Embed Size (px)
Citation preview

HEALTH PLAN & FORMULARYCOMPARISON GUIDE
A Simple Resource to Help YouUnderstand Your Benefits


Contents
What Does Prescription Drug Formulary Mean? . . . . . . . . . . . . . 3
How To Use This Comparison Guide . . . . . . . . . . . . . . . . . . . . . . 3
A Note To Members . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Health Plan Accreditation Status . . . . . . . . . . . . . . . . . . . . . . . . . 4
Prescription Drug Benefits/Copays . . . . . . . . . . . . . . . . . . . . . . . 5-6
Non-Formulary & Mail Order Rx Benefits/Copays . . . . . . . . . . . . 7-8
Brand Name/Generic Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . 9-12
Physician Access & Referral . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13-14
Well Woman & Infertility Benefits . . . . . . . . . . . . . . . . . . . . . . . . 15-16
Prescription Drug Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17-20
Diabetes Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21-22
Important Health Plan Telephone Numbers . . . . . . . . . . . . . . . . . Back Cover
PAGE
2

A Note To MembersPrior to using this Comparison Guide to make a benefit or Healthcare Service Plan decision, please call the
Healthcare Service Plan directly to confirm the accuracy of the information provided . Healthcare Service
Plan phone numbers are listed on the back cover of this booklet . This booklet is a summary only.
The Evidence of Coverage (EOC) and the Certificate of Insurance (COI) contain a complete explanation of
benefits, exclusions, and limitations . The information provided in this brochure is not intended for use
as a benefit summary, nor is it designed to serve as the Evidence of Coverage or Certificate of Insurance.
Please note that you can access your Summary of Benefits and Coverage (SBC), EOC or COI by logging in to
www .calchoice .com/documents/ . If you would like a printed copy of the SBC please contact our Customer
Service Department at 866 .451 .7587 .
What Does Prescription Drug Formulary Mean?A Prescription Drug formulary is an approved list of drugs that have been reviewed for safety, quality, effectiveness
and cost by the physicians and pharmacists on a Healthcare Service Plan’s Rx review panel . A non-formulary
drug refers to a drug that is not included on the approved Rx list for a Healthcare Service Plan . Each Healthcare
Service Plan has its own formulary or approved drug list that is reviewed on a regular basis .
How To Use This Comparison GuideIf you are currently using a brand name drug prescription:
Proceed to the alphabetical listing of brand drugs on pages 9-12 . Next to each brand name drug is its
formulary/non-formulary status in each Healthcare Service Plan . For your convenience, a generic equivalent—
if one is available—is listed directly underneath each brand listing .
If you can’t find your prescription drug in this booklet, or your drug is considered non-formulary:
Visit our online formulary guide at www.calchoiceplus.com or contact your Healthcare Service Plan .
3

NCQA Health Plan Accreditation StatusWhat is NCQA Accreditation?
NCQA stands for the National Committee for Quality Assurance, a not-for-profit organization that evaluates how
well a Healthcare Service Plan manages its clinical and administrative systems in order to improve health care
quality for its members .
An NCQA team of physicians and managed care experts conducts rigorous on and off site evaluations . A national
oversight committee — made up of physicians — analyzes the team’s findings and assigns an Accreditation
level based on the plan’s performance compared to NCQA standards . NCQA has purposely set high standards
to encourage Healthcare Service Plans to enhance their quality . Below are the latest ratings from the NCQA for
health plans participating in CaliforniaChoice 51+ .
The following HMOs have an “Excellent” rating from the NCQA for their commercial products:
Kaiser Foundation Health Plan, Inc . - Southern California (HMO) Kaiser Foundation Health Plan, Inc . - Northern California (HMO)
Western Health Advantage (HMO)
The following HMO has a “Commendable” rating from the NCQA for their commercial products:
Health Net of California, Inc . (HMO)
4

CalChoice® 51+ HMO 15*
CalChoice 51+ HMO 15 Value
CalChoice 51+ HMO 20/$500 Value
CalChoice 51+ HMO 25*
CalChoice 51+ HMO 25*
Participating Health Plans
Health Net, Kaiser Permanente, Western Health
AdvantageHealth Net Kaiser Permanente Health Net, Western Health
Advantage Kaiser Permanente
Generic $10 copay $15 copay $10 copay $15 copay $10 copay
Brand $20 copay $150 ded-$30 copay $100 ded-$30 copay $25 copay $25 copay
* The copay shall be the designated amount or the provider’s contract rate, whichever is less .** HSA-Qualified Health Savings Plan
CalChoice® 51+ HMO 25 Value
CalChoice 51+ HMO 40*
CalChoice 51+ HMO 40*
CalChoice 51+ HMO 40 Value Elect Open Access
Participating Health Plans Health Net Health Net, Western Health
Advantage Kaiser Permanente Health Net Health Net
Generic $20 copay $20 copay $15 copay $20 copay $15 copay
Brand $200 ded-$40 copay $35 copay $30 copay $250 ded-$40 copay $25 copay
Salud HMO y Más HDHP 1500** HSA 1800
Participating Health Plans Health Net Kaiser Permanente Western Health Advantage
Generic $15 copay $0 Per Rx After Ded $0 Per Rx After Ded
Brand $25 copay $0 Per Rx After Ded $0 Per Rx After Ded
Prescription Drug Benefits/Copays
Based on the benefit level you choose, each CaliforniaChoice 51+ HMO offers copay benefits for brand and generic drugs included on each Healthcare Service Plan’s Formulary Listing . Each Healthcare Service Plan maintains a different Formulary Listing of prescription drugs that they will cover . Our Health Plan & Formulary Comparison Guide is provided to assist you in looking up some of the more commonly prescribed drugs . These are the standard HMO prescription benefits for brand and generic drugs (covers a 30 day supply or 100 unit dose):
HMO Rx Benefits:
For HMO Non-Formulary Prescription and Mail Order Benefits/Copays, see page 7
5

