Embed Size (px)
Citation preview

HEALTH EFFECTS AND ACADEMIC PERFORMANCE OF PRIMARY
SCHOOL CHILDREN EXPOSED TO TOBACCO SMOKE AT HOME IN
MOROGORO MUNICIPAL
By
MASOTA P. JOHN
A Dissertation Submitted in Partial Fulfillment of the Requirements for the Degree
of Master of Science in Health Systems Management (MHSM) of Mzumbe
University.
2016

i
CERTIFICATION
We, the undersigned, certify that we have read and hereby recommend for acceptance by
the Mzumbe University, a Dissertation entitled “Health effects and academic
performance of primary school children exposed to tobacco smoke’’ in partial/
fulfilment of the requirements for award of the degree of Master of Health System
Management of Mzumbe University.
Major Supervisor
…………………………………
Internal Examiner
…………………………………
External Examiner
………………………………..
Accepted for the Board of School of Public Administration and Management
……………………………………………..…
DEAN/SCHOOL BOARD

ii
DECLARATION
AND
COPYRIGHT
I, MASOTA P. JOHN declare that this dissertation is my own original work and that it
has not been presented and will not be presented to any other university for similar or
other degree award.
Signature ___________________
Date_______________________
©
COPY RIGHT
This dissertation is a copyright material protected under the Berne convention, the
copyright Act 1999 and other international and national enactments, in that behalf, on
intellectual property. It may not be reproduced by any means in full or in part, except for
short extracts in fair dealings, for research or private study, critical scholarly review or
discourse with an acknowledgement without the written permission of Mzumbe
University, on behalf of the author.
iii
ACKNOWLEDGEMENT
First and foremost, I would like to thank our almighty GOD for giving me strength and
keeping me healthy throughout the period of conducting my research.
I would like to thank my lovely parents Mr&Mrs Charles Masota for material and moral
support during the entire time of my study. My sincere appreciation goes to my
supervisor Dr Bunini Manyilizu (PhD Epidem-Toxicologist) despite of his busy
schedule he took time to review my work, provide seminars, advise and direct me how
to conduct this research, also I would like to thank all pupils and teachers who involved
and participated in this study, just a few to mention head mistress Agnes. T. William,
academic teacher Nusura. E. Kiobya and Majabu. M. Lugendo for allowing me to
conduct this study in their school. Great thanks should go to my fiancée Miriam Mafuru
for her support and encouragement during all time of doing this research; I would also
give thanks to my brother Mussa and Sister Maria. Finally I thank my best friend
Mihayo Alfred for assisting me in data collection.

iv
DEDICATION
This research report is dedicated to my family for their love, care, support and prayers.

v
ABSTRACT
Involuntary tobacco smoking exposure at home had been reported to be associated with
health effects and decreasing children academic performance in school, but no similar
study conducted in Tanzania.
This study aimed at determining human health effects and academic performance of
primary school children exposed to tobacco smoking at home. The study Used case
control study, a total of 120 respondents were recruited in this study, where exposed
group were 60 and other 60 were compared group, all respondents came from class five,
six and seven at Kikundi primary school in Morogoro.
In order to determine the association of exposure the outcome variables for health effects
were asthma, wheezing, breathing, antisocial behavior, attention deficit disorders, ears
problem, nose (sense of smell), throat problems and respiratory disease like nasal
passages. Pupil’s class participation, class position, average score, and general academic
performance were considered as outcome variables for academic performance, whereas
smoking tobacco at home by Parents/guardians or any family members were considered
as risk factors.
Questionnaires were used to acquire information. The study determined strong
association between involuntary tobacco smoking at home, health effects and pupils
poor/decrease in academic performance at school. Heart diseases 2.5%, anti-social
5.8%, nose fail sense 7.5%, asthma 11.7%, respiratory problem 14.2%, ear diseases
16.7%, wheezing 23.3%, deficit disorders 23.3% and throat diseases 33.3. The Pearson
Chi- Square and fisher’s exact test shows 0.000, 0.017, 0.000, 0.036 and 0.014. The
study found the strong association for wheezing, anti-social, throat diseases, nose
sensing problem and ear problem respectively. For academic general performance 0.038,
average first term (0.015, 0.043 & 0.050) and end term report (0.000-0.003). Therefore
there is no self point/position of exposing children on involuntary tobacco smoking,
even a single cigarette is harmful to children’s health and academic performance.
vi
TABLE OF CONTENTS
CERTIFICATION .............................................................................................................. i
DECLARATION .............................................................................................................. ii
COPY RIGHT ................................................................................................................... ii
ACKNOWLEDGEMENT ............................................................................................... iii
DEDICATION .................................................................................................................. iv
ABSTRACT ....................................................................................................................... v
LIST OF ABBREVIATIONS ......................................................................................... xii
CHAPTER ONE .............................................................................................................. 1
INTRODUCTION ............................................................................................................ 1
1.0 Background .................................................................................................................. 1
1.1 Statement of the problem ............................................................................................. 3
1.2 Objective ...................................................................................................................... 4
1.3 Specific objectives ....................................................................................................... 4
1.4 Study hypothesis .......................................................................................................... 4
1.5Rationale of the study.................................................................................................... 4
CHAPTER TWO ............................................................................................................. 5
LITERATURE REVIEW ................................................................................................ 5
2.0 Theoretical review ........................................................................................................ 5
2.1 Empirical literature ....................................................................................................... 5
2.2 Involuntary tobacco exposure and children health effects ........................................... 7
2.2.0 Adverse effect on immune system ............................................................................ 7
2.2.1 Antisocial behaviors .................................................................................................. 7
2.2.2 Breathing problems (wheezing) ................................................................................ 8
2.2.3 Nose problem ............................................................................................................ 8
2.2.4 Nose sensing and throat diseases .............................................................................. 8
2.2.5 Middle ear disease ..................................................................................................... 9
2.2.6 Hearing problem (Otitis media) ................................................................................ 9

vii
2.2.7 Pneumonia ................................................................................................................. 9
2.2.8 Lower respiratory ...................................................................................................... 9
2.3 Others health effects to children exposed on tobacco cigarette smoke ...................... 10
2.3.0 Respiratory morbidity ............................................................................................. 10
2.3.1 Asthma…………………………………………………………………………….10
2.3.2 Low birth weight ..................................................................................................... 10
2.3.3 Harm of lung capacity ............................................................................................. 11
2.3.4 Cardiovascular Disease ........................................................................................... 11
2.3.5 Sudden death ........................................................................................................... 11
2.3.6 Lung cancer and brain tumors ................................................................................. 11
2.4 Involuntary smoking in related to academic performance ......................................... 12
2.4.0 Involuntary smoking and its relation to Pupil’s participation and school
attendance……. ................................................................................................................ 12
2.4.1 Learning ability ....................................................................................................... 12
2.6 Background variables ................................................................................................. 14
2.7 Life style variables ..................................................................................................... 15
2.8 Factors for good academic performance to children .................................................. 16
2.9 Health effects to children exposed to tobacco smoke ................................................ 16
2.10 ..... Exposing children to tobacco smoke in relation to class academic performance at
school ……………………………………………………………………………….......16
CHAPTER THREE ....................................................................................................... 17
METHODOLOGY ......................................................................................................... 17
3.0 Introduction ................................................................................................................ 17
3.1 Study area ................................................................................................................... 17
3.2 Study population ........................................................................................................ 17
3.3 Target population ....................................................................................................... 17
3.4 Study design ............................................................................................................... 18
3.5 Tools and techniques for data collection .................................................................... 19
3.5.1 Methods for data collection ..................................................................................... 19
3.6 Sample size, sampling and procedures ....................................................................... 20
3.6.1Sample size............................................................................................................... 20
viii
3.6.2 Sampling ................................................................................................................. 20
3.6.3 Sampling procedures ............................................................................................... 21
3.7 Pre-testing tools for data collection............................................................................ 21
3.8 Data management ....................................................................................................... 21
3.8.1 Data collection and quality control ......................................................................... 21
3.8.2 Data entry and cleaning techniques......................................................................... 21
3.8.3 Data variables and analysis ..................................................................................... 22
3.9 Ethical considerations ................................................................................................ 22
CHAPTER FOUR .......................................................................................................... 23
PRESENTATION OF THE FINDINGS ...................................................................... 23
4.0 Introduction ................................................................................................................ 23
4.1 Characteristics of respondents.................................................................................... 23
4.1 .0Respondents distribution by gender and class ........................................................ 23
4.1.1 Respondents distribution by age ............................................................................. 23
4.1.2 Number of smokers at home ................................................................................... 24
4.1.3 Respondents distribution by parent/guardian education ......................................... 24
4.1.4 Respondent’s parent/guardian distribution by job .................................................. 24
4.2 Association between causes variable and outcome in health ..................................... 27
4.2.0 Smoking on child presence and wheezing outcome ............................................... 28
4.2.1 Tobacco smoking in relation to ant-social behavior ............................................... 28
4.2.2 Association between parent/guardians smoking and throat diseases ...................... 29
4.2.3 Number of cigarette smoked on presence of children per day in association to nose
problems……….. ............................................................................................................. 29
4.2.4 Exposing children to involuntary tobacco smoke at home in association to ear
problem……….. ..................................................................................................... ………30
4.2.5 Smoking tobacco in association to nose problem among children ......................... 30
4.2.6 Children exposure to involuntary smoking in association with ear problems ........ 30
4.3 Environmental and life style variables ....................................................................... 30
4.3.0 Poor ventilated house in association with respiratory diseases ............................... 31
4.3.1 Association between number of sleeping room and wheezing ............................... 31
4.3.2 Population at home, plastic bag burning in association with nose problems .......... 31
4.3.3 Use of plastic material, burning plastic and type of fuel use associated to attention
deficit disorders, asthma and throat problem ................................................................... 32

ix
4.4 Requirements for academic performance in primary school ..................................... 33
4.4.0 Relationship between pupils term average and general performance to adequate
teachers and availability of text books in class ................................................................ 33
4.4.1 Association between private study, pupil participation and average ...................... 34
4.4.2 Parents/community support and pupils home work factor associated to class
participation and general performance ............................................................................. 35
4.5 Number of smoker(s) at home and general academic performance for children ....... 36
4.5.0 Association between class and average performance of children ........................... 36
4.5.1 Smoker(s) in family and smoking on children presence in association with pupils
academic performance ..................................................................................................... 37
CHAPTER FIVE ............................................................................................................ 46
DISCUSSION OF RESEARCH RESULTS ................................................................ 46
5.0 Introduction ................................................................................................................ 46
5.1 Primary children exposure to involuntary tobacco smoking at home and health
effects…………………………………………………………………………………………………………………………46
5.2 Exposing children to tobacco smoke and academic performance at school .............. 48
CHAPTER SIX .............................................................................................................. 51
CONCLUSION, ADVICES AND RECOMMENDATION ....................................... 51
6.0 Introduction ................................................................................................................ 51
6.1 Conclusion .................................................................................................................. 51
6.2 Advices ....................................................................................................................... 52
6.3 Recommendation ........................................................................................................ 52
REFERENCES ................................................................................................................. 53
APPENDICES ................................................................................................................. 61

x
LIST OF FIGURES
Figure 1 Pictures show among of effect associated by tobacco smoke…………….….13
Figure 2 Conceptual frame work………………………………………………………14

xi
LIST OF TABLES
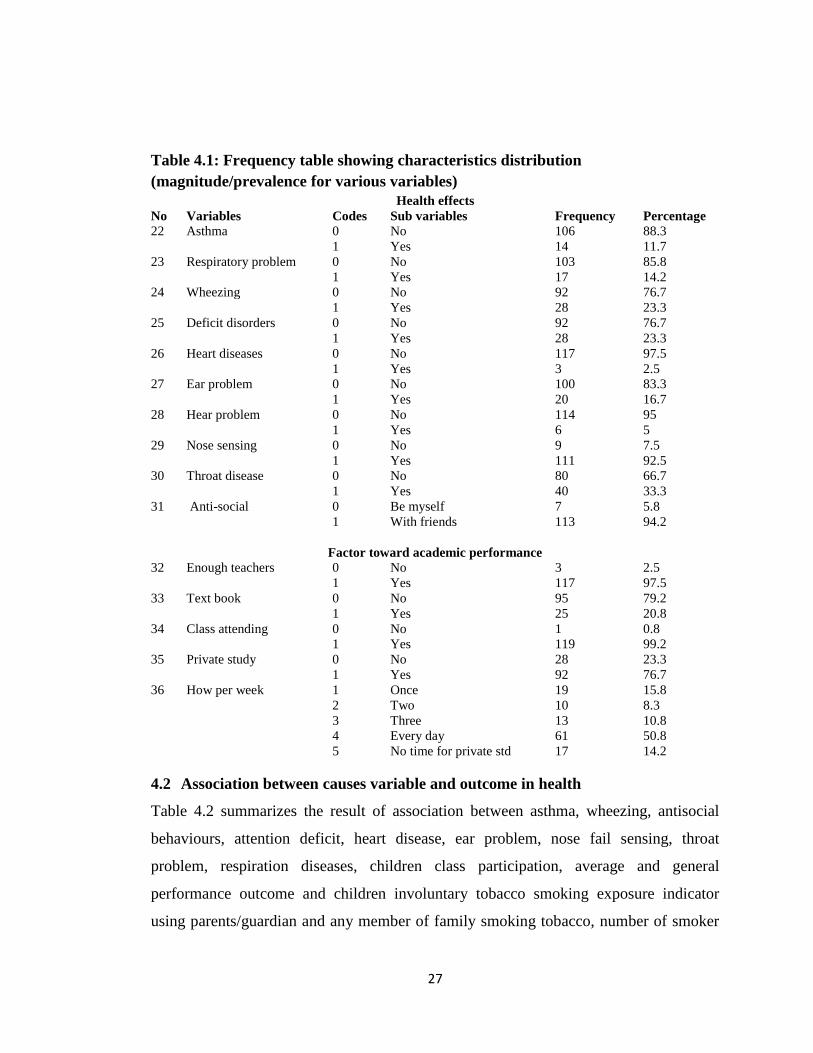
Table 4.1: Frequency table showing characteristic distribution (magnitude/prevalence for
various variables)...………………………………………………………………….…..27
Table 4.2: Cross tabulation and crude analysis of exposure variables …..……………..37

xii
LIST OF ABBREVIATIONS
AIDS……………………….Acquired immune deficiency
CHI………………………...The Pearson chi- square
DHHS………………………Department of Health and Human Services, 2010)
DR…………………….…....Doctor
ETS…………………………Exposure tobacco smoke
HIV…………………….…. Human immunodeficiency virus
MS…………………………Microsoft
PV……………………….…Probability value
SHS…………………………Second hand smoking
SPSSS……………………...Statistical package for social science
SSA………………………...Sub Saharan Africa
SOPAM…………………....School of Public Administration and management
TDHS………………….……Tanzania demographical health
UK……………………….…United Kingdom
US……………………….…United State
WHO…………………….…World health organization

