Embed Size (px)
Citation preview

Featuring a live event on January 28, 201512 p.m.–3 p.m. ET (9 a.m.–12 p.m. PT) Scripps Health | San Diego
2 Analysis Case Studies 4 Lesson 1: Restructure the Leadership
Matrix to Build Accountability and Reduce Variation
7 Lesson 2: Empower the Healthcare Team to Experiment and Drive Value by Design
13 Lesson 3: Drive for Population Health Through Primary Care Redesign
16 Resource Guide Additional Resources From HealthLeaders Media
HealthLeaders Media LIVE at Scripps Health
Value by DesignA Blueprint for Slashing Waste, Lowering Costs, and Improving Quality

2January 28, 2015 I HealthLeaders Media LIVE I Value by Design
Can Value Ever Be Designed?
Analysis
Look behind what passes for
value-based healthcare these
days and you will see there
isn’t much design to it. Instead, many
so-called value-based systems are
chopped-up versions of existing sys-
tems that have been subjected to the
wringer of cost cutting.
The problem with the subtrac-
tive view of creating value is that it
uses efficiency tricks to sustain weak
systems of care. To truly create value
means taking a merciless, brutally
self-critical view of the system, its
leadership, and its ability to sustain
itself in the future. The board and
chief executive at Scripps Health
went through that in 2010, and they
didn’t like what they saw. President
and CEO Chris Van Gorder under-
stood that many health systems are
too vertically oriented around hos-
pital C-suite leadership teams, each
competing to push their hospital to
the top of the performance chart. In
a volume-based reimbursement envi-
ronment, that will work to drive up
efficiency and chase procedural care
dollars, but it is poison to creating
efficient systems of care between dif-
ferent parts of the health system.
But going too horizontal has its
fatal flaws as well, creating a top-
down layer of management detached
from the concerns of the ED or the
primary care office. With excessive
horizontal management, account-
ability becomes broader but more dif-
ficult to define. So Scripps is aiming
to achieve appropriate emphasis on
elements of both horizontal and verti-
cal management, with some success
so far.
The team was rebuilt in 2010
with four system leaders overseeing
the medical, clinical operations, sup-
port, and administrative divisions,
with a fifth for population health
added in 2012. But leadership teams
under a CEO and CNO are left at each
of Scripps’ five hospital campuses.
What has started under that
hybrid structure is a new way of look-
ing at healthcare process improve-
ment. By definition, improvement is
almost universally at the unit level—
fixing lab report delays in the ED, for
Leadership Programs DirectorHealthLeaders Media
JimMolpus

3January 28, 2015 I HealthLeaders Media LIVE I Value by Design
example, or strengthening patient access to primary care. To do that, you need
to empower the front line with resources and have the performance improve-
ment staff put some metrics on the problem and commit the resources to invest
capital when a solution is needed.
So far, Scripps leaders say they have taken $320 million in waste out of the
system, almost all of it on the inpatient side. The next steps will be to extend the
underlying system into ambulatory care and population health, which may be
considered a leap of faith in expertise for many hospital-based systems.
Jim Molpus is leadership programs director for HealthLeaders Media. He
may be contacted at [email protected].

4January 28, 2015 I HealthLeaders Media LIVE I Value by Design
What are defined as
health systems today
are not really health
systems at all, but loosely held con-
federations of healthcare providers
tied together by a marketing brand
and a Medicare number. The leader-
ship team at Scripps Health knew
at the start of this decade that com-
peting in the future of value-based
healthcare would require a new way
of providing healthcare—starting
with a change in the leadership struc-
ture.
By 2010, Scripps Health
President and CEO Chris Van Gorder
had already spent several years laying
a foundation of strong leadership
and accountability across Scripps’
five hospital campuses. Van Gorder
installed a chief executive (CE) and
chief nurse at each campus, giving
them numbers to hit and a mandate
for performance turnaround. “And it
worked magnificently,” Van Gorder
says.
