Embed Size (px)
Citation preview

Department of Veterans Affairs Office of Inspector General
Office of Healthcare Inspections
Report No. 13-01123-249
Healthcare Inspection
Quality and Patient Safety Concerns in the Community Living Center
W.G. (Bill) Hefner VA Medical Center Salisbury, North Carolina
July 22, 2013
Washington, DC 20420

To Report Suspected Wrongdoing in VA Programs and Operations: Telephone: 1-800-488-8244
E-Mail: [email protected]
Web site: www.va.gov/oig

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Contents
Page
Executive Summary ..............................................................................................i
Purpose
Appendixes
.................................................................................................................1
Background ..........................................................................................................1
Scope and Methodology......................................................................................3
Inspection Results ...............................................................................................4
Issue 1 - Quality of Care .....................................................................................4
Issue 2 - Electronic Resident Monitoring System ...............................................6
Issue 3 - Rehabilitation and VERA Funding .......................................................8
Issue 4 - Staff Training and Oversight ............................................................. 10
Conclusions ....................................................................................................... 11
Recommendations ........................................................................................... 12
A. Additional Case Summaries ...................................................................... 13
B. VISN Director Comments ........................................................................... 20
C. Facility Director Comments ........................................................................ 21
C. OIG Contact and Staff Acknowledgments .................................................. 24
D. Report Distribution ...................................................................................... 25
VA Office of Inspector General

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Executive Summary
The VA Office of Inspector General (OIG) Office of Healthcare Inspections conducted an inspection in response to a complainant’s allegations of poor quality of care and patient safety concerns in the Community Living Center (CLC) at the W.G. (Bill) Hefner VA Medical Center in Salisbury, North Carolina.
We did not substantiate that patients were improperly admitted to the CLC, and as a result, did not receive appropriate treatment and services. With the exception of one case, the residents named by the complainant received appropriate care and services. In the excepted case, the resident did not receive care consistent with VHA’s defined concept of Hospice and Palliative Care. There were no order sets for managing this resident’s symptoms in the final hours, and CLC nurses expressed frustration as to their own limited level of training and preparedness in caring for hospice patients in general.
While we did not identify any actual cases of patient harm, we substantiated that a high-risk resident could wander or elope from a CLC unit and exit the building before being located. Several factors contributed to this condition including an outdated electronic monitoring system; an inadequate policy regarding the management of monitored residents; inconsistent staff practices when an exit alarm is activated; and staff training deficits. We also confirmed that some nursing staff had not received training that would have enhanced their ability to care for certain patient populations. Specific training deficits included behavior management techniques, end-of-life care provision, and post-alarm procedures related to the electronic monitoring system.
We did not substantiate that, to increase Veterans Equitable Reimbursement Allocation funding, CLC leaders admitted patients for rehabilitation even though those patients had no rehabilitation potential. We also did not substantiate that the CLC physician does not properly supervise the CLC nurse practitioners or that the geriatrics and Extended Care Chief Nurse Executive does not adequately address and follow-up on staff concerns and complaints. We did note, however, that facility leaders did not conduct a risk assessment of the electronic monitoring system in spite of ongoing safety concerns.
The Veterans Integrated Service Network and Facility Directors concurred with our recommendations and provided an acceptable action plan. (See Appendixes B and C, pages 20–23 for the Directors’ comments.) We will follow up on the planned actions until they are completed.
JOHN D. DAIGH, JR., M.D. Assistant Inspector General for Healthcare Inspections
VA Office of Inspector General i

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Purpose
The VA Office of Inspector General (OIG) Office of Healthcare Inspections conducted an inspection in response to a complainant’s allegations of poor quality of care and patient safety concerns in the Community Living Center (CLC) at the W.G. (Bill) Hefner VA Medical Center in Salisbury, NC. The purpose of the review was to determine whether the allegations had merit.
Background
The facility is a tertiary care medical center with 159 hospital and 270 CLC beds located within Veterans Integrated Service Network (VISN) 6. The facility provides inpatient and outpatient medical, surgical, rehabilitative, and long-term care services and is affiliated with Wake Forest University School of Medicine.
VHA’s transformation of the culture of care in CLCs emphasizes resident-centered care in a stimulating and home-like environment that encourages resident mobility and socialization. The CLC’s physical layout centers around a “Main Street” atrium featuring plants and trees, café-style seating, walking “paths,” and a pond. The area also includes a small retail shop, barbershop, movie theatre, and live music. The four operational CLC units, referred to as “neighborhoods,” are shaped in a horseshoe surrounding the atrium. Units 42-1C and 42-1D are located on the 1st floor and are connected by a common hallway between the units; units 42-2C and 42-2D are located on the 2nd floor and are similarly arranged. Two additional units are currently under construction. A bridge on the second floor, which overlooks “Main Street,” connects the CLC units to the onsite physical therapy clinic and other clinical and administrative areas.
The CLC’s four operational units have a mix of long term/custodial, rehabilitation, dementia care, and hospice residents. While some residents in the CLC are cognitively impaired and at-risk for wandering and elopement, a majority of the residents are not. To give non-impaired residents reasonable freedom of movement within and outside of the CLC, while also protecting impaired or otherwise at-risk residents, facility leaders eliminated secured/locked units from the CLC in May 2012 in favor of an electronic monitoring program.
Electronic wristband and anklet tracking devices are placed on patients who are cognitively impaired or otherwise at high risk for wandering or elopement. When a monitored patient attempts to leave a unit through a monitored exit, an alarm is triggered, notifying employees of the breach. Employees then redirect those patients away from exit doors. At the time of our visit, there were a total of 12 CLC residents on the electronic monitoring program.
The Associate Chief of Staff for Geriatrics and Extended Care (ACOS/G&EC) is a physician who has overall responsibility for the G&EC programs, including the CLC and
VA Office of Inspector General 1
Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Hospice House. The former physician director of the facility’s hospice program left more than 1 year ago, so the ACOS/G&EC and two geriatric nurse practitioners (NPs) provide the primary medical care to CLC and hospice-care residents. In the remainder of this report, we refer to the ACOS/G&EC as the CLCMD. We make this distinction to clarify the CLCMD’s role as a patient care provider and member of the treatment team, rather than as the G&EC Service Line director and administrator.
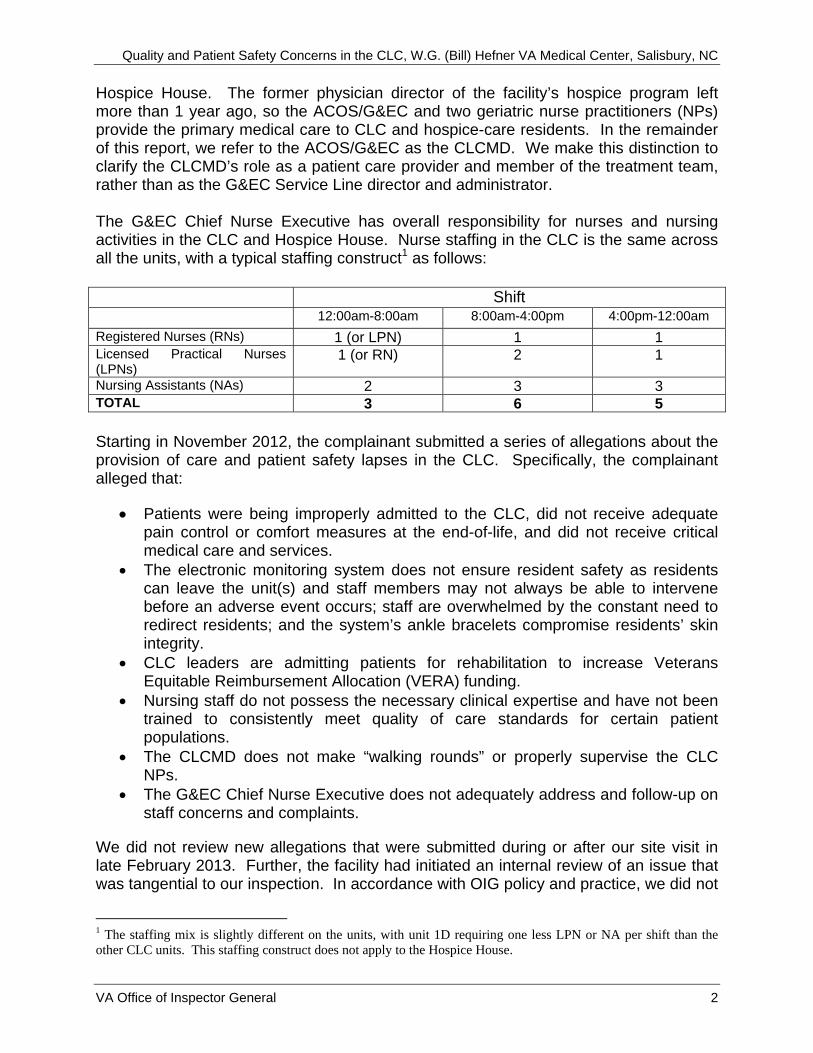
The G&EC Chief Nurse Executive has overall responsibility for nurses and nursing activities in the CLC and Hospice House. Nurse staffing in the CLC is the same across all the units, with a typical staffing construct1 as follows:
Shift 12:00am-8:00am 8:00am-4:00pm 4:00pm-12:00am
Registered Nurses (RNs) 1 (or LPN) 1 1 Licensed Practical Nurses (LPNs)
1 (or RN) 2 1
Nursing Assistants (NAs) 2 3 3 TOTAL 3 6 5
Starting in November 2012, the complainant submitted a series of allegations about the provision of care and patient safety lapses in the CLC. Specifically, the complainant alleged that:
Patients were being improperly admitted to the CLC, did not receive adequate pain control or comfort measures at the end-of-life, and did not receive critical medical care and services.
The electronic monitoring system does not ensure resident safety as residents can leave the unit(s) and staff members may not always be able to intervene before an adverse event occurs; staff are overwhelmed by the constant need to redirect residents; and the system’s ankle bracelets compromise residents’ skin integrity.
CLC leaders are admitting patients for rehabilitation to increase Veterans Equitable Reimbursement Allocation (VERA) funding.
Nursing staff do not possess the necessary clinical expertise and have not been trained to consistently meet quality of care standards for certain patient populations.
The CLCMD does not make “walking rounds” or properly supervise the CLC NPs.
The G&EC Chief Nurse Executive does not adequately address and follow-up on staff concerns and complaints.
We did not review new allegations that were submitted during or after our site visit in late February 2013. Further, the facility had initiated an internal review of an issue that was tangential to our inspection. In accordance with OIG policy and practice, we did not
1 The staffing mix is slightly different on the units, with unit 1D requiring one less LPN or NA per shift than the other CLC units. This staffing construct does not apply to the Hospice House.
VA Office of Inspector General 2

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
pursue this issue in order to permit the facility time to complete its investigation. We will review that report when it is complete.
Scope and Methodology
We conducted a site visit February 25–28, 2013. Prior to our visit, we interviewed the complainant by telephone. We reviewed facility and Veterans Health Administration (VHA) policies, directives, and handbooks; patients’ electronic health records; patient advocate and facility-level reviews and reports; nurse staff training records; and CLC and Hospice House census and nurse staffing ratios.
While on site we interviewed the Hospice House and CLC nurse managers and staff; the CLCMD; the Chief of Infectious Disease; the G&EC Chief Nurse Executive; the Chief of Facilities Management and engineering staff; the G&EC NPs, social workers, and psychologist; and other clinical and administrative staff knowledgeable about the issues. In addition, we conducted a safety and physical inspection of the CLC, Hospice House, and the connecting hallways and elevators.
We conducted the inspection in accordance with Quality Standards for Inspection and Evaluation published by the Council of the Inspectors General on Integrity and Efficiency.
VA Office of Inspector General 3

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Inspection Results
Issue 1: Quality of Care
The complainant alleged that some CLC residents were not receiving adequate care. To support the allegations, the complainant provided the names of several residents who:
a) were improperly admitted to the CLC and staff were not equipped to manage their care; or
b) did not receive adequate pain control or comfort measures at the end-of-life, and were not referred to Hospice House; or
c) did not receive critical medical care and services.
We did not substantiate allegation (1a). We found that patients were appropriately screened for admission through the designated interdisciplinary screening committee as required by policy. However, we confirmed that some CLC nursing staff had not received training to assist them in managing patients with challenging behaviors.
We substantiated that one of the residents named by the complainant in allegation (1b) did not receive care consistent with VHA’s defined concept of Hospice and Palliative Care (HPC); however, we could not confirm that he was refused admission to the Hospice House. Again, we found that some CLC nursing staff had not received specialized training that would have enhanced their ability to care for patients at the end of life.
We did not substantiate allegation (1c). The residents named by the complainant received appropriate care and services.
We reviewed the electronic health records (EHRs) of 11 residents whose names were provided by the complainant. We found one case, as noted in (1b) above, where the resident received substandard care in relation to HPC goals and policy. We discuss this resident’s case in detail below. We did not substantiate the allegations related to the remaining residents. Detailed case summaries can be found in Appendix A. Further, we found staff training deficits. See Issue 4-Staff Training and Oversight, for details.
Case 1
The patient was in his early 60s and had a complex medical history including hypertension, diabetes mellitus, vascular dementia, heart failure, and chronic pain. He had been a CLC resident since February 2012. In early October, the patient complained of chest pain, was transferred to the emergency department (ED) for evaluation, and was sent via ambulance to a private-sector hospital for emergency cardiac catheterization. The patient returned to the CLC 6 days later, but EHR documentation cited a progressive decline in his functional status and a survival prognosis estimate of “weeks to months.” The patient was found to meet criteria for
VA Office of Inspector General 4