1
CHAPTER ONE
INTRODUCTION
1.0 Background
Involuntary tobacco smoking (involuntary exposure to tobacco or secondhand smoking)
refers to smoke from burning tobacco products, generated by people who are smoking
(WHO, 2007). The tobacco industry named involuntary tobacco smoking as
environmental tobacco smoke. Tobacco smoke pollutes the air particularly in enclosed
spaces, both smokers and non smokers are exposed to harmful health effects (WHO,
2010). U.S. Surgeon General (2010) reported that cigarette smoke have more than 7,000
chemicals, hundreds are poisonous (toxic) and at least sixty nine of the chemicals cause
cancer.
Immediate effects of exposure to involuntary smoking include eye irritation, headache,
cough, sore throat, dizziness and nausea (ASH, 2014). Adults with asthma can
experience a significant decline in lung function when exposed to tobacco; while new
cases of asthma may be induced in children whose parent were smokers, tobacco smoke
also has a measurable effect on the heart of non-smokers. (World Health Organisation,
2010)
Globally it was estimated that more than 40 % of children were exposed to tobacco
smoke, while in adult are below 40%, (Oberg et al 2011). Children seem to be affected
with tobacco smoke exposure because most of the times are with their parents/
guardians. Also they use a lot of time at home and it is very difficult to them to express
what they feel about tobacco smoke to their parents even if they smoke in children
presence.
It is reported that exposure to involuntary smoking was estimated to cause 379 000,165
000, 369000, and 21400 deaths from ischemic heart diseases, lower respiratory

2
infections, asthma, and lung cancer respectively…. It is also estimated that tobacco
smoke use, is currently responsible for almost six million deaths each year where one
death occurs in every six seconds (WHO, 2007).
Several interventions to prevent public smoking like non smoking campaign have been
in place for more than a decade worldwide. For example, WHO have introduced a policy
and regulation to stop involuntary smoking in public places, it enforces that public
smoke should be avoided so as to protect the health of all staff, patients, customer and
visitors (WHO, 2013).
In Africa involuntary smoking is still a problem, it has been associated with adverse
effects on health, including premature birth, problem on health of the children during
period of growth, prenatal mortality, respiratory illness, antisocial behavior and
decreased academic performance in school. Involuntary smoking to children in Africa
reported to be 34.3% (Sang, 2012).
More efforts implemented to reduce secondhand smoking (SHS) in Africa are such as
education strategies, recognizing that smoking in open areas like some of workplace,
home and station increases the likelihood that people (both smokers and non-smokers)
will rise involuntarily in second hand smoking, WHO support member states to follow
these recommendations and apply lessons to all people on the side effect of the tobacco
smoke. WHO (2007)
In Tanzania tobacco is among of the cash crops, it contributes 13.2% of cash crops
earning for the ministry of Agriculture and cooperatives, it is cultivated in Morogoro,
Songea and Tabora also it is the core source of the earnings for the families that cultivate
tobacco (Mbatia, 1998).
In spite of the financial income to the country, it has effects to the environment as it uses
wood in process of tobacco. The outcome of these can be deforestation, soil corrosion
and land degradation.
3
Prevalence of tobacco smoking in Tanzania is 24% .The research done in Tanzania (Dar
es salaam) about human health effect caused by involuntary smoking and the outcome
explained that a good estimated of passive tobacco smoking occurred in children is still
a problem (Jagoe, 2002).
According to Tanzania demographic health survey it is shown that the prevalence of
tobacco smoking in Morogoro is 18.5% (TDHS, 2010).
Tanzanian Government came up with different ways to reduce the problems of tobacco
smoke, some of them were to increase the cigarette price through adding more tax, and
to implement WHO policy which requires people stop smoking in public, public offices
and in any health service centre. Due to high prevalence of tobacco smoking in
Tanzania, this research will focus on examining health effects and academic
performance of children exposed to tobacco smoke and to come up with new means to
solve the problem.
1.1 Statement of the problem
It is reported that globally 600,000 deaths take place every year due to involuntary
tobacco smoke, 33% of the deaths are children often exposed to tobacco smoke at home.
Passive smoking is dangerous for children health as it results to heart diseases,
respiratory, infant death syndrome, pneumonia, asthma, attention deficit disorders,
stroke, antisocial behavior and wheezing (WHO, 2012).
Sub-Saharan countries particularly Tanzania, Prevalence of tobacco smoking is high
compared to other regions of the world. Tanzania has reached the early stages of the
tobacco cigarette smoking epidemic. However, data from demographic health surveys
WHO (2012) shows different smoking prevalence rates: Nigeria, Ethiopia, and Ghana
are below 10%, smoking prevalence rates for Mozambique, Lesotho, Zambia, Namibia,
Uganda and Rwanda are below 20%, Zimbabwe and Kenya (22.9%) but prevalence rate
in Tanzania is 24% (Matheka, 2012).
4
Involuntary tobacco smoke has effects in health and poor academic performance to
children at school. As it is presented in the statistic above, Tanzania remains to be one of
the countries with high prevalence rate than other countries in sub Saharan regions.
Thus, this study has found out health effects and academic performance of primary
school children exposed to tobacco smoke at Kikundi primary school in Morogoro
Municipal.
1.2 Objective
The general objectives had to find out health effects and academic performance of
primary school children exposed to tobacco smoke at Kikundi primary school in
Morogoro Municipal.
1.3 Specific objectives
i. To determine health effects of primary school children exposed on to tobacco
smoke at home.
ii. To determine effects on academic performance for primary school children
exposed to tobacco smoke at home.
1.4 Study hypothesis
Involuntary exposure to tobacco smoke increases the risk of poor academic performance
and occurrence of adverse on health effects among primary school children.
1.5 Rationale of the study
Health effects and poor academic performance to primary school children resulting to
involuntary tobacco smoking exposure can be preventable. This study focused on
finding out health effects and academic performance to school children exposed to
tobacco smoke at home. Findings from this study are recognized to be preventive
measures for children health exposed to secondhand smoking and improvement on
academic performance.
There are no studies published in developing countries, about health effects and
academic performance of primary school children exposed to tobacco smoke.

5
CHAPTER TWO
LITERATURE REVIEW
2.0 Theoretical review
WHO (2007) defines Involuntary smoking as second hand tobacco smoke or passive
smoking. Tobacco industry named the involuntary tobacco smoking as environmental
tobacco smoke. When tobacco smoke pollutes the air particularly in enclosed spaces,
both smokers and non smokers are exposed to harmful health effects (WHO, 2010).
Involuntary smoking takes place when tobacco cigarette smoke extends in the air and
inhaled by people who are around the environment. Globally the involuntary smoking is
found to be dangerous to human health compared to the direct smoking, because one
smoker can affect more than one people for the same time (Apelberg, 2007).
Involuntary tobacco smoking affects the health of people by air movement especially
children who closely to parents/guardians and spending most of their time at home, the
effects to children health is higher compared to adults. (Riboli, 1990 and Pirkle, 1996).
The side flow of tobacco smoke contains higher levels of cancer compounds, such as
nicotine, carbon monoxide and formaldehyde than mainstream smoke. Involuntary
smoking is a common indoor pollutant at home, making passive smoking a mostly
health risk for both direct and indirect tobacco smokers. Children are mostly at danger of
serious health effects from involuntary smoking (Chen, 1986).
2.1 Empirical literature
Involuntary smoking happens when tobacco cigarette smoke spreads in atmosphere and
inhaled by people who are around. Globally it is reported that secondhand smoking is as
harmful to health as the real smoking itself, scientists have proved that there is no
secure point of exposure to involuntary smoking since smoke from involuntary smoke
cause serious disease in human body to both adults and children (WHO, 2007).

6
U.S. DHHS, (2010) argued that involuntary smoke have numerous chemicals about
seven thousand toxics, most of these chemicals cause cancer, furthermore the chemicals
lead to failure of blood vessels, and in long run it causes heart attack and stroke. WHO
(2011) further reported that 7000 chemicals found in involuntary smoke are such as
acetic acid, ammonia, arsenic found in poison, butane found in lighters, cadmium in
batteries, carbon monoxide created gas, hexamine, methane found in sewer gas,
methanol created in rocket fuel, nicotine found in insecticide, paint, acid found in candle
wax, toluene found in industrial solvent, to mention just a few.
The General’s report (2010) stipulated that some groups of people use different ways to
protect children from exposure to tobacco smoke, like opening the door and windows
and others smoke outside the rooms, still this is not a safe way, since the tobacco smokes
move viscously to non smokers. Effects originated from involuntary smoke do not
depend on the time a person is exposed on tobacco smoke. You don’t need to be a heavy
smoker or exposed for long time in order to get smoking related disease like heart attack
or asthma... low level of smoke exposure has effects to human health, including quick
redness of the coating of the blood vessels, which are related to heart attacks and stroke
(Acevedo-Estefania, 2000).
Oberg, (2011) reported that in 2003 predictable 617 people in UK died from the effects
of involuntary smoking at work, of which fifty four were extended term employees of
the hospitality industry, other 11,000 deaths were caused by involuntary smoking
exposure at home. Tobacco cigarette is also reported to increase the rate of HIV in the
world (Ezzati, 2003). Approximately 40–70% of HIV-infected people are associated
with substantial morbidity among HIV-positive patients (Crothers, 2005). Tobacco
smoke and HIV infection are independent risk factors for many of the same illnesses.
The rate of involuntary smoking exposure among children in their homes have been
reported to vary in the world where, 34.3% in Southeast Asia, 50.6% in Western Pacific,
and 77.8% in Europe (Warren, 2008). Sub Saharan Africa unlike other regions of the
world has early stage of the cigarette smoking epidemic. additionally SSA shows

7
variation of Europe and America in result of involuntary smoking, East Africa is at a
standstill compared to Europe and America, however Tanzania has high rate (24%) of
smoking effects than other countries in East Africa (Surgeon General’s report, 2010).
Jagoe, 2002 suggested that deaths from smoking occurs more to children, women and
men. The health effects of involuntary smoking to children affects their academic
performance at school, it has also been associated with adverse effects on health,
including premature birth to woman, growth retardation, prenatal mortality, respiratory
illness, neurobehavioral problems, and decreased performance in school (Hwang,
2012).
2.2 Involuntary tobacco exposure and children health effects
Children are likely to be more affected by second hand smoking in family. The
following are some of health effects to children exposed to tobacco smoking at home;
asthma, wheezing breathing, antisocial behavior, attention deficit disorders, heart
diseases, ears, nose (sense of smell), throat problem, respiratory disease like nasal
passages the bronchi and cardiovascular diseases.
2.2.0 Adverse effect on immune system
The mixture of chemicals in tobacco smoke such as nicotine, hydrocarbons, carbon
monoxide, volatile organic compounds, and reactive nitrogen moieties are thought to be
the primary components of tobacco smoke that modify the immune response. The effects
of these chemicals after inhalation lead to local respiratory effects and affect nearly
every cell in the immune system (Ciaccio, 2013).
2.2.1 Antisocial behaviors
Researchers from Harvard School of Public Heath in 2007 conducted a research and
analyzed the responses of parents or guardians of more than 55,000 children, they found
that children who were exposed to secondhand smoke are twice more likely to develop
antisocial behaviors or neurobehavioral disorders including learning disabilities, and
behavior disorders than children who lived in smoke-free homes (Zubair, 2011).

8
2.2.2 Breathing problems (wheezing)
Exposure to secondhand smoking decreases lung efficiency and impairs lung function in
children of all ages; it increases both the frequency and harshness of childhood asthma
(Lynch, 2014). Secondhand smoke can make worse sinusitis, rhinitis, cystic fibrosis, and
chronic respiratory problems such as cough and postnasal drip, it also increases the
number of children’s colds and sore throats. Studies have shown that older children
whose parents smoke get sick more often, particularly bronchitis and pneumonia
(Grazuleviciene et al, 2014).Wheezing and coughing are also more common in children
who breath secondhand smoke than children who do not breath secondhand smoke
(Action on smoking and health, 2014).
2.2.3 Nose problem
Involuntary smoking results to rhinitis; rhinitis is an inflammatory of the mucous inner
lining of the nasal passages and results in symptoms of sneezing, congestion, runny
nose, itchy eyes, ears and nose. Secondhand smoking causes rhinitis by damaging the
same clearing mechanism involved in sinusitis, also rhinitis can cause sleep
disturbances, activity limitations, irritability, moodiness, and decreased school
performance in children (Jurgita, 2014).
2.2.4 Nose sensing and throat diseases
Involuntary smoking leads to sinuses, Sinuses are spaces in the skull that are in direct
communication with the nose and mouth. They are important for warming and
moisturizing inhaled air. The lining of the sinuses consists of the same finger-like hairs
found in the lungs. These hair clear mucus and foreign substances and are therefore
critical in preventing mucus buildup and subsequent infection. Cigarette smoke slows or
stops the movement of these hairs, resulting in inflammation and infection (Benninger,
1999). Sinusitis can cause headaches, facial pain, tenderness and swelling, it can also
cause fever, cough, runny nose, sore throat, bad breath and decreased sense of smell,
children’s exposed to secondhand smoke are at risk to develop sinusitis compared to
children who are not exposed (Reh, 2012).

