Embed Size (px)
Citation preview

HEARSAYJournal of the Ohio Speech-Language-Hearing Association Vol. 19 2007
Ohio Speech-Language-Hearing AssociationNancy Bailey, Executive DirectorP.O. Box 309Germantown, Ohio 45327-0309
Standard PresortU.S. Postage
PAIDCincinnati, OhioPermit No. 5645 Introducing New Faculty from Ohio Universities
In This Issue:• Functional Communication
Camp for Nonverbal Children
• Informed Consent in ClinicalResearch with Adults withCognitive
• Mealtime Experiences inPediatric Feeding andSwallowing Disorders:Caregivers’ Perspectives
• Travels of an AuditoryResearcher
• Evidence-Based Practice:Where Do We Go From Here?
• Getting Ready for the Next BigThing in AudiologicCounseling
• The Audiology CounselingGrowth Checklist for StudentSupervision
• The University of CincinnatiBioacoustics Lab and CanineAudiology Clinic
• Crisis Intervention TrainingEffects on Graduate Students’Counseling Perceptions
• Detective work by the SLP:Two Cases of UndiagnosedNeurological Damage
Hearsay Cover 07 1/26/08 11:00 AM Page 1

Ohio University
The University of Akron
University of Cincinnati
University of Toledo
Baldwin-Wallace College
The College of Wooster
For detailed information about these Universities go to: www.ohioshla.org, select professional services and then select Ohio Universities.
The following Universities have supported the development of this journal and offer programs in
Speech-Language Pathology and Audiology:
Bowling Green State University
Case Western Reserve University
Cleveland State University
Kent State University
Miami University
The Ohio State University
In The Next IssueHearsay is under renovation! Beginning with the next issue, we will be
updating the structure of the journal’s featured forums and columns inorder to reflect OSLHA’s designated Practice Areas. Each issue of Hearsaywill include a column for Health Care, Mental Retardation/DevelopmentalDisabilities, Non-Profit Agencies, Private Practice, Schools, Supervision,and University and Student Affairs. We will retain Hearing Is Believing asour Audiology Column. The forums for Research, Technology, and GettingDown to Business will continue to appear.
To enact this revision, the next issue of Hearsay will not have a specifictheme but will be composed around spotlighting each of the columnsand forums. We welcome articles that encompass a wide range of subjectmatter. We invite research and reports on professional techniques orpractices regarding any topics that are relevant to the Practice Areas orthat pertain to technology and the business aspects of speech-languagepathology and audiology.
We invite you to submit articles, to seek out others who might beinterested in writing, or to contact the column and forum editors whoare listed in the front of this journal to discuss your ideas. Please sendsubmissions for the next issue by e-mail to Laura W. Kretschmer, Ed.D.,Managing Editor, at [email protected], phone 513/558-8514.
Monica Gordon Pershey, Ed.D.
Associate [email protected]
Hearsay Cover 07 1/26/08 11:00 AM Page 2

1
Welcome to Hearsay for 2007-08. The theme for this issue is getting toknow the wonderful new or nearly new faculty in the university speechand hearing programs in the great state of Ohio. All the university andcollege programs in Ohio were contacted for contributions and we arepleased to feature articles from Baldwin-Wallace (Colleen Visconti,Christie Needham, Crysten Skebo & Julianne Wolf), Kent StateUniversity (Kate Krival, Erin Redle) the Ohio State University (LauraJustice and Allison Breit), Ohio University (F.C. Jeng), University ofAkron (Kris English), University of Cincinnati (John G. Clark and PeterScheifele). Miami University is represented in the Research Forum byBarbara Weinrich. We look forward to publishing articles from new facultyin the remaining programs in the new (Public) University System ofOhio. (So designated by the new Chancellor, Eric Fingerhut. For informa-tion on the USO, go to the web site: http://universitysystem.ohio.gov/)
In the interests of full disclosure, I should mention that the new KentState University faculty are both recent doctoral graduates from theUniversity of Cincinnati, as is Allison Breit. It would have been verydifficult for them to turn me down, but I think you will find that theirarticles clearly stand on their own. OK, complete disclosure then; fourof these articles are on audiology or hearing science topics and yes, Iam an audiologist.
There is an additional article that was submitted in response to ourrequest for neurogenic articles about a year ago. The author, JamesCoyle, is completing his doctorate at the University of Pittsburgh.
If you peruse the Staff page, you will notice some differences thatMonica Gordon Pershey, Associate Editor, explains. See In the NextIssue column. We are changing to columns that will feature OSLHAPractice areas. You will note that some of these new forums have editors listed and some do not. If the editorship of a practice area thatyou are involved in is open, please consider volunteering to help out.Having your name listed as an editor does not mean that you have towrite the column but we will encourage you can be on the lookout formanuscripts from your practice area that you know your colleagueswould benefit from reading.
Yvonne Gillette and Tina Veale will continue to edit the Technologyand Getting Down to Business columns. For those persons who havehelped us but chose not to continue as editors, a big OSLHA thankyour for your years of service in writing columns and your support inhelping to producing a state journal of which we can all be proud.
Laura W. Kretschmer, Managing Editor
OSLHA Director of Public Information
In This Issue
2
STAFFManaging EditorLaura KretschmerAssociate Editor Monica Gordon Pershey
Editorial Advisory Board Wayne Secord
Bob Glaser
John ClarkJean Blosser
Director of Public InformationLaura Kretschmer
Research ForumFofi Constantinidou
University & Student Affairs CaucusColleen Visconti
Health Care CaucusDiane Geiger
School CaucusAnn Slone
MR/DD Caucusopen
Non-profits Caucusopen
Private Practice Caucusopen
Getting Down to BusinessTina Veale
Supervision CaucusJanice Wright
Audiology CaucusLaura KellyKathleen Hutchinson
Technology in Communication Yvonne Gillette
Graphic DesignJody Johnson
PrinterBerman Printing Company
HEARSAY is a publication of the Ohio Speech–Language–Hearing Association for thebenefit of its membership and other individuals committed to the highest quality of serv-ice to people with communication challenges.
The purpose of this journal is to expand the level of information, research, and clinical sci-ence in our professions. It is provided as a vehicle for reporting studies relevant to humancommunication and its disorders and to provide information on the activities and affairsof members and directors of the Ohio Speech–Language–Hearing Association. Each issuecontains (1) invited articles on journal themes or other topics important to state andnational issues, (2) peer reviewed research articles, and (3) caucus columns or articles ontopics of interest to audiologists and speech-language pathologists employed in a varietyof settings, as well as pre-service students, whether undergraduate or graduate.
The appearance of advertising in HEARSAY does not constitute a guarantee or endorsementof the quality or value of such products or of the claims made for it by its manufacturer.
©2007 by the Ohio Speech–Language–Hearing Association.
HEARSAY is published one time per year, in the Fall/Winter. Business address isHEARSAY: Journal of the Ohio Speech–Language–Hearing Association, c/o NancyBailey, Executive Director, P.O. Box 309, Germantown, OH 45327. E-mail address:[email protected]. Individuals interested in submitting articles, columns, oradvertising should direct all correspondence in care of the OSLHA ExecutiveDirector. Letters to the editor should be sent to Laura Kretschmer, Department ofCommunication Sciences and Disorders, Mail Location 0394, University of Cincinnati,Cincinnati, OH 45267-0394.
Claims for missing issues can be honored only up to 3 months for domestic issues and 6months for foreign addresses. Subscribers should notify the OSLHA Office Administratorof any change in mailing address. Single copy and back volume information is availableupon request. Current subscription rates are: Individual rates—$15 per year; Institutionaland library rates—$25 per year; Foreign—$25 per year (individual or institutional).
Submissions to any of the HEARSAY forums or columns are encouraged. Material maybe sent to the OSLHA Executive Director c/o the specific forum or column editor forconsideration. Individuals interested in submitting material to the Research Forumshould follow the guidelines outlined below. All submissions will be considered forpublication. Articles submitted to Research Forum are carefully reviewed. Membershipin the Ohio Speech–Language–Hearing Association is not a requirement for contributors.No manuscript or other material or content that has been published or is under consideration elsewhere should be submitted. Material should be submitted electronically,saved as a Word document (.doc or .docx). Images should be included separately electronically. All electronically images need to be provided at their actual size at 300dpi and formatted as a jpeg, tiff or eps. A high quality hard copy may be provided to be scanned, either black and white or color but electronic copies are preferred. A blackand white head shot photo of all authors would be appreciated as well.
GENERAL INFORMATION FOR AUTHORS
PURPOSE AND SCOPE

3
IN THIS ISSUE 1
INVITED ARTICLES FROM NEW FACULTYAT OHIO UNIVERSITIES
Baldwin-Wallace 4Functional Communication Camp for Nonverbal ChildrenBy: Colleen F. Visconti, Christie A. Needham,Crysten M. Skebo and Julianne Wolf
Kent State University 13Informed Consent in Clinical Research with Adults with Cognitive By: Kate Krival
Kent State University 16Mealtime Experiences in Pediatric Feeding and Swallowing Disorders: Caregivers’ PerspectivesBy: Erin Redle
Ohio University 21Travels of an Auditory Researcher By: Fuh-Cherng Jeng
Ohio State University 23Evidence-Based Practice: Where Do We Go From Here?By: Laura Justice and Allison Breit
HEARSAYJournal of the Ohio Speech-Language-Hearing Association Vol. 19 2007
Introducing New Faculty from Ohio Universities
CONTENTSUniversity of Akron 25Getting Ready for the Next Big Thing in Audiologic CounselingBy: Kristina English
University of Cincinnati 29The Audiology Counseling Growth Checklist for Student SupervisionBy: John Clark
University of Cincinnati 36The University of Cincinnati Bioacoustics Lab and Canine Audiology ClinicBy: Peter Scheifele
RESEARCH FORUM 38Crisis Intervention Training Effects on Graduate Students’ Counseling PerceptionsBy: Barbara Weinrich, Kimberly Beecroft andMichael Hughes
INVITED ARTICLE 50Detective work by the SLP: Two Cases ofUndiagnosed Neurological DamageBy: James Coyle
IN THE NEXT ISSUE Inside Back Cover

AbstractPurpose: The purpose of the present
study was to determine if enrollmentof children who are functionally non-verbal in an intensive summer campprogram involving interaction withpeers and highly responsive clini-cians would lead to improvement infunctional communication.
Methods: Ten children (ages 3years 5 months to 14 years) with avariety of communication disorders(e.g., speech/language disorder,autism, apraxia, Angelman’s syndrome,and cerebral palsy) were randomlyassigned to one of two groups for anintensive summer functional languagecamp. The children attended thefunctional communication camp fortwo hours, three days a week, for fourconsecutive weeks. Pre- and post-evaluation measures were collected.During the camp the children partici-pated in individual activities alongwith small and large group activitiesprovided by two trained undergradu-ate students and a licensed and certi-fied speech-language pathologist. Inaddition, once a week, picture bookcarryover activities were sent homewith each child.
Results: The results demonstratedsignificant increases in the use of func-tional communication. Specifically, thechildren improved by attempting touse more communication functions,using more sophisticated modes ofcommunication, using more successfulcommunication attempts, and attempt-ing to communicate with both famil-iar and unfamiliar communicationpartners.
Clinical Implications: The resultssuggest that an intensive speech-lan-guage therapy approach that incor-porates peer interaction and highlyresponsive clinicians can lead to sig-nificant improvements in the use offunctional communication by chil-dren who are functionally nonverbal.
IntroductionFor most young children, social
interaction with peers takes placeduring play time. However, for children with deficits in communica-tion, play time can be, and frequentlyis, very difficult. Difficulties in theinitiation of play and entering peergroups have been studied in childrenwith specific language impairmentand autism. Children with languageimpairments have been found todemonstrate difficulties in socialinteraction and have less sophisticat-ed play skills than their typicallydeveloping peers (DeKroon, Kyte,&Johnson, 2002). The more severethe deficit in communication, themore severe the social and playdeficits tend to be.
Children with autism spectrum disorders (ASD) demonstrate signifi-cant deficits in social interaction andcommunication skills. Communicationskills in children with ASD have beenfound to be highly correlated with thedevelopment of social behaviors(Garfin & Lord, 1986). Childrenwith ASD have been found to use awide variety of conventional andunconventional forms of communica-tion (Keen, Sigafoos, & Woodyatt,2005). Furthermore, “children withautism may rely on idiosyncratic,informal, or problematic behaviors tocommunicate” (Keen et al., 2005, p. 19).When examining teacher responsive-ness to the communicative attempts ofchildren with autism, Keen and col-leagues (2005) found that 38% of thetime teachers did not respond to thechildren’s communicative attempts,even though they identified those
behaviors as intentional communica-tion forms on a checklist. The find-ings suggested that intervention shouldfocus on training adults to attend toacceptable “forms of prelinguisticbehaviors as a means of increasing thechild’s communicative effectiveness andfacilitate the transition from prelinguis-tic to more symbolic forms of communi-cation” (Keen et al., 2005, p. 31).
The role of peers in language inter-vention has also been examined.DeKroon and colleagues (2002) stud-ied children with language impair-ment and compared their play skillsto those of typically developing peers,as well as to peers with languageimpairment. The children with lan-guage impairment took turns partici-pating in two different play groups:one with children who were typicallydeveloping and another with peerswho also had language disorders. Itwas hypothesized that the childrenwould engage in play that is moresuccessful with typically developingpeers than language impaired peers,but the findings did not support this.The language skills of the childrendid not determine the quality of thepretend play they participated in.The results suggested that childrenwith language impairments may ben-efit from interventions that includepeers with or without language disor-ders (DeKroon et al., 2002).
Based on the previous research, alanguage intervention approachincorporating peers and highlyresponsive adults should lead toimprovements in communication andsocial interaction. Therefore, the pur-pose of the present study was to deter-mine if enrollment of functionally non-verbal children in an intensive sum-mer camp program involving interac-tion with peers and highly responsiveclinicians would lead to improvementin functional communication.Specifically, the study examinedwhether the children attempted touse more communication functions,
4
INVITED ARTICLE - Functional CommunicationCamp for Nonverbal Children
Colleen F. ViscontiChristie A. NeedhamCrysten M. SkeboJulianne Wolf
Baldwin-Wallace College

use more sophisticated modes ofcommunication, would be more suc-cessful in their communicationattempts, and whether they wouldattempt to communicate with bothfamiliar and unfamiliar communica-tion partners as a result of their par-ticipation in the summer camp.
MethodsParticipants
The Functional CommunicationSpeech Camp was developed to pro-vide services to children with nonver-bal communication needs, with thegoal of increasing communication,whether it was verbal or nonverbal.The children that participated in thecamp were self-referred from the met-ropolitan Cleveland, Ohio area. Thesechildren ranged in age from 3 years 5months to 14 years and were dividedinto two groups of five. Childrenwere selected for the camp on a first-come, first-serve basis. The onlyenrollment requirements were that thechildren were functionally nonverbalat the beginning of the camp andwere between the ages of 2 and 18years. For the purpose of the camp,functionally nonverbal was defined asnot using verbal communication toconvey wants and needs within thehome environment. Both groups ofchildren attended the speech campfor two hours, three days a week forfour consecutive weeks.
Children were randomly assignedto one of two groups based on whenthey signed up for the camp andscheduling convenience for the fami-ly. Group 1 consisted of five boys,ages 3 years 5 months to 5 years (M =4.45 years or 53 months; SD = 0.63years or 7.57 months), while Group 2consisted of two girls and three boys,ages 3 years 6 months to 14 years (M= 8.2 years or 99.40 months; SD =3.85 years or 46.26 months). The chil-dren presented with disordersincluding speech/language disorder,autism, apraxia, Angelman’s syn-drome, and cerebral palsy. Two ofthe ten children were blind and bothof these children were in Group 2.Seven of the children had previousexperience with some form of aug-
mentative/alternative communica-tion. Specifically, two of the childrenused high-tech dynamic screendevices and the other five used tradi-tional picture exchange communica-tion. Of the two children that usedhigh-tech dynamic screen devices,one had been using it inconsistentlyfor several years and the other hadjust received the device and had notbegun to use it.
The camp was led by a certifiedand license speech-language patholo-gist and two undergraduate studentsmajoring in communicative disorderswho were entering their senior year.One undergraduate clinician hadcompleted three semesters of clinicalexperience and the other undergrad-uate had completed two semesters.Both of the undergraduate studentsparticipated in six hours of trainingprior to the beginning of the camp,where they learned about communi-cation devices and methods of treat-ing children who are nonverbal.
ProceduresEach child participated in an indi-
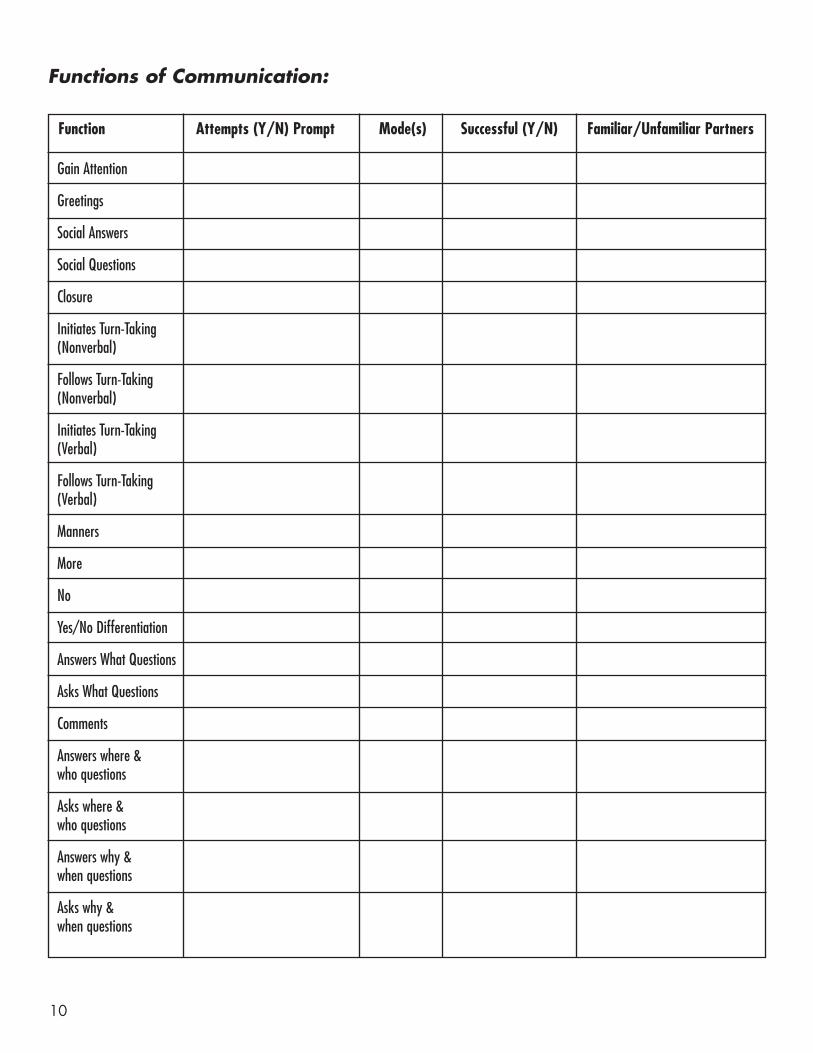
vidual pre-camp evaluation. Thisevaluation was two hours in lengthand involved the child, the parents,the speech/language pathologist, andat least one undergraduate clinician.The evaluation used direct assess-ment/observation along with an inten-sive parent interview, which includedthe Functions of CommunicationChecklist (Appendix A). Specifically,the parents were asked to provide a listof communication partners, describehow their child communicated witheach of those partners, and report ifthe child attempted to use a variety offunctional forms of communication(e.g., greetings, manners, asking andanswering questions, initiating turntaking, etc.). For each function ofcommunication that the child attempt-ed, the parents listed what mode ofcommunication was used (e.g., verbal,gestural/sign, AAC, physical contact,etc.), if they were successful, andwhether that form of communicationwas used with familiar and/or unfa-miliar communication partners.
During the assessment, probes wereconducted to assess each of the itemson the Functions of Communicationchecklist. These items were coded bythe undergraduate student clinician.The skills included on the checklistwere meant to address the many indi-vidual components needed to partici-pate in functional communicationwithin the home environment. Thedata obtained from the parentsregarding functional communicationwere combined with the assessmentof functional communication, withthe lower of the two scores beingused for data analysis purposes.
Therapy goals were developed foreach child through the collaborationof the child’s parents, the speech-lan-guage pathologist, and the undergrad-uate student clinicians. The childrenthen participated in the FunctionalCommunication Speech Camp andwere reassessed at the end of thecamp using the same measures.
The daily routine of the FunctionalCommunication Speech Campremained consistent throughout thecamp. All children participated in alarge group time upon arriving atcamp. This time focused on increas-ing instances of verbal turn-takingand improving pragmatic communi-cation among the campers. Followingthis time, the children were separatedinto three groups. One group workedon pre-literacy activities, anothergroup worked on small group play,and the third group worked on anindividual art activity. The childrenwere rotated through these activitiesfor the majority of the two-hour ses-sion. During this time, the childrenhad a minimum of 15 minutes work-ing one-on-one with a clinician. Theremainder of their time was spent ina small group with two to three oftheir peers. Following the work ses-sion, the children were given anotherperiod of large group play time, inwhich they either engaged in freeplay or a group game (i.e., musicalchairs, ball games, etc.) led by theundergraduate student clinicians.The remainder of the session wasspent in a “circle time” which includ-ed a snack and reading a themedchildren’s picture book.
5

