Embed Size (px)
Citation preview

HEALTH DISPARITIES AFFECTING CHICANO/LATINO COMMUNITIES IN
MINNESOTA
A COMMUNITY-DRIVEN PARTICIPATORY PROCESS FOR IDENTIFYING HEALTH DISPARITY INDICATORS
Final Report
Written by:
José William Castellanos, MD
Andrés Flores Fioravanti Ingrid Anne Giles
Planning grant awarded to Chicanos Latinos Unidos en Servicio (CLUES) by Participatory Research Partnership / Urban Coalition / Allina Foundation
April 2004

i
Table of Contents
INDEX OF TABLES ......................................................................................................III
ABSTRACT....................................................................................................................... 1
INTRODUCTION............................................................................................................. 4
I. LITERATURE REVIEW AND HEALTH DISPARITIES INDICATORS INVENTORY .................................................................................................................... 9
LITERATURE REVIEW .................................................................................................................................. 9 HEALTH DISPARITIES INDICATORS INVENTORY ........................................................................................ 13
II. SURVEYS AND FOCUS GROUPS......................................................................... 18 SURVEY METHODOLOGY .......................................................................................................................... 19 FOCUS GROUPS METHODOLOGY ............................................................................................................... 20
Planning and Logistics ......................................................................................................................... 20 Recruitment of Participants.................................................................................................................. 21 Supporting Material ............................................................................................................................. 22 Technology ........................................................................................................................................... 22 Structure of the Group Discussion ....................................................................................................... 22 Moderation ........................................................................................................................................... 23 Structure ............................................................................................................................................... 23 Initiative................................................................................................................................................ 24 Participation......................................................................................................................................... 24
CONFIDENTIALITY..................................................................................................................................... 25 LIMITATIONS............................................................................................................................................. 25 DEMOGRAPHICS ........................................................................................................................................ 27
Community Based Organizations ......................................................................................................... 27 Health Care Providers.......................................................................................................................... 30 Faith Organizations.............................................................................................................................. 32 Focus Groups ....................................................................................................................................... 36
ANALYSIS OF FINDINGS, SURVEYS AND FOCUS GROUPS ........................................................................... 40 Community Based Organizations ......................................................................................................... 40 Health Care Providers.......................................................................................................................... 44 Faith Organizations.............................................................................................................................. 60 Focus Groups ....................................................................................................................................... 63
Mankato............................................................................................................................................ 63 Minneapolis ...................................................................................................................................... 75 St. Paul.............................................................................................................................................. 82
CONCLUSIONS ........................................................................................................................................... 90 Lack of Awareness................................................................................................................................ 92 Education.............................................................................................................................................. 93 Poverty.................................................................................................................................................. 94 Discrimination...................................................................................................................................... 95 Job Conditions...................................................................................................................................... 95 Health Insurance .................................................................................................................................. 96 Culture and Language.......................................................................................................................... 96 Weather ................................................................................................................................................ 97 Medical Model...................................................................................................................................... 97 Immigrant Status .................................................................................................................................. 97 Research ............................................................................................................................................... 98

ii
Access ................................................................................................................................................... 98 Offer of Health Care Services .............................................................................................................. 98 Morbidity and Mortality ....................................................................................................................... 99 Health Promotion and Disease Prevention .......................................................................................... 99
III. RECOMMENDATIONS....................................................................................... 100 EDUCATION............................................................................................................................................. 100 COMMUNICATION.................................................................................................................................... 101 HEALTH INSURANCE ............................................................................................................................... 102 COMMUNITY PARTICIPATION .................................................................................................................. 102 CULTURALLY COMPETENT HEALTH CARE SERVICES.............................................................................. 103 COMMUNITY BASED PARTICIPATORY RESEARCH ................................................................................... 103
APPENDICES............................................................................................................... 106 APPENDIX A: SURVEY INSTRUMENT ....................................................................................................... 107 APPENDIX B: LITERATURE REVIEW ........................................................................................................ 108

iii
Index of Tables Table 1, Key Words, 9 Table 2, Health Related Indicators, 13 Table 3, Ranking of Health Priority Areas of Hispanic Latino Population, 14 Table 4, Age Adjusted Mortality Rates Hispanic/White Population, 14 Table 5, Eliminating Health Disparities Initiative Measurable Outcomes, 16 Table 6, Health Care Provider Indicators, 17 Table 7, CBO Respondents, 27 Table 8, CBO Respondents Age Distribution in Years, 27 Table 9, CBO Respondents Country of Origin, 28 Table 10, CBO Respondents Years in the US, 28 Table 11, CBO Respondents Language Used, 28 Table 12, CBO Respondents Years Working with Latino Community, 29 Table 13, CBO Services, 29 Table 14, CBO Respondents Interested in Planning, 29 Table 15, HCP Respondents, 30 Table 16, HCP Respondents Age Distribution in Years, 30 Table 17, HCP Representatives Country of Origin, 30 Table 18, HCP Respondents Years in the US, 31 Table 19, HCP Respondents Language Used, 31 Table 20, HCP Respondents Years Working with Latino Community, 31 Table 21, HCP Respondents Other Services, 32 Table 22, HCP Respondents Interested, 32 Table 23, FO Respondents by Gender and Place, 33 Table 24, FO Respondents Average Age Distribution and Range, 33 Table 25, FO Respondents by Country of Origin, 34 Table 26, FO Respondents Average Years Living in the US, 34 Table 27, FO Respondents Language Used, 35 Table 28, FO Representatives Average Years Working with Latino Communities, 35 Table 29, FO Services Provided, 36 Table 30, FO Representatives Interested in the Planning Process, 36 Table 31, FG Participants by Gender, 37 Table 32, FG Participants Average Age Distribution and Range, 37 Table 33, FG Participants Country of Origin, 37 Table 34, FG Participants Average Years in the US and Range, 38 Table 35, FG Participants Language Used, 38 Table 36, FG Participants Average Years Working within Latino Community, 38 Table 37, FG Participants Leadership, 39

1
Abstract
“Health disparities affecting Chicano/Latino communities in Minnesota” is the beginning
of a community-driven participatory process for identifying intermediate indicators to
asses health disparities and monitor Minnesota's progress toward eliminating this major
health problem in minority communities.
Minnesota is a national leader in quality of life; its health care system is nationally and
internationally recognized for its innovations and developments. However, Minnesota’s
minority communities, particularly the Chicano/Latino community -the fastest growing
community in the state- suffer some of the worst health disparities in the US. Therefore,
the goal for this participatory research was to identify community based organizations
(CBO) interested in planning a participatory process for developing health disparities
indicators that make sense for the Chicano/Latino communities living in Minnesota, and
to help to monitor the improvements made in this area.
To accomplish the goal a three-stage process was developed. The first stage was a
literature review of the scientific publications on health disparities affecting
Chicano/Latino population and a comprehensive inventory of current indicators gathered
by organizations serving the Chicano/Latino communities in Minnesota; the second one
was the development of the survey “Health Disparities Affecting the Latino
Community;” and the last stage included three focus groups conducted in Mankato,
Minneapolis, and Saint Paul.
2
The literature review provided a better understanding of the scientific publications on
health disparities. Most of the articles are related to clinical issues; no publications were
found focusing on social indicators in the Chicano/Latino communities.
The “Health Disparities Affecting the Latino Community” survey was developed to
understand the meaning of “disparities” and its implications on the health disparities
affecting Minnesota’s Chicano/Latino population.
Thirty-one formal leaders responded to the survey; their answers and the results of the
twenty-two formal and informal Chicano/Latino leaders participating in three focus
groups in Mankato, Minneapolis, and Saint Paul provided the insights reflected in this
report.
“Disparities” has a broad meaning from unequal access to services to the lack of
Chicano/Latino community participation. It is a complex concept that could be difficult
to understand. It depends on the context in which it is used and it is reflected on the
disproportionate incidence of health disparities affecting the communities.
The study found that poverty, discrimination, job conditions, culture and language, and
immigrant status are the perceived causes of the lack of awareness, education, health
insurance, and access to health care, health promotion and prevention services. In
addition, the lack of health care services offered, lack of culturally competent and
linguistically appropriate programs available, lack of research, and the disease centered

3
medical model in a state that has extreme weather conditions that are a novelty especially
for a recent immigrants, are the main causes associated with health disparities affecting
the Chicano/Latino communities in Minnesota.
These health disparities are partially reflected on the morbidity and mortality indicators;
however, in order to better understand the roots of the problem and its current
implications to real people, families, and communities affected by these disparities, a
community based participatory approach is recommended.
Recognizing the real social dimensions of the problem is the first step to building
together, in a participatory manner, innovative solutions for the leader state in quality of
life in the US. A comprehensive strategy of education, communication, health insurance
coverage, culturally competent health care services, and community based participatory
research is part of the solutions proposed in this report.

4
Introduction
Minnesota is a world-leader in health care innovations and has been consistently
recognized as one of the states with the highest standards of quality of life in the USA.
Minnesota’s health care systems, insurance coverage, and access to health care providers
are on the top among the states and have been for a long time; morbidity and mortality in
Minnesota show a healthy community. However, when data are disaggregated by race
and ethnicity, there are major disparities affecting minorities.
According to the 2000 census, minorities account for about twelve percent of the five
million in Minnesota’s population; from the total, Chicano/Latino communities represent
about three percent.1 Although relatively few in numbers, Chicano/Latinos are the fastest
growing communities in the state, increasing 446 % since 1980’s census and 166% since
the 1990 census. 2 But as the “Eliminating Health Disparities Initiative” 2003 report to
the legislature stated, the disparities affecting minorities in some cases are the worst in
the US, and several of them tend to increase. 3
As a response, the Eliminating Health Disparities Initiative (EHDI) was created to reduce
disparities and improve the health of minorities in Minnesota. It was understood that
improving health status in minority communities is beneficial for all Minnesotans.
1 Census 2000. Current Population Survey. U.S. Department of Labor. Bureau of Labor Statistics. U.S. Department of Commerce Economics and Statistics Administration US Census Bureau. 2 Census 2000. Minnesota State Demographic Center. 3 Eliminating Health Disparities Initiative 2003 Report to the Legislature, Minnesota Department of Health.

5
As part of this effort, the Participatory Research Partnership (PRP) was formed as a
subcommittee of the Steering Committee for the Eliminating Health Disparities Initiative
(EHDI). This is a collaborative effort between community-based organizations (CBO),
community representatives, the University of Minnesota, the Minnesota Department of
Health (MDH), and the EHDI. Chicanos Latinos Unidos En Servicio (CLUES) is a CBO
founder member of the PRP committed to eliminating health disparities in fulfillment of
its mission to enhance the quality of life of Chicano/Latino communities in Minnesota
since 1982.
CLUES was granted to identify CBO interested in planning a Community-Driven
Participatory Process for identifying indicators related to health disparities in the
Chicano/Latino communities living in Minnesota. This is a major effort to address one of
the most important problems that minorities are facing today in the state. It involved a
great collaboration between Chicano/Latino CBO, faith organizations (FO),
Chicano/Latino health care providers (HCP), and community formal and informal
leaders.
It was understood by organization representatives and community leaders who
participated that this is the beginning of a journey that cannot be finished by working
isolated and alone. We learn that the historical factors that have contributed to the current
reality must be addressed in a participatory manner in collaboration with the community-
based organizations, communities, formal and informal leaders, and the state.

6
The state has the resources and the technology to address most of the health disparities
affecting the Chicano/Latino communities; however, the lack of expertise and
partnerships with community based organizations and community leaders made the effort
insufficient, expensive, and time consuming. Today, there is an opportunity to work
together in a common goal that will result in tangible benefits for the people that need
them the most.
This report is the result of an active collaboration of more than fifty leaders who
discussed and examined, in a very participatory manner, people’s feelings, beliefs, ideas,
ideals, fears, and perspectives about “disparities” to better understand the reality of
“health disparities” affecting the Chicano/Latino individuals, families, and communities
in Minnesota.
Discussing “health disparities” in a safe environment in a candid manner with experts and
community leaders provided invaluable information useful for developing strategies,
programs, and research that will help bridge this vital gap. Without their participation it
would not have been possible to achieve the goal of better understanding disparities and
its implications on health disparities affecting the Chicano/Latino communities in
Minnesota. We would like to express our gratitude to all the organizations and
community leaders that answered the survey, participated in the focus groups, and
collaborated in this community-based participatory research.

7
The intent was to illustrate the complex process to understand “disparities” affecting the
Chicano/Latino communities from a community perspective. The literature review and
the indicators inventory were an important input to know the trend in peer review
publications and the health indicators currently used in Minnesota.
It was no surprise that the larger percentage of the publications is focused on clinical
issues, mortality, and most of them on morbidity. Very few were looking for the causes
and none for the solutions.
To identify the profound origin of the health disparities in Minnesota’s fastest growing
minority, the survey “Health Disparities Affecting the Latino Community” was
developed. The perspective of diverse representatives of CBO, FO, and HCP serving the
Chicano/Latino communities around the state was complemented with the focus groups
conducted in Minneapolis, St. Paul and Mankato.
The health disparities were described from a people’s perspective in a unique way that
permitted one to sense their feelings and emotions, their hopes and their frustrations; that
we believe, are the same feelings, emotions and frustrations that affect any person in
similar circumstances.
The results obtained are consistent with previous research4,5 and will help to find new
avenues to bridge the gap on the current knowledge. This participatory approach creates
4 Smaida. S. A, et al. Disparities in Health Access: Voices from Minnesota’s Latino Communities, HACER. 2002.

8
new opportunities to implement solutions that reach the communities that need them the
most. Individuals and organizations included in this initial phase of the community based
participatory research are willing to continue participating in further research, and most
important, they want to be part of the solutions.
The recommendations presented in this report emphasized the social side of the problem.
People, family, and community contributions are essential for the success in eliminating
health disparities. The clinical indicators will show the progress made; however, the
community participation is critical to make this improvement a reality in Minnesota.
5 Ulrich, E. M. Public Health and Health Care Access: Minnesota’s Latino Community. Report of the Minnesota Chicano/Latino/Hispanic Health Care Access Project.

9
I. Literature Review and Health Disparities Indicators Inventory
a. Literature Review
The literature review included a comprehensive Medline® search of articles published
from 1966 to 2003 related to health disparities affecting Chicano/Latino communities.
The key words used were the following:
Table 1 Medline® Key words
Medline® Key words Results 1. exp Minority Groups/ or exp Health Services Accessibility/ or exp Health Status/ or exp United States/ or health disparities.mp. or exp Health Promotion/ or exp Hypertension/ or exp Cardiovascular Diseases/ or exp Health Priorities/ or exp Racial Stocks/ or exp Ethnic Groups/
644656
2. exp Hispanic Americans/ or exp Culture/ 24893 3. 1 and 2 12167 4. limit 3 to ovid full text available 1386 5. exp "OUTCOME ASSESSMENT (HEALTH CARE)"/ or outcomes.mp. 213437 6. 5 and 4 99 7. 5 and 3 782
Seven hundred seventy-two abstracts were reviewed (please see Appendix B), of which
one hundred forty-four dealt with racial or ethnic health disparities among the
Hispanic/Latino community in the United States. Those articles covered a variety of
different types of disparities, as described below.
The type of disparity that was covered by the most articles was miscommunication
between physician and patient, due to cultural misunderstanding. A couple of those
articles had to do with recruiting and training minorities to work in health care. Most had
to do with cultural competency training for health care workers. Topics included why
such training is important, what it should include, and how it can be done, as well as
some suggestions for how to make the health care workers aware of their need for

10
cultural competence. (45 articles) There were a few articles about research. These
included the necessity of taking race or culture into account in research, as well as the
issue of recruiting participants. (7 articles)
Many articles were related to diabetes. These articles focused on such topics as
predictors of disease management in Latino and mainstream cultures, whether glycemic
control is related more to socioeconomic status or to ethnicity, and higher incidences of
amputation among Hispanics. (13 articles)
There were a few articles about ethnic differences in cancer survivorship or quality of life
among survivors. (12 articles)
There were also articles on mental health issues. Most of these were related to how
acculturation and ethnic identity relate to mental health treatment outcomes. One article
found that the recommended dose of a psychotropic medication might be different for
Hispanic than for mainstream population. Another had to do with the relationship
between perceived discrimination and depression, and another with how factors such as
race can affect physician awareness of mental health problems. (10 articles)
Some articles had to do with insurance. These included reaching out to the uninsured,
consequences of un-insurance, and racial and ethnic differences in health insurance
coverage. (5 articles) Other articles had to do with access barriers in general. (4 articles)

11
Several articles were related to asthma among Latino families, dealing with changing the
home environment, reducing disparities related to research, and elevated asthma
morbidity among Puerto Rican children. (8 articles)
A few articles were related to cardiovascular health. There are some racial differences in
cardiovascular care and outcomes. Although there are some disparities in treatment,
Hispanics are more likely to survive myocardial infarction than whites are. (6 articles)
Some articles talked about the paradox of better than expected health and mortality for
most Hispanic groups despite low socioeconomic status. This relates especially to issues
such as infant mortality and birth weights. (5 articles)
A small number of articles dealt with substance abuse prevention and treatment, and the
importance of people seeing their own culture represented in the message. (5 articles)
Some articles had to do with kidney health: hemodialisis survival and quality of life of
survivors, effects of certain drugs on minority transplant recipients. (4 articles)
Other articles had to do with a miscellany of health disparities, including overdose
mortality trends, outcomes of gestational hypertension treatment, institutional and
individual racial discrimination, insurance issues, nutritional outcomes, occupational
risks, higher risk for caries, use of poison control centers, HIV survival, childhood
leukemia, effects of race and ethnicity on outcomes in arthritis, use of dental care or
12
benefits, and tendency toward obesity. (18 articles) One article detailed some public
health care issues for Central Americans living in Houston, including disproportionate
amounts of care for STD’s and small amounts for chronic illness or mental health
problems.
Another article was a review of the available data on the health of the Latino population
in North Carolina. It included several specific disparities, including the following: high
death rates from motor vehicle injuries and homicide, less likelihood than other groups to
have health insurance, much higher pregnancy rates both for teens and older women,
more likely to begin prenatal care late or have no prenatal care, rates of sexually
transmitted disease higher than for whites but lower than for African-Americans, more
likely to initiate breastfeeding, higher rate of neural tube defects, less likely to take folic
acid every day before pregnancy, and lowest rates of low birth weight and infant
mortality despite other risks (possibly due to lower rates of smoking during pregnancy).
The article stated that “these findings may provide a basis for designing more effective
health improvement programs for the Latino population of North Carolina.”

13
b. Health Disparities Indicators Inventory
The inventory of current indicators gathered by the Minnesota Department of Health and
a community based health care provider serving the Chicano/Latino Communities in
Minnesota is described as follows.
From the Eliminating Health Disparities Initiative 2003 report to the legislature, the
health indicators with higher incidence among the Chicano/Latino communities are the
following:
Table 2 Health related indicators6
Birth Related Indicators o Low Birth Weight o Premature Birth o Growth restrictions Prior to Birth · Infant Mortality o Prior to First Birthday · Prenatal Care o Intensive Prenatal Care o Adequate Prenatal Care · Teen Birth Rates · Cancer o Breast cancer o Cervical cancer Injury and Violence · Homicidal cut/pierce injuries o Adults · Unintentional Fires o Under 9 years old · Firearm Homicides o All ages · Firearm Suicides o All Ages Rates of Uninsured
6 SOURCE: Eliminating Health Disparities Initiative 2003 Report to the Legislature. Appendix B. Pages 1 – 12.
14
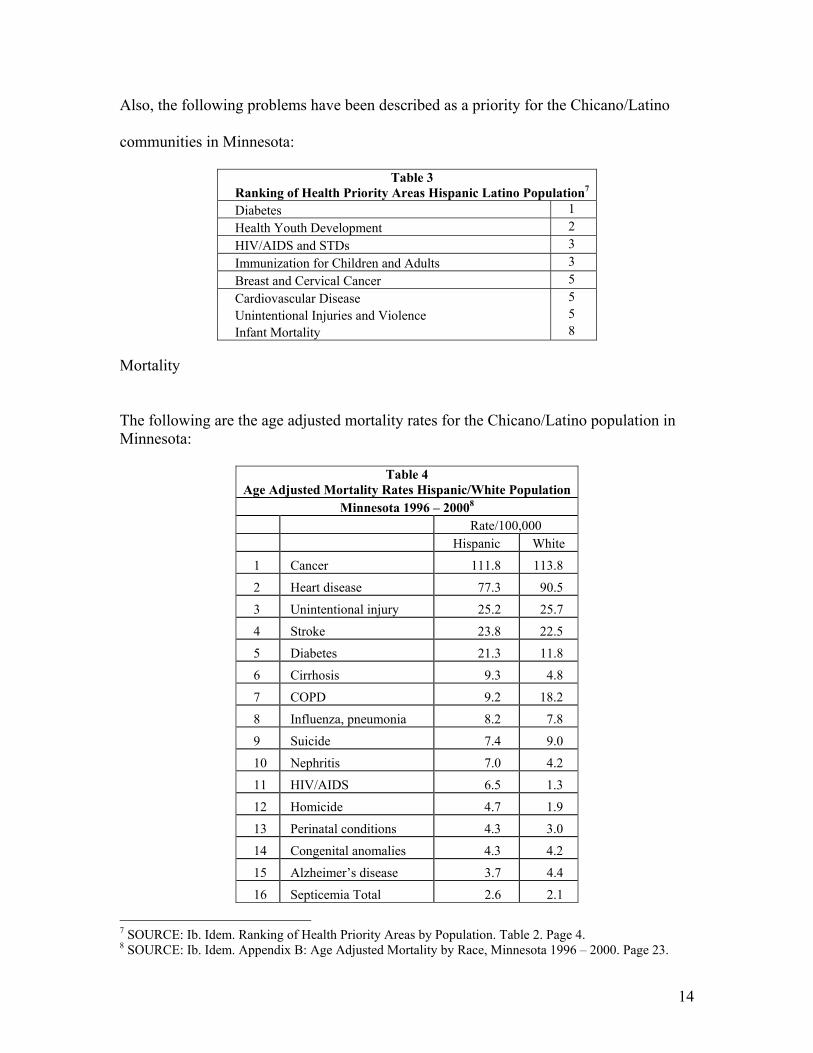
Also, the following problems have been described as a priority for the Chicano/Latino
communities in Minnesota:
Table 3 Ranking of Health Priority Areas Hispanic Latino Population7 Diabetes 1 Health Youth Development 2 HIV/AIDS and STDs 3 Immunization for Children and Adults 3 Breast and Cervical Cancer 5 Cardiovascular Disease 5 Unintentional Injuries and Violence 5 Infant Mortality 8
Mortality
The following are the age adjusted mortality rates for the Chicano/Latino population in Minnesota:
Table 4 Age Adjusted Mortality Rates Hispanic/White Population
Minnesota 1996 – 20008 Rate/100,000 Hispanic White
1 Cancer 111.8 113.8
2 Heart disease 77.3 90.5
3 Unintentional injury 25.2 25.7
4 Stroke 23.8 22.5
5 Diabetes 21.3 11.8
6 Cirrhosis 9.3 4.8
7 COPD 9.2 18.2
8 Influenza, pneumonia 8.2 7.8
9 Suicide 7.4 9.0
10 Nephritis 7.0 4.2
11 HIV/AIDS 6.5 1.3
12 Homicide 4.7 1.9
13 Perinatal conditions 4.3 3.0
14 Congenital anomalies 4.3 4.2
15 Alzheimer’s disease 3.7 4.4
16 Septicemia Total 2.6 2.1
7 SOURCE: Ib. Idem. Ranking of Health Priority Areas by Population. Table 2. Page 4. 8 SOURCE: Ib. Idem. Appendix B: Age Adjusted Mortality by Race, Minnesota 1996 – 2000. Page 23.

15
As a result of the high incidence and prevalence of the listed health problems, the
following programs have been developed by the Minnesota Department of Health
targeting Chicano/Latino communities:
• Diabetes
• Healthy Youth Development
• HIV/AIDS and Sexually Transmitted Infections
• Adult and Child Immunization
• Breast And Cervical Cancer
• Cardiovascular Disease
• Accidental Injuries and Violence

16
Eliminating Health Disparities Initiative has developed the following outcomes:
9 SOURCE: Ib. idem. Appendix F: Measurable Outcomes. Table 5. Page 50.
Table 5 Eliminating Health Disparities Initiative
Measurable Outcomes9
Long Term Measurable Outcomes1 Decrease by 50%, the disparity in Infant mortality rates among targeted populations. Decrease by 50%, disparities in the immunization rates of children from targeted groups (% up-to-date for 4 doses of DTP, 3 doses polio, 1 dose MMR vaccine at 24 months) Decrease by 50%, disparities in immunization rates of adults from targeted groups (influenza and pneumococcal disease.) Decrease breast and cervical cancer mortality rates among targeted populations. Decrease the incidence and prevalence rates for gonorrhea, chlamydia, syphilis, and HIV infections between targeted groups and the white population Decrease the age adjusted CVD, heart disease, and cerebrovascular death rates among targeted groups. Increase the proportion of persons with diabetes who have an Annual lipid and HbA1c measurement Decrease the disparities in teen pregnancy rates and subsequent births to women in targeted groups. Decrease the rates of deaths due to unintentional injury, suicide, homicide, and motor vehicle accidents in targeted populations Intermediate (e.g.) 2 Health Behaviors Health System Tobacco Use Health Care Coverage Alcohol Use Cultural Competency Physical Activity Clinic Hours Community Assets Environmental Factors Social Support Childhood Poverty Accessible clinics Affordable Housing Program Level (e.g.)3 Schools in the district who use WOLF diabetes curriculum Home visiting assessment and referrals of women and infants These measures identify long-term outcomes for the initiative. They have been identified primarily through the technical expertise of state and national consultants and are the traditional measures related to the eight health priority areas for the EHDI. With the exception of the measure for diabetes, data is available from MDH vital records and public health surveillance systems. These outcomes measure the impact on the overall health priority area and, as such, tend to be long-term indicating change in the health status of a population (frequently described in terms of morbidity or mortality, e.g. infant mortality rates). 2 Intermediate outcomes can have an effect on the desired long-term outcome. These outcomes are monitored in shorter time frames and are clearly focused on measures which have a high probability of reducing a health problem or increasing individual and/or community resiliency/capacity (e.g. Prenatal Quality of Care Index.) 3 Short term, process or program-level outcomes are measures of the effect of an intervention. They detail the specific tasks that will be carried out by the EHDI grantees. Process outcomes measure the effectiveness of the EHDI grantee intervention or strategy (e.g. number of women who attend prenatal care classes.)

17
Chicano/Latino Health Care Provider Indicators
From a Chicano/Latino community based health care provider, the following indicators
have been developed to measure health disparities affecting the Chicano/Latino
communities:
Table 6 Health Care Provider Indicators · Poverty · Un-insurance
Adults Children
· Insurance Access · Use of Public Hospitals · Use of Emergency Room · Health Status in Rural and Urban · Direct Care in Rural and Urban · English Fluency (patient) · Preventive Care · Welfare · Quality and Service · Financial issues

18
II. Surveys and Focus Groups
The aim of the Latino community-driven participatory process for identifying indicators
related to health disparities was to identify Community Based Organizations (CBO),
Community Based Health Care Providers (HCP), Faith Organizations (FO), and formal
and informal Latino community leaders interested in participating in the development of
intermediate indicators of health disparities affecting the Latino communities of
Minnesota.
To accomplish this goal, the survey “Health Disparities Affecting the Latino
Community” was developed and mailed to seventy CBO and HCP; seven were returned
because of incorrect address and re-mailed. Eleven responses arrived in the mail between
November 18th and February 29th 2004.
Fifty-nine calls were attempted, sixteen of those calls were answered by actual people
and five of those calls resulted in interviews. One interview was completed face-to-face.
In total, 17 survey responses were logged. Eight were from community health care
providers (HCP) and nine from other community-based organizations.
Fourteen interviews were performed with faith organization representatives working with
Latino communities around the state. Three interviews, all in the Metropolitan area, were
completed face-to-face and the other eleven were done by telephone.

19
The information collected through the surveys and the semi-structured interviews was the
basis for the focus groups discussion. A total of three focus groups were conducted, in
Minneapolis on December 15th, St. Paul on December 16th, and Mankato on December
20th.
a. Survey Methodology
The survey instrument is comprised of two parts. The first one includes socio-
demographic questions to characterize the respondents (Questions 1 to 7); the second part
of the instrument was developed to understand what “disparities” means to the
respondents in order to develop a culturally meaningful construct for the Latino
communities living in Minnesota.
An important part of the process was exploring whether the Latino communities were
aware of the impact of these health disparities on their families and communities. Also, a
necessary stage for the success of the planning process was researching the people’s
descriptions of health disparities and their ideas and opinions about the causes of the
disparities.
Finally, respondents were asked for solutions to eliminate health disparities, and how to
engage organizations, families, and individuals in identifying indicators that make sense
to the communities, to monitor the progress toward eliminating health disparities
affecting Chicanos/Latinos in Minnesota.

20
A first draft of the survey was developed by the research team at CLUES; it was tested
and emailed to the PRP partners. The suggestions and recommendations were included in
the final instrument. (Please see appendix A)
The survey and the answers were used to develop the guide for the focus groups
conducted in urban and rural settings in December 2004.
b. Focus Groups Methodology
The focus group methodology was primary based on “The Power of Focus Groups”10 by
Janet Mancini Billson, Ph. D. The project coordinator was certified in “Conducting
Professional Focus Group Research” workshops, in 2002. Also, the coordinator brings
experience from facilitating focus groups with the Latino community at Chicanos Latinos
Unidos En Servicio (CLUES), and Hispanic Advocacy and Community Empowerment
through Research (HACER).
i. Planning and Logistics
The focus groups had an estimated time frame of at least one hour and a half to two
hours. Normally, time was allowed in which to explain again what the activity is about
and how it will be facilitated. The first fifteen to twenty minutes were dedicated to
10 Billson, J. M. “The power of Focus Groups: A Training Manual for Social and Policy Research” Second edition. Skywood Press. Rhode Island. 2002.

21
answering questions and explaining any liability of confidentiality assurance to the
participants, with a written document.
ii. Recruitment of Participants
Recruitment was done in three geographical locations in the state, two in the Metro area
and one in Greater Minnesota by Chicanos Latino Unidos En Servicio (CLUES) staff.
Formal and informal Chicano/Latino leaders were contacted at each location. A total of
eight people, four men and four women, were included in each group; with the exception
of Minneapolis, in which five women and one man were included. The country of origin
and the time lived in Minnesota were some of the characteristics taken into account for
the selection of participants.
The participants received incentives for their participation. Each participant received a
$50 gift certificate from retail stores, or $50 cash; refreshments and some snacks also
were provided. Daycare was available in Minneapolis. However, the participants
expressed that the most important incentive for them was the opportunity to participate in
an activity that would benefit their communities.
Each location offered a friendly, comfortable, familiar, and safe environment to perform
this activity. In all three locations, we chose CLUES facilities.

22
iii. Supporting Materials
We utilized a written guide and the demographic questions of the survey. The material
was translated into Spanish by the facilitator.
iv. Technology
The facilitator used a tape recording system to audiotape the response from the focus
groups. He also used the assistance of a second person on two occasions to take notes;
otherwise the facilitator took notes himself. The tape was used for the written report of
each focus group in word 2000. The demographic data were entered in Microsoft Excel
2000, and the notes were transcribed in Microsoft Word 2000.
v. Structure of the Group Discussion
The group discussion basically followed a sequence showed in most focus group
performances. The following was covered:
• Moderator’s Opening Statement
• Ice-Breaking
• Main Body of Group Discussion
• Closure

23
This structure followed the guidelines in chapter five of “The Power of Focus Groups”
training manual by Billson.
vi. Moderation
The facilitator used the “Norm of Even Participation” mentioned by Billson in the
training manual.
vii. Structure
The group had a simple system in which the moderator was carefully mentioning each
topic after allowing each participant to freely participate with their thoughts, ideas, and
experiences. There was no a specific order; instead it was left to the participants’
initiative to begin talking. Every time the topic was obstructed by other topics, the
moderator carefully brought back the attention that allowed the group to obtain an
optimal discussion.
It was also important to create the best atmosphere where the participant felt secure and
open to express any thought that they wanted to mention. The moderator at the beginning
of the activity provided a brief explanation and answered concerns of confidentiality
issues. Overall the group was active and content with the purpose of this activity.

24
viii. Initiative
In each group the authenticity of each participant expressing their answers to others was
well projected at a good level as the facilitation was taking place. There was a better
expression after the first half hour after the focus group started. That is understandable
because the participants at that point had more confidence to exercise in the group.
ix. Participation
All groups presented different situations that challenged to some degree the even
participation possible. It was the moderator’s responsibility to make the pauses or
necessary comments to allow a better flow of input from the participants. In most groups
there were three to four people leading the conversation of the group. An explanation led
to this action to the leaders. Therefore in most cases, these leaders allowed others to
speak before them in order to listen to their contributions to the discussion.
The facilitator showed a lot of flexibility to the participants without damaging the
activity. The activity was an educational experience for the participants, as they
commented and to the facilitator as well.

25
c. Confidentiality
All the survey respondents and the focus groups’ participants were informed about the
voluntary nature of their participation. Permission to tape the session was formally
requested and granted by each one of the focus groups participants. Also, the confidential
statement was read and accepted by each participant.
They were told about the anonymity of the information and the secure issues to prevent
their identification. Only the moderator knows participant identities and it is not possible
to identify respondents in any way in this report.
d. Limitations
Important limitations of this study are the following:
Participants were not randomly sampled according to the diversity of the Chicano/Latino
communities in Minnesota; this is a significant limitation to generalize the findings of
this study. However, the participants’ deep understanding of the communities
significantly reduces this limitation.

26
The lack of awareness about health disparities limits the scope of the research. However
the same issue provided a good opportunity to explore in a most comprehensive way the
social origin and the community context in which health disparities make sense for the
Chicano/Latino communities.

27
e. Demographics
The following is the description of the data from the demographic questionnaire of the
survey answered by the community based organizations, the community based health
care providers, the faith organizations representatives, and by the focus groups
participants.
i. Community Based Organizations (CBO)
Nine CBO representatives responded the survey including four females and five males.
Six respondents answered the survey by mail (4 females, 2 males) and three males
answered by phone. Their average age was 40 years (range 28 to 52 years), 36 years for
females (range 32 to 42 years), and 43 years for males (range 28 to 52 years). One CBO
representative was from Greater Minnesota.
Table 7 CBO Respondents
Gender Female Male TotalMail 4 2 6 Phone 0 3 3 Face to face 0 0 0 Total 4 5 9
Table 8 CBO Respondents
Age Distribution in Years Gender Average Range Female 36 32 – 42 Male 43 28 – 52 Total 40 28 – 52

28
Respondents were from 5 countries including the US; many of them (4) did not answer
this question. Females were from Colombia and the US; males were from Bolivia,
Guatemala, and Mexico.
The average time living in the US reported by the CBO representatives was 25 years,
with a large range between 5 and 46 years.
Table 10 CBO Respondents
Years in the US Gender Average RangeFemale 26 8 – 38Male 24 5 – 46Total 25 5 – 46
Most of the respondents usually speak with their friends and relatives equally in Spanish
and English or mostly English; only one male speaks mostly Spanish.
Table 11 CBO Respondents
Language Used Female Male TotalOnly Spanish - - - Mostly Spanish - 1 1 Equal 2 2 4 Mostly English 2 2 4 Only English - - - Total 4 5 9
Table 9 CBO Respondents Country of Origin
Female Male TotalBolivia 1 1 Colombia 1 1 Guatemala 1 1 Mexico 1 1 USA 1 1 N/A 3 1 4 Total 5 4 9

29
In average the CBO representatives have been working nine years with Latino
communities; females have a larger average, 13 years, compared with males, 6 years. The
range varies from 4 to 24 years.
Table 12 CBO Respondents
Years Working with Latino CommunitiesGender Average Range Female 13 5 – 24 Male 6 4 – 10 Total 9 4 – 24
Most of the CBO provide education (7) and justice (2) services; it is important to mention
that each CBO provides more than one service to the Latino communities. The following
are the services provide by the CBO:
Table 13 CBO Services
Female Male Total Education 4 3 7 Justice 2 - 2 Health care - - - Social services - 1 1 Media - 1 1 Faith 1 - 1 Government 1 1 Other Leadership dev 1 1
Four CBO representatives are interested in participating in a participatory planning
process for refining and expanding the list of intermediate outcomes of health disparities
affecting Chicano/Latinos in Minnesota.
Table 14 CBO Respondents
Interested in Planning Yes No TotalFemale 0 5 5 Male 4 0 4 Total 4 5 9

30
ii. Health Care Providers (HCP)
Eight HCP representatives were interviewed including five females and three males. Five
respondents answered the survey by mail (2 females, 3 males), two females answered by
phone, and one female was interviewed face to face. Their average age was 44 years
(range 35 to 54 years), 44 years for females (range 35 to 50 years), and 42 years for males
(range 36 to 54 years). One of the HCP respondents was from Greater Minnesota.
Table 15 HCP Respondents Female Male Total
Mail 2 3 5 Phone 2 0 2 Face to face 1 0 1 Total 5 3 8
Table 16
HCP Respondents Age Distribution in Years
Gender Average Range Female 44 35 - 50 Male 42 36 - 54 Total 44 35 - 54
HCP representatives were from 4 countries including the US; most of them were from the
US (2 females and 2 males); one female did not answer this question. Females were also
from Mexico and Puerto Rico; one male was from Venezuela.
Table 17 HCP Representatives
Country of Origin Female Male TotalMexico 1 1 Puerto Rico 1 1 USA 2 2 4 Venezuela 1 1 N/A 1 1 Total 5 3 8

31
The HCP representatives reported an average of was 31 years living in the US, with a
range between 7 and 54 years.
Table 18 HCP Respondents
Years in the US Average RangeFemale 29 8 - 50Male 33 7 – 54Total 31 7 – 54
Most of the HCP respondents usually speak with their friends and relatives mostly in
English (1 female, 2 males), or only English (1 female, 1 male); two females speak
mostly Spanish.
Table 19 HCP Respondents
Language Used Female Male TotalOnly Spanish - - - Mostly Spanish 2 2 Equal 1 1 Mostly English 1 2 3 Only English 1 1 2 Total 5 3 8
HCP representatives have been working with Latino communities an average of sixteen
years; females 15 years and males 16 years. The range varies from 5 to 34 years.
Table 20 HCP Respondents
Years Working with Latino Communities Average Range Female 15 5 - 25 Male 16 5 - 34 Total 16 5 - 34

32
In addition to health care services the HCP respondents indicated that their organizations
provide other services like education, social services, and justice. The following are the
services provided by the HCP:
Table 21 HCP Respondents Other Services
Female Male TotalHealth care 5 3 8 Education 2 3 5 Social services 3 2 5 Justice 2 2 4 Government 1 1 2 Other Domestic/Sexual Violence 1 1 Policy and Advocacy 1 1
Three HCP respondents are interested in participating in a participatory planning process
for refining and expanding the list of intermediate outcomes of health disparities affecting
Chicano/Latinos in Minnesota; one may be interested.
Table 22 HCP Respondents
Interested Yes No Maybe N/A TotalFemale 1 2 1 1 5 Male 2 1 0 0 3 Total 3 3 1 1 8
iii. Faith Organizations (FO)
Fourteen FO representatives responded the survey, eight females and six males. Six
respondents were from the Greater Minnesota (four females and two men); eight
respondents were from the Metropolitan Area (four females and four males). Three
representatives were interviewed face-to-face (one woman and two men in the Metro

33
area) and eleven were interviewed by phone (seven females and four males). The average
age was 45 years (range 21 to 63 years), 41 years for females (range 21 to 51 years), and
49 years for males (range 40 to 63 years); the average age for the Greater Minnesota area
respondents was 44 years (range 21 to 63 years) and for the Metro area it was 46 years
(range 35 to 54 years). The average age for females in the Greater Minnesota area was 39
years (range 21 to 51 years) and 44 years in the Metro area (range 35 to 51); for males the
average age in the Greater Minnesota area was 52 years (range 41 to 63 years), and 47
years in the Metro area (range 40 to 54 years).
Table 23 FO Respondents by Gender and PlaceLocation Female Male TotalMetro Area 4 4 8 Greater 4 2 6 Total 8 6 14
Table 24 FO Respondents Average Age Distribution and Range in Years
Location Female Male Total Average Range Average Range Average Range Metro Area 44 35-51 47 40-54 46 35-54 Greater MN 39 21-51 52 41-63 44 21-63 Total 41 21-51 49 40-63 45 21-63
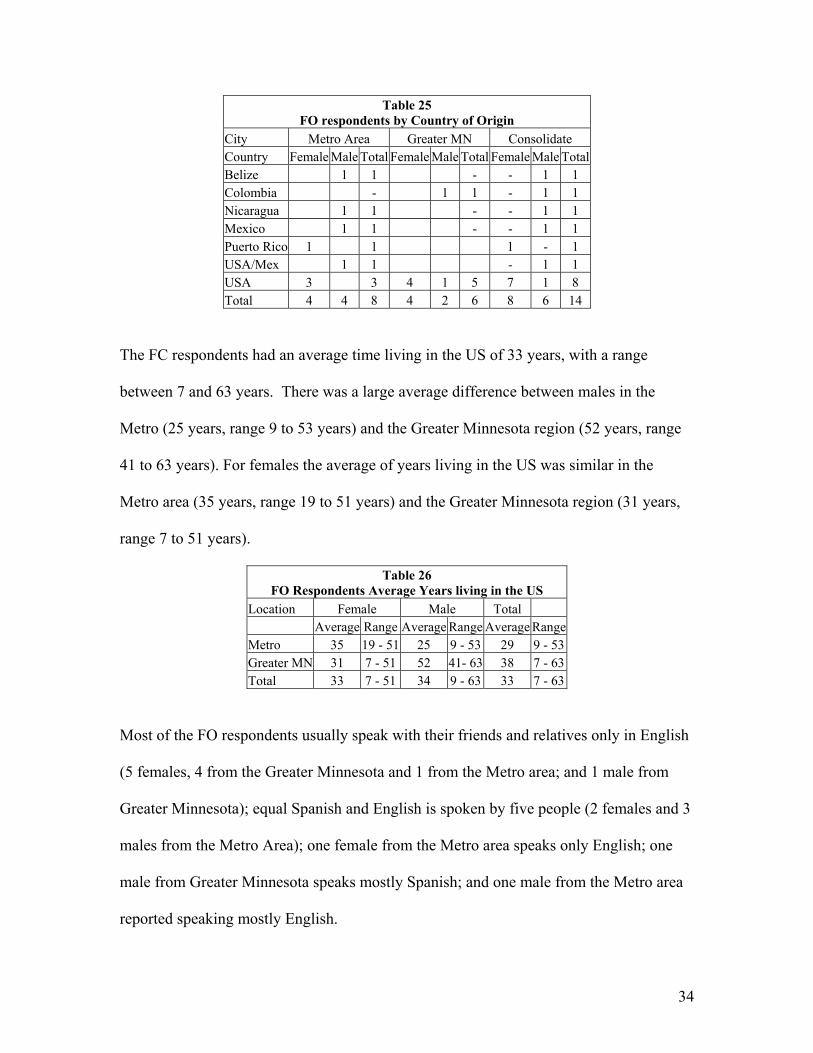
Respondents were from six countries including the US; Nine were from the US (7
females, 3 from the Metro area and 4 from the Greater Minnesota region; one male from
Greater Minnesota and one male in the Metro area from Mexican descent); one female
was also from Puerto Rico; males in the Greater Minnesota region were from Belize,
Nicaragua, and Mexico; and one male in the Metro Area was from Colombia.
34
Table 25 FO respondents by Country of Origin
City Metro Area Greater MN Consolidate Country Female Male Total Female Male Total Female Male Total Belize 1 1 - - 1 1 Colombia - 1 1 - 1 1 Nicaragua 1 1 - - 1 1 Mexico 1 1 - - 1 1 Puerto Rico 1 1 1 - 1 USA/Mex 1 1 - 1 1 USA 3 3 4 1 5 7 1 8 Total 4 4 8 4 2 6 8 6 14
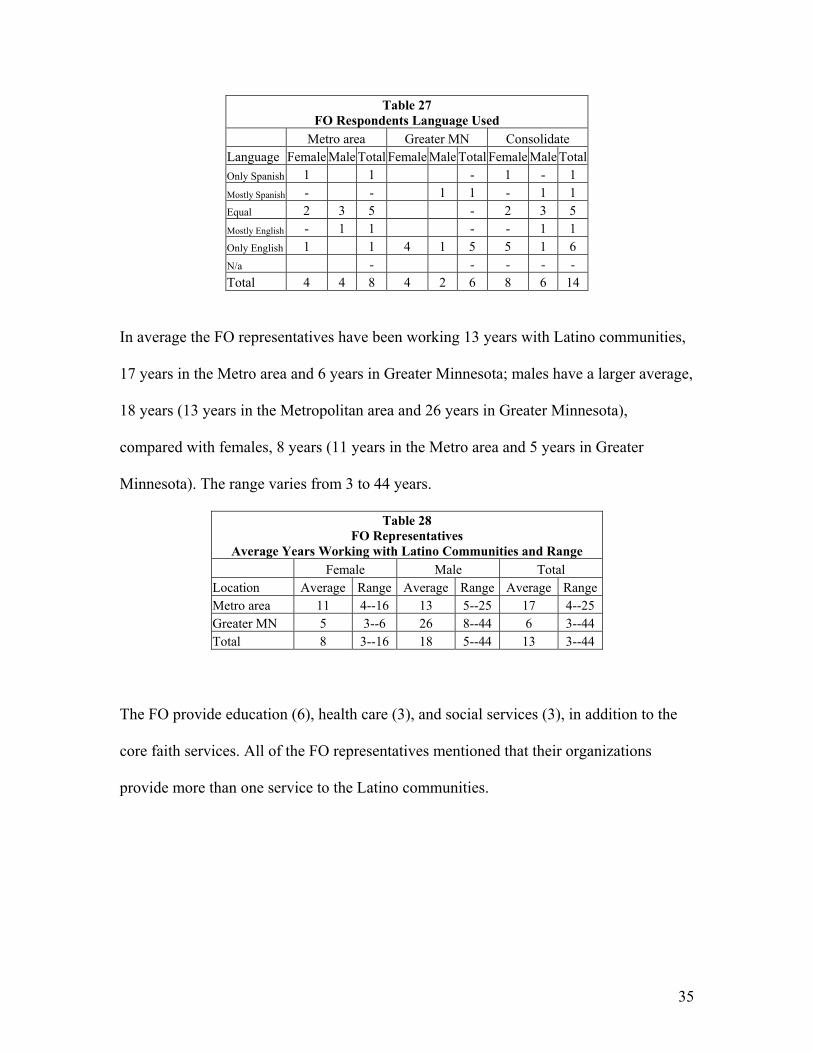
The FC respondents had an average time living in the US of 33 years, with a range
between 7 and 63 years. There was a large average difference between males in the
Metro (25 years, range 9 to 53 years) and the Greater Minnesota region (52 years, range
41 to 63 years). For females the average of years living in the US was similar in the
Metro area (35 years, range 19 to 51 years) and the Greater Minnesota region (31 years,
range 7 to 51 years).
Table 26 FO Respondents Average Years living in the US
Location Female Male Total Average Range Average Range Average RangeMetro 35 19 - 51 25 9 - 53 29 9 - 53Greater MN 31 7 - 51 52 41- 63 38 7 - 63Total 33 7 - 51 34 9 - 63 33 7 - 63
Most of the FO respondents usually speak with their friends and relatives only in English
(5 females, 4 from the Greater Minnesota and 1 from the Metro area; and 1 male from
Greater Minnesota); equal Spanish and English is spoken by five people (2 females and 3
males from the Metro Area); one female from the Metro area speaks only English; one
male from Greater Minnesota speaks mostly Spanish; and one male from the Metro area
reported speaking mostly English.
35
Table 27 FO Respondents Language Used
Metro area Greater MN Consolidate Language Female Male Total Female Male Total Female Male Total Only Spanish 1 1 - 1 - 1 Mostly Spanish - - 1 1 - 1 1 Equal 2 3 5 - 2 3 5 Mostly English - 1 1 - - 1 1 Only English 1 1 4 1 5 5 1 6 N/a - - - - - Total 4 4 8 4 2 6 8 6 14
In average the FO representatives have been working 13 years with Latino communities,
17 years in the Metro area and 6 years in Greater Minnesota; males have a larger average,
18 years (13 years in the Metropolitan area and 26 years in Greater Minnesota),
compared with females, 8 years (11 years in the Metro area and 5 years in Greater
Minnesota). The range varies from 3 to 44 years.
Table 28 FO Representatives
Average Years Working with Latino Communities and Range Female Male Total
Location Average Range Average Range Average Range Metro area 11 4--16 13 5--25 17 4--25 Greater MN 5 3--6 26 8--44 6 3--44 Total 8 3--16 18 5--44 13 3--44
The FO provide education (6), health care (3), and social services (3), in addition to the
core faith services. All of the FO representatives mentioned that their organizations
provide more than one service to the Latino communities.

36
Table 29 FO Services Provided
Service Female Male Total Metro Greater Metro Greater Metro Greater Total Education 1 1 3 1 4 2 6 Justice - - - - - - - Health care 1 1 1 - 2 1 3 Social services 1 - 2 - 3 - 3 Media - - - - - - - Faith 4 4 4 2 8 6 14 Government - - - - - - - Other 1 - - - - - -
Twelve FO representatives are interested in participating in a participatory planning
process for refining and expanding the list of intermediate outcomes of health disparities
affecting Chicano/Latinos in Minnesota, only two FO representatives from Greater
Minnesota did not answer this question.
Table 30 FO Representatives Interested in the Planning Process Location Female Male Consolidate
Yes No N/A Yes No N/A Yes No N/A Metro 4 4 - - 8 - - Greater MN 2 - 2 2 - - 4 - 2 Total 6 - 2 6 - - 12 - 2
iv. Focus Groups (FG)
Three FG were conducted, in Mankato, Minneapolis, and St. Paul. The demographic
questions of the survey were answered by each participant. Twenty-two people
participated, eight in Mankato and St. Paul, and six in Minneapolis. A total of thirteen
females and nine males were included.

37
Table 31 FG Participants by Gender
Female Male TotalMankato 4 4 8 Minneapolis 5 1 6 St Paul 4 4 8 Total 13 9 22
The FG participants’ age average was 39 years in Mankato (range 25 to 48 years), 33
years in Minneapolis (range 17 to 47 years), and 50 years in St. Paul (range 28 to 71
years).
Table 32 FG Participants Average Age Distribution and Range in Years Female Male Total Average Range Average Range Average Range Mankato 37 28 - 42 41 25 - 48 39 25 – 48 Minneapolis 33 17 - 47 32 32 33 17 – 47 St Paul 46 38 - 64 53 28 - 71 50 28 – 71
FG participants were from 4 countries including the US; most of them (18) were from
Mexico (10 females and 8 males), two were from El Salvador (1 female and 1 male), one
male was from Ecuador and other from the US from Mexican descent. All the FG
participants in Saint Paul and seven in Mankato were from Mexico; the most diverse FG
was Minneapolis with three female participants from Mexico, two participants from El
Salvador (1 female and 1 male), and one female participant from Ecuador.
Table 33 FG Participants Country of Origin
City Mankato Minneapolis St. Paul Total Country Female Male Total Female Male Total Female Male Total Female Male Total Ecuador - 1 1 - 1 - 1 El Salvador - 1 1 2 - 1 1 2 Mexico 3 4 7 3 3 4 4 8 10 8 18 USA/Mexico 1 1 - - 1 - 1 Total 4 4 8 5 1 6 4 4 8 13 9 22

38
The average time living in the US for the FG participants’ was 21 years for Mankato
(range 9 to 39 years), four years for Minneapolis (range less than one year to 7 years),
and ten years for St. Paul (range 6 to 25 years).
Table 34 FG Participants Average Years in the US and Range
City Female Male Total Average Range Average Range Average RangeMankato 26 9 - 39 16 15 – 20 21 9 - 39Minneapolis 4 .17 - 7 6 6 4 .17 - 7St Paul 8 6 - 14 12 7 – 25 10 6 - 25
Most of the respondents usually speak with their friends and relatives equally Spanish
and English (11) or mostly Spanish (10); one FG participant did not answer this question.
Table 35 FG Participants Language Used
Mankato Minneapolis St. Paul Total Female Male Total Female Male Total Female Male Total Female Male Total Only Spanish - 1 1 5 1 6 1 2 3 6 4 10 Mostly Spanish - - - - - - - - Equal 3 3 6 - 3 2 5 6 5 11 Mostly English - - - - - - Only English - - - - - - N/A 1 1 - - 1 - 1 Total 4 4 8 5 1 6 4 4 8 13 9 22
The FG participants have been working within Latino communities an average of thirteen
years in Mankato (range from 5 to 19 years), three years in Minneapolis (from two
months to six years), and seven years in St. Paul (range from six years to 13 years).
Table 36 FG Participants Average Years Working within Latino Communities
Female Male Total Average Range Average Range Average Range Mankato 14 5 - 19 13 12 - 14 13 5 – 19 Minneapolis 3 0.17 - 4.5 6 6 3 0.17 – 6 St Paul 8 6 - 13 7 9 - 4 7 6 –13
39
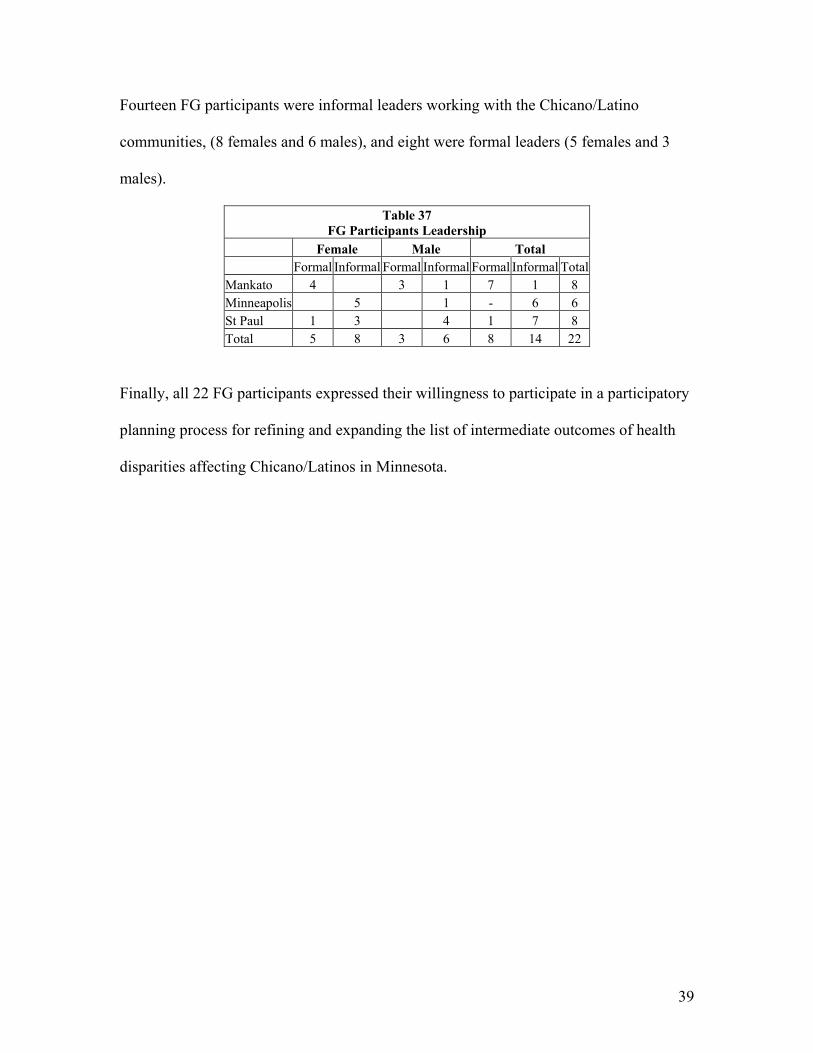
Fourteen FG participants were informal leaders working with the Chicano/Latino
communities, (8 females and 6 males), and eight were formal leaders (5 females and 3
males).
Table 37 FG Participants Leadership
Female Male Total Formal Informal Formal Informal Formal Informal Total
Mankato 4 3 1 7 1 8 Minneapolis 5 1 - 6 6 St Paul 1 3 4 1 7 8 Total 5 8 3 6 8 14 22
Finally, all 22 FG participants expressed their willingness to participate in a participatory
planning process for refining and expanding the list of intermediate outcomes of health
disparities affecting Chicano/Latinos in Minnesota.

40
f. Analysis of Findings, Surveys and Focus Groups
The following is the analysis of the answers of questions eight to fifteen of the survey
answered by CBO, HCP, and FO representatives; these questions were the guide used by
the facilitator for the focus groups.
The intent was to facilitate the discussion about the meaning of disparities, the
description of health disparities, the awareness of the Latino communities of their impact
on their families and communities, to understand their causes, to know community-
proposed solutions, and to identify their personal approach to participating in the
community process to develop the intermediate indicators.
i. Community Based Organizations (CBO)
From your perspective, what does “disparities” mean?
The main theme to the responses was unequal access to services. There was also a theme
of one group being treated unfairly, taken advantage of, or underrepresented compared to
another group. A couple of respondents mentioned differences in outcome among
specific demographic groups. Some of the respondents referred specifically to health
disparities.

41
How would you describe the health disparities affecting Chicanos/Latinos living in
Minnesota?
An overwhelming majority of the respondents specifically cited the lack of insurance or
inadequate insurance as the main health disparity. A few mentioned legal status as an
issue. Others mentioned lack of access to education compared to other populations, and
language barriers. A couple of respondents talked about research and data collection that
does not properly include the Hispanic population or take into account its diversity. One
respondent said that “there are socio-economic variables that cause an impact on the
disparities” and that it is necessary to approach the problem at the community level.
Is the Chicano/Latino community in Minnesota aware of the impact of health disparities
on their families?
Of the respondents, about two thirds thought that the community was aware of the
impact, about a third thought they were not aware, and a few were unsure or in between.
One respondent said:
“Sí, yo creo que todo el mundo sabe porque lo sienten, lo sienten en carne propia.”
(Yes, I believe that everyone knows because they feel it, they feel it in their own skin.)
One respondent commented that statistics are meaningless to people; they need context to
understand the problem and “direction for how it could be different.” Another said that
people easily recognize that the services available to them are not linguistically or
culturally proficient.

42
What do you think are the causes of health disparities and other disparities affecting
Chicanos/Latinos living in Minnesota?
Two themes were overwhelmingly apparent in the responses. Many people talked about
the lack of insurance and poverty. Others talked about the fact that there are not enough
social service or health care providers who are culturally competent or even able to speak
the language, and not enough partnering between mainstream and Latino agencies.
Quite a few people also listed racism or ethnocentrism, legal status, and lack of
knowledge or education about where to go for help.
What solutions would you propose to eliminate health disparities and other disparities
affecting Chicanos/Latinos in Minnesota?
Again, there were two significant themes. Many proposed more clinics, more personnel,
more funding. Respondents mentioned that clinics need to be low-cost so that the needy
people can afford to receive care. They also said that clinic and agency staff needs to
develop cultural proficiency and translators need to be used in case there is a language
barrier.
An equal number of responses said that everyone should have insurance. Several
mentioned changes in immigration laws, so that everyone who works will have insurance
regardless of their documented status. Others mentioned “affordable insurance” as a
solution.

43
Several also talked about community education. A few said that it was necessary to
educate the community about health issues. One said that it was necessary to educate the
community to ask Congress for help.
Please tell us your ideas for how we should engage organizations, individuals, families
and communities in identifying community indicators that could be used to monitor the
progress that is being made toward eliminating health disparities affecting
Chicanos/Latinos in Minnesota:
Respondents had different ideas. Some mentioned surveys: conducting one-on-one
interviews at community events, churches, and free clinics; surveying everyone
connected to health issues and asking specific questions; logging referrals made to health
organizations. One respondent explained that we should come up with some numbers to
back up our requests for change.
One respondent said that we should focus on a specific program, area, or organization,
and define our priorities and evaluating tactics. Another suggested putting together a
team to assess each community, develop strategies, and propose ways for mainstream and
Chicano/Latino organizations to implement the strategies. Still another mentioned
outreach advocates and holding accountable those who deny treatment. One respondent
was not optimistic; he said there doesn’t seem to be anything we can do,
“…just try to be calm.”

44
Please share any other comments, suggestions, or recommendations about this survey or
this process:
The comment that was repeated the most was that research in this community does not
always lead into action, which it should do if it is to be worthwhile. One respondent
requested that the results be shared with the public “in a form that is easily accessible &
frequent.” Another said that we need more health screening in the community and more
community advocates.
ii. Health Care Providers (HCP)
To the question “what does ‘disparities’ mean?” there was a broader range of answers,
from “I don’t know” to a holistic approach including “…a difference, inequality,
disproportion or a gap...”
When we asked them to go deeper into the concept, HCP respondents explained that for
example if “the problem we have to analyze is why and even if we have insurance do we
take advantage and take care of ourselves?” then we need to ask also “How much is the
lack of service and how much is our lack of participation?” which implied a relationship
between disparities and participation.
Some respondents emphasized that “disparities mean the over representation of one
group or population of focus in a given socio-economic or health aspect.”

45
Some respondents associated disparities as a measure against the mainstream populations
“…often disparity is any measure against whites as the "standard" but disparity should
be comparisons any and all grouping including "class, race/ethnicity, geography,
education, gender, etc” and its relationship in the population outcomes: “…disparities
are differences in outcome of "whatever" that cannot be accounted for without
considering the above.”
Disparities were also signaled as failure, “…areas were there is inequality, not meeting
the needs or failing in that area.” For example, “Illnesses and discrimination” are
identified as the causes of disparities, because people “face difficulties or barriers with
basic needs,” particularly barriers to health care services. That led to the current health
disparities identified.
For the Latino community based HCP, disparities are identified as a failure that reflects a
gap in services that affects outcomes by socio-economics status, race, ethnicity, gender,
and level of education. Illnesses and discrimination unveil the difficulties and barriers to
access basic needs services, principally health care services that result in a disproportion
in the incidence and prevalence of the burden of diseases among specific populations that
show a lack of participation.
“Health disparities mean the disproportionate representation in the incidence,
prevalence, mortality and burden of diseases that exist among specific
populations.”
46
Community participation seems to be an important factor to improve disparities, and the
lack of participations appears to prevent such improvement.
How would you describe the health disparities affecting Chicanos/Latinos living in
Minnesota?
Respondents described the health disparities affecting the Latino communities living in
Minnesota in several different ways that lead to a measurable lack of health insurance
coverage, underinsurance, and lack of economic resources to pay the co-pay for
prescription drugs or the price of the over the counter medicines that is a sign of people
facing difficulties or barriers to basic needs.
They identified the following causes of the health disparities affecting Latinos in
Minnesota:
Employers are not providing health insurance coverage to some Chicano/Latino
employees, even if they have been working for a long time in the same company.
“We get a lot of clients that are working and they don't give them insurance or nothing
even though they work a lot of time with the same company,” also some mentioned that
they have “jobs without benefits...”
Underinsurance was one of the issues described as health disparities affecting Latino
communities.

47
“…Many probably do not have sufficient insurance coverage. Basic health care
services as yearly exams are not available.”
In addition, access to prescription drugs or over the counter medicines is not possible
because “…no medication is dispensed due to co-pays for prescription or because over
the counter are not covered by insurance…”
Limited income prevents solving their and their children’s health care needs:
“…Having no insurance or limited income to meet their medical needs and that of
their children.”
“Health care services are denied if the patient has no insurance or make an
advance payment.”
Data collection was also described as one of the health disparities affecting the Latino
communities in Minnesota:
“…One disparity is in data collection; often "country of origin" is not asked for
example…”
These issues are reflected in the morbidity affecting the Latino communities:

48
“...The incidence of health issues among Hispanics is high, obviously in such
diseases as heart disease, diabetes and cancer, asthma, obesity and others.”
Respondents described the most important disparities as a result of multiple issues:
“disparities can be caused by several issues but I believe we need to address the
more prevalent of these issues systematically, which are as follow: access to
health education and services; lack of nutrition, diet, physical Activity by
population that cause heart disease, diabetes, cancer, and obesity; lack of sex
education is related to the HIV/Aids epidemic, STD, and TPP; and Lack of
insurance…”
Others referred that “…there are disparities in multiple areas, including but not limited
to cancer, heart disease, diabetes and domestic violence.”
The respondents concluded that:
“…to understand these disparities we need to take a systemic approach, meaning
that there are socio-economic variables that cause an impact on the disparities.
Also, we need to take a proactive approach, meaning that we need to undertake
initiatives at the community level, health promotion and intervention tactics, as
well as increasing awareness within the health system.”

49
Is the Chicano/Latino community in Minnesota aware of the impact of health disparities
on their families?
The answers ranged from a plain no to a conclusive yes. That could reflect the different
stage of disparities affecting Latinos, the different levels of awareness among Latino
communities, and the different understanding of the community awareness by the health
care provider.
For example, one respondent affirmed that:
“No, they don't see the impact on the community at-large. They see their
immediate needs and focus on overcoming immediate challenges. Given the
burden that immediate needs cause on Latino community members, they are not
able to have a comprehensive approach of the problem. They see that their family
members are not being served, but they don't make the connection with the
disparities problem.”
Another mentioned that community awareness is not enough, but the first step:
“…some are, but most are not. Health Disparity is a complex set of parameters
that can only be accurately measured over many years. Also is often not
meaningful to toss stats at people. There is no context for the disparity. Aware is
just a beginning step; people need context and direction for how it could be
different.”

50
The lack of awareness was explained from diverse perspectives including individual
behavior, class approaches, and the strong family relationship among Latino family
members.
A reflection was made of the behavioral causes of the health disparities and the individual
responsibility in the illness occurrence in the Latino communities, highlighting the
importance of culturally competent education programs and information campaigns
aimed to the Latino communities:
“…I could blame someone for my obesity or my overeating. But the fact of the
matter is that, we all know that overeating will result in weight gain. Most
Hispanic families have a history of heart disease, diabetes and other illness. And
they have a pretty good idea why it happens and how it happened, however
rudimentary. The question is do they do anything about their particular situation
when they learn that a death from a heart disease occurred in their family?
Probably not, they live with the idea that it won't happen to 'me' or justify to them
selves that they are eating healthy. Certainly, more education is needed and
informational material on how to avoid these diseases and in particular, what can
we do about it. But the ultimate decision to change one life style is up to the
person. Hispanics probably do not have actual data depicting the disparities, as
we know, professional or otherwise, if you do not work in the area of health. But
they do have their own family histories to fall back on…”

51
Some respondents explained the lack of awareness from a class approach:
“No, they don't see the impact on the community at-large. They see their
immediate needs and focus on overcoming immediate challenges. Given the
burden that immediate needs cause on Latino community members, they are not
able to have a comprehensive approach of the problem. They see that their family
members are not being served, but they don't make the connection with the
disparities problem,” and “it depends on the group that we are talking about for
example: White collar people are usually not in touch with the community and
they probably have a poor idea of it.”
Other respondents were not sure and identified the lack of access as one of the causes of
some Latino patients relying on home remedies “…some are but… not able to do much
and rely on home remedies…”
The strong relation among Latino relatives is addressed as cause of awareness of health
disparities:
“…Yes, when your relatives have ailments and illnesses that are not treated it
affects the entire family…”
Discrimination was also indicated as cause of awareness:

52
“Yeah. Because we know... We know, especially in my point of view, West St
Paul is really a racist county…”
What do you think are the causes of health disparities and other disparities affecting
Chicanos/Latinos living in Minnesota?
Community based HCP respondents identified discrimination, racism, level of education,
lack of resources, poverty, occupational hazards, and the medical model as some of the
multiple causes of the disparities affecting Latino communities in Minnesota.
Some of the most important causes of health disparities addressed by the respondents
were discrimination and racism; one informant described discrimination as:
“...discrimination, not having equal opportunities for fair wages and benefits,
labor positions with limited hours, education, language barriers limited to almost
none medical staff available to communicate their health needs, etc…”
Racism was described from a personal experience:
“…I don't know, maybe some people still, you know, the American people don’t
like some other race or something… One time my son in West St Paul was in a
public phone and the police stopped him and asked him what he was doing, they
thought he might have drugs or a gun or something.”

53
Level of education was also shown as one of the causes of disparities between urban and
rural areas:
“Level of education due to funding assigned to certain areas, such as rural and
urban.”
Lack of resources included:
“…Lack of resources, preventative health care, language, etc...”
“…Language barriers,” and “…fear of changing lifestyle…”
Poverty was mentioned, “…poverty, undocumented status, thus fears of accessing
services and delay in seeking treatment, diet…” and its consequences were explained:
“…We know that a high percentage of Hispanics lack insurance. Hispanics feel
more comfortable attending doctors and health services that provide health care
in Spanish. This will certainly impact on the disparities issue. But, more
important, Hispanics’ poverty, frequent mobility, low literacy, language, cultural
and logistic barriers impede Hispanics from access cost effective primary health
care. Economic pressure makes Hispanics reluctant to miss work, when it is
available. In addition, they are not protected by sick leave, risk losing their jobs,
if they miss a day of work. These circumstances cause Hispanics to postpone
seeking health care unless their condition becomes so severe that they cannot

54
work. At this point, Hispanics must rely on expensive emergency room care for
their needs.”
Occupational hazards and other health concerns were addressed:
“Health concerns can also be attributable to the occupational hazards of work
and also housing conditions. Hypertension has also been associated with
occupational class and transition, mobility of person or families. Depression is
often related to isolation, economic hardship, weather conditions and lack of
recreational opportunities, which can lead to substance abuse and smoking.”
The medical model as cause of health disparities was described as “…the medical model
treats particular illness rather than person…” also it was mentioned as part of a more
comprehensive approach:
“…health disparities must be caused by multiple factors, including but not limited
to: lack of understanding on the importance of regular check ups and screenings,
fear of diagnoses and preconceived ideas about diseases, traditional medicine vs.
Western medicine, medical system [being] seen as intimidating and cumbersome,
lack of knowledge on available resources, lack of awareness within the
medical/Health systems, lack of connection between existing health promotion
programs and intervention tactics…”

55
What solutions would you propose to eliminate health disparities and other disparities
affecting Chicanos/Latinos in Minnesota?
The solutions proposed to eliminate health disparities ranged from funding the services
provided by the health care providers including health care initiatives, health insurance,
health care programs, and direct services, to the Latino community self-addressing
solutions including taking responsibilities by their own health.
Some respondents stated that Latinos must take responsibility for their own health:
“…Chicanos/Latinos should address the disparities... We should start taking
responsibility for our own health…”
The answers reflect that eliminating health disparities is a difficult task that had been
tried for a long time, and people are skeptical:
“…I'll just tell you the truth; it's really hard because this has been for a long
time…”
However, respondents are aware of the possibilities as funding key programs and
organizations to provide culturally appropriate health care services and insurance to
Latinos:

56
“…Funding to services to meet cultural and language needs of Latinos in the
medical field, translators. Insurance they can afford…”
They recommend going to the “…root of the problem, language…” Also that:
“…Organizations obviously need money to direct services. Agencies need to
work together more. Address issues in ways to change cultural norms. Good jobs
and great education.”
They know that:
“…there is not a magical solution. I recommend continuing nurturing the
implementation of cultural specific programs that have intervention components.
For instance, those programs that "navigate" people through the health system in
order to get services... Simultaneously, raise awareness on the disparities within
the Health system.”
However they are not optimistic under today’s circumstances:
“…More funding for low cost health care for everyone. There are so many cuts
no one is watching out for needy people. Even clerical services that treat people
are decreased or eliminated...”

57
Please tell us your ideas for how we should engage organizations, individuals, families
and communities in identifying community indicators that could be used to monitor the
progress that is being made toward eliminating health disparities affecting
Chicanos/Latinos in Minnesota:
Respondents proposed several ideas including doing nothing but remain calm, using
outreach health advocates, public forums, partnerships, and research. The following were
the respondents’ points of view:
Some respondents are afraid of the consequences of exposing the health disparities:
“That one's really hard. It seems like there's nothing we can do, because if you
can go to court or something like that, they hit us really hard. Just try to be
calm.”
Others believed that it is important to expose the disparities and take action:
“Outreach health advocates, accountability to those that deny access to treatment due to
their language barriers or ability to pay…” in “Public forum, where the community has
a chance to speak up and dialogue different topics.” including “community events,
churches family and friends…” and providing “…Free clinics.”
Partnerships with organizations and health care networks is an important alternative for
some respondents:

58
“Partners with organizations to provide information to families and individuals and
develop partnerships with health service providers…”
The better use of existing resources was also proposed:
“Try to make better use of existing networks, meetings, gatherings. If it's an issue
for everyone, then it works best, is more sustainable, and more likely to become a
movement.”
Research is seen as necessary to evaluate the progress made toward eliminating health
disparities affecting the Latino communities in Minnesota:
“Progress should be evaluated/measured by research. Establishing measurable
outcomes is the only way to determine whether a program is working or not.
Recommendation: Focus on specific program, specific areas, specific
organizations, and then define priorities and evaluating tactics.”
Particularly respondents recommended:
“…the best community indicators are few in number, culturally relevant, and
measurable. Why identify new ones? Better to get community to understand
known ones.”
59
Please share any other comments, suggestions, or recommendations about this survey or
this process.
Some respondents recommended strategies to eliminate racism and discrimination like:
“I think people have to realize everybody is almost the same. If people could just
trust everyone, you know, because we are human beings anyway.”
Others insisted on research as an important way but they were cautious:
“It's difficult because recommendation and brain storming… and this process
often just gets put away with just being research, and tabled or placed in a
parking lot…”
They requested some practical solutions for difficult times as:
“…need for more health screening in community. More community advocates,
etc. The budget has jeopardized our State in many areas no jobs, no health
coverage. No plans to assist those who are not being reached, elderly, young, the
poor…”
Finally respondents recommended being practical and brought advice from their own
experience:

60
“…don't try to reinvent the wheel. Try to use existing research data. Encourage
partnerships among community-based organizations. Identify best practices.
Don't recruit community members unless you have something beneficial to offer
them. They want to see tangible benefits not long-term outcomes.”
iii. Faith Organizations (FO)
From your perspective, what does “disparities” mean?
Several of the respondents said that they did not know what “disparities” means. Others
talked about unequal treatment or unfairness. A couple of people said that it is the
opposite of parity. The most specific responses said that some people have or can afford
certain benefits while others do not have them.
How would you describe the health disparities affecting Chicanos/Latinos living in
Minnesota?
The overwhelming response had to do with the prohibitive cost of insurance. One
respondent said that the cost of insurance is a general problem not specific to Latinos, but
another respondent said that many Asians receive better benefits than the Latinos do.
One respondent talked about language barriers and two people mentioned discrimination.
Two people said there is no disparity or that “there are resources.”

61
Is the Chicano/Latino community in Minnesota aware of the impact of health disparities
on their families?
Two thirds of the respondents thought the community was aware. One respondent said
“no” and two were unsure or in between.
What do you think are the causes of health disparities and other disparities affecting
Chicanos/Latinos living in Minnesota?
The main theme in the responses was related to the high cost of medical care. People
talked about high cost, lack of funding, and legal status that does not allow people access
to insurance.
A few people also talked about stereotypes or racism as a factor. One respondent said
that people thought they might die if they went to the doctor. Also mentioned were the
lack of the language, lack of education, accidents at work, and drug use.
What solutions would you propose to eliminate health disparities and other disparities
affecting Chicanos/Latinos in Minnesota?
The main theme to the proposed solutions was education. Some talked about educating
the community, specifically families to create good family values, and the older
generation. Others talked about educating legislators through political action such as
phone calls and letters, and educating schools and agencies through diversity training.
One respondent mentioned educating both professionals and patients to close the gap.

62
Other ideas mentioned included restructuring existing services, providing more jobs with
the possibility of being legalized, and presenting a more unified front.
Please tell us your ideas for how we should engage organizations, individuals, families
and communities in identifying community indicators that could be used to monitor the
progress that is being made toward eliminating health disparities affecting
Chicanos/Latinos in Minnesota.
These answers were all about education. One idea was to use government resources to
bring education to families. Two people suggested having meetings at churches that
would be open to the community, where discussion could take place and the community
could work together toward health improvement. Another respondent suggested
educating professionals.
Please share any other comments, suggestions, or recommendations about this survey or
this process:
The only comment was that doing this survey was important and that it showed the
interest and initiative to work toward solving the problem.

63
iv. Analysis Focus Groups
1. Mankato Focus Group
To start the discussion, the participants were asked to discuss their thoughts about the
concept “disparities.”
They were not completely sure about the meaning of “disparities.” Some participants
claimed not knowing the word, even in Spanish.
“¿Qué significa disparidad?” (What does “disparities” mean?)
“No sé lo que significa” (I don’t know what it means)
Other participants just mentioned a succinct concept by using only one word describing
its meaning, as a synonym; for example:
“desigualdad” (inequality)
“diferencia” (difference)
Notice that all the participants from the group claimed to understand both languages very
well. It is important to point out that the term used is not familiar to our participants in
any language. However, overall, the group waited for an explanation from the facilitator
in Spanish, in order to continue. Participants explained that it was important for the group
to have a good idea of the definition of disparity in order to continue the discussion.

64
The facilitator proposed thinking about services provided to someone from the
mainstream community and comparing the same services provided to someone from a
minority community in Minnesota under the same circumstances.
The discussion then continued around some key words describing the definition. Some of
these words used by participants were the following:
Access to resources and education:
“No tener acceso igual” (not equal access)
“Calidad de acceso” (Quality of access)
It was stated by some of the participants that their communities suffer from a lack of
accessibility to their health services, for a variety of reasons, including the following:
• Poor education within the community about the topic explains the lack of use of
resources already available for the Chicano/Latino communities.
• The lack of resources, such as the low income that the population has, which is a
barrier to health care services in Minnesota.
“En el área de doctores, no hay muchos”
(There are not many doctors available.)

