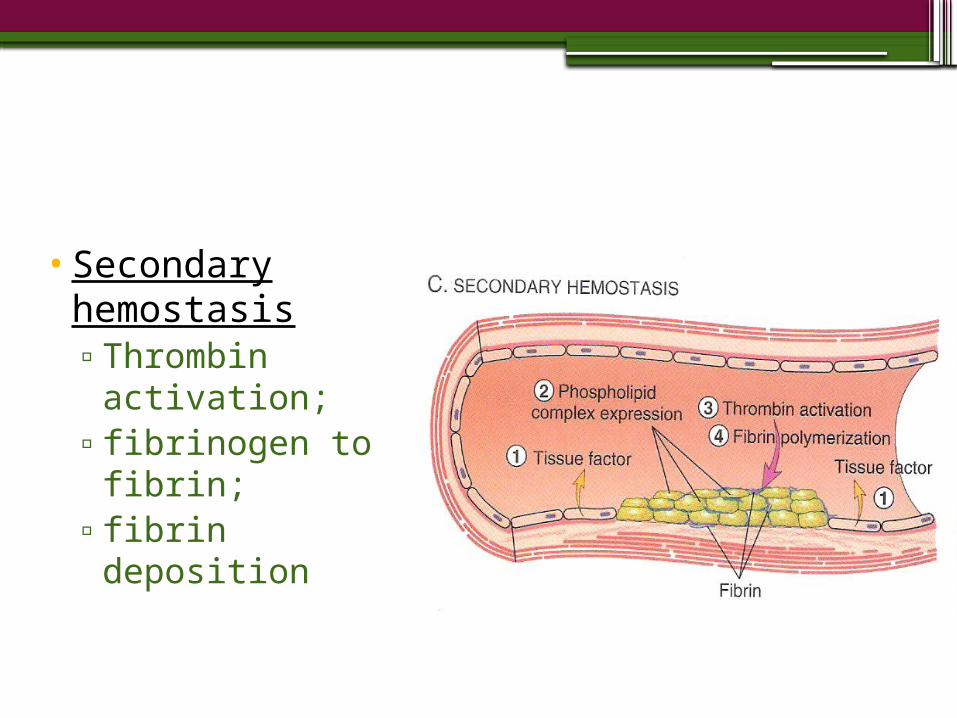
•Secondary hemostasis▫Thrombin activation; ▫fibrinogen to fibrin; ▫fibrin deposition

•Thrombus and antithrombotic events▫Fibrin polymerizes▫TPA limits plug

Hemorrhage

Hemorrhage•Extravasation of blood into the extravascular space.•Hemorrhagic Diathesis▫ increased tendency to hemorrhage that occurs in a
variety of clinical disorders •within tissue – hematoma

•Petechiae - 1 - 2 mm; skin + mucosa▫ Intravascular pressure, platelets
•Purpura - ≥ 3 mm▫trauma, vasculitis, vascular fragility
•Ecchymoses - > 1 to 2 cm▫B ruise; R B C phagocytosis by macrophages: Hb (red -
blue) ®bilirubin (blue-green) hemosiderin (golden - brown)

•Accumulation of blood in the Cavity▫Hemothorax▫Hemopericardium▫Hemoperitoneum▫Hemarthrosis
Hemorrhage sequelae• Loss volume▫>20% - hemorrhagic shock
• Loss rate▫Acute - hemorrhagic shock▫Chronic - peptic ulcer, menstrual bleeding
Iron deficiency anemia•Site of hemorrhage▫Subcutaneous tissues - fatal in brain

Thrombosis

Thrombosis
•The formation of a blood clot (thrombus) in an uninjured vessel after an injury.
•The THROMBUS is formed of blood elements essentially platelets.