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
outpatient hospice care by the Palliative Care Consult Team (PCCT). The stated objective of the PCCT in accepting him into hospice was to meet the traditional hospice care goals of ‘total comfort and support’ in end-of-life care.” In early November, the patient was admitted to a private-sector hospital for an acute coronary event and then transferred to the facility for further care and evaluation. As care requirements had proven problematic in the home setting, the patient was admitted to the facility’s CLC in mid-November, designated as hospice-level care.
Over a 2 day period in early December, the patient experienced increasing restlessness, repeatedly attempting to get out of bed. Concurrently, his wife voiced concerns to the nurses about her husband’s comfort level. Vital signs revealed rapid heart and respiratory rates and a reduced arterial oxygen level despite ongoing oxygen supplementation. Due to the patient’s clinical deterioration, CLC nurses attempted to contact the medical officer of the day (MOD) in the early hours of day 2. Despite multiple calls, the nurses were unable to readily reach the MOD and, at one point, were redirected to a recorded message that offered “no one is available.” After approximately 1 hour, a nurse reached an on-call physician who issued a telephone order for the patient to receive a one-time narcotic dose. Later in the day, nurses documented that the patient’s pain levels were increasing. His wife again voiced her concern as to the patient’s “overall comfort level.” During the afternoon hours of day 2, CLC nurses described the patient as continuing to be restless and anxious, with rapid breathing and “air hunger.” Due to the patient’s continuing distress, a CLC nurse contacted the duty nurse at the facility’s Hospice House for further guidance. The Hospice House nurse observed the patient to be “gasping for air, restless…unable to speak.” There were no order sets for contingency comfort measures. The MOD issued another one-time telephone order for oral narcotic.
Later in the afternoon of day 2, the Hospice House nurse telephoned the CLCMD who issued an order for oral morphine (as needed) and contacted the hospitalist on duty to see the patient at the bedside. In seeing the patient later that afternoon, the hospitalist noted continuing “agitation, confusion, and shortness-of-breath with labored breathing.” The hospitalist felt the patient’s clinical circumstances equated to “end-of-life care” and offered guidance on supportive measures. Later in the evening, the CLCMD evaluated the patient and documented that he was “restless and in moderate distress.” Following additional medication adjustment and comfort measures, the patient stabilized. He died the following morning.
Facility policy defines hospice as a mode of palliative care with the stated goal of achieving the best possible quality of life through relief of suffering and control of symptoms. When designated for hospice by the facility’s PCCT, the patient’s EHR stated his goals for care were “total comfort and support” with targeted symptoms to include “agitation, anxiety, and pain.”
The patient’s final 48 hours of life, as chronicled by those caregivers who were at bedside, portray ongoing, heightened distress manifested by increased difficulty breathing, agitation, anxiety, and pain. There were initially no order sets for managing
VA Office of Inspector General 5

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
these foreseeable developments as the patient entered his final hours. Several nurses expressed frustration over their own limited level of training and preparedness in caring for hospice patients as well as the ready availability of on-call physician support during the patient’s initial period of clinical deterioration. A senior clinician involved in this case stated that the patient’s care during the final 48 hours of life was not consistent with the defined HPC goals of “total comfort and support.”
Issue 2: Electronic Resident Monitoring System
The complainant alleged that despite suggestions to lock one CLC unit, managers continue to utilize an electronic resident monitoring system that does not ensure resident safety. The complainant alleged that:
a) Residents can still leave the unit(s) and staff members may not always be able to find and redirect them before an adverse event occurs.
b) Staff are overwhelmed because they must constantly respond to the alarms and redirect residents.
c) The system’s ankle bracelets compromise residents’ skin integrity.
We substantiated allegation (2a). While we did not identify any cases of actual patient harm, it is possible that a high-risk resident could wander or elope from a CLC. Contributing factors include: (i) an outdated electronic monitoring system; (ii) an inadequate policy regarding the management of monitored residents; (iii) inconsistent staff practices in response to activated exit alarms; and (iv) staff training deficits (covered in detail under Issue 4 of this report).
A. Resident monitoring system weaknesses
The CLC’s electronic monitoring system notifies staff via an alarm that a monitored patient has approached or passed through a monitored doorway. It does not restrict the patient from leaving the unit. As nursing or other unit staff can be engaged in patient care or activities that are not in the vicinity of the alarmed exit, they may not see who left the unit and which direction they went. The potential for a patient breach increases when staff are involved in an emergency situation and are not able to immediately respond to the alarm.
Facility policy did not include instructions on how staff should respond when a monitoring alarm is activated, nor did staff receive training on the required follow-up actions. Most of the employees we interviewed told us that they would go look for a wandering patient who may have activated the alarm and would return him to the unit. Some staff reported they did not turn off the alarm until they found the patient, while others said they turn off the alarm first because the noise is “irritating.” Some staff said they routinely call their sister unit when an alarm is sounding to ensure their monitored patients are accounted for; other staff members did not indicate this was part of their practice.
VA Office of Inspector General 6

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Staff also told us about “alarm fatigue,” stating that staff have become somewhat desensitized to the alarm because it is often activated several times per shift. We had an opportunity to observe this desensitization first-hand during our site visit when an alarm just outside our workroom (which was in a common hallway outside a CLC unit) sounded multiple times during our 3-day visit. In one case, the alarm sounded for more than 10 minutes without an apparent response from unit staff.
In another case that occurred around 8:15 a.m., the alarm sounded and we heard housekeeping staff comment that “it must be in the trash” which the housekeeper had just rolled through the doorway. Several nursing employees shouted down the hallway to the nursing station to get the alarm’s deactivation code. An employee shouted back with the code and the nursing employees turned the alarm off. We saw no evidence of any staff members looking for a patient or questioning why the alarm sounded in the first place. Staff members did not conduct a head count of all the monitored patients on the two units until we asked for intervention. While the actual sequence of events was unclear, we noted that a resident from the sister unit was found outside the secured area around the same time the alarm was sounding. All monitored residents were later accounted for.
One interviewee told us that on occasion, staff members have thrown non-functional monitoring bracelets in the trash. We learned that the CLCs did not have a policy or a standard practice for excessing or returning monitoring bracelets when they expired or became inoperable.
One passenger elevator and one freight elevator in a common hallway outside the CLC units permitted unrestricted access to the basement. The basement had two hallways—one to the Hospice House and the other past the Audiology Clinic and Hoptel unit. Both had electronic monitoring sensors installed at the beginning of the hallways nearest the elevators, but neither had staff that could visualize or otherwise monitor the hallways. Engineering staff told us that a red light/alarm in the nursing station of a 1st
floor CLC unit would activate if a monitored patient breached one of the basement alarms. This was not common knowledge, however, as the G&EC Chief Nurse Executive and CLC unit nurse manager were unaware of its existence
Units 42-1C and 42-1D had double doors that opened directly into the atrium. To accommodate residents in wheelchairs, the doors could be activated from the atrium side via a palm-press pad. From inside the unit, the doors should have required key/card access to open. During our tour of the area, we found one double door accessible from the inside without a key; the condition was remediated before we left site.
During the course of our interviews, we were also told of patients removing electronic monitoring bracelets, sometimes as many as 10 times, and bracelets not triggering the alarms although they had been tested and deemed functional. The facility reported one incident since October 1, 2012, when a monitored patient left the unit and was later found outdoors in the gazebo area. The facility determined that the patient was able to
VA Office of Inspector General 7