65
“Muchos no tienen seguros médicos”
(A lot of people have no health insurance)
Some participants made a direct link between income and health disparities:
“Low access to dollars, means health disparities”
Their previous experience using health care services was an important reference that was
discussed at this point. A few participants explained that families that had requested
health care services and had had a hard experience might have something to say related to
discrimination, for example:
“Duré tres meses buscando una cita con el odontólogo porque no estaban dando
citas, sin ninguna explicación. Pero cuando mi hija habló sin acento la
atendieron inmediatamente.”
(I spent three months asking for a dental appointment because they were not
booking appointments, without any explanation. However, when my daughter
called them without an accent, she was attended immediately.)
Some referred the high cost of health care as a barrier when it is compared to the cost in
their country of origin.
“Muchos van a su país por servicios de salud. El costo tiene mucho que ver.”

66
(A lot of people are going back to their countries of origin for health care services.
It happens because of the cost.)
“Las compras de medicinas son más baratas allá”
(Medicines are cheaper there)
“También la gente compra en mayoreo, por ejemplo anticonceptivos”
(In addition people buy wholesale, for example contraceptives)
Participants also mentioned that the quality of the insurance carried makes a huge
difference:
“Existen preferencias por seguros médicos por la comercialización”
(There are health insurance preferences, because of the marketing.)
Other participants described how the patient’s lack of knowledge of current services
prevented them from having a fair opportunity to know if they are receiving all the
available service. Therefore people do not know what are they missing or if they are
missing anything at all.
Some stated that some Chicano/Latino people in Minnesota are not aware of the impact
of health disparities because they never have received health care services in their
country of origin, and any kind of health assistance received by this people is already

67
more than they are used to receiving. Consequently, it will be challenging to bring a point
of comparison for “disparities.”
“Hay gente que nunca han recibido servicios de salud, y cuando llega acá
cualquier cosa ya es mucho.”
(There are people that never have received health care services, and when they
arrive here any thing is a lot for them.)
Some of the causes of disparities described by participants were the following:
• There is a lack of education about how to use health care resources.
• People in the community normally don’t go to the doctor as a first resource for a
health problem, because it is too expensive, and not many people have good
health insurance coverage. Then they are forced to use other alternatives, like
travel to their country of origin for health services.
• Some use home remedies or they ask somebody who goes to their country of
origin to bring them back medicines bought there.
• The emergency service is the last resource when nothing else works and when
they understand that they will receive health care services regardless of their
condition; but it is very expensive, for this reason, this is the last choice people
will make.

68
• The lack of resources available to Chicano/Latino communities in Greater
Minnesota including culturally sensitive health practitioners and interpreters that
may facilitate simple tasks in the health care service facilities was also mentioned.
“Falta de concientización que conecte la educación y la información con la
persona”
(There is a lack of understanding of education and information by the people.)
“Muchos van a su país por servicios de salud. El costo tiene mucho que ver. La
gente trae antibióticos, algunos traen encargos.”
(Some people come back to their country of origin for health care services. The
cost is one of the major reasons. People bring antibiotics, some by others’
request.)
In some cases people use their sons/daughters as interpreters:
“...Usan a sus hijos como interpretes.”
(…They use their sons/daughters as interpreters)
When the interpreter is provided, in some cases he/she is not competent in health care
terminology:
“No todos los interpretes que hay son buenos o competentes, ellos dicen: ‘sí le
entiendo pero cómo le digo’.”

69
(Not all the interpreters are very good or competent. They say, “I understand, but
I don’t know how to say that.”)
“Los Buenos interpretes generalmente necesitan ‘ride’ y hasta el paciente
también.”
(The good interpreters often need a ride as well as the patient)
At this moment the solutions for these disparities were discussed. The first one mentioned
was education. They explained the importance of education in their communities to help
alleviate some of their beliefs that do not contribute to better practices of health care in
their families:
“Educación en la prevención como miedo a las mala noticias; cómo gastar
menos por las aseguranzas; la falta de confianza en los doctores en ciertas
ocasiones y no en todas.”
(Education in prevention to prevent bad news; how spend less on health
insurance; lack of trust on doctors some times, but not always.”
“Falta decirles a qué tienen derecho en la asistencia médica”
(Lack of information about their rights in health care)
They referred to the use of information in their community to help them understand the
available resources and how to use them and how to access appropriately:

70
“...Los proveedores de servicio que tengan anuncios de lo que ofrecen.”
(The service providers should announce what they offer.)
They even mentioned some of the possible ways that could help to improve
communication:
“Hacer campañas publicitarias usando información básica, por aquello de
preguntas. Es importante dar una buena información completa y correcta. Ser
muy directo.”
(Make public campaigns, giving complete and correct information to answer
questions. Be very direct.)
One participant proposed as a solution “Universal health care coverage:”
“Cobertura universal para todas las personas que incluya por ejemplo cuidado
de niños para mujeres solteras o sistema de reembolso para day care, transporte,
medicinas, interpretes... Que todos tengan derecho y oportunidad de que los
cubra a bajo precio.”
(Universal Coverage for all people that could include for example daycare or
daycare reimbursement for single mothers, transportation, medication,
interpreters... Everyone should have the right and opportunity to be covered at a
low price.”

71
The following were other aspects discussed:
One issue was what was missing in services and also the quality of the already existent
services in the community:
“(Son necesarios) más doctores y trabajadores bilingües”
(More bilingual doctors and workers are needed.)
Cultural sensitivity was an issue also:
“...Se siente mas a gusto el paciente a la hora de recibir el servicio.”
(The patient feels more comfortable receiving culturally sensitive services.)
Participants also proposed finding solutions from the community’s perspective:
“Hablemos de solución de abajo hacia arriba.”
(Let’s talk about solutions from the bottom up.)
Finally, some participants agreed that part of the solution to eliminate health disparities
working with the communities would be the participatory planning process. However,
when we discussed the possibility of working on identifying community indicators to
monitor the progress that is being made toward eliminating health disparities affecting
Chicanos/Latinos in Minnesota, it was difficult for the focus group participants to

72
understand the concept. For instance, many in the group did not understand the word
“indicator” in English, even when it was translated into Spanish.
The facilitator explained that in a process of eliminating health disparities it is necessary
first to identify them. In the participatory planning process proposed we would work with
the communities’ representatives to identify the specific health disparities that affect each
community and find the best way to identify each disparity.
Participants then made clear that communities need to get information of what is
available now in the community and agreed that it is necessary to make a cooperative
effort to work together in this important issue, even with other existent efforts in the state:
“Colaboración con otros esfuerzos existentes en el estado.”
(Collaborations with other existent efforts in the state.)
Doing that creates a need to form a group that also can get collaboration from diverse
groups interested in this area. Then bring solutions to improve the situation of health
disparities.
“Planeación, que se reúnan otras organizaciones de salud coordinadas; para
evitar perdida de recursos... duplicidad de servicios.”
(Planning, health care organizations meeting together, to avoid loss of resources
and duplication of services.)

73
(Surveys of different agencies and hospitals.) “Por medio de la radio, e-mail; or
ask directly to the people.”
(By means of radio, email, or asking the people directly)
Some remarked on the importance of collaboration with community leaders:
“Tomar en cuenta la participación de lideres naturales en la comunidad”
(Take into account the participation of natural leaders in the community.)
Participants requested a copy of the report as form of access to information:
“Compartir la información del reporte como forma de acceso”
(Share the information from the report as a form of access.)
Some participants also mentioned that legalization, particularly for professionals that are
not recognized here, is an important step to improve the health disparities affecting the
Chicano Latino communities in Minnesota.
“Acceso para la comunidad para arreglar sus situaciones.”
(Access for the community to fix their situations.)
“legalización para estudiantes para que sirvan a la comunidad; o que se criaron
aquí pero que son ilegales.”
74
(Legalizations for students so they can serve the community, or for those who
grew up here but are illegal.)
The importance of political participation and advocacy for policy change was also
mentioned as an important part of the solution.
When participants were asked about their willingness to participate in a planning process
to identify health disparities indicators it was a consensus that all of them are willing to
participate in the planning process.
“Sí, claro”
(Yes, of course.)
Finally, participants shared some past experiences with efforts that started well but were
never completed; for instance, some services were different than proposed. These
experiences make future community based participatory projects in this area more
difficult; however, because the process will be lead by a Latino community based
organization they are confident that it will be a success.
Participants are very interested in helping the community. They wanted to learn what
other Chicano/Latino leaders think about health disparities affecting our communities.
However they made it clear that false promises will not be accepted at all.

75
“...Porque organizaciones prometen servicios de salud mental y luego nada… Es
una burla a la comunidad.”
(Because organizations promise mental health services and then nothing… It is a
mockery of the community.)
2. Minneapolis Focus Group
The facilitator introduced the discussion starting with the meaning of the word
“disparities” from their perspective. Most of the participants used the word inequality as a
synonym. Only one participant referred that he did not know completely the meaning of
“disparities.”
Some of the expressions used to define disparities were the following:
“Disparidad es desigualdad, algo que no va igual, que no encaja.”
(Disparity is inequality, something that is not equal or that doesn’t fit.)
“Disparidad es desigualdad o disbalance”
(Disparity is inequality or unbalance.)
“Cuando no concuerda algo.”
(When something doesn’t match.)

76
A participant mentioned did not knowing the meaning of the word “disparidad” (disparity
in Spanish)
“No sé lo que significa.”
(I don’t know what it means.)
All of the answers were originally in Spanish, because Spanish-speaking participants
composed this group predominantly.
After the meaning of disparities was discussed, the facilitator advanced the discussion
with a brief explanation of why “disparities” are important in public health. He proposed
thinking about services provided to someone from the mainstream community and then
comparing the same services provided to someone from a minority community in
Minnesota under the same circumstances.
In the context of health, one participant, who recently arrived to Minnesota from a Latin
American country, confirmed her limited knowledge of health disparities and
consequences. However, the participant showed interest in knowing more about the topic.
“La verdad es que no sé mucho, más bien no estoy informada sobre estos
programas de salud, no sé cuales son las disparidades que existen aquí, en el
sector de salud, sí me gustaría saber cómo es que funciona esto.”

77
(The truth is that I don’t know much, I’m not really informed about these health
programs, I don’t know what the disparities are that exist here, in the area of
health; I would like to know how this works.)
Then the participants agreed that health disparities do affect our communities in a
negative form. The following are some of the comments expressed from the participants:
“Afecta a todas aquellas personas que no tienen la posibilidad de pagar los
‘biles’ médicos por falta de dinero que algunas personas tenemos la posibilidad y
otras no.”
(It affects all those people who don’t have the possibility of paying medical bills
for lack of money, some of us have that possibility and others don’t.)
“Las disparities: Nos afecta en todo sentido como usuario de los medios
(servicios) de salud. 1- No disfruto de un completo servicio de salud. 2. Como ser
humano tengo derecho a un servicio completo de salud. 3. Es necesario trabajar
más serio en las disparities.”
(Disparities: Affect us in every sense as users of the health care services. 1- I
don’t have a complete health care service. 2- As a human being I have the right to
a complete health care service. 3-It is necessary to work more seriously on
disparities.)

78
The lack of money is perhaps one of the more significant issues related to health
disparities. It is reflected in the high cost of health insurance versus low income; other
related problems were also discussed, like the language barriers to communicate between
providers and patients; and the lack of information transmitted to the Chicano Latino
communities to be aware of its existence.
Then the group moved to the awareness of health disparities among the Chicano/Latino
communities, most of the participants agreed that the communities might be not aware
about how health disparities impact their communities.
“…en caso que yo me enferme a donde voy?”
(If I get sick, where will I go?”
This was a comment by a participant who has been in Minnesota for a short period of
time. The concern expressed by the participant also reflects the suspicion that
Chicano/Latino communities are not really aware of the health care services available in
their neighborhoods, which is an important health disparity.
In fact they were all agreed that there is a negative impact and that there is something that
needs to be done, which could help improve the reality.

79
The causes of health disparities affecting Chicano/Latinos in Minnesota were discussed.
Some participants expressed lack of knowledge of the available resources for the Chicano
Latino communities in Minnesota.
“…la verdad no sabe a quien acudir y las organizaciones no se dan cuenta de
que es lo que necesita la comunidad…”
(The truth is they don’t know where to turn, and the organizations don’t realize
what the community needs.)
“...la comunidad necesita estar bien informada acerca de esto..”
(The community needs to be well informed about this.)
“No todos saben sobre todos los servicios de salud que ofrecen..”
(Not everyone knows the health services that are offered.)
Another participant mentioned that the immigrant status and the fear of discrimination are
important circumstances that Chicano/Latino residents in Minnesota face when they look
for health insurance or health care services:
“Pienso que el estatus legal... porque si no tienes de seguro no puedes tener para
tus hijos un plan de salud.”
(I think the legal status… because if you don’t have it, you certainly can’t have a
health plan for your children.)

80
The solution discussed in the group was that information and its dissemination to the
Chicano Latino community must be considered as a priority:
“Que se brinde más orientación acerca de los servicios actuales.”
(We need more orientation about the current services.)
Also, it was discussed that migrant status must be improved in order to eliminate the
health disparities in Minnesota. Some participants proposed including discrimination as
an indicator of health disparities.
Some participants did not understand what an indicator is or how it is used, even when it
was translated into Spanish. Then the facilitator explained that in the process of
eliminating health disparities it is necessary to identify them. In the participatory
planning process proposed, we would work with the communities’ representatives to
identify the health disparities that affect each community and the best way to identify
each one.
Some of the participants said then that one indicator could be the number of clinics
available for the Hispanic population, and also the flexibility of their office hours, for
example on Saturdays and Sundays, to increase the access.
“Abrir más clínicas que ayuden a la gente hispana…”
(Open more clinics that help the Hispanic people.)

81
“A veces la causa que la gente no acude al doctor por causa de tiempo ( por el
trabajo.) Yo opino que se pudiera dar servicio de salud el día sábado.”
(Sometimes the reason people don’t turn to the doctor is because of time [because
of work]. I think that health service could be offered on a Saturday.)
It was also recommended to get information about what resources are available in the
communities. By doing this, there is a need to form a group that can collaborate with
diverse organizations interested in this area and then come up with solutions lead to
improve the health disparities affecting Chicano/Latinos in Minnesota.
Health insurance coverage for everyone was also discussed. They thought that solving the
health insurance coverage would solve most of the health problem discussed in the focus
group. However, there was not a clear explanation of how to fund this kind of initiatives.
Participants were very enthusiastic to participate in future activities related to the topic.
One participant mentioned that she found this activity relevant because the interchange of
opinions between all participants helped her to understand much better health disparities.
“...Sí, focus groups para intercambiar opiniones.”
(Yes, Focus Groups to exchange opinions.)
Some participants expressed their satisfaction for being invited to this activity. As long as
the facilitator was expressing a sincere appreciation for their efforts, their response was

82
reciprocal. The group elevated its interest and they empowered us to put together efforts
to diminish health disparities affecting the Chicano/Latino communities in Minnesota.
3. St. Paul Focus Group
To start the discussion in the focus group, the concept “disparities” was proposed, but it
was not understood at the beginning. The facilitator then used Spanish equivalent words.
However participants expressed difficulties understanding its meaning. At this point the
facilitator proposed the following example to collectively built the meaning of
“disparities:” Please think about services provided to someone from the mainstream
community, and then compare the same services provided to someone from a minority
community in Minnesota under the same circumstances.
Then participants agreed that disparities means inequality in service, in our case
inequality in health care services provided to the Chicano/Latino population. They
explained that this is one of the most important problems for our communities.
“Unequal access and distribution of goods and services”
“Disparities means problems that the Chicano/Latino are facing regarding health
care”
Another concept used to describe “disparities” was the “unequal distribution of goods
and services.”
83
“Other words that come to mind for me include: gaps, problematic differences,
unfairly treated, inequality, unfavoratized, disrespected, disenfranchised”
Everyone had a fair idea of what disparity means, except one participant who just
expressed that he did not know:
“I don’t know”
The group described the health disparities affecting Chicano/Latino communities in
Minnesota as a real problem that currently affects the community and needs to be solved
promptly.
Lack of health insurance in many occasions prevents Latinos from going to the doctor’s
office; they delay the medical appointment until the health problem becomes a medical
emergency.
“Es grave porque mucha gente no tiene seguro y en muchos casos no van al
médico hasta que ya están en la última; y se van a la emergencia a ver si los
atienden.”
(It’s serious because many people don’t have insurance and in many cases they
don’t go to the doctor except as a last option; then they go to the emergency room
to see if they’ll attend them there.)

84
The affordability of health care services for the Chicano/Latino communities was referred
as another disparity:
“Often I observed Latinos being left out in consideration in studies or clumped
with another groups. Health care and affordability for Latinos seems disparate.”
“Most of the people that I work with are underemployed or working low-wage
jobs with few or not benefits.”
Participants remarked that there is a lack of health care services for the Chicano/Latino
communities. They are not being provided effective health care services in the first place.
In some occasions due to language barriers and cultural appropriateness of the health care
provider. For example educative and informative brochures sometimes are translated
inaccurately, so the message is not clearly understood or it is misleading the patient and
his/her family. The cost of health care services also was showed as one of the health
disparities affecting the Chicano/Latino communities.
“Sometimes when you receive services there are not Spanish speaking services
available, maybe because they are too expensive.”
Another form of disparity mentioned by participants was “disparities” at the work place,
and some kind of discrimination in salaries and other worker’s compensations. These
disparities were referred that have a direct impact on health disparities.

85
“Also at work there are a lot of disparities. The blonde get the less hard jobs, and
that would affect us emotionally because we would feel with disadvantage to say
or to do something”
“The Americans have better paychecks and salary than Latinos.”
Most of the participants affirmed that the Chicano/Latino communities are aware of the
negative impact that health disparities cause to their families and their communities in
Minnesota.
“Sí, en algunos casos sí...”
(Yes, in some cases, yes.)
However, this awareness is very limited, according to some of the participants. People
become aware when they get some kind of experience with health care services in
Minnesota. After they knew how to operate the system they become frustrated, even
depressed because of the lack of services available to the Chicano/Latino families:
“...there is a lack of information about existent services.”
“Tú estás deprimida de todos los servicios que su familia puede recibir, es muy
frustrante.”
(You’re depressed from all the services that your family can receive; it’s very
frustrating.)
86
“It is very frustrating to our families. For example: if our people have benefit of
health care but doesn’t know the language, they won’t be able to obtain
completely everything they are entitled.”
Therefore, participants stated that our community might be somehow aware but not
enough aware to begin a stronger movement to inform us more about the health
disparities problem and thus move forward to work on its solution.
Some of the major causes of health disparities affecting Chicano/Latino communities
living in Minnesota described by participants were the following:
• Being an immigrant in this country involves proper documentation. Then you will
have access to health insurance; however, the lack of employment, the emotional
stress, lack of English proficiency and other language and cultural barriers are
preventing Chicano/Latino communities from being aware of the health
disparities affecting them.
• Some refer to discrimination as an important issue for health disparities.
• The lack of resources in the health care area for Latinos, the lack of understanding
of Latino health care needs, and the health care providers’ lack of knowledge
about Chicano/Latino communities were also mentioned as sources of health
disparities in Minnesota.
The discussion moved forward possible solutions to prevent the occurrence of health
disparities. Participants provided the following approaches:

87
• To educate the Chicano/Latino communities and the health care providers;
• To increase health care resources and make them available to the Chicano/Latino
communities living in Minnesota;
• To work in comprehensive strategies to improve the quality of life of the Latino
communities in Minnesota.
As participants were discussing possible solutions, they quoted some anecdotes and past
personal experiences to prove their point. These included the high cost of health services
and difficult choices that they encountered when they were in need of health care
services, especially dental services.
“Sometimes you have to choose from a dentist or a doctor because it is very
expensive.”
“Con lo que pagas para arreglar una carie, usted puedes pagar un tiquete de
vuelo para México, arreglarlo y regresar de vuelta.”
(What you pay to fix a cavity, you can pay a ticket to fly to Mexico, fix it and fly
back.)
“Eso para los que pueden ir, para los que no pueden ir, se quedan ahí, y
terminan por arrancarse la muela o el diente en vez de arreglarlo”

88
(That’s for those who can go; those who can’t go stay here and end up pulling out
their molar or tooth instead of fixing it.)
Some participants emphasized that some people cannot discuss health disparities because
they do not even have access. So they cannot compare the health care service because it
is not provided. They discussed that access is an important issue for the Chicano/Latino
communities living in Minnesota. They expect that this kind of research will provide
accurate information to eliminate health disparities. Also they proposed education as one
of the key solutions.
“Have some people educate me and then I will share what I know.”
They believe that accurate information about what health services are available, the
requirements to access, and a flexible schedule are part of the solution. Those elements
would be complemented by appropriate channels of dissemination like churches,
community based Latino organizations, Latino media, television, local radio, and face-to-
face communication to reach illiterate populations, which suffer most of the health
disparities affecting our communities.
“Muchos son analfabetos y no andan mucho afuera; solo del trabajo a la casa.
Entonces la única cosa que hacen es ver televisión o escuchar la radio”
(Many are illiterate and they don’t go out much, just from work to home. So the
only thing they do is watch television or listen to the radio.)

89
One of the activities suggested by the group was the use of surveys to learn more about
the community and the use of churches and schools as a physical area that can be
contemplated as a possible strategic place to develop these activities with success.
There was a consensus that education, research and community involvement are key
elements to eliminate health disparities affecting the Chicano/Latino communities.
When the facilitator asked who was willing to participate in future events, almost
everybody expressed that he/she was willing to participate in future events such as this
one.

90
g. Conclusion
In conclusion, from the surveys that were answered by the Chicano/Latino CBO, HCP,
and FO representatives, and from the concepts discussed in the FG, “disparities” has a
broad meaning from unequal access to services to the lack of Chicano/Latino community
participation. It is a complex concept that could be difficult to understand. It depends on
the context in which it is used.
From the Chicano/Latino perspective, “disparities” are seen as: difference, unequal
access, inequality in access to services, unequal distribution of goods and services,
difference in quality, something that is not equal or that does not fit, unbalance, when
something does not match, gaps, problematic differences, unfairly treated, disrespected,
disenfranchised.
In a general perspective “disparities” were described as the opposite of parity, also as the
possibility for certain population to afford certain benefits while others do not have them
in similar circumstances; this is one of the most important problems affecting the
Chicano/Latino communities in Minnesota. “Disparities” mean problems for the
Chicano/Latino communities.
Our communities are daily facing “disparities” in health care services as the result of an
unfairly treatment that the Chicano/Latino population suffers for several reasons
including historical ones and their under-representation in the decision making areas.

91
The relation between disparities and the lack of community participation was discussed.
This is an important question that must be answered in future community based
participatory research efforts. In this complex context, community participation seems to
be an important factor to improve “disparities,” and the lack of participation appears to
prevent such improvement. It is necessary to approach the problem at the community
level to find adequate solutions.
From a different perspective “disparities” were interpreted as a failure of the society to
provide equal opportunities to every body. There are some areas where there is
inequality, not meeting the basic needs or failing to meet people’s needs, like illnesses
and discrimination when people face difficulties or barriers to deal with their economic or
health burdens.
In the case of “health disparities,” illnesses and discriminations unveil the difficulties and
barriers to access basic needed services, principally health care services that result in a
disproportionate representation in the incidence, prevalence, mortality and morbidity that
exist among specific populations.
Health disparities affecting the Chicano/Latino communities in Minnesota were described
as the consequences of multiple factors combined in different ways to different
individuals, families, and communities. To understand these disparities, a systematic
approach was proposed to address all the variables involved. Health disparities were seen
as a complex set of parameters as a result of multiple variables, including the following:

92
i. Lack of awareness
From the people’s perspective, there is a lack of awareness, knowledge, and information
about health care services available in Minnesota; people do not know how to navigate
the complex health care system; they need time and resources to access accurate
information. This issue is particularly critical for recent Chicano/Latino immigrants. It
prevents people from accessing information and health care services.
When services are provided, Chicano/Latino patients do not know if the quality of the
services provided met the accepted standards. Therefore people do not know what they
are missing or if they are missing anything at all.
The medical/health systems in Minnesota are not aware of the Chicano/Latino
community health care needs, culture, feelings, and beliefs, which results in a
disconnection between existing health care services, health promotion programs,
prevention strategies, and community participation.
There are different levels of awareness among Chicano/Latino communities; most of the
communities are aware of the impact that “disparities” have in their families and
communities; however people are focused on overcoming immediate challenges and
needs that prevent them from seeing health disparities as a community problem.

93
Communities are not aware enough to begin a stronger movement to provide information
about the health disparities problem and move forward to work on its solution.
They are aware of the causes not the solutions. This situation prevents an effective
community participation to bridge the gap in health disparities. It was recognized that
being aware is just a beginning step.
ii. Education
Illiteracy and low level of formal education prevent people from accessing better jobs;
they are linked to poverty and result in significant health disparities especially in rural
areas. They also make it more difficult to learn how to use the services and how to
improve their health behavior; in some cases people are afraid of changing their lifestyle.
It was mentioned that the most educated Chicano/Latino population, white-collar
professionals, probably are not aware of how the rest of the community suffers unless
their profession involves contact with such people. More education is needed
complemented with informational material on how to prevent diseases including change
in a person’s life style.
A self-reflection was made of the behavioral causes of the health disparities and the
individual responsibility in the illness occurrence in the Chicano/Latino communities,
highlighting the importance of culturally competent education programs and information

94
campaigns aimed to the Chicano/Latino communities. People mentioned a lack of
understanding of the importance of regular check ups and screenings, fear of diagnoses,
and preconceived ideas about diseases that should be addressed in educational
campaigns.
iii. Poverty
The socio-economic burden as a consequence in most cases of poverty was linked to low
levels of education and illiteracy; this burden leads to a vicious circle of low level of
education, poverty, and health disparities. It was identified as a barrier to health care
services. It prevents patients and their families from accessing health care services; and
when access is possible, the prescription drugs become unaffordable because of the cost
of the medicines or the co-payment.
The high cost of health care services is a well-known barrier that prevents the
Chicano/Latino communities from affording them when needed. This is a sign of people
facing difficulties, and it is an important barrier to solve their basic needs. A direct link
was made between income and health disparities.

95
iv. Discrimination
Stereotypes, discrimination, racism, and ethnocentrism are some of the most important
causes of health disparities addressed by the respondents. Immigrants frequently are not
aware of the antidiscrimination laws and they do not know that their rights are protected
in Minnesota.
v. Job Conditions
Employment conditions, underemployment and very low-wage jobs with few or no
benefits were referred to as another cause of “disparities.” Discrimination in salaries and
other worker’s compensations and benefits also were mentioned.
Employers are not providing health insurance coverage to some Chicano/Latino
employees, even if they have been working for a long time in the same company. As a
consequence, Chicano/Latino employees are reluctant to miss work because they have no
sick leave and they risk losing their jobs if they miss a day of work.
Accidents at work, occupational hazards, and housing conditions were also referred to
have a direct impact on health disparities, especially because of the frequent mobility of
workers and their families from job to job.
96
vi. Health Insurance
The lack of health insurance, underinsurance, and the quality of the health insurance
when available prevent Chicano/Latinos from accessing health care services when
needed.
vii. Culture and Language
Cultural and logistic barriers impede our communities from accessing primary health care
services. For Chicano/Latino patients, the lack of understanding of the American culture,
especially the language, prevents them from having adequate access and health care
services and makes them vulnerable for disparities.
Culturally competent and linguistically appropriate services are not available for all the
Chicano/Latino communities in Minnesota. There are no sufficient partnerships between
mainstream and Chicano/Latino agencies to provide health care services, especially in
rural areas. This situation prevents the Chicano/Latino communities from having the
same quality and quantity of health care services provided to the mainstream community
in Minnesota.

97
viii. Weather
The extreme weather conditions in Minnesota in some cases were pointed out as a cause
of isolation and lack of recreational opportunities, which leads to depression, substance
abuse, and smoking. Also, immigrants are exposed to new diseases like influenza and
Lyme disease.
ix. Medical Model
The medical model was described as privileging the disease over the person. For a
Chicano/Latino patient this approach prevents the development of an adequate health
care provider-patient relationship and makes it difficult to comply with the health related
recommendations, including adherence to drug prescription, screening, and health
promotion and prevention recommendations. The medical system is seen as intimidating
and cumbersome.
x. Immigrant Status
Immigrant status on occasion does not allow people access to insurance. Recent
immigrants believe that their immigrant status is a barrier to accessing health care
services.

98
xi. Research
The idea that research and data collection does not properly include the Chicano/Latino
population or take into account its diversity was mentioned as a cause of health
disparities.
xii. Access
The lack of access to information, health education, culturally competent and
linguistically appropriate health care and social work service providers results in
inadequate nutrition, diet, and physical activities, a disproportionately low rate of
inclusion of Chicano/Latino patients in clinical trials and other studies, and in the
increasing morbidity and mortality affecting the Chicano/Latino communities.
xiii. Offer of Health Care Services
There is a lack of resources available to Chicano/Latino communities, especially in
Greater Minnesota, including culturally sensitive health practitioners and interpreters that
may facilitate simple tasks in the health care service facilities. A comprehensive health
care service is not available for all the Chicano/Latino communities in Minnesota.

99
xiv. Morbidity and Mortality
The incidence of some health problems among our communities is higher than in the
mainstream community, diseases like heart diseases, diabetes, cancer, asthma, obesity,
the disproportionate incidence and prevalence of HIV/Aids and other STD, and domestic
violence are clear examples of the health disparities affecting the Chicano/Latino
communities identified in the present research.
xv. Health Promotion and Disease Prevention
The quality and quantity of the information, education, prevention, and health promotion
provided to the Chicano/Latino population are disproportionately lower than those
provided to the mainstream community; the message is not reaching the people who need
it most.

100
III. Recommendations
From the process of this participatory research project, we have learned a broad number
of strategies to eliminate health disparities including the following:
a. Education
It is necessary to bridge the gap of education at different levels including: education
about health promotion, health care services, and how to navigate the health care system,
how find information about available health care providers, health care services and the
requirements to access. Adequate communication and culturally appropriate messages are
necessary to bridge the gap of awareness among Chicano/Latino communities in
Minnesota.
It is also essential to educate legislators through political action such as phone calls and
letters, and educating schools and agencies through diversity training.
Access to formal education for Chicano/Latino students is also recommended, including
opening opportunities to Chicano/Latino health professionals to validate their degrees.
Educating both professionals and patients to close the gap is suggested as well.

101
Educate immigrants about extreme weather conditions and how to protect themselves and
their families against the freezing temperatures in winter and sunburns and dehydration in
summer, and inform them regarding seasonal vaccines like the flu shot and locations
where they are available. Educating, informing, and providing access to seasonal
recreation programs in Minnesota is also recommended.
It is also important to educate the mainstream community and employers about the
Chicano/Latino communities’ rich culture and their contribution to the cultural diversity
and economic progress of Minnesota. Educating employers on how to improve job
conditions is also a key element to eliminate poverty in Minnesota.
b. Communication
A culturally competent, linguistically appropriate, permanent, and comprehensive
communication strategy is suggested. This includes making public campaigns, giving
complete and correct information, and answering questions from the communities that
would be complemented by appropriate channels of dissemination like churches,
community based Chicano/Latino organizations, Chicano/Latino media, television, local
radio, and face-to-face communication to reach illiterate populations, which suffer most
of the health disparities affecting our communities.

102
c. Health Insurance
Developing strategies is recommended to provide affordable health care insurance. It is
thought that solving the health insurance coverage would solve most of the health access
problems discussed.
d. Community Participation
The proposed recommendation is a proactive approach, in which the Chicano/Latino
communities undertake initiatives at the community level, developing health promotion
and intervention strategies as well as increasing awareness within the health system.
The recommendation also includes working in comprehensive strategies to improve the
quality of life of the Chicano/Latino communities in Minnesota in all the decision-
making levels from the state level to the community level. That includes political
participation, outreach health advocates, public forums, partnerships, research, and
changes in immigration laws, so that everyone who works will have insurance regardless
of their status.

103
e. Culturally Competent Health Care Services
To bridge the health disparities gap affecting the Chicano/Latino communities, the
recommendation is to increase the offer of culturally competent and linguistically
appropriate health care services. Change in office hours including services in Saturdays
and Sundays and extending the schedule to night hours, when parents have some time to
go the health care services especially in Greater Minnesota, is also proposed as part of the
solution.
Forming partnerships with organizations and health care networks is proposed as an
important alternative to provide information, health promotion, and social and health care
services to families and individuals in order to improve the use of existing resources like
networks, meetings, and gatherings. The development of such partnerships will
contribute to the improvement of the medical model, facilitating a friendlier and patient-
centered health care provider-patient relationship.
f. Community Based Participatory Research
Community participation in research is necessary to evaluate the progress made toward
eliminating health disparities affecting the Chicano/Latino communities in Minnesota.
Establishing measurable outcomes will facilitate determining whether a program is
working or not.

104
The recommendation is to focus on specific programs, areas, and organizations, and then
define priorities and evaluating tactics. The best community indicators should be few in
number, culturally relevant, and measurable.
The use of surveys or face-to-face interviews is suggested at community events,
churches, and clinics; surveying everyone connected to health issues and asking specific
questions to bring the necessary information useful to understand the problem and
relevant to eliminate health disparities.
Cooperation is needed with other existent efforts in the state to create a committee like
the Participatory Research Partnership (PRP) that collaborates with diverse groups
interested in solving this problem in partnership with community leaders. Also, a
participatory planning process is suggested, involving health care organizations, health
insurers, and communities to avoid loss of resources and duplication of services.
It is necessary to develop community teams to create strategies, use outreach advocates,
and home visits to monitor the pulse of the situation and together keep the problem and
possible ideas at the forefront. The “promotora” model is proposed to be implemented in
Minnesota to reach the Chicano/Latino communities.
Developing partnerships among community-based organizations is encouraged to identify
best practices. However, recruiting community members is discouraged unless something

105
beneficial is offered to their communities, because communities want to see tangible
benefits, not long-term outcomes.
Continuing and updating the participatory research led by a Chicano/Latino community
based organization working with the participants in the planning process to identify
health disparities indicators is encouraged.
Eliminating health disparities is a difficult task; there is some skepticism because there
are historical causes that have not been addressed. However, Chicano/Latino
communities are aware of the possibilities for developing key programs with
Chicano/Latino CBO to go to the roots of the problem and find together culturally
appropriate solutions for the health disparities described.
Finally, it is our recommendation to implement the solutions and recommendations
proposed in this report in existing and future health and social programs targeted to the
Chicano/Latino communities.
It is necessary to complement the clinical indicators, morbidity, mortality, and other
disease-based indicators with social community-developed indicators that make sense for
the people, in order to address in a culturally competent manner the gap in the quality of
life reflected in the health disparities affecting the Chicano/Latino communities.

106
Appendices

107
Appendix A
Survey Instrument
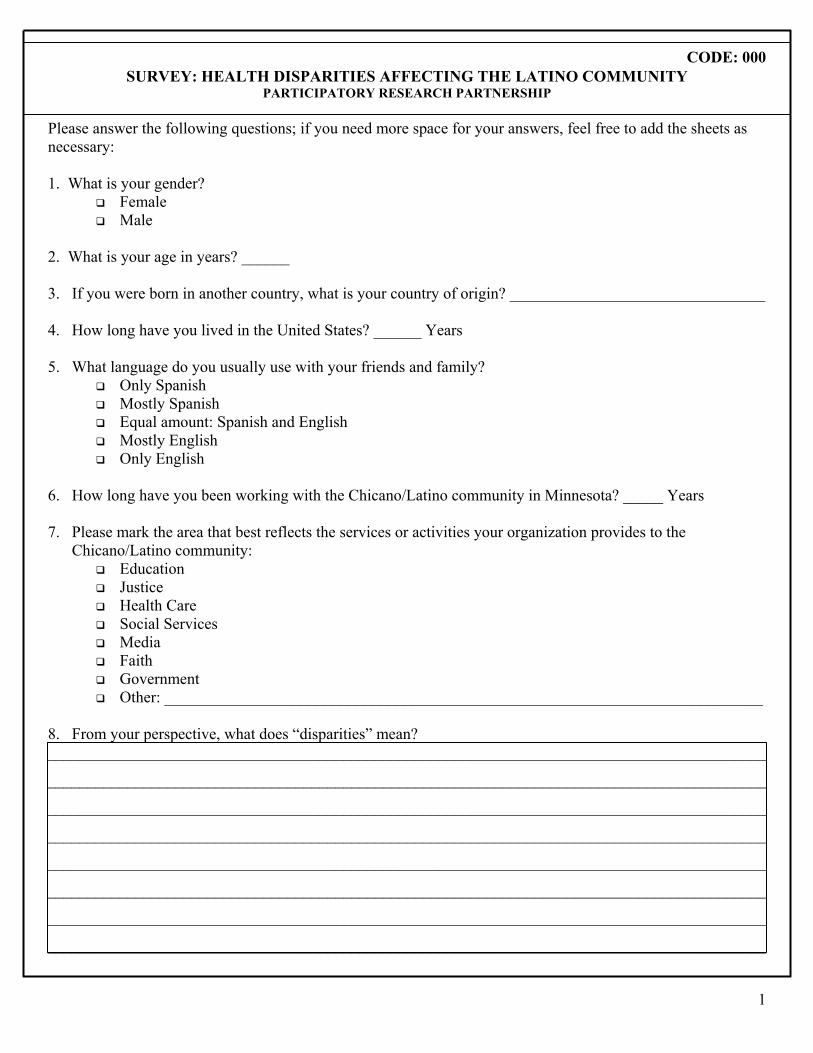
CODE: 000
1
SURVEY: HEALTH DISPARITIES AFFECTING THE LATINO COMMUNITY PARTICIPATORY RESEARCH PARTNERSHIP
Please answer the following questions; if you need more space for your answers, feel free to add the sheets as necessary: 1. What is your gender?
Female Male
2. What is your age in years? ______ 3. If you were born in another country, what is your country of origin? ________________________________ 4. How long have you lived in the United States? ______ Years 5. What language do you usually use with your friends and family?
Only Spanish Mostly Spanish Equal amount: Spanish and English Mostly English Only English
6. How long have you been working with the Chicano/Latino community in Minnesota? _____ Years 7. Please mark the area that best reflects the services or activities your organization provides to the
Chicano/Latino community: Education Justice Health Care Social Services Media Faith Government Other: ___________________________________________________________________________
8. From your perspective, what does “disparities” mean? __________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________

CODE: 000
2
9. How would you describe the health disparities affecting Chicanos/Latinos living in Minnesota? __________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
10. Is the Chicano/Latino community in Minnesota aware of the impact of health disparities on their families? __________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
11. What do you think are the causes of health disparities and other disparities affecting Chicanos/Latinos
living in Minnesota? __________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________

CODE: 000
3
12. What solutions would you propose to eliminate health disparities and other disparities affecting
Chicanos/Latinos in Minnesota? __________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
13. Please tell us your ideas for how we should engage organizations, individuals, families and communities in
identifying community indicators that could be used to monitor the progress that is being made toward eliminating health disparities affecting Chicanos/Latinos in Minnesota.
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
14. Would you be interested in participating in a participatory planning process for refining and expanding the
list of intermediate outcomes of health disparities affecting Chicanos/Latinos in Minnesota? Yes No
15. Please share any other comments, suggestions, or recommendations about this survey or this process. __________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Thank you very much. Please return this survey in the pre-paid envelope attached.

108
Appendix B
Literature Review

1-200.txt<1>Unique Identifier 14987176Authors Tang TS. Hernandez EJ. Adams BS.Institution Department of Medical Education, University of Michigan Medical School, Ann Arbor 48109, USA. [email protected] "Learning by teaching": a peer-teaching model for diversity training in medical school.Source Teaching & Learning in Medicine. 16(1):60-3, 2004 Winter.Abstract BACKGROUND: The sociocultural medicine teaching experience examines the viability and efficacy of a peer teaching model in enhancing diversity-focused attitudes, knowledge, and skills in medicine among advanced level medical students. DESCRIPTION: This experience recruited 4th year students to facilitate diversity-focused case-based discussions for 2nd year students. Peer teachers participated in a training session that addressed personal exploration of sociocultural background, health care disparities, biosociocultural aspects of the patient case, and facilitation skills. Evaluation assessed learning outcomes, teaching experience; and attitudes, knowledge, and skills related to sociocultural medicine. EVALUATION: Paired t tests revealed a greater understanding of the relation among sociocultural background, health, and medicine (p <.05), and greater proficiency with teaching sociocultural medicine topics to peers (p <.01). Overall, peer teachers agreed the experience increased their exposure to sociocultural factors in patient care, enhanced their case conceptualization skills, and encouraged them to consider personal belief systems. CONCLUSION: Findings suggest peer teaching can be an effective model to refine knowledge, attitudes, and skills related to diversity issues in health care. The model may be a viable approach for diversity training in graduate and continuing medical education.
<2>Unique Identifier 14672499Authors Gamst G. Aguilar-Kitibutr A. Herdina A. Hibbs S. Krishtal E. Lee R. Roberg R. Ryan E. Stephens H. Martenson L.Institution Department of Psychology, University of La Verne, 1950 Third St., La Verne, California 91750, USA. [email protected] Effects of racial match on Asian American mental health consumer satisfaction.Source Mental Health Services Research. 5(4):197-208, 2003 Dec.Abstract This study investigated the effects of consumer-provider racial match on consumer service satisfaction and treatment outcomes (i.e., Client Satisfaction Questionnaireand GAF-Posttest) of 96 outpatient consumers, 66 of whom were adults and 30 of whom were parent/caregivers of child consumers. Data was obtained by telephone interviewsover a 6-week period. After controlling for four other variables, client satisfaction was higher for racially matched consumers. Racially matched child consumers also had higher GAF-Posttest scores. Implications of these findings are discussed.
<3>Unique Identifier 14606201Authors Chesla CA. Fisher L. Skaff MM. Mullan JT. Gilliss CL. Kanter R.
Page 1

1-200.txtInstitution Department of Family Health Care Nursing, University of California at San Francisco, San Francisco, CA 94143-0606, USA. [email protected] Family predictors of disease management over one year in Latino and European American patients with type 2 diabetes.Source Family Process. 42(3):375-90, 2003 Fall.Abstract Family context is thought to influence chronic disease management but few studies have longitudinally examined these relationships. Research on families and chronic illness has focused almost exclusively on European American families. In this prospective study we tested a multidimensional model of family influence on disease management in type 2 diabetes in a bi-ethnic sample of European Americans and Latinos. Specifically, we tested how baseline family characteristics (structure, world view, and emotion management) predicted change in disease management over one year in 104 European American and 57 Latino patients with type 2 diabetes. We found that emotion management predicted change in disease management in both groups of patients as hypothesized, while family world view predicted change in both ethnic groups but in the predicted direction only for European Americans. Examining family context within ethnic groups is required to elucidate unique cultural patterns. Attending to culturally unique interpretations of constructs and measures is warranted. The import of family emotion management, specifically conflict resolution, in disease management deserves further study to support clinical intervention development. Examining multiple domains of family life and multidimensional health outcomes strengthens our capacity to develop theory about family contexts and individual health.
<4>Unique Identifier 14637290Authors Renzaho AM.Institution School of Health Sciences, Deakin University, Burwood, Vic. 3125, Australia. [email protected] Fat, rich and beautiful: changing socio-cultural paradigms associated with obesityrisk, nutritional status and refugee children from sub-Saharan Africa. [Review] [65 refs]Source Health & Place. 10(1):105-13, 2004 Mar.Abstract There has been an increase in Australia's intake of refugees and migrants from sub-Saharan Africa over the last two decades. These refugees have been exposed to nutritional risks prior to migration, which, together with changes associated with acculturation, impact on their health and nutritional status post-migration. However, there is a paucity of data in Australia that has examined the health and nutritional status of this ethnic minority in Australia. Despite basic research assessing the nutritional status of children, none have specifically concentrated onthe health and nutritional situation of sub-Saharan refugee children. In the absenceof such studies, this paper explores issues relating to obesity in sub-Saharan African refugee children within a cultural and public health framework. We begin by outlining the history of obesity and its cultural meaning. We then move to a consideration of predisposing factors for obesity and how these factors translate into obesity risk contexts of sub-Saharan refugees post-migration. We argue there are a number of key challenges related to culture and the relationship between socio-economic factors post-migration that require addressing by health professionals, dieticians and health educators to ensure the delivery of successful health outcomes. [References: 65]
Page 2

1-200.txt<5>Unique Identifier 14709192Authors Unson CG. Siccion E. Gaztambide J. Gaztambide S. Mahoney Trella P. Prestwood K.Institution Claude Pepper Older Americans Independence Center, UConn Center on Aging, University of Connecticut Health Center, Farmington, Connecticut 06030-6147, USA. [email protected] Nonadherence and osteoporosis treatment preferences of older women: a qualitative study.Source Journal of Women's Health. 12(10):1037-45, 2003 Dec.Abstract BACKGROUND: Physicians must have an understanding of patients' medication beliefs in order to enhance medication adherence. To increase understanding, this study examined how beliefs about medication and four osteoporosis treatments influenced treatment selection and adherence. METHODS: Six focus groups, three with 28 African Americans and one with 11 non-Hispanic white women, were conducted in English. Two groups with 16 Hispanics were conducted in Spanish. The convenience sample was recruited from senior centers and housing in lower socioeconomic geographic areas. The average age was 74.8 +/- 1.1 years. RESULTS: Adherence was associated with recognition of the serious consequences of nonadherence, realization of the beneficial effects, and the belief that medicines are not harmful. Doubts about physicians' competence to prescribe appropriate drugs were also revealed. Women who thought they were unlikely to fracture or perceived fracture outcomes as not severe chose no treatment. If they identified a need, they weighed benefits against the attendant risks to find the best alternative among the affordable options. Price considerations eliminated raloxifene and alendronate. Consideration of side effects eliminated estrogen and raloxifene. Calcium was viewed as a low-cost, low-risk alternative. Those who could afford alendronate and who viewed its side effects as preventable preferred it. Benefit and risk assessments may have been biased by fear of cancer and thromboembolic events. CONCLUSIONS: Women's beliefs about necessity oftreatment, medication safety, cost of treatment, and treatment goals appear criticalto osteoporosis treatment selection and adherence.
<6>Unique Identifier 14759940Authors Unger JB. Chou CP. Palmer PH. Ritt-Olson A. Gallaher P. Cen S. Lichtman K. Azen S. Johnson CA.Institution Transdisciplinary Tobacco Use Research Center, Department of Preventive Medicine, University of Southern California Keck School of Medicine, Los Angeles, 91803, USA. [email protected] Project FLAVOR: 1-Year Outcomes of a Multicultural, School-Based Smoking Prevention Curriculum for Adolescents.Source American Journal of Public Health. 94(2):263-5, 2004 Feb.Abstract To evaluate a multicultural smoking prevention curriculum, 16 schools were randomized to receive the multicultural curriculum or a standard curriculum and program effects on 1-year smoking initiation among 1430 never smokers were assessed.Hispanic boys who received the multicultural curriculum were less likely to initiatesmoking than were those who received the standard curriculum; effects were insignificant among other groups. The prevention effect among Hispanic boys is encouraging, but additional research is needed to improve prevention effects among other groups.
Page 3

1-200.txt
<7>Unique Identifier 14598996Authors Hecht ML. Marsiglia FF. Elek E. Wagstaff DA. Kulis S. Dustman P. Miller-Day M.Institution Department of Communication, Arts and Sciences, The Pennsylvania State University,University Park, Pennsylvania 16802, USA. [email protected] Culturally grounded substance use prevention: an evaluation of the keepin' it R.E.A.L. curriculum.Source Prevention Science. 4(4):233-48, 2003 Dec.Abstract This paper reports on the evaluation of a culturally grounded prevention intervention targeting substance use among urban middle-school students. The curriculum consists of 10 lessons promoting antidrug norms and teaching resistance and other social skills, reinforced by booster activities and a media campaign. Three versions were delivered: Mexican American, combined African American and European American, and Multicultural. Thirty-five middle schools were randomly assigned to 1 of the 3 versions or the control. Students completed baseline and follow-up questionnaires over a 2-year period (total 6,035 respondents). Analyses utilizing a generalized estimating equations approach assessed the overall effectiveness of cultural grounding and the cultural matching hypothesis. Support was found for the intervention's overall effectiveness, with statistically significant effects on gateway drug use as well as norms, attitudes, and resistance strategies but with little support for the cultural matching hypothesis. Specific contrasts found the Mexican American and Multicultural versions impacted the most outcomes.
<8>Unique Identifier 12850998Authors Jintrawet U. Harrigan RC.Institution Department of Pediatric Nursing, Faculty of Nursing, Chiang Mai University, ChiangMai, Thailand. [email protected] Beliefs of mothers in Asian countries and among Hmong in the United States about the causes, treatments, and outcomes of acute illnesses: an integrated review of theliterature. [Review] [21 refs]Source Issues in Comprehensive Pediatric Nursing. 26(2):77-88, 2003 Apr-Jun.Abstract An understanding of mothers' beliefs regarding the causes of illness, treatment, and outcome is an important component of culturally competent care. However, little is known about the beliefs of Asian parents related to acute illnesses. The purpose of our article is to synthesize what is known about the beliefs of mothers regardingthe causes, treatment, and outcome of acute illnesses in Asian countries and Hmong in the United States. The literature review covers the period from 1990-2000. The electronic bibliographic databases explored included Pub Med, MEDLINE, HealthSTAR, CINAHL, and PsycINFO. Keywords used were beliefs, health beliefs, mothers or parents, cause of illness or etiology, treatment, diarrhea, acute respiratory infection, measles, Asia, and Hmong. A total of 15 articles were retrieved and examined. Using the matrix method, each article was evaluated according to five frames of reference: journal, purpose, sample, method, and findings. Content analysis was used to generate themes. Expressions of belief related to the causes ofillnesses among mothers from Asian countries and Hmong who have emigrated from Laos
Page 4

1-200.txtto the United States of America were found to be quite similar. Beliefs about practices were primarily related to feeding and home care. The majority of mothers first provided treatment for their children using traditional practices. When the child did not recover, the mother sought medical advice. [References: 21]
<9>Unique Identifier 14768416Authors Wittig DR.Institution Department of Social Sciences, Gardner-Webb University, USA.Title Knowledge, skills and attitudes of nursing students regarding culturally congruentcare of Native Americans.Source Journal of Transcultural Nursing. 15(1):54-61, 2004 Jan.Abstract The provision of culturally congruent care for Native Americans can improve healthcare compliance and outcomes. The purpose of this survey was to determine the knowledge, skills, and attitudes students deem essential to provide culturally competent healthcare for Native American clients. This information provides nurse educators with critical information regarding the cultural competence of nursing students and may be used to direct curriculum development. An open-ended survey was administered to associate degree nursing students, and conceptual analysis was used for data analysis. The researcher identified four knowledge themes, two skill themes, and two attitude themes. These themes were interrelated and connected. Findings from this study indicate that the current nursing curriculum supports the development of cultural competence among the student nurses who will practice in a multicultural climate. Practice implications include the use of a cultural assessment tool by the students.
<10>Unique Identifier 14742109Authors Acharya PP. Alpass F.Institution School of Health Sciences, Massey University, Palmerston North, New Zealand. [email protected] Birth outcomes across ethnic groups of women in Nepal.Source Health Care for Women International. 25(1):40-54, 2004 Jan.Abstract This study was conducted at the Western Regional Hospital (WRH), Pokhara, Nepal. We investigated the relationship between selected socioeconomic variables, pregnancyindices, birth weight, and maternal health in women of different ethnic origins. In our cross-sectional data set, 29.8% of infants were born with a low birth weight. Our data analysis showed Indo-Aryan and lower caste ethnic groups had significantly lower weight babies than Tibeto-Burman and Newar groups. Further analysis showed that the Tibeto-Burman group received better care during pregnancy. Similarly, the Newar groups had significantly better nutritional intake than the Indo-Aryan and lower caste groups. The outcome of food restriction and antenatal care during pregnancy in specific ethnic groups has important implications for the health care delivery system. Health policymakers should target those ethnic groups and develop culturally based policies to reduce the incidence of low birth weight in Nepal.
<11>Unique Identifier
Page 5

1-200.txt 14617512Authors Burchard EG. Avila PC. Nazario S. Casal J. Torres A. Rodriguez-Santana JR. Toscano M. Sylvia JS. Alioto M. Salazar M. Gomez I. Fagan JK. Salas J. Lilly C. Matallana H. Ziv E. Castro R. Selman M. Chapela R. Sheppard D. Weiss ST. Ford JG. Boushey HA. Rodriguez-Cintron W. Drazen JM. Silverman EK. Genetics of Asthma in Latino Americans (GALA) Study.Institution University of California, San Francisco, 94143-0833, USA. [email protected] Lower bronchodilator responsiveness in Puerto Rican than in Mexican subjects with asthma.Source American Journal of Respiratory & Critical Care Medicine. 169(3):386-92, 2004 Feb1.Abstract In the United States, Puerto Ricans and Mexicans have the highest and lowest asthma prevalence, morbidity, and mortality, respectively. To determine whether ethnicity-specific differences in therapeutic response, clinical response, and/or genetic factors contribute to differences in asthma outcomes, we compared asthma-related clinical characteristics among 684 Mexican and Puerto Rican individuals with asthma recruited from San Francisco, New York City, Puerto Rico, and Mexico City. Puerto Ricans with asthma had reduced lung function, greater morbidity, and longer asthma duration than did Mexicans with asthma. Bronchodilator responsiveness, measured as percentage change from baseline FEV1, was significantly lower among Puerto Ricans with asthma than among Mexicans with asthma. Puerto Ricanswith asthma had on average 7.3% (95% confidence interval [CI], 4.6 to 9.9; p < 0.001) lower bronchodilator reversibility in FEV1, higher risk of an emergency department visit in the previous year (odds ratio, 2.63; 95% CI, 1.6 to 4.3; p < 0.001), and of previous hospitalization for asthma (odds ratio, 1.94; 95% CI, 1.2 to3.2; p = 0.009) than Mexicans. Subgroup analysis corroborated that Puerto Ricans with asthma had more severe disease than did Mexicans on the basis of lung function measurements, responsiveness to beta2-adrenergic agonists, and health care use. We conclude that Puerto Ricans with asthma respond less to albuterol than do Mexicans with asthma. These findings underscore the need for additional research on racial/ethnic differences in asthma morbidity and response to therapy.
<12>Unique Identifier 14687735Authors Vangen S. Johansen RE. Sundby J. Traeen B. Stray-Pedersen B.Institution Department of Obstetrics and Gynecology, the National Hospital, and Divison of Epidemiology, Norweigian Institute of Public Health, Oslo, Norway. [email protected] Qualitative study of perinatal care experiences among Somali women and local health care professionals in Norway.Source European Journal of Obstetrics, Gynecology, & Reproductive Biology. 112(1):29-35,2004 Jan 15.Abstract OBJECTIVE: To explore how perinatal care practice may influence labor outcomes among circumcised women. STUDY DESIGN: In-depth interviews were conducted with 23 Somali immigrants and 36 Norwegian health care professionals about their experiencesfrom antenatal care, delivery and the management of circumcision. RESULTS: Circumcision was not recognized as an important delivery issue among Norwegian health care professionals and generally the topic was not addressed antenatally. TheSomalis feared lack of experience and sub-optimal treatment at delivery. All of the women expressed a strong fear of cesarean section. Health care professionals were uncertain about delivery procedures for infibulated women and occasionally cesarean
Page 6

1-200.txtsections were performed in place of defibulation. CONCLUSION: We hypothesize that neglect of circumcision may lead to adverse birth outcomes including unnecessary cesarean sections, prolonged second stage of labor and low Apgar scores. We suggest that infibulated women need a carefully planned delivery, correctly performed defibulation and adequate pain relief.
<13>Unique Identifier 14646031Authors Shen J. Crane P. Gao S.Institution Division of Biostatistics, Indiana University School of Medicine, 1050 Wishard Boulevard, RG4101, Indianapolis, IN 46202, USA. [email protected] A latent variable model approach for assembling and scoring screening tests for dementia.Source Journal of Alzheimer's Disease. 5(5):399-407, 2003 Oct.Abstract In dementia studies, the diagnosis of dementia often relies on results of screening tests aimed at measuring various dimensions of cognitive functions. The current practice of scoring a screening test involves simply summing the correct responses from each item. However, this method may be imprecise and inefficient in the predictive power of the score for dementia. We propose a latent variable model approach for the scoring and item selection of such tests. We model the item responses to be random variables based on latent variables. We also model the disease outcomes to be a function of the latent variables. Maximum likelihood estimates are obtained by maximizing the joint likelihood functions of disease and the item responses over a specified distribution function for the latent variables. Variances of model parameters are estimated using a nonparametric bootstrap method. We illustrate the approach using a screening test for dementia from a community-based study.
<14>Unique Identifier 12937336Authors Gallagher-Thompson D. Coon DW. Solano N. Ambler C. Rabinowitz Y. Thompson LW.Institution Older Adult and Family Center, Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine and VA Palo Alto Health Care System, 795 Willow Road, mail code 182C/MP, Menlo Park, CA 94025, USA. [email protected] Change in indices of distress among Latino and Anglo female caregivers of elderly relatives with dementia: site-specific results from the REACH national collaborativestudy.Source Gerontologist. 43(4):580-91, 2003 Aug.Abstract PURPOSE: Few empirical studies have compared the efficacy between psychoeducational (skill-building) approaches for reducing caregivers' psychologicaldistress and interventions modeled after typical community-based support groups. We compare the impact of two distinct interventions on Anglo and Latino caregivers of elderly relatives with dementia. DESIGN AND METHODS: The change from preassessment to postassessment (baseline to 3 months) for 213 female caregivers (122 Anglo and 91Latino) is presented. They were seen weekly for 10 weeks in either the Coping With Caregiving psychoeducational program (instruction and practice in small groups to learn specific cognitive and behavioral skills) or in the Enhanced Support Group condition (guided discussion and empathic listening to develop reciprocal support within the group). Both programs were tailored to be sensitive to the cultural
Page 7

1-200.txtconcerns of Anglo and Latino caregivers, and they were delivered in either English or Spanish by trained interventionists. RESULTS: Overall, participants in the CopingWith Caregiving condition reported a significant reduction in depressive symptoms, increased use of adaptive coping strategies, and a trend toward decreased use of negative coping strategies when compared with those in the Enhanced Support Group condition. Results were similar for both ethnic groups: there were no main effects for ethnicity, and no significant ethnicity by treatment interaction effects. IMPLICATIONS: This study provides empirical support that female caregivers benefit more from a skill-building approach to managing their distress than from support group membership alone. We find it very encouraging that the Latino caregivers responded well on key outcome variables, suggesting that Latinos will participate inclinical research and will benefit from their involvement when services are providedto meet their specific needs.
<15>Unique Identifier 14672510Authors Vogel SA. Holt JK.Institution Department of Literacy Education, Northern Illinois University, DeKalb, Illinois 60115, USA.Title A comparative study of adults with and without self-reported learning disabilitiesin six English-speaking populations: what have we learned?.Source Dyslexia: the Journal of the British Dyslexia Association. 9(4):193-228, 2003 Nov.Abstract The purpose of this study was to compare adults with and without self-reported learning disabilities (SRLD and NSRLD) from six English-speaking populations including: English-speaking Canada, Great Britain, The Republic of Ireland, New Zealand, Northern Ireland, and the United States. These six populations were selected because they were all English-speaking populations, participated in the first administration of the International Adult Literacy Survey (IALS), and includedthe optional questions regarding the presence of a disability. In this study, we compared the groups on prevalence by population, percentage of each group by age andgender, awareness of learning disabilities and problems in school, document and quantitative literacy proficiency, educational attainment, reasons for dropping out of school, and employment, occupational and financial status. Findings were reportedamong these six populations within an historical perspective including differences in awareness and definition of learning disabilities, public policy, special education services, reading pedagogy, and teacher preparation. Recommendations are made for improving literacy and long-term outcomes for those with learning disabilities in all nations as well as future research directions.
<16>Unique Identifier 14566953Authors Roberts MC. Lazicki-Puddy TA. Puddy RW. Johnson RJ.Institution Clinical Child Psychology Program, University of Kansas, Lawrence, KS 66045, USA. [email protected] The outcomes of psychotherapy with adolescents: a practitioner-friendly research review. [Review] [45 refs]Source Journal of Clinical Psychology. 59(11):1177-91, 2003 Nov.Abstract This article summarizes the outcome findings of psychotherapy with adolescents
Page 8

1-200.txtthrough an examination of the research literature. In this problem-focused review ofthe research literature, we consider adolescent treatment of anxiety disorders, depression, eating disorders, disruptive behavior disorders, multiple problems of adolescence, and health risk behaviors. The evidence base for the effectiveness of various psychotherapies for adolescents is mixed. Psychotherapy in general has been a ripe field in which unsupported approaches have grown, and this is certainly true for psychotherapeutic interventions with adolescents. Nonetheless, there is a growing body of evidence to support various types of interventions as effective for different presenting problems. Researchers and clinicians need to recognize the complexity of the diverse characteristics of adolescents, including variations of culture, race, ethnicity, gender, class, physical disability, family definitions andconstellation, and sexual orientation. These require sensitivity, responsiveness, and competence by the therapist, but clinical research has not fully examined these considerations. Copyright 2003 Wiley Periodicals, Inc. [References: 45]
<17>Unique Identifier 14690991Authors Satterfield JM. Mitteness LS. Tervalon M. Adler N.Institution Division of General Internal Medicine, Department of Medicine, University of California, San Francisco, School of Medicine, USA. [email protected] Integrating the social and behavioral sciences in an undergraduate medical curriculum: the UCSF essential core.Source Academic Medicine. 79(1):6-15, 2004 Jan.Abstract Dramatic global-migration patterns over recent decades have forever changed the racial, ethnic, social, and cultural makeup of the people of the United States. Simultaneously, the patterns of disease and risk factor distribution within the U.S.population are changing in ways that accentuate the role of lifestyle, behavior, andsocial and economic differences in the onset and outcomes of disease. Medical schoolcurricula must prepare students to address these demographic realities. The University of California, San Francisco's (UCSF's) redesigned curriculum, launched in September 2001, integrates social, behavioral, and biomedical science education in an early and sustained way. The traditional undergraduate medical structure of two years of basic science plus two years of clinical rotations was replaced with a model divided into three stages spanning four years: the Essential Core, the Clinical Core, and Advanced Studies. The authors summarize the role of the social and behavioral sciences in the UCSF Essential Core-the first 16 months of instruction divided into integrated blocks, each centered on clinical cases. Basic thematic areas (e.g., behavior change, health disparities), content illustrations (e.g., Introduction to the Biopsychosocial Model, The Culture of Medicine), and process considerations (e.g., integration, content order, evaluations) are presented. Special challenges and limitations are also discussed.
<18>Unique Identifier 14726771Authors Van Cleve L. Bossert E. Beecroft P. Adlard K. Alvarez O. Savedra MC.Institution Loma Linda University School of Nursing, Loma Linda, California 92450, USA. [email protected] The pain experience of children with leukemia during the first year after diagnosis.Source Nursing Research. 53(1):1-10, 2004 Jan-Feb.
Page 9

1-200.txtAbstract BACKGROUND: Children with cancer experience pain related to the disease process, the treatment, and the associated procedures. For children with leukemia, the pain experienced after diagnosis has received scant attention. OBJECTIVE: To examine the pain experience, management strategies, and outcomes during the first year after thediagnosis of acute leukemia. METHODS: A longitudinal descriptive approach was used to collect data at seven data points from 95 English- and Spanish-speaking children,ages 4 to 17 years, receiving care in one of three southern California hospitals, and from their English- and Spanish-speaking parents. Age-appropriate instruments were used to examine the variables of pain intensity, location, pattern over time, and quality, as well as strategies for managing pain, perceived effectiveness of management strategies, and functional status. RESULTS: All the children reported pain over the course of the year. Pain intensity scores incorporated the full range of possible responses. For the children 4 to 7 years old, the highest and lowest mean scores, respectively, were 2 and 1.6 (scale, 0-4). For the children 8 to 17 years old, the highest and lowest mean scores, respectively, were 50.1 and 39.5 (scale, 0-100). The most common location of pain was the legs (26.5%) in all seven interviews. Other frequently noted sites were the abdomen (16.6%), head/neck (16.6%), and back (14.2%). The words used most frequently by the older English- and Spanish-speaking children to describe pain were "uncomfortable" (incomodo) and "annoying" (molesto). According to the interviews, the most frequently used strategyfor pain management was stressor modification (e.g., medication, sleep, hot/cold, and massage). The most common coping strategies according to a Likert scale rating were "watch TV" (n = 426), "lie down" (n = 421), "wish for it to go away" (n = 417),and "tell my mother or father" (n = 416). The pain intensity scores after pain management were significantly lower for the younger children in three of the seven interviews and for the older children in all seven interviews. For both the younger and older children, functional status (i.e., the ability to engage in routine activities) was above the median score at the seven interviews. CONCLUSIONS: Children with leukemia experience pain throughout the first year of treatment. In this study, the pain was responsive to the management strategies used by the parentsand children.
<19>Unique Identifier 14702583Authors Silver HJ. Wellman NS. Galindo-Ciocon D. Johnson P.Institution Vanderbilt Center for Human Nutrition, Vanderbilt University, Nashville, TN 37232-2713, USA. [email protected] Family caregivers of older adults on home enteral nutrition have multiple unmet task-related training needs and low overall preparedness for caregiving.Source Journal of the American Dietetic Association. 104(1):43-50, 2004 Jan.Abstract OBJECTIVES: We used stress process theory to identify family caregiving variables that are salient to the experience of managing older adults' home enteral nutrition.In this article, we describe the specific tasks family caregivers performed and their unique training needs in the context of caregiver preparedness, competence, effectiveness, and health care use. DESIGN: Hospital billing lists from two university-affiliated institutions in Miami, FL, were used to identify older adults who had enteral tubes placed over a 6-month period. Consent was obtained from those older adults discharged for the first time on home enteral nutrition and their family caregivers at the first scheduled outpatient visit. SUBJECTS/SETTING: In-homeinterviews were conducted with a diverse sample of 30 family caregivers (14 white, 8Hispanic, 7 African-American, 1 Asian) during their first 3 months (mean=1.83+/-0.69months) of home enteral nutrition caregiving. STATISTICAL ANALYSES PERFORMED: Descriptive statistics were used to summarize data for all variables; chi(2) analysis was conducted to analyze differences in categorical variables. One-way analysis of variance was used to analyze mean differences among caregivers grouped
Page 10

1-200.txtby ethnicity for total number of hours and tasks performed. Post hoc comparisons were conducted using the Tukey HSD test. The Spearman rho correlations were calculated to assess bivariate associations between quantitative variables. RESULTS:Caregivers reported providing from 6 to 168 hours of care weekly (mean=61.87+/-49.67hours), in which they performed an average of 19.73+/-8.09 caregiving tasks daily. Training needs identified were greatest for technical and nutrition-related tasks. Preparedness for caregiving scores were low (mean=1.72, maximum=4.0) and positively correlated with caregiver competence (P<.001) and self-rated caregiver effectiveness(P=.004). Preparedness negatively correlated with health care use (P=.03). CONCLUSIONS: Caregivers of older adults on home enteral nutrition need training for multiple nutrition-related and caregiving tasks. Multidisciplinary interventions, involving dietitian expertise, are needed to better prepare caregivers to improve both caregiver effectiveness and enteral nutrition outcomes.
<20>Unique Identifier 14746666Authors van Servellen G. Carpio F. Lopez M. Garcia-Teague L. Herrera G. Monterrosa F. Gomez R. Lombardi E.Institution Acute Care Section, UCLA, Los Angeles, California.Title Program to enhance health literacy and treatment adherence in low-income HIV-infected Latino men and women.Source AIDS Patient Care & Stds. 17(11):581-94, 2003 Nov.Abstract This paper reports the initial results of a pilot study to evaluate the acceptability and effectiveness of a program to enhance health literacy in low-income HIV-infected Latino men and women receiving antiretroviral therapy. Participants rated the program highly on measures of satisfaction, providing evidence of its acceptability. The effectiveness of the program was assessed in comparisons of the intervention (n = 41) and standard care only (n = 40) groups at baseline and 6-week intervals. Program participants showed significant improvement over comparison group participants on measures of HIV/AIDS and treatment-related knowledge and recognition and understanding of HIV terms. Although there were no significant changes in adherence mastery and behaviors during the 6-week follow up period, there were significant changes in program participants' knowledge about medication adherence. Future steps to examine the sustainability of the program in the medical management of patients are planned in addition to determining its long-range relative impact.
<21>Unique Identifier 14717414Authors Moy JA. McKinley-Grant L. Sanchez MR.Institution Department of Dermatology, New York University Medical Center, 560 First Avenue, Office H-100, New York, NY 10016, USA.Title Cultural aspects in the treatment of patients with skin disease. [Review] [69 refs]Source Dermatologic Clinics. 21(4):733-42, 2003 Oct.Abstract As the cultural distance between patient and physician widens, so does miscommunication. Negotiation between the belief systems of the physician and the patient may create a therapeutic environment of mutual trust and respect that increases the possibility of successful clinical outcomes. [References: 69]
Page 11

1-200.txt
<22>Unique Identifier 14717409Authors Sanchez MR.Institution Department of Dermatology, New York University School of Medicine, 560 First Avenue, Office H-100, New York, NY 10016, USA. [email protected] Cutaneous diseases in Latinos. [Review] [53 refs]Source Dermatologic Clinics. 21(4):689-97, 2003 Oct.Abstract The knowledge of many specific skin diseases that predominantly affect Latinos hasbeen increasing; however, the understanding of common skin disease in Latinos is superficial. There are few prospective studies done in the Latino population and none that differentiate between diverse Latino backgrounds. In view of the expandingLatino population in this country, such research is timely. [References: 53]
<23>Unique Identifier 14707754Authors Tennant A. Penta M. Tesio L. Grimby G. Thonnard JL. Slade A. Lawton G. Simone A. Carter J. Lundgren-Nilsson A. Tripolski M. Ring H. Biering-Sorensen F. Marincek C. Burger H. Phillips S.Institution Academic Unit of Musculoskeletal and Rehabilitation Medicine, University of Leeds,36 Clarendon Road, Leeds, LS2 9NZ, United Kingdom. [email protected] Assessing and adjusting for cross-cultural validity of impairment and activity limitation scales through differential item functioning within the framework of the Rasch model: the PRO-ESOR project.Source Medical Care. 42(1 Suppl):I37-48, 2004 Jan.Abstract INTRODUCTION: In Europe it is common for outcome measures to be translated for usein other languages. This adaptation may be complicated by culturally specific approaches to certain tasks; for example, bathing. In this context the issue of cross-cultural validity becomes paramount. OBJECTIVE: To facilitate the pooling of data in international studies, a project set out to evaluate the cross-cultural validity of impairment and activity limitation measures used in rehabilitation from the perspective of the Rasch measurement model. METHODS: Cross-cultural validity is assessed through an analysis of Differential Item Functioning (DIF) within the context of additive conjoint measurement expressed through the Rasch model. Data from patients undergoing rehabilitation for stroke was provided from 62 centers across Europe. Two commonly used outcome measures, the Mini-Mental State Examination(MMSE) and the Functional Independence Measure (FIM) motor scale are used to illustrate the approach. RESULTS: Pooled data from 3 countries for the MMSE were shown to fit the Rasch model with only 1 item displaying DIF by country. In contrast, many items from the FIM expressed DIF and misfit to the model. Consequently they were allowed to be unique across countries, so resolving the lack of fit to the model. CONCLUSIONS: Where data are to be pooled for international studies, analysis of DIF by culture is essential. Where DIF is observed, adjustmentscan be made to allow for cultural differences in outcome measurement.
<24>Unique Identifier 14632718
Page 12

1-200.txtAuthors Bachmann MO. Eachus J. Hopper CD. Davey Smith G. Propper C. Pearson NJ. Williams S. Tallon D. Frankel S.Institution Medical Research Council Health Services Research Collaboration, Department of Social Medicine, University of Bristol, Bristol, UK. [email protected] Socio-economic inequalities in diabetes complications, control, attitudes and health service use: a cross-sectional study.Source Diabetic Medicine. 20(11):921-9, 2003 Nov.Abstract AIMS: To investigate socio-economic inequalities in diabetes complications, and toexamine factors that may explain these differences. METHODS: Cross-sectional questionnaire survey of 770 individuals with diabetes among 40 general practices in Avon and Somerset. General practice, optometrist and eye hospital records over time (median 7 years) were analysed. Slope indices of inequality, odds ratios and incidence rate ratios were calculated to estimate the magnitude of inequality between the most and least educated, and the highest and lowest earning patients, adjusted for age, sex and type of diabetes, and clustering of outcomes within practices. RESULTS: The least educated patients were more likely than the most educated patients to have diabetic retinopathy [adjusted odds ratio (OR) 4.3; 95% confidence interval 0.8, 23.7] and heart disease (adjusted OR 3.6; 1.1, 11.8), had higher HbA1c levels (adjusted slope index of inequality 0.9; 0.3, 1.5), felt that diabetes more adversely affected their social and personal lives (adjusted slope index of inequality 0.8; 0.5, 1.1 Diabetes Care Profile units), were more likely to be recorded as non-compliant by their health professionals, and had lower rates of hospital attendance (adjusted rate ratio 0.43; 0.26, 0.71). However, they did not see themselves as less compliant, and had higher general practice attendance rates (adjusted rate ratio 1.5; 1.1, 2.2). CONCLUSIONS: Less educated and lower earning individuals with diabetes bear a larger burden of morbidity but use hospital care less. Health service resource allocation should reflect the distribution of chronic illness.
<25>Unique Identifier 14692068Authors Luna E.Institution New Mexico State University, USA.Title Las que curan at the heart of Hispanic culture. [Review] [50 refs]Source Journal of Holistic Nursing. 21(4):326-42, 2003 Dec.Abstract Bilingual nurse-curanderas are an emerging group of health care providers who blend the profession of nursing with Hispanic folk healing, thus providing culturally competent care to one of the largest growing minority groups in the United States. Nurse-curanderas integrate curanderismo (Hispanic folk healing) with allopathic health care, evaluate safety and efficacy, and implement appropriate interventions. This balance reduces cultural conflict and improves outcomes by increasing patient compliance with the treatment regimen. A Spanish-English glossaryof terms used is included. [References: 50]
<26>Unique Identifier 14692176Authors Tsai JH.Institution
Page 13

1-200.txt School of Nursing, Seattle University, University of Washington, Seattle, Washington, USA. [email protected] Contextualizing immigrants' lived experience: story of Taiwanese immigrants in theUnited States.Source Journal of Cultural Diversity. 10(3):76-83, 2003 Fall.Abstract Immigration involves extensive changes in living environments. Nonetheless, the predominant approach in the health science literature has been to utilize individualcharacteristics (including ethnic background) to explain and predict immigrants' lived experiences and health outcomes. Contexts, particularly the larger societal contexts by which immigrants are constituted, are generally ignored. Data from a critical ethnography regarding immigrants' experiences with language, occupation, and economic survival in the United States are utilized to illustrate that immigrants' lives are inseparable from the larger societal contexts, such as immigration policy, Western imperialism, and structural discrimination. The implications for practice, education, and research are discussed.
<27>Unique Identifier 12943561Authors Pomerleau J. McKee M. Lobstein T. Knai C.Institution European Centre on Health of Societies in Transition, London School of Hygiene andTropical Medicine, Keppel Street, WC1E 7HT, UK. [email protected] The burden of disease attributable to nutrition in Europe.[see comment]. [Review] [76 refs]Source Public Health Nutrition. 6(5):453-61, 2003 Aug.Abstract OBJECTIVE: This review examines the extent to which differences in nutrition couldexplain the diversity of health in Europe and how dietary patterns might contribute to the overall burden of disease in the region. SETTING: Europe. DESIGN: Between-country variations and time trends in dietary and health patterns in Europe are described, taking into account recent evidence on east-west mortality differentials. Existing information on the contribution of dietary factors to the overall burden of disease in Europe and to the burden of cardiovascular diseases andcancer is then reviewed, including a discussion of the methodological challenges that face those seeking to quantify this burden accurately. RESULTS: While evidence from ecological data have long suggested that variations in health patterns in Europe may be at least partly attributed to differences in dietary intake, recent research into the major risks to disease, disability and death is confirming the importance of poor nutrition to major health problems and overall disease burden in Europe. Findings from the Global Burden of Disease 2000 study suggest that 4.4% of the overall burden of disease in the region could be attributed to low fruit and vegetable intake, and 7.8% to overweight and obesity. CONCLUSIONS: The burden of disease attributed to poor nutrition in Europe appears to be substantial and probably underestimated. However, better quantification of the contribution of nutrition to the region's burden of disease awaits further research to assess the dietary intake of Europeans and to explore the relationship between nutritional factors and health outcomes in diverse parts of Europe. [References: 76]
<28>Unique Identifier 14671231Authors Chamorro A. Planas AM.Title
Page 14