9
2.2.5 Middle ear disease
Recent studies had shown that children exposed to cigarette smoke are associated with
increased risk for middle ear disease; middle ear effusions are also associated with
tobacco involuntary smoke. Inhaled smoke irritates the eustachian tube, which connects
the back of the nose with the middle ear, this causes abnormal enlargement and
obstruction which interferes with pressure adjusting in the middle ear, leading to pain,
fluid and infection. Ear infections and middle ear fluid are the most common cause of
children’s hearing loss (Fabry, et al 2010).
2.2.6 Hearing problem (Otitis media)
The middle ear is the space immediately behind the eardrum it turns received vibrations
into sound and it is very vulnerable to infection. Children exposed to involuntary
tobacco smoking have more ear infections than unexposed ones (WHO, 2011). Tobacco
smoke interrupts the normal clearing mechanism of the ear canal, facilitating infectious
organism entry into the body. The resulting middle ear infection can be very painful, as
pressure and fluid buildup in the ear. Continued exposure to tobacco smoke may result
in constant middle ear infections and eventually, hearing loss to the children
(Alessandra, 2013).
2.2.7 Pneumonia
Pneumonia is an inflammation of the lining of the lungs; this inflammation causes fluid
to accumulate deep in the lungs, making it an ideal region for bacterial growth.
Pneumonia results in a persistent (constant) cough and difficulty in breathing. Smoking
increases the body’s weakness to the most common bacterial causes of pneumonia and is
therefore a risk factor for pneumonia, regardless of age (WHO, 2011)
2.2.8 Lower respiratory
Environmental tobacco smoke, a complex mixture of smoke and non inhaled, side
stream smoke, also contributes to respiratory morbidity to children. Tobacco combustion
produces multiple toxic compounds; exposure to toxic compounds in early children
development was particularly problematic because early lung development appears to be

10
a critical determinant of respiratory health. It has been found that infants whose mothers
smoked at least one packet per day had 2.8 times the risk of developing a lower
respiratory infection than non smokers (Batstra, 2003; Jones, 2011).
2.3 Others health effects to children exposed on tobacco cigarette smoke
Not only the above discussed diseases have been caused by SHS but also the following
are reported to be associated with involuntary tobacco smoking to children namely
asthma, cardiovascular diseases, sudden death especially to children, low birth weight,
damage of lung its capacity, lung cancer and brain tumors.
2.3.0 Respiratory morbidity
Tobacco smoke and its products affect the lungs and organs of respiration to children
and adolescents, passive exposure resulted from maternal smoking produced by parents,
care takers or any member of family leads to lung failures which end to death (WHO,
2011).
2.3.1 Asthma
When Tobacco smoke enters human body is destroys cilia, cilia is the small hair found
inside eukaryotic cell, it looks the same as hair keeping lungs clean by cleaning away
mucus and dust particles, at the end cilia fails to keep lung safe. When cilia become less
effective at keeping the lungs clean an involuntary smoker may get routine cough
because he/she has failed to remove mucus from lungs finally this leads to respiratory
disease and asthma (Jones, 2011).
2.3.2 Low birth weight
Over the past decade tobacco cigarette smoking during pregnancy had been associated
with adverse pregnancy outcomes, including increased incidences of low birth weight
(baby born with weight less than 2500 g) and prematurity. The mean duration of
gestation was not affected by maternal smoking; therefore, premature delivery (delivery
before 37 weeks of gestation) is not associated with smoking, however, smoking is
associated with a decrease in mean birth weight this increase the proportion of lower

11
birth weight young children (infants) at all gestational ages and infant mortality
(Catherine, 2011).
2.3.3 Harm of lung capacity
During childhood the lung completes its development as formation of the alveoli, the
lung function grows parallel to increase in height. Damage to the lung during childhood
may have lasting effects and compromise the lung’s keep back capacity (Yang, 2015).
2.3.4 Cardiovascular Disease
Cardiovascular disease is the risk disease that takes place to blood liner, tobacco smoke
can lead heart disease and stroke, exposure to tobacco smoke rapidly causes an effect on
blood chemistry and costs the weak cells to line blood vessel all over the body. These
important cells help to maintain proper blood flow. When they were damaged by
chemicals in tobacco smoke, they do not work properly. As a result, blood flow to and
from the heart can be impaired and lead to blood pressure increase (Surgeon General’s
report, 2010a).
2.3.5 Sudden death
Involuntary smoking formulates cover like plate in the blood, attaches the joints and
form clots. These joints like plates are probable broken arteries or blood vessel channels
which are associated to sudden death (Royal College of physicians, 2010). Clots are able
to obstruct blood flow to and from the heart and cause chest ache and heart attack; also
strokes can occur when blood fails to flow to the brain. The failure of blood supply in
limbs can lead to skin irritation where total blocked blood veins can lead to sudden death
(U.S. Department of Health and Human Services, 2010).
2.3.6 Lung cancer and brain tumors
Chemical in tobacco smoke move quickly from lungs via bloodstream all over the body,
poisons in tobacco smoke spoils tissue, cell arrangement and obstruct the whole body
normal procedure. Involuntary smoking causes more than eighty five percentages (85%)
of lung cancers it can also cause cancer in mouth, nose, throat, stomach, kidneys bone
marrow and blood (Surgeon General’s report, 2010b).
12
Royal College of physicians (2010) reported on abnormal growth of brain or cells, they
argue that these occur after tobacco chemicals damage genes which control normal cell
growing and function, when genes are spoiled by tobacco smoke, cells can start
increasing abnormally and form cancer, the body’s protected structure react to abnormal
cell enlargement and sends out “tumor fighters” to hit and kill these cells. However,
chemical in tobacco (toxic) weaken this action and makes simple for abnormal cell
growth, in turn forms cancer or brain tumor.
2.4 Involuntary smoking in related to academic performance
Children performance is influenced by different things such as active attendance in
classroom session, participation in school activities, private study and presence of
teachers and books. Involuntary tobacco smoke causes poor school attendance to
children since. Children are obstructed by numerous health problems such as respiratory,
circulatory, and cancer. These health problems results in low class participation, poor
attendance hence poor academic performance (Sindelar, 2005).
2.4.0 Involuntary smoking and its relation to Pupil’s participation and
school attendance
Human body organs are interdependent the proper function of one organ depends on the
other, children exposure to involuntary smoke hinders their immune system as a result it
leads to related health effects. These health problems result to poor children academic
performance in school (Reynolds, 1994).
2.4.1 Learning ability
Involuntary tobacco smoking and maternal smoking during pregnancy is assessed as a
risk factor for a variety of neurodevelopment problems in children, it reduces general
development of the brain and nervous system that affects intellectual quotient , growth,
emotion, learning ability, memory, skills in language, self control and auditory tasks
hence poor academic performance (Bandiera, 2015)
Figure1 : showing health effect associated with tobacco smoke

13
Throat diseases
Nose problem Lung cancer
Eye affected loose learning ability Anti-social behavior
Ear disease Asthma and wheezing
Source: WHO, ASH, Web site & Field 2016.
2.5 Conceptual frame work

14
Background information
(Independent) (Dependent)
Outcome variables
Exposure variables
2.6 Background variables
Children age, gender, class, parent/guardian/family member/friends
smoking tobacco on your presence-education-job- and number of the
smoker at home.
Risk factors
Parents, guardians or any family member
smoking tobacco at home.
Environment and life style
House close to tobacco farm-factory
processing, close to solid waste mixed
dumpsite pollution, burning mixed solid
waste around home, population of the
households, fuel use for cooking. Inherit
diseases and eating polished food.
Academic requirements
Behavior, participant, presence of
teachers, availability of text books,
children class attending, availability of
equipment for learning, enough time for
private study at home, how often you
study per week, parents/ guardians and
community support
Health effects Asthma, wheezing,
antisocial behavior,
attention deficit
disorders, increase risk
of heart attack and heart
diseases, ears/ nose and
throat problem,
respiratory disease like
nasal passages.
Academic effects
Class participation, class
position, average score,
low mark performance,
high mark performance,
general academic
performance

15
Children age.
Gender.
Class.
If their friends are smoking at home.
Parent/guardian smoking tobacco.
Number of the smoker at home.
Parent/ guardian education.
Parent/guardian job.
Parent/guardian smoking on your presence.
Number of the cigarettes smoked in the presence.
2.7 Life style variables
Type of house.
Number of sleeping rooms at home.
Household populations.
House located near to tobacco farm, factory processing, solid waste mixed dumpsite.
How long from home (kilometer).
Smoke drift to your home from factory processing tobacco, tobacco farm and solid
waste mixed dumpsite.
Burning mixed solid waste around home.
Use plastic to make fire like time of cooking.
Type of fuel household mainly use for cooking.
Inherit diseases in your family.
Use of polished food.

16
2.8 Factors for good academic performance to children
Presence of teachers.
Availability of text books.
Class attending.
Availability of equipment for learning.
Enough time for private study at home.
How often you study per week.
Working toward assignment given.
Parents/guardians and community support.
2.9 Health effects to children exposed to tobacco smoke
Asthma.
Wheezing.
Breathing.
Antisocial behavior.
Attention deficit disorders.
Heart diseases.
Ears, nose (sense of smell) and throat problem.
Respiratory disease like Nasal passages the bronchi and lungs.
2.10 Exposing children to tobacco smoke in relation to class academic performance
at school
Class participation.
Class position.
Average score.
What do you like to do for this age?
Which subject do you like?
17
CHAPTER THREE
METHODOLOGY
3.0 Introduction
This chapter explains the study area, study population, target population, study design,
tools and techniques for data collection, method for data collection, unit of study, sample
size, sampling procedure, data collection and quality control, data entry and cleaning,
data variable and analysis and ethical consideration. The chapter also presents research
schedule which shows allocated time and the research activities.
3.1 Study area
The present study was conducted at Kikundi primary school in Morogoro Municipal,
this was due to the fact that the school had students of brain disability, accessibility of
problem and recourses available for study. Involuntary smoking is among the factor for
that disability; also it helped the researcher to determine the relationship between health
effects caused by involuntary tobacco smoking and their outcome to primary school
children academic performance.
3.2 Study population
The study populations were primary school children and academic teacher at Kikundi
primary school in Morogoro Municipal.
3.3 Target population
The target population was pupils from class five, six and seven also academic teacher.
The academic teacher helped to provide results of respondents from Kikundi primary
school in Morogoro Municipal. The researcher compared exposed group and comparison
group. Exposed group were all children whom their parents/guardians or any member of
family smoking tobacco at home. The source of exposure or risk factor were
parents/guardians or any member of family.

18
None exposed group also called control or comparison group, these were children whom
their parents/guardians or any member of family do not smoke tobacco. The aim was to
find out whether tobacco involuntary smoking contributed to children health effect like
respiratory diseases (nasal passages the bronchi), increase risk of heart attack and heart
diseases, brain problem, ear problems, nose (sense of smell) and throat, death, asthma,
attention deficit disorders, stroke, antisocial behavior, wheezing in relation to children
academic performance at school.
Not only tobacco smoke chemical causes health effects but also other harmful chemicals
available in the air such as solid waste smoke from plastic burning, staying close to
dumpsite, working in factories producing smoke, asbestos, petroleum refinery, leaving
in poor ventilated house, number of sleeping rooms at home, population of the
households, house location, burning waste plastic at home, use plastic bags in fire
lighting, type of fuel used for cooking and inherited diseases in family.
Academically, children need presence of teachers, availability of text books, active class
attendance, availability of equipment for learning, enough time for private study at
home, parents/guardians and community support toward academic performance in
school. This helped the researcher to determine whether poor academic performance is
caused by tobacco smoke or inefficient academic requirements.
3.4 Study design
The study used a case control to explore and describe the data in real life situation with
its complexities in environment. Qualitative analysis was used in this study to describe
the behavior relating to the study. Due to this research design, its result, conclusion and
recommendation can be used in any place in the world.
The study involved open and ended questionnaire, the data available from field helped to
answer two specific objectives, to determine the health effect and academic performance
to pupils exposed to tobacco involuntary smoking at home.

19
3.5 Tools and techniques for data collection
The study used semi structured written questionnaires; both open and close ended
questions were used. The questions covered, involuntary smoking and its effects to
children health and academic performance among pupils from class five, six and seven
at Kikundi primary school in Morogoro Municipal. Health effects were brain tumors,
middle ear disease, respiratory illness, heart disease, asthma antisocial behavior,
wheezing, stroke, lung cancer, sudden death in relation to poor performance of children
at school.
Apart from asking health effect children were asked to give background information to
determine age, parent/guardian education and whether there is presence of smokers at
family. The third issue asked based on life style to know whether there was any cause of
diseases mentioned above apart from tobacco smoke like location of the house to damp
areas, burning of plastic bags at home. Furthermore respondents were asked whether the
school has enough requirements manifesting good academic performance like text
books, class attendance, community support and enough professional teachers.
Tools used in study were questionnaire, pen, school desk and camera.
3.5.1 Methods for data collection
Primary and secondary methods of data collection were employed in this study. A
questionnaire was used to collect primary data where both open ended questions and
close ended questions were prepared in English and interpreted in Swahili to help pupils
understanding, because most of them are familiar with swahili than English language.
The questionnaire had 49 questions, in close ended questions respondents were asked to
select the correct answer from many provided answers, in open ended questions, the
respondents were provided space to fill in the answer. Academic teacher help on
determine the nature of student in academic performance.

20
3.6 Sample size, sampling and procedures
3.6.1 Sample size
Class five were 59, six 54 and seven 57 total numbers were 200. The time for research
was four months means 120 days, per year we had 365days. The calculation below
shows how the researcher obtained the sample size;-
200pupils =365 days
120 days
(200 × 120) ÷ 365 = 66
Time for working per day was 8 hours (1/3). 66 ×1/3=22, and it needed range of sample
size 25%-30%. 22 × 30%=7
To make the research reasonable for data collection the researcher used 40 pupils from
each class, for exposed 20 and the rest for comparison group also 20, total respondents
were 120. Exposed group were 60 children and comparison group were 60, 0.05 was the
significance of study.
The study intentionally needed academic teacher to explain more about respondent’s
results from class five to seven for the pupils that were selected as respondents. She
helped in filling the annual average, class position, participation and behavior. Apart
from asking children also teacher proved the academic performance of children. .
3.6.2 Sampling
The researcher used both purposive and random sampling to select 60 respondents from
exposed group and 60 from non exposed group. However this sampling method had a
number of weaknesses including bias since the researcher could select respondents
without relevant information and abandon respondents with correct data. Children were
selected based on characteristic due to number required. Also the sampling techniques
lacked heterogeneous representation hence affected validity of the findings.
21
3.6.3 Sampling procedures
The researcher collected information from all available respondents at Kikundi primary
school. From each class the researcher determined respondents who were exposed to
tobacco smoke and non-exposed respondents. Parents/guardians, and any members of
family smoking tobacco were risk factor. The required number were 120 respondents, 60
as a case group and 60 as control group, all agreed pupils were joining the study for
questionnaire administration according to required sample.
3.7 Pre-testing tools for data collection
Before data collection, the well designed questionnaire was tested using 10 children
from Morogoro primary school. This aimed at improving the questions, the participants
for pre testing questionnaire are outside the calculated sample size.
3.8 Data management
Data management contains all aspects of data collection, quality control, data entry,
cleaning techniques, data variables and data analysis planning. The objective was to
create a reliable data base containing high quality of data.
3.8.1 Data collection and quality control
The data collection was performed by the researcher himself and his friend Alfraid
Mihayo on March 2016 during working hours from 8 AM to 3 PM noon. Data was
collected from pupils of class five, six and seven who were purposively and randomly
selected at Kikundi primary school.
3.8.2 Data entry and cleaning techniques
After data collected from the field, the researcher coded data from text into numerals and
entered into MS excel by double entrants and later cleaned to remove errors in terms of
accuracy, consistence, and responses. Each possible answer was assigned number to
ease the determination of correctness of data during the whole process of data entry and
cleaning. Then, analysis of the clean data was done by Statistical Package for Social
Science (SPSS) according to research objectives.

