Embed Size (px)
Citation preview

MedactManchesterreport October2017
1
Healthcareprofessionals’viewsand
experiencesofdealingwithrefugees
andasylumseekers:asurveyofNorth-
Westpractitioners
AreportbyMedactManchester
October2017

MedactManchesterreport October2017
2
TableofContents
Acknowledgements 4
Declarationofinterests 4
Terminology 5
Glossaryofterms,acronymsandabbreviations 5
1.ExecutiveSummary 6
2.Introduction 8
3.Aims 12
4.Methods 12
5.Results 14
5.1Surveyresponses 14
5.2HCPs’understandingofthedefinitionsofimmigrationstatus 15
5.3HCPs’understandingofmigrantgroups’eligibilityforNHScare 16
PrimaryCare 16
FreeEmergencyCare 18
Freenon-emergencycare 19
5.4Identifying,documentingandtreatingtorture 21
5.5HCPs’trainingneeds 24
6.Discussion 25
7.Limitations 29
8.Recommendations 31

MedactManchesterreport October2017
3
AppendixA:SurveyQuestions 33
AppendixB:ResponderFeedback 34

MedactManchesterreport October2017
4
Healthcareprofessionals’viewsand
experiencesofdealingwithrefugees
andasylumseekers:asurveyofNorth-
Westpractitioners
ThisreporthasbeenauthoredbymembersofMedactManchester:DrKatieLawton,DrAlice
Lee,DrNadiaMahmood,DrMayaTickell-Painter,DrPiyushPushkar,DrAmySquire,DrLouise
Tomkow,DrRuthWiggans,DrEmilyWhitehouseandDrRebeccaWilson.
MedactManchesterisagroupofdoctorsbasedintheNorthWestofEnglandwithaninterestin
thesocialdeterminantsofhealth.TheyareaffiliatedtothenationalcharityMedact.
AcknowledgementsDrDavidMcCoy
DrRebeccaFarrington
DrJoanneMiller
EstelleWorthington
DeclarationofinterestsMedact Manchester has received no specific funding for the writing of this report. Medact
Manchesterhasnoconflictofinterestwithregardtoanyissuesarisinginthisreport.

MedactManchesterreport October2017
5
TerminologyThis report seeks toexaminehealthprofessionals’understandingofhealthneeds in refugees,
asylumseekers,andfailedasylumseekers.Asylumseekersareindividualswhohaveappliedfor
protectionasrefugees.Refugeesaredefinedbythe1951RefugeeConventionaspersonsfleeing
conflict or persecution, and are afforded special protection under international law. Failed
asylumseekersareindividualswhohavehadtheirasylumclaimrejected,orareundergoingan
appealsprocess.Theterms‘migrant’and‘refugee’aresometimesusedinterchangeably,andin
practice making a distinction between the two groups can be very difficult. Distinguishing
between people who are refugees and those who are migrants is a highly political and
controversial issue.Whilstwe recognise that refugees and asylum seekers sharemanyhealth
issueswithothermigrantgroups,wefocusonhealthissuesinthefirsttwogroupsinthisreport.
Glossaryofterms,acronymsandabbreviationsAS–Asylumseeker
AHP–AlliedHealthProfessional
COMPASS-CommercialandOperationalManagersProcuringAsylumSupportServices
FAS–Failedasylumseeker
GP–GeneralPractitioner
HCP–Healthcareprofessional
NHS–NationalHealthService
PTSD–PostTraumaticStressDisorder
MedactManchesterreport October2017
6
1.ExecutiveSummary
1.1 Numbersofrefugeesandasylumseekersareincreasingacrosstheworld
Globally, levels of forcedmigration are at their highest on record. In the UK specifically, the
numberofasylumapplicationsincreasedby30%in2016comparedtopreviousyears.
1.2 Refugeesandasylumseekershavespecifichealthcareneeds
Individuals seeking asylum experience a range of healthcare problems related to the
circumstancesintheirhomecountry,thenatureoftheirjourneyandthesituationinwhichthey
findthemselvesintheUK.
1.3 LocalNHSservicesreceivenoextrasupportorfinancialhelptoprovidecarefor
refugeesorasylumseekers
ThereisnonationalcoordinationofhealthcareprovisionforasylumseekersintheUK.Assuch,
existingNHSservicesareexpectedtoprovidecareforasylumseekersintheirlocalareawithno
extrasupport.
1.4Atundergraduateandpostgraduatelevels,medicaltrainingonthespecifichealthissues
facedbyasylumseekersandrefugeesintheUKispatchyandinconsistent.
Confusion amongst healthcare professionals regarding eligibility for NHS healthcare has been
reportedbutneverquantified.Concernshavebeenvoicedthatthisconfusioniscontributingto
thepoorerhealthoutcomesseeninasylumseekersandrefugees.
1.5 We conducted a survey of 198 NHS healthcare professionals working in Greater
ManchesterandLancashire
We sought to examine North-West of England NHS healthcare professionals’ current
understanding of refugee and asylum seeker health issues, identify healthcare professionals’
trainingneedsonthesetopicsandexploreavenuesforfutureresearchonrefugeeandasylum
healthintheUK

MedactManchesterreport October2017
7
Our sample included doctors, nurses, psychologists and non-clinical staff, working across a
broadrangeofspecialties.
1.6Our resultsdemonstrate significantgaps in theknowledgeandconfidenceofhealthcare
professionals when dealing with asylum seekers and refugees, across all specialties and
grades.
• Only 21% of responders felt confident defining the terms “asylum seeker”, “failed
asylum seeker”, “economic migrant” and “refugee”, with only a quarter correctly
identifyingwhichgroupswereeligibleforfreeprimarycare.
• 32%failedtoidentifyfailedasylumseekersaseligibleforfreeemergencycare.
• Although55% said they had treated a patient sufferingwith psychological or physical
effectsoftorture,only12%feltconfidentaskingapatientaboutprevioustorture.23%
feltthattheywerenotcompetenttoenquireaboutexperiencesoftorture.
• 88% felt that they would benefit from further training on issues surrounding asylum
seeker and refugeehealth,with79% saying that theywouldprefer training ledby an
expertinthefield.53%alsosaidtheywouldlikeonlinetraining.
1.7 ThereisanurgentneedfortrainingforfrontlineNHSstaffonthehealthneedsofrefugees
andasylumseekersandtheireligibilityforNHScare.
Thistrainingshouldcoverfivekeyareas:
a. Understanding thecomplexhealthneedsof refugeesandasylumseekers,and
howtheymaydiffertotheordinarilyresidentpopulation.
b. Understanding terminology used to describe refugees and asylum seekers,
including how this may change over time. This would require a basic
understandingoftheasylumprocess.
c. Exploring the moral, ethical, and legal responsibility healthcare professionals
haveinassessingindividuals’rightstohealthcareintheUK.Thismustbedone
inkeepingwithprofessionalcodesofpracticesuchas‘GoodMedicalPractice’.
d. Identifying and appropriately documenting evidence of torture. This should
include information on signposting to groups experienced in dealing with
refugeesandasylumseekerhealth.
MedactManchesterreport October2017
8
e. Wesuggest this trainingbeprovidedby individualswithexperience indealing
withthecomplexitiesofrefugeesandasylumseekerhealth.Thisshouldinclude
allstakeholders,andcouldincludeNHSprofessionals,thirdsectororganisations,
andmembersoftherefugeeandasylumseekercommunity.
1.8 Refugeeandasylumhealthshouldbeintroducedasacoretopicinmedicaleducation
fromundergraduateleveltoseniorcontinuingprofessionaldevelopmentprograms.
1.9 ThereisaneedforfurtherresearchonHCPsandrefugeeandasylumhealthintheUK.
Avenuesforfurtherresearchinclude:
a. expandingtolookatHCPsinotherregionsoftheUK;
b. greater inclusionofHCPsotherthandoctorse.g.nursing,midwifery,dentistryand
otherAHPs;
a. exploringthe impactof thenew legislationonHCPsunderstandingof refugeeand
asylumhealth.
1.10 Refugees and asylum seekers must continue to receive healthcare in line with their
humanrightsandthecodesofpracticethatgoverntheprovisionofhealthcareintheUK.
2.Introduction2.1AsylumissuesworldwideandintheUK
Complexhumanitariancrisesareincreasinginfrequency.Levelsofforcedmigrationareattheir
highestonrecord;onein113peoplegloballywereforciblydisplacedfromtheirhomesdueto
conflictorpersecutionin20161.IntheUKasylumapplicationsareincreasing,withapplications
madefor44,323peopleintheyearendingJune2106,up34%fromthepreviousyear.In2016,
thelargestnumberofapplicationsforasylumcamefromIran(4,910),followedbyIraq(3,199),
1http://www.unhcr.org/uk/news/latest/2016/6/5763b65a4/global-forced-displacement-hits-record-high.html