1-200.txt Yin and yang of uric acid in patients with stroke.[comment].Source Stroke. 35(1):e11-2; author reply e11-2, 2004 Jan.
<29>Unique Identifier 14634679Authors Poston WS. Reeves RS. Haddock CK. Stormer S. Balasubramanyam A. Satterwhite O. Taylor JE. Foreyt JP.Institution Mid America Heart Institute and University of Missouri-Kansas City, Kansas City, MO 64110, USA. [email protected] Weight loss in obese Mexican Americans treated for 1-year with orlistat and lifestyle modification.Source International Journal of Obesity & Related Metabolic Disorders: Journal of the International Association for the Study of Obesity. 27(12):1486-93, 2003 Dec.Abstract OBJECTIVE: To evaluate the effectiveness of a culturally appropriate lifestyle intervention combined with orlistat in producing weight loss with obese Mexican-American women. SUBJECTS: Mexican-American women (N=108), aged 21-65 y, witha body mass index (BMI) > or =27 kg/m(2) were randomized to 1 y of treatment with orlistat and a culturally tailored lifestyle modification intervention (OLM; n=56) or a wait-list control group (WLC; n=52). DESIGN: A randomized, controlled, open-label 12-month study. Orlistat was dosed at 120 mg, three times per day. The OLM intervention included behavior modification, a low-fat (< or =30% of total dailycalories) diet, and moderate physical activity (> or =150 min/week). MEASUREMENT: Primary outcomes included changes in body weight (kg), BMI, waist circumference, blood pressure, glucose, and lipids. RESULTS: A total of 72 (37 OLM, 35 WLC) and 66 participants (32 OLM, 34 WLC) completed the 6- and 12-month follow-ups, respectively. Repeated-measures ANOVA demonstrated a significant time x treatment interaction (Wilks' lambda=12.61; P<0.001), indicating that OLM-treated patients achieved significant weight loss relative to the WLC group during the study (mean percentage weight loss+/-s.e.m.; -8.1%+/-1.2 vs -1.6%+/-0.7 at 6 months and -8.8%+/-1.5 vs -0.2%+/-1.0 at 12 months, respectively). OLM-treated patients also experienced significant reductions in waist circumference, low-density-lipoprotein, and total cholesterol. CONCLUSIONS: This study demonstrates the effectiveness of an intervention combining orlistat and lifestyle modification with Mexican-American women, a population with substantial risk for obesity.
<30>Unique Identifier 14655523Authors Huang TT. Goran MI.Institution Energy Metabolism Laboratory, Jean Mayer USDA Human Nutrition Research Center, Tufts University, Boston, USA.Title Prevention of type 2 diabetes in young people: a theoretical perspective. [Review][214 refs]Source Pediatric Diabetes. 4(1):38-56, 2003 Mar.Abstract Type 2 diabetes in youth is an increasing public health concern, especially in certain minority populations. The current paper consists of four sections. First, weestablish the significance of the problem by presenting an overview of epidemiological and physiological evidence. Second, we discuss behavioral issues relevant to the prevention of type 2 diabetes in youth. Third, a qualitative review
Page 15

1-200.txtof existing prevention interventions specific to type 2 diabetes in youth is presented. Results suggest that modest improvements in social cognitive, dietary, and exercise outcomes are possible with diabetes intervention studies, although beneficial changes are difficult to sustain over the long term. Although theoreticalframeworks are not always explicit, most studies have utilized elements of the social cognitive theory. Less attention has been paid to sociocultural and communityorganization variables. Finally, the paper discusses issues of risk definition and intervention sustainability, and presents a comprehensive, theoretically diverse model for the prevention of type 2 diabetes in youth. In summary, we suggest that theories of the natural history and pathophysiology of type 2 diabetes are importantto identify modifiable risk factors, while theories of behavioral change are essential to modify the risk factors identified. The combination of sound physiological and behavioral theories should form the basis of prevention intervention design. In addition, an ecologic approach that takes into considerationthe dynamic interactions of personal, social, and environmental factors would best promote the long-term adoption of healthful behaviors in a supportive, meaningful, and personally enjoyable context. [References: 214]
<31>Unique Identifier 14655519Authors Gallegos-Macias AR. Macias SR. Kaufman E. Skipper B. Kalishman N.Institution Department of Family and Community Medicine, University of New Mexico School of Medicine, New Mexico, USA.Title Relationship between glycemic control, ethnicity and socioeconomic status in Hispanic and white non-Hispanic youths with type 1 diabetes mellitus.Source Pediatric Diabetes. 4(1):19-23, 2003 Mar.Abstract OBJECTIVES: To determine if there is a disparity in glycemic control between Hispanic and white non-Hispanic children and adolescents with type 1 diabetes mellitus (DM) and to delineate the factors associated with glycemic control in thesepopulations. STUDY DESIGN: This cross-sectional study included 183 youths with type 1 DM (99 white non-Hispanics and 84 Hispanics) and their parents/guardians cared forin a well-defined, private pediatric endocrine diabetes clinic, where the same physician and diabetes educators treat all patients. The youths were invited to participate if they had been diagnosed with diabetes at least 3 months before the study and were < 21 yr of age. Self-report questionnaires and chart reviews were used to assess individual familial and sociodemographic variables. OUTCOMES MEASURED: Mean hemoglobin A1c (HbA1c) levels, compliance with home monitoring of blood sugar, level of parental supervision of treatment, and socioeconomic status ofHispanic and white non-Hispanic families in the study. RESULTS: Hispanic youths withtype 1 DM were in poorer metabolic control than their white non-Hispanic counterparts (0.45% difference in HbA1c levels, p = 0.02). Hispanic youths exhibitedlower compliance with home monitoring of blood sugar but their parents reported greater supervision of their diabetes treatment. Hispanic families were found to have significantly lower income, rate of health insurance, father's educational attainment, and mother's educational attainment. Lower family socioeconomic status, but not ethnicity or educational attainment of parents, was associated with a significantly higher HbA1c, regardless of ethnicity. CONCLUSIONS: This study suggests that Hispanic youths with type 1 diabetes may be at greater risk for poor glycemic control because of their lower socioeconomic status rather than their ethnicity.
<32>Unique Identifier 14659379Authors
Page 16
1-200.txt Lee MS. Jang JW. Jang HS. Moon SR.Institution Center for Integrative Medicine, Institute of Medical Science, Wonkwang University, Iksan, South Korea.Title Effects of Qi-therapy on blood pressure, pain and psychological symptoms in the elderly: a randomized controlled pilot trial.Source Complementary Therapies in Medicine. 11(3):159-64, 2003 Sep.Abstract Recently, we reported that Qi-therapy may be beneficial in reducing negative psychological symptoms and increasing melatonin levels, neutrophil function and natural killer cell cytotoxicity in young subjects. However, there is little scientific evidence of its efficacy in elderly subjects. Therefore, this study was designed to investigate the effects of Qi-therapy on anxiety, depression, fatigue, pain and blood pressure in elderly subjects. Ninety-four elderly subjects were randomly assigned to either Qi-therapy (n=47) or mimic therapy (n=47) groups. Both groups received a 10-min intervention period once using similar procedures. The Qi-therapy group exhibited greater reduction in anxiety, depression, fatigue, pain level and blood pressure compared to the placebo group; the difference in anxiety was significant (P=0.014). These results suggest that even a brief application of Qi-therapy may exert a positive psychological and physiological effect. However, further research is necessary in order to fully understand the long-term impact of Qi-therapy on psychological health and the cardiovascular system.
<33>Unique Identifier 12936700Authors Pongjaturawit Y. Harrigan RC.Institution Faculty of Nursing, Chiang Mai University, Thailand. [email protected] Parent participation in the care of hospitalized child in Thai and Western cultures. [Review] [20 refs]Source Issues in Comprehensive Pediatric Nursing. 26(3):183-99, 2003 Jul-Sep.Abstract This integrated literature review provides state-of-the-science information regarding parent participation in the care of hospitalized child. The database search revealed only 12 articles on this subject published between 1996-2002. Ganong's (1987) integrative research review process guided this study, and the matrix method of Garrard (1999) was modified to develop the data collection tool. The rules of inference for data analysis and interpretation were identified. Research outcomes were systematically analyzed and reported using a qualitative descriptive approach. Three major themes emerged from the investigation: parents, nurses, and child care interactions. As there were both similar and different findings between Thai and Western cultures, cultural differences regarding parent participation in the care of hospitalized child must be considered in future investigations. Because cultural competence in parent participation has not been well addressed in the literature, further research is needed to delineate the cultural underpinnings of parent participation in the care of hospitalized child. [References: 20]
<34>Unique Identifier 14672486Authors Ickovics JR. Kershaw TS. Westdahl C. Rising SS. Klima C. Reynolds H. Magriples U.Institution
Page 17

1-200.txt Department of Epidemiology and Public Health, Yale University School of Medicine, New Haven, Connecticut 06520-8034, USA. [email protected] Group prenatal care and preterm birth weight: results from a matched cohort study at public clinics.Source Obstetrics & Gynecology. 102(5 Pt 1):1051-7, 2003 Nov.Abstract OBJECTIVE: To examine the impact of group versus individual prenatal care on birthweight and gestational age. METHODS: This prospective, matched cohort study includedpregnant women (N = 458) entering prenatal care at 24 or less weeks' gestation; one half received group prenatal care with women of the same gestational age. Women werematched by clinic, age, race, parity, and infant birth date. Women were predominantly black and Hispanic of low socioeconomic status, served by one of threepublic clinics in Atlanta, Georgia or New Haven, Connecticut. RESULTS: Birth weight was greater for infants of women in group versus individual prenatal care (P < .01).Among those born preterm, infants of group patients were significantly larger than infants of individual-care patients (mean, 2398 versus 1990 g, P < .05). Although not statistically significant, infants of group patients were less likely than thoseof individual-care patients to be low birth weight (less than 2500 g; 16 versus 23 infants); very low birth weight (less than 1500 g; three versus six infants); early preterm (less than 33 weeks; two versus seven infants); or to experience neonatal loss (none versus three infants). There were no differences in number of prenatal visits or other risk characteristics (patient age, race, prior preterm birth). CONCLUSIONS: Group prenatal care results in higher birth weight, especially for infants delivered preterm. Group prenatal care provides a structural innovation, permitting more time for provider-patient interaction and therefore the opportunity to address clinical as well as psychological, social, and behavioral factors to promote healthy pregnancy. Results have implications for design of sustainable prenatal services that might contribute to reduction of racial disparities in adverse perinatal outcomes.
<35>Unique Identifier 14628325Authors Stacy C.Institution Michigan Health Council, Okemos, USA. [email protected] Michigan hospitals and kids SCORE big.Source Michigan Health & Hospitals. 39(6):16, 2003 Nov-Dec.Abstract The Michigan Health Council, in cooperation with four Michigan hospital systems, initiated Strive for Challenging Outcomes and Reach Excellence (SCORE) to develop a more diverse health care work force for Michigan. This project is aimed at helping minorities and underrepresented youth learn about careers in health care and helpinghospitals get started toward building diversity programs in their communities.
<36>Unique Identifier 14617958Authors Pinquart M. Sorensen S. Davey A.Institution Department of Development Psychology, University of Jena, Am Steiger 3 Haus 1, 07743 Jena, Germany.Title National and regional differences in preparation for future care needs: a comparison of the United States and Germany.
Page 18

1-200.txtSource Journal of Cross-Cultural Gerontology. 18(1):53-78, 2003 Mar.Abstract Planning for future care needs is likely to be influenced by both policy and culture. We compared attitudes regarding the usefulness of planning ahead for futurecare needs, processes of preparation for these needs (becoming aware of the risk of future care needs, gathering information about available options, deciding on preferences, concrete planning), and outcomes of preparation (e.g., knowledge about services) in 294 East German, 288 West German, and 590 American seniors. American respondents had higher preparation scores. Compared to the size of national differences, differences between East and West German seniors were generally smaller. East Germans made fewer decisions on preferences and engaged in less concrete planning. Most of the national and regional differences in preparation for future care needs were reduced or eliminated by controlling for differences in the perceived usefulness of planning.
<37>Unique Identifier 14510096Authors Matias-Carrelo LE. Chavez LM. Negron G. Canino G. Aguilar-Gaxiola S. Hoppe S.Institution Graduate School of Public Health, Medical Sciences Campus, University of Puerto Rico, San Juan, Puerto Rico.Title The Spanish translation and cultural adaptation of five mental health outcome measures.Source Culture, Medicine & Psychiatry. 27(3):291-313, 2003 Sep.Abstract In this paper we report on the process of translating five mental health outcome measures into Spanish and adapting them to Latino culture. The instruments considered are the World Health Organization-Disability Assessment Scale, the BurdenAssessment Scale, the Family Burden Scale, Lehman's Quality of Life Interview and the Continuity of Care in Mental Health Services Interview. A systematic process of translation and adaptation of the instruments was followed with the goal of achieving cultural equivalence between the English and Spanish versions of the instruments in five dimensions: semantic, content, technical, construct, and criterion equivalence. In this paper we present data about the semantic, content, and technical equivalence. Various steps were taken to achieve equivalence in these dimensions, including the use of a bilingual committee, a multi-national bilingual committee, back-translation, and focus groups with mental health patients and their relatives.
<38>Unique Identifier 14629679Authors Ohm R.Institution University of Kansas, Baker University School of Nursing, Topeka, Kansas 66604, USA. [email protected] The Arican American experience in the Islamic faith.Source Public Health Nursing. 20(6):478-86, 2003 Nov-Dec.Abstract Disparity of health outcomes has been identified as a key concern in the health ofAmericans. Marginalization of the African American population may be a contributing factor. Identification of health protectors may prove key in decreasing disparities.The effect of spirituality on health is discussed. A historical overview of the
Page 19
1-200.txtAfrican American experience in the Islam faith, from the Nation of Islam to universal Islam, is presented. A systematic assessment of the Islamic faith, with emphasis on the African American Muslim, was conducted as an assessment for a Community Health Nursing class. Leininger's Sunrise Model of Culture Care Diversity and Universality, with the ethnonursing model of data collection, served as the framework for data collection and analysis. The Islamic faith was noted to offer holistic direction for a "way of life" that promotes health and harmony of the mind,body, and soul. Implications for research were discussed.
<39>Unique Identifier 14518800Authors Gitlin LN. Belle SH. Burgio LD. Czaja SJ. Mahoney D. Gallagher-Thompson D. Burns R. Hauck WW. Zhang S. Schulz R. Ory MG. REACH Investigators.Institution Community and Homecare Research Division, Thomas Jefferson University, Philadelphia, Pennsylvania 19107, USA. [email protected] Effect of multicomponent interventions on caregiver burden and depression: the REACH multisite initiative at 6-month follow-up.Source Psychology & Aging. 18(3):361-74, 2003 Sep.Abstract Meta-analysis was used to examine pooled parameter estimates of 9 active compared with 6 control conditions of the Resources for Enhancing Alzheimer's Caregiver Health (REACH) project at 6 months on caregiver burden and depressive symptoms. Associations of caregiver characteristics and outcomes were examined. For burden, active interventions were superior to control conditions (p = .022). Also, active interventions were superior to control conditions for women versus men and for caregivers with lower education versus those with higher education. For depressive symptoms, a statistically significant association of group assignment was found for Miami's family therapy and computer technology intervention (p = .034). Also, activeinterventions were superior to control conditions for Hispanics, nonspouses, and caregivers with lower education. Results suggest interventions should be multicomponent and tailored.
<40>Unique Identifier 12971816Authors Laing SP.Institution University of Alabama, Speech and Hearing Center, #7 Rowand Johnson Hall, Tuscaloosa, AL 35487-0242, USA. [email protected] Assessment of phonology in preschool African American Vernacular English speakers using an alternate response mode.Source American Journal of Speech-Language Pathology. 12(3):273-81, 2003 Aug.Abstract The purpose of this study was to determine whether an adapted stimulus elicitationformat would reduce the amount of final consonant absence in African American Vernacular English (AAVE) speakers and to determine the extent to which the adapted and standard response formats would differ in their predictions of membership in a delayed and a typical group. Findings revealed that the alternate response mode resulted in statistically significant decreases in the use of final consonant absence and that it was less likely than the standard response mode to penalize the AAVE speaker to a degree that was clinically significant.
Page 20

1-200.txt<41>Unique Identifier 12721705Authors Offenbacher M. Ewert T. Sangha O. Stucki G.Institution Klinik und Poliklinik, fur Physikalische Medizin und Rehabilitation, Ludwig-Maximilian Universitat, Munchen Marchioninistr. 15 81377 Munich, Germany.Title Validation of a German version of the 'Disabilities of Arm, Shoulder and Hand' questionnaire (DASH-G).Source Zeitschrift fur Rheumatologie. 62(2):168-77, 2003 Apr.Abstract OBJECTIVE: In 1994 the American Academy of Orthopedic Surgeons' outcome research committee developed and validated a functional outcome questionnaire for disabilities of the upper extremity (DASH). The objective of our study was to translate the DASH into German and to evaluate its reliability and validity for German-speaking patients with shoulder pain. METHODS: Translation-backtranslation ofthe DASH was performed according to published guidelines. Psychometric properties and validity were assessed in 49 consecutive patients with shoulder pain originatingfrom within the shoulder girdle. Age, duration of symptoms and current pain were obtained. Test-retest reliability was assessed in a subset of 18 patients who filledin the questionnaire 10 days later. Internal consistency was evaluated with Cronbach's alpha coefficient. Test-retest reliability was assessed using Spearman correlations and the Bland and Altman plot. To study the validity, we examined the correlation of the DASH with other measures of function of the upper extremity including the HAQ subscales relating to the upper extremity and pain measures (e.g. numerical rating scale, SF-36 pain scale). We also examined our hypothesis that the DASH is moderately correlated with measures of range-of-motion (e.g., forward flexion and abduction). RESULT: Translation-backtranslation revealed no major difficulties. The mean age of the patients was 59 years, mean duration of symptoms 60 months and current pain score 5.6 (NRS). Test-retest reliability was 0.90 for thetotal DASH. The internal consistency was 0.96. Strong correlations (p<0.01) were found between the DASH and the mean among the five subscales of the HAQ representingupper extremity function (0.88) and pain as measured with the SF-36 bodily pain scale (-0.79). As hypothesized, the DASH was also moderately correlated with measures of range-of-motion (e.g. forward flexion rho=-0.49; abduction rho=-0.57). CONCLUSION: Our data confirm that the German version of the DASH retains the characteristics of the American original and is a reliable and valid instrument to measure functional disability in German speaking patients with shoulder pain.
<42>Unique Identifier 14682338Authors Ryan J.Title Sailing SCHIP through troubled waters.Source NHPF Issue Brief. (795):1-7, 2003 Nov 13.Abstract As the State Children's Health Insurance Program (SCHIP) enters its sixth year of operation, states have continued their commitment to children's coverage and to reaching out to the uninsured. This issue brief explores the current status of SCHIPin light of fiscal pressures that have been created by the state budget crisis. It highlights some of the key successes in the program thus far and notes several examples of state initiatives to serve particularly vulnerable populations and collect outcomes data and information about access to care.
<43>Page 21

1-200.txtUnique Identifier 13678228Authors Hikiami H. Goto H. Sekiya N. Hattori N. Sakakibara I. Shimada Y. Terasawa K.Institution Department of Japanese Oriental (Kampo) Medicine, Faculty of Medicine, Toyama Medical and Pharmaceutical University, Sugitani, Toyama, Japan. [email protected] Comparative efficacy of Keishi-bukuryo-gan and pentoxifylline on RBC deformabilityin patients with "oketsu" syndrome.Source Phytomedicine. 10(6-7):459-66, 2003.Abstract Keishi-bukuryo-gan (Gui-Zhi-Fu-Ling-Wan) (KBG) is one of the prescriptions in Japanese traditional medicine for improving the "oketsu" syndrome, so-called blood stasis syndrome. "Oketsu" syndrome is an important pathological conception in Japanese traditional medicine and often accompanies cerebro-vascular disorders. Previously, we were able to reveal a deterioration of RBC (Red blood cell) deformability and viscoelasticity in patients with "oketsu" syndrome. The purpose ofthe present study was to evaluate whether KBG has an effect on RBC deformability in comparison with pentoxifylline (PXF). The subjects were 30 male patients with multiple lacunar infarctions. Eighteen patients (44-79 yrs, mean +/- SD, 66.1 +/- 10.7 yrs) were treated with 12 g of KBG daily for 4 weeks (KBG group). Twelve patients (59-78 yrs, 70.7 +/- 6.4 yrs) were treated with 300 mg of PXF daily for 4 weeks (PXF group). Based on the "oketsu" score, the patients of each group were divided into two subgroups, a non-"oketsu" group ("oketsu" score 20 points or less) and an "oketsu" group ("oketsu" score 21 points or higher). KBG had significant effects on RBC deformability as evaluated by filtration method. KBG also significantly increased intracellular ATP content, as did PXF. Moreover, KBG was more effective for patients with a more severe "oketsu" state. However, PXF was effective only in patients with "oketsu" syndrome, who might have deteriorated RBC deformability. In conclusion, the effect of KBG on RBC deformability was by no meansinferior to PXF.
<44>Unique Identifier 12707700Authors Daffertshofer M. Grips E. Dempfle CE. Hennerici M.Institution Neurologische Klinik, Universitatsklinikum Mannheim, Ruprecht-Karls-Universitat, Heidelberg. [email protected] [Heparin during acute ischemic stroke. Present data and clinical situation]. [Review] [71 refs] [German]Source Nervenarzt. 74(4):307-19, 2003 Apr.Abstract Therapy with low- or high-dose heparin in acute stroke is changing. Despite several clinical studies (>20), some with quite large numbers of patients, no statistically significant benefit was found for the clinical endpoints of death and functional outcome. This negative result remains even when considering the preventive effect of high-dose heparin on secondary acute embolic events (e.g., cardiac emboli-arrhythmia) and low-dose heparin on venous thrombosis. Based on studyresults, most reviews and therapy recommendations for the treatment of acute stroke generally decline the use of high-dose heparins and heparinoids with full anticoagulation for improving outcome or preventing secondary embolic events as wellas low-dose applications for venous thrombosis prophylaxis. This paper reviews the literature and presents the data of a standardised survey on coagulation therapy in acute stroke patients from all university and major stroke units in Germany (n=33). Contrary to the restrictive recommendations, therapy with heparin is firmly
Page 22

1-200.txtestablished in most stroke units. Full anticoagulation with heparin ("full dose") isperformed on selected patients in 32/33 stroke units (97%). The selection criteria and thus the frequency of high-dose heparin use varies widely among the different centers. Almost all German stroke units (97%) routinely use low-dose heparin to prevent venous thrombosis and pulmonary embolism.The heparin agents and dosage, however, vary. These data correspond to those from the USA and Canada,where daily routine also departs from evidence-based treatment recommendations. That may be due to individual pathophysiological and aetiological considerations and of course the low acceptance of treatment recommendations based on classic, randomised trials. This underlines the need for new concepts (e.g.observational trials, continuous registers, etc.) addressing the adaptation of study-related conditions to the much more complex situation of daily routine (with risk/benefit, safety, and economic variables). [References: 71]
<45>Unique Identifier 14654674Authors Shone LP. Dick AW. Brach C. Kimminau KS. LaClair BJ. Shenkman EA. Col JF. Schaffer VA. Mulvihill F. Szilagyi PG. Klein JD. VanLandeghem K. Bronstein J.Institution Strong Children's Research Center, Department of Pediatrics, University of Rochester School of Medicine and Dentistry, Rochester, New York 14642, USA. [email protected] The role of race and ethnicity in the State Children's Health Insurance Program (SCHIP) in four states: are there baseline disparities, and what do they mean for SCHIP?.Source Pediatrics. 112(6 Pt 2):e521, 2003 Dec.Abstract BACKGROUND: Elimination of racial and ethnic disparities in health has become a major national goal. The State Children's Health Insurance Program (SCHIP) has the potential to reduce disparities among the children who enroll if they exhibit the same disparities that have been documented in previous studies of low-income children. To determine the potential impact of SCHIP on racial and ethnic disparities, it is critical to assess baseline levels of health disparities among children enrolling in SCHIP. OBJECTIVE: To use data from the Child Health Insurance Research Initiative (CHIRI) to 1) describe the sociodemographic profile of new enrollees in SCHIP in Alabama, Florida, Kansas, and New York; 2) determine if there were differences in health insurance and health care experiences among white, black,and Hispanic SCHIP enrollees before enrollment in SCHIP; and 3) explore whether raceor ethnicity, controlled for other factors, affected pre-SCHIP access to health coverage and health care. SETTING: SCHIP programs in Alabama, Florida, Kansas, and New York, which together include 26% of SCHIP enrollees nationwide. DESIGN: Telephone interview (mailed survey in Alabama) about the child's health, health insurance, and health care experiences conducted shortly after SCHIP enrollment to assess experience during the time period before SCHIP. SAMPLE: New SCHIP enrollees (0-17.9 years old in Alabama, Kansas, and New York and 11.5-17.9 years old in Florida). Stratified sampling was performed in Kansas and New York, with results weighted to reflect statewide populations of new SCHIP enrollees. MEASURES: Sociodemographic characteristics including income, education, employment, and other characteristics of the child and the family, race and ethnicity (white non-Hispanic,black non-Hispanic, and Hispanic [any race]), prior health insurance, health care access and utilization, and health status. ANALYSES: Bivariate analyses were used tocompare baseline measures upon enrollment for white, black, and Hispanic SCHIP enrollees. Multivariate analyses were performed to assess health status and health care access measures (prior insurance, presence of a usual source of care (USC), anduse of preventive care), controlling for demographic factors described above. Weighted analyses (where appropriate) were performed by using SPSS, STATA, or SUDAAN. RESULTS: Racial and ethnic composition varied across the SCHIP cohorts studied, with black and Hispanic children comprising the following proportion of
Page 23
1-200.txtenrollees, respectively: Alabama, 33% and <1%; Florida, 16% and 26%; Kansas, 12% and15%; and New York, 24% and 36%. Black and Hispanic children were more likely to reside in single-parent and lower-income families. With some variation by state, children from minority groups were more likely to report poorer health status than were white children. Relative to white children, children from minority groups in Florida and New York were more likely to have been uninsured for the entire year before SCHIP enrollment. In all states, children from minority groups who had prior coverage were more likely to have previously been enrolled in Medicaid than in private health insurance and were less likely to have had employer-sponsored coverage compared with white children. Except in Alabama, there was a difference in having a USC, with children from minority groups less likely to have had a USC before SCHIP enrollment compared with white children. No consistent pattern of health care utilization before SCHIP was noted across states with respect to race orethnicity. Findings from multivariate analyses, controlling for sociodemographic factors, generally confirmed that black and Hispanic children were more likely to have lacked insurance or a USC before enrollment in SCHIP and to have poorer health status compared with white children. CONCLUSIONS: SCHIP is enrolling substantial numbers of racial and ethnic minority children. There are baseline racial and ethnicdisparities among new enrollees in SCHIP, with black and Hispanic children faring worse than white children on many sociodemographic and health system measures, and there are differences among states in the prevalence and magnitude of these disparities. After controlling for sociodemographic factors, these disparities persisted. IMPLICATIONS FOR MONITORING AND IMPROVING SCHIP: SCHIP has the potential to play a critical role in efforts to eliminate racial and ethnic disparities in health among the children it serves. However, study findings indicate that programmatic efforts are necessary to ensure that disparities are not perpetuated. Program effectiveness and outcomes should be monitored by race and ethnicity to ensure equity in access, use, and outcomes across all racial and ethnic groups. Assessing the health characteristics and needs of new SCHIP enrollees can provide a benchmark for evaluating the program's impact on eliminating racial and ethnic disparities in health and inform service delivery enhancements.
<46>Unique Identifier 12938812Authors Goodwin JL. Kaemingk KL. Fregosi RF. Rosen GM. Morgan WJ. Sherrill DL. Quan SF.Institution Arizona Respiratory Center, University of Arizona College of Medicine, Tucson, AZ 85724, USA. [email protected] Clinical outcomes associated with sleep-disordered breathing in Caucasian and Hispanic children--the Tucson Children's Assessment of Sleep Apnea study (TuCASA).Source Sleep. 26(5):587-91, 2003 Aug 1.Abstract STUDY OBJECTIVES: This report describes clinical outcomes and threshold levels of respiratory disturbance index (RDI) associated with sleep-disordered breathing in children participating in the Tucson Children's Assessment of Sleep Apnea study. DESIGN: A community-based, prospective cohort study designed to assess the severity of sleep-related symptoms associated with sleep-disordered breathing in children aged 6 to 11 years. SETTING: Students attending elementary school in the Tucson Unified School District. PARTICIPANTS: Unattended home polysomnograms were completedon 239 children-55.2% boys, 51% Hispanic, and 55% between the ages of 6 and 8 years.MEASUREMENTS AND RESULTS: Based on full home polysomnography, levels of RDI that correspond to a higher prevalence of clinical symptoms of sleep-disordered breathingin children aged 6 to 11 were observed. An RDI of at least 5 was associated with frequent snoring (20.3% vs 9.1%, P<.01), excessive daytime sleepiness (22.9% vs 10.7%, P<.01), and learning problems (8.5% vs 2.5%, P<.04) when no oxygen desaturation accompanied the respiratory event. An RDI of at least 1 was associated with these symptoms when a 3% oxygen desaturation was required, snoring (24.0% vs
Page 24

1-200.txt10.4%, P<.006), excessive daytime sleepiness (24.0% vs 13.4%, P<.04), and learning problems (10.7% vs 3.0%, P<.02). Hispanic or Caucasian ethnicity, sex, age category,obesity, insomnia, and witnessed apnea were not associated with RDI regardless of event definition. CONCLUSIONS: The Tucson Children's Assessment of Sleep Apnea studyhas shown that there are values of RDI based on polysomnography that correspond to an increased rate of clinical symptoms in children ages 6 to 11 years.
<47>Unique Identifier 14622624Authors Davidson P. Hancock K. Leung D. Ang E. Chang E. Thompson DR. Daly J.Institution School of Nursing, Family and Community Health (SNFCH), College of Social and Health Sciences (CSHS), University of Western Sydney, Sydney, NSW, Australia.Title Traditional Chinese Medicine and heart disease: what does Western medicine and nursing science know about it?. [Review] [68 refs]Source European Journal of Cardiovascular Nursing. 2(3):171-81, 2003 Sep.Abstract BACKGROUND: Interest in Traditional Chinese Medicine (TCM) is growing rapidly beyond China. This interest is driven by a combination of factors including recognition of potential benefits of TCM; dissatisfaction with the traditional Western medical model; an increasing commitment to holistic care and increasing evidence for the interaction of psychological factors and outcomes of disease and treatment and health consumer demand. AIMS: This review article was prompted by the need to understand and interpret the increasing trend towards the use of TCM in heart disease. In particular, this article defines and describes TCM, and analyses implications and challenges for Western health care delivery models. LITERATURE SEARCH: This article provides a review of accessible evidence, to English speaking health care professionals. The CINAHL, MEDLINE, HealthSTAR, Academic ASAP and Cochrane databases were searched, identifying literature published from 1982. Searchengines on the Internet were also used. Examples of keywords used were "Traditional Chinese Medicine" and "heart". CONCLUSION: Difficulties in accessing information regarding TCM have implications for health education in coronary heart disease and patient safety. The rapid uptake of TCM in both Western and Chinese societies mandates an understanding of the principles and potential interactions when TCM is complemented with Western medical treatment for heart disease. Development of this knowledge and understanding is essential in order to provide safe and effective health care to patients who use combination therapies. [References: 68]
<48>Unique Identifier 12971114Authors Jenkins KR. Fultz NH. Fonda SJ. Wray LA.Institution Institute for Social Research, University of Michigan, Ann Arbor, USA. [email protected] Patterns of body weight in middle-aged and older Americans, by gender and race, 1993-2000.Source Sozial- und Praventivmedizin. 48(4):257-68, 2003.Abstract OBJECTIVES: Despite evidence of poor health outcomes associated with excessive weight gain or loss, longitudinal patterns of body weight over the adult life coursehave not been fully described. This article seeks to address this by examining body weight patterns for middle-aged and older adults. METHODS: Panel data from the Health and Retirement Study (HRS) original cohort and the original cohort of the
Page 25

1-200.txtAsset and Health Dynamics Among the Oldest Old (AHEAD) study are used to compare, bysocial group, characteristics of respondents and non-respondents, baseline weight (1993 and 1994) to year 2000 weight, and explore various weight change trajectories over time. RESULTS: Overall, a greater proportion of middle-aged adults are heavier over time than at baseline and a greater proportion of older adults lose weight overtime compared to baseline. Examining the transitions across weight trajectories for all of the social groups suggests considerable variability. CONCLUSIONS: These findings suggest that differing physiologic and social or environmental experiences may have implications for body weight patterns. Understanding these patterns by race/ethnicity and gender could provide insight into health disparities among different social groups.
<49>Unique Identifier 12716801Authors Lavery LA. Armstrong DG. Wunderlich RP. Tredwell J. Boulton AJ.Institution Department of Surgery, Diabetex Research Group, Baltimore, Maryland, USA. [email protected] Diabetic foot syndrome: evaluating the prevalence and incidence of foot pathology in Mexican Americans and non-Hispanic whites from a diabetes disease management cohort.Source Diabetes Care. 26(5):1435-8, 2003 May.Abstract OBJECTIVE: To report the incidence of diabetes-related lower-extremity complications in a cohort of patients enrolled in a diabetes disease management program. RESEARCH DESIGN AND METHODS: We evaluated screening results and clinical outcomes for the first 1,666 patients enrolled in a disease management program for aperiod of 24 months (50.3% men, aged 69.1 +/- 11.1 years). RESULTS: The incidence ofulceration, infection, amputation, and lower-extremity bypass was 68.4, 36.5, 5.9, and 7.7 per 1,000 persons with diabetes per year. Amputation incidence was higher inMexican Americans than in non-Hispanic whites (7.4/1,000 vs. 4.1/1,000; P = 0.003, odds ratio [OR] 1.8, 95% CI 1.2-2.7). The amputation-to-ulcer ratio was 8.7%. The incidence of Charcot arthropathy was 8.5/1,000 per year. Charcot was more common in non-Hispanic whites than in Mexican Americans (11.7/1,000 vs. 6.4/1,000; P = 0.0001,1.8, 1.3-2.5). The prevalence of peripheral vascular disease was 13.5%, with no significant difference based on ethnicity (P = 0.3). There was not a significant difference in incidence of foot infection (P = 0.9), lower-extremity bypass (P = 0.3), or ulceration (P = 0.1) based on ethnicity. However, there were more failed bypasses in Mexican Americans (33%) than in non-Hispanic whites (7.1%). Mexican Americans were 3.8 times more likely to have a failed bypass (leading to an amputation) or be diagnosed as "nonbypassable" than non-Hispanic whites (75.0 vs. 44.0%; P = 0.01, 3.8, 1.2-11.8). CONCLUSIONS: The incidence of amputation is higher in Mexican Americans, despite rates of ulceration, infection, vascular disease, and lower-extremity bypass similar to those of non-Hispanic whites. There may be factorsassociated with failed or failure to bypass that mandate further investigation.
<50>Unique Identifier 14635289Authors Escalante A. del Rincon I. Mulrow CD.Institution Division of Clinical Immunology and Rheumatology, University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78284, USA.Title Symptoms of depression and psychological distress among Hispanics with rheumatoid arthritis.
Page 26

1-200.txtSource Arthritis Care & Research. 13(3):156-67, 2000 Jun.Abstract OBJECTIVE: To explore the roles played by Hispanic ethnic background and acculturation to the mainstream English language culture of the United States in thedepressive symptoms and mental health of rheumatoid arthritis (RA) patients. METHODS: Members of a consecutive cohort of patients with RA were studied cross-sectionally. All underwent a comprehensive clinical and psychosocial evaluation. Depressive symptoms were measured with the Center for Epidemiologic Studies Depression Scale (CES-D), and psychological distress was measured with the Medical Outcomes Study Short Form 36 (SF-36) mental health scale. RESULTS: Two hundred thirty-six patients were studied. Women had significantly higher median CES-D scores than men (19 versus 14, P = 0.0004), Hispanics scored higher than non-Hispanics (14 versus 8, P = 0.0002), and foreign-born scored higher than US-bornpatients (14 versus 10, P = 0.009). Compared with those who were fully acculturated,patients who were partially acculturated were more likely to have a score > or = 16 on the RA-adjusted CES-D (odds ratio [OR] = 1.79, 95% confidence interval [95% CI] 1.37 to 2.35, P < or = 0.001). Among unacculturated patients, the likelihood of a score > or = 16 increased 6-fold (OR = 6.68; 95% CI 3.50 to 12.72; P < or = 0.001). A similar, inverse pattern was observed for the SF-36 mental health scale. In multivariate models accounting for age, sex, education, income, articular pain, deformity, and the level of disability, low acculturation was independently associated with high depressive symptoms, and a Hispanic background was independently associated with lower SF-36 mental health. CONCLUSIONS: In this consecutive series of RA patients, Hispanics, particularly those who are not fully acculturated to the mainstream Anglo society, had more depressive symptoms and psychological distress than did non-Hispanics.
<51>Unique Identifier 14609392Authors Sue S.Institution Department of Psychology, University of California, Davis 95616-8686, USA. [email protected] In defense of cultural competency in psychotherapy and treatment.Source American Psychologist. 58(11):964-70, 2003 Nov.Abstract Cultural competency guidelines and policies are being widely established. Yet somecritics have challenged the evidence for cultural competency and the lack of efficacy studies that demonstrate its outcomes. Various positions are examined that discuss cultural competency research. They include the need for more resources for research, scientific practices that overlook ethnic research findings, fruitfulness of theory-driven rather than population-based research, problems in defining cultural competency as a technique, and development of policies in the absence of research. Implications of these positions are discussed. (c) 2003 APA, all rights reserved.
<52>Unique Identifier 14649534Authors Wade V. Jackson D. Daly J.Institution School of Nursing, Family and Community Health, University of Western Sydney, Sydney, Australia.Title Coronary heart disease in Aboriginal communities: towards a model for
Page 27

1-200.txtself-management. [Review] [57 refs]Source Contemporary Nurse. 15(3):300-9, 2003 Oct.Abstract Coronary heart disease (CHD) is one of the main causes of death and disability in the Aboriginal population, and is the major cause of the twenty-year gap in life expectancy of Aboriginal and non-Aboriginal Australians. This paper explores Aboriginal health in relation to CHD, and suggests self-management as a culturally acceptable therapeutic and sustainable ideology from which positive outcomes may be achieved. [References: 57]
<53>Unique Identifier 14639082Authors Lorig KR. Ritter PL. Gonzalez VM.Institution Department of Medicine, Stanford University School of Medicine, California, USA. [email protected] Hispanic chronic disease self-management: a randomized community-based outcome trial.Source Nursing Research. 52(6):361-9, 2003 Nov-Dec.Abstract BACKGROUND: In light of health disparities and the growing prevalence of chronic disease, there is a need for community-based interventions that improve health behaviors and health status. These interventions should be based on existing theory.OBJECTIVE: This study aimed to evaluate the health and utilization outcomes of a 6-week community-based program for Spanish speakers with heart disease, lung disease, or type 2 diabetes. METHOD: The treatment participants in this study (n = 327) took a 6-week peer-led program. At 4 months, they were compared with randomizedwait-list control subjects (n = 224) using analyses of covariance. The outcomes for all the treatment participants were assessed at 1 year, as compared with baseline scores (n = 271) using t-tests. RESULTS: At 4 months, the participants, as compared with usual-care control subjects, demonstrated improved health status, health behavior, and self-efficacy, as well as fewer emergency room visits (p <.05). At 1 year, the improvements were maintained and remained significantly different from baseline condition. CONCLUSIONS: This community-based program has the potential to improve the lives of Hispanics with chronic illness while reducing emergency room use.
<54>Unique Identifier 14601809Authors Frank G. Fishman M. Crowley C. Blair B. Murphy ST. Montoya JA. Hickey MP. Brancaccio MV. Bensimon EM.Institution New Stories/New Cultures, Department of Occupational Science and Occupational Therapy, University of Southern California, 1540 Alcazar, CHP-133, Los Angeles, California 90033-1091, USA. [email protected] The New Stories/New Cultures after-school enrichment program: a direct cultural intervention.Source American Journal of Occupational Therapy. 55(5):501-8, 2001 Sep-Oct.Abstract This article describes the organization, curriculum, and outcomes for New Stories/New Cultures, an activity-based program for after-school enrichment in five schools in the low-income neighborhood near a major American university. The program
Page 28

1-200.txtencourages students (70% Hispanic-American, 30% African-American) to experience themselves as producers of culture, not just as consumers. Its methods include (a) creative team use of video equipment and other expressive media and (b) lessons about media literacy (i.e., making critical choices about images and activities depicted in popular culture and commercials). Outcome measures with the cohort of fifth and sixth graders support the programs occupation-based philosophy. They show that students are more likely to experience themselves as building skills when engaged in activities that are both challenging and enjoyable. The students reportedgreatest engagement and enjoyment in activities that were creative, team-based, and involving media production. These same activities were correlated with increased self-esteem. The term direct cultural intervention is used to describe the application of occupational principles and critical perspectives to provide a population with conceptual tools and skills for interpreting and successfully navigating the social world.
<55>Unique Identifier 14621325Authors Nunez AE. Robertson C.Institution Division of General Internal Medicine, Drexel University College of Medicine, Philadelphia, PA 19129, USA. [email protected] Multicultural considerations in women's health.Source Medical Clinics of North America. 87(5):939-54, 2003 Sep.Abstract As patient practices continue to diversify, clinical skills need to extend beyond disease manifestation and treatment modalities into awareness of health statistics that highlight disparities, training, cross-cultural health care delivery at the individual and system-based levels. and skills of health care advocacy. Excellent care for multicultural women implies the ability to assess the health issues applicable to all women as well as the issues specific to the women in the clinician's office. It implies enabling the patient to share with her individual andcultural influences. Incorporating both of these influences at the same time and integrating them into her context of care can result in developing the best fit for health care goals, eliminating disparities and improving health outcomes in terms ofquantity and quality of lives for all women.
<56>Unique Identifier 14528739Authors Mateo MA. Smith SP.Institution Northeastern University, School of Nursing, Bouve College of Health Sciences, Boston, MA 02115, USA. [email protected] Workforce diversity in hospitals.Source Nursing Leadership Forum. 7(4):143-9, 2003 Summer.Abstract With an increasingly diverse population and staff, leaders of organizations must play an active role in diversity management. Nurse leaders (n = 231) responded to a survey concerning diversity initiatives, outcomes, and issues related to staff and patients. The findings suggest that most respondents have not made diversity management an important issue. Few have goals related to diversity with indices to measure outcomes. The majority of the respondents did not report that diversity in their staffs or patients resulted in management or patient care issues. The authors suggest that managers revisit the policies, procedures, and practices related to
Page 29

1-200.txttheir diversity management initiatives.
<57>Unique Identifier 12890012Authors Benfield MR. McDonald RA. Bartosh S. Ho PL. Harmon W.Institution Division of Pediatric Nephrology, University of Alabama at Birmingham, Birmingham,AL, USA.Title Changing trends in pediatric transplantation: 2001 Annual Report of the North American Pediatric Renal Transplant Cooperative Study.Source Pediatric Transplantation. 7(4):321-35, 2003 Aug.Abstract The North American Pediatric Renal Transplant Cooperative Study has collected clinical information on children undergoing a renal transplantation since 1987. Thiscooperative group now includes over 150 participating medical centers in the United States, Canada, Mexico, and Costa Rica. This report covers the years from 1987 through 2001 and includes data on 7545 renal transplants in 6878 patients. This report demonstrates changing trends in many areas of pediatric transplantation including increasing numbers of African American and Hispanic children receiving transplantation, remarkable improvements in the rate of acute rejection, rejection reversal, and short- and long-term allograft survival. In the most recent cohorts ofpatients, we now see that 1-yr allograft survival is no different in cadaver donor compared to living donor recipients and in infants compared to all other age groups.However, this analysis also reveals areas of continued challenges including inferioroutcomes in African American and adolescent populations, chronic rejection, and the adverse effects of immunosuppression.
<58>Unique Identifier 12605075Authors Barnett NP. Monti PM. Cherpitel C. Bendtsen P. Borges G. Colby SM. NordqvistC. Johansson K.Institution Center for Alcohol and Addiction Studies, Brown University, Providence, Rhode Island 02912, USA. [email protected] Identification and brief treatment of alcohol problems with medical patients: an international perspective.Source Alcoholism: Clinical & Experimental Research. 27(2):262-70, 2003 Feb.Abstract This article summarizes the proceedings of a symposium at the 2002 RSA meeting in San Francisco, California. The chair was Peter Monti and co-chair was Nancy Barnett.The aim of the symposium was to bring together researchers from the United States, Sweden, and Mexico to present current findings on the development and implementationof screening and intervention research in Emergency Departments (ED). Cheryl Cherpitel presented findings on the performance of the Rapid Alcohol Problems Screen(RAPS4), a 4-item instrument used for screening for alcohol dependence and harmful drinking in the ED. Dr. Cherpitel also presented for her collaborator, Guilherme Borges, their research on the performance of a number of screening measures including the RAPS among Mexicans and Mexican-Americans with alcohol-related disorders in the ED. Preben Bendtsen described the implementation of an alcohol screening and intervention procedure delivered by ordinary ED staff in Sweden. NancyBarnett presented data on characteristics related to readiness to change alcohol usein a sample of young adults who were treated in an ED for injury or intoxication.
Page 30

1-200.txt
<59>Unique Identifier 14557737Authors Payne TJ. Diefenbach L.Institution Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, USA. [email protected] Characteristics of African American smokers: a brief review. [Review] [29 refs]Source American Journal of the Medical Sciences. 326(4):212-5, 2003 Oct.Abstract The Public Health Service Guideline, Treating Tobacco Use and Dependence, containsa wealth of information regarding current treatment practices. Unfortunately, guidance for tailoring standardized treatments to meet the needs of specific ethnic subgroups is limited. This article highlights features unique to African American smokers, a necessary precursor to developing intervention programs that hold promisefor improving outcomes. [References: 29]
<60>Unique Identifier 14557080Authors Mutchnick IS. Moyer CA. Stern DT.Title Expanding the boundaries of medical education: evidence for cross-cultural exchanges. [Review] [50 refs]Source Academic Medicine. 78(10 Suppl):S1-5, 2003 Oct.Abstract PROBLEM STATEMENT AND BACKGROUND: Cross-cultural experiences are in increasing demand by both graduate and undergraduate medical students, yet the benefits of these experiences are not clearly established. METHOD: A review of the literature was conducted to identify articles on the outcomes of cross-cultural experiences. Themes were identified and categorized into domains. RESULTS: Forty-two studies werefound; 27 articles used qualitative methods, nine used quantitative methods, and sixused both. Most (24) were from the nursing literature, 18 were from the medical literature. All studies reported positive outcomes along four domains: students' professional development, students' personal development, medical school benefits, and host population benefits. CONCLUSIONS: Studies reviewed were primarily case controlled or case series. Future research is needed that more clearly defines outcome measures and uses more rigorous methods. Although results suggest positive outcomes in all domains, additional research is needed before cross-cultural rotations can be supported based on evidence. [References: 50]
<61>Unique Identifier 14534231Authors Lucas JW. Barr-Anderson DJ. Kington RS.Institution Division of Health Interview Statistics, National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, MD 20892, USA.Title Health status, health insurance, and health care utilization patterns of immigrantBlack men.Source American Journal of Public Health. 93(10):1740-7, 2003 Oct.Abstract
Page 31

1-200.txt OBJECTIVES: This study sought to describe the health status, health insurance, andhealth care utilization patterns of the growing population of immigrant Black men. METHODS: We used data from the 1997-2000 National Health Interview Survey to examineand then compare health variables of foreign-born Black men with those of US-born Black and White men. Logistic regression analyses were used to examine health outcomes. RESULTS: Foreign-born Black men were in better overall health than their US-born Black counterparts and were much less likely than either US-born Black or White men to report adverse health behaviors. Despite these health advantages, foreign-born Black men were more likely than either US-born Black or White men to beuninsured. CONCLUSIONS: In the long term, immigrant Black men who are in poor healthmay be adversely affected by lack of health care coverage.
<62>Unique Identifier 14534224Authors Brown AF. Gerzoff RB. Karter AJ. Gregg E. Safford M. Waitzfelder B. Beckles GL. Brusuelas R. Mangione CM. TRIAD Study Group.Institution School of Medicine at the University of California, Los Angeles, CA 90095, USA. [email protected] Health behaviors and quality of care among Latinos with diabetes in managed care.Source American Journal of Public Health. 93(10):1694-8, 2003 Oct.Abstract OBJECTIVES: We evaluated whether ethnicity and language are associated with diabetes care for Latinos in managed care. METHODS: Using data from 4685 individualsin the Translating Research Into Action for Diabetes (TRIAD) Study, a multicenter study of diabetes care in managed care, we constructed multivariate regression models to compare health behaviors, processes of care, and intermediate outcomes forWhites and English- and Spanish-speaking Latinos. RESULTS: Latinos had lower rates of self-monitoring of blood glucose and worse glycemic control than did Whites, higher rates of foot self-care and dilated-eye examinations, and comparable rates ofother processes and intermediate outcomes of care. CONCLUSIONS: Although self-management and quality of care are comparable for Latinos and Whites with diabetes, important ethnic disparities persist in the managed care settings studied.
<63>Unique Identifier 14532792Authors Rosser CJ. Kuban DA. Levy LB. Pettaway CA. Chichakli R. Kamat AM. Sanchez-Ortiz RF. Pisters LL.Institution Department of Urology, University of Texas M.D. Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030, USA.Title Clinical features and treatment outcome of Hispanic men with prostate cancer following external beam radiotherapy.Source Journal of Urology. 170(5):1856-9, 2003 Nov.Abstract PURPOSE: We retrospectively analyzed the clinical characteristics and outcomes of Hispanic men compared with other groups who underwent radiotherapy alone for localized or locally advanced prostate cancer. MATERIALS AND METHODS: Between April 1987 and January 1998, 964 men who underwent full dose external beam radiotherapy alone for localized or locally advanced prostate cancer were included in the study. Patient medical records were reviewed for pertinent information. RESULTS: Of the 964men 810 were non-Hispanic white, 54 were Hispanic and 86 were black Americans. The most significant difference among the groups was in the proportion of patients who
Page 32

1-200.txtpresented with initial prostate specific antigen (PSA) greater than 20 ng/ml (22% ofHispanic vs 11% of white men, p = 0.0012). In addition, 17% of Hispanic men had a Gleason score of 8 or greater compared with 11% of white men (p = 0.0265). A greaterproportion of Hispanic patients also had a less favorable posttreatment PSA nadir ofgreater than 1 ng/ml compared with white patients, (44% vs 26%, p = 0.0214), which may have translated into a trend toward a lower 5-year disease-free survival rate inHispanics vs white men (52% vs 65%, p = 0.07). CONCLUSIONS: Hispanic men presented with higher PSA and higher grade prostate cancer than white men. Furthermore, a higher percent of Hispanic men had a PSA nadir of 1 ng/ml or greater after radiotherapy, which may have been responsible for their trend toward a decreased 5-year disease-free survival rate compared with white men. Improved screening and early detection may improve disease-free survival in Hispanic men with localized prostate cancer.
<64>Unique Identifier 14528135Authors Williams PB.Institution Graduate Public Health Program, Morgan State University, Baltimore, MD 21237-0001,USA.Title HIV/AIDS case profile of African Americans: guidelines for ethnic-specific health promotion, education, and risk reduction activities for African Americans.Source Family & Community Health. 26(4):289-306, 2003 Oct-Dec.Abstract There are discrepancies in health care services for the poor and ethnic minoritiesin the United States. Within the past decade widespread concerns regarding the need to reform the nation's health care services, including the problem of human immunodeficiency virus/acquired immune syndrome (HIV/AIDS) among African Americans has continued. These inequalities have been the cornerstone of the U.S. Healthy People 2010 national priority objectives. The objectives focus on health and social outcomes such as low quality of life and mortality rates, poverty, lack of accessibility to and appropriateness of care, and the prevalence of certain degenerative conditions and infectious diseases. The dearth of preventive health services for the high-risk groups, particularly children, adolescents, young adults,and older African American adults undermines early intervention efforts, including prompt HIV/AIDS identification and diagnosis, prevention education, health promotion, effective substance abuse treatment, and counseling services. This work reviews the magnitude of HIV/AIDS among African Americans between 1996 and 1999 by race/ethnicity, gender, and age groups. It also addresses the major factors responsible for the continued upward trend in the distribution and rate of infectiousness of HIV/AIDS among African Americans. The study recommends and discusses culturally sensitive and ethnic-specific intervention strategies for the prevention and control of HIV/AIDS among African Americans.
<65>Unique Identifier 12930465Authors Nguyen JD. Carson ML. Parris KM. Place P.Institution Orange County Health Care Agency, Santa Ana, California 92706, USA. [email protected] A comparison pilot study of public health field nursing home visitation program interventions for pregnant Hispanic adolescents.Source Public Health Nursing. 20(5):412-8, 2003 Sep-Oct.
Page 33

1-200.txtAbstract OBJECTIVE: Improve pregnancy outcomes in first-time Hispanic adolescent mothers and their infants. SETTING: Urban communities in Orange County, California. DESIGN AND METHODS: A comparison of the Nurse-Family Partnership pilot study home visitation program with traditional Public Health Field Nursing (PHFN) home visitation. PARTICIPANTS: Two hundred twenty-five Hispanic adolescent mothers and their infants. INTERVENTIONS: Participants in the control group received the traditional PHFN services; the intervention group received interventions from advanced trained public health nurses The control group received a minimum of three home visits: one initial client assessment and family profile, one antepartum visit,and one postpartum visit, including newborn assessment. Participants in the intervention group received weekly home visits for the first 4 weeks, followed by visits every other week until delivery, weekly visits for the next 6 weeks, visits every other week until the child was 20 months, and monthly visits until the child was 24 months of age. RESULTS: Preliminary results indicate that home visitation by public health nurses (PHNs) positively affected the health of adolescents mothers and their infants. The incidence of premature births to adolescent mothers in the intervention group was lower than that found in the California population of adolescent mothers. CONCLUSION: Preliminary results from this program showed that PHN home visitation (control and intervention groups) positively affects the birth outcomes of adolescent mothers and their infants.
<66>Unique Identifier 14574275Authors Centers for Disease Control and Prevention (CDC).Title Infant health among Puerto Ricans--Puerto Rico and U.S. mainland, 1989-2000.Source MMWR. Morbidity & Mortality Weekly Report. 52(42):1012-6, 2003 Oct 24.Abstract Although the overall U.S. infant mortality rate (IMR) declined dramatically duringthe 1900s, striking racial/ethnic disparities in infant mortality remain. Infant health disparities associated with maternal place of birth also exist within some racial/ethnic populations. Eliminating disparities in infant health is crucial to achieving the 2010 national health objective of reducing the infant death rate to 4.5 per 1,000 live births (objective 16-1c). Hispanics comprise the largest racial/ethnic minority population in the United States. Among U.S. Hispanics, considerable heterogeneity exists in infant health, with the poorest outcomes reported among Puerto Rican infants. This report compares trends during the previousdecade in IMRs and major determinants of these rates such as low birthweight (LBW), preterm delivery (PTD), and selected maternal characteristics among infants born to Puerto Rican women on the U.S. mainland (50 states and the District of Columbia) with corresponding trends among infants born in Puerto Rico. The findings indicate that despite having lower prevalence of selected maternal risk factors, Puerto Rico-born infants are at greater risk for LBW, PTD, and infant death than mainland-born Puerto Rican infants. This report also highlights a persistent disparity in IMRs and an emerging disparity in LBW and PTD rates between Puerto Rico-born infants and mainland-born Puerto Rican infants. Future research should focus on identifying factors responsible for these disparities to improve infant health in Puerto Rico.
<67>Unique Identifier 14563501Authors Fang J. Alderman MH.Institution Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, New York 10461, USA. [email protected]
Page 34

1-200.txtTitle Is geography destiny for patients in New York with myocardial infarction?.Source American Journal of Medicine. 115(6):448-53, 2003 Oct 15.Abstract PURPOSE: The use of coronary revascularization among patients with myocardial infarction varies by race/ethnicity and socioeconomic status. The objective of this study was to determine whether local availability of facilities might influence apparent racial disparities in revascularization and health outcomes. METHODS: UsingStatewide Planning and Research Cooperative System data (1988-1999) from the New York State Department of Health, we determined revascularization rates among patients hospitalized with myocardial infarction in two socioeconomically disadvantaged communities in New York City (the South Bronx, which has no hospitals that have revascularization facilities, and Harlem, which has three revascularization facilities), as well as in its most advantaged community (mid-Manhattan, which has six such facilities). The rest of New York City served as reference. We measured demographic and clinical characteristics and revascularization rates in each community. RESULTS: Among patients hospitalized withmyocardial infarction, the age-adjusted revascularization rates were 29.2% for whites, 12.5% for blacks, and 19.9% for Hispanics (P <0.01). Rates were 12.0% in theSouth Bronx, 24.0% in Harlem, 38.4% in mid-Manhattan, and 21.2% in the rest of New York City (P <0.05). Logistic regression analysis, adjusting for age, sex, race, insurance status, comorbidity, clinical complications, and year of admission, revealed that South Bronx patients were about 20% less likely to be revascularized than those in the rest of New York City, whereas patients living in Harlem were twice as likely to receive such treatment as residents in the rest of New York City.Among patients admitted to hospitals with cardiac revascularization facilities, lower use among South Bronx residents persisted, but after adjusting for patient characteristics, Harlem residents were significantly less likely to be revascularized than those from the rest of New York City. CONCLUSION: Race and socioeconomic factors influence the likelihood of revascularization after myocardialinfarction among residents of New York City. In addition, lack of availability of revascularization further reduces its use by residents of disadvantaged neighborhoods.
<68>Unique Identifier 14560167Authors Pina AA. Silverman WK. Fuentes RM. Kurtines WM. Weems CF.Institution Department of Psychology, University Park Campus, Florida International University, Miami, FL 33199, USA.Title Exposure-based cognitive-behavioral treatment for phobic and anxiety disorders: treatment effects and maintenance for Hispanic/Latino relative to European-American youths.Source Journal of the American Academy of Child & Adolescent Psychiatry. 42(10):1179-87,2003 Oct.Abstract OBJECTIVE: To examine treatment response and maintenance to exposure-based cognitive-behavioral therapy (CBT) for Hispanic/Latino relative to European-Americanyouths with phobic and anxiety disorders. METHOD: A total of 131 Hispanic/Latino andEuropean-American youths (aged 6-16 years) who participated in two previous clinicaltrials for phobic and anxiety disorders were compared along diagnostic recovery rates, clinically significant improvement, and youth- and parent-completed questionnaire scores using traditional hypothesis tests, including effect sizes, andstatistical equivalence tests. RESULTS: After treatment, Hispanic/Latino and European-American youths responded similarly to exposure-based CBT in their diagnostic recovery rates and questionnaires. Effect sizes for questionnaire data were also more similar than different across the two groups. With regard to
Page 35

1-200.txttreatment maintenance, Hispanic/Latino and European-American youths also responded more similarly than differently, albeit with some variations within specific assessment points in questionnaire data. CONCLUSIONS: Exposure-based CBT for phobic and anxiety disorders produced positive treatment gains and maintenance for Hispanic/Latino youths who participated in the trials. The treatment response that can be expected is generally similar (i.e., favorable) and equivalent to that found with European-American youths based on all the available indices of change.
<69>Unique Identifier 14551472Authors Malloch K. Davenport S. Hatler C.Institution Kathy Mallock and Associates, Glendale, AR 85308, USA. [email protected] Nursing workforce management: using benchmarking for planning and outcomes monitoring.Source Journal of Nursing Administration. 33(10):538-43, 2003 Oct.Abstract The goal of maintaining the balance between demand for nursing care and the supplyof nurses is the basis for state and regional planning to meet future nursing workforce needs. Projecting nursing supply needs solely on the basis of historical registered nurse to population ratios does not specifically consider the healthcare needs of the population. The authors present a model in which state population data and nursing resource data are compared with national data to assist state planning groups in developing an effective workforce management plan. Integrating population demographic data, healthcare needs of citizens, and nurse resource factors at the state level can improve the accuracy of projection statistics.
<70>Unique Identifier 14535297Authors Grantmakers In Health, Washington, D.C., USA.Title In the right words: addressing language and culture in providing health care.Source Issue Brief (Grantmakers in Health). (18):1-44, 2003 Aug.Abstract As part of its continuing mission to serve trustees, executives, and staff of health foundations and corporate giving programs, Grantmakers In Health (GIH) convened a group of experts from philanthropy, research, health care practice, and policy on April 4, 2003, to discuss the roles of language and culture in providing effective health care. During this Issue Dialogue, In the Right Words: Addressing Language and Culture in Providing Health Care, health grantmakers and experts from policy and practice participated in an open exchange of ideas and perspectives on language access and heard from fellow grantmakers who are funding innovative programs in this area. Together they explored ways to effectively support comprehensive language services, including the use of interpreters and translation of written materials. This Issue Brief synthesizes key points from the day's discussion with a background paper previously prepared for Issue Dialogue participants. It focuses on the challenges and opportunities involved with ensuring language access for the growing number of people who require it. Sections include: recent immigration trends and demographic changes; the effect of language barriers on health outcomes and health care processes; laws and policies regarding the provision of language services to patients, including an overview of public financing mechanisms; strategies for improving language access, including enhancing access in delivery settings, promoting advocacy and policy change, improving interpreter training, and advancing research; and roles for foundations in
Page 36

1-200.txtsupporting improved language access, including examples of current activities. The Issue Dialogue focused mainly on activities and programs that ensure linguistic access to health care for all patients. Although language and culture are clearly inseparable, a full exploration of the field of cultural competence and initiatives that promote its application to the health care setting are beyond the scope of thisIssue Brief. The day's discussion did, however, raise provocative issues of culture that are reflected throughout this report.
<71>Unique Identifier 14518843Authors Gates PE. Ganey JH. Brown MD.Institution Bronx Lebanon Hospital Center, Department of Dentistry, NY 10457, USA. [email protected] Building the minority faculty development pipeline.Source Journal of Dental Education. 67(9):1034-8, 2003 Sep.Abstract The shortage of faculty in dental education is well documented, but the data also show a shortage of minorities in postgraduate programs, which develop future faculty. In the last ten years, ADEA's effort to address minority issues in dental education has made some progress. In addition, examples of pipelines for minority faculty development that have shown some success include: a partnership between Harlem Hospital and Columbia University School of Dentistry and Oral Surgery in which the school dedicates one position in its postgraduate training programs to an individual participating in the Harlem Hospital General Practice Residency program; a partnership between the National Dental Association Foundation and Colgate-Palmolive Company, which provides scholarships for advanced dental educationstudy; and the Bronx Lebanon Hospital Center Department of Dentistry, which enrolls underrepresented minorities in its General Practice Residency Program, a new Pediatric Dentistry Residency Program, and a unique program providing hands-on experience in HIV/AIDS health care policy and AIDS development management. Critical elements in the relative success of these programs are environment, selection criteria, mentoring, networking, and finance. The true measure of the outcomes is still to be seen.
<72>Unique Identifier 14512767Authors Rodriguez VM. Conway TL. Woodruff SI. Edwards CC.Institution San Diego State University, San Diego, California, USA.Title Pilot test of an assessment instrument for Latina community health advisors conducting an ETS intervention.Source Journal of Immigrant Health. 5(3):129-37, 2003 Jul.Abstract Community health advisors (CHAs), also known as promotores, are lay individuals inthe community that others tend to look toward for advice and support. Studies incorporating CHAs are relatively rare, and CHAs have not been used in previous intervention studies to reduce environmental tobacco smoke (ETS) exposure. The present study pilot tested a CHA assessment instrument and examined the effects of promotora training on CHAs' knowledge, attitudes, and beliefs concerning ETS reduction. Participants were 11 women recruited from the local community. CHA training produced changes on several psychosocial constructs. Anticipated outcomes regarding ETS reduction and emotional reactions related to volunteering in the
Page 37

1-200.txtcommunity were more positive after training. Self-esteem and self-efficacy showed increases after training. Future research will investigate the relationship between the psychosocial characteristics measured in the assessment instrument and subsequent success implementing the ETS reduction intervention.
<73>Unique Identifier 12949480Authors Villarruel AM.Institution Center for Health Promotion, University of Michigan School of Nursing, Ann Arbor, MI 48109-0482, USA. [email protected] Commentary on: Race as a variable in cross-cultural research.[comment].Source Nursing Outlook. 51(4):189, 2003 Jul-Aug.
<74>Unique Identifier 12945657Authors Powers P.Institution South Dakota State University College of Nursing, Brookings, SD 57007-0098, USA. [email protected] Empowerment as treatment and the role of health professionals.Source Advances in Nursing Science. 26(3):227-37, 2003 Jul-Sep.Abstract This article argues that the concept of empowerment has been co-opted by health professionals and redefined as an intervention to produce compliance. Patients are considered empowered by health professionals only if they make the correct choices as defined by the health care provider. Patients are not informed about all possiblechoices and are not free to make their own choices for their own reasons. Empowerment is a coercive strategy that is justified by its outcomes and creates dependent populations.
<75>Unique Identifier 12939004Authors Anderson JD. Szalai JP.Institution Craniofacial Prosthetic Unit, Toronto Sunnybrook Regional Cancer Centre, Toronto, Ontario, Canada. [email protected] The Toronto outcome measure for cranlofacial prosthetics: a condition-specific quality-of-life instrument.Source International Journal of Oral & Maxillofacial Implants. 18(4):531-8, 2003 Jul-Aug.Abstract PURPOSE: The objective was to develop a patient-based outcome measure of condition-specific quality of life that would minimize measurement error related to the instrument when used with patients requiring extraoral craniofacial prostheses. MATERIALS AND METHODS: An item pool of potential questionnaire items covered 10 clinical/technical and social/psychologic domains. They sought how frequently the issue in the item affected patients and how important the problem in the item was.
Page 38

1-200.txtThe 139 items were administered to 94 treated patients in 5 centers in the United States, Canada, and the United Kingdom. Items were eliminated using relevance (frequency x importance), frequency of answer endorsement, Cronbach's alpha (internal consistency), and correlation of items on the same subject. International cultural agreement was tested using analysis of variance and Tukey comparisons within each domain. Scoring was transformed to a scale (0 to 100). RESULTS: The final instrument contained 52 items yielding a mean quality of-life score of 72.5% and a standard deviation of 17.9. Very high internal consistency was demonstrated with a final Cronbach's alpha of 0.967. No international cultural disagreement was found in 9 of the 10 domains. DISCUSSION: The relative weight of each of the domainsis (partially) based on the relevance to the patients. Of the 52 items, 29 were identified that do not mention a prosthesis. This subscale has a Cronbach's alpha of0.976. These items may therefore be useful where within-patient change is of interest. CONCLUSION: A patient-based outcome measure of condition-specific quality of life has been developed with control of bias and demonstrated performance characteristics.
<76>Unique Identifier 12934873Authors Whaley AL.Institution Department of Community Health and Social Medicine, City University of New York Medical School, New York, NY 10031, USA. [email protected] Ethnicity/race, ethics, and epidemiology.[see comment]. [Review] [44 refs]Source Journal of the National Medical Association. 95(8):736-42, 2003 Aug.Abstract Ethnicity/race is a much-studied variable in epidemiology. There has been little consensus about what self-reported ethnicity/race represents, but it is a measure ofsome combination of genetic, socioeconomic, and cultural factors. The present article will attempt to: 1.) Elucidate the limitations of contemporary discourse on ethnicity/race that emphasizes the genetic and socioeconomic dimensions as competingexplanatory frameworks; 2.) Demonstrate how considerable attention to the cultural dimension facilitates understanding of race differences in health-related outcomes; and 3.) Discuss interpretations of disparities in health status of African Americansversus European Americans from an ethical perspective. A major challenge to the discourse on ethnicity/race and health being limited to socioeconomic and genetic considerations is the lack of attention to the third alternative of a cultural perspective. The combined cultural ideologies of individualism and racism undermine the utility of epidemiologic research in health promotion and disease prevention campaigns aimed at reducing the racial gaps in health status. An ethical analysis supplements the cultural perspective. Ethics converge with culture on the notion of values influencing the study of ethnicity/race in epidemiology. A cultural approach to the use of ethnicity/race in epidemiologic research addresses methodological limitations, public health traditions, and ethical imperatives. [References: 44]
<77>Unique Identifier 12929705Authors Gosin M. Marsiglia FF. Hecht ML.Institution Ethnic Studies Department, University of California San Diego, La Jolla 92093-0522, USA.Title Keepin' it R.E.A.L.: a drug resistance curriculum tailored to the strengths and needs of pre-adolescents of the southwest.Source
Page 39

1-200.txt Journal of Drug Education. 33(2):119-42, 2003.Abstract Research has shown that students respond more favorably to drug prevention programs when they see their culture and themselves represented in the prevention message. Additionally, studies highlight important ethnic differences in drug behaviors and attitudes, indicating that students' ethnic culture should be considered in the creation of prevention programs. Because there are few effective, culturally grounded programs, new approaches are needed, particularly among Mexican American youth. This need inspired the Drug Resistance Strategies Project (DRS) to develop and test the keepin' it R.E.A.L curriculum serving ethnically diverse seventh grade students residing in a large southwestern city. This article describesdevelopment of the keepin' it R.E.A.L. curriculum, focusing on the methods used to ensure cultural grounding. The article also reviews literature on cultural approaches in prevention, presents a theoretical framework, summarizes key outcomes of the curriculum evaluation, and concludes with recommendations for the developmentof prevention programs for ethnically diverse youth.
<78>Unique Identifier 12925312Authors Mendelson C.Institution College of Nursing, University of New Mexico, Albuquerque, NM 87131, USA. [email protected] Creating healthy environments: household-based health behaviors of contemporary Mexican American women.Source Journal of Community Health Nursing. 20(3):147-59, 2003 Fall.Abstract This article describes the household-based health behaviors of a sample of contemporary Mexican American women.1 Using the Household Production of Health (HHPH) as a conceptual framework and ethnographic methods of inquiry, 13 moderately to highly acculturated women of Mexican ancestry participated in multiple interviewsabout their health beliefs and household health behaviors. This article examines thefindings related to the following research question: What are the health-producing and help-seeking behaviors (proximate determinants of health) used by Mexican American women to produce health? Themes focusing on creating healthy environments and treating illness are discussed. Awareness of the activities that women use to create and support household health can enhance the practice of nurses interested insupporting women's health work and improving health outcomes in the Mexican Americancommunity.
<79>Unique Identifier 12921499Authors Raji MA. Ostir GV. Markides KS. Espino DV. Goodwin JS.Institution Memory Loss Clinics and The University of Texas Medical Branch Geriatric Fellowship Training Program, Sealy Center on Aging, Department of Internal Medicine,The University of Texas Medical Branch, Galveston, TX 77555-0460, USA. [email protected] Potentially inappropriate medication use by elderly Mexican Americans.Source Annals of Pharmacotherapy. 37(9):1197-202, 2003 Sep.Abstract BACKGROUND: Use of inappropriate medications by the elderly is a public health concern with potentially serious health consequences. Research indicates relatively
Page 40

1-200.txthigh rates of inappropriate prescription drug usage for older whites and African Americans. However, rates for older Mexican Americans are unknown. OBJECTIVE: To examine the prevalence and predictors of inappropriate prescription medication use by older Mexican Americans. METHODS: A cross-sectional study of 3050 Mexican Americans aged > or =65 years living in the southwestern US was conducted. In-home interviews in 1993 and 1994 assessed prescription medication use. Descriptive statistics and logistic regression models were used to estimate prevalence and risk of inappropriate prescription drug use. RESULTS: Approximately 12% (n = 365) of the sample had used at least 1 of 32 potentially inappropriate prescription medications within 2 weeks of the baseline assessment. Four drugs, chlorpropamide, propoxyphene,amitriptyline, and dipyridamole, accounted for 54% of all inappropriate prescribing.Unmarried subjects, those with >/=1 chronic diseases, high depressive symptoms, frequent physician visits, and combined Medicaid and Medicare insurance were more likely to have used at least 1 of the 32 potentially inappropriate drugs. CONCLUSIONS: The prevalence of inappropriate medication use is lower in older Mexican Americans than in similar white and African American populations. More studies are needed on the pattern of inappropriate prescribing over time and on intervention programs to reduce potentially adverse health outcomes in older MexicanAmericans most at risk.
<80>Unique Identifier 12914014Authors Fultz NH. Ofstedal MB. Herzog AR. Wallace RB.Institution Institute for Social Research, University of Michigan, Ann Arbor, MI, USA. [email protected] Additive and interactive effects of comorbid physical and mental conditions on functional health.Source Journal of Aging & Health. 15(3):465-81, 2003 Aug.Abstract Objective: To understand the role of cognitive impairment and depressive symptoms on functional outcomes of stroke and diabetes. Evaluation approaches to functional outcomes have rarely focused on the presence of specific comorbidities, particularlythose involving mental health disorders. Methods: Data are from the AHEAD cohort of the Health and Retirement Study (HRS), a nationally representative panel of persons 70+ years of age in 1993. Analyses are limited to 5,646 self-respondents for whom functional outcome data are available in 1995. Additive and interactive multiple regression models are compared for each outcome and focal condition combination. Results: The additive model is sufficient for the majority of outcome and focal condition combinations. The interaction term is significant in 4 of 12 comparisons. Discussion: Stroke, diabetes, cognitive impairment, and depressive symptoms exhibit strong independent effects on physical functioning. Support for the hypothesis that cognitive impairment and depression exacerbate the impact of stroke and diabetes is more limited.
<81>Unique Identifier 12746255Authors LoBue PA. Moser KS.Institution Centers for Disease Control and Prevention, National Center for HIV, STD, and TB Prevention, Division of Tuberculosis Elimination, Field Services Branch, P.O. Box 85222, Mail Stop P511D, San Diego, CA 92186-5222, USA. [email protected] Use of isoniazid for latent tuberculosis infection in a public health clinic.[see comment].
Page 41

1-200.txtSource American Journal of Respiratory & Critical Care Medicine. 168(4):443-7, 2003 Aug 15.Abstract Isoniazid is an efficacious treatment for latent tuberculosis. Concerns remain, however, regarding hepatotoxicity associated with this medication. In addition, adherence may be suboptimal because at least 6 months of treatment is required. We extracted information from our latent tuberculosis treatment database to determine adverse effects and treatment completion rates associated with the use of isoniazid at a county tuberculosis clinic. Outcomes were available for 3,788 patients started on isoniazid between 1999 and 2002. Six hundred seventy-two patients (18%) experienced one or more adverse effects, including 10 (0.3%) determined to have isoniazid-associated liver injury. No hospitalizations or deaths occurred in patients experiencing an adverse effect. A higher incidence of adverse effects was associated with increasing age. Sixty-four percent of patients completed at least 6 months of isoniazid. Higher completion rates were associated with younger age, Hispanic ethnicity, and non-U.S. country of birth. Lower completion rates were associated with being homelessness, using excess alcohol, and having experienced an adverse effect. In summary, we conclude that in our clinic population isoniazid is asafe therapy for latent tuberculosis, but its effectiveness is limited by modest completion rates.
<82>Unique Identifier 12902366Authors Eisenman DP. Gelberg L. Liu H. Shapiro MF.Institution Division of General Internal Medicine and Health Services Research, Department of Medicine, University of California, Los Angeles 90095-1736, USA. [email protected] Mental health and health-related quality of life among adult Latino primary care patients living in the United States with previous exposure to political violence.[see comment].Source JAMA. 290(5):627-34, 2003 Aug 6.Abstract CONTEXT: Although political violence continues in parts of Central America, South America, and Mexico, little is known about its relationship to the health of Latino immigrants living in the United States. OBJECTIVE: To determine (1) rates of exposure to political violence among Latino adult primary care patients who have immigrated to the United States from Central America, South America, and Mexico and its impact on mental health and health-related quality of life and (2) frequency of disclosure of political violence to primary care clinicians. DESIGN, SETTING, AND PARTICIPANTS: Two-stage cluster design survey of a systematic sample of Latino immigrant adults in 3 community-based primary care clinics in Los Angeles, conductedfrom July 2001 to February 2002. MAIN OUTCOME MEASURES: Reports of exposure to political violence in home country before immigrating to the United States and communication with clinicians about political violence; self-reported measures of health-related quality of life using the Medical Outcomes Study Short Form 36 (MOS SF-36); symptoms of depression, anxiety, and alcohol disorders using the Primary Care Evaluation of Mental Disorders (PRIME-MD); and symptoms of posttraumatic stressdisorder (PTSD) using the PTSD Checklist-Civilian Version (PCL-C). RESULTS: A total of 638 (69%) of 919 eligible patients participated. The nonresponse rates did not differ by age, sex, recruitment sites, or clinic sessions. In weighted analyses, 54%of participants reported political violence experiences in their home countries, including 8% who reported torture. Of those exposed to political violence, 36% had symptoms of depression and 18% had symptoms of PTSD vs 20% and 8%, respectively, among those not exposed to political violence. Controlling for age, sex, country, years lived in the United States, acculturation, income, health insurance status, and recruitment site in a subsample of 512 participants (56%), those who reported
Page 42

1-200.txtpolitical violence exposure were more likely to meet symptom criteria for PTSD (adjusted odds ratio [AOR], 3.4; 95% confidence interval [CI], 1.4-8.4) and to have symptoms of depression (AOR, 2.8; 95% CI, 1.4-5.4) and symptoms of panic disorder (AOR, 4.8; 95% CI, 1.6-14.4) than participants not reporting political violence. Those exposed to political violence reported more chronic pain and role limitations due to physical problems, as well as worse physical functioning and lower perceptions of general health than those who were not exposed to political violence.Only 3% of the 267 patients who had experienced political violence reported ever telling a clinician about it after immigrating; none reported their current physician asking about political violence. CONCLUSION: Latino immigrants in primary care in Los Angeles have a high prevalence of exposure to political violence before immigrating to the United States and associated impairments in mental health and health-related quality of life.
<83>Unique Identifier 12894963Authors Winkleby MA. Snider J. Davis B. Jennings MG. Ahn DK.Institution Stanford Center for Research in Disease Prevention, Stanford University School of Medicine, Palo Alto, California 94304-1825, USA. [email protected] Cancer-related health behaviors and screening practices among Latinos: findings from a community and agricultural labor camp survey.Source Ethnicity & Disease. 13(3):376-86, 2003 Summer.Abstract OBJECTIVE: To examine whether cancer-related health behaviors and screening practices differ within a population of Latino adults, including those often missed by cancer surveys. DESIGN: Cross-sectional survey, conducted in 2000. Sample of 461 women and 356 men from the community (75% with unlisted telephones) and 188 men fromagricultural labor camps, 18-64 years of age. SETTING: Monterey County, California. OUTCOMES: Six health behaviors and risk factors: obesity, poor nutrition, physical inactivity, high alcohol use, and smoking. Five health practices and screening testsused to detect cervical, breast, and colorectal cancer. RESULTS: Most respondents were born in Mexico, spoke Spanish, and had lived in the United States 10 years or more. In both surveys, more than 60% were overweight including more than 20% who were obese. Men, especially from labor camps, reported high dietary fat intake, low fruit intake, and high alcohol use. For every additional 5 years lived in the UnitedStates, the odds of obesity increased 25% for women, and the odds of high-fat/fast food intake and high alcohol use increased 35% and 50%, respectively for labor camp men. Screening rates for cervical and breast cancer were high and met Healthy People2000 objectives. In contrast, screening rates for colorectal cancer were low; among those 50 and older, approximately 70%-80% of women and men from the community sampleand 100% of men from the labor camp sample had never had a blood stool test. Unmarried women, in particular, had poor nutrition and low screening rates. CONCLUSIONS: Cancer control programs for Latinos need a particular focus on weight, nutrition, physical activity, alcohol, and colorectal screening.
<84>Unique Identifier 12894959Authors Kehoe KA. Melkus GD. Newlin K.Institution Yale University School of Nursing, New Haven, Connecticut 06536-0740, USA.Title Culture within the context of care: an integrative review.[see comment]. [Review] [29 refs]Source
Page 43