Daily Communication Logs(Appendix B) were developed toinform the parents/caregivers of theirchild’s progress and to assist themwith communication at home. Thesecommunication logs listed specificexamples of utterances produced orused by the child during the camp,activities completed, and behaviormonitoring. There were also com-ments regarding special accomplish-ments (e.g., a good painting or makinga new friend) for the parents to discusswith their child at home. The parentswere then invited to write any ques-tions or observations that they hadregarding their child’s communication.
Once a week, picture books weresent home. These books came in twoforms as appropriate for each child’slanguage skills. Some of the bookswere created by the speech-languagepathologist and undergraduate stu-dent clinicians to facilitate anincrease in the length of the child’sutterances when commenting athome. These were colored andassembled by the children as part oftheir individual work. The otherbooks were published children’sbooks that were adapted to reflect theindividual child’s expressive skillswith a picture computer program(e.g., if the child was using two wordphrases to request, then two wordphrases were developed to follow thestory with pictures and placed intothe book itself).
ResultsPre- and post-test data were collected
using the Functions of CommunicationChecklist. All of the children demon-strated an increase in communication fol-lowing the Functional CommunicationSpeech Camp. Specifically, when exam-ining the attempts children made on theskills listed on the Functions ofCommunication Checklist, the childrendemonstrated improvements on all ofthe items except asking and answeringquestions containing where, who, why,and when, and following nonverbalturns. Paired sample t-tests were con-ducted to determine whether the chil-dren attempted more functions ofcommunication following treatment.The results indicated significant dif-ferences (p< .05) on the followingfunctions of communication items:gaining attention, greeting, socialanswers, social questions, manners,more, and comments (see Table 1).
A second set of paired sample t-testswas conducted to determine whetherthe mode of communication variedfor each of the functions of communi-cation following treatment. Themodes of communication included thefollowing (from least to most sophisti-cated): stopping the activity, physicalcontact, sign or gesture, verbal pro-duction with sign or gesture, AAC,and verbal production alone.Improvements were found in all ofthe functions of communicationexcept asking and answering where,who, why, and when questions. Theresults indicated significant differ-ences (p< .05) on the modes of com-
munication for the following func-tions of communication items: gainingattention, greeting, social answers, clo-sure, manners, more, yes/no differen-tiation, and comments (see Table 2).
The child’s success in improvingfunctions of communication was ana-lyzed pre- and post-treatment. Again,improvements with regard to the suc-cessfulness of communication werenoted in all of the functions of com-munication except asking and answer-ing where, who, why, and when ques-tions and following nonverbal turns.Paired sampled t-tests found signifi-cant differences (p<.05) for the follow-ing functions of communications:greetings, social answers, social ques-tions, closure, manners, more, yes/nodifferentiation, and comments (seeTable 3).
The final area examined was thechild’s familiarity with the communica-tion partner. Once again improvementswith regard to the familiarity with thecommunication partner were noted forall of the functions of communicationexcept asking and answering where,who, why, and when questions. Pairedsampled t-tests found results approach-ing significance on several variables,such as social answers, manners, andyes/no differentiation (p= 0.051), withsignificant differences found on the useof more (p = 0.025).
DiscussionTen children participated in the
Functional Communication SummerCamp that provided interaction withpeers, highly responsive clinicians,
Table 1: Attempts on Functions of Communication
Functions of Communication Pre-test Post-Test
Gains attention M = 0.60 (SD=.516) M=1.00 (SD= .00)
Greeting M = 0.50 (SD=.527) M=1.00 (SD= .00)
Social Answers M = 0.50 (SD=.972) M=1.20 (SD= .632)
Social Questions M = 0.10 (SD=.316) M=0.50 (SD= .527)
Manners M = 0.30 (SD=.483) M=0.80 (SD= .422)
More M = 0.60 (SD=.516) M=1.0 (SD= .00)
Comments M = 0.20 (SD=.422) M=0.60 (SD= .516)
6

and an intensive individualized ther-apy program targeted at increasingtheir communication skills. Pre- andpost-camp test results revealed thatall of the children used more commu-nication functions. This may beattributed to the structure of the campitself. The client to clinician ratio was5:3, which allowed the clinicians tofacilitate interaction within smallgroups and effectively manage indi-vidual behaviors during large groupplay time and circle time. In additionto the client to clinician ratio, the con-sistency of the camp routine allowedthe children to quickly adjust to eachother and their environment andbegin making progress in a relativelyshort period of time. Campers wereindividually taught to use the com-munication functions during individ-ual intervention periods. These com-munication functions were immedi-ately carried over to small group and
large group activities. In addition toimmediately practicing the samecommunication functions in bothindividual and small group settings,communication with the families inthe form of the Communication Logand take-home activities allowed forcarryover of activities and communi-cation to be facilitated at home. Thiscarryover was consistently reportedby parents/caregivers over the courseof the camp.
The manner in which the camperscommunicated was also addressed.At the initiation of the camp, all chil-dren were functionally nonverbal.Throughout the course of the camp,the campers were exposed to a vari-ety of modes of communication, suchas verbal communication, gestures,signs, picture exchange systems, andAAC. All of the participants demon-strated a change in their communica-
tion, with more sophisticated modesof communication being attempted.Once again, this was most likely dueto the structure and schedule of thecamp itself. It should also be notedthat all of the children participatingwere nonverbal and passive commu-nicators. During the camp, one ofthe techniques actively utilized wassilence. The speech-language pathol-ogist and/or the undergraduate stu-dent clinicians would create motivat-ing activities which required commu-nication. These activities were thenfollowed by silence as the clinicianwaited for the child’s communicationattempts. While it is not possible todetermine if this strategy directlyinfluenced the change in the sophisti-cation of communication, it is onepossible explanation.
Additional improvements werealso noted in the campers’ successful-
7
Table 2: Modes on Functions of Communication
Functions of Communication Pre-test Post-Test
Gains attention M = 3.60 (SD=.2.99) M=6.30 (SD= 1.25)
Greeting M = 3.10 (SD=3.38 M=6.00 (SD= 1.05)
Social Answers M =2.80 (SD=3.62) M=6.40 (SD= 0.97)
Closure M = 3.80 (SD=3.39) M=5.90 (SD= 1.10)
Manners M = 2.10 (SD=3.38) M=5.20 (SD= 2.82)
More M = 3.60 (SD=3.31) M=6.70 (SD= 0.48)
Yes/no differentiation M = 3.40 (SD=3.60) M=5.80 (SD= 2.25)
Comments M = 1.40 (SD=2.95) M=4.00 (SD= 3.46)
Table 3: Successfulness on Functions of Communication
Functions of Communication Pre-test Post-Test
Greeting M = 0.50 (SD=.527) M=1.00 (SD= .00)
Social Answers M = 0.30 (SD=.483) M=1.00 (SD= .00)
Social Questions M = 0.10 (SD=.316) M=0.50 (SD= .527)
Closure M = 0.50 (SD=.527) M=1.00 (SD= .00)
Manners M = 0.30 (SD=.483) M=0.80 (SD= .422)
More M = 0.60 (SD=.516) M=1.00 (SD= .00)
Yes/No Differentiation M = 0.50 (SD=.527) M=0.90 (SD= .316)
Comments M = 0.20 (SD=.422) M=0.60 (SD= .516)
ness of communication and their abil-ity to communicate with both familiarand unfamiliar partners. Childrenwere given practice using communi-cation functions with the speech-lan-guage pathologist and the under-graduate student clinicians. Thesefunctions were then directly reportedto the parents/caregiver on the DailyCommunication Log. It should benoted that the improvements in thesuccessfulness of communicationwith a variety of communicationpartners were demonstrated towardsthe end of the intensive summercamp program. This is possibly dueto the fact that the children devel-oped the skills to be successful com-municators during the camp sessionsand then carried over these communi-cation skills to a variety of situationswithin the camp setting and then witha variety of communication partnersoutside of the camp setting.
Significant changes occurred in all ofthe campers’ communication skillsduring the Functional Communication
Camp. Intensive intervention utilizingindividual therapy, along with peerinteraction in small and large groupactivities, directly contributed to thesechanges. However, it is difficult todetermine which part of this interven-tion was responsible for the changesseen. It is hypothesized that the com-bination of the interventions wasresponsible for the improvementsdemonstrated by the participants,since all of the participants had previ-ously received individual communica-tion intervention.
In the future, research should con-tinue to examine programming fornonverbal communicators. Somepossible areas of research includeexamining the effect of this type ofprogram for a longer period of time;instead of a month-long summercamp, possibly create a semester longprogram. Many of the parentsinvolved expressed their desire tocontinue the program throughout theschool year. Additional areas ofresearch may include the effect of
typically developing peer models onintensive intervention for the nonver-bal communicator. In addition, theparents’/caregivers’ perceptions oftheir child’s communication abilitiesshould be assessed. Finally, the useof literacy in intervention with thenonverbal communicators should bedirectly assessed.
In conclusion, all of the childrenwho participated in the FunctionalCommunication Summer Campdemonstrated improvements in func-tional communication. The childrenattempted to use more communica-tion functions. In addition, theirmodes of communication becamemore sophisticated. They were usingsigns/gestures, AAC devices, and ver-bal communication more frequently.The children were also more success-ful in their attempts to communicate.Furthermore, they attempted to com-municate not only with familiar com-munication partners, but also withunfamiliar partners.
8
DeKroon, D. M. A., Kyte, C. S., & Johnson, C. J. (2002).Partner influence on the social pretend play of childrenwith language impairments. Language, Speech, and HearingServices in Schools, 33, 253-267.
Garfin, D., & Lord, C. (1986). Communication as a social prob-lem in autism. In E. Schopler & G. Mesibov (Eds.). SocialBehavior in Autism (pp. 237-261). New York: Plenum Press.
Keen, D., Sigafoos, J., & Woodyatt, G. (2005). Teacher responses tothe communicative attempts of children with autism. Journalof Developmental and Physical Disabilities, 17, 19-33.
REFERENCES
Join OSHLA and Receive
HEARSAYFree of Charge

9
Appendix ABaldwin-Wallace College
Speech ClinicSummer Speech Camp Assessment
Client Name: _________________________________________________________________________________________________
Birthday: _______________________________________________ Age:________________________________________________
Medical Diagnosis: ___________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Speech/Language Diagnosis: __________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Current Modes of Communication: (patient preferred mode, circle family preferred mode)_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
People children encounter everyday:
Are there any people who the child shows interest in communicating with, but the child is not successful in communicating with:_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Person: Role: Mode of Communication
10
Function Attempts (Y/N) Prompt Mode(s) Successful (Y/N) Familiar/Unfamiliar Partners
Functions of Communication:
Gain Attention
Greetings
Social Answers
Social Questions
Closure
Initiates Turn-Taking (Nonverbal)
Follows Turn-Taking (Nonverbal)
Initiates Turn-Taking (Verbal)
Follows Turn-Taking (Verbal)
Manners
More
No
Yes/No Differentiation
Answers What Questions
Asks What Questions
Comments
Answers where & who questions
Asks where & who questions
Answers why & when questions
Asks why & when questions

11
Requesting:
Question words used: __________________________________________________________________________________________
Number of words per request: ___________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Daily Schedule:
Parents Goals for Summer Session:
1. __________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
2. __________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
3. __________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Family Needs for Education:• Programming for current communication aid• Parents Grandparents• Siblings • Caregivers• Babysitters • Others-Specify_________________________• Creation of communication aid for home• Creation of communication aid for caregivers• Use of “My Communication Book”• Creation of “My Communication Book”• Development and use of leisure activities for child• IEP/MFE information • Networking with other parents• Networking for siblings
Other:_________________________________________________________________________________________________________
______________________________________________________________________________________________________________
Time of Day Activity People involved

12
Appendix BDaily Communication Log
Date:___________________
Today I had a: good great so/so Day
Here are some things I did:
Here are some things I said:
Be sure to ask me about:
Consider submittingyour research or clinical article to
HEARSAYContact Laura Kretschmer
University of Cincinnati
513-558-8514

13
Given the need to study the efficacyof treatment (American Speech-Language-Hearing Association, 2005),an increasing number of speech-lan-guage pathologists (SLPs) may be plan-ning clinical research. Clinical studiesdesigned to empirically examinepatient responses to treatment requireapproval from a governing InstitutionalReview Board (IRB). An IRB is a localcommittee formally designated by theUnited States Department of Healthand Human Services Office for HumanResearch Protections (OHRP) toapprove, monitor and review biomed-ical and behavioral research and protectthe rights and welfare of human sub-jects. Unless the design of the studyexempts it from the requirement (e.g.,data collected from existing records insuch a way that subjects cannot beidentified), a researcher must obtain theinformed consent of potential subjects,based on the OHRP Code of FederalRegulations Title 45 Part 46 (45 CFR46) “Protection of Human Subjects”(Department of Health and HumanServices, 2005). Informed consentinvolves establishing that an individ-ual has been provided with relevantinformation regarding the study,demonstrates a level of comprehen-sion or appreciation of this informa-tion sufficient for making a decisionabout consent, is able to make thisdecision in the absence of coercion,and has the cognitive capacity tomake this decision (Beauchamp &Childress, 1994; Savage, 2006).
Clinical researchers in several prac-tice areas (e.g. adult traumatic braininjury and stroke) are likely to studyadults who have cognitive or com-municative difficulties. By definitionunder Subpart A of 45 CFR 46 (alsoknown as the Common Rule andadhered to by most Federal agenciessponsoring human subjects research),such individuals are members of avulnerable population. Although there
are specific guidelines for managingthe consent process with some vul-nerable populations, including (a)children; (b) pregnant women, fetus-es and neonates; and (c) prisoners,the approach to informed consent forindividuals who may have cognitiveimpairment is not explicitly pre-scribed. Nevertheless, researchers areobliged to carefully consider issues ofvulnerability alongside concerns forautonomy when enrolling individu-als with cognitive (or communica-tive) impairment in clinical researchstudies. Together with informationexplaining the rationale for the studyand its methodology, the IRB willrequire a clear plan for how theinvestigator will obtain informedconsent. The purpose of this article isto provide clinician-researchers withan initial discussion of selected issuesinherent in obtaining informed con-sent from potential subjects who mayalso be persons with cognitiveimpairment.
Informed Consent The concept of informed consent is
built upon the foundation of threeguiding principles governing humansubjects research: autonomy of the indi-vidual, beneficence, and justice (NationalCommission for the Protection ofHuman Subjects of Biomedical andBehavioral Research, 1979). Autonomyof the individual refers to the capacityof people to make independent deci-sions without controlling influencefrom others. Beneficence ensures theproposed project’s potential risks andbenefits are reasonably balanced andpresented fairly to prospective sub-jects for incorporation in their deci-sion (Levine, 1986). Justice refers tothe integration of fairness throughoutthe research plan and involvement ofhuman subjects. For example, sub-jects should be selected because theyrepresent a population likely to bene-fit from the research. Additionally,research should be designed so thatthe participation of subjects is notwasted on projects whose results
have little chance of being meaning-ful (e.g. studies with too few partici-pants, without control groups, orwith other methodological deficien-cies). Ensuring adherence to these cri-teria in clinical research requires care-ful planning and implementation ofthe informed consent procedure. Thefollowing paragraphs will providesome examples of how clinicalresearchers might approach informedconsent with adults who are cogni-tively impaired.
Who should obtain consent?In clinical research, the researcher
may have a therapeutic relationshipwith the prospective study partici-pants; e.g., the researcher is thespeech-language pathologist manag-ing their care. Patients under a clini-cian’s care expect the practitioner tohave their best interests at heart andmay not always understand the dif-ference between clinical care andresearch activities (Appelbaum, Lidz,& Grisso, 2004). Appelbaum andcolleagues (2004) described this asthe “therapeutic misconception”. In atypical example, a patient listening toher therapist describe a research proj-ect might be more likely to believe,perhaps mistakenly, that the researchwill benefit her than if a less involvedperson presented the research infor-mation. To ensure the ethical consid-eration of autonomy is preserved,clinical researchers should not sharethe role of researcher and therapist; ifthis is impossible, the researchershould assign a disinterested party toobtain consent.
Determining Capacity andCompetence to Consent to Participation in Research
The principles of autonomy andbeneficence drive the need to deter-mine a potential subject’s capacityand competence to consent to partici-pation. Conservatively defined,capacity is a health care professional’s
INVITED ARTICLE - Informed Consent in ClinicalResearch with Adults with Cognitive Impairment
Kate Krival, Ph.D.Kent State University

clinical judgment about an individ-ual’s demonstrated ability to analyzeinformation and draw conclusionsand competence is a judge’s legal find-ing regarding the person’s right tomake decisions (Marson, 2001). Inpractice, however, experts use theterm capacity to describe the cognitiveskills a potential subject uses to pro-vide informed consent in a given situ-ation; the term competence is used torefer to a judgment, either by a healthcare or legal professional, aboutwhether a person is able to provideinformed consent (Appelbaum &Grisso, 2001; Sturman, 2005).
In order to judge whether aprospective subject with cognitiveimpairment is competent to provideinformed consent to participate, aresearcher needs to assess the indi-vidual’s cognitive skills relative to thetask of autonomous decision makingfor the given research study. Toassume the patient is not capable (e.g.,because he has cognitive impairment,or because he was judged incompe-tent to make a treatment decision aweek earlier during the acute phase ofhis stroke) is to deny him autonomy.On the other hand, to assume that apatient’s decision-making capacity issufficient to consent to research with-out specific evidence about his capac-ity to consent is not beneficent.Beneficence requires that we do goodand protect others from harm; there-fore, we should not accept a patient’sautonomous decision if we assess hiscapacity to be insufficient to appreci-ate the situation or weigh the risks(Appelbaum et al., 2004). So howshould a speech pathologist deter-mine capacity to consent to research?
Because capacity should be assessedas a means to judging competency,clinical researchers should include aprocedure for this assessment in theresearch protocol. Researchers shoulduse an instrument that clearly meas-ures functional capacities related tocompetence (i.e., evidencing a choice,understanding, reasoning, and appre-ciation) (Appelbaum & Roth, 1982).Most informal cognitive assessmentsand even standardized cognitivescreening tools such as the MiniMental Status Examination (MMSE)(Folstein, Folstein, & McHugh, 1975)do not meet this criterion, and werenot developed to assess competency.
Sturman (2005) reviewed twelve stan-dardized instruments that claim tomeasure competency to consent totreatment or research or both. Thereader is referred to this review fordetailed information about instrumentsnot discussed here (Sturman, 2005). Of the tools reviewed, two stand outbased on their design and validation inappropriate populations as instru-ments that might suit the needs of clin-ical researchers including patients withcognitive impairment in studies.
The Capacity to Consent toTreatment Instrument (CCTI)(Marson, Ingram, Cody, & Harrell,1995) assesses competency in rela-tionship to five legal standards:
(1) evidencing a choice; (2) makinga reasonable decision; (3), appreciat-ing the consequences of a treatmentchoice; (4) providing rational reasonsfor a treatment choice and (5) under-standing of the treatment situation andchoices. The initial development of theCCTI included construct validation inadults with Alzheimer’s disease (AD)compared to a normal, elderly controlgroup (Marson et al., 1995). Althoughpatients with AD have impaired deci-sion-making capacity relative to nor-mal older control groups (Kim, 2001,2002; Marson et al., 1995) and few mayhave the capacity for consent, the prin-ciples of autonomy, beneficence, andperhaps justice require that researchersmake this determination before decid-ing that proxy consent should beused.. The CCTI has also been used tostudy capacity in patients withParkinson’s disease (PD) (Dymek,Atchison, Harrell, & Marson, 2001).Compared to a normal control groupof older adults, patients with PD per-formed significantly worse on mostlegal standards, and as the legal stan-dards increased in complexity, theadults with PD demonstrated increas-ing incapacity (Dymek et al., 2001).One limitation of the CCTI is the useof vignettes (one about neoplasm,another about cardiac care) as thebasis for the questions, which maynot elicit the same responses as dis-closures related to participation inclinical research. Despite this limita-tion, the use of the CCTI would be abetter tool for assessing capacity toconsent in individuals with AD orPD than informal assessment or theMMSE.
The MacArthur CompetenceAssessment Tool for Clinical Research(MacCAT-CR) (Appelbaum & Grisso,2001) is a more comprehensive assess-ment than the CCTI. The tool consistsof a semi structured interview thatassesses a person’s decision makingcapacities to understand, appreciate,reason and make choices (Appelbaum& Grisso, 2001). Understanding repre-sents the ability to know the meaningof information disclosed; appreciationcharacterizes the ability to recognizethat information applies to the indi-vidual being questioned; reasoningdescribes the ability to compare anddescribe personal consequences ofoptions and choice reflects the abilityto consistently select an option givenseveral opportunities. The MacCAT-CR is designed so that the examinercan modify standard questions todescribe the specific research project,and then rate the response to eachquestion according to a three pointscale. There is a training manual tohelp the researcher learn how topresent the stimuli and grade theresponses. Although the MacCAT-CRhas been primarily validated inadults with psychiatric disorderssuch as schizophrenia (Appelbaum &Grisso, 2001), it has also been testedin patients with AD (Karlawish, 2002)and cancer (Casarett, 2003), amongother populations.
Assent in The Absence ofCompetence to Consent
Many individuals with cognitiveimpairment will not be competent toconsent to research; others with com-municative impairment may beunable to exhibit competence. Evenso, the consent process must remainguided by the principles of autono-my, beneficence and justice. In thesesituations clinical researchers shouldstill seek the person's assent andrespect his or her dissent, if the sub-ject is capable of providing a clearopinion. Assent is the process ofobtaining permission for participationin a research project from a subjectwho does not possess the legal abilityto give consent. Karlawish (2003) rec-ommended that researchers shouldindicate how measures of decision-making ability demonstrate that a
14

15
person can assent, and the informedconsent form should include a sectionto document whether the subject ade-quately understood key itemsrequired for assent, even if a legalproxy is used to consent.
Who May Provide InformedConsent if the Subject Lacks theCapacity?
States and IRBs have interpretedthe Common Rule’s instruction toensure that a legal health-care proxyprovides research consent for indi-viduals who lack the capacity to con-sent in different ways (Karlawish,2003). For example, an IRB maydetermine that although a DurableMedical Power of Attorney (DPOA)may legally make proxy decisions fortreatment, the DPOA may not consentto research on the patient’s behalfunless explicitly instructed to do soin the DPOA document. Other IRBs
accept the DPOA as suitable to pro-vide consent for research. Some IRBswill accept a person who is not theDPOA as a surrogate for research con-sent; this is an individual who althoughnot a legally authorized representativefor a subject, is able, in specificallydefined situations, to provide researchconsent. Clinical researchers shoulddetermine their governing IRB’s policyand include specific language in theresearch protocol regarding who mayserve as the informed consent forresearch proxy if the subject lacks thecapacity to consent.
Concluding RemarksAdditional issues should attract the
interest of speech language patholo-gists who want to apply best practiceto the ethical conduct of clinicalresearch. How best to present therisks and benefits of the project, how toensure that the methodology is optimalfor the study and the results will have
sufficient meaning, and how to modifythe informed consent process forresearch involving children are amongthe topics that clinical researchers mustconsider. Professors in many universitydepartments are often excellentresources for learning more aboutthese considerations. Clinicians whowant to collaborate with researchers inacademic institutions are likely to findgreat support for their efforts. Manyprofessors enjoy mentoring and work-ing with clinical researchers; such col-laboration in clinical investigationscan also alleviate many of the issuesof the “therapeutic misconception”(Appelbaum et al., 2004). Finally, forthose who work in hospitals, the IRBsof larger institutions are generally gladto provide new investigators with edu-cational materials, training, andanswers to questions in the interest ofpromoting improved protection ofhuman subjects.
REFERENCESAmerican Speech-Language-Hearing Association. (2005).
Evidence-Based Practice in Communication Disorders[Position statement]. [Electronic Version]. Retrieved December2, 2007 from http://www.asha.org/members/deskrefjour-nals/deskref/default.
Appelbaum, P. S., & Grisso, T. (2001). MacArthur CompetenceAssessment Tool for Clinical Research (MacCAT-CR).Sarasota, FL: Professional Resource Press.
Appelbaum, P. S., Lidz, C., & Grisso, T. (2004). Therapeuticmisconception in clinical research: frequency and risk fac-tors. IRB: Ethics in Human Research, 26(2), 1-8.
Appelbaum, P. S., & Roth, C. R. (1982). Competency to con-sent to research. A psychiatric overview. Archives of GeneralPsychiatry, 39, 951–958.
Beauchamp, T. L., & Childress, J. F. (1994). Principles ofBiomedical Ethics. New York: Oxford University Press.
Casarett. (2003). Identifying ambulatory cancer patients at riskof impaired capacity to consent to research. Journal of Painand Symptom Management, 26(1), 615.
Department of Health and Human Services. (2005). 45 CFR46. Retrieved. from http://www.hhs.gov/ohrp/human-subjects/guidance/45cfr46.htm.
Dymek, M. P., Atchison, P., Harrell, L. E., & Marson, D. C.(2001). Competency to consent to medical treatment incognitively impaired patients with Parkinson’s disease.Neurology, 56(17–24).
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state" : A practical method for grading the cogni-tive state of patients for the clinician. Journal of PsychiatricResearch, 12(3), 189-198.
Karlawish, J. H. T. (2002). Alzheimer's disease patients' andcaregivers' capacity, competency, and reasons to enroll in
an early-phase Alzheimer's disease clinical trial. Journal ofthe American Geriatrics Society, 50(12), 2019.
Karlawish, J. H. T. (2003). Research involving cognitivelyimpaired adults. New England Journal of Medicine, 348 (14),1389.
Kim, S. Y. (2001). Assessing the competence of persons withAlzheimer's disease in providing informed consent forparticipation in research. The American Journal OfPsychiatry, 158(5), 712.
Kim, S. Y. (2002). Impaired decision-making ability in subjectswith Alzheimer's disease and willingness to participate inresearch. The American Journal Of Psychiatry, 159(5), 797.
Levine, R. J. (1986). Ethics and Regulation of Clinical Research.(2nd ed.). Baltimore: Urban & Scwarzenberg.
Marson, D. C. (2001). Loss of competency in Alzheimer’s dis-ease: Conceptual and psychometric approaches.International Journal of Law and Psychiatry, 24, 267–283.
Marson, D. C., Ingram, K. K., Cody, H. A., & Harrell, L. E.(1995). Assessing the competency of patients withAlzheimer’s disease under different legal standards. Aprototype instrument. Archives of Neurology (52), 949–954.
National Commission for the Protection of Human Subjectsof Biomedical and Behavioral Research. (1979). TheBelmont Report. Retrieved November 14, 2007, fromhttp://www.hhs.gov/ohrp/humansubjects/guidance/belmont.htm#xinform
Savage, T. A. (2006). Ethical issues in research with patientswho have experienced stroke. Topics in Stroke Rehabilitation,13(4), 1-10.
Sturman, E. D. (2005). The capacity to consent to treatmentand research: A review of standardized assessment tools.Clinical Psychology Review, 25, 954–974.

IntroductionThe number of children with feed-
ing and swallowing disorders contin-ues to increase, largely due to theincreased survival of children withcomplex medical conditions (Lefton-Greif & Arvedson, 2007). The preva-lence of feeding and swallowing dis-orders is estimated to be as high as25% in the general pediatric popula-tion; in children with developmentaldelays this number may be as high as80% (Manikam & Perman, 2000).Speech language pathologists (SLPs)conduct research with and clinicallyevaluate and treat children with thesedisorders. Limited research exists inthis area and the majority of previousstudies have focused primarily onswallowing physiology (Lefton-Greif etal., 2000; Newman, Keckley, Petersen,& Hamner, 2001). Investigationsexploring the functional impact ofthese disorders on families and chil-dren are emerging but still provide alimited representation. To provide thebest services to these families, SLPsneed to recognize the daily strugglesand challenges these families endure(Parrish, 1997). Given that SLPs fre-quently make direct recommenda-tions of modifications and strategiesto try during feeding, understandingthe caregiver’s experiences with feed-ing their child is imperative.
Previous investigations identifiedchallenges in finding caregiversbesides the parent (s) with skills andpatience to feed the child, whichresults in an increased burden on theprimary caregiver (Chamberlin,Henry, Roberts, Sapsford, &Courtney, 1991; Sleigh, 2005). A lackof child care, combined with theadditional time spent caring for and
feeding the child, limits social oppor-tunities for the family (Franklin &Rodger, 2003). An increased sense ofstress was the most commonlyreported emotional response to thesedisorders (Chamberlin et al., 1991;Franklin & Rodger, 2003; Rouse,Herrington, Assey, Baker, & Golden,2002; Sleigh, 2005). Other emotionalresponses included guilt (Craig,Scambler, & Spitz, 2003; Rouse et al.,2002), worry about the child’s nutri-tion (Sleigh, 2005), and fear for thechild’s survival (Franklin & Rodger,2003). The qualitative nature of previ-ous studies on the effects of feedingand swallowing disorders provides adetailed framework to explore theconcerns and challenges. These stud-ies have been however, limited bythe inclusion of only those childrenwith feeding tubes (Craig et al., 2003)or only those children with specificdiagnoses (e.g. cerebral palsy) (Sleigh,2005). None of the previous studieshave included a sample representa-tive of the various types of feedingand swallowing disorders SLPs eval-uate and treat, and none of thesestudies focus on the caregiver’s expe-riences with mealtimes and feeding.
Drewett and colleagues (2002)examined the interactions of childrendiagnosed with failure-to-thrive(FTT) and their caregivers duringmealtime through video analysis.Failure-to-thrive is a common diag-nosis of children with feeding andswallowing disorders, secondary totheir inability to gain weight(Kedesdy & Budd, 1998). There isevidence to support the idea thatchildren with FTT may have subtleoral-motor delays (Reilly, Skuse,Wolke, & Stevenson, 1999).Compared to typical peers, childrenwith FTT consume significantly lessfood and liquid, are more likely tobe fed by their caregiver, and lesslikely to accept a caregiver placingfood into their hand. Although not
statistically significant (p=.05), thechildren with FTT are also proportion-ally more likely to refuse presenta-tions of food. While the Reilly et al.study illustrates the increased chal-lenge of feeding children with FTT, itexamines behaviors from the investi-gator’s perspective, not from the care-givers’ experience. Additionally, noneof the children studied were reportedto have diagnosed oral-motor or swal-lowing disorders.
Currently, few reports of the care-givers’ perspective of the daily chal-lenges associated with caring for achild with a feeding and swallowingdisorder exist in the literature. Thereare no published investigations of thecaregivers’ perspective of feedingchildren with a diverse group of feed-ing and swallowing disorders. Thefocus of this qualitative investigationwas to explore the caregiver’s experi-ence with feeding their child throughtheir own detailed descriptions.
MethodsParticipants
Twenty primary caregivers of chil-dren with feeding and swallowingdisorders aged 1 year to 4 years, 11months were recruited for the thisstudy. They were recruited from thelarge pediatric hospital where theirchild was referred for feeding and/orswallowing problems. All 20 of theprimary caregivers in this study werefemale; this is consistent with previ-ous investigations (Rouse et al., 2002;Sleigh, 2005). The mean caregiver agewas 30.7 years (SD=6.6). Fifteen of theparticipants were Caucasian, fourwere African-American, and one wasAsian-American. The majority (14) ofthe participants were currently mar-ried, four had never married, and twowere divorced. Their highest level offormal education ranged from highschool through a master’s degree.
16
INVITED ARTICLE - Mealtime Experiences inPediatric Feeding and Swallowing Disorders:Caregivers’ Perspectives
Erin E. Redle, Ph.D CCC-SLPKent State University

Descriptive information about thechildren was also collected. The chil-dren had a mean age of 33.4 months(SD=11.2). Eleven of the childrenwere male, nine were female. Theracial diversity was consistent withthat of their primary caregiver. Ten ofthe children were orally fed while tenwere fed via tube (gastrostomy tubeand gastrojejunal tube). Informationregarding past medical history andspecific information about the feedingand swallowing problem was gath-ered from the oral motor/feedingassessments, video swallow studies,fiberoptic endoscopic evaluation ofswallowing (FEES) exams, and inter-disciplinary feeding team reports.
Feeding and swallowing disorderswere categorized by the terms feedingdisorders, oral phase disorders, and pha-ryngeal phase disorders. Feeding disor-ders included food refusal, textureselectivity, and inappropriate meal-time behaviors (Arvedson & Brodsky,2002; Babbitt et al., 1994). Oral phasedisorders consisted of deficits in boththe oral-motor skills necessary to pre-pare the bolus and the necessary poste-rior propulsion of the bolus (Arvedson& Brodsky, 2002; Logemann, 1998).Pharyngeal phase disorders includedobserved delayed swallow initiation,penetration, aspiration, and the pres-ence of pharyngeal residue (Arvedson& Brodsky, 2002; Logemann, 1998).These three categories rarely existed inisolation and multiple combinationswere found. Fifteen children presentedwith feeding-oral phase disorders, onewith an oral phase-pharyngeal phasedisorder, and four with feeding-oralphase-pharyngeal phase disorders.Underlying medical etiologies con-tributing to the feeding and swallow-ing disorders are presented in Table 1.
Data collection and analysis
Participants were individuallyinterviewed using a semi-structuredinterview format with an interviewguide to facilitate consistency in thequestions while allowing the examin-er to probe areas in more depth(Patton, 2002). The interview guidecontained questions exploring theimpact that caregivers perceived thattheir child’s the feeding or swallow-ing disorder had on their daily life,
including the specific impact onmealtimes. Audio recordings of allinterviews were collected and initial-ly stored on a digital voice recorder.Following the interview, the digitalinterview files were transferred to acomputer for storage. The interviewswere then transcribed by the primaryinvestigator into a word processingdocument for editing and storageand then imported into NVivo? soft-ware (QSR-International, 2006) forqualitative analysis.
Content analysis was used to ana-lyze interview transcripts. Theprocess of content analysis stratifiesthe information contained in the inter-views into an organized hierarchythrough the identification of themes,coding, and categorization of data(Patton, 2002). The procedures forcontent analysis were consistent withthe methods outlined by Patton (2002)but modified to allow for electroniccoding. In qualitative research, dataare coded to provide a name or labelto specific passages representing reoc-curring themes and topics (Frankel &Wallen, 2003; Patton, 2002).
Coding was completed in two dis-tinct phases. First, free coding wasused to analyze the data. Free cod-ing facilitates an initial review of thedata to examine for themes and ideaswithout predetermined definitions orclassifications. These free codes werethen analyzed for redundancy andcodes with similar features were col-lapsed into a single code. Operationaldefinitions were created for the sec-ond set of codes and the primaryinvestigator then re-coded all of theinterview data to ensure all codingwas consistent. Using the establishedcodes, a graduate student in speechlanguage pathology coded 33% of thecoded data for reliability. Theseresults were analyzed using aMezzich’s kappa (Eccleston, Werneke,Armon, Stephenson, & MacFaul,2001); reliability was substantial(Î=.70) (Fink, 2003).
ResultsMultiple themes were identified
across the interviews as part of alarger study. The results presented in
this report are specific to the care-givers’ experiences with feeding theirchild. For all information presentedbelow, feeding refers to oral feedings.The results of the different experi-ences, along with supporting quota-tions, are presented below.
Caregiver Experiences withFeeding/Mealtimes
Caregivers illustrated the burden ofbeing the only person to feed their childat mealtimes. One mother stated“It’s usually just [name] and I sittingdown… you know there’s no bigfamily meals anymore.” Anothermother described mealtime as “I’llspend 15-20 minutes trying to get herto eat, and her dad’s eating at thattime too…until she’s done or I’m tootired of trying to feed her.” In this sit-uation, although the family is togetherthey are not sharing a mealtime expe-rience; rather the mother is focused oncaring for the child at the expense ofher own eating and interaction withother family members. “He wouldn’teat for Mike [dad] all day, he wouldwait for me to get home from workevery day.” Mothers also describedbeing the only one in the family withthe experience and patience to feedtheir child, “He [referring to thefather] doesn’t work with her at all.And every time I ask him to workwith her he gets very frustrated andhis answer is [he] just takes it away.”
Parents in this study also describedapproaches to oral feedings and a vari-ety of approaches were described,largely due to their child’s level ofresistance. Some parents describedtheir efforts to facilitate oral eatingincluding more persistent approach-es, “He usually clenches his jaw ormost of the time and I have to forcehis food into him” and placingmashed potatoes “on her lips reallyquick and she’ll lick them off but shegags.” Other parents have relin-quished control to the child, describ-ing their experiences “We’ve tried thetricking him and it backfires becauseif he realizes that’s in it his food hewon’t finish eating his regular food”and “you can't force him to do some-thing because it's not going to work.”Another mother reported “We justhave to totally leave up to her what’s
17

she’s going to eat and what she’s notgoing to eat. Because we’ve found inthe last two years that if you make hereat something she regresses.” Othercaregivers described how they incor-porated suggestions from therapists toencourage interaction … “[name] sitsin a high chair and we give him hisfood and he usually doesn't eat it andin order for him to get out of his chairhe needs to kiss or lick some part ofthe meal.”
A unique finding was the reportedfear of feeding children with bothfeeding and swallowing disorders.One mother stated having a child witha feeding and swallowing problemwas, in general, “scarier, I mean youare more concerned.” Caregivers wereafraid of both the child’s choking andthe complications of aspiration. “I’mafraid to give her anything big becauseI’m afraid she’d really have issues try-ing to swallow it,” and “She still hasan occasional choking…. if she goessomewhere is she going to choke?”
Children’s Responses to Mealtime
Children with feeding and swal-lowing disorders are known to havenegative behaviors associated withfeeding and mealtimes (Arvedson &Brodsky, 2002; Babbitt et al., 1994). Inthis investigation, these behaviors aredescribed directly by the parent.Caregivers frequently described theirchild’s negative reactions to mealtimeusing words like “fight” and “battle”to describe their interactions withchildren with feeding including“Sometimes he sees me getting thoseout [crackers] and he starts kickingand…you know it’s going to be afight” and, “We give her food and wetry to get her to eat it or taste it… it’s abattle.” Another caregiver describedher daughter’s intense reactions to thespoon, “You try to go at her with herspoon and she knows something’s onthere she’s, I mean she’s, flying herselfbackwards and having a fit.” Eventhe sight of food was reported to elic-it negative responses, “Even when hesees food coming he will start to cry.”
Another dilemma for caregiverswas the child’s inconsistency witheating. Parents reported their chil-dren were inconsistent in what they
would accept on a day-to-day basis.“I mean one day he may eat some-thing so we try to give that to himthe next day. And he won’t haveanything to do with it.” Parent’s alsoreported inconsistency between whatthe children would do in therapy andfor the parents. “The professionalscan get him to eat. But I take himhome and I can’t and I try the samethings that they do.”
DiscussionThis qualitative study explored the
experience of feeding a child with afeeding or swallowing disorder fromthe caregiver’s perspective. Theirdescriptions are generally consistentwith previous investigations on theimpact of feeding and swallowingdisorders on daily life with somethemes novel for the pediatric popu-lation emerging. Because the chil-dren in this study had feeding, oral,and pharyngeal phase swallowingdisorders, the experiences reportedare more representative of caregiverexperiences for children and familiesseen on an SLP’s caseload. Theexperiences of the role as the onlyone who can feed their child, a fear offeeding their child, altered approaches tofeeing their child, the child’s reactionsto eating, and the child’s inconsistencyare discussed below.
Within the caregivers’ experiences,multiple caregivers reported being theonly one to feed their child. This isconsistent with previous investigationsof limited population (Chamberlin etal., 1991; Sleigh, 2005) This places asignificant burden on the primarycaregiver. In a child without a feedingtube, a constant concern exists regard-ing proper nutrition and this burdengenerally seems to fall entirely on theprimary caregiver. Even in childrenwith a feeding tube, the interactionbetween child and caregiver duringoral feeding is a unique experience.(Sleigh, 2005). Many caregivers arewilling to take on this challenge as away of attempting to improve theirskills and the care of their child.
The fear of feeding in this study is acombination of concerns regardingaspiration and choking. Concernsregarding choking are described in
studies of children with cerebralpalsy (Sleigh, 2005) and adults withdysphagia (McHorney et al., 2000).Caregiver concerns about aspirationdirectly contrast the findings of Craiget al. (2003) in which parents report-ed they did not believe the childrenwere aspirating and would feed thechild unless overt signs of aspirationwere present.
The child’s reactions to eating, andmore specifically, their negative reac-tions with eating, are well document-ed in children with feeding and swal-lowing problems (Arvedson &Brodsky, 2002; Babbitt et al., 1994;Crist, Dobbelsteyn, Brousseau, &Napier-Phillips, 2004; Turner, Sanders,& Wall, 1994). Descriptions of meal-time as “battles” and “struggles” arealso consistent with previous reports(Sleigh, 2005; Turner et al., 1994).However, the caregivers’ responses tothese behaviors through their alteredapproaches to feeding have not beenspecifically identified in the litera-ture. These altered approaches rangedfrom more assertive attempts to feedthrough a resolve to follow the child’slead. In this investigation no attemptwas made to investigate why care-givers used these different approachesand if any, or all, were successful. Themotivation and success of alteredapproaches to feeding should beinvestigated in further detail.
Implications for Clinical PracticeThe inclusion of parents in the ther-
apeutic process is crucial for the treat-ment of their children with feedingand swallowing disorders (Arvedson& Brodsky, 2002; Manikam & Perman,2000). Parents routinely receive directtraining as a component of treatmentprograms for children with feedingproblems (Birch, Gunder, Grimm-Thomas, & Laing, 1998; Farrell,Hogopian, & Kurtz, 2001; Galensky,Miltenberger, Stricker, &Garlinghouse, 2001; Werle, Murphy,& Budd, 1993). However, the resultsof this study indicate the experienceof the caregivers of these children isvery stressful The SLP must insurehe/she understands the family cir-cumstances when a parent is asked tocarryout activities and exercises.
18

Clinicians need to be acutely awareof the caregiver’s level of stress.Previous studies have documentedthe increased stress in caring for achild with a feeding and swallowingproblem (Chamberlin et al., 1991;Franklin & Rodger, 2003; Rouse et al.,2002; Sleigh, 2005). Having a sensi-tivity to stress does not mean that cli-nicians should not offer strategiesand activities to implement in thehome. Rather, clinicians need to usethe caregiver’s capacity to help theirchild as an opportunity to empowerthe caregiver by interviewing themabout their day to day feeding expe-riences. Providing caregivers withthe opportunity to feel they areassisting their child may empowerthe family, a key component to suc-cessful families (Luterman, 1996).
Caregivers must be provided withopportunities to successfully imple-ment therapy strategies. Frequentlyin clinical practice caregivers aregiven a “take home recommenda-tion” the therapist has tried with thechild during the session or that hasnever been tried with the child.Clinicians need to provide caregiversthe opportunity to try out recommen-dations with the therapist present toensure the caregiver understands therecommendation and how to imple-ment it. Further, if the therapist cansee the child’s reaction and be avail-able for immediate feedback to theparent, outcomes at home may besignificantly improved. Providingpositive feedback to the caregiverregarding their efforts is also recom-mended to increase the caregiver’s
confidence and self-esteem (Hanson& Lynch, 1995; Luterman, 1996).
SummaryFurther investigations of the func-
tional impact of feeding and swallow-ing disorders, especially from the per-spective of the caregiver, are greatlyneeded. Additionally, we need to findways to help families to have moresuccessful feeding experiences, both tohelp the child, and just as importantlyto help the caregiver and family.Doing so will improve the child’s longterm health and development, and fos-ter an improved parent/child andfamily/SLP relationship.
19
Diagnosis Primary Diagnosis Secondary Diagnoses(n=20) (n=20, can have 2
secondary)
Shaken baby syndrome 1Cardiac disorders 2 1Chiari malformation 1Chronic vomiting 2Congenital neurological disorder 4Genetic syndrome 4GERD 3 5Metabolic disorders 1Neural tube defect 2Seizures 1Sensory Integration Disorders 2 4Classified as complex medical disorders* 4* Children with >3 secondary conditions were categorized as medically complex
Table 1: Primary and Secondary Diagnoses of the Participants Children

20
REFERENCESArvedson, J. C., & Brodsky, L. (2002). Pediatric Swallowing and
Feeding: Assessment and Management. (2nd ed.). Albany, N.Y.:Singular Publishing Group.
Babbitt, R. L., Hoch, T. A., Coe, D. A., Cataldo, M. F., Kelly, K. J.,Stackhouse, C., et al. (1994). Behavioral assessment andtreatment of pediatric feeding disorders. Developmental andBehavioral Pediatrics, 15, 278-291.
Birch, L. L., Gunder, L., Grimm-Thomas, K., & Laing, D. G.(1998). Infants’ consumption of a new food enhances accept-ance of similar foods. Appetite, 30, 283-295.
Chamberlin, J. L., Henry, H. M., Roberts, J. D., Sapsford, A. L.,& Courtney, S. E. (1991). An infant and toddler feedinggroup program. American Journal of Occupational Therapy, 45,907-911.
Craig, G. M., Scambler, G., & Spitz, L. (2003). Why parents ofchildren with neurodevelopmental disabilities requiring gas-trostomy feeding need more support. Developmental Medicineand Child Neurology, 45, 183-188.
Crist, W., Dobbelsteyn, C., Brousseau, A. M., & Napier-Phillips,A. (2004). Pediatric assessment scale for severe feeding prob-lems: Validity and reliability of a new scale for tube-fed chil-dren. Nutrition in Clinical Practice, 19, 403-408.
Drewett, R. F., Kasese-Hara, M., & Wright, C. (2002). Feedingbehaviour in young children who fail to thrive. Appetite, 40,55-60.
Eccleston, P., Werneke, U., Armon, K., Stephenson, T., &MacFaul, R. (2001). Accounting for overlap? An applicationof Mezzich's kappa statistic to test inter-rater reliability ofinterview data on parental accident and emergency atten-dance. Journal of Advanced Nursing, 33(6), 784-790.
Farrell, D. A., Hogopian, L. P., & Kurtz, P. F. (2001). A hospital-and home-based behavioral intervention for a child withchronic food refusal and gastrostomy tube dependence.Journal of Developmental and Physical Disabilities, 13(4), 407-418.
Frankel, J. R., & Wallen, N. E. (2003). How to Design and EvaluateResearch in Education. Boston: McGraw Hill.
Franklin, L., & Rodger, S. (2003). Parents' perspectives on feed-ing medically compromised children: Implications for occu-pational therapy. Australian Occupational Therapy Journal, 50,137-147.
Galensky, T. L., Miltenberger, R. G., Stricker, J. M., &Garlinghouse, M. A. (2001). Functional assessment andtreatment of mealtime behavior problems. Journal of PositiveBehavior Interventions, 3(4), 211-224.
Hanson, M. J., & Lynch, E. W. (1995). Early Intervention:Implementing Child and Family Services for Infants andToddlers Who Are At Risk or Disabled (Second Edition ed.).Austin, TX: Pro-Ed.
Kedesdy, J. H., & Budd, K. S. (1998). Childhood Feeding Disorders:Biobehavioral Assessment and Intervention. Baltimore: Paul H.Brookes Publishing Company.
Lefton-Greif, M. A., & Arvedson, J. (2007). Pediatric feeding andswallowing disorders: State of health, population trends, andapplication of the International Classification of Functioning,Disability, and Health. Seminars in Speech and Language, 28(3),161-165.
Lefton-Greif, M. A., Crawford, T. O., Winkelstein, J. A.,Loughlin, G. M., Koerner, C. B., Zahurak, M., et al. (2000).Oropharyngeal dysphagia and aspiration in patients withataxia-telangiectasia. The Journal of Pediatrics, 2, 225-231.
Logemann, J. (1998). Evaluation and Treatment of SwallowingDisorders (Second edition ed.). Austin: PRO-ED, Inc.
Luterman, D. M. (1996). Counseling Persons with CommunicationDisorders and Thier Families. Austin, TX: Pro-Ed.
Manikam, R., & Perman, J. A. (2000). Pediatric feeding disorders.Journal of Clinical Gastroenterology, 30(1), 34-46.
McHorney, C. A., Bricker, D. E., Kramer, A. E., Rosenbek, J. C.,Robbins, J., Chignell, K. A., et al. (2000). The SWAL-QOLoutcomes tool for oropharyngeal dysphagia in adults: I.Conceptual foundation and item development. Dysphagia, 15,115-121.
Newman, L. A., Keckley, C., Petersen, M. C., & Hamner, A.(2001). Swallowing function and medical diagnoses in infantssuspected of dysphagia. Pediatrics, 108(6), 1-4.
Parrish, M. (1997). Family adaptation to a child's feeding andswallowing disorder: a social work perspective. Seminars inSpeech and Language, 18(1), 71-77.
Patton, M. Q. (2002). Qualitative Research and Evaluation Methods.Thousand Oaks, CA: Sage Publications, Inc.
QSR-International. (2006). NVivo (Version 7): QSR International.
Reilly, Skuse, D. H., Wolke, D., & Stevenson, J. (1999). Oral-motor dysfunction in children who fail to thrive: organic ornon-organic? Developmental Medicine and Child Neurology,41(2), 115-122.
Rouse, L., Herrington, P., Assey, J., Baker, R., & Golden, S.(2002). Feeding problems, gastrostomy and families: a qualita-tive pilot study. British Journal of Learning Disabilities, 30, 122-128.
Leigh, G. (2005). Mother's voice: A qualitative study on feedingchildren with cerebral palsy. Child: Care, Health, andDevelopment, 31(4), 373-383.
Turner, K. M. T., Sanders, M. R., & Wall, C. R. (1994).Behavioural parent training versus dietary education in thetreatment of children with persistent feeding difficulty.Behaviour Change, 11, 249-258.
Werle, M. A., Murphy, T. B., & Budd, K. (1993). Treating chronicfood refusal in young children: Home based parent training.Journal of Applied Behavior Analysis, 26, 412-433.