MedactManchesterreport October2017
9
Pakistan (2,992), Eritrea (2,790), Afghanistan (2,690) and Syria (2,563).2 In addition to these
numbers, theUKgovernmenthaspledged to resettleanadditional20,000Syrian refugeesby
2020, a commitment that would require the resettlement of 10 times asmany refugees per
monththaniscurrentlyhappening,3aswellasayetundeterminednumberofunaccompanied
asylumseekingchildrenfromEuropeundertheDubsamendmenttothe2016ImmigrationAct.4
2.2AsylumissuesinGreaterManchester
Asylum seekers are unevenly distributed across the UK. Greater Manchester has one of the
highestnumbersofasylumseekersintheUK,anumberthathasincreasedsignificantlyoverthe
last threeyears.5Approximately5000asylumseekerswere living inGreaterManchesterasof
June 2015, with uneven dispersal throughout the region.5 Under the Commercial and
Operational Managers Procuring Asylum Support Services (COMPASS) programme, the UK
government has awarded private providers such as SERCO and G4S contracts for providing
asylum seekers with accommodation. The desire to provide this accommodation in a cost-
effectivemannerhasledtomanyasylumseekersbeinghousedinareaswhereaccommodation
ischeap.However,notonlyisthestandardofhousingprovidedoftenunacceptablypoor,6but
alsolarge-scaleresettlementofasylumseekersinareasofsignificantsocioeconomicdeprivation
has exacerbated existing social tensions in some of the most deprived areas of Greater
Manchester.9,7
2https://www.gov.uk/government/publications/immigration-statistics-april-to-june-2016/asylum3ManchesterCityCouncilCommunitiesScrutinyCommittee-28thOctober2015.SupportAvailabletoAsylumSeekersandRefugeesinManchester.StrategicDirector,AdultSocialServices.4https://www.gov.uk/government/news/unaccompanied-asylum-seeking-children-to-be-resettled-from-europe5http://www.manchestereveningnews.co.uk/news/greater-manchester-news/rochdale-mp-simon-danczuk-attacks-99578366http://www.parliament.uk/business/committees/committees-a-z/commons-select/public-accounts-committee/news/asylum-accommodation-substantive/7http://www.manchestereveningnews.co.uk/news/greater-manchester-news/asylum-seekers-greater-manchester-cost-10874865

MedactManchesterreport October2017
10
2.3Asylumandhealth
Individuals seeking asylum experience a range of healthcare problems that may differ from
those of local populations.8 Prior to arrival in the UK, asylum seekers may have endured
imprisonment,tortureorsexualassault,andmayexperienceongoingphysicalorpsychological
effectsofthese.9Poornutritionandsubstandardsanitationcanplaceasylumseekersathigher
risk of communicable diseases. Many asylum seekers come from areas where existing
healthcareinfrastructureispoor,meaningchronicdiseasecangoundetectedandmanagement
isneglected.10Inadditionthereisevidencethatthehealthandwellbeingofasylumseekersand
refugeesdeteriorateonarrival to theUK,owing to separation, stigmatisation, social isolation,
lossofstatusandlackofaccesstoservices.11Aprolongedasylumapplication,withitslegaland
financialcomplexities,hasbeenshowntocausephysicalcomplaints,lowself-reportedqualityof
lifeandfunctionaldisabilities.12Furthermore,mentalhealthdisorderssuchasmooddisorders,
anxiety,somatoformdisordersandPTSDaremorecommoninasylumseekers.13
However, despite this population having specific health needs, medical professionals are not
currently being provided with training on these issues. In ‘Tomorrow’s Doctors’, the GMC
stipulatesthatUKmedicalschoolgraduatesshouldbeabletodiscussthewiderdeterminantsof
healthandhealthinequalities.14Despitethis,notallmedicalschoolsprovidespecifictrainingto
medical students on the health of asylum seekers and, where it is provided, training for
undergraduates is fragmented. Many specialties including general practice, paediatrics and
psychiatry require their trainees to appreciate some of the global health issues that they
encounter during their practice. However, there is no uniform programme of postgraduate
8Burnett,A.,&Peel,M.(2001).Healthneedsofasylumseekersandrefugees.BritishMedicalJournal,322(7285),544.9Carlsson,J.M.,Mortensen,E.L.,&Kastrup,M.(2005).Afollow-upstudyofmentalhealthandhealth-relatedqualityoflifeintorturedrefugeesinmultidisciplinarytreatment.TheJournalofnervousandmentaldisease,193(10),651-657.10http://www.fph.org.uk/uploads/bs_aslym_seeker_health.pdf11Woodhead,D.(2000).Thehealthandwell-beingofasylumseekersandrefugees.King'sFund.12Laban,C.J.,Komproe,I.H.,Gernaat,H.B.,&deJong,J.T.(2008).Theimpactofalongasylumprocedureonqualityoflife,disabilityandphysicalhealthinIraqiasylumseekersintheNetherlands.Socialpsychiatryandpsychiatricepidemiology,43(7),507-515.13http://www.rcpsych.ac.uk/pdf/Appendix%201_EPA%20statement%20on%20Refugees%2020151023_sent.pdf14http://www.gmc-uk.org/Tomorrow_s_Doctors_1214.pdf_48905759.pdf

MedactManchesterreport October2017
11
education for traineedoctorsonmanaging the specific health issues facedbyasylum seekers
withintheUK.
2.4AsylumandaccesstoNHShealthcare
Inadditiontothelackoftrainingonthespecifichealthneedsoftheasylumseekerpopulation,
therehasbeenconsiderableconfusionamonghealthcareprofessionalsaboutwhichgroupsare
eligible to access NHS care.15 Lack of training, confusion about definitions, lack of clarity on
HomeOfficedecisionsandmultiple changes in legislationhavemade it extremelydifficult for
healthcareprofessionalstokeepuptodateoneligibilityforhealthcare.Thereisevidencethat
asylumseekersandrefugeesdeferseekinghealthcarebecauseofconcernsabout immigration
status,possiblechargesandpoortreatment,allleadingtopoorerhealthoutcomesforpatients
andraisingconcernamongdoctorsabouttheirroleinassessingimmigrationstatus.16Doctorsof
theWorldrecentlyfoundthat13%ofrefugeesandasylumseekerswhoattemptedtoregister
with a local general practitioner (GP) were incorrectly refused because of their immigration
status.17Thissituationislikelytoworseninlightofrecentchangestochargingpracticesinthe
UK.FromOctober2017,chargingforhealthcarehasbeenextendedtocommunitysettingsand
costsaretobepaidupfrontbeforenon-emergencytreatmentisgiven.18Thereisconcernthat
introducing such charges will not lead to cost savings in the long term, and may negatively
impact health outcomes in some of the most vulnerable, such as pregnant women seeking
asylum.19
2.5Previousliterature
Althoughonerecentstudyhasdocumentedtheperspectivesofasmallnumberofprimarycare
providers on the barriers to providing healthcare to migrant patients, including asylum
15http://www.rcgp.org.uk/policy/rcgp-policy-areas/asylum-seekers-and-vulnerable-migrants.aspx16AsylumMattersreport17http://www.independent.co.uk/news/uk/health-concerns-as-english-gp-surgeries-refuse-to-register-asylum-seekers-and-refugees-a7008081.html18https://www.gov.uk/government/publications/guidance-on-overseas-visitors-hospital-charging-regulations/summary-of-changes-made-to-the-way-the-nhs-charges-overseas-visitors-for-nhs-hospital-care19FarringtonR,SalehS,CampbellSetal.ImpactofproposaltoextendchargingforNHSinEngland.Lancet2016;388:459