1-200.txt Ethnicity & Disease. 13(3):344-53, 2003 Summer.Abstract The purpose of this integrative review was to examine the literature on culturallyrelevant healthcare interventions, and their effect on health outcomes, in an attempt to determine whether culture matters in the context of healthcare delivery. Research literature on culturally relevant interventions from the past 20 years was reviewed using computerized searches of Medline and CINAHL databases. Results of thereview indicate that culturally relevant interventions significantly improve health outcomes for patients with diabetes mellitus (DM), drug addiction, sexually transmitted infections (STIs), and other health problems. It appears that the designof culturally relevant interventions does not require specific knowledge of particular ethnic or cultural groups, but of cross-cultural process principles. Because the studies are highly variable with respect to design and method, it is difficult to isolate which particular aspects of the interventions are specifically associated with favorable outcomes. In addition, few of the studies examined long-term effects of the interventions on outcomes. [References: 29]
<85>Unique Identifier 12893504Authors Holt DJ. Phillips KA. Shapiro ER. Becker AE.Institution Department of Psychiatry, Harvard Medical School, Massachusetts General Hospital, Charlestown, MA 02129, USA. [email protected] "My Face Is My Fate": biological and psychosocial approaches to the treatment of awoman with obsessions and delusions.Source Harvard Review of Psychiatry. 11(3):142-54, 2003 May-Jun.
<86>Unique Identifier 12891093Authors Elhai JD. Forbes D. Creamer M. McHugh TF. Frueh BC.Institution Disaster Mental Health Institute, University of South Dakota, 414 E. Clark Street,SDU 114, Vermillion, South Dakota 57069-2390, USA.Title Clinical symptomatology of posttraumatic stress disorder-diagnosed Australian and United States Vietnam combat veterans: an MMPI-2 comparison.Source Journal of Nervous & Mental Disease. 191(7):458-64, 2003 Jul.Abstract The authors compared MMPI-2 scores of 95 Australian and 96 US Vietnam combat veterans diagnosed with posttraumatic stress disorder (PTSD) from structured PTSD clinical interviews. Groups were strikingly similar on the MMPI-2 clinical and validity scales but were different on two content scales, with higher scores on FRS (fears) and BIZ (bizarre mentation) for the US sample. Employment status was included as a factor, because it too discriminated groups, but it did not interact with the veteran group variable to produce scale differences. The roles of employment status and disability payments are considered in accounting for differences in the psychiatric presentations of the groups. Results suggest that American and Australian Vietnam combat PTSD samples are very similar to each other, with implications for the treatment outcome literature.
<87>Unique Identifier 12886712
Page 44

1-200.txtAuthors Baker B. Evans M. DeCastro F. Schosser R.Institution University of Kentucky Medical Center, USA.Title Leprosy in a Mexican immigrant.Source Journal of the Kentucky Medical Association. 101(7):289-94, 2003 Jul.Abstract A new diagnosis of borderline lepromatous leprosy was established in a man who hadimmigrated to Kentucky from Mexico. He was placed on a World Health Organization treatment regimen consisting of dapsone, clofazimine, and rifampin. The biology of leprosy, its diagnosis, treatment, and worldwide impact are reviewed. Because of thepotential for highly mobile populations to export endemic diseases, Kentucky physicians must expand their lists of differential diagnoses.
<88>Unique Identifier 12882849Authors Davidson MB.Institution Clinical Trials Unit, Charles R. Drew University, Los Angeles, California 90059, USA. [email protected] Effect of nurse-directed diabetes care in a minority population.Source Diabetes Care. 26(8):2281-7, 2003 Aug.Abstract OBJECTIVE: To determine whether diabetes care directed by nurses following detailed protocols and algorithms and supervised by a diabetologist results in meeting the evidence-based American Diabetes Association (ADA) process and outcome measures more often than care directed under usual care in a minority population. RESEARCH DESIGN AND METHODS: Studies were mainly conducted in two Los Angeles Countyclinics. In clinic A, nurse-directed diabetes care was provided to 252 patients (92%Hispanic and 2% African-American) referred by their primary care providers. These patients were hierarchically matched with 252 diabetic patients in clinic B (79% Hispanic and 19% African American). When nurse-directed care was abruptly discontinued in clinic A for administrative reasons, it was reestablished in clinic B. Those patients were randomly selected from a teaching clinic, and the outcomes in114 patients who completed 1 year were compared with outcomes derived the year before receiving nurses' care. The following process and outcome measures were assessed in the study: 1) number of visits, 2) diabetes education, 3) nutritional counseling, 4) HbA(1c), 5) lipid profiles, 6) eye exams, 7) foot exams, 8) renal evaluations, and 9) ACE inhibitor therapy in appropriate patients. RESULTS: For patients under nurse-directed diabetes care in both clinics A and B, almost all process measures were carried out significantly more frequently than for the appropriate control patients. Under the care of nurses in clinic A, HbA(1c) levels fell 3.5% from 13.3 to 9.8% in the 120 patients who were followed for at least 6 months, as compared with a 1.5% fall from 12.3 to 10.8% under usual (physician-directed) care in clinic B. During the year before enrolling in nurse-directed care in clinic B, mean HbA(1c) levels decreased from 10.0 to 8.5%. Atthe end of a year under the nurses' care, the values fell further to 7.1%. The median value fell from 8.3 to 6.6%. CONCLUSIONS: Specially trained nurses who followdetailed protocols and algorithms under the supervision of a diabetologist can markedly improve diabetes outcomes in a minority population. This approach could help blunt the increased morbidity and mortality noted in minority populations.
<89>Unique Identifier 12866785
Page 45

1-200.txtAuthors Gillmore MR. Stielstra S. Huang B. Baker SA. Beadnell B. Morrison DM.Institution School of Social Work, University of Washington, Seattle, USA. [email protected] Heterosexually active men's beliefs about methods for preventing sexually transmitted diseases.Source Perspectives on Sexual & Reproductive Health. 35(3):121-9, 2003 May-Jun.Abstract CONTEXT: Most research on heterosexual transmission of HIV and other sexually transmitted diseases (STDs) has focused on women. However, heterosexual transmissionof STDs cannot be prevented without a better understanding of men's, as well as women's, sexual beliefs and behaviors. METHODS: Heterosexually active men's beliefs about four methods of STD prevention--abstinence, mutual monogamy, use of male condoms and use of female condoms--were elicited through open-ended interviews. A survey based on these responses was administered to a random sample of 486 heterosexually active men, and scores were calculated to examine their beliefs abouteach behavior. Additional analyses explored how these beliefs were related to men's characteristics and to their actual behavior. RESULTS: The men held both positive and negative beliefs about the outcomes of using each method and thought that their partners, close friends, health care providers, family members and, to some extent, friends at church had opinions about whether they should use each method. Multiple regression analyses showed that the men's beliefs were related to their marital status and, to some extent, their race or ethnicity and education. Beliefs about theoutcomes of practicing abstinence, practicing mutual monogamy and using male condomswith steady partners were significantly related to these behaviors; beliefs about whether they had support for practicing monogamy or using male condoms with steady partners were significant predictors of doing so. CONCLUSIONS: Encouraging safer-sexpractices among heterosexually active men will require addressing their beliefs and perceived norms about alternative methods of preventing STDs.
<90>Unique Identifier 12862185Authors Asplund K. Ashburner S. Cargill K. Hux M. Lees K. Drummond M. GAIN International Investigators.Institution Department of Medicine, University Hospital, Umea, Sweden. [email protected] Health care resource use and stroke outcome. Multinational comparisons within the GAIN International trial.Source International Journal of Technology Assessment in Health Care. 19(2):267-77, 2003Spring.Abstract BACKGROUND AND PURPOSE: Outcome in patients hospitalized for acute stroke varies considerably between populations. Within the framework of the GAIN International trial, a large multicenter trial of a neuroprotective agent (gavestinel, glycine antagonist), stroke outcome in relation to health care resource use has been compared in a large number of countries, allowing for differences in case mix. METHODS: This substudy includes 1,422 patients in 19 countries grouped into 10 regions. Data on prognostic variables on admission to hospital, resource use, and outcome were analyzed by regression models. RESULTS: All results were adjusted for differences in prognostic factors on admission (NIH Stroke Scale, age, comorbidity).There were threefold variations in the average number of days in hospital/institutional care (from 20 to 60 days). The proportion of patients who metwith professional rehabilitation staff also varied greatly. Three-month case fatality ranged from 11% to 28%, and mean Barthel ADL score at three months varied
Page 46

1-200.txtbetween 64 and 73. There was no relationship between health care resource use and outcome in terms of survival and ADL function at three months. The proportion of patients living at home at three months did not show any relationship to ADL function across countries. CONCLUSIONS: There are wide variations in health care resource use between countries, unexplained by differences in case mix. Across countries, there is no obvious relationship between resource use and clinical outcome after stroke. Differences in health care traditions (treatment pathways) andsocial context seem to be major determinants of resource use. In making comparisons between countries, great care should be exercised in using outcome variables as indicators of quality of stroke care.
<91>Unique Identifier 12860807Authors Paz SH. Globe DR. Wu J. Azen SP. Varma R. Los Angeles Latino Eye Study.Institution Doheny Eye Institute, Department of Ophthalmology and Preventive Medicine, Keck School of Medicine, Los Angeles, CA 90033-9224, USA.Title Relationship between self-reported depression and self-reported visual function inLatinos.Source Archives of Ophthalmology. 121(7):1021-7, 2003 Jul.Abstract OBJECTIVE: To validate and assess the relationship between self-reported depression as measured by a single item on the Medical Outcomes Study Short-Form 12 (SF-12) and self-reported visual function. METHODS: The Los Angeles Latino Eye Studyis population-based and designed to assess the prevalence of visual impairment, ocular disease, and visual functioning in Latinos. Both the 25-item National Eye Institute-Visual Function Questionnaire (NEI VFQ-25) (self-reported visual function)and the SF-12 (health-related quality of life) were administered. A single item fromthe SF-12 was used to measure self-reported depression and validated against the Center for Epidemiologic Studies-Depression measure of depression. Covariate-adjusted NEI VFQ-25 subscale scores were contrasted across the 6 response choices of the SF-12, as well as across 3 combined response categories of the SF-12 using analysis of covariance. Covariate-adjusted regression analyses assessed the contribution of self-reported depression in explaining self-reported visual function. RESULTS: The sensitivity and specificity of the SF-12 single item with theCenter for Epidemiologic Studies-Depression measure was 0.96 and 0.50, respectively.Using the 3 combined response categories of the SF-12 single item, it was found that(1) all covariate-adjusted subscales of the NEI VFQ-25 were statistically significantly different across the self-reported depression categories (P<.001) and (2) covariate-adjusted self-reported depression was a significant predictor of self-reported visual function (P<.001). CONCLUSIONS: A single SF-12 item may be usedas a measure of self-reported depression. In addition, self-reported depression is an important covariate to consider when assessing self-reported visual function in Latinos.
<92>Unique Identifier 12861963Authors Sarkisian CA. Brown AF. Norris KC. Wintz RL. Mangione CM.Institution Division of Geriatrics, UCLA School of Medicine, Los Angeles, California 90095-1687, USA. [email protected] A systematic review of diabetes self-care interventions for older, African American, or Latino adults. [Review] [37 refs]Source
Page 47

1-200.txt Diabetes Educator. 29(3):467-79, 2003 May-Jun.Abstract PURPOSE: This study systematically identified and examined published self-care interventions designed to improve glycemic control or quality of life (QoL) among older, African American, or Latino adults. METHODS: Six electronic databases were searched. Eligible publications were those that described an intervention to change knowledge, beliefs, or behavior among adults with diabetes who were either older than 55 years, African American, or Latino, and that measured the outcomes of glycemic control or QoL. RESULTS: Twelve studies met the inclusion criteria, of which 8 were randomized controlled trials (RCTs). Of the 8 RCTs, improved glycemic control was reported in the intervention arm of 5 RCTs compared with the control arm. Of the 4 RCTs that examined QoL, improved QoL was reported in the intervention arm of 1 study. Characteristics of successful interventions included poor glycemic control at baseline (A1C > 11%), cultural or age-tailoring the intervention, use of group counseling or support, and involvement of spouses and adult children. CONCLUSIONS: Large-scale clinical trials designed according to cultural and age criteria specific for older Latinos and African Americans with diabetes are needed to determine how best to address this growing public health problem. [References: 37]
<93>Unique Identifier 12854303Authors Buescher PA.Institution State Center for Health Statistics, North Carolina Division of Public Health, 1908Mail Service Center, Raleigh, NC 27699-1908, USA. [email protected] A review of available data on the health of the Latino population in North Carolina.Source North Carolina Medical Journal. 64(3):97-105, 2003 May-Jun.Abstract OBJECTIVE: To portray major health problems and conditions in the Latino population of North Carolina. STUDY DESIGN: Presentation of descriptive information from North Carolina data sets on Latino health issues, with whites and African Americans as comparison groups. DATA SOURCES/STUDY SETTING: Statewide data on the health of the Latino population are provided from the following data sets: North Carolina Behavioral Risk Factor Surveillance System (BRFSS), death certificates, North Carolina Office of the Chief Medical Examiner records, sexually transmitted disease reports, reported pregnancies, certificates of live birth, North Carolina Pregnancy Risk Assessment Monitoring System (PRAMS), and North Carolina Birth Defects Monitoring Program (BDMP) cases. DATA COLLECTION METHODS: Review of existingdata systems. PRINCIPAL FINDINGS: Latinos in North Carolina have high death rates from motor vehicle injuries and homicide. Latinos who die from unintentional injuries, homicide, and suicide are much more likely than whites or African Americans to have a high blood alcohol level. Latinos are less likely than other groups to have health insurance. Latinos have much higher pregnancy rates, both for teens and older women, and are more likely to begin prenatal care late or have no prenatal care. Rates of sexually transmitted disease are higher than those for whites but lower than those for African Americans. Latinos are more likely to initiate breastfeeding. Latinos have a higher rate of neural tube defects compared to the other groups, while being less likely to take folic acid every day before pregnancy. Despite lower family incomes, later entry into prenatal care, and higher rates of certain birth defects, Latinos had the lowest rates of low birth weight andinfant mortality. Lower rates of smoking during pregnancy among Latinos may partially account for the better birth outcomes. CONCLUSIONS: Many of the health issues among Latinos in North Carolina are consistent with the fact that they are a very young, mainly recently-arrived, immigrant population with more males than females. RELEVANCE: These findings may provide a basis for designing more effective health improvement programs for the Latino population of North Carolina.
Page 48

1-200.txt
<94>Unique Identifier 12847537Authors Petrova A. Mehta R. Anwar M. Hiatt M. Hegyi T.Institution Department of Pediatrics, University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, Saint Peter's University Hospital, New Brunswick, NJ 08903-0591, USA.Title Impact of race and ethnicity on the outcome of preterm infants below 32 weeks gestation.Source Journal of Perinatology. 23(5):404-8, 2003 Jul-Aug.Abstract OBJECTIVES: To determine the impact of race/ethnicity on mortality and morbidity such as intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), bronchopulmonary dysplasia (BPD) and bacteriologically confirmed sepsis, assisted ventilation, surfactant administration, intrauterine growth retardation (IUGR), and patent ductus arteriosus (PDA) among very prematurely delivered infants. STUDY DESIGN: Retrospective study of a cohort of 1006 preterm neonates with gestational age ranging from 22 to 32 weeks discharged from the Neonatal Intensive Care Unit (NICU) between 1998 and 2001. Subgroup analysis according to gestational age (GA) (22 to 24, 25 to 28, and 29 to 32 weeks) and plurality (singleton and multiple) was performed using the chi(2) test and an analysis of variance. RESULTS: Of the 1006 infants, 54.3% were white, 21.7% black, 13.7% Hispanic, and 10.3% were classified asOther. Multiple births among white infants were approximately twice that in (42.4%) black infants (22.1%), and was also significantly higher than in the Hispanic (28.3%) and other race/ethnic groups (25.2%). Overall, a higher proportion of black infants were born with a GA <or=28 weeks (n=115, 55.3%) than white (n=201, 37.1%) and Hispanic (n=53, 38.4%), p<0.05. Therefore, black neonates had a lower GA (27.9+/-2.9 weeks) and birth weight (1170+/-463 g) as compared to white (p<0.0002) and Hispanic infants (p<0.0001). There was no significant impact of race/ethnicity on the mean gestational age in any of the gestational age categories. Infant mortality and morbidity in each gestational age category by race/ethnicity were comparable. The multiple birth black infants were seen to have a lower gestational age and birth weight as compared to singleton black as well as to white, Hispanic and other race/ethnic groups. However, this did not influence morbidity and mortality in multiple birth black neonates. The result of this study showed that thelevel of prematurity and not plurality predominantly influences the rate of infant mortality and morbidity in each race/ethnic category. CONCLUSIONS: The reduction in gestational age and birth weight in black neonates is not associated with an increased risk of infant mortality and morbidity. In general, the outcomes of black singleton and multiple pregnancies were comparable with those of white, Hispanic andother race/ethnic groups.
<95>Unique Identifier 12845930Authors Huxtable LM. Borowski D.Title Evaluation of lipid-lowering therapies at an ethnically diverse clinic.Source American Journal of Health-System Pharmacy. 60(12):1282-3, 2003 Jun 15.
<96>Unique Identifier 12841972
Page 49
1-200.txtAuthors Gerbert B. Berg-Smith S. Mancuso M. Caspers N. Danley D. Herzig K. Brand R.Institution School of Dentistry and School of Medicine, University of California at San Francisco, San Francisco, CA 94117, USA. [email protected] Video study of physician selection: preferences in the face of diversity.Source Journal of Family Practice. 52(7):552-9, 2003 Jul.Abstract OBJECTIVES: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member's sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections. STUDY DESIGN: Participants selected a video doctor after viewing a briefintroduction and again after viewing the delivery of a prevention message. POPULATION: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other). OUTCOMES MEASURED: Initialand final video doctor selections; ratings of video doctors on interpersonal qualities. RESULTS: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans).In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non-European American video doctor. CONCLUSIONS: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients' preferences.
<97>Unique Identifier 12836142Authors Thomas MD. Olivares SA. Kim HJ. Beilke C.Institution Department of Psychosocial & Community Health, School of Nursing, University of Washington, Seattle, WA 98195-7263, USA. [email protected] An intensive cultural experience in a rural area.Source Journal of Professional Nursing. 19(3):126-33, 2003 May-Jun.Abstract More well-trained mental health professionals serving rural and minority populations are needed. This article describes an intensive clinical experience for psychiatric mental health nursing graduates in the rural, culturally diverse Tri-Cities (Pasco, Richland, and Kennewick) of Washington. Before discussing the short-term learning experience and outcomes, the social history of the area is explained because of its impact on current health needs and the kinds of learning opportunities available. In addition, personal reflections of student participants are included.
<98>Unique Identifier 12834376Authors Dijkstra A. Coleman M. Tomas C. Valimaki M. Dassen T.Institution
Page 50

1-200.txt Northern Centre For Healthcare Research, University of Groningen, Groningen, The Netherlands. [email protected] Cross-cultural psychometric testing of the Care Dependency Scale with data.Source Journal of Advanced Nursing. 43(2):181-7, 2003 Jul.Abstract BACKGROUND: The importance of the present study lies in addressing whether it is justified to compare the care dependency status of older patients from different settings and cultures using the same instrument. AIM: The aim of this international study was to compare the psychometric properties of the Care Dependency Scale (CDS) by analysing data gathered in Finland, Spain and the United Kingdom (UK). METHOD: The Finnish, Spanish and UK research instruments were translations of the original Dutch CDS. Psychometric evaluations of this were carried out for each country separately as well as for the three countries combined, based on a convenience sample of 378 older patients. RESULTS: High alpha coefficients between 0.94 and 0.97were obtained. Subsequent test-retest and interrater reliability revealed moderate to almost perfect kappa values. CONCLUSION: One of the main outcomes of the international comparison was that the findings between the three countries showed more similarities than differences in psychometric assessment, indicating that the CDS can be used for care dependency assessment in different countries.
<99>Unique Identifier 12833470Authors Sherman ME. Devesa SS.Institution Department of Health and Human Services, National Institutes of Health, National Cancer Institute, Bethesda, Maryland 20892, USA. [email protected] Analysis of racial differences in incidence, survival, and mortality for malignanttumors of the uterine corpus.Source Cancer. 98(1):176-86, 2003 Jul 1.Abstract BACKGROUND: In the United States, incidence rates for malignant tumors of the uterine corpus are lower among blacks than among whites, whereas mortality rates arehigher among blacks. Reasons for the higher level of mortality among blacks have been debated. METHODS: Using data from the Surveillance, Epidemiology, and End Results program, the authors compared incidence rates by histopathologic type for malignant tumors of the uterine corpus (including uterus, not otherwise specified) during the period 1992-1998 among white Hispanic, black, and white non-Hispanic patients. The authors also compared cumulative relative survival rates for blacks and whites by histopathologic type and by other factors, and they calculated estimated type-specific mortality rates. RESULTS: Overall incidence (per 100,000 woman-years) of corpus malignancy was significantly lower among white Hispanics (14.04; 95% confidence interval [CI], 13.39-14.72) and blacks (15.31; 95% CI, 14.61-16.04) compared with white non-Hispanics (23.43; 95% CI, 23.06-23.81). Compared with white non-Hispanics, blacks had significantly higher incidence rates of serous/clear cell carcinoma (rate ratio, 1.85; 95% CI, 1.61-2.12), carcinosarcoma(rate ratio, 2.33; 95% CI, 1.99-2.72), and sarcoma (rate ratio, 1.56; 95% CI, 1.31-1.86). Survival was worse for blacks than for whites in every histopathologic category and in 'usual' types of endometrial adenocarcinoma, stratified by stage, grade, and age. Rare aggressive tumor types accounted for 53% of mortality among blacks, compared with 36% among whites. CONCLUSIONS: Less favorable outcomes for usual types of endometrial adenocarcinoma and for rare aggressive tumors contribute equally to the relatively high mortality due to corpus cancer among black women.
<100>Unique Identifier
Page 51

1-200.txt 12823785Authors May KM. Phillips LR. Ferketich SL. Verran JA.Institution University of Texas at Austin School of Nursing, 1700 Red River, Austin, TX 78701,USA. [email protected] Public health nursing: the generalist in a specialized environment.Source Public Health Nursing. 20(4):252-9, 2003 Jul-Aug.Abstract In implementing a generalist model of public health nursing (the Comprehensive Multi-level Nursing Practice Model) in a rural county health department, a research team encountered critical challenges. The framework for the model was a philosophy of public health nursing practice and action research to support the public health nurse generalist role. Challenges in implementing the model stemmed from conflicts between the research team and the health department that were rooted in philosophical differences about how to implement care and the nature of nursing and the public health nursing role. Key factors were the subtle forces operating in the public health environment that constrain the public health nurse generalist role. Based on conflicts that arose in implementing the model, implications for public health nursing practice are in opportunities to influence policy at health department and other levels and responsibility for assuring professional practice.
<101>Unique Identifier 12815492Authors Lee JE. Fos PJ. Zuniga MA. Kastl PR. Sung JH.Institution School of Dentistry, University of Nevada, Las Vegas, NV, USA.Title Health-related quality of life of cataract patients: cross-cultural comparisons ofutility and psychometric measures.Source Ophthalmic Epidemiology. 10(3):177-91, 2003 Jul.Abstract BACKGROUND: This study was conducted to assess the presence and/or absence of cross-cultural differences or similarities between Korean and United States cataractpatients. A systematic assessment was performed using utility and psychometric measures in the study population. RESEARCH DESIGN: A cross-sectional study design was used to examine the comparison of preoperative outcomes measures in cataract patients in Korea and the United States. Study subjects were selected using non-probabilistic methods and included 132 patients scheduled for cataract surgery in one eye. PARTICIPANTS: Subjects were adult cataract patients at Samsung and Kunyang General Hospital in Seoul, Korea, and Tulane University Hospital and Clinicsin New Orleans, Louisiana. MEASUREMENTS: Preoperative utility was assessed using theverbal rating scale and standard reference gamble techniques. Current preoperative health status was assessed using the SF-36 and VF-14 surveys. Current preoperative Snellen visual acuity was used as a clinical measure of vision status. RESULTS: Korean patients were more likely to be younger (p = 0.001), less educated (p = 0.001), and to have worse Snellen visual acuity (p = 0.002) than United States patients. Multivariate analysis of variance (MANOVA) revealed that in contrast to Korean patients, United States patients were assessed to have higher scoring in general health, vitality, VF-14, and verbal rating for visual health. This higher scoring trend persisted after controlling for age, gender, education and Snellen visual acuity. The difference in health-related quality of life (HRQOL) between the two countries was quite clear, especially in the older age and highly educated group. CONCLUSIONS: Subjects in Korea and the United States were significantly different in quality of life, functional status and clinical outcomes. Subjects in the United States had more favorable health outcomes than those in Korea. These differences may be caused by multiple factors, including country-specific
Page 52

1-200.txtdifferences in economic status, health care system, cultural value system, and health policy. Cross-cultural differences should be considered when making international comparisons of quality of life.
<102>Unique Identifier 12814215Authors Rew L. Becker H. Cookston J. Khosropour S. Martinez S.Institution School of Nursing, The University of Texas at Austin, Austin, Texas 78701-1499, USA. [email protected] Measuring cultural awareness in nursing students.Source Journal of Nursing Education. 42(6):249-57, 2003 Jun.Abstract Recognizing the need for a valid and reliable way to measure outcomes of a programto promote multicultural awareness among nursing faculty and students, the authors developed a cultural awareness scale. In the first phase of the study, a scale consisting of 37 items was generated from a literature review on cultural awareness,sensitivity, and competence in nursing. A Cronbach's alpha reliability coefficient of .91 was obtained from a sample of 72 student nurses. In the second phase, the items were presented to a panel of experts in nursing and culture to determine content validity. A content validity index of .88 was calculated, and the total number of items on the scale was reduced to 36. The scale then was administered to 118 nursing students. Data from the two samples then were combined, and factor analysis was conducted to support construct validity. Cronbach's alpha for the combined samples was .82.
<103>Unique Identifier 12806712Authors Mkoka S. Vaughan J. Wylie T. Yelland H. Jelsma J.Institution School of Health and Rehabilitation Sciences, University of Cape Town.Title The pitfalls of translation--a case study based on the translation of the EQ-5D into Xhosa.Source South African Medical Journal. 93(4):265-6, 2003 Apr.Abstract There is an evident need for standardised, internationally recognised instruments to measure health-related outcomes that are also locally applicable. The European Quality of Life 5-Dimensions (EQ-5D) is a widely used measure of health-related quality of life (HRQoL) that was translated into Xhosa. This communication outlines some of the different cultural and linguistic issues that had to be addressed duringthe translation process. The translation guidelines provided by the EuroQol group were followed. This involved both forward and backward translations by Xhosa speakers, with consensus meetings after each. Thereafter, lay panel respondent testing of the consensus version was performed. Eventually a credible Xhosa version of the EQ-5D was produced. Concepts which proved surprisingly difficult to transfer across the languages and cultures included 'mobility', 'confined to bed' and the choice of word to denote 'male'. The translation process prompted lengthy discussionand proved more challenging than initially anticipated. Despite the rigorous processfollowed, later additions had to be made to the questionnaire after field testing. It would appear that extreme caution should be exercised when using a questionnaire in a culture and language different from the one in which it was originally developed and validated. If this is not done, the validity of cross-cultural research projects may be open to question.
Page 53

1-200.txt
<104>Unique Identifier 12805037Authors Crandall SJ. George G. Marion GS. Davis S.Institution Department of Family and Community Medicine, Wake Forest University School of Medicine, Wiston-Salem, NC 27157, USA. [email protected] Applying theory to the design of cultural competency training for medical students: a case study.Source Academic Medicine. 78(6):588-94, 2003 Jun.Abstract Although literature suggests that providing culturally sensitive care promotes positive health outcomes for patients, undergraduate medical education currently does not provide adequate cultural competency training. At most schools, cultural competency, as a formal, integrated, and longitudinal thread within the overall curriculum, is still in its infancy. In this article, the authors summarize the current practice of cultural competency training within medical education and describe the design, implementation, and evaluation of a theoretically based, year-long cultural competency training course for second-year students at Wake Forest University School of Medicine. Evaluation of the results indicate that the course was successful in improving knowledge, attitudes, and skills related to cultural competence as well as bringing about positive changes in the medical school's approach to cultural competency training. Also discussed are the implications of the outcomes for the development of culturally competent physicians and how using appropriate theory can help achieve desired outcomes.
<105>Unique Identifier 12805036Authors Kagawa-Singer M. Kassim-Lakha S.Institution UCLA School of Public Health and Asian American Studies, Los Angeles, California 90095, USA. [email protected] A strategy to reduce cross-cultural miscommunication and increase the likelihood of improving health outcomes.Source Academic Medicine. 78(6):577-87, 2003 Jun.Abstract Encounters between physicians and patients from different cultural backgrounds arebecoming commonplace. Physicians strive to improve health outcomes and increase quality of life for every patient, yet these discordant encounters appear to be a significant factor, beyond socioeconomic barriers, in creating the unequal and avoidable excess burden of disease borne by members of ethnic minority populations in the United States. Most clinicians lack the information to understand how cultureinfluences the clinical encounter and the skills to effectively bridge potential differences. New strategies are required to expand medical training to adequately address culturally discordant encounters among the physicians, their patients, and the families, for all three may have different concepts regarding the nature of the disease, expectations about treatment, and modes of appropriate communication beyondlanguage. The authors provide an anthropological perspective of the fundamental relationship between culture and health, and outline systemic changes needed within the social and legal structures of the health care system to reduce the risk of cross-cultural miscommunication and increase the likelihood of improving health outcomes for all populations within the multicultural U.S. society. The authors define the strengths inherent within every culture, provide a guideline for the
Page 54

1-200.txtclinician to evaluate disease and illness within its cultural context, and outline the clinical skills required to negotiate among potential differences to reach mutually desired goals for care. Last, they indicate the structural changes requiredin the health care setting to enable and support such practice.
<106>Unique Identifier 12805034Authors Betancourt JR.Institution Institute for Health Policy, Massachusetts General Hospital, Boston, Massachusetts, USA. [email protected] Cross-cultural medical education: conceptual approaches and frameworks for evaluation.Source Academic Medicine. 78(6):560-9, 2003 Jun.Abstract Given that understanding the sociocultural dimensions underlying a patient's health values, beliefs, and behaviors is critical to a successful clinical encounter, cross-cultural curricula have been incorporated into undergraduate medical education. The goal of these curricula is to prepare students to care for patients from diverse social and cultural backgrounds, and to recognize and appropriately address racial, cultural, and gender biases in health care delivery. Despite progress in the field of cross-cultural medical education, several challenges exist. Foremost among these is the need to develop strategies to evaluatethe impact of these curricular interventions. This article provides conceptual approaches for cross-cultural medical education, and describes a framework for student evaluation that focuses on strategies to assess attitudes, knowledge, and skills, and the impact of curricular interventions on health outcomes.
<107>Unique Identifier 12794955Authors Kartchner R. Callister L.Institution Brigham Young University, College of Nursing, USA.Title Giving birth. Voices of Chinese women.Source Journal of Holistic Nursing. 21(2):100-16, 2003 Jun.Abstract The meaning of the childbirth experience for Chinese women living in the People's Republic of China is described in this phenomenological study. Ten primiparous womenparticipated in audiotaped interviews within 5 months of giving birth, 9 from Beijing and 1 from Chongqing. The interviews were translated by a bilingual native Chinese speaker and transcribed by the researcher. Themes were identified from the rich narrative data, including the One Child Policy's influence on childbearing, thetransition to motherhood, and the influence of the cultural practice of "doing the month" (zuo yue zi). The findings provide insights into how nurses can provide better nursing care by learning about and validating specific cultural practices related to childbearing. The rising number of Chinese immigrants to the United States reflects the increasing need for more culturally competent care by nurses to ensure positive perinatal health outcomes.
<108>Unique Identifier 12795316
Page 55

1-200.txtAuthors Hoppe E. Carnevali T. Dobies P.Institution Southern California College of Optometry, Optometric Center of Los Angeles, Los Angeles, California, USA. [email protected] Characteristics of urban Hispanic patients with diabetes presenting for eye care services.Source Optometry (St. Louis, Mo.). 74(5):291-8, 2003 May.Abstract BACKGROUND: Studies have demonstrated the differential impact of diabetic complications among Hispanic patients. This study profiles 50 patients seen in an urban optometric setting and compares them with a hospital-based ophthalmology clinic in the same community. METHODS: A sample of 50 Hispanic patients with diabetes was selected. Descriptive statistics were calculated and compared with the literature. RESULTS: Demographics show an equal split between genders, with a mean age of 52.7 years. Duration of diabetes ranged from 1 month to 22 years. Most patients had type II diabetes and were using oral hypoglycemics. Few had insurance coverage, with a wide range in time since last physical examination and last eye examination. Only 28% had an eye examination in the past year. The majority had goodocular outcomes. CONCLUSIONS: Compared with published reports from the literature, the patients in this sample were more likely to be male, and were less likely to have insurance and more likely to be newly diagnosed with diabetes. Patients in thissample were more likely to use oral hypoglycemics, and ophthalmic surveillance was more appropriate. While they were more likely to have had a previous eye examination, they were also more likely to have a BVA of 20/40 or worse. This suggests that the patients seen in the optometric setting differ from those seen in the hospital-based clinic.
<109>Unique Identifier 12792258Authors McClowry SG. Halverson CF. Sanson A.Institution Division of Nursing, Steinhardt School of Education, New York University, New York, 10003, USA. [email protected] A re-examination of the validity and reliability of the School-Age Temperament Inventory.Source Nursing Research. 52(3):176-82, 2003 May-Jun.Abstract BACKGROUND: As a construct, temperament provides a framework for understanding differences among individuals in reaction to their life experiences. The measurementof the construct concerns both researchers and clinicians. OBJECTIVE: The purpose ofthis study was to examine whether the School-Age Temperament Inventory continued to demonstrate reliability and validity when retested with three existent samples of parent respondents. METHOD: Sample 1 was a sociodemographically and racially heterogeneous group of 200 children from New England in the United States. Data for Sample 2 was provided by 589 mothers and fathers from the state of Georgia in the United States. In Sample 3, data was provided by parents (principally, mothers) of 1,391 adolescents from Australia. Orthogonal Procrustes rotations were conducted to examine the underlying structure of the inventory when it was contrasted with the results obtained in the original standardization of the tool. RESULTS: The total coefficients of congruence for the samples were .88 to .97, while those of the four factors ranged from .84 to .98. Across the samples, Cronbach alphas for the dimensions ranged from .80 to .92. Independent t-tests identified that boys were significantly more active and less task persistent than girls. However, regression analyses revealed that sex accounted for only 5% of the variance in task persistenceand activity. DISCUSSION: The results provide substantial additional support for the
Page 56

1-200.txtreliability and validity of the School-Age Temperament Inventory. Recommendations for future research are offered which include exploring the role of temperament in contributing to developmental outcomes in children and examining cross-cultural samples.
<110>Unique Identifier 12791796Authors Galea S. Ahern J. Tardiff K. Leon A. Coffin PO. Derr K. Vlahov D.Institution Center for Urban Epidemiologic Studies, New York Academy of Medicine, New York, New York 10029-5283, USA. [email protected] Racial/ethnic disparities in overdose mortality trends in New York City, 1990-1998.Source Journal of Urban Health. 80(2):201-11, 2003 Jun.Abstract Racial/ethnic disparities in health and disease have been present in the United States for the past century. Although differences such as individual access to health care and health-related behaviors account for some of these health disparities, it is likely that a combination of individual and contextual-level factors determine the differential rates of disease between racial/ethnic groups. Westudied fatal accidental drug overdose in New York City between 1990 and 1998 to describe differences in racial/ethnic patterns over time and to develop hypotheses about factors that might contribute to these differences. During this period, rates of overdose death were consistently higher among blacks and Latinos compared to whites. In addition, cocaine was more common among black decedents, while opiates and alcohol were more common among Latino and white decedents. Differences in situational factors, such as differential likelihood of activating emergency medicalresponse, may in part explain the consistently higher overdose mortality rates observed among minorities. Further study to determine the individual and contextual factors that explain these observed disparities in overdose death may identify effective areas for public health intervention and provide insight into factors underlying racial/ethnic disparities in other health outcomes.
<111>Unique Identifier 12785564Authors Miranda J. Duan N. Sherbourne C. Schoenbaum M. Lagomasino I. Jackson-Triche M. Wells KB.Institution Department of Psychiatry, Georgetown University Medical Center, Washington, DC, USA.Title Improving care for minorities: can quality improvement interventions improve care and outcomes for depressed minorities? Results of a randomized, controlled trial.Source Health Services Research. 38(2):613-30, 2003 Apr.Abstract OBJECTIVE: Ethnic minority patients often receive poorer quality care and have worse outcomes than white patients, yet practice-based approaches to reduce such disparities have not been identified. We determined whether practice-initiated quality improvement (QI) interventions for depressed primary care patients improve care across ethnic groups and reduce outcome disparities. STUDY SETTING: The sample consists of 46 primary care practices in 6 U.S. managed care organizations; 181 clinicians; 398 Latinos, 93 African Americans, and 778 white patients with probable depressive disorder. STUDY DEIGN: Matched practices were randomized to usual care orone of two QI programs that trained local experts to educate clinicians; nurses to
Page 57

1-200.txteducate, assess, and follow-up with patients; and psychotherapists to conduct Cognitive Behavioral Therapy. Patients and physicians selected treatments. Interventions featured modest accommodations for minority patients (e.g., translations, cultural training for clinicians). DATA EXTRACTION METHODS: Multilevellogistic regression analyses assessed intervention effects within and among ethnic groups. PRINCIPAL FINDINGS: At baseline, all ethnic groups Latino, African American,white) had low to moderate rates of appropriate care and the interventions significantly improved appropriate care at six months (by 8-20 percentage points) within each ethnic group, with no significant difference in response by ethnic group. The interventions significantly decreased the likelihood that Latinos and African Americans would report probable depression at months 6 and 12; the white intervention sample did not differ from controls in reported probable depression at either follow-up. While the intervention significantly improved the rate of employment for whites and not for minorities, precision was low for comparing intervention response on this outcome. It is important to note that minorities remained less likely to have appropriate care and more likely to be depressed than white patients. CONCLUSIONS: Implementation of quality improvement interventions that have modest accommodations for minority patients can improve quality of care for whites and underserved minorities alike, while minorities may be especially likely to benefit clinically. Further research needs to clarify whether employment benefits are limited to whites and if so, whether this represents a difference in opportunities. Quality improvement programs appear to improve quality of care without increasing disparities, and may offer an approach to reduce health disparities.
<112>Unique Identifier 12785426Authors Ard JD. Carter-Edwards L. Svetkey LP.Institution Duke Hypertension Center, Duke University Medical Center, Durham, NC 27710, USA.Title A new model for developing and executing culturally appropriate behavior modification clinical trials for African Americans. [Review] [49 refs]Source Ethnicity & Disease. 13(2):279-85, 2003 Spring.Abstract Past clinical trials addressing behavior modification for cardiovascular disease (CVD) prevention have not been culturally appropriate for African Americans. This supposition is borne out by the continued challenges researchers face not only in recruiting and retaining African Americans in clinical trials, but also in achievingthe desired outcomes among this population. Investigators have limited resources to develop culturally appropriate CVD prevention trials. The scientific literature reveals 2 models for implementing culturally appropriate interventions applicable toCVD prevention among African Americans; however, these models are not easily appliedto the clinical trial setting. We propose a new model for developing a culturally appropriate clinical trial. The clinical trial is a function of the investigator's cultural framework, meaning that an investigator will have more difficulty designingclinical trials appropriate for use with cultures other than his or her own, a definite limitation when attempting to effectively reach diverse populations. Differences between the cultural frameworks of most clinical trials and African Americans' cultural frameworks lead to intrinsic biases, limiting the ability of African Americans to achieve the desired outcomes for any particular trial. An African-American participant's degree of immersion in traditional African-American culture, or acculturation, influences the magnitude of these biases. Investigators must be aware of, and attempt to mitigate, such biases so that the trial's potentialfor success is equitable across ethnic groups. In addition, investigators must understand how to effectively address relevant biases of African Americans without challenging their ethnic identity. Steps to decrease biases are described. [References: 49]
Page 58

1-200.txt
<113>Unique Identifier 12785044Authors Lewis CR. de Vedia A. Reuer B. Schwan R. Tourin C.Institution Center for Palliative Studies, San Diego Hospice, San Diego, California, USA.Title Integrating complementary and alternative medicine (CAM) into standard hospice andpalliative care. [Review] [38 refs]Source American Journal of Hospice & Palliative Care. 20(3):221-8, 2003 May-Jun.Abstract In the United States, there are 629 million visits to complementary and alternative medicine (CAM) providers each year. Many adults appear to value both conventional and CAM approaches. Because of this public interest and promising evidence that CAM relieves suffering and improves quality of life, we established a program of CAM, known as Integrative Palliative Care (IPC), in a US hospice. This paper outlines our strategy of collaborative relationships with community schools oftraditional Chinese medicine (TCM), massage, and harp therapy. It also describes theuse of volunteers and small grants and donations to develop and maintain a program of CAM in the hospice setting. The difficulties of research design, problems with tracking outcomes, and the shortcomings of providing therapies with this model are discussed. [References: 38]
<114>Unique Identifier 12784823Authors Rollins G.Title Study outlines relationship between racial/ethnic differences and breast cancer outcomes.Source Report on Medical Guidelines & Outcomes Research. 14(3):10, 12, 2003 Feb 7.
<115>Unique Identifier 12774644Authors Ryan MJ.Title Interview with a quality leader. Sister Mary Jean Ryan on the first Baldrige Awardin healthcare. Interview by Susan V. White and Mary Savitsky.Source Journal for Healthcare Quality. 25(3):24-5, 2003 May-Jun.Abstract Sr. Mary Jean Ryan, Franciscan Sister of Mary, is president/chief executive officer of SSM Health Care (SSMHC), one of the largest Catholic healthcare systems in the United States, with 23,000 employees and 5,000 affiliated physicians serving in 21 hospitals and 3 nursing homes. This year SSMHC became the first healthcare recipient of the Malcolm Baldrige National Quality Award. During her 16-year tenure,Sr. Mary Jean has emphasized three key themes: preservation of the earth's resources, valuing ethnic and gender diversity, and commitment to continuous qualityimprovement (CQI). She is co-author of CQI and the Renovation of an American Health Care System: A Culture Under Construction, published by ASQ Quality Press in 1997. Sr. Mary Jean has received numerous honors, including the Brotherhood/Sisterhood Award from the National Conference of Community and Justice; (one of) 20 Distinguished Women/St. Louis area; Governor's Quality Leadership Award (Missouri); (one of) 25 Most Influential Women in Business in St. Louis; and the Corporation
Page 59

1-200.txtthat Makes a Difference Award from the International Women's Forum. She serves on a number of healthcare and local, state, and national boards. She received a master's degree in hospital and health administration from Xavier University in Cincinnati. She is a nurse and has been a Franciscan Sister of Mary for more than 40 years.
<116>Unique Identifier 12771697Authors Corbett RW. Ryan C. Weinrich SP.Institution School of Nursing, East Carolina University, Rivers Building, Greenville, NC 27858, USA. [email protected] Pica in pregnancy: does it affect pregnancy outcomes?.Source MCN, American Journal of Maternal Child Nursing. 28(3):183-9; quiz 190-1, 2003 May-Jun.Abstract PURPOSE: To discover the prevalence of pica, the documentation of pica on medical records, and any relationship of pica to pregnancy outcomes in rural socioeconomically disadvantaged pregnant women. STUDY DESIGN AND METHODS: Prospective, descriptive, correlational investigation with 128 women who sought prenatal care from two rural community health agencies. Demographic and sociocultural variables, pica practices, pica substances ingested, and pregnancy outcomes were collected. RESULTS: Thirty-eight percent of these pregnant women practiced pica. African-American women reported practicing pica more often than other ethnicities. Substances ingested included ice (>1 cup/day), freezer frost, laundry starch, cornstarch, clay dirt, and baked clay dirt. Polypica (ingestion of more than one substance) was practiced by 11 women. Women practicing pica were more likely to have been underweight prior to pregnancy, and smoked fewer cigarettes. Women reporting daily pica practice were significantly more likely to have lower prenatal hematocrits than women who did not practice pica, or who practiced pica less frequently than daily. No specific pregnancy complication was associated with the practice of pica. CLINICAL IMPLICATIONS: Pica exists, and might be more common than healthcare providers assume. Although this study did not show specific pregnancy complications associated with pica, other studies have shown anemia and lead poisoning among women who practice pica. It is not clear that patients volunteer information about pica, so it would be helpful if nurses queried patients at each prenatal visit regarding pica practice. Discussion of pica practices should be based on a nonjudgmental model, for pica may have strong cultural implications, and may be practiced for cultural reasons unknown to the nurse.
<117>Unique Identifier 12765706Authors Reidpath DD.Institution School of Health Sciences, Deakin University, 221 Burwood Hwy, Burwood VIC 3125, Australia. [email protected] "Love thy neighbour"-it's good for your health: a study of racial homogeneity, mortality and social cohesion in the United States.Source Social Science & Medicine. 57(2):253-61, 2003 Jul.Abstract This paper explores the idea that in societies that experience racial tension, increasing racial heterogeneity will be associated with poorer health outcomes, and this effect will be observable in the health of both the minority and the majority group. Here, the association between mortality and racial homogeneity in the United
Page 60

1-200.txtStates is examined. The level of racial homogeneity, indexed by the proportion of blacks in each state of the 50 states in the US, was examined in relation to all-cause mortality, adjusted for age and disaggregated by race and sex. The level of poverty in each state was controlled for in ordinary least squares regression models. The level of racial homogeneity was significantly associated with age adjusted mortality rates for both blacks and whites, accounting for around 30% of the variance in mortality rates in the total population and the white population. Every 1% increase in the percentage of the state population who were black was associated with an increase in the total mortality rate of 5.06 per 100000 and an increase in the white mortality rate of 3.58 per 100000. Based on the data, this suggests, for example, that racial heterogeneity in Mississippi accounts for around 14% of the white mortality rate and in New York and Delaware it accounts for around 7%. These results appear to support the social cohesion thesis that in societies that are intolerant, mortality rates will increase as the proportion of racial or ethnic minorities increase in population. Limitations and explanations for the findings are discussed.
<118>Unique Identifier 12766629Authors Treno AJ. Grube JW. Martin SE.Institution Prevention Research Center, Berkeley, CA, USA. 2150 Shattuck Avenue, Suite 900, Berkeley, CA 94704, USA. [email protected] Alcohol availability as a predictor of youth drinking and driving: a hierarchical analysis of survey and archival data.Source Alcoholism: Clinical & Experimental Research. 27(5):835-40, 2003 May.Abstract BACKGROUND: Much attention has recently been directed toward developing preventiveinterventions to reduce drinking and driving through efforts to limit the numbers and locations of alcohol outlets at the community level. Although evaluations of these efforts have suggested linkages between alcohol outlets and problem outcomes, they have not addressed the linkage between outlets and drinking and driving among youth. The analysis reported here investigates the relationship between alcohol outlet densities and underage drinking and driving as self-reported on two telephonesurveys conducted in California. METHODS: These analyses were based on data obtainedfrom two telephone surveys conducted by the Prevention Research Center and archival data collected by the California Department of Alcoholic Beverage Control and the USCensus Bureau. The sample for the first survey consisted of 15- to 20-year-old adolescents and young adults contacted by telephone, using a random digit dialing ofexchanges in the greater San Francisco Bay Area. A second set of survey data was similarly collected by a random sample of households throughout California, and the Bay Area subset was also used for this analysis. RESULTS: At the individual level, older respondents were more likely to report drinking and driving and riding with drinking drivers, whereas females and Asians were less so. At the aggregate or city-level, alcohol outlet density, as measured by the number of on- and off-premises establishments licensed to sell alcohol, was associated with both drinking and driving and riding with drinking drivers. These effects were moderated by a number of individual level effects, with younger respondents and females more likely to be affected by outlet densities. CONCLUSIONS: The findings here provide support for the implementation of policies targeting alcohol outlet density reductions. Areas with large numbers of such outlets provide ample opportunities to youth for alcohol purchases.
<119>Unique Identifier 12762084Authors
Page 61

1-200.txt Mosher WD. Deang LP. Bramlett MD.Title Community environment and women's health outcomes: contextual data.Source Vital & Health Statistics - Series 23, Data From the National Survey of Family Growth. (23):1-72, 2003 Apr.Abstract OBJECTIVES: This report presents some illustrative data and analyses from the Contextual Data File for the 1995 National Survey of Family Growth (NSFG). Data are shown by the woman's race and Hispanic origin, and selected characteristics of the community in which she lived. METHODS: Cycle 5 of the NSFG was based on in-person interviews with a national sample of 10,847 women 15-44 years of age in the United States in 1995. The interview included questions on the woman's births, marriages, contraceptive use, and characteristics such as her race and education. Measures of the characteristics of the woman's neighborhood were added to the interview data. RESULTS: This report shows that several simple measures of the social and economic status (SES) and resources of the woman's community of residence are closely associated with outcomes such as delayed childbearing, unwanted births, current marital status, the use of male or female contraceptive sterilization, breast-feeding, vaginal douching, and cigarette smoking. CONCLUSIONS: It is well-documented that the outcomes studied in this report are closely associated withindividual characteristics such as age, race, education, and household income. But this report shows that these outcomes are also related to characteristics of the communities in which the individuals live. Researchers are encouraged to use the NSFG Contextual Data File to study these relationships further.
<120>Unique Identifier 12760605Authors Carroll N.Institution Department of Health and Human Services, National Institutes of Health, Bethesda, Maryland, USA.Title Implications of menopausal hormonal therapy for African American and Hispanic women.Source Journal of the National Medical Association. 95(2):114-7, 2003 Feb.
<121>Unique Identifier 12751647Authors Kerr MH. Beck K. Shattuck TD. Kattar C. Uriburu D.Institution Shattuck and Associates, Annapolis, MD 21401, USA. [email protected] Family involvement, problem and prosocial behavior outcomes of Latino youth.Source American Journal of Health Behavior. 27 Suppl 1:S55-65, 2003.Abstract OBJECTIVE: To explore the relations between familial factors and behavioral outcomes in Latino adolescents using a youth development framework. METHODS: A convenience sample of Latino youth (n = 446) completed an anonymous survey. Multiplelinear regression was used to examine the associations between levels of family involvement and problem and prosocial behavior outcomes. RESULTS: Higher levels of parental monitoring and familial connectedness were consistently associated with less problem-behavior involvement. Sociocultural encouragement was consistently associated with more prosocial-behavior involvement. CONCLUSION: The family context is critical to the prevention of problem behaviors and the promotion of prosocial
Page 62
1-200.txtbehaviors among Latino adolescents.
<122>Unique Identifier 12751646Authors Bloomberg L. Ganey A. Alba V. Quintero G. Alcantara LA.Institution Program Planning and Evaluation Specialist, Bloomberg Consulting, Mahtomedi, MN 55115, USA. [email protected] Chicano-Latino Youth Leadership Institute: an asset-based program for youth.Source American Journal of Health Behavior. 27 Suppl 1:S45-54, 2003.Abstract OBJECTIVE: To describe the theory of action that links the Chicano-Latino Youth Leadership Institute with positive youth development and to highlight promising practices. METHODS: A logic model provided the basis for data collection through written surveys, focus groups, reflection forms, and analysis of Minnesota Student Survey Results. RESULTS: Primary participant outcomes include increased levels of community service, improved peer relationships, and higher graduation rates than those of Chicano-Latino non-participants. CONCLUSION: Based on the first 3 years of program evaluation data, this culturally specific youth development model is positively impacting a significant number of participants.
<123>Unique Identifier 12751620Authors Ralston PA.Institution College of Human Sciences, Florida State University, Tallahassee, FL. 32306, USA. [email protected] Diversifying the health professions: a model program.Source American Journal of Health Behavior. 27(3):235-45, 2003 May-Jun.Abstract OBJECTIVE: To describe a university-based mentoring program in the food and nutritional sciences that addresses the need for multicultural professionals in allied health fields. METHODS: The conceptual model for the program includes inputs (goals, resources), transformational process (professional development, social support and recognition) and outcomes (student participation, graduation and placement rates). Outcome data were analyzed using descriptive statistics. RESULTS: Between 1993 and 2001, 49 students completed the program, 43 (88%) graduated, 23 were placed in graduate or professional schools, and 21 obtained professional positions. CONCLUSION: This mentoring model resulted in multicultural students who successfully entered health professions.
<124>Unique Identifier 12748490Authors Leslie JC. Galvin SL. Diehl SJ. Bennett TA. Buescher PA.Institution Department of Obstetrics and Gynecology, Mountain Area Health Education Center, 93Victoria Road, Asheville, NC 28801, USA.Title Infant mortality, low birth weight, and prematurity among Hispanic, white, and African American women in North Carolina.
Page 63

1-200.txtSource American Journal of Obstetrics & Gynecology. 188(5):1238-40, 2003 May.Abstract OBJECTIVES: The study was undertaken to compare Hispanic birth outcomes with thoseof white and African American women in North Carolina and to examine variables associated with adverse birth outcomes among Hispanic women. STUDY DESIGN: Retrospective comparison of birth outcomes by ethnicity/race, from linked birth/infant death certificates in North Carolina (1993-1997) was conducted. Multivariate, binary logistic regression and chi(2) analysis were used to examine relationships between available medical and sociodemographic index values and composite birth outcomes among Hispanic women. RESULTS: Infant mortality rates were lowest among Hispanic women. Low birth weight and prematurity rates were similar to those of white women and lower than those of African American women. Variables significantly related to healthy composite birth outcomes among Hispanic women included higher education, no preterm delivery history, prenatal care, marriage, andno daily tobacco use. CONCLUSION: Hispanic birth outcomes in North Carolina were better than those of African American women and similar to those of white women, despite use of prenatal care and socioeconomic characteristics similar to African American women.
<125>Unique Identifier 12748488Authors Drescher KM. Monga M. Williams P. Promecene-Cook P. Schneider K.Institution Department of Obstetrics, Gynecology, and Reproductive Science, University of Texas Houston Medical School, 6431 Fannin, Houston, TX 77030, USA.Title Perceived quality of life in pregnant adolescent girls.Source American Journal of Obstetrics & Gynecology. 188(5):1231-3, 2003 May.Abstract OBJECTIVE: The purpose of this study was to describe the perceived quality of lifeand functional status of pregnant adolescent girls. STUDY DESIGN: The Medical Outcomes Survey-Short Form 36, version 2, is a multi-item scale that measures a subject's perception of eight health components. These questionnaires and demographic surveys were completed by teen patients aged 14 to 18 years during antenatal visits to a university-based resident continuity clinic. Mean scores (0 points indicates the poorest perceived health and functional status, 100 points indicates the highest perceived health and functional status) were then compared with mean scores for women in the general population of all ages and, specifically, women aged 18 to 24 years. RESULTS: Forty-two pregnant adolescent girls participated(median age, 16 years; median education level, 10th grade). Ninety-two percent of the girls belonged to a racial-ethnic minority, and all qualified for Medicaid. Pregnant adolescent girls had slightly lower overall scores for all components of perceived quality of life, with the exception of the vitality component. Scores weresignificantly lower than normative scores (by >1 SD) for only the physical functioning component. CONCLUSION: There appears to be little change in perceived quality of life in pregnant adolescent girls. This information may be useful in the provision of comprehensive care to pregnant adolescent girls.
<126>Unique Identifier 12745638Authors Stansbury JP. Mathewson-Chapman M. Grant KE.Institution Rehabilitation Outcomes Research Center at the North Florida/South Georgia Veterans Health System, Gainesville, FL 32608, USA.Title
Page 64

1-200.txt Gender schema and prostate cancer: veterans' cultural model of masculinity.Source Medical Anthropology. 22(2):175-204, 2003 Apr-Jun.Abstract Coming to terms with disease, chronic illness, and aging may be challenging for men who adhere to an inflexible gender schema. In this study of elder U.S. veterans'ideas about masculinity, we find that prostate cancer patients reaffirm a strongly moral normalizing discourse about "being a man" yet tend to separate roles and values from male physical and sexual attributes. Using systematic data collection methods taken from cognitive anthropology, we map veterans' schema of masculinity and examine the relative importance that cancer patients and non-patients give to gender attributes. The results demonstrate the complementarity between cognitive andnarrative approaches in medical anthropology. This research also suggests the hypotheses that (1) coming to terms with iatrogenesis may involve a subtle reformulation of masculinity and that (2) men with a fixed view of masculinity may have worse health outcomes than do those who accept the changes accompanying their treatment for prostate cancer.
<127>Unique Identifier 12745027Authors Howard DL.Institution Department of Natural and Sciences and Mathematics, Environmental Science Program and Office of Research and Sponsored Programs, Shaw University, 118 E. South Street,Raleigh, NC 27601, USA. [email protected] Are the treatment goals of culturally competent outpatient substance abuse treatment units congruent with their client profile?.Source Journal of Substance Abuse Treatment. 24(2):103-13, 2003 Mar.Abstract This study examines whether organizational treatment goals varied among outpatientsubstance abuse treatment (OSAT) units identified as providing a level of culturallycompetent care for African Americans. Cross-sectional data from the 1995 National Drug Abuse Treatment System Survey (NDATSS) was used. Of the nationally representative, stratified sample of 699 units, 618 (88%) participated. Spearman correlation, analysis of variance, Behrens-Fisher t-tests, chi-square, and multivariate logistic regression were used. Culturally competent units, even after controlling for organizational and client characteristics, were more apt than non-culturally competent units to indicate that achieving steady employment, spiritual strength, and physical health were important treatment goals. A congruencyexists among culturally competent OSAT units between the client profile, which is more distressful than that for non-culturally competent units, and the orientation of treatment goals, which are more holistic; that is, treating the total individual,rather than the addiction only.
<128>Unique Identifier 12745026Authors Howard DL.Institution Department of Natural Sciences and Mathematics, Environmental Science Program, Office of Research and Sponsored Programs, Shaw University, 118 E. South Street, Raleigh, NC 27601, USA. [email protected] Culturally competent treatment of African American clients among a national sampleof outpatient substance abuse treatment units.Source
Page 65

1-200.txt Journal of Substance Abuse Treatment. 24(2):89-102, 2003 Mar.Abstract This study measures the level of cultural competency with respect to African American clients that exists among a national sample of outpatient substance abuse treatment (OSAT) units and determines the relationship of cultural competency to various characteristics of these units and their clients. The study utilizes cross-sectional data from the 1995 National Drug Abuse Treatment System Survey (NDATSS). The sample for NDATSS was randomly selected from a comprehensive list of OSAT programs compiled by the Institute for Social Research at the University of Michigan in 1994. Of the nationally representative, stratified sample of 699 units, 618 (88%) participated. Spearman correlation, analysis of variance, Behrens-Fisher t-tests, and chi-square were used for bivariate comparisons. Culturally competent units are typically public, federal-funded organizations. Staffs of culturally competent units are typically college-educated with specialized treatment certification. High severity of illness as well as increased social distresses is pervasive among the clients of culturally competent units. Consideration of this client profile may be a key determinant in evaluating the effectiveness of cultural competency for African American substance abusers.
<129>Unique Identifier 12742601Authors Kennelly B. O'Shea E. Garvey E.Institution Department of Economics, The National University of Ireland, Galway, Ireland. [email protected] <[email protected]>Title Social capital, life expectancy and mortality: a cross-national examination.Source Social Science & Medicine. 56(12):2367-77, 2003 Jun.Abstract This paper analyses the relationship between social capital and population health.The analysis is carried out within an econometric model of population health in 19 countries in the Organisation for Economic Co-operation and Development countries using panel data covering three different time periods. Social capital is measured by the proportion of people who say that that they generally trust other people and by membership in voluntary associations. The model performs well in explaining health outcomes. We find very little statistically significant evidence that the standard indicators of social capital have a positive effect on population health. By contrast, per capita income and the proportion of health expenditure financed by the government are both significantly and positively associated with better health outcomes. The paper casts doubt upon the widely accepted hypothesis that social capital has a positive effect on health and illustrates the importance of testing this kind of hypothesis in an extended model.
<130>Unique Identifier 12742776Authors Bollinger LC.Institution Columbia University College of Physicians and Surgeons, New York, New York, USA.Title The need for diversity in higher education.Source Academic Medicine. 78(5):431-6, 2003 May.Abstract The author states that there is a need in all higher education, including the health professions, for racial, ethnic, and other kinds of diversity, and describes two court cases involving the University of Michigan's undergraduate and law school
Page 66

1-200.txtaffirmative action admission policies. The outcomes of these cases will profoundly affect the quality of U.S. higher education, professional education, and graduate education. Affirmative action is one of the tools that many universities use to ensure the kind of comprehensively diverse student body that helps teach students toparticipate fully in this country's heterogeneous democracy and the global economy. Students are exposed to classmates with different life experiences, their prior assumptions are challenged, and they discover what they and their classmates have incommon. And a variety of Fortune 500 corporations state that employees and managers who graduated from institutions with diverse student bodies demonstrate a variety ofkey skills that are crucial in the U.S. workplace. The author discusses why "colorblind" and "socioeconomically oriented" admission policies do not work and that they have only a tiny effect on white students' chances of acceptance. Until K-12 education is greatly improved for minorities, affirmative action is needed to give a "leg up" to students who might not otherwise be admitted but who can do the academic work. In medical education, there is a special urgency for diversity, sinceit is known that minority physicians are more likely to practice in areas where there are high concentrations of minorities.
<131>Unique Identifier 12738696Authors Ohtaki S. Ohtaki T. Fetters MD.Institution Department of English Language, Kanazawa Medical University, 1-1 Daigaku Uchinada-machi, Kahoku-gun, Ishikawa-ken 920-0293, Japan. [email protected] Doctor-patient communication: a comparison of the USA and Japan.Source Family Practice. 20(3):276-82, 2003 Jun.Abstract BACKGROUND: Little is known about the differences and similarities between doctor-patient communication patterns in different cultures. OBJECTIVES: The aim of this study was to examine communication patterns of doctor-patient consultations in two different cultures, namely the USA and Japan, and to elucidate linguistic differences and similarities in communication. METHODS: This cross-sectional study used quantitative discourse analysis from linguistics to compare 40 doctor-patient consultations: 20 out-patient consultations of five physicians in the USA and 20 out-patient consultations of four physicians in Japan. The main outcomes measured were time spent in each phase of the encounter, number of categorized speech acts, distribution of question types and frequencies of back-channel responses and interruptions. RESULTS: The average length of doctor-patient encounters was 668.7 s in the USA and 505 s in Japan. US physicians spent relatively more time on treatmentand follow-up talk (31%) and social talk (12%), whereas the Japanese had longer physical examinations (28%) and diagnosis or consideration talk (15%). Japanese doctor-patient conversations included more silence (30%) than those in the USA (8.2%). The doctor-patient ratios of total speech acts were similar (USA 55% versus 45%; Japan 59% versus 41%). Physicians in both countries controlled communication during encounters by asking more questions than the patients (75% in the USA; 78% inJapan). The Japanese physicians and patients used back-channel responses and interruptions more often than those in the USA. CONCLUSIONS: While doctor-patient communication differed between the USA and Japan in the proportion of time spent in each phase of the encounter, length of pauses and the use of back-channel responses and interruptions, physician versus patient ratios of questions and other speech acts were similar. The variations may reflect cultural differences, whereas the similarities may reflect professional specificity stemming from the shared needs to fill the information gap between physician and patient. Adequate awareness of these differences and similarities could be used to educate clinicians about the best approaches to patients from particular cultural backgrounds.
Page 67

1-200.txt<132>Unique Identifier 12736889Authors Otiniano ME. Du XL. Ottenbacher K. Markides KS.Institution Department of Internal Medicine, Sealy Center on Aging, University of Texas Medical Branch, Galveston 77555-0460, USA.Title The effect of diabetes combined with stroke on disability, self-rated health, and mortality in older Mexican Americans: results from the Hispanic EPESE.Source Archives of Physical Medicine & Rehabilitation. 84(5):725-30, 2003 May.Abstract OBJECTIVE: To examine how diabetes in combination with stroke affects functional activities of daily living (ADLs) and instrumental activities of daily living (IADLs), self-rated health, and 5-year mortality in elderly Mexican Americans with or without other comorbid conditions. DESIGN: Longitudinal study. SETTING: Five southwestern states. PARTICIPANTS: A total of 3050 subjects of age 65 years or older, of whom 23% had diabetes and 6% had a stroke. INTERVENTIONS: Not applicable. MAIN OUTCOME MEASURES: ADL and IADL disabilities, self-rated health, and 5-year mortality. RESULTS: Subjects with both diabetes and stroke but without other comorbid conditions had almost 18 times higher risk of having any ADL disability (odds ratio [OR]=18.8; 95% confidence interval [CI], 3.3-105.2) and 10 times higher risk of having any IADL disability (OR=10.6; 95% CI, 1.1-101.5), compared with subjects without either of the 2 conditions. The risk of disability was further increased if the subject had a comorbid condition (hypertension, heart attack, cancer, hip fracture, arthritis). The risk of fair or poor self-rated health was 3.5(95% CI, 1.4-8.6) and the hazard ratio for 5-year mortality was 2.4 (95% CI, 1.7-3.4) in people with both diseases. CONCLUSIONS: Diabetes and stroke in combination is strongly associated with a higher risk of disabilities, poor self-rated health, and 5-year mortality in elderly Mexican Americans. The effect on outcomes appears to follow an additive model. Information on disability risk and morbidity and mortality should be useful to rehabilitation professionals in discharge planning and allocation of therapy resources.
<133>Unique Identifier 12734024Authors Berkowitz RJ.Institution Eastman Department of Dentistry, School of Medicine and Dentistry, Eastman Dental Center, University of Rochester, Rochester, New York 14620, USA. [email protected] Causes, treatment and prevention of early childhood caries: a microbiologic perspective.Source Journal (Canadian Dental Association). 69(5):304-7, 2003 May.Abstract Early childhood caries (ECC) is a virulent form of dental caries that can destroy the primary dentition of toddlers and preschool children. It occurs worldwide, afflicting predominantly disadvantaged children. High-risk North American populations include Hispanic and Native American children, as well as children enrolled in Head Start, a federally funded program for preschool children living in poverty. The prevalence of EEC among these children ranges from 11% to 72%. ECC is an infectious disease, and Streptococcus mutans is the most likely causative agent; diet also plays a critical role in the acquisition and clinical expression of this infection. Early acquisition of S. mutans is a key event in the natural history of the disease. Acquisition may occur via vertical or horizontal transmission. Primary oral colonization by S. mutans coupled with caries-promoting feeding behaviours
Page 68

1-200.txtresults in accumulation of these organisms to levels exceeding 30% of the total cultivable plaque flora which in turn leads to rapid demineralization of tooth structure. Treatment of ECC is costly because the cooperative capacity of babies andpreschool children usually necessitates the use of general anesthesia. Treatment usually consists of restoration or surgical removal of carious teeth along with recommendations regarding feeding habits. However, this approach has resulted in unacceptable clinical outcomes, and relapse rates of approximately 40% have been reported within the first year after dental surgery. Primary prevention of ECC has largely been restricted to counselling parents about caries-promoting feeding behaviours. This approach has also had minimal success. Newer strategies addressing the infectious component through use of topical antimicrobial therapy appear promising.
<134>Unique Identifier 12727702Authors Lee S. Chan YY. Hsu LK.Institution Department of Psychiatry-11F, The Chinese University of Hong Kong, Tai Po Hospital, Tai Po, Hong Kong. [email protected] The intermediate-term outcome of Chinese patients with anorexia nervosa in Hong Kong.Source American Journal of Psychiatry. 160(5):967-72, 2003 May.Abstract OBJECTIVE: The authors determined the intermediate-term outcome of anorexia nervosa for Chinese patients in Hong Kong. METHOD: A consecutive series of 88 patients who fulfilled DSM-III-R criteria for typical (i.e., fat phobic [N=63]) and atypical (i.e., no fat phobia [N=25]) anorexia nervosa were contacted at least 4 years after onset of their illness for semistructured and self-rated assessments of outcome. RESULTS: Three patients (3.4%) died; the mortality ratio for this group against the expected standard for subjects of similar age and gender was 10.5 to 1. Eighty (94.1%) of the remaining 85 patients were successfully traced 9.0 years afteronset of their illness. Good, intermediate, and poor outcomes were seen in 61.8%, 32.9%, and 5.3% of the subjects, respectively. Anorexia nervosa, bulimia nervosa, oreating disorder not otherwise specified was exhibited by 55.0% of the subjects (N=44). Lifetime depressive (81.6%) and anxiety (27.6%) disorders were common. Olderage at onset and the presence of fat phobia independently predicted poor outcome. Patients with atypical anorexia nervosa were symptomatically stable, less likely to demonstrate bulimia, and had a better eating disorder outcome than patients with typical anorexia nervosa. CONCLUSIONS: The outcome profile of Chinese patients supported the cross-cultural disease validity of anorexia nervosa. The cultural fearof fatness not only shaped the manifest content but also added to the chronicity of the illness.
<135>Unique Identifier 12723644Authors Calvo MS. Whiting SJ.Institution Office of Applied Research and Safety Assessment, Center for Food Safety and Applied Nutrition, Food and Drug Administration, HFS-025, 8301 Muirkirk Road, Laurel, MD 20708, USA.Title Prevalence of vitamin D insufficiency in Canada and the United States: importance to health status and efficacy of current food fortification and dietary supplement use. [Review] [30 refs]Source
Page 69

1-200.txt Nutrition Reviews. 61(3):107-13, 2003 Mar.Abstract Several recent studies have identified a surprisingly high prevalence of vitamin Dinsufficiency in otherwise healthy adults living in Canada and the United States. Most striking are the effects of latitude, season, and race. Also noteworthy is thatdietary vitamin D is not reaching the population in greatest need, nor is it very protective against insufficiency. Fluid milk, as the predominant vehicle for vitaminD fortification, is apparently not very effective in staving off vitamin D insufficiency in adults in all populations at all times of the year. [References: 30]
<136>Unique Identifier 12716399Authors Norr KF. Crittenden KS. Lehrer EL. Reyes O. Boyd CB. Nacion KW. Watanabe K.Institution Maternal-Child Nursing, UIC Neighborhoods Initiative (Great Cities Institute), University of Illinois at Chicago, Chicago, Illinois, USA. [email protected] Maternal and infant outcomes at one year for a nurse-health advocate home visitingprogram serving African Americans and Mexican Americans.Source Public Health Nursing. 20(3):190-203, 2003 May-Jun.Abstract This article describes the outcomes at 1 year for a randomized clinical trial of Resources, Education and Care in the Home-Futures: a program to reduce infant mortality through home visits by a team of trained community residents led by a nurse. Low-income, inner-city pregnant women who self-identified as African Americanor Mexican American were recruited in two university prenatal clinics in Chicago. Because African Americans and Mexican Americans differed greatly at intake, we compared their outcomes at 12 months and then examined the effects of the intervention separately for these two groups. Participants were randomly assigned tothe intervention or control group and were interviewed during the last trimester of pregnancy and at 2, 6, and 12 months after birth. The effects of the program varied by race/ethnicity. For African Americans, the program was associated with better maternal documentation of infant immunizations, more developmentally appropriate parenting expectations, and higher 12-month infant mental development scores. For Mexican Americans, the program had positive effects on maternal daily living skills and on the play materials subscale of the Home Observation for the Measurement of the Environment assessment. This study, along with previous research, suggests that home visits by a nurse-health advocate team can improve maternal and infant outcomeseven for inner-city, low-income, minority families. Effective programs must be culturally sensitive, intensive, and adequately staffed and financed.
<137>Unique Identifier 12714994Authors Deconinck H.Institution Geneva Foundation, To Protect Health in War, 6 Route de Ferney, 1202 Geneva, Switzerland.Title The health condition of spinal cord injuries in two Afghan towns.Source Spinal Cord. 41(5):303-9, 2003 May.Abstract STUDY DESIGN: Cross-sectional. OBJECTIVES: To describe the population with spinal cord injury (SCI) in two major towns of Afghanistan. SETTING: Kabul and Herat, Afghanistan, March-July 2001. METHODS: The residents of Kabul and Herat (N=311) with
Page 70

1-200.txttraumatic SCI were retrieved and investigated. They underwent standardised interviews and clinical examinations assessing socio-demographic characteristics andinformation on health condition, injury, quality of life and rehabilitation outcome.RESULTS: The study population could be considered as the survivors in the harsh living conditions in Afghanistan of a supposedly much larger group, counting proportionately fewer females and fewer cervical lesions than expected. Acute care was practically nonexistent. Prevalences of urinary tract infections and pressure sores were high as no good management was available. Basic rehabilitation helped persons with SCI to attain a fairly good level of independence (total functional independence measure score mean=95, SD=19). Their quality of life was significantly lower than their neighbours of same age and sex (P< 0.0001). Along with the economicsecurity and good access to the home, the use of the orthopaedic centre of the International Committee of the Red Cross (ICRC) contributed to a better quality of life. CONCLUSION: Thanks to the rehabilitation programme of the ICRC providing a basic but comprehensive rehabilitation, persons with SCI in Afghanistan are coping rather well. This result is remarkable considering the difficult economic and sanitary circumstances in the poorest country in the world.
<138>Unique Identifier 12713071Authors Serrano VA. Woodruff SI.Institution San Diego State University, Graduate School of Public Health, Center for Behavioral and Community Health Studies, CA 92123, USA.Title Smoking-related attitudes and their sociodemographic correlates among Mexican-origin adult smokers.Source Journal of Community Health. 28(3):209-20, 2003 Jun.Abstract The purpose of the study was to describe smoking-related knowledge and attitudes of a specific group of Latino smokers, and to identify sociodemographic correlates. This study is one of the few to provide information about smoking-related psychosocial variables and their correlates among a Latino subgroup. A survey was administered to a volunteer sample of adult smokers of Mexican-origin (n = 278) to assess their sociodemographic characteristics, and smoking-related knowledge and attitudes. Measures of smoking-related attitudes targeted six constructs: self-efficacy for quitting smoking, anticipated outcomes, intentions to quit, normative expectations, social support, and barriers to quitting. Smoking/cessation knowledge was assessed with a 14 item test. This sample of smokers had high knowledge and positive attitudes about quitting smoking. Several sociodemographic variables were associated with attitudinal knowledge variables, although no consistent pattern of association was seen. Results underscore the complexity between smoking-related attitudes and sociodemographic factors, and are discussed interms of implications for culturally-tailored interventions.
<139>Unique Identifier 12708888Authors Seid M. Castaneda D. Mize R. Zivkovic M. Varni JW.Institution Center for Child Health Outcomes, San Diego, CA 92123, USA. [email protected] Crossing the border for health care: access and primary care characteristics for young children of Latino farm workers along the US-Mexico border.Source Ambulatory Pediatrics. 3(3):121-30, 2003 May-Jun.Abstract
Page 71

1-200.txt OBJECTIVES: To examine prevalence and correlates of cross-border health care for children of Latino farm workers in counties near the US-Mexico border and to compareaccess and primary care in the United States and Mexico. METHODS: Two hundred ninety-seven parents at Head Start centers in San Diego and Imperial counties were surveyed regarding percentage of health care received in Mexico and the United States, access, and primary care characteristics. RESULTS: More than half of all health care was reported as received in Mexico. Reasons for Mexican use revolved around cost, accessibility, and perceptions of effectiveness. Parents of insured children reported slightly more US care, yet even this group reported approximately half of health care in Mexico. Insurance status was related to having a regular source of care, while uninsured children reporting most care in Mexico were less likely than uninsured children in the United States to have had a routine health care visit. Primary care characteristics were related to insurance status and sourceof care. Uninsured children reporting most care in Mexico fared better in some aspects of primary care than uninsured children reporting most care in the United States and as well as children with insurance receiving care in the United States orMexico. CONCLUSIONS: Children of farm workers living along the US-Mexico border, almost irrespective of insurance status, receive a large proportion of care in Mexico. Especially for uninsured children, parent reports of Mexican care characteristics compare favorably with that received in the United States. Mexican health care might be a buffer against vulnerability to poor health outcomes for these children.
<140>Unique Identifier 12696855Authors Wheat JR. Brandon JE. Carter LR. Leeper JD. Jackson JR.Institution University of Alabama School of Medicine, Tuscaloosa, USA. [email protected] Premedical education: the contribution of small local colleges.Source Journal of Rural Health. 19(2):181-9, 2003 Spring.Abstract CONTEXT: Small local colleges may be sources of medical students with the gender, ethnicity, and background that promote identity with and empathy for underserved populations. PURPOSE: This study examined the impact of attendance at these premedical colleges on outcomes of medical education. METHODS: Data for 2508 matriculates to the University of Alabama School of Medicine, a state-supported medical school, were examined according to premedical colleges attended. FINDINGS: Medical students who had graduated from small local colleges were more diverse in gender, race, and rural background than other students. They had slightly lower academic performance in medical school, were more likely to drop out (10.6% versus 5.3% overall), and were more likely to locate in rural areas of the host state. CONCLUSIONS: Small local colleges may be rich sources of student diversity and medical students who choose rural practice, outcomes that are gained at a cost in terms of drop-out rate. Compared with other students, minor differences in performance and larger differences in the drop-out rate raise the question of cultural context and social support during medical school as points for intervention.
<141>Unique Identifier 12692770Authors Hahn EA. Cella D.Institution Evanston Northwestern Healthcare and Institute for Health Services Research and Policy Studies, Northwestern University, Evanston, IL, USA. [email protected]
Page 72

