Embed Size (px)
Citation preview

Health Policy Seminar on Sunday, April 19th, 2009 Washington, D.C.
Shannon Brownlee
Visiting Scholar, NIH Clinical Center Dept. of Bioethics
Schwartz Senior Fellow, New America Foundation
Overtreated: Why Too Much Medicine is Making Us Sicker and Poorer

These views are mine alone, not the NIH’s
No financial conflicts of interest

1. Covering everybody is the right thing to do.
2. Rising healthcare costs hurt the economy.
3. We getting poor value for the dollar.

Poor Value for the Dollar
Source: WHO



Source: CBO

Source: CBO


1. Why do spending and quality vary so much in different parts of the country?
2. Why don’t we get better outcomes where we spend more?
3. Can looking at variation help us improve quality and outcomes without spending even more?

$8,600 – 14,300
$7,800 – 8,600
$7,200 – 7,800
$6,600 – 7,200
$5,280 – 6,600
Not populated
Medicare Spending per Beneficiary, 2005
Source: Dartmouth Atlas
$8,600 – 14,300
$7,800 – 8,600
$7,200 – 7,800
$6,600 – 7,200
$5,280 – 6,600
Not populated

1. Effective Care: Evidence-based care that all with need should receive
2. Preference-Sensitive Care: Elective procedures and tests whose use should depend upon the patient’s choice
3. Supply-Sensitive Care: Discretionary hospitalizations, visits, and procedures

63%12%
25%
Preference Sensitive Care
Effective Care
Supply Sensitive Care
Source: John E. Wennberg and Dartmouth Atlas

Wennberg has conducted pioneering research on variation in the delivery of healthcare services.Named the most influential health policy researcher of the past 25 years by Health Affairs in 2007 14
John Wennberg, MD, MPH., Founder, Center for Evaluative Clinical Sciences at Dartmouth Medical School

$8,600 – 14,300
$7,800 – 8,600
$7,200 – 7,800
$6,600 – 7,200
$5,280 – 6,600
Not populated
Medicare Spending per Beneficiary, 2005
Source: Dartmouth Atlas
$8,600 – 14,300
$7,800 – 8,600
$7,200 – 7,800
$6,600 – 7,200
$5,280 – 6,600
Not populated


Source: 2006 Dartmouth AtlasNote: Each dot represents Medicare spending in a single hospital referral region.


WHAT DRIVES UTILIZATION?


1. Defensive medicine -- 15 % of variation
2. Patient demand3. Tech arms race4. Local practice patterns5. LOCAL CAPACITY

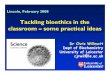
The Association Between Hospital Beds per 1,000 Residents (1996) and Discharges per 1,000 Medicare Enrollees (1995-96)


In other words: Do higher spending (and
higher utilization) buy better outcomes?


1. Lower quality2. More hospitalizations, tests, drugs,
procedures; same volume of elective surgery
3. Worse communication between physicians4. Worse coordination of care5. Worse access to care; longer waiting times6. Lower patient satisfaction
7. Higher mortalitySource: 2008 Dartmouth Atlas of Chronic Care

Fisher et al (2003) Annals of Int. Med. Vol. 138 no. 4


•The frequency of use is governed by the assumption that resources should be fully utilized, i.e. that more is better
•Specific medical theories and medical evidence play little role in governing frequency of use
•In the absence of evidence and under the assumption that more is better, available supply governs frequency of use

Fisher E et al. N Engl J Med 2009;360:849-852
Annual Growth Rates of per Capita Medicare Spending in Five U.S. Hospital-Referral Regions,
1992-2006

THE BAD $600 – 800 billion of unnecessary and potentially harmful care
THE GOOD $600 B on useless care -- We can cut costs without rationing.
IMPLICATIONS

1. $19 Billion in health IT2. Comparative effectiveness research3. Slash Medicare Advantage4. Bundled payment for surgical procedures5. Pay four Performance:
1. Non-payment for never events2. Non-payment for rehospitalization3. Bonus for evidence based care4. Outcomes reporting

1. $19 BILLION to automate bad practices -- sand down a rat hole
2. Comparative effectiveness research is too narrow and too slow to make a dent in supply sensitive spending (62 % of Medicare)
3. Bundled payments equal price control4. Non-payment leads to gaming the rules5. Medicare advantage could be helping

$8,600 – 14,300
$7,800 – 8,600
$7,200 – 7,800
$6,600 – 7,200
$5,280 – 6,600
Not populated
Sucking Sound of $$ going from low spending to high spending regions
Source: Dartmouth Atlas
$8,600 – 14,300
$7,800 – 8,600
$7,200 – 7,800
$6,600 – 7,200
$5,280 – 6,600
Not populated

MEDICARE1.Contain payments to high-spending hospitals
1.Do NOT increase physician workforce
1.Encourage more primary care

EMPLOYERS
1.HSAs that encourage primary care
2.Give employees benefit of choosing cheaper options like Kaiser
3.Encourage EFFICIENT organized group practices (like Kaiser)
4.Offer Patient Decision Aids

HOW DO WE RE-DESIGN THE
DELIVERY SYSTEM?(It’s the delivery system, stupid)

THE HEALTH CARE TRAIN WRECK