Embed Size (px)
Citation preview

HEMIHYPERTROPHY AS POSSIBLE SIGN OF RENAL CELL CARCINOMA
LAWRENCE PARKER, M.D. JOZEF KOLLIN, M.D. DANIEL VICARIO, M.D. THANH NGUYEN, M.D.
From the Medical Service and Laboratory Service, University of California, Irvine, and Veterans Affairs Medical Center, Long Beach, California
ABSTRACT-In infants and children there is a well-recognized association of hemihypertrophy with visceral malignancies, including those of the kidney as well as benign renal disorders, As a result of OUT report on an adult with segmental hemihypertrophy and renal cell carcinoma, we suggest that if this combination represents an association similar to that found in children, a ra- diographic-urologic evaluation is needed to diagnose renal neoplasms at an early stage, and to disclose the presence of treatable benign renal disease.
We report on an adult patient with prominent segmental hemihypertrophy of the right leg who had undergone a right nephrectomy for re- nal cell carcinoma three years earlier. He was admitted to the VA Medical Center for evalua- tion of tumor recurrence. The association be- tween hemihypertrophy and visceral malignan- cies, including those of the kidney, is sufficiently well established in pediatric prac- tice to require radiologic investigation of asymptomatic children.1,2 We present this case report to suggest that radiologic investigation may be desirable as part of routine evaluation of this physical finding in adults in order to dis- cover neoplasms at the earliest possible stage.
Case Report The patient is a fifty-three-year-old man
with lifelong hypertrophy of the right leg, who was admitted to the medical center for evalua- tion of left flank pain and a recent report of mi- croscopic hematuria. He had been hospitalized three years previously for transient renal failure, which was probably due to indometha- tin therapy given for gout. During the course of
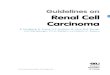
a renal ultrasound examination to rule out hy- dronephrosis, a renal mass was noted, and sub- sequently confirmed as a solid mass by ab- dominal computerized tomography (CT) scan. At nephrectomy, a renal cell carcinoma of the clear cell type was removed (Fig. 1). No metas- tases were noted. On discharge, laboratory values of 40 mg/dL and 2.3 mg/dL were ob- tained for blood urea nitrogen (BUN) and serum creatinine, respectively.
The patient was admitted once for congestive heart failure, and subsequently followed up as an outpatient for several medical problems, in- cluding obstructive lung disease, gout, and hy- pertension. He was managed with medications including allopurinol, nifedipine, minoxidil, and clonidine. He reported no bone pain and no neurologic dysfunction except some weakness in the right leg.
On admission, the patient was alert and cooperative and in no apparent distress, with a temperature of 98.8 “F and a blood pressure of 140/90 mm Hg. Pertinent physical findings in- cluded arteriovenous nicking on fundoscopic examination, no abdominal tenderness or
266 UROLOGY I SEPTEMBER 1992 I VOLUME 40, NUMBER 3

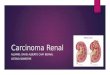
masses, no hemangiomas, and marked hy- pertrophy of right calf musculature (Fig. 2). Evaluation by a neurologic consultant disclosed a sensorimotor deficit in the right lower part of leg and foot, with sparing of deep tendon re- flexes.
Laboratory data included the following: BUN 27 mg/dL, creatinine 1.4 mg/dL, uric acid 8.8 mg/dL, protein (4 + ) and no red blood cells on urinalysis, and a 24-hour protein of 2.5 g. Creatinine clearance was calculated to be 53 ml/minute. Radiographs of the tibia and fib- ula showed soft tissue hypertrophy on the right (Fig. 2).
An ultrasound examination of the left kidney indicated a possible mass, but this was not veri- fied on a CT scan or magnetic resonance imag- ing (MRI). Chest radiographs showed no masses. Electromyographic and nerve conduc- tion studies demonstrated a moderate-to-severe right tibial nerve lesion distal to the knee. The flank pain resolved, and the patient was dis- charged, to be followed up as an outpatient.
Comment While some asymmetry is common in so-
matic development, extreme degrees have been classified as hemihypertrophy. Hemihy- pertrophy has been designated as total when
FIGURE 1. Histologic view of tumor removed from patient. Normal renal parenchyma shown in right lower area, while well-dif- ferentiated renal cell carcinoma of clear cell type shown in remain- der (hematorylin and eosin, original magniji- cations x 40 and inset x 200).
FIGURE 2. Frontal (A) and radiologic (B) views of patient’s legs, demon- strating segmental mu- cular hemihypertrophy on right side.
UROLOGY / SEPTEMBER1992 / VOLUME40,NUMBER3 287

neurologic, muscular, skeletal, and vascular systems are simultaneously involved, and as limited when there is less complete involve- ment. Also, if there is only regional involve- ment, this has been designated as segmental, as in the aforementioned case. The range of hemi- hypertrophy extends from single digital enlargement to that of an entire half of the body. 3 If internal organ abnormalities are noted contralateral to the somatic hemihypertrophy, this has been termed crossed hemihypertrophy.4 Although the distinction between hemihy- pertrophy and herniatrophy might seem arbi- trary in severe cases, it has been reported that there is bone age advancement on the involved side, and an autopsy study demonstrated an in- creased cell number in various tissues and or- gans on the involved side.5pe Another form of hemihypertrophy (ruled out in the present case) is the Klippel-Trenaunay- Weber syndrome, in which prominent hemangiomas are also present.’
The association of hemihypertrophy with tu- mors of infancy and childhood, such as Wilms tumor, hepatoblastoma, and adrenocortical carcinoma has been well documented.8-11 Al- though less common, some cases of adults with hemihypertrophy and visceral tumors, such as Wilms tumor, have also been reported.2,12 In addition, a number of childhood and some adult cases have been reported in which other renal abnormalities or developmental variants have been discovered in association with hemi- hypertrophy, such as benign nephromegaly, medullary sponge kidney, renal ectopia, and re- nal cyst. 13-18
We are unaware, however, of any reported cases of renal cell carcinoma reported in adults with hemihypertrophy. We therefore suggest that if cases similar to the present one begin to be recognized, that radiographic urologic eval- uation of asymptomatic adults with hemihy- pertrophy may eventually prove to be useful from the points of view of morbidity, mortality, and cost effectiveness. Aside from the possibility of tumor discovery at an early stage, a cause may be found for nonmalignant renal prob- lems, such as renal stones or recurrent urinary tract infection.
University of California at Irvine Long Beach Medical Program
Department of Veterans Affairs Medical Center 5901 East 7th Street
Long Beach, California 90822 (DR. PARKER)
1. Haicken BN, Schulman NH, and Schneider KM: Adreno- cortical carcinoma and congenital hemihypertrophy, J Pediatr 83: 284 (1973).
2. Hennessy WT, Cromie WJ, and Duckett JW: Congenital hemihypertrophy and associated abdominal lesions, Urology 18: 576 (1981).
3. Gorlin RJ, and Meskin LH: Congenital hemihypertrophy: review of the literature and report of a case with special emphasis on oral manifestations, J Pediatr 61: 870 (1962).
4. Parra G, Seery W, Buchbinder M, and Cole AT: Congenital total hemihypertrophy and carcinoma of undescended testicle: a case report, J Urol 118: 343 (1977).
5. Geiser CF, Baez A, Schindler AM, and Shih VE: Epithelial hepatoblastoma associated with congenital hemihypertrophy and cystathioninuria: presentation of a case, Pediatrics 46: 66 (1970).
6. Wiedemann HR, et al: The proteus syndrome: partial gi- gantism of the hands and/or feet, nevi, hemihypertrophy, subcu- taneous tumors, macrocephaly or other skull anomalies and possi- ble accelerated growth and visceral affections, Eur J Pediatr 140: 5 (1983).
7. Brooksaler F: The angio-osteohypertrophy syndrome, Am J Dis Child 112: 161 (1966).
8. Miller RW, Fraumeni JF, and Manning MD: Association of Wilms tumor with aniridia, hemihypertrophy and other congeni- tal malformations, N Engl J Med 270: 922 (1964).
9. Fraumeni JF, Geiser CF, and Manning MD: Wilms tumor and congenital hemihypertrophy report of f&e new cases and re- view of literature. Pediatrics 46: 886 (1967).
10. Meadows AT, Lightenfeld JL, and Koop CE: Wilms tumor in three children of a woman with congenital hemihypertrophy, N Engl J Med 291: 23 (1974).
11. Pendergrass TW: Congenital anomalies in children with Wilms tumor: a new survey, Cancer 37: 403 (1976).
12. Ringrose RE, Jabbour JT, and Keele DK: Hemihy- pertrophy, Pediatrics 36: 434 (1965).
13. Parker DA, and Skalko RG: Congenital asymmetry: report of 10 cases with associated developmental abnormalities, Pediat- rics 44: 584 (1969).
14. Roggensack G, and McAlister WH: Bilateral nephro- megaly in a child with hemihypertrophy, Am J Roentgen01 Ra- dium Ther Nucl Med 110: 546 (1970).
15. Harrison AR, and Williams JP: MeduIlary sponge kidney and congenital hemihypertrophy, Br J Urol43: 553 (1971).
16. Saypol DC, and Laudone VP: Congenital hemihy- pertrophy with adrenal carcinoma and medullary sponge kidney, Urology 21: 510 (1983).
17. Kirks DR, and Shackelford GD: Idiopathic congenital hemihypertrophy with associated ipsilateral benign nephromeg- sly, Radiology 115: 145 (1975).
18. Pfister RC, et al: Congenital asymmetry (hemihy- pertrophy) and abdominal disease, Radiology 116: 685 (1975).
288 UROLOGY I SEPTEMBER 1992 I VOLUME 40, NUMBER 3