1-200.txt Health outcomes assessment in vulnerable populations: measurement challenges and recommendations. [Review] [97 refs]Source Archives of Physical Medicine & Rehabilitation. 84(4 Suppl 2):S35-42, 2003 Apr.Abstract With growing recognition that some population subgroups are particularly vulnerable to receiving suboptimal health care and achieving poor health outcomes, innovative techniques are required for collecting and evaluating health outcomes data. Research is also needed to better understand the causal pathways linking vulnerability with health outcomes. This article focuses on patients with a chronic illness (cancer) who also have low literacy and/or poor English language skills. We summarize the association among literacy, language, ethnicity, and health outcomes; describe innovative technologies to enhance communication; and discuss the advantages of using psychometric measurement models in health outcomes assessment. Results from our ongoing research projects are presented, including the development of an audiovisual computer-based testing platform for self-administration of questionnaires. Such innovative multimedia technologies allow patients with limited or even no reading ability to participate in outcomes assessment and have the potential to be incorporated into a clinical setting with minimal burden on staff and patients. Appropriate methods are also needed to evaluate measurement equivalence across diverse patient groups, that is, the extent to which items in a questionnaire perform similarly across groups. Item response theory measurement models provide a strategy for differentiating between measurement bias and real differences that may exist between groups. Recommendations for clinical practice andresearch are offered specifically to address medically underserved and vulnerable populations. [References: 97]
<142>Unique Identifier 12671020Authors Freedman AN. Graubard BI. Rao SR. McCaskill-Stevens W. Ballard-Barbash R. Gail MH.Institution Division of Cancer Control and Population Sciences, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892-7344, USA. [email protected] Estimates of the number of US women who could benefit from tamoxifen for breast cancer chemoprevention.Source Journal of the National Cancer Institute. 95(7):526-32, 2003 Apr 2.Abstract BACKGROUND: The Breast Cancer Prevention Trial demonstrated that tamoxifen treatment produced a 49% reduction in the risk of invasive breast cancer among womenat elevated risk for the disease. The U.S. Food and Drug Administration (FDA) subsequently approved tamoxifen for women aged 35 years or older with a 5-year breast cancer risk of 1.67% or higher for breast cancer chemoprevention. However, tamoxifen use has been associated with adverse outcomes, and not all eligible women have a positive benefit/risk ratio. METHODS: We used weighted data from the year 2000 National Health Interview Survey Cancer Control Module to estimate the total number of U.S. women, aged 35-79 years, who were eligible for tamoxifen chemoprevention based on the FDA eligibility criteria. We also estimated the numbersof white and black women who would benefit from tamoxifen chemoprevention on the basis of a positive benefit/risk index developed by Gail et al. RESULTS: Of the 65,826,074 women aged 35-79 years without reported breast cancer in the United States in 2000, 10,232 816 women (15.5%, 95% confidence interval [CI] = 14.7% to 16.3%) would be eligible for tamoxifen chemoprevention. The percentage of U.S. womenwho would be eligible varied dramatically by race, with 18.7% (95% CI = 17.8% to 19.7%) of white women, 5.7% (95% CI = 4.3% to 7.5%) of black women, and 2.9% (95% CI= 2.1% to 3.9%) of Hispanic women being eligible. Of the 50,104,829 white U.S. womenaged 35-79 years, 2,431,911 (4.9%, 95% CI = 4.3% to 5.4%) would have a positive benefit/risk index for tamoxifen chemoprevention. Of the 7,481,779 black U.S. women
Page 73

1-200.txtaged 35-79 years, only 42,768 (0.6%, 95% CI = 0.2% to 1.3%) would have a positive benefit/risk index. Among white women, 28,492 (95% CI = 24,693 to 32,292) breast cancers would be prevented or deferred if those women who have a positive net benefit index took tamoxifen over the next 5 years. CONCLUSION: A substantial percentage of U.S. women would be eligible for tamoxifen chemoprevention according to FDA criteria, but a much smaller percentage would have an estimated net benefit. Nevertheless, this latter percentage corresponds to more than two million women.
<143>Unique Identifier 12666468Authors Santisteban DA. Coatsworth JD. Perez-Vidal A. Kurtines WM. Schwartz SJ. LaPerriere A. Szapocznik J.Institution Department of Psychiatry, University of Miami School of Medicine, Miami, Florida, USA. [email protected] Efficacy of brief strategic family therapy in modifying Hispanic adolescent behavior problems and substance use.Source Journal of Family Psychology. 17(1):121-33, 2003 Mar.Abstract This study investigated the efficacy of brief strategic family therapy (BSFT) withHispanic behavior problem and drug using youth, an underrepresented population in the family therapy research literature. One hundred twenty-six Hispanic families with a behavior problem adolescent were randomly assigned to 1 of 2 conditions: BSFTor group treatment control (GC). Results showed that, compared to GC cases, BSFT cases showed significantly greater pre- to post-intervention improvement in parent reports of adolescent conduct problems and delinquency, adolescent reports of marijuana use, and observer ratings and self reports of family functioning. These results extend prior findings on the efficacy of family interventions to a difficultto treat Hispanic adolescent sample.
<144>Unique Identifier 12665181Authors Fisher JA. Bowman M. Thomas T.Institution Department of Family Practice and Community Medicine, University of Pennsylvania, Philadelphia 19104, USA.Title Issues for South Asian Indian patients surrounding sexuality, fertility, and childbirth in the US health care system.[see comment].Source Journal of the American Board of Family Practice. 16(2):151-5, 2003 Mar-Apr.Abstract BACKGROUND: In 1998 ethnic minorities comprised 28% of the US population, and India is the third most common country of origin for immigrants. Many recently immigrated South Asian Indian patients are seen in health care settings in the United States. To deliver health care effectively to these patients, it is helpful for physicians to understand common cultural beliefs and practices of South Asian Indian patients. METHODS: Two illustrative cases are reported. One author's observations of the care of pregnant and parturient women in India and similar experiences in our own office spurred a literature search of the cultural behaviors surrounding sexuality, fertility, and childbirth. A literature search was conducted in Index Medicus, Grateful Med, and the catalogue of the University of Pennsylvania Arts and Sciences library, using the terms "Indian," "South Asian," "male and femalegender roles," "gynecology in third world," "sexuality," "sexual health," "women's health," "women's health education," "obstetrical practices/India," and "female
Page 74

1-200.txtroles/India." RESULTS: Issues surrounding sexuality and childbirth that arise duringthe US physician-South Asian Indian patient encounter might not correspond to the commonly held knowledge, beliefs, and behaviors of the US health care system. Commoncultural beliefs and behaviors of South Asian Indian patients around sexuality and childbirth experience include the role of the individual patient's duty to society, the patient's sense of place in society, lack of formal sexual education, prearranged marriages, importance of the birth of the first child, little premaritalcontraceptive education, dominance of the husband in contraceptive decisions, and predominant role of women and lack of role for men (including the husband) in the childbirth process. CONCLUSION: Lack of understanding of the Indian cultural mores surrounding sexual education, sexual behavior, and the childbirth experiences can form barriers to Indian immigrants in need of health care. These misunderstandings can also lead to patient dissatisfaction with the health provider and health system,underutilization of health services, and poorer health outcomes for Indian immigrants and their families. For this reason, it is important to teach cultural issues during undergraduate, graduate, and continuing medical education.
<145>Unique Identifier 12657988Authors Koniak-Griffin D. Verzemnieks IL. Anderson NL. Brecht ML. Lesser J. Kim S. Turner-Pluta C.Institution Center for Vulnerable Populations Research, UCLA School of Nursing, Los Angeles, California, 90095, USA. [email protected] Nurse visitation for adolescent mothers: two-year infant health and maternal outcomes.Source Nursing Research. 52(2):127-36, 2003 Mar-Apr.Abstract BACKGROUND: Children of adolescent mothers have higher rates of morbidity and unintentional injuries and hospitalizations during the first 5 years of life than dochildren of adult mothers. OBJECTIVE: The purpose of this study was to evaluate the 2-year postbirth infant health and maternal outcomes of an early intervention program (EIP) of home visitation by public health nurses (PHNs). METHODS: In a randomized controlled trial, a sample of predominantly Latina and African American adolescent mothers was followed from pregnancy through 2 years postpartum. The experimental group (EIP, n = 56) received preparation-for-motherhood classes plus intense home visitation by PHNs from pregnancy through 1 year postbirth; the controlgroup (TPHNC, n = 45) received traditional public health nursing care (TPHNC). Health outcomes were determined based on medical record data; other measures evaluated selected maternal behaviors, social competence, and mother-child interactions. RESULTS: The total days of non-birth-related infant hospitalizations during the first 24 months was significantly lower in the EIP (143 days) than the TPHNC group (211 days) and episodes of hospitalization were fewer; more EIP than THHNC infants were never seen in the emergency room. The EIP mothers had 15% fewer repeat pregnancies in the first 2 years postbirth than TPHNC mothers. The TPHNC mothers significantly increased marijuana use over time, whereas EIP mothers did not. CONCLUSIONS: The EIP improved in selected areas of infant and maternal health, and these improvements were sustained for a period of 1 year following program termination. These findings have important implications for healthcare services.
<146>Unique Identifier 12650729Authors Davis-Floyd R.Institution Department of Anthropology, Case Western Reserve University, Cleveland, OH 44106,
Page 75

1-200.txtUSA. [email protected] Home-birth emergencies in the US and Mexico: the trouble with transport.Source Social Science & Medicine. 56(9):1911-31, 2003 May.Abstract Proponents of the global Safe Motherhood Initiative stress that primary keys to safe home birth include transport to the hospital in cases of need and effective care on arrival. In this article, which is based on interviews with American direct-entry midwives and Mexican traditional midwives, I examine what happens when transport occurs, how the outcomes of prior transports affect future decision-making, and how the lessons derived from the transport experiences of birthing women and midwives in the US and Mexico could be translated into improvements in maternity care. My focus is on home birth in urban areas in Mexico and the US. In both countries, biomedicine and home-birth midwifery exist in separate cultural domains and are based on distinctively different knowledge systems. When a midwife transports a client to the hospital, she brings specific prior knowledge that can be vital to the mother's successful treatment by the hospital system. But the culture of biomedicine in general tends not to understand or recognize as valid the knowledge of midwifery. The tensions and dysfunctions thatoften result are displayed in midwives' transport stories, which I identify as a narrative genre and analyze to show how reproduction can go unnecessarily awry when domains of knowledge conflict and existing power structures ensure that only one kind of knowledge counts. This article describes: (1) disarticulations that occur when there is no correspondence of information or action between the midwife and thehospital staff; and (2) fractured articulations of biomedical and midwifery knowledge systems that result from partial and incomplete correspondences. These twokinds of disjuncture are contrasted with the smooth articulation of systems that results when mutual accommodation characterizes the interactions between midwife andmedical personnel. The conclusion links these American and Mexican transport storiesto their international context, describing how they index crosscultural markers, andsuggest solutions, for "the trouble with transport."
<147>Unique Identifier 12646597Authors Burr JA. Mutchler JE.Institution Gerontology Institute and Department of Gerontology, University of Massachusetts, Boston, 02125-3393, USA.Title English language skills, ethnic concentration, and household composition: older Mexican immigrants.Source Journals of Gerontology Series B-Psychological Sciences & Social Sciences. 58(2):S83-92, 2003 Mar.Abstract OBJECTIVES: The authors examine the living arrangements of older Mexican immigrants to demonstrate how the formation of complex households is related to English language proficiency. Specifically, they examine whether the ability to use the English language is a determinant of an older Mexican immigrant persons' capacity to maintain residential independence. They also examine how living in communities with a relatively high proportion of Hispanic persons impacts household structure. METHODS: Data from the 1990 U.S. Census of Population are used to evaluate multilevel multinomial logistic regression models of living arrangements among older Mexican immigrants. RESULTS: The authors found that strong English language skills increase the likelihood of living independently and increase the likelihood of being the head of a household. They also found that living in an area with a relatively high proportion of Hispanic persons increases the likelihood that older Mexican immigrants will live independently as compared with living with otherswithout headship. Finally, interaction models were examined, demonstrating that
Page 76

1-200.txtliving in a community with a relatively high proportion of Hispanics reduces the strength of the relationship between English language proficiency and living arrangement outcomes for older Mexican immigrants. DISCUSSION: The authors discuss the implications of their findings and point out possible avenues for further research.
<148>Unique Identifier 12643022Authors O'Donnell L. Myint-U A. O'Donnell CR. Stueve A.Institution Education Development Center, Inc., 55 Chapel St., Newton, MA 02458, USA. [email protected] Long-term influence of sexual norms and attitudes on timing of sexual initiation among urban minority youth.Source Journal of School Health. 73(2):68-75, 2003 Feb.Abstract This study assessed whether sexual norms and attitudes expressed during early adolescence by minority youth from economically disadvantaged urban areas produce a sustained influence on the timing of sexual initiation. African American and Latino youth attending three middle schools were enrolled in the Reach for Health study in seventh grade and followed from an average age of 12.2 to 16.1 years. Some 849 respondents answered the question, "Have you ever had sexual intercourse" at four time points: fall seventh, spring seventh, spring eighth, and spring 10th grade. Culturally tailored scales assessed sex norms and outcome expectancies, sexual responsibility, and refusal attitudes at fall seventh grade. Influence of these norms and attitudes in early adolescence on timing of first reported sexual intercourse was examined using ANOVA controlling for gender. At fall seventh grade, 30.7% of boys and 7.7% of girls reported sexual intercourse; by spring 10th grade, the figures were 74.8% and 56.4%, respectively. Those reporting greater peer involvement in sex and more positive sex outcome expectancies were more likely to have initiated sex by fall seventh grade. Through 10th grade, the higher the scores on peer norms (f = 41.08, p < .0001) and outcome expectancies (f = 5.87, p = .002) at entry into seventh grade, the earlier the timing of initiation. Higher scores on sex responsibility at baseline were associated with delayed sexual intercourse (f = 7.36, p < .001), as are refusal attitudes (f = 15.62, p < .0001). Despite significant gender differences in timing of initiation and mean scale scores, these relationships were similar for males and females. Findings suggest the importance ofaddressing sexual norms and attitudes of minority youth in interventions to delay early sexual initiation in urban environments where this risk is high. Given their sustained influence on timing of sexual initiation, such interventions must begin prior to middle school and continue through mid-adolescence, years when early sexualexperience can lead to negative health and social outcomes.
<149>Unique Identifier 12635453Authors Jun JK. Gong WC. Mathur R.Institution College of Pharmacy, Western University of Health Sciences, Pomona, CA, USA.Title Effects of pioglitazone on diabetes-related outcomes in Hispanic patients.Source American Journal of Health-System Pharmacy. 60(5):469-73, 2003 Mar 1.
<150>Page 77

1-200.txtUnique Identifier 12623688Authors Greig R.Institution University of Florida, Gainesville, Florida, USA. [email protected] Ethnic identity development: implications for mental health in African-American and Hispanic adolescents. [Review] [43 refs]Source Issues in Mental Health Nursing. 24(3):317-31, 2003 Apr-May.Abstract One of the key tasks of adolescence is identity development. This includes ethnic identity, or the aspect of identity related to one's membership in an ethnic group. Ethnic identity development has implications for mental health. Those adolescents who achieve a secure sense of themselves as ethnic group members have higher self-esteem and tend to have better mental health overall. This paper reviews the pertinent literature that connects ethnic identity to mental health outcomes in African-American and Hispanic adolescents. The relevance to mental health nursing isalso highlighted. [References: 43]
<151>Unique Identifier 12614296Authors Kadambi PV. Josephson MA. Williams J. Corey L. Jerome KR. Meehan SM. Limaye AP.Institution Department of Internal Medicine, Pathology, University of Chicago, Chicago, IL, USA.Title Treatment of refractory BK virus-associated nephropathy with cidofovir.Source American Journal of Transplantation. 3(2):186-91, 2003 Feb.Abstract BK virus-associated nephropathy (BKVN) has become recognized as an important causeof allograft dysfunction in renal transplant recipients and despite reduction in immunosuppression, 30-40% of recipients ultimately progress to allograft loss. Cidofovir is an antiviral agent that demonstrates in vitro activity against murine polyomavirus and has been proposed for treatment of BKVN in renal allograft recipients. We describe the clinical course, renal function, serial renal histology and urine and blood viral load measurements in two consecutive patients with refractory BKVN who were treated with low-dose cidofovir (0.25 mg/kg IV). In each case, renal dysfunction and BK viral load progressed despite reduced immunosuppression, and persistent BK virus infection was documented in serial renal allograft biopsy specimens. Administration of low-dose cidofovir was associated withclearance of BK virus DNA from blood and allograft, and stabilization of renal function in both patients, without significant toxicity. These preliminary data suggest that low-dose cidofovir may be tolerated, even among renal transplant recipients with significant renal dysfunction due to BKVN. Prospective, controlled trials are warranted to further define the optimal dose, toxicity and potential roleof cidofovir in renal transplant recipients with BK virus nephropathy.
<152>Unique Identifier 12612984Authors Lopes AA. Bragg-Gresham JL. Satayathum S. McCullough K. Pifer T. Goodkin DA. Mapes DL. Young EW. Wolfe RA. Held PJ. Port FK. Worldwide Dialysis Outcomes andPractice Patterns Study Committee.Institution
Page 78

1-200.txt Department of Medicine, Federal University of Bahia, Brazil.Title Health-related quality of life and associated outcomes among hemodialysis patientsof different ethnicities in the United States: the Dialysis Outcomes and Practice Patterns Study (DOPPS).Source American Journal of Kidney Diseases. 41(3):605-15, 2003 Mar.Abstract BACKGROUND: In the United States, an association between mortality risk and ethnicity has been observed among hemodialysis patients. This study was developed toassess whether health-related quality of life (HRQOL) scores also vary among patients of different ethnic backgrounds. Associations between HRQOL and adverse dialysis outcomes (ie, death and hospitalization) also were assessed for all patients and by ethnicity. METHODS: Data are from the Dialysis Outcomes and PracticePatterns Study for 6,151 hemodialysis patients treated in 148 US dialysis facilitieswho filled out the Kidney Disease Quality of Life Short Form. We determined scores for three components of HRQOL: Physical Component Summary (PCS), Mental Component Summary (MCS), and Kidney Disease Component Summary (KDCS). Patients were classifiedby ethnicity as Hispanic and five non-Hispanic categories: white, African American, Asian, Native American, and other. Multiple linear regression models were used to estimate differences in HRQOL scores among ethnic groups, using whites as the referent category. Cox regression models were used for associations between HRQOL and outcomes. Regression models were adjusted for sociodemographic variables, delivered dialysis dose (equilibrated Kt/V), body mass index, years on dialysis therapy, and several laboratory/comorbidity variables. RESULTS: Compared with whites, African Americans showed higher HRQOL scores for all three components (MCS, PCS, and KDCS). Asians had higher adjusted PCS scores than whites, but did not differ for MCS or KDCS scores. Compared with whites, Hispanic patients had significantly higher PCS scores and lower MCS and KDCS scores. Native Americans showed significantly lower adjusted MCS scores than whites. The three major components of HRQOL were significantly associated with death and hospitalization forthe entire pooled population, independent of ethnicity. CONCLUSION: The data indicate important differences in HRQOL among patients of different ethnic groups inthe United States. Furthermore, HRQOL scores predict death and hospitalization amongthese patients. Copyright 2003 by the National Kidney Foundation, Inc.
<153>Unique Identifier 12608489Authors Arroyo JA. Miller WR. Tonigan JS.Institution Center on Alcoholism, Substance Abuse, and Addictions (CASAA), University of New Mexico, Albuquerque, New Mexico 87106, USA.Title The influence of Hispanic ethnicity on long-term outcome in three alcohol-treatment modalities.Source Journal of Studies on Alcohol. 64(1):98-104, 2003 Jan.Abstract OBJECTIVE: Prior research has suggested that treatment-seeking Hispanic clients are not likely to affiliate with Alcoholics Anonymous (AA). It was hypothesized thatAA 12-step facilitation therapy (TSF) would therefore be less effective than cognitive behavioral therapy (CBT) and motivational enhancement therapy (MET) for Hispanics, particularly for those with low acculturation. METHOD: Outcomes for non-Hispanic white (n = 105; 70% male) and Hispanic (n = 100; 80% male) clients at the New Mexico site within Project MATCH were analyzed for evidence of differential treatment response. A pretreatment measure of acculturation to non-Hispanic white culture was available for 80 of the Hispanic clients. RESULTS: Self-identified ethnicity mediated treatment response at distal follow-up, as measured by frequency and intensity of alcohol consumption (p < .02). Hispanics drank with more intensity than did non-Hispanic whites when assigned to TSF; non-Hispanic whites in TSF drank
Page 79

1-200.txtwith less frequency than those in the combined CBT and MET conditions. The modest outcome advantage for TSF observed in Project MATCH appears to have been limited to non-Hispanic clients. Contrary to prediction, level of acculturation did not mediatetreatment response at proximal (Months 1-6 after treatment) or distal follow-up (Months 7-12). CONCLUSIONS: Ethnic self-identification may interact with treatment outcomes in complex ways that are not directly associated with the factors tapped bycommonly used measures of acculturation.
<154>Unique Identifier 12605729Authors Ruiz M. Rejas J. Soto J. Pardo A. Rebollo I.Institution Departamento de Metodologia. Facultad de Psicologia. Universidad Autonoma de Madrid. Madrid. Spain.Title [Adaptation and validation of the Health Utilities Index Mark 3 into Spanish and correction norms for Spanish population]. [Spanish]Source Medicina Clinica. 120(3):89-96, 2003 Feb 1.Abstract BACKGROUND AND OBJECTIVE: The Health Utilities Index Mark III (HUI-3) is a psychometric instrument developed to assign utilities to patients' health states. Wepresent its Spanish adaptation and validation. Moreover, we estimate its utility in the Spanish population and compare it to Canadian patients. PATIENTS AND METHOD: TheAdaptation process has been carried out following the original protocol by Furlong. A panel of experts was selected in order to warrant the process, the questionnaire translation and the training of interviewers. Two different samples were used: a modelling sample to develop the Multi Attribute Utility function (MAUF) and a directed measure sample to validate the MAUF. Both samples are representative of theSpanish population according to gender and age quota. In order to estimate the utilities associated with each health state, Visual Analogue Scale (VAS) and Standard Gamble (SG) procedures were used. The instrument's dimensionality was assessed by means of Factor Analysis, and the convergent validity was checked against EuroQoL. RESULTS: The HUI-3 Spanish version is feasible (< 2% missing valuesand 7.34 1.27 minutes completion time) and reliable (Cronbach's (= 0.792 in modelling sample, 0.707 in direct measure sample, and 0.760 as a whole), showing a good test-retest correlation (0.909, p < 0.001). Convergent validity is good (correlation with EuroQoL: within 0.788 and 0.793). Factor solution met 5 factors: Speech & Dexterity, Ambulation & Pain, Vision, Emotion & Cognition, and Hearing. TheSpanish and Canadian utility function differed significantly; 0.07 pts, p < 0.001). CONCLUSIONS: This questionnaire can be applied to individuals or collectively, either self-administered or through an interview. Psychometric indexes are good. Differences between Spanish and Canadian utility functions suggest the need of usingthe specific function for each population.
<155>Unique Identifier 12597935Authors Karakiewicz PI. Kattan MW. Tanguay S. Elhilali MM. Bazinet M. Scardino PT. Aprikian AG.Institution Department of Urology, Memorial Sloan-Kettering Cancer Center, New York, New York,USA.Title Cross-cultural validation of the UCLA prostate cancer index.Source Urology. 61(2):302-7, 2003 Feb.Abstract
Page 80

1-200.txt OBJECTIVES: To explore the impact of cross-cultural differences on University of California, Los Angeles, Prostate Cancer Index (PCI) reliability and validity, whichis unknown. The PCI represents the most widely used prostate cancer-specific health-related quality-of-life assessment tool. METHODS: The PCI sexual and urinary scales, the RAND SF-36 survey, and the Prostate Outcomes Research Team (PORT) prostate cancer treatment complication profile were self-administered. The principalsample consisted of 2415 men (anglophone 256, francophone 2159) treated with radicalprostatectomy in Quebec between 1988 and 1996. An additional 35 men (anglophone 17, francophone 18) formed the retest sample. RESULTS: The PCI demonstrated excellent internal consistency and test-retest reliability in tests based on the entire cohortand in tests addressing the two linguistically different groups. The instrument showed a lack of convergence with the SF-36 scales, confirming the distinctness of the generic and prostate cancer-specific constructs. The PCI sexual scales convergedwith the aggregate PORT sexual items (r = 0.8), and the PCI urinary scales were strongly related to the aggregate PORT urinary items (r = 0.7). Convergence between PCI urinary bother and function was strong (r = 0.8), but only moderate convergence was noted between PCI sexual bother and function (r = 0.4). The relation between bother and function in both urinary and sexual domains was weaker in anglophone participants relative to their francophone counterparts. CONCLUSIONS: The PCI is reliable and, at best, only modestly affected by cultural differences when administered to culturally distinct English-speaking men or when translated into French.
<156>Unique Identifier 12590996Authors Lawrence D. Graber JE. Mills SL. Meissner HI. Warnecke R.Institution Division of Cancer Control and Population Sciences, National Cancer Institute, 6130 Executive Boulevard, EPN Suite 4005, MSC 7344, Bethesda, MD 20892-7344, USA. [email protected] Smoking cessation interventions in U.S. racial/ethnic minority populations: an assessment of the literature. [Review] [53 refs]Source Preventive Medicine. 36(2):204-16, 2003 Feb.Abstract BACKGROUND: Smoking prevalence rates in some ethnic minority groups are elevated relative to the majority population. Thus, identifying cessation interventions that are effective for these groups is important. This article reviews published studies that examine effects of smoking cessation interventions relevant to racial ethnic minority populations. METHODS: A literature search of tobacco interventions, reporting smoking cessation outcomes (including quit rates) in U.S. minority populations, was conducted for the period 1985 to 2001. RESULTS: Thirty-six studies met preset criteria for inclusion. Twenty-three reported quit rates for African Americans, 4 for Asian/Pacific Islanders, 3 for Native Americans, and 10 for Hispanics. CONCLUSIONS: The disproportionate number of studies that focused on African American smokers compared with the other major racial/ethnic groups suggeststhe need for continued efforts to develop and evaluate the effectiveness of smoking cessation interventions for all ethnic minority populations. Abstinence rates variedconsiderably depending on study design and intervention strategy. Moreover, a relatively small percentage of studies that were randomized trials reported statistically significant findings, and most used intervention strategies that do not reflect the current state-of-the-art. These results strongly suggest that more research is needed to identify successful smoking cessation interventions in these populations. [References: 53]
<157>Unique Identifier 12589322
Page 81

1-200.txtAuthors Barr JT. Schumacher GE.Institution School of Pharmacy, Northeastern University, Boston, MA, USA. [email protected] The need for a nutrition-related quality-of-life measure.Source Journal of the American Dietetic Association. 103(2):177-80, 2003 Feb.
<158>Unique Identifier 12588206Authors Barnhart JM. Fang J. Alderman MH.Institution Department of Epidemiology and Social Medicine, Albert Einstein College of Medicine, 1300 Morris Park Ave, Belfer Building, Room 1306A, Bronx, NY 10461. [email protected] Differential use of coronary revascularization and hospital mortality following acute myocardial infarction.Source Archives of Internal Medicine. 163(4):461-6, 2003 Feb 24.Abstract BACKGROUND: The effect of racial/ethnic disparity in the use of cardiac procedureson short-term outcomes, such as hospital mortality, is limited. We sought to determine the association of revascularization procedures (percutaneous transluminalcoronary angioplasty or coronary artery bypass graft) to hospital mortality in non-Hispanic black and white patients and Hispanic patients with acute myocardial infarction. METHODS: Analysis of the New York State Department of Health Statewide Planning and Research Cooperate System (SPARCS) data for 12 555 patients admitted toNew York City hospitals with acute myocardial infarction in 1996. Revascularization procedure frequencies and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for hospital mortality were calculated. RESULTS: Whites were older than Hispanics and blacks (mean +/- SD age, 70 +/- 13.3 vs 64 +/- 13.3 and 64 +/- 12.9 years, respectively; P<.001) and more likely to have heart failure (36.3% vs 29.1% and 29.6%, respectively; P<.001). Blacks were least likely to be revascularized compared with Hispanics and whites (15.8% vs 25.8% and 25.2%, respectively; P<.001).Hispanics were more likely to survive than whites (adjusted OR, 0.73 [95% CI, 0.59-0.91]); this difference was not significant for blacks (adjusted OR, 0.83 [95% CI, 0.69-1.00]). Nonrevascularized blacks and Hispanics were more likely to be discharged alive than nonrevascularized whites (OR, 0.80 [95% CI, 0.66-0.98] for blacks; OR, 0.74 [95% CI, 0.59-0.93] for Hispanics). There were no significant racial/ethnic differences in hospital survival among revascularized patients. CONCLUSIONS: Nonclinical and clinical factors appear to account for blacks being least likely to have been revascularized. Despite these differences in revascularization rates, survival was similar for blacks and whites, whereas Hispanics were more likely to survive than whites.
<159>Unique Identifier 12556604Authors Miranda J. Azocar F. Organista KC. Dwyer E. Areane P.Institution San Francisco General Hospital, University of California, USA. [email protected] Treatment of depression among impoverished primary care patients from ethnic minority groups.Source Psychiatric Services. 54(2):219-25, 2003 Feb.
Page 82

1-200.txtAbstract OBJECTIVE: The aim of this study was to determine whether supplementing traditional cognitive-behavioral therapy for depression with clinical case management would reduce the rate of dropout from care and improve outcomes for ethnically diverse, impoverished medical outpatients. METHODS: The study was a randomized trial that compared cognitive-behavioral group psychotherapy alone (N=103) with the same therapy supplemented by clinical case management (N=96). RESULTS: The patients who received supplemental case management had lower dropout rates than those who received cognitive-behavioral group therapy alone. Supplementalcase management was associated with greater improvement in symptoms and functioning than cognitive-behavioral therapy alone for patients whose first language was Spanish (N=77) but was less effective for those whose first language was English (N=122). CONCLUSIONS: Supplemental case management improves retention in traditionalmental health outpatient care and can improve outcomes for Spanish-speaking patients.
<160>Unique Identifier 12519002Authors Katz RV. Kegeles SS. Green BL. Kressin NR. James SA. Claudio C.Institution Department of Epidemiology & Health Promotion, New York University College of Dentistry, 345 East 24th Street, New York, NY 10010, USA. [email protected] The Tuskegee Legacy Project: history, preliminary scientific findings, and unanticipated societal benefits.Source Dental Clinics of North America. 47(1):1-19, 2003 Jan.Abstract This article is intended to provide a relatively complete picture of how a pilot study--conceived and initiated within an NIDCR-funded RRCMOH--matured into a solid line of investigation within that center and "with legs" into a fully funded study within the next generation of NIDCR centers on this topic of health disparities, theCenters for Research to Reduce Oral Health Disparities. It highlights the natural opportunity that these centers provide for multicenter. cross-disciplinary research and for research career pipelining for college and dental school students; with a focus, in this case, on minority students. Futhermore, this series of events demonstrates the rich potential that these types of research centers have to contribute in ways that far exceed the scientific outcomes that form their core. In this instance, the NMOHRC played a central--and critical, if unanticipated--role in contributing to two events of national significance, namely the presidential apologyto the African American community for the research abuses of the USPHS--Tuskegee syphilis study and the establishment of the National Center for Bioethics in Research and Health Care at Tuskegee University. Research Centers supported by the NIH are fully intended to create a vortex of scientific activity that goes well beyond the direct scientific aims of the studies initially funded within those centers. The maxim is that the whole should be greater than the sum of its initial constituent studies or parts. We believe that NMOHRC did indeed achieve that maxim--even extending "the whole" to include broad societal impact. well beyond the scope of important, but mere, scientific outcomes--all within the concept and appropriate functions of a scientific NIH-funded research center.
<161>Unique Identifier 12509596Authors Alexander GR. Kogan M. Bader D. Carlo W. Allen M. Mor J.Institution Department of Maternal and Child Health, School of Public Health, University of Alabama at Birmingham, Birmingham, Alabama 35294-0022, USA. [email protected]
Page 83

1-200.txtTitle US birth weight/gestational age-specific neonatal mortality: 1995-1997 rates for whites, hispanics, and blacks.Source Pediatrics. 111(1):e61-6, 2003 Jan.Abstract OBJECTIVE: In recent years, gains in neonatal survival have been most evident among very low birth weight, preterm, and low birth weight (LBW) infants. Most of the improvement in neonatal survival since the early 1980s seems to be the consequence of decreasing birth weight-specific mortality rates, which occurred during a period of increasing preterm and LBW rates. Although the decline in neonatal mortality has been widely publicized in the United States, research suggests that clinicians may still underestimate the chances of survival of an infant who is born too early or too small and may overestimate the eventuality of serious disability. So that clinicians may have current and needed ethnic- and race-specific estimates of the "chances" of early survival for newborn infants, we examined birth weight/gestational age-specific neonatal mortality rates for the 3 largest ethnic/racial groups in the United States: non-Hispanic whites, Hispanics, and non-Hispanic blacks. Marked racial variation in birth weight and gestational age-specific mortality has long been recognized, and growing concerns have been raised about ongoing and increasing racial disparities in pregnancy outcomes. Our purpose for this investigation was to provide an up-to-date national reference for birth weight/gestational age-specific neonatal mortality rates for use by cliniciansin care decision making and discussions with parents. METHODS: The National Center for Health Statistics linked live birth-infant death cohort files for 1995-1997 wereused for this study. Singleton live births to US resident mothers with a reported maternal ethnicity/race of non-Hispanic white, non-Hispanic black, or Hispanic (n = 10 610 715) were selected for analysis. Birth weight/gestational age-specific neonatal mortality rates were calculated using 250 g/2-week intervals for each ethnic/racial group. RESULTS: The overall neonatal mortality rates for whites, Hispanics, and blacks were 3.24, 3.45, and 8.16 neonatal deaths per 1000 live births, and the proportion of births <28 weeks was 0.35%, 0.45%, and 1.39%, respectively. Newborns who weighed <1500 g comprised <2.5% of all births in each racial/ethnic group but accounted for >50% of neonatal deaths. For whites, Hispanics, and blacks, >50% of newborns 24 to 25 weeks of gestational age survived. For most combinations of birth weights <3500 g and gestational ages of <37 weeks, the neonatal mortality rate was lowest among blacks, compared with whites or Hispanics. At these same gestational age/birth weight combinations, Hispanics have slightly lower mortality rates than whites. For combinations of birth weights >3500 g and gestational ages of 37 to 41 weeks, Hispanics had the lowest neonatal mortality rate. In these birth weight/gestational age combinations, where approximately two thirds of births occur, blacks had the highest neonatal mortality rate. CONCLUSIONS: Compared with earlier reports, these data suggest that a substantial improvement in birth weight/gestational age-specific neonatal mortality has occurred in the United States. Regardless of ethnicity/race, the risk of a neonatal death does not exceed 50% (the suggested definition for the limit of viability), except for birth weights below 500 g and gestational ages <24 weeks. Notwithstanding, ethnic/racial variations in neonatal mortality rates continue to persist, both in overall rates and within birth weight/gestational age categories. Blacks continue to have higher proportions for preterm and LBW births, compared witheither whites or Hispanics. At the same time, blacks experience lower risks of neonatal mortality for preterm and LBW infants, while having higher risks of mortality among term, postterm, normal birth weight, and macrosomic births.
<162>Unique Identifier 12506150Authors Frankenfield DL. Rocco MV. Roman SH. McClellan WM.Institution Centers for Medicare & Medicaid Services, Center for Beneficiary Choices, Baltimore, Maryland 21244, USA. [email protected]
Page 84

1-200.txtTitle Survival advantage for adult Hispanic hemodialysis patients? Findings from the end-stage renal disease clinical performance measures project.Source Journal of the American Society of Nephrology. 14(1):180-6, 2003 Jan.Abstract One-year follow-up mortality in Hispanic and non-Hispanic patients and its association with intermediate outcomes of dialytic care were examined utilizing the Center for Medicare & Medicaid Services' (CMS) ESRD Clinical Performance Measures (CPM) Project and administrative data. Demographic and clinical information was collected on a national random sample of adult in-center hemodialysis (HD) patients for the period of October through December, 1998. Patients were categorized as Hispanic, non-Hispanic White, or non-Hispanic Black. Of 8336 patients 994 (12%) wereidentified as Hispanic, 3618 (43%) as non-Hispanic White, and 3111 (37%) as non-Hispanic Black. The adjusted 12-mo mortality risk (99% CI) for Hispanics was 0.76 (0.60 to 0.96; P < 0.01) and for non-Hispanic Blacks 0.66 (0.56 to 0.78, P < 0.001) compared with non-Hispanic Whites (referent). Similar 12-mo mortality risks were noted in the groups with diabetes mellitus or hypertension as the causes of ESRD and among patients > or = 65 yr. After controlling for demographic and geographic variables, Hispanics compared with the referent group, non-Hispanic Whites, were more likely to have a mean serum albumin > or = 4.0/3.7 g/dL (BCG/BCP) (1.5 [1.2 to 1.7]; P < 0.001) and as likely to have a mean Kt/V > or = 1.2, mean hemoglobin > or = 11 g/dL, and an arteriovenous fistula as their vascular access. These data suggest that adult Hispanic HD patients have a 12-mo survival intermediate to non-Hispanic Blacks and non-Hispanic Whites and experience equivalent or better intermediate outcomes of dialytic care compared with non-Hispanic Whites.
<163>Unique Identifier 12491515Authors Shavers VL. Harlan LC. Stevens JL.Institution Applied Research Program, Health Service and Economics Branch, Division of Cancer Control and Population Science, National Cancer Institute, 6130 Executive Boulevard,MSC 7344, EPN Room 4005, Bethesda, MD 20892-7344, USA. [email protected] Racial/ethnic variation in clinical presentation, treatment, and survival among breast cancer patients under age 35.Source Cancer. 97(1):134-47, 2003 Jan 1.Abstract BACKGROUND: The age specific breast cancer incidence rate for African-American women under age 35 is more than twice the rate for white women of similar age, and the mortality rate is more than three times higher. To determine factors that may explain racial/ethnic variation in outcomes among young women diagnosed with breast cancer, the authors examined the clinical presentation, treatment, and survival of African-American, Hispanic, and white women under age 35 years. METHODS: Surveillance, Epidemiology, and End Results (SEER) Program data for 1990-1998 and SEER Patterns of Care data for 1990, 1991, and 1995 were used for this analysis. Multivariate logistic regression analyses were performed to examine factors associated with the receipt of selected breast cancer treatments. Kaplan-Meier survival analyses and Cox proportional hazards regression analyses were used to examine 5-year overall survival and disease-specific survival. RESULTS: The authors found racial/ethnic variation in clinical presentation, treatment, and survival. Both African-American and Hispanic women presented with higher disease stage and a higher prevalence of adverse prognostic indicators compared to white women. African-American and Hispanic women received cancer-directed surgery and radiation less frequently after undergoing breast-conserving surgery. Racial/ethnic differences in clinical presentation and treatment were associated with poorer overall survival in unadjusted analyses. African-American and Hispanic women also
Page 85

1-200.txthad poorer overall survival after controlling for clinical and demographic characteristics and type of treatment. CONCLUSIONS: Future research studies should further examine the factors that influence racial/ethnic differences in incidence, clinical presentation, and treatment differentials among young women diagnosed with breast cancer. A better understanding of these factors will facilitate the development of strategies to help eliminate this health disparity. Published 2003 bythe American Cancer Society.
<164>Unique Identifier 12938253Authors Brach C. Fraser I.Institution Center for Organization and Delivery Studies, Agency for Healthcare Research and Quality, Rockville, Maryland, USA.Title Reducing disparities through culturally competent health care: an analysis of the business case. [Review] [102 refs]Source Quality Management in Health Care. 10(4):15-28, 2002 Summer.Abstract Finding ways to deliver high-quality health care to an increasingly diverse population is a major challenge for the American health care system. The persistenceof racial and ethnic disparities in health care access, quality, and outcomes has prompted considerable interest in increasing the cultural competence of health care,both as an end in its own right and as a potential means to reduce disparities. Thisarticle reviews the potential role of cultural competence in reducing racial and ethnic health disparities, the strength of health care organizations' current incentives to adopt cultural competence techniques, and the limitations inherent in these incentives that will need to be overcome if cultural competence techniques areto become widely adopted. [References: 102]
<165>Unique Identifier 12939121Authors Lopez-Candales A.Institution University of Pittsburgh Medical Center, Cardiovascular Institute, Pittsburgh, PA 15213, USA. [email protected] Cardiovascular diseases: a review of the Hispanic perspective. Awareness is the first step to action. [Review] [79 refs]Source Journal of Medicine. 33(1-4):227-45, 2002.Abstract Coronary heart disease is the leading cause of death in adults in the United States, accounting for about one-third of all deaths in subjects over age 35 (Thom et al., 1998). Mortality rates for cardiovascular disease and coronary heart diseasein men and women and in blacks and whites have fallen in most countries by 24 to 28 percent since 1975, although the decline has slowed since 1990 (Kuulasmaa et al., 2000; McGovern et al., 1996; Capewell et al., 1999; Capewell et al., 2000; Cooper etal., 2000; McGovern et al., 2001; Gillum, 1994). This favorable trend is related partly to a decrease in the rate of fatal myocardial infarction (Gillum, 1987; Goldberg et al., 1988; Pashos et al., 1993; de Vreede et al., 1991), but it is also associated with a decline in the prevalence of risk factors for coronary artery disease (Gillium, 1994; Gillium 1987; Pearson, 1989). These risk factors strongly influence the severity of coronary atherosclerosis (Rhoads et al., 1978; Sorlie et al., 1981; Feinleib et al., 1979; Freedman et al., 1993; Reed and Yano, 1991), a major predictor of survival in patients with coronary disease (Humphries et al.,
Page 86

1-200.txt1974). These observations suggest that the decline in mortality from coronary arterydisease is related to a parallel decline in coronary atherosclerosis. Despite great strides regarding the knowledge of coronary artery risk factors and some of its demographic aspects, the incidence and nature of each individual variable in certainethnic and racial groups remain poorly defined. Over a decade ago the American HeartAssociation issued a statement regarding cardiovascular disease and stroke in racialminorities in the United States and urged for more participation of minority groups in research studies in order to assess their particular trends and outcomes (American Heart Association Medical/Scientific Statement, 1991). The purpose of thisarticle is to review the current enrollment and participation of Hispanics in major clinical trials relating to cardiovascular disease and propose possible explanationsfor the observed results as well as suggestions to improve the shortcomings found. [References: 79]
<166>Unique Identifier 12790003Authors Martinez E.Institution San Ysidro Health Center, San Ysidro, California, USA.Title Children's Dental Safety Net--a collaborative initiative of San Diego County's Council of Community Clinics.Source Compendium of Continuing Education in Dentistry. 23(12 Suppl):36-8, 2002 Dec.
<167>Unique Identifier 12772547Authors Palafox NA. Buenconsejo-Lum L. Riklon S. Waitzfelder B.Institution Department of Family Practice and Community Health, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, USA.Title Improving health outcomes in diverse populations: competency in cross-cultural research with indigenous Pacific islander populations. [Review] [41 refs]Source Ethnicity & Health. 7(4):279-85, 2002 Nov.Abstract OBJECTIVE: There is a large disparity in health status between the indigenous peoples of the US Associated Pacific compared to any population in the USA. The research process that has been supported by US academic institutions and federal agencies has been limited in its ability to address the disparate health issues and may be part of the problem. We define culturally competent research and review approaches to developing competency in cross-cultural research with indigenous Pacific Islander populations. DESIGN: This is a descriptive review of the investigators' experience in the Hawaii MEDTEP Center experience and of the experience of others conducting research with the indigenous people of the Pacific Islands. RESULTS: Culturally competent cross-cultural research with the indigenous peoples of the Pacific requires an understanding and application of indigenous peoples' paradigms of health, knowledge, science, and research. It is not sufficientto train more indigenous Pacific Islanders to do more Western-style research. Unraveling the complex health situation and determining the changes that need to be made is dependent on the dominant culture engaging the indigenous Pacific populations in a way that bridges cultural paradigms. CONCLUSION: Positively affecting the disparity of health in the indigenous populations of the Pacific is, in part, dependent on employing an indigenous-peoples-centered model of research. The model can have application to the study of indigenous peoples in other parts of the world. [References: 41]
Page 87

1-200.txt
<168>Unique Identifier 12772543Authors Washington AE. Napoles-Springer A. Forte DA. Alexander M. Perez-Stable EJ.Institution Medical Effectiveness Research Center for Diverse Populations, Center for Aging inDiverse Communities, University of California, San Francisco (UCSF), USA.Title Establishing centers to address treatment effectiveness in diverse ethnic groups: the MEDTEP experience.Source Ethnicity & Health. 7(4):231-42, 2002 Nov.Abstract OBJECTIVE: To investigate racial, ethnic, and socioeconomic disparities in health outcomes amenable to improvement through more effective delivery of health care services. DESIGN: The Medical Treatment Effectiveness Program (MEDTEP) Research Centers on Minority Populations were a group of centers in the USA funded to improvethe effectiveness of medical diagnosis and treatment, to provide technical assistance to ethnic minority health researchers, to train new researchers, and to disseminate information to help ethnic minority patients and their health care providers. RESULTS: Centers often provided many specific findings related to assessment of the magnitude of disparities in health outcomes and to approaches for eliminating these outcomes. The Centers were able to build community partnerships using an approach now defined as community-based participatory research. Centers changed the culture of their institutions by making them more aware of the need to train diverse investigators and do more to eliminate health disparities. CONCLUSION:A key to the success of the Centers has been the unification of a cadre of committedinvestigators dedicated to the mentoring of minority health researchers and to the elimination of ethnic and socioeconomic disparities in health. The MEDTEP Centers provide a model but there remains a need for continued work.
<169>Unique Identifier 12772542Authors Tilley BC. Elm JJ.Title Improving health outcomes in diverse and vulnerable populations: building on the experience of the Centers for Medical Treatment Effectiveness in Diverse Populations(MEDTEP).Source Ethnicity & Health. 7(4):227-30, 2002 Nov.
<170>Unique Identifier 12626088Authors Phipps MG. Sowers M. DeMonner SM.Institution Brown Medical School, Women & Infant Hospital of Rhode Island, Department of Obstetrics and Gynecology, Providence, Rhode Island 02905-2401, USA. [email protected] The risk for infant mortality among adolescent childbearing groups.Source Journal of Women's Health. 11(10):889-97, 2002 Dec.Abstract OBJECTIVE: To evaluate risk disparities and risk factors for infant mortality
Page 88

1-200.txtamong adolescent childbearing age groups. METHODS: We combined the 1995 and 1996 comprehensive U.S. birth cohorts provided by the National Center for Heath Statistics. Our analysis included 777,762 singleton, first births to women aged 12-19 years linked to 4631 infant deaths. We used both bivariate comparisons and multivariable logistic regression for our analysis, with infant mortality as our main outcome measure. RESULTS: Rates of infant mortality are substantially higher for < or =15-year-olds (8.1/1000 live births) compared with 16-17-year-olds (6.3/1000 live births) and 18-19-year-olds (5.4/1000 live births). Even after adjusting for risk factors associated with poor outcomes, including alcohol use, tobacco use, and prenatal care use, the risk for infant mortality was 1.6 (95% confidence interval [95% CI] 1.4, 1.7) times greater for infants of mothers < or =15years old as compared with those mothers 18-19 years old. In the < or =15-year-old group, 62% of fathers were not reported on the child's birth certificate. Not reporting the father was associated with a 24% increased risk for infant mortality after adjusting for maternal and infant risk factors. CONCLUSIONS: Childbearing in <or =15-year-olds is associated with a substantial increased risk for infant mortality compared with childbearing in older adolescence. This study suggests that not reporting the father on a birth certificate is a potential risk marker. Risk differences among adolescent age groups may be important to consider when creating tailored intervention and prevention strategies.
<171>Unique Identifier 12616781Authors Rivers R. Freeman J.Institution Nursing and Patient Care, Shands Hospital, University of Florida, Gainesville, Florida, USA.Title Diversity is our strength!.Source Sci Nursing. 19(4):181-3, 2002 Winter.Abstract Valuing and appreciating diversity are key requirements for health care organizations faced with increasingly diverse workforces and patient populations. Diversity issues are central to effectively functioning teams, patient outcomes, staff satisfaction, recruitment, and retention. Shands HealthCare, a health care system containing a large teaching medical center and several community hospitals and clinics centered around Gainesville, Florida, made a commitment to take the necessary steps to make diversity a priority and strategic initiative. A systemwide diversity initiative was launched in 1998. Diversity was defined, and organizationalleaders were developed as "Ambassadors for Diversity." The Ambassadors developed an extensive training program that all staff and managers attend upon hiring. The primary goal of the program is to create a culture of respect and appreciation for diversity. Over 2,500 employees and managers have attended the training.
<172>Unique Identifier 12613155Authors Fisher CB. Hoagwood K. Boyce C. Duster T. Frank DA. Grisso T. Levine RJ. Macklin R. Spencer MB. Takanishi R. Trimble JE. Zayas LH.Institution Department of Psychology, Center for Ethics Education, Fordham University, Dealy Hall, Bronx, NY 10458, USA. [email protected] Research ethics for mental health science involving ethnic minority children and youths.Source American Psychologist. 57(12):1024-40, 2002 Dec.
Page 89

1-200.txtAbstract In response to U.S. Public Health Service projects promoting attention to disparities in the outcomes of mental health treatments, in July 2001, the American Psychological Association, the National Institute of Mental Health, and the Fordham University Center for Ethics Education convened a group of national leaders in bioethics, multicultural research, and ethnic minority mental health to produce a living document to guide ethical decision making for mental health research involving ethnic minority children and youths. This report summarizes the key recommendations distilled from these discussions.
<173>Unique Identifier 12585523Authors Katerndahl DA. Amodei N. Larme AC. Palmer R.Institution Department of Family and Community Medicine, University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78229-3900, USA. [email protected] Psychometric assessment of measures of psychological symptoms, functional status, life events, and context for low income Hispanic patients in a primary care setting.Source Psychological Reports. 91(3 Pt 2):1121-8, 2002 Dec.Abstract This study assessed the psychometric properties of a set of nine commonly used lists in an English-speaking Hispanic sample taken from a primary care setting. Those were the General Health Questionnaire-12, the Anxiety, Depression, and Somatization scales from the SCL-90, the Medical Outcomes Study Short Form-36, the Holmes and Rahe Family Life Changes, abbreviated versions of the Daily Hassles and Uplifts, the Herth Hope Index, Duke Social Support and Stress scales, Alcohol Use Disorders Identification Test, and Marlowe-Crowne Brief Social Desirability Scale. 68 adult patients completed the measures via structured interview. Internal consistency was measured using Cronbach alpha and the Kuder-Richardson-20. Constructvalidity was assessed using Pearson correlations among sets of scores. Internal consistencies were good-to-excellent for all measures except for the Duke Social Support and Stress scales (Stress scale), and the Brief Social Desirability Scale. Construct validity was suggested for all except the Mental Health and Energy/Fatiguescales of the Short Form-36. Further study is needed to verify these results in other Hispanic populations and to address other forms of reliability and validity.
<174>Unique Identifier 12534014Authors Jordan J.Institution Franz-Volhard-Klinik, Zentrum f.Herz-Kreislaufforschung, Charite, Humboldt-Univ. Berlin. [email protected] [Effective "home remedies" in orthostatic hypotension. A glass of water before getting up and a brick under the bed]. [German]Source MMW Fortschritte der Medizin. 144(43):33-5, 2002 Oct 24.Abstract The symptoms of orthostatic hypotension can be considerably improved by non-pharmacological treatment, and patients with such symptoms should not initially be given medication. Many patients, for example, show a pronounced increase in bloodpressure shortly after drinking water, and this phenomenon can be utilized to ameliorate symptoms. In patients who respond inadequately, treatment with pharmacological agents is indicated. The most appropriate drug needs to be selected
Page 90

1-200.txtindividually on the basis of its action and tolerability. All medications suitable for treating orthostatic hypotension can appreciably increase the blood pressure in the prone patient.
<175>Unique Identifier 12530340Authors Frackiewicz EJ. Herrera JM. Sramek JJ. Collazo Y. Lawson WB.Institution Howard University, Washington, DC, USA. [email protected] Risperidone in the treatment of Hispanic inpatients with schizophrenia: a pilot study.Source Psychiatry. 65(4):371-4, 2002 Winter.Abstract A growing body of scientific evidence over the last two decades suggests that certain ethnic groups may require lower dosages of standard antipsychotics for the treatment of schizophrenia symptoms. Recent studies have implicated the role of genetic and environmental factors in the metabolism of these drugs as the basis for this differential response. In this pilot study, 10 Hispanic and 8 non-Hispanic patients with schizophrenia were enrolled in a double-blind, parallel-group, inpatient risperidone dosing (daily versus twice daily) trial with the novel antipsychotic risperidone. The result of repeated measures ANOVA reveals a significant interaction effect for race, indicative of a faster rate of symptom improvement (PANSS General) in Hispanic patients. The findings suggest that this novel agent may be preferable for certain ethnic groups. A trend toward more frequently occurring extrapyramidal symptoms among Hispanics was also found, which suggests that dosages lower than those typically recommended may be necessary in Hispanic schizophrenics.
<176>Unique Identifier 12528090Authors Evangelista LS. Dracup K. Doering LV.Institution University of California, Los Angeles, School of Nursing, USA.Title Racial differences in treatment-seeking delays among heart failure patients.[see comment].Source Journal of Cardiac Failure. 8(6):381-6, 2002 Dec.Abstract BACKGROUND: Treatment-seeking delays for heart failure (HF) symptoms are significantly high. However, earlier studies did not closely examine race as a characteristic that could potentially influence delay times. The purpose of this study was (1) to describe racial differences in treatment-seeking delays for HF symptoms and (2) to identify racial differences in hospital readmission rates, functional status, and total length of stay. METHODS AND RESULTS: A retrospective chart review of all patients admitted with HF at a Veterans Administration facility was conducted. The study sample consisted of 753 patients: 456 Caucasians (60.6%), 220 African Americans (29.2%), 41 Asians (5.4%), and 36 Hispanics (4.8%). The average prehospital delay time was 2.9 +/- 0.7 days. Mean delay times were significantly longer for African Americans than for Caucasians, Asians, and Hispanics (P =.019). African Americans also had significantly higher readmission rates (P =.001) and lower functional status (higher New York Heart Association functional class) (P =.034). There were no significant racial differences in total length of stay for HF admissions. CONCLUSION: The current study supports that racialdifferences exist in treatment-seeking behaviors for HF symptoms, hospital
Page 91

1-200.txtreadmission rates, and functional status. A better understanding of treatment-seeking behaviors of HF patients with different racial characteristics maybe key to early recognition and prevention of complications in this high-risk population; it may be beneficial in identifying patients at risk for treatment delays and potentially poorer outcomes.
<177>Unique Identifier 12523944Authors Carvajal SC. Hanson CE. Romero AJ. Coyle KK.Institution Research Department, Education, Training, Research (ETR) Associates, Santa Cruz, CA, USA. [email protected] Behavioural risk factors and protective factors in adolescents: a comparison of Latinos and non-Latino whites.Source Ethnicity & Health. 7(3):181-93, 2002 Aug.Abstract OBJECTIVES: This study investigated differences in behavioural health protective and risk factors in US Latino and non-Latino White adolescents as well as differences among Latinos with different levels of acculturation using a bicultural acculturation model. The bicultural model is consistent with current understanding of cultural change processes; however it has infrequently been applied to understandadolescent health outcomes. The outcomes included risk and health behaviours as wellas mental health factors consistent with Jessor's framework for describing adolescents' health status. DESIGN: Participants included 1119 students randomly selected from all middle schools of a Northern California district. Respondents completed project staff administered self-reports surveys in their schools that included assessments of health behaviours, mental health, and socio-cultural variables-including acculturation level. RESULTS: Latinos were at higher risk than non-Latino Whites in the following areas: academic orientation, physical activity, and sunscreen use. Boys and those of lower social class were more likely to report use of various substances and violence. Among Latinos, those in the marginalised acculturation group-those with less attachments and adaptations to Latino and other cultures, showed less desirable mental health outcomes than the bicultural group. CONCLUSION: These results extend prior research by assessing the health needs of early adolescent youth. The study found important differences within Latinos using abicultural acculturation model. The use of a bicultural acculturation model, or cultural orientation approach more generally, may have special utility for addressing health issues wherever minority populations interact with a dominant society.
<178>Unique Identifier 12516805Authors Schweitzer J. Casillas RA. Collins JC.Institution Department of Surgery, Kaiser Permanente Los Angeles Medical Center, Los Angeles, California 90027, USA.Title Acute diverticulitis in the young adult is not "virulent.".Source American Surgeon. 68(12):1044-7, 2002 Dec.Abstract Acute diverticulitis historically has been considered rare before the age of 40 but "virulent" when it does occur and frequently requiring emergency operation. Recent experience suggests that the demographics and management of this disease are changing. Outcomes at Kaiser Permanente Los Angeles Medical Center were reviewed.
Page 92

1-200.txtBetween January 1997 and July 2001 261 patients were discharged with the diagnosis of acute diverticulitis; 46 or 18 per cent of these were aged < or = 40. Patients' mean age was 35, 76 per cent were men, 65 per cent were Latino, and 72 per cent wereobese (body mass index > or = 30 kg/m2). An operation at initial presentation was performed on 35 per cent (16/46) patients. Only 19 per cent of these (3/16) had a correct preoperative diagnosis. The 30 patients who were treated nonoperatively all were managed successfully; one required a percutaneous drain. Given the apparent increasing frequency of acute diverticulitis in young adults and the high success rate of initial nonoperative management surgeons should consider this diagnosis in selected patients who present with abdominal symptoms. Knowledge of typical clinicalfeatures and judicious use of computed tomography may decrease the number of unnecessary emergency operations in young adults with acute diverticulitis. Our datado not support a "virulent" label for this disease in the young.
<179>Unique Identifier 12507054Authors Clark RF. Phillips M. Manoguerra AS. Chan TC.Institution San Diego Division, California Poison Control System, San Diego, California, USA. [email protected] Evaluating the utilization of a regional poison center by Latino communities.Source Journal of Toxicology - Clinical Toxicology. 40(7):855-60, 2002.Abstract BACKGROUND: Penetrance values estimate the utilization of poison centers services.For a variety of reasons, penetrance values may vary greatly among geographic areas of population. We examined the relationship between ethnicity and penetrance in our population. METHODS: We conducted a retrospective review of data from January 1, 2000 through December 31, 2000 from our poison center's database. Home calls to the center were evaluated by zip code, age, gender, substance, route of exposure, and outcome. These data were compared with U.S. Census 2000 geographic and community demographic data for San Diego by zip code. From this information, we identified zipcode regions with substantial Latino populations (>50%), and substantial Caucasian populations (>70%). Study groups were limited to those zip codes with median household incomes of $20,000-$50,000. Aggregate total and pediatric penetrance values were calculated for each group and compared. RESULTS: Our study group consisted of 6 zip codes with significant numbers of Latino residents, and 11 zip codes with significant numbers of Caucasian residents. Aggregate call volume for thecounty was 6.5 calls per 1000 population, while that for children less than age 5 was 43. Penetrance values for the study zip codes with large Latino populations weresignificantly lower with a mean value of 22.4 for children, and 5.0 for all ages. These values were statistically significant when compared to county data and that from the control zip codes with largely Caucasian residents (61 aggregate and 49.6 pediatric). CONCLUSION: Penetrance values were significantly lower in zip codes withlarge numbers of Latino residents. Reasons for this variation are being investigated.
<180>Unique Identifier 12492650Authors Shannon C.Institution Indigenous Health Division, School of Population Health, University of Queensland,Medical School, Herston Road, Herston, QLD, 4006. [email protected] Acculturation: Aboriginal and Torres Strait Islander nutrition. [Review] [0 refs]Source
Page 93

1-200.txt Asia Pacific Journal of Clinical Nutrition. 11 Suppl 3:S576-8, 2002.Abstract The health status of Australia's indigenous people remains the worst of any subgroup within the population, and there is little evidence of any significant improvement over the past two decades, a situation unprecedented on a world scale. Compared with non-indigenous Australians, adult life expectancy is reduced by 15-20 years, with twice the rates of mortality from heart disease, 17 times the death ratefrom diabetes and 10 times the deaths from pneumonia. Despite improvements in perinatal mortality, they continue to represent a major cause of death, with infant deaths up to 2.5 times higher than the general population. The problems of educational disadvantage and unemployment are reflected in twice the rates of smoking and high obesity levels. Seven percent of indigenous families are homeless, with many more in inadequate and overcrowded housing, sometimes lacking water or sewerage. Economic disadvantage is real: 23% worry about going without food. Nutritional deficiencies in children have resulted in failure to thrive, contributing greatly to the problems of pneumonia and infectious diseases. The remoteness and isolation of many Aboriginal communities limit education and employment opportunities. It is important to consider the historical context of Aboriginal and Torres Strait Islander people, in order to gain an understanding of current health problems. The impact of past policies and practices and the 'introduced diet' are reflected in the poor health outcomes described above. This session will explore some of the underlying historical, cultural, structural and political factors that can be linked to the current problems. [References: 0]
<181>Unique Identifier 12487704Authors Berg JA. Cromwell SL. Arnett M.Institution University of Arizona College of Nursing, Tucson, Arizona 85721-0203, USA. [email protected] Physical activity: perspectives of Mexican American and Anglo American midlife women.Source Health Care for Women International. 23(8):894-904, 2002 Dec.Abstract Despite the well-known health benefits of physical activity (PA), most midlife andolder adults lead sedentary lifestyles. Anglo American women and Mexican Americans of both genders are two of the least physically active groups. We conducted three focus groups to identify attitudes and beliefs about PA among Mexican American and Anglo American midlife women. Our long-term goal was to identify culture-specific interventions that promote long-term PA continuation. Significant differences were found between the two groups. While Anglo American women valued individual outcomes,and spoke of personal factors promoting or preventing exercise, Mexican American women viewed PA as prescriptive, important for restoring health, and cited family responsibilities and family attitudes as factors that promoted or prevented them from exercising. We found that in order for PA interventions to be successful in each group, they must be tailored to the values of each cultural group.
<182>Unique Identifier 12480248Authors Ausman JI.Title Why the International Study of Unruptured Intracranial Aneurysms has lost credibility with neuroscientists.[comment].Source Surgical Neurology. 58(3-4):287-90, 2002 Sep-Oct.
Page 94
1-200.txt
<183>Unique Identifier 12477157Authors Fortin AH 6th.Institution Department of Medicine, Yale University School of Medicine, New Haven, Connecticut06520, USA. [email protected] Communication skills to improve patient satisfaction and quality of care.Source Ethnicity & Disease. 12(4):S3-58-61, 2002 Fall.Abstract While clinicians face increasing time pressure in caring for patients, communication with the patient can suffer. Communication is especially important in caring for the increasingly culturally diverse patient population in the United States. Different values, beliefs, and attitudes about health, illness, and health care can affect illness outcomes. These are best understood through dialogue. Patient-centered communication skills are associated with improved health outcomes, improved patient and clinician satisfaction, and less risk of malpractice suits. This paper reviews techniques to efficiently incorporate patient-centered communication into the medical encounter, with emphasis on interacting with patientsof different cultures.
<184>Unique Identifier 12477134Authors Shen JJ.Institution Health Administration Program, College of Health Professions, Governors State University, University Park, Illinois 60466, USA. [email protected] Severity of illness, treatment environments, and outcomes of treating acute myocardial infarction for Hispanic Americans.Source Ethnicity & Disease. 12(4):488-98, 2002 Fall.Abstract OBJECTIVE: To examine associations of ethnicity with severity of illness, treatment environments, outcomes, as well as their interactions among acute myocardial infarction (AMI) patients. DESIGN, SETTING, AND PARTICIPANTS: 182,374 Hispanic and non-Hispanic White AMI discharges in the 1998-1999 National Inpatient Sample. MAIN OUTCOME MEASURES: In addition to measuring severity of illness and the treatment environments defined as care-seeking characteristics and process of care, the principal outcome measure was hospital mortality. RESULTS: Compared to non-Hispanic White patients, Hispanic patients were associated with a greater comorbidity index, less likely to be treated in small (odds ratios [OR], 0.67), rural (OR, 0.39), or low-volume hospitals (OR, 0.90), but more likely to be treated in teaching hospitals (OR, 1.74). Further, Hispanic patients were less likely to receive arteriography, PTCA, and CABG, but positively associated with more resource use; also, Hispanic patients were less likely to be discharged to non-acute health facilities (OR, 0.80) or to die in hospital (OR, 0.78). Finally, comorbidities and the receiving of PTCA interacted with ethnicity, respectively, to affect mortality. CONCLUSIONS: Substantial differences in the hospital care for AMI existed between Hispanic and non-Hispanic White patients. While the treatment environments were lessfavorable for Hispanics, their survival advantage over non-Hispanic Whites remains to be unexplained. Biological or other social or clinical factors need to be identified to better explain the lower mortality rates of Hispanics. Enhancing access to specialized services should improve health outcomes for non-Hispanic Whites.
Page 95

1-200.txt
<185>Unique Identifier 12477133Authors de la Rosa IA.Title Perinatal outcomes among Mexican Americans: a review of an epidemiological paradox. [Review] [83 refs]Source Ethnicity & Disease. 12(4):480-7, 2002 Fall.Abstract This article presents a review of 3 possible explanations for the seemingly apparent paradox of favorable birthweight outcomes among Mexican Americans. Evidenceis grouped into 3 explanations: cultural, under-reporting, and bio-medical. With an emphasis on the link between acculturation among Mexican Americans and their perinatal outcomes, the key correlates associated with lower rates of low birth weight (LBW) are examined and critiqued. This review of the literature also explorespolicy and health implications for this important public health issue. [References: 83]
<186>Unique Identifier 12477132Authors Wildsmith EM.Institution Department of Sociology, Population Research Center, University of Texas at Austin, Austin, Texas 78712-1127, USA. [email protected] Testing the weathering hypothesis among Mexican-origin women.Source Ethnicity & Disease. 12(4):470-9, 2002 Fall.Abstract OBJECTIVE: To examine the "weathering hypothesis," as proposed by Geronimus (1986;1987; 1992; 1996), among US-born and foreign-born Mexican-origin women. This hypothesis specifically argues that the relationship between age and a variety of reproductively related heath outcomes varies by socioeconomic and environmental context. METHODS: 1989-1991 National Center for Health Statistics (NCHS) linked birth-death files. These files include all women who experienced a live birth in theUnited States and whose infants were issued a birth certificate during the years 1989 to 1991 (NCHS 1995). Age and nativity specific distributions on infant mortality, low birth weight, anemia, pregnancy related hypertension, and smoking were estimated for Mexican-origin women. RESULTS: For the foreign-born, levels of neonatal mortality are highest for younger women and tend to increase again in womenat the oldest ages. For the US born, the lowest levels are for women aged 17 and 18 years, and 27-29 years. Levels for women aged 19-24 years and 30-34 years are higherthan those for 17-and 18-year-olds. For both groups of women, giving birth to infants with low birth weight is most common at the earlier ages, declining more or less until the mid twenties when the rate begins to rise again slowly. Patterns for the maternal health indicators vary, with pregnancy related hypertension most strongly following the pattern suggested by weathering. CONCLUSION: Overall, this analysis suggests that there is evidence of weathering within the Mexican-origin population, particularly for the US-born population, and this is most clearly seen in levels of neonatal mortality and pregnancy related hypertension.
<187>Unique Identifier 12474937Authors
Page 96

1-200.txt Kohn LP. Oden T. Munoz RF. Robinson A. Leavitt D.Institution Department of Psychology, University of Michigan, Ann Arbor 48109, USA. [email protected] Adapted cognitive behavioral group therapy for depressed low-income African American women.Source Community Mental Health Journal. 38(6):497-504, 2002 Dec.Abstract In this study we examine the degree to which a manualized cognitive-behavioral therapy intervention can be adapted to be culturally sensitive in treating depressedlow-income African American women with multiple stressors. We describe the adaptations we made to an existing intervention, a group treatment developed for depressed low-income medical patients. We also describe our evaluation of the adapted treatment in which outcomes of African American women treated in the culturally adapted group were compared to African American women treated in the non-adapted group. Following treatment, women in the adapted group exhibited a larger drop in average BDI scores. Implications are discussed in terms of challengesrelated to the development and evaluation of culturally adapted treatment.
<188>Unique Identifier 12472344Authors Chiller KG. Passaro D. Frieden IJ.Institution Department of Dermatology, University of California, San Francisco, USA.Title Hemangiomas of infancy: clinical characteristics, morphologic subtypes, and their relationship to race, ethnicity, and sex.Source Archives of Dermatology. 138(12):1567-76, 2002 Dec.Abstract BACKGROUND: Hemangiomas of infancy vary widely in appearance, size, and depth of cutaneous involvement. There is currently no standard classification system for these lesions. While they occur in any race, an increased incidence occurs in girls,light-skinned whites, and premature infants, especially those weighing less than 1500 g. Other epidemiologic and demographic factors have not been well characterized. OBJECTIVE: To determine any correlations between hemangioma subtype and anatomic location with demographic factors, complications, and other associated anomalies. DESIGN: Retrospective chart review of 327 patients with hemangioma of infancy seen between 1997 and 2000 in an ambulatory referral center. MAIN OUTCOMES MEASURES: Demographic and gestational information, lesion size, associated anomalies, complications, treatments, and outcomes were analyzed together with classification of hemangiomas into 4 groups: localized, segmental, indeterminate, and multifocal. Subtypes were correlated with race and ethnicity, the incidence of complications, and overall outcome. RESULTS: Of 472 hemangiomas (327 patients), 339 (72%) were localized, 84 (18%) were segmental, 37 (8%) were indeterminate, and 12 (3%) were multifocal (8 or more noncontiguous lesions). Segmental lesions were larger and were more frequently associated with developmental abnormalities. They also required more intensive and prolonged therapy and were associated with more complications and a poorer overall outcome (P<.001). Lesions on Hispanic patients were more likely to involve mucous membranes, to be segmental (P<.004), to be associated with abnormalities (P =.05), especially PHACE syndrome (P =.05), and to have more complications (P =.01). Increased incidence of segmental hemangiomas was the only factor in Hispanic infants associated with complications, more extensive treatment, or associated anomalies. CONCLUSIONS: Hemangiomas of infancy can usually be classified as localized, segmental, indeterminate, and multifocal, based on clinical features. Segmental lesions have a higher frequency of complications and associated abnormalities, and this type of hemangioma seems to present with increased frequency in Hispanic infants.
Page 97

1-200.txt
<189>Unique Identifier 12472187Authors Callister LC. Birkhead A.Institution College of Nursing, Brigham Young University, Provo, Utah, USA.Title Acculturation and perinatal outcomes in Mexican immigrant childbearing women: an integrative review. [Review] [91 refs]Source Journal of Perinatal & Neonatal Nursing. 16(3):22-38, 2002 Dec.Abstract Despite several sociocultural factors associated with increased risk for low birthweight and infant mortality, the rate for infants born to first-generation and less acculturated Mexican immigrant women is the same as that of non-Hispanic whites, andhalf that of African Americans with similar risks. It appears that sociocultural rather than genetic variables are the primary factors associated with this phenomenon. Higher levels of acculturation to North American values and lifestyle inMexican American childbearing women have been correlated with poor perinatal outcomes, including low birth weight. Acculturation is emerging as an important variable that should be considered when providing health care to Mexican immigrant childbearing women and their families. [References: 91]
<190>Unique Identifier 12469703Authors Kondrat ME. Greene GJ. Winbush GB.Institution College of Social Work, Ohio State University, Columbus 43210, USA. [email protected] Using benchmarking research to locate agency best practices for African American clients.Source Administration & Policy in Mental Health. 29(6):495-518, 2002 Jul.Abstract Using a collective case study design with benchmarking features, research reportedhere sought to locate differences in agency practices between public mental health agencies in which African American clients were doing comparatively better on specific proxy outcomes related to community tenure, and agencies with less success on those same variables. A panel of experts from the Ohio Department of Mental Health matched four agencies on per capita spending, percentage of African American clients, and urban-intensive setting. The panel also differentiated agencies on the basis of racial group comparisons for a number of proxy variables related to successful community tenure. Two agencies had a record of success with this client group (benchmark agencies); and two were less successful based on the selected criteria (comparison agencies). Findings indicated that when service elements explicitly related to culture were similar across study sites, the characteristics that did appear to make a difference were aspects of organizational culture. Implications for administration practice and further research are discussed.
<191>Unique Identifier 12467254Authors Laveist TA. Nuru-Jeter A.Institution
Page 98

1-200.txt Johns Hopkins University, Bloomberg School of Public Health, Department of Health Policy and Management, 624 North Broadway, Room 441, Baltimore, Maryland 21205, [email protected] Is doctor-patient race concordance associated with greater satisfaction with care?.Source Journal of Health & Social Behavior. 43(3):296-306, 2002 Sep.Abstract We examined a national sample of African American, white, Hispanic, and Asian American respondents to test the hypothesis that doctor-patient race concordance is predictive of patient satisfaction. Our analysis examined racial/ethnic differences in patient satisfaction among patients in multiple combinations of doctor-patient race/ethnicity pairs. Additionally, we outline the determinants of doctor-patient race concordance. The analysis used the 1994 Commonwealth Fund Minority Health Survey to construct a series of multivariate models. We found that for respondents in each race/ethnic group, patients who had a choice in the selection of their physician were more likely to be race concordant. Whites were more likely to be raceconcordant with their physician compared to African American, Hispanic, and Asian American respondents. Among each race/ethnic group, respondents who were race concordant reported greater satisfaction with their physician compared with respondents who were not race concordant. These findings suggest support for the continuation of efforts to increase the number of minority physicians, while placinggreater emphasis on improving the ability of physicians to interact with patients who are not of their own race.
<192>Unique Identifier 12461303Authors Finkielman JD. Schwartz GL. Chapman AB. Boerwinkle E. Turner ST.Institution Division of Hypertension, Department of Internal Medicine, Mayo Clinic, Rochester,MN, USA.Title Reproducibility of blood pressure response to hydrochlorothiazide.Source Journal of Clinical Hypertension. 4(6):408-12, 2002 Nov-Dec.Abstract Few studies have investigated the reproducibility of responses to antihypertensivetherapies. The purpose of this study was to assess the reproducibility of the blood pressure response to a thiazide diuretic, a preferred initial treatment for hypertension. Twenty-two subjects who underwent monotherapy with hydrochlorothiazideas part of a study to identify predictors of blood pressure response agreed to undergo the same protocol a second time, 26.6+/-11.8 (range, 4-52) months after their first participation. The mean systolic and diastolic blood pressure responses to hydrochlorothiazide did not differ significantly between the first and second participation (systolic response, -14.2+/-16.4 mm Hg vs. -16.0+/-16.5 mm Hg; diastolic response, -7.1+/-11.8 mm Hg vs. -6.6+/-8.6 mm Hg), and these responses were significantly correlated between the two trials (systolic response, r=0.61 and p<0.01; diastolic response, r=0.64 and p<0.01). However, both the direction and magnitude of responses for individual subjects varied considerably, with the limits of agreement between the first and second participations (i.e., 2 standard deviations above and below the mean difference between responses) ranging from 27.4 mm Hg to -23.8 mm Hg for systolic blood pressure response and from 17.4 mm Hg to -18.4 mm Hg for diastolic blood pressure response. These results show that the average systolic and diastolic blood pressure responses to hydrochlorothiazide for agroup of subjects are reproducible; however, the responses for individual subjects are unpredictable. Copyright 2002 Le Jacq Communications, Inc.
<193>Page 99