Restructure the Leadership Matrix to Build Accountability and Reduce Variation
Case Study // LESSON 1
“We went from about 50–55 days
cash on hand and losing money to
where we are today, which is a very,
very strong balance sheet, strong
operations across the board, and a
real sense of accountability along
the way. But what it also did was
created variation, because every chief
executive did it their own way.”
But the structure also created
unhealthy internal competition, he
notes. “It was a constant competition
for capital resources,” Van Gorder
says. “Each believed that their
campus was more important than
any other campus, even if that meant
duplicating services that existed
relatively close by in the healthcare
system.”
By 2010, it became apparent
that a decentralized organizational
chart was going to create too much
variation—which translates into
waste and cost—for Scripps to
move forward. But creating a central
office model took away site-based
» Five hospital campuses
» More than 13,000 employees
» 1,980,000 annual patient visits
» 1,372 total licensed acute care beds
Scripps HealthSan Diego
BY JIM MOLPUS

5January 28, 2015 I HealthLeaders Media LIVE I Value by Design
accountability and incentive to change.
So Scripps developed a hybrid featuring four horizontal divisions that
crossed the healthcare system: corporate medical, clinical operations, support
services, and administrative services. Each division is headed by a corporate
senior vice president, each with goals to standardize clinical operations and
reduce variation across the system.
Under this hybrid model, campus CEs remain, but all capital requests go
through the system vice presidents for team and system analysis and approval.
CEs are still involved in final capital decisions through the Capital Requests
Committee, after they have been vetted through the corporate vice presidents
(and clinical care lines, where appropriate).
One of the cultural goals was not to lose the importance of accountability,
but to spread it around.
“It’s a shift from an individual-based accountability to a team-based
accountability,” Van Gorder says. “We didn’t really express it that way to begin
with, but we understood that healthcare is not administered by individuals. It’s
administered by teams of caregivers.”
That cultural shift required new ways of thinking about improvement, says
Barbara Price, corporate senior vice president of business and service line
development, and one of the senior leaders in the new structure.
“We discovered a few things that inherently run a little bit counter to
our culture overall in healthcare. One is that the concept of testing and doing
experiments is not a comfortable thing when you’re dealing with patients’ lives,”
Price says. “So we are actively engaged in training and helping people just get
comfortable with that.”
Another cultural shift involved moving away from the typical method of
healthcare problem solving, she says. “Over the years, if something needed to
be done, we would add another person to do it, right? We wouldn’t redesign the
process. We’d add more cost, and then we could turn around and charge the
payer because they would pay. We’re not in that environment anymore, so we
“SHIFTING THE CULTURE IS UGLY AND MESSY. SOME PEOPLE MAKE IT AND SOME PEOPLE DON’T.”
—Chris Van Gorder, president and CEO, Scripps Health
6January 28, 2015 I HealthLeaders Media LIVE I Value by Design
have to ask tough questions and simplify those processes that we’ve made so
complex by that historical approach.”
Still another challenge involved how people work and are motivated.
“In healthcare, we have a tendency toward heroics just by the nature of how
a health organization exists,” Price says. “So people come into the emergency
department: You have all kinds of resources that swarm around them to deal
with an emergent issue. So heroics are important, but so is consistency in how
we get day-to-day systems in place to prepare for patients.”
The system leaders recognized early on that the cultural transition would
be somewhat painful, Van Gorder says. However, an organizational philosophy
against layoffs gave staff members some reassurance. The system leadership
team also met regularly with the existing Scripps physician leaders and
the Scripps Leadership Academy alumni to answer questions and sustain
momentum.
“There’s a natural tendency to resist change,” Van Gorder says. “And the
horizontal model really meant everybody needed to change. Shifting the culture
is ugly and messy. Some people make it and some people don’t.”