CaliforniaChoice 51+ features 4 different Health Net PPO benefit levels, a plan for out-of-state employees and 2 Health Savings Account (HSA) options: CalChoice 51+ HSA 1500 and 2000:
CalChoice® 51+ PPO 250 CalChoice 51+ PPO 500 CalChoice 51+ PPO 1000 CalChoice 51+ PPO 1500
ParticipatingPharmacy
Non-ParticipatingPharmacy*
ParticipatingPharmacy
Non-ParticipatingPharmacy*
ParticipatingPharmacy
Non-ParticipatingPharmacy*
ParticipatingPharmacy
Non-ParticipatingPharmacy*
Generic $10 $10 + 50%* $10 $10 + 50% $10 $10 + 50% $10 $10 + 50%
FormularyBrand $20 $20 + 50%* $20 $20 + 50%* $20 $20 + 50%* $20 $20 + 50%
BrandDeductible N/A N/A $100 $100* $150 $150 $150 $150
CalChoice 51+ HSA 1500 CalChoice 51+ HSA 2000 Flex Net Indemnity(out-of-state)
ParticipatingPharmacy
Non-ParticipatingPharmacy*
ParticipatingPharmacy
Non-ParticipatingPharmacy*
ParticipatingPharmacy
Non-ParticipatingPharmacy*
Generic $10 after plan deductible
$10 + 50%after plan deductible
$15 after plan deductible
$15 + 50%after plan deductible 20% Not Covered
FormularyBrand
$25 after plan deductible
$25 + 50%after plan deductible
$30 after plan deductible
$30 + 50%after plan deductible 20%* Not Covered
BrandDeductible
All prescription drug benefits are subject to combined medical and prescription drug
deductible of $1500 per individual .
All prescription drug benefits are subject to combined medical and prescription drug
deductible of $1500 per individual .
All prescription drug benefits are subject to combined medical and prescription drug
deductible of $2000 per individual .
All prescription drug benefits are subject to combined medical and prescription drug
deductible of $2000 per individual .
$75 applies to all Rx’s Not Covered
Prescription Drug Benefits/Copays
Based on the benefit level you choose, each CaliforniaChoice 51+ PPO offers copay benefits for brand and generic drugs included on each Healthcare Service Plan’s Formulary Listing . Each Healthcare Service Plan maintains a different Formulary Listing of prescription drugs that they will cover . Our Health Plan & Formulary Comparison Guide is provided to assist you in looking up some of the more commonly prescribed drugs . These are the standard PPO prescription benefits for brand and generic drugs (covers a 30 day supply):
PPO Rx Benefits:
For PPO Non-Formulary Prescription and Mail Order Benefits/Copays, see page 8
6
* Member must try and fill with the generic first . If the member opts for brand without first trying the generic an additional ancillary copay may apply .

An Rx Formulary is an approved list of drugs that have been reviewed for safety, quality, effectiveness and cost by the physicians and pharmacists on a Healthcare Service Plan’s Rx review panel . A non-formulary drug refers to a drug that is not included on the approved Rx list for a Healthcare Service Plan . Each Healthcare Service Plan has its own formulary, or approved drug list, which is reviewed on a regular basis .
Experimental, non-FDA approved, not medically necessary and over-the-counter drugs are not covered under the Non-Formulary benefit of any Healthcare Service Plan . As always, please confirm all information directly with the Healthcare Service Plan prior to making an enrollment decision or accessing coverage .
Non-Formulary & Mail Order Rx Benefits/Copays—HMO
7
Health Net HMO, Elect Open Access & Salud HMO y Más
Kaiser Permanente HMO and HDHP
Western Health Advantage HMO and HSA
HMO 15: Generic $20Brand $40Non-Formulary $100
HMO 15 Value: Generic $30Brand $60Non-Formulary $100$150 Deductible Brand
HMO 25 Generic $30Brand $50Non-Formulary $100 HMO 25 ValueGeneric $40Brand $80Non-Formulary $100$200 Deductible Brand
HMO 40: Generic $40 Brand $70Non-Formulary $100
HMO 40 Value: Generic $40Brand $80Non-Formulary $100$250 Deductible Brand
Elect Open Access: Generic $30Brand $50Non-Formulary $100
Salud HMO y Más: Generic $30Brand $50Non-Formulary $100
Up to 100 Day Supply:
HMO 15: Generic $20Brand $40
HMO 20/$500 Value: Generic $10Brand $30
HMO 25: Generic $20 Brand $50
HMO 40: Generic $30 Brand $60
HDHP 1500: Applies to plan deductible, then $0 copay
No mail order benefit for Non-Formulary
90 Day Supply:
HMO 15: Generic $25Brand $50Non-Formulary $125
HMO 25: Generic $38Brand $63Non-Formulary $125
HMO 40: Generic $50 Brand $88Non-Formulary $125
HSA 1800: Applies to plan deductible, then $0 copay
Non-Formulary Benefits—HMOHealth Net HMO, Elect Open Access
and Salud HMO y MásKaiser Permanente
HMO and HDHPWestern Health Advantage
HMO and HSA
$50 Non-Formulary copay applies
Prior authorization may be required .
HMO:If deemed medically necessary by Kaiser Permanente
Physician .
HDHP 1500:If deemed medically necessary by Kaiser Permanente
Physician .
Applies to plan deductible, then $0 copay
HMO:$50 Non-Formulary copay applies .
HSA 1800: Applies to pan deductible, then $0 copay .
Prior authorization may be required .
Mail Order Benefits—HMO
90 Day Supply:

