Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Health-Related Quality of Life in Adolescents with InflammatoryBowel Disease Depends on Disease Activity and PsychiatricComorbidity
G. Engelmann • D. Erhard • M. Petersen • P. Parzer •
A. A. Schlarb • F. Resch • R. Brunner • G. F. Hoffmann •
H. Lenhartz • A. Richterich
� Springer Science+Business Media New York 2014
Abstract Adolescent patients with inflammatory bowel
disease (IBD) show an increased risk for behavioral and
emotional dysfunction. Health-related quality of life
(HRQoL) is influenced by medical illnesses, as well as by
psychiatric disorders, but for adolescents with IBD, the
extent to which HRQoL is influenced by these two factors
is unclear. For 47 adolescent IBD patients, we analyzed
disease activity, HRQoL and whether or not a psychiatric
disorder was present. Disease activity was estimated using
pediatric Ulcerative Colitis Activity Index and pediatric
Crohn’s Disease Activity Index. The IMPACT-III and the
EQ-5D were used to measure HRQoL and QoL, respec-
tively. In addition, patient and parent diagnostic interviews
were performed. 55.3 % patients fulfilled DSM-IV criteria
for one or more psychiatric disorders. In all patients, psy-
chiatric comorbidity together with disease activity con-
tributed to a reduction in quality of life. Adolescents with
IBD are at a high risk for clinically relevant emotional or
behavioral problems resulting in significantly lower
HRQoL. We conclude that accessible, optimally structured
psychotherapeutic and/or psychiatric help is needed in
adolescent patients with IBD.
Keywords Health related quality of life � Adolescent �IMPACT III � Inflammatory bowel disease
Introduction
The symptoms of inflammatory bowel diseases (IBD) can
dramatically interfere with daily life. The adolescent
patient with Crohn’s disease (CD) may have concerns
regarding short stature, delayed puberty, tiredness, loss of
energy and feeling restricted in pursuing daily activities
like regular school attendance or sports. Patients suffering
from UC are more disturbed by gastrointestinal symptoms
G. Engelmann (&)
Department of Pediatrics, Lukas Hospital, 41464 Neuss,
Germany
e-mail: [email protected]
G. Engelmann � D. Erhard � M. Petersen � G. F. Hoffmann
Department of Pediatrics, University Medical Center, University
of Heidelberg, Heidelberg, Germany
P. Parzer � F. Resch � R. Brunner
Department of Child and Adolescent Psychiatry, University of
Heidelberg, Heidelberg, Germany
A. A. Schlarb
Faculty of Psychology and Sports Science, University of
Bielefeld, Bielefeld, Germany
H. Lenhartz
Catholic Children’s Hospital Wilhelmstift, Hamburg, Germany
A. Richterich
Department of Psychosomatics in Children and Adolescents,
University Medical Center Hamburg-Eppendorf, Hamburg,
Germany
A. Richterich
Department of Child and Adolescent Psychiatry, Psychotherapy
and Psychosomatics, HELIOS St.-Josefs-Hospital Bochum-
Linden, Bochum, Germany
123
Child Psychiatry Hum Dev
DOI 10.1007/s10578-014-0471-5

like bloody diarrhea, flatulence, urge or tenesms [1]. All
patients have worries about relapses, future health prob-
lems, medical tests and treatments as well as the impact of
their disease on their families [2]. Obviously, these
symptoms reduce the health related quality of life
(HRQoL) in adolescents [3, 4]. In large studies the reported
quality of life (QoL) in adolescents with IBD was signifi-
cantly lower compared to control groups and to the general
population [5].
Quality of life is defined by the WHO [6] as ‘‘an indi-
vidual’s perception of their position in life in the context of
the culture and value systems in which they live and in
relation to their goals, expectations, standards, and con-
cerns’’. Health in general is a major factor of QoL. Ques-
tionnaires developed to address the influence of diseases on
QoL, measure the HRQoL. These can either be generic
(focus on health in general as a factor influencing QoL) or
disease-specific. HRQoL ‘‘describes health status from the
patients’ perspective and serves as a powerful tool to assess
and explain disease outcomes’’ [7]. For pediatric patients
with IBD the disease specific questionnaire ‘‘IMPACT’’
was published in 2002 [8] and is used in our study.
Disease activity in IBD patients is dependent on frequency
of diarrhea, blood loss, weakness due to active inflammation
and other aspects of the disease. With pediatric Crohn’s
Disease Activity Index (PCDAI) [9] and pediatric Ulcerative
Colitis Activity Index (PUCAI) [10] two powerful tests have
been developed that enable pediatric gastroenterologists to
classify the burden of disease in children with IBD due to easy
to asses values. Both tests have proven reliable and are widely
used in studies on children and adolescents with IBD. The
PCDAI consists of subjective reporting of stool pattern,
degree of abdominal pain and general well-being, presence of
extraintestinal manifestations, physical examination find-
ings, height, weight and laboratory tests (ESR, haematocrit,
albumin). The PUCAI includes abdominal pain, rectal
bleeding, stool consistency and number of stools per 24 h,
nocturnal stools and the activity level.