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
leave the unit undetected because his electronic monitoring bracelet was inoperable. The patient was not harmed in this incident.
B. Staff responsibilities
We did not substantiate allegation (2b). We acknowledge that some cognitively impaired patients exhibit challenging behaviors requiring substantial staff time and resources. However, we did not substantiate the complainant’s implication that the facility should reinstitute a locked/secured unit for these patients to relieve nursing staff of the need to monitor and redirect them.
It is widely understood that in relation to special memory care units, “Demands on staff are greater in terms of oversight of both the people and the environment.”2 Further, VHA Directive 2010-052, Management of Wandering and Missing Patients, December 3, 2010, states, “The use of electronic technology (e.g., patient tracking bracelets, for those patients considered to be at-risk) may only be used as one tool to enhance and augment other processes for minimizing the risk of patients wandering away from a designated area or care site. This use must not be considered as a substitute for professional vigilance and systematic verification of patients’ location.” While facility leadership’s decision to eliminate locked units places additional patient oversight responsibilities on staff, it supports VHA’s transformational goals in CLCs.
C. Skin integrity
We did not substantiate allegation (2c) that the system’s ankle bracelets compromised patients’ skin integrity. The complainant provided the name of one patient whose skin had allegedly broken down as a result of an improperly-fitted monitoring anklet. We reviewed that patient’s EHR and the EHRs of the nine other patients on the electronic monitoring system in January 2013.
The patient named by the complainant is in his mid-80s and has a history of bilateral lower extremity stasis dermatitis resulting from poor circulation. He has been a resident of the CLC since 2008 and was placed on the electronic monitoring program after he was transferred to an open/unsecured unit in May 2012. Nursing skin reassessment notes, both prior to and after placement of the monitoring anklet, have repeatedly reflected “bilateral discoloration to lower legs” or some similar descriptor consistent with the patient’s circulatory status. Further, we noted that nurses completed weekly skin assessments per facility protocol and that none of the 10 patients had documented skin breakdown related to the ankle bracelets.
Issue 3: Rehabilitation and VERA Funding
We did not substantiate that, to increase VERA reimbursements, CLC leaders admitted patients for rehabilitation even though those patients had no rehabilitation potential. In this case, rehabilitation refers to physical therapy, occupational therapy, or
2 Nursing Home Design Guide, Dementia Care Facility 2006
VA Office of Inspector General 8

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Kinesiotherapy designed to improve patients’ physical functioning. Depending on the individual patient, the rehabilitation goal could be to regain strength and mobility after hip replacement so the patient can return to independent living in his own home; in other cases, the rehabilitation goal is to increase upper body range of motion so a wheelchair-bound patient can feed himself and brush his own teeth.
The VERA model of funding utilizes workload and complexity data to ensure that funding follows the workload and that more complex workload receives greater resources. There are 60 VERA classes and 11 price groups. In general, patients meeting criteria for a rehabilitation level of care are funded at a higher VERA reimbursement rate than patients meeting only basic custodial care criteria. However, many factors influence the patient’s VERA category. Because VERA is a reimbursement model of funding, changes to patients’ VERA categories affect future funding, not current funding.
The complainant and another interviewee provided the names of two patients who were allegedly improperly admitted to the CLC for rehabilitation. We reviewed the EHRs of those two patients as well as eight additional patients that had received rehabilitation from October 1, 2012, to the time of our site visit in late February 2013.
Case 2. One of the patients named by the complainant was a male in his eighties with metastatic prostate cancer who was experiencing decreased strength and endurance due to his multiple medical conditions. The patient was transferred from a general medical unit to the CLC in mid-November. His medical unit discharge summary reflects that during his hospitalization, the patient’s ability to ambulate improved with physical therapy (PT). It further stated, “His daughter is willing to take care of him once he is strong enough to go home. In the meantime, he will probably require nursing home placement for strengthening.” A physical therapist evaluated the patient upon his admission to the CLC the same day and documented mobility, transfer, strength, and gait goals. The PT plan was for the patient to participate in 4-5 PT sessions per week, with an anticipated discharge home in 14 days. Unfortunately, the patient became increasingly ill and was unable to meaningfully participate in PT. He was placed in hospice care and died in the CLC in early December.
Case 3. The second named patient is a male in his nineties who suffers from progressive dementia and was no longer able to care for himself in a community setting. The patient was initially screened in early February for CLC long-stay continuous care (the highest VERA classification and price group). Due to some pending medical appointments, the patient was not admitted immediately. He was rescreened and admitted to the CLC for short-stay restorative care with a plan for discharge home or to an assisted living facility. Although an occupational therapist noted in mid-February that the resident’s cognitive impairment inhibited his ability to participate in rehabilitation therapy, the patient has nonetheless continued to receive daily restorative care services to maintain function. It does not appear that there is any plan to discharge the patient. In this case, the resident will likely convert to a long-term continuous stay status after he exhausts the 90 days of restorative care. According to VA eligibility rules, this resident’s
VA Office of Inspector General 9

