Embed Size (px)
Citation preview

Heinz Reichmann, FRCP, FAANNeurologische Universitätsklinik
Dresden
Idiopathisches Parkinson-SyndromWas gibt es Neues?Dresden, 05.05.2011

Figure 2. Change in 18 F-Fluorodopa Uptake in the Brains of Patients with Parkinson ’s Disease after Transplantation,as shown in Fluorodopa PET Scans.
Freed et al (2001)


Figure 2 -synuclein–positive Lewy bodies in host substantia nigra and grafted dopaminergic neurons.Li J-Y et al. (2008)


Methods and Results
Administration of rotenone intragastrically to one-year-old mice using a gastric tube
Rotenone could not be measured by HPLC using blood and brain tissue
There was no decrease in complex I activity in muscle and brain
Rotarod test was used to show that there was a significant decrease in the rodents‘ ability to remain on the rod between 3 months treated mice and controls
A-synuclein aggregation was only detected in treated animals
A-synuclein aggregation was detected in the ENS and after longer periods in the intermediolateral nucleus in the spinal cord and the dorsal motor nucleus of the vagus
After three months of treatment a-synuclein could be detected in the SN pars compacta combined with a 15% decrease in the number of TH-pos neurons
OB and ENS are the only nervous system structures directly exposed to environmental substances


Figure 2: Change in unified Parkinson’s disease rating scale part 3 score in the off state(A) Mean change from baseline for all patients with at least one assessment after surgery. (B) Mean change from baseline in the subgroup of patients who had masked visits after month 12 (n=30), with last observation carried forward for those who had completed assessments only to month 15 (n=16). Solid lines represent patients who were followed up for longer than 12 months. Dotted lines represent patients who were followed for only 12 months. Bars=SE.
Marks WJ et al. (2010)

Zeit
Neu
rone
nfun
ktio
n
Symptomatisch
Diagnose
Natürlicher Verlauf des IPSohne Behandlung
Klin
isch
e R
atin
gs
?Hyposmie REM Schalf-Verhaltensstörung
DepressionObstipation

Welcher Patient sollte behandelt werden?
Uhrmacher
Maurer

Monotherapy withany anti-PD drug
Grosset. et al JNNP 2007; 78 (5): 465
Treatment-naïvepatients
Det
erio
ratio
n
Baseline 9 180
Follow-up period (months)
10
20
30
40
50
60
PDQ
-39
sing
le in
dex
PD-LIFE: multi-centre prospective audit-based study, on-going, N=198
Behandeln oder nicht behandeln ?


Hauser R
A et al. (2009)

Hauser R
A et al. (2009)
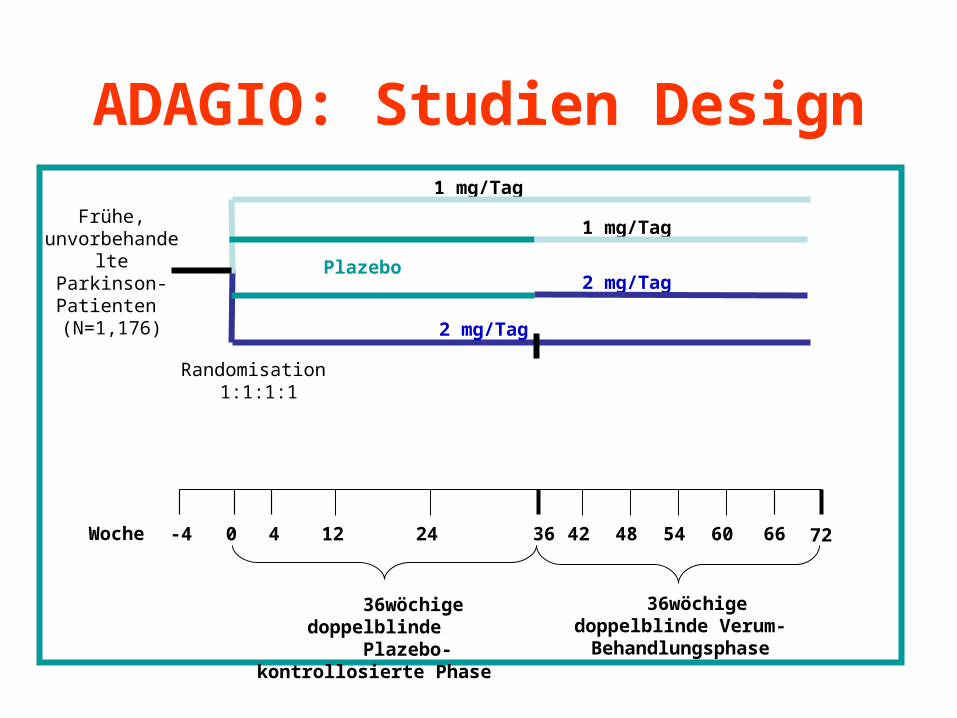
ADAGIO: Studien Design
36wöchige doppelblinde Verum-Behandlungsphase
0 24 54 60 66
72-4 4 36 48
Plazebo
1 mg/Tag
Woche
2 mg/Tag
1 mg/Tag
36wöchige doppelblinde Plazebo-kontrollosierte
Phase
12-4 42
Frühe, unvorbehandelte
Parkinson-Patienten (N=1,176)
Randomisation 1:1:1:1
2 mg/Tag