Various studies have demonstrated that children and
adolescents with chronic medical illness carry a two to four
times greater risk for psychosocial and psychiatric prob-
lems than the general population [11–13]. However, com-
pared to individuals with other chronic diseases like cystic
fibrosis or diabetes mellitus, children with IBD were more
at risk [14, 15]. Patients with IBD are at a high risk for
difficulties in behavioral and emotional functioning [16]. In
a study with 15 IBD patients aged 9–14 years, Szajnberg
et al. [17] reports a rate of up to 73 % for psychiatric
comorbidity, especially anxiety and mood disorders.
Studies regarding pediatric and adolescent IBD have shown
that direct symptoms of disease (e.g. diarrhea, abdominal
pain) have a negative effect on the QoL and that QoL is
also influenced by associated problems as delayed puberty,
below average stature, fear of side effects of medications,
regular medical tests (e.g. blood tests, colonoscopies) and
long periods of absence from school [3, 18]. In a com-
prehensive review, Szigethy et al. [19] lists studies that
found higher rates for depression and anxiety in IBD
patients and discusses several psychological and biological
explanations for these findings. Furthermore, Szigethy
reviews the connection between health status and QoL,
stating that ‘‘the patient’s current health status is believed
to have the greatest influence on responses to the IMPACT
questionnaire’’ as a disease specific HRQoL-instrument.
Treating adolescents with IBD at the Department of Pedi-
atrics in the University Medical Center and at the Depart-
ment for Child and Adolescent Psychiatry, University of
Heidelberg, the authors wondered if alterations in QoL
were also connected to psychiatric comorbidity, because
many patients required help from both departments. Thus,
we have conducted a prospective study, aiming to compare
the influence of psychiatric comorbidity and disease
activity on the HRQoL in a representative sample of ado-
lescent patients with IBD. Structured parent and patient
interviews, IMPACT-III and EQ-5D patient questionnaires
and disease activity indices PUCAI and PCDAI were
analyzed. The study sought to make clear which of these
two aspects has the greater influence on HRQoL.
Methods
Participants
A cross-sectional survey was performed. All patients with
IBD, treated at the Department of Pediatric Gastroenter-
ology at the University Children’s Hospital Heidelberg that
fulfilled the inclusion criteria were approached and asked
to participate. Inclusion criteria were: confirmed IBD and
age between 10 and 18 years and sufficient skills in the
German language. All patients were recruited with
informed consent.
Procedure
Anthropometric data (age, body weight, height) were
measured and all patients underwent physical examination
by an experienced pediatrician. A complete laboratory
work-up (white blood cell count, c-reactive protein,
erythrocyte sedimentation rate (ESR), creatinine and
albumin) was performed. Pediatricians filled out a struc-
tured report form for clinical evaluation. A child and
adolescent psychiatrist performed a structured parent and
patient interview on psychopathology. Patients and their
parents filled out self-report questionnaires including the
IMPACT-III and EQ-5D.
Child Psychiatry Hum Dev
123

Measures
Inflammatory bowel disease activity was measured using
standardized tests: The PCDAI for CD and PUCAI for UC.
In PCDAI increasing scores are noted with increasing
disease severity (score \11: no disease activity, score of
11–30: mild disease activity, score[30: moderate to severe
disease activity). The PUCAI includes (1) abdominal pain,
(2) rectal bleeding), (3) stool consistency of most stools,
(4) number of stools per 24 h, (5) nocturnal stools and (6)
the activity level. For the index averaging the last 48 h is of
relevance. The maximum score is 85 (\10: remission,\30:
mild disease activity, 30–65: moderate and [65 points:
severe disease activity).
An experienced child- and adolescent psychiatrist per-
formed the patient- and parent interviews. Psychopathol-
ogy was documented using the Clinical Assessment Scale
for Child and Adolescent Psychopathology (CASCAP)
[20]. The CASCAP is a standardized protocol for psy-
chopathology in children and adolescents, using data
derived from patient and parent interviews. Psychiatric
diagnoses were based on Diagnostic and Statistical Manual
of Mental Disorders (DSM) IV-criteria [21].