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
service-connected status entitles him to long-term custodial care for as long as is clinically indicated. We found no evidence that the resident’s admission for restorative care was an attempt to gain a higher VERA reimbursement level as the resident was eligible from the day of admission for the highest VERA reimbursement level.
In each of the other eight cases, we found that patients were admitted for valid rehabilitation-related needs, that rehabilitation goals were appropriately documented, and that progress towards achieving those goals (or the reasons that goals were not met) was consistently recorded.
Issue 4: Staff Training and Oversight
We confirmed that some nursing staff had not received training that would have enhanced their ability to care for certain patient populations. We reviewed a total of 31 training records of CLC and Hospice House nursing personnel to determine whether staff received training related to the electronic monitoring system, hospice/palliative care, and behavior management. The training records selected belonged to registered nurses, licensed practical nurses, and nursing assistants, and included those who were directly involved in the care of the patients identified in the allegations.
Of the 31 training records reviewed: None of the staff had received training on post-alarm procedures related to the
electronic monitoring system. 16 staff members had not been trained in behavior management techniques. Of
the 15 who had been trained, a majority had received the training more than 5 years ago.
14 staff members had not received adequate training related to end-of-life care as required by The Joint Commission. Of the 17 who had been trained, 7 received the training more than 4 years ago.
We could not confirm or refute the allegation that the CLCMD does not go on “walking rounds.” However, we did not substantiate that this condition was evidence of a clinical or procedural lapse. VHA does not require providers to go on “walking rounds” (discussing patients’ care at their bedsides). We determined that the CLCMD participates in weekly interdisciplinary treatment planning sessions, is routinely consulted by the CLC NPs and other staff as needed, and thoroughly documents patient care and consultation activities in the EHRs.
We did not substantiate that the CLCMD does not properly supervise the CLC NPs. The complainant did not provide any specific examples, so we reviewed a convenience sample of 20 residents’ EHRs (10 residents assigned to NP #1 and 10 residents assigned to NP #2) for evidence of supervision and oversight. By design, the NPs provide the majority of routine clinical care to CLC residents. Local policy requires the CLCMD to “be in daily contact with regard to the [NP’s] patient care activities.” The CLCMD must also cosign the NPs’ history and physical (H&P) notes and discharge summaries. During our interviews and through EHR reviews, we found that the CLCMD meets daily with the two NPs and cosigns H&Ps and discharge summaries as required.
VA Office of Inspector General 10

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Further, the NPs’ progress notes reflect discussion and consultation with the CLCMD when more complex clinical concerns arise.
We did not substantiate the allegation that the G&EC Chief Nurse Executive does not adequately address and follow-up on staff concerns and complaints. The examples cited to support this allegation related to patient safety and the electronic monitoring system, and to suggestions for a secured dementia care unit and a designated hospice care area within the CLC.
Because we could not determine with certainty which, if any, G&EC leaders or CLC managers were informed of patient safety concerns related to the electronic monitoring system, or when they were informed (if at all), we could not say that any one G&EC leader or CLC manager failed to follow-up. However, enough staff members voiced concerns during our interviews that we believe it must have been a topic of discussion in some forum at some time. The CLC adopted the open-unit concept almost 1 year ago, and based on what we heard from several interviewees, concerns about the electronic monitoring system and the safety of dementia patients has persisted since that time. We confirmed multiple system weaknesses and patient safety concerns during our visit.
The decision to not implement the suggested changes has been unpopular with some nursing staff. Nevertheless, the management decision to care for wandering dementia patients and provide end-of-life care to hospice patients on open CLC units conforms to VHA’s transformational goals for CLCs.
Conclusions
We did not substantiate that patients were improperly admitted to the CLC, and as a result, did not receive appropriate treatment and services. With the exception of one case, the residents named by the complainant received care and services. In the excepted case, the resident did not receive care consistent with VHA’s defined concept of HPC. There were no order sets for managing this resident’s symptoms in the final hours, and CLC nurses expressed frustration as to their own limited level of training and preparedness in caring for hospice patients in general.
While we did not identify any actual cases of patient harm, we substantiated that a high-risk resident could wander or elope from a CLC unit. Several factors contributed to this condition including an outdated electronic monitoring system; an inadequate policy regarding the management of monitored residents; inconsistent staff practices when an exit alarm is activated; and staff training deficits.
We did not substantiate that, to increase VERA funding, CLC leaders admitted patients for rehabilitation even though those patients had no rehabilitation potential. We found that patients were admitted for valid rehabilitation-related needs, that rehabilitation goals were appropriately documented, and that progress towards achieving those goals (or the reasons that goals were not met) was consistently recorded.
VA Office of Inspector General 11

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
We confirmed that some nursing staff had not received training that would have enhanced their ability to care for certain patient populations. Specific training deficits included behavior management techniques, end-of-life care provision, and post-alarm procedures related to the electronic monitoring system.
We did not substantiate that the CLCMD does not properly supervise the CLC NPs. EHRs reflected that the CLCMD cosigns the NPs’ H&P notes and discharge summaries as required, routinely consults with the NPs on more clinically complex cases, and participates in regular patient care and treatment planning meetings.
We did not substantiate the allegation that the G&EC Chief Nurse Executive does not adequately address and follow-up on staff concerns and complaints. We did note, however, that facility leaders did not conduct a risk assessment of the electronic monitoring system in spite of ongoing safety concerns.
Recommendations
1. We recommended that the facility Director ensure that the patient (case 1) endof-life care undergoes a quality review.
2. We recommended that the facility Director ensure that CLC staff are appropriately trained and competent to care for all CLC residents, regardless of the residents’ special care needs.
3. We recommended that the facility Director conduct a risk assessment of the electronic monitoring system and implement improvements, as indicated.
VA Office of Inspector General 12

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Appendix A
Additional Case Summaries
Case 4 – We did not substantiate the complainant’s allegations that the patient was improperly admitted to a [non-secure] CLC unit; that staff did not properly notify his primary providers that the patient was refusing medications; that an incident in early December 2012, was not properly documented or communicated; that staff did not call a Code Red (a psychiatric emergency code) related to said incident; and that the patient was unstable but was still returned to his CLC unit after evaluation in the ED.
The patient is in his late 50s and has a diagnosis of Wernicke-Korsakoff Syndrome.3
He was accepted in April 2012 for a long stay (90+ days) admission to the facility’s secured CLC unit after several failed discharges to community-based nursing facilities due to behavioral and safety concerns.4 In June, the secured unit was closed for renovations and he was moved to an open unit on the 2nd floor and placed on the electronic monitoring program. EHR documentation reflects that the patient frequently wandered from his unit to the sister unit, but that staff members were able to redirect him to his unit with minimal resistance.
In early June, the patient was moved to a 1st floor unit because of renovations on the 2nd
floor. The EHR reflects that between June and September, he was adjusting well to the open unit but that he still had wandering behaviors which required redirection.
In early December, the patient wandered from his unit. The alarm sounded and two staff members followed the patient up the atrium stairway to the 2nd floor balcony. The EHR described the patient as standing near and looking over the railing.5 A staff member from an adjoining unit who knew the patient was able to redirect him away from the railing and into the dayroom. That staff member later documented that the patient had muttered while at the railing, “I’m going to do it.” Once in the dayroom, he voiced that he wanted to leave and became agitated, kicking a glass partition and swinging at the staff member with his fist. Another staff member summoned the facility police. The staff member and the officers were able to redirect the patient back to his 1st floor unit where he was given an injection of lorazepam6 1 milligram (mg). After being medically cleared in the ED, he returned to his unit but wandered away again. After being returned to the unit, he was given haloperidol7 5 mg, which appeared to calm him down. Two days later, staff had to redirect the patient back to his unit after he wandered again. His provider and nursing staff evaluated him and documented that his behavior had returned to baseline.
3 Damage to areas of the brain involved with memory, aka alcoholic dementia. 4 The resident did not meet administrative eligibility for long-term CLC care; however, the patient’s condition and lack of family support made his discharge to any community setting virtually impossible. 5 The facility installed 43-inch railing which exceeded the standard 36-inch railing for patient safety. 6 Medication used to treat anxiety. 7 Antipsychotic medication used to treat acute psychotic state.
VA Office of Inspector General 13

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
We found that while the patient presented a behavior management challenge for the staff, the CLC was the most appropriate setting to ensure his care and safety. We also found that staff did notify the patient’s primary providers that he was refusing medications, and those refusals were documented in the EHR. The balcony incident in early December was documented in the EHR by two different nurses, and it appeared that CLC staff were able to safely and effectively remove the patient from a harmful situation and provide necessary follow-up and treatment. As such, a Code Red (psychiatric emergency team response) was not indicated. Further, EHR documentation reflected that the patient was stable when he returned to the unit, and his continued wandering was part of his baseline behavior. Nurse staffing on that unit that day met the facility’s established standards.
Case 5 – We did not substantiate the allegation that the patient is not placed on the correct CLC unit, and as a result, is not receiving the appropriate level of care. The complainant specifically noted that due to the patient’s severe dementia, he frequently wanders into other patients’ rooms and must be redirected, and that he has had multiple falls. The complainant also reported that the patient was routinely restrained, which was forbidden by facility policy.
The patient is a man in his mid-80s with multiple medical problems including severe dementia. He was admitted to the CLC in August 2012 after transferring from a skilled nursing facility that could no longer handle his needs. The EHR reflects multiple episodes of wandering, restlessness/anxiety at night, and repeated falls. In early December, the interdisciplinary treatment (IDT) team discussed the patient’s recent behaviors and noted that many sedatives/sleep medications may not be prudent given his advanced dementia, fall risk, and frailty. The IDT team also discussed the possibility that pain may be contributing to the patient’s difficulty relaxing well enough to sleep at night and ordered acetaminophen 1000 mg every 12 hours. The plan was to re-assess the following week, and if the patient’s sleep had not improved, then a low-dose sleep medication and other non-pharmacological approaches (warm shower/bath 1–2 hours before bedtime, sleep hygiene, etc.) would be considered.
In late December, the patient was treated for fever, shortness of breath, and decreased oxygen saturation thought to be related to aspiration pneumonia due to esophageal dysfunction. His condition returned to baseline after a course of antibiotics. In late February 2013, staff noted a decrease in physical mobility with recent “out of character level of activity/mobility.” The EHR reflected “No focal findings or illnesses. No pain or discomfort noted or reported. Only new medication is midodrine.” The EHR also reflected a recent fall with no apparent injury, and “Severe Dementia, may indicate terminal decline, consider depression.” A palliative care consult was placed at that time.
During a February family meeting, the patient’s family requested that he not be transferred to Hospice House unless he developed a symptom that his CLC unit could not address. His family indicated that they wanted to keep him in a familiar environment for as long as possible. The patient continues to reside in the CLC.
VA Office of Inspector General 14

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Based on the patient’s service-connected status, he is entitled to long-term CLC care for as long as is clinically necessary. The CLC screening committee approves admissions, and unit placements are determined by a variety of clinical and administrative factors. During our interviews, we were told that, in an effort to redistribute the workload somewhat, residents with challenging dementia-related behaviors could be placed on any of the CLC’s four units (which are all equipped with electronic monitoring sensors). In addition, nursing staff on any of the CLC’s units would be trained and qualified to redirect a wandering patient, and intervene accordingly, and implement fall-reduction strategies. We found no evidence that the patient was improperly placed.
We could not confirm or refute the allegation that the patient was routinely restrained, a practice that was forbidden by facility policy. If any staff members knew of a patient being improperly restrained, those staff members would have been required to report the incident(s). We found no reports of improper restraint usage or alleged patient abuse involving the patient, nor had selected interviewees heard about such problems. Facility policy includes an addendum outlining the specific steps and requirements for initiating and maintaining restraints on residents in the CLC. The patient’s EHR entries reflect that staff consulted occupational therapy, documented actions to avoid initiation of restraints, and routinely provided 1:1 observation as required.
Case 6 – We did not substantiate the complainant’s allegation that the CLCMD failed to order a needed swallowing study or that the CLCMD’s order to raise the head of the patient’s bed to 75 degrees was improper and would have likely caused aspiration.
The patient was in his 80s and had lived in the CLC since 1999. He had a medical history including cerebral vascular disease with hemiplegic stroke and severe vascular dementia, hypertension, and diabetes. The complainant alleged that in November 2012, she notified the CLCMD that the patient’s condition was declining and that he was unable to swallow. The CLCMD evaluated the patient and documented that his decline was possibly related to several factors, including hypoglycemia or a urinary tract infection. The CLCMD’s plan included a urine culture and one dose of antibiotics; to restart the oral [anti-diabetic] agent (which had been discontinued several days earlier due to the patient’s erratic eating patterns and weight loss); bed rest with the head of bed elevated to >75 degrees for oral intake; to call the family/guardian; and to observe for changes. We also noted that the patient had undergone a swallowing study less than 3 weeks earlier. The speech-language pathologist (SLP) documented that the patient was known to require significant staff assistance and coaxing at meal times, but could take food and fluids orally and could consume 100-percent of his meal if given enough time. The SLP documented, “He will often turn his head away and refuse to open his mouth” and “It appears that his weight loss is due to him declining to eat.” We found that the CLCMD’s documented treatment plan for the patient in November was reasonable given his medical history and presentation, and that there was no indication for another swallowing study. The order to raise the head of the patient’s bed to >75 degrees was not problematic; in fact, it may have promoted his safe consumption of food and fluids.
VA Office of Inspector General 15
Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
We also did not substantiate the complainant’s implication that the CLCMD improperly delayed the patient’s referral for palliative care. In late November, the patient was transferred to the intensive care unit (ICU) after becoming unresponsive. His EHR reflected that he had poor blood flow in his lower extremities, and that some tissue appeared necrotic. The ICU provider documented concerns about dehydration, sepsis, and multi-system organ failure. The next day, the ICU provider requested a palliative care consult which the CLCMD completed the same day. The CLCMD documented that he had spoken with the patient’s wife and that she was accepting of hospice care but aware that no beds were available in Hospice House at the time. The CLCMD wrote, “She voiced understanding that he is gravely ill and that death may be expected at any time and is likely this weekend. She prefers that he stay in the [intensive care] unit.” Three days later, the patient was admitted to the Hospice House for end-of-life care. He died the following day.
The patient had been a long-term CLC resident whose medical care needs and behavioral patterns were well known to the staff. His presenting symptoms in late November were likely related to several potentially treatable conditions as outlined in the CLCMD’s progress note and treatment plan. It was not until after the patient’s admission to the ICU that his poor prognosis for recovery became clear. The PCCT consult was placed and answered the following day, and per the wife’s request, the patient remained in the ICU until a bed became available and he could be transferred to Hospice House.
Case 7 – We did not substantiate the allegation that when the patient’s level of care changed to hospice status, the CLCMD refused to talk with the next-of-kin (NOK) about Hospice House, its services, and its amenities.
The resident is a male in his sixties who has significant brain damage due to carbon monoxide poisoning. He has been a resident of the facility for 40 years. The patient’s condition began to deteriorate in February 2013 and he was treated for presumed aspiration pneumonia. In early March, the NP placed a palliative care consult noting a prognosis/life expectancy of less than 1 week. The patient’s NOK requested that he remain in the CLC (rather than be transferred to the Hospice House) because he is familiar with the staff. The PCCT consultation response states, “At this time, niece requests NO TRANSFER to hospital OR HOSPICE until she visits this weekend.” We found multiple progress notes reflecting discussions between the CLCMD and NOK regarding the patient’s condition and the utility of transfer to the Hospice House.
We also did not substantiate that the patient’s NP ordered inappropriate medications and did not have the specialty training required to care for hospice residents. Specifically, the complainant questioned the appropriateness of the NP’s orders for Tylenol™ suppositories and diazepam (IM-intramuscular) as needed for seizures. We found that the suppositories were an acceptable pain control method given that the patient had recently aspirated and had had repeated bouts of vomiting. Further, the use of an injectable, fast-acting medication in the event of an isolated, acute-onset seizure would be more appropriate than a sublingual tablet administered on a scheduled basis
VA Office of Inspector General 16