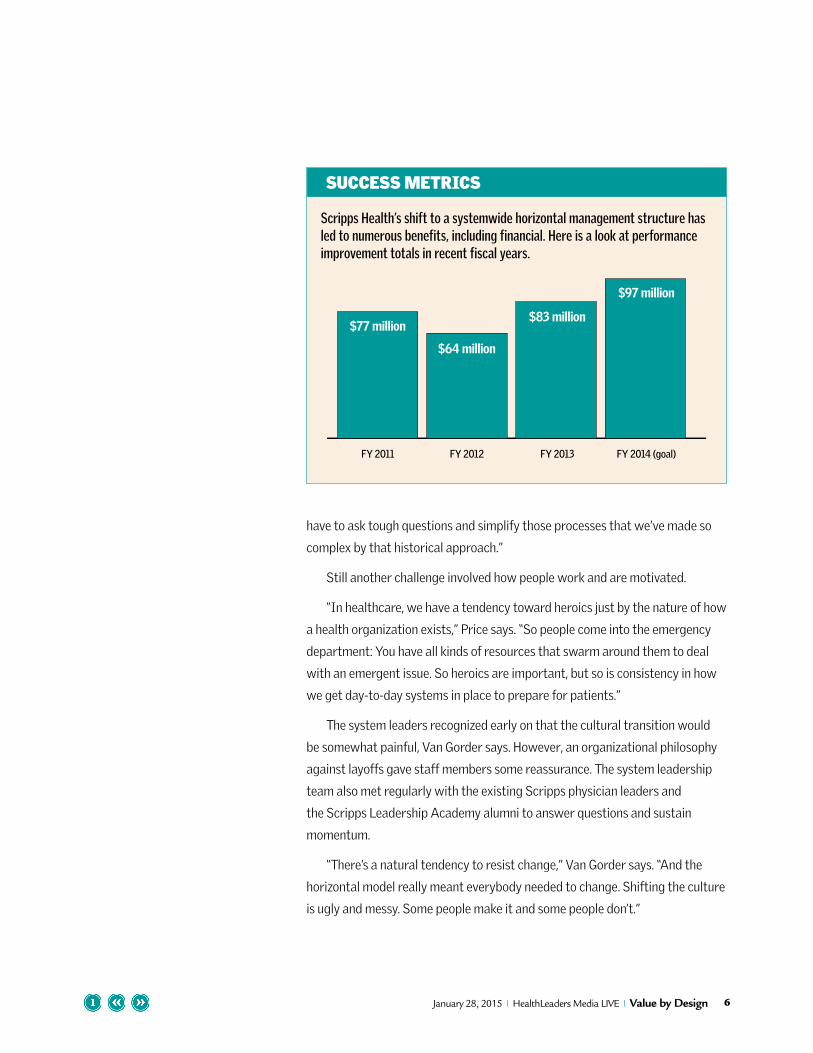
SUCCESS METRICS
Scripps Health’s shift to a systemwide horizontal management structure has led to numerous benefits, including financial. Here is a look at performance improvement totals in recent fiscal years.
0
20
40
60
80
100
FY 2011 FY 2012 FY 2013 FY 2014 (goal)
$77 million
$64 million
$83 million
$97 million

7January 28, 2015 I HealthLeaders Media LIVE I Value by Design
Even the most diligent, com-
mitted health systems run
into a fundamental flaw in
system improvement very soon in the
process: how to drive system change
at the unit level. If you view system
improvement at the highest level,
then the initiatives often fail because
they are seen as top-down mandates.
If you let small units randomly chase
whatever quirk they identify, then
projects may not map to system goals
or add value overall to the patient.
Michelle Tressler, PhD, assistant
vice president for project manage-
ment and head of the Value by Design
internal staff, says sustainable
improvement blends both top-down
and bottom-up. Tressler says top-
down improvement works for a while,
but things eventually fail.
“Leaders try to fix things as an
organization, but they were not the
ones who were doing the work,”
Tressler says. “So it all falls apart
once you actually have to implement
because the devil’s in the details.
Empower the Healthcare Team to Experiment and Drive Value by Design
Case Study // LESSON 2
When you implement, you find the
holes between what sounds good on
paper versus what happens in reality.”