Patient questionnaires included the IMPACT-III, a dis-
ease specific HRQoL questionnaire established for children
and adolescents with IBD, and the EQ-5D. The IMPACT-
III is a disease-specific HRQoL-instrument that has been
translated into German from the original English (Canada)
version [4] according to the criteria of Brislin [22]. This
self report questionnaire is used to measure health-related
problems and concerns in IBD patients and contains the
following domains: IBD symptoms (abdominal pain, diar-
rhea, blood in stool), body image (height, weight, look),
social functioning (e.g. daily activities, friendships, wor-
ries), emotional functioning (e.g. worries about a flare up,
chronic condition, angriness), systemic symptoms (energy,
tiredness), treatments and interventions (e.g. operations,
taking medication). Every question has five possible
answers to which 1-5 points have been assigned. Points for
each answer are summed for the total score; the maximum
score is 175 points. The EQ5D is a standardized Instrument
to measure generic QoL in 5 dimensions and one 100 mm
visual analogue scale. In the 100 mm visual analogue
scale, high values represent high QoL with expected values
in a reference population ranging from 77 to 83 [23].
Statistical Methods
Means and standard deviations were calculated from the
following parameters: age, time intervals and score points.
The student’s t test was used to assess statistical signifi-
cance of the data. To determine effects of different items
on the quality of life an analysis of variance (ANOVA) was
used.
In boxplots, the boundaries of the box are Tukey’s
hinges (25th and 75th percentile), the median is identified
by a horizontal line. The length of the box is the inter-
quartile range (IQR) computed from Tukey’s hinges. Val-
ues more than 1.5 IQR from the end of the box are plotted
as single points. The last value within 1.5 IQRs defines the
length of the whisker.
All quantitative data analyses were conducted using the
Statistical Package for Social Sciences (SPSS Version 19
for Windows, SPSS Inc., Chicago, IL, USA). After creating
a list of variables, data was entered into charts of SPSS for
Windows 19.0 (SPSS Inc., USA). Stata 13 was used to
perform the analyses.
The local ethic committee approved the study protocol.
Written informed consent was obtained for all patients.
Results
Patients
All 50 adolescent IBD patients treated at our center at the
time of the study agreed to participate. Three patients were
excluded based on lack of appropriate German language
skills. Of the 47 remaining adolescents, 27 were male, 21
were suffering from CD and 26 from UC. The mean age at
the time of the study was 15.2/12 years (SD 1.8/12), the
mean age at onset 11.5/12 years. The male/female ratio
was 11/10 for CD and 16/10 for UC, respectively
[v2(1) = 0.399, p = 0.528; cf. Table 1].
The mean duration of treatment at the time of the study
was 3.5/12 years (SD 2.42) with an average period of
symptom onset prior to diagnosis of 5 months (cf.
Table 1). 13 patients (27 %) had a positive family history
of IBD. Out of the 47 patients, 11 (23.4 %) had previously
been in contact with a child and adolescent psychologist or
psychiatrist.
Disease Activity
According to the PCDAI and PUCAI, 24 adolescents (cf.
Table 2) had no current disease activity (12 CD and 12 UC
patients), 12 had mild (6 CD, 6 UC) and 11 moderate or
severe activity (3 CD, 8 UC). Results showed no significant
difference in disease activity between the two disease
groups [v2(2) = 1.76; p = 0.415]. Adolescents suffering
from CD did not significantly differ from patients with UC
regarding ‘‘age at presentation’’ (t = 0.67, df = 45,
p = 0.506) or ‘‘duration of treatment’’ (t = 1.24, df = 45,
p = 0.22).
Child Psychiatry Hum Dev
123

Health Related Problems and Concerns (IMPACT-III)
In the disease specific HRQoL questionnaire (IMPACT-III)
all patients reported difficulties and ‘‘every day problems’’.
Most common were ‘‘worries that the illness just doesn‘t
go away’’; ‘‘feeling it is unfair to have that illness’’ and
problems related to diarrhea. Patients with psychiatric
comorbidity had significantly more disease related prob-
lems and difficulties as measured by the IMPACT-III,
75.91 versus 62.46 respectively (two-tailed t test
p = 0.006), cf. Table 5.
Psychiatric Comorbidity
In the structured psychiatric interview using the CASCAP
manual and DSM IV criteria, 61.9 % of patients with CD
and 50 % of adolescents with UC fulfilled criteria for one
or more psychiatric disorders (cf. Table 3). Adjustment
(n = 12) and major depressive disorders (n = 8) were the
most common diagnoses. Taken together, 55.3 % of ado-
lescent patients with IBD (26 of 47) suffered from psy-
chiatric disorder according to DSM IV criteria. In detail, no
significant difference between patients with CD and UC
according to the total number of patients with DSM IV
relevant disorders was found [v2(1) = 0.666, p = 0.414,
cf. Table 4]. Girls showed a higher prevalence of psychi-
atric disorders than boys, although the difference was not
statistically significant [70 vs. 45 %, v2(1) = 3.04,
p = 0.081]. Adolescents with psychiatric diagnoses
showed higher parental-scored SDQ difficulties scores than
those without (t = 2.78, df = 45, p = 0.008).