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
to prevent potential seizures. The goal of CLCs is to reduce poly-pharmacy whenever possible.
The patient’s NP (NP #1) is a certified gerontological NP with many years of clinical experience. In this case, we saw multiple EHR entries reflecting the NP’s notification of, or consultation with, the CLCMD regarding treatment and end-of-life care.
We did note, however, that NP #1 had recently been given a collateral assignment to support the Hospice House team. The NP confirmed to us that she did not possess specialized skills in this area and indicated her intention to complete the requisite training.
Case 8 – We did not substantiate the allegation that the patient, who was suffering an acute medical event, was improperly left on the CLC unit to receive acute care and monitoring. We also did not substantiate that the CLC was not staffed or equipped to handle this level of care.
The patient, a veteran in his 80s with a medical history of congestive heart failure and Type II diabetes, experienced multiple falls while at home and was admitted to the CLC in mid-December 2012 for short-term restorative care. In late December, NP #2 noted the patient’s elevated blood sugar of 916 mg/ deciliter (dL)8 and current medication regimen, and documented “Veteran's blood sugar has been consistently elevated in 400 and 500s since admission” several weeks earlier. The note also reflects that despite his elevated blood sugar, the patient said he felt fine and that his blood sugars were “always high."
NP #2 developed a plan of care which included additional insulin and intravenous (IV) fluids, and NP #2 discussed this plan of care with the covering physician. That evening, the covering physician received a call from the patient’s nurse reporting that his blood sugar was greater than 500 mg/dL. Nursing notes indicated that the patient denied any feelings of excessive thirst, urination, or excessive sweating. The nurse also documented the patient’s desire to remain in the CLC, stating “I don't want to go to the hospital, you can do just as good of a job here, and I'm going to stay here." The covering physician documented that the patient was asymptomatic and did not appear to be in diabetic ketoacidosis.9 At that time, the facility had no available acute care beds and was on diversion status.
The CLC covering physician placed orders for a urinalysis, basic metabolic panel, insulin, and a continuation of IV fluids previously ordered by NP #2. Within 1 hour of the physician’s orders, nursing notes reflected improvement in the patient’s blood sugar from 916 to 717 mg/dL. His condition continued to improve and laboratory results
8 According to the American Diabetes Association, diabetic patients should be 70 – 130 (mg/dL) before meals, and less than 180 mg/dL after meals (as measured by a blood glucose monitor).9 Ketoacidosis is a serious complication of diabetes that occurs when the body produces high levels of blood acids because of its inability to produce enough insulin.
VA Office of Inspector General 17

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
documented shortly after midnight noted a blood glucose of 211 mg/dL. The patient has since been discharged home.
Because the facility was on diversion, the patient would have had to have been transferred to a private-sector facility for acute care. Given that he was asymptomatic during the entire event and expressed a desire to stay in the CLC and receive care there, the covering physician’s decision to treat the patient in place was reasonable. The physician’s orders were routine, and the CLC nurses were not required to provide care outside of their basic skill sets. The EHR reflects ongoing communication between the covering physician and nursing staff. Also, nurse staffing during those shifts met the facility’s established standards.
Case 9 – We did not substantiate the complainant’s implication that the CLCMD did not adequately respond to the patient’s cough, congestion, and elevated white blood cell count (a sign of possible infection). The complainant alleged that the CLCMD ordered blood work and a urine culture although the patient did not complain of urinary symptoms, and did not prescribe antibiotics to clear a respiratory infection.
The patient is a long-term CLC resident in her 60s with a history of chronic obstructive pulmonary disease. In mid-November, a nurse noted that the patient was continuing to exhibit cold symptoms with congestion and a non-productive cough. The nurse notified the patient’s NP (NP #1), who ordered a chest x-ray which was negative. A nutritional supplemental was added to her diet, and she received cough medications as ordered.
Four days later, the patient continued to exhibit a non-productive cough. The nurse documented the patient reported feeling "poorly" with a decreased appetite and oral intake at meals. The CLCMD evaluated the patient about 2 hours later, who at that time reported feeling better with a decrease in her coughing and a return of her appetite and energy. She denied fever, chills, sputum production, or congestion. She also denied urinary symptoms. The CLCMD documented:
Impression: 1. Resolving Upper Respiratory Tract Infection, probable viral with
Lymphocytosis. 2. Leukocytosis, impressive 3. Nursing reports urinary symptoms that are not volunteered by
Veteran, consider UTI [urinary tract infection].
The CLCMD’s plan of care included a urinalysis and culture; to repeat the blood work in 3 days; and to continue the plan of care. No antibiotic was ordered at that time.
Ten days later, the CLCMD evaluated the patient and documented that she still had a non-productive cough, but she denied fever or feeling ill. The CLCMD prescribed antibiotics to treat for possible bronchitis. He also noted that the patient continued to smoke. One week later, the patient’s symptoms were resolving, and she was no longer wearing an oxygen mask or complaining of cough or shortness of breath.
VA Office of Inspector General 18