Non-Formulary & Mail Order Rx Benefits/Copays—PPO
* Prescription Drugs are subject to the medical deductible . The submission of a prescription drug claim is required for reimbursement of all outpatient prescription drugs .
8
Non-Formulary Benefits—PPO
Health Net PPO & Indemnity
CalChoice® 51+PPO 250
Participating Pharmacy:
$35
Non-Participating Pharmacy:$35 + 50%
CalChoice 51+PPO 500
Participating Pharmacy:
$35
Non-Participating Pharmacy:$35 + 50%
($100 per individual Brand deductible
applies)
CalChoice 51+PPO 1000
Participating Pharmacy:
$35
Non-Participating Pharmacy:$35 + 50%
($150 per individual Brand deductible
applies)
CalChoice 51+PPO 1500
Participating Pharmacy:
$35
Non-Participating Pharmacy:$35 + 50%
($150 per individual Brand deductible
applies)
CalChoice 51+HSA 1500
Participating Pharmacy:
$50 after plandeductible
Non-Participating Pharmacy:
$50 + 50% after plan deductible
CalChoice 51+HSA 2000
Participating Pharmacy:
$50 after plandeductible
Non-Participating Pharmacy:
$50 + 50% after plan deductible
Flex Net Indemnity(out of state) Participating Pharmacy:
Member has a 20% copay for all
medications regardless of formulary alternatives
Non-Participating Pharmacy:Not Covered
Health Net PPO & Indemnity
CalChoice 51+
PPO 25090 Day Supply:
Generic $20Brand $40Non-Formulary $70
CalChoice 51+
PPO 50090 Day Supply:
Generic $20Brand $40Non-Formulary $70
A separate $100 per individual deductible applies to Formulary and Non-Formulary
Brand drugs
CalChoice 51+
PPO 100090 Day Supply:
Generic $20Brand $40Non-Formulary $70
A separate $150 per individual deductible applies to Formulary and Non-Formulary
Brand drugs
CalChoice 51+
PPO 150090 Day Supply:
Generic $20Brand $40Non-Formulary $70
A separate $150 per individual deductible applies to Formulary and Non-Formulary
Brand drugs
CalChoice 51+
HSA 1500*90 Day Supply:
Generic $20Brand $50Non-Formulary $100
All prescription drug benefits are subject to combined medical and prescription drug deductible of $1500
per individual
CalChoice 51+
HSA 200090 Day Supply:
Generic $30Brand $60Non-Formulary $100
All prescription drug benefits are subject to combined medical and prescription drug deductible of $2000
per individual
Flex Net IndemnityMembers are allowed
to use the Rx by mail program, however they are not given
any type of discount . Therefore, it is their 20% coinsurance x 3 months
Mail Order Benefits—PPO

Generic equivalentin italics
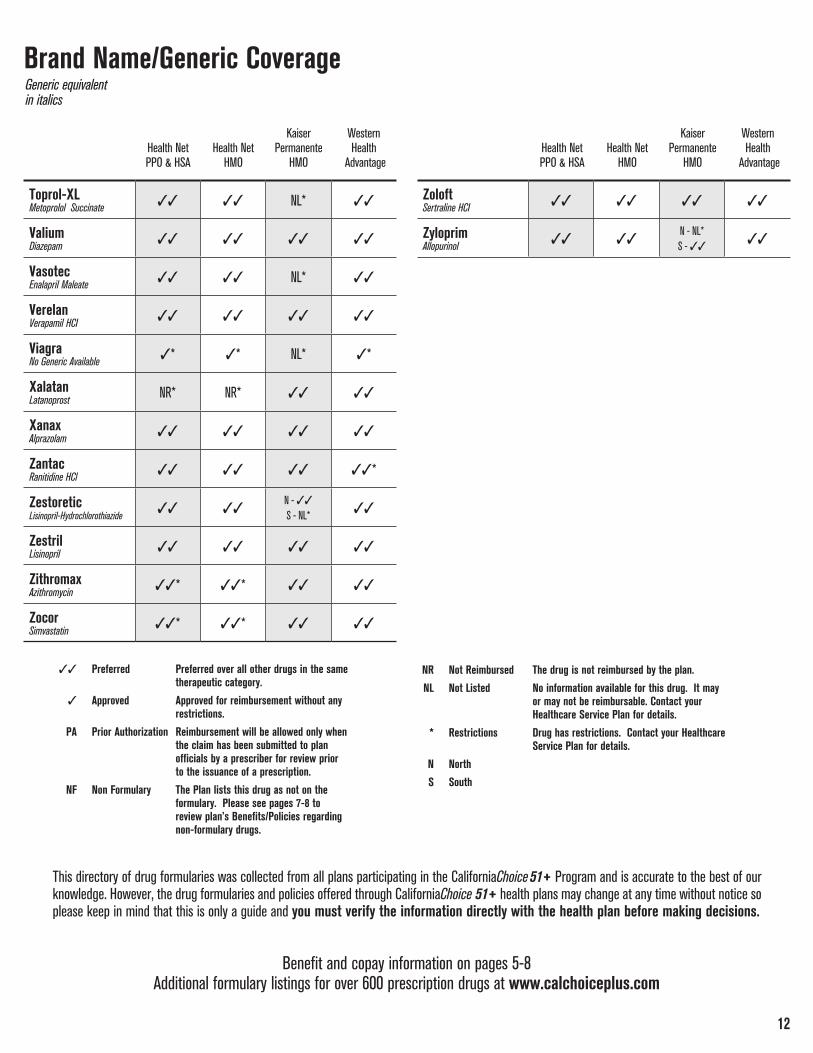
Brand Name/Generic Coverage
Benefit and copay information on pages 5-8Additional formulary listings for over 600 prescription drugs at www.calchoiceplus.com
This directory of drug formularies was collected from all plans participating in the CaliforniaChoice 51+ Program and is accurate to the best of our knowledge . However, the drug formularies and policies offered through CaliforniaChoice 51+ health plans may change at any time without notice so please keep in mind that this is only a guide and you must verify the information directly with the health plan before making decisions.
9
33 Preferred Preferred over all other drugs in the same therapeutic category.
3 Approved Approved for reimbursement without any restrictions.
PA Prior Authorization Reimbursement will be allowed only when the claim has been submitted to plan officials by a prescriber for review prior to the issuance of a prescription.
NF Non Formulary The Plan lists this drug as not on the formulary. Please see pages 7-8 to review plan’s Benefits/Policies regarding non-formulary drugs.
NR Not Reimbursed The drug is not reimbursed by the plan.
NL Not Listed No information available for this drug. It may or may not be reimbursable. Contact your Healthcare Service Plan for details.
* Restrictions Drug has restrictions. Contact your Healthcare Service Plan for details.
N North
S South
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
AccolateZafirlukast NR* NR* NL* NL
AccuprilQuinapril HCI 33 33 NL* 33
Adalat CCNifedipine 33 33 33 33
AllegraFexofenadine HCI NL NL NL* NL
AltaceRamipril NR* NR* NL* NL
AmbienZolpidem NR* NR* 33 33*
AtivanLorazepam 33 33 33 33
Atrovent Ipratropium Bromide 33 33 33 33
AvitaTretinoin 33 33 33 33*
AxidNizatidine 33 33 NL* NL
Bactrim DSSulfamethoxazole-Trimethoprim 33 33 33 33
Beconase AQNo Generic Available 3* 3* NL* 3
BiaxinClarithromycin 33* 33* 33 33
Cardizem CD Diltiazem HCl Coated Beads 3 3
N - NL*S - 33
NL
Cardura Doxazosin Mesylate 33 33 33 33
Catapres Clonidine HCl 33 33 33 33
Celexa Citalopram Hydrobromide 33 33 33 33
Ciloxan Ciprofloxacin HCl 33 33
N - NL*S - 33 33
Cipro Ciprofloxacin 33 33 33 33
CortisporinNeomycin-Polymyxin-HC 33 33 33 33
Coumadin Warfarin Sodium 33 33 33 33
Cozaar Losartan NR NR 33 33*
Cutivate Fluticasone Propionate 33 33 NL* 33
Daypro Oxaprozin 33 33 NL* 33

Generic equivalentin italics
Brand Name/Generic Coverage
Benefit and copay information on pages 5-8Additional formulary listings for over 600 prescription drugs at www.calchoiceplus.com
This directory of drug formularies was collected from all plans participating in the CaliforniaChoice 51+ Program and is accurate to the best of our knowledge . However, the drug formularies and policies offered through CaliforniaChoice 51+ health plans may change at any time without notice so please keep in mind that this is only a guide and you must verify the information directly with the health plan before making decisions.
10
33 Preferred Preferred over all other drugs in the same therapeutic category.
3 Approved Approved for reimbursement without any restrictions.
PA Prior Authorization Reimbursement will be allowed only when the claim has been submitted to plan officials by a prescriber for review prior to the issuance of a prescription.
NF Non Formulary The Plan lists this drug as not on the formulary. Please see pages 7-8 to review plan’s Benefits/Policies regarding non-formulary drugs.
NR Not Reimbursed The drug is not reimbursed by the plan.
NL Not Listed No information available for this drug. It may or may not be reimbursable. Contact your Healthcare Service Plan for details.
* Restrictions Drug has restrictions. Contact your Healthcare Service Plan for details.
N North
S South
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Desogen Desogestrel-Ethinyl Estradiol NR NR NL* NL
Diflucan Fluconazole 33* 33* 33 33
Dilacor XR Diltiazem HCl 33 33 33 33
Diovan No Generic Available 3* 3* NL* 3*
Dyazide Triamterene - HCTZ 33 33 33 33
Effexor Venlafaxine HCI 33* 33* 33 33
Estrace Estradiol 33* 33* 33 33
Estraderm Estradiol 33* 33* 33 33
FlexerilCyclobenzaprine HCl 33* 33* 33 33
Fosamax Alendronate NR* NR* N - 33*
S - 3333
Hycodan Hydrocodone-Homatropine 33 33 33 NL
Hyzaar Losartan-Hydrochlorothiazide 33* 33* 33 33*
Imdur Isosorbide Mononitrate 33 33 33 33
Imitrex Sumatriptan NR* NR* 33 33*
Keflex Cephalexin 33 33 33 33
Kenalog in OrabaseTriamcinolone Acetonide 33 33
N - NL*S - 33
33
Lanoxin Digoxin 33 33 33 33
Lasix Furosemide 33 33 33 33
Levaquin Levofloyacin 3* 3* 33 33
Lipitor No Generic Available??? NR* NR* 33 33
Lopressor Metoprolol Tartrate NL NL 33 33
Lorabid No Generic Available NL NL NL* NL
Lotensin Benazepril HCl 33 33 NL* 33
Lotensin HCT Benazepril-Hydrochlorothiazide 33 33 NL* 33

11
Brand Name/Generic Coverage
33 Preferred Preferred over all other drugs in the same therapeutic category.
3 Approved Approved for reimbursement without any restrictions.
PA Prior Authorization Reimbursement will be allowed only when the claim has been submitted to plan officials by a prescriber for review prior to the issuance of a prescription.
NF Non Formulary The Plan lists this drug as not on the formulary. Please see pages 7-8 to review plan’s Benefits/Policies regarding non-formulary drugs.
NR Not Reimbursed The drug is not reimbursed by the plan.
NL Not Listed No information available for this drug. It may or may not be reimbursable. Contact your Healthcare Service Plan for details.
* Restrictions Drug has restrictions. Contact your Healthcare Service Plan for details.
N North
S South
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Lotrisone Clotrimazole-Betamethasone 33* 33* NL* 33
Macrobid Nitrofurantoin Monohyd Macro 33 33 33 33
Macrodantin Nitrofurantoin Macrocrystal 33 33 33 33
Micro-K Potassium Chloride 33 33 33 33
Neurontin Gabapentin 33 33 33 33
Nitrostat Nitroglycerin 33* 33* 33 33
Norvasc Amlodipine Besylate 33* 33* 33 33
Plendil Felodipine 33 33 NL* 33
Pravachol Pravastatin Sodium 33* 33* 33 33
Prevacid Lansoprazole NR* NR* NL* 33
Prinivil Lisinopril 33 33 33 33
Prinzide Lisinopril-Hydrochlorothiazide 33 33
N - 33
S - NL* 33
Procardia XL Nifedipine 33 33 33 33
Provera Medroxyprogesterone Acetate 33 33 33 33
Prozac Fluoxetine HCI 33* 33* 33 33
Restoril Temazepam 33* 33* 33 33*
Retin-A Tretinoin 33 33 33 33*
Risperdal No Generic Available NR NR 33 33
Septra DS Sulfamethoxazole-Trimethoprim 33 33 33 33
Soma Carisoprodol 33 33 NL* 33
Tenormin Atenolol 33 33 33 33
Tiazac Diltiazem HCI ER Beads 33 33 NL* NL
Timoptic XE Timolol Maleate 33 33 33 33
TobraDex Tobramycin-Dexamethasone 3* 3*
N - 3S - 33
33
Generic equivalentin italics
Benefit and copay information on pages 5-8Additional formulary listings for over 600 prescription drugs at www.calchoiceplus.com
This directory of drug formularies was collected from all plans participating in the CaliforniaChoice 51+ Program and is accurate to the best of our knowledge . However, the drug formularies and policies offered through CaliforniaChoice 51+ health plans may change at any time without notice so please keep in mind that this is only a guide and you must verify the information directly with the health plan before making decisions.
33 Preferred Preferred over all other drugs in the same therapeutic category.
3 Approved Approved for reimbursement without any restrictions.
PA Prior Authorization Reimbursement will be allowed only when the claim has been submitted to plan officials by a prescriber for review prior to the issuance of a prescription.
NF Non Formulary The Plan lists this drug as not on the formulary. Please see pages 7-8 to review plan’s Benefits/Policies regarding non-formulary drugs.
NR Not Reimbursed The drug is not reimbursed by the plan.
NL Not Listed No information available for this drug. It may or may not be reimbursable. Contact your Healthcare Service Plan for details.
* Restrictions Drug has restrictions. Contact your Healthcare Service Plan for details.
N North
S South
12
Brand Name/Generic Coverage
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Western Health
Advantage
Kaiser Permanente
HMOHealth Net
HMOHealth Net PPO & HSA
Toprol-XL Metoprolol Succinate 33 33 NL* 33
ValiumDiazepam 33 33 33 33
Vasotec Enalapril Maleate 33 33 NL* 33
Verelan Verapamil HCI 33 33 33 33
Viagra No Generic Available 3* 3* NL* 3*
Xalatan Latanoprost NR* NR* 33 33
Xanax Alprazolam 33 33 33 33
Zantac Ranitidine HCl 33 33 33 33*
Zestoretic Lisinopril-Hydrochlorothiazide 33 33
N - 33
S - NL* 33
Zestril Lisinopril 33 33 33 33
Zithromax Azithromycin 33* 33* 33 33
Zocor Simvastatin 33* 33* 33 33
Zoloft Sertraline HCI 33 33 33 33
Zyloprim Allopurinol 33 33
N - NL*S - 33
33
Generic equivalentin italics
Benefit and copay information on pages 5-8Additional formulary listings for over 600 prescription drugs at www.calchoiceplus.com
This directory of drug formularies was collected from all plans participating in the CaliforniaChoice 51+ Program and is accurate to the best of our knowledge . However, the drug formularies and policies offered through CaliforniaChoice 51+ health plans may change at any time without notice so please keep in mind that this is only a guide and you must verify the information directly with the health plan before making decisions.