22
3.8.3 Data variables and analysis
Data variables for analysis included background variables like children age, gender,
class; he/she smokes tobacco, friends who are smoking, parent/guardian smoking habit,
number of the smoker at home, parent/ guardian education and their job.
Variables for frequency and percentages on heath effect to children included asthma,
wheezing breathing, sudden death, antisocial behavior, brain tumors, attention deficit
disorders, cancer like lung cancer, increase risk of heart attack and heart diseases, ears
nose (sense of smell) and throat problem, respiratory disease like nasal passages the
bronchi and lungs among children.
Life style of respondents included in the study to determine if there was association
between affected respondents of SHS and academic performance.
3.9 Ethical considerations
A researcher was aware of the ethical issues during the research study. A researcher
submitted research ethics application for approval before the research. The researcher
ethically bound to respect the participant’s human dignity, free and informed consent,
privacy and confidentiality, justice and inclusiveness. Before the study, the participants
were informed about the nature, purpose and procedures of the study. Participants were
free to answer specific questions, and withdraw from the study at any time, for any
reason.
3.10 Research work plain
ACTIVITIES JAN FEB MAR APL MAY JUNE JUL
Proposal writing and developing
research tools from supervisor
Test research tools and data Collection Data entering and cleaning Report analysis and writing
Preparation for master sheet and
supervisor recommendations
Dissemination of report findings

23
CHAPTER FOUR
PRESENTATION OF THE FINDINGS
4.0 Introduction
In this chapter, the researcher explains the findings, which were highlighted during the
study. The researcher observed, analyzed, and discussed the findings from the practical
data by considering research questions, objectives and hypothesis. The researcher also
attempted to analyze the data and interpret the results with respect to the research
propositions developed to guide the study.
4.1 Characteristics of respondents
Respondent’s characteristics were children age, gender, education level, class level,
parents/ guardian and all people around who are smoking tobacco, these characteristics
were important for the reasons that, they may propose the nature of responses and
possible essential reasons provided by the respondents.
4.1.0 Respondents distribution by gender and class
One hundred and twenty pupils/respondents from class five, six and seven at Kikundi
primary school were involved in the study, also one academic teacher was involved in
the study to provide information about academic performance of all pupils included in
the study with 40% (n=48) male and 60% (n=72) female. Where class five were 37.5%
(n=45), six 22.5% (n=27) and seven 40% (n=48).
4.1.1 Respondents distribution by age
The age of respondents was divided into five groups: 9-10, 11-12, 13-14, 15-16 and 17-
18. The findings in table 4.1 shows that the greater number of respondents were aged
between 13-14 n=54 (45%) the next group were aged between 11-12 n=37 (30%)
followed by those aged 9-19 n=16 (13.3%) next to them aged to 15-16 n=11 (9.2%) the
last group in study aged 17-18 n=2 (1.7%). The aim behind this aspect is to determine
the relationship between age and effects of involuntary smoking related to academic
performance of primary school children.

24
4.1.2 Number of smokers at home
The study divided respondents into two group, the first one was all children whom their
parents/guardians or any member of family smoke tobacco. Findings show that families
with no smokers were n=60 (50%), families with one smoker n=35 (29.2famiies with
two smokers were n=10 (8.3), three smokers were n=13 (10.8%) and the last group were
families with four smokers which showed n=2 (1.7%). Findings also show the number
of smokers smoking on presence of children at home were n=56 (46.7) and n=64 were
not using tobacco on presence of children. This shows that the number of smoker and
non smoker were the same.
4.1.3 Respondents distribution by parent/guardian education
Parents/guardian education level was divided into five groups: Illiteracy, primary
education, secondary education, college education and university or higher education
level. The results in table 4.1 show that eight male (6.7%) and four female (33.3%) had
not attained school. Forty two (35%) male and fifty four (45%) female had attained
primary level. Secondary level was fifty male (41.7%) and forty one female (35.2%).
Fifteen (12.5%) male and sixteen (13.3%) female have attained college level. The last
group was university or higher level who were five male and female (4.2%). These show
that in this study most of the parents and guardians have primary and secondary
education level. The aim of data is to determine the relationship between smoking and
level of education. Data are clearly presented in Table 4.1
4.1.4 Respondent’s parent/guardian distribution by job
Parents/ guardians job distribution was categorized into four groups, peasant, employed,
self employed and last group was parents/guardian with no job. Male 13(10.8%) and
female 19(15.8%) were peasants, employed parents/guardian were 38(31.7%) male and
25(20.8%) female, male 66(55%) and female 45(37%) were self employed the last group
was jobless parents/guardians s female jobless parents were 31(25.8%) male were
3(2.5%). The purpose for this aspect was to determine the relationship between income
and tobacco smoking. The result shows the number of parents and guardians work to

25
raise their family income are self employed others are employed in different private and
public sectors.
Background information for respondents
No Variables Codes Sub variables Frequency Percentage
1 Children age 1 9-10 16 13.3
2 11-12 37 30.8
3 13-14 54 45.0
4 15-16 11 9.2
5 17-18 2 1.7
Total N=120 %=100
2 Gender 1 Male 48 40
2 Female 72 60
3 Class 1 Five 45 37.5
2 Six 27 22.5
3 Seven 48 40.0
4 Friend smoking 0 No 108 90.0
1 Yes 12 10.0
5 Parent smoking 0 No 60 50.0
1 Yes 60 50.0
6 Smoker(s) at home 0 Not smoking 60 50
1 Cigarette 35 29.2
2 Cigarette 10 8.3
3 Cigarette 13 10.8
4 Cigarette 2 1.7
7 Parent education 1 Illiteracy
Male
Female
8
4
6.7
33.3
2 Primary Male
Female
42
54
35.0
45.0
3 Secondary Male
Female 50
41
41.7
35.2
4 College Male
Female
15
16
12.5
13.3
5 University Male
Female 5
5
4.2
4.2
8 Parent job 1 Peasant
Male
Female
13
19
10.8
15.8
2 Employed
Male
Female
38
25
31.7
20.8
3 Self employed Male
Female 66
45
55.0
37.0
4 Home mother Male
Female
3
31
2.5
25.8
9 Smoking presence 0 No 64 53.3
1 Yes 56 46.7

26
10 Cigarette per day 0 Non smoker 60 50.0
1 1-5 Cigarette 33 27.5
2 6-10 Cigarette 14 11.7
3 11-15 Cigarette 13 10.8
Respondent’s environmental and life style 11 Types of house 1 Built 61 50.8
2 Rent 54 45.0
Children camp 5 4.2
12 Sleeping room 1 1-3 Rooms 63 50.8
2 4-6 Rooms 54 45.0
3 7-9 Rooms 5 4.2
13 Population at home 1 1-5 Peoples 45 37.5
2 6-10 Peoples 66 55.0
3 11-25 Peoples 9 7.5
14 House located 1 Tobacco factory 2 1.7
2 Tobacco farm 7 5.8
3 Solid mixed dumpsite 3 2.5
4 Burning plastic area 3 2.5
5 Not close 105 87.5
15 How long to home 1 Half kilometer 4 3.3
2 One km 2 1.7
3 Two km 4 3.3
4 Three km 5 4.2
5 Not close 105 87.5
16 Smoke drift 0 No 103 85.8
1 Yes 17 14.2
17 Burning plastic 0 No 87 72.5
1 Yes 33 27.5
18 Using plastic to make
fire
0 No 65 54.2
1 Yes 55 45.8
19 Inherit diseases 0 No 96 80
1 Yes 24 20
20 Fuel use 1 Gas 13 10.8
2 Fire wood 9 7.5
3 Electricity 1 0.8
4 Charcoal 85 70.8
5 Kerosene 3 2.5
6-8 More than one fuel 9 7.5
21 Eating polish food 0 No 11 9.2
1 Yes 109 90.8
27
Table 4.1: Frequency table showing characteristics distribution
(magnitude/prevalence for various variables)
Health effects No Variables Codes Sub variables Frequency Percentage
22 Asthma 0 No 106 88.3
1 Yes 14 11.7
23 Respiratory problem 0 No 103 85.8
1 Yes 17 14.2
24 Wheezing 0 No 92 76.7
1 Yes 28 23.3
25 Deficit disorders 0 No 92 76.7
1 Yes 28 23.3
26 Heart diseases 0 No 117 97.5
1 Yes 3 2.5
27 Ear problem 0 No 100 83.3
1 Yes 20 16.7
28 Hear problem 0 No 114 95
1 Yes 6 5
29 Nose sensing 0 No 9 7.5
1 Yes 111 92.5
30 Throat disease 0 No 80 66.7
1 Yes 40 33.3
31 Anti-social 0 Be myself 7 5.8
1 With friends 113 94.2
Factor toward academic performance
32 Enough teachers 0 No 3 2.5
1 Yes 117 97.5
33 Text book 0 No 95 79.2
1 Yes 25 20.8
34 Class attending 0 No 1 0.8
1 Yes 119 99.2
35 Private study 0 No 28 23.3
1 Yes 92 76.7
36 How per week 1 Once 19 15.8
2 Two 10 8.3
3 Three 13 10.8
4 Every day 61 50.8
5 No time for private std 17 14.2
4.2 Association between causes variable and outcome in health
Table 4.2 summarizes the result of association between asthma, wheezing, antisocial
behaviours, attention deficit, heart disease, ear problem, nose fail sensing, throat
problem, respiration diseases, children class participation, average and general
performance outcome and children involuntary tobacco smoking exposure indicator
using parents/guardian and any member of family smoking tobacco, number of smoker

28
at home, number of cigarette smoking on children presence, age, gender and class to
pupils, job and education to parent/guardians.
The results show that other variables do not show statistically significant association
with outcome of involuntary tobacco smoke. For example class, age and gender of
pupils had no positively association to asthma, probability value show 0.5. Other
independent variables were job and education; these show weak association to some
outcome. For example the association between parents/guardians education for male and
wheezing the result shows 0.08 which implies that there is no relation between outcome
and causes.
4.2.0 Smoking on child presence and wheezing outcome
Wheezing is one among health effect to children exposed to involuntary smoke that
makes difficulties for the child to breath. The study shows that parents/guardians who
smoke on children presence had strong association with children wheezing, in 56
parents/guardians who smoke in the presence of children 26 had wheezing problem and
30 had no wheezing problem. 64 Parent/guardians were not smoking on children
presence, among them 62 children had no wheezing problem 2 children had wheezing
problem. The probability value shows that there is strong association (relationship,
significant positive associations) between smoking on children presence and wheezing
problem to children as the fisher’s exact test tested 0.000, These have been explained
clearly on table 4.2 above.
4.2.1 Tobacco smoking in relation to ant-social behavior
Anti-social behavior to children is associated with involuntary smoking. The
questionnaire distributed to 60 respondents showed that families with no smokers have
zero anti-social children; families with one smoker had four anti-social children among
thirty five respondents. The family with two smokers had one anti-social among ten
children. The family with three smokers had two anti-social children among thirteen
children. The PV shows that there is strong significant positive association between

29
number of smokers at home and anti-social behaviors to children. The fisher’s exact test
shows 0.017, these have been demonstrated clearly on table 4.2.
4.2.2 Association between parent/guardians smoking and throat diseases
Living in families with smoker(s) have association to children with throat diseases like
pain, irritation, throat and mouth cancer, this was proved to be influenced by tobacco
involuntary smoking. The result shown that seven (7) children out of sixty (60) who
came from families with smoker(s) had the above mentioned diseases, thirty three
children out of sixty have throat disease. The study further realized the increasing
number of children with throat disease in case group compared to control group. The PV
shows strong positive association between parents/guardians or any member of family
using tobacco in relation to throat diseases. The fisher’s exact test shows 0.000, these
have been demonstrated clearly on table 4.2.
4.2.3 Number of cigarette smoked on presence of children per day in
association to nose problems
Table 4.2 also summarizes the results of association between outcome of children nose
problems and children exposure to numbers of tobacco cigarette smoked per day. The
number of cigarette smoked per day on children presence was divided into four groups
as follows. The first group was non smokers who were 60 out of that only 1 child had
nose problem, the second group was parents/guardians and other smokers at home who
smoke 1-5 cigarette per day, it was shown that 5 children had nose problem out of 33,
another group was parents/guardian smoking 6-10 cigarette it was shown that 2 had nose
problem out of 14 children, the last group was smokers smoking 11-15 cigarette per day
only 1 child had nose problem out of 13 children. The above results are well presented in
table 4.2. PV shows strong significant positive associations between number of cigarette
smoked by parents/guardians per day on children presence and outcome of nose sensing
problems, the fisher’s exact test shows 0.036.