A logistic regression showed no influence of ‘‘duration
of treatment’’ (p = 0.526) and ‘‘age at presentation’’
(p = 0.178) on the presence of a DSM IV-relevant
disorder.
Of the 26 patients with a current diagnosis of one or
more behavioral and emotional problems, only 7 (26.9 %)
had previously been in contact with a child and adolescent
psychiatrist or psychotherapist.
Influence of Disease Activity and Psychiatric
Comorbidity on Health-Related Problems and Concerns
A higher disease activity was associated with higher self-
ratings in the Impact-III questionnaire for health-related
problems and concerns. Patients with psychiatric comor-
bidity showed more health-related problems and concerns
than patients without, regardless of the disease activity
(none, low or high; cf. Fig. 1). The extent of health-related
problems and concerns was also influenced by disease
Table 1 Patients characteristics
Crohn’s
disease
n = 21
Ulcerative
colitis
n = 26
Total
Male/female 11/10 16/10 27/20
Mean age at diagnoses (years) 11.7/12 11.4/12 11.6/12
Mean age at time of the study
(years)
15.0 15.4/12 15.2/12
Average duration of symptoms
before diagnoses (months)
6.6 4.0 5.0
Already in contact with
psychologist or psychiatrist
(no/yes)
18/3 18/8 36/11
Table 2 Disease activity measured as PCDAI in patients with Cro-
hn’s disease and PUCAI in patients with ulcerative colitis
(v2 = 1.4133; Pr = 0.493)
IBD Disease activity Total
No/remission Mild Moderate
to severe
PCDA \11 11–30 [30
PUCAI \10 10–30 [30
Crohn’s disease (n) 12 6 3 21
Ulcerative colitis (n) 11 8 7 26
Total 23 14 10 47
Table 3 Diagnostic and statistical manual of mental disorders
(DSM) IV diagnoses in the 26 patients with psychiatric comorbidity
Diagnoses Total CD/CU Percentage
Adjustment disorders 12 6/6 25.6
Major depressive disorder 8 5/3 17.0
Anxiety disorder 3 2/1 6.4
Learning/developmental disorders 2 0/2 4.2
Attention deficit/hyperactivity
disorder
1 0/1 2.1
Total 26 of 47 55.3
According to DSM-IV criteria, 26 of 47 or 55.3 % of all patients
showed one or more psychiatric disorder, mainly adjustment and
emotional disorders
Table 4 Number of patients with DSM IV relevant diagnoses
Inflammatory bowel disease DSM IV relevant disorders
No Yes Total
Crohn’s disease (n) 8 13 21
% of patients with CD 38.10 61.90
Ulcerative colitis (n) 13 13 26
% of patients with UC 50 50
Total 21 26 47
The difference between patients with CD and UC was not significant
in v2 test (v2 = 0.666)
Child Psychiatry Hum Dev
123
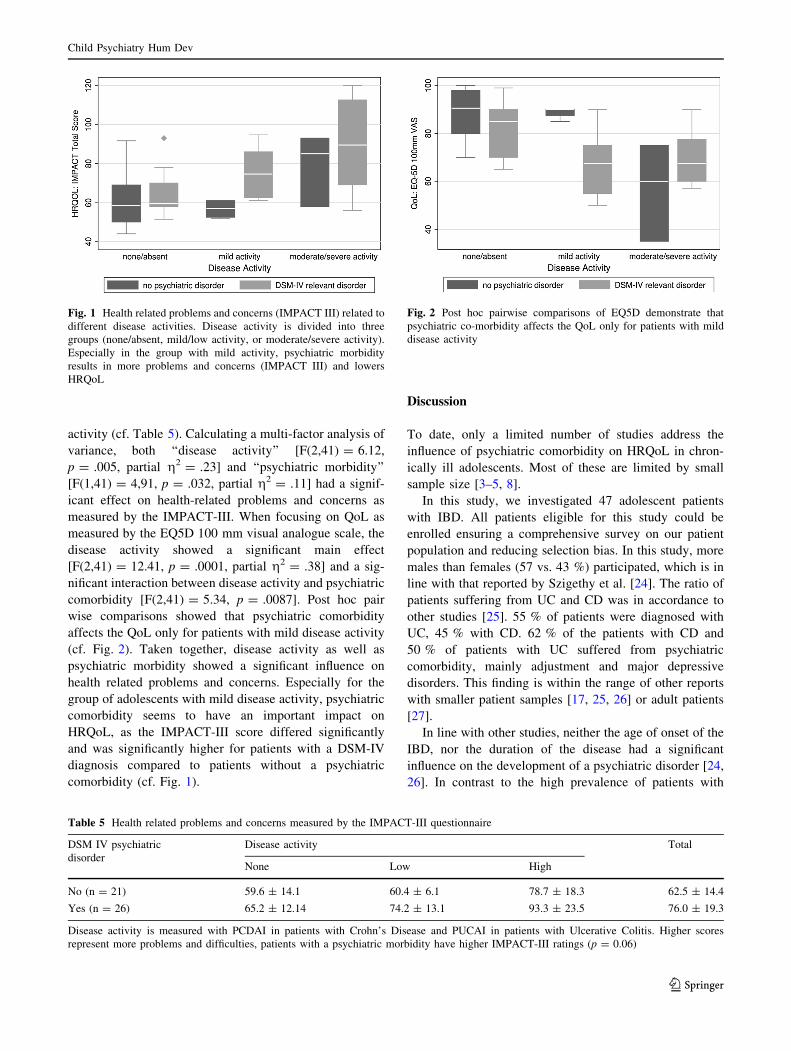
activity (cf. Table 5). Calculating a multi-factor analysis of
variance, both ‘‘disease activity’’ [F(2,41) = 6.12,
p = .005, partial g2 = .23] and ‘‘psychiatric morbidity’’
[F(1,41) = 4,91, p = .032, partial g2 = .11] had a signif-
icant effect on health-related problems and concerns as
measured by the IMPACT-III. When focusing on QoL as
measured by the EQ5D 100 mm visual analogue scale, the
disease activity showed a significant main effect
[F(2,41) = 12.41, p = .0001, partial g2 = .38] and a sig-
nificant interaction between disease activity and psychiatric
comorbidity [F(2,41) = 5.34, p = .0087]. Post hoc pair
wise comparisons showed that psychiatric comorbidity
affects the QoL only for patients with mild disease activity
(cf. Fig. 2). Taken together, disease activity as well as
psychiatric morbidity showed a significant influence on
health related problems and concerns. Especially for the
group of adolescents with mild disease activity, psychiatric
comorbidity seems to have an important impact on
HRQoL, as the IMPACT-III score differed significantly
and was significantly higher for patients with a DSM-IV
diagnosis compared to patients without a psychiatric
comorbidity (cf. Fig. 1).
Discussion
To date, only a limited number of studies address the
influence of psychiatric comorbidity on HRQoL in chron-
ically ill adolescents. Most of these are limited by small
sample size [3–5, 8].
In this study, we investigated 47 adolescent patients
with IBD. All patients eligible for this study could be
enrolled ensuring a comprehensive survey on our patient
population and reducing selection bias. In this study, more
males than females (57 vs. 43 %) participated, which is in
line with that reported by Szigethy et al. [24]. The ratio of
patients suffering from UC and CD was in accordance to
other studies [25]. 55 % of patients were diagnosed with
UC, 45 % with CD. 62 % of the patients with CD and
50 % of patients with UC suffered from psychiatric
comorbidity, mainly adjustment and major depressive
disorders. This finding is within the range of other reports
with smaller patient samples [17, 25, 26] or adult patients
[27].
In line with other studies, neither the age of onset of the
IBD, nor the duration of the disease had a significant
influence on the development of a psychiatric disorder [24,
26]. In contrast to the high prevalence of patients with
Fig. 1 Health related problems and concerns (IMPACT III) related to
different disease activities. Disease activity is divided into three
groups (none/absent, mild/low activity, or moderate/severe activity).
Especially in the group with mild activity, psychiatric morbidity
results in more problems and concerns (IMPACT III) and lowers
HRQoL
Table 5 Health related problems and concerns measured by the IMPACT-III questionnaire
DSM IV psychiatric
disorder
Disease activity Total
None Low High
No (n = 21) 59.6 ± 14.1 60.4 ± 6.1 78.7 ± 18.3 62.5 ± 14.4
Yes (n = 26) 65.2 ± 12.14 74.2 ± 13.1 93.3 ± 23.5 76.0 ± 19.3
Disease activity is measured with PCDAI in patients with Crohn’s Disease and PUCAI in patients with Ulcerative Colitis. Higher scores
represent more problems and difficulties, patients with a psychiatric morbidity have higher IMPACT-III ratings (p = 0.06)
Fig. 2 Post hoc pairwise comparisons of EQ5D demonstrate that
psychiatric co-morbidity affects the QoL only for patients with mild
disease activity
Child Psychiatry Hum Dev
123

psychiatric comorbidity in our study, only 11 of 47 (23 %)
had ever been in contact with a psychiatrist or a
psychologist.
As part of the KIGGS-study, which determined the state
of health of children and adolescents in Germany in 2006,
the BELLA-study asked 2,863 families with children or
adolescents about symptoms in different fields, including
psychiatric disorders’’ [28]. In 12.2 % of respondents there
were indications of a psychiatric disorder, 9.6 % most
likely had a psychiatric disorder. Similarly, Dopfner et al.
[29] found the general prevalence of psychiatric disorders
in children and adolescents to be around 18 %. In our
study, the number of patients with a psychiatric disorder is
much higher (55 %) which emphasizes the need to deal
with the quality of life of IBD patients and psychiatric
comorbidity. This is in line with other studies [11–13]. As a
result of these findings, we have implemented a low
threshold psychiatric liaison service for patients and their
families as part of our pediatric outpatient clinic for IBD.
The incidence of a psychiatric diagnosis in female
patients is 70 % compared to 45 % in males. That is sim-
ilar to a finding in another study by Szigethy et al. [30]
where female IBD adolescents had a higher risk for
depression compared to male patients. Another study found
a high percentage of anxiety disorders in patients with CD
[31]. Andrews et al. [32] reported a 33 % prevalence of
psychiatric disorders in adults with CD and 34 % in adults
with UC. Our data show an even higher burden of psy-
chiatric comorbidity in adolescent patients.
In our study the reported HRQoL in adolescent IBD
patients with psychiatric comorbidity was significantly
lower compared to those without a psychiatric comorbidity
(cf. Table 5). Three different explanations may contribute
to an understanding of this effect. Psychiatric comorbidity
can be seen as an additional burden lowering HRQoL. An
alternative hypothesis would be that, if disease activity has
an impact on HRQoL, it is more likely for these patients to
develop depressive symptoms, anxiety or adjustment dis-
orders. Finally, as a third rationale, cytokines, other
inflammatory and immune parameters or side effects of
medication could affect a vulnerable subgroup of patients
more than others, with a direct biological impact on brain
physiology evoking behavioral changes and psychosocial
consequences.
The multi-factor analyses of variance showed that dis-
ease activity had a major influence on HRQoL. This is in
line with previously reported findings [19] Disease activity
and psychiatric comorbidity together contributed signifi-
cantly to the amount of health-related problems and con-
cerns in the IMPACT III test, explaining 30 % of the
variance. Only in the subgroup of patients with mild dis-
ease, the psychiatric comorbidity contributed significantly
to the HRQoL. Our hypothesis to explain this effect can be
summarized as follows: in the extreme cases of no disease
activity (remission) and moderate or severe disease activ-
ity, the impact of disease activity on HRQoL overrides any
other effect (flooring/ceiling effect). For a subgroup of
patients who show a different coping style, with more
tendencies to depressive withdrawal and trait anxiety
independent of actual disease activity, these psychological
parameters show their effect on HRQoL. This group would
profit most from psychotherapeutic interventions, and it
should be a concern of future studies to evaluate treatment
response in relation to disease activity.
Although pediatric gastroenterologists are aware of
potential psychiatric comorbidity and compromised
HRQoL in IBD patients, in daily gastroenterology practice
this has a minor influence on therapy decisions. As pedi-
atric gastroenterologists are not trained to evaluate psy-
chiatric comorbidity, it is not easy for them to find out
which patient needs psychosocial or psychotherapeutic
help. The main focus of actions is optimizing therapy to
achieve remission, if possible, or at least alleviate symp-
toms and reduce disease severity. Our results imply rec-
ommendation for screening for psychiatric comorbidity
and the need for easy accessible support by a trained child
and adolescent psychiatrist or for example through struc-
tured consultation/liaison services.
To date, it is widely accepted that IBD in adolescents
with all its implications will raise the vulnerability for
psychiatric comorbidity [14, 27]. Adolescents with IBD are
at a very high risk for clinically relevant emotional or
behavioral problems. Since adjustment disorders account
for almost half of the present clinically relevant problems,
models for effective coping with these chronic diseases
need to be developed. Disease specific HRQoL instruments
(IMPACT-III) can support the pediatrician with informa-
tion on the course of the disease and with therapeutic
decisions. Generic screening instruments (SDQ) for psy-
chiatric disorders exist and can help to identify adolescents
in need.
Health-related quality of life was measured only at one
single time point. Therefore changes of the HRQoL over
time in association with changes in the severity of IBD
cannot be predicted from our data [33].
Furthermore, we can not make any judgments to trait
coping styles or the direction of effects based on cross-
sectional data. The study is a single center study. Diag-
noses and treatment of children with IBD were performed
in line with national and international standards [34, 35],
however an influence of the treatment practice in our centre
on the outcome of the study cannot be excluded.
In conclusion psychiatric comorbidity is a major prob-
lem in adolescent patients with IBD, irrespective of disease
activity. HRQoL in adolescents with IBD is influenced
by both disease activity and psychiatric comorbidity.
Child Psychiatry Hum Dev
123

However, disease activity contributes more to HRQoL than
psychiatric comorbidity in patients that are in remission or
suffer from high disease activity. The number of patients in
our setting with psychiatric comorbidity underlines the
need for a better understanding of the interaction of chronic
diseases and psychiatric diseases in adolescents. Further-
more, this confirms the importance of a multidisciplinary
treatment of adolescent patients with IBD including a child
psychiatrist. Only 23 % of the families participating in this
study had ever received specialized help in this field,
though 55 % had a psychiatric disorder based on DSM IV
criteria. Therefore, the need for accessible and acceptable
professional (psychotherapeutic and/or psychiatric) help is
obvious. New models of cooperation between child and
adolescent psychiatrist/psychotherapists and pediatricians
must be established to support IBD-affected patients and
their families.
Summary
Health-related quality of life in adolescents and children
with IBD was significantly reduced in patients with psy-
chiatric comorbidity. In all patients, psychiatric comor-
bidity together with disease activity contributed to a
reduction in quality of life, but the impact of disease
activity overrides any other effects when disease activity is
very high or very low. In addition to somatic care, there is a
need for accessible and acceptable, preferably structured
professional (psychotherapeutic and/or psychiatric) help
for adolescent patients with IBD.
Acknowledgments This study was supported by a Grant from the
Dietmar Hopp Stiftung.
References
1. Timmer A, Behrens R, Buderus S, Findeisen A, Hauer A, Keller
K-M et al (2011) Childhood onset inflammatory bowel disease:
predictors of delayed diagnosis from the CEDATA German-
language pediatric inflammatory bowel disease registry. J Pediatr
158(3):467.e2–473.e2
2. Mackner LM, Greenley RN, Szigethy E, Herzer M, Deer K,
Hommel KA (2013) Psychosocial issues in pediatric inflamma-
tory bowel disease: report of the North American Society for
Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr
Gastroenterol Nutr 56(4):449–458
3. Akobeng AK, Miller V, Firth D, Suresh-Babu MV, Mir P, Tho-
mas AG (1999) Quality of life of parents and siblings of children
with inflammatory bowel disease. J Pediatr Gastroenterol Nutr
28(4):S40–S42
4. Otley AR, Griffiths AM, Hale S, Kugathasan S, Pfefferkorn M,
Mezoff A et al (2006) Health-related quality of life in the first
year after a diagnosis of pediatric inflammatory bowel disease.
Inflamm Bowel Dis 12(8):684–691
5. Loonen HJ, Grootenhuis MA, Last BF, Koopman HM, Derkx
HHF (2002) Quality of life in paediatric inflammatory bowel
disease measured by a generic and a disease-specific question-
naire. Acta Paediatr 91(3):348–354
6. Saxena S, Orley J, WHOQOL Group (1997) Quality of life
assessment: the World Health Organization perspective. Eur
Psychiatry 12(Suppl 3):263–266
7. Borgaonkar MR, Irvine EJ (2000) Quality of life measurement in
gastrointestinal and liver disorders. Gut 47(3):444–454
8. Otley A, Smith C, Nicholas D, Munk M, Avolio J, Sherman PM
et al (2002) The IMPACT questionnaire: a valid measure of
health-related quality of life in pediatric inflammatory bowel
disease. J Pediatr Gastroenterol Nutr 35(4):557–563
9. Hyams JS, Ferry GD, Mandel FS, Gryboski JD, Kibort PM,
Kirschner BS et al (1991) Development and validation of a
pediatric Crohn’s disease activity index. J Pediatr Gastroenterol
Nutr 12(4):439–447
10. Turner D, Otley AR, Mack D, Hyams J, de Bruijne J, Uusoue K
et al (2007) Development, validation, and evaluation of a pedi-
atric ulcerative colitis activity index: a prospective multicenter
study. Gastroenterology 133(2):423–432
11. Thompson RJJ, Hodges K, Hamlett KW (1990) A matched
comparison of adjustment in children with cystic fibrosis and
psychiatrically referred and nonreferred children. J Pediatr Psy-
chol 15(6):745–759
12. Cadman D, Boyle M, Szatmari P, Offord DR (1987) Chronic
illness, disability, and mental and social well-being: findings of
the Ontario Child Health Study. Pediatrics 79(5):805–813
13. Thompson RD, Delaney P, Flores I, Szigethy E (2011) Cognitive-
behavioral therapy for children with comorbid physical illness.
Child Adolesc Psychiatr Clin N Am 20(2):329–348
14. Burke P, Meyer V, Kocoshis S, Orenstein DM, Chandra R, Nord
DJ et al (1989) Depression and anxiety in pediatric inflammatory
bowel disease and cystic fibrosis. J Am Acad Child Adolesc
Psychiatry 28(6):948–951
15. Engstrom I (1992) Mental health and psychological functioning
in children and adolescents with inflammatory bowel disease: a
comparison with children having other chronic illnesses and with
healthy children. J Child Psychol Psychiatry 33(3):563–582
16. Casati J, Toner BB, de Rooy EC, Drossman DA, Maunder RG
(2000) Concerns of patients with inflammatory bowel disease: a
review of emerging themes. Dig Dis Sci 45(1):26–31
17. Szajnberg N, Krall V, Davis P, Treem W, Hyams J (1993) Psy-
chopathology and relationship measures in children with
inflammatory bowel disease and their parents. Child Psychiatry
Hum Dev 23(3):215–232
18. Moody G, Eaden JA, Mayberry JF (1999) Social implications of
childhood Crohn’s disease. J Pediatr Gastroenterol Nutr 28(4):
S43–S45
19. Szigethy E, McLafferty L, Goyal A (2010) Inflammatory bowel
disease. Child Adolesc Psychiatr Clin N Am 19(2):301–18–ix
20. Angold A, Costello EJ (2000) The child and adolescent psychi-
atric assessment (CAPA). J Am Acad Child Adolesc Psychiatry
39(1):39–48
21. Association AP (1994) Dsm IV: diagnostic and statistical manual
of mental disorders, 4th edn. American Psychiatric Publication,
USA, p 1
22. Brislin RW (1970) Back-translation for cross-cultural research.
J Cross-Cult Psychol 1(3):185–216
23. Tarride J-E, Burke N, Bischof M, Hopkins RB, Goeree L,
Campbell K et al (2010) A review of health utilities across
conditions common in paediatric and adult populations. Health
Qual Life Outcomes 8:12
24. Szigethy E, Levy-Warren A, Whitton S, Bousvaros A, Gauvreau
K, Leichtner AM et al (2004) Depressive symptoms and
Child Psychiatry Hum Dev
123

inflammatory bowel disease in children and adolescents: a cross-
sectional study. J Pediatr Gastroenterol Nutr 39(4):395–403
25. Engstrom I (1991) Family interaction and locus of control in
children and adolescents with inflammatory bowel disease. J Am
Acad Child Adolesc Psychiatry 30(6):913–920
26. Engstrom I (1999) Inflammatory bowel disease in children and
adolescents: mental health and family functioning. J Pediatr
Gastroenterol Nutr 28(4):S28–S33
27. Hauser W, Janke KH, Klump B, Hinz A (2011) Anxiety and
depression in patients with inflammatory bowel disease: com-
parisons with chronic liver disease patients and the general
population. Inflamm Bowel Dis 17(2):621–632
28. Ravens-Sieberer U, Kurth B-M (2008) The mental health module
(BELLA study) within the German Health Interview and
Examination Survey of Children and Adolescents (KiGGS):
study design and methods. Eur Child Adolesc Psychiatry
17(Suppl 1):10–21
29. Dopfner M, Metternich TW, Berner W, Englert E, Lenz K, Le-
hmkuhl U et al (1997) Psychopathological evaluation of children
and adolescents in 4 child and adolescent psychiatry referral
groups—a multicenter study. Prax Kinderpsychol Kinderpsychi-
atr 46(8):548–565
30. Szigethy E, Carpenter J, Baum E, Kenney E, Baptista-Neto L,
Beardslee WR et al (2006) Case study: longitudinal treatment of
adolescents with depression and inflammatory bowel disease.
J Am Acad Child Adolesc Psychiatry 45(4):396–400
31. Addolorato G, Capristo E, Stefanini GF, Gasbarrini G (1997)
Inflammatory bowel disease: a study of the association between
anxiety and depression, physical morbidity, and nutritional status.
Scand J Gastroenterol 32(10):1013–1021
32. Andrews H, Barczak P, Allan RN (1987) Psychiatric illness in
patients with inflammatory bowel disease. Gut 28(12):1600–1604
33. Thompson RD, Craig A, Crawford EA, Fairclough D, Gonzalez-
Heydrich J, Bousvaros A et al (2012) Longitudinal results of
cognitive behavioral treatment for youths with inflammatory
bowel disease and depressive symptoms. J Clin Psychol Med
Settings 19(3):329–337
34. IBD Working Group of the European Society for Paediatric
Gastroenterology, Hepatology and Nutrition (2005) Inflammatory
bowel disease in children and adolescents: recommendations for
diagnosis—the Porto criteria. J Pediatr Gastroenterol Nutr
41(1):1–7
35. Turner D, Levine A, Escher JC, Griffiths AM, Russell RK,
Dignass A et al (2012) Management of pediatric ulcerative
colitis: joint ECCO and ESPGHAN evidence-based consensus
guidelines. J Pediatr Gastroenterol Nutr 55(3):340–361
Child Psychiatry Hum Dev
123

















