Embed Size (px)
Citation preview
Authors: Dr. Nakiwala Stella Regina, Programme Manager
Maale Julius Kayongo, Chief of Party David Muhumza, Monitoring and Evaluation Manager
Jennifer Stockert, Director Date: December 31, 2013
HealthPartners Collaborations Project
Semi-Annual Report July-December 2013 OAA-A-11-00010

Abbreviations and Acronyms
AD
Ankole Diocese Cooperative
AGM Annual General Meeting BCC Behavior Change Communication CDP Cooperative Development Programs CLARITY Cooperative Law and Regulation Initiative Coop Cooperative CRI Criterion Referenced Instruction DHC Diocesan Health Coordinator DHT District Health Team HP HealthPartners HMIS Health Management Information System ID Identification KIUTH Kampala International University Teaching Hospital MAD Mbarara Archdiocese Cooperative MMB Muslim Medical Bureau MOH Ministry of Health MOU Memorandum of Understanding OCDC Overseas Cooperative Development Council PNFP Private not for profit provider PQA Provider Quality Assessment UCBHFA Uganda Community Based Health Financing Association UCCC Uganda Crane Creameries Cooperative UCMB Catholic Medical Bureau UGX Uganda Shillings UHC Uganda Health Cooperative UPMB Uganda Protestant Medical Bureau US United States VHT Village Health Teams VSLA Village Savings and Loan Associations WAD West Ankole Diocese Cooperative WRA Women of Reproductive Age

Table of Contents
Abbreviations and Acronyms .................................................................................................. 2
I. Project Summary .............................................................................................................. 4
II. Development Challenge ................................................................................................... 4
II. Progress Report .............................................................................................................. 11
III. Priorities and Lessons Learned July to December 2013 ................................................... 16
IV. What Works and What Will be Changed ......................................................................... 16
V. Plans for the Next Six Months......................................................................................... 16
Annex A: Map of Health Coops in South Western Uganda .................................................... 18

I. Project Summary
HealthPartners provides resources for capacity building and network development that empower local stakeholders to start and manage health cooperatives in order to benefit through their participation.
HealthPartners development hypothesis is that by building the capacity of rural stakeholders, including health care providers, women of reproductive age and the poor, enabling them to maintain community owned prepaid health coops with linkages to strengthened health systems, local stakeholders can sustain increased access to quality preventive care and treatment with increased accountability and improved health outcomes for the community. II. Development Challenge
Development goals of the Government of Uganda include accelerating economic growth to reduce poverty ensuring that all people have equitable access to the basic package of health care and improving the health status of the people of Uganda. Twenty five percent of Ugandans were living below the poverty line in 2009i and Uganda remains one of the poorest countries ranking 161 on the global Human Development Index. A direct relationship has been demonstrated between poverty and health. Poverty reduces access to health care and catastrophic illness can lead to poverty. Incidence of malaria, dysentery and diarrhea are more prevalent among the poor than the rich ii. Nearly two-thirds of the households in the Central and Western regions of Uganda descended into poverty over the past 25 years as a result of ill health and health related costsiii. The Ministry of Health (MOH) in Uganda has been working to put in place a National Health Insurance Scheme for many years; a national health plan has been drafted but the implementation of this plan and its impact on the rural poor may still be years away. The lack of a comprehensive social security system makes the poor more vulnerable in terms of affordability and choice of health care provider. This situation is compounded for women in Uganda since the rural birth rate is 6.05iv children per woman, women are traditionally primary care takers, culturally women lack power and control to make decisions, and women have less access to capital. The Collaborations project design includes strategic approaches that draw on the significant motivation that coops have to deal with endemic disease threats, increased purchasing power of the group, taking advantage of their potential roles in education and service delivery, and the availability of the resources needed to realize that potential. The Collaborations project was crafted to avoid contributing to dependency by 1) including stakeholders in program design and planning to ensure their priority needs are being
addressed and to build ownership; 2) basing all activities and interventions on sustainable systems including using MOH Health
Management Information System (HMIS) tools and timelines; 3) promoting partnerships based on documented responsibilities with measures of accountability; 4) developing a graduation plan with stakeholders as a measure of success; 5) including the Uganda Health Cooperative (UHC) as a “graduate” from direct development
assistance, now in a position to mentor new coops through the process of orientation, implementation, support supervision and eventually leading to their graduation from external support.