Quality improvement initiatives
are just that—initiatives. They are
fragile introductory steps that can
quickly fail if they do not become
embraced and systematized into
workflow.
“We didn’t really have a mecha-
nism to be able to link those togeth-
er,” Tressler says. “If we did manage
to create a process that worked
well, we didn’t have a good manage-
ment system in place to be able to
verify and ensure that that process
was being kept up to date and being
worked every single day, consistently
and reliably, to be able to produce the
outcomes that we knew they could.”
Scripps recognized it needed to
empower frontline staff to identify
gaps in care, but with support from
experts. The performance improve-
ment team now consists of nine proj-
ect engineers, many of whom have
management engineering or indus-

8January 28, 2015 I HealthLeaders Media LIVE I Value by Design
trial engineering backgrounds. All are trained in principles of Lean improvement,
Tressler says.
“They are the coaches for these teams that take on performance improve-
ment work,” she says. “They are there working with those managers, helping to
coach them every single day, not just on the tools and techniques, but also really
about how to ask the question differently and how to elicit ownership from the
front line.”
What makes the system work is the teams are assigned based on processes
that map to system goals.
“We are disseminated based on the needs of the organization,” Tressler says.
“Every year our organizational goals are outlined, and those goals prioritize
where our team works first. So there’s a lot of focus right now on the inpatient
setting of lowering costs and transforming work flow.”
Value by Design Project: Medication ReconciliationTo identify waste, the team started by mapping a patient’s journey through a
typical inpatient hospital stay (registration through discharge), says Mary Ellen
Doyle, corporate vice president for nursing operations.
“One of the things we discovered was how much time the nurse spends
when a patient is admitted, trying to collect and redo medication reconciliation,”
Doyle says. “When we did the initial time studies, we found the inpatient admit-
ting nurses spent anywhere from 40 to 50 minutes on a complicated medication
reconciliation.” Even then, there were times when getting an accurate medica-
tion list took two days of duplicating efforts. Occasionally, the medication list
remained incomplete.
Medication reconciliation had been “just a bunch of activity going on, not
a process,” says James LaBelle, MD, corporate senior vice president and chief
medical officer.
“You come into the ER and the nurse takes a medication history and writes it
“WHEN YOU IMPLEMENT, YOU FIND THE HOLES BETWEEN WHAT SOUNDS GOOD ON PAPER VERSUS WHAT HAPPENS IN REALITY.”
—Michelle Tressler, PhD, assistant vice president for project management, Scripps Health

9January 28, 2015 I HealthLeaders Media LIVE I Value by Design
down, a list,” LaBelle says. “The doc comes in, does the same thing. [But] the lists
are not concordant. The family brings in the medications. There are new, old, and
expired medications on there, and it gets altered. Then the patient goes up to
the floor, and the nurse takes a fourth medication history, and on and on it goes,
right? There isn’t a process by which a medication list is acquired on the initial
encounter and successive refinement occurs until we have a final medication list
that actually is accurate and the system is shown to be accurate.”
The team did a rapid improvement event and mapped out a goal of having
an accurate preliminary medication list by the time the physician writes the
admitting orders. When a patient is registered in the emergency department,
the patient access representative enters basic patient identifiers, and a soft-
ware solution automatically mines local regional and national pharmacies for
prescriptions that the patient has filled. Once the software list is downloaded,
a pharmacy technician meets with the patient, if possible, to review and revise
before the medication list is reviewed by the admitting ED physician.
Jeremy Delashmit, RN, an ED nurse who was involved in the medication
reconciliation project and other Value by Design projects, says the time that
ED nurses spend on medication reconciliation has dropped from 15 minutes to
three, and has saved the inpatient nurse anywhere from 27 to 45 minutes. In
addition to the time savings, of course, are the obvious quality and patient safety
benefits from having an accurate medication list with the physician before treat-
ment starts.