Figure 3. Changes in Scores on the Unified Parkinson’s Disease Rating Scale (UPDRS) in the Four Study Groups.The mean (±SE) change from baseline in the UPDRS score in the efficacy cohort for the second and third primary end points for patients receiving rasagiline at a dose of 1 mg per day (Panel A) and those receiving 2 mg per day (Panel B) are shown. The dashed lines indicate placebo, and the solid lines indicate rasagiline.


‘Floor’-Effekt in der UPDRS-SkalaV
ersc
hlec
hter
ung
Ver
bess
erun
g
Nur symptomatisch(Potenzielle Verbesserung
von X UPDRS-Einheiten)
Symptomatisch + KM(Potenzielle Verbesserung
von X+Y UPDRS-Einheiten)
Zeit
Höhere UPDRS vor BehandlungsbeginnKM Wirkung ist nachweisbar
X
Y
Arzneimittel
Niedrigere UPDRS vor BehandlungsbeginnKM Wirkung ist nicht nachweisbar
Zeit
Nur symptomatisch (Potenzielle Verbesserung
von X UPDRS-Einheiten)
Nur symptomatisch + KM(Potenzielle Verbesserung
von X+Y UPDRS-Einheiten)
Floor-Effekt
X
Y
Arzneimittel
KM=krankheitsmodifizierend


Sch
apira
AH
V e
t al.,
(201
0) M
ovem
ent D
isor
ders
, Vol
. 25,
No.
11

Figure 2. 15-Month Time Course of UPDRS Total ScoreThe ratings, by blinded study investigators, are graphed, with 95%-Cls, as mean change adjusted for baseline and country. Negative values signify improvement from baseline.
Sch
apira
et a
l. (2
009)
Delayed start
Pramipexol
Plazebo
PROUD-Studie


Grosset et al. (2009)

Ropinirol als “controlled release”-Tablette (ReQuip-Modutab®)


Monotherapie-Studie: Verbesserung des UPDRS Motor Scores nach Titrationsphase
-8,9-10,4
-12
-10
-8
-6
-4
-2
0
n.s.
ReQuip-MODUTABReQuip
Abnahme UPDRS Motor Score

Add-on-Studie: Signifikanter Therapieeffekt vs. Placebo ab Woche 2
1 2 3 4 6 8 10 12 16 20 24Woche
PlaceboReQuip-MODUTAB
Mitt
lere
Änd
erun
g vs
. Bas
elin
e (+
/- 2
S.E.
)
-0.5
-1.0
-1.5-2.0
-2.5-3.0-3.5
24(LOCF)
0.0
0.51.0
Mittlere Änderung von Baseline zu Woche 24 in den “Off”-Zeiten im Wachzustand (ITT)
** * * * * * * * * *
* = signifikant

-4
-3
-2
-1
0
1
2
ReQuip-MODUTAB
Adjustierte mittlere
Veränderung gegenüber
Baseline(Parkinson
Disease Sleep Scale)
Placebo
+1,33
–3,33
PDSS Score zu Baseline: ReQuip-MODUTAB 99,2 ; Placebo 98,0 in Validierungsstudie: Differenz zwischen Parkinsonpatienten und gesunden Gleichaltrigen ca. 20 Punkte
Verbesserung
Pahwa et al. Neurology 2007, Chaudhuri et al. JNNP 2002
Schlaf unter ReQuip-MODUTAB verbessert
Differenz: 4,66 Punktep=0,0196