HealthPartners believes that these design, planning and management principles will significantly accelerate progress toward self-reliance while, at the same time, minimizing the possibilities of creating dependency. Collaboration project objectives are: Objective 1: Six coops develop and implement public/ private partnership action plans for improved
health Objective 2: Six health coop boards/ management committees maintain their coop cost balance with
annual provider surpluses and reserve fund Objective 3: Partnership activities with Cooperative Development Partners (CDP) and the MOH result
in adoption of promising practices and lessons Purpose of this Report
HealthPartners documents achievements biannually, and routinely seeks to document and incorporate lessons learned in order to increase impact. The July-December 2013 Semi-annual report includes a progress report, and focuses on priorities and lessons learned, what works and what will be changed, and plans for the next six months.
Progress to-date
An important lesson learned in this project was that time spent orienting leaders of the largest and most influential organizations has much greater impact than working from a bottom up approach where time and money were initially invested in sub-county level orientation. At the recommendation of Daryl Martyris, Uganda Mission, HealthPartners initiated high level partnerships with the Uganda Protestant and Uganda Catholic Medical Bureaus (UPMB and UCMB). UCMB’s top leader, Dr. Sam Orach provided helpful recommendations for adjusting training guides. Dr. Orach requested proof of concept and review of adjusted training tools which will be delivered during a site visit in January 2014. Over 270 faith-based health facilities are owned by Protestant Churches in Uganda. UPMB found the health coop model to be an excellent fit with their health improvement goals and they appreciated HP’s sustainable capacity building approach. UPMB invited HealthPartners to speak at their annual meeting where the theme for the year was “Consolidating Jubilee: Strengthening Partnership for sustainable and accountable Quality Health Care” (Exodus 17: 8-17)". The aim of the meeting was to enable members to identify ways of maintaining and strengthening service delivery within the network. The forum made a resolution and requested HealthPartners to support all of their health facilities in Uganda to offer health coop coverage. The Uganda Mission earlier recommended that HP focus implementation in Southwestern Uganda only. Mission advice is requested to enable HP to respond to UPMB’s request. Current Collaborations project funding for staff and transport is not sufficient to support a country wide network however adjustments may be possible if USAID Washington and USAID Uganda support that way forward. Support from HP has led to the development of four health coops Mbarara archdiocese (MAD) health coop, West Ankole diocese (WAD) health coop and Ankole Diocese (AD) and the Uganda Health Cooperative (UHC.) Two new high level stakeholders, the Northern Ankole Diocese and Kampala International University Teaching Hospital, based on Bushenyi District have requested support to start health coops and are reviewing MOU terms. Discussions with leaders of the Uganda Crane Creameries

Coop (UCCC) who expressed interest to start a health coop have continued but they have yet to request an MOU for support. UCCC requested HealthPartners write a story for their 2013-2014 annual Year Book, outlining the benefits of a health cooperative for dairy farmers. Overall, a total of ten (10) stakeholder workshops were conducted between October 2012 and October 2013 with 383 participants (257 males & 126 females.) Two (2) stakeholder workshops brought coop stakeholders together to discuss what was working and what they want to change going forward. Seven (7) UHC providers conducted a workshop to review their health coop performance in order to develop an action plan to fill gaps. That workshop was attended by 23 participants (12 males, 11 females.) Health care provider staffs for MAD, WAD and AD health coops conducted a workshop with 22 participants (11 males, 11 females.) Two other stakeholders’ meetings were held to review coop performance and plan for each coop’s annual general meeting (AGM.) WAD attendance included 67 participants (36 females, 31 males) and 18 participants (12 females, 6 males) from MAD joined the meeting. Eighteen (18) health care providers who offer coop services developed action plans detailing public/private partnerships to close gaps identified in September 2013. That workshop was attended by 45 participants (23 males and 22 females.) Providers received individual support supervision performance report data to help them identify priorities to address in their action plans. A primary focus this year was on closing gaps so that providers can profit financially from health coop partnerships. During the workshop, in order to overcome the time consuming and expensive process of making coop member photo identification (ID) cards, alternative methods of making ID cards were introduced. Currently one of the ID options involves utilizing a member’s thumb print and identifying physical characteristics and is being piloted in Buhweju district. The New Member ID, as it is called, is significantly less expensive since photo IDs required digital cameras and the capacity to use them, computers, power, and laminators. Additionally, coop members had to all be in the same location at the same time in order to have photos taken. Despite these challenges, photo IDs have become a standard in Southwestern Uganda. Many donor supported organizations make IDs for scheme members. HealthPartners has been researching sustainable options to replace photo IDs for a very long time. The thumb print ID was recommended by the Global Training team from the National Collegiate Inventors and Innovators Alliance. Thumb print IDs are less about the capacity of data entrants to technically read the lines of the print, but rather act as a deterrent for non-members who in the absence of photo IDs often seek care under coverage from health coops. Thumb print ID cards require only paper and ink. The IDs also include characteristics like age, height, hair, complexion, eye size, and identifying marks like scars and moles. Thumb prints are made when members arrive at the facility for care and those prints are compared to the print and characteristics on file (both members and providers keep a copy of each ID.) Lessons learned from the providers who are piloting new IDs will be shared during the next provider workshop. Out of 18 providers oriented on the health coop model, 17 signed MOUs for support from HealthPartners. Seventeen providers offer health care to coop members, while 1 new provider has been trained but has yet to enroll members. In the last year 358 health workers (198 females & 160 males) from 15 health facilities were trained on health coop management. A total of 105 health coop member groups signed MOUs for care with the health care provider of their choice. HealthPartners encourages providers who offer health coop services, to create partnerships with Village Health Team (VHT) volunteers who are trained by the MOH. VHT are tasked with visiting families in their villages to provide accurate information and to encourage uptake of preventive healthy behaviors and early treatment seeking. Partnerships with VHT, can improve provider impact since members who seek care early are