“It’s been highly accurate and highly successful for us,” Delashmit says. “I
get numerous comments from patients who come to us from anywhere in the
United States—Las Vegas, Hawaii, and so forth—who have just been thankful
for this because no one had ever done that for them before. It’s helped us treat
them more effectively.”
Value by Design Project: Physician Preference ItemsAnyone who says that physician preference items are the low-hanging fruit
of supply chain savings should try to pluck that fruit sometime and see what
happens. “When you pull doctors together who are very passionate about their
spinal implant device and the particular company they get it from and the assis-
tance they get from the sales representatives literally in the operating room,
that’s not really low-hanging fruit,” Van Gorder says.
What Scripps did four years ago was the typical tactic of reducing the

10January 28, 2015 I HealthLeaders Media LIVE I Value by Design
number of approved vendors and devices down to a very select few. Pretty soon
the savings didn’t look like savings at all, says James Bruffey, MD, an orthopedic
surgeon and spine specialist at Scripps Clinic.
“Within the spine care line, we do a bunch of complex procedures,” Bruffey
says. “We have surgeons that approach things differently. The goal is always
the same, to take good care of your patients. One surgeon may want to do this
operation one way and the validity is there to support it versus another surgeon
having a preference for something else.”
When Scripps went to a restricted list of devices, no one fully considered the
actual volume and variety of procedures that were being done.
“So the decisions were made kind of in a vacuum and, for example, in my hos-
pital, once the vendors were picked, it excluded 50% of our current operational
activity,” Bruffey says. “So in other words, half of what we did was no longer
available to us from an implant standpoint.”
There was a better way, which involved all of the spine surgeons agreeing
to a system where new devices are tested and validated, and then added to the
formulary as long as the vendor meets the price defined for that category by the
Scripps surgical team.
“We are routinely reviewing the categories we’ve created to make sure that
there’s nothing that’s falling out,” Bruffey says. “If we need to create a new cat-
egory, we all look at the pricing that’s been requested and we will say to vendors,
‘No, you can’t have a new category. This falls into this category. We have a price
for that category. If you would like to participate with that product, you have to
place it into this category.’ ”
The cooperation among spine surgeons has saved $1,040,234 for the
system and created a new dialogue for improvement. So far, the program has
worked on a sense of team spirit, but evaluating incentives and gainsharing with
physicians remain goals for the future.
“The reality is, physicians want to help us save money. And they also want to
retain choice, if they can,” Van Gorder says. “So all of a sudden, the administra-
tors and the physicians are aligned to deal with a distributor who’s trying to
gouge us on, you know, ridiculous prices for a screw or something like that.”

11January 28, 2015 I HealthLeaders Media LIVE I Value by Design
Value by Design Project: ED FlowIt really doesn’t take sophisticated computer algorithms to go through what
happens in emergency department flow. It just takes some painstaking work to
go step by step through weeks of typical patient encounters. Rose Colangelo,
patient care manager for the emergency department, says that when the ED
team actually looked at what happened to patients, some bottlenecks immedi-
ately rose to the surface.
One huge area of wasted time for the patient was between the ED and radi-
ology, she says.
“So the order went into the computer, then radiology would get the order,”
Colangelo says. “Radiology would dispatch transport and then transport would
come to the ED, pick up the patient, and then take the patient to radiology.
When the test was done, radiology would again page transport. So we found
that there was about 40 minutes of just wasted time in that, which then adds
up because then the next patient has to wait that additional 40 minutes. By
the time you get to the fourth of fifth patient who’s waiting for a test, it could
already be like an hour and a half by that point.”
Dramatic results don’t always take dramatic changes, as the team found.
“So what we did is we took ownership of that transport by having a desig-
nated technical partner in the emergency department facilitate patient trans-
port,” Colangelo says. “So when a patient’s order goes into the system, radiology
calls directly to one of our technical partners who then facilitates that patient
going to radiology or CT. We’ve actually reduced our times from 40 minutes to
five minutes for our average now.”