Q U E S T I O N SHealth Net HMO,
Elect Open Access and Salud HMO y Más
Kaiser PermanenteHMO and HDHP
Western Health AdvantageHMO and HSA
How often can my family members and I change Primary Care Physicians (PCP)?
Once a month Anytime
Once a month - changes are effective at the beginning of the following month, provided the member is not in the course of
treatment or hospitalized and no pending authorizations
Can each family member choose a different Primary Care Physician from different medical groups?
Yes Yes—but only from Health Plan Physicians
Yes—but only from network physicians
Can I refer myself to a specialist?(For OB/GYN referral information, see pages 15-16)
Yes—if using a Rapid Access Provider
OB/GYN: Yes
Other Specialties:Yes—to certain specialties .
Self-refer specialties list varies by geographical region
Yes—to an ophthalmologist only, for your annual eye exam
Does the Health Carrier offer a program to help speed up the specialist referral process?
Yes—some Rapid Access Providers offer express referrals
Yes—referrals come directly from PCP; no other approval is needed
Yes—Advantage Referral Program allows PCP to refer member to
any specialist in the WHA network who participates in the Advantage
Referral Program
Are dependents who live out-of-area covered?
Yes—they may enroll based on the subscriber’s work address (within the
service area) . The dependent must travel to that PPG for non-emergency/non-urgent care services they receive . Services that are covered outside the
HN Service Area are for limited to emergency/urgent services only
Dependent children of Subscriber or Subscriber’s Spouse - Yes .
Other dependents are eligible as long as they do not live in or move
to the service area of another Kaiser Permanente region
Yes—full-time student dependents outside of the service area are covered for emergency
and urgently needed services only
Physician Access & Referral—HMO
CaliforniaChoice 51+ HMO 15, 15 Value, 20/$500 Value, 25, 25 Value, 40, 40 Value and EOA members may go to an Urgent Care Facility contracted through their medical group (PMG) or Individual Practice Association (IPA) for the same copay as their Primary Care Physician (PCP) office visit copay . Please contact your selected PMG or IPA to find out if they contract with an Urgent Care Facility and where it is located, so you will have this information handy when needed .Note: All HMO benefits are covered in-network only .All CaliforniaChoice 51+ Health Plans cover life threatening emergencies anywhere in the world .
13
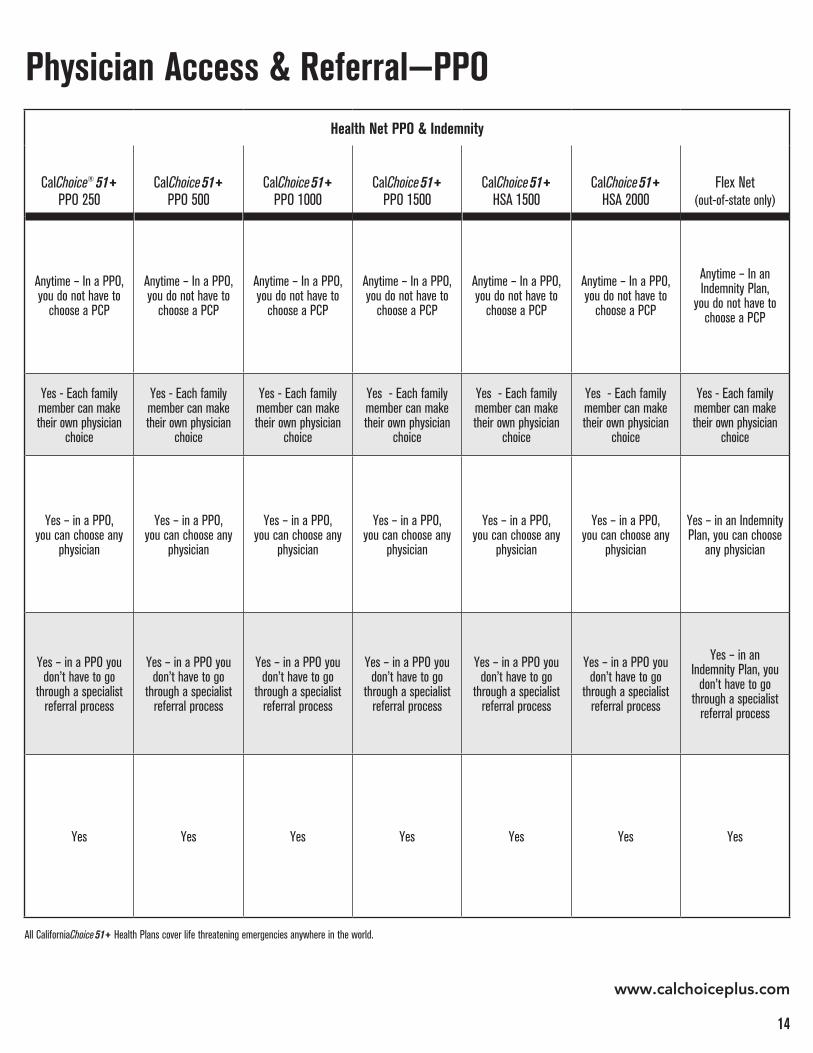
Health Net PPO & Indemnity
CalChoice® 51+
PPO 250CalChoice 51+
PPO 500CalChoice 51+
PPO 1000CalChoice 51+
PPO 1500CalChoice 51+
HSA 1500CalChoice 51+
HSA 2000Flex Net
(out-of-state only)
Anytime – In a PPO, you do not have to
choose a PCP
Anytime – In a PPO, you do not have to
choose a PCP
Anytime – In a PPO, you do not have to
choose a PCP
Anytime – In a PPO, you do not have to
choose a PCP
Anytime – In a PPO, you do not have to
choose a PCP
Anytime – In a PPO, you do not have to
choose a PCP
Anytime – In an Indemnity Plan,
you do not have to choose a PCP
Yes - Each family member can make their own physician
choice
Yes - Each family member can make their own physician
choice
Yes - Each family member can make their own physician
choice
Yes - Each family member can make their own physician
choice
Yes - Each family member can make their own physician
choice
Yes - Each family member can make their own physician
choice
Yes - Each family member can make their own physician
choice
Yes – in a PPO, you can choose any
physician
Yes – in a PPO, you can choose any
physician
Yes – in a PPO, you can choose any
physician
Yes – in a PPO, you can choose any
physician
Yes – in a PPO, you can choose any
physician
Yes – in a PPO, you can choose any
physician
Yes – in an Indemnity Plan, you can choose
any physician
Yes – in a PPO you don’t have to go
through a specialist referral process
Yes – in a PPO you don’t have to go
through a specialist referral process
Yes – in a PPO you don’t have to go
through a specialist referral process
Yes – in a PPO you don’t have to go
through a specialist referral process
Yes – in a PPO you don’t have to go
through a specialist referral process
Yes – in a PPO you don’t have to go
through a specialist referral process
Yes – in an Indemnity Plan, you
don’t have to go through a specialist
referral process
Yes Yes Yes Yes Yes Yes Yes
www.calchoiceplus.com
Physician Access & Referral—PPO
All CaliforniaChoice 51+ Health Plans cover life threatening emergencies anywhere in the world .
14

Q U E S T I O N SHealth Net HMO,
Elect Open Access and Salud HMO y Más
Kaiser PermanenteHMO and HDHP
Western Health AdvantageHMO and HSA
Can a member self-refer to an OB/GYN?
Yes—OB/GYN must be in same medical group* or IPA*
as your PCPAnytime Yes—anytime to an OB/GYN
in the WHA network
How often does health carrier allow a routine PAP smear?
Annually(or as deemed necessary
by physician)
Annually (or as deemed necessary
by plan physician)Annually**
How often does health carrier allow a routine Mammogram?
Annually**As recommended
by Health PlanPhysician
Ages 35 - 39: One during five year period
Ages 40 & over: One every calendar year
Does the carrier cover oral contraceptives?
Plans will cover most female prescription contraceptives at $0
cost share . Coverage on some drugs may not follow the generic and brand
tier system . Please refer to your plan documents1 and Health Net’s
[Recommended Drug List (RDL)], cost share and tier information .
Yes Yes
Well Woman & Infertility Benefits—HMO
* A Medical Group or PMG consists of a group of physicians who are in partnership . The Medical Group makes referrals to specialists and handles its own administration .
** O r as recommended by the U .S . Preventive Services Task Force or the American College of Obstetricians and Gynecologists .
1 Evidence of Coverage (EOC) or Certificate of Insurance (COI) are legal binding documents . If the information in this brochure differs from the information in the EOC or COI, the EOC or COI applies .
An IPA is an Individual Practice Association, made up of a group of physicians who practice in their own separate offices but are part of a central administrator that oversees referrals and other HMO issues . Ask your PCP for the name of the IPA or medical group to which he or she belongs .
15