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
The CLCMD’s orders and plan of care in late November were appropriate given the patient’s presenting symptoms, self-report of “feeling better,” and the nursing report of urinary symptoms. As the CLCMD believed the upper respiratory infection was probably viral, antibiotics were not indicated at that time. The urine culture was appropriate as nursing staff reported urinary symptoms that the patient did not “volunteer.”10 The CLCMD took a reasonable and cautious approach to the patient’s treatment to see if her condition would resolve on its own. When it did not, he prescribed antibiotics to treat possible bronchitis.
Cases 10 and 11 – We did not substantiate the allegation that two other CLC residents may have been “hit” or “manhandled” by two specific staff members. The complainant did not witness the alleged abuse but described how these two patients could be heard “yelling for help” when they were receiving assistance with personal care activities. The employee who reportedly witnessed the alleged abuse was on extended leave and unavailable for interview.
Employees are required by policy to report actual or suspected patient abuse or neglect; however, CLC managers and facility leaders were unaware of any concerns about these two patients. One interviewee told us that some of her colleagues do not make an effort to learn residents’ preferences and what techniques work best when caring for them. The interviewee had not witnessed any patient abuse or mistreatment. However, the two patients in question both have dementia and have been noted in the past to be agitated and resistant to care at times.
10 UTIs in the elderly may not cause clear symptoms or involve pain or discomfort; therefore, patients may not believe they have anything to report.
VA Office of Inspector General 19

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Appendix B
VISN Director Comments
Department of Veterans Affairs Memorandum
Date: June 13, 2013
From: Director, VA Mid-Atlantic Health Care Network (10N6)
Subject: Healthcare Inspection – Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
To: Director, Atlanta Office of Healthcare Inspections (54AT)
Thru: Director, VHA Management Review Service (VHA 10AR MRS OIG Hotlines)
1. Attached is the action plan developed by the W.G. (Bill) Hefner VA Medical Center, in response to the recommendations received.
2. The facility concurs with the findings and will ensure the corrective action plan is implemented.
3. If you have any questions please contact Lisa Shear, VISN 6 QMO, at (919) 956-5541.
(original signed by:)
DANIEL F. HOFFMANN, FACHE
VA Office of Inspector General 20

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Appendix C
Facility Director Comments
Department of Veterans Affairs Memorandum
Date: June 13, 2013
From: Director, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC (659/00)
Subject: Healthcare Inspection – Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
To: Director, VA Mid-Atlantic Health Care Network (10N6)
1. I have reviewed the draft report of the Office of Inspector General and I concur with the recommendations.
2. I have included my response in the attached Director’s Comments.
3. Please contact me if you have any questions or comments.
(original signed by:)
Kaye Green FACHE Director, W. G. (Bill) Hefner VA Medical Center (659/00)
VA Office of Inspector General 21

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Comments to OIG’s Report
The following Director’s comments are submitted in response to the recommendations in the OIG report:
OIG Recommendations
Recommendation 1. We recommended that the facility Director ensure that case 1”s end-of-life care undergoes a quality peer review.
Concur
Target date for completion: July 23, 2013
Facility response: One May 28, 2013 the Risk Manager sent a request for peer review to the VISN Lead for Geriatrics and Extended Care. The peer review is expected to be completed no later than July 12, 2013. The review will be presented to the Medical Center Peer Review committee on July 23, 2013. A peer review will also be completed for the nursing care rendered to [the patient]. The nursing peer review will be presented to the peer review committee on July 23, 2013.
Recommendation 2. We recommended that the facility Director ensure that CLC staff are appropriately trained and competent to care for all CLC residents, regardless of the residents’ special care needs.
Concur
Target date for completion: August 1, 2013
Facility response: Patient Care Services reassigned a full time nurse educator to increase availability of training and provide additional face to face education tailored to long term care needs. Training for the three recommended areas began in February 2013. Training for the Wander guard system has been completed for 98% (128/131) of patient care services staff currently assigned to the CLC. There are three staff; one on FMLA and two detailed to other services that have not completed the training. Those employees will be trained upon returning to the CLC. Secondly, training continues on the End of Life Nursing Education Consortium (ELNEC). 50% (66/131) of patient care services staff have completed the training. The three hour class is offered four times per month. All patient care services staff are expected to complete the program by August 1, 2013. Lastly, 71% (94/131) of patient care services staff have completed the phase I of the Prevention and Management of Disruptive Behaviors (PMDB) class. In addition, 54% (72/131) have completed Phase II. Additional classes are offered three times per month to ensure all patient care services staff attends. Training for PMDB is expected to be completed by August 1, 2013.
VA Office of Inspector General 22

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Recommendation 3. We recommended that the facility Director conduct a risk assessment of the electronic monitoring system and implement improvements, as indicated.
Concur
Target date for completion: October 1, 2013
Facility response: A risk assessment was completed and it was determined that the current electronic monitoring system does not meet safety expectations for prevention of wandering at risk residents. The risk assessment team has evaluated the risks and steps have been taken to mitigate or avoid any potential risks during the installation of a newer electronic monitoring system. CLC leadership, with direct care staff input, reviewed products to determine the best option for electronic monitoring for wandering residents. The Roam Alert electronic monitoring system, used in conjunction with the Renault 5 Nurse Call System was selected. As the CLC is currently under construction, installation will occur as each resident care area is constructed or renovated. The entire project is slated to be completed by October 2014. The first renovated area is expected to be completed for initial move-in early October 2013. The area will house the rehabilitation unit on the first floor and our most vulnerable residents in the dementia unit on the second floor. The remaining areas will follow and will continue to use the present electronic monitoring system if needed and operate under the contingency plan currently implemented.
VA Office of Inspector General 23

Quality and Patient Safety Concerns in the CLC, W. G. (Bill) Hefner VA Medical Center, Salisbury, NC
Appendix D
OIG Contact and Staff Acknowledgments
Contact For more information about this report, please contact the OIG at (202) 461-4720.
Contributors Victoria Coates, LICSW, MBA, Team Leader Karen Sutton, BSHCM Sheyla Desir, RN, MSN Thomas Jamieson, MD
VA Office of Inspector General 24

Quality and Patient Safety Concerns in the CLC, W.G. (Bill) Hefner VA Medical Center, Salisbury, NC
Appendix F
Report Distribution VA Distribution
Office of the Secretary Veterans Health Administration Assistant Secretaries General Counsel Director, Mid-Atlantic Healthcare System (10N6) Director, W.G. (Bill) Hefner VA Medical Center (659/00)
Non-VA Distribution
House Committee on Veterans’ Affairs House Appropriations Subcommittee on Military Construction, Veterans Affairs, and
Related Agencies House Committee on Oversight and Government Reform Senate Committee on Veterans’ Affairs Senate Appropriations Subcommittee on Military Construction, Veterans Affairs, and Senate Committee on Homeland Security and Governmental Affairs Related Agencies National Veterans Service Organizations Government Accountability Office Office of Management and Budget U.S. Senate: Richard Burr and Kay R. Hagan U.S. House of Representatives: Virginia Foxx, Richard Hudson, and Melvin L. Watt
This report is available on our web site at www.va.gov/oig
VA Office of Inspector General 25





