MedactManchesterreport October2017
12
seekers,20 to our knowledge, there have been no studies examining the perspectives of
healthcareprofessionals inotherspecialtiesonthe issuessurroundingprovidinghealthcare to
refugees and asylum seekers. Furthermore,we are unaware of any evidence that specifically
examines trainees’ experiences indealingwith thehealth issuesexperiencedby refugeesand
asylum seekers. In view of this gap in our knowledge, coupled with an appreciation that as
global displacement continues to rise, and the increasing pressures on UK healthcare
professionalstoactasgatekeeperstohealthcareforasylumseekersandrefugees,wesetoutto
examinehealthcareprofessionals’ currentunderstandingof refugeeandasylumseekerhealth
issues,identifyanytrainingneedsandexploreavenuesforfutureresearch.
3.AimsThissurveyaimedto:
1. examine NHS healthcare professionals’ current understanding of refugee and asylum
seekerhealthissues
2. identifyhealthcareprofessionals’trainingneedsonrefugeesandasylumseekerhealth
andexplorehowhealthcareprofessionalswouldlikethesetrainingneedstobemet;
3. identifyavenuesforfutureresearchonrefugeeandasylumhealthintheUK.
4.Methods4.1Pilotstudy
Tohelpusdevelopour survey,we conductedapilot surveyofHCPs. In this, individualswere
asked about their experiences of treating refugees and asylum seekers. Key themes that
emerged fromthis survey included: theeligibilityofdifferentgroups forNHScare, identifying
andtreatingvictimsoftorture,andtheneedfortrainingtoaddressknowledgegaps.
20LindenmeyerA,RedwoodS,GriffithLetal.Experiencesofprimarycareprofessionalsprovidinghealthcaretorecentlyarrivedmigrants:aqualitativestudy.BMJOpen2016;6:e012561
MedactManchesterreport October2017
13
4.2Surveydevelopment
Followingthepilotsurvey,tenmultiplechoicesurveyquestionsweredevelopedaroundthese
key themes (Appendix A). The online software SurveyMonkeywas used to create the survey.
Thequestions focussedonHCPs’understandingof thedefinitionsof,andhealthcarerightsof,
asylum seekers and refugees, as well as exploring individuals’ professional experiences of
workingwiththevictimsoftorture.Thequestionnairewasdesignedtobeconciseandquickto
completeinordertomaximiseresponserate.Thequestionswerepeerreviewedpriortosurvey
distributionbyaGPwithspecialistexpertiseinmigranthealthandmedicaleducation.
4.3Samplingmethod
In order to reach as many participants as possible, we employed an opportunistic sampling
method. A hyperlink to the survey was distributed to over 1000 HCPs in the NorthWest of
England throughpre-existinghospitalemaildistribution lists, traineeemail lists, locumagency
emaillists,socialmediaandpersonalcontactswiththeauthors.
4.4Datacollection
Results were collected over 30 days in September 2016. SurveyMonkey software provided
overall responses to eachof the10questions. Responseswere further evaluatedby gradeof
trainingandspecialty.Responderswerebrokendownintothefollowingspecialtygroups:GPs;
hospitalmedicine;paediatrics;mentalhealthprofessionals,andotherhospital specialties.The
followinggradedistinctionsweremade:foundationyeartrainee;specialisttrainee;consultant;
qualified GPs and nurses and other health professionals (for brevity hereafter referred to as
alliedhealthcareprofessionalsorAHPs).Whileresponseswereanonymous,participantswere
askedtodisclosetheirspecialtyandgradetoallowstratificationoftheresultsformoretargeted
educationalinterventions.
MedactManchesterreport October2017
14
5.Results
5.1Surveyresponses
Keyfindings
● 198peoplerespondedtothesurvey
● Theapproximateresponseratewas20%
● Participantsincludeddoctors,nursesandAHPsfromavarietyofspecialitiesandgrades
ofexperience.
198peoplerespondedtothesurvey(Tables1and2).Respondersweremostlydoctors,witha
smallernumberofnursesandAHPs.Gradeof trainingamongdoctorsvaried from foundation
doctors to consultants and among nurses from Band 5 to Band 8 (Table 1). Allied health
professionals who answered the survey included two psychologists, a safeguarding children
practitionerandanNHSmanager.Specialtybackgroundswhereencounterswithasylumseekers
maybemorecommon, suchas generalpractice,mentalhealth,paediatricsand sexualhealth
andgenitourinarymedicine,werewellrepresentedamongresponders.Inaddition,therewere
responders from a wide range of other specialty backgrounds including oncology, renal
medicine,strokemedicine,geriatrics,occupationalmedicine,orthopaedics,infectiousdiseases,
surgery, anaesthetics, radiology and emergency medicine. Only one responder declared a
specialist interest in working with refugees and asylum seekers. Three responders failed to
specifyagradeoraspecialty.
The approximate response rate to the survey was 20% (198 HCPs from approximately 1000
contacted).
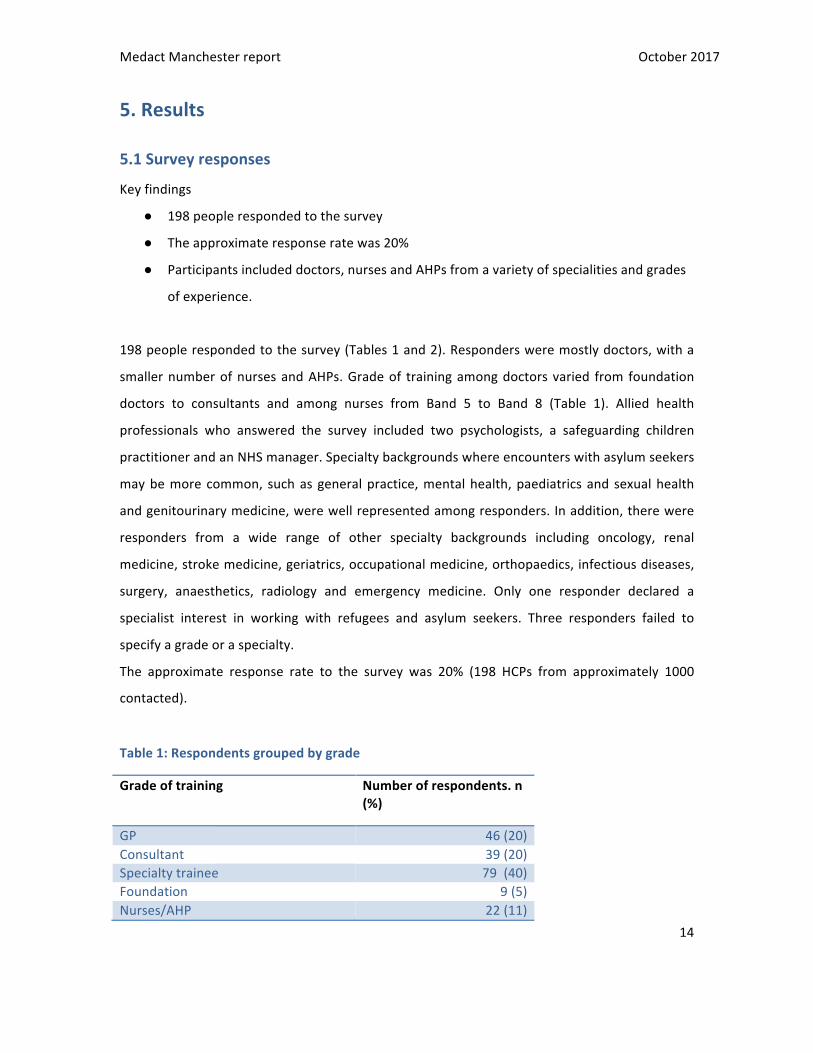
Table1:Respondentsgroupedbygrade
Gradeoftraining Numberofrespondents.n(%)
GP 46(20)Consultant 39(20)Specialtytrainee 79(40)Foundation 9(5)Nurses/AHP 22(11)
MedactManchesterreport October2017
15
Unknown 3(2)Total 198
Table2:Respondentsgroupedbyspecialty
Specialty NumberofrespondentsGP 48(24)Hospitalmedicine 50(25)Mentalhealth 40(20)Paediatrics 16(8)Otherhospital 41(21)Unknown 3(2)Total 198
5.2HCPs’understandingofthedefinitionsofimmigrationstatus
Keyfindings:
● Only21% (n=41)of respondents felt confident indefining the terms “asylum seeker”,
“failedasylumseeker”and“refugee”.
● GPswerethemostconfidentintheirknowledgeofthesedefinitions,whilstfoundation
doctorsweretheleastconfident.
● Havingpreviously treatedvictimsof torturedidnot increase individuals’confidence in
definingdifferentgroups.
Of 198 respondents, 21% (n=41) felt confident in defining the terms “asylum seeker, “failed
asylumseeker”,“economicmigrant”and“refugee”.63%(n=125)hadsomeideaofterminology
butwerenotconfident,and16%(n=32)werenotsureofthedifferences(figure1).