1-200.txtUnique Identifier 12457781Authors Power C.Institution Institute of Child Health, WC1N 1EH, London, UK. [email protected] Childhood adversity still matters for adult health outcomes.[comment].Source Lancet. 360(9346):1619-20, 2002 Nov 23.
<194>Unique Identifier 12455339Authors Davidson PL. Calhoun JG. Sinioris ME. Griffith JR.Institution Department of Health Services, School of Public Health, University of California, Los Angeles, USA.Title A framework for evaluating and continuously improving the NCHL transformational leadership initiative. National Center for Healthcare Leadership.Source Quality Management in Health Care. 11(1):3-13, 2002 Fall.Abstract The National Center for Healthcare Leadership transformational leadership project is a broad and ambitious initiative that seeks to bring to the table top leaders from industry and academe. Their charge is to accomplish nothing short of resetting the course for health management education and practice in the coming decades. Four councils were recruited to launch the four major interventions: (1) recruitment and diversity, (2) core competencies, (3) the advanced learning institute, and (4) accreditation and certification. After describing intervention goals, we provide examples of baseline measures for tracking educational and performance outcomes longitudinally. We believe this transformation is only beginning, and it will take many years or decades. The transformation will be most successful if it is guided bydata and systematic evaluation.
<195>Unique Identifier 12450475Authors Morell VW. Sharp PC. Crandall SJ.Institution Wake Forest University School of Medicine, Department of Family and Community Medicine, Winston-Salem, NC 27157, USA. [email protected] Creating student awareness to improve cultural competence: creating the critical incident.Source Medical Teacher. 24(5):532-4, 2002 Sep.Abstract Teaching medical students to recognize the need for cultural competence and accepttheir shortcomings in this area is a challenge. A simulated patient scenario was developed to address this challenge. The objective of the simulation is to enhance students' readiness to learn by moving them from 'unconscious incompetence' to 'conscious incompetence'. The patient scenario presents a Cherokee Indian woman witha complaint of abnormal menstrual bleeding who is resistant to gynaecologic care from male providers. A faculty member facilitates a small-group videotape review of student interviews. As students discuss their encounters, they realize they 'misdiagnose' and mishandle the interview. They are confronted by their inability torecognize cultural cues and the impact they may have on health outcomes and begin to
Page 100
1-200.txtquestion whether cultural beliefs are affecting the care of other patients. This simulation creates an eye-opening situation that must be handled carefully. This activity is an effective method to create awareness in students who feel they 'know all this stuff.'
<196>Unique Identifier 12446062Authors Rumsfeld JS. Plomondon ME. Peterson ED. Shlipak MG. Maynard C. Grunwald GK. Grover FL. Shroyer AL.Institution Cardiology (111B), Denver VA Medical Center, 1055 Clermont Street, Denver, Colorado 80222, USA. [email protected] The impact of ethnicity on outcomes following coronary artery bypass graft surgeryin the Veterans Health Administration.Source Journal of the American College of Cardiology. 40(10):1786-93, 2002 Nov 20.Abstract OBJECTIVES: We evaluated the effect of African American (AA) and Hispanic American(HA) ethnicity on mortality and complications following coronary artery bypass graft(CABG) surgery in the Veterans Health Administration (VHA). BACKGROUND: Few studies have examined the impact of ethnicity on outcomes following cardiovascular procedures. METHODS: This study included all 29,333 Caucasian, 2,570 AA, and 1,525 HA patients who underwent CABG surgery at any one of the 43 VHA cardiac surgery centers from January 1995 through March 2001. We evaluated the relationship between ethnicity (AA vs. Caucasian and HA vs. Caucasian) and 30-day mortality, 6-month mortality, and 30-day complications, adjusting for a wide array of demographic, cardiac, and noncardiac variables. RESULTS: After adjustment for baseline characteristics, AA and Caucasian patients had similar 30-day (AA/Caucasian odds ratio [OR] 1.07; 95% confidence interval [CI] 0.84 to 1.35; p = 0.59) and 6-month mortality risk (AA/Caucasian OR 1.10; 95% CI 0.91 to 1.34; p = 0.31). However, amongpatients with low surgical risk, AA ethnicity was associated with higher mortality (OR 1.52, CI 1.10 to 2.11, p = 0.01), and AA patients were more likely to experiencecomplications following surgery (OR 1.28; 95% CI 1.14 to 1.45; p < 0.01). In contrast, HA patients had lower 30-day (HA/Caucasian OR 0.70; 95% CI 0.49 to 0.98; p= 0.04) and 6-month mortality risk (HA/Caucasian OR 0.66; 95% CI 0.50 to 0.88; p < 0.01) than Caucasian patients. CONCLUSIONS: Ethnicity does not appear to be a strongrisk factor for adverse outcomes following CABG surgery in the VHA. Future studies are needed to determine why AA patients have more complications, but ethnicity should not affect the decision to offer the operation.
<197>Unique Identifier 12439154Authors Leach J.Institution Department of Otolaryngology-Head and Neck Surgery, University of Texas Southwestern Medical Center, Dallas, Texas 75390-9035, USA.Title Aesthetics and the Hispanic rhinoplasty.Source Laryngoscope. 112(11):1903-16, 2002 Nov.Abstract OBJECTIVES/HYPOTHESIS: Current aesthetic standards for rhinoplasty have been formulated for an Anglo-American population. Nevertheless, these standards vary, andit is doubtful that these norms are universally applicable to Anglo populations, much less Hispanic ones. STUDY DESIGN: A retrospective study was carried out to determine how the Western norms apply to rhinoplasty populations of Anglo and
Page 101

1-200.txtHispanic background. The effectiveness of rhinoplasty techniques used in Hispanic rhinoplasty were assessed. METHODS: The open approach was used frequently to augmentthe nasal skeleton in this population with thick skin. Techniques were primarily aimed at achieving symmetry, straightening the dorsum, and improving projection, since these Hispanic patients were less interested in tip definition or alar base narrowing. RESULTS: Hispanics were significantly more likely to have dorsal humps, saddle deformities, dependent alae, retracted columellae, and poor tip projection. The nasolabial (columellar-labial) angle method of assessing tip rotation was not accurate in the Hispanic population. Tip definition was better in Anglos, and skin thickness and base width were greater among Hispanics. Rhinoplasty can be effective in achieving aesthetic norms: As a group, the Hispanic profile was brought into greater conformity with the aesthetic norms than their Anglo counterparts who did not have surgery. CONCLUSIONS: Thick nasal skin does not adapt well to a small osteocartilaginous framework, and it is better to augment and strengthen the skeleton with cartilage grafts. Even among Anglos, the Western artistic canons are merely guidelines. Good communication with the patient is more important than adhering to aesthetic norms.
<198>Unique Identifier 12435834Authors Walters KL. Simoni JM. Evans-Campbell T.Institution School of Social Work, University of Washington, 4101 15th Avenue, NE, Seattle, WA98105-6299, USA. [email protected] Substance use among American Indians and Alaska natives: incorporating culture in an "indigenist" stress-coping paradigm.Source Public Health Reports. 117 Suppl 1:S104-17, 2002.Abstract OBJECTIVES: This article proposes a new stress-coping model for American Indians and Alaska Natives (AIs) that reflects a paradigmatic shift in the conceptualizationof Native health. It reviews sociodemographic information on AIs, rates of substanceabuse and related health outcomes, and the research supporting the model's pathways.OBSERVATIONS: Although health outcomes among AIs are improving, large disparities with other racial and ethnic groups in the United States remain. Many health-relatedproblems are directly linked to high rates of substance use and abuse. CONCLUSION: Eurocentric paradigms focus on individual pathology. An "indigenist" perspective of health incorporates the devastating impact of historical trauma and ongoing oppression of AIs. The model emphasizes cultural strengths, such as the family and community, spirituality and traditional healing practices, and group identity attitudes.
<199>Unique Identifier 12435828Authors Schoenbaum EE. Lo Y. Floris-Moore M.Institution AIDS Research Program, Montefiore Medical Center, 111 East 210th Street, Bronx, New York 10467, USA. [email protected] Predictors of hospitalization for HIV-positive women and men drug users, 1996-2000.Source Public Health Reports. 117 Suppl 1:S60-6, 2002.Abstract OBJECTIVE: This study sought to determine whether health outcomes differed by gender in a cohort of African American, Hispanic American, and white drug users.
Page 102

1-200.txtMETHODS: The authors studied hospitalization rates and discharge diagnoses in the HERO Study, an ongoing prospective study of drug users that included HIV-positive and HIV-negative opiate users. The data are from 1996-2000, when highly active antiretroviral therapy (HAART) was available. RESULTS: Women had higher rates of hospitalization than men independent of HIV status, and there was no association between ethnicity and hospitalization. Being a woman was an independent risk factor for HIV and non-HIV-related hospitalization. CONCLUSION: Health disparities between men and women extend to HIV.
<200>Unique Identifier 12434169Authors Kaminogo M. Yonekura M.Institution Department of Neurosurgery, Nagasaki University School of Medicine, Nagasaki, Japan.Title Trends in subarachnoid haemorrhage in elderly persons from Nagasaki, Japan: analysis of the Nagasaki SAH Data Bank for cerebral aneurysm, 1989-1998.Source Acta Neurochirurgica. 144(11):1133-8; discussion 1138-9, 2002 Nov.Abstract BACKGROUND: Many industrialized countries are facing a volumetric growth of the senior population. We studied the trends in the incidence and outcome of subarachnoid haemorrhage (SAH) in patients aged >or=70 years. METHOD: We retrospectively reviewed the cases of 1030 patients registered in the Nagasaki SAH Data Bank from 1989 to 1993 and 1274 patients registered from 1994 to 1998. FINDINGS: The annual age-adjusted incidence of SAH per 100,000 increased only in women, from 15.4 in the 1989-1993 period to 19.7 in the 1994-1998 period. The average annual incidence of SAH per 100,000 women in the elderly aged >or=70 years increased significantly from 44.3 in the first period to 58.2 in the second period. In patients aged >or=70 years, the proportion of high-grade SAH (Hunt & Kosnik GradeIV and V) significantly increased from 27.2% in the first 5 years to 38.2% in the second 5 years. In patients aged<70 years, it increased slightly from 23.4% to 26.7%. The rate of favorable outcomes significantly fell from 43.9% (first period) to 30.9% (second period) in patients aged >or=70 years but was stable in patients aged<70 years. INTERPRETATION: Although the incidence of elderly patients with SAH in our study is compatible with or higher than that of other reports, we believe that elderly patients (especially women) with high-grade SAH may not have all been identified. When we discuss the management of ruptured and unruptured aneurysms in the elderly, we should bear these trends of SAH in mind.
Page 103

201-400.txt<1>Unique Identifier 12431552Authors Fukunishi I. Paris W. Mitchell S. Nour B.Institution Tokyo Institute of Psychiatry, Tokyo Metropolitan Organization for Medical Research, Tokyo, Japan.Title Posttraumatic stress disorder in the families of cadaveric and living donor population: a comparison of Japanese and American outcomes.Source Transplantation Proceedings. 34(7):2627, 2002 Nov.
<2>Unique Identifier 12431551Authors Fukunishi I. Paris W. Mitchell S. Nour B.Institution Tokyo Institute of Psychiatry, Tokyo Metropolitan Organization for Medical Research, Tokyo, Japan.Title Emotional conditions of donor families: a comparison of Japanese and American outcomes.Source Transplantation Proceedings. 34(7):2626, 2002 Nov.
<3>Unique Identifier 12427395Authors Chandra PC. Schiavello HJ. Ravi B. Weinstein AG. Hook FB.Institution Department of Obstetrics and Gynecology, Wyckoff Heights Medical Center, Brooklyn,NY, USA. [email protected] Pregnancy outcomes in urban teenagers.Source International Journal of Gynaecology & Obstetrics. 79(2):117-22, 2002 Nov.Abstract OBJECTIVES: To compare pregnancy outcomes for teenagers with those for older gravidas. METHODS: A retrospective case control study was undertaken to compare teenagers who delivered between January 1996 and October 1999 at a public urban hospital with a group of older gravidas. RESULTS: Young pregnant teenagers were morelikely to be nulliparous. They weighed less and gained less in pregnancy. More teen pregnancies occurred among Hispanics than other ethnic groups. The younger the teenager, the more likely for her infant to be of low or very low birth weight or growth restricted. There were fewer postmature deliveries, macrosomic fetuses and cesarean deliveries in young gravidas. Perinatal mortality was unaffected by maternal age. CONCLUSIONS: This investigation demonstrates that, while pregnancy outcomes in teenagers have improved in recent years relative to historical patterns,teenagers face continuing problems requiring special attention by care givers.
<4>Unique Identifier 12424781Authors Lange JW.Institution
Page 1

201-400.txt Fairfield University School of Nursing, North Benson Road, Fairfield, CT 06430, USA.Title Testing equivalence of Spanish and English versions: the LaMonica-Oberst (revised)patient satisfaction with nursing care scale.Source Research in Nursing & Health. 25(6):438-51, 2002 Dec.Abstract Despite recent emphasis on outcome measurement and an increasing proportion of Spanish speakers in the United States, most patient satisfaction studies exclude Spanish-speaking participants because Spanish versions of instruments are not available. A Spanish translation of the 15-item LaMonica-Oberst Patient SatisfactionScale, completed by 64 Spanish-speaking patients living in the northeast and of predominantly Puerto Rican ancestry, produced two factors explaining 86.3% of score variation (alpha=.94 and.58). Evidence for equivalence to the English version and concurrent validity is presented. Generalizability and decision studies indicate that four additional items are needed on the dissatisfaction subscale to attain an acceptable dependability coefficient. Copyright 2002 Wiley Periodicals, Inc. Res Nurs Health 25:438-451, 2002.
<5>Unique Identifier 12419000Authors Chan CC. Lee TM. Fong KN. Lee C. Wong V.Institution Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong. [email protected] Cognitive profile for Chinese patients with stroke.Source Brain Injury. 16(10):873-84, 2002 Oct.Abstract PRIMARY OBJECTIVE: This study aimed to investigate the usefulness of the Chinese version of Cognistat for patients with stroke in a Chinese community. METHODS AND PROCEDURES: A total of 53 patients and 34 normal elderly with age, gender and literacy level matched were tested with the Chinese translated version of Cognistat.OUTCOMES AND RESULTS: The results suggest that the patients performed significantly lower than their normal counterparts on the test. The Orientation, Attention and Calculation sub-tests were the most significant contributors to its high sensitivity(0.79) and specificity (0.85), which is largely consistent with the original Englishversion. A two-factor structure was confirmed with the 10 sub-tests clustered into the areas of fluid and crystallized abilities, which indicates that the translation of the test content did not alter the structure of the instrument. However, the low level of literacy of the local elderly population and language structure tends to slightly alter the cognitive profile of the patients. CONCLUSIONS: Further studies are recommended to further explore the cross-cultural issues and clinical implications on establishing cognitive profile for patients with stroke with Cognistat.
<6>Unique Identifier 12414332Authors Young JM. Bennett C. Gilhooly P. Wessells H. Ramos DE.Institution South Orange County Urological Medical Associates, Laguna Woods, California 92653,USA. [email protected] Efficacy and safety of sildenafil citrate (Viagra) in black and Hispanic American men.
Page 2

201-400.txtSource Urology. 60(2 Suppl 2):39-48, 2002 Sep.Abstract The objective of this study was to assess the efficacy and safety of sildenafil citrate (Viagra) in black American and Hispanic American men with erectile dysfunction (ED) of broad-spectrum etiology. A total of 246 black American and 197 Hispanic American men were randomized to sildenafil (50 mg, adjustable to 25 mg or 100 mg, depending on efficacy and tolerability; n = 124 and n = 99, respectively) ormatching placebo (n = 122 and n = 98, respectively). After 6 weeks, patients were given the option of switching to the other blinded treatment for the following 6 weeks. The 12 weeks of double-blind treatment were followed by 12 weeks of open-label extension. Despite differences in prevalence of hypertension, diabetes mellitus, hyperlipidemia, and use of concomitant antihypertensive agents between the2 study groups, sildenafil was efficacious and well tolerated. After 6 weeks, scoresfor questions 3 and 4 from the International Index of Erectile Function (IIEF) were significantly higher among sildenafil-treated black and Hispanic patients than in placebo-treated patients. In addition, compared with placebo, a significantly largerproportion of sildenafil patients reported improved erections and improved ability to have sexual intercourse. When efficacy results were stratified by ED severity or number of risk factors, scores for IIEF questions 3 and 4 were lower in men with severe ED versus mild-to-moderate ED. Similarly, the percentage of patients reporting improved erections decreased with ED severity and number of risk factors. The proportion of patients switching to the other treatment after 6 weeks was significantly higher in the placebo group (71% to 85%) than in the sildenafil group (27% to 28%). The most common adverse events included headache and vasodilation, which were mild to moderate in nature and were comparable between groups. These datademonstrate that despite differences in prevalence rates of comorbidities, efficacy and safety of sildenafil is maintained across different ethnic groups.
<7>Unique Identifier 12415035Authors Hovell MF. Meltzer SB. Wahlgren DR. Matt GE. Hofstetter CR. Jones JA. Meltzer EO. Bernert JT. Pirkle JL.Institution Center for Behavioral Epidemiology and Community Health, Graduate School of PublicHealth, San Diego State University, San Diego, California 92123, USA. [email protected] Asthma management and environmental tobacco smoke exposure reduction in Latino children: a controlled trial.Source Pediatrics. 110(5):946-56, 2002 Nov.Abstract OBJECTIVES: This study tested the efficacy of coaching to reduce environmental tobacco smoke (ETS) exposure among asthmatic Latino children. DESIGN: After asthma management education, families were randomly assigned to no additional service (control condition) or to coaching for ETS exposure reduction (experimental condition). SETTING: The study was conducted in San Diego, California. PARTICIPANTS:Two hundred four Latino children (ages 3-17 years) with asthma participated. INTERVENTION: Approximately 1.5 hours of asthma management education was provided; experimental families also obtained 7 coaching sessions ( approximately 45 minutes each) to reduce ETS exposure. OUTCOME MEASURES: Reported ETS exposure and children'surine cotinine were measured. RESULTS: Parents in the coached condition reported their children exposed to significantly fewer cigarettes than parents of control children by 4 months (postcoaching). Reported prevalence of exposed children decreased to 52% for the coached families, but only to 69% for controls. By month 4,mean cotinine levels decreased among coached and increased among control children. Cotinine prevalence decreased from 54% to 40% among coached families, while it increased from 43% to 49% among controls. However, cotinine levels decreased among controls to the same level achieved by coached families by the 13-month follow-up.
Page 3
201-400.txtCONCLUSIONS: Asthma management education plus coaching can reduce ETS exposure more than expected from education alone, and decreases in the coached condition may be sustained for about a year. The delayed decrease in cotinine among controls is discussed.
<8>Unique Identifier 12407964Authors Morales LS. Lara M. Kington RS. Valdez RO. Escarce JJ.Institution University of California, Los Angeles, USA.Title Socioeconomic, cultural, and behavioral factors affecting Hispanic health outcomes. [Review] [102 refs]Source Journal of Health Care for the Poor & Underserved. 13(4):477-503, 2002 Nov.Abstract Evidence suggests that social and economic factors are important determinants of health. Yet, despite higher porverty rates, less education, and worse access to health care, health outcomes of many Hispanics living in the United States today areequal to, or better than, those of non-Hispanic whites. This paradox is described inthe literature as the epidemiological paradox or Hispanic health paradox. In this paper, the authors selectively review data and research supporting the existence of the epidemiological paradox. They find substantial support for the existence of the epidemiological paradox, particularly among Mexican Americans. Census undercounts ofHispanics, misclassification of Hispanic deaths, and emigration of Hispanics do not fully account for the epidemiological paradox. Identifying protective factors underlying the epidemiological paradox, while improving access to care and the economic conditions among Hispanics, are important research and policy implications of this review. [References: 102]
<9>Unique Identifier 12406802Authors Lin SS. Clarke CA. O'Malley CD. Le GM.Institution Northern California Cancer Center, Union City 94587, USA. [email protected] Studying cancer incidence and outcomes in immigrants: methodological concerns.Source American Journal of Public Health. 92(11):1757-9, 2002 Nov.
<10>Unique Identifier 12406481Authors Elder JP. Litrownik AJ. Slymen DJ. Campbell NR. Parra-Medina D. Choe S. Lee V. Ayala GX.Institution San Diego State University Graduate School of Public Health, San Diego, California92123, USA. [email protected] Tobacco and alcohol use-prevention program for Hispanic migrant adolescents.Source American Journal of Preventive Medicine. 23(4):269-75, 2002 Nov.Abstract OBJECTIVE: Evaluate a community-based tobacco/alcohol use-prevention program groupcompared with an attention-control condition (first aid/home safety) group. METHODS:
Page 4

201-400.txtA total of 660 adolescents and 1 adult caregiver for each were recruited through theMigrant Education Program to participate in an 8-week intervention. Random assignment to the two groups occurred in 22 schools. Seventy 8-week intervention groups (37 tobacco/alcohol and 33 attention-control) were conducted. Assessments occurred at baseline, immediate post-intervention, and 1- and 2-year follow-ups. Susceptibility to smoking and alcohol as well as smoking and drinking over the past 30 days were the primary outcomes of interest. RESULTS: Following intervention, no between-group differences in smoking or drinking were significant. Thirty-day smoking started and remained at very low levels, with the highest group prevalence at any measurement period being 4.7% and the lowest 2.5%. Those considered susceptible to smoking dropped by nearly 40% in the attention-control group and by 50% in the intervention group from baseline to the final follow-up. (The overall reduction from post-test to final follow-up was statistically significant.) Less-acculturated children were less likely to report drinking in the past 30 days. CONCLUSIONS: The current intervention was not demonstrated to be effective in preventing cigarette or alcohol consumption. This perhaps is due to very low baseline levels of smoking and drinking in the migrant youth participants.
<11>Unique Identifier 12398858Authors Stein JA. Leslie MB. Nyamathi A.Institution Department of Psychology, University of California, 1282 Franz Hall, Los Angeles, CA 90095-1563, USA.Title Relative contributions of parent substance use and childhood maltreatment to chronic homelessness, depression, and substance abuse problems among homeless women:mediating roles of self-esteem and abuse in adulthood.[see comment].Source Child Abuse & Neglect. 26(10):1011-27, 2002 Oct.Abstract OBJECTIVE: This study, using latent variable methodology, explores simultaneously the relative effects of childhood abuse and early parental substance abuse on later chronic homelessness, depression, and substance abuse problems in a sample of homeless women. We also examine whether self-esteem and recent violence can serve asmediators between the childhood predictors and the dysfunctional outcomes.METHOD: The sample consists of 581 homeless women residing in shelters or sober living centers in Los Angeles (54% African-American, 23% Latina, 22% White, mean age=33.5 years). Multiple-indicator latent variables served as predictors and outcomes in structural models. Childhood abuse was indicated by sexual, physical, and verbal abuse.RESULTS: Childhood abuse directly predicted later physical abuse, chronic homelessness, depression, and less self-esteem. Parent substance use directly predicted later substance use problems among the women. Recent physical abuse predicted chronic homelessness, depression, and substance use problems. Greater self-esteem predicted less depression and fewer substance use problems. Childhood abuse also had significant indirect effects on depression, chronic homelessness, anddrug and alcohol problems mediated through later physical abuse and self-esteem.CONCLUSIONS: Although there was a strong relationship between childhood abuse and parent drug use, childhood abuse was the more pervasive and devastating predictor of dysfunctional outcomes. Childhood abuse predicted a wider range of problems including lower self-esteem, more victimization, more depression, and chronic homelessness, and indirectly predicted drug and alcohol problems. The mediating roles of recent physical abuse and self-esteem suggest salient leverage points for change through empowerment training and self-esteem enhancement in homeless women.
<12>Unique Identifier 12389956
Page 5

201-400.txtAuthors Astrom AN. Blay D.Institution Department of Odontology, Community Dentistry, Centre for International Health, University of Bergen, Norway.Title Multidimensional health locus of control scales: applicability among Ghanaian adolescents.Source East African Medical Journal. 79(3):128-33, 2002 Mar.Abstract BACKGROUND: Primary preventive approaches are likely to be more effective if the motivational factors of health behaviours are known. Beliefs about control over health outcomes are among the most important motivational factors, commonly assessedwith the multidimensional health locus of control scale (MHLC). OBJECTIVES: To examine the validity, reliability and cross-cultural correspondence of the MHLC scales among Ghanaian adolescents. DESIGN: Cross-sectional questionnaire survey. SETTING: Secondary schools in the Awutu-Effutu-Senya district of Ghana, 1998. SUBJECTS: The analysis is based on 504 secondary school children constituting a response rate of 86%. INTERVENTIOn: Non-intervention study. MAIN OUTCOME MEASURES: The MHLC score comprising beliefs in own control over health, beliefs in provider control over health and beliefs in chance health outcomes. RESULTS: Fifty per cent urban and 48% rural pupils recorded health as an important issue. More than 90% of the participants were correctly informed regarding oral health consequences of toothcleaning, tobacco smoking and sugar consumption. Exploratory factor analysis gave two sub-factors of the MHLC corresponding to internal and provider control over health and having internal consistency reliability of 0.72 and 0.76, respectively. CONCLUSION: The results lend support to the cultural correspondence of the MHLC instrument, several aspects of its validity and internal consistency reliability.
<13>Unique Identifier 12387558Authors Kumpfer KL. Alvarado R. Smith P. Bellamy N.Institution Department of Health Promotion and Education, University of Utah, Salt Lake City 84112, USA. [email protected] Cultural sensitivity and adaptation in family-based prevention interventions.Source Prevention Science. 3(3):241-6, 2002 Sep.Abstract Because of the substantial impact of families on the developmental trajectories ofchildren, family interventions should be a critical ingredient in comprehensive prevention programs. Very few family interventions have been adapted to be culturally sensitive for different ethnic groups. This paper examines the research literature on whether culturally adapting family interventions improves retention and outcome effectiveness. Because of limited research on the topic, the prevention research field is divided on the issue. Factors to consider for cultural adaptationsof family-focused prevention are presented. Five research studies testing the effectiveness of the generic version of the Strengthening Families Program (SFP) compared to culturally-adapted versions for African Americans, Hispanic, Asian/Pacific Islander, and American Indian families suggest that cultural adaptations made by practitioners that reduce dosage or eliminate critical core content can increase retention by up to 40%, but reduce positive outcomes. Recommendations include the need for additional research on culturally-sensitive family interventions.
<14>Unique Identifier
Page 6

201-400.txt 12385922Authors Serretta V. Morgia G. Fondacaro L. Curto G. Lo bianco A. Pirritano D. Melloni D. Orestano F. Motta M. Pavone-Macaluso M. Members of the Sicilian-Calabrian Society of Urology.Institution Institute of Urology, University of Palermo, Palermo, Italy.Title Open prostatectomy for benign prostatic enlargement in southern Europe in the late1990s: a contemporary series of 1800 interventions.Source Urology. 60(4):623-7, 2002 Oct.Abstract OBJECTIVES: Contemporary series of open prostatectomies from Western countries arerare. Frequently, the analysis of the outcome of open prostatectomy refers to old experiences or to series from developing countries. Any comparison with transurethral resection of the prostate can be invalidated by complications of open surgery because of the lack of an adequate healthcare system and technology. METHODS: The Sicilian-Calabrian Society of Urology performed a retrospective study to assess the surgical management of benign prostatic hyperplasia in Sicily and Calabria in 1997 and 1998. A three-page questionnaire was sent to the 36 urologic units of these two Italian regions with more than 7.5 million inhabitants. RESULTS: Twenty-six units (72.3%) replied. Of 31,558 patients treated for symptomatic benign prostatic hyperplasia, 5636 underwent surgery. Open prostatectomy (n = 1804) accounted for 32% of all surgical treatment. The median prostate volume was 75 cm(3)and the median serum prostate-specific antigen level was 3.7 ng/mL. The postoperative median hospitalization time was 7 days. Concomitant low urinary tract disease was present in 25% of the patients. Severe bleeding occurred in 11.6% of open prostatectomies. Blood transfusions were given in 8.2% of cases. Sepsis was reported in 8.6% of the patients. Reinterventions, within 2 years, mainly due to bladder neck stenosis, were reported in 3.6% of cases. CONCLUSIONS: The results of the present survey provide a current picture of open prostatectomy. This procedure, even if performed nowadays and in Western countries, shows the same significant rateof early and late complications reported in the past or in less-developed countries.
<15>Unique Identifier 12385912Authors Isotani S. Fujisawa M. Ichikawa Y. Ishimura T. Matsumoto O. Hamami G. Arakawa S. Iijima K. Yoshikawa N. Nagano S. Kamidono S.Institution Division of Urology, Department of Organs Therapeutics, Kobe University Graduate School of Medicine, Kobe, Japan.Title Quality of life of living kidney donors: the short-form 36-item health questionnaire survey.Source Urology. 60(4):588-92; discussion 592, 2002 Oct.Abstract OBJECTIVES: To determine the psychological and social effects of kidney donation on kidney donors by using the short-form 36-item health survey (SF-36) as the quality-of-life questionnaire. METHODS: A total of 104 living donor nephrectomies have been performed at Kobe University Hospital and Nishinomiya Prefectural Hospital. We mailed the questionnaires to donors or handed them out directly at the outpatient clinic. The first part of the questionnaire consisted of the SF-36 (limitations on physical functioning because of health problems) and the second partconsisted of 15 questions about donation-related stress, expenses incurred, physicalchanges, and pre-existing factors such as relationship to the recipients. RESULTS: The SF-36 and the questionnaire about donor satisfaction were completed by 69 donors(48 women and 21 men; mean age 52.1 +/- 8.2 years), only 6 of whom (9%) reported minor complications with the donor operation. The SF-36 scores of our donors were
Page 7

201-400.txtnot significantly different from that of the general U.S. population and U.S. donors. In some categories (physical functioning, role-physical, bodily pain, general health, vitality, and mental health), our donors scored slightly higher thanthe U.S. general population. Although 97% of the donors would make the same choice again, 3% believed that donating had had a negative impact on their health, and 16% reported negative financial consequences. CONCLUSIONS: The quality of life for kidney donors was not affected by donor nephrectomy. Living kidney transplantation seems to be suitable for the rescue of patients with end-stage renal disease. Betterpsychological and technical preparation for surgery and more consistent follow-up may reduce the negative outcomes even further.
<16>Unique Identifier 12386605Authors Gorek B. Martin J. White N. Peters D. Hummel F.Institution United Medical Center in Cheyenne, WY, USA.Title Culturally competent care for Latino elders in long-term care settings.Source Geriatric Nursing. 23(5):272-5, 2002 Sep-Oct.Abstract The decision to place a family member in a long-term care (LTC) facility results in a variety of experiences for families. The experience of Latino families can be particularly problematic for the different relatives involved in the process. Placing a loved one in an LTC facility goes against cultural norms for Hispanic families that can lead to problems for both the family and the facility staff. Information about the cultural norms that are violated along with ways that the careproviders and administrative staff can make adjustments in the environment to assistthese residents will improve outcomes and meet the needs of diverse health care consumers.
<17>Unique Identifier 12385486Authors Hobfoll SE. Jackson A. Hobfoll I. Pierce CA. Young S.Institution Applied Psychology Center, Kent State University, Ohio 44242, USA. [email protected] The impact of communal-mastery versus self-mastery on emotional outcomes during stressful conditions: a prospective study of Native American women.Source American Journal of Community Psychology. 30(6):853-71, 2002 Dec.Abstract Past research has examined the stress resiliency of individuals high in sense of personal-mastery. However, it has been theorized that within more collectivist cultures, a sense of shared efficacy, which we call communal-mastery, may be more central to people's resiliency in the face of challenging life circumstances. We compared the impact of sense of self-mastery (ie., "I am the key to my success") to that of communal-mastery (ie., "I am successful by virtue of my social attachments")in a prospective study among a group of rural 103 Native American women residing on Indian Reservations in Montana. We found that women high in communal-mastery experienced less increase in depressive mood and anger, especially when faced with high stress circumstances, than women who were low in communal-mastery. In addition,the beneficial impact of communal-mastery was found to be more effective than self-mastery for these women.
Page 8

201-400.txt<18>Unique Identifier 12376977Authors McNeil DE. Cote TR. Clegg L. Mauer A.Institution Division of Cancer Epidemiology and Genetics, Genetic Epidemiology Branch, National Cancer Institute/NIH, EPS Room 7125, 6120 Executive Boulevard, MSC 7236, Rockville, MD 20892-7236, USA. [email protected] SEER update of incidence and trends in pediatric malignancies: acute lymphoblasticleukemia.[see comment].Source Medical & Pediatric Oncology. 39(6):554-7; discussion 552-3, 2002 Dec.Abstract BACKGROUND: Acute lymphoblastic leukemia (ALL) represents the most common malignancy of childhood. Its incidence peaks in children just before school entry age; i.e., in 2-3 year olds. It is known to be more common in white children in the USA; the incidence is also higher in boys than girls. PROCEDURE: We reviewed the 5,379 cases of ALL among persons under 20 years of age in the National Cancer Institute's Surveillance Epidemiology and End Results (SEER) database. RESULTS: The overall incidence of ALL was 26/10(6) person-years between 1973 and 1998, but increased from 19/10(6) person-years in 1973-77 to 28/10(6) person-years in 1993-98 (P < 0.0001). Rates were 44% higher among Whites compared to Blacks (27/10(6) person-years vs. 15/10(6) person-years, P < 0.0001). In 1992-1998, the incidence rate for Hispanics was 43/10(6) person-years, significantly higher than non-Hispanics (28/10(6), P < 0.0001). White children with ALL had better 5-year survival rates than Black children with ALL (71% vs. 58%, P < 0.0001), and 5-year survival was poorest among black males. CONCLUSIONS: ALL incidence has increased over the examined 25-year period. The rate in US whites is higher than that of US Blacks, and the rates in the Hispanic subgroup are the highest of all. While the median survival period is now more than 10 years overall, the 5-year survival rate remains poor for Black males under 4 years of age. Socioeconomic factors do not account for this difference, which may relate to ALL subtype distribution. Copyright2002 Wiley-Liss, Inc.
<19>Unique Identifier 12376307Authors Huang Y. Xia DB.Institution Department of TCM, First Military Medical University, Guangzhou 510515, China. [email protected] Treatment of stroke with "five-center needling": clinical observation of 78 cases.Source Di Yi Junyi Daxue Xuebao. 22(7):657-8, 2002 Jul.Abstract OBJECTIVE: To observe the efficacy of "five center needling" in the management of stroke. METHOD: Seventy-eight patients suffering stroke were divided into 2 groups to receive either routine acupuncture (control group, n=38) treatment or "five-center needing" therapy besides the routine treatment (treatment group, n=40).The curative effect between the 2 groups was compared after 30 days treatment. RESULT: No significant differences were noted between the 2 groups in terms of the curative effect in general (P>0.05). But "five-center needling" showed better effectin treating the syndromes of wind-fire stirring up the orifices and phlegm stagnation leading to mental disorder, and was more effective in the management of hemorrhagic stroke than in ischemic stroke, and in treating the left-side cerebral injuries than in treating those on right side (P<0.05).
Page 9

201-400.txt<20>Unique Identifier 12365758Authors Shera W. Aviram U. Healy B. Ramon S.Institution Faculty of Social Work, University of Toronto, Canada.Title Mental health system reform: a multi country comparison.Source Social Work in Health Care. 35(1-2):547-75, 2002.Abstract In recent years many countries have embarked on various types of health and mentalhealth reform. These reforms have in large part been driven by governments' concernsfor cost containment which has, in turn, been driven by an increasing process of global marketization and the need to control national deficits. A critical issue in these reforms is the increased emphasis on the use of "market mechanisms" in the delivery of health and mental health services. This paper uses a policy analysis framework to compare recent developments in the mental health sector in Canada, the United States, Britain and Australia. The common framework to be used for this will focus on: the defining characteristics of the society; legislative mandate; sectorial location (within or separate from health sector); funding streams; organising values of the system; locus of service delivery; service technologies; the role of social work; interprofessional dynamics; the role of consumers; and evaluation of outcomes at multiple levels. This analysis provides an opportunity to explore similarities and differences in mental system reform and in particular identify the challenges for social work in the field of mental health in the 21st century.
<21>Unique Identifier 12365749Authors Brenner B.Institution Mount Sinai Medical Center, and Department of Community Medicine, Mount Sinai School of Medicine, USA.Title Implementing a community intervention program for health promotion.Source Social Work in Health Care. 35(1-2):359-75, 2002.Abstract High rates of cardiovascular disease (CVD) among low income African American and Latinos are well documented. While health promotion interventions leading to personal behavior change are known to reduce CVD in white, middle class, more educated populations, these approaches have not been widely tested in poor, minorityethnic communities. This paper describes a community intervention program to reduce cardiovascular disease risk factors in East Harlem, a low income New York City community in Manhattan, whose population is 53% Latino and 39% African American. This primary prevention model seeks to change attitudes, norms and values regarding behaviors that contribute to chronic disease within a defined population through initiating changes in the social, educational, cultural and physical environment. Environmental and organizational conditions that predict successful outcomes for themodel and strategies, methods and skills, borrowed from social work and other behavioral sciences to implement and institutionalize community wide lifestyle changes, are highlighted.
<22>Unique Identifier 12361668Authors
Page 10

201-400.txt Alexopoulos GS. Buckwalter K. Olin J. Martinez R. Wainscott C. Krishnan KR.Institution Weill Medical College of Cornell University, Cornell Institute of Geriatric Psychiatry, White Plains, New York 10605, USA.Title Comorbidity of late life depression: an opportunity for research on mechanisms andtreatment. [Review] [189 refs]Source Biological Psychiatry. 52(6):543-58, 2002 Sep 15.Abstract Late life depression principally affects individuals with other medical and psychosocial problems, including cognitive dysfunction, disability, medical illnesses, and social isolation. The clinical associations of late life depression have guided the development of hypotheses on mechanisms predisposing, initiating, and perpetuating specific mood syndromes. Comorbidity studies have demonstrated a relationship between frontostriatal impairment and late life depression. Further research has the potential to identify dysfunctions of specific frontostriatal systems critical for antidepressant response and to lead to novel pharmacological treatments and targeted psychosocial interventions.The reciprocal interactions of depression with disability, medical illnesses, treatment adherence, and other psychosocial factors complicate the care of depressed older adults. Growing knowledge of the clinical complexity introduced by the comorbidity of late life depression can guide the development of comprehensive treatment models. Targeting the interacting clinical characteristics associated with poor outcomes has the potential to interrupt the spiral of deterioration of depressed elderly patients. Treatment models can be most effective if they focus on amelioration of depressive symptoms, but also on treatment adherence, prevention of relapse and recurrence, reduction of medical burden and disability, and improvement of the quality of life of patients and their families. [References: 189]
<23>Unique Identifier 12361322Authors Caughy MO. O'Campo PJ. Randolph SM. Nickerson K.Institution University of Texas Health Science Center at Houston School of Public Health, [email protected] The influence of racial socialization practices on the cognitive and behavioral competence of African American preschoolers.Source Child Development. 73(5):1611-25, 2002 Sep-Oct.Abstract The association between parent racial socialization and child competence was examined in a socioeconomically diverse sample of African American preschoolers living in an urban setting. Interviews were conducted in the homes of 200 families. Racial socialization was assessed by parent report as well as by observation of the sociocultural context of the home, and child outcomes were assessed using the Kaufman Assessment Battery for Children and the Child Behavior Checklist. Results indicated that African American parents who provided homes that were rich in AfricanAmerican culture had preschool children who had greater amounts of factual knowledgeand better developed problem-solving skills. African American parents who socializedtheir preschool children to be proud of their heritage reported fewer problem behaviors.
<24>Unique Identifier 12356597Authors Bodeker G. Kronenberg F.
Page 11

201-400.txtInstitution Green College, University of Oxford Medical School, Oxford OX2 6HG, England. [email protected] A public health agenda for traditional, complementary, and alternative medicine.Source American Journal of Public Health. 92(10):1582-91, 2002 Oct.Abstract Traditional medicine (a term used here to denote the indigenous health traditions of the world) and complementary and alternative medicine (T/CAM) have, in the past 10 years, claimed an increasing share of the public's awareness and the agenda of medical researchers. Studies have documented that about half the population of many industrialized countries now use T/CAM, and the proportion is as high as 80% in manydeveloping countries. Most research has focused on clinical and experimental medicine (safety, efficacy, and mechanism of action) and regulatory issues, to the general neglect of public health dimensions. Public health research must consider social, cultural, political, and economic contexts to maximize the contribution of T/CAM to health care systems globally.
<25>Unique Identifier 12356593Authors Park CM.Institution Department of Medicine, Richard and Hinda Rosenthal Center for Complementary and Alternative Medicine, Columbia University College of Physicians and Surgeons, Box 75, 630 W 168th Street, New York, NY 10032, USA. [email protected] Diversity, the individual, and proof of efficacy: complementary and alternative medicine in medical education.Source American Journal of Public Health. 92(10):1568-72, 2002 Oct.Abstract Patients will always have access to a variety of possibly effective, but unproved,therapies directed at maintaining health or treating illness. And there will always be complex, potentially therapeutic regimens that cannot be adequately tested for financial, ethical, or methodological reasons. Furthermore, even after adequate study of a given regimen, there will always be the fundamental uncertainty of medical practice: the fact that epidemiological research produces probabilistic results that cannot predict with certainty the best treatment for the single unique patient before us. The exploration of complementary and alternative medicine topics in the medical school curriculum helps to elucidate the complex and uncertain natureof medical practice, sharpens skills for clinical decisionmaking, increases culturalsensitivity, and provides ideas for future research.
<26>Unique Identifier 12239739Authors Davidoff MJ. Petrini J. Damus K. Russell RB. Mattison D.Institution Perinatal Data Center, March of Dimes Birth Defects Foundation, National Office, 1275 Mamaroneck Avenue, White Plains, NY 10605, USA. [email protected] Neural tube defect-specific infant mortality in the United States.Source Teratology. 66 Suppl 1:S17-22, 2002.Abstract BACKGROUND: Significant resources have been devoted to decreasing the rate of neural tube defects (NTDs) in the United States. Both surveillance data and birth
Page 12

201-400.txtrecords have strengths and limitations for evaluating the outcomes of this resource allocation. Cause-specific infant mortality data can be used as one measure to support evaluation efforts. METHODS: Using period linked birth/infant death data from the National Center for Health Statistics (NCHS), a retrospective analysis was performed to assess the NTD-specific IMR at the national, state, and regional level.NTD-specific IMRs for the United States were calculated from 1996 to 1998; stratified rates by race/ethnicity, maternal age, age at death, and gestational age and birthweight by type of NTD for the total US population were based on three-year aggregates (1996-98); state and regional rates were based on four-year aggregates (1995-98). RESULTS: Annual US NTD-specific IMRs significantly decreased between 1996and 1998. Black infants were significantly less likely to die from an NTD when compared to white infants, largely attributed to the high rate of NTD-specific deaths among white Hispanic infants. Infants born to women less than 20 years were more likely than infants born to women in other age groups to die from an NTD. Seventy-six percent of all NTD-specific deaths occurred in the first 23 hours of life. Seventy-four percent of NTD-specific infant deaths were low birthweight and 58percent were preterm. The Midwest had the highest rate of NTD-specific infant deathsamong US regions. CONCLUSION: Enhanced prevention efforts are needed to address the disparities in infant deaths due to NTDs between Hispanics and other populations, aswell as women under 20 years. Decreases in NTD-specific IMRs may have been impacted by fortification of enriched grain products with folic acid since these efforts wereoptional beginning in 1996. While there are limitations in cause-specific IMRs, NTD-specific IMRs can be used as one measure to assess the impact of public health interventions aimed at reducing NTDs, respectful of the relatively small numbers. Copyright 2002 Wiley-Liss, Inc.
<27>Unique Identifier 12233802Authors Herron RE. Fagan JB.Institution Institute of Science, Technology and Public Health Policy, Maharishi University ofManagement, Fairfield, Iowa, USA.Title Lipophil-mediated reduction of toxicants in humans: an evaluation of an ayurvedic detoxification procedure.Source Alternative Therapies in Health & Medicine. 8(5):40-51, 2002 Sep-Oct.Abstract CONTEXT: Lipophilic toxicants have been associated with hormone disruption, immunesystem suppression, reproductive disorders, several types of cancer, and other diseases. Due to environmental persistence and bioaccumulation, body burdens of certain toxicants, such as dichlorodiphenyldichloroethylene (DDE) and polychlorinated biphenyls (PCBs), appear to be a health risk despite the toxicants' having been banned for decades. OBJECTIVE: To determine whether a safe, standardized, Ayurvedic detoxification procedure can mobilize lipid-soluble toxicants and stimulate their excretion. DESIGN: Cross-sectional and longitudinal evaluations. SETTING: Southeastern Iowa. PARTICIPANTS: In the cross-sectional study,48 participants who had undertaken lipophil-mediated detoxification were compared with 40 control subjects. In the prospective, longitudinal evaluation, serum levels were measured in 15 subjects before and after they underwent the detoxification procedure. These 15 subjects served as their own controls. INTERVENTION(S): Ayurvedic lipophil-mediated detoxification procedure. MAIN OUTCOME MEASURE: Gas chromatographic analysis of 17 serum toxicant levels (9 PCB congeners and 8 pesticides or metabolites) on a lipid-adjusted and wet-weight basis (ng/g) as parts per billion. RESULTS: In the cross-sectional study, gas chromatographic analysis of 9 PCB congeners and 8 pesticides revealed that serum PCB levels were significantly lower in the detoxification subjects than in controls. Trans-nonachlor (TNC), p,p'-dichlorodiphenyldichloroethylene (p,p'-DDE), oxychlordane, and hexachlorobenzene (HCB) levels were also markedly lower in the detoxification group.All subjects had undetectable levels of p,p'-DDT, lindane, and
Page 13
201-400.txta-hexachlorocyclohexane (a-HCH). Beta-hexachlorocyclohexane (beta-HCH) levels were significantly higher in detoxification subjects than in controls. In the longitudinal evaluation, after treatment, mean levels of PCBs (46%) and beta-HCH (58%) declined significantly in the subjects. CONCLUSIONS: The higher beta-HCH levels in the subjects in the longitudinal study appear to be an anomaly related to diet. The results of the 2 studies generally suggest that lipophil-mediated detoxification may be effective in reducing body burdens of fat-soluble toxicants. As numerous people worldwide are at risk from high body burdens of such lipid-soluble agents, further studies to evaluate this procedure appear warranted.
<28>Unique Identifier 12211327Authors Jacobson E.Institution Department of Social Medicine, Harvard Medical School, Boston, MA 02115, USA.Title Panic attack in a context of comorbid anxiety and depression in a Tibetan refugee.Source Culture, Medicine & Psychiatry. 26(2):259-79, 2002 Jun.
<29>Unique Identifier 12199735Authors Cramer JA. ILAE Subcommission on Outcome Measurement in Epilepsy (Carol Camfield,Hans Carpay, Christopher Helmstaedter, John Langfitt, Kristina Malmgren, and Samuel Wiebe).Institution Department of Psychiatry, Yale University School of Medicine, New Haven, Connecticut 06516-2770, USA. [email protected] Principles of health-related quality of life: assessment in clinical trials. [Review] [7 refs]Source Epilepsia. 43(9):1084-95, 2002 Sep.
<30>Unique Identifier 12196430Authors Keyserling TC. Samuel-Hodge CD. Ammerman AS. Ainsworth BE. Henriquez-Roldan CF. Elasy TA. Skelly AH. Johnston LF. Bangdiwala SI.Institution Department of Medicine, School of Medicine, University of North Carolina at ChapelHill, Chapel Hill, North Carolina 27599, USA. [email protected] A randomized trial of an intervention to improve self-care behaviors of African-American women with type 2 diabetes: impact on physical activity.Source Diabetes Care. 25(9):1576-83, 2002 Sep.Abstract OBJECTIVE: To determine whether a culturally appropriate clinic- and community-based intervention for African-American women with type 2 diabetes will increase moderate-intensity physical activity (PA). RESEARCH DESIGN AND METHODS: In this randomized controlled trial conducted at seven practices in central North Carolina, 200 African-American women, > or =40 years of age with type 2 diabetes, were randomized to one of three treatment conditions: clinic and community (group A), clinic only (group B), or minimal intervention (group C). The clinic-based
Page 14

201-400.txtintervention (groups A and B) consisted of four monthly visits with a nutritionist who provided counseling to enhance PA and dietary intake that was tailored to baseline practices and attitudes; the community-based intervention (group A) consisted of three group sessions and 12 monthly phone calls from a peer counselor and was designed to provide social support and reinforce behavior change goals; and the minimal intervention (group C) consisted of educational pamphlets mailed to participants. The primary study outcome was the comparison of PA levels between groups assessed at 6 and 12 months by accelerometer, which was worn while awake for 7 days. RESULTS: Totals of 175 (88%) and 167 (84%) participants completed PA assessment at 6 and 12 months, respectively. For comparison of PA, the P value for overall group effect was 0.014. Comparing group A with C, the difference in the average adjusted mean for PA was 44.1 kcal/day (95% CI 13.1-75.1, P = 0.0055). Comparing group B with C, the difference in the average adjusted mean was 33.1 kcal/day (95% CI 3.3-62.8, P = 0.029). The intervention was acceptable to participants: 88% were very satisfied with clinic-based counseling to enhance PA, and 86% indicated that the peer counselor's role in the program was important. CONCLUSIONS: The intervention was associated with a modest enhancement of PA and wasacceptable to participants.
<31>Unique Identifier 12188052Authors Birman D. Trickett EJ. Vinokurov A.Institution Department of Psychology, University of Illinois at Chicago, 60607, USA. [email protected] Acculturation and adaptation of Soviet Jewish refugee adolescents: predictors of adjustment across life domains.Source American Journal of Community Psychology. 30(5):585-607, 2002 Oct.Abstract This study explores how acculturation is related to adaptation across different life spheres for 162 Soviet Jewish refugee adolescents in a suburban community in Maryland. Because the different contexts of refugee adolescents' lives vary in acculturative demands, different patterns of acculturation should be related to adaptation in different life spheres. The study uses a multidimensional measure of acculturation and assesses acculturation to both American and Russian cultures as itrelates to psychological adaptation, peer relations, and school and family outcomes.Findings support the general ecological thesis that acculturation to different cultures is differentially related to adaptation across life domains. Acculturation to American culture predicted better grades and perceived support from American peers. Acculturation to Russian culture predicted perceived support from Russian peers. Both American acculturation and Russian acculturation predicted reduced loneliness and perceived support from parents. Further, different dimensions of acculturation, such as language and identity, were differentially related to adaptation. Implications for acculturation theory and measurement are drawn, and cautions are offered about the interpretation of acculturation studies using single proxies such as language use or preference.
<32>Unique Identifier 12185986Authors Altshuler LH. Maher JH.Institution Balanced Healing Medical Center, 2520 NW Expressway, Oklahoma City, OK 73112, [email protected] Acupuncture: a physician's primer, Part I. [Review] [49 refs]
Page 15

201-400.txtSource Journal - Oklahoma State Medical Association. 95(8):527-33, 2002 Aug.Abstract Acupuncture is one of the alternative therapies that is quickly gaining popularityand acceptance among both patients and doctors. The NIH has supported its use for many conditions, alone or as adjunctive therapy to conventional methods. Research has now demonstrated several physiological mechanisms to explain acupuncture's benefits. However, there are many different schools of acupuncture, and methodology and techniques vary widely, all contributing to the success or failure of acupuncture treatment. With proper use, acupuncture can be an effective treatment for a variety of medical conditions, but used incorrectly, it can be a waste of timeand resources. [References: 49]
<33>Unique Identifier 12176508Authors Ciancio G. Burke GW. Suzart K. Roth D. Kupin W. Rosen A. Gomez C. MattiazziA. Esquenazi V. Miller J.Institution Department of Surgery, Division of Transplantation, University of Miami School of Medicine, Highland Professional Building, 5th Floor, 1801 NW 9th Avenue, Suite 517, Miami, FL 33136, USA. [email protected] Effect of daclizumab, tacrolimus and mycophenolate mofetil in racial minority first renal transplant recipients.Source Transplantation Proceedings. 34(5):1617-8, 2002 Aug.
<34>Unique Identifier 12171696Authors Snooks MK. Hall SK.Institution University of Houston-Clear Lake, Houston, Texas 77058-1098, USA. [email protected] Relationship of body size, body image, and self-esteem in African American, European American, and Mexican American middle-class women.Source Health Care for Women International. 23(5):460-6, 2002 Jul-Aug.Abstract In this study we examined the influence of ethnicity on weight, body image, and self-esteem among adult women while controlling for socioeconomic status (SES). Fifty women of African American (AA), European American (EA), and Mexican American (MA) descent completed interviews and questionnaires related to body size and self-esteem, and were measured for weight and height. AA women were significantly heavier than EA women, but MA women did not differ materially from either grouping. Regardless of ethnic descent, all reported congruence between real and ideal body size. In addition no differences were found in self-esteem. This new comparative study calls into question variations previously attributed to race or ethnicity. It also provides a view of middle-class women missing from recent research. Based on the outcomes of our research, we suggest that socioeconomic differences could be more important than ethnic background. Health educators and providers may find thesedata helpful when designing prevention and intervention strategies for middle-class women regardless of their ethnic origin.
<35>Unique Identifier 12171383
Page 16

201-400.txtAuthors Herrman H. Patrick DL. Diehr P. Martin ML. Fleck M. Simon GE. Buesching DP.Institution University of Melbourne and St Vincent's Mental Health Service, VIC, Australia.Title Longitudinal investigation of depression outcomes in primary care in six countries: the LIDO study. Functional status, health service use and treatment of people with depressive symptoms.Source Psychological Medicine. 32(5):889-902, 2002 Jul.Abstract BACKGROUND: Screening surveys of depressive symptoms were conducted among primary care patients at six sites in different countries. The LIDO Study was designed to assess quality of life and economic correlates of depression and its treatment in culturally diverse primary health care settings. This paper describes: (1) the association between depressive symptoms and functional status, global health-relatedquality of life (QoL), and use of general health services across different cultural settings; and (2) among subjects with depressive symptoms, the factors associated with recent treatment for depression. METHODS: Subjects aged 18 to 75 were recruitedfrom participating primary care facilities in Be'er Sheva (Israel), Porto Alegre (Brazil), Melbourne (Australia), Barcelona (Spain), St Petersburg (Russian Federation) and Seattle (USA). Depressive symptoms were measured using the CES-D. Also administered were the SF-12, global questions on QoL, selected demographic and social measures, and questions on recent treatment for depression, use of health care services, and lost workdays. RESULTS: A total of 18,489 patients were screened,of whom 37% overall (range 24-55%) scored > or = 16 on the CES-D and 28% (range 17-42%) scored > or = 20. Overall, 13% reported current treatment for depression (range 4 to 23%). Patients with higher depressive symptom scores had worse health, functional status, QoL, and greater use of health services across all sites. Among those with a CES-D score > or = 16, subjects reporting treatment for depression weremore likely than those reporting no treatment to be dissatisfied with their health (except in St Petersburg), and to have higher depressive symptom scores. CONCLUSIONS: Higher depressive symptom scores in primary care patients were consistently associated with poorer health, functional status and QoL, and increasedhealth care use, but not with demographic variables. The likelihood of treatment fordepression was associated with perceptions of health, as well as severity of the depression.
<36>Unique Identifier 12166020Authors Folkes CE.Institution San Diego State University/Claremont, CA, USA. [email protected] Thought field therapy and trauma recovery.Source International Journal of Emergency Mental Health. 4(2):99-103, 2002 Spring.Abstract People who have been repeatedly exposed to traumatic events are at high risk for Post Traumatic Stress Disorder (PTSD). Refugees and immigrants can certainly be in this category, but seldom seek professional therapy due to cultural, linguistic, financial, and historical reasons. A rapid and culturally sensitive treatment is highly desirable with communities new to Western-style healing. In this study of 31 clients, a pre-test was given, all participants received Thought Field Therapy (TFT), and were then post-tested after 30 days. Pre-test and post-test total scores showed a significant drop in all symptom sub-groupings of the DSM criteria for PTSD.The findings of this study contrast with the outcomes of other methods of treatment,and are a significant addition to the growing body of data on refugee mental health.
Page 17
201-400.txt<37>Unique Identifier 12160805Authors Somaiya MD. Burns JD. Mintz R. Warren RE. Uchida T. Godley BF.Institution Department of Ophthalmology and Visual Sciences, University of Texas Medical Branch, Galveston, TX, USA.Title Factors affecting visual outcomes after small-incision phacoemulsification in diabetic patients.Source Journal of Cataract & Refractive Surgery. 28(8):1364-71, 2002 Aug.Abstract PURPOSE: To examine the factors affecting visual outcome after phacoemulsificationand evaluate the use of preoperative visual potential in assessing the visual prognosis in diabetic patients. SETTING: Department of Ophthalmology, University of Texas Medical Branch, Galveston, Texas, USA. METHODS: In a retrospective chart review of 1345 consecutive patients who had uneventful small-incision phacoemulsification, operated eyes from 106 diabetic and 55 nondiabetic control patients were selected. Data on demographics, level of retinopathy, perioperative glycosylated hemoglobin (HbA(Ic)), surgical duration, preoperative best corrected visual acuity (BCVA), and visual potential were collected. RESULTS: The age, sex, preoperative BCVA, and visual potential in the diabetic and control eyes were comparable. Throughout the postoperative period, BCVA was worse of the diabetic group. At 1 year, BCVA was 20/40 in 82.1% of the diabetic group and 94.7% of the control group (P =.01). The most important factors affecting postoperative BCVA included coexisting diabetes and preoperative level of retinopathy. No correlation was found between perioperative and postoperative BCVA. Diabetic patients were less likely than control patients to achieve a BCVA better than or equal to the preoperative visual potential at 4 years (hazard ratio 0.6; 95% confidence interval,0.4-0.9; P =.011). Patients with nonproliferative diabetic retinopathy were nearly 5times less likely (P =.023) and patients with proliferative diabetic retinopathy 30 times less likely (P <.0001) to achieve a postoperative BCVA of 20/40 than diabetic patients without retinopathy. CONCLUSIONS: Although uneventful small-incision phacoemulsification improved visual acuity in diabetic patients, this group had an overall worse visual outcome than nondiabetic patients. The most important predictors of visual outcome were coexisting diabetes and the extent of preoperativeretinopathy. Methods used to assess preoperative visual potential provided a reasonable estimate of postoperative BCVA in diabetic patients. Given the inverse association between the level of retinopathy and visual outcome, it may be better toperform cataract extraction in diabetic patients during earlier stages of retinopathy.
<38>Unique Identifier 12153121Authors Vinokurov A. Trickett EJ. Birman D.Institution Department of Psychology, University of Maryland, Baltimore County, USA. [email protected] Acculturative hassles and immigrant adolescents: a life-domain assessment for Soviet Jewish refugees.Source Journal of Social Psychology. 142(4):425-45, 2002 Aug.Abstract In a sample of 146 adolescents, the authors developed and validated a measure of acculturative hassles for Soviet Jewish refugees. They based the measure on an ecological perspective, which focuses on hassles involving person-environment transactions occurring in life domains of school, family, peers, and language. The
Page 18

201-400.txtauthors reviewed conceptual and methodological issues in existing instruments and incorporated efforts to address current limitations into instrument development. Themeasure was correlated with psychological distress, level of acculturation to Russian and U.S. cultures, and outcomes in life domains; it contributed to outcomes over and above effects of nonacculturative hassles. Implications for measurement of acculturative hassles are discussed.
<39>Unique Identifier 12146552Authors Kaiser LL. Melgar-Quinonez HR. Lamp CL. Johns MC. Sutherlin JM. Harwood JO.Institution Department of Nutrition, University of California at Davis, 95616, USA. [email protected] Food security and nutritional outcomes of preschool-age Mexican-American children.Source Journal of the American Dietetic Association. 102(7):924-9, 2002 Jul.Abstract OBJECTIVE: To examine the relationship of food insecurity to nutrition of Mexican-American preschoolers. DESIGN: Cross-sectional survey of low-income Mexican-American families with children of preschool age (3 to 6 years). Data included food security using the Radimer/ Cornell scale; acculturation; parental education; monthly income; past experience of food insecurity; and child weight, height, and frequency of consuming 57 foods. Weight-for-height z scores (WHZ), height- for-age z (HAZ) scores, and the percentage of overweight (> or = 85th percentile WHZ) were calculated. SUBJECTS/SETTING: A convenience sample of Mexican-American families (n=211) was recruited through Head Start, Healthy Start, Migrant Education, and the Special Supplemental Nutrition Program for Women, Infants, and Children in Tulare, Fresno, Monterey, and Kern counties in California. Statistical analyses Analysis of variance, t tests, Spearman's correlations, and Mantel Haenszel chi2. RESULTS: Limited education, lack of English proficiency, and low income were negatively correlated with food security (r = -0.31 to -0.44, P<.0001). After controlling for acculturation, children in severely food-insecure households were less likely to meet Food Guide Pyramid guidelines than other children (median number of food groups > or = recommended levels [interquartile range]: 2.0 (2.0) vs 3.0 (2.0), P<.006). Although WHZ (mean +/- SD = 1.28 +/- 1.80) and percent overweight (48%, N=19) tended to peak among children from household level food insecure families, no significant differences were found in weight or height status of children by level of food insecurity. APPLICATIONS/CONCLUSIONS: Dietetics professionals working with low-income Hispanic-American families should screen for different levels of food insecurity to determine needs for nutrition education and other services.
<40>Unique Identifier 12143320Authors Abbott P. Close G.Institution Daruk Aboriginal Community Controlled Medical Service, Mt Druitt.Title Vascular health risks in the Aboriginal community. A cultural approach.Source Australian Family Physician. 31(7):605-10, 2002 Jul.Abstract BACKGROUND: Diabetes, heart disease and other vascular diseases are a great problem in Aboriginal communities and there are many reasons for this. As a health professional it is easy to feel overwhelmed by both the magnitude of the problem andthe feeling that it is just too hard when patients don't seem to take charge of
Page 19

201-400.txttheir own health. OBJECTIVE: This article aims to outline the increased vascular disease and vascular risk factors in the Aboriginal community and explore some of the historical, socio-economic, cultural and genetic reasons for this. The barriers to health care and self management are discussed and some positive developments in the area of Aboriginal vascular health are noted. DISCUSSION: To improve health outcomes we need to focus on two parts of the same problem. First, we need to tacklethe vascular diseases at their roots--the vascular risk factors. Second, we need to look at ways to promote self management so that our patients can identify personal barriers to self care and be partners in their health care. There is evidence that better organised systems of care, such as recall systems and improved screening systems, are very beneficial. The most successful interventions are culturally appropriate and developed and implemented with Aboriginal community control.
<41>Unique Identifier 12137289Authors Chakraborty BM.Institution Department of Environmental Health, University of Cincinnati, OH 45267, USA.Title Formulation and validation of a composite migration history score for epidemiological research in Mexican American women.Source Collegium Antropologicum. 26(1):1-9, 2002 Jun.Abstract This research developed a composite migration history score, using data on birth places of subjects, and their parents and grand parents, and the length of residencein US from 390 overweight Mexican American women. The derived migration history score is validated through a factor analysis of the nine dimensional migration history variables. The importance of this methodology of defining migration history score for epidemiological research is discussed in the context of studying the role of migration-related health behavior changes and their consequent impact on risks ofuntoward health outcomes in migrants.
<42>Unique Identifier 12125087Authors Pransky G. Moshenberg D. Benjamin K. Portillo S. Thackrey JL. Hill-Fotouhi C.Institution Liberty Mutual Center for Disability Research, 71 Frankland Road, Hopkinton, Massachusetts 01701, USA. [email protected] Occupational risks and injuries in non-agricultural immigrant Latino workers.Source American Journal of Industrial Medicine. 42(2):117-23, 2002 Aug.Abstract BACKGROUND: To investigate occupational health in urban immigrant Latino workers, using a community-based method. METHODS: A survey was administered through consecutively selected door-to-door interviews. RESULTS: Response rate was 80% (n = 427). Average time in the US was 7.6 years, and average job tenure was 2.8 years. Twenty-five reported exposures to over 10 different hazards, and 18% thought these hazards had harmed their health. Only 31% received any job safety training; 55% had no workers' compensation coverage. Of the 47 (11%) with a work injury in the past 3 years, 27% reported difficulty obtaining treatment, 91% lost time from work (median = 13 days) and 29% had to change jobs because of the injury. The annual occupationalinjury rate was 12.2/100 full-time workers, compared to an expected rate of 7.1. CONCLUSIONS: Urban immigrant workers have increased risk of occupational injuries, with adverse outcomes. Copyright 2002 Wiley-Liss, Inc.
Page 20
201-400.txt
<43>Unique Identifier 12121270Authors Gray B.Institution South Bank University, London, UK. [email protected] Working with families in Tower Hamlets: an evaluation of the Family Welfare Association's Family Support Services.Source Health & Social Care in the Community. 10(2):112-22, 2002 Mar.Abstract This paper describes an evaluation carried out by South Bank University of the work of the Family Welfare Association's (FWA's) Family Support Services (FSSs) in Tower Hamlets, London. Tower Hamlets is a multi-racial area in east London that, according to the 1991 census, has high levels of poverty, overcrowding and unemployment. Increasing poverty and social exclusion, which further entrench inequalities in health, are reported by sources such as government, health and social services and research as requiring innovative local responses to meet pressing welfare needs. The evaluation reported here examined three projects: FamilySupport, Building Bridges and Quality Protects - these are referred to collectively as FSSs. The evaluation shows that FSSs are innovative services that demonstrate effective ways of working with vulnerable families affected by experiences of racism, bullying, mental health difficulties, domestic violence or child abuse. In common with other successful initiatives in the UK and abroad, FSSs are aimed to be non-stigmatising, non-intrusive and responsive to the ethnicity, views and specific needs of families. This paper focuses on the participatory work of FSSs with families to illustrate effective methods of quality support, detail outcomes, and draw lessons for policy and practice.
<44>Unique Identifier 12110074Authors Iwashyna TJ. Chang VW.Institution School of Medicine, Harris Graduate School of Public Policy Studies, Center on Aging and Population Research Center, University of Chicago, Chicago, Illinois, [email protected] Racial and ethnic differences in place of death: United States, 1993.Source Journal of the American Geriatrics Society. 50(6):1113-7, 2002 Jun.Abstract OBJECTIVES: To examine racial and ethnic differences in place of death, adjusting for likely confounders. DESIGN: A retrospective cohort analyzed using multinomial logistic regression. SETTING: United States in 1993. PARTICIPANTS: A nationally representative sample of 22,658 deaths in 1993 from the National Mortality Followback Survey. MEASUREMENTS: Place of death as determined on the death certificate, with controls for age, sex, income, education, and cause of death. The outcomes of interest were death in a hospital during an inpatient stay, death in a nursing home, death in a private residence, or death in some other place. RESULTS: After adjustment, 43% of whites die after an inpatient hospital stay, as do 50% of blacks and 56% of Mexican Americans. Twenty percent of whites, 22% of Mexican Americans, and 14% of blacks die in nursing homes. Twenty-two percent of whites, 18%of blacks, and 9% of Mexicans die in a private residence. CONCLUSIONS: There are substantial differences between whites, blacks, and Mexican Americans in place of death that cannot be explained by differences in age, sex, income, education, and causes of death between the groups.
Page 21

201-400.txt
<45>Unique Identifier 12112490Authors Bastida E. Pagan JA.Institution Department of Sociology and Center on Aging and Health, College of Social and Behavioral Sciences, The University of Texas-Pan American, Edinburg 78539, USA.Title The impact of diabetes on adult employment and earnings of Mexican Americans: findings from a community based study.Source Health Economics. 11(5):403-13, 2002 Jul.Abstract Epidemiological studies indicate that minority populations in the US - including African Americans, Native Americans and Mexican Americans - are particularly at riskfor diabetes and that their complications are more frequent and severe. Using microdata from a 1994-1999 population based study of middle aged and older Mexican Americans in the Southwest, this study analyzes the impact of diabetes on the employment and earnings outcomes of adults 45 years of age and older. The empirical results from estimating maximum likelihood employment and earnings models suggest that diabetes leads to lower productivity and earnings for women but has no statistically significant impact on their employment probability. In the case of men, however, diabetes leads to a lower employment propensity but has no effect on earnings. Thus, the problems associated with this condition could lead to potential future financial difficulties particularly for high-risk populations in their later years. Copyright 2002 John Wiley & Sons, Ltd.
<46>Unique Identifier 12110113Authors Sakai F. Iwata M. Tashiro K. Itoyama Y. Tsuji S. Fukuuchi Y. Sobue G. Nakashima K. Morimatsu M.Institution Department of Neurology, Kitasato University, Kitasato 1-15-1, Sagamihara-Shi, Kanagawa, Japan. [email protected] Zolmitriptan is effective and well tolerated in Japanese patients with migraine: adose-response study.Source Cephalalgia. 22(5):376-83, 2002 Jun.Abstract This phase II study investigated the efficacy, tolerability and dose-response relationship of oral zolmitriptan in the treatment of a single migraine attack in Japanese patients. A bridging analysis then assessed the validity of extrapolating western clinical data to these Japanese patients. In this multicentre, randomized, double-blind, placebo-controlled study, patients received a single dose of placebo or zolmitriptan 1, 2.5 or 5 mg. The primary endpoints were 2-h headache response andthe tolerability of zolmitriptan. A statistically significant dose-response relationship was observed for the 2-h headache response (P=0.003). The 2.5 mg group had significantly greater 2-h headache response than the placebo group (P=0.032). The adverse event profile was similar to that reported in western patients, and no adverse events unique to the Japanese population were observed. The bridging analysis report confirmed similar efficacy and tolerability of zolmitriptan in Japanese and western populations. In the Japanese patients, the estimated response rates were 34.3%, 45.2%, 57.7% and 66.2% for placebo, and zolmitriptan 1, 2.5 and 5 mg, respectively, while in the western population the corresponding rates were 39.9%, 49.6%, 61.2% and 71.7%. Zolmitriptan is effective and well tolerated in the acute treatment of migraine in Japanese patients. The optimal dose was 2.5 mg, although the 5 mg dose may provide further benefit for some patients. The bridging
Page 22

201-400.txtanalysis supports extrapolation of data from western to Japanese patients.
<47>Unique Identifier 12096165Authors Mathews CA. Glidden D. Murray S. Forster P. Hargreaves WA.Institution Department of Psychiatry at the University of California, San Diego, 9500 Gilman Drive, 0810 La Jolla, California 92093-0810, USA. [email protected] The effect on treatment outcomes of assigning patients to ethnically focused inpatient psychiatric units.Source Psychiatric Services. 53(7):830-5, 2002 Jul.Abstract OBJECTIVE: The authors examined whether assigning patients from three ethnic groups-blacks, Latinos, and Asians-to three ethnically focused psychiatric inpatientunits would affect treatment outcome. METHODS: Retrospective administrative data for5,983 inpatients at a large urban community hospital with several ethnically focusedunits were examined. The data represented 10,645 admissions between 1989 and 1996. Cox proportional-hazards models, logistic and multinomial regressions, and chi square analyses were used to assess the relationship between matching patients to ethnically focused units and time to rehospitalization, referral destination on discharge, and length of stay for Asian, black, and Latino patients. RESULTS: Ethnicmatching status was strongly associated with referral destination for Asian and Latino patients but not for black patients. Asian and Latino patients who had been treated on the appropriate ethnically focused units were more frequently sent to outpatient or residential treatment (71 to 73 percent of discharges) than unmatched patients, black patients, and white patients (44 to 49 percent of discharges), who more frequently refused follow-up or were sent to locked facilities. No association was found between matching status and time to rehospitalization or length of stay for any ethnic group. CONCLUSIONS: Matching inpatients to ethnically focused psychiatric units was related to referral destination at discharge. Matched patientswere more likely than unmatched patients to accept referral to postdischarge treatment, which has been shown previously to reduce readmission rates. Among persons with serious mental illness, matching patients to ethnically focused units may be important for enhancing communication and trust as a means of improving participation in ongoing treatment programs.
<48>Unique Identifier 12090966Authors Romo LF. Lefkowitz ES. Sigman M. Au TK.Institution Departments of Child and Adolescent Development and Chicano Studies, California State University, Northridge, California, USA. [email protected] A longitudinal study of maternal messages about dating and sexuality and their influence on Latino adolescents.Source Journal of Adolescent Health. 31(1):59-69, 2002 Jul.Abstract PURPOSE: To learn more about the nature of mother-adolescent discussions about sexuality and their influence on adolescents' behaviors and attitudes in Latino families. METHODS: Fifty-five Latino mothers and their midadolescent children (35 girls, 20 boys, mean age 13 years) were observed talking about dating and sexuality.The videotaped conversations were coded for the prevalence of five maternal message types: beliefs and values, advice, cautionary messages, comments about the adolescents' everyday experiences, and maternal self-disclosure about her own dating
Page 23

201-400.txtand sexuality experiences. A structural equation model was used to examined how timespent on the various message types was related to three adolescent-related outcomes collected about 1 year later: sexual behavior, attitudes toward premarital sex, and reports of openness in the mother-child relationship. RESULTS: Latino mothers focused the conversation on their personal beliefs and values about dating and sexuality. Discussions about beliefs and values were accompanied by more parental advice and cautionary messages. More maternal self-disclosure about personal dating and sexuality experiences was related to the adolescents' reporting a better functioning relationship with their mothers and having more conservative attitudes toward premarital sex. Sexuality communication was both positively and negatively related to adolescent sexual behavior, but the messages were not the same. CONCLUSIONS: Maternal communication in Latino families influences adolescents' behaviors and attitudes toward sex and adolescents' perceptions of openness in the mother-child relationship. Observational methods are useful for studying the complexity of the communication process and for studying participants from ethnic minority populations who may be unfamiliar with or uncomfortable filling out questionnaires.
<49>Unique Identifier 12090837Authors Mazor SS. Hampers LC. Chande VT. Krug SE.Institution Division of Emergency Medicine, Department of Pediatrics, Children's Memorial Hospital, 2300 Children's Plaza, Box 62, Chicago, IL 60614, USA. [email protected] Teaching Spanish to pediatric emergency physicians: effects on patient satisfaction.[see comment].Source Archives of Pediatrics & Adolescent Medicine. 156(7):693-5, 2002 Jul.Abstract BACKGROUND: Language barriers are known to negatively affect patient satisfaction.OBJECTIVE: To determine whether a course of instruction in medical Spanish for pediatric emergency department (ED) physicians is associated with an increase in satisfaction for Spanish-speaking-only families. DESIGN, SETTING, PARTICIPANTS, AND INTERVENTION: Nine pediatric ED physicians completed a 10-week medical Spanish course. Mock clinical scenarios and testing were used to establish an improvement ineach physician's ability to communicate with Spanish-speaking-only families. Before (preintervention period) and after (postintervention period) the course, Spanish-speaking-only families cared for by these physicians completed satisfaction questionnaires. Professional interpreters were equally available during both the preintervention and postintervention periods. MAIN OUTCOME MEASURES: Responses to patient family satisfaction questionnaires. RESULTS: A total of 143 Spanish-speaking-only families completed satisfaction questionnaires. Preintervention (n = 85) and postintervention (n = 58) cohorts did not differ significantly in age, vital signs, length of ED visit, discharge diagnosis, or self-reported English proficiency. Physicians used a professional interpreter less often in the postintervention period (odds ratio [OR], 0.34; 95% confidence interval[CI], 0.16-0.71). Postintervention families were significantly more likely to strongly agree that "the physician was concerned about my child" (OR, 2.1; 95% CI, 1.0-4.2), "made me feel comfortable" (OR, 2.6; 95% CI, 1.1-4.4), "was respectful" (OR, 3.0; 95% CI, 1.4-6.5), and "listened to what I said" (OR, 2.9; 95% CI, 1.4-5.9). CONCLUSIONS: A 10-week medical Spanish course for pediatric ED physicians was associated with decreased interpreter use and increased family satisfaction.
<50>Unique Identifier 12083174Authors
Page 24

201-400.txt Dreachslin JL. Sprainer E. Jimpson G.Institution Penn State Great Valley School of Graduate Professional Studies, Malvern, USA.Title Communication: bridging the racial and ethnic divide in health care management.Source Health Care Manager. 20(4):10-8, 2002 Jun.Abstract The emerging body of literature on racial and ethnic diversity in health services management reveals four pervasive and formidable challenges for health care industryleadership. These are: under-representation of people of color in health services management, persistent gaps in both compensation and satisfaction between managers of color and white managers, and racial and ethnic disparities in medical care process and outcomes. Focus groups of health care managers were assembled to explorethe intersection of race, ethnicity, and health care management. Results of the focus group discussions support the need for meaningful dialogue that aims to identify common ground and shared purpose so that appropriate actioncan be taken to bridge the racial and ethnic divide.
<51>Unique Identifier 12080463Authors Dijkers MP. Yavuzer G. Ergin S. Weitzenkamp D. Whiteneck GG.Institution Department of Rehabilitation Medicine, Mount Sinai School of Medicine, New York, NY 10029-6574, USA.Title A tale of two countries: environmental impacts on social participation after spinal cord injury.Source Spinal Cord. 40(7):351-62, 2002 Jul.Abstract STUDY DESIGN: Comparative analysis of survey data produced in two countries. OBJECTIVES: To assess the degree to which environmental barriers impact social participation, and to identify the aspects of participation most affected. SETTING: Community-dwelling individuals with spinal cord injury in the USA and Turkey. METHODS: Subjects completed the Functional Independence Measure (FIM) motor score, the Craig Hospital Inventory of Environmental Factors (CHIEF), and the Craig Handicap Assessment and Reporting Technique (CHART). Analysis of co-variance was used to analyze CHIEF and CHART differences within and between country. RESULTS: US subjects reported higher participation scores (CHART) and lower barriers (CHIEF), however, when controls for age, gender, time since injury and motor ability (FIM) were applied, country differences in reports of barriers were limited. Motor abilitywas the major predictor of participation, which was minimally affected by barriers. CONCLUSION: Conceptualization and measurement issues may have been the reason for the minimal support for the hypothesis that environment affects participation. Suggestions for future research are made. SPONSORSHIP: National Institute on Disability and Rehabilitation Research, Centers for Disease Control and Prevention.
<52>Unique Identifier 12075386Authors Toursarkissian B. Jones WT. D'Ayala MD. Shireman PK. Harrison A. Schoolfield J. Sykes MT.Institution Section of Vascular Surgery, University of Texas Health Science Center at San Antonio, TX 78229-3900, USA. [email protected] Does the efficacy of dorsalis pedis artery bypasses vary among diabetic patients
Page 25