There were other bottlenecks identified and fixed:
• Instead of having patients repeat their history several times, the initial
encounter asks for the chief complaint and the history is taken bedside
with both the nurse and physician.
• The lab would get backed up on blood work, often with only one lab tech
drawing blood. So, instead of paging the lab and having the tech walk in to
do blood work, nurses now do all routine blood draws, which has reduced
the time ordered to time reported from 35 minutes to 19.

12January 28, 2015 I HealthLeaders Media LIVE I Value by Design
• The computer system sometimes would indicate that an ED room was not
ready, even though the patient had been discharged much earlier. This was
the result of a workaround so nurses would not put patients in a room that
had not been cleaned, Colangelo says. But by simply adding a screen note
for rooms that are empty but need to be cleaned, the staff saved 10 min-
utes of wasted time by being more aware of which rooms were actually
ready.
In any process stream, improvement comes in managing and fixing many
small snags. The first step is to look at the stream, though. “It really is an amaz-
ing experience because we actually got to look at even the simplest things,”
Colangelo says.

13January 28, 2015 I HealthLeaders Media LIVE I Value by Design
In the first four years of Scripps’
move to Value by Design, most
of the emphasis has been on
the inpatient side, Van Gorder says.
Why? “Because revenue is
mostly on the hospital side,” he says.
“But we had the dialogue that if we
really wanted a robust healthcare
delivery system, we wouldn’t start
in the hospital. We’d start on the
ambulatory side, where most
healthcare is delivered.”
Even as the work started on
reducing waste on the inpatient
side, Scripps leaders hedged for an
ambulatory future. From a base of
only a half-dozen ambulatory sites a
decade ago, Scripps has more than
26 now, with property purchased
throughout the county for future
growth. In addition, two years
after the horizontal system leaders
were added, Van Gorder hired Anil
Keswani, MD, as corporate senior vice
president of ambulatory care and
population health management.
“I wanted a physician executive to
Drive for Population Health Through Primary Care Redesign
Case Study // LESSON 3
lead strategy and tactics to move the
organization into population health,”
Van Gorder says. “And every time
we’ve done something in the hospital,
we recognized it was eventually
going to shift into the ambulatory
environment.”
By the time Keswani started,
Scripps had already seen gains in
efficiency on the inpatient side, and
care navigators were starting to fill
gaps in the continuum, particularly
around areas like readmission that
were tied to reimbursement.
“When I came on, we had some
wildly successful programs, but we
also need to improve the primary care
design so that there is still a captain
of the ship,” he says. “So the last two
years have been heavily focused on
primary care redesign. One could
argue it’s really primary care design,
because we never really designed
things in the first place in healthcare.”
The goal was to “develop a team
around the primary care provider” to
help them manage patients, Keswani
14January 28, 2015 I HealthLeaders Media LIVE I Value by Design
says. “We purposefully steered away from the official medical home programs,
because the literature did not show improved value for patients.”
Siu Ming Geary, MD, a primary care provider and vice president of
ambulatory care at Scripps Clinic, says the redesigned care team consists of two
full-time physicians, one physician extender who is either a nurse practitioner
or physician assistant, plus a licensed vocational nurse. In a conventional PCP
model, the physicians and the extender each would have a panel of patients, but
in the Scripps care team, the extender spends 75% of the time seeing patients
who are part of the two physicians’ panels. The other 25% of the time is spent
“on population management, answering phone calls or returning messages.”
“We accomplish several things with this care team. One is that everyone
works at the top of their license,” Geary says. “What we find is that physicians
are much more efficient when they’re not interrupted multiple times during
the day doing things that could be potentially done by an LVN or a nurse
practitioner. The PCPs don’t have to wait until the end of the day to catch up,
which enhances both physician and staff satisfaction. And there’s significant
decrease in turnaround time for messages, forms, or orders.”
New teams needed new standardized work and communication, as well. The
standard work sets designate certain kinds of patients to be seen by physicians
and other kinds to be treated by the nurse practitioner. The care team holds a
huddle every morning to review the day and make any necessary adjustments to
get patients in.
Geary says this care team improves patient flow over the standard team of
one nurse and one physician.
“If you have one physician and one nurse, the nurse is managing patients,
but they also do your phone calls, they do your messages. They may do your
authorizations. If they’re busy doing something and it has to be done, they can’t
get on to the next patient,” Geary says. “That is a blockage that can follow you
the rest of the day.”
“WE ACCOMPLISH SEVERAL THINGS WITH THIS CARE TEAM. ONE IS THAT EVERYONE WORKS AT THE TOP OF THEIR LICENSE.”
—Siu Ming Geary, MD, primary care provider and vice president of ambulatory care, Scripps Clinic

15January 28, 2015 I HealthLeaders Media LIVE I Value by Design
Keswani says he started the work knowing that the path to improved
patient care and access in primary care meant raising physician and staff
engagement. In his previous job, he had seen a transformation at Advocate
Health Care in Illinois that took physician satisfaction from the fourth percentile
to the 97th. He says he has seen the same upward movement at Scripps.
“Once the physicians know that you do care for them and you do genuinely
care for their needs and you’re willing to measure it and focus on it, they’re more
apt to want to do more than what you ask. We’ve built the model by asking
them what is going to work in terms of physician and staff engagement, and
then the metrics will come afterwards.”
16January 28, 2015 I HealthLeaders Media LIVE I Value by Design
For Further StudyLeadership at Scripps Health has developed a Value by Design program that improves clinical and operational processes and leads to improved outcomes. For further study, consider the following resources:
RESOURCE
GUIDE
Clinical Quality: Reassessing Care Metrics and Leadership Models
This piece is adapted from Senior
Research Analyst Michael Zeis’ piece
in the July 2014 HealthLeaders Media
Intelligence Report, The New Quality
Equation: Measuring Success and
Eliminating Waste.
Clinical quality is fundamental
to healthcare, and while that won’t
change, the industry itself is. Payers,
increasingly, are requiring better
clinical results in return for better
reimbursements. Providers, too, are
developing initiatives and incentives
around clinical quality processes and
outcomes. Technology offers more
ways to measure and communicate,
but it also can be a burden. And, of
course, there is continuing pressure
to control the cost of care, creating both challenges and opportunities for the
clinical team. The HealthLeaders Media survey on clinical quality uncovers some
areas where change is prompting rethinking and recalibration.
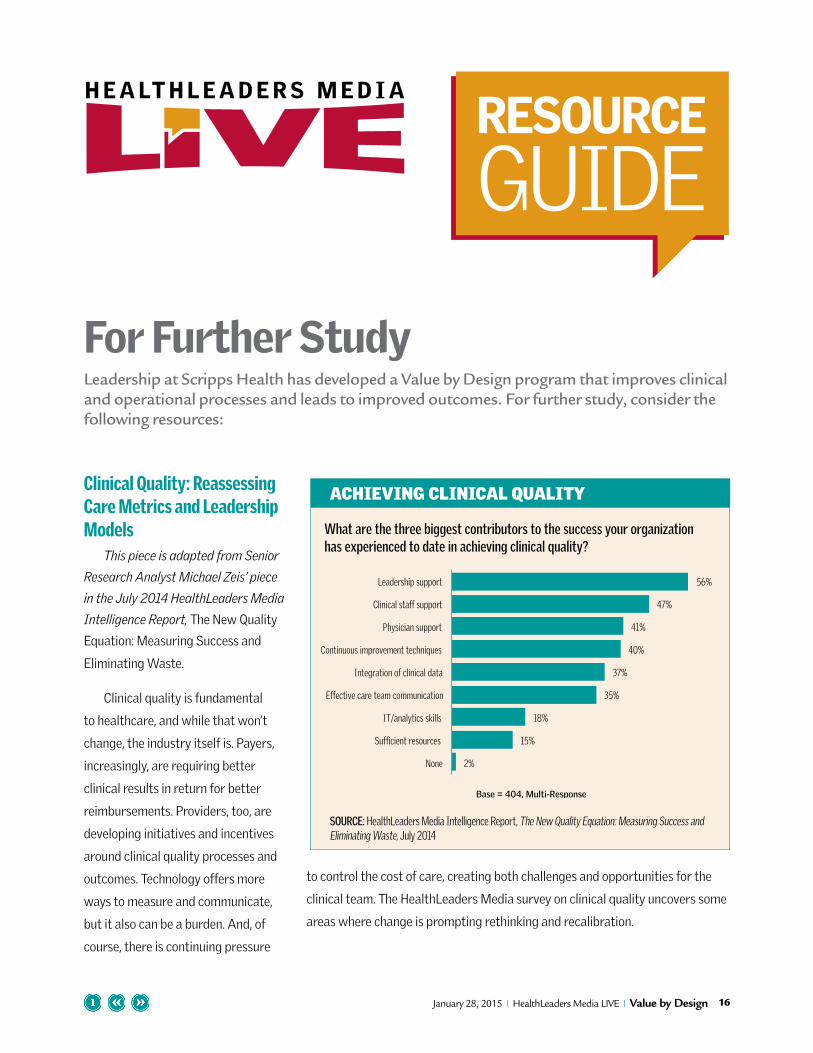
ACHIEVING CLINICAL QUALITY
SOURCE: HealthLeaders Media Intelligence Report, The New Quality Equation: Measuring Success and Eliminating Waste, July 2014