MedactManchesterreport October2017
16
Figure1:Responsestothequestion"Howconfidentareyouaboutthedifferentdefinitionsof"refugee","asylumseeker"and"failedasylumseeker"
GPsweremost likely to describe themselves as confident in defining the difference between
refugees,asylumseekers,andfailedasylumseekers,with37%(n=17)ofGPssayingtheywere
confident.Foundationtraineesweretheleastconfidentwithdefinitions,with22%(n=2)being
unsureofthedifference.
HCPswhohadpreviouslybeeninvolvedintreatingvictimsoftorturewerenomoreconfidentin
theirabilitytodefinedifferentmigrantgroups.Approximatelyonethird(n=27)ofrespondents
whohadpreviouslytreatedtorturevictimsdescribedthemselvesasconfidentwhereasanother
third(n=24)wereunsuresureofthedifference.
5.3HCPs’understandingofmigrantgroups’eligibilityforNHScare
PrimaryCare
Keyfindings:
0 20 40 60 80 100 120 140
Confident- Iwouldbeabletoexplainthedifference
Someidea- Imayneedtorevisethedefinitionsbuthavesomeunderstanding
Notsureofthedifference
Definining"asylumseekers","refugees"and"failedasylumseekers"
MedactManchesterreport October2017
17
● Atthetimeofsurveydistribution,NHSregulationsstatedthatrefugees,asylumseekers,
andfailedasylumseekerswerealleligibleforfreeprimarycare.
● Only26%ofrespondents(n=51)correctlyidentifiedrefugees,asylumseekers,andfailed
asylumseekersaseligibleforfreeprimarycare.
● 62% (n=123) of respondents believed that failed asylum seekerswere not eligible for
freeprimarycare.
● 28%(n=56)ofrespondentswereunsureabouteligibilityforfreeprimarycare
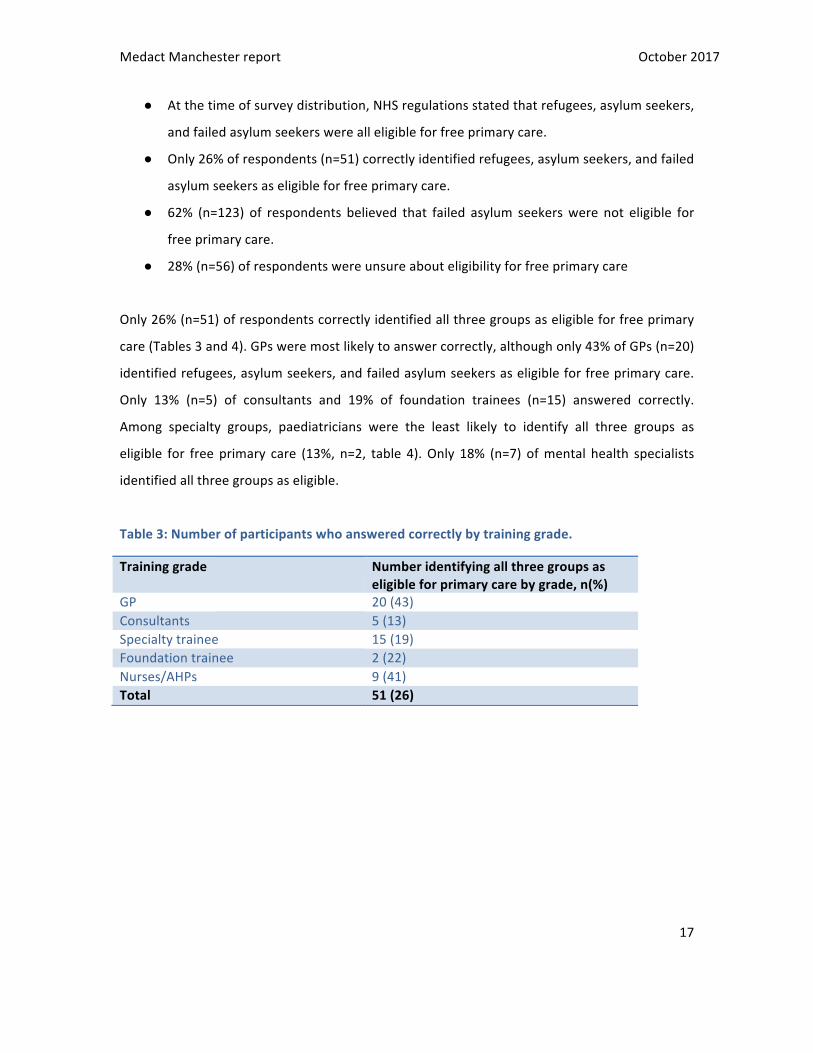
Only26%(n=51)ofrespondentscorrectlyidentifiedallthreegroupsaseligibleforfreeprimary
care(Tables3and4).GPsweremostlikelytoanswercorrectly,althoughonly43%ofGPs(n=20)
identifiedrefugees,asylumseekers,andfailedasylumseekersaseligibleforfreeprimarycare.
Only 13% (n=5) of consultants and 19% of foundation trainees (n=15) answered correctly.
Among specialty groups, paediatricians were the least likely to identify all three groups as
eligible for free primary care (13%, n=2, table 4).Only 18% (n=7) ofmental health specialists
identifiedallthreegroupsaseligible.
Table3:Numberofparticipantswhoansweredcorrectlybytraininggrade.
Traininggrade Numberidentifyingallthreegroupsaseligibleforprimarycarebygrade,n(%)
GP 20(43)Consultants 5(13)Specialtytrainee 15(19)Foundationtrainee 2(22)Nurses/AHPs 9(41)Total 51(26)

MedactManchesterreport October2017
18
Table4:Numberofparticipantswhoansweredcorrectlybyspecialty.
Specialty Numberofparticipantsidentifyingallthreegroupsaseligibleforprimarycarebyspecialty,n(%)
GP 20(42)Hospitalmedicine 10(20)Mentalhealth 7(18)Otherhospital 12(29)Paediatrics 2(13)Total 51(26)
62% (n=123) respondents thought that asylum seekers whose claims for asylum had been
refusedbytheHomeOfficewerenoteligibleforfreeprimarycare,whilstrefugeesandasylum
seekerswithongoingclaimswereeligible.Onlyonehealthcareprofessional surveyed thought
thatnoneof thegroupswasentitledto freeGPservices.Almosta thirdof respondents (28%,
n=56)wereunsureabouttheeligibilityofthesegroupsforfreeprimarycare.
FreeEmergencyCare
Keyfindings:
● Atthetimeofsurveydistribution,NHSregulationsstatedthatrefugees,asylumseekers,
andfailedasylumseekerswerealleligibleforfreeemergencycare.
● 68%(n=128)ofrespondentsansweredcorrectly, identifyingallthreegroupsaseligible
forfreeemergencyhealthcare.
● Onethirdofrespondents(n=60)answeredincorrectlyanddidnotrecognisethatfailed
asylumseekersareentitledtofreeemergencycare.
Over two thirds (68%, n=128) of respondents identified all three groups of refugees, asylum
seekersandfailedasylumseekersaseligibleforemergencyhealthcarefreeofcharge(Tables5
and6).Onethirdofrespondents (n=60,32%)didnot identify failedasylumseekersaseligible
forfreeemergencyNHScare.

MedactManchesterreport October2017
19
Table5:Numberofparticipantsstatingrefugees,asylumseekersandfailedasylumseekersentitledtofreeemergencycare,bygrade.
Numberidentifyingallthreegroupsaseligibleforemergencycarebygrade,n(%)
GP 36(78)Consultant 23(59)Specialtytrainee 49(62)Foundationtrainee 5(56)Nurses/AHPs 15(68)Total 128(68)
Table6:Numberofparticipantsstatingrefugees,asylumseekersandfailedasylumseekersentitledtofreeemergencycare,byspecialty.
Specialty Numberofparticipantsidentifyingallthreegroupsaseligibleforemergencycarebyspecialty,n(%)
Generalpractice 37(77)Hospitalmedicine 34(68)Mentalhealth 23(58)Otherhospital 26(63)Paediatrics 8(50)Total 128(68)
Grade of training did not appear to impact ability to identify those groups eligible for free
emergencycare;knowledgeappearedtobesimilarbetweenfoundationtrainees(56%,n=5)and
consultants (59%, n=23). WhilstmostGPs and hospital doctors surveyed knew that all three
groups were eligible for free emergency care, only 50% (n=8) of paediatricians answered
correctly(Table6).
Freenon-emergencycare
Keyfindings
● At the time of survey distribution, NHS regulations stated that refugees and asylum
seekers were eligible for non-emergency hospital care. In Scotland andWales, failed
asylumseekerswereentitled to freenon-emergency secondary care. InEngland,only
failed asylum seekers who received section 4(2) support from the Home Office or