30
4.2.4 Exposing children to involuntary tobacco smoke at home in
association to ear problem
Parents/guardians were divided into two groups, the smoking parents/guardians and non
smoking parents/guardians or any member of family. The result shows that there is
association between parent/guardians smoking tobacco and ear problem to children. Non
smokers were 60 participants only 5 reported to have ear problem. Smokers group had
60 participants in which 15 were reported to have ear problem. The table 4.2 shows the
PV implies strong significant positive associations between parents/guardians or any
member of family smoking tobacco and outcome of ear problem. The Pearson Chi-
Square shows 0.014.
4.2.5 Smoking tobacco in association to nose problem among children
According to the findings there is association between the families with smoker(s) and
outcome of nose problem to children who are exposed to tobacco smoke. The numbers
of smokers were divided in three groups. The first group was 60 participants from
families with zero smokers, only 1 child had nose problem. The second group was
families with one smoker, the result shows 7 children found with nose problem out of
35, and the families with 3 smokers had 1 child with nose problem out of 13
respondents, fisher’s exact test shows 0.023.
4.2.6 Children exposure to involuntary smoking in association with ear
problems
Children exposure to involuntary smoking and its association to ear problem is clearly
presented in table 4.2. 6 respondents were found with ear problem out of 60
parent/guardians smokers group. 14 respondents were found with ear problems out of 60
parents or guardians non smokers group, PV shows strong significant positive
associations between children exposure to involuntary smoking with ear problem. The
Pearson Chi- Square shows 0.022.
4.3 Environmental and life style variables
Other variables which create problems to human health and hinder children academic
performance other than involuntary tobacco smoking are such as burning plastic bags,

31
living in poor ventilated house, dust, and using fire woods. The health problems that
may occur as the result of the above mentioned variables are such as asthma, wheezing,
antisocial behaviours, attention deficit, heart disease, ear problem, nose fail sensing,
throat problem, and respiration diseases.
4.3.0 Poor ventilated house in association with respiratory diseases
The results shows negative association between poor ventilated house and respiratory
diseases. It was found that 8 children out of 61 respondents living in their own houses
had respiratory diseases, while 9 children out of 54 respondents living in rented houses
had respiratory diseases; also it was found that out of 5 children living in children camps
none of them were found with respiratory diseases. . PV presented in table 4.2 shows
negative significant associations between respondents’ houses and respiratory diseases.
The fisher’s exact test shows 0.821.
4.3.1 Association between number of sleeping room and wheezing
Wheezing has been associated with number of sleeping rooms and sleeping population,
Population in single room can cause wheezing due to shortage of air in the room. The
result shows no significance positive association between number of sleeping rooms and
wheezing. The number of room were divided into three groups, 14 children out of 63
respondents living 1-3 children in a room were found with wheezing problems, 13
children out of 53 living 4-6 children in a room were having wheezing problems and 1
child out of 4 living 7-9 children in a room was having wheezing problems, fisher’s
exact test shows 0.926 and PV shows negative association between number of sleeping
rooms and wheezing. The above data are well presented in table 4.3
4.3.2 Population at home, plastic bag burning in association with nose
problems
There is no significant positive association between number of people living in the one
room and nose problems. The fisher’s exact test shows 1.000. Home population was
divided into four groups, the population of 1-5 people in family were 45 and 4 children
had nose sensing problem, another group of 6-10 people in single family were 66 and 5

32
children had nose sensing problem, the last group were 9 people from group of 11-15
and 16-25 people, one respondent had nose problem. PV shows 1.000 implying that
there is no significant association between respondents’ population at home and nose
sensing problems. The above data are presented in table 4.2
There were also non-significance positive associations for house located more than three
kilometers near tobacco factory, tobacco farm, solid mixed dumpsite, burning plastic
area and asthma. The result shows that respondents that their houses located near
tobacco factory were 2, no one found with asthma, the second group’s houses were
located near tobacco farm were 7 and 2 had asthma, another group is of children living
near solid mixed dumpsite area who were 3 and no one had asthma, the fourth group of
respondents living near burning plastic area were 3, 1 had asthma and the last group of
pupils living more than three kilometers from dangerous areas were 94, 11 had asthma.
The fisher’s exact test shows 0.299.
Another mediating factor tested in study was burning of mixed plastic at home and
attention deficit disorders. PV on table 4.2 shows no significant positive associations
between burning of mixed plastic at home and attention deficit disorders problem
outcome. The Pearson Chi- Square shows 0.735. Groups were divided into two, in the
first group respondents who do not burn mixed plastic at home were 87 and 21 had
attention deficit disorders, the next group who were burning mixed plastic at home were
33 and 7 children had attention deficit disorders.
4.3.3 Use of plastic material, burning plastic and type of fuel use associated
to attention deficit disorders, asthma and throat problem
Table 4.2 shows association between plastic burning in charcoal lighting with attention
deficit disorders, respondents were divided into two groups, the first group was non
plastic users on charcoal lighting these were 65 out of this group 5 respondents had
attention deficit disorders the rest had no problem of attention deficit disorders. The
second group was respondents using plastic on charcoal lighting who were 55, 12 had
attention deficit disorders and the rest had no problem. The PV shows strong significant

33
positive associations between charcoal lighting using plastic bags with attention deficit
disorders. The Pearson Chi- Square shows 0.027.
Table 4.2 also shows PV with no significance positive association between burning
plastic bags at home and asthma disease, the fisher’s exact test shows 0.755, children
who were not burning mixed plastic at home were 87 and 11 had asthma, the
respondents who were burning mixed plastics at home were 33 and 3 had asthma.
The researcher also found no association between types of fuel respondent’s use and
throat disease; types of fuel used were in eight groups such as gas, firewood, electricity,
charcoal, kerosene, gas-electricity and charcoal, gas and fire wood and last group using
fire wood and electricity. Fisher’s exact test shows 0.859 which implies no significance
positive association between types of fuel use and throat problem. Respondents using
gas were 13 and 5 had throat problem, in the group of 9 respondents who were using fire
wood, 3 had throat problem, 1 electricity user had no problem, Out of 85 respondents
using charcoal, 28 had throat problem, and only 2 respondents had throat problem out
of 9 respondents using more than one fuel.
4.4 Requirements for academic performance in primary school
The researcher also investigated the requirement for academic performance in primary
school such as presence of books in class, presence of teachers, private study for
respondents, class attending, availability of learning equipment and parents/guardians
supporting.
4.4.0 Relationship between pupils term average and general performance to
adequate teachers and availability of text books in class
The study tested availability of teachers for each class to see if it relates to pupil average
score, averages for two terms were taken, January to June and July to December,
children who said teachers are not enough were shown as follows, On the first term no
child scored A and F average, 18 children scored B, C were 55, 22 scored D but no one
said teacher are inadequate, E were 22 and argued that teachers are enough, fisher’s

34
exact test shows 1.000, There is no significant associations between availability of
teachers and half term average scores as presented in table 4.2.
The end term average of a year is shown on table 4.2 as follows, 3 pupils who score D,
C=2 and E=1 these said teachers are not enough, the rest 117 pupils scored A, B, D and
F said teachers are enough, PV shows no significant associations between availability of
teachers and end term average scored as the fisher’s exact test shows 0.451.
The researcher investigated the association between shortage of books in association to
general performance of a child, pupils performance were divided into three groups;
increase, decrease and stagnant performance. Pupils who said books were not enough
were 95, 41 had their performance increased, 45 decreased and 9 were stagnant.
Whereas out of 25 respondents who said books are enough, 10 had increased
performance, 15 decreased and none had stagnant performance. The fisher’s exact test
shows 0.270, means there is no significant associations between availability of text
books and general performance.
Class attendance was used to determine if pupils are attending to school every day as
required, out of 120 respondents, 1 respondent had both poor class attendance and poor
academic performance, 51 had increased performance, 59 decreased and 9 stagnant
performance, fisher’s exact test shows 1.000, hence there is no significant associations
between class attendances and general performance.
4.4.1 Association between private study, pupil participation and average
Result shows no association between pupil private study and outcome of pupil’s
participation in class, fisher’s exact test shows 0.479, table 4.2 shows the results on how
pupils use time for private study. Respondents who had no private study their
participation in class were marked as follows; 13 scored very good, 13 good and 2 pupils
scored poor class participation. Respondents who had private study were as follows; 47
scored very good in class participation, 43 good and 2 pupils scored poor class
participation.

35
Association between how often per week pupil get time for study and the outcome on
average score. Children who study privately once per week had the following average
scores A=0, B=1, C=10, D=2, E=6 and F=0. Those who study twice per week had
average scores of A=0, B=0, C=4, D=3, E=3 and F=3. Pupils who study thrice per week
had average scores of A=0, B=2, C=4, D=5, E=2 and F=0. Those who study forth per
week had average scores of A=0, B=14, C=28, D=11, E=8 and F=0. While pupils with
no time for private study had average scores of A=0, B=1, C=11, D=1, E=4 and F=0.
Fisher’s exact test was 0.141 meaning no association between how often per week pupil
gets time for study and the outcome on average score.
4.4.2 Parents/community support and pupils home work factor associated
to class participation and general performance
The probability value between parents/guardians and community support to primary
pupils toward class participation shown by fisher’s exact test is 0.835. This means that
there is no association between parents support factor and pupils participation outcome.
Children from family whom parents/community did not support them on their studies
scored differently in class participation where 5 scored very good, 6 scored good and no
one scored poor or very poor. Out of 112 respondents who were supported by their
parents/community, 55 scored very good, 50 scored good and 4 scored poor.
Table 4.2 also shows association between pupils home works, assignments and class
participation. Negative association was found between pupils used to work on
assignment provided in class and those who did not, fisher’s exact test was 0.787, and
meaning there is no any association.
Further analysis among mediating factor for academic performance outcome was about
use of polished food to children associated to general performance at school. Children
need nutrients for growth and develop properly. Polished food normally doesn’t help
anything in body growth and brain. The study shows no association between using
polished food and general academic performance, 4 respondents were not using polished
food their results in academic performance increased. Other 4 pupils decreased in

36
performance and 3 stagnant. For those who were using polished food 47 performance
increase, 56 decrease and 6 stagnant, fisher’s exact test shows 0.074.
Generally as presented on table 4.2 mediating factors toward academic performance
were not associated to outcome meaning that cofounder are not sources of outcome to
academic performance.
4.5 Number of smoker(s) at home and general academic performance for children
Table 4.2 shows strong association between number of smoker(s) at home and general
academic performance for children. There were five groups, the first group was for non
smoker’s parents/guardians where 30 pupils were increasing in general academic
performance, 25 decreasing and five were stagnant in performance. The second group
was family with one smoker, the results shows that 13 pupils performance increased, 20
decreased and 2 stagnated. The group with two smokers in family 6 pupils performance
was increasing, 2 decreasing and 2 stagnant, the group with three smokers 2 pupils
performance were increasing, 11 decreasing and 0 stagnant, families with four smokers
0 pupils performance increased, 2 decreased and 0 stagnant, fisher’s exact test shows
0.038.
4.5.0 Association between class and average performance of children
The average of children was categorized into two groups first and second term.. The
average score was divided into six groups, A(81-100), B(61-80), C(41-60), D(31-40),
E(21-30) and F(0-20), first term result shows that class five were 45 in study but A(0),
B(12), C(19), D(4), E (10) and F (0). Class six were 27 in study A (0), B (4), C (13), D
(6), E (4) and F (0). Class seven were 48 in study A (0), B (2), C (25), D (12), E (9) and
F (0). The result shows the association between class and average academic
performance, the fisher’s exact test shows 0.043.
In the second term the result showed stronger and positive association than first term,
class five were 45 in study but A (1), B (16), C (15), D (6), E (4) and F(3). Class six
were 27 in study A (0), B (5), C (12), D (7), E (3) and F (0), class seven were 48 in study
A (0), B (2), C (23), D (15), E (8) and F (0). There is association between class and

37
average academic performance in the second term. Fisher’s exact test in table 4.2 shows
0.003.
4.5.1 Smoker(s) in family and smoking on children presence in association
with pupils academic performance
Presence of smoker(s) in family and smoking on presence of children had positively
associated with outcomes of poor average scores for pupils compared to non exposed
group. Table 4.2 shows non smokers families and average performance of pupils, the
average report of pupils shows A (0), B (12), C (32), D (6), E (10) and F (0). The result
also presents pupils average from smoking families, their average were B (6), C (25), D
(16), E (3) and F (0). The fisher’s exact test shows 0.050, however fisher’s exact test
average report for second term was 0.000, this shows pupils performance were poor
compared to first term, see table 4.5.
Parents/guardian or any member of family smoking tobacco on children presence had
shown strong association than families with non smoker(s). The fisher’s exact test
average report was 0.000-0.015. Meaning that smoking on children presence had more
effect on children academic performance. See table 4.2.
Table 4.2: Cross tabulation and crude analysis of exposure variables, disease and
academic outcomes
No Variables Sub variables No Asthma Had Asthma Total Pv
1 Children age 9-10 14 2 16
0.596
11-12 31 6 37
13-14 50 4 54
15-16 9 2 11
17-18 2 0 2
No disease
respiratory
Had disease
respiratory
2 Children age 9-10 14 2 16
0.411
11-12 30 7 37
13-14 49 5 54
15-16 8 3 11
17-18 2 0 2
No wheezing Had wheezing
0.825
3 Children age 9-10 13 3 16
11-12 29 8 37
13-14 41 13 54
15-16 7 4 11
17-18 2 0 2

38
Participation Very good Good Poor
0.682
4 Children age 9-10 8 8 0 16
11-12 18 18 1 37
13-14 30 21 3 54
15-16 4 7 0 11
17-18 0 2 0 2
5 Children age Anti-social To be my self To join other
0.657
9-10 2 14 16
11-12 2 35 37
13-14 3 51 54
15-16 0 11 11
17-18 0 2 2
6 Gender No disorder Disorder
0.159 Male 40 8 48
Female 52 20 72
7 Gender No ear problem Ear problem
0.50
Male 44 4 48
Female 56 16 72
8 Gender Performance Increase decrease stagnant
0.882 Male 21 23 4 48
Female 30 37 5 72
9 Class No heart attack
diseases
Heart attack
Five 43 2 45 0.334
Six 26 1 27
Seven 48 0 48
10 Class and ear problem Five 38 7 45
Six 21 6 27 0.674
Seven 41 7 48
No Variables Codes Sub variables Frequency Percen
tage
pv
No throat Throat diseases
11 Parents/guardian smoking No 53 7 60 0.000
Yes 27 33 60
Ear had no
problem
Ear had problem 0.014
12 Parents/guardian smoking No 55 5 60
Yes 45 15 60
No respiratory Respiratory
13 Parents/guardian smoking No 53 7 60 0.432
Yes 50 10 60
No wheezing Wheezing
14 Parents/guardian smoking No 58 2 60 0.000
Yes 34 26 60
No deficit Deficit
15 Parents/guardian smoking No 47 13 60 0.666
Yes 45 15 60
Not hearing clear Hearing clear
16 Parents/guardian smoking No 1 59 60 0.207
Yes 5 55 60