3 Primary abnormalities
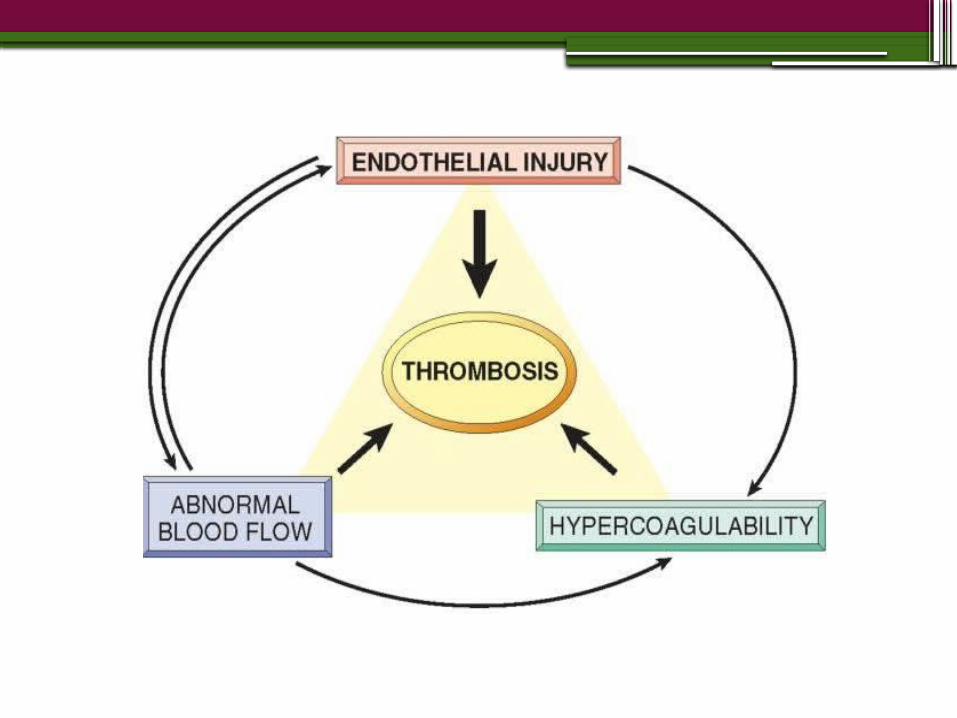
•Virchow’s triad▫Endothelial injury▫Stasis or turbulence of blood flow▫Blood hypercoagulability

Types of Thrombi•Pale Thrombus▫In a flowing blood
as in cardiac chambers or in
arteries.▫Formed mainly of
platelets▫FIRM PALE
REDDISH G RE Y
•Red Thrombus▫In a stagnant blood adjacent to complete
vascular occlusion▫Formed of fibrin
platelets▫SOFT DARK RED &
G ELATI N O U S
•Mixed Thrombus▫ In a slowly flowing blood usually in veins
& arteries.▫ Formed of
alternating layers of platelets and fibrin▫ALTER N ATI N G
RED & PALE LAY ERS

Pale Thrombus•Site: heart valve,
artery•Component: Platelet,
fibrin

Red Thrombus

•Site: heart chamber, vein
•Component: Platelet, fibrin, R B C
Mixed Thrombus

Mural thrombosis
• Thrombi occurring in heart chambers or in the aortic lumen.
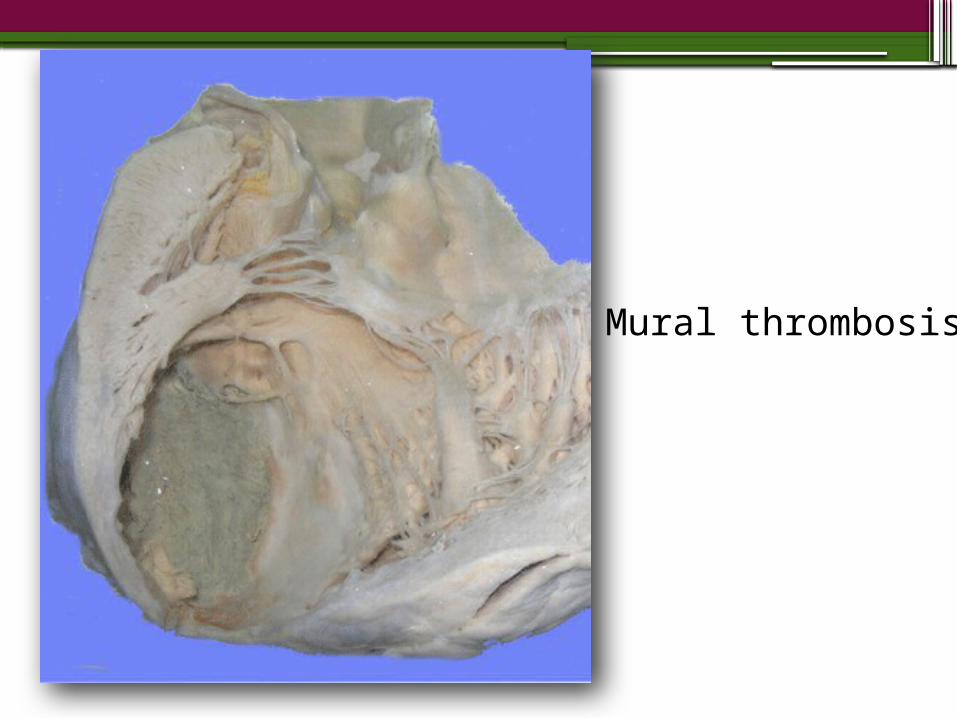
Mural thrombosis

Fibrinous thrombi are
visible within parts of capi.
of the glomerulus
•hyaline thrombi in a glomerulus

Pathogenesis

Pathogenesis
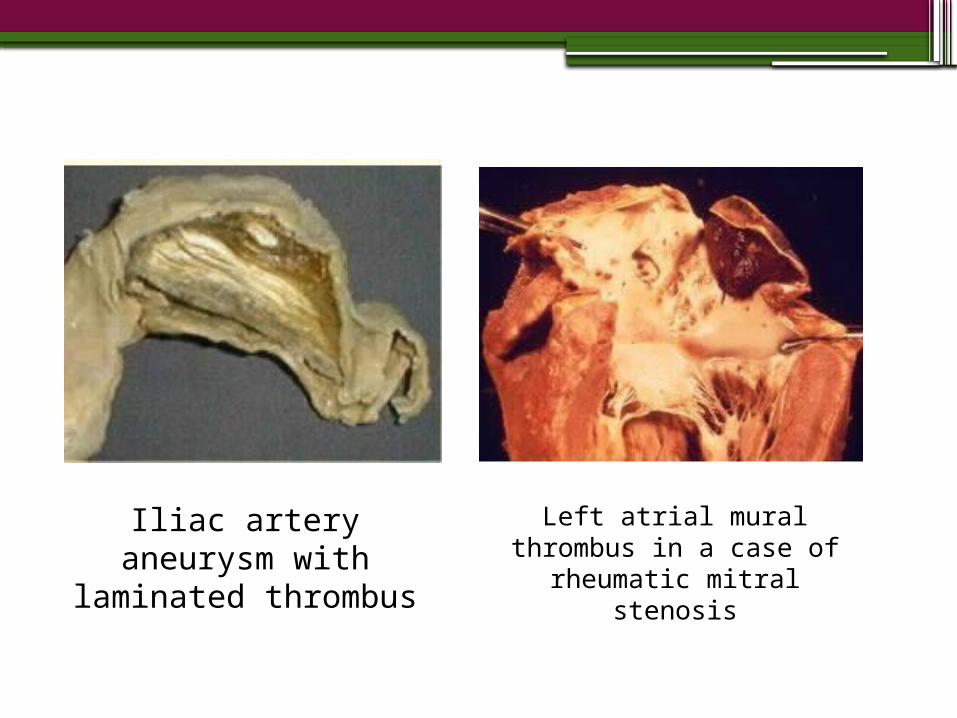
Iliac artery aneurysm with laminated thrombus
Left atrial mural thrombus in a case of rheumatic
mitral stenosis

Pathogenesis
Fate of Thrombus▫Propagation
Thrombi accumulate additional platelets and fibrin.
▫Embolization Thrombi dislodge and travel to other sites in the vasculature
▫Dissolution the result of fibrinolysis, which can lead to the rapid
shrinkage and total disappearance of recent thrombi.
▫Organization and recanalization Older thrombi become organized by the ingrowth of
endothelial cells, smooth muscle cells, and fibroblasts


Morphology•Thrombi may develop anywhere inside the C V S.•They are variable in size and shape depending on its
site of origin and the causes of their development.•Thrombi are significant because they cause
obstruction of arteries and veins, and are sources of emboli.

Arterial or Cardiac Thrombi Venous Thrombi

Arterial/Cardiac Thrombosis•Atherosclerosis – major cause.
Loss of endothelial integrity with abnormal vascular flow•Acute Myocardial infarction = old atherosclerosis +
fresh thrombosis

Occlusive arterial thrombus

Venous Thrombosis (Phlebothrombosis)
•Occlusive▫occur in the superficial or deep veins of the leg.
•Superficially,▫venous thrombi typically occur in the saphenous veins
in the setting of varicosities.•Gross: firm, red, attached to wall•Microscopically: RBC + fibrin•known as red, or stasis.

•Deep Venous Thrombosis (DVT)▫In the larger veins (at or above the knee)▫more serious because thrombi embolize to the
lungs.
Disseminated Intravascular Coagulation (DIC)• the sudden or insidious onset of widespread fibrin
thrombi in the microcirculation.▫Obstetric complications▫Advanced Malignancy▫Shock
•Not a primary disease but rather a potential complication.

Embolism

Embolus•An embolus is a detached intravascular solid, liquid,
or gaseous mass that is carried by the blood to a site distant from its point of origin.
•Coined by Rudolf Virchow in 1848.
▫fat droplets, nitrogen bubbles, atherosclerotic debris (cholesterol emboli), tumor fragments, bone marrow, or even foreign bodies.
Types of Embolism•Pulmonary embolism▫95% venous emboli from deep leg veins▫Depending on the size may lodge pulmonary artery
bifurcation (saddle embolus) or in the small arterioles.▫Most pulmonary emboli are clinically silent (small)▫Sudden death, right heart failure (cor pulmonale)
occurs when more 60% or more of the pulmonary circulation is obstructed by emboli

Types of Embolism•Systemic thromboembolism▫Emboli traveling in arterial circulation▫80% from intracardiac mural thrombi▫Aortic aneurysm, thrombi, atherosclerotic plaques,
paradoxical thrombi▫Lower extremities (75%); brain (10%)
Types of Embolism
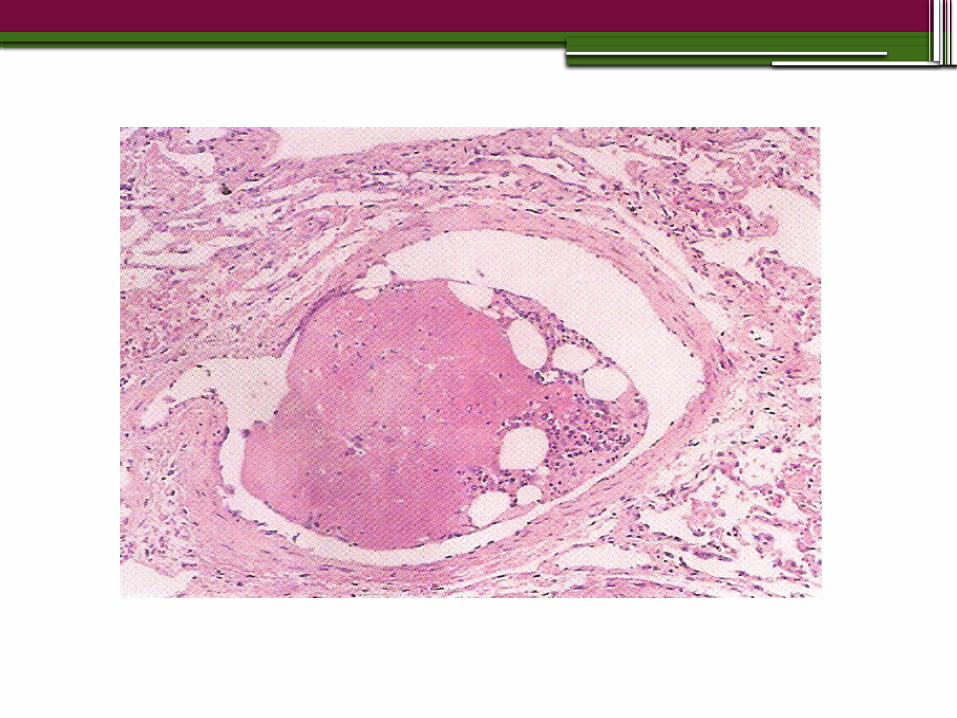
•Fat embolism▫Microscopic fat globules seen in circulation▫90% with severe skeletal injuries▫Pulmonary insufficiency, neurologic symptoms,
anemia and thrombocytopenia (1-3 days after injury)

Types of Embolism•Air embolism▫Excess of more than 100cc is required to have clinical
effect▫Decompression sickness- sudden change in
atmospheric pressure▫Bends (gas bubbles within skeletal muscles) (caisson’s
disease)

Types of Embolism•Amniotic fluid embolism▫1 in 50,000 deliveries▫Infusion of amniotic fluid or fetal tissue into the
maternal circulation via tear in the placenta or rupture of uterine veins.


Infarction
Infarction•Ischemic necrosis caused by occlusion of
either arterial supply or the venous drainage•99% of all infarcts results from thrombotic
episodes•Almost all result from arterial occlusion

Infarction
•Red infarct – venous occlusion, loose tissues, tissue with dual circulation
•White infarct – arterial occlusions solid organs•Mostly ischemic coagulative necrosis•Brain-liquefactive necrosis

Infarction Factors
•NATURE of VASCULAR SUPPLY•RATE of DEVELOPMENT▫SLOW (BETTER)▫FAST (WORSE)
•VULNERABILITY to HYPOXIA▫MYOCYTE vs. FIBROBLAST
•BLOOD OXYGEN CONTENT

Morphology•1. red infarcts▫venous occlusion▫ loose tissue (lung) – blood collection▫dual circulation – lung + bowel▫previously congested organs▫ reperfusion (angioplasty, drug-induced thrombolysis)
•2. white infarcts▫arterial occlusion▫ solid organs – heart (yellow), spleen, kidney

RED VS. WHITE

Morphology•wedge shape▫apex to occluded artery▫base to organ periphery
+ fibrinous exsudate (pleuritis, pericarditis epistenocardiaca)
•onset – poorly defined, hemorrhagic• in time – sharper margins + hyperemic rim

WEDGE SHAPED SCARRED INFARCT following the distribution of an end
artery branch of the renal artery. FIBROSIS implies that it is old
(months to years)

•ischemic coagulative necrosis – 3 zones▫dominant histologic characteristic of infarction
•1. total necrosis - centre▫loss of nuclei, eosinophilia of cytoplasm,
architecture is preserved•2. partial necrosis▫some cells survive▫inflammation (neutrophils) – 1-2 days
degradation of dead tissue

•healing ▫granulation tissue (5-7 day) fibrous scar (6-8
weeks)▫In brain – liquefactive necrosis pseudocyst

•Septic infarctions▫occur when infected cardiac valve vegetations
embolize or when microbes seed necrotic tissue. ▫the infarct is converted into an abscess, with a
correspondingly greater inflammatory response.

Shock
Shock
•characterized by systemic hypotension due either to reduced cardiac output or to reduced effective circulating blood volume.
•Consequences:▫impaired tissue perfusion ▫cellular hypoxia

Shock•the final common pathway for several
potentially lethal clinical events:▫severe hemorrhage, ▫extensive trauma or burns, ▫large myocardial infarction, ▫massive pulmonary embolism, and microbial
sepsis.

Shock•Features:▫hypotension, tachycardia, tachypnea, cool
cyanotic skin•Causes:▫Cardiogenic▫Septic▫Hypovolemic

Cardiogenic Shock• results from low cardiac output due to myocardial
pump failure. •This can be due to intrinsic myocardial damage
(infarction), ventricular arrhythmias, extrinsic compression, or outflow obstruction.▫MI▫Ventricular rupture▫Arrythmia▫Cardiac tamponade▫Pulmonary embolism

Hypovolemic Shock
•results from low cardiac output due to the loss of blood or plasma volume▫Hemorrhage▫Fluid loss (e.g. vomiting, diarrhea, burns)
Septic Shock• results from vasodilation and peripheral pooling of
blood as part of a systemic immune reaction to bacterial or fungal infection.▫Overwhelming microbial infection▫Endotoxic shock▫Gram positive septicemia▫Fungal sepsis▫Superantigens

Shock
•Neurogenic Shock▫loss of vascular tone – e.g. spinal cord injury

Shock
•Anaphylactic Shock▫denotes systemic vasodilation and increased
vascular permeability caused by an IgE–mediated hypersensitivity reaction.
▫acute widespread vasodilation results in tissue hypoperfusion and hypoxia.
Clinical Stages
Non-progressive Progressive Irreversible

Morphology•brain - ischemic encephalopathy ▫tiny ischemic infarctions (border zones)
•heart ▫ subendocardial hemorrhage + necroses, contr. bands
•kidney - acute tubular necrosis (shock kidney)▫pale, edematous▫ tubular epithelium necroses casts
• lung – diffuse alveolar damage (shock lung)▫heavy, wet▫ congestion + edema + hyaline membranes
Morphology•adrenal gland▫ lipid depletion
•GIT – hemorrhagic enteropathy▫mucosal hemorrhages + necroses
• liver ▫fatty change, central necrosis

Clinical Stages•1. nonprogressive▫Compensatory mechanism (neurohumoral)
activation▫centralization of blood circulation
•2. progressive▫tissue hypoperfussion – metabolic dysbalancies
•3. irreversible▫incurred cellular damage + tissue injury

Clinical Progression of Symptoms• Hypotension
• Tachycardia
• Tachypnea
• Warm skin Cool skin Cyanosis
• Renal insufficiency
• Obtundance
• Death





