MedactManchesterreport October2017
20
section21support froma localauthoritywereentitled to freesecondaryhealthcare.
Failed asylum seekers were entitled to complete any course of treatment already
underwaybeforetheirapplicationwasrefused,freeofcharge.
● 32% of respondents (n=59) were unsure which migrant groups were entitled to free
non-emergencyNHScare.
● 4%(n=7)believednoneofthegroupswereentitledtofreenon-emergencyNHScare.
32% of respondents (n=60) said they were unsure which groups were entitled to free non-
emergency NHS care (Figure 2). Just over half of respondents answered correctly, with 56%
(n=107) identifying refugeesandasylumseekersaseligible for freenon-emergencyNHScare.
Seven(4%)saidnoneofthegroupswereentitledforfreenon-emergencycare(Figure2).
Figure2:Overallresponsestothequestion'whichgroupsareentitledtofreenon-emergencyNHScare'?
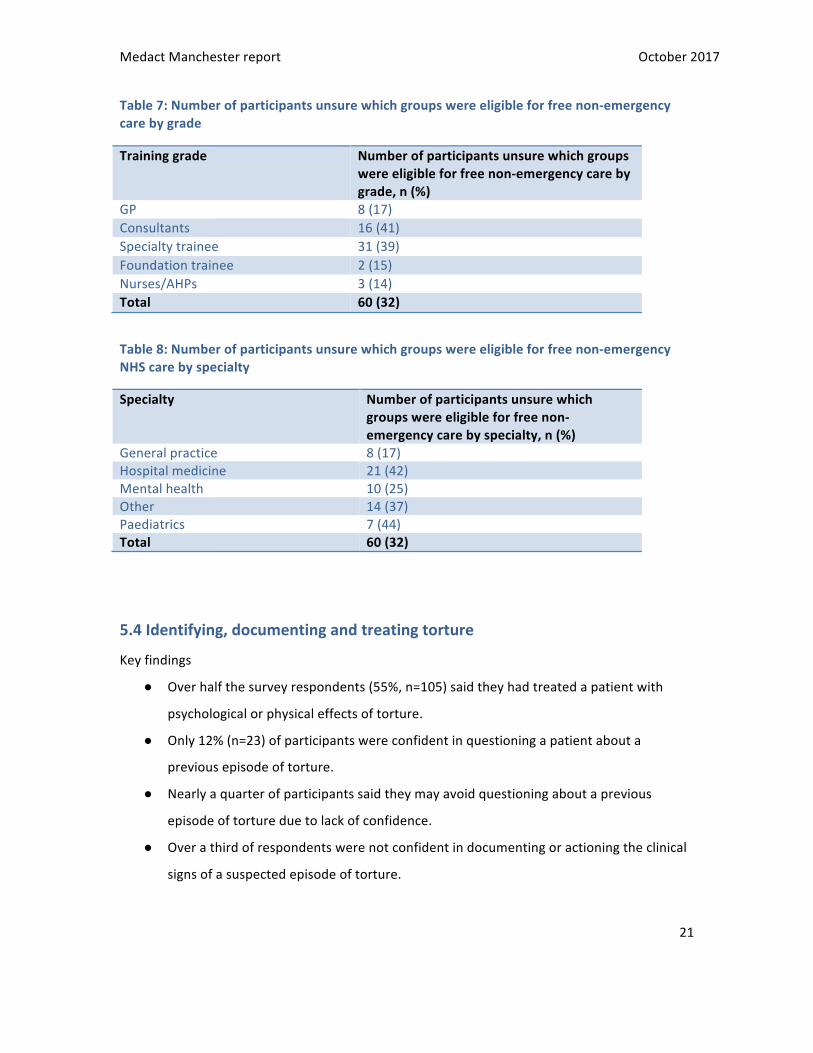
41%ofconsultants(n=16)and39%(n=31)ofspecialtydoctorswereunsurewhichgroupswere
eligible toaccessnon-emergencycare (Table7).Ratesofuncertaintyabouteligibility fornon-
emergency NHS care were high among HCPs, ranging from 25% (n=10) for mental health
professionalsto44%(n=7)forpaediatricians(Table8).
0 20 40 60 80 100 120 140
Asylumseekers
Refugees
Failedasylumseekers
Noneoftheabove
Notsure
Whichgroupsareentitledtofreenon-emergencyNHScare?
MedactManchesterreport October2017
21
Table7:Numberofparticipantsunsurewhichgroupswereeligibleforfreenon-emergencycarebygrade
Traininggrade Numberofparticipantsunsurewhichgroupswereeligibleforfreenon-emergencycarebygrade,n(%)
GP 8(17)Consultants 16(41)Specialtytrainee 31(39)Foundationtrainee 2(15)Nurses/AHPs 3(14)Total 60(32)
Table8:Numberofparticipantsunsurewhichgroupswereeligibleforfreenon-emergencyNHScarebyspecialty
Specialty Numberofparticipantsunsurewhichgroupswereeligibleforfreenon-emergencycarebyspecialty,n(%)
Generalpractice 8(17)Hospitalmedicine 21(42)Mentalhealth 10(25)Other 14(37)Paediatrics 7(44)Total 60(32)
5.4Identifying,documentingandtreatingtorture
Keyfindings
● Overhalfthesurveyrespondents(55%,n=105)saidtheyhadtreatedapatientwith
psychologicalorphysicaleffectsoftorture.
● Only12%(n=23)ofparticipantswereconfidentinquestioningapatientabouta
previousepisodeoftorture.
● Nearlyaquarterofparticipantssaidtheymayavoidquestioningaboutaprevious
episodeoftortureduetolackofconfidence.
● Overathirdofrespondentswerenotconfidentindocumentingoractioningtheclinical
signsofasuspectedepisodeoftorture.

MedactManchesterreport October2017
22
Over half of respondents (n=105, 55%) said they had treated a patientwith psychological or
physicaleffectsoftorture(Figure3).
Figure 3: Responses to the question 'have you ever treated a patient with physical or psychological effects oftorture?'
More experienced doctors were most likely to have treated victims of torture, with 64% of
consultants and 65% of GPs saying that they had treated these patients (Table 9). However,
treating individualswithpsychologicalorphysicaleffectsof torturewasnot rareamongother
HCPs,with47%ofspecialtydoctors,55%ofnurses/AHPs,and11%offoundationtraineessaying
theyhadtreatedatorturevictimatsometime(Table9).
0 20 40 60 80 100 120
Yes
No
Notsure
Haveyouevertreatedapatientwithphysicalorpsychologicaleffectsoftorture?

MedactManchesterreport October2017
23
Table9:Participantswhohadpreviouslytreatedavictimoftorturebytraininggrade
Traininggrade Numberofparticipantswhohadpreviouslytreatedavictimoftorture,n(%)
GP 30(65)Consultant 25(64)Specialtytrainee 37(47)Foundation 1(11)Nurse/AHP 12(55)Total 105(55)
Onlyaminorityofrespondentsfeltconfidentquestioningapatientaboutapreviousepisodeof
torture.Only23(12%)saidtheywereconfidentquestioningapatientwhohadpreviouslybeen
tortured,with56%able,but lessconfident thannormal (Figure4).Of the23respondents felt
confident questioning patients about previous torture, 91% (21 of 23) had previously been
involvedincaringforpatientsknowntobetorturevictims.
Figure4:Responsestothequestion‘howconfidentwouldyoube inquestioningapatientonpreviouseffectsoftorture?’
Over a fifthof all respondents (22%,n=43) said that theydidnot feel competentquestioning
patients about previous torture, and so may avoid this. Foundation trainees (78%, n=7) and
specialtytrainees(25%,n=20)weremostlikelytoavoidaskingabouttorture.
0 10 20 30 40 50 60 70 80
Confident
Lessconfidentthannormal,butstillable
Iwouldnotknowhowtodocumentandactionfindings
Notsure
Howconfidentwouldyoufeeldocumentingandactioningclinical
evidenceoftorture?