3016
Trenkwalder C. et al. Parkinsonism & Related Disorders 2009; 15:S136UCB data on file
RECOVER-Studie - Wirksamkeit
Morgendliche Bewegungsstörungen (UPDRS III) und Schlafqualität (PDSS-2)
-8-7-6-5-4-3-2-10
Verbesserung
Änd
erun
gen
im U
PD
RS
III
bzw
. PD
SS
-2 (F
AS
/LO
CF)
UPDRS III PDSS-2
7,0
1,9
3,9
5,9
(± 7,3)
(± 7,6)
(± 8,2)
(± 7,6)
-3,55 (LS-Mean)p=0,0002
-p<0,0001
Rotigotin (n=191)Plazebo (n=96)


Watts RL et al. (2010)

Aufbau der Hydrogel Matrix


Hauser RA (2010)

FIG. 2. UPDRS II 1 III scores over time (without and with L-dopa data censored).Hauser RA (2010)

– rote, linsenförmige, retardiert freisetzende Tabletten
– Nichtergoliner Dopaminagonist
– Wenig Oedeme
– Evtl. bessere kognitive Leistungsfähigkeit
– Wirkstärke 50 mg
Piribedil-Eigenschaften


FIGURE 1: Kaplan-Meier survival curves show that patients randomized to L-dopa/carbidopa/entacapone (LCE) had greater risk of developing dyskinesia than patients receiving L-dopa/carbidopa (LC) (Cox proportional hazard ratio, 1.29; 95% confidence interval [CI], 1.0 – 1.65; p = 0.038). Survival time estimates for the first quartile of patients were 90.7 weeks (95% CI, 65.3 –104.0) for the LCE group and 117.1 weeks (95% CI, 92.1 – 132.6) for LC-treated patients.
Stocchi F et al. (2010)

Häufigkeit neuropsychiatrischer Symptome bei Patienten mit Parkinsonerkrankung (N=1.331)
alle drei Symptome
6,09 %keine
neuropsych.Symptome
36,44 %
Demenz14,94%
Depression17,81%
Depression u.Psychose
2,63 %
Demenz u.Depression
10,82 %
Demenz u.Psychose
9,02 %
Psychose2,25%
Riedel et al. 2006

Demenz bei Morbus Parkinson
• Patienten mit Morbus Parkinson (Parkinson’s disease / PD) weisen häufig eine Beeinträchtigung der kognitiven Funktionen auf
• Bis zu 40% entwickeln eine Demenz
• Die Symptome der Demenz entwickeln sich nach den motorischen Parkinson-Symptomen
• Dabei kommt es zu einer deutlichen Beeinträchtigung der Aufmerksamkeit und der exekutiven Funktionen sowie zu Gedächtnis- und Verhaltensstörungen
• Die Demenz bei PD zeigt viele klinische und pathologische Gemeinsamkeiten mit der Lewy-Körperchen-Demenz (dementia with Lewy bodies / DLB)
Gelb DJ et al. Arch Neurol 1999;56:33–9Emre M. Lancet Neurol 2003;2:229–37
McKeith I et al Lancet Neurol 2004;3:19-28

Die Diagnose der Demenz bei PD
Diagnostischer Ablauf: Diagnose von Morbus Parkinson (PD) Diagnose der Demenz (nach >1 Jahr motorischer Symptome)
DSM-IV-Kriterien für eine Demenz: Multiple kognitive Defizite
– Gedächtnisstörungen– Aphasie, Apraxie, Agnosie oder Störungen von exekutiven
Funktionen Signifikante Verschlechterung gegenüber dem ursprünglichen
Funktionsniveau
“Kognitive Defizite, die so schwerwiegend und umfassend sind, dass sie die DSM-IV-Kriterien für die Diagnose einer Demenz erfüllen”
Emre M. Lancet Neurol 2003;2:229–37DSM-IV 2000



Kriterien für die klinische DiagnoseDiffuse Lewy-Körperchen Erkrankung
1. Essenzielle Symptome 2. Fakultative Symptome
• progressives, kognitives Defizit das zu einer Beeinträchtigung sozialer oder beruflicher Kompetenzen führt
• eindeutige Beeinträchtigung mnestischer Funktionen in Anfangsstadien oder dominierend im weiteren Verlauf
• Aufmerksamkeitsstörung• Dysfunktion des Frontallappens• visuospatiale Defizite• fluktuierende Intensität der Aufmerksamkeit
und Vigilanz• intermittierende visuelle Halluzinationen• Parkinson-Syndrom mit Rigor, Ruhetremor
und Akinese mit variablen Symptomdominanzen ähnlich wie bei Morbus Parkinson
• häufige Stürze in Anfangs-stadien der Erkrankung
• Synkopen• intermittierende Somnolenzen• abnorme Sensitivität für Neuro-
leptika• systematisierte Verkennungen• nichtvisuelle Halluzinationen

Figure 3. Schematic representation of the progression of pathology in the three main clinical phenotypes of PD from longitudinal epoch data. Dopamine cell loss in the substantia nigra is represented as the solid color over the midbrain region, with darker colors indicating greater cell loss over time. Pink-colored brain stem Lewy bodies and brown-colored cortical Lewy bodies are represented separately. Larger lighter brown cortical plaques are also shown.
Hal
liday
GM
, McC
ann
H (2
009)

ChA
T-A
k ti v
i tät i
m m
edio
f ront
a len
Co r
t ex
(nm
ol/ h
/100
mg)
Tiraboschi P et al. Neurology 2000;54:407–11
0
50
100
150
200
250
300
Kontrollen AD
Cholinerge Defizite bei der mit PD, DLB und AD einhergehenden Demenz
DLBDemenzbei PD

In einem 48-wöchigen Studienprogramm wurde die Wirksamkeit von Rivastigmin bei PDD
bewiesen.
Woche 0-24 Woche 25-48
RandomisiertDoppelblind
Plazebo-kontrolliert3-12mg Rivastigmin
Offene VerlängerungsphaseAlle Patienten auf Rivastigmin
3-12mg Rivastigmin
EXPRESSEXPRESS Extensions-StudieExtensions-Studie
Emre M et al. NEJM 2004; 351: 2509-2518Poewe et al. Movement Disorders 2006; 21: 456-461
Woche 0-24 Woche 25-48
EXPRESSEXPRESS Extensions-StudieExtensions-Studie

Rivastigmin versus PlaceboEffekte auf die kognitive Leistung (ADAS-
cog)
*p = 0,002; **p < 0,001, ITT-RDO Analyse
–2.5
–2.0
–1.5
–1.0
–0.5
0.5
1.00 16 24
Änd
erun
gen
von
base
line,
AD
AS-
cog
Woche:
Rivastigmin (n = 329)Placebo (n = 161)
Verbesserung
Verschlechterung
Baseline
***
0
Emre M et al. NEJM 2004; 351: 2509-2518

Baseline
-2.5
-2-1.5
-1-0.5
00.5
11.5
2
Woche: 0 16 24 48
Rivastigmine, n = 180 177 178 171 Placebo, n = 99 99 96 95
Doppelblind Phase Offene Verlängerung(alle Patienten erhalten Rivastigmin)
Verä
nder
ung
vs. B
asel
ine,
A
DC
S-A
DL
RivastigminPlacebo
Verbesserung
Rivastigmin verbessert die Alltagskompetenz (ADCS-ADL) über 48 Wochen
Poewe et al. Movement Disorders 2006; 21: 456-461


Aarsland et al. (2009)


Menza et al., Neurology 2009;72:886–892


Barone et al. (2009)



Verhaltensstörungen bei M. Parkinson
– Spielsucht (Molina et al. 2000)• Internetspiele • Automatenspiele • TV-Shows • Kasino
– Hypersexualität (Vogel et al. 1983)• Libidosteigerung • Gesteigerte sex.
Aktivität• Sex. Aggressivität
• Punding •Stereotype, irrationale motorische Handlungen
• Hyperphagie (Nirenberg et al. 2005)
• Exzessives Shopping (Maja et al. 2003)
• Andere Internetsurfen Sport

Impulskontrollstörungen beim IPS
Prävalenz•Weintraub et al. 2006
– ICS-Prävalenz 6,6 %
•Voon et al. 2006 – ICS-Prävalenz
• total 6,1% • DA-agonist 13,7%
•Normalkollektiv 0,4-1%


Danke für IhreAufmerksamkeit





