Health Net PPO & Indemnity
CalChoice® 51+
PPO 250CalChoice 51+
PPO 500CalChoice 51+
PPO 1000CalChoice 51+
PPO 1500CalChoice 51+
HSA 1500CalChoice 51+
HSA 2000Flex Net
(out-of-state only)
In a PPO, you can choose any OB/GYN
anytime
In a PPO, you can choose any OB/GYN
anytime
In a PPO, you can choose any OB/GYN
anytime
In a PPO, you can choose any OB/GYN
anytime
In a PPO, you can choose any OB/GYN
anytime
In a PPO, you can choose any OB/GYN
anytime
In an Indemnity Plan, you can choose any
OB/GYN anytime
Once a year* Once a year* Once a year* Once a year* Once a year* Once a year* Once a year*
Once a year* Once a year* Once a year* Once a year* Once a year* Once a year* Once a year*
Yes Yes Yes Yes Yes Yes Yes
Infertility Treatment: After you are approved for coverage, you can call your health carrier directly to determine what infertility procedures are covered . All cases are reviewed on a case-by-case basis .
* O r as recommended by the U .S . Preventive Services Task Force or the American College of Obstetricians and Gynecologists .
Well Woman & Infertility Benefits—PPO
16
www.calchoiceplus.com

Q U E S T I O N SHealth Net HMO,
Elect Open Access and Salud HMO y MásKaiser Permanente
HMO
If generic drug is available and doctor has not indicated “dispense as written,” will member receive a generic equivalent rather than the brand name drug?
Yes—or you must pay the brand copay plus the difference
in cost between the brand name & generic equivalent
Yes
If doctor writes “dispense as written” on prescription, is brand name available at the brand copay?
Yes Yes
If doctor writes a prescription and there is no generic available, will member receive brand name drug at generic copay?
No—brand name dispensed at
brand name copay
No—brand name dispensed at brand
name copay
What are my prescription copays for formulary drugs?
Are Non-Formulary drugs covered?$50 Non-Formulary
copay applies
Prior authorization may be required
If deemed medically necessary by Plan Physician
Mail Order
Prescription Drug Benefits—HMO
CalChoice® 51+ HMO 15*:CalChoice 51+ HMO 15 Value:CalChoice 51+ HMO 20/$500 Value: CalChoice 51+ HMO 25*:CalChoice 51+ HMO 25 Value:CalChoice 51+ HMO 40*:CalChoice 51+ HMO 40 Value:Elect Open Access:Salud HMO y Más:
* The copay shall be the designated amount, or 50% of the provider’s contract rate, whichever is less
$10$15
$15$20$20$20$15 $15
Generic $20$30
$25$40$35$40$25$25
Brand
The Brand Rx deductible will apply
90 Day Supply:
All plans: self-injectables are covered in full
* The copay shall be the designated amount, or 50% of the provider’s contract rate, whichever is less
Generic $20$30
$30$40$40$40$30$30
Brand$40$60
$50$80$70$80$50$50
$100$100
$100$100$100$100$100$100
Non-Formulary
17
CalChoice 51+ HMO 15*:CalChoice 51+ HMO 15 Value:CalChoice 51+ HMO 20/$500 Value: CalChoice 51+ HMO 25*:CalChoice 51+ HMO 25 Value:CalChoice 51+ HMO 40*:CalChoice 51+ HMO 40 Value:Elect Open Access:Salud HMO y Más:
No mail order benefit for Non-Formulary
$10
$10$10
$15
Generic $20
$30$25
$30
Brand
Up to a 30 day supply
The Brand Rx deductible will apply
Generic 90 Day Supply:
$20
$10$20
$30
Brand$40
$30$50
$60

Kaiser Permanente HDHP
Western Health Advantage HMO
Western Health Advantage HSA
Yes
Yes—or you must pay the brand copay plus the difference
in cost between the brand name & generic equivalent
Yes—or you must pay the brand copay plus the difference
in cost between the brand name & generic equivalent
Yes Yes Yes
No—brand name dispensed at
brand name copay
No—brand name dispensed at
brand name copay
No—brand name dispensed at brand
name copay
Covered at $0 copayafter plan deductible
has been met
Covered at $0 copayafter plan deductible
has been met
Yes–if deemed medically necessary by Plan Physician
HMO - $50 Non-Formulary copay applies
Covered at $0 copayafter plan deductible
has been met
Covered at $0 copayafter plan deductible
has been met
Covered at $0 copayafter plan deductible
has been met
Prescription Drug Benefits—HMO
18
$10
$15
$20
Generic $20
$25
$35
Brand
All plans: self-injectables are covered at 80%
Generic $25
$38
$50
Brand$50
$63
$88
$125
$125
$125
Non-Formulary

Q U E S T I O N S
Health Net PPO & Indemnity
CalChoice® 51+ PPO 250 CalChoice 51+ PPO 500 CalChoice 51+ PPO 1000
If generic drug is available and doctor has not indicated “dispense as written,” will member receive a generic equivalent rather than the brand name drug?
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
If doctor writes “dispense as written” on prescription, is brand name available at the brand copay?
Yes Yes Yes
If doctor writes a prescription and there is no generic available, will member receive brand name drug at generic copay?
No—brand name dispensed at brand
name copay
No—brand name dispensed at brand
name copay
No—brand name dispensed at brand
name copay
What are my prescription copays for formulary drugs?
Participating Pharmacy:Generic: $10Brand: $20
Non-Participating Pharmacy:Generic: $10 + 50%Brand: $20 + 50%
Participating Pharmacy:Generic: $10Brand: $20
Non-Participating Pharmacy:Generic: $10 + 50%Brand: $20 + 50%
$100 per individual brand deductible applies
Participating Pharmacy:Generic: $10Brand: $20
Non-Participating Pharmacy:Generic: $10 + 50%Brand: $20 + 50%
$150 per individual brand deductible applies
Are Non-Formulary drugs covered? Participating Pharmacy:$35
Non-Participating Pharmacy:$35 + 50%
Participating Pharmacy:$35
Non-Participating Pharmacy:$35 + 50%
$100 per individual brand deductible applies
Participating Pharmacy:$35
Non-Participating Pharmacy:$35 + 50%
$150 per individual brand deductible applies
Mail Order 90 Day Supply: Generic: $20Brand: $40Non-Formulary: $70
90 Day Supply: Generic: $20Brand: $40Non-Formulary: $70
$100 per individual brand deductible applies
90 Day Supply: Generic: $20Brand: $40Non-Formulary: $70
$150 per individual brand deductible applies
* Prescription Drugs are subject to the medical deductible . The submission of a prescription drug claim is required for reimbursement of all outpatient prescription drugs .
Prescription Drug Benefits—PPO
19

Health Net PPO & Indemnity
CalChoice® 51+ PPO 1500 CalChoice 51+ HSA 1500 CalChoice 51+ HSA 2000 Flex Net (out-of-state only)
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
Yes—or you must pay the brand copay plus the difference between the cost of the brand
name & generic
Yes Yes Yes The copay is the same as it is for generic medications
No—brand name dispensed at brand
name copay
No—brand name dispensed at
brand name copay
No—brand name dispensed at brand
name copay
The copay is the same as it is for generic medications
Participating Pharmacy:Generic: $10Brand: $20
Non-Participating Pharmacy:Generic: $10 + 50%Brand: $20 + 50%
$150 per individual brand deductible applies
Participating Pharmacy:Generic: $10 after plan deductibleBrand: $25 after plan deductible
Non-Participating Pharmacy:Generic: $10 + 50% after plan deductibleBrand: $25 + 50% after plan deductible
Participating Pharmacy: Generic: $15 after plan deductibleBrand: $30 after plan deductible
Non-Participating Pharmacy:Generic: $15 + 50% after plan deductibleBrand: $30 + 50% after plan deductible
20% for all medications after Rx deductible
Participating Pharmacy:$35
Non-Participating Pharmacy:$35 + 50%
$150 per individual brand deductible applies
Participating Pharmacy:$50 after plan deductible
Non-Participating Pharmacy:$50 + 50% after plan deductible
Participating Pharmacy:$50 after plan deductible
Non-Participating Pharmacy:$50 + 50% after plan deductible
Yes—non formulary medications are covered, however the
member must first try the generic drug
90 Day Supply: Generic: $20Brand: $40Non-Formulary: $70
$150 per individual brand deductible applies
90 Day Supply: Generic: $20Brand: $50Non-Formulary: $100
All prescription drug benefits are subject to combined
medical and prescription drug deductible of $1500 per individual
90 Day Supply: Generic: $30Brand: $60Non-Formulary: $100
All prescription drug benefits are subject to combined
medical and prescription drug deductible of $2000 per individual
90 Day Supply with a 20%
coinsurance for each month
* Prescription Drugs are subject to the medical deductible . The submission of a prescription drug claim is required for reimbursement of all outpatient prescription drugs .
Prescription Drug Benefits—PPO
20

Q U E S T I O N SHealth Net HMO,
Elect Open Access and Salud HMO y Más
Kaiser Permanente
HMO
Kaiser Permanente
HDHP
Western Health Advantage
HMO Western Health Advantage HSA
InsulinCovered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Needles/SyringesCovered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Glucose Monitor
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
CalChoice® 51+ HMO 15—90% CalChoice 51+ HMO 15 Value—85%
CalChoice 51+ HMO 25—80%CalChoice 51+ HMO 25 Value—80%
CalChoice 51+ HMO 40—80%CalChoice 51+ HMO 40 Value—80%
Elect Open Access—80%Salud HMO y Más—80%
Covered as Durable Medical Equipment,
rather than Prescription Drug Benefit:
CalChoice 51+ HMO 15—100%
CalChoice 51+ HMO 20/$500 Value—80%
CalChoice 51+ HMO 25—80%CalChoice 51+ HMO 40—50%
Covered as Durable Medical Equipment,
rather than Prescription Drug Benefit:
Covered at$0 copay, after
Plan deductible hasbeen met
Covered as Durable Medical Equipment,
rather than Prescription Drug Benefit:
CalChoice 51+ HMO 15—90% CalChoice 51+ HMO 25—70%CalChoice 51+ HMO 40—50%
Up to max $2,500/year
Covered as Durable Medical Equipment,
rather than Prescription Drug Benefit:
$0 copay, afterPlan deductible has
been met
Chem-Strips and/or Testing Agents
Covered under the Prescription
Drug Benefit
Blood Test Strips are covered as Durable Medical Equipment .
Urine Test Strips are covered under the Prescription Drug
Benefit
Blood Test Strips are covered as Durable Medical Equipment .
Urine Test Strips are covered under the Prescription Drug
Benefit
Covered under the Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Insulin Pump
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Insulin Pump Supplies
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Covered as Durable Medical Equipment rather than Prescription
Drug Benefit
Diabetes Benefits—HMO
21

Health Net PPO & Indemnity
CalChoice® 51+
PPO 250CalChoice 51+
PPO 500CalChoice 51+
PPO 1000CalChoice 51+
PPO 1500CalChoice 51+
HSA 1500CalChoice 51+
HSA 2000Flex Net
(out-of-state only)
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered under thePrescription Drug
Benefit
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
In-Network: 90%
Out-of-Network: 70%
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
In-Network: 80%
Out-of-Network: 60%
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
In-Network: 80%
Out-of-Network: 60%
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
In-Network: 80%
Out-of-Network: 60%
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
In-Network: 80%
Out-of-Network: 60%
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
In-Network: 80%
Out-of-Network: 50%
Covered as Medical Supplies,
rather than Prescription Drug Benefit:
80%
Covered under the Prescription Drug
Benefit
Covered under the Prescription Drug
Benefit
Covered under the Prescription Drug
Benefit
Covered under the Prescription Drug
Benefit
Covered under the Prescription Drug
Benefit
Covered under the Prescription Drug
Benefit
Covered under the Prescription Drug
Benefit
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 90%
Out-of-Network: 70%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 50%
Covered as Durable Medical Equipment(Medical Deductible
applies): 80%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 90%
Out-of-Network: 70%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 60%
Covered as Durable Medical Equipment(Medical Deductible
applies)
In-Network: 80%
Out-of-Network: 50%
Covered as Durable Medical Equipment(Medical Deductible
applies): 80%
Diabetes Benefits—PPO
22

Health Net 800.361.3366
English/Español, Mon-Fri 8:00 a.m. - 6:00 p.m.
Kaiser Permanente English 800.464.4000
Español 800.788.0616
7 days a week 7:00 a.m. - 7:00 p.m.
Western Health Advantage 888.563.2250
English/Español, Mon-Fri 8:00 a.m. - 5:00 p.m.
PL5008.12.12
866.451.7587www.calchoiceplus.com





