39
Nose not sensing Nose sensing
17 Parents/guardian smoking No 1 59 60
Yes 8 52 60 0.032
Average term
first
A B C D E F
18 Parents/guardian smoking No - 12 32 6 10 - 60 0.050
Yes - 6 25 16 3 - 60
End term A B C D E F
No 0 16 30 4 8 2 60 0.000
Yes 1 7 20 24 7 1 60
Nose not sensing Nose sensing
19 Smoker(s) home Non smoker 1 59 60 0.023
One person 7 28 35
Two person 0 10 10
Three person 1 12 13
Four person 0 2 2
No wheezing Wheezing
20 Smoke(s) home Non smoker 58 2 60
One person 19 16 35
Two person 7 3 10 0.000
Three person 8 5 13
Four person 0 2 2
No deficit Deficit
21 Smoke(s) home Non smoker 47 13 60
One person 29 6 35
Two person 8 2 10 0.218
Three person 7 6 13
Four person 1 1 2

40
No Variables Codes Sub variables Frequency Percen
tage
pv
Nose not sensing Nose sensing
Not hearing clear Hearing clear
22 Smoker(s) home Non smoker 1 59 60
One person 1 34 35
Two person 2 8 10 0.040
Three person 2 11 13
Four person 0 2 2
General
performance
Increase decrease Stagnan
t
23 Smoker(s) home Non smoker(s) 30 25 5 60
One smoker 13 20 2 35 0.038
Two smokers 6 2 2 10
Three smokers 2 11 0 13
Four smokers 0 2 0 2
No throat Throat pleasant
24 Smoker(s) home Non smoker(s) 53 7 60
One smoker 15 20 35
Two smokers 5 5 10 0.000
Three smokers 6 7 13
Four smokers 1 1 2
25 Smoke on child presence No 62 2 64 0.000
Yes 30 26 56
No throat Throat
26 Smoke on child presence No 56 8 64 0.000
Yes 24 32 56
No sensing Nose sensing
27 Smoke on child presence No 3 61 64 0.301
Yes 6 50 56
Not hearing clear Hearing clear
28 Smoke on child presence No 1 63 64 0.065
Yes 5 51 56
First term A B C D E F
29 No of cigarette per day Non smoker - 12 32 6 10 - 60
1-5 Cigarette - 3 15 8 7 - 33 0.330
6-10 Cigarette - 2 5 3 4 - 14
11-15Cigarette - 1 5 5 2 - 13
End term A B C D E F
Non smoker 0 16 30 4 8 2
1-5 Cigarette 1 4 12 13 2 1 0.023
6-10 Cigarette 0 2 2 7 3 0
11-15Cigarette 0 1 6 4 2 0
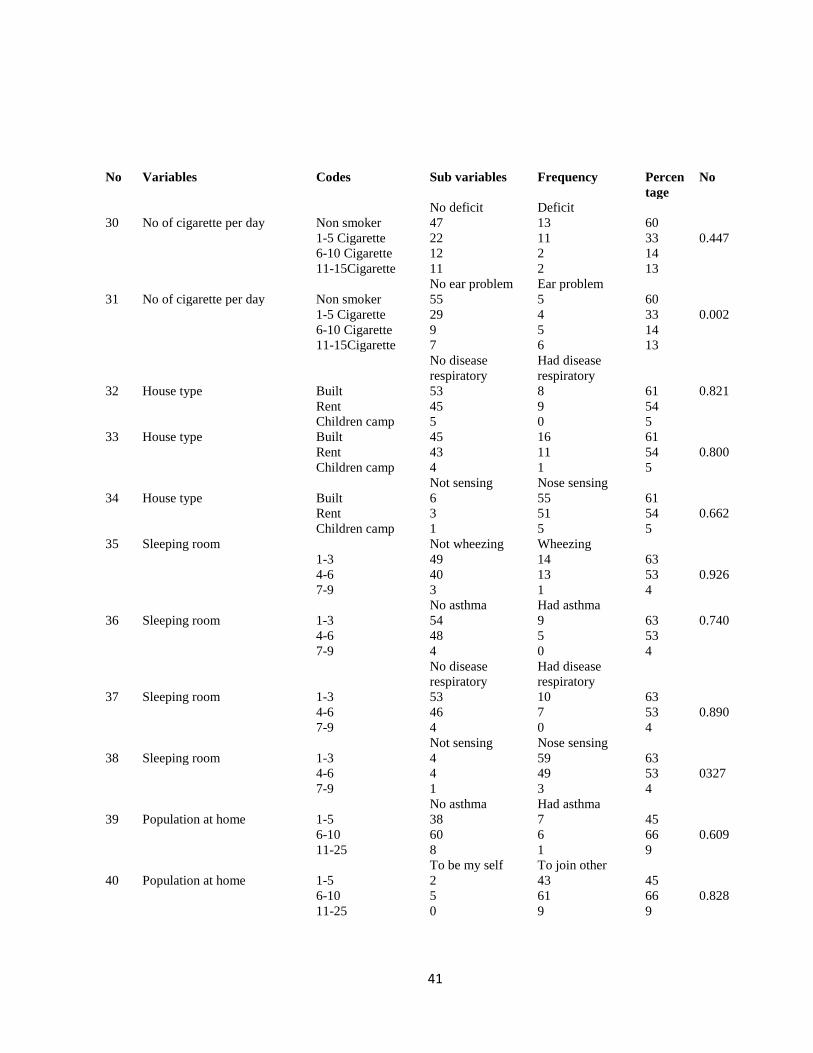
41
No Variables Codes Sub variables Frequency Percen
tage
No
No deficit Deficit
30 No of cigarette per day Non smoker 47 13 60
1-5 Cigarette 22 11 33 0.447
6-10 Cigarette 12 2 14
11-15Cigarette 11 2 13
No ear problem Ear problem
31 No of cigarette per day Non smoker 55 5 60
1-5 Cigarette 29 4 33 0.002
6-10 Cigarette 9 5 14
11-15Cigarette 7 6 13
No disease
respiratory
Had disease
respiratory
32 House type Built 53 8 61 0.821
Rent 45 9 54
Children camp 5 0 5
33 House type Built 45 16 61
Rent 43 11 54 0.800
Children camp 4 1 5
Not sensing Nose sensing
34 House type Built 6 55 61
Rent 3 51 54 0.662
Children camp 1 5 5
35 Sleeping room Not wheezing Wheezing
1-3 49 14 63
4-6 40 13 53 0.926
7-9 3 1 4
No asthma Had asthma
36 Sleeping room 1-3 54 9 63 0.740
4-6 48 5 53
7-9 4 0 4
No disease
respiratory
Had disease
respiratory
37 Sleeping room 1-3 53 10 63
4-6 46 7 53 0.890
7-9 4 0 4
Not sensing Nose sensing
38 Sleeping room 1-3 4 59 63
4-6 4 49 53 0327
7-9 1 3 4
No asthma Had asthma
39 Population at home 1-5 38 7 45
6-10 60 6 66 0.609
11-25 8 1 9
To be my self To join other
40 Population at home 1-5 2 43 45
6-10 5 61 66 0.828
11-25 0 9 9
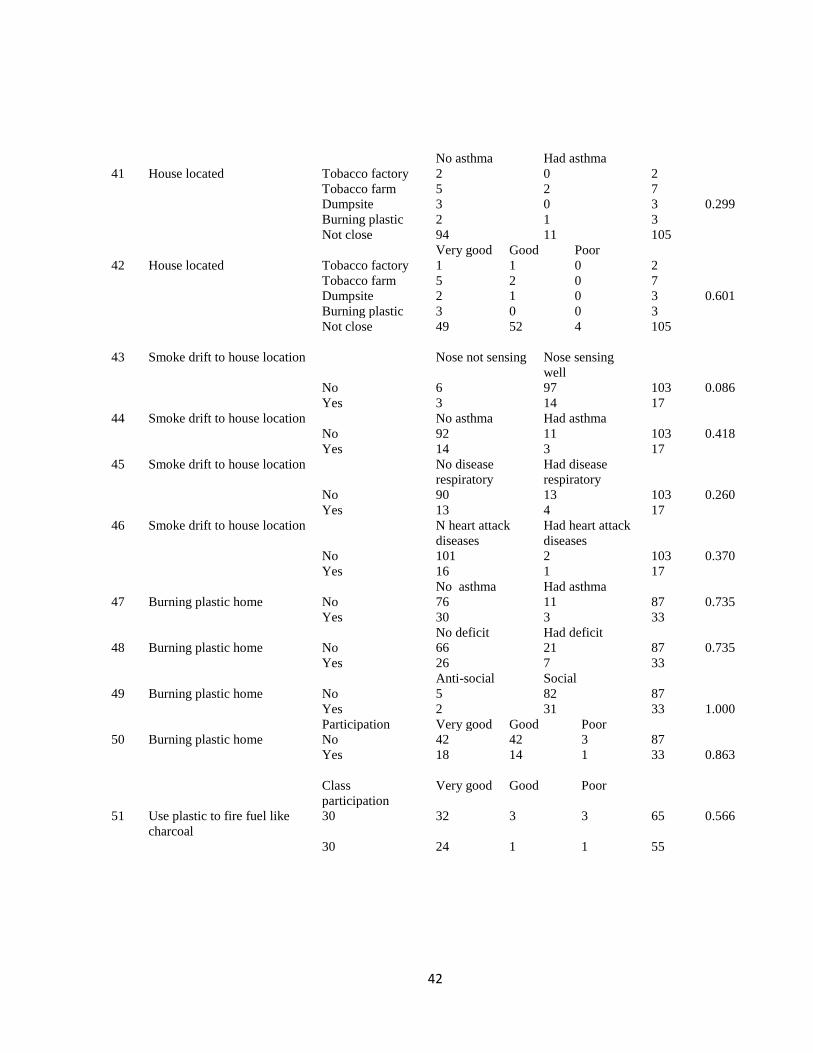
42
No asthma Had asthma
0.299
41 House located Tobacco factory 2 0 2
Tobacco farm 5 2 7
Dumpsite 3 0 3
Burning plastic 2 1 3
Not close 94 11 105
Very good Good Poor
42 House located Tobacco factory 1 1 0 2
Tobacco farm 5 2 0 7
Dumpsite 2 1 0 3 0.601
Burning plastic 3 0 0 3
Not close 49 52 4 105
43 Smoke drift to house location Nose not sensing Nose sensing
well
No 6 97 103 0.086
Yes 3 14 17
44 Smoke drift to house location No asthma Had asthma
No 92 11 103 0.418
Yes 14 3 17
45 Smoke drift to house location No disease
respiratory
Had disease
respiratory
No 90 13 103 0.260
Yes 13 4 17
46 Smoke drift to house location N heart attack
diseases
Had heart attack
diseases
No 101 2 103 0.370
Yes 16 1 17
No asthma Had asthma
47 Burning plastic home No 76 11 87 0.735
Yes 30 3 33
No deficit Had deficit
48 Burning plastic home No 66 21 87 0.735
Yes 26 7 33
Anti-social Social
49 Burning plastic home No 5 82 87
Yes 2 31 33 1.000
Participation Very good Good Poor
50 Burning plastic home No 42 42 3 87
Yes 18 14 1 33 0.863
Class
participation
Very good Good Poor
51 Use plastic to fire fuel like
charcoal
30 32 3 3 65 0.566
30 24 1 1 55

43
General
performance
Increase decrease Stagnant
53 Use plastic to fire fuel like
charcoal
No 30 29 6 65 0.423
Yes 21 31 3 55
No attention
disorders
Had attention
deficit
Use plastic to fire fuel like
charcoal
No 54 11 65
Yes 38 17 55 0.071
General
performance
Increase decrease Stagnant
54 Inheritance diseases No 44 45 7 96 0.316
Yes 7 15 2 24
No asthma Had asthma
55 Inheritance diseases No 87 9 96 0.118
Yes 19 5 24
No heart diseases Had heart
diseases
56 Inheritance diseases No 93 3 96 1.000
Yes 24 0 24
No asthma Had asthma
57 Types of fuel use Gas 11 2 13
Fire wood 7 2 9
Electricity,
kerosene, more
11 2 13 0.154
Charcoal 77 8 85
Not hearing clear Hearing clear
58 Types of fuel use Gas 0 13 13
Fire wood 1 8 9
Electricity,
kerosene, more
0 13 13 0.764
Charcoal 5 80 85
Nose not sensing Nose sensing
59 Types of fuel use Gas 1 12 13
Fire wood 1 8 9
Electricity,
kerosene, more
3 10 13 0.072
Charcoal 4 81 85
Class
participation
Very
good
Good Poor
60 Using polish food No 3 7 1 11 0.133
Yes 57 49 3 109
General
performance
Increase decrease Stagnant
61 Using polish food No 4 4 3 11 0.074
Yes 47 56 6 109
A B C D E F
62 Using polish food No - 0 6 1 4 - 11 0.264
Yes - 18 51 21 19 - 109
A B C D E F 11
Using polish food No 0 1 5 3 2 0 109 0.856
Yes 1 22 45 25 1 3

44
Requirements for academic performance
No Variables Sub variables Total Pv
1 term average A B C D E F
1.000
63 Enough teachers No - 0 2 0 1 - 3
Yes - 18 55 22 22 - 117
End term average
No 0 0 2 0 1 0 3
0.451 Yes 1 23 48 28 14 3 117
Class
participation
Very good Good Poor
64 Enough teachers No 2 1 0 3 1.000
Yes 58 55 4 117
General
performance
Increase decrease Stagnant
65 Enough teachers No 2 0 1 3 0.055
Yes 49 60 8 117
Class
participation
Very good Good Poor
66 Enough text books No 43 49 3 95 0.078
Yes 17 7 1 23
General
performance
Increase decrease Stagnant
67 Enough text books No 41 45 9 95 0.270
Yes 10 15 0 25
Half term A B C D E F
68 Enough text books No - 14 48 17 16 - 95 0.492
Yes - 4 9 5 7 - 25
End term A B C D E F
69 Enough text books No 1 18 42 20 13 1 95 0.290
Yes 0 5 8 8 22 2 25
Class
participation
Very good Good Poor
70 Class attending No 0 0 1 1 0.033
Yes 60 56 3 119
General
performance
Increase decrease Stagnant
71 Class attending No 0 1 0 1 1.000
Yes 51 59 9 119
Half term A B C D E F
72 Class attending No - 0 1 0 0 - 1 1.000
Yes - 18 56 22 23 - 119
End term A B C D E F
0 0 1 0 0 0 1 1.000
1 23 49 28 15 3 119
Half term A B C D E F
73 Pupils private study No - 1 15 4 8 - 28 0.131
Yes - 17 42 18 15 - 92
End term A B C D E F 28
0 4 13 5 6 0 92
1 19 37 23 9 3