201-400.txtof different ethnic backgrounds?.Source Vascular & Endovascular Surgery. 36(3):207-12, 2002 May-Jun.Abstract Hispanic patients suffer from a high rate of leg amputations, far beyond what would be expected from the high prevalence of diabetes in this population. This raises questions about the efficacy of bypass operations across ethnic lines. We focused this review on dorsalis pedis bypasses, as these are frequently performed indiabetic patients. We compared outcomes between Hispanics and non-Hispanics and sought to identify factors predictive of failure or complications. The authors conducted a retrospective review of 144 dorsalis pedis bypasses in 106 men and 29 women with a mean age of 62 years. Eighty-two percent were Hispanic; 96% of cases were done for tissue loss, and 4% for rest pain. Twenty-five percent of patients experienced perioperative complications; these were more frequent in non-Hispanics than Hispanics (40% vs 22%, p = 0.05). The most frequent complications were wound related (11%). The 30-day mortality was 1.5% and 30-day graft thrombosis was 5%. Follow-up ranged from 1 to 62 months and averaged 12 months. Eighty-one percent of the limbs at risk were saved, although 36% of cases required minor foot amputations.Estimated primary graft patency was 68% at 30 months. The 30-month Kaplan-Meier curves for primary patency, assisted patency, and limb salvage were not statistically different between Hispanics and non-Hispanics (p > 0.4). Grafts that remained patent had higher duplex-derived intraoperative flow velocities in the dorsalis pedis artery than grafts that eventually failed (121 +/-69 vs 74 +/-26 cm/sec, p = 0.02). In grafts that remained patent, dorsalis pedis velocity decreasedfrom the perioperative period to the 8 to 12 weeks time point, whereas no change wasseen in grafts that eventually failed (mean decline of 48 +/-76 vs 1 +/-58 cm/sec, p= 0.02). No other factors were predictive of graft failure. The results of dorsalis pedis bypass in Hispanic patients compare favorably to those seen in other ethnic groups. This suggests that other factors must account for the high amputation rates seen in Hispanics, such as a frequent occurrence of nonreconstructible disease or unaccounted for cardiovascular risk factors. The usefulness of duplex-derived flow velocities in the dorsalis pedis to predict long-term graft patency warrants furtherinvestigation.
<53>Unique Identifier 12073874Authors Jongbloed L. Wendland T.Institution School of Rehabilitation Sciences, UBC, T325-2211 Wesbrook Mall, Vancouver, V6T 1B5. [email protected] The impact of reimbursement systems on occupational therapy practice in Canada andthe United States of America. [Review] [44 refs]Source Canadian Journal of Occupational Therapy - Revue Canadienne d Ergotherapie. 69(3):143-52, 2002 Jun.Abstract Different funding and cost-control mechanisms in Canada and the United States of America (USA) have a powerful influence on occupational therapy practice in each country. Canada's public health insurance system emphasizes access to health care services based on medical need. Costs are controlled at the provincial government level by limiting the capacity of facilities and personnel. Occupational therapists in publicly-funded settings have considerable professional autonomy to use occupational therapy theoretical models and to be client-centred. The measurement ofoutcomes is not always required and the interventions of individual occupational therapists are infrequently scrutinized. The USA has no universal, publicly-funded, comprehensive health insurance. Health care policies are driven by financial priorities and cost control occurs at the service delivery level. Insurance companies define the scope of occupational therapy practice by identifying what services they will pay for and they scrutinize occupational therapy interventions.
Page 26

201-400.txtThe emphasis on effectiveness and efficiency leads to critical examination of interventions by therapists. Canadian occupational therapists can learn much from their colleagues in the USA in this area. [References: 44]
<54>Unique Identifier 12072326Authors Mejia A. Halff GA. Esterl R. Cigarroa F. Speeg KV. Villarreal R. Washburn K.Institution Department of Surgery, Division of Transplantation, The University of Texas HealthScience Center at San Antonio, San Antonio, Texas 78229, USA.Title Outcome of liver transplantation in Hispanics versus non-Hispanics: is there a difference?.Source Transplantation Proceedings. 34(4):1236-8, 2002 Jun.
<55>Unique Identifier 12069220Authors Zumo LA. Terzian C. Brannan T.Institution JFK Neuroscience Institute, JFK Medical Center, Edison, New Jersey, USA.Title Thyrotoxic hypokalemic periodic paralysis in a Hispanic male.Source Journal of the National Medical Association. 94(5):383-6, 2002 May.Abstract We report a case of a Hispanic male presenting with acute onset of bilateral lowerextremity weakness, without any antecedent viral or bacterial illness, dietary changes, infiltrative orbitopathy, diffuse goiter, infiltrative dermopathy, and family history of periodic paralysis, who was later found to have Graves' disease. This demonstrates a rare case of periodic paralysis as the initial presentation of hyperthyroidism. Thyrotoxic hypokalemic periodic paralysis is common in Asian and Hispanic individuals and uncommon in whites and African Americans.
<56>Unique Identifier 12069218Authors Carter JH.Institution Department of Psychiatry, Duke University Medical Center, Durham, North Carolina 27710, USA.Title Religion/spirituality in African-American culture: an essential aspect of psychiatric care.Source Journal of the National Medical Association. 94(5):371-5, 2002 May.Abstract There is an astonishing diversity of religious beliefs and practices in the history of African Americans that influences the presentation, diagnosis, and management of both physical and mental disorders. The majority of African Americans,however, are evangelical Christians with religious experiences originating in the regions of ancient Africa (Cush, Punt, and to a great extent, Egypt), as well as black adaptation of Hebraic, Jewish, Christian, and Islamic beliefs and rituals. Consequently, more than 60 of the nation's 125 medical schools offer classes in spirituality and health. Although there is a lack of empirical evidence that
Page 27

201-400.txtreligion improves health outcomes, physicians should understand patients as a biopsychosocial-spiritual whole. Asking about religion/spirituality during a health assessment can help the physician determine whether religious/spiritual factors willinfluence the patient's medical decisions and compliance. Two psychiatric case histories of African Americans are presented in which religion/spirituality significantly influenced treatment decisions and results. Neither of these patients suffered major debilitating medical comorbidity.
<57>Unique Identifier 12063418Authors Baumann LC. Chang MW. Hoebeke R.Institution Academic Nursing Practice, University of Wisconsin-Madison School of Nursing, 53792-2455, USA. [email protected] Clinical outcomes for low-income adults with hypertension and diabetes.Source Nursing Research. 51(3):191-8, 2002 May-Jun.Abstract BACKGROUND: Long-term management of hypertension and diabetes, which are more prevalent in minority and socioeconomically disadvantaged populations, presents challenges for healthcare providers in community health centers. OBJECTIVES: The purpose of the study was twofold: to examine health outcomes for persons with hypertension and diabetes and to compare these outcomes for disparities in patients who were Black, Hispanic, or White. METHODS: Medical records (N = 280) from an urbancommunity health center that serves predominantly uninsured adults were reviewed forselected clinical outcomes of primary care. Measures included outcomes of hypertension and diabetes control, lifestyle behaviors, preventive care, and patientstatus. Chi-square tests, t tests, and one-way analysis of covariance were used to analyze racial/ethnic group differences. RESULTS: Data revealed significant differences in smoking status, influenza immunization, and blood pressure. Racial/ethnic group differences were minimal compared with the overall high prevalence of risk factors such as smoking and obesity. Regular access to primary care did not result in improved clinical outcomes. CONCLUSION: The findings support the need for more effective interventions that promote healthy lifestyle if health disparities in low-income populations with chronic conditions are to be reduced.
<58>Unique Identifier 12059999Authors Heaney DC. Beran RG. Halpern MT.Institution Institute of Psychiatry at the Maudsley, King's College London, Denmark Hill, England. [email protected] Economics in epilepsy treatment choices: our certain fate?. [Review] [44 refs]Source Epilepsia. 43 Suppl 4:32-8, 2002.
<59>Unique Identifier 12058155Authors Phillips J. Weekes D.Institution National Institutes of Nursing Research, Bethesda, MD, USA. [email protected]
Page 28
201-400.txtTitle Incorporating multiculturalism into oncology nursing research: the last decade. [Review] [31 refs]Source Oncology Nursing Forum. Online. 29(5):807-16, 2002 Jun.Abstract PURPOSE/OBJECTIVES: To use the Oncology Nursing Society's cultural competence guidelines to review research studies conducted by oncology nurse researchers with racial and ethnic minorities and published in the Oncology Nursing Forum during 1990-2000. DATA SOURCES: Using selected key words (e.g., cultural competence, cultural diversity, multiculturalism, minorities, African American/Black American, Hispanic/Latino, Asian/Pacific Islander, Native American/Alaskan Natives) the authors identified 27 studies that met the inclusion criteria for review. Case studies, sponsored lectureships, review articles, commentaries, editorials, and the like were excluded. DATA SYNTHESIS: Within the context of the cultural competence guidelines, the primary strengths included sufficient background information and literature to establish the existence of the problem in the targeted culture, use ofconceptual and theoretical frameworks to guide the study, identification of salient study limitations, and recommendations for dissemination of the findings to a general audience. Limitations included discussion of culture beyond the background and literature review, consideration of potential ethical concerns the target population may have about the methods to be used, inclusion of racial and ethnic minorities in the design and implementation of the study, and implications for oncology nursing education. CONCLUSIONS: Although much has been gleaned from previous oncology nursing research published from 1990-2000, more fully incorporatedcontent related to cultural competence is needed. This is needed particularly in studies specifically targeting racial and ethnic minority populations. IMPLICATIONS FOR NURSING: Including cultural competence when designing and reporting research hasa greater potential to inform oncology nursing practice, design future research studies, strengthen existing nursing curricula, and help to shape health policy related to racial and ethnic minority populations. The Oncology Nursing Society Multicultural Outcomes: Guidelines for Cultural Competence provides guidance for enhancing the next generation of oncology nursing research with ethnically and culturally diverse populations. [References: 31]
<60>Unique Identifier 12058154Authors Aziz NM. Rowland JH.Institution National Cancer Institute, National Institutes of Health, U.S. Department of Health and Human Services, Bethesda, MD, USA. [email protected] Cancer survivorship research among ethnic minority and medically underserved groups. [Review] [92 refs]Source Oncology Nursing Forum. Online. 29(5):789-801, 2002 Jun.Abstract PURPOSE/OBJECTIVES: To review the current state of knowledge about the impact of cancer on ethnoculturally diverse and medically underserved survivors. DATA SOURCES:MEDLINE, CancerLit, and Psychlit searches from 1966-present were conducted to locatearticles about survivorship outcomes among minority and underserved populations. DATA SYNTHESIS: 65 articles were identified and grouped into one of four content areas: physiologic; psychosocial; health services, patterns of care, and quality of care; and health-promoting behaviors and lifestyles. CONCLUSIONS: Despite limited information, researchers found a consistent theme: the need to recognize and addressthe socioeconomic and cultural variables that affect adaptation to and survival fromcancer among diverse groups of survivors. IMPLICATIONS FOR NURSING: The researchers found specific variations in risk for, response to, and recovery from cancer that provide direction for changes in nursing practice that may reduce the burden of cancer in these often vulnerable populations. [References: 92]
Page 29
201-400.txt
<61>Unique Identifier 12057880Authors Larkey LK. Staten LK. Ritenbaugh C. Hall RA. Buller DB. Bassford T. AltimariBR.Institution Women's Cancer Prevention Office, Arizona Cancer Center, University of Arizona, Phoenix, AZ 85006, USA. [email protected] Recruitment of Hispanic women to the Women's Health Initiative. the case of Embajadoras in Arizona.Source Controlled Clinical Trials. 23(3):289-98, 2002 Jun.Abstract This study examined the use of lay advocates (i.e., women enrolled in a study who advocate to others) to improve recruitment among Hispanic women in the Arizona recruitment sites for a large-scale, national prevention study, the Women's Health Initiative (WHI). We examined whether trained, Hispanic lay advocates (called Embajadoras) brought more women into the study than a matched group of Hispanic and Anglo enrollees in the WHI who were supplied with brochures. Fifty-six Hispanic participants in the WHI were randomized to receive training or no training on advocacy, and continued to meet quarterly for 18 months. Also, 42 Anglo women were assigned to control. All groups received brochures to use for advocating the WHI. The number of women referred and enrolled was tracked as well as other factors expected to influence outcomes. Embajadoras were more successful at referral and enrollment than untrained Hispanic women and more successful at enrollment than untrained Anglo controls. Embajadoras were also found to distribute significantly more brochures than control groups. Therefore, a culturally aligned training programto encourage current Hispanic participants in a clinical trial to advocate the studyto others may be an effective way to boost referrals and enrollments. Other potential influences on enrollment or referral success could not be determined due to the small sample size. Further study is needed to examine the best methods to encourage enrollment for women referred to the study.
<62>Unique Identifier 12042396Authors Seibert PS. Stridh-Igo P. Zimmerman CG.Institution Idaho Neurological Institute at Saint Alphonsus Regional Medical Center, Boise, Idaho 83706, USA. [email protected] A checklist to facilitate cultural awareness and sensitivity.Source Journal of Medical Ethics. 28(3):143-6, 2002 Jun.Abstract United States of America demographic profiles illustrate a nation rich in culturaland racial diversity. Approximately 29% of the population are minorities and demographic projections indicate an increase to 50% by the year 2050. This creates ahighly mobile and constantly changing environment, revealing the need for new levelsof cultural awareness and sensitivity. These issues are particularly critical in themedical community where medical professionals must understand the impact cultural differences and barriers can have on evaluation, treatment, and rehabilitation. During times of stress, such as when injury strikes, problems associated with lack of cultural sensitivity are intensified. Cultural diversity is of particular concernwhen standard measures for diagnosis and prognosis are derived from established norms for responding, because culture defines norms. This paper details a ten point checklist designed to facilitate cultural awareness and sensitivity in medical
Page 30

201-400.txtsettings to ensure maximum successful recovery and outcomes for all patients.
<63>Unique Identifier 12033539Authors Walker LO. Kim M.Institution School of Nursing, The University of Texas at Austin 78701-1499, USA. [email protected] Psychosocial thriving during late pregnancy: relationship to ethnicity, gestational weight gain, and birth weight.Source JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing. 31(3):263-74, 2002May-Jun.Abstract OBJECTIVE: To test the relationships between psychosocial thriving (depressive symptoms, health-related lifestyle) and gestational weight gain and birth weight. Totest the influences of ethnicity on the relationships between psychosocial thriving and gestational weight gain and birth weight. DESIGN: Baseline data taken from the Austin New Mothers Study. SETTING: A community hospital in Texas. PARTICIPANTS: 305 low-risk African American, Hispanic, and White women with full-term pregnancies, singleton births, and Medicaid coverage. MAIN MEASURES: Center for Epidemiologic Studies Depression Scale, Self Care Inventory, Food Habits Questionnaire, gestational weight gain, and birth weight. RESULTS: Newborns of African American women had lower birth weights (3,240 g) than newborns of Hispanic (3,422 g) or Whitewomen (3,472 g), even though no ethnic differences were found among the mothers on psychosocial variables. Late in pregnancy, women had high levels and prevalence (> 70%) of depressive symptoms regardless of ethnicity, and 50% exceeded recommended gestational weight gains. In full regression models, psychosocial variables were notsignificant predictors of gestational weight gain or birth weight. Ethnicity also was not a significant moderator of weight outcomes. CONCLUSIONS: Psychosocial thriving late in pregnancy was unrelated to gestational weight gain or birth weight.Ethnicity did not moderate psychosocial-weight relationships. Although ethnic differences were not found on psychosocial variables, high levels of depressive symptoms and greater than recommended gestational weight gains were prevalent. Thesefindings have implications for maternal health during and beyond pregnancy.
<64>Unique Identifier 12019990Authors Timmins CL.Institution Yale University, USA.Title The impact of language barriers on the health care of Latinos in the United States: a review of the literature and guidelines for practice. [Review] [68 refs]Source Journal of Midwifery & Women's Health. 47(2):80-96, 2002 Mar-Apr.Abstract Although Spanish was the primary language of an estimated 11 % of adults in the year 2000, the U.S. health care system is largely geared toward serving English speakers. A systematic review was conducted of studies published in biomedical journals from 1990 to 2000 examining language barriers in health care for Latino populations. Aspects of the problem examined were access to health care, quality of care, and health status/health outcomes. Five (55%) of the nine studies examining access to care found a significant adverse effect of language; three (33%) found mixed or weak evidence that language affected access. Six (86%) of the seven studiesevaluating quality of care found a significant detrimental effect of language
Page 31

201-400.txtbarriers. Two of the three studies examining health status or outcomes found language to be a risk factor for adverse outcomes. Evidence was mixed as to the level of importance attributable to language when access to care is considered; however, non-English-speaking status was a marker of a population at risk for decreased access. Solid evidence showed that language barriers can adversely affect quality of care. Health care practitioners are recommended to devise an effective strategy to bridge language barriers in their setting. National laws and policies are discussed; practical guidelines and resources for providing language access in health care are provided. This article is intended to supply basic knowledge for providers and institutions in devising effective strategies for bridging the language barrier. [References: 68]
<65>Unique Identifier 12015506Authors Barton CB. Barton JR. O'Brien JM. Bergauer NK. Sibai BM.Institution Department of Obstetrics and Gynecology, University of Kentucky Medical Center, Lexington, USA.Title Mild gestational hypertension: differences in ethnicity are associated with altered outcomes in women who undergo outpatient treatment.Source American Journal of Obstetrics & Gynecology. 186(5):896-8, 2002 May.Abstract OBJECTIVE: The purpose of this study was to evaluate the impact of ethnicity on outcome in women with mild gestational hypertension that is remote from term. STUDY DESIGN: Nulliparous women with mild gestational hypertension who participated in an outpatient monitoring program between January 1995 and December 1999 were candidates. Patients had a singleton pregnancy at <37 weeks of gestation and were followed up for a minimum of 2 days as an outpatient. Maternal and perinatal outcomes were compared between groups by the Student t test, Mann-Whitney U test, and Pearson chi2 analyses. RESULTS: One thousand one hundred eight-two women were included in the analysis. No clinically remarkable differences in gestational age orincidence of proteinuria at the start of observation were noted. Newborn infants of Hispanic and African American women had significantly smaller birth weights comparedwith those of white women. African American women had a higher incidence of abruptioplacentae (n = 5), stillbirths (n = 3), and neonatal deaths (n = 2) versus the othergroups (n = 0 for all). The frequency of progression to thrombocytopenia/HELLP (hemolysis, elevated liver enzymes, and low platelet count syndrome) and cesarean delivery rates were similar between groups. CONCLUSION: Differences in outcomes are observed between ethnic groups even when the women undergo the same intensive outpatient monitoring for mild gestational hypertension.
<66>Unique Identifier 12011612Authors Ortega AN. Rosenheck R.Institution Yale University School of Medicine, Department of Epidemiology and Public Health, Division of Health Policy and Administration, 60 College Street, P. O. Box 208034, New Haven, Connecticut 06520-8034, USA.Title Hispanic client-case manager matching: differences in outcomes and service use in a program for homeless persons with severe mental illness.Source Journal of Nervous & Mental Disease. 190(5):315-23, 2002 May.Abstract Mental health professionals have responded to ethnic and racial disparities in
Page 32

201-400.txtmental health care by advocating increasing cultural relevancy in treatment. A central component of cultural relevancy is ethnic and racial pairing of clients and providers. This study examined the effects of client-case manager ethnic and racial matching among white and Hispanic clients who received assertive community treatmentin the Access to Community Care and Effective Services and Supports Program. Twelve-month outcomes and service use were examined among 242 Hispanic and 2333 white clients seen in the first 3 years of the program. Analysis of covariance was used to evaluate the association of client-case manager ethnic and racial matching with changes in health status and service use from baseline to 12 months after program entry. At baseline, Hispanics had more serious problems than whites on several measures of psychiatric and substance abuse domains, and they also showed less improvement than whites over the next year on several measures of psychiatric status and service use. One significant association with ethnic matching was found: when treated by a Hispanic clinician, Hispanic clients showed less improvement in symptoms of psychosis. These results do not support the hypothesis that ethnic and racial matching improves outcomes or service use. Several explanations are offered for the results.
<67>Unique Identifier 12003468Authors Licciardone JC. Brittain PD. Coleridge ST.Institution Department of family medicine at the University of North Texas Health Science Center at Fort Worth--Texas College of Osteopathic Medicine, 76107-2644, USA. [email protected] Health status and satisfaction of patients receiving ambulatory care at osteopathic training clinics.Source Journal of the American Osteopathic Association. 102(4):219-23, 2002 Apr.Abstract Little is known about the health status and level of satisfaction of patients receiving care at osteopathic training clinics. Previous studies report favorable responses to medical student participation in ambulatory clinics. The health status and level of satisfaction for 2700 patients attending six family medicine training clinics at a college of osteopathic medicine were measured from 1996 through 1998. Clinic response rates ranged from 74% to 98%. Data from the Medical Outcomes Study 36-Item Short Form (SF-36) were used to compute standardized scores in the followingeight health scales for English- and Spanish-speaking patients: physical functioning, role limitations because of physical problems, bodily pain, general health perceptions, vitality, social functioning, role limitations because of emotional problems, and mental health. Patients at these osteopathic training clinics reported poorer health than the general population on all eight scales (P < .001). Patients who were English speakers reported significantly better health than their Spanish-speaking counterparts on four of the eight health scales, although theSpanish-speaking patients reported greater vitality. There were significant differences in patient health across clinics. More than 92% of patients at these sixosteopathic training clinics reported that they were satisfied or very satisfied with their healthcare. This study suggests that osteopathic medical students are well accepted in ambulatory clinic encounters and that these students may encounter differing levels of patient health depending on where they receive their training.
<68>Unique Identifier 11999484Authors Moss NE.Institution Center for AIDS Prevention Studies, University of California San Francisco, 94105,
Page 33

201-400.txtUSA. [email protected] Gender equity and socioeconomic inequality: a framework for the patterning of women's health.Source Social Science & Medicine. 54(5):649-61, 2002 Mar.Abstract This paper explores the interrelationship of gender equity and socioeconomic inequality and how they affect women's health at the macro- (country) and micro- (household and individual) levels. An integrated framework draws theoretical perspectives from both approaches and from public health. Determinants of women's health in the geopolitical environment include country-specific history and geography, policies and services, legal rights, organizations and institutions, and structures that shape gender and economic inequality. Culture, norms and sanctions at the country and community level, and sociodemographic characteristics at the individual level, influence women's productive and reproductive roles in the household and workplace. Social capital, roles, psychosocial stresses and resources.health services, and behaviors mediate social, economic and cultural effects on health outcomes. Inequality between and within households contributes to the patterning of women's health. Within the framework, relationships may vary dependingupon women's lifestage and cohort experience. Examples of other relevant theoreticalframeworks are discussed. The conclusion suggests strategies to improve data, influence policy, and extend research to better understand the effect of gender and socioeconomic inequality on women's health.
<69>Unique Identifier 11990232Authors Bonner S. Zimmerman BJ. Evans D. Irigoyen M. Resnick D. Mellins RB.Institution Center for Urban Epidemiologic Studies, New York Academy of Medicine, New York 10029, USA. [email protected] An individualized intervention to improve asthma management among urban Latino andAfrican-American families.Source Journal of Asthma. 39(2):167-79, 2002 Apr.Abstract We hypothesized that an educational intervention based on a readiness model would lead to improved health outcomes among patients with asthma. Within a randomized control design in an urban Latino and African-American community we conducted an intensive three-month pediatric intervention. A Family Coordinator provided patient education based on a readiness-to-learn model, and facilitated improved interactionsbetween the patient and the doctor. Family education addressed the most basic learning needs of patients with asthma by improving their perception of asthma symptom persistence using asthma diaries and peak flown measures. The physician intervention focused cliniciancs' attention on patients' diary records and peak flowmeasures, and encouraged physicians to use stepped action plans. Patients were also tested for allergic sensitization and provided strategies to reduce contact with allergens and other asthma triggers. The results showed significant improvements by intervention group families on measures of knowledge, health belief, self-efficacy, self-regulatory skill, and adherence; decreases in symptom persistence and activity restriction; and increased prescription of anti-inflammatory medication by the physicians of the intervention group families.
<70>Unique Identifier 11978216Authors Blair AS. Lloyd-Williams F. Mair FS.
Page 34

201-400.txtInstitution Mersey Primary Care Research Development Consortium, Department of Primary Care, University of Liverpool, England L69 3GB.Title What do we know about socioeconomic status and congestive heart failure? A review of the literature. [Review] [55 refs]Source Journal of Family Practice. 51(2):169, 2002 Feb.Abstract OBJECTIVE: To examine and assess the available literature concerning the effects of socioeconomic status (SES) and congestive heart failure (CHF). STUDY DESIGN: We examined electronic databases, including: MEDLINE, EMBASE, Social Science Citation Index, Science citation index, the Cochrane Database, and Bandolier. We hand searched recent copies of appropriate journals and scrutinized lists of identified papers. The search terms we used included "heart failure," "cardiac failure," "ventricular dysfunction," "social class," "socioeconomic," "poverty," and "deprivation." Two reviewers independently examined and selected papers for inclusion. A standardized data collection form was used for data extraction. OUTCOMES MEASURED: We measured (1) prevalence; (2) differences in care (eg, use of diagnostic tests); (3) morbidity (eg, health care use); and (4) mortality. DATA SOURCES: We examined all English-language abstracts or papers concerning human research related to the subject of SES and CHF, including all clinical trials, reviews, discussion papers, and editorials. RESULTS: Only 8 clinical studies were identified that specifically examined aspects of the relationship between socioeconomic status and CHF. Key themes included increased hospitalization rates with increasing social deprivation; lower income inversely associated with being placed on a waiting list for transplantation; and that those of lower socioeconomic status had a greater severity of illness on admission. CONCLUSIONS: There is a paucity of generalizable high-quality research in this subject area. Crucial issues not addressed include the effects, if any, of socioeconomic status on the behaviors of health care providers. Further investigation, with a more holistic approach, is necessary to inform future intervention strategies aimed at reducing excess mortality from CHF. [References: 55]
<71>Unique Identifier 11979025Authors Waldron S. Hanas R. Palmvig B.Institution Leicestershire Nutrition and Dietetic Service, Leicestershire and Rutland Healthcare NHS Trust, Leicester, UK. [email protected] How do we educate young people to balance carbohydrate intake with adjustments of insulin?.Source Hormone Research. 57 Suppl 1:62-5, 2002.Abstract The dietary management of childhood diabetes is complex. Is it possible to educateyoung people to balance carbohydrate with their insulin? Can dietary knowledge be translated into lasting behaviour change? Do present teaching methods provide the skills necessary for children and parents to adjust their insulin therapy adequately? Evidence shows great variation in glycaemic control between centres and countries but the impact of dietary education methods is poorly evaluated and its links with clinical and psychosocial outcomes is virtually unknown. There is also little evidence to suggest cohesive teamworking with clear dietary targets for glycaemic control, lipids, incidence of hypoglycaemia, compliance, effect on peer and sibling relationships, and evaluation of individual dietary components, e.g. fibre, fat, antioxidants. There is wide variation in methods of dietary education, which are often based on historic practice. They include rigid counting of grams of carbohydrate, carbohydrate portion assessments, qualitative diets, low glycaemic index diets and the more recent 'intensified' carbohydrate measures with daily
Page 35

201-400.txtadjustments of insulin (the basis also of pump management). This last method has many benefits although it requires extensive nutrition education, it allows greater flexibility and variety of food intake, is sensitive to the varying daily energy expenditure of childhood and it addresses postprandial glycaemic excursions, all of which are inadequately managed by conventional therapy. However, one of the problemsof overemphasizing carbohydrate measurement is that total carbohydrate intake may besuppressed, with a resulting increase in fat, this may contribute to an increase in cardiovascular risk. The ISPAD Consensus Guidelines 2000 contain dietary recommendations but scientific evidence is often lacking. Limited dietary studies show that some countries can meet guidelines more successfully than others. There are many reasons for this, such as food availability, types of food eaten, food preferences and family/cultural/religious influences. Educational methods must be adapted to local customs. Is there enough evidence to recommend a particular dietaryeducation method? What outcomes do we hope to achieve? The workshop explored these issues in order to develop a deeper understanding of the complexity of dietary modification in childhood diabetes. Copyright 2002 S. Karger AG, Basel
<72>Unique Identifier 11974675Authors Shire N.Institution Procter & Gamble Pharmaceuticals, Cincinnati, OH, USA. [email protected] Effects of race, ethnicity, gender, culture, literacy, and social marketing on public health. [Review] [22 refs]Source Journal of Gender-Specific Medicine. 5(2):48-54, 2002 Mar-Apr.Abstract Societies globally have a long road ahead in eliminating health risks and discrepancies due to race and ethnicity, gender, culture, and illiteracy. In terms of race, for example, females and African-Americans are less likely to be referred for cardiac catheterization, and Caucasians are more likely than minorities to receive pain management in the emergency room. Regarding gender, physiologic differences certainly account for some divergent health outcomes, but they do not explain how women and men have different prevalences of diseases that are not obviously gender-specific. Cultural beliefs play a vital role in determining health choices, and health care professionals need a deeper understanding of these beliefs prior to promoting certain health interventions. Illiteracy may also prevent a person from following health instructions, and the strong association between illiteracy and poverty may exert powerful, negative influences on health outcomes. Employing the characteristics of social marketing (synchronous messages, reinforcement, and actionability) may help society to overcome some of the obstacles. [References: 22]
<73>Unique Identifier 11962178Authors Anonymous.Title Developing cultural competence in health care settings. National Center for Cultural Competence.Source Pediatric Nursing. 28(2):133-7, 2002 Mar-Apr.Abstract Increasing cultural and linguistic competence in health care settings is importantfor several reasons, including: responding to current and projected demographic changes in the United States; eliminating long-standing disparities in the health status of people of diverse racial, ethnic, and cultural backgrounds; improving
Page 36

201-400.txtquality of both services provided and health outcomes; meeting legislative, regulatory, and accreditation mandates; gaining a competitive edge in the market place; and decreasing the likelihood of liability/malpractice claims. Changes in policies, structures, practices, and procedures are often needed to bring about improvements in this arena. To support the process of change, The National Center for Cultural Competence (NCCC) was funded to increase the capacity of health care and mental health systems, institutions, programs, and providers to design, implement, and evaluate service delivery systems for cultural and linguistic competence. Several checklists developed by the NCCC are presented here for use by individual practitioners, programs, and institutions in assessing aspects of cultural competence.
<74>Unique Identifier 11952461Authors Vangen S. Stoltenberg C. Johansen RE. Sundby J. Stray-Pedersen B.Institution Department of Obstetrics and Gynecology, National Hospital, Oslo, Norway. [email protected] Perinatal complications among ethnic Somalis in Norway.Source Acta Obstetricia et Gynecologica Scandinavica. 81(4):317-22, 2002 Apr.Abstract BACKGROUND: The majority of ethnic Somali women in Norway have undergone an elaborate form of circumcision (infibulation). The aim of this study was to examine the risk of perinatal complications among ethnic Somalis and to discuss its relationto circumcision. METHODS: We conducted a cross-sectional population-based registry study. Data on all births to women born in Somalia (1733) and Norway (702 192) from 1986 to 1998 was provided from the Medical Birth Registry of Norway. We analyzed therisk of perinatal complications among women of Somali origin vs. ethnic Norwegians using univariate and multivariate methods. RESULTS: Perinatal complications were more frequent among women of Somali origin than among ethnic Norwegians. These included induction of labor, fetal distress, secondary arrest, prolonged second stage of labor, operative delivery and perinatal death. Particularly elevated odds ratios were found for fetal distress (odds ratio=2.6, 95% confidence interval (CI); 2.2-3.0), emergency cesarean sections (odds ratio=3.0, 95% confidence interval 2.6-3.4), Apgar scores below seven (odds ratio = 3.1, 95% confidence interval 2.4-4.0) and prelabor fetal deaths (odds ratio=2.5, 95% confidence interval 1.7-3.7). CONCLUSION: Similar findings in infibulated vs. noncircumcised women have been demonstrated previously in other studies indicating that circumcision could play a role. The current study is the first to be conducted among Somali women in Europe. However, the results are not informative on whether the adverse birth outcomes are caused by infibulation as such or in combination with suboptimal perinatal care, intercurrent diseases and sociocultural factors. Somali women represent a high-risk group in obstetrics, calling for special attention and care.
<75>Unique Identifier 11944952Authors Schwarz RE. Zagala-Nevarez K.Institution City of Hope National Medical Center, Department of General Oncologic Surgery, Duarte, CA, USA. [email protected] Ethnic survival differences after gastrectomy for gastric cancer are better explained by factors specific for disease location and individual patient comorbidity.Source
Page 37

201-400.txt European Journal of Surgical Oncology. 28(3):214-9, 2002 Apr.Abstract INTRODUCTION: Different outcomes after resection of gastric cancer between variousethnic patient groups have been described. It remains unclear whether disparity of treatment forms, disease-related variables, or individual patients accounts for thiseffect. METHODS: In the 10 years between 1989 and 1999, 75 patients with gastric adenocarcinoma underwent gastrectomy at a single institution, with constant surgicalstandards during this time period, including complete (R0) resection attempt and extended lymphadenectomy. Ethnicity, disease characteristics, and treatment variables were analysed for their impact on survival. RESULTS: There were 40 males and 35 females, with a median age of 67 years (range 31-97). The gastrectomy extent was total (n=25), proximal (n=18), subtotal (n=17), distal (n=14), and segmental (n=1). The mean lymph-node count was 25+/-17 (SD). There was one post-operative death, and an overall complication rate of 27%; the median hospital stay was 11 days. Overall actuarial 5-year survival was 33% (95% CI: 19-47); potentially curabledisease (stage 1A-IIIB) led to a median survival of 49 months. Asian (n=18) and Hispanic patients (n=20) had significantly better survival than Caucasian (n=31) or other patients (n=6) (P=0.01). Ethnicity was linked to the location of the primary tumour ( P=0.002), the gastrectomy extent (P=0.003), and the patient's prior abdominal operation (P=0.01) or tobacco history (P=0.03), but not to resection extent parameters (such as number of lymph nodes retrieved) or differences in pathologic characteristics. When controlling for differences of disease site, stage,R status, and patient comorbidity, ethnicity did not retain an independent prognostic impact on survival. CONCLUSIONS: Obvious survival differences after gastrectomy for gastric adenocarcinoma favouring Asian and Hispanic patients in thisexperience can be explained by different disease patterns (distal location), the related need for fewer extensive procedures (such as total gastrectomy), and diminished patient risks (tobacco, prior operations, non-cancer deaths). Our therapeutic approach remains an aggressive gastrectomy/lymphadenectomy combination for potentially curable gastric cancer, irrespective of ethnic patient factors. Copyright Harcourt Publishers Limited.
<76>Unique Identifier 11942187Authors Champion JD. Kelly P.Institution School of Nursing, University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78284, USA. [email protected] Protective and risk behaviors of rural minority adolescent women.Source Issues in Mental Health Nursing. 23(3):191-207, 2002 Apr-May.Abstract Studies of adolescent risk and protective behaviors have focused on identifying modifiable psychosocial variables that predict differential outcomes for subsequent intervention efforts. Research has been scarce in studies of rural minority adolescent women. This study examined the protective and risk behaviors of these women and their relationship to physical or sexual abuse. Rural minority adolescent women endured high levels of psychological distress and many high risk behaviors, yet experienced many protective behaviors. Barriers to health care included access and confidentiality. Physically or sexually abused adolescents endured relatively greater risk and fewer protective behaviors than nonabused adolescents. The prevalence of risk behaviors and abuse among rural minority adolescent women presents a need for development of psychotherapeutic interventions as part of behavioral interventions for risk reduction. These women may benefit from confidential identification and assessment of abuse history and risk and protective behaviors so that appropriate psychological treatment can accompany accessible medical treatment.
Page 38

201-400.txt<77>Unique Identifier 11937623Authors Cocroft JR. Hauck WW. Cosler L. Turner BJ.Institution Division of Genetic and Preventive Medicine, Jefferson Medical College of Thomas Jefferson University, Philadelphia, Pennsylvania, USA.Title The effect of ethnicity and maternal birthplace on small-for-gestational-age deliveries to HIV-infected women.Source Journal of Urban Health. 79(1):147-60, 2002 Mar.Abstract OBJECTIVE: To examine the relative role of ethnicity and maternal birthplace on small-for-gestational-age (SGA) deliveries of a cohort of mothers in New York who were infected with human immunodeficiency virus. METHODS: Medicaid claims and linkedvital statistics records were examined for 2,525 singleton deliveries to HIV-infected women from 1993 through 1996. We estimated adjusted odds ratios (AORs) and 95% confidence intervals (CIs) of SGA delivery associated with ethnicity (i.e., white, white-Latina, black, and black-Latina) and maternal birthplace (i.e., native US/Puerto Rican vs. foreign born) in a series of multivariate regression models to which we sequentially added demographic, health services, and lifestyle factors (i.e., alcohol, tobacco, and illicit drug use). RESULTS: Of the deliveries, 10% wereSGA. The odds of SGA infants for black and white women did not differ by maternal birthplace. Foreign-born white-Latinas and black-Latinas had lower unadjusted odds of a SGA delivery than their US-born counterparts (OR 0.29, CI 0.14, 0.61 and OR 0.22, CI 0.07, 0.71, respectively). After adjustment for maternal lifestyle characteristics, the odds of SGA delivery were 0.50 (CI 0.23, 1.09) for white-Latinamothers and 0.60 (CI 0.17, 2.08) for black-Latina mothers. CONCLUSIONS: SGA outcomesdid not differ by maternal birthplace for black and white women. Differences in lifestyle factors appear to contribute to lower odds of SGA delivery for foreign-born versus US-born white- and black-Latina HIV-infected women.
<78>Unique Identifier 11933009Authors Skelly AH. Arcury TA. Gesler WM. Cravey AJ. Dougherty MC. Washburn SA. Nash S.Institution School of Nursing, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599-7460, USA.Title Sociospatial knowledge networks: appraising community as place.Source Research in Nursing & Health. 25(2):159-70, 2002 Apr.Abstract This article introduces a new theory of geographical analysis, sociospatial knowledge networks, for examining and understanding the spatial aspects of health knowledge (i.e., exactly where health beliefs and knowledge coincide with other support in the community). We present an overview of the theory of sociospatial knowledge networks and an example of how it is being used to guide an ongoing ethnographic study of health beliefs, knowledge, and knowledge networks in a rural community of African Americans, Latinos, and European Americans at high risk for, but not diagnosed with, type 2 diabetes mellitus. We believe that the geographical approach to understanding health beliefs and knowledge and how people acquire healthinformation presented here is one that could serve other communities and community health practitioners working to improve chronic disease outcomes in diverse local environments. Copyright 2002 Wiley Periodicals, Inc.
Page 39

201-400.txt<79>Unique Identifier 11933008Authors Brown SA. Becker HA. Garcia AA. Barton SA. Hanis CL.Institution University of Texas at Austin School of Nursing, Austin, TX, USA.Title Measuring health beliefs in Spanish-speaking Mexican Americans with type 2 diabetes: adapting an existing instrument.Source Research in Nursing & Health. 25(2):145-58, 2002 Apr.Abstract Mexican Americans bear a disproportionate burden of type 2 diabetes, and although clinicians and researchers are beginning to develop culturally competent interventions, few instruments are available for measuring variables relevant to health outcomes. The purpose of this study was to determine the psychometric properties of a diabetes-related health belief instrument translated for use with Spanish-speaking Mexican Americans. Three hundred and twenty-six Spanish-speaking Mexican Americans from Starr County, a Texas-Mexico border community, diagnosed withtype 2 diabetes participated in the study. Factor analysis was used to examine the factor structure of the instrument, and reliability testing was conducted to determine the internal consistency of the resulting factors. The final instrument had 25 items with four subscales-Barriers, Social Support for Diet, Impact of Job onTherapy, and Benefits of Therapy-and one item to measure, Control. Internal consistency coefficients for these subscales were .56, .62, .86, and .90, respectively. The translated instrument needs to be tested over time with other Hispanic populations. Copyright 2002 Wiley Periodicals, Inc.
<80>Unique Identifier 11928771Authors Cherniss C.Institution GSAPP, Rutgers University, Piscataway, New Jersey 08854, USA. [email protected] Emotional intelligence and the good community.Source American Journal of Community Psychology. 30(1):1-11, 2002 Feb.Abstract Suggests various ways in which the concept of emotional intelligence (EI) can inform community research and action. Begins by defining EI and reviewing the growing body of research on its contribution to educational, health, and occupational outcomes. Next distinguishes between EI and the related concept of emotional and social competence. Then considers the connection between EI and several topics of interest to community action researchers including prevention and wellness promotion, implementation and dissemination of innovative programs, community development, and the value of diversity. Concludes by suggesting that the ecological perspective can help inform research and practice relating to EI.
<81>Unique Identifier 11924302Authors Anderson-Loftin W. Barnett S. Sullivan P. Bunn PS. Tavakoli A.Institution University of South Carolina, College of Nursing, Columbia, SC 29208, USA. [email protected]
Page 40
201-400.txt Culturally competent dietary education for southern rural African Americans with diabetes.Source Diabetes Educator. 28(2):245-57, 2002 Mar-Apr.Abstract PURPOSE: The purpose of this article is to describe a culturally competent, dietary self-management intervention designed to improve physiological outcomes, diabetes self-management, and costs of care for high-risk African Americans with type 2 diabetes. METHODS: A longitudinal, quasi-experimental design was used to evaluate the effectiveness of the intervention for 23 adult African Americans from aphysician practice group in rural South Carolina. The intervention consisted of 4 low-fat dietary education classes, 6 discussion groups, and follow-up. Intervention sessions were provided by a dietitian and nurse case managers and framed as social events; families were encouraged to participate. RESULTS: Data suggest that the intervention significantly improved fat-related dietary habits, A1C values, fasting blood glucose, and frequency of acute care visits. A trend in reduction of lipids and weight also was observed. CONCLUSIONS: Culturally competent dietary self-management provides a meaningful approach to focused diabetes education for rural African Americans. Integrating nursing case management provides an innovative method of addressing the more global issues of delivery of care to underserved ruralpopulations and decreasing the high costs of care.
<82>Unique Identifier 11921326Authors Gotay CC. Holup JL. Pagano I.Institution Cancer Research Center of Hawaii, University of Hawaii, Honolulu 96813, USA. [email protected] Ethnic differences in quality of life among early breast and prostate cancer survivors.[see comment].Source Psycho-Oncology. 11(2):103-13, 2002 Mar-Apr.Abstract This study assessed quality of life (QOL) in recently diagnosed breast and prostate cancer patients of European American and Asian Pacific Islanders (specifically, individuals of Filipino, Japanese, and Native Hawaiian ancestry) to investigate whether QOL varied according to ethnicity and the relative importance ofethnicity as a predictor of QOL. Participants were identified through consecutive registrations on the Hawaii Tumor Registry, based on a diagnosis of breast or prostate cancer 4-6 months previously. QOL was measured by the QLQ-C30, a standardized questionnaire widely used in cancer patient populations. Two hundred and twenty-seven individuals participated (101 prostate and 126 breast cancer patients). QOL was similar across ethnic groups in most areas of QOL. However, differences were found in several areas, all in the direction of Filipino patients reporting worse outcomes. Hierarchical stepwise regressions supported the importanceof ethnicity, controlling for clinical and demographic predictors. We conclude that additional research is needed to understand the relationship between ethnicity and QOL in cancer survivors. Copyright 2002 John Wiley & Sons, Ltd.
<83>Unique Identifier 11919062Authors Gee GC.Institution Training Program in Identity, Self, Role, and Mental Health, Department of Sociology, Indiana University, Ballantine Hall 744, 1020 E Kirkwood Avenue, Bloomington, IN 47405-7103, USA. [email protected]
Page 41

201-400.txtTitle A multilevel analysis of the relationship between institutional and individual racial discrimination and health status.Source American Journal of Public Health. 92(4):615-23, 2002 Apr.Abstract OBJECTIVES: This study examined whether individual (self-perceived) and institutional (segregation and redlining) racial discrimination was associated with poor health status among members of an ethnic group. METHODS: Adult respondents (n =1503) in the cross-sectional Chinese American Psychiatric Epidemiologic Study were geocoded to the 1990 census and the 1995 Home Mortgage Disclosure Act database. Hierarchical linear modeling assessed the relationship between discrimination and scores on the Medical Outcomes Study Short-Form 36 and revised Symptom Checklist 90 health status measures. RESULTS: Individual and institutional measures of racial discrimination were associated with health status after control for acculturation, sex, age, social support, income, health insurance, employment status, education, neighborhood poverty, and housing value. CONCLUSIONS: The data support the hypothesis that discrimination at multiple levels influences the health of minority group members.
<84>Unique Identifier 11919057Authors Kritek PB. Hargraves M. Cuellar EH. Dallo F. Gauthier DM. Holland CA. Ilkiw C. Swanson JW. Swanson R.Institution Medical Branch, University of Texas, Galveston, TX, USA. [email protected] Eliminating health disparities among minority women: a report on conference workshop process and outcomes.Source American Journal of Public Health. 92(4):580-7, 2002 Apr.Abstract A national conference convened in May 2001 explored health disparities among minority women. It included 5 one-hour workshops that randomly assigned each participant to 1 of 4 groups. Groups generated recommendations on conference topics and from these identified priority recommendations. Trained facilitators guided groups through brainstorming and weighted voting processes; individual recommendations were submitted in writing. Participants generated 598 recommendations, 71 of them voted as priorities; these were analyzed to capture participants' "messages." Central themes focused on access issues and cultural incompetence as deterrents to the elimination of health disparities and on education, funding, and community-based, community-driven research as mechanisms forchange. Strategies for change included reinventing or expanding the role of minoritycommunities and changing health care itself and "how" it does its work. The essential element in all recommendations was community leadership and control.
<85>Unique Identifier 11919051Authors Musgrave CF. Allen CE. Allen GJ.Institution Henrietta Szold Hadassah Hebrew University School of Nursing, Jerusalem, Israel.Title Spirituality and health for women of color.[see comment].Source American Journal of Public Health. 92(4):557-60, 2002 Apr.Abstract Spirituality among African American and Hispanic women has been associated with a
Page 42

201-400.txtvariety of positive health outcomes. The purposes of this commentary are (1) to define spirituality, comparing it with religiosity, and briefly examine the historical, cultural, and contextual roots of spirituality among women of color; (2)to explore research data that support a relationship between spirituality and health, particularly among women of color; and (3) to present several examples of how spirituality may enhance public health interventions designed to promote health and prevention.
<86>Unique Identifier 11919043Authors Walters KL. Simoni JM.Institution School of Social Work, University of Washington, 4101 15th Avenue NE, Seattle, WA 98105-6299, USA. [email protected] Reconceptualizing native women's health: an "indigenist" stress-coping model.Source American Journal of Public Health. 92(4):520-4, 2002 Apr.Abstract This commentary presents an "indigenist" model of Native women's health, a stress-coping paradigm that situates Native women's health within the larger contextof their status as a colonized people. The model is grounded in empirical evidence that traumas such as the "soul wound" of historical and contemporary discrimination among Native women influence health and mental health outcomes. The preliminary model also incorporates cultural resilience, including as moderators identity, enculturation, spiritual coping, and traditional healing practices. Current epidemiological data on Native women's general health and mental health are reconsidered within the framework of this model.
<87>Unique Identifier 11914467Authors Dilworth-Anderson P. Williams IC. Gibson BE.Institution Department of Human Development and Family Studies, University of North Carolina at Greensboro, 27402-6170, USA. [email protected] Issues of race, ethnicity, and culture in caregiving research: a 20-year review (1980-2000). [Review] [169 refs]Source Gerontologist. 42(2):237-72, 2002 Apr.Abstract PURPOSE: The goals of this review are to synthesize what is known about caregivingamong diverse groups and to identify gaps in knowledge to guide future research on caregiving. The review focuses on conceptual and theoretical approaches, sampling strategies, measurement techniques, and similarities and differences found among groups and across studies. DESIGN AND METHODS: A narrative approach was used to review 59 articles published between 1980 and 2000, with particular attention to race, ethnicity, and/or culture. Primary sources of relevant articles included electronic databases, other review articles, and reference lists. RESULTS: Caregiving experiences and outcomes varied across racial and ethnic groups. However,the use of nontheoretical approaches, nonprobability samples, and inconsistent measures among studies has limited understanding of caregiving among diverse populations. IMPLICATIONS: It is important that conceptualization and theorizing broaden with increasing numbers of studies that include diverse groups. Future caregiving research needs to give more attention to such issues as acculturation, assimilation, and cultural values, beliefs, and norms, while also improving theoretical and methodological rigor. [References: 169]
Page 43

201-400.txt
<88>Unique Identifier 11913854Authors Chen MS.Institution Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan. [email protected] Oral health status and its inequality among education groups: comparing seven international study sites.Source International Journal of Health Services. 32(1):139-61, 2002.Abstract This study compares oral health status and its inequality among education groups across seven study sites in five countries: Erfurt, Germany; Lodz, Poland; Yamanashi, Japan; New Zealand; and Baltimore and the Lakota and Navajo Indian HealthService sites in the United States. The data, from the International Collaborative Study of Oral Health Outcomes, were collected through personal interviews and clinical examinations. The research group measured the study sites' overall oral health, examining the percentage of the population with five or more missing and twoor more decayed teeth. The group also assessed the magnitude of inequality among education groups by using indices of excess morbidity. Baltimore had the lowest percentage (10.8 percent) of decayed teeth and second lowest percentage (17.3 percent) of missing teeth, but the greatest indices of excess morbidity (79.2 percent for missing, 73.1 percent for decayed). Lodz, by contrast, had the worst overall dentition status (75.3 percent for missing, 70.3 percent for decayed) but the lowest inequality indices (10.6 percent for missing, 13.8 percent for decayed). This study demonstrates the need for policymakers in the study countries to considernot only overall levels but also the distribution of oral health, and it presents various challenges for oral health professionals in designing and implementing oral health programs.
<89>Unique Identifier 11913599Authors Keenan LA. Marshall LL. Eve S.Institution Department of Psychology, University of North Texas, Denton 76203, USA.Title Extension of the behavioral model of healthcare utilization with ethnically diverse, low-income women.Source Ethnicity & Disease. 12(1):111-23, 2002 Winter.Abstract OBJECTIVE: Psychosocial vulnerabilities were added to a model of healthcare utilization. This extension was tested among low-income women with ethnicity addressed as a moderator. DESIGN: Structured interviews were conducted at 2 points in time, approximately 1 year apart. The constructs of psychosocial vulnerability, demographic predisposing, barriers, and illness were measured by multiple indicatorsto allow use of Structural Equation Modeling to analyze results. The models were tested separately for each ethnic group. SETTING: Community office. PARTICIPANTS: African-American (N = 266), Euro-American (N = 200), and Mexican-American (N = 210) women were recruited from the Dallas Metropolitan area to participate in Project HOW: Health Outcomes of Women, a multi-year, multi-wave study. Face-to-face interviews were conducted with this sample. Participants had been in heterosexual relationships for at least 1 year, were between 20 and 49 years of age, and had incomes less than 200% of the national poverty level. MAIN OUTCOME MEASURES: Healthcare utilization, defined as physician visits and general healthcare visits.
Page 44

201-400.txtRESULTS: Illness mediated the effect of psychosocial vulnerability on healthcare utilization for African Americans and Euro-Americans. The model for Mexican Americans was the most complex. Psychosocial vulnerability on illness was partially mediated by barriers, which also directly affected utilization. CONCLUSIONS: Psychosocial vulnerabilities were significant utilization predictors for healthcare use for all low-income women in this study. The final models for the 2 minority groups, African Americans and Mexican Americans, were quite different. Hence, women of color should not be considered a homogeneous group in comparison to Euro-Americans.
<90>Unique Identifier 11911378Authors van Servellen G. Chang B. Lombardi E.Institution School of Nursing, UCLA, USA.Title Acculturation, socioeconomic vulnerability, and quality of life in Spanish-speaking and bilingual latino HIV-infected men and women.Source Western Journal of Nursing Research. 24(3):246-63, 2002 Apr.Abstract Little is known about the health-related QOL (HRQOL) of low-income, Latino men andwomen living with HIV Monolingual Spanish-speaking Latino individuals may be at greater risk than bilingual men and womenforpoor HRQOL due to problems associated with language and cultural barriers. This study examined the health status and HRQOLof these two groups of clinic patients. The monolingual group had significantly lower levels of acculturation butdid not differ from the bilingual group on any dimension of health status. This group also reported more disruptions on several dimensions of HRQOL. In a multivariate context, health status variables (as a block)accountedfor the greatest proportion of variance in all three measures of HRQOL. Theresults did not support the hypothesis that acculturation mediates the impact of health status on HRQOL. More studies are needed to examine the impact of acculturation and socioeconomic vulnerability on health outcomes.
<91>Unique Identifier 11903775Authors Perkins HS. Geppert CM. Gonzales A. Cortez JD. Hazuda HP.Institution Department of Medicine, University of Texas Health Science Center at San Antonio, 78229, USA.Title Cross-cultural similarities and differences in attitudes about advance care planning.Source Journal of General Internal Medicine. 17(1):48-57, 2002 Jan.Abstract OBJECTIVE: Culture may have an important impact on a patient's decision whether toperform advance care planning. But the cultural attitudes influencing such decisionsare poorly defined. This hypothesis-generating study begins to characterize those attitudes in 3 American ethnic cultures. DESIGN: Structured, open-ended interviews with blinded content analysis. SETTING: Two general medicine wards in San Antonio, Texas. PATIENTS: Purposive sampling of 26 Mexican-American, 18 Euro-American, and 14African-American inpatients. MEASUREMENTS AND MAIN RESULTS: The 3 groups shared someviews, potentially reflecting elements of an American core culture. For example, majorities of all groups believed "the patient deserves a say in treatment," and "advance directives (ADs) improve the chances a patient's wishes will be followed." But the groups differed on other themes, likely reflecting specific ethnic cultures.
Page 45
201-400.txtFor example, most Mexican Americans believed "the health system controls treatment,"trusted the system "to serve patients well," believed ADs "help staff know or implement a patient's wishes," and wanted "to die when treatment is futile." Few Euro Americans believed "the system controls treatment," but most trusted the system"to serve patients well," had particular wishes about life support, other care, and acceptable outcomes, and believed ADs "help staff know or implement a patient's wishes." Most African Americans believed "the health system controls treatment," fewtrusted the system "to serve patients well," and most believed they should "wait until very sick to express treatment wishes." CONCLUSION: While grounded in values that may compose part of American core culture, advance care planning may need tailoring to a patient's specific ethnic views.
<92>Unique Identifier 11891489Authors McClowry SG.Institution Division of Nursing, New York University, 246 Greene Street, 8th Floor, New York, NY 10003-6677, USA. [email protected] The temperament profiles of school-age children.Source Journal of Pediatric Nursing. 17(1):3-10, 2002 Feb.Abstract Maternal reports of child temperament were used to develop temperament profiles ofschool-age children. The subjects were 883 children who were between 4 and 12 years of age. The children's families varied substantially in their socioeconomic status and race/ethnicity. To develop the profiles, the dimensions derived from the School-Age Temperament Inventory were subjected to a second order principal factor analysis with varimax rotation. Pearson chi-squares were used to determine whether sociodemographic variables were proportionally represented among the profiles. Forty-two percent of the children were classified into four temperament profiles. High maintenance and cautious/slow to warm up were deemed as challenging temperaments. Industrious and social/eager to try were mirror images of those profiles and were labeled easy. Some children were both types of challenging or easyprofiles. The generalizability of the profiles in relation to the sociodemographic variables of gender, age, race/ethnicity, and socioeconomic status was also examined. Challenging temperament profiles were disproportionately represented by boys, Hispanic children, and those from lower socioeconomic families. Girls were over represented in the group that included both types of easy temperaments. Social/eager to try children were more often from higher rather than lower socioeconomic status families. Clinical applications and research implications for the profiles are discussed. The profiles can be used as exemplars that parents can use to recognize their child's temperament. Further research is needed to explore whether different developmental outcomes are associated with the profiles. Copyright2002, Elsevier Science (USA).
<93>Unique Identifier 11891158Authors Drouin J. Jean P.Institution Faculty of Medicine, University of Ottawa, Ottawa, Ontario, Canada. [email protected] Educating future physicians for a minority population: a French-language stream atthe University of Ottawa.Source Academic Medicine. 77(3):217-21, 2002 Mar.
Page 46

201-400.txtAbstract The Faculty of Medicine at the University of Ottawa has recently developed a French-language undergraduate medical education stream in order to train physicians for the francophone minority population of the province of Ontario. This new programwas planned with the following societal requirements in mind: the need to receive health care in one's mother tongue, the need to have physicians who know the community, and the expectation of receiving good medical care in an ambulatory setting. A systematic educational planning model was used in order to develop three educational innovations in response to these needs and expectations: a communicationskills laboratory; early student exposure to the ambulatory, primary care setting for development of clinical skills; and clerkship rotations in a francophone community hospital. Program developers provided ongoing faculty development activities in order to prepare francophone faculty for their new roles. They also considered student participation in program development an essential element of its success. The program has positive outcomes both within and outside the Faculty of Medicine. These include an enrichment effect on the English-language stream, an increased interest in medical education, student satisfaction with their community hospital clerkship rotations, and the recognition of the educational program as a national resource for francophone minority groups. Medical schools that serve minority population groups may benefit from the experience gained at the University of Ottawa.
<94>Unique Identifier 11891153Authors Green AR. Betancourt JR. Carrillo JE.Institution Cornell Internal Medicine Associates, New York, NY 10021, USA. [email protected] Integrating social factors into cross-cultural medical education.[see comment].Source Academic Medicine. 77(3):193-7, 2002 Mar.Abstract The field of cross-cultural medical education has blossomed in an environment of increasing diversity and increasing awareness of the effect of race and ethnicity onhealth outcomes. However, there is still no standardized approach to teaching doctors in training how best to care for diverse patient populations. As standards are developed, it is crucial to realize that medical educators cannot teach about culture in a vacuum. Caring for patients of diverse cultural backgrounds is inextricably linked to caring for patients of diverse social backgrounds. In this article, the authors discuss the importance of social issues in caring for patients of all cultures, and propose a practical, patient-based approach to social analysis covering four major domains--(1) social stress and support networks, (2) change in environment, (3) life control, and (4) literacy. By emphasizing and expanding the role of the social history in cross-cultural medical education, faculty can better train medical students, residents, and other health care providers to care for socioculturally diverse patient populations.
<95>Unique Identifier 11876562Authors Barfield WD. Tomashek KM. Flowers LM. Iyasu S.Institution Epidemic Intelligence Service, Division of Applied Public Health Training Epidemiology Program Office, Centers for Disease Control and Prevention, Atlanta, GA, USA. [email protected] Contribution of late fetal deaths to US perinatal mortality rates, 1995-1998.Source
Page 47
201-400.txt Seminars in Perinatology. 26(1):17-24, 2002 Feb.Abstract We analyzed US fetal death and linked infant birth-death certificate data for 1995-1998 to evaluate perinatal deaths (late fetal deaths [> or = 28 weeks' gestation] and early neonatal deaths [< or = 7 days of life]) by race, Hispanic ethnicity, state of residence, and selected demographic characteristics. We also compared components of perinatal mortality, late fetal deaths, and early neonatal deaths, by birthweight, gestational age, and selected maternal medical conditions during pregnancy. From 1995 through 1998, there were 221,767 fetal deaths at > or = 20 weeks' gestation and infant deaths at less than 1 year. Of these, 113,421 (51%) were perinatal deaths; late fetal deaths accounted for 47% of perinatal deaths. The total perinatal mortality rate declined 5.3%, from 7.5 to 7.1 per 1,000 live births plus late fetal deaths. Blacks experienced higher perinatal mortality rates than whites (rate ratio = 2.1). Among perinatal deaths > or = 28 weeks' gestation, the ratio of fetal to neonatal deaths was 3.4 among blacks and 2.4 among whites. State-specific rates ranged from 5.2 to 13.1 per 1,000 live births plus late fetal deaths. Although late fetal deaths are not included in routine statistics of pregnancy outcomes, these deaths represent a large proportion of adverse pregnancy outcomes. Surveillance of perinatal mortality provides a more complete picture of the health of women, fetuses, and newborns. Improving the quality of surveillance data regarding fetal deaths is essential for more effective use of these data. This information can be used to prevent excess perinatal deaths and reduce disparities inpregnancy outcomes among high-risk subgroups identified by individual and populationcharacteristics.
<96>Unique Identifier 11876561Authors Hoyert DL. Martin JA.Institution Division of Vital Statistics, National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, MD 20782, USA.Title Vital statistics as a data source. [Review] [10 refs]Source Seminars in Perinatology. 26(1):12-6, 2002 Feb.Abstract A focus group convened at a National Institutes of Health (NIH) Stillbirth Conference discussed issues related to vital statistics as a data source on fetal mortality. Fetal death is a tragic occurence and part of the continuum of pregnancy outcomes. A primary source of data is the National Vital Statistics System fetal death component, which is routinely used to track mortality trends and to provide the context for nonrepresentative investigations. The data are also used to examine differentials in mortality by characteristics and to evaluate data quality. Issues concerning how to improve the vital statistics data include culture and context; data instrument; persons providing information; what information is available to theinformation provider; processing issues; and use of data. Perhaps most important is to enhance recognition of fetal death both for the individual confronting a loss andto promote research. Other studies are needed to augment the information obtainable through vital records. [References: 10]
<97>Unique Identifier 11874938Authors LaGasse JM. Brantley MS. Leech NJ. Rowe RE. Monks S. Palmer JP. Nepom GT. McCulloch DK. Hagopian WA. Washingtno State Diabetes Prediction Study.Institution Pacific Northwest Research Institute, Seattle, Washington 98122, USA.Title
Page 48

201-400.txt Successful prospective prediction of type 1 diabetes in schoolchildren through multiple defined autoantibodies: an 8-year follow-up of the Washington State Diabetes Prediction Study.Source Diabetes Care. 25(3):505-11, 2002 Mar.Abstract OBJECTIVE: Almost 90% of type 1 diabetes appears in individuals without a close family history. We sought to evaluate the best current predictive strategy, multipledefined autoantibodies, in a long-term prospective study in the general population. RESEARCH DESIGN AND METHODS: Autoantibodies to pancreatic islets (islet cell antibodies [ICAs]) and defined autoantibodies (d-aab) to human GAD, IA2/ICA512, and insulin were tested in 4,505 Washington schoolchildren. Eight years later, 3,000 (67%) subjects were recontacted, including 97% of subjects with any test >99th percentile. RESULTS: Six subjects developed diabetes (median interval 2.8 years), all from among the 12 individuals with multiple d-aab, representing 50% positive predictive value (95% CI 25-75%) and 100% sensitivity (58-100%). Among the others, diabetes occurred in 0 of 6 with one d-aab plus ICA, 0 of 26 with ICA only, 0 of 7 with one d-aab equaling the 99th percentile and another d-aab equaling the 97.5th percentile, 0 of 86 with one d-aab, and 0 of 2,863 with no d-aab or ICA. Adjusted for verification bias, multiple d-aab were 99.9% specific (99.86-99.93%). At this age, new d-aab seldom appeared. Once present, d-aab usually persisted regardless of disease progression, although less so for insulin autoantibodies. Insulin secretion by sequential glucose tolerance testing remained normal in four multiple d-aab subjects not developing diabetes. Of children developing diabetes, five of six (83%)would be included if HLA-DQ genotyping preceded antibody testing, but HLA-DQ did notexplain outcomes among high-risk subjects, even when considered along with other genetic markers. CONCLUSIONS: Multiple d-aab were established by age 14 years and prospectively identified all schoolchildren who developed type 1 diabetes within 8 years.
<98>Unique Identifier 11870160Authors Potosky AL. Harlan LC. Kaplan RS. Johnson KA. Lynch CF.Institution Division of Cancer Control and Population Sciences, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892, USA. [email protected] Age, sex, and racial differences in the use of standard adjuvant therapy for colorectal cancer.Source Journal of Clinical Oncology. 20(5):1192-202, 2002 Mar 1.Abstract PURPOSE: Dissemination of efficacious adjuvant therapies for resectable colorectalcancer has not been comprehensively described. Trends, patterns, and outcomes of adjuvant therapy for colorectal cancer, focusing on age, sex, and racial/ethnic differences, are reported. MATERIALS AND METHODS: Population-based random samples ofpatients diagnosed with colorectal cancer diagnosed in nine geographic areas were collected annually between 1987 and 1991 and in 1995 (n = 4,706). Data were obtainedfrom medical record reviews. Multiple logistic regression was used to assess the useof standard adjuvant chemotherapy for colon and rectal cancers. The Cox proportionalhazards model was used to assess 9-year mortality. RESULTS: From 1987 until 1995, the use of adjuvant therapy increased in all age groups. There was an increase starting in 1989 for colon and in 1988 for rectal cancer. Use of standard therapy was 78% for those younger than 55 years and 24% for those older than 80 years. Whitepatients received standard therapy more frequently than African-Americans (odds ratio, 1.75; 95% confidence interval [CI], 1.09 to 2.83). All-cause and cancer-specific mortality exceeding 9 years were lower in those who received standard therapy (all-cause risk ratio [RR], 0.73; 95% CI, 0.61 to 0.88; cancer-specific RR, 0.87; 95% CI, 0.70 to 1.09). CONCLUSION: Standard adjuvant therapies for colorectal cancer disseminated into community practices during the
Page 49

201-400.txt1990s. However, evidence exists of differential use of therapies by older patients and by African-Americans. The use of standard therapies in the general population isassociated with lower mortality. Improved dissemination of standard adjuvant therapies to all segments of the population could help reduce mortality.
<99>Unique Identifier 11862950Authors Kramer MS. Platt RW. Yang H. Haglund B. Cnattingius S. Bergsjo P.Institution Department of Pediatrics, McGill University Faculty of Medicine, Montreal, [email protected] Registration artifacts in international comparisons of infant mortality.Source Paediatric and Perinatal Epidemiology. 16(1):16-22, 2002 Jan.Abstract Large differences in infant mortality are reported among and within industrialisedcountries. We hypothesised that these differences are at least partly the result of intercountry differences in registration of infants near the borderline of viability(<750 g birthweight) and/or their classification as stillbirths vs. live births. We used the database of the International Collaborative Effort (ICE) on Perinatal and Infant Mortality to compare infant mortality rates and registration practices in Norway (n = 112484), Sweden (n = 215 908), Israeli Jews (n = 148123), Israeli non-Jews (n = 52 606), US Whites (n = 6 074 222) and US Blacks (n = 1328332). To avoid confounding by strong secular trends in these outcomes, we restricted our analysis to 1987-88, the most recent years for which data are available in the ICE database for all six groups. Compared with Norway (with an infant mortality rate of 8.5 per 1000), the crude relative risks [95% confidence intervals] were 0.75 [0.69,0.81] in Sweden, 0.97 [0.90,1.06] in Israeli Jews, 1.98 [1.81,2.17] in Israelinon-Jews, 0.95 [0.89,1.01] in US Whites and 2.05 [1.95,2.19] in US Blacks. For borderline-viable infants, fetal deaths varied twofold as a proportion of perinatal deaths, with Norway reporting the highest (83.9% for births <500 g and 61.8% for births 500-749 g) and US Blacks the lowest (40.3% and 37.6% respectively) proportions. Reported proportions of live births <500 g varied 50-fold from 0.6 and 0.7 per 10000 in Sweden and Israeli Jews and non-Jews to 9.1 and 33.8 per 10000 in US Whites and Blacks respectively. Reported proportions 500-749 g varied sevenfold from 7.5 per 10000 in Sweden to 16.2 and 55.4 in US Whites and Blacks respectively. After eliminating births <750 g, the relative risks (again with Norway as the reference) of infant mortality changed drastically for US Whites and Blacks: 0.82 [0.76,0.87] and 1.42 [1.33,1.53] respectively. The huge disparities in the ratio of fetal to infant deaths <750 g and in the proportion of live births <750 g among these developed countries probably result from differences in birth and death registration practices. International comparisons and rankings of infant mortality should be interpreted with caution.
<100>Unique Identifier 11859439Authors McColl MA. Charlifue S. Glass C. Savic G. Meehan M.Institution Queen's University, School of Rehabilitation Therapy, Kingston, Canada.Title International differences in ageing and spinal cord injury.Source Spinal Cord. 40(3):128-36, 2002 Mar.Abstract DESIGN: The present study is part of a programme of longitudinal research on ageing and spinal cord injury involving three populations - American, British and
Page 50

201-400.txtCanadian. The design was multivariate. OBJECTIVE: To identify international differences in outcomes associated with ageing and spinal cord injury. SETTING: A sample of 352 participants was assembled from five large, well-established databases. The Canadian sample was derived from the member database of the Canadian Paraplegic Association (Ontario and Manitoba divisions). The British sample was recruited from Southport Hospital's Northwest Regional Spinal Injuries Centre and Stoke-Mandeville Hospital's National Spinal Injuries Centre. The American sample hasbeen recruited through Craig Hospital in Denver, Colorado. METHODS: The sample included individuals who had incurred a spinal cord injury at least 20 years previously; were admitted to rehabilitation within 1 year of injury; were between age 15 and 55 at the time of injury. Data were collected using a combination of self-completed questionnaires and interviews. Data included medical information, general health, hospitalisations, and changes in bladder and bowel management, equipment, pain, spasticity, the need for assistance, and other health issues. RESULTS: Clear international differences existed between the three samples in the three different countries. After controlling for sampling differences (ie, differences in age, level of lesion, duration of disability, etc.), the following differences were seen: (1) American participants had a better psychological profile and fewer health and disability-related problems; (2) British participants had less joint pain and less likelihood of perceiving they were ageing more quickly; (3) Canadians had more health and disability-related complications (particularly bowel, pain and fatigue problems). CONCLUSION: These differences are discussed in terms of socio-political, health care system and cultural factors that might be used to explain them, and to generate hypotheses for future research.
<101>Unique Identifier 11845768Authors Petersen WO. Trapp MA. Vierkant RA. Sellers TA. Kottke TE. de Groen PC. Nicometo AM. Kaur JS.Institution Department of Health Sciences Research, Mayo Clinic Comprehensive Cancer Center, Rochester, Minnesota, USA.Title Outcomes of training nurses to conduct breast and cervical cancer screening of Native American women.Source Holistic Nursing Practice. 16(2):58-79, 2002 Jan.Abstract Native WEB (Women Enjoying the Benefit) is a unique training program for nurses employed by the Indian Health Service (IHS), tribal clinics, and other clinics with large, underserved populations. It teaches nurses breast and cervix cancer screeningtechniques and trains them to administer and maintain high-quality screening programs that include patient outreach, education, and training. We review American Indian (AI)/Alaska Native (AN) women's need for screening services, identify some ofthe obstacles to screening, and present our evaluation of the Native WEB's impact onclinics, nurses, and patients. Findings show that Native WEB training is associated with increased screening activity at all three levels.
<102>Unique Identifier 11845642Authors Dong Q. Wang Y. Ollendick TH.Institution Institute of Developmental Psychology, Beijing Normal University, Beijing, China 100875.Title Consequences of divorce on the adjustment of children in China.Source
Page 51

201-400.txt Journal of Clinical Child & Adolescent Psychology. 31(1):101-10, 2002 Mar.Abstract Explored the consequences of divorce on children in China. In contrast to Western countries, divorce in China is relatively rare, occurring in approximately 10% to 15% of the population. Children from divorced families (n = 174) and matched intact families (n = 174) were selected from a larger sample of 1,294 children between 8 and 14 years of age. Divorce was relatively low in this sample (13.45%) of participants, consistent with rates observed in epidemiological studies in China. Mothers of divorced children reported higher levels of education but lower levels ofincome than mothers in intact families. Children in divorced families reported higher levels of anxiety and depression, and their mothers and teachers rated them as possessing more behavior problems on the Achenbach (1991) Child Behavior Checklist scales. Regression analyses revealed that rejecting and inattentive parenting styles, along with family status (divorce or intact), high maternal depression, and sex (boys) predicted significant amounts of variance associated withthese negative outcomes. Results are discussed in terms of familial and cultural issues associated with these findings.
<103>Unique Identifier 11846287Authors Fulton P. Tierney J. Mirpourian N. Ericsson JM. Wright JT Jr. Powel LL.Institution School of Nursing, University of Maryland, Baltimore 21201, USA.Title Engaging black older adults and caregivers in urban communities in health research.Source Journal of Gerontological Nursing. 28(2):19-27, 2002 Feb.Abstract The under-representation of the Black population in research may lead to poor health outcomes for them and a decreased capacity to generalize results to Black populations. This article describes ways in which sensitivity to cultural distinctions of Black older adults and their current or future caregivers can enhance their recruitment and retention in research. Cultural mores play an important role in the shaping of one's perceptions, definitions, responses to disease, and participation in health regimens. Similarly, one's cultural orientationplays a role in how a person is effectively recruited and retained in resear Wenger's translation process model uses cultural meaning to inform research decisions. This model was used in a recent study of Black older adults and their caregivers and will be described in this article. Effectively engaging Black individuals in health research is essential for improving their health.
<104>Unique Identifier 11842290Authors Strunk RC. Ford JG. Taggart V.Institution Department of Pediatrics, Washington University School of Medicine, St. Louis, MO 63108, USA.Title Reducing disparities in asthma care: priorities for research--National Heart, Lung, and Blood Institute workshop report.Source Journal of Allergy & Clinical Immunology. 109(2):229-37, 2002 Feb.Abstract Minority groups with diverse racial and ethnic heritages and persons living in poverty are much more likely to die of asthma and to require emergency care for exacerbations of asthma than white persons not living in poverty. The National
Page 52

201-400.txtHeart, Lung, and Blood Institute convened a multidisciplinary group of expert scientists and clinicians to review current research aimed at understanding risk factors for these disparities in asthma health outcomes, to describe key barriers toimproving asthma outcomes, and to establish priorities for future research. Education programs for asthma and other chronic diseases were reviewed. Successful elements of clinic and community-based programs were identified. Factors potentiallyinvolved in producing disparities include gene-environment interaction, psychologic and social factors, and socioeconomic status. Stress potentially contributes to asthma morbidity at both the individual and community level. Recommendations are made to stimulate research to understand risk factors for disparities and their mechanisms (e.g., gene-by-environment interactions and the role of stress), to define appropriate research designs and methods for evaluating behavioral and community interventions, and to examine how differential access to care contributes to morbidity. Research is encouraged to identify strategies that improve cultural adaptation and adoption of proven programs in a variety of populations.
<105>Unique Identifier 11839079Authors Seefeldt V. Malina RM. Clark MA.Institution Institute for the Study of Youth Sports, Michigan State University, East Lansing, Michigan 48823, USA. [email protected] Factors affecting levels of physical activity in adults. [Review] [246 refs]Source Sports Medicine. 32(3):143-68, 2002.Abstract A large proportion of adults in Western cultures are physically inactive, despite several decades of warnings about the potentially negative health consequences of a sedentary lifestyle. Efforts to promote physical activity have focused on identifying its determinants and designing interventions that might effectively promote regular physical activity. The multitude of factors that induce adults to initiate and maintain programmes of physical activity have been divided into those that are invariable (age, gender, race, ethnicity) and those that are presumed to bemodifiable (behavioural and personality characteristics, environmental circumstancesand community settings). The lack of consistency in the design, analysis and reporting of interventions in the lives of inactive or sedentary individuals has produced equivocal results. However, several social and environmental factors have systematically emerged as determinants of physical activity in adults. In ethnic minorities, the removal of barriers such as unaffordable facilities and unavailable childcare, high crime rates, fear for personal safety and culturally inappropriate activities are of primary importance. Social support from family, peers, communitiesand healthcare providers has resulted in modest improvements across cultures, ages and genders in selected settings, but the definition of specific interventions and their outcomes deserve additional attention. Longitudinal studies indicate that components of physical fitness are relatively transitory, with low to modest correlations between physical activity and measures of physical fitness in childhoodand adolescence and in adulthood. Attempts to explain the activity behaviour of adults by applying various theories in programmes of intervention have also producedmixed results. Successful interventions tailor programmes to individual needs, account for personal levels of fitness, allow for personal control of the activity and its outcomes, and provide for social support by family, peers and communities. The initiation and maintenance of regular physical activity in adults depends on a multitude of biological and sociocultural variables that demand attention across thelifespan. [References: 246]
<106>Unique Identifier 11836201
Page 53

201-400.txtAuthors Bryant LL. Shetterly SM. Baxter J. Hamman RF.Institution Department of Preventive Medicine and Biometrics, University of Colorado School ofMedicine, 4200 East Ninth Avenue, Box C245, Denver, CO 80262, USA.Title Changing functional status in a biethnic rural population: the San Luis Valley Health and Aging Study.Source American Journal of Epidemiology. 155(4):361-7, 2002 Feb 15.Abstract The San Luis Valley Health and Aging Study, was designed to examine Hispanic versus non-Hispanic White differences in prevalence and incidence of aging-related outcomes in a rural population (1,358 community dwellers and 75 nursing home residents). Data presented here were gathered between 1993 and 1997. Previously reported analyses identified greater prevalence of functional dependence in daily living activities among Hispanic elderly, especially females, than among non-Hispanic White elderly. This analysis explored the degree to which incident changes explain these patterns. Comparisons of incidence, recovery, and mortality rates after 22 months revealed no significant ethnic differences, although trends were as hypothesized: greater Hispanic incidence, lower Hispanic recovery rates, andless Hispanic mortality. Overall age-adjusted incidence (activities of daily living = 9.5; instrumental activities of daily living = 15.1 per 100 person-years) exceededreports from most other studies, while rates of recovery (activities of daily living= 14.5; instrumental activities of daily living = 9.9) and mortality (4.8 among community dwellers; 6.7 including nursing home residents) were similar to those of other reports. Patterns of new dependence, recovery, and mortality did not increase the previously observed disparity. Greater prevalent disability in the Hispanic cohort, especially in women, may reflect a reservoir accumulated during younger years and related to culture and socioeconomic status as well as to older age.
<107>Unique Identifier 11834670Authors Sirio CA. Tajimi K. Taenaka N. Ujike Y. Okamoto K. Katsuya H.Institution Department of Anesthesiology and Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA. [email protected] A cross-cultural comparison of critical care delivery: Japan and the United States.[see comment][erratum appears in Chest. 2003 Mar;123(3):967].Source Chest. 121(2):539-48, 2002 Feb.Abstract OBJECTIVE: To compare the utilization and outcomes of critical care services in a cohort of hospitals in the United States and Japan. DESIGN: Prospective data collection on 5,107 patients and detailed organizational characteristics from each of the participating Japanese study hospitals between 1993 and 1995, with comparisons made to prospectively collected data on the 17,440 patients included in the US APACHE (acute physiology and chronic health evaluation) III database. SETTING: Twenty-two Japanese and 40 US hospitals. PATIENTS: Consecutive, unselected patients from medical, surgical, and mixed medical/surgical ICUs. MEASUREMENTS: Severity of illness, predicted risk of in-hospital death, and ICU and hospital length of stay (LOS) were assessed using APACHE III. Japanese ICU directors completed a detailed survey describing their units. MAIN RESULTS: US and Japanese ICUs have a similar array of modalities available for care. Only 1.0% (range, 0.56 to 2.7%) of beds in Japanese hospitals were designated as ICUs. The organization of the Japanese and US ICUs varied by hospital, but Japanese ICUs were more likely to be organized to care for heterogeneous diagnostic populations. Sample case-mix differences reflect different disease prevalence. ICU utilization for women is significantly lower (35.5% vs 44.8% of patients) and there were relatively fewer
Page 54