easier and less expensive to treat and they recover faster. Eight (8) Village Health Team (VHT) groups are currently coop members. Fourteen women’s groups were trained to start Village Savings and Loan Associations (VSLA) to improve their ability to save money to join health coops. Out of the 11 VSLA groups that continue savings, 224 women are currently enrolled in health coops. A total of UGX. 19,839,900 ($7,780 US dollars) has been saved to-date by these women, and a total of UGX 16,446,300 ($6,450 US dollars) has been given out in form of loans to coop members. Overall, 13 interactive drama shows have been conducted to promote health coops. Thirty (30) radio talk shows and 485 radio spots were aired to promote health coops. One radio talk show conducted on Radio West with panelists from Kathe Medical Care and Kakoma Health Centre, focused on the social, economic and health benefits of health coops. In addition, testimonies of 9 health coop members and leaders were recorded and edited for airing on radio as recommended by the midterm evaluation report. A total of 807 promotional items were distributed to stakeholders during meetings, workshops, enrolment sessions, and other consultative sessions. Participatory provider quality assessments (PQA) between coop members and service providers were facilitated for 4 providers. PQA scorecards rated Kathe Medical care at 86.5%, Buredo 71.8% and St. Joseph’s at 76.7%. At Comboni Hospital the service users rated the provider at 77%. Equal health care services for all members rated highest with 95%, followed by positive attitude of provider staff towards patients 79%, quality of services was rated at 71% and management of the facility scored 64.5%. Provider staff also filled a scorecard for self-assessment. Together members and provider staff developed action plans based on the lessons they learned during the process. PQAs will be repeated after 6 months to support providers and members to document progress toward the objectives of their joint action plan. Financial performance for providers offering health coop coverage was very low at the beginning of the year. After investigation, it became clear that HealthPartners had failed to emphasize the importance of provider enforcement of a few insurance rules. The insurance rules were detailed in our work plan and a new section of the Health Coop Cascade and Trainers guides is dedicated to this important topic. These rules are so critical to health coop performance that they are again listed below. Prepare fully before launching a new group. Obtain an up-to-date group member premium paid list; Sign MOU with the group; Make IDs for all group members. Why is this important? Without current ID cards or member lists, non-members can charge treatment to the coop. MOUs are important tools to be sure members and providers know what they are entitled to through the coop and know the roles they must fill for the partnership to be successful. There is a critical window of opportunity where new members are eager to seek care. Providers are now being advised to take advantage of that opportunity by ensuring all ID cards, current member lists and signed MOUs are on file before members are invited to start seeking care. Target existing groups and enroll at least 60 percent of all group members to prevent adverse selection. New providers had been sensitizing informal community groups which are harder to manage because they often lack communication and leadership structures. Members must be held accountable to pay premiums on time. Members who fail to pay on time must be required to pay out of pocket until the next premium payment period. Providers who enforce this

rule shall have financial benefits as a result. Why is this important? When members do not have the benefit of coverage, they usually pay on time the next period and thereafter. When groups are allowed to pay late, members often pay only when they need care. As a result, the coop is not sharing risk and provider deficits rapidly increase. Coop members join in groups of four or more. Individuals may join but the premium for one to four people is the same as the total for four people. This rule is important to avoid adverse selection. Individual members are more expensive to enroll, more expensive to track and more expensive to retain. They tend to drop out sooner due a lack of systems for premium collection and sharing positive experiences as a result of membership. Ensuring success for providers at the trial stage has been the primary project focus for the period under review. As a result, providers with surpluses increased significantly from 50% during the January – May reporting period to 70.6% for June – November 2013. Monthly meetings were held where 17 data entrants (8 females & 9 males) attended throughout the review period. Seventeen (17) out of 18 health care providers are turning in monthly coop performance data. The remaining one provider recently enrolled their first coop group; their members are expected to start accessing health care at the beginning of school term in February 2014. Coops, providers, groups, and location detail can be found in Annex A. While many providers began the year with deficits, co-op performance shows that 70.6% (12 out of 17) of the health care providers reported a surplus in 2013. These providers include: BMC, Mitooma, Nyakatsiro, Buredo, St. John’s, Ibanda Mission Health Center, Katungu Mission Hospital, Ruharo, Buhungiro, St. Lucia, St. Mary’s and Rubaare. An average of 62% of UHC members pay premiums on time; while 82.3% of MAD member groups pay premiums on time; 99.4% of AD member groups pay on time and 0% of WAD members pay on time. WAD has such a large risk pool, that enforcing on time payment is not significantly impacting their financial performance however WAD leaders are also being advised about the importance of enforcing insurance rules. Only UHC has opened a reserve fund bank account to date. UHC uses reserve funds to lead their Annual General Meeting (AGM), to conduct an external audit and for quarterly performance review meetings. UHC paid for and led their AGM in January 2013. On November 30, 2013, the UHC reserve fund total was UGX. 2,494,600 ($978 US dollars.) Plans for opening coop reserve fund bank accounts will be introduced at the first AGM for new Coops. AGM planning meetings took place for MAD, AD, and WAD, attended by 130 participants (70 females & 60 males) in November and December 2013. All four coop AGMs are planned for January and February 2014. Training of UHC stakeholders on board governance took place in September and included 3 females and 9 males. The training lasted five days enabling the UHC Board of Directors to develop plans and policies to improve transparent management of their coop in the best interests of their members. By the end of the training, participants: defined governance, defined the health cooperative ownership, reviewed two types of committees, reviewed policy governance concept, developed end result policies, developed an orientation plan for new coop leaders, reviewed and updated cooperative by laws, developed a governing conduct policy, developed an election plan for committee members, developed a cooperative performance monitoring plan, developed a communication plan with the coop members, developed a statement of commitment to the coop members, reviewed and identified characteristics of great board/committee, developed an orientation plan for new coop leaders and completed a post test. The

UHC board appreciated the training lessons and the time provided for them to develop policies and action plans that they intend to implement and share with members at their AGM in January, 2014. HealthPartners is committed to reducing redundancy and coordinating efforts with local stakeholders in each district. HP staffs attend quarterly district coordination meetings and in collaboration with district health officers of Bushenyi, and Mbarara districts, two (2) district health team (DHT) meetings were conducted to review project work plan progress and project tools including the provider support supervision tool. DHT recommendations were incorporated in the support supervision tool. DHT encouraged HP to make sure VHT are included in provider leadership of coop orientation days and recommended production of job aids on health coops to enable the DHT to integrate coop messages in their routine support supervision to health coop providers. Collaborating with DHT through quarterly performance reviews is important because it increases ownership and creates coop advocates that will remain long after the project ends. A total of 20 DHT from Bushenyi and Mbarara attended the 2 meetings that were conducted during the period under review. Uganda Community Based Health Financing Associations (UCBHFA), an umbrella association for community health financing in Uganda was supported to conduct a scheme managers’ meeting which was held on August 30, 2013 at Cielo hotel in Bushenyi district with the theme “Making the sustainability of Community Health Insurance Schemes a reality”. The meeting drew a lot of attention from the managers of schemes because sustainability is considered a major challenge by most health insurance schemes in South Western Uganda. During the meeting, each scheme manager was given an opportunity to share key issues affecting the sustainability of their schemes and the practical strategies that can be undertaken to overcome these factors. Follow up on the action plans that had been developed during the scheme managers meeting in June was done; 70% of the managers had implemented or had plans to implement what they had pledged to do in relation to lessons learned. UCBHFA with support from HealthPartners also conducted two exchange visits for eighteen health financing schemes during the months of July and August 2013. The schemes that participated in exchange visits included: BUREDO Health Center III, Bwindi Hospital e-quality scheme, Kabohwe Clinical Research Center, Ishaka Health Plan, Mitoma Central Clinic, Integrated Community Based Initiative, Nyamwegabira Community Health Scheme (Kabale), Kabale Diocese Community Health Scheme, Kyeibuza Health Centre III, Katunga Mission Hospital, Kibirizi Health Insurance scheme, Kabale diocese health insurance office, Shine Africa Ministries, Munno Mubulwadde Union of schemes, Nyakibale Hospital, Comboni Hospital and Save for Health Uganda. The visits benefited 29 participants (8 female and 21 male.) Scheme managers were able to compare operations to learn from the different management processes. HealthPartners was pleased to welcome new Peace Corps Volunteer, Elmy Wong to the team. Elmy is working on Global Information System mapping for HealthPartners project and is providing cross cutting support to all projects with a wide variety of learning and capacity building objectives. Maale Julius Kayongo, Operations and Finance Manager was promoted to Chief of Party replacing Dr. Wilberforce Owembabazi who moved on to support the Uganda Mission. Dr. Stella Regina was a welcome addition to the team, bringing excellent new strategic thinking and planning strengths to the position of Program Manager. A new accountant joined the team in September. Criterion Referenced Instruction training was held for new team members and Global Communities Uganda based staff in November 2013. HealthPartners leaders visited Kampala in August to provide program progress updates for the Uganda Mission, Ministry of Health, UPMB and UCMB. On September 26, HP’s Chief of Party and Monitoring
and Evaluation (M&E) Manager attended a Health and Nutrition workshop led by USAID to facilitate lesson sharing and provide feedback on work plans. On November 6, HealthPartners Chief of Party, Maale Julius Kayongo attended a USAID Implementing Partners’ meeting focused on improving security systems within each organization. Strategies for enhancing collaboration to avoid duplication of efforts were also discussed. Mission staff shared policies on zero tolerance to corruption, waste and abuse especially regarding use of project vehicles; requirements for taxation reporting for USAID refunds and they emphasized involvement of youth in project cycle management. HealthPartners had identified corruption as an area for review in early 2013 and policies were already in place that support Mission recommendations. In response to recommendations to increase engagement and impact with youth, HealthPartners accepted a student intern who will work with the project team from January through March 2014. If this is successful, additional internship opportunities will be provided in the future. HealthPartners is also looking for ways to target youth with coop and leadership messages and activities. In December, 2013 Dr. Nakiwala Stella Regina the Collaborations project Program Manager attended a USAID Uganda meeting on branding. The meeting covered basic video production skills, branding with US government initiatives, photo consent issues, policy regarding journalists, USAID media guidelines, and USAID Uganda event checklists. HealthPartners Senior Vice President Scott Aebischer, together with Paul Walters, Mama Coop Program Manager visited in October 2013 to observe progress and impact to-date. As a result of this visit, recommendations were made to increased visibility of all coops by strategically adjusting use of logos and branded materials. At AGM planning meetings, new coops began to design their own logos which will be shared for member vote at AGMs in January and February 2014. Coop logos were removed from the HP promotional plan for 2014. Instead, brochures and posters include space for each coop to add their logo stamp. New providers were encouraged to transition to new coop member ID cards. Communication of innovation was emphasized through identifying advocates that will be invited to participate in radio shows, coop orientation days and to join coop meetings to share testimonies. Through linkages by US Mission representative Daryl Martyrs, stakeholders including M-cash, World Vision, and Opportunity Bank Mbarara branch picked interest in learning more about the health coop model. Opportunity bank identified three of their borrower groups and HealthPartners staff linked these groups to nearest health care providers for coop enrollment. HealthPartners will invite Opportunity bank to attend the UHC AGM scheduled in January so they can share their services and products. HealthPartners continues to work with and support Overseas Cooperative Development Council (OCDC) activities. HealthPartners staffs serve on the OCDC Board of Directors, Policy Committee and the Impact Working Group. Staffs attend quarterly working group meetings and participate in conference calls once a month. Three of the four quarterly meetings are typically held at OCDC member offices in the Washington, DC area while one out of the four meetings is held in the Midwest. During meetings, OCDC members report on progress from their CDP projects and share lessons learned. Impact and Cooperative Law and Regulation Initiative (CLARITY) projects are also reported and worked on. Currently, the Impact working group is utilizing the services of consultant Keith Taylor to gather and analyze cooperative data from OCDC members. Mr. Taylor is also in the process of finalizing a standardized data collection tool that can be used by all OCDC members to measure a cooperative, or pre-cooperative (if possible) performance. The data collection tool is focusing on Financial Performance