2%
15%
18%
35%
37%
40%
41%
47%
56%
None
Sufficient resources
IT/analytics skills
Effective care team communication
Integration of clinical data
Continuous improvement techniques
Physician support
Clinical staff support
Leadership support
Base = 404, Multi-Response
What are the three biggest contributors to the success your organization has experienced to date in achieving clinical quality?
17January 28, 2015 I HealthLeaders Media LIVE I Value by Design
About the HostScripps Health is a $2.6 billion, non-profit
501(c)(3) healthcare system in San Diego,
California. Scripps treats nearly 500,000
patients annually through the dedication of
more than 2,600 affiliated physicians and
nearly 13,000 employees across five hospital
campuses, plus an ambulatory care network
of clinics, physicians’ offices, outpatient
centers, and home healthcare services.
The Scripps legacy of providing healthcare
services in San Diego originated in 1924,
when philanthropist Ellen Browning Scripps
founded Scripps Memorial Hospital and
Scripps Metabolic Clinic in La Jolla, California.
About UsHealthLeaders Media is a leading multi-
platform media company dedicated to
meeting the business information needs
of healthcare executives and professionals.
To keep up with the latest on trends in
physician alignment and other critical
issues facing healthcare senior leaders,
go to www.healthleadersmedia.com.
Vice President and PublisherRAFAEL [email protected]
Leadership Programs DirectorJIM [email protected]
Editorial Director EDWARD [email protected]
Managing EditorBOB [email protected]
Media Sales Operations ManagerALEX [email protected]
SponsorshipFor information regarding underwriting opportunities for HealthLeaders Media LIVE, contact [email protected] or 800-753-0131.
Copyright ©2014 HealthLeaders Media, 100 Winners Circle, Suite 300, Brentwood, TN 37027 • Opinions expressed are not necessarily those of HealthLeaders Media. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions.
Strategies for Managing the Postacute EnvironmentThis piece is adapted from Senior Leadership Editor Philip Betbeze’s
September 5, 2014, online column. To see his weekly column, visit www.
healthleadersmedia.com/Leadership.
Managing the entire continuum of care may be beyond your organization’s
current capabilities, but that doesn’t mean you can’t try risk-based
reimbursement through Medicare’s bundled payment program. Hospitals and
health systems at the vanguard of managing a patient’s entire spectrum of
healthcare needs are few. Years of fee-for-service reimbursement combined
with a desire to focus on their core competency has left many hospitals and
health systems without owned components for managing the post-discharge
experience for patients.