Embed Size (px)
Citation preview

Hemodynamic and Endocrine Changes Associated with
Captopril in Diuretic-Resistant Hypertensive Patients
TOSHIRO FUJITA, M.D. KATSUYUKI ANDO, M.D. HIROSHI NODA, M.D. YUJI SATO, Ph.D. NOBUKI YAMASHITA, M.D. KAMEJIRO YAMASHITA, M.D.
Ibaraki, Japan
To evaluate the therapeutic efficacy of oral angiotensin-converting enzyme inhibition with tow-dose (average 30 mg/day) captoprii in diuretic-resistant hypertension, its lone_term cardioc&cuietory action was determined by dye-dilution method and venous-occlusion forearm piethysmography in 11 uncontrolled patients taking a thiazide diuretic. Significant declines in mean blood pressure (av- erage 12.4 f 1.4 percent) and systemic vascular resistance (28.7 f 3.2 percent) accompanied an increase in cardiac &put (24.8 f 4.1 percent). Forearm vascular resistance (18.0 f 2.7 percent) decreased considerably, but the decrease in limb vascular resis- tance did not parallel the fail in systemic vascular resfstance in magnitude (p <O.Ol), indicating that arterioiar dUatatt@ occurred on a selective basis. Plasma renin activity increased after therapy as plasma aidosterone levels consistently fell, white plasma nor- epinephrine concentrations were not changed. There was a dtrect correlation between pretreatment plasma renin activity and the magnitude of the decline in systemic vascular resistance (p <0.05).
These findings suggest that the inhibition of angbteW+converting enzyme with captoprii in diuretic-resistant hypertensfve patients improves cardiocircutatory functbn through seiective dtt#aWn. The reordering of regional blood flow, which appears to result from re- lease of angiotensin-mediated vasoconstrictfon as welt as the suppression of aktosterone, may underlie the prolonged benefit observed in these patients. This oral vasodiiator in very low dose appears to represent an effective adjunct for the treatment of hy- pertension refractory to diuretics.
Therapy for hypertension is often initiated with a diuretic, which in- duces natriuresis, depletion of extracellular fluid, and reduction of cardiac output [ l-31. A resultant fall in blood pressure is attended by activation of the renin-angiotensin system and the sympathetic nervous system which, in turn, through its pressor properties, may prevent a fall in blood pressure [3,4].
From the Department of Internal Medicine, Insti- tute of Clinical Medicine, University of Tsukaba, Ibaraki, Japan. Requests for reprints should be addressed to Dr. Toshiro Fuji& Department of Internal Medicine, University of Tsukaba, Sa- kura-mura, Ibaraki-ken 305, Japan. Manuscript accepted January 26. 1982.
Captopril, an oral angiotensin-converting enzyme inhibitor, which eliminates circulating angiotensin II, a potent vasopres$or peptide, lowers blood pressure in hypertensive patients [5-71. Since several investigators have demonstrated that the hypotensive effects of captopril were more pronounced in the presence of augmentation of the renin-angiotensin system induced by sodium depletion, captopril is able to potentiate the hypotensive effect of a thiazide diuretic [8-lo].
September 1982 The American Journal of Medklne Volume 73 341

CAPTOPRIL IN DIURETIC-RESISTANT HYPERTENSION-FUJITA ET AL.
TABLE I Clinical Characteristics of Patients Studied (mean f S.E.M.)
Patient Sex/Age Blood Pressure in Outpatient Clinic (mm Hg)
Before l’hiazide After Thiaride
Electrocardiographic Lefl Ventricular
Hypertrophy
Crealinine
Clearance (milmin)
1 F, 36 160/100 140190 2 M,51 162/115 125194 3 F, 45 1751106 152194 4 M,57 190/126 165/119 5 M,55 150/110 1441106 6 M,47 165197 140192 7 M,52 1701116 1661114 a M,50 182iioa 160192 9 M,34 1641106 1461108 10 M,56 iao/io4 1621102 11 M,51 1701112 162/110
48.5 f 3.3 170/109f 312 153/102f 513
- 98.2 90.4 80.3 75.4 92.2 104.6 74.4 102.4 84.2 86.4 80.2
88.1 f 3.2
In uncontrolled hypertensive patients taking a thiazide diuretic, systemic vascular resistance is frequently el- evated with reduced cardiac output, and thus the elim- ination of circulating angiotensin II with captopril would be expected to reduce systemic vascular resistance, leading to the fall in blood pressure. Since a reduction of systemic vascular resistance with captopril causes an improvement in cardiac output in patients with heart failure and low cardiac output [ 1 l-161, important he- modynamic effects can occur with the use of captopril in hypertensive patients taking a thiazide diuretic with elevated plasma renin activity. We have correlated the hemodynamic changes observed with alterations in plasma renin activity and aldosterone levels as well as with the degree of blood pressure control.
Moreover, inhibition of the converting enzyme can cause redistribution of regional blood flow in favor of the brain, heart, and kidneys in situations in which the renin-angiotensin system is stimulated [ 171. Recently, Faxon et al. [ 18,191 have demonstrated that, in contrast to the actions of generally available vasodilator drugs, essentially no limb vasodilation occurred in either ar- teries or veins following administration of teprotide and captopril to patients with chronic congestive heart failure. Accordingly, in the present study, we have in- vestigated the long-term systemic and peripheral he- modynamic effects as well as the interplay of several hormonal factors during treatment with captopril.
METHODS
Patients. Twenty-five patients with “essential” hyperten- sion were studied. informed consent was obtained from each patient. The diagnosis was based on history, and results of physical examination, appropriate laboratory tests, and in- travenous pyeiography. Renal arteriography and renal vein blood sampling for measurement of plasma renin activity were performed when indicated.
All patients had been untreated. They began a regimen of 4 to 6 mg per day of trichiorthiazide, and were followed up on an outpatient basis for about two months. in 14 of 25 pa- tients, diastolic pressure was decreased below 90 mm Hg after two-month treatment with the diuretic. Conversely, 11 of 25 patients had a diastolic pressure above 90 mm Hg de- spite ceiling doses of the diuretic. “Diuretic-resistant” hy- pertension was diagnosed in these 11 patients, and they were followed up for the next study. Captopril Protocol. Eleven patients were studied in the diuretic-treated state. Systemic and forearm hemodynamic measurements were repeated until three similar determi- nations 15 minutes apart demonstrated homeostasis. Patients were followed up on an outpatient basis at weekly intervals, and the initial dosage of captopril (5 mg, three times daily) was increased at each visit until control of blood pressure was obtained (up to a dosage of 45 mg/day). On the fourth week of captopril treatment, the patients took their morning dose of captoprii (5 to 15 mg) in the laboratory, and the hemody- namic data were obtained about 60 to 75 minutes later. Systemic Hemodynamics. Systemic blood pressure was measured by sphygmomanometer. Cardiac output was de- termined by dye-dilution (indocyanine green). Total systemic vascular resistance was calculated as the ratio of mean blood pressure to cardiac output, expressed in dynes/sec/cmT5. Peripheral Hemodynamks. Forearm piethysmography was carried out using the mercury-filled rubber strain gauge placed around the midforearm. Patients were studied in the supine position with the forearm elevated so that venous pressure in the arm approached zero; the hand was isolated from the forearm by inflation of a wrist cuff to suprasystolic pressures. Forearm venous occlusion was rapidly achieved by inflation of a sphygmomanometer cuff wrapped around the upper arm and attached to a container of compressed air with a special pressure gauge preset at 40 mm Hg. Forearm blood flow was calculated from the change in forearm circumference during acute venous occlusion and was expressed as ml/100 ml tissue/min. Forearm vascular resistance was calculated as the ratio of mean blood pressure to forearm blood flow ex- pressed in units of mm Hg/mi/lOO ml tissueimin. Ail values for forearm blood flow and forearm vascular resistance were
342 September 1982 The American Journal of Medicine Volume 73

CAPTOPRIL IN DIURETIC-RESISTANT HYPERTENSION-FUJITA ET AL.
TABLE ii Responses of Plasma Renin Activity, Aidesterone, and Norepinephrfne Concentrations to Captoprii (mean f S.E.M.)
Patient
Plasma Renin Activity
(nglmllhr) Before After
Aldosterone Norepinqhrine (Wd)) Wm))
Before Afler Before After
1 1.69 3.70 10.5 8.1 102 82 2 4.36 8.08 5.4 4.4 279 184 3 1.74 2.72 9.1 5.6 185 94 4 5.18 9.41 6.6 6.0 89 98 5 4.62 8.23 5.8 4.9 309 462 6 2.26 3.54 12.3 11.2 278 121 7 4.50 7.06 15.2 10.6 290 246 8 4.41 12.50 8.0 7.2 120 127 9 4.85 9.41 12.4 9.6 85 125
10 3.60 4.68 13.7 11.0 341 124 11 3.45 8.53 8.8 6.8 242 198
Mean f S.E.M. 3.70 f 0.38 7.08 f 0.92 9.8 f 1.0 7.8 f 0.8 211f29 169f33
P <O.OOl <O.OOl NS
obtained by averaging at least six individual determinations
that were within 5 percent of each other.
Hormonal Factors. Before and after captoprii treatment,
blood for hormonal determinations was drawn with the patient
in the supine position, and the plasma was frozen at -7OOC.
Plasma renin activity was determined by radioimmunoassay
of angiotensin I generated during incubation of plasma at pH 6.5 and 37’C (normal range 0.4 to 2.2 ng/mi/hour). Plasma aidosterone concentration was quantitated by the radioim- munoassay technique, using a commercial kit (CEA-IRE- SOFUN). Plasma norepinephrine was measured by the method of Schwedt [20], using high-pressure liquid chromatography combined with automatic fiuorimetric detector.
The statistical methods used were regression analysis and two-tailed Student t test for paired data. Ail data are ex- pressed as mean values f standard error of the mean.
RESULTS
The clinical characteristics of the patients studied are presented in Table I. After treatment with a diuretic, declines in both systolic (10 percent) and diastolic (6 percent) pressures were statistically significant (both p <O.OOl), but ail 11 patients had diastolic pressures above 90 mm Hg.
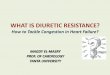
Details of changes in plasma renin activity and nor- epinephrine and aldosterone concentrations are pre- sented in Table IL Baseline plasma renin activity ex- ceeded 4 ng/ml/hour in six patients, and increased in ail patients after captoprii administration. This rise is consistent with the known negative feedback action of angiotensin ii on renal renin release. A direct correlation was identified between pretreatment plasma renin activity and the magnitude of the decline in systemic vascular resistance (r = 0.648, p <0.05) (Figure 1). Plasma norepinephrine concentrations did not change significantly after captopril treatment from the mean treatment value of 211 f 29 pg/ml. Control norepi-
nephrine concentration did not correlate with alterations in systemic vascular resistance. Plasma aidosterone concentration decreased in ail patients (p <O.OOl) and did not correlate with plasma renin activity.
The administration of iowdose captoprii was not associated with side effects such as proteinuria, neu- tropenia, or skin rash. Systemic Hemodynamic Response. Hemodynamic benefit was demonstrated in ail patients during captoprii treatment, as shown in Flgure 2. Mean blood pressure decreased significantly (p <O.OOl) from the average pretreatment value of 119 f 3 mm Hg to 104 f 3 mm Hg after treatment. Declines in both systolic (14 percent) and diastolic (12 percent) pressures were statistically significant (both p KO.001).
/ Pretreatment PRA (ng/ml/hr)
2 lu ai b d ae I y=-5.52x-8.29 .
-50’
Figure 1. Relationship between the pretreatment plasma renin activity (PRA) and percent decrease in systemic vas- cular resistance (SW) after captopril in 11 patients with hypertension refractory to a diuretic.
September 1982 The American Journal of Medicine Volume 73 343

CAPTOPRIL IN DIURETIC-RESISTANT HYPERTENSION-FLlJITA ET AL.
60-
50-
:: s .” .
.
TH - TH+CP
HR
P<O.OOl
TH - TH+CP
MBP
3OOOr \pco’ool 4.5 r
P<O.OOl
500 L TH - TH+CP 2.0 L TH - TH+CP
SVR
Ffgure 2. Changes in cardi~irculatory dynamics producs by low-dose captopril (CP) (mean daily dose 30 mg) in 17 hypertensive patients treated with a thiaride on heart rate (HR), mean blood pressure (MBP), systemic vascular resis- tance (SW?), and cardiac index (Cl). 7li = during the treatment with a thiazide. TH i- CP values were obtained four weeks after oral captopril administration.
Systemic vascular resistance fell substantially, from the elevated resting level of 1,909 f 163 to 1,330 f 86 dynes/set/cm-5 after captopril treatment. Cardiac index improved 25 percent from a mean value of 2.9 f 0.1 to 3.6 f 0.1 liter/min/m* after treatment, while stroke volume index increased 23 percent from 40.5 f 2.1 to 49.7 f 2.7 ml/beat/m*; increments in both indexes were significant (p X0.001). Heart rate did not significantly change. In all patients, the magnitude of the decrease in mean blood pressure resulting from converting enzyme inhibition was related to the con- current changes in systemic vascular resistance (r = 0.759, p <O.Ol). In turn, the changes in systemic vas- cular resistance induced by the inhibitor were related to the concurrent changes in cardiac index (r = 0.957, p <O.Ol). Forearm Hemodynamic Response. Basal forearm blood flow was 1.44 f 0.11 ml/100 ml tissue/min; this
SVR FVR
8 I IPCO.01 _J I
F&ure 3. Comparative percent change in systemic vas- Cuiar resistance @VP) and foreamI vascular resistance (FVR) four weeks after captopril administration.
did not change significantly after captopril treatment (1.5 1 f 0.12 ml/100 ml tissue/min; N.S.) despite im- proved cardiac output. Calculated forearm vascular resistance diminished from an average value of 88.3 f 7.8 to 73.5 f 6.0 units after captopril treatment (p <0.005). Figure 3 compares the changes in systemic and forearm vascular resistances after captopril treatment. The reduction in systemic vascular resis- tance (29 f 3 percent) was significantly greater (p <O.Ol) than that in forearm vascular resistance (16 f 3 percent).
COMMENTS
The purpose of the present study was to evaluate the hemodynamic and endocrine effects of lowdose cap- topril, an oral angiotensin-converting enzyme inhibitor, in uncontrolled hypertensive patients treated with a thiazide diuretic alone. Results indicate that this drug in very low dose may be beneficial for the treatment of diuretic-resistant hypertension. The undesirable he- modynamic changes observed with salt depletion, i.e., increased peripheral vascular resistance and decreased cardiac index, were due to renin stimulation and could be easily reversed by angiotensin blockade. The pa- tients seem to have been responsive to small doses of captopril, in the presence of augmentation of the renin-angiotensin system resulting from diuretic treat- ment. The results of our study also demonstrate that the decrease in blood pressure by captopril is due to a de- crease in systemic vascular resistance. There are significant correlations between the pretreatment plasma renin activity and the changes in blood pressure and systemic vascular resistance induced by the in- hibitor. Similar findings regarding relationships between blood pressure and renin have been reported in previous
344 September 1982 The American Journal of Yedtclne Volume 73

CAPTOPRIL IN DIURETIC-RESISTANT HYPERTENSION-FUJITA ET AL.
studies with teprotide and captopril in hypertension [6,7], for systemic vascular resistance in heart failure [11,12,21], and in normal man [22].
From the hemodynamic responses demonstrated in our patients with diuretic-resistant hypertension, cap- topril appears most efficacious in the subset of di- uretic-treated patients whose cardiac dysfunction is hemodynamically characterized by marked elevation of systemic vascular resistance with moderately re- duced cardiac output. Almost all patients in this study showed a substantial decrease in systemic vascular resistance, and there was also a concomitant increase in cardiac output and stroke volume. According to the effect of captopril on cardiac function, short-term ad- ministration for up to several days in patients with hy- pertension usually had no significant effect on heart rate, stroke volume, or cardiac output [23,24]. In pa- tients with high-renin hypertension, however, cardiac output is increased by short-term administration of captopril [25]. During longer-term administration, moreover, cardiac output and stroke volume increased slightly [24,26]. Based on the correlation between the changes in systemic vascular resistance and those in cardiac output in our study and in previous studies of heart failure [ 12,2 11, the increase in stroke volume may be mainly due to the reduction in afterload and hence better ventricular emptying, although an increase in myocardial contractility due to coronary artery vaso- dilation may contribute to this effect. Coronary artery vasodilation, with the increase in coronary blood flow during converting enzyme inhibition, has been docu- mented previously by Gavras et al. [ 171. Furthermore, improvement in cardiac function has been observed in patients with heart failure treated with captopril [lo- 151. Therefore, long-term blockade of the renin system, when routinely available, might prove preferable, since it would be expected to counteract some of the unde- sirable effects of sodium depletion due to diuretics alone, such as decreased cardiac output and increased peripheral resistance.
The rise in plasma renin activity following captopril administration is compatible with the negative feedback control of renal renin release and serves to confirm angiotensin blockade in these patients. In addition, we found a simultaneous reduction in aldosterone levels, as might be expected following angiotensin inhibition. Furthermore, aldosterone has cardiovascular actions of its own [27,28]. These findings taken together sup- port the view that the renin-angiotensin-aldosterone system possibly participates not only in the mainte- nance of blood pressure but also in abnormal cardio- vascular homeostasis in diuretic-resistant hypertensive patients.
Plasma norepinephrine concentrations did not sig-
nificantly change, as in previous experience with cap- topril and teprotide [ 12,13,19]; reflex tachycardia was absent despite a reduction in blood pressure after therapy, suggesting that substantial adrenergic stimu- lation did not occur. The absence of reflex tachycardia could be explained on the basis not only that the an- tagonists of angiotensin II abolish the positive chrono- tropic effect of angiotensin on the heart, which could occur either directly or by interaction with the sympa- thetic nervous system [29], but also that reduced cir- culating angiotensin II decreases catecholamine release
[131. Because converting enzyme participates also in the
degradation of the vasodilator bradykinin to inactivate peptides, it is possible that the cardiovascular effects of captopril are due not only to the elimination or de- crease in the level of circulating (or local tissue) an- giotensin II, but also to cumulation of bradykinin and/or prostaglandin E [30-321. Bradykinin (admittedly in high dosage), however, increases cardiac output because it markedly increases heart rate, while its effects on stroke volume are inconsistent-that is, the hemody- namic pattern of response to bradykinin is the opposite of the one observed in the present and previous studies
]331. Although cardiac output increased 25 percent fol-
lowing captopril therapy, no increase in forearm blood flow was detected in this study. These findings are consistent with the experience of Faxon et al. [ 191 with captopril, in patients with severe congestive heart failure. These data indicate that converting enzyme inhibitor does not significantly increase regional flow to the limb circuit in patients with congestive heart failure nor in hypertensive patients treated with a di- uretic. Regional redistribution of blood flow has been verified in sodium-depleted dogs given teprotide [ 151 and in spontaneously hypertensive rats given captopril [34], and flow to the renal, cerebral, and myocardial vasculature increased at the expense of cutaneous and skeletal muscular flow. Possible mechanisms for this phenomenon of regional redistribution of flow after converting enzyme inhibition include differences in tissue concentrations of converting enzyme or in local affinity of angiotensin II receptors. Moreover, converting enzyme inhibition may influence the tissue concen- trations of bradykinin and prostaglandins.
Recent experimental evidence suggests that the vasculature of different organs may display various degrees of sensitivity to the action of vasoconstrictive factors [35-371. The renal and coronary vessels were found to exhibit the greatest increase in local resistance after administration of exogenous angiotensin, while the muscular and cutaneous vessels exhibit greater con- striction than the coronary vessels after adrenergic
September 1992 The American Journal of Medicine Volume 73 345

CAPTOPRIL IN DIURETIC-RESISTANT HYPERTENSION-FUJITA ET AL.
stimulation [35]. Since during captopril administration, mg/day) normalizes blood pressure without any side the renin-angiotensin system was suppressed but effects, associated with ventricular afterload reduction substantial adrenergic stimulation did not occur despite and resultant increase in cardiac output, and the reor- a reduction in blood pressure, the converting enzyme dering of regional blood flow, suggesting that it may be inhibitor might be expected to cause more pronounced a useful adjunct to the therapy of severe hypertensive vasodilation resulting from elimination of angiotensin patients treated with a diuretic. Therefore, captopril and II, possibly because of the relative contribution of the a diuretic probably should be used in combinations at adrenergic factors just mentioned to the observed low dosage to minimize not only humoral and hemo-
changes. dynamic compensatory mechanisms but also percep- In summary, captopril in very low dose (average 30 tible side effects.