but is also exploring modules for: Societal Indicators; Member Governance and Executive Governance. Mr. Taylor worked with OCDC CDOs to complete IMPACT Milestones: 23, 24, 27, and 29v. The CLARITY project finalized a manual for cooperatives in developing countries to better advocate for the cooperative model and supportive cooperative legal frameworks in their countries. The manual is titled: Cooperative Advocacy: A Practical Guide for Advocating Cooperative Legal and Regulatory Reform and was presented at a workshop in South Africa. A consultant worked with the OCDC CDOs to complete CLARITY Milestones 10, 11, 14, 17, 25 and 26vi. OCDC facilitated collaborative meetings where both IMPACT and CLARITY projects were reviewed and supported. In person collaboration meetings occurred on July 29 – 30 (in Washington, DC) and October 17 – 18 (in Minneapolis, MN). Monthly conference calls among all CDOs to discuss IMPACT and CLARITY projects were held on: July 16; August 20; September 17; October 15; December 3; and December 17. II. Progress Report
The table below summarizes achievements between June 2013 and November 2013 compared to FY14 Work Plan targets and End of Project goals.
Objective/ Activity End of Project Goals FY14 goals Achievements June-December 2013
O1: Six coops develop and implement public/ private partnership action plans for improved health
1.1. Orientation of institutional heads on HealthPartners coop model
1.1: 6 Coop stakeholders develop and implement action plans for public/private partnerships to improve health
4 Coop stakeholders develop and implement action plans for public/private partnerships to improve health
Eighteen health care providers from 4 health coops developed action plans detailing public/private partnerships to close gaps identified in September 2013.
1.2: On-site training of service provider staffs
1.1.2: 21 coop providers who signed MOUs with member groups
12 coop providers who signed MOUs with member groups
18 providers have current coop health partnership MOUs with a total of 105 member groups
1.3. Conduct integrated provider support supervisions
1.1 6 health coops can sustainably manage partnerships for access to quality health care with consistent provider revenue
4 health coops can manage partnerships for access to quality health care with consistent provider revenue
18 providers developed action plans detailing public/private partnerships to close gaps identified for financial profitability; workshops were attended by 45 participants (23 males & 22 females)
1.4. Conduct interactive drama shows in strategic locations to promote health financing using HealthPartners cooperative model
1.2 52 Interactive drama shows conducted with support from CDP to encourage community
1 Interactive drama show conducted to encourage joining Health Coops
Bwera drama group conducted 1 interactive drama show at Butanda in Ihunga sub county, Ntungamo district during community sensitization by St. Lucia Kagamba Health Centre.

Objective/ Activity End of Project Goals FY14 goals Achievements June-December 2013
members join Health Coops
1.5. Air radio spots and talk shows to promote health financing using HealthPartners cooperative model
1.3 and 1.4 52 approved radio talk shows and 624 radio jingles/spots aired to promote community health financing.
Radio talk shows, recorded segments and 576 radio spots aired to promote community health financing.
Thirty (30) radio talk shows and 485 radio spots were aired to promote health coops.
1.6. Print and distribute BCC materials to the community to promote community Health Financing.
1.5 16,030 materials distributed to support VHT to help people join health cooperatives
Brochures, posters, billboards, t-shirts, calendars, umbrellas, newsletters distributed to promote community Health Financing.
807 promotional items including t-shirts, newsletters, posters and brochures were distributed.
1.7. Provision of health coop startup kits to providers to support providers to start and launch new member groups
1.1.2 18 coop providers sign MOUs with member groups
12 coop providers sign MOUs with member groups
18 providers have current coop health partnership MOUs with a total of 105 member groups.
1.8. Conduct provider quality assessments and share results
1.1.3 90% of providers have improved ratings on their member quality assessment scores 1.1.4: 90% of staff in health facilities working on the day of the serve 1.1.5: 100% of coop health facilities with first line medication 1.1.6: 100% of health facilities with guidelines for care of children and adults 2.1: Provider surplus
70% of providers have improved ratings on their member quality assessment scores 70% of staff in health facilities working on the day of the survey 90% of health facilities with guidelines for care of children and adults Provider surplus averages at least
1.1.3 PQA scorecards rated Kathe Medical care at 86.5%, Buredo 71.8%, St. Joseph’s at 76.7% and Comboni 77%. 1.1.4 72.3% of staff in health facilities were found working on the day of the serve 1.1.5 95.4% of coop health facilities were found with first line medication on the day of the survey. 1.1.6 94% of health facilities were found with clinical guidelines for care of children and adults 2.1 Provider surplus for the 4 coops are stated below: Uganda Health Co-op: UGX.0 Ankole Health Co-op: UGX.1,288,533 West Ankole Diocese: UGX.50,260,025 Mbarara Archdiocese: UGX.0 2.2 UHC reserve fund bank account total was UGX. 2,494,600 ($978 US dollars) Nov. 30, 2013.
1.9. Conduct quarterly meetings with service providers to share support supervision results, Cooperative performance summary, and mapping tool
1.10 Conduct premium recalculation for health providers

Objective/ Activity End of Project Goals FY14 goals Achievements June-December 2013
averages at least 500,000 2.2 Total annual coop reserve balance of at least 3,000,000 2.3: 80% of health care providers with annual surplus 2.4: 80% of coop members pay premiums on time 2.1.2: 100% of health facilities maintain up to date records on sick clients
300,000 Total annual coop reserve balance of at least 500,000 45% of health care providers with annual surplus 45% of coop members pay premiums on time 85% of health facilities maintain up to date records on sick clients
2.3 providers with surpluses increased from 50% during the January – May reporting period to 70.6% for June – November 2013. 2.4 An average of 62% of UHC members pay premiums on time; while 82.3% of MAD member groups pay premiums on time; 99.4% of AD member groups pay on time and 0% of WAD members pay on time. 2.1.2 100 % of health facilities maintain up to date records on sick clients
1.11: Health care providers conduct quarterly cooperative orientation days to increase scheme enrolment
85,000 people covered by US supported health financing arrangements
33,000 people covered by US supported health financing arrangements
30,448 people are covered by US supported health financing arrangements
1.12: Provider enrollment of new member group
42 MOUs signed annually between coops and local health stakeholders
24 MOUs signed annually between coops and local health stakeholders
18 providers have current coop health partnership MOUs with a total of 105 member groups
1.13: Biannual meetings between providers and group members to deliver health education, review scheme performance and close health coop gaps identified
42 MOUs signed annually between coops and local health stakeholders
24 MOUs signed annually between coops and local health stakeholders
18 providers have current coop health partnership MOUs with a total of 105 member groups
O2: Six health coop boards/ management committees maintain their coop cost balance with annual provider surpluses and reserve fund
2.1. Ensure coop stakeholders are a success by facilitating coop stakeholders conduct support supervision of service providers
Provider surplus averages 500,000 or more per co-op
Provider surplus averages 300,000 or more per coop
Uganda Health Co-op: UGX.0 Ankole Health Co-op: UGX.1,288,533 West Ankole Diocese: UGX.50,260,025 Mbarara Archdiocese: UGX.0
2.2. Conduct monthly Total coop reserve Coop stakeholders
Objective/ Activity End of Project Goals FY14 goals Achievements June-December 2013
meetings with data entrants to strengthen their capacity in data management
fund balance is 3,000,000 or more 100% of providers turn in coop tracking tools on time
open reserve fund bank accounts 85% of providers turn in coop tracking tools on time
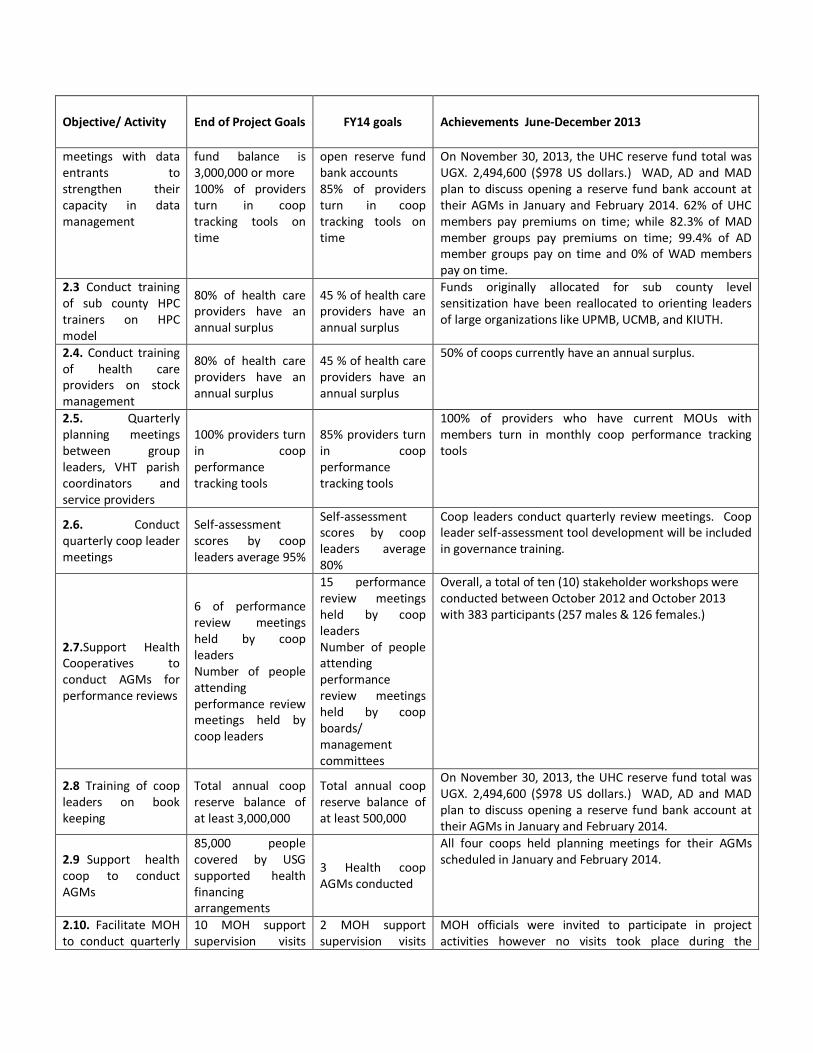
On November 30, 2013, the UHC reserve fund total was UGX. 2,494,600 ($978 US dollars.) WAD, AD and MAD plan to discuss opening a reserve fund bank account at their AGMs in January and February 2014. 62% of UHC members pay premiums on time; while 82.3% of MAD member groups pay premiums on time; 99.4% of AD member groups pay on time and 0% of WAD members pay on time.
2.3 Conduct training of sub county HPC trainers on HPC model
80% of health care providers have an annual surplus
45 % of health care providers have an annual surplus
Funds originally allocated for sub county level sensitization have been reallocated to orienting leaders of large organizations like UPMB, UCMB, and KIUTH.
2.4. Conduct training of health care providers on stock management
80% of health care providers have an annual surplus
45 % of health care providers have an annual surplus
50% of coops currently have an annual surplus.
2.5. Quarterly planning meetings between group leaders, VHT parish coordinators and service providers
100% providers turn in coop performance tracking tools
85% providers turn in coop performance tracking tools
100% of providers who have current MOUs with members turn in monthly coop performance tracking tools
2.6. Conduct quarterly coop leader meetings
Self-assessment scores by coop leaders average 95%
Self-assessment scores by coop leaders average 80%
Coop leaders conduct quarterly review meetings. Coop leader self-assessment tool development will be included in governance training.
2.7.Support Health Cooperatives to conduct AGMs for performance reviews
6 of performance review meetings held by coop leaders Number of people attending performance review meetings held by coop leaders
15 performance review meetings held by coop leaders Number of people attending performance review meetings held by coop boards/ management committees
Overall, a total of ten (10) stakeholder workshops were conducted between October 2012 and October 2013 with 383 participants (257 males & 126 females.)
2.8 Training of coop leaders on book keeping
Total annual coop reserve balance of at least 3,000,000
Total annual coop reserve balance of at least 500,000
On November 30, 2013, the UHC reserve fund total was UGX. 2,494,600 ($978 US dollars.) WAD, AD and MAD plan to discuss opening a reserve fund bank account at their AGMs in January and February 2014.
2.9 Support health coop to conduct AGMs
85,000 people covered by USG supported health financing arrangements
3 Health coop AGMs conducted
All four coops held planning meetings for their AGMs scheduled in January and February 2014.
2.10. Facilitate MOH to conduct quarterly
10 MOH support supervision visits
2 MOH support supervision visits
MOH officials were invited to participate in project activities however no visits took place during the