45
Participation Very good Good Poor
0.479 74 Pupils private study No 13 13 2 28
Yes 47 43 2 92
General
performance
Increase decrease Stagnant
75 Pupils private study No 9 15 4 28 0.179
Yes 42 45 5 92
Class
participation
Very good
God
Poor
75 Parents/guardians follow up
No
5
6
0
11
0.835
Yes 55 50 4 109
General
performance
Increase decrease Stagnant
76 Parents/guardians follow up No 1 7 3 11 0.011
Yes 50 53 6 109
Half term A B C D E F
77 Parents/guardians follow up No - 1 5 2 3 - 11
Yes = 17 52 20 20 - 109
End term A B C D E F
Parents/guardians follow up No 0 1 5 2 3 0 11 0.623
Yes 1 22 45 26 12 3 109
Class
participation
Very good
God
Poor
78 Home work assignment No 5 3 0 8 0.787
Yes 55 53 4 112
General
performance
Increase decrease Stagnant
Home work assignment No 2 5 1 8 0.348
Yes 49 55 8 112

46
CHAPTER FIVE
DISCUSSION OF RESEARCH RESULTS
5.0 Introduction
This Chapter presents discussion of the findings presented in chapter four; the discussion
mainly focuses on explaining two specific objectives, first is to determine human health
effects of involuntary smoking to primary children exposed on tobacco smoke at home
and the second to determine whether exposing children to tobacco smoke at home results
to poor academic performance to primary children at school.
The results proved that involuntary tobacco smoking exposure to children has effects to
children health and academic performance to primary school pupils. The most problems
found in this study associated to expose factor are wheezing, throat problem and ant
social behaviors to children, academically the most problems are average and class
participation of children in school.
5.1 Primary children exposure to involuntary tobacco smoking at home and health
effects
Strong positive association were observed between exposure variable of
parent/guardians or any member of family smoking tobacco on presence of children at
home, number of smokers at home, number of cigarette smoked per day these results to
wheezing, ant-social behavior, throat problem, nose sensing problems and ear problem
for children. The study found that children exposed to tobacco smoke are strongly
associated with wheezing, this happens when other factors such as burning mixed solid
waste around home, house location, population at home and types of fuel using were
controlled. These consequences are consisted with the results of past studies in other
location that had shown a high probability value of association.
A substantial body of evidence indicates that involuntary exposure to tobacco smoke
adversely affects children’s respiratory health by decreasing lung growth and increasing
the risk of respiratory infections, respiratory symptoms, including wheezing, and

47
exacerbation of asthma, maternal smoking has been most strongly associated with
adverse respiratory effects in children, suggesting that fetal exposure to maternal
smoking may have long-term effects to children’ respiratory health (Frank, at el 2001.
US general surgeon, 2006. Ehrlich, et al 1996. Murray, et al 2004 & Hannah, 2012).
Ant-social behavior was also found to be associated with tobacco smoking. The study
determined that exposing children even to a single tobacco smoker has effect to children
behavior. Families with more than one smoker increase the chance for health effects to
children and other family member at large. Researcher conducted by Wakschlag,
Eichborn and Olds depicted that “Severe antisocial behavior are approximately 1.5 to 4
times greater for exposed than for non exposed youths” { (Wakschlag, 2002).,
(Eichborn, 2015) and (Olds, . 1997)}.
The study further stipulated that there is a positive association between
parents/guardians tobacco smoking with throat diseases, the study shows that throat is
one of the problem facing children exposed to tobacco involuntary smoking. The study
showed half of the children exposed to tobacco smoke have throat diseases compared to
non exposed children. It was also shown that children exposure to dumpsite, burning
waste area, tobacco farm, tobacco factory and burning plastic material around home had
no association with throat problem. The association happens to children using most of
their time at home doing daily activities such as playing, reading and social works while
their parents/guardians or any other relatives are smokers. A study was done by U.S
health and human service, (1986) to find whether children exposed to involuntary
tobacco smoking is associated with health problems, they found that there is a strong
association since children are affected by throat and wheezing it was further found that it
causes other symptoms including stuffy nose, headache, sore throat, mouth and throat
cancer, eye irritation and hoarseness. The study also stipulated that health problems
affect children school attendance. {(ASH, 2013)., (Sangar, 2016)., (U.S. Department of
Health and Human Services, 1986)., (Johnson, 2001). (And Boston University Pupil
Health Services, 2013) }.

48
Number of cigarettes parents/guardians smoked per day is associated with nose sensing
problem to children. The study showed strong association between causes and outcome,
results found that children exposed to parents/guardians smoking one cigarette packet
per day are more likely to get nose sensing problems, these problems affects children
eight times compared to non exposed ones. However The involuntary smoking do
depend on a number of cigarette a person smokes par day in order to get health effects.
Table 4.2 One study has shown that children living with parents smoking one cigarette
packet a day were more likely to misidentify the aromas of vanilla, roses, mothballs and
cough drops compared with a non exposed children.{( Australian Government DH,
2011) (Hirayama, 1990); (WHO, 2002) and (GreenFacts, 2002).
Involuntary tobacco smoking is associated with ear problems; it was found that exposing
children to involuntary tobacco smoking at home was significantly associated with ear
infection particularly middle ear diseases. The study shown that exposed group has ten
more children affected by ear diseases due to tobacco smoke compared to non exposed
group
The scientific evidence indicates that there was no risk-free level of exposure to
secondhand smoke; children exposed to secondhand smoke were at an increased risk for
acute respiratory infections and ear problems. (Jones, 2012., Samet, et al 1994., Surgeon
General, 2007 and Wilson, 2010 ).
5.2 Exposing children to tobacco smoke and academic performance at school
Class participation, class position, average score, low mark performance, high mark
performance, general academic performance were tested on this study to determine
academic performance of respondents. Presence of teachers, availability of text books,
respondents class attending, availability of equipment for learning, enough time for
private study at home, how often you study per week, working toward assignment given
parents/guardians and community support were tested to analysis if rider to the
outcomes which as well can cause poor academic performance to children at school.

49
The studies sketch out in table 4.2, general academic performances of respondents were
compared between the past results scores and the present, the results shows high
numbers of pupils from non exposed group improved in academic performance, but few
numbers of exposed group improved academic performance however their academic
performance decreased as the number of tobacco smoking increased in their families.
This shows high number of smokers in family increases the effect to children exposed in
academic performance, the result showed thirty pupils from compared group improving
in academic performance, twenty decreasing, however twenty one from exposed group
were improving and thirty five become poor in academic.
Children exposures to involuntary tobacco smoking have strong adverse effects on
academic performance or behavior. Evidence from other studies conducted previously
shows that poor academic performance either as measured by school progress or by
achievement test scores in relation to paternal, maternal, or household smoking as
reported at the time of the follow-up during childhood (Eskenazi, 1999., Rantakallio, P.,
1983 and Byrd, 1994).
Pupils exposed to tobacco involuntary smoking decreased in academic performance in
second term than in the first term when they were not exposed to tobacco involuntary
smoking. Association of class performance and average became stronger than before,
Chi test shown 0.043 to 0.003 this implies that children exposure to involuntary smoking
has effects to pupil’s academic performance. First term result shown no F in pupils
average while second term result pupils who were exposed to involuntary smoke scored
F.
These were evidence how involuntary tobacco smoking decrease academic performance.
The postnatal ETS has been reported to be associated with decreased intellectual
capacity, behavioral problem and poor academic achievement (Cho, S.-C., 2010.,
Kremer, 2016., Melissa, 2008 Yolton, K., 2005).

50
Association between children exposed to tobacco smoking with academic average scores
for respondents. The results determine that compared group was performing better than
exposed group
Other study demonstrated these are, (Hofhuis, 2003). Pupils exposed to SHS at home
more likely, respectively, to report poor academic performance and reduced general
intellectual ability and attention deficit and hyperactivity disorder compared with pupils
who were not exposed to SHS (Ho, 2010., Anderko, et al 2010., Hermann, 2008 and
Kukla, 2008).

51
CHAPTER SIX
CONCLUSION, ADVICES AND RECOMMENDATION
6.0 Introduction
This chapter presents the research conclusion, advices and recommendation which
different peoples, societies, countries, worldwide, actors and research consumers should
work on. Conclusion, advices and recommendation can give chance for improvement
according to the changes occurs in society.
6.1 Conclusion
This study, involved two groups of pupils from Kikundi primary school. One was
exposed group from involuntary tobacco smoking by parents/guardians or any
member(s) of family smoking tobacco at home and the second group was none exposed
group, total numbers of all respondents were 120, The general objectives was to
determine health effects and academic performance of primary school children exposed
to tobacco smoke.
The study shown strong association between involuntary tobacco smoking and human
health effect (children), diseases observed were wheezing breathing, antisocial behavior,
attention deficit disorders, ears problem like middle diseases, nose fail sensing (sense of
smell), throat diseases and respiratory disease like nasal passages the bronchi.
The study also shows strong association between involuntary tobacco smoking and
academic performance. The results were observed on class participation, average score
and general academic performance in class.
The study supported the evidence that large numbers of children are still exposed to
involuntary tobacco smoking. The study shows poor association of health effects to
variables of life style and environmental factors, Variables observed were type of house,
number of sleeping rooms at home, population of the households, house located near to
tobacco farm, factory processing, solid waste mixed dumpsite, smoke drift at home from
factory processing tobacco, tobacco farm and solid waste mixed dumpsite, burning

52
mixed solid waste around home, use plastic to make fire like time of cooking, type of
fuel household mainly use for cooking, inherent diseases and using polished food.
Academic performance to children is related with availability of teaching materials in
school the study shows poor association. Variable observed were presence of teachers in
class involved in study, availability of text books, class attending, learning facilities,
time for private study, working toward assignment given, parents/guardians and
community support.
6.2 Advices
Parents/guardians or any member of family smoking tobacco should stop smoking
because is the best way to prevent children, not only at home and indoor, in car, public
place, public and private office, at school, resting place like beach and any place used to
expose human to tobacco smoke.
6.3 Recommendation
The study used case control this is one of the study perform worldwide. The study will
be used worldwide by its findings, results, conclusion, advices and recommendation. It
was limited by a small area; therefore it requires large area for further study. Issues of
cofounder were not addressed until far study. People must stop smoking to prevent
children from effects of involuntary tobacco smoking and most way to make them to
stop is education about effects of involuntary tobacco smoking, because this study shows
that even educated parent/guardians are exposing children to involuntary smoking.

53
REFERENCES
Anderko, L. et al. (Jan-Feb, 2010). Contribution of tobacco smoke exposure to learning
disabilities. Journal of obstetric, gynecologic & neonatal nursing, Volume 39
, Issue 1 , 111 – 117.
Acevedo-Estefania, C., Gonzalez, C., Soto, K.R., Eric, D., Summerville, E.D., Song, B
and Castillo-Chavez, C. (2000). A mathematical model for lung cancer, the
effects of secondhand smoke and education. BU-1525-M: 521-548.
Apelberg, B.J., Onicescu, G., Avila-Tang, E. and Samet, J.M. (2007). Estimating the
risks and benefits of nicotine replacement therapy for smoking cessation in
the United States. American Journal of Public Health.. 100(2): 341-348.
ASH (July, 2013). secondhand smoke: action on smoking and health. Fact Sheet on
secondhand smoke.
ASH (February, 2014). secondhand smoke: action on smoking and health. Fact Sheet on
secondhand smoke.
Australian Government Department of Health and Ageing. (26 Aug , 2011). The health
effects of secondhand smoke. Tobacco in Australia: Facts and Issues. Fourth
Edition.
Benninger, M. S. (December, 1999). The impact of cigarette smoking and environmental
tobacco smoke on nasal and sinus disease: A review of the literature.
American journal of Rhinology. Vl 13, No 6, pp. 435-438(4).
Boston University Pupil Health Services. (January, 2013). A sore throat often makes it
painful to swallow and feel dry and scratchy. Sore throats. overview of a sore
throat.
Byrd, S.R and Weitzman, L.M., (March, 1994). Predictors of early grade retention among
children in the united states. American academy volume 93 / issue 3.
Chen, Z and Li, N. (1986). The effect of passive smoking on children’s pulmonary
function in Shanghai. American Journal of Public Health. 76(5): 515-518.

54
Ciaccio, C. E and Gentile, D. (December,2013). Effects of tobacco smoke exposure in
childhood on atopic diseases, Curr allergy asthma rep.
Cho, S.-C., et al, (2010), Effect of environmental exposure to lead and tobacco smoke on
inattentive and hyperactive symptoms and neurocognitive performance in
children. Journal of Child Psychology and Psychiatry, 51: 1050–1057.
doi: 10.1111/j.1469-7610.2010.02250.x
Crothers, K., T. A., Griffith. et al. (2005). "The Impact of Cigarette Smoking on
Mortality, Quality of Life, and Comorbid Illness Among HIV-Positive
Veterans." J Gen Intern Med 20(12): 1142-1145.
Ehrlich, R.I., Du Toit D., Jordaan E. et al. (1996). “Risk factors for children hood
asthma and wheezing.” importance of maternal and household smoking. Am
J Respir Crit Care Med ;154:681–688.
Eskenazi, B and Castorina, R., (December 1999). Association of prenatal maternal or
postnatal child environmental tobacco smoke exposure and
neurodevelopmental and behavioral problems in children. Environmental
health perspectives Vl 107.
Eichborn, S.V and Abshagen, M.L. (2015). Tobcco:Antisocial, unfair, harmful to the
environment , tobacco production and consumtion as an example of the
complexity of sustainable development goals(SDGs).
Ezzati, M and Lopez, A.D. (2000). Estimates of global mortality attributable to smoking
in, Lancet. 2003; 362(9387):847–852. [PubMed: 13678970].
Fabry, D. A. et al. (April, 2011). Secondhand smoke exposure and the risk of hearing
loss, Tob Control. 20(1): 82–85.
Frank D., Gilliland., Yu-fen li. et al. (2001). “Effects of maternal smoking during
pregnancy andenvironmental tobacco smoke on asthma and wheezing in
children” American journal of respiratory and critical care medicine vol 163.