REFERENCES
1.
2.
3.
4.
8.
9.
10.
11.
12.
13.
14.
15.
16.
Fujita T, Henry WL. Barber FC, et al.: Factors influencing blood pressure in salt-sensitive patients with hypertension. Am J Med 1980; 69: 334-344.
Carey RM, Douglas JG, Schweikert JR, et al.: The syndrome of essential hypertension and suppressed plasma renin activity; normalization of blood pressure with spironolac- tone. Arch Intern Med 1972; 130: 849-854.
Vaughan ED, Carey RM, Peach MJ, et al.: The renin response to diuretic therapy. A limitation of antihypertensive potential. Circ Res 1978; 42: 376-381.
Gavras H, Waeber B, Kershaw GR, et al.: Role of reactive hyperreninemia in blood pressure changes induced by sodium depletion in patients with refractory hypertension. Hypertension 1981; 3: 441-447.
Brunner HR, Gavras H, Waeber B, et al.: Oral angiotensin- converting enzyme inhibitor in long-term treatment of hy- pertensive patients. Ann Intern Med 1979; 90: 19-23.
Gavras H, Brunner HR, Turini GA, et al.: Antihypertensive effect of the oral angiotensin converting enzyme inhibitor Xl 14225 in man. N Engl J Med 1978; 298: 991-995.
Fujita T, Yamashita N, Yamashita K: Effects of angiotensin- converting enzyme inhibition on blood pressure and plasma renin activity in essential hypertension. Am Heart J 1981; 101: 259-368.
Atkinson AB, Brown JJ, Leber AF, et al.: Combined treatment of severe intractable hypertension with captopril and di- uretic. Lancet 1980; II: 105-108.
White NJ, Rajagopalan B, Yahaya H, et al.: Captopril and fu- rosemide in severe drug-resistant hypertension. Lancet 1980; II: 108-l 10.
Koffer H, Vlasses PH. Ferguson RK: Captopril in diuretic- treated hypertensive patients. JAMA 1980; 244: 2532- 2535.
Gavras H, Flessas A, Ryan TJ, et al.: Angiotensin II inhibitor: treatment of congestive heart failure in a high renin hy- pertension. JAMA 1977; 238: 880-882.
Gavras H, Faxon DP, Berkoben J, et al.: Angiotensin converting enzyme inhibition in patients with congestive heart failure. Circulation 1978; 58: 770-778.
Curtiss C, Cohn JN, Urobel T, et al.: Role of the renin-angio- tensin system in the systemic vasoconstriction of chronic congestive heart failure. Circulation 1978; 58: 763-769.
Davis R, Ribner HS, Keung E, et al.: Treatment of chronic congestive heart failure with captopril, oral inhibitor of angiotensin converting enzyme. N Engl J Med 1979; 301: 117-121.
Turini GA, Brunner HR, Gribic M, et al.: Improvement in chronic congestive heart failure by oral captopril. Lancet 1979; I: 1213-1215.
Awan NA, Evenson MK, Needham KE, et al.: Efficacy of oral angiotensin-converting enzyme inhibition with captopril
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
therapy in severe chronic normotensive congestive heart failure. Am Heart J 1981; 101: 22-31.
Gavras H, Liang C-S, Brunner HR: Redistribution of regional blood flow after inhibition of the angiotensin converting enzyme. Circ Res 1978; 43 (Suppl I): l-59-l-63.
Faxon DP, Creager MA. Halperin JL, et al.: Central and pe- ripheral hemodynamic effects of angiotensin inhibition in patients with refractory congestive heart failure. Circulation 1980; 61: 925-930.
Faxon DP. Halperin JL, Creager MA, et al.: Angiotensin inhi- bition in severe heart failure: acute central and limb he- mcdynamic effects of captopril with observations on sus- tained oral therapy. Am Heart J 1981; 101: 548-556.
Schwedt G: Separation and fluorimetric determination of adrenaline and noradrenaline. Combination of a high- pressure liquid chromatography with an automatic analysis system. J Chromatogr 1977; 143: 463-471.
Curtis C. Cohn JN, Vrobel I, et al.: Role of the renin-angiotensin system in the systemic vasoconstriction of chronic con- gestive heart failure. Circulation 1978; 58: 763-770.
Niarchos AP, Pickering TG, Case DB, et al.: Role of the renin-angiotensin system in blood pressure regulation: the cardiovascular effects of converting enzyme inhibition in normotensive subjects. Circ Res 1979; 45: 829-837.
Turini GA, Brunner HR. Waeber B, et al.: Long term cardiac responses of hypertensive patients treated by an inhibitor of angiotensin converting enzyme. Clin Res 1979; 27: 319A.
Fagard R, Amery A, Lijnen P, et al.: Haemodynamic effects of captopril in hypertensive patients: comparison with sa- ralasin. Clin Sci 1979; 57: 131A-134s.
Niarchos AP, Pickering TG, Wallace JM, et al.: Hemodynamic effects of the converting enzyme inhibitory teprotide in normal- and high-renin hypertension. Clin Pharmacol Ther 1980; 28: 592-610.
Fagard R, Amery A, Reybrouck T. et al.: Acute and chronic systemic and pulmonary hemodynamic effects of angio- tensin converting enzyme inhibition with captopril in hy- pertensive patients. Am J Cardiol 1980; 46: 295300.
Ballard K. Lefer A, Sayers G: Effect of aldosterone and plasma extracts on a heart-lung preparation. Am J Physiol 1960; 199: 221-225.
Tanz RD: Studies on the inotropic action of aldosterone on isolated cardiac tissue preparations: including the effects of pH, ouabain and SC 8109. J Pharmacol Exp Ther 1962; 135: 71-78.
Kairallah PA, Davila D, Papanicolaou N, et al.: Effects of an- giotensin infusion on catecholamine uptake and reactivity in blood vessels. Circ Res 1971; 28-29 (suppl II): 11-96.
Williams GH, Hollenberg NK: Accentuated vascular and en- docrine response to SQ 20881 in hypertension. N Engl J
346 September 1962 The American Journal of Medicine Volume 73

CAPTOPRIL IN DIURETIC-RESISTANT HYPERTENSION-FUJITA ET AL.
Med 1977; 297: 184-188. 31. Swantz SL, Williams GH, Hollenberg NK, et al.: Converting
enzyme inhibition in essential hypertension. The hypo- tensive response does not reflect only redoced angiotensin II formation. Hypertension 1979; 1: 106-l 11.
32. Fujita T, Yamashita N, Yamashita K: Effect of indomethacin on antihypertensive action of captopril in hypertensive patients. Clin Exp Hypertens 1981; 3: 939-952.
33. DeFreita FM, Faraco EZ, DeAzevedo DF: General circulatory alterations induced by intravenous infusion of synthetic bradykinin in man. Circulation 1964; 29: 66-70.
34. Koike H, Ito K, Miyamoto M, Nishino N: Effects of long-term
blockade of angiotensin converting enzyme with captopril (SQ 14225) on hemodynamics and circulating blood volume in SHR. Hypertension 1980; 2: 299-303.
35. Mark AL, Abboud FM, Schmid PG, et al.: Differences in direct effects of adrenergic stimuli on coronary, cutaneous and muscular vessels. J Clin Invest 1972; 51: 279-281.
36. Freeman RH. Davis JD, Vitale SJ, et al.: lntrarenal role of angiotensin II: homeostatic regulation of renal blood flow in the dog. Circ Res 1973; 32: 692-698.
37. Barbour JA, Bailie MD: Effect of the synthetic peptide SQ 20881 on distribution of blood flow in the rat. Proc Sot Exp Biol Med 1973; 143: 400-403.
September 1982 The American Journal of Medlclna Volume 73 347