Objective/ Activity End of Project Goals FY14 goals Achievements June-December 2013
support supervision visits to health coops
conducted conducted
reporting period.
2.11. Conduct quarterly review meetings with WRA VSLA trainers to review VSLA performance
30,000 cooperative members are WRA
6 VSLA groups join health coops
A total of UGX. 19,839,900 has been saved to-date by the 11 WRA VSLAs, and a total of UGX 16,446,300 has been given out in form of loans to coop members.
2.12 Conduct advocacy to Regional stakeholders
85,000 people covered by USG supported health financing arrangements 30,000 cooperative members are WRA
2 new health cooperatives started
Leaders of North Ankole Dioceses and KIUTH are in the process of signing MOUs for cooperative development support from HealthPartners so they can launch their health coops.
O3: CDP partner collaborations outputs on lessons learned in co-op health financing shared with MOH and partners
3.1. Conduct quarterly meetings with DHTs to share progress on health coop performance and integrate their recommendations
1 85,000 people covered by USG supported health financing arrangements 2 30,000 cooperative members are WRA
4 exchange visits by coop groups 1 national stakeholder workshop 4 exchange visits
by coop groups
1 action research conducted with coop 2 Technical support to coop 1 regional stakeholder workshop
In collaboration with UCBHFA, stakeholders in SW Uganda were supported to conduct three exchange visit visits attended by 29 participants (8 Female and 21 male) in Kabale diocese, Luweero schemes to Bwindi eQuality health scheme in Kabaale.
3.2. Support UCBHFA to organize a national forum
An MOU for HP partnership with UCBHFA in FY14 is currently being negotiated.
3.3. Conduct regional scheme managers meeting to share coop and other health financing experiences
A regional scheme manager meeting was held in June led by UCBHFA with support from HP. Thirty participants from 22 organizations attended.

III. Priorities and Lessons Learned July to December 2013
Principles from communication of innovation have been helpful. Linking champions of one
organization to share impact with others created opportunities for more partnerships. Diocesan Health Coordinator (DHC) for Ankole Health Cooperative shared experiences with DHC for North Ankole Diocese who is now working with HP to start a NAD health coop. Ensuring success for providers at the trial stage is a major focus of the project and led to realization that insurance rules were not being trained or followed.
Implementation of coop insurance rules by providers increased membership and amount of premium turned in by groups. Provider profits are increasing.
Use of collaborative approach at all stages of implementing project through drafting and negotiating MOUs between various stakeholders continues to build ownership and accountability between partners and stakeholders.
Advocacy at the National level enhanced awareness and interest for cooperative health insurance among national partners. UPMB made a resolution to implement health coops and Uganda Episcopal Conference made a directive to Uganda Catholic Dioceses to ensure that cooperative health insurance is implemented. The overwhelming response from partners calls for HealthPartners to review opportunity of expanding geographical coverage in the country.
IV. What Works and What Will be Changed
HealthPartners staff required additional technical training on health coop development in order to provide effective support. A new provider support supervision tool was developed and staffs were trained to apply principles of Criterion Referenced Instruction (CRI) through the Support Supervision process.
Integrated provider support supervision with provider staff and administrators includes the following objectives: As part of CRI, learners must demonstrate the capacity to fill training objectives in actual settings. Provider support supervision, allows HP staff to provide knowledge of results and individual differentiation for the last stages of training on the following objectives: Provider enrollment of new member groups; provider creation of new member ID cards; provide ability to lead effective coop orientation days; data entrant’s ability to use data to make effective actions plans, sharing those plans and progress toward goals routinely with top administrators at health facilities in order to receive support for implementation.
V. Plans for the Next Six Months
Jennifer Stockert, Director, will be visiting January 5-17, 2014
Gordon Lindquist, Cooperative Consultant, will lead governance training for Collaborations project supported coops including UHC, WAD, AD and MAD. HealthPartners Mama Coop leaders will also benefit from this partnership coordinated training where costs are being leveraged through HealthPartners Health and Economic Livelihoods project with Global Communities.

Focus on KIUTH and NAD to start 2 new coops.
Continued follow up with UCCC, UCMB and UPMB.
AGMs will be led by all four coops and governance training will be provided for newly elected coop leaders. During this training, coop stakeholders develop or review by-laws and develop locally appropriate communication plans to keep members informed and in control of coop activities. Stakeholders will also develop: end results policies to define board of director fiduciary responsibilities and risk priorities; Board Conduct Policy; and a Monitoring Organizational Performance Plan that holds the board accountable to its policies and members.
Using telephone text message reminders to improve on time premium payment will be explored and tested for possible scale up.
New coops will be encouraged to open reserve fund bank accounts after their AGMs.
Opportunities will be created for those who have embraced and benefitted from new coop ID membership card formats so those providers can share what they have learned and they impact enjoyed as a result of this cheaper, faster, sustainable way to make IDs.
Data will be shared to help coop leaders learn from different benefit packages, premium prices and enforcement of insurance rules.
In order to continue realizing annual provider surplus, the contracted health care providers will be trained in stock management focusing on medicine management.
Training of coop leaders on book keeping
HealthPartners will research and develop support plans for health savings accounts
Terms of an MOU for continued support to UCBHFA, an apex organizational for health financing scheme managers, is currently being negotiated.

Annex A: Map of Health Coops in South Western Uganda
Created by Elmy Wong, Peace Corps Volunteer
i World Bank, 2009 ii Government of Uganda Health Sector Strategic Plan III 2010/11-2014/15 iii “Escaping poverty and becoming poor in 36 villages of central and western Uganda.” The Journal of the Development Studies 42:346-370. Krishna, Anirudh, Daniel Lumonya, Milissa Markiewicz, Firminus Mugumya, Agatha Kafuko, and Jonah Wegoye. 2007 iv Uganda Demographic and Health Survey 2011 v IMPACT Milestone 23: Hold a series of meetings with cooperative development leaders to agree upon a commonly accepted set of measures for future objective and comparative measurement of cooperative IMPACT Milestone 24: Complete protocol and standardization of data collected and deliver plan for the storage and manipulation of the data. Provide a final report of treads, patterns and conclusions drawn for the data sets to demonstrate the functionality of the platform

Milestone 27: Implement strategies for communicating the unique impact of cooperatives on the development process with a serious effort to research and analyze the performance data that is targeted at key constituencies Milestone 29: Organize various collaborative group meetings, activities and managing the IMPACT project vi CLARITY Milestone 10: Write draft of Cooperative Advocacy: A Practical Guide for Advocating Cooperative Legal and Regulatory Reform for publication Milestone 11: Publish Cooperative Advocacy: A Practical Guide for Advocating Cooperative Legal and Regulatory Reform Milestone 14: Organize various collaborative group meetings, activities and managing the CLARITY project. Milestone 17: Conduct a series of public events such as workshops, exhibitions and meetings to disseminate information about the CLARITY Initiative and Collaborative Group member projects. Milestone 25: Organize various collaborative group meetings, activities and managing the CLARITY project. Milestone 26: Conduct a series of public events such as workshops, exhibitions and meetings to disseminate information about the CLARITY Initiative and Collaborative Group member projects.





