55
Grazuleviciene, R. et al (July, 20142014). The impact of tobacco smoke exposure on
wheezing and overweight in 4–6-year-old children, BioMed research
international. ID 240757, p8.
GreenFacts, (2002). Scientific Facts on Tobacco Active and Passive Smoking. Facts on
health and the environment.
Hannah, B., Jo Leonard-Bee, J., Ahmed, H. et al. (April, 2012). “Prenatal and passive
smoke exposure and incidence of asthma and wheeze.” systematic review and
meta-analysis. volume 129 / issue 4.
Hermann, M., King, K. and Weitzman, M. (Apr, 2008). Prenatal tobacco smoke and
postnatal secondhand smoke exposure and child neurodevelopment. Current
Opinion in Pediatrics. ;20(2):184-90. doi: 10.1097/MOP.0b013e3282f56165.
Hirschtick, R.E., Glassroth, J., Jordan, M.C et al (1995). Bacterial pneumonia in persons
infected with the human immunodeficiency virus: Pulmonary complications
of HIV Infection Study Group. New England Journal of Medicine, 845–85.
Hirayama, T. (1990). passive smoking and cancer, the association between husbands
smoking and cancer in the lung of non-smoking wives. Indoor air quality.
Bohseidai: Tokai university.
Hofhuis, W. et al. (2003). Adverse health effects of prenatal and postnatal tobacco
smoke exposure on children, arch dis child;88:1086–1090.
Ho, Sai-Yin et al. (December, 2010). Exposure to secondhand smoke and academic
performance in non-smoking adolescents. The Journal of Pediatrics, Volume
157 , Issue 6 , 1012 - 1017.e1
Hwang, S., Hwang, J.H., Moon, J.S., Lee, D.H. (February 14, 2012). Environmental
tobacco smoke and children's health. The Korean Pediatric Society. (2):35-41.

56
Jagoe, K and E.R. (2002). Tobacco smoking in Tanzania, East Africa: population based
smoking prevalence using expired alveolar carbon monoxide as a. Tobacco
control, 210-214.
Johnson N. (2001). Tobacco use and oral cancer: A global perspective. Journal of
Dental Education; 65 (4): 328–339.
Jones, L.L., Hashim, A.,, McKeever T., Cook, D.G., Britton, J., Leonardi-Bee, J. (2011).
Parental and household smoking and the increased risk of bronchitis,
bronchiolitis and other lower respiratory infections in infancy: systematic
review and meta-analysis.Respiratory Research. 12:5.
Jones L.L., (2012). Parental smoking and the risk of middle ear disease in children a
systematic review and meta-analysis. Archives of pediatrics & adolescent
medicine. Vol 166. No1>.
Kremer P.K, (Jun 08, 2016). Behavior problems and children's academic achievement, a
test of growth-curve models with gender and racial differences. Children and
Youth Services Review 67. Vl 95–104.
Kukla, L., Hruba, D. and Tyrlik, M. (Jun, 2008). Maternal smoking during pregnancy,
behavioral problems and school performances of their school-aged
children. Central european journal of public health;16(2):71–6.
Lynch,S. V. et al. (2014). Effects of early life exposure to allergens and bacteria on
recurrent wheeze and atopy in urban children, Allergy Clin Immunol. 134(3):
593–601.
Melissa, H. et al. (April 2008). Prenatal tobacco smoke and postnatal secondhand smoke
exposure and child neurodevelopment. Therapeutics and toxicology. Volume
20 - Issue 2- p 184–190. doi: 10.1097/MOP.0b013e3282f56165.
Murray, C.S., Woodcock, A., Smillie, F.I. et al. (2004). “Tobacco smoke exposure,
wheeze, and atopy” pediatric pulmonology 37;492-498.
Mbatia J and Gad Paul Kilonzo (1998). A handbook of educators in Tanzania
MEHATA Publication Pg46-55.
57
Sangar, N. (April, 2016). Tobacco smoking: Death, disease and potential health hazards.
Asian journal of multidisciplinary studies.Vl.4, 2348-7186.
Oberg, M., Jaakkola, M., Woodward, A., Peruga, A., Pruss-Ustun, A., (2011).
Worldwide burden of disease from exposure to second hand smoke: a
retrospective analysis of data from 192 countries, 139-46.
Reh, D. D. et al. (2012). Impact of tobacco smoke on chronic rhinosinusitis – a review
of the literature, Int forum Allergy Rhinol. 2(5): P 362–369.
Rantakallio, P., (1983), a follow-up study up to the age of 14 of children whose mothers
smoked during pregnancy. acta paediatrica, 72: 747–753. doi: 10.1111/j.1651-
2227.1983.tb09805.x
Report, A. R. (March 2014). Secondhand smoke: the impact on children. Health effects
of secondhand smoke.
Reynolds, K.L., Heckel, H.A., Witt, C.E., Martin, J.W., Pollard, J.A., Knapik, J.J and
Jones, B.H. (1994). Cigarette smoking, physical fitness, and injuries in
infantry soldiers. Am J Prev Med;10:145–50.
Riboli, E. A. E. ( 1990). Exposure of nonsmoking women to environmental tobacco
smoke: a 10-country collaborative study. Cancer Causes Control , 1:243 – 52.
Royal College of physicians. (2010). Passive smoking and children. A report of the
tobacco advisory group of the Royal College of Physicians. London: Royal
College of Physicians.
Samet, M.J et al. (1994). Involuntary smoking and children’s health. The future of
children critical health issues for children and youth vol. 4 • no. 3 – winter.
Sang Hyun Hwang,J.H.(2012). Environmental tobacco smoke and children’s health. The
Korean pediatric socity.

58
Saulyte , J. Regueira, C. Montes-Martı´, A. Khudyakov, P. Takkouche, B. (March
2014). Active or passive exposure to tobacco smoking and allergic rhinitis,
allergic dermatitis, and food allergy in adults and children: A Systematic
review and meta-analysis, PLOS medicine. Volume 11 | Issue 3 | e1001611.
Sindelar, J., Duchovny, N., Falba, T., Busch, S. (2005). If smoking increases absences,
does quitting reduce them? Tobacco Control, 14(2), 99–105.
http://doi.org/10.1136/tc.2003.005884
Surgeon General’s report, (2010). How tobacco smoke cause disease, report of the
Surgeon General. (Full port and its related materials
www.surgeongeneral.gov)
TDHS ( 2010). Percentage of men age 15-49 who smoke cigarettes or a pipe or use other
tobacco products and the percent distribution of cigarette smokers by number
ofcigarettes smoked in preceding 24 hours, according to background
characteristics.
Tsai, S., Wen, C., Hu, S,. Cheng, T and Huang, S. (2005). Workplace smoking related
absenteeism and productivity costs in Taiwan. Tobacco Control,14(Suppl 1),
i33–i37. http://doi.org/10.1136/tc.2003.005561
U.S. Surgeon General and Department of Health and Human Services (2010), how
tobacco smoke causes disease: the biology and behavioral basis for smoking
attributable disease: A report of the Surgeon General.
U.S. Department of health and human service, (2010). How tobacco smoke cause
disease, Centers of disease control and prevention, National centers for
chronic disease prevention and health promotion, office on smoking and
health. A report of the surgeon General how it affect children
U.S. Department of Health and Human Services (2014). Centers for disease control and
prevention, National Center for Chronic Disease Prevention and Health
Promotion, Office on Smoking and Health, 666.

59
U.S. Department of Health and Human Services. (1986). “The main effects of the
irritants present in ETS [environmental tobacco smoke] occur in the
conjunctiva of the eyes and the mucous membranes of the nose, throat, and
lower respiratory tract. These irritant effects are a frequent cause of
complaints about poor air quality due to environmental tobacco smoke.” (p.
252).
Wilson, K.M., et al. (December 13, 2010). Tobacco-smoke exposure in children who
live in multiunit housing. Pediatrics: American academy of pediatrics. Vl 127.
WMA (1964). "Ethical Principles for Medical Research Involving Human Subjects."
General Assembly, Helsinki, Finland, Declaration 18th Assembly(First
adoption).
WMA (1964). "Ethical Principles for Medical Research Involving Human Subjects."
General Assembly, Helsinki, Finland, Declaration 18th Assembly(First
adoption).
WHO. (July, 2002). Monographs on the evaluation of carcinogenic risks to humans
tobacco smoke and involuntary smoking. summary of data reported and
evaluation agency for research on cancer: volume 83.
World Health Organization (February 2010). Effects of passive smoking on Children,
Geneva.
World Health Organization (2007). Policy recommendations on protection from
exposure to second-hand tobacco smoke. policy recommendation WHO report
2007.
WHO (2013). recommendations for the prevention and management of tobacco use and
SHS exposure in pregnancy. Smoking prevention and control.
www.who.int/features/factfiles/tobacco/tobacco_facts/en/index5.html 5:38PM
Warren, C.W at el. (January 25, 2008). Global youth tobacco surveillance, 2000-2007.
Surveillance Summaries57(SS01);1-2.
Wakschlag, S.L. et al. (June 2002). Maternal Smoking During Pregnancy and Severe

60
Antisocial Behavior in Offspring. American Journal of Public Health. Vol
92, No. 6.
Yolton, K., et al. (January 2005). Exposure to environmental tobacco smoke and
cognitive abilities among u.s. children and adolescents. Children’s health
article, Volume 113 number.
61
APPENDICES
THE QUESTIONNAIRE FOR RESEARCH
MZUMBE UNIVERSITY (MU)
SOPAM
QUESTIONNAIRE FOR RESEARCH ON
HEALTH EFFECTS AND ACADEMIC PERFORMANCE ON PRIMARY SCHOOL
CHILDREN EXPOSED TO TOBACCO SMOKE AT HOME IN MOROGORO
MUNICIPAL.
BY
MASOTA P. JOHN
MASTER OF HEALTH SYSTEMS MANAGEMENT
My name is Masota P. John, I am a pupil at Mzumbe University pursuing ( MSc).
Master of Science in Health System Management. I am doing a study on health effects
and academic performance on primary school children exposed to tobacco smoke at
home in morogoro municipal Tanzania. As a compulsory part of my programme. The
aim of the research is to determine the adverse health effects of involuntary smoking to
children in relation to class academic performance, so as to help community to stop or
avoid effect from involuntary smoking. I would be very grateful if you would spare
some few minutes to fill in this questionnaire. The information that you give will be
treated confidential and your identity will not be exposed.
Instructions:
Please the answer you are going to select put its number in the box
provided at the end of row and write text to provided space where appropriate.
Name...………………………………………………………………………...………

62
1: Background characteristics of respondent
No Questions Response Options
Codes
1 What is your age?
…………………................................
2 What is your gender? 1. Male
2. Female
3 What is your class?
1. Class five
2. Class six
3. Class seven
4 Your friends are using to smoke at
your home place?
0. No
1. Yes
5 Your parent/guardians are smoking
tobacco?
0. No
1. Yes
6 How many numbers of the smokers at
home?
……………………………….
7 What is level of your parent/guardian
education?
Father……………………………………
8 What is level of your parent/guardian
education?
Mother…………………………………
9 Parent/guardian job? Father…….
10 Parent/guardian job? Mother……
11 Does your parent/guardian smoking
on your presence?
0. No
1. Yes
12 Number of the cigarettes smoked in
your presence?
………….……………………………….

63
2: Life style
13 What are types of house you live? 1.Home owner
2.Rent
3.Other
14 How many rooms for sleeping in
house?
1.One
2.Two
3.Three
4.More
15 What is the population of the
households?
……………………………………
16 Your house is located close to?
1. Tobacco factory
2.Tobacco farm
3.Solid mixed dumpsite
4.Burning plastic area
5.Not close
17 If yes how long kilometer? 1.Half
2.One
3.Two
4.Three
5.Not near
18 Smoke drift to your home from like
dumpsite, burning waste area and
tobacco farm and tobacco factory?
0.No
1. Yes
19 Are you burning waste plastic at
home?
0. No
1. Yes
20 Did you use plastic to make fire like
charcoal fuel?
0. No
1. Yes
21 Did you have any inherit born
diseases in your family?
0. No
1. Yes
22 What type of fuel does your 1.Gas

64
household mainly use for cooking? 2.Firewood
3.Electricity
4.Charcoal
5.Kerosene
23 Do you use polished food at home like
‘sembe’?
0. No
1. Yes
3: Among of factors to good academic performance to children
24 Do you have enough teachers for your class
subjects?
0. No
1. Yes
25 Do you have enough text books for studying? 0. No
1. Yes
26 Do you attending class every day as required? 0. No
1. Yes
27 Do you getting time for private study at home? 0. No
1. Yes
28 How often you study per week?
1.Once
2.Two
3.Three
4.Every day
5.No time
29 Parent/guardian make follow-up for your
academic performance at school?
0. No
1. Yes
30 Are you working toward home work
assignment given in class?
0. No
1. Yes

65
4: Human health effects of involuntary smoking to children exposed to tobacco
smoke
31 Do you have asthma? 0. No
1. Yes
32 Do you have Respiratory disease? 0. No
1. Yes
33 Do you have wheezing breath problem? 0. No
1. Yes
34 If yes, when? 1.Night
2.Day
3.Any time
4.Don’t have
35 Do you have attention deficit disorders?
0. No
1. Yes
36 Do you have heart disease? 0. No
1. Yes
37 Do you have ears problem?
0. No
1. Yes
38 Do you hear proper when teacher is teaching? 0. No
1. Yes
39 Your nose sensing is active? 0. No
1. Yes
40 Do you have throat problem? 0. No
1. Yes
41 What are you doing during the break time? 1.I like to be myself
2.Playing with other

66
5) Children academic performance at school
42 Class participation?
1.Very good
2.Good
3.Bad
4.Very bad
43 Which subject you like?
44 How do you see in general academic
performance?
1.Performance increasing
2.Performance decreasing
3.Performance Stagnant
45 By this age what do you like to do? 1.Study
2.Business
3.Enterprenuer
4.Other
6: Academic result about pupil average and position
No Children name Q =46
Average first
term
Q=47
Class
position
first term
Q=48
Average
End
term
Q=49
Class
position
1
2
3

67
Average in %
1. A (81-100) 2. B (61-80) 3. C (41-60)
4. D (31-40) 5. E (21-30) 6 .E (0-20)
What is your Suggestion?
…………………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………...
End and Thanks.

![The Effects of Fishing Activities on Attendance and Academic Performance of Primary and Junior High School Pupils.[1]](https://img.dokumen.tips/doc/110x75/55cf9e36550346d033b0750f/the-effects-of-fishing-activities-on-attendance-and-academic-performance-of.jpg)


