21
This brief article describes the back-ground and travels of Dr. F.C. Jeng whohas been employed at Ohio Universitysince September, 2006 as the PrincipalInvestigator at OU’s AuditoryElectrophysiology Lab.
Dr. Jeng received an MD degree inat the China Medical University(Taiwan) in 1992 and specialized inOtolaryngology after a four-year resi-dent training at the Cathay GeneralHospital in Taiwan. He practiced inTaiwan until January 2002 when hebegan a Ph.D. program in Speechand Hearing Science at theUniversity of Iowa . He completedand received a PhD in 2006. Hisstudy interests are in auditory physi-ology with emphases in evokedpotentials and mechanisms of per-ception of complex sounds in normaland hearing-impaired listeners.
His 2004 pre-dissertation researchproject on estimating air-bone gaps byusing auditory steady-state responsesin human subjects with simulated con-ductive hearing losses was publishedin the Journal of the AmericanAcademy of Audiology. In 2005 thearticle, “Estimating air-bone gapsusing auditory steady-state responses”was selected by the Hearing Journal(2005, 58(6) page 40-46) as one of thebest articles published in 2004 in the“Diagnostic Audiology” category. Hisdissertation entitled “ElectricallyEvoked Auditory Steady-StateResponses (ESSR) in Guinea Pigs”,won the 2005 Student InvestigatorResearch Award from the AmericanAcademy of Audiology. This projectmanaged to record the auditoryresponse that reflects the periodicityof electrical stimulation, similar tothe type of stimulus produced by the
speech processors of cochlearimplants. In his dissertation, Dr. Jengsuccessfully separated the responsefrom the continuous electric stimulusartifact and the background noise byusing frequency analysis techniquesimplemented in custom-madeLabView and MatLab programmingcodes. Furthermore, the divergenceof modulation transfer function atlow (13 -55 Hz) and high (65 – 320Hz) modulation frequencies suggest-ed that the sources of these potentialsmight be different. The electricallyevoked responses at the high rates ofmodulation show a latency of 2.23 ±0.68 ms, while those to the lowerrates show a latency of 22.13 ± 4.84ms. Based on the latency derivedfrom the modulation transfer func-tion, it is likely that nuclei in theauditory brainstem pathway areimportant participants of the evokedresponse elicited by using amplitudemodulated electric sinusoids at thehigher rates but rather that the corti-cal, subcortical areas and the thala-mus play important roles for thelower modulation rates (Jeng et al.,2007, 2008).
Dr. Jeng continues explanations ofhis research in his own words:
Since the very beginning of mystudy of the ear, I dreamed to find aplace that would allow me to contin-ue my work in the field of auditoryelectrophysiology and to fulfill mydream to develop a technique thatcan be used to record a response thatreflects the modulation of speech sig-nals. For this reason, I moved to theSchool of Hearing, Speech andLanguage Sciences at Ohio Universityin 2006 and am currently setting upan Auditory ElectrophysiologyLaboratory. The Lab is housed in anewly renovated Grove Center atOhio University and is a state-of-the-art facility which contains equipmentto conduct basic and applied research
projects. I am currently expandingthe research lines that I have beendoing during the past five years aswell as developing new ideas andresearch projects.
As a continuation of my research inIowa, I am currently developing acollaborative research project with mycolleagues at the University of Iowa.The purpose of this project is to 1)determine the auditory origin of theelectrically evoked auditory steady-state response in human cochlearimplant users, 2)to examine the vari-ous generator sites and signal process-ing mechanisms of the elicitedresponse, and 3) to assess the utility ofthe elicited response to programspeech processors for cochlear implantusers. Electrical activities of the brainwill be recorded from the scalp using amulti-channel recording system inadult cochlear implant users and age-matched normal hearing subjects.Dipole source analysis and modula-tion transfer functions will be derivedto evaluate the various generator sitesand signal processing mechanisms ofthe evoked response in cochlearimplant users. Linear regression willbe used to estimate and predict therelationship between the electrophysi-ological measures and behaviorallyestimated programming levels.Although the proposed study is pri-marily concerned with the fundamen-tal principles and potential clinicalapplications of the elicited response inadult cochlear implant users, it hasimportant implications for young chil-dren and those who cannot providereliable behavioral clinical responses.A better understanding of the signalprocessing mechanisms of the electri-cally stimulated auditory system willbe helpful in future designs of cochlearimplants and of speech processor fit-ting strategies. Thus, results of theproposed project have strong potentialto improve the quality of life for manycochlear implant users.
INVITED ARTICLE - Travels of an Auditory Researcher
Fuh-Cherng Jeng, MD, PhDOhio University

In addition to the collaborativeresearch project with the Universityof Iowa, I am currently expandingnew lines of research at OhioUniversity. These projects focus onexploring how our ears and brainsrespond to sounds and how the sen-sory information of simple and com-plex sounds is represented in these
responses. Specifically, I plan to con-tinue pursuing investigation of theamplitude-modulation and frequencyfollowing responses, lexical-toneelicited responses, and cognitiveauditory potentials in normal andpathological populations. Theseobjectively obtained electrophysiolog-ical responses will then be compared
with each individual’s behavioralmeasurements. For people who areinterested in my research, details canbe found on the OU AEP website:http://oak.cats.ohiou.edu/~jeng/jeng.htm
22
REFERENCESJeng, F.-C., Abbas, P. J., Brown, C. J., Miller, C. A., Nourski, K.
V., & Robinson, B. K. (2007). Electrically evoked auditorysteady-state responses in guinea pigs. Audiol Neurotol;12:101-112 (DOI: 10.1159/000097796).
Jeng, F.-C., Abbas, P. J., Brown, C. J., Miller, C. A., Nourski, K.V., & Robinson, B. K. (2008). Electrically evoked auditorysteady-state responses in a guinea pig animal model:Latency estimates and effects of stimulus parameters.Audiol Neurotol, 13, 161-171 (DOI: 10.1159/000112424).
Jeng, F.-C., Brown, C. J., Johnson, T. A., & Vander Werff, K. R.(2004). Estimating air-bone gaps using auditory steady-stateresponses. J Am Acad Audiol, 15(1), 67-78. [Awarded “Best of2004” in “Diagnostic Audiology” category, The HearingJournal, 2005, 58 (6), 40-46].
Consider Joining the
HEARSAYEditorial Staff
Contact Laura Kretschmer([email protected])
University of Cincinnati
513-558-8514

23
Researchers, practitioners, and pro-gram administers are increasinglyinterested in identifying and address-ing the gaps in knowledge that limitthe effectiveness of speech-languagepathology services. At least in part, thisinterest is derived from the paradigmshift towards engaging in evidence-based practice (EBP), in which clinicalprofessionals are expected to integrateknowledge of the empirical evidence intheir decision-making practices(Dollaghan, 2004; Fey & Justice, 2006).Of particular import is clinicians’ aware-ness of and access to specific techniquesor approaches that have been shown to“work” with specific populations orunder specific conditions.Characteristically, the type of researchthat attempts to show whether some-thing works (or not) uses experimentalmethodologies, such as the randomizedcontrolled trial (RCT). In the RCT, theresearcher manipulates an independentvariable and looks at its presumablecausal relation with a particular out-come. Although there are othermethodologies that allow one to makecausal inferences, the RCT, when con-ducted well, can provide quite strongevidence regarding the causal relationsbetween a particular treatment (theindependent variable) and a specificoutcome (the dependent variable).
Large-scale experimental RCTs, inparticular, can help us identify impor-tant gaps in our understanding of treat-ment. For instance, in a forthcomingarticle, Gillam et al. (in press) willreport findings from the largest andmost rigorously conducted study of theefficacy of language intervention forschool-aged children with languageimpairment (LI). In this randomizedcontrolled trial, 216 children (ages 6 to9 years) were randomly assigned toone of four conditions. Two conditionsfeatured computer-assisted languageintervention (Fast ForWord (ScientificLearning Corporation, 2007), Earobics(Houghton Mifflin, 2007)), one featured
academic enrichment, and one featuredone-on-one language intervention witha certified speech-language pathologist(SLP). Children in all groups receivedintervention for more than 45 hoursover a 6-week period of daily sessions.Although children showed “clinicallysignificant gains” over time in terms ofeffect-size estimates on standardizedmeasures of language ability (Cohen’s dvalues for pretest/posttest comparisonsranged from .56 to .79), there were no sta-tistically significant differences across con-ditions. While the primary hypothesistested in this study concerned the useof computer-assisted instruction, thefinding of a general null effect for allconditions is quite troubling, as it sug-gests that one-on-one treatment by acertified SLP using ‘gold standard’ clin-ical protocols does not accelerate lan-guage growth beyond that we see forenrichment or computer-based instruc-tion. Clearly, the results of the Gilliamand colleagues study suggest that RCTscan offer speech-language pathologistsimportant information regarding “whatworks” in the way of current practice.This type of experimental methodology,however, has yet to be implementedwidely among language interventionresearchers and practitioners. Therefore,the field of speech-language pathologywould greatly benefit from more large-scale “use-inspired research” that estab-lishes testable hypotheses regardingpossibly potent approaches to languageintervention that can then be studied incontrolled trials.
Our own research interests are direct-ly aligned with the EBP paradigm inthat we are deeply invested in improv-ing the capacity of clinicians to engagein EBP by asking and answering press-ing questions about “what works.” Aparticular interest of ours is the issue ofspeech-language therapy dosage. Todate, we know surprisingly very littleabout dosage (see Warren, Fey, &Yoder, 2007) even though many SLPsview dosage as a critical component oftreatment delivery. While textbookstoday typically steer clear of makingexplicit recommendations regardingintervention dosage, the tacit assump-tion in treatment manuals is thatdosage matters greatly. For instance,
Klein and Moses (1999) describe a man-agement plan for 5-year-old “Darryl”in which four long-term goals will be“achieved within three years” (p. 113),although more specific dosage recom-mendations are vague (e.g., “individualsessions may range from 15-min to 45-min”). At least in part, this stems fromthe dearth of information regardinghow intervention dosage is associatedwith children’s language growth.Drawing from the work of Warren andcolleagues (2007), we define dosage asthe cumulative intervention intensitywhich consists of the product of threecomponents: (1) dose, (2) dose frequen-cy, and (3) total intervention duration.Dose refers to the number of times theSLP addresses a target or uses a tech-nique during a given therapy session(e.g., 30 models in 30 minutes). Dose fre-quency refers to how long a therapy ses-sion lasts in minutes and how oftentherapy is delivered throughout a weekor month (e.g., 1 hr. per wk). Total inter-vention duration refers to the time peri-od during which intervention is deliv-ered (e.g., 9 months). Taken as a whole,dosage refers to the overall intensity ofintervention that a given child experi-ences. As Warren and colleaguesrecently noted, intervention dosagemay indeed play a critical role in maxi-mizing the effects of language interven-tion. Yet, virtually no studies in the lit-erature on child language impairmentto date have studied dosage as an inde-pendent variable. Therefore, we informour work through the empirical consid-eration of dosage in the adult aphasialiterature, a literature which has care-fully considered the way in whichdosage alone – particularly interven-tion intensity – may impact languagegains for adults whose language abili-ties have been compromised due to lefthemisphere damage.
Theoretically, research in the field ofaphasia on dosage effects is based onthe notion that individuals who experi-ence more intensive intervention willmake greater gains in language, andstudies involving adults with aphasialend support to this notion. Contrast-comparisons based on the same lan-guage intervention delivered at regularand intensive rates (i.e., 60 sessions vs.
INVITED ARTICLE - Evidence-Based Practice:Where Do We Go From Here?
Laura M. JusticeAllison BreitThe Ohio State University

130 sessions in 6 months) indicate thatindividuals receiving intensive therapyachieve higher language scores (Basso& Caporali, 2001; Denes, Perazzolo,Piani, & Piccione, 1996; Hinckley &Craig, 1998). However, despite theseemingly direct comparison betweenvariations in intervention dosage,aphasia dosage studies have focusedexclusively on dose frequency and havefailed to account for the distribution oflearning trials within each session –that is, the actual dose in learningopportunities. As a result, it is some-what unclear as to whether dose fre-quency is a critical determinant of lan-guage gains or whether dosage (learn-ing opportunities within a session) ismost important.
Several meta-analyses designed toestimate the effects of language inter-vention techniques on child languageoutcomes have included considerationof the intensity of the intervention,focusing exclusively on dose frequency(and not dosage per se). These reviewsoffer no consensus on optimal dosageof intervention or even whether dosagematters to treatment effectiveness. Themost recent meta-analysis to date, byLaw, Garrett and Nye (2004), suggestedthat language interventions lastinglonger than eight weeks are more effec-tive than those of shorter duration.Nye, Foster, and Seaman (1987), how-ever, found interventions lastingbetween 4 and 12 weeks to have thehighest effect sizes (over those of short-
er or longer duration), whereas Fey,Cleave, and Long (1997) proposed anoptimum length of 4.5 months (18weeks). Despite the lack of agreementregarding whether dosage matters andwhether SLPs ought to configuredosage for children on the basis of spe-cific language profiles (e.g., highertreatment dosage for more severe casesof impairment) or background charac-teristics (e.g., lower treatment dosagefor children who access more language-learning supports in the classroom orat home), dosage is one of the most-highly specified and at times one of themore contentious features of a stud-dent’s Individualized EducationProgram (IEP).
Given the pressing nature of thisclinical question and lack of research,in the next several years we will studydosage by generating hypothesesregarding the association of dosage tochildren’s language gains within inter-vention in descriptive work that usescausal modeling. In descriptive workwe do not manipulate an independentvariable; rather, we study the associa-tions among variables. By collectingdata on dosage of treatment and lan-guage growth over time for a largegroup of children who receive lan-guage intervention within schools, wecan explore whether dosage (e.g.,cumulative amount of time spent intherapy) is associated with the magni-tude of language growth. If dosageemerges as an operative variable (i.e., is
associated with children’s languagegrowth, particularly when we controlfor other potentially influential vari-ables, like age or severity of languageimpairment), we can then design andimplement RCTs in which we activelymanipulate dosage. For instance, wemight study language growth in chil-dren with language disabilities who areassigned to two different conditions. Inone condition children receive lan-guage intervention two times perweek, whereas in the other conditionchildren receive language interventionfour times per week. Although manySLPs would argue on a theoretical basisthat more treatment is better, we are notaware of any experimental data whichsupport this contention. In the age ofevidence-based practice, it is not desir-able (although it is common) to relysolely on theoretical understandings asthe basis for such important clinicaldecisions as how many treatment ses-sions a child should receive in a week.As tedious as it may be to practice inthe midst of yet another paradigm shift– the movement to EBP – a likely out-come will be that we do have moreempirical guidance when we seek toanswer pressing issues in our practice,even ones which seem relatively simple(e.g., How many times should I providetreatment to a child in a week?) in com-parison to the host of more complexissues that we face everyday.
24
REFERENCESBasso, A., & Caporali, A. (2001). Aphasia therapy or the impor-
tance of being earnest. Aphasiology, 15(4), 307-332.Denes, G., Perazzolo, C., Piani, A., & Piccione, F. (1996).
Intensive versus regular speech therapy in global aphasia: Acontrolled study. Aphasiology, 10(4), 385-394.
Dollaghan, C. A. (2004). Evidence-based practice in communica-tion disorders: What do we know, and when do we knowit? Journal of Communication Disorders, 37(5), 391-400.
Fey, M. E., Cleave, P. L., & Long, S. H. (1997). Two models ofgrammar facilitation in children with language impair-ments: Phase 2. Journal of Speech, Language, and HearingResearch, 40(1), 5-19.
Fey, M. E., & Justice, L. M. (2006). Evidence-based decision-making in communication intervention. In R. Paul, (Ed)(Ed.), Introduction to Clinical Methods in Communication (2nded.). Baltimore, MD: Paul Brookes.
Gillam, R., Loeb, D. F., Hoffman, L., Bohman, T., Champlin, C.,Thibodeau, L., et al. (In Press). The efficacy of Fast-Forwardlanguage intervention in school-age children with languageimpairment: A randomized controlled trial. Journal of Speech,Language, and Hearing Research.
Hinckley, J. J., & Craig, H. K. (1998). Influence of rate of treat-ment on the naming abilities of adults with chronic aphasia.Aphasiology, 12(11), 989-1006.
Houghton Mifflin. (2007). Earobics [Computer software].Evanston, IL.
Klein, H. B., & Moses, N. (1999). Intervention Planning forChildren with Communication Disorders: A Guide for ClinicalPracticum and Professional Practice (2nd ed.). NeedhamHeights, MA: Allyn & Bacon.
Law, J., Garrett, Z., & Nye, C. (2004). The efficacy of treatmentfor children with developmental speech and languagedelay/disorder: A meta-analysis. Journal of Speech,Language, and Hearing Research, 47(4), 924-943.
Nye, C., Foster, S. H., & Seaman, D. (1987). Effectiveness of lan-guage intervention with the language/learning disabled.Journal of Speech & Hearing Disorders, 52(4), 348-357.
Scientific Learning Corporation. (2007). Fast ForWord[Computer software]. Oakland, CA.
Warren, S. F., Fey, M. E., & Yoder, P. J. (2007). Differential treat-ment intensity research: A missing link to creating optimallyeffective communication interventions. Special Issue:Language and Communication, 13(1), 70-77.

25
1. I’m not even going to guess atwhat your title might mean,so give it to me straight. Whatis the Next Big Thing in audi-ologic counseling?Actually, if you had asked me that
5 years ago, I would have said theNext Big Thing was a growing inter-est in preparing audiology studentsto address our patients’ psychologi-cal and emotional reactions to livingwith hearing problems. As you know,patients have a lot to work throughbefore they successfully use hearingaids, and I don’t mean getting usedto new auditory input. Their chal-lenges are considerable. They mustwork and grapple with: (1) the dis-couraging reality that they have aproblem, (2) the uncomfortable factthat they need to ask for help, (3) thedisappointing news that help comes inthe shape of hearing aids, (4) changesin body image and self-concept of“who I am,” (5) deciding not to worryabout what others think about thesechanges, and (6) calibrating their highhopes (expectations) with the inherentlimitations of hearing aid use. Andthat’s just with adult patients! Thereare also significant others in their livesto consider, and when the patient is achild, the entire family struggles withits own challenges.
2. Wait a minute! Nobody evertrained me to address allthese issues!
You are in the majority. For years,audiology training programs report-ed no concerted effort to prepare stu-dents to interact with these aspects ofpatient care.1,2 Most students knewabout these reactions, passively wit-nessed them, perhaps even docu-mented them. However, they werenot taught any interpersonal or coun-seling skills to provide support topatients as they struggle, to inter-
cede, and to facilitate the adjustmentprocess. Consequently, patients havereported a disconnect between whatthey seek from audiology (personalsupport for the hard work of adjust-ing to a chronic disability) and whataudiology tends to provide (informa-tion and technology).3
3. Sounds a little grim. Anyimprovement on that front?
Yes, I’m happy to say. A recentstudy collected information fromaccredited AuD programs in the USand found that 71% of them requireda course in counseling, while another14% had actively integrated counsel-ing content into existing coursework.4That’s 85% of the programs address-ing counseling training, which is quitea change compared with the 12%-18%rates reported in the days of master’sdegree programs. So, what used to bethe Next Big Thing is actually here:AuD programs are preparing theirstudents as non-professional coun-selors. And my informal observationsindicate that counseling is showingup more and more often in confer-ence programs, suggesting that prac-ticing audiologists are sensing a gapin their training and are eager togrow into counseling as well.
4. When will we know if thisdevelopment of counselingskills is having a positiveeffect on patient care?
As soon as several randomizedcontrolled trials indicate an increasein patient satisfaction and adherenceto audiologic recommendation. Inother words, not any time soon. Fornow we can only extrapolate fromother research. For instance, the med-ical literature is replete with outcomedata indicating that when practition-ers attentively listen to their patients’stories, actively acknowledge theiremotional state, and respect theirabilities to handle their problems(fundamental counseling strategies),patients are more likely to adhere totheir recommendations. 5-8 We hopeto find the same outcomes.
5. Great! It sounds as if we’removing in the right direction.But you still haven’t told mewhat is the current Next BigThing.
Be patient. Remember that I men-tioned literature from the medicalfield, and it is important to note thatmedicine has been putting itselfunder a microscope, examining itsown philosophical foundations withsome pretty big questions, includinghow do we interact with patients, andwhat are the outcomes. The consensusis that the historic “clinical method”(or medical model) of service deliveryis inadequate. It is not a big leap inlogic to consider that if it isn’t ade-quate for medicine, it probably isn’tadequate for audiology, either.
6. What exactly is the clinicalmethod?
Interestingly, it wasn’t until the late1800s that physicians began to treatpatients by making observations,using instruments, and collectingdata, with a tunnel visioned focus onthe pathology. This approach is ana-lytical and impersonal; patients’ reac-tions to the health problem and theirlife experiences are not acknowl-edged. So, for well over 100 years,the clinical (or biomedical) methodwas the only paradigm for patientcare, and it didn’t even have a name.It was just the way things were done9,10 It’s important to remember thebroader historical context. Thisapproach developed during theIndustrial Revolution, and scientistsdeveloped the philosophical constructthat humans are complex machines,requiring a type of service like what amechanic would give to a brokenmachine. Physicians were trained toattend to their patients’ bodies, not totheir “problems of living.”10 Does thatapproach sound familiar? Mightaudiologists also tend to “treat theaudiogram” rather than the patient’sproblems of living?
INVITED ARTICLE - Get ready for the Next BigThing in Audiologic Counseling
Kris EnglishUniversity of Akron

26
7. Are you saying the clinicalmodel is inadequate becauseit views the body as a mechanism?
Exactly. By definition, this model ofcare does not address the humanaspects of disease or disability: emo-tional reactions, life events, relation-ships, environmental challenges. Theclinical method sees disease as an enti-ty located in the body unrelated to thesick person. Research abounds describ-ing how unimpressed patients are withthis approach. And audiology’s adop-tion of this model certainly leaves uswith a problem, since hearing loss can-not be separated from the person.11
8. Have any alternatives beenproposed?
In 1964, Balint proposed a “patient-centered” model of care, and finallythere was a model to compare withthe clinical method.12 He pointed outthat two perspectives are involved ina healthcare encounter: the clinicianinterprets the health problem interms of symptoms and signs, andthe patient interprets it in terms ofexperience (e.g., what it’s like to suf-fer from hearing loss). The exchangeof perceptions between clinician andpatient should result in the develop-ment of mutual understanding, ofcommon ground. In the patient-cen-tered model, clinicians do not seethemselves as detached observersand dispassionate dispensers of ther-apy. Being patient-centered means toattend carefully to those “problemsof living” and provide help to reducethose problems. In audiology, we usethis approach when we relate alltreatment to self-reported patientconcerns, using a selfassessment scalesuch as the Client Oriented Scale ofImprovement (COSI)13 or other self-assessments. The treatment addressesthe problems of living with hearingloss, not the audiogram. Engel laterproposed a “biopsychosocial” model,to help practitioners consider at leastthree domains of human existence(biological, psychological, and social)and focus attention on the integratednature of health problems.14 Bothapproaches view patients not asmachines with broken parts, but ratheras organisms that can grow, heal,learn, and transcend problems. 15
9. Any objections to either ofthese models?
Although the biopsychosocialmodel attempts to focus attention onthe integrated nature of illness, somefeel this model still objectifiespatients as a sum of their parts. Therehave been no criticisms of the patient-centered model to date. But, what hascaught my eye in this literature is thesuggestion to evolve even beyondpatient-centered care, to what is beingcalled “relationship-centered care.” Itseems to suit audiology particularlywell, and that’s what I am referring toas the Next Big Thing.
10. Before you explain why,where did relationship- centered care come from?
In 1992, the Pew Health ProfessionsCommittee and the Fetzer Institute
collaborated to consider patient dis-satisfaction regarding healthcare andto develop an integrated approach tohealthcare. While the biopsychosocialand patient centered models stronglyinfluenced this task force’s thinking,the members felt yet another evolu-tionary step was in order. Afterreviewing the research, they conclud-ed that “for patients, the relationshipwith their provider frequently is themost therapeutic aspect of the health-care encounter” (italics added).15 Thetask force then coined the term “rela-tionshipcentered care” (RCC), whichemphasizes the centrality of thepatient-provider relationship.
11. Why “relationships”?Medicine offers compelling data
indicating that when relationshipsbetween healthcare provider and
“The Next Big Thing.”What will it be? A lot of people think The Next Big Thing will be small— as
in nanotechnology. Could be. Blogging could be The Next Big Thing, thoughit’s pretty big already. If you’re an NPR listener, you know that The Next BigThing is a weekly feature, and you country music fans recognize “Next BigThing” as the title of a CD released a couple of years ago by Vince Gill. Buthow about audiology? Or, more specifically, audiologic counseling? Thismonth’s Page Ten author thinks she knows what The Next Big Thing in this areawill be. Rehabilitative audiology encompasses a wide area. Already this yearon Page Ten we’ve talked about tests that might predict who will be a successfulhearing aid candidate, measures that assist us in prescribing a successful hear-ing aid fitting, digital noise-reduction technology that might help improve listen-ing in noise, and auditory training that might help overall speech understanding.We know, however, that much of this will not be successful without appropriatecounseling. While it is interesting and important to focus on technology, historyhas taught us that our new technology is only as good as the patient’s willing-ness to use it, and his or her understanding of the overall communication prob-lem. When we think of audiologic counseling, we often think of Kris English,PhD, who just happens to be our Page Ten author this month. Dr. English is anassociate professor at the University of Pittsburgh. An internationally recognizedexpert on counseling, she has authored or edited five books and written numer-ous articles and book chapters on the topic, including, you probably recall, aPage Ten article a few years back. She also is having quite an impact on thefuture of audiologic counseling, as nearly 500 residential and distance-learningAuD students have taken her counseling classes. I’m sure you will enjoy readingthis article. You can always count on Kris to help us understand how to under-stand our patients. Perhaps her ability to understand people was influenced byher early career as a pre-school teacher and sign language teacher, or maybe,just maybe, she has inside information on “The Next Big Thing.”
Gus Mueller

27
patient are supportive, caring, per-sonal, and trusting, i.e., central to thecare provided, the patient is morelikely to adhere to recommendations.3,15,17,18 The Pew-Fetzer Task Forceconcluded, “Relationships form thecontent within which people arehelped to maintain their functioningand grow in the face of changes with-in themselves and their environ-ments.”15 We already know this tobe true in audiology. Our colleaguesin private practice know that theirsuccess depends on the relationshipsthey develop with their patients.Pediatric and educational audiolo-gists know that the relationships theydevelop with families have a directimpact on children’s audiologic care.
12. If we already know relation-ships are important, why isthis the Next Big Thing?
RCC gives us a framework todescribe how we function, a name forwhat we instinctively know. Andeven when we “know” this, we maynot “really know” it, you know?
13. Uh… can you try that again?When I talk to audiologists in
counseling workshops, questionsarise about “difficult” patients or“overanxious” parents: “What shouldwe do when a patient is chronicallydissatisfied and drops into the officeexpecting immediate attention everyweek or more?” “Why does this par-ent keep calling me almost daily withquestions about information shefound on the Internet, or about ques-tions I have already answered?” I askthe audiologist to empathize, to try tosee things from the patient’s perspec-tive in order to understand the rea-sons for this person’s distress and theneed to hang on so fearfully. That hasbeen helpful to a point. But lately I’vebeen also asking audiologists, “Howwould you describe your relationshipwith this patient?” Not surprisingly,the answers are along the lines of“contentious,” “tense,” “strained.”Therein lies the heart of the problem.
14. The problem is the relationship?
Yes, or more accurately, the lack oftrust in the relationship. Lutermanreminds us, “In initial stages of a
relationship, where trust is not high,there are usually a great many ques-tions. As the relationship developsand grows, the client becomes morewilling to offer statements and obser-vations. The professional can facili-tate this therapeutic movement bynot always answering questions andsupplying content” (italics added).19
When relationships with patients arestrained or tense, we can safely assumethat they still do not trust us. That’swhy they are still asking so many ques-tions. And, chances are, the questionsasked are not content questions, yet weare giving content answers—a classiccase of communication mismatch.20Here’s an example: The patient asks,“Does everyone struggle with hearingaids the way I am?” The audiologistanswers, “Yes, your brain is rewiringitself with the new input.” This audiol-ogist should simply have asked,“You’re struggling?” This responsefocuses directly on the patient, not onthe apparent question about “every-one” or adjustment. Luterman suggestsnot even answering some questions,but instead finding out why the patientis asking them.
15. If the relationship is notdeveloping, what do we do?
We need to appreciate that only thepractitioner can advance patient rela-tionships. By drawing on our counsel-ing and interpersonal skills, we givepatients reasons to trust us with theirhearing problems. Granted, somepatients’ problems are quite deep-rooted, and in these instances a refer-ral for professional counseling wouldbe in order. Most patients, however,are psychologically healthy; they arejust “stuck” in their adjustment totheir hearing problem, and audiolo-gists can help get them “unstuck.”
16. Then a key word in RCC istrust, right?
Yes, and trust in patient relation-ships is where we might not be“walking the walk.” Audiology hasbeen known to impose the “expert”approach with patients (“follow myrecommendation and you will befine”), but the expert approach doesnothing to develop trust. A goodexample is our classic description ofgroup aural rehabilitation: The audi-
ologist establishes the agenda,decides what will be taught, and thenteaches it, as if patients were audiolo-gy students. An RCC approachwould turn this process on its head:The audiologist would ask the groupof attendees, “What are your ques-tions? What do you want to learn?”The patients then determine the agen-da and decide what they want tolearn, and the audiologist facilitatesthat process.21 This approach impliestrust in patients’ abilities to definetheir problems, determine their goals,and reach those goals. How manyaudiologists are truly comfortablewith this approach? How many audi-ologists are willing to give that con-trol to patients? When I ask about it, Isee fear in audiologists’ eyes! Theyworry that somehow patients willleave the room not learning whataudiologists feel they should havelearned. Not a lot of trust expressedthere. Of course, some patients dosimply want information or technicalhelp, and are not interested in havinga relationship with their audiologistor other healthcare providers. It’s justnot their style or personality. This istheir call; our task is to take care notto misread or overlook any cues oneway or the other.
17. Audiology is practiced in somany settings. Some audiol-ogists have no opportunityto develop relationshipswith patients. What then?
Good point. In medical settings, forinstance, audiologists see a patientonce, conduct the prescribed tests,and advance the patient forward inhis medical care. RCC would notapply to audiology in this circum-stance. The unique contribution ofrelationship-centered care is its threedimensions. We’ve looked at the firstone: the patientaudiologist relation-ship. But the developers of the RCCmodel also recognized the need forrelationships between practitionersand other professionals, and betweenpractitioners and their community.
18. Can you give an example ofan audiologist- professionalrelationship?
One that jumps to mind is the men-tal health field. How many audiolo-

28
gists have working relationships withcounselors, social workers, psycholo-gists, psychiatrists? Not many itseems, based on my informal queries.Yet how many of those professionalsunderstand hearing loss, and how tohelp patients with impaired hearingwhen they seek mental healthcare?Simmons and colleagues wrote avaluable article about the details thatmental healthcare providers need toconsider when their client has a hear-ing loss: the counseling setting (e.g.,lighting and seating distance mayneed to be changed), auditory access,visual attention, patient fatigue, andso on.22 Are the mental healthcareprofessionals in our work settingaware of these concerns? If moreaudiologists develop professionalrelationships with them, they will be.
19. And the audiologist-com-munity relationship?
We fret over the number of personswho do not seek hearing help, but
we usually do not try to reach themexcept through marketing. Marketingdoes not develop relationships. Ifrankly have no great ideas on howto develop relationships betweenaudiologists and their communities,but surely some bright minds outthere can crack this problem, makeaudiology a household word, andhelp patients know they can trust theprofession when they need help witha hearing problem.I encourage everyaudiologist to ask him/herself, “Whatis my relationship with my communi-ty?” If the answer is “non-existent,”“distant,” or “vague,” well, we haveour work cut out for ourselves.
20. Final question: Audiologyhas not exactly receivedrave reviews for beingphilosophical. Why shouldwe start now?
Thanks for making the last questionan easy one. The answer is, because weare becoming a doctoring profession.
As doctors, we have a greater responsi-bility than ever to develop wisdom aswell as techniques, to understand our-selves as well as our patients.Audiologists should be “reflective prac-titioners” who regularly analyze theirpractices, their philosophies, theirunderlying assumptions of care. 23 Inevery profession, the most importantareas of practice actually lie beyond theconventional description of profession-al competence. These areas are wherethe “artistry” of the profession can befound. In audiology, our artistry lies inour ability to connect with patients,develop therapeutic relationships withthem, and help them face their chal-lenges. Given how many patients havenot asked for hearing help, I’d say wehaven’t developed our artistic or philo-sophical sides enough yet. It’s been saidad nauseam that the world’s best hear-ing technology is useless if patientswill not accept it. Patients typically donot get to the acceptance stage bythemselves; relationship centered caremay be a model to help get them there.
1. Crandell C: An update on counseling instruction in audiolgytraining programs. J Acad Rehab Audiol 1997; 30: 1-10.
2. Culpepper B, Mendel L, McCarthy P: Counseling experi-ence and training offered by ESB-accredited programs.Asha 1994;36 (6): 55-58.
3. Glass L, Elliot H: The professionals told me what it was, butthat’s not enough. SHHH J 1992; 13 (1): 26-29.
4. English K, Weist D: Proliferation of AuD programs found toincrease training in counseling. Hear J 2005; 58 (4): 54-58.
5. Squier R: A model of empathic understanding and adher-ence to treatment regimens in practitioner-patient relation-ships. Soc Sci Med 1990; 30: 325-339.
6. Stewart M: Effective physician-patient communication andhealth outcomes: A review. Canad Med Assoc J1995;152:1423-1433.
7. Stewart M, Brown J, Boon H, et al.: Evidence in patient-doctorcommunication. Cancer Prevention Control 1999; 3 (10): 25-30.
8. Wilson B: Promoting compliance: The patient-providerpartnership. Advanced Renal Replacement Therapy 1995; 2(3): 199-206.
9. Smith R: Patient-Centered Interviewing: An Evidence-Based Method, 2nd ed. Philadelphia: Lippincott Williams& Wilkins, 2002.
10. Chimney I: The evolution of clinical method. In Stewart M,Brown J, Freeman T, eds. Patient-Centered Care:Transforming the Clinical Method, 2nd ed. Abington, UK:Radcliffe Medical Press, 2003.
11. Duchan J: Maybe audiology is too attached to the medicalmodel. Sem Hear 2004; 25 (4): 347-354.
12. Balint M: The Doctor, His Patient, and the Illness. New York:International Universities Press, 1964.
13. Dillon H, James A, Ginis J: Client Oriented Scale ofImprovement (COSI) and its relationship to several othermeasures of benefit and satisfaction provided by hearingaids.JAAA 1997; 8: 27-43.
14. Engel G: The need for a new medical model: A challenge forbiomedicine. Science 1977; 196 (4286): 129-136.
15. Tresolini CP: Health Professions Education and Relationship-CenteredCare. San Francisco: Pew-Fetzer Professions Commission, 1994. Atwww.futurehealth.ucsf.edu/pdffiles/RelationshipCentered.pdf.
16. Golin C, DiMatteo M, Gelberg L: The role of patient participa-tion in the doctor visit: Implications for adherence to diabetescontrol. Diabetes Control 1996; 19(10): 1153-1164.
17. House JS, Landis KR, Umberson D: Social relationships andhealth. Science 1988; 241: 540-545.
18. Smith T, Thompson T: The inherent, powerful, therapeuticvalue of a good physicianpatient relationship. Psychosomatics1993; 34: 166-169.
19. Luterman D: Counseling Persons with Communication Disordersand Their Families, 4th ed., 2001. Austin, TX: Pro-Ed.
20. Clark JG, English K: Counseling in Audiologic Practice: HelpingPatients and Families Adjust to Hearing Loss. Boston: Allyn &Bacon, 2004.
21. Brueggeman P, English K: Adult patients are not graduate stu-dents. Presentation at the American Academy of AudiologyConvention, Washington, DC, 2005.
22. Simmons M, Rosenbaum M, Sheridan K: Counseling yourclient with hearing loss. J Mental Health Couns 1996;18(1):80-87.
23. Schön D: The Reflective Practitioner: How Professionals Think inAction. New York: Basic Books, 1983.
REFERENCES

29
AbstractMost of the new professional doc-
torate programs in audiology haveacknowledged the importance of thedevelopment of student’s counselingskills through the establishment ofseparate courses in audiologic coun-seling or the incorporation of coun-seling education within their existingcourse offerings. A recent survey hassuggested that many clinical supervi-sors/preceptors affiliated with Au.D.programs may not be fully preparedto nurture student development inthis area. Yet training in the develop-ment of a trusting relationshipbetween health-care providers andtheir patients is paramount to clinicalsuccess. This article discusses the useof the Audiology Counselor GrowthChecklist as a means to facilitate thedevelopment of positive clinical rela-tionships. Through examination offive distinct areas of clinical interac-tion, supervisors can help studentsincrease their confidence within theclinician-patient dynamic, feel morecomfortable when delivering the badnews of hearing loss, and respond toangry or confrontational patients in amanner which may help move ses-sions in a more positive direction.
Key words: supervision
counseling
patient-centered
Abbreviations: ACGC –Audiology Counselor GrowthChecklist
The University of Cincinnati Bioacoustics LabThe Audiology Counseling Growth Checklist for
John Greer Clark, Ph.D.University of Cincinnati
Learning Objectives:1. The reader will be able to identify at least three areas of patient counseling that
concern students and describe an approach to alleviate student concerns in eachof these areas.
2. The reader will be able to discuss how student clinicians can help put patients atease and increase patient confidence in student-delivered services.
3. The reader will be able to demonstrate to students means of assisting patients toexplore viable treatment options.
Multiple Choice Questions1. Today’s hearing instrument technology
a. provides greater benefit than ever before.b. eliminates the need for tailored counseling for patients.c. may impede student’s development of personalized delivery of care.d. a and c
2. When patients clearly lack motivation to improve hearing, students shoulda. fit them with appropriate amplification under supervised direction with a
refundable adjustment period.b. guide patients through a re-visit of problem areas which were identified
through self-assessment questionnaires.c.provide an opportunity to reflect on their communication difficulties with a
follow-up appointment scheduled in a few months.d. b & c
3. Patients should be made to feel comfortable in the clinical environment. Toattain this goal students should
a. greet patients with a handshake and good eye contact calling patients bytheir first name whenever possible.
b. be seated as soon as the patient and others are seated.c. ensure that they can be heard as well as possible using a personal amplifi-
er as needed.d. all of the abovee. b & c only
4. Students should be encouraged to a. be conscious of the impact their non-verbal behaviors may have on clini-
cal exchanges.b. provide clear and concise explanations of all test findings for all patients. c. make opportunities to demonstrate appropriate use of professional vocabu-
lary thereby increasing patients’ confidence in their skill level.d. avoid silences in clinical discussions which can be both awkward and
suggest less than full competence on the part of the student.
5. When parents or patients become angry or confrontational it most frequently isa. not related to anything the student has done or has failed to do.b. an indication that they are uncomfortable with the student’s lack of experi-
ence.c. a reflection of the emotions they are working through following diagnosis.d. b & ce. a & c
Key: 1 = d 2=d 3=e 4=a 5=e

Through the years audiology hasswung on a pendulum from servicedelivery steeped within rehabilitativepractice to a profession immersedwithin the wonders of a bourgeoningtechnology. The person-centeredpractice of audiology has often takena backseat to the more mechanicaladministration and interpretation ofdiagnostic measures and the electroa-coustics of hearing instrumentation.It is unfortunate that the rapidexpansion in the computerized elec-tronics of corrective amplification,which has afforded sometimes nearmiraculous sound manipulation forthe improvement of hearing, fre-quently serves to stunt students’development of a truly personalizeddelivery approach to the care theyare learning to provide.
Many of today’s audiologists grewup professionally within the techno-logical boon already beginning tosurround diagnostic testing and hear-ing aid fittings. As a result, directtraining and supervision in the per-sonal care/counseling aspects ofservice delivery often were notemphasized, and sometimes ignored.However, time, experience, and thelearning afforded through our ownmistakes have allowed most of us tohone our personal patient counselingskills, much to the benefit of thosewe serve.
While many of the professions’new Au.D. programs are embracingthe importance of counseling skilldevelopment, the supervisors andpreceptors affiliated with these pro-grams may not fully be prepared tonurture skills in this area. Many ofus had a strong past experience withour own clinical supervisors whenwe were in training which nowserves as a guide for our supervisionof developing diagnostic and amplifi-cation skills. What we often lack,because we frequently did notreceive it, is this same type of pastexperience to guide our supervisionof counseling skills.
When surveyed, current audiologystudents are aware of this imbalance,reporting meaningful and construc-tive guidance from their supervisorsin the development of diagnostic and
hearing aid fitting expertise with lit-tle or no mentoring in the develop-ment of strong counseling skills. Thereason for this perception may liedirectly within the history of our pro-fession which led us from our rehabil-itative roots as technology progressed.
What Are Students Looking For?Although clinicians frequently
report they may feel ill-prepared toprovide needed personal adjustmentcounseling to their patients withhearing loss, such counseling haslong been recognized as a vital com-ponent to successful intervention.Student clinicians quickly becomecomfortable in the administration ofroutine diagnostic tests and funda-mental information transfer.However, they correctly recognizethat successful management entailsmuch more than the simple deliveryof information in a clear and concisefashion, free of jargon (English andZoladkiewicz, 1).
To help our students develop com-fort in their clinical interactions andsuccess in their interventions, weneed to provide guidance andinstruction in aspects of service deliv-ery which may bolster patient andfamily trust. The success of the carewhich future audiologists providedepends, as does our own, upon thepositive and interactive relationshipthey develop with those seeking theircare. The Audiology CounselingGrowth Checklist (ACGC) (Clark andEnglish, 2) was designed to fosterpositive patient-practitioner dynam-ics in five specific areas of clinicalinteraction: the manner in which stu-dents greet the patient and open thesession; their clinical demeanor andstyle of information delivery; theirability to affirm the worth of theirpatients; their success in encouragingpatients to share their stories; and themanner in which they help patientsexplore potential solutions to theirhearing difficulties (see appendix).
Greeting and OpeningThe first section of the ACGC rec-
ognizes that the manner in whichpatients are greeted can shape the
way the session will unfold in a vari-ety of ways. While the tone is initial-ly set by front office personnelthrough their telephone manners andthe tone with which patients aregreeted when arriving at the office, itquickly becomes the student audiolo-gist’s responsibility to carry this for-ward. Over the past several decades,American culture has drifted towardinformality within almost all inter-personal exchanges. However, ourpatients, frequently older than our-selves and significantly older thanthe students we are mentoring, mayfind some of the informalities thatseem natural to us somewhat discon-certing within a professional setting.
Those entering our door seekingprofessional care should be greetedby students with an introductionwhich identifies themselves by nameand position as well as the preceptorwith whom they are working.Students may need instruction thaton first meeting, all adult patientsshould be addressed by their title(Mr. Ms. or Mrs.) and their last nameand that this should be continuedunless the patient expressly states adesire to be addressed on a first-name basis. To do otherwise mayseem presumptuous to many of ourelderly patients and only serves todiminish their sense of dignity. Anintroduction such as the following,accompanied by a firm yet gentlehandshake and direct eye contact isalways appropriate: “Hello, Mr.Robinson. I’m Kathy Littleton, an audiolo-gy doctoral student at the university. I’ll beworking with you under Mrs. Albertson’ssupervision today.” Certainly studentsshould be instructed to avoid speakingin “elderese” in which elderly and morefeeble adults are spoken to as if theywere children.
When all parties are within the treat-ment room, the best protocol is for theaudiologist to have a seat as soon asthe patient and others are seated. Thegoal always is to make patients feel atease in the new environment they findthemselves in. Allowing for an eye-to-eye dialogue, rather than toweringover patients while obtaining case his-tory information makes an empathicdelivery possible.
30
Finally, it is often best to ask thepatient why they have sought theconsultation, if they have had a pre-vious hearing evaluation and whatthey hope to gain from the presentevaluation. Answers to these ques-tions permit the student to assess thepatient’s awareness and understandingof the current situation and to see theproblem as the patient perceives it.Certainly the student’s opening ques-tions may follow a brief period ofsmall talk which many believe mayhelp put patients at ease. However,students need to be aware that suchsocial “niceties,” especially if excessive,can be viewed by patients as irrelevantto the real business at hand and mayeven imply that we are not taking theirconcerns seriously.
Demeanor and DeliveryVerbal and nonverbal communica-
tions both play an important role inthe development and maintenance ofa strong professional/patient rela-tionship and students frequentlyrequire feedback to aid in the devel-opment of appropriate communica-tion skills. Students are frequentlyproud of the professional vocabularythey are learning and may feel a needto demonstrate mastery of new termswhen working with patients in frontof their supervisors. Sometimes theuse of professional jargon becomes ahabit as these words become increas-ingly familiar to students and practi-tioners alike. We have all been guiltyof using a word in our clinicalexchanges with patients that oncewas on a vocabulary quiz in an intro-duction to audiology class. Even aterm as simple as “pitch” can createconfusion if a patient interprets it asreferring to how one “pitches theirvoice” (projects their voice).
Students may also need to bereminded to be sure that their voicesare loud enough to be heard, thatthey do not speak too loudly or rap-idly, and that they address thepatient directly whenever possibleusing a personal amplifier as needed.It can be quite disconcerting topatients to be left on the sidelines asmarginal participants while othersdiscuss findings and recommenda-
tions that impact them directly.
It is not enough for audiologistsonly to understand patient’s difficul-ties from their perspective but wemust also continually demonstrateour desire to gain this understanding.Toward this end, our nonverbalresponses are frequently as critical aswhat we say. A variety of nonverbalbehaviors can facilitate or impededialogue and students need frequentfeedback to develop their own vigi-lance of the manner in which theyinteract with patients (Table 1.)
A particularly strong nonverbalresponse that is frequently underused in clinical interactions is silence.Silences are often felt to be uncom-fortable and we are quick to fill in thegap with what is often an ill-timedquestion or remark. When silence isallowed to stand by itself, it permitsa temporal space for reflection aswell as an opportunity for patients toassume some of the responsibility fortheir own progress.
Students who are afforded oppor-tunities to role play their interactionswith patients frequently find theirconcerns of appearing nervous orincompetent begin to diminish.When health care providers, whetherprofessionals or students in training,demonstrate their respect for thepatients they are working with
through their introductions and theirclinical demeanor positive percep-tions of their abilities will naturallyfollow.
When working with parents ofyoung children, students are quick tolearn that the presentation of diagnos-tic information is not a simple deliveryof findings. The astute student clini-cian also realizes the emotional impactof receiving the audiological diagnosisis often present in adult patients, evenif less apparent (Martin, Krall, &O’Neal, 3). Guidelines for breaking thebad news of hearing loss to parents(Clark & English, 2) are also appropri-ate for adults. Key among these guide-lines may be to ensure for a private,unhurried time together; encouragefeelings to be expressed (i.e.: “I knowthis must be very difficult for you.”);respond with empathy and warmth(i.e.: “I’m sorry. I know that’s not the rec-ommendation you were hoping for.”); andarrange for a follow-up appointment.
Not all parents or adult patientsdesire the detailed description of testresults that students have proudlymastered, and when emotions arehigh, research indicates that the abili-ty to process new information is low(Sprenger4). As Martin5 cautions, adetailed disclosure of all we havefound is not appropriate for mostpatients immediately subsequent to
31
Table 1Nonverbal Behaviors to Facilitate Communication*• Achieve eye-level communication to place others at ease
• Come from behind your desk to enhance a more open dialogue
• Maintain good eye contact and an attentive expression to display yourinterest
• Refrain from multitasking behaviors that convey less than full attention
• Allow for silent reflection to encourage expansion of a thought or statement
• Lean forward to display heightened interest and a desire to hear theother’s story
• Use purposeful head nodding to convey agreement and a desire for theother to continue
* From Clark, J.G. & English, K.E. Counseling in Audiologic Practice: Helpingpatients and families adjust to hearing loss. Published by Allyn and Bacon,Boston, MA. Copyright © 2004 by Pearson Education. Reprinted by permissionof the publisher.

the examination. Students need tolearn that this is the time to beginwith a statement such as, “Would youlike an overall summary of the findingsor would you prefer a detailed descrip-tion of these test results.” Allowingsome control over the direction of theappointment often helps parents andadult patients ask the questionsweighing most heavily on theirhearts and minds. Once again, stu-dents learn that it is the manner inwhich they interact with patientswhich will contribute most highly tothe success of clinical relationships.
Patient AffirmationEnglish and Zoladkiewicz1 report
three of the top six concerns audiolo-gy doctoral students have in clinicalinteractions are how to respondwhen the patient or family memberbecomes angry; how to minimizehostility; and how to redirect con-frontation (see Table 2). It is impor-tant for students to understand thatstress and aggravation frequentlyattend the communication failureswhich may accompany hearing lossand that this is not isolated to just theindividual with the hearing problembut also to family members who findthemselves confronting ineffectualcommunication on a daily basis withtheir loved one.
We know that all communicationproblems are not resolved with hear-ing loss treatment and we can antici-pate that frustrations leading to stressand aggravation, while hopefully less-ened with hearing aids, for many willcontinue to some degree. When stu-dents are faced with anger, hostility or aconfrontational demeanor it is easy toview statements and actions as anaffront to their training or level of expe-rience. In reality, the behavior exhibitedis most often an expression of that per-son’s inner stress and has little to dowith the provider of services.
Rather than feeling threatened orchallenged, students need to learnhow to diffuse hostility by showingtheir own respect and understandingfor the other person’s feelings and byhelping that person recognize theuniversality of those feelings.
Sometimes all that is needed is a pos-itive listening posture and anacknowledgement such as, “It mustbe extremely frustrating when you don’thear as well as you feel you should.”The patient affirmation section of theACGC looks specifically at a stu-dents’ ability to demonstrate a desireto understand the feelings whichmay underlie patient statements andto respond to these feelings appropri-ately.
English and Zoladkiewicz alsoreport that not knowing the answerto a patient’s questions is another fre-quently cited concern among stu-dents. Students need to be helped torealize that hearing loss managementis not an exact science and clearanswers are not always available.They must also realize that it is a signof professional strength, not weak-ness, to admit that an answer is notknown, if this admission is coupledwith a clear promise to seek theanswer or to refer to those who mayhave an answer. One aspect ofpatient affirmation is helping patientsperceive the strengths they maybring toward their own treatment.Encouraging questions, even whenstudents fear they may not have theanswer, allows patients to be strongerpartners in their own treatment – aposition that can be both empower-ing and affirming.
Patient EncouragementIn the course of their education and
clinical training, students learn agreat deal of information regardinghearing and balance disorders, and
management strategies. Armed withthis new-found knowledge, studentsare eager to share insights withpatients. While this is entirely appro-priate, they also need to be aware ofa potential problem: when they areviewed as the experts, patients maybecome more dependent. The stu-dent’s goal, of course, is for theirpatients to achieve greater independ-ence and an ability to define andsolve the communication difficultiesthey face. Students may need to bereminded of this. An atmospherethat encourages patients to dialogueas they discover solutions is para-mount to building the trusting rela-tionships that make for successfulhearing loss treatment. Items 18through 23 of the ACGC reflect onhow well students set the stage forpatients and family members toexplore solutions to the communica-tion difficulties they face.
ExplorationPatient encouragement and solu-
tion exploration often go hand-in-hand. Student skill development inone area will frequently facilitatehearing loss management attempts inthe second. When students encour-age patients to talk of the communi-cation difficulties they experience,they can begin to perceive thepatient’s own level of acceptance.The level of motivation that exists totackle the problems encountereddepends on whether the patient hastaken ownership of the problem orwhether a certain level of denial ofpersonal responsibility still persists.
32
Table 2. Primary Student Concerns When Counseling Patients*• The patient becomes angry, hostile.
• Not knowing the answer to the patient’s questions.
• Informing parents that their baby has a hearing loss.
• Appearing nervous or incompetent.
• The patient is confrontational.
• The patient challenges my credentials ("Are you sure you know what youare doing?").
*As reported by English & Zoladkiewicz1.

33
At times patients are reluctant toact on recommendations due to pre-conceptions that lead them to dismissrecommendations before they fullyconsider them. In order to help apatient examine the validity of theactions they are choosing to take, stu-dents need to know how to addressthese preconceptions directly. Apatient who feels he may be viewedas less competent at work if he showsup with hearing aids may be asked toexplore this statement with questionslike, “In what ways do you think yourco-workers will treat you differently ifyou have hearing aids?” “If they dotreat you as you suspect, how would youfeel?” “Have you ever felt that waybefore?” “What did you do?” “Do youthink the potential benefits of hearingaids we have discussed would be worththe test to see if your thoughts (fears) onthis pan out?”
Some of the direct questioning ofpersonal thoughts inherent in a cogni-tive counseling exploration may bebeyond what many students can effec-tively deliver. However, modeling thisexploratory approach for students,with discussion after the patient leavesthe office, can be a valuable instructionin a supervisory setting.
Students also need to recognizethrough their explorations withpatients when it is time to proceedand when the requisite motivationfor success is lacking. When motiva-tion is clearly lacking students mayfind it most beneficial to revisit theself-assessment questionnaire theymay have had the patient complete.The following statement may helpdrive home the need to take action:“Mr. Robinson, you indicated earlier thatyour hearing loss sometimes causes youto feel embarrassed when meeting people
[Hearing Handicap Inventory forAdults] (or that difficulty with yourhearing upsets you at times [Self–Assessment of Communication]; orthat people sometimes avoid you becauseof your hearing loss [Denver Scale ofCommunication Function]; or thatpeople sometimes act annoyed when youdon’t understand what was said[McCarthy-Alpiner Scale of HearingHandicap]; etc.). If you and I couldmake it so that happened less frequently,would that be a good thing.”
A valuable counseling lesson for allaudiology students is recognizingwhen the best present solution is tooffer guidance in building the internalmotivation necessary for success.Rather than proceeding with treat-ment, students need to know when itmight be best to give a patient time toreflect on their hearing loss throughjournaling, a hearing aid diary, atten-dance in a hearing loss support groupor some other avenue. A follow-upappointment some months later maythen prove more fruitful.
When patients do proceed withhearing aid amplification, studentsmust recognize that hearing aids areonly part of the answer and that it istheir responsibility to help patients toexplore tactics for improving commu-nication behaviors and settings. Thefinal items in the ACGC help explorethe students’ effectiveness in this area.
SummaryA large part of the counseling that
students must learn to provide is set-ting the stage for the exploration ofsolutions patients seek. The first sec-tions of the ACGC help supervisorsand students evaluate ways in whichpatients and family members may be
put at ease in the sometimes foreignenvironment presented by a clinicalsetting. Clinical comfort is attainedwhen a trusting relationship evolveswhich is built upon a mutual respect,a reflective and attentive listeningposture, a non-judgmental accept-ance, and a full recognition of theindividual differences we all bring tothe table.
While providing needed direction,we would all be wise to reflect ontwo comments students provided inthe English and Zoladkiewicz study.Students requested that their super-visors step back a bit when studentsare speaking so that students canbegin to form what they already per-ceive as an important bond withpatients. Yet, of even greater impor-tance was a message from one stu-dent pertaining to the critical area ofconstructive criticism: that supervi-sors be careful not to criticize theirstudents directly in front of patients.
Clearly supervisors and preceptorsof audiology students need to pro-vide clear direction and supervisionin patient interaction if students aregoing to master development of posi-tive relationships with their patients.Research has shown that how readilyhealth-care provider recommenda-tions are accepted and implementedoften hinges upon the nature of thisrelationship (Smith & Thompson6)and as such supervision in this areabecomes as important as clinicalguidance in audiological diagnosis.The Audiology Counselor GrowthChecklist may proof useful to super-visors as they strive to incorporate agreater amount of counseling guid-ance for their students.
REFERENCES1. English, K. & Zoladkiewicz, L. (2005). Au.D. Student’s con-
cerns about interacting with patients and families. AudiologyToday, in press.
2. Clark, J.G. & English, K.M. (2004). Counseling in AudiologicPractice: Helping patients and families adjust to hearing loss.Boston: Allyn & Bacon.
3. Martin, F.N., Krall, L., & O’Neal, J. (1989). The diagnosis ofacquired hearing loss. Asha, 31 (11), 47-50.
4. Sprenger, M. (1999). Learning and Memory: The brain in action.Alexandria, VA: Association for Supervision and CurriculumDevelopment.
5. Martin, F.N. (1994). Conveying diagnostic information. In J.G.Clark & F.N. Martin (Eds.), Effective Counseling in Audiology:Perspectives and Practice. Needham Heights, MA: Prentice Hall.
6. Smith, T. & Thompson, T (1993). The inherent, powerful, ther-apeutic value of a good physician-patient relationship. 34:166-169.
34
AppendixAudiology Counseling Growth Checklist (ACGC)
The ACGC may be used as a self-assessment measure for those wishing to increase their awareness of effective audiolo-gist/patient dynamics or as a means to appraise the effectiveness of others whose service delivery approach may serve asa springboard toward growth in counseling. While observing another, or upon reflection of a concluding patient visit thatyou have conducted, simply circle the most appropriate response to the statements presented. All items are worded so thata yes response signifies a positive behavior on the part of the audiologist. The word “patient” refers to the individual seek-ing services during the session whether this is the individual with the hearing loss, or that individual's parent, guardian, orspouse. If you are working with a supervisor, comparison of your self-assessment on the ACGC with that of the supervisorcan be beneficial in developing a constructive dialogue toward growth. Notation of examples of observed behaviors orresponses, or examples of lost opportunities to present a behavior or response, can further discussion and facilitate thedevelopment of counseling skills.
GREETING AND OPENING1. The audiologist introduced him/herself by name (or greeted the
patient if formerly met), with a handshake and direct eye contact.Yes No NA
2. The audiologist seated him/herself at eye level with the patient.Yes No NA
3. The audiologist began with an appropriate opening that invitedthe patient to express his/her immediate concern and activelyacknowledged and addressed this concern.
Yes Example: _______________________________________No Example: _______________________________________NA
DEMEANER AND DELIVERY4. The audiologist maintained eye contact with the patient.Yes Example: _______________________________________No Example: _______________________________________NA
5. The audiologist’s facial expressions were appropriate to the con-text at hand.
Yes Example: _______________________________________No Example: _______________________________________NA
6. The audiologist maintained an attentive yet relaxed posture con-veying a responsiveness of an undivided attention.
Yes Example: _______________________________________No Example: _______________________________________NA
7. The audiologist’s nonverbal expressions were appropriate to thedialogue and not distracting.
Yes Example: _______________________________________No Example: _______________________________________NA
8. The audiologist’s voice was easily heard by the patient and main-tained a tone of interest.
Yes Example: _______________________________________No Example: _______________________________________NA
9. The audiologist spoke at an appropriate rate to enhance under-standing.
Yes Example: _______________________________________No Example: _______________________________________NA
10. The audiologist avoided jargon within his/her comments makingevery effort to ensure that meaning was understood.
Yes Example: _______________________________________No Example: _______________________________________NA
11. The audiologist avoided both verbal statements and nonverbalexpressions that might appear judgmental.
Yes Example: _______________________________________No Example: _______________________________________NA
12. The audiologist seemed aware of potential conflicts betweenhis/her social style and that of the patient.
Yes Example: _______________________________________No Example: _______________________________________NA
PATIENT AFFIRMATION13. The audiologist appeared conscious of multicultural issues that
might influence the dynamics of the interaction.Yes Example: _______________________________________No Example: _______________________________________NA
14. The audiologist employed reflective listening responses to ensurepatient’s meanings were understood correctly and to display a desireto attain that understanding.Yes Example: _______________________________________No Example: _______________________________________NA
15. The audiologist made affirmative statements regarding perceivedpatient strengths.
Yes Example: _______________________________________No Example: _______________________________________NA

35
16. The audiologist seemed aware of and responded to the feelingsunderlying the patient’s statements.
Yes Example: _______________________________________No Example: _______________________________________NA
17. The audiologist used statements that affirmed somethingexpressed by the patient.
Yes Example: _______________________________________No Example: _______________________________________NA
PATIENT ENCOURAGEMENT18. The audiologist avoided closed questions that might elicit simple
yes/no responses.Yes Example: _______________________________________No Example: _______________________________________NA
19. The audiologist made appropriate use of silence to encouragefurther comment from the patient on a current topic beforechanging the direction of discussion.
Yes Example: _______________________________________No Example: _______________________________________NA
20. The audiologist’s nonverbal expressions were encouraging to thecontinuation of dialogue.
Yes Example: _______________________________________No Example: _______________________________________NA
21. The audiologist interjected positive affirmations (yes, mm-mm, etc.)to encourage continuation or expansion of the patient’s comments.
Yes Example: _______________________________________No Example: _______________________________________NA
22. The audiologist encouraged the patient to express his/her feelings.Yes Example: _______________________________________No Example: _______________________________________NA
23. The audiologist avoided signs of defensiveness of expressed feel-ings of anger, frustration, etc., that may have appeared directedat the audiologist.
Yes Example: _______________________________________No Example: _______________________________________NA
EXPLORATION24. The audiologist appropriately challenged statements made by the
patient that might impede the positive actions taken by thepatient and helped him/her to identify more positive views.
Yes Example: _______________________________________No Example: _______________________________________NA
25. If exploring solutions for specific communication breakdowns, theaudiologist asked the patient to identify at least one action thatmight be taken to address the problem.
Yes Example: _______________________________________No Example: _______________________________________NA
26. The audiologist suggested alternative actions that might be useful.Yes Example: _______________________________________No Example: _______________________________________NA
27. The audiologist helped the patient to develop actions that mightfacilitate an identified goal.
Yes Example: _______________________________________No Example: _______________________________________NA
28. The audiologist provided an opportunity to practice identifiedactions.
Yes Example: _______________________________________No Example: _______________________________________NA
29. The audiologist encouraged the patient to critique the effective-ness of actions taken to address the identified goal whenattempted at home, work, or during social activities.
Yes Example: _______________________________________No Example: _______________________________________NA
30. The audiologist recognized when a topic could not be fullyexplored during current time constraints and offered an opportu-nity to return for further exploration.
Yes Example: _______________________________________No Example: _______________________________________NA
From Clark, J.G. & English, K.E. Counseling in Audiologic Practice:Helping patients and families adjust to hearing loss. Published byAllyn and Bacon, Boston, MA. Copyright © 2004 by PearsonEducation. Reprinted by permission of the publisher.

36
This article will introduce one of thenew audiology faculty at the University ofCincinnati, Dr. Peter M. Scheifele, whohas opened the University of CincinnatiBioacoustics Lab and Canine AudiologyClinic.. His collaborators are Dr. MichaelT. Johnson- Marquette University, Speechand Signal Processing Laboratory, Dr.Frank E. Musiek and Dr. Michael J.Darre- University of Connecticut(UCONN), Bioacoustics Lab, Dr. DavidBrowning- University of Rhode Island(URI), Physics Department, and Mr.Robert Michaud, Director of the Groupede Researche et D’Education sur lesMammifers Marins (GREMM), Quebec,Canada. and the entire audiology facultyand clinicians at UC. Co-PI is Dr. DavidBrown. Cincinnati Children’s MedicalCenter, Division of DevelopmentalDisabilities, Director of Audiology. TheLab collaborating veterinarian is Dr.Debbie Kemper DVM
The University of CincinnatiBioacoustics Lab is currently servingthe Georgia Aquarium on two proj-ects. The first regards the exhibitacoustics for the Cold Water Quest(Beluga Whale) exhibit and theOcean Voyager (open-ocean exhibit).We are working with the keepers,trainers and Life Support System(LSS) engineers to ensure that theLSS remains quiet and that theexhibits are audiologically safe andcomfortable for the animals thatreside in them. Dr. Scheifele and aUCONN collaborating student(Kristine Sonstrom, MS) performedthe original pool system acousticmapping before the GeorgiaAquarium opened. In October, 2007,this team with the addition of Ms.Katie Starke and Ms. Sara Tremblay(UCONN) performed an acousticmaintenance and upgrade check onthese two systems since 8 new
pumps and filters were added to theLSS. Our own students: Ms. ShawnMakepeace, Ph.D. student in HearingScience and Ms. Jennifer Dively, andMs. Katie Brinkman , first year AuDstudents are currently engaged in theacoustical analysis of these measure-ments.
We are tasked with an secondacoustic project that merges humanaudiology with animal bioacoustics.The Georgia Aquarium’s OceanBallroom is a beautiful 16,400 squarefoot facility that can host up to 1,100people for dinner. (See Figure 1)Many events including weddings areheld there with dining, music anddancing. The ballroom allows visi-tors to have a direct view into theOcean Voyager and Cold WaterQuest exhibits. The aquarium staff iscommitted to keeping animals safewhile allowing the visitors to enjoythe spectacular view of theseexhibits. Our job is to determinehow much sound enters theseexhibits from the ballroom duringvarious events and to assist theaquarium staff in setting appropriatelimits for sound in the ballroom rela-tive to the two exhibits both for theanimals that inhabit them as well asfor the people attending such events.This requires knowledge of noise,hearing thresholds of humans andeach animal species, hearing in-noise,and signal processing. StudentsKatie Starke (UCONN) and HillaryVargas (URI) are working on aspectsof this second project.
More than Marine MammalsThe lab is also working closely
with the University of CincinnatiInstitutional Animal Care and UseCommittee to obtain approval for aprotocol that will allow us to openour canine audiology clinic.Deafness is not an uncommon prob-lem for dogs. Congenital deafnesshas been reported for approximately
80 breeds, with the list growing at aregular rate so that it can appear inany breed. For the person seeking tobuy or adopt a pet, failing to checkfor deafness can cause unexpectedhardships and may ultimately endthe relationship. Deafness can occurby two processes. Sometimes dogshave congenital or early onset deaf-ness that develops within a monthafter birth. Just as humans, dogs candevelop deafness at any time later inlife. due to the use of ototoxic drugs,noise trauma, ear infections and age-related hearing loss. The current waythat most veterinarians test for deaf-ness is behaviorally, by making aloud noise and then observing thedog’s behavior. There are, of course,inherent weaknesses to this casualexamination. Dropping a large bookmay convince you that the dog actu-ally "heard" a sound. In reality, hemay have felt the vibration of thefloor. Banging pots and pans togethermay also prove futile. A puppy thathas spent its life devoid of soundoften learns to constantly scan forvisual cues. If the puppy perceives asubtle change in ambient light, shad-ows or peripheral movement, as youbang a pot, it may still beat the loudnoise test.
The Canine Audiology Clinic willperform Auditory BrainstemResponse (ABR) testing in conjunc-tion with Otoacoustic Emission tests(OAE). These tests are equally asvaluable with assessing auditory sta-tus in dogs as they are in humans. Itis very important to be able to accu-rately determine if there is a com-plete or partial deafness becausethere is a greater likelihood of deathfrom being hit by cars or otherinjuries from objects coming towardthem. Dogs who cannot hear can bemore prone to injuries, since theycannot hear commands or avoidenvironmental dangers. There arealso behavioral concerns. A deaf dogcan startle easily when asleep and
INVITED ARTICLE - The University of CincinnatiBioacoustics Lab
Peter B. Scheifele Ph.D.University of Cincinnati
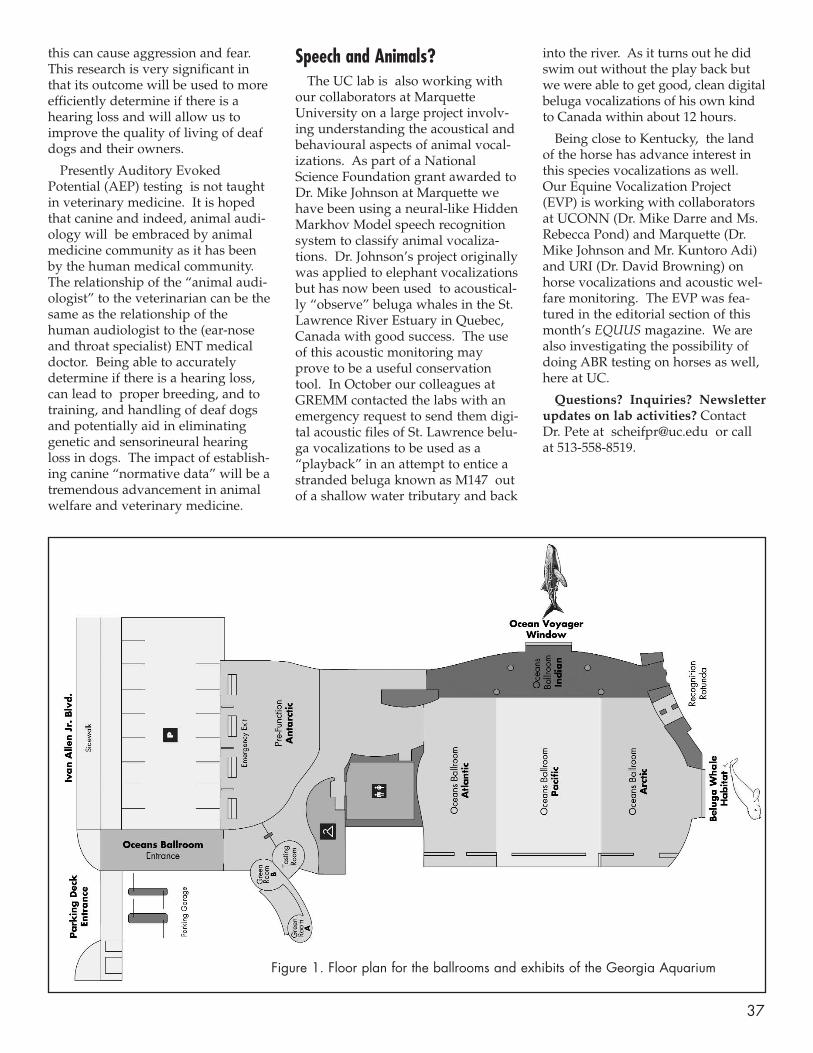
37
this can cause aggression and fear.This research is very significant inthat its outcome will be used to moreefficiently determine if there is ahearing loss and will allow us toimprove the quality of living of deafdogs and their owners.
Presently Auditory EvokedPotential (AEP) testing is not taughtin veterinary medicine. It is hopedthat canine and indeed, animal audi-ology will be embraced by animalmedicine community as it has beenby the human medical community.The relationship of the “animal audi-ologist” to the veterinarian can be thesame as the relationship of thehuman audiologist to the (ear-noseand throat specialist) ENT medicaldoctor. Being able to accuratelydetermine if there is a hearing loss,can lead to proper breeding, and totraining, and handling of deaf dogsand potentially aid in eliminatinggenetic and sensorineural hearingloss in dogs. The impact of establish-ing canine “normative data” will be atremendous advancement in animalwelfare and veterinary medicine.
Speech and Animals?The UC lab is also working with
our collaborators at MarquetteUniversity on a large project involv-ing understanding the acoustical andbehavioural aspects of animal vocal-izations. As part of a NationalScience Foundation grant awarded toDr. Mike Johnson at Marquette wehave been using a neural-like HiddenMarkhov Model speech recognitionsystem to classify animal vocaliza-tions. Dr. Johnson’s project originallywas applied to elephant vocalizationsbut has now been used to acoustical-ly “observe” beluga whales in the St.Lawrence River Estuary in Quebec,Canada with good success. The useof this acoustic monitoring mayprove to be a useful conservationtool. In October our colleagues atGREMM contacted the labs with anemergency request to send them digi-tal acoustic files of St. Lawrence belu-ga vocalizations to be used as a“playback” in an attempt to entice astranded beluga known as M147 outof a shallow water tributary and back
into the river. As it turns out he didswim out without the play back butwe were able to get good, clean digitalbeluga vocalizations of his own kindto Canada within about 12 hours.
Being close to Kentucky, the landof the horse has advance interest inthis species vocalizations as well.Our Equine Vocalization Project(EVP) is working with collaboratorsat UCONN (Dr. Mike Darre and Ms.Rebecca Pond) and Marquette (Dr.Mike Johnson and Mr. Kuntoro Adi)and URI (Dr. David Browning) onhorse vocalizations and acoustic wel-fare monitoring. The EVP was fea-tured in the editorial section of thismonth’s EQUUS magazine. We arealso investigating the possibility ofdoing ABR testing on horses as well,here at UC.
Questions? Inquiries? Newsletterupdates on lab activities? ContactDr. Pete at [email protected] or callat 513-558-8519.
Figure 1. Floor plan for the ballrooms and exhibits of the Georgia Aquarium

38
AbstractCrisis intervention workshops may
be a valuable tool in the education ofspeech-language pathology and audi-ology graduate students. The currentresearch focused on the affects that afour-hour crisis intervention counsel-ing workshop had on 33 first and sec-ond year graduate students’ perceivedknowledge of information about coun-seling and on their perceived confi-dence in their counseling abilities.Participants completed pre- and post-workshop questionnaires to rate theircounseling knowledge and confidence.Significant differences were foundbetween pre- and post-workshopresponses. Results would support theuse of crisis intervention workshops ingraduate education programs.
KEY WORDS: crisis intervention,counseling, speech-language patholo-gy, audiology, graduate students,ASHA-accredited training programs
A communication disorder maycreate a negative impact on the psy-chosocial well-being of affected indi-viduals and their families (Shipley,1997). A person with a communica-tion disorder can be alienated fromher family, her friends, and her cul-ture. Affected persons and their fami-lies may experience feelings of anger,guilt, shame, anxiety, frustration, anddisappointment. Counseling individ-uals with communication disordersand their families is a crucial compo-nent of therapeutic interventions forcommunication disorders.
Counseling Training in GraduateEducation Programs
Preservice speech-language pathol-ogists (SLPs) and audiologists mayask what role they play in effectivelycounseling individuals with commu-nication disorders and their families.The American Speech-Language-Hearing Association (ASHA) hasdeveloped a preferred practice pat-tern regarding counseling. Preferredpractice standard 07.0 states that,
Professionals assist patients/clientsand their families to develop appro-priate goals for recovery from,adjustment to, or prevention of acommunication or related disorderby facilitating change and growth inwhich patients/clients become moreautonomous, more self-directing, andmore responsible for achieving theirpotential and realizing their goals tocommunicate more effectively(ASHA, 1997, p. 23).
Counseling services include assess-ing clients’ counseling needs, provid-ing information on clients’ disorders,modifying clients’ behaviors, modify-ing clients’ environments, developingclients’ coping mechanisms and sys-tems for emotional support, and coor-dinating client and family self-help andsupport groups. Referrals to mentalhealth professionals are an integralpart of the counseling process.Documentation of counseling interven-tions should include background infor-mation, results of counseling, recom-mendations, and referrals.
Despite these professional expecta-tions, many SLPs and audiologists donot feel comfortable attempting tomeet the counseling needs of theirclients (Stone & Olswang, 1989). Thisdiscomfort may be due to the relativelack of educational requirements forcoursework in counseling and lack ofexperience providing counseling dur-ing pre-professional practica. Thecurrent standards of the Council onAcademic Accreditation in Speech-Language Pathology and Audiology(CAA) require that institutions of
higher education provide graduatestudents with knowledge of thenature of the psychological correlatesof communication disorders and dif-ferences (ASHA, 2001). Academicprograms have various options forproviding counseling knowledge tostudents, such as offering courses orworkshops.
Exposure to knowledge is requiredbut skills training and demonstrationof skills is not required. Student clini-cians are permitted to count the timespent counseling clients toward theirrequired 400 clinical training hoursbut counseling experience is notrequired. Professionals who super-vise novice clinicians are required toevaluate the effectiveness of counsel-ing performed by graduate studentsand clinical fellows under theirsupervision (ASHA, 2001).
Because counseling training maybe new to academic programs inspeech-language pathology and audi-ology, it would be useful for academ-ic programs to have potential modelsto consult. For example, Rosenberg(1997) proposed training in informa-tive counseling and personal adjust-ment counseling. Informative coun-seling is when clinicians provideresources to clients. Personal adjust-ment counseling delves into the feel-ings and attitudes associated withcommunication impairments.Rosenberg’s (1997) survey of gradu-ate students revealed that studentswere fairly satisfied with their abilityto provide informative counselingbut wanted further training in per-sonal adjustment counseling.
Crisis Intervention CounselingCrisis intervention counseling is
the specific type of personal adjust-ment counseling that is needed dur-ing temporary periods of upset anddisequilibrium. Individuals experi-ence crisis as a result of a hazardousevent or situation. Crisis is chieflycharacterized by an individual’s inabil-ity to cope with an event by utilizingfamiliar coping strategies (Aguilera,
RESEARCH FORUM - Crisis Intervention Training Effectson Graduate Students’ Counseling Perceptions
Barbara D. WeinrichKimberly A. BeecroftMichael R. HughesMiami University

39
1998; France, 1989; Roberts, 1995).Persons in crisis could experienceideations of suicide, anxiety, depres-sion, frustration, and hopelessness.
Roberts (2000) developed a seven-stage crisis intervention model. Theultimate goal of crisis intervention isfor the individual in crisis to progressfrom maladaptive thinking to a health-ier outlook on the situation. Roberts’stages for this model consist of thecounselor (a) assessing the lethality ofthe situation, (b) establishing rapportwith the individual in crisis, (c) defin-ing the problem, (d) exploring theclient’s feelings and emotions, (e)exploring the client’s past copingmechanisms, (f) exploring the client’salternative coping mechanisms andestablishing a plan, and (g) providingfollow-up after the crisis.
Crisis intervention counseling hastraditionally been performed in men-tal health settings by trained profes-sionals. Various other disciplines uti-lize crisis intervention as a means toassist the individuals in their care.Crisis intervention counseling is car-ried out by health care workers, schoolteachers, and professionals who workwith developmentally delayed indi-viduals and psychiatric patients(Davidson et al., 1995; Eldred, 1995;Nassar-McMillan & Borders, 1999;Taylor, Brady, & Swank 1991; Vinzant,1989). Clients may be children, adoles-cents, or adults (Baronet & Gerber,1997). For professionals in speech-lan-guage pathology and audiology, crisisintervention is a short-term means ofdealing with emotions. SLPs and audi-ologists can be trained to utilize crisis
intervention counseling techniques. Ofcourse, professionals treating commu-nication disorders need to be aware ofwhen to make referrals to mentalhealth professionals for persons withlong-term counseling needs.
The purpose of the current researchwas to examine how a crisis interven-tion counseling workshop affectedspeech-language pathology and audi-ology graduate students’ knowledge ofcounseling techniques and their confi-dence in their abilities to counsel indi-viduals with communication disorders.
MethodsParticipants
Thirty-three graduate studentsenrolled in accredited master’s levelprograms for speech-languagepathology or audiology voluntarilyattended a four-hour workshop oncrisis intervention. Sixteen of the 18first year students (89%) and 10 ofthe15 second year graduate students(67%) had never taken a counselingskills workshop. Four of the first yearstudents (22%) and three of the sec-ond year graduate students (20%)had received crisis intervention train-ing prior to this workshop.
Materials
A crisis intervention counselingskills questionnaire (Appendix A)was administered to participants toexamine participants’ perceptions oftheir (a) knowledge of crisis interven-tion counseling techniques, and (b)their confidence in their abilities tocounsel clients and their families.
Procedures
Participants completed the ques-tionnaire prior to attending a four-hour crisis intervention workshopconducted by Carol Middendorf,DEGREE AND CERTIFICATION,from Columbus, Ohio. Ms./Dr.Middenorf provided informationfrom the professional literature oncrisis intervention and from her ownclinical experiences. Using lecture,discussion, role play, and simulationof scenarios, the workshop leaderdefined the characteristics of crisis,taught the steps of crisis intervention,and described techniques for effec-tive communication. A workshophandout (Appendix B) was providedfor all participants. At the completionof the workshop the crisis interven-tion counseling skills questionnairewas re-administered to participants.
Results
Descriptive statistics were used tocompare differences in group meanscores on the pre- and post-workshopquestionnaires. Statistical significancewas determined using t-tests fordependent samples at an alpha levelof p < 0.01.
To compare participants’ percep-tions of their knowledge about coun-seling, aggregate measures weretaken of questions #10a, 11a, 12a, 13a,and 14a. The difference between pre-and post-workshop responses wassignificant for first year graduate stu-dents (p = .0001), for second yeargraduate students (p = .0001), and forall participants combined (p = .0001)(Table 1).
Total Subjects (N = 33) 1st Year (N = 18) 2ndYear (N = 15)
Pre Mean 2.6303 2.5000 2.7866Pre SD 0.6857 0.5667 0.7980
Post Mean 4.1575 4.0888 4.2400Post SD 0.3192 0.3007 0.3312
Mean Change 1.5273 1.3773 1.4533SD 0.6261 0.4255 0.8158
t 14.01 15.84 6.90p 0.0001 0.0001 0.0001
Table 1: Aggregate Measures of Knowledge

40
Regarding participants’ perceptionsof their confidence in their ability toprovide counseling, aggregate meas-ures were taken of questions #10b,11b, 12b, 13b, 14b. There was a signif-icant increase from pre- to post-work-shop scores for first year graduatestudents (p = .0001), for second yeargraduate students (p = .0001), and forall participants combined (p = .0001)(Table 2).
Conclusions
Similar to the situation describedby Rosenberg (1997), graduate stu-dents who participated in this studywere beginning their professionalcareers without adequate knowledgeabout counseling. The results of thisstudy provide support for the use ofa crisis intervention training work-shop. Interestingly, at pre-workshop,the second year graduate students had
more clinical experience than the firstyear students but they did not reporthaving counseling knowledge andconfidence in their counseling abilities.This might imply that the second yearstudents had not received adequatecounseling training during clinicalpracticum. Therefore, graduate pro-grams may find it necessary to addressthe need for supplemental counselingtraining. A crisis intervention work-shop would be a viable option.
Total Subjects (N = 33) 1st Year (N = 18) 2ndYear (N = 15)
Pre Mean 2.4727 2.3888 2.5733Pre SD 0.6797 0.7275 0.6273
Post Mean 3.8484 3.8000 3.9066Post SD 0.4062 0.3564 0.4651
Mean Difference 1.3758 1.5889 1.3333SD 0.6398 0.4255 0.6335
t 12.35 9.08 8.13p 0.0001 0.0001 0.0001
Table 2: Aggregate Measures of Confidence
REFERENCESAguilera, D. C. (1998). Crisis intervention: Theory and manage-
ment (8th ed.). Beverly Hills, CA: Mosby.American Speech-Language-Hearing Association. (1997b).
Preferred practice patterns for the profession of speech-lan-guage pathology. Rockville, MD: Author.
American Speech-Language-Hearing Association. (2001).Standards and implementation for the certificate of clinicalcompetence in speech-language pathology [On-line].Available: www.asha.org/students/caa_programs/stan-dards.htm
Baronet, A., & Berber, G. (1997). Client satisfaction in a com-munity crisis center. Evaluation and Program Planning,20(4), 443-453.
Davidson, P., Cain, N., Sloane-Reeves, J., Giesow, V.,Quijano, L., Van Heyningen, J., & Shoham, I. (1995).Crisis intervention for community-based individualswith developmental disabilities and behavioral and psy-chiatric disorders. Mental Retardation, 33(1), 21-30.
Eldred, S. M. (1995). The effects of crisis intervention team train-ing on coping skills, anxiety and readiness for incidents ofschool violence. Unpublished doctoral dissertation, UnitedStates International University, Washington, D.C.
France, K. (1989). Crisis intervention: A handbook of immediate per-son-to-person help (2nd ed.). Springfield, IL: Thomas Books.
Nassar-McMillan, S. C. & Borders, L. D. (1999). A workbehavior analysis of volunteers in social service agencies.Journal of Social Service Research, 24(3/4), 39-65.
Roberts, A. R. (Ed.). (1995). Crisis intervention and time-limitedcognitive treatment. Thousand Oaks, CA: Sage Publications.
Roberts, A. R. (Ed.). (2000). Crisis intervention handbook:Assessment, treatment, and research (Rev. ed.). New York:Oxford University Press.
Rosenberg, M. A. (1997). The role of counseling psychology in thefield of communication disorders. Unpublished doctoral dis-sertation, University of Wisconsin-Madison.
Shipley, K. G. (1997). Interviewing and counseling in communica-tion disorders: Principles and procedures (2nd ed.). Boston:Allyn and Bacon.
Stone, J. R., & Olswang, L. B. (1989). The hidden challenge incounseling. Asha, 31, 27-31.
Taylor, R. D., Brady, M. P., & Swank, P. R. (1991). Crisis inter-vention: Longer-term training effects. PsychologicalReports, 68, 513-514.
Vinzant, D. R. (1989). From coma to community reintegration:Crisis intervention and the head injury client. CPI NationalReport, 8(3), 15-17.
ADDITIONAL REFERENCESBehavioral Connections of Wood County, Inc. (1999). The Link
Crisis Consultant Training Manual. Unpublished manual.Dattilio, F. M. & Freeman, A. (1994). Cognitive-behavioral strate-
gies in crisis intervention. New York: The Guliford Press.Luterman, D. M. (1996). Counseling persons with communication
disorders and their families (3rd ed.). Austin, TX: Pro-Ed.Pollin, I., & Baird-Kanaan, S. (1995). Medical crisis counseling:
Short-term therapy for long-term illness. New York: W.W.Norton & Company.
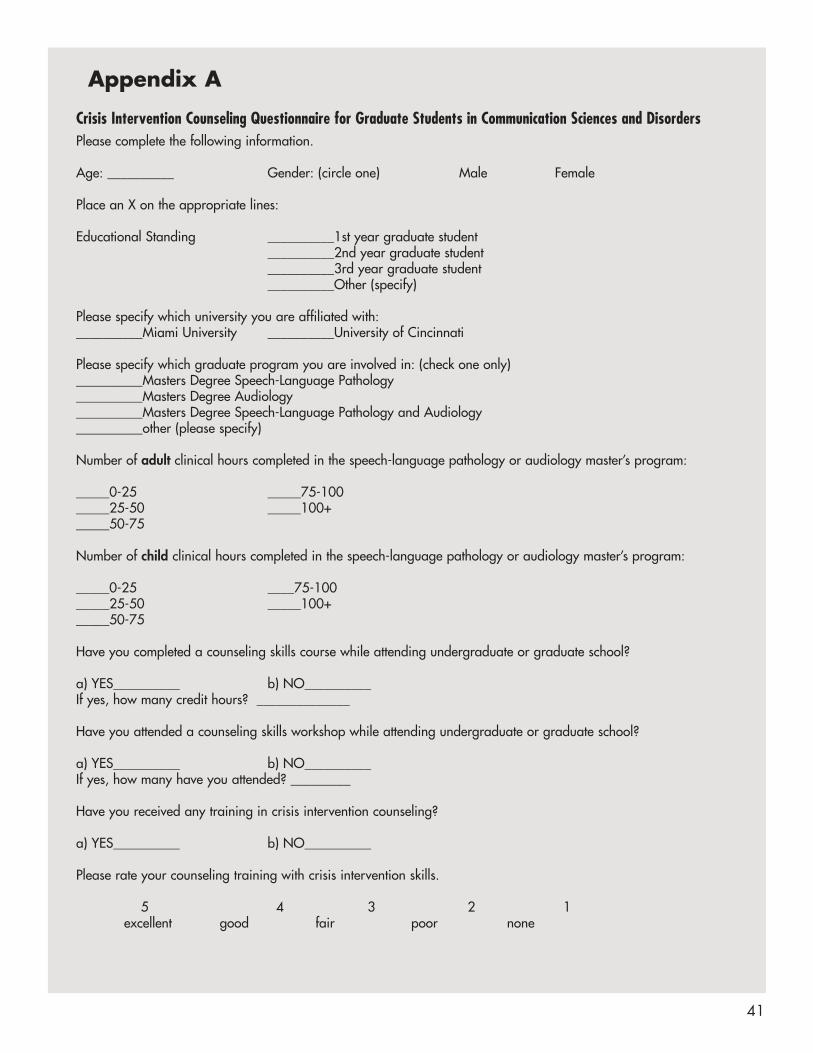
41
Appendix A
Crisis Intervention Counseling Questionnaire for Graduate Students in Communication Sciences and DisordersPlease complete the following information.
Age: __________ Gender: (circle one) Male Female
Place an X on the appropriate lines:
Educational Standing __________1st year graduate student__________2nd year graduate student__________3rd year graduate student__________Other (specify)
Please specify which university you are affiliated with:__________Miami University __________University of Cincinnati
Please specify which graduate program you are involved in: (check one only)__________Masters Degree Speech-Language Pathology__________Masters Degree Audiology__________Masters Degree Speech-Language Pathology and Audiology__________other (please specify)
Number of adult clinical hours completed in the speech-language pathology or audiology master’s program:
_____0-25 _____75-100_____25-50 _____100+_____50-75
Number of child clinical hours completed in the speech-language pathology or audiology master’s program:
_____0-25 ____75-100_____25-50 _____100+_____50-75
Have you completed a counseling skills course while attending undergraduate or graduate school?
a) YES__________ b) NO__________If yes, how many credit hours? ______________
Have you attended a counseling skills workshop while attending undergraduate or graduate school?
a) YES__________ b) NO__________If yes, how many have you attended? _________
Have you received any training in crisis intervention counseling?
a) YES__________ b) NO__________
Please rate your counseling training with crisis intervention skills.
5 4 3 2 1excellent good fair poor none
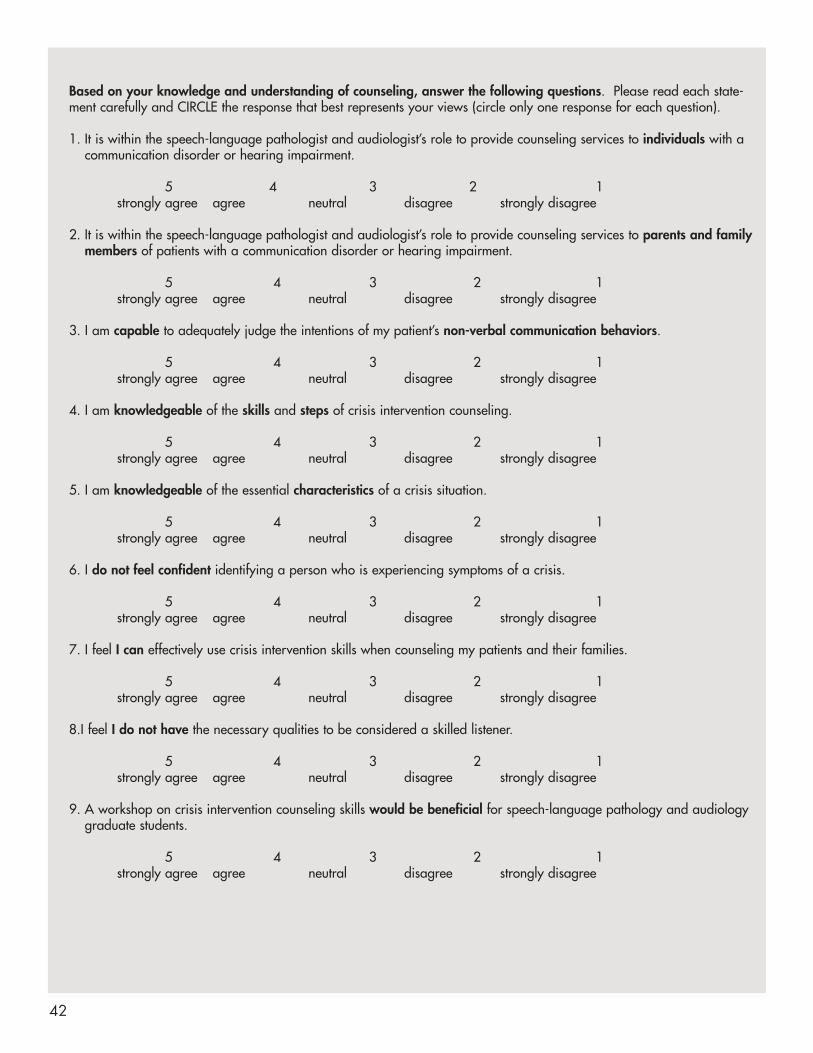
42
Based on your knowledge and understanding of counseling, answer the following questions. Please read each state-ment carefully and CIRCLE the response that best represents your views (circle only one response for each question).
1. It is within the speech-language pathologist and audiologist’s role to provide counseling services to individuals with acommunication disorder or hearing impairment.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
2. It is within the speech-language pathologist and audiologist’s role to provide counseling services to parents and familymembers of patients with a communication disorder or hearing impairment.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
3. I am capable to adequately judge the intentions of my patient’s non-verbal communication behaviors.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
4. I am knowledgeable of the skills and steps of crisis intervention counseling.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
5. I am knowledgeable of the essential characteristics of a crisis situation.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
6. I do not feel confident identifying a person who is experiencing symptoms of a crisis.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
7. I feel I can effectively use crisis intervention skills when counseling my patients and their families.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
8.I feel I do not have the necessary qualities to be considered a skilled listener.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
9. A workshop on crisis intervention counseling skills would be beneficial for speech-language pathology and audiologygraduate students.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree

43
10. During the therapy session a patient becomes upset and agitated due to her/his inability to communicate effectively.a) I feel I have the knowledge to counsel this patient regarding attitudes and feelings about her/his
communication disorder.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
b) I feel confident counseling this patient regarding attitudes and feelings about her/his communication disorder.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
11. A mother has been recently informed that her child has a disability. She has come to you for assessment and treat-ment of her child’s communication problem. She confides in you some of the emotions she is experiencing.
a) I feel I have the knowledge to counsel this patient regarding attitudes and feelings about her/his communication disorder.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
b) I feel confident counseling this patient regarding attitudes and feelings about her/his communication disorder.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
12. Your patient’s husband has become extremely agitated because he is not satisfied with the quality of hospital care hiswife is receiving.
a) I feel I have the knowledge to address this man’s feelings and attitudes about this situation.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
b) I feel confident addressing this man’s feelings and attitudes about this situation.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
13. A patient expresses suicidal ideations. a) I feel I have the knowledge to address a patient’s suicidal ideations.
5 4 3 2 1strongly agree agree neutral disagree strongly disagree
b) I feel confident addressing a patient’s suicidal ideations.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
14. A husband and wife come in for an outpatient therapy session. Throughout the session the wife indicates that she ishaving difficulty dealing with her husband’s communication deficit and that his communication deficit is having a negative impact on their marriage.
a) I feel I have the knowledge to address the attitudes and feelings she is expressing.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
b) I feel confident addressing the attitudes and feelings she is expressing.5 4 3 2 1
strongly agree agree neutral disagree strongly disagree
Comments or Suggestions:

44
Appendix BCrisis Intervention Counseling Skills Workshop for the Pre-ProfessionalSpeech-Language Pathologist and Audiologist
Please Listen!
When I ask you to listen to me, and you start giving advice,You have not done what I have asked.
When I ask you to listen to me, and you begin to tell me why I shouldn’t feel that way, You are trampling on my feelings.
When I ask you to listen to me, and you feel you have to do something to solve my problem,You have failed me, strange as that may seem.
LISTEN!All I asked was that you listen,Not talk or do--just hear me.
Advice is cheap;Twenty-five cents will get you both Dear Abby and Billy Graham in the same newspaper.
And I can do for myself.I’m not helpless.Maybe discouraged and faltering, but not helpless.
When you do something for me, that I can and need to do for myself,You contribute to my fear and inadequacy.
BUT, when you accept, as a simple fact,That I do feel what I feel, no matter how irrational, Then I can quit trying to convince you,And can get about this business of understanding what’s behind this irrational feeling.
And, when that’s clear the answers are obvious, I don’t need advice.Irrational feelings make sense when we understand what’s behind them.
So, please listen, and just hear me.And, if you want to talk,Wait a minute for your turn,And I’ll listen to you.
-Dr. Ray Hought

45
Defining a Crisis and Crisis ConceptsWhat is a Crisis?The term crisis can be defined as a temporary period of upset and disequilibrium, experienced as a result of haz-ardous event or situation, chiefly characterized by an individual’s inability to cope with that event utilizing familiarcoping strategies (Roberts, 1995; Roberts, 2000).
What are the essential characteristics of crisis?
1. Crises are precipitated by an event that is thought to be meaningful or threatening. Ultimately the event is toomuch for the person’s typical problem solving skills.
2. Crises are normal. Everyone has felt overwhelmed at one time or another. Today you may be the one helpingsomeone with his or her crisis, but tomorrow you may be the one reaching out for help.
3. Crises are personal. A situation that is difficult for one individual may not even phase another. It is the individ-ual’s perception and interpretation of the event that is crucial, not the nature of the event.
4. Crises are resolved within a brief period of time.
5. The resolution of the crisis can be adaptive, as reflected by the individual’s use of new problem solving skills ormaladaptive by the person demonstrating continued distress (France, 1990).
How do you know when someone is in crisis?
A person in crisis can exhibit a number of different symptoms (Link, 1999).
Short Attention Span
• Exhibits a fixed span of attention
• Returns to the topic of crisis, despite a person’s attempt to move the conversation forward.
Change in Attachments
• This person is willing to talk to anyone who will listen.
Distress
• Person will indicate they are having a difficult time coping.
Change in Performance
• Person’s normal level of functioning whether it is with work, school, or social life is decreased.
Reduced Decision Making Ability
• Person’s ability to make even the most basic decisions is greatly reduced.
Altered State of Consciousness
• Person puts blinders on. They cannot see what is obvious

46
Crisis Intervention Counseling What is crisis intervention?Through the techniques of crisis intervention, the crisis situation can be reevaluated with the hopes of coming to ahealthy resolution. Therefore the individual can emerge with greater strength, self-confidence, and empowermentover one’s own life (Roberts, 1995). A key factor of crisis intervention is that it is a form of short-term treatment.Several systematic practice models and techniques have been developed for crisis intervention work. The crisis inter-vention model applied for this workshop has been adapted from Roberts’s Seven-Stage Crisis Intervention Model.
Five Basic Steps of Crisis Intervention Counseling
1. Establish a Rapport/Relationship:
• Proceed slowly; allow the patient to set the pace of the conversation.
• Reinforce the patient’s willingness to seek help.
• Provide unconditional support, positive regard, and concern.
2. Define the Problem:
• Define the problem with the patient’s vocabulary.
• Explore the depth and implications of the situation.
• Utilize open-ended questions.
• Focus on now and how rather than then and why.
• Use key questions, “What event led you to seek help at this time?” and “When did this take place?”
3. Explore Feelings and Emotions:
• Participate in active listening: This involves listening in an empathetic and supportive way to the patient’sfeelings of what happened and the precipitating crisis event.
• Accept, acknowledge, and promote hope.
• Reduce anxiety, denial, and blame.
4. Explore and Assess Coping Attempts:
• Bring to the conscious level the patient’s past coping attempts.
• Transition from the problem to a solution.
• Focus on the patient’s strengths, “The patient is an untapped resource!”
• Explore possible solutions that were prematurely rejected.
• Avoid already failed solutions.
5. Explore Alternatives and Develop a Plan
• Collaborate with the patient to generate multiple solutions. (Allow the patient to do this independentlywith you assisting.)
• Explore possible consequences of each solution.
• Explore the patient’s feelings regarding each solution and consequence.
• Have the patient commit to a plan of action.
• Follow up with patient’s response to the crisis event and solution.

47
Basic Skills of CrisisIntervention1. Attending Behavior (Active
Listening)
Five key concepts comprise active lis-tening:
• Eye Contact: If you are talkingwith someone, maintain eye con-tact. Breaking eye contact indicatesto the patient that you are notinterested.
• Attentive Body Language:Everyone establishes his or herown active listening style. Chooseone that you feel comfortable with.
• Patient-Clinician Positioning(Proxemics): Respect your patient’spersonal space.
• Vocal Tone and Rate: Be aware ofyour consistency, pitch and soft-ness. This is a key skill that con-veys to your patient you care abouttheir well-being. Your voice is apowerful instrument.
• Silence: Silence can be powerful. Itallows the patient more opportuni-ty to share. “The silence is a primaryvehicle for responsibility assumption,and it is vital that I do not take thatresponsibility from the clients”(Luterman, 1996, p.102).
2. Questions and MinimalEncouragers
Questions can be categorized intotwo types: open and closed. To bean effective counselor, one mustknow the difference between the two.
• Open questions probe for broadinformation. They allow the per-son to express him or herself with-out any sort of restrictions.Questions should be developed tohelp the patient clarify his or herproblem, rather than provide infor-mation for the clinician. Clientsretain the freedom to select thenature and amount of informationrevealed. “Can you tell me moreabout…?”
• Closed questions specify the pre-cise information needed. Theyrequest a small bit of usually factu-al information in which a simple“yes” or “no” suffices. Closed
questions demonstrate to thepatient a lack of interest in what heor she is feeling. When the clini-cian relies on closed questions tostructure the interaction, he or sheis often consumed with thinking ofnew questions rather than listeningto the client. “Are you…?”
Minimal encouragers are small indi-cators to the patient that you are fol-lowing them. The purpose of thisskill is to encourage the patient tokeep talking. There are two types:non-verbal and verbal.
• Verbal Minimal Encouragers: Briefutterances that indicate to thepatient that you are tuned intothem. Some verbal minimalencouragers are: “Oh?”, “So?”,“Then?” or “And?”, “Tell memore.”, “Umm-hummm.”, repeat-ing key words, restating thepatient’s last statement, andsilence.
• Non-verbal minimal encouragers:Elaboration of the body languagefor attending and active listening.Some non-verbal minimal encour-agers are: making eye contact, leaningforward with interest, head nods, andgestures.
3. Paraphrasing
The purpose of paraphrasing is toclarify complex issues and recognizeimportant emotions. It requires thatthe clinician demonstrate his/herability to give back the informationto the patient. Paraphrasing requiresthe clinician to actively attend,empathize with the patient, and takeon the patient’s point of view. If par-aphrasing is successful the patientwill typically respond with a “Yes!”
An example of paraphrasing is givenbelow.
Patient: “I’m really not involvedwith the autism society. I’m intoother parental organizations.”
Clinician: “The autism society isn’timportant to you.”
Patient: “Right. I used to be a mem-ber but then I found another organi-zation where I felt more useful.”
The key to paraphrasing is to find theessence of what is said, rather thanrepeating the exact statement.
4. Reflection of Feelings
The purpose is to reflect the emotionsthat are underlying the problem. Donot attend solely to content and deci-sion issues. Rather take time tounderstand the patient’s feelings. Aclinician must be very alert andresponsive. For this skill it is notimportant what the patient said, buthow the patient said it. Reflectingfeelings is a skill that is appropriateat any time regardless of the nature.
5. Summarizing
The purpose of summarizing is toorganize complex information andhelp the patient problem solve.When summarizing, the clinicianselectively attends to the patient’sstatement over a period of time andthen re-states for her or him as accu-rately as possible.
This allows the clinician the checkhis/her perception of the conversa-tion with the patient. Summarizingindicates to the patient that youunderstand his/her story.
Summarizing is very similar to reflec-tion of feelings and paraphrasing.Not only are you summarizing con-tent but also emotional feelings.There are specific behaviors to usewhen summarizing.
• Use questions, minimal encour-agers, paraphrasing, and reflectionof feelings to indicate to the clientyou are actively listening.
• Note the patient’s inconsistencieswith their feelings. Many patientsfeel very torn with their emotions.Acknowledging this will allow thepatient to feel someone under-stands what he or she is goingthrough.
• Pay close attention to the mainissues. Summarizing them to thepatient will help him/her make aninformed decision.
• Time your summarizations appro-priately. Allow the patient to finishhis/her thought before jumping in.

48
Nonverbal Communicationand What it Communicates1. Anger:
Speech
• Fast rate and loud intonation
• Short duration of phrases withbrief pausing
Facial Expressions
• Frowning
• Tense neck and facial area
• Chin and head tilted forward
• Wide eyed
2. Anxiety:
Speech
• Fast rate with little silence
• Repetitive
• Change in volume
• Stuttering
• Frequent shift of topic
Body Language
• Grandiose gestures
• Perspiration and flushed appearance
• Frequent fidgeting
• Increased participation in unhealthybehaviors (i.e. drinking and smoking)
3. Grief, Sadness, and Depression:
Speech
• Slow rate
• Frequent pauses
• Frequent sighing
• Crying
Facial Expression
• Flat affect
• Drooped eyes
4. Warmth, Content, and Happiness:
Speech
• Consistent rate, inflection, and intonation
Body Language
• Smiling
• Eye-contact
• Open posture
How To Become a Skilled ListenerListening is the foundation uponwhich communication is built upon.Listening not only creates successfulcommunication, it also provides anavenue for understanding. In orderto become a skilled listener, it isimportant that the following activi-ties take place.
1. Find the Time to Talk. Providingthe person the opportunity toshare their emotions enables thatindividual to become calm andrelaxed, thereby empowering themto cope with his/her disability.
2. Give Your Undivided Attention.Don’t be easily distracted by otherongoing events. Giving your undi-vided attention demonstrates will-ingness to listen and support.
3. Listen Between the Lines. Peopleget caught up in what is beingsaid, rather than how it is beingsaid. Sometimes more informationis communicated through emotion.Active listening means hearing thewords and perceiving the feelingsbehind them.
4. Put Yourself in Their Shoes.People are too quick to condonepatient/family decisions. Take astep back and reexamine. Bydoing this you are showing empa-thy. This demonstrates to thepatient your true interest withhis/her well being.
5. Allow Full Expression ofEmotion. Listen carefully to thepoint of view and emotions beingexpressed. Each situation is indi-vidualized. People differ fromeach other in what they believeand how it affects their life.
6. Evaluate and Process What IsBeing Communicated. Make sureyou understand what is being saidbefore reacting. Utilize the basicskills of crisis intervention.
7. Treat Private Conversations asPrivileged Communication.This allows trust and rapport to bebuilt with your patients.
Ineffective Communicationfor Crisis Intervention1. Advice: “You should not see her
again.”
• The intent of advice is to tell anindividual what to do
• This takes the power of choiceaway from someone
• It decreases the patient’s willing-ness to freely discuss issues
2. Analysis: “You are having troublebecause your expectations are toohigh.”
• The intent of analysis is to explainthe underlying cause of the concern
• Analysis changes the focus fromwhat the patient has to share to theideas the clinician has to give
• Discussion of feelings decline whileintellectual explanation increases
3. Sympathy: “I feel bad for you.”
• The intent of sympathy is todecrease feelings of loneliness,depression, and isolation
• Sympathy shifts the discussionfrom the patient’s feelings to theclinician’s feelings
4. Interrogation: “Why did you dothat?”
• The intent of interrogation is togain information
• Interrogation inhibits the patientfrom talking freely, especially if thepatient is asked questions repeatedly

49
SuicideThe suicide crisis is defined as aprocess where the person loses, overa period of time, the capacity to cope.The inability to cope with unbearablepain is the primary issue of suicide.The suicidal person has the mind setthat his/her problems are chronic. Fora suicidal person, death appears to bethe ultimate solution to the problem.When working with a person who issuicidal it is important to rememberthat suicide cannot be prevented if theperson really wants to die. Whenworking with a person who is suicidalthere are four steps, which can helpassess the lethality of the situation.
1. Identify:
• Look for warning signs. They maybe verbal, “I am going to kill myself”or an indirect statement, “I can’t takeit anymore”. Eight percent of indi-viduals with suicide ideations willexhibit warning signs. These include:
• Hopelessness
• Helplessness
• Depression
• Anxiety
• Inability to cope
• Recent loss
• Change in physical well being
• Difficulty at home with care takers
• Increased alcohol/drug con-sumption
• No life pleasure with activities
2. Clarify:
• Ask the person if he/she is suici-dal. Use the word suicide. Usingthe word suicide will not put theidea in the person’s mind. Explainto the person that you haveobserved warning signs and thatyou are concerned.
• Anything but a firm NO is a YES.
3. Assess:
• Ask the person if he/she has a plan
• Discuss the lethality of the method,availability of the means, and thedetails of the plan
• The more time and energy put intothe implementation of the plan, thehigher the risk.
4. Communicate:
• Discuss what the suicide will solve
• Do not express shock or belittle thecrisis
• Be a reflective listener
• Reassure that he/she has someoneto turn to.
• Provide referral information
Some Good Open-EndedQuestions• How does that make you feel?
• How do you think this treatmentwill turn out?
• How do you feel about what happened?
• How did that affect you?
• How are you going to explain thisto…?
• How does your husband feel aboutthis?
• How do you plan to…?
• What will that mean to you?
• What have you tried in the past?
• What would you like to see happen?
• What do you mean by that?
• What was the significance of thatevent for you?
• What are some other things youcould try?
• What is the worst thing that couldhappen?
• What is important to you?
• When did this happen?
• When do you think is the best timeto deal with this?
• When did you first feel this way?
• When did you first notice your…?
• When can you…?
• Where do you think we can start?
• Where do you see this going?
Some Good Reflection ofFeeling Statements• Perhaps you were feeling…
• It sounds like…
• It seems that…
• Are you saying…?
• It seems to me…
• You appear to be feeling…
• If I’ve understood you, …
• Let me see if I understand whatyou are saying…
• I get the impression you…
• You feel…because…

50
Speech-language pathologists(SLPs) are sometimes obliged toassess and treat “mysterious” cases.Along with the entire medical team,SLPs directly contribute to the med-ical and surgical care of patients. Forexample, in acute care settings neu-rology patients may be admittedwith unknown diagnoses and numer-ous co-morbidities. In these cases theneurological causes of upper aero-digestive tract dysfunction may bedifficult for doctors to identify.Physicians and SLPs sometimes needto discover hidden or occult condi-tions that are not explained by symp-toms and that can be easily over-looked. There are many abnormalitieswhose symptoms mimic or maskanother condition (Hand, Kwan,Lindley, Dennis, & Wardlaw, 2006). Tocompound the mystery, patients eval-uated by SLPs may have impairedcommunication abilities and cannotreport their symptoms or respond toan examiner’s questions regardingsymptoms. Other patients areunaware of their sensory or motorabnormalities. The SLP is sometimesthe first person to observe a sign of apotentially catastrophic disorder.
Case ExamplesThese cases are presented to pro-
voke thought about the importancethe SLP’s neuroscientific knowledgeand to illustrate the practical effec-tiveness of this knowledge in patientcare. The cases are fictional compos-ites of actual clinical cases seen bythe author in community and teach-ing hospitals within a large universi-ty health care system.
Case Example 1
A 72-year-old patient visits his fam-
ily practice physician complaining ofchoking episodes while drinking flu-ids. The physician refers the patientto the speech-language pathologyclinic for consultation. During theclinical examination and interview,the patient admits to numeroussymptoms he had not related to thephysician. The patient admits tocoughing after swallowing, typicallywhen drinking liquids, though a fewoccasions of choking were noted afterhe had eaten particulate solids. Hecomplains of finding masticated rem-nants of food in the left side of hismouth after meals, which he cannotfeel. He has bitten the left side of histongue but did not notice until bleed-ing was observed. The lower left sideof his face is “tingly” and the skinover his left cheek is partially numb.He is edentulous and tends not weardentures and eats soft foods, but hedenies trouble chewing. His left eyefeels “dry all the time.” His tongueand soft palate are symmetrical andhis voice and speech are typical forage and gender.
Videofluoroscopy with repeated tri-als of various conditions reveals 1)every liquid bolus travels to the vallec-ulae before hyolaryngeal elevationbegins; 2) there is laryngeal penetra-tion to the level of the laryngealvestibule with postprandial laryngealresidue; 3) a Penetration AspirationScale score of “3” is obtained whileaspiration is not observed (Rosenbek,Robbins, Roecker, Coyle, & Wood,1996); 4) oral residue is observed. Achin-down posture causes the bolushead to remain anterior to the pharynxuntil hyolaryngeal elevation begins.The SLP trains the patient in the use ofthis compensatory positioning tech-nique and the patient is very happywith the results. But what is the prob-lem causing his abnormal swallow?What further evaluation is necessary?What factors need to be included toarrive at a differential diagnosis?
First, it is true that head postures
often improve swallowing disorderscaused by delayed pharyngeal onset.It is also true that aging changes thetiming of biomechanical and sensori-motor functions (Kim, McCullough,& Asp, 2005). Laryngeal penetrationis a frequent and possibly normalfinding in many older adults, as isslowing of the onset of the pharyn-geal stage in relation to bolus transittoward the pharynx (Gleeson, 1999;Robbins, Coyle, Rosenbek, Roecker,& Wood, 1999). This patient exhibitedage related biomechanical changes. Itis speculative whether his reportedhistory of choking was associatedwith the observed bolus transitevents described above. However,there are also the issues of previouslyunexplained sensory symptoms andundetected motor abnormalities.
It is necessary that the SLP conductadditional neurological examinationof the patient. First, like a neurologistassessing cranial nerve functions, theSLP can test facial sensation using acotton swab to stroke the threeregions of the face repeatedly whileasking the patient whether symmetri-cal sensation is present. The patienttries to discern if one side of the facefeels “stronger” or “weaker”(Murray, 1999; Wilson-Pauwels,Akesson, & Stewart, 2002). Second,the SLP can assess facial motions byobserving facial expressions. Third,mandibular motion is sampled byhaving the patient enact active jawmovements. Dentate patients will beasked to “clamp down” on a tonguedepressor placed between upper andlower molars and to clench theirteeth while the SLP pulls on thetongue depressor. This cannot be per-formed in edentulous patients but itis possible to test the resistance of theelevated mandible by pressingagainst the mandible in the “openposition.” This should not be done inpatients with temporomandibularjoint problems or with prior radiationor surgery to the mandible. Patients
INVITED ARTICLE - Detective Work by the SLP:Two Cases of Undiagnosed Neurological Damage
James L. Coyle, M.A., CCC-SLP, BRS-SUniversity of Pittsburgh

51
can also be asked to hold theirmouths closed against resistanceapplied to the jaw.
The Case 1 patient exhibited asym-metrical mandible elevation. Theright (stronger) side elevated whilethe left did not. The SLP concludedthat the patient exhibited the patternof unilateral motor and sensory dys-function that would be seen in aperipheral injury to the trigeminalnerve. A visit to the hospital library toreview relevant literature helped theSLP prepare a report to the physicianthat suggested some potential differ-ential diagnoses that would coexistwith this pattern of impairment.
The disposition of this case was that,after conferring with the SLP, the refer-ring physician diagnosed the patientwith trigeminal neuralgia and referredthe patient to a neurologist. The neurol-ogist examined the patient and request-ed a thin-slice MRI of the brain andskull base which detected a mass in themiddle cranial fossa compressing thetrigeminal nerve distal to its pontineexit. It was found to be a meningioma.The “choking” was caused by unde-tected postprandial oral remnantsentering the pharynx. The patient wassuccessfully treated before the masscaused irreversible damage.
Patients with oral sensory anesthe-sia (loss of sensation) do not respondnormally to tactile stimuli such asremnants of food or liquids remain-ing in the affected areas of the oralcavity after the swallow. To detectsuch a case, the SLP needs to be surethat the sensory components of theoral-facial examination are not over-looked. In this case the damage to thetrigeminal nerve was discovered bythe SLP. The pathways of the facialand trigeminal nerve are often con-fused. It is the trigeminal nerve thatcarries facial sensation back to thecentral nervous system. All sensoryinformation for the face and oral cav-ity from the soft palate to the lips iscarried through the trigeminal senso-ry nerve fibers. All of the muscles ofmandible elevation and lateralizationand two of the three muscles ofmandible depression (which are alsohyolaryngeal elevators) are suppliedby the trigeminal motor fibers.
Knowledge of the function of the cra-nial nerves and the peripheral nervefields enables the SLP to investigatesensorimotor abnormalities.Familiarity with the effects of injuriesto cranial nerves allows the SLP tobetter diagnose their patients.
Case Example 2
A 68-year-old man exhibited anacute onset of dizziness, nausea andvomiting, weakness in one arm,falling, fever, productive cough, anddiplopia. His spouse called thepatient’s primary care physician whorecommended the paramedics becalled to transport the patient to thelocal hospital. He was admitted to themedical surgical unit with a tentativediagnosis of a possible stroke andgastroenteritis. His usual medicationsand a clear liquid diet were ordered.The patient’s oral medications wereoffered by his nurse. The patientcoughed violently. The nurse askedthe unit secretary to call the speech-language pathology department.
A summary of case informationfrom the medical record is lacking forthis patient. The patient has not beenhospitalized in this institution priorto this admission. The patient’s med-ical record is brand new.
The SLP initiated a neurologicalexamination of the patient. Thepatient is oriented and provides aconcise history of his symptoms. Hestates that he is unable to swallowand the room is spinning, makinghim nauseous. Articulation is precise.The patient displays gurgling phona-tion, diplophonia, and hypernasalresonance. His left eyelid droopsslightly though he can open andclose it; the sclera is red and thepupil is constricted. The eyes seem tobe twitching from side to side andthey do not appear to converge onthe examiner. He is sweating on onlythe right side of his face. The softpalate elevates only on the right side.The tongue protrudes at midline.Sensory testing reveals diminishedtactile detection in all three trigemi-nal fields on the left side of the face,and the patient reports that henotices the absence of taste on the leftside of his left tongue. His elicited
cough is weak without audible sharpglottic closure. He is unable to holdhis breath with his mouth open. Hisright arm is weak and uncoordinat-ed. Palpation during elicited salivaswallowing reveals absent motion ofthe larynx with immediate coughingafter the attempted swallow. At thetime of the examination the patientwas overdue for his embolus controlmedication.
The disposition of this case wasthat the SLP phoned the admittingphysician to discuss the observationsobtained during the clinical examina-tion and interview and to offer somethoughts on possible etiology. Thispatient exhibited signs consistentwith damage to the fields innervatedby cranial nerves V, VII, IX, and X.The SLP had worked with severallateral medullary stroke (LMS)patients over the years. Given thepatient’s fever, productive cough, andneurological signs, the SLP discussedthis possibility with the physician.
An LMS can damage the motornucleus (ambiguus) from which theipsilateral laryngeal and pharyngealmotor supplies emanate, along withassociated interneurons and centers.These lesions are notorious for pro-ducing aphagia (absent swallowing)and vocal fold and ipsilateral pha-ryngeal paralysis in the acute phase(Robbins & Levine, 1993). LMS iscaused by occlusion or hemorrhageof the vertebral or posterior inferiorcerebellar artery. They can produce acluster of other signs including con-tralateral limb weakness and discon-nection of some autonomic (sympa-thetic) reflexes on the side of lesion.Some studies have reported bilateralpharyngeal paresis after unilateralLMS (Aydogdu et al., 2001).
A neurology consult was entered. Itwas agreed that any oral medicationswould be administered intravenous-ly. The neurologist later confirmedthe diagnosis of LMS withWallenberg’s syndrome. MRI of thebrainstem confirmed the causativelesion. Otolaryngology consult con-firmed left vocal fold paralysis. Serialinstrumental evaluations of swallow-ing revealed the absence of upperesophageal sphincter opening with

52
asymptomatic aspiration during theswallow and symptomatic aspirationafter the swallow. The patient’supper esophageal sphincter functionremained unchanged and the patientunderwent placement of a gastrosto-my tube at approximately 16 dayspost onset. In the long term heunderwent thyroplasty to treat theparalyzed vocal fold. After ninemonths of recovery and aggressiveswallowing treatment including seri-al assessment with videofluoroscopy,
he recovered the ability to swallowsafely with compensatory maneu-vers. His gastrostomy tube was sub-sequently removed.
The SLP’s recognition of the speechand non-speech signs of laryngealand pharyngeal denervation facilitat-ed the medical team’s rapid responseand averted a potential disastrousoutcome. The SLP’s understanding ofthe cranial nerve fields contributed tothe team’s preventive care of thispatient.
In summary, the SLP must conductsystematic testing of the patient’s sen-sorimotor status. The SLP understandsany abnormalities observed during theexamination and investigates thepotential causes of the patient’s dys-phagia. The SLP needs to be preparedto identify potentially life-threateningconditions and can be the first temmember to be alert to the need for fur-ther medical assessment of patientswith neurological symptoms.
REFERENCESAydogdu, I., Ertekin, C., Tarlaci, S., Turman, B., Kiylioglu, N.,
& Secil, Y. (2001). Dysphagia in lateral medullary infarction(Wallenberg's syndrome): an acute disconnection syndromein premotor neurons related to swallowing activity? Stroke,32, 2081-2087.
Gleeson, D. C. (1999). Oropharyngeal swallowing and aging: areview. Journal of Communication Disorders, 32, 373-395.
Hand, P. J., Kwan, J., Lindley, R. I., Dennis, M. S., & Wardlaw,J. M. (2006). Distinguishing between stroke and mimic atthe bedside: the brain attack study. Stroke, 37, 769-775.
Kim, Y., McCullough, G. H., & Asp, C. (2005). Temporal meas-urements of pharyngeal swallowing in normal populations.Dysphagia, 20, 290-296.
Murray, J. T. (1999). Manual of Dysphagia Assessment in Adults.San Diego: Singular.
Robbins, J. & Levine, R. (1993). Swallowing after lateralmedullary syndrome plus. Clinics in CommunicationDisorders, 3, 45-55.
Robbins, J. A., Coyle, J. L., Rosenbek, J. C., Roecker, E. B., &Wood, J. L. (1999). Differentiation of normal and abnormalairway protection during swallowing using the penetration-aspiration scale. Dysphagia, 14, 228-232.
Rosenbek, J. C., Robbins, J. A., Roecker, E. B., Coyle, J. L., &Wood, J. L. (1996). A penetration-aspiration scale. Dysphagia,11, 93-98.
Wilson-Pauwels, L., Akesson, E. J., & Stewart, P. A. (2002).Cranial Nerves in Health and Disease. (2nd ed.) London: B.C.Decker.
Join OSHLA and Receive
HEARSAYFree of Charge