MedactManchesterreport October2017
24
Confidenceratesindocumentingandactioningclinicalevidenceoftorturewerelow.Only19%
(n=37)of respondents said theywere confidentdoing this,with33% (n=66) saying theywere
lessconfidentbutstillable,and36%(n=72)sayingtheywouldnotknowhowtodocumentand
actionevidenceoftorture(Figure5).
Figure5:Responsestothequestion‘howconfidentwouldyoufeeldocumentingandauctioningclinicalevidenceoftorture?’
Similarly, levels of confidence in documenting and acting on clinical evidenceof torturewere
low across all training grades (range of ‘confident’ responses from 0-23%). In general, more
experienced doctorsweremost comfortable, however only 22% (n=10) of GPs, 23% (n=5) of
AHPsand21%(n=8)ofconsultantsdescribedthemselvesasconfident.
5.5HCPs’trainingneeds
Keyfindings
● 88%(n=164)ofparticipantsfelttheywouldbenefitfromfurthertrainingonissues
surroundingasylumseekerandrefugeehealth
● 79%(n=146)saidtheywouldprefertrainingledbyanexpertinthefield.
0 10 20 30 40 50 60 70 80
Confident
Lessconfidentthannormal,butstillable
Iwouldnotknowhowtodocumentandactionfindings
Notsure
Howconfidentwouldyoufeeldocumentingandactioningclinical
evidenceoftorture?
MedactManchesterreport October2017
25
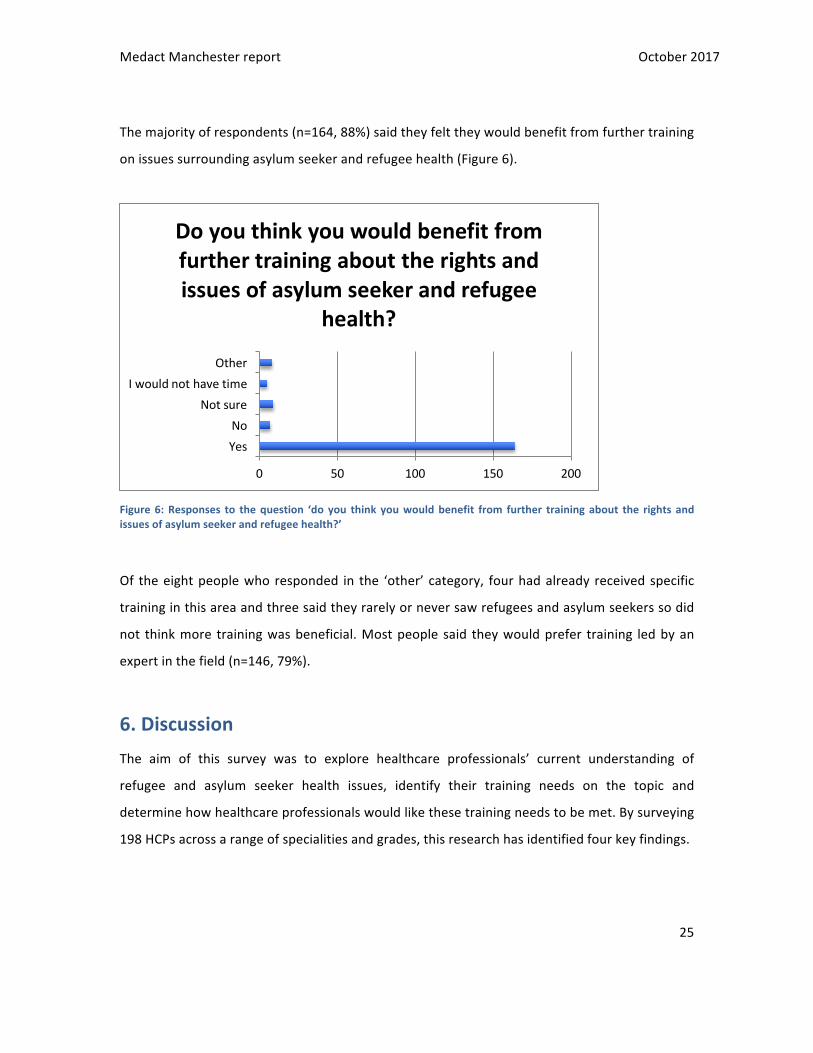
Themajorityofrespondents(n=164,88%)saidtheyfelttheywouldbenefitfromfurthertraining
onissuessurroundingasylumseekerandrefugeehealth(Figure6).
Figure6:Responses to thequestion ‘do you think youwouldbenefit from further trainingabout the rights andissuesofasylumseekerandrefugeehealth?’
Of theeightpeoplewhoresponded in the ‘other’ category, fourhadalready receivedspecific
traininginthisareaandthreesaidtheyrarelyorneversawrefugeesandasylumseekerssodid
not thinkmore trainingwasbeneficial.Mostpeople said theywouldprefer training ledbyan
expertinthefield(n=146,79%).
6.DiscussionThe aim of this survey was to explore healthcare professionals’ current understanding of
refugee and asylum seeker health issues, identify their training needs on the topic and
determinehowhealthcareprofessionalswouldlikethesetrainingneedstobemet.Bysurveying
198HCPsacrossarangeofspecialitiesandgrades,thisresearchhasidentifiedfourkeyfindings.
0 50 100 150 200
YesNo
NotsureIwouldnothavetime
Other
Doyouthinkyouwouldbenefitfromfurthertrainingabouttherightsandissuesofasylumseekerandrefugee
health?

MedactManchesterreport October2017
26
6.1HCPshavelimitedunderstandingofasylumandrefugeeterminology
HCPshaveapoorunderstandingofthedefinitionsofthesegroups.Only21%ofrespondentsfelt
confidentdifferentiatingbetweenthegroups‘asylumseeker’,‘failedasylumseeker’,‘economic
migrant’, and ‘refugee’, with 61% having only some idea of terminology. Though GPs rated
themselvesmostabletodifferentiatedifferentgroups,only37%ofthisgroupfelt ‘confident’.
ThisresponsemayreflectHCPs’approachtopatientcare,which,inaccordancewiththeGMC’s
‘Good Medical Practice’ should: ‘treat patients and colleagues fairly and without
discrimination’.21
However, under recent government changes in NHS charging regulations, some groups of
asylumseekersandmigrantwillnowbesubjecttoup-frontchargingforarangeofcommunity
andhospitalhealthservicesinEngland.22Moreover,thelegalresponsibilityforidentifyingthese
patientsnowlieswiththehealthcareprovider;inshort,patientswillneedtoprovideHCPswith
documentationtoprovetheyareentitledforNHScarebeforetheycanbetreated.Asidefrom
thedeeplyproblematicmoralimplicationsofapolicythatextends,andshifts,theroleofHCPs
to that of immigration officers, this research identifies practical difficulties with these new
regulations.Putsimply,theHCPsinoursurveywereunclearaboutbasicterminologythatiskey
to identifying individuals subject to charging.Considerable resource is likely tobe required to
addressthistrainingneed,toensureadherencetotherulesof‘GoodMedicalPractice’outlined
above,andpreventprofilingofpatients.
6.2HCPsareunclearaboutwhoiseligibleforNHScare
Onlyaminorityofrespondentswereawareof theNHSregulations inplaceat thetimeof the
survey regarding access to NHS care Only 26% of respondents identified all three groups as
beingeligible for freeprimarycareandtherewerehigh levelsofuncertaintyregardingwho is
eligible for free non-emergency secondary health care, even amongst senior clinicians.
Worryingly, 32% of respondents were not aware that asylum seekers are eligible for free
emergencyNHScareirrespectiveoftheirimmigrationstatus.Ofsimilarconcern,only42%ofGP
respondents were aware that all forced migrants are eligible for free primary care. By21GMC:GoodMedicalPractice22https://www.gov.uk/guidance/nhs-entitlements-migrant-health-guide

MedactManchesterreport October2017
27
highlightingasignificantknowledgegapamongstcliniciansintheirownfieldofexpertise,these
resultssupportandexpandonthefindingsoftheaforementionedDoctorsoftheWorldstudy,
suggestingthatlackofunderstandingofNHSeligibilityregulationsisafurtherbarriertotimely
access to healthcare among these vulnerable groups. Further academic enquiry into the
treatment of asylum seekers across a range of care settings, especially emergency care, is
needed,asbarriers tohealthcareamongthesegroupsmay leadtopreventablemorbidityand
mortality.ThisraisesimportantmoralandethicalquestionsforHCPsdelayingtreatmentonthe
basisofimmigrationstatus.Furtherinvestigationisrequiredexaminingwhetherlong-termcost
effectsofdelaysintreatmentwillneutraliseanyshort-termsavingsmadebyrestrictingaccess
toservices.
6.3NHSHCPsaretreatingpatientswhohavebeensubjecttotorture
Over half of the survey respondents (55%, n=105) said they had treated a patient with
psychologicalorphysicaleffectsoftorture.Tortureisthoughttobecommoninasylumseekers
andrefugees, thoughprevalencevariesacrossstudies,dependingonthedefinitionof torture,
samplingandreportingmethods.23TwoprevalencestudiesfromamentalhealthclinicinBoston
USAidentifiedtheprevalenceoftortureas84.3%and86.2%inaconveniencesampleofaround
200 asylum seekers.24 Torture prevalence is also dependent on the country of origin of the
asylum seeker or refugee; for example, in one study twice as many Afghan asylum seekers
reportedtortureincomparisontothosefromIraq(67.3%and30.6%respectively).25,26
23Kalt,A.,Hossain,M.,Kiss,L.,&Zimmerman,C.Asylumseekers,violenceandhealth:Asystematicreviewofresearchinhigh-incomehostcountries.AmericanJournalofPublicHealth2016;103(3):e30–42.24PiwowarczykL.AsylumseekersseekingmentalhealthservicesintheUnitedStates:clinicalandlegalimplications.JNervMentDis.2007Sep;195(9):715-2225Laban,C.J.,Gernaat,H.B.,Komproe,I.H.,vanderTweel,I.,&DeJong,J.T.PostmigrationlivingproblemsandcommonpsychiatricdisordersinIraqiasylumseekersintheNetherlands.JNervMentDis.2005;193(12):825-83226Ichikawa,M.,Nakahara,S.,&Wakai,S.Effectofpost-migrationdetentiononmentalhealthamongAfghanasylumseekersinJapan.AustralianandNewZealandJournalofPsychiatry.2006;40:341-346.
MedactManchesterreport October2017
28
Despitethehighprevalenceoftortureamongstasylumseekersandrefugees,andthehighrates
of clinical encounters with the victims of torture reported in this survey, the majority of
respondentsdidnotdescribe themselves as confident in enquiring about torture.Worryingly,
23%ofrespondentsstatedthat,asaconsequenceofthis lackofconfidence,theymightavoid
askingquestionsaboutexperiencesoftorture.Similarly,confidencetodocumentandactupon
evidenceoftorturewaslowacrossallspecialtiesandallgrades;only20%ofrespondersstated
they were ‘confident’. This lack of confidence in identifying victims of torture is particularly
concerningsince thechanges in legislationmade inAugust2017 thatmandate thatvictimsof
torture,femalegenitalmutilation,anddomesticorsexualviolencearenotrequiredtopayfor
treatmentofanyconditioncausedbythatviolence.27Thepsychologicalandphysicalsequelae
of torture can be profound, and include treatable conditions such as major depression and
PTSD.28Appropriatelydocumentingverbalaccountsandphysicalevidenceof torturecanhave
life-alteringimplications,especiallyforasylumseekerswhoselegalrighttoremainintheUKis
uncertain. The lack of knowledge and confidence highlighted in this survey has serious
implications;byavoidingquestionsabouttortureinhigh-riskpatients,HCPsmaydenyvictimsof
torturetheirhealthcareentitlements.Furthermore,theymayhinderanindividuals’immigration
applicationifthetorturegoesunrecognised.
6.4HCPswantmoretrainingonasylumandrefugeehealth
The vast majority of respondents stated they would benefit from further training on issues
surrounding asylum seeker and refugee health,withmost (80%) preferring training led by an
expert in the field. These findings extend across a broad range of specialties and experience.
Despite a relative increase in confidenceamongmore seniorhealthprofessionals, there is an
acceptanceoftheneedforeducationacrosstheboard.Thisisevenmorepressinginlightofthe
27https://www.gov.uk/government/publications/guidance-on-overseas-visitors-hospital-charging-regulations/summary-of-changes-made-to-the-way-the-nhs-charges-overseas-visitors-for-nhs-hospital-care28SteelZ,CheyT,SiloveD,MarnaneC,BryantRA,vanOmmerenM.Associationoftortureandotherpotentiallytraumaticeventswithmentalhealthoutcomesamongpopulationsexposedtomassconflictsanddisplacement:asystematicreviewandmeta-analysis.JAMA.2009;302:537–49.

MedactManchesterreport October2017
29
recentchangestochargingwhichplaceevenmoreresponsibilityonfront-lineNHSstafftocheck
individuals’immigrationstatusesbeforeprovidingtreatment.Thesechargeswerenotinplaceat
thetimethissurveywasconducted,but,toourknowledge,theUKGovernmenthasprovidedno
specifictrainingforHCPsinlightofthechangeinlegislation.
Appropriate training and education for staff determining who is, or is not, eligible for NHS
treatment isvital.Weneedtobeabletoensurethatpatientsaretreatedfairly,promptlyand
without discrimination in accordance with their human rights and the codes of practice that
governhealthcarepracticeinthiscountry.It isalsoimperativethattherearenoinappropriate
treatmentdelaysandorincorrectchargingduetoHCPs’lackofunderstandingandknowledge.
Weneedtoensuretheprocessofeligibilityassessmentisdoneinatimelyfashion,minimising
theadditionalworkloadforalreadyoverburdenedNHSstaff,aswellassafeguardingagainstthe
profiling of individuals based on race, country of origin, religion or language, rather than in
accordancewiththelaw
7.LimitationsThesurveyhasanumberoflimitationsthatshouldbeconsideredwheninterpretingtheresults.
7.1.Samplingmethod
The samplingmethodwas opportunistic, designed to capture asmany responses as possible
within a limited timeframe and with limited resources. With this method we achieved a
responserateofaround20%(198fromapproximately1000HCPscontacted),anditispossible
thatthoserespondingtothequestionnaireactedasaself-selectinggroupwithsomedegreeof
pre-existinginterestinthetopic.
The numbers of respondents in grade and specialty sub-groups varied significantly.
Consequently, the cross-group comparisons are to be interpretedwith caution. Some groups,
suchasfoundationdoctors,wereunderrepresented(5%,n=9),whilstspecialisttraineedoctors
(40%, n=79) and consultant and GP grades (43%, n=85) represented the majority of survey

MedactManchesterreport October2017
30
respondents. Furthermore, although nurses and AHPswere included in the survey, they only
madeup11%(n=22)ofresponders.
However,theprimaryaimofthisprojectwasnottoproducehighlypoweredstatisticaldata,but
rathertoprovideanoverviewofHCPs’understandingoftheissuesaroundrefugeeandasylum
health,identifygapsintheirknowledgebaseandexploreavenuesforfurtherresearch.Thus,if
thesampledidhaveapre-existinginterestinthetopic,theprevalenceofsuchuncertaintywhen
dealingwiththesepopulationgroupsinahealthcaresettingisanimportantfinding.
Apotentialavenue for furtherworkon this topicwouldbe thedevelopmentofa surveywith
specificsamplingmethodsdesignedtoreduceanyself-selectionbiasandallowformorerobust
cross-specialty comparisons. These measures would help us to design specialty and grade-
specificinterventionsandtrainingtoincreaseHCPs’understandingandconfidenceinthisarea.
7.2Datacollection
Wedesignedasurveywithconcisequestionsandmultiplechoiceanswers.Thesurveyhasnot
been independently validated. It can be argued that asking clinicians to choose between
‘confident’ and ‘some idea’ in reference to an aspect of their clinical knowledge is not a fair
representationofrespondents’real-worldknowledgeandclinicalpractice,asthequestiononly
measures the confidence they have in their ability to cite definitions. A more accurate
knowledgeassessmentmayhavebeenachievedbyaskingparticipantstoselectthedefinitions
fromalistofoptionsortypethemfree-text.However,thechosensurveydesignofferstwokey
advantages.Firstly,itkeptthesurveysimpleandshort,akeyfactorinmaximisingresponserate.
Secondly,itmeetstheaimsofthestudy:exploringtheperspectivesofHCPs.Whilstthelackof
confidenceamongstHCPsidentifiedbythisresearchmaynotalwaystranslatetoreal-worldsub-
optimal practice, it does imply that there is a large knowledge gap among HCPs about a
populationtheyarecaringfor,theirlegalresponsibilities,andentitlementtoNHScareforthese
groupsofpatients.
MedactManchesterreport October2017
31
8.RecommendationsThisreporthashighlightedasignificantgapinHCPs’knowledgeofthehealthneedsofrefugees
and asylum seekers and their eligibility for NHS care. This appears to translate to a lack of
confidenceinidentifyingandtreatingsuchpatients.Inlightofthesefindings,andoftherecent
changes to charging for NHS care,MedactManchester recommends the following actions to
increaseawarenessoftheissuesandencouragebettertrainingformedicalprofessionals.
8.1 ThereisanurgentneedfortrainingforfrontlineNHSstaffonthehealthneedsofrefugee
andasylumseekersandtheireligibilityforNHScare.
Thistrainingshouldcoverfivekeyareas:
a. understanding the complexhealthneedsof refugeesandasylumseekers, and
howtheymaydifferfromtheordinarilyresidentpopulation;
b. understanding terminology used to describe refugees and asylum seekers,
including how this may change over time. This would require a basic
understandingoftheasylumprocess;
c. exploring the moral, ethical, and legal, responsibility healthcare professionals
haveinassessingindividuals’rightstohealthcareintheUK.Thismustbedone
inkeepingwithprofessionalcodesofpracticesuchas‘GoodMedicalPractice’;
d. identifying and appropriately documenting evidence of torture. This should
include information on signposting to groups experienced in dealing with
refugeesandasylumseekerhealth;
e. we suggest this training beprovidedby individualswith experience in dealing
withthecomplexitiesofrefugeesandasylumseekerhealth.Thisshouldinclude
allstakeholders,andcouldincludeNHSprofessionals,thirdsectororganisations,
andmembersoftherefugeeandasylumseekercommunity.
8.2 Refugeeandasylumhealthshouldbeintroducedasacoretopicinmedicaleducation
fromundergraduateleveltoseniorlevelcontinuingprofessionaldevelopment.

MedactManchesterreport October2017
32
8.3 ThereisaneedforfurtherresearchonHCPsandrefugeeandasylumhealthintheUK
Avenuesforfurtherresearchinclude:
b. ExpandingtolookatHCPsinotherregionsoftheUK
c. GreaterinclusionofHCPsotherthandoctorse.g.nursing,midwifery,dentistryand
otherAHPs
d. ExploringtheimpactofthenewlegislationonHCPs’understandingofrefugeeand
asylumhealth
8.4Refugeesandasylumseekersmustcontinuetoreceivehealthcareinlinewiththeirhuman
rightsandthecodesofpracticethatgoverntheprovisionofhealthcareintheUK.
MedactManchesterreport October2017
33
AppendixA:SurveyQuestions
MedactRefugeeandAsylumSeekerHealthSurvey
1. Pleaseenteryourgradeandspecialty2. WhichgroupsareentitledtofreeGPservices?(Selectallthatapply)
a. Asylumseekersb. Refugeesc. ‘Failed’asylumseekersd. Noneoftheabovee. Notsure
3. Howconfidentareyouaboutthedifferentdefinitionsofasylumseeker,refugee,‘failed’asylumseeker,andeconomicmigrant?
a. Confident–Iwouldbeabletoexplainthedifferenceb. Someidea–Imayneedtorevisethedefinitionsbuthavesomeunderstandingc. Notsureofthedifferenced. Other(pleasespecify)
4. Whichgroupsareentitledtofreeemergencycare?(Selectallthatapply)a. Asylumseekersb. Refugeesc. ‘Failed’asylumseekersd. Noneoftheabovee. Notsure
5. Whichgroupsareentitledtofreenon-emergencyNHScare?(Selectallthatapply)a. Asylumseekersb. Refugeesc. ‘Failed’asylumseekersd. Noneoftheabovee. Notsure
6. Haveyouevertreatedapatientwithphysicalorpsychologicaleffectsoftorture?a. Yesb. Noc. Notsure
7. Howconfidentwouldyoufeelquestioningapatientaboutprevioustorture?a. Confident–nodifferenttonormalclinicalenquiryb. Lessconfidentthannormalbutstillablec. Notcompetent–Imayavoidquestionsaboutprevioustortured. Notsuree. Other(pleasespecify)
8. Howconfidentwouldyoufeeldocumentingandactioningclinicalevidenceoftorture?a. Confident
MedactManchesterreport October2017
34
b. Lessconfidentthannormal–butstillablec. Iwouldnotknowhowtodocumentandactionfindingsd. Notsuree. Other(pleasespecify)
9. Doyoufeelthatyouwouldbenefitfromfurthertrainingabouttherightsandissuesofasylumseekerandrefugeehealth?
a. Yesb. Noc. Notsured. Iwouldnothavetimee. Other(pleasespecify)
10. Whatformatofeducationalsupportwouldbemostusefultoyou?a. Trainingsessionledbyexpertinthefieldb. Onlineeducationalmaterialc. Posterorflyerd. Helpline/help-emaile. Noneoftheabove
AppendixB:ResponderFeedback
Thankyousomuchfortakingthetimetocompletethesurvey.Thiswillhelpustoseewhat
medicalprofessionalsalreadyknow,aswellaswhatkindoftrainingmightbeusefulinthe
future.Wethoughtitmightbehelpfulforustoprovidetheanswerstosomeofthequestionsaskedin
thesurvey.Sohereyougo.
(N.B.Ifyouwouldlikeustoemailyoua1pagehandoutwiththeinformationbelowand/or
wouldliketojointheMedactManchesteremaillist,thenpleaseemail
Definitions
Accordingtothedictionary,arefugeeissimplyapersonwhoisfleeingtheirhomeforrefugeor
safety.FollowingthemassexodusofpeoplesfromtheirhomesafterWW2,theUNheldseveral
conventionsinordertoclarifythelegalstatusofsuchpeople.The1948UniversalDeclarationof
HumanRightsrecognisedtherightofpersonstoseekasylumfrompersecutioninother
countries.The1951RefugeeConventiondefinedarefugeeas:

MedactManchesterreport October2017
35
Apersonwhoowingtoawell-foundedfearofbeingpersecutedforreasonsofrace,religion,
nationality,membershipofaparticularsocialgrouporpoliticalopinion,isoutsidethecountryof
hisnationalityandisunableor,owingtosuchfear,isunwillingtoavailhimselfoftheprotection
ofthatcountry;orwho,nothavinganationalityandbeingoutsidethecountryofhisformer
habitualresidenceasaresultofsuchevents,isunableor,owingtosuchfear,isunwillingto
returntoit.
However,apersonwhoarrivesinanewcountryandclaimstomeettheabovedefinitionhas
notlegallygained‘refugeestatus’untilithasbeenbestoweduponhim/herbythehostcountry.
IntheUK,thisisdonebytheUKBorderAgency(UKBA).Peoplewhoarriveinthiscountryhave
toapplytotheUKBAforasylum.Whentheydoso,theyaredefinedasasylumseekers(i.e.
peoplewhoareseekingasylum/refugeestatus).IftheUKBArejectsaperson’sclaim,then
he/sheisafailedasylumseeker.
Aneconomicmigrantisapersonwhohasmovedtoanewregiontoseekanimprovementin
livingstandards,mostoftenbecausethelivingconditionsinhis/herownregionarenotstable.1
EntitlementtoNHSCare
AsylumseekersareentitledtofreehealthcarefromallNHSserviceswhiletheyarewaitingfor
theoutcomeoftheirasylumapplicationandappeals.Thosewhoseasylumapplicationhasbeen
successful(i.e.thosewhohavegainedrefugeestatus)cancontinueaccessingallhealthcare
servicesindefinitely.
Thosewhoseasylumapplicationhasbeenrefused(“failedasylumseekers”)areentitledtofree
primaryhealthcare,emergencytreatmentinA&E,testsandtreatmentforinfectiousdiseases,
familyplanning,anytreatmentforaphysicalormentalconditionresultingfromtorture,FGM,
domesticviolenceorsexualviolence,NHSdentalandeyecare,andprescriptions.Furthermore,
anyhospitaltreatmentstartingpriortoapersonbecominga“failedasylumseeker”shouldbe
continuedfreeofchargeuntilthatpersonleavestheUK.

MedactManchesterreport October2017
36
Thismeansthatfailedasylumseekersareliabletopayachargeforanynewaccesstohospital
servicesthatisnotoutlinedabove.However,trustsmustnotdelayanytreatmentdeemed
necessarypriortothepersonbeingsenthome,andcanstillprovidehealthservicesattheir
discretiontothesepatientswhenthereisnoprospectofthatpersonpayingforit.
Workingwhetherapersonfitsintooneoftheabovedefinitions,orrememberingwhetheror
notapersonisentitledtocareisNOTtheresponsibilityoftheclinician.Treatingcliniciansare
notobligatedtodeterminewhetherindividualpatientsareeligibleforfreenon-emergency
treatment,orwhethertheyareabletopayforit,beforetheyadministertreatment.Incontrast,
cliniciansmustfollowclearguidancesetoutbytheGeneralMedicalCouncilandensurethey
makethecareofthepatienttheirfirstconcern.Forthisreason,treatmentshouldbegivento
patientsbasedontheirneed,nottheirimmigrationstatus.
1Agrowingliteratureisfindingthatowingtotheongoingturmoil,particularlyinNorthAfricaandthe
MiddleEast,thedifferencebetweenaneconomicmigrantandarefugeeisbecomingincreasinglyblurred.
Thishasledtotheuseofanewterm:forcedmigrant.





