201-400.txtpatients > or = 85 years old in the Japanese ICU cohort (1.2% vs 4.6%), despite a higher per capita rate of individuals > or = 85 years old in Japan. The utilization of ICUs for patients at low risk of death significantly less in Japan (10.2%) than in the United States (12.9%). The APACHE III score stratified patient risk. Overall mortality was similar in both national samples after accounting for differences in hospital LOS, utilizing a model that was highly discriminating (receiver operating characteristic, 0.87) when applied to the Japanese sample. The application of a US-based mortality model to a Japanese sample overestimated mortality across all butthe highest (> 90%) deciles of risk. Significant variation in expected performance was noted between hospitals. Risk-adjusted ICU LOS was not significantly longer in Japan; however, total hospital stay was nearly twice that found in the US hospitals,reflecting differences in hospital utilization philosophies. CONCLUSIONS: Similar high-technology critical care is available in both countries. Variations in ICU utilization reflect differences in case-mix and bed availability. Japanese ICU utilization by gender reflects differences in disease prevalence, whereas differences in utilization by age may reflect differences in cultural norms regarding the limits of care. Such differences provide context from which to assess the delivery of care across international borders. Miscalibration of predictive models applied to international data samples highlight the impact that differences in resource use and local practice cultures have on outcomes. Models may require modification in order to account for these differences. Nevertheless, with large databases, it is possible to assess critical care delivery systems between countriesaccounting for differences in case-mix, severity of illness, and cultural normative standards facilitating the design and management such systems.
<108>Unique Identifier 11815493Authors Brown SA. Garcia AA. Kouzekanani K. Hanis CL.Institution School of Nursing, The University of Texas at Austin, P.O. Box 7996, Austin, TX, USA. [email protected] Culturally competent diabetes self-management education for Mexican Americans: theStarr County border health initiative.Source Diabetes Care. 25(2):259-68, 2002 Feb.Abstract OBJECTIVE: To determine the effects of a culturally competent diabetes self-management intervention in Mexican Americans with type 2 diabetes. RESEARCH DESIGN AND METHODS: A prospective, randomized, repeated measures study was conductedon the Texas-Mexico border in Starr County. A total of 256 randomly selected individuals with type 2 diabetes between 35 and 70 years of age, diagnosed with type2 diabetes after 35 years of age, and accompanied by a family member or friend were included. The intervention consisted of 52 contact hours over 12 months and was provided by bilingual Mexican American nurses, dietitians, and community workers. The intervention involved 3 months of weekly instructional sessions on nutrition, self-monitoring of blood glucose, exercise, and other self-care topics and 6 months of biweekly support group sessions to promote behavior changes. The approach was culturally competent in terms of language, diet, social emphasis, family participation, and incorporation of cultural health beliefs. Outcomes included indicators of metabolic control (HbA(1c) and fasting blood glucose), diabetes knowledge, and diabetes-related health beliefs. RESULTS: Experimental groups showed significantly lower levels of HbA(1c) and fasting blood glucose at 6 and 12 months and higher diabetes knowledge scores. At 6 months, the mean HbA(1c) of the experimental subjects was 1.4% below the mean of the control group; however, the mean level of the experimental subjects was still high (>10%). CONCLUSIONS: This study confirms the effectiveness of culturally competent diabetes self-management education on improving health outcomes of Mexican Americans, particularly for those individuals with HbA(1c) levels >10%.
Page 55

201-400.txt
<109>Unique Identifier 11808400Authors Jones ME. Bond ML. Gardner SH. Hernandez MC.Institution University of Texas, Arlington School of Nursing, 411 S. Nedderman Drive, Box 19407, Arlington, TX 76019-0407, USA. [email protected] A call to action. Acculturation level and family-planning patterns of Hispanic immigrant women.Source MCN, American Journal of Maternal Child Nursing. 27(1):26-32; quiz 33, 2002 Jan-Feb.Abstract PURPOSE: To describe family-planning patterns of Hispanic women and to determine their relationship to acculturation level and to selected maternal demographic, pregnancy, and infant birth indices. DESIGN: Descriptive correlational. METHODS: A convenience sample of 376 Hispanic women was drawn from prenatal clinics in a large,public teaching hospital in the Southwest United States. Acculturation status was assessed during the prenatal period using the Acculturation Rating Scale for MexicanAmericans II. Maternal data concerning pregnancy, infant birth, postpartum, and family planning were abstracted from the hospital record. Data were analyzed using descriptive, correlational, and multiple regression procedures. RESULTS: Most women were of Mexican origin, first generation in the United States, and oriented toward traditional Mexican cultural beliefs and values. Most were married, had less than aneighth-grade education, and experienced a first or second healthy pregnancy with healthy birth outcomes. Over 66% of the women returned for at least one visit in thefirst year postbirth; compliance at 1 yr declined to 28%. Five variables were significantly correlated with family-planning visit compliance: number of pregnancies, generation in the United States, acculturation level, trimester of first prenatal visit, number of prenatal visits, and gestational age of newborn. CLINICAL IMPLICATIONS: Nurses are in a pivotal position to educate the Mexican immigrant woman about healthcare for herself and for her family, but need to recognize cultural influences on family-planning behavior. Effective interventions build on existing knowledge, beliefs, and practices of traditional immigrant women. It is important to include the generation in the United States as an indicator of adherence to traditional values and beliefs.
<110>Unique Identifier 11796429Authors Reich JM.Institution Center for Health Research, Kaiser Permanente, Northwest Region, Portland, OR, USA. [email protected] Mortality of intrathoracic sarcoidosis in referral vs population-based settings: influence of stage, ethnicity, and corticosteroid therapy.Source Chest. 121(1):32-9, 2002 Jan.Abstract STUDY OBJECTIVES: To compare the sarcoidosis mortality in referral settings (RS) and population-based settings (PS), and to identify the contribution of stage, ethnicity, and corticosteroid therapy (CST) to their disparate outcomes. DESIGN: Allobservational studies identified in a MEDLINE search and bibliographic review published in the English language since 1960 dealing with the course and prognosis of sarcoidosis in large, unsorted, adult, ambulatory RS and PS providing long-term follow-up were reviewed and subjected to meta-analysis. Measurements and results: Sarcoidosis mortality in RS (4.8%), in which 17% of patients had the most
Page 56

201-400.txtunfavorable prognosis as judged by stage (stage III), was 10-fold that reported in PS (0.5%), in which 11% of patients were identified at this stage. The magnitude of this disparity could not be accounted for solely by adverse selection, as indicated by stage or by ethnicity. Patients in RS received CST with sevenfold the frequency of PS, and its provision was highly correlated with stage-normalized mortality. CONCLUSION: The prognosis of patients with intrathoracic sarcoidosis in PS is far more favorable than that obtained in RS. Sarcoidosis mortality is largely independent of ethnicity. The possibility cannot be excluded that excessive employment of CST may unfavorably influence the long-term course of the disease in some individuals.
<111>Unique Identifier 11789625Authors Walsh ME. Katz MA. Sechrest L.Institution Southern Arizona Veterans Affairs Health Care System, Tucson, USA. [email protected] Unpacking cultural factors in adaptation to type 2 diabetes mellitus.Source Medical Care. 40(1 Suppl):I129-39, 2002 Jan.Abstract BACKGROUND: Race and ethnicity are used as predictors of outcome in health services research. Often, however, race and ethnicity serve merely as proxies for the resources, values, beliefs, and behaviors (ie, ecology and culture) that are assumed to correlate with them. "Unpacking" proxy variables-directly measuring the variables believed to underlie them-would provide a more reliable and more interpretable way of looking at group differences. OBJECTIVE: To assess the use of ameasure of ecocultural domains that is correlated with ethnicity in accounting for variance in adherence, quality of life, clinical outcomes, and service utilization. DESIGN: A cross-sectional observational study. PARTICIPANTS: Twenty-six Hispanic and29 non-Hispanic white VA primary care patients with type 2 diabetes mellitus. MEASURES: The independent variables were patient ethnicity and a summed score of ecocultural domains representing patient adaptation to illness. The outcomes were adherence to treatment, health-related quality of life, clinical indicators of disease management, and utilization of urgent health care services. RESULTS: Patientadaptation was correlated with ethnicity and accounted for more variance in all outcomes than did ethnicity. The unique variance accounted for by adaptation was small to moderate, whereas that accounted for by ethnicity was negligible. CONCLUSIONS: It is possible to identify and measure ecocultural domains that better account for variation in important health services outcomes for patients with type 2diabetes than does ethnicity. Going beyond the study of ethnic differences alone andmeasuring the correlated factors that play a role in disease management can advance understanding of the phenomena involved in this variation and provide better direction for service design and delivery.
<112>Unique Identifier 11789623Authors Collins TC. Johnson M. Henderson W. Khuri SF. Daley J.Institution Houston Center for Quality of Care and Utilization Studies, Houston VA Medical Center, Texas, USA. [email protected] Lower extremity nontraumatic amputation among veterans with peripheral arterial disease: is race an independent factor?.Source Medical Care. 40(1 Suppl):I106-16, 2002 Jan.
Page 57

201-400.txtAbstract OBJECTIVES: To determine if race/ethnicity is independently associated with an increased risk for nontraumatic lower extremity amputation versus lower extremity bypass revascularization among patients with peripheral arterial disease (PAD). METHODS: Data were analyzed from the National VA Surgical Quality Improvement Program (NSQIP) and from the Veterans Affairs Patient Treatment File (PTF). Race/ethnicity was defined as non-Hispanic white, black, or Hispanic. Variables thatwere univariately associated (P < or = 0.05) with the outcome of amputation were placed into a multiple logistic regression model to determine independent predictorsfor the dependent variable, lower extremity amputation versus lower extremity bypassrevascularization. RESULTS: Three thousand eighty-five lower extremity amputations and 8409 lower extremity bypass operations were identified. Among all cases included, there were 416 Hispanic patients (3.6%), 2337 black patients (20.3%), and 8741 non-Hispanic white patients (76.1%). Among all variables within the model, Hispanic and black race were each associated with a greater risk for amputation thana history of rest pain/gangrene (Hispanic race 1.4, 95% CI 1.1, 1.9; black race 1.5,95% CI 1.4, 1.7; rest pain/gangrene 1.1, 95% CI 1.0, 1.3). The final model had a c statistic of 0.83. CONCLUSION: Hispanic race and black race were independent risk factors for lower extremity amputation in patients with PAD. Although the burden of certain atherosclerotic risk factors (eg, diabetes and hypertension) is higher in minority patients, the impact of this burden does not account for the increased riskfor the outcome of lower extremity amputation in these two populations. Further research is needed to better understand the reason(s) why race/ethnicity is independently associated with poor outcomes in PAD.
<113>Unique Identifier 11789632Authors Rosenheck R. Fontana A.Institution Department of Veterans Affairs Northeast Program Evaluation Center, West Haven, Connecticut 06516, USA.Title Black and Hispanic veterans in intensive VA treatment programs for Posttraumatic Stress Disorder.Source Medical Care. 40(1 Suppl):I52-61, 2002 Jan.Abstract OBJECTIVES: This study examines differences in treatment process and outcomes among minority veterans treated in specialized intensive VA programs for war-relatedPosttraumatic Stress Disorder (PTSD). DESIGN: A concurrent panel study assessing four different types of intensive PTSD treatment program. SUBJECTS: Black (n = 2,906; 23.4%), Hispanic (n = 661, 5.3%), and white veterans. METHODS: Hierarchical linear modeling was used to compare black and Hispanic veterans with white veterans on admission characteristics, treatment process, and outcomes, overall, and to determine whether treatment in three newer types of programs, each designed to improve efficiency, was associated with in changes in minority group experiences. RESULTS: At the time of program admission, black patients had less education, were less likely to be married or to receive VA compensation, and had more severe alcoholand drug problems, but had less severe PTSD symptoms than either white patients or Hispanic patients. There were no differences among groups on 8 of 11 measures of treatment process or outcome but black patients showed greater improvement than white patients on one measure of PTSD symptoms and Hispanic patients were more satisfied with their treatment than white patients although they showed smaller gains in employment income. There were few changes associated with newer program types: gains for minorities were observed on three measures and losses on two. CONCLUSIONS: Using data from a large national sample, this study found little evidence of systematic differences in either treatment process or outcome between white, black, and Hispanic patients overall, or in association with the implementation of more efficient program types.
Page 58

201-400.txt
<114>Unique Identifier 11789630Authors Horner RD. Oddone EZ. Stechuchak KM. Grambow SC. Gray J. Khuri SF. HendersonWG. Daley J.Institution VA Epidemiologic Research and Information Center, Center for Health Services Research in Primary Care, Stroke QUERI Program, Durham, North Carolina, USA. [email protected] Racial variations in postoperative outcomes of carotid endarterectomy: evidence from the Veterans Affairs National Surgical Quality Improvement Program.Source Medical Care. 40(1 Suppl):I35-43, 2002 Jan.Abstract CONTEXT: Black patients and Hispanic patients receive carotid endarterectomy (CEA)at lower rates than white patients. It is unclear whether worse surgical outcomes are influencing clinical decision-making regarding use of the operation among minority group patients. OBJECTIVE: To determine if there are racial differences in postoperative outcomes for patients undergoing CEA at Veterans Affairs (VA) medical centers. DESIGN: Secondary analysis of data from an ongoing, prospective study on surgical quality and outcomes in the VA health care system. SETTING: One hundred thirty-two VA Medical Centers that were part of the VA National Surgical Quality Improvement Program. PATIENTS: A cohort of 6551 men (91.4% white, 5.3% black, and 3.3% Hispanic) who had CEA performed between October 1, 1994 and September 30, 1997.MAIN OUTCOME MEASURES: Primary outcomes were stroke or death and stroke, myocardial infarction (MI), or death within 30 days of the operation. RESULTS: Thirty-day postoperative rates of stroke or death and of stroke, MI, or death were generally low for all racial/ethnic groups, ranging between 2.6% and 6.5%. Within clinical states that define indications for CEA, rates were also low (1.6% to 3.2%) among asymptomatic patients across racial/ethnic groups. However, among patients with transient ischemic attack (TIA), Hispanic patients had significantly worse outcomes than white patients with a postoperative rate of stroke or death of 10.5% (P < 0.05)and stroke, MI, or death of 13.2% (P < 0.05) compared with 3.1% to 3.5% for white patients. Hispanic patients did not differ from black patients for stroke, death/stroke, death, or MI. CONCLUSION: Rates of major postoperative complications after CEA are low within the VA and similar across racial/ethnic groups with the possible exception of Hispanic men with TIA. Further investigation of this elevated complication rate among Hispanic men with TIA may be warranted.
<115>Unique Identifier 11772766Authors Gould JB. Chavez G. Marks AR. Liu H.Institution School of Public Health, University of California, 309 Earl Warren Hall, Berkeley,CA 94720-7630, USA. [email protected] Incomplete birth certificates: a risk marker for infant mortality.Source American Journal of Public Health. 92(1):79-81, 2002 Jan.Abstract OBJECTIVES: This study assessed the relationship between incomplete birth certificates and infant mortality. METHODS: Birth certificates from California (n = 538 945) were assessed in regard to underreporting of 13 predictors of perinatal outcomes and mortality. RESULTS: Of the birth certificates studied, 7.25% were incomplete. Underreporting was most common in the case of women at high risk for poor perinatal outcomes and infants dying within the first day. Increasing numbers of unreported items were shown to be associated with corresponding increases in
Page 59

201-400.txtneonatal and postneonatal mortality rates. CONCLUSIONS: Incomplete birth certificates provide an important marker for identifying high-risk women and vulnerable infants. Because data "cleaning" will result in the removal of mothers and infants at highest risk, birth certificate analyses should include incomplete records.
<116>Unique Identifier 11755800Authors Koniak-Griffin D. Anderson NL. Brecht ML. Verzemnieks I. Lesser J. Kim S.Institution UCLA School of Nursing, Box 956919, Los Angeles, CA 90095-6919, USA. [email protected] Public health nursing care for adolescent mothers: impact on infant health and selected maternal outcomes at 1 year postbirth.Source Journal of Adolescent Health. 30(1):44-54, 2002 Jan.Abstract PURPOSE: To compare effects of an early intervention program (EIP) of intense homevisitation by public health nurses (PHNs) with effects of traditional public health nursing care (TPHN) on infant health and selected maternal outcomes of adolescent mothers. METHODS: EIP adolescents (N = 102) received preparation-for-motherhood classes and individual home visits (from pregnancy through 1 year postpartum) from PHNs employed in a county health department. Participants were predominantly Latina (64%) and African-American (11%) and from impoverished backgrounds. Infant health outcomes were determined based on medical record data; interviews and standardized questionnaires evaluated other program effects (e.g., maternal educational achievement and psychological status). Data were analyzed using Chi-square and repeated measures ANOVA. RESULTS: Infants of EIP mothers experienced significantly fewer total days (n = 74) and actual episodes (n = 14) of hospitalization during thefirst year of life than those receiving TPHN (n = 154, n = 24, respectively). Similarly, positive program effects were found for immunization rates. There were nogroup differences in emergency room visits or repeat pregnancy rates. Alcohol, tobacco, and marijuana use significantly increased from pregnancy through 1 year postpartum in both groups but remained markedly lower than rates prior to pregnancy (lifetime rates). CONCLUSIONS: These findings demonstrate the positive effects of a PHN home visitation program on health outcomes for children of adolescent mothers. Days of infant hospitalization were substantially reduced and immunization rates increased during the first year of life for children of EIP mothers. Greater effortsneed to be directed toward preventing repeat pregnancy and return to substance use following childbirth in at-risk adolescent mothers.
<117>Unique Identifier 12180523Authors Mokuau N. Hishinuma E. Nishimura S.Institution School of Social Work, University of Hawai'i at Manoa, Honolulu 96822, USA. [email protected] Validating a measure of religiousness/spirituality for Native Hawaiians.Source Pacific Health Dialog. 8(2):407-16, 2001 Sep.Abstract Religiousness and spirituality are integral to the human experience. There is emerging literature that shows that religiousness and spirituality are associated with various mental and physical health outcomes. Yet, the development of measures to accurately assess these phenomena in health settings is still in its early
Page 60

201-400.txtstages. The difficulties in developing standardized definitions and measures relate to varying interpretations of religiousness and spirituality, a reluctance to utilize a scientific approach to understand an existential and personal experience, and multicultural distinctions. The potential for designing health interventions in which religiousness and spirituality are integrated rests upon the development of measures that are psychometrically sound. This paper reports on preliminary researchthat empirically assesses one measure of religiousness and spirituality for Native Hawaiians--a group besieged with an array of health problems. The measure is the Brief Multidimensional Measure of Religiousness/Spirituality (BMMRS) developed by the National Institute on Aging and the Fetzer Institute. This instrument has shown to have appropriate reliability and validity scores. A modified BMMRS was administered to 15 Native Hawaiians who underwent a cultural intervention of exercise, diet, and education in a program called Uli'eo Koa (warrior fitness). The BMMRS was slightly modified based on the literature and earlier research to be more specific to Native Hawaiians. Overall, measures of internal consistency supported the reliability of the BMMRS. The strongest subscales included the domains of "dailyspiritual experiences," "religious and spiritual coping," and "religious support." Low internal consistency estimates for the items, "watches/listens to religious programs," "family makes demands," and "significant loss in faith," suggest that these items do not measure the same concept for participants. Although the intercorrelations among the subscales were generally low and with wide variability, 10 of the 17 subscales/single items were moderately to highly correlated with one another, indicating concurrent validity. These subscales, some of which assessed, "daily spiritual experiences," "religious and spiritual coping," and "organizationalreligiousness," suggest that core ideas on spirituality and religiousness for these participants, broadly reflect both "personal" and "organizational" viewpoints. Caution should be used in interpreting the results of the study because of limitations in the study's design. However, despite these limitations in design, this study provides empirical support for future research on religiousness and spirituality for Native Hawaiians.
<118>Unique Identifier 12180520Authors Palafox NA. Buenconsejo-Lum L. Ka'ano'i M. Yamada S.Institution Department of Family Practice and Community Health, John A. Burns School of Medicine, University of Hawai'i at Manoa, Mililani 96789, USA. [email protected] Cultural competence: a proposal for physicians reaching out to Native Hawaiian patients.Source Pacific Health Dialog. 8(2):388-92, 2001 Sep.Abstract Many physicians of Native Hawaiian ancestry, as well as others, have noted a cultural gap between themselves and their Native Hawaiian patients. This cultural gap could potentially lead to discordance in the physician-patient relationship, andin turn, result in less than adequate therapeutic outcomes. Native Hawaiian physicians and those who treat Native Hawaiian patients are seeking ways to improve therapeutic relationships. Developing cultural competency in Native Hawaiian physicians and those who treat Native Hawaiian patients may be expected to improve therapeutic relationships. Principles of cultural competency, including increasing awareness of self and others, enhancing one's cultural knowledge base, and developing skills to communicate effectively, could be applied to physician-patient encounters with Native Hawaiian patients. The principles and skills of cultural competency could be learned during the formal and continuing medical education process. Developing an educational system that promotes cultural competency in physicians is necessary to address the health needs of Native Hawaiians and other diverse populations in Hawai'i.
Page 61

201-400.txt
<119>Unique Identifier 12166434Authors Pacquiao DF.Title Ethics and cultural diversity--a framework for decision-making.Source Bioethics Forum. 17(3-4):12-7, 2001.Abstract Believing that healthcare outcomes will be more satisfying if the patients' cultural knowledge and values are understood and integrated appropriately in care planning, the author proposes a culturally competent ethical decision making model based on human rights--the fundamental right of individuals, families, groups, and populations to healthcare that is meaningful, supportive, and beneficial--and a reconceptualization of ethical principles to include the values and assumptions of clients. The ideal result is culturally congruent healthcare in which practitioners learn about their clients' lifeways and work with them to find satisfying ways to resolve clinical and ethical issues.
<120>Unique Identifier 11080607Authors Jones JA. Wahlgren DR. Meltzer SB. Meltzer EO. Clark NM. Hovell MF.Institution Center for Behavioral Epidemiology and Community Health, Graduate School of PublicHealth, San Diego State University, San Diego, CA, USA.Title Increasing asthma knowledge and changing home environments for Latino families with asthmatic children.Source Patient Education & Counseling. 42(1):67-79, 2001 Jan.Abstract We tested an asthma education program in 204 underserved Latino families with an asthmatic child. The education program consisted of one or two sessions delivered ineach family's home in the targeted participant's preferred language by a bilingual, bicultural educator. We encouraged, but did not require, attendance by the child. The curriculum was culturally-tailored, and all participants received education on understanding asthma, preventing asthma attacks, and managing asthma. Outcomes included change in asthma knowledge and change in home environment asthma managementprocedures. Asthma knowledge increased significantly (39 to 50% correct from pre- topost-test, P < 0.001) and participants made significant changes to the child's bedroom environment (mean number of triggers decreased from 2.4 to 1.8, P < 0.001; mean number of controllers increased from 0.7 to 0.9, P < 0.001). The results support the value of asthma education and its importance in the national agenda to reduce health disparities among minorities.
<121>Unique Identifier 11975795Authors Longhurst JC.Title Alternative approaches to the medical management of cardiovascular disease: acupuncture, electrical nerve, and spinal cord stimulation.[comment].Source Heart Disease. 3(4):215-6, 2001 Jul-Aug.
Page 62

201-400.txt<122>Unique Identifier 11885117Authors Jones ME. Kubelka S. Bond ML.Institution Center for Hispanic Studies in Nursing and Health, University of Texas, Arlington School of Nursing, USA.Title Acculturation status, birth outcomes, and family planning compliance among Hispanic teens.Source Journal of School Nursing. 17(2):83-9, 2001 Apr.Abstract This study examined acculturation status, selected demographic and pregnancy indices, and the relationship to birth outcomes and family planning patterns among aconvenience sample of 63 Hispanic adolescents aged 13 to 19 years and attending community-based prenatal clinics. Findings suggest that Hispanic teenagers who are the first generation in the United States and traditional in their world view are compliant with prenatal and postpartum care and have healthy babies and birth outcomes. Gravidity and gestational age of the infant were significant predictors ofbirth weight, accounting for 30% of the variability in birth weight. Generation in the United States accounted for 8% of the variance in family planning compliance. Higher gravidity was associated with increased infant birth weight and a decreased likelihood for return for family planning visits during the 1st year postbirth. Teens who were first generation in the United States were more likely to return for family planning visits during the 1st year. School nurses are in a pivotal position to design intervention programs that build on traditional cultural prescriptions forhealthy behaviors during and after pregnancy.
<123>Unique Identifier 11876350Authors Hanna L.Institution La Trobe University, Shepparton, Australia.Title Continued neglect of rural and remote nursing in Australia: the link with poor health outcomes.Source Australian Journal of Advanced Nursing. 19(1):36-45, 2001 Sep-Nov.Abstract Difficulties facing Australian rural and remote nurses first emerged decades ago and recent Australian Federal Government rural health strategies have promised improvements in health outcomes. However closer scrutiny of the funding allocation supporting these claims reveals that although nurses provide the majority of health care, they receive only a small fraction of funding support. Successive rural healthstrategies have continued to overlook nurses' concerns regarding the nurse-practice environment interface. This persistent lack of political support stifles organisational support for the nursing role, resulting in frustration, resignation and diminished health care delivery. Meanwhile, rural and remote population health outcomes fail to show signs of improvement.
<124>Unique Identifier 11876189Authors Sambo BH. Strong Heart Study Investigators.Institution Center for American Indian Health Research, College of Public Health, University
Page 63

201-400.txtof Oklahoma, Oklahoma City 73190, USA. [email protected] The Strong Heart Study: interaction with and benefit to American Indian communities.[republished from Am J Med Sci. 2001 Nov;322(5):284-7; PMID: 11721803].Source American Journal of the Medical Sciences. 322(5):282-5, 2001 Nov.Abstract The Strong Heart Study (SHS) is a large, multi-community study to investigate the high incidence of cardiovascular disease (CVD) among American Indians and to improvelong-term health outcomes within the communities. CVD is the No. 1 cause of death for three geographically and culturally diverse American Indian populations. The SHSinvestigated the prevalence and incidence of CVD as well as the distribution of riskfactors in members of 13 American Indian tribes in Oklahoma, Arizona, and (as one region) North and South Dakota. The SHS enrolled more than 4500 participants rangingin age from 45 to 74 years. During the three-phase study, which began with baseline examinations from 1989 through 1991 and concluded in 1999, participants received medical examinations in each phase. To build trust and cooperation, SHS investigators worked closely with tribal leaders and community members, including establishing empowered committees and hiring community members for jobs within the study. As a result of such cooperation, the SHS maintained retention rates of about 90% across all three phases. Benefits to tribal communities also included health care improvements and education for healthy lifestyles. The SHS could serve as a model for similar studies of American Indians or other minority groups.
<125>Unique Identifier 11863143Authors Palazzo MO.Institution Georgetown University Hospital, Washington, DC 20007, USA. [email protected] Teaching in crisis. Patient and family education in critical care. [Review] [23 refs]Source Critical Care Nursing Clinics of North America. 13(1):83-92, 2001 Mar.Abstract Although the critical care setting is not always a positive teaching environment, it is possible to achieve the goal of optimal patient and family education. The critical care nurse must understand the unique learning needs of patients and families who are experiencing a life crisis a recognize that there are substantial obstacles to overcome to educate in this setting. In addition, it takes experience and resources to develop the teaching skills of the bedside nurse, so that those teachable moments are easily recognized and suitably used to give patients and family members valuable information in small doses. The advanced practice nurse is an essential nursing resource who can spearhead the development of teaching skills for all members of the health care team. In addition, the advanced practice nurse isa clinical expert who can assess the educational needs of patients and their families and provide more detailed and individualized health information from a different perspective. Achieving good patient and family education outcomes is possible when patient care continuity is a priority and the advanced practice nurse is an active part of the nursing team. Exploring the use of new technologies and resources to meet patient and family education needs is absolutely necessary. As hospitals continue to evolve and react to the financial demands placed on them, nursing leadership and critical care nurses will need to articulate clearly all of the essential components of patient care, including patient and family education. Inkeeping with the rich nursing tradition of patient and family education, critical care nurses and advanced practice nurses have the opportunity to demonstrate their unique teaching skills and continue to promote health education as a priority of patient care. [References: 23]
Page 64

201-400.txt
<126>Unique Identifier 11837358Authors Auslander G. Dobrof J. Epstein I.Institution Hebrew University, School of Social Work, Mt Scopus, Jerusalem, Israel. [email protected] Comparing social work's role in renal dialysis in Israel and the United States: the practice-based research potential of available clinical information.Source Social Work in Health Care. 33(3-4):129-51, 2001.Abstract This paper demonstrates the use of clinical data-mining in a study of social work interventions with dialysis patients in two countries, the US and Israel. We aimed to examine the role of social workers in improving kidney patient outcomes and to determine the potential of readily available patient information for studying this process. The findings showed considerable differences between the patient samples inboth countries, as far as the socio-demographic background was considered. In spite of this, there were numerous similarities in the type of psycho-social problems and reactions, as well as the social workers' interventions. Differences which arose in various patient states and outcomes were examined in light of variations in the health care systems and socio-cultural contexts of renal dialysis in both sites.
<127>Unique Identifier 11813732Authors Choi NG. Schlichting-Ray L.Institution Portland State University, USA.Title Predictors of transitions in disease and disability in pre- and early-retirement populations.Source Journal of Aging & Health. 13(3):379-409, 2001 Aug.Abstract OBJECTIVES. This study analyzed rates of prevalence and incidence of, and transitions in, disease and disability statuses of those aged 51 to 61 years and thepredictors of the transition outcomes-remaining free of disease or disability, getting better, or getting worse-over a 2-year period. METHODS. Data from the 1992 and 1994 interview waves of the Health and Retirement Study were used for gender-separate binary and multinomial logistic regression analyses. RESULTS. Despite high prevalence and incidence rates of chronic disease and functional limitations, the improvement rates in disabilities were also high. For both genders,age, years of education, health-related behaviors, and comorbidity factors were significant predictors of the transition outcomes. DISCUSSION. The significance of health-related behaviors as predictors of transitions suggests that lifestyle factors may have a bigger influence on this age group than on older groups.
<128>Unique Identifier 11805981Authors Warden GL. Griffith JR.Institution Henry Ford Health System, Detroit, MI 48202, USA. [email protected] Ensuring management excellence in the health care system.
Page 65

201-400.txtSource Journal of Health Administration Education. Spec No:19-32, 2001.
<129>Unique Identifier 11781031Authors Rivas-Vazquez RA. Rivas-Vazquez A. Blais MA. Rey GJ. Rivas-Vasquez F. Jacobo M. Carrazana EJ.Institution Neurologic Center of South Florida and University of Miami School of Medicine, USA.Title Development of a spanish version of the Schwartz Outcome Scale-10: a brief mental health outcome measure.Source Journal of Personality Assessment. 77(3):436-46, 2001 Dec.Abstract The lack of culturally appropriate psychometric instruments for the assessment of cognitive and emotional functioning in minority populations has been a concern oftendiscussed in the assessment literature. With the increased focus on the measurement of outcome in mental health treatment, the lack of appropriate instruments for minorities has become readily apparent in this venue as well. We report on the Spanish translation of a brief and reliable measure of psychological health and well-being that has been shown to be sensitive to treatment outcomes. The original and Spanish translated versions of this measure are highly correlated, providing clinicians and organizations with a instrument that can be used for assessment of psychological well-being and treatment outcomes with Hispanic patients.
<130>Unique Identifier 11775302Authors Domian EW.Institution University of Kansas, School of Nursing, 3901 Rainbow Boulevard, Kansas City, KS 66160-7502, USA. [email protected] Cultural practices and social support of pregnant women in a northern New Mexico community.Source Journal of Nursing Scholarship. 33(4):331-6, 2001.Abstract PURPOSE: To describe the experience of social support in Hispanic families during pregnancy. DESIGN: Ethnographic investigation, conducted from November 1995 to November 1997 in Rio Arriba County of northern New Mexico. METHODS: Seventy-two transcribed verbatim interviews with Hispanic mothers, family members, and health care providers, along with fieldnotes from participant observation, historical data of the region, and area demographics comprised the data for qualitative analysis. FINDINGS: Pregnancy outcomes were positive because of a socialization process that helped pregnant Hispanic women and family members adapt and change to support the pregnancy. This mutual shaping helped reinforce the family structure, integrate cultural beliefs, define roles for both mother and family members, define the natureof mother-child and family-child relationships, and facilitate a positive process through a supportive orientation. CONCLUSIONS: Findings showed the dynamics and context of relationships that constituted social support conducive to healthy birth outcomes in Hispanic families of northern New Mexico. The findings were enlighteningconcerning the pregnancy process, role adaptation, integration of health care beliefs, and provided ideas for intervention models that might benefit pregnant women, infants, family members, community members, and health care professionals.
Page 66

201-400.txt
<131>Unique Identifier 11771906Authors Cicchetti D. Manly JT.Title Operationalizing child maltreatment: developmental processes and outcomes.Source Development & Psychopathology. 13(4):755-7, 2001 Fall.
<132>Unique Identifier 11771793Authors Murry VM. Bynum MS. Brody GH. Willert A. Stephens D.Institution Center for Family Research, Institute for Behavioral Research, University of Georgia, Athens 30602, USA. [email protected] African American single mothers and children in context: a review of studies on risk and resilience.Source Clinical Child & Family Psychology Review. 4(2):133-55, 2001 Jun.Abstract This paper presents a comprehensive review of research linking single-parent family structure to parenting processes, maternal well-being, and child developmental outcomes among African Americans. The approaches used to study these families, related methodological and conceptual concerns, and the factors linked to maternal well-being, effective parenting processes, family functioning, and child outcomes are addressed. Much work remains to be done on conceptualizing and assessing parenting processes among African Americans in general and single African American mothers in particular. Researchers must examine more carefully the circumstances that foster or impede successful parenting among these mothers. Studies also are needed to disentangle the interactions between economic stress and parenting behavior and to determine the extent to which the findings can be applied to middle-income single African American parents.
<133>Unique Identifier 11768147Authors Walker-Barnes CJ. Mason CA.Institution Department of Psychology, University of North Carolina at Chapel Hill, 27599-3270,USA. [email protected] Ethnic differences in the effect of parenting on gang involvement and gang delinquency: a longitudinal, hierarchical linear modeling perspective.Source Child Development. 72(6):1814-31, 2001 Nov-Dec.Abstract This study examined the relative influence of peer and parenting behavior on changes in adolescent gang involvement and gang-related delinquency. An ethnically diverse sample of 300 ninth-grade students was recruited and assessed on eight occasions during the school year. Analyses were conducted using hierarchical linear modeling. Results indicated that, in general, adolescents decreased their level of gang involvement over the course of the school year, whereas the average level of gang delinquency remained constant over time. As predicted, adolescent gang involvement and gang-related delinquency were most strongly predicted by peer gang involvement and peer gang delinquency, respectively. Nevertheless, parenting
Page 67

201-400.txtbehavior continued to significantly predict change in both gang involvement and gangdelinquency, even after controlling for peer behavior. A significant interaction between parenting and ethnic and cultural heritage found the effect of parenting to be particularly salient for Black students, for whom higher levels of behavioral control and lower levels of lax parental control were related to better behavioral outcomes over time, whereas higher levels of psychological control predicted worse behavioral outcomes.
<134>Unique Identifier 11746068Authors Keller C. Trevino RP.Institution University of Texas Health Science Center at San Antonio, School of Nursing, 7703 Floyd Curl Drive, San Antonio, TX 78284, USA.Title Effects of two frequencies of walking on cardiovascular risk factor reduction in Mexican American women.Source Research in Nursing & Health. 24(5):390-401, 2001 Oct.Abstract The beneficial effects of moderate-intensity exercise on cardiorespiratory fitnessand body composition are well documented, with the greatest health benefits reportedin sedentary individuals who engage in moderate levels of exercise. The published literature contains no quantification of the threshold of lower limits of beneficialexercise or estimates of benefits derived from lower exercise levels. The specific aim of this study was to compare the effects of two walking frequencies, holding intensity and duration constant, on blood lipids, body composition, and exercise maintenance regimens of Mexican American women. A quasi-experimental design, with two treatment groups and one comparison group, was used to explore the dose-responseeffects of low-intensity exercise on cardiovascular outcomes. Significant interactions were found between walking and total serum cholesterol and skin-fold sums. This study demonstrated the clinical efficacy of a low-intensity exercise regimen on cardiovascular risk factors and exercise adherence. Copyright 2001 John Wiley & Sons, Inc.
<135>Unique Identifier 11743841Authors Kagawa-Singer M. Blackhall LJ.Institution Commuity Health Sciences, University of California, Los Angeles School of Public Health and Asian American Studies, Los Angeles, CA, USA.Title Negotiating cross-cultural issues at the end of life: "You got to go where he lives".Source JAMA. 286(23):2993-3001, 2001 Dec 19.Abstract Culture fundamentally shapes how individuals make meaning out of illness, suffering, and dying. With increasing diversity in the United States, encounters between patients and physicians of different backgrounds are becoming more common. Thus the risk for cross-cultural misunderstandings surrounding care at the end of life is also increasing. Studies have shown cultural differences in attitudes towardtruth telling, life-prolonging technology, and decision-making styles at the end of life. Using 2 case studies of patients, one of an African American couple in the southern United States and the other of a Chinese-American family in Hawaii, we outline some of the major issues involved in cross-cultural care and indicate how the patient, family, and clinician can navigate among differing cultural beliefs,
Page 68

201-400.txtvalues, and practices. Skilled use of cross-cultural understanding and communicationtechniques increases the likelihood that both the process and outcomes of care are satisfactory for all involved.
<136>Unique Identifier 11763826Authors Balcazar H. Krull JL. Peterson G.Institution Department of Social and Behavioral Sciences, School of Public Health, University of North Texas, USA. [email protected] Acculturation and family functioning are related to health risks among pregnant Mexican American women.Source Behavioral Medicine. 27(2):62-70, 2001 Summer.Abstract The authors examined the independent and interactive effects of acculturation status and family cohesiveness on a series of psychosocial and medical risk factors of pregnancy among 500 women of Mexican origin. In general, both higher and lower levels of acculturation produced positive or negative psychosocial and healthcare consequences, and the operative relationships depended heavily on the particular outcome chosen. Higher levels of family cohesiveness tended to foster the most constructive health and psychosocial outcomes. However, in some circumstances higherlevels of family cohesiveness resulted in less coping and a lower quality of prenatal care for less acculturated women. An important implication of this study isthat psychosocial and health information can be obtained through assessments that identify different subgroups of Mexican American women and depend on women's level of acculturation and family cohesiveness. Culturally competent health practitioners or clinicians can conduct these assessments in a prenatal healthcare setting.
<137>Unique Identifier 11761636Authors Lauzon S. Corbiere M. Bonin JP. Bonsack C. Lesage AD. Ricard N.Institution Faculte des sciences infirmieres, Universite de Montreal, Montreal, CP 6128, Succursale Centre-ville, Montreal, QC H3C 3J7. [email protected] [Validation of the French version of the Health of the Nation Outcome Scales (HoNOS-F)]. [French]Source Canadian Journal of Psychiatry - Revue Canadienne de Psychiatrie. 46(9):841-6, 2001 Nov.Abstract OBJECTIVE: This study reports the validation of the French version of the Health of the Nation Outcome Scales (HoNOS-F), a questionnaire developed to measure health and social functioning of people with mental illness. METHOD: Once each statement was tested for readability, the scale was administered to 3 samples of people suffering from severe mental disorders to estimate its reliability and validity. More specifically, tests were run to establish the internal consistency, the stability, and the interrater reliability of the HoNOS-F. Confirmative factor analyses and mean differences according to age, sex, and diagnosis were also conducted to evaluate respectively construct- and criterion-related validity. RESULTS: Coefficients obtained from the various tests show that the scale is reliable only when the total score is used. The confirmatory factor analyses indicate that the observed data do not fit the 2 proposed models, a unidimensional model and a 4-dimension model. However, the scale did show criterion-related validity. CONCLUSIONS: Results of the present study converge with those obtained on
Page 69
201-400.txtthe original widely used English version. Therefore, we suggest that clinicians use the questionnaire by referring to each item separately and by considering such patient characteristics as age, sex, and diagnosis. We also suggest that researcherswishing to evaluate health and social functioning of persons with serious mental disorders use the total score. Caution is, however, warranted when interpreting the total score for a French-speaking population, because the factorial solution 1-dimension model did not prove to be satisfactory.
<138>Unique Identifier 11763302Authors Daniels IN. Harrell JP. Floyd LJ. Bell SR.Institution Department of Psychology, Howard University, Washington, DC 20059, USA.Title Hostility, cultural orientation, and casual blood pressure readings in African Americans.Source Ethnicity & Disease. 11(4):779-87, 2001 Fall.Abstract Evidence suggests that hostility correlates with blood pressure levels in African-American samples. However, some studies have reported an inverse relationship, while others have found the relationship between blood pressure and hostility to be positive. Other literature suggests health outcomes in general, and blood pressure in particular, are related to cultural orientation in African-American samples. In the present study, six casual measures of blood pressure and heart rate in a sample of 90 African-American college students were aggregated and correlated with measures of hostility and cultural orientation. Correlational and regression analyses revealed a weak positive relationship between hostility and systolic blood pressure. The relationships between the cardiovascular measures and cultural orientation were more consistent. The tendency to embrace mainstream Euro-American values, such as materialism, individuality, and competitiveness, was associated with more rapid heart rate and higher diastolic blood pressure levels for both men and women. The relationship between systolic blood pressure and cultural orientation emerged for men only. The findings encouragefurther research into the relationship between personality variables and cardiovascular activity in African-American samples.
<139>Unique Identifier 11763296Authors Shelton AJ. Lees E. Groff JY.Institution Epidemiology Discipline, University of Texas-Houston, School of Public Health TX 77030, USA. [email protected] Hysterectomy: beliefs and attitudes expressed by African-American women.Source Ethnicity & Disease. 11(4):732-40, 2001 Fall.Abstract OBJECTIVE: Racial/ethnic differences in the rates of hysterectomy have been noted historically. The aim of this study was to explore the beliefs and attitudes of African-American women regarding hysterectomy recommended for non-life threatening conditions. METHODS: Women, aged 30-65 years, were recruited from public health clinics and community agencies for participation in focus groups guided by a semi-structured questionnaire. Transcripts were analyzed both manually and using NUD*IST software. RESULTS: Thirty-eight women participated in six focus groups. Hysterectomy had been recommended for 15% of the women. Four categories and 11 themes emerged from the sessions. Categories included: definitions of hysterectomy
Page 70

201-400.txtand medical indications; resources consulted in the decision-making process; outcomes of hysterectomy; and interactions with the health care community. CONCLUSION: It is important to assess a patient's perceptions and preferences regarding treatment options. The women in this study advocated the delay or avoidance of surgery, or the use of alternative methods of treatment in lieu of hysterectomy for non-cancerous conditions. Physicians who recommend hysterectomy should consider the attitudes, beliefs, and knowledge of patients.
<140>Unique Identifier 11763295Authors Jenny AM. Schoendorf KC. Parker JD.Institution Infant and Child Health Studies Branch, National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland 20782, USA. [email protected] The association between community context and mortality among Mexican-American infants.Source Ethnicity & Disease. 11(4):722-31, 2001 Fall.Abstract Mexican-American infants have surprisingly low mortality rates, given their high-risk demographic characteristics. One explanation for this well-known paradox is the beneficial influence of a traditional Mexican cultural orientation. However, many studies have focused on individual, rather than contextual, markers of acculturation to explain the reasons for this paradox. This study incorporated community-level data into the analysis to further elucidate the Mexican paradox. Data from the National Linked Birth and Infant Death files for 1995-1997 were used to stratify infants born in counties of Arizona, California, New Mexico, and Texas into tertiles based on the proportion of Mexican births in each county. We calculated mortality rates for infants in each tertile. Logistic regression, with generalized estimating equations, was used to calculate odds ratios comparing infantmortality in low and medium concentration counties to high concentration counties. Odds ratios were adjusted for maternal age, education, parity, marital status, and maternal nativity status. Among Mexican-American infants, mortality rates ranged from 4.3 in counties with high proportions of Mexican births to 5.5 in counties withlow proportions of Mexican births. However, this association was limited to US-born mothers, whose rates ranged from 4.4 in high concentration counties to 7.0 in low concentration counties (adjusted OR, 1.56 [1.35-1.81]); a substantial proportion of that difference was due to lower birth-weight specific mortality among normal birth-weight infants (1.9 vs. 3.1 deaths/1,000 live births). Among infants with Mexico-born mothers, there was no association between community context and mortality (OR, 1.01). Residence in counties with high proportions of Mexican births had a positive influence on birth outcomes among women of Mexican origin born in theUnited States. Exposure to the Mexican culture may reinforce healthy behaviors that Mexican-American women may lose through acculturation.
<141>Unique Identifier 11761342Authors Wilcox S. Irwin ML. Addy C. Stolarczyk L. Ainsworth BE. Whitt M. Tudor-LockeC.Institution Department of Exercise Science, Norman J. Arnold School of Public Health, University of South Carolina, Columbia, SC 29208, USA. [email protected] Agreement between participant-rated and compendium-coded intensity of daily activities in a triethnic sample of women ages 40 years and older.
Page 71

201-400.txtSource Annals of Behavioral Medicine. 23(4):253-62, 2001 Fall.Abstract Participant-rated and compendium-coded intensity of daily physical activities werecompared in 148 African American, 144 Native American, 51 non-Hispanic White women ages 40 to 91 years who completed 4 days of activity records. For compendium-coded intensity, reported activities were classified as light (< 3 metabolic equivalents [METS]), moderate (3-6 METS), or vigorous (> 6 METS) using the Compendium of Physical Activities (1), whereas these categories were self-assigned for participant-rated intensity. Minutes per day (min/d) spent in activities at each intensity level were computed. Relative to compendium-coded min/d, participants reported significantly greater time spent in light (+10 min/d; p < .01) and vigorous(+17 min/d; p < .001) activities, and less time spent in moderate activities (-27 min/d; p <.001). Similarly, compendium-coded estimates yielded higher rates ofparticipants meeting Centersfor Disease Control and Prevention-American College ofSports Medicine and Surgeon General recommendations than participant-rated estimates(11-18% differences) but substantially lower rates meeting American College of Sports Medicine vigorous recommendations (22% difference). Further, 247 greater kilocalories per day were estimated based on compendium-coded intensity. Kilocalories per day estimates based on compendium codings were more highly associated with pedometer counts than those based on participant ratings (p < .05). Studypatterns were generally seen across all sample subgroups. Discrepancies betweenparticipant and compendium estimates are likely to be most meaningful in studies estimating energy expenditure as it relates to health outcomes and in studies estimating vigorous activities.
<142>Unique Identifier 11761281Authors Bird HR. Canino GJ. Davies M. Zhang H. Ramirez R. Lahey BB.Institution Department of Psychiatry, N.Y. State Psychiatric Institute/Columbia University, New York 10032, USA. [email protected] Prevalence and correlates of antisocial behaviors among three ethnic groups.Source Journal of Abnormal Child Psychology. 29(6):465-78, 2001 Dec.Abstract Using data from the MECA Study, this report examines the prevalence of Conduct Disorder (CD), Oppositional Defiant Disorder (ODD), and various levels of antisocialbehavior and their correlates among three ethnic groups: Hispanics, subdivided into Island Puerto Ricans and Mainland Hispanics; African Americans; and Mainland Non-Hispanic, Non-African Americans. Correlates considered include stressful life events, birth defects, low birth weight, learning difficulties, teen mothers, familyenvironment, marital adjustment, social competence, parental monitoring, and family relationships. Logistic regression was used to determine the association of outcomeswith individual correlates and of interaction terms with ethnicity. Differences between adjusted rates and observed rates of disorders and levels of antisocial behaviors are compared to estimate the extent to which each correlate explains the group differences in rates. Island Puerto Ricans had a lower prevalence of CD, ODD, and various levels of antisocial behavior than mainland Hispanics, African Americans, and non-Hispanic Whites. The lower prevalence appears to be associated with differences in the extent to which a number of these correlates are found on the island, the most salient being better family relations between the target children and their parents and siblings.
<143>Unique Identifier 11759305Authors
Page 72

201-400.txt Meade CD. Calvo A.Institution Interdisciplinary Oncology Program, University of South Florida, USA. [email protected] Developing community-academic partnerships to enhance breast health among rural and Hispanic migrant and seasonal farmworker women.Source Oncology Nursing Forum. 28(10):1577-84, 2001 Nov-Dec.Abstract PURPOSE/OBJECTIVES: To examine effective strategies for building community-academic partnerships for the promotion of breast cancer education and outreach among rural and Hispanic migrant and seasonal farmworker women, mostly fromMexican descent. DATA SOURCES: Published research and education articles and books, community-education models, personal experiences, and community key informant feedback. DATA SYNTHESIS: Effective community partnerships for enhanced education and outreach include a framework based on a network of partners with common goals, communication processes based on trust, and bilingual/bicultural and culturally competent staff. CONCLUSIONS: A sustainable community partnership can be achieved through systematic but flexible approaches to community planning. Involvement of community members in the development and implementation of education and screening activities helps ensure that community needs are met. Relationships based on mutual respect are key. IMPLICATIONS FOR NURSING PRACTICE: Nurses can act as catalysts through community capacity building to create community-academic partnerships to reach medically underserved populations with cancer screening, outreach, and education through the delivery of strategies that are based on common goals.
<144>Unique Identifier 11721803Authors Sambo BH.Institution Center for American Indian Health Research, College of Public Health, University of Oklahoma, Oklahoma City 73190, USA. [email protected] The Strong Heart Study: interaction with and benefit to American Indian communities.[republished in Am J Med Sci. 2001 Nov;322(5):282-5; PMID: 11876189].Source American Journal of the Medical Sciences. 322(5):284-7, 2001 Nov.Abstract The Strong Heart Study (SHS) is a large, multi-community study to investigate the high incidence of cardiovascular disease (CVD) among American Indians and to improvelong-term health outcomes within the communities. CVD is the No. 1 cause of death for three geographically and culturally diverse American Indian populations. The SHSinvestigated the prevalence and incidence of CVD as well as the distribution of riskfactors in members of 13 American Indian tribes in Oklahoma, Arizona, and (as one region) North and South Dakota. The SHS enrolled more than 4500 participants rangingin age from 45 to 74 years. During the three-phase study, which began with baseline examinations from 1989 through 1991 and concluded in 1999, participants received medical examinations in each phase. To build trust and cooperation, SHS investigators worked closely with tribal leaders and community members, including establishing empowered committees and hiring community members for jobs within the study. As a result of such cooperation, the SHS maintained retention rates of about 90% across all three phases. Benefits to tribal communities also included health care improvements and education for healthy lifestyles. The SHS could serve as a model for similar studies of American Indians or other minority groups.
<145>Unique Identifier 11721224
Page 73

201-400.txtAuthors Yagdiran O. Haasen C. Krausz M.Institution Klinik fur Psychiatrie und Psychotherapie, Universitatsklinikum [email protected] [Psychotic experiences in a transcultural context - case report analysis on the importance of the second language for the therapeutic process]. [German]Source Psychiatrische Praxis. 28(8):380-2, 2001 Nov.Abstract The use of the second language among migrants can lead to a separation of affect and content of speech, which can be used in therapy when touching upon emotionally strenuous events. On the basis of 3 case reports of migrants of Turkish origin with a psychotic disorder, the importance of the second language when used by a native speaking therapists is analyzed. This can lead to the establishment of a therapeuticalliance, even though emotionally central themes are avoided in the process.
<146>Unique Identifier 11708668Authors Barrio C.Institution School of Social Work, San Diego State University, California 92182-4119, USA.Title Culture and schizophrenia: a cross-ethnic growth curve analysis.Source Journal of Nervous & Mental Disease. 189(10):676-84, 2001 Oct.Abstract This study examined the longitudinal trajectory of a sociocentric construct among African-Americans, Latinos, and nonminorities. Participants were 163 individuals diagnosed with schizophrenia who were admitted to community-based psychosocial programs. Previous research had established empathy and social competence as sociocentric cultural mediators of a benign symptom profile for ethnic minorities. Data on sociocentric indicators were collected every 6 months for over 3 years. Growth curve methodology was used to examine the empathy and social competence outcomes over time and across ethnic groups. The results revealed a dynamic course for both sociocentric mediators. However, the dynamic growth curve for empathy was related to ethnicity; for social competence it was not. Empathy levels for African-Americans decreased and then attenuated, whereas empathy levels for Latinos decreased over the entire study. Nonminorities showed very little change overall. The nature of sociocentric phenomena is dynamic and complex. These qualities can apparently be cultivated or diminished over time.
<147>Unique Identifier 11705160Authors McNeill JA. Sherwood GD. Starck PL. Nieto B.Institution Department of Nursing for Target Populations, University of Texas-Houston Health Science Center School of Nursing, 1100 Holcombe Blvd, Room 5.537, Houston, TX 77030,USA. [email protected] Pain management outcomes for hospitalized Hispanic patients.Source Pain Management Nursing. 2(1):25-36, 2001 Mar.Abstract The purposes of the study were to describe outcomes of pain management and predictors of patient satisfaction in a minority sample. By using a survey design, 3
Page 74

201-400.txtinstruments were used to collect data: (1) The American Pain Society's Patient Outcome Questionnaire-Modified, a 16-item self-report tool about pain and patient satisfaction; (2) a demographic form; and (3) the Pain Management Index. The sample consisted of 104 hospitalized Hispanic inpatients in a Rio Grande Valley hospital. Mean ratings for current and average pain were moderate, whereas severe mean ratingswere reported for worst pain. High interference caused by pain was found for walkingand sleep. Patients were satisfied with pain management. However, a negative correlation was found between satisfaction and current pain intensity (r = -.49, p =.001). Pain Management Index scores revealed that 36% of the participants were inadequately treated for pain; also, negative correlations with age indicated less effective management for elders. Reliability estimates for tool subscales were greater than 0.70 except for the Beliefs subscale (0.63). By using logistic regression, satisfaction with pain management was predicted by general pain in the last 24 hours (odds ratio = 4.02), pain-related interference with mood (odds ratio =7.31), and age (odds ratio = 1.8). Clinical implications include the need to apply standardized guidelines, such as those from the Agency for Health Care Policy and Research, and to educate patients, particularly minority elders, about pain management approaches. The emergence of Hispanics as the fastest growing minority group increases the need for research regarding pain management outcomes to plan more effective intervention.
<148>Unique Identifier 11694693Authors Racine AD. Kaestner R. Joyce TJ. Colman GJ.Institution Albert Einstein College of Medicine, Children's Hospital at Montefiore, Bronx, NewYork 10461, USA. [email protected] Differential impact of recent Medicaid expansions by race and ethnicity.Source Pediatrics. 108(5):1135-42, 2001 Nov.Abstract OBJECTIVE: Between 1989 and 1995, expansions in Medicaid eligibility provided publicly financed health insurance to an additional 7 million poor and near-poor children. It is not known whether these expansions affected children's insurance coverage, use of health care services, or health status differently, depending on their race/ethnicity. The objective of this study was to examine, by race/ethnicity,the impact of the recent Medicaid expansions on levels of uninsured individuals, health care service utilization, and health status of the targeted groups of children. METHODS: Using a stratified set of longitudinal data from the National Health Interview Surveys of 1989 and 1995, we compared changes in measures of healthinsurance coverage, health services utilization, and health status for poor white, black, and Hispanic 1- to 12-year-old children. To control for underlying trends over time, we subtracted 1989 to 1995 changes in these outcomes among nonpoor children from changes among the poor children for each race/ethnicity group. Measures of coverage included uninsured rates and Medicaid rates. Utilization measures included annual probability of visiting a doctor, annual number of doctor visits, and annual probability of hospitalization. Health status measures included self-reported health status and number of restricted-activity days in the 2 weeks before the interview. Differences in means were analyzed with the use of Student's ttests accounting for the clustering sample design of the National Health Interview Surveys. RESULTS: Among poor children between 1989 and 1995, uninsured rates declined by 4 percentage points for whites, 11 percentage points for blacks, and 19 percentage points for Hispanics. Medicaid rates for these groups increased by 16 percentage points, 22 percentage points, and 23 percentage points, respectively. With respect to utilization, the annual probability of seeing a physician increased 7 percentage points among poor blacks and Hispanics but only 1 percentage point among poor whites (not significant) for children in good, fair, or poor health. Among those in excellent or very good health, the respective increases were 1 percentage point for poor whites (not significant), 7 percentage points for poor
Page 75
201-400.txtblacks, and 3 percentage points for poor Hispanics (not significant). Significant increases in numbers of doctor visits per year were recorded only for poor Hispanicswho were in excellent or very good health, whereas significant decreases in hospitalizations were recorded for Hispanics who were in good fair or poor health. Measures of health status remained unchanged for poor children over time. The recorded decreases in uninsured rates and increases in Medicaid coverage remained robust to adjustments for underlying trends for all 3 race/ethnicity groups. With respect to adjusted measures of utilization and health status, the only significant differences found were among poor blacks who were in good, fair, or poor health and who registered increases in the likelihood of hospitalization and in poor Hispanics who were in excellent or very good health and who registered decreases in the numbers of restricted-activity days. CONCLUSIONS: Recent expansions in the Medicaid program from 1989 to 1995 produced greater reductions in uninsured rates among poor minority children than among poor white children. Regardless of race/ethnicity, poorchildren did not seem to experience significant changes during the period of the expansions in either their level of health service utilization or their health status.Medicaid, health insurance, health status, health services.
<149>Unique Identifier 11694205Authors Murray RP. Connett JE. Buist AS. Gerald LB. Eichenhorn MS.Institution Department of Community Health Sciences, University of Manitoba, Winnipeg, MB, Canada. [email protected] Experience of Black participants in the Lung Health Study smoking cessation intervention program.Source Nicotine & Tobacco Research. 3(4):375-82, 2001 Nov.Abstract This paper evaluates the hypothesis that Black smokers will respond differently than Whites to a smoking cessation intervention program where no adjustments are made in recognition of cultural differences. The responses of Black smokers who wererecruited into the Lung Health Study (LHS) to the smoking cessation intervention aredescribed. Black quit rates are compared with those of Whites. The LHS enrolled 5887men and women smokers, aged 35-60 years, of whom 3923 were randomized to a group cessation intervention and 1964 to usual care. Blacks and Whites from six clinics who had complete covariate data (200 Blacks and 2868 Whites) were compared on baseline smoking characteristics and subsequent smoking cessation outcomes. Logisticmodels were constructed to adjust for baseline smoking variables and demographic characteristics to evaluate the effect of treatment group on smoking cessation amongBlacks and Whites. At baseline, Blacks reported smoking fewer cigarettes than Whites, but had higher mean levels of salivary cotinine. The adjusted odds ratio of quitting at 1 year for the smoking intervention group vs. the usual care group was 1.48 for Blacks and 5.99 for Whites. This difference between Blacks and Whites was highly significant (p = 0.002). Across 5 years, the adjusted odds ratios of quittingwere 1.87 for Blacks and 3.34 for Whites (p = 0.06). Although the treatment effect was stronger for Whites than for Blacks, over the 5 years of the study there was a significant treatment effect for Blacks. Indicators of physical dependence on nicotine at baseline were inconsistent in indicating whether Blacks were more dependent. We conclude that Blacks and Whites differed significantly in their response to the LHS group smoking intervention program.
<150>Unique Identifier 11688924Authors Jasinski JL.Institution
Page 76

201-400.txt Department of Sociology and Anthropology, University of Central Florida, Orlando 32816, USA.Title Physical violence among Anglo, African American, and Hispanic couples: ethnic differences in persistence and cessation.Source Violence & Victims. 16(5):479-90, 2001 Oct.Abstract Research on violence against women has developed exponentially over the past 20 years, however, there are still many areas in which knowledge is scarce. In particular, there is very little empirical information regarding the cessation and persistence of intimate violence against women. There is even less research that looks at racial and ethnic differences in patterns of violence. This study uses datafrom the first and second waves of the National Survey of Families and Households toexamine changing patterns of physical violence in a sample of approximately 3,000 married and cohabiting couples. The results from the current study suggest that the same factors that might increase the initial risk for violent behavior may not affect whether or not this behavior continues. Additionally, the same risk factors may be related in different ways to different patterns of violence for different racial/ethnic groups.
<151>Unique Identifier 11684616Authors Joyce T. Bauer T. Minkoff H. Kaestner R.Institution Baruch College, City University of New York, and the National Bureau of Economic Research, New York, NY 10016-4309, USA. [email protected] Welfare reform and the perinatal health and health care use of Latino women in California, New York City, and Texas.[see comment].Source American Journal of Public Health. 91(11):1857-64, 2001 Nov.Abstract OBJECTIVES: This study analyzed changes in the financing of prenatal care and delivery, the use of prenatal care, and birth outcomes among foreign-born vs US-bornLatino women following enactment of the Personal Responsibility and Work OpportunityReconciliation Act (PRWORA) in August 1996. METHODS: We used a pre-post design with a comparison group. The sample consisted of resident Latinas in California, New YorkCity, and Texas who delivered a live infant in 1995 or 1998. RESULTS: The proportionof births to Latinas that initiated prenatal care in the first 4 months of pregnancyincreased for all foreign-born Latinas in California, New York City, and Texas between 1995 and 1998 (P <.05). Except for non-Dominicans in New York City, there was no increase in the proportion of low- or very-low-birthweight births among foreign-born vs US-born Latinas in the 3 localities between 1995 and 1996. CONCLUSIONS: There is little evidence from vital statistics in California, New York City, and Texas that PRWORA had any substantive impact on the perinatal health and health care utilization of foreign-born relative to US-born Latinas.
<152>Unique Identifier 11681563Authors Weinehall L. Lewis C. Nafziger AN. Jenkins PL. Erb TA. Pearson TA. Wall S.Institution Department of Public Health and Clinical Medicine, Umea University, Sweden. [email protected] Different outcomes for different interventions with different focus!--A cross-country comparison of community interventions in rural Swedish and US
Page 77

201-400.txtpopulations.Source Scandinavian Journal of Public Health. Suppl 56:46-58, 2001.Abstract OBJECTIVES: There is a need among healthcare providers to acquire more knowledge about small-scale and low budget community intervention programmes. This paper compares risk factor outcomes in Swedish and US intervention programmes for the prevention of cardiovascular disease (CVD). The aim was to explore how different intervention programme profiles affect outcome. METHODS: Using a quasi-experimental design, trends in risk factors and estimated CVD risk in two intervention areas (Norsjo. Sweden and Otsego-Schoharie County, New York state) are compared with thosein reference areas (Northern Sweden region and Herkimer County, New York state) using serial cross-sectional studies and panel studies. RESULTS: The programmes wereable to achieve significant changes in CVD risk factors that the local communities recognized as major concerns: changing eating habits in the Swedish population and reducing smoking in the US population. For the Swedish cross-sectional follow-up study cholesterol reduction was 12%, compared to 5% in the reference population (p for trend differences <0.000). The significantly higher estimated CVD risk (as assessed by risk scores) at baseline in the intervention population was below that of the Swedish reference population after 5 years of intervention. The Swedish panelstudy provided the same results. In the US, both the serial cross-sectional and panel studies showed a > 10% decline in smoking prevalence in the intervention population, while it increased slightly in the reference population. When pooling the serial cross-sectional studies the estimated risk reduction (using the Framingham risk equation) was significantly greater in the intervention populations compared to the reference populations. CONCLUSIONS: The overall pattern of risk reduction is consistent and suggests that the two different models of rural county intervention can contribute to significant risk reduction. The Swedish programme hadits greatest effect on reduction of serum cholesterol levels whereas the US programme had its greatest effect on smoking prevention and cessation. These outcomes are consistent with programmatic emphases. Socially less privileged groups in these rural areas benefited as much or more from the interventions as those with greater social resources.
<153>Unique Identifier 11681562Authors Jenkins PL. Weinehall L. Erb TA. Lewis C. Nafziger AN. Pearson TA. Wall S.Institution The Mary Imogene Bassett Research Institute, Cooperstown, New York 13326-1394, USA. [email protected] The Norsjo-Cooperstown healthy heart project: a case study combining data from different studies without the use of meta-analysis.Source Scandinavian Journal of Public Health. Suppl 56:40-5, 2001.Abstract OBJECTIVES: This paper aims to develop and describe a method for combining. comparing, and maximizing the statistical power of two longitudinal studies of risk factors for cardiovascular disease that did not have identical data collection methodologies. METHODS: Subjects from a 1986 cross-sectional study (n = 180) were pair-matched with subjects of corresponding gender and age (+5 years) from a 1990 cross-sectional study. The methodology is described and results are calculated for various measures of cardiovascular risk or risk factors (e.g. cholesterol. Finnish Risk Score). RESULTS: Box's test of equality and symmetry of covariance matrices gave chi-square values of 223.8 and 710.0 for two cardiovascular risk factors (cholesterol and cardiac risk score, respectively); these values were highly significant (p=0.0001) For the North Karelia Risk Score, repeated measures ANOVA revealed a borderline significant interaction for treatment by time (p=0.054) and a significant interaction for treatment by time by country (p=0.035). These probabilities compared favorably with a randomized blocks model. CONCLUSIONS:
Page 78

201-400.txtCreation of a synthetic longitudinal control group resulted in a statistically validANOVA model that increased the statistical power of the study.
<154>Unique Identifier 11603242Authors Ortega AN. Rosenheck R.Institution Division of Health Policy and Administration, Department of Epidemiology and Public Health, Yale University School of Medicine, New Haven, CT, USA.Title Mental and physical health and acculturation among Hispanic Vietnam Veterans.Source Military Medicine. 166(10):894-7, 2001 Oct.Abstract This study tested the associations between acculturation and mental and physical health among Hispanic Vietnam veterans. Secondary data analyses of the National Vietnam Veterans Readjustment Survey, an epidemiological study of a representative sample of veterans who served during the Vietnam era (N = 1,195), were conducted. Anacculturation index was constructed using standard acculturation measures (range, 0-13), and its predictive validity was tested using nine outcome measures of physical health and eight measures of mental health. Among Puerto Rican and Mexican-American veterans, the scores on the acculturation index ranged from 0 to 12. Hispanic veterans were distributed across the acculturation continuum as follows: 0 to 3 (24%), 4 to 7 (59%), 8 to 12 (17%). The acculturation scores were not associated with mental or physical health risks for Hispanic veterans. Mexican Americans and Puerto Ricans did not differ in mental or physical health risk compared with non-Hispanic whites. The association between acculturation and mental and physical health among Hispanics may not be generalized to Hispanic veterans. Hispanics who have been through an intensive assimilating experience, such as being in the military, appear to have health outcomes similar to whites.
<155>Unique Identifier 11589331Authors Bhui K. Bhugra D.Institution Department of Psychiatry, University of London. [email protected] Transcultural psychiatry: some social and epidemiological research issues.Source International Journal of Social Psychiatry. 47(3):1-9, 2001 Autumn.Abstract BACKGROUND: Mental Health Research across cultural groups is often criticised for using imprecise measures of cultural group and for using outcome measures as if theyhave universal validity. AIMS: 1. To Investigate the effect of using different cultural group variables on the findings of a survey of prevalence of Common Mental Disorders. 2. To demonstrate that assumptions of validity for outcomes measures can affect the interpretation of data from prevalence surveys. METHODS: We recruited Punjabi and English subjects to a phase prevalence survey that included the AmritsarDepression Inventory and the General Health Questionnaire as screening instruments. The Clinical Interview Schedule was the outcome measure. This paper reports on a secondary analysis of the data. We used ethnic group, place of birth, religion, first language and language spoken at interview as possible cultural group variablesand compared the prevalence estimates. We then considered the limitations of conventional methods to assess prevalence, by looking at mean scores on each of the three instruments in both cultural groups. RESULTS: Cultural group variables did notinfluence the prevalence estimates for Common Mental Disorder. Although conventionalscoring methods showed no difference in prevalence across cultures, the mean scores
Page 79

201-400.txton each instrument, when compared across cultural groups, differed for the Amritsar Depression Inventory. This instrument showed a higher mean score for the Punjabis suggesting a higher prevalence. The findings are discussed in the context of value laden 'assumptions' about validity. CONCLUSIONS: The findings of prevalence surveys depend on assumptions of validity. The 'culture' of psychiatry is a closed system inwhich validation studies support its basic assumptions.
<156>Unique Identifier 11581097Authors Luchsinger JA. Tang MX. Stern Y. Shea S. Mayeux R.Institution Taub Institute for Research of Alzheimer's Disease and the Aging Brain, Columbia University, New York, NY, USA.Title Diabetes mellitus and risk of Alzheimer's disease and dementia with stroke in a multiethnic cohort.Source American Journal of Epidemiology. 154(7):635-41, 2001 Oct 1.Abstract Research on the relation between diabetes mellitus and dementia has produced conflicting results, and the relation has not been investigated among Blacks and Hispanics. In this study, Cox proportional hazards models were used to analyze longitudinal data from 1,262 elderly subjects without dementia at baseline (1991-1996) who were followed for an average of 4.3 years between 1992 and 1997. Outcomes were incident Alzheimer's disease and dementia associated with stroke. The prevalence of diabetes was 20% at baseline. The adjusted relative risk of Alzheimer's disease among persons with diabetes as compared with those without diabetes was 1.3 (95% confidence interval (CI): 0.8, 1.9). The adjusted relative risk for the composite outcome of Alzheimer's disease and cognitive impairment without dementia (without stroke) in subjects with diabetes was 1.6 (95% CI: 1.2, 2.1). The adjusted relative risk of stroke-associated dementia in persons with diabetes was 3.4 (95% CI: 1.7, 6.9). Among Blacks and Hispanics, approximately one third of the risk of stroke-associated dementia was attributable to diabetes (33% (95% CI: 31, 36) and 36% (95% CI: 33, 37), respectively), as compared with 17% (95% CI: 13, 22) among Whites. The finding of an association between diabetes and the composite outcome of Alzheimer's disease and cognitive impairment without dementia (without stroke) is consistent with prior reports of a modest relation between diabetes and Alzheimer's disease.
<157>Unique Identifier 11578006Authors Hobcraft J. Kiernan K.Institution Department of Social Policy, and ESRC Centre for Analysis of Social Exclusion, London School of Economics and Political Science.Title Childhood poverty, early motherhood and adult social exclusion.Source British Journal of Sociology. 52(3):495-517, 2001 Sep.Abstract Childhood poverty and early parenthood are both high on the current political agenda. The key new issue that this research addresses is the relative importance ofchildhood poverty and of early motherhood as correlates of outcomes later in life. How far are the 'effects' of early motherhood on later outcomes due to childhood precursors, especially experience of childhood poverty? Subsidiary questions relate to the magnitude of these associations, the particular levels of childhood poverty that prove most critical, and whether, as often assumed, only teenage mothers are
Page 80

201-400.txtsubsequently disadvantaged, or are those who have their first birth in their early twenties similarly disadvantaged? The source of data for this study is the National Child Development Study. We examine outcomes at age 33 for several domains of adult social exclusion: welfare, socio-economic, physical health, emotional well-being anddemographic behaviour. We control for a wide range of childhood factors: poverty; social class of origin and of father; mother's and father's school leaving age; family structure; housing tenure; mother's and father's interest in education; personality attributes; performance on educational tests; and contact with the police by age 16. There are clear associations for the adult outcomes with age at first birth, even after controlling for childhood poverty and the other childhood background factors. Moreover, we demonstrate that the widest gulf in adult outcomes occurs for those who enter motherhood early (before age 23), though further reinforced by teenage motherhood for most adult outcomes. We also show that any experience of childhood poverty is clearly associated with adverse outcomes in adulthood, with reinforcement for higher levels of childhood poverty for a few outcomes.
<158>Unique Identifier 11574437Authors Fisher L. Chesla CA. Mullan JT. Skaff MM. Kanter RA.Institution Department of Family & Community Medicine, University of California, San Francisco94143, USA. [email protected] Contributors to depression in Latino and European-American patients with type 2 diabetes.Source Diabetes Care. 24(10):1751-7, 2001 Oct.Abstract OBJECTIVE: To determine the independent and cumulative contributions of diabetes and other life stresses on depression and anxiety in Latino and European-American (EA) patients with diabetes. RESEARCH DESIGN AND METHODS: A total of 75 Latino and 113 EA patients with type 2 diabetes, recruited from managed care settings, were assessed regarding three groups of potential stresses: demographics (age, sex, and education), disease status (functional impact, time since diagnosis, comorbidities, HbA(1c), and BMI), and family stress (financial stress, spouse conflict resolution, and family closeness). Dependent variables were depression (Center for Epidemiological Studies-Depression scale [CES-D]) and anxiety (Symptom Checklist [SCL-90]). Multiple regression equations assessed the independent contribution of each predictor on depression and anxiety. RESULTS: For both ethnic groups, education, functional impact, and financial stress significantly and independently predicted depression; poor spouse conflict resolution was a fourth significant predictor for EA patients only. The equations accounted for a high percentage of variance (43- 55%). Excluding education, the same variables predicted anxiety for both ethnic groups. The disease status and family stress variable groups significantly predicted outcomes independently. The relationships among these variables and depression and anxiety generally occurred for all patients, not only for those classified as likely depressed. CONCLUSIONS: The findings suggest the utility of considering many life stresses, not just diabetes alone, that combine to affect depression and anxiety. We suggest that these effects are experienced cumulatively as general psychological distress for all patients with diabetes, not just those classified as likely depressed. Taken together, the findings emphasize a life-centered, patient-focused approach to the treatment of depression, rather than an exclusive disease-related perspective.
<159>Unique Identifier 11572416Authors
Page 81

201-400.txt Franzini L. Ribble JC. Keddie AM.Institution Center for Society and Population Health, University of Texas Health Science Center, School of Public Health, Houston 77030-3900, USA.Title Understanding the Hispanic paradox. [Review] [94 refs]Source Ethnicity & Disease. 11(3):496-518, 2001 Autumn.Abstract PURPOSE: This paper reviews the literature on the nature of the Hispanic paradox and the major explanations provided for it. We conclude by suggesting directions forfuture research. DATA IDENTIFICATION AND STUDY SELECTION: Articles were selected by a systematic review procedure using Medline (1966 through 1999) and Sociological Abstracts (1963 through 1999), as well as focused searches on specific diseases or factors believed to influence Hispanic health. FINDINGS: For the past twenty years there has been widespread evidence of an Hispanic paradox in the United States, in which most Hispanic groups are characterized by low socioeconomic status, but betterthan expected health and mortality outcomes. A closer look reveals variations by age, gender, Hispanic subgroup, acculturation, country of birth, and cause of death.Possible under-reporting of Hispanic deaths, "salmon bias" and healthy migrant effects, and risk profile may contribute to, but do not explain, the paradox. The reasons for this paradox are likely to be multifactorial and social in origin. CONCLUSIONS: Empirical studies should be conducted on the protective effects of immigrant status, identification with a subculture, interaction between acculturation and socioeconomic status, and supportive aspects of Hispanic culture. [References: 94]
<160>Unique Identifier 11569764Authors Chapman GB.Institution Psychology Department, Rutgers University, Piscataway, NJ 08854-8020, USA. [email protected] Time preferences for the very long term.Source Acta Psychologica. 108(2):95-116, 2001 Sep.Abstract Many important decisions concern outcomes delayed by decades or centuries. Whereassome economists have argued that inter-generational discount rates should be lower than intra-generational rates, three experiments found that inter- and intra-generational discount rates were quite similar. Experiment 1 found that discount rates for long delays (30-900 years) were lower than those for shorter delays (1-30 years) but that, holding delay constant, discount rates for outcomes occurring to future generations were similar to those for outcomes occurring to the present generation. Experiment 2 compared inter-generational discount rates for three different types of outcomes and found similar discount rates for saving lives,improving health, and financial benefits. Experiment 3 found similar inter-generational discounting of life-saving programs that benefit people close to or distant from the decision maker. These studies indicate that the discount rate applied to outcomes occurring to future generations depends on the length of the time delay but not on other factors.
<161>Unique Identifier 11565591Authors Sormanti M. Pereira L. El-Bassel N. Witte S. Gilbert L.Institution
Page 82

201-400.txt Columbia University School of Social Work, New York, NY 10025, USA. [email protected] The role of community consultants in designing an HIV prevention intervention.Source AIDS Education & Prevention. 13(4):311-28, 2001 Aug.Abstract This article describes the significant role of community members during the intervention development phase of a randomized clinical trial of an HIV prevention intervention for African American and Latina women and their main sexual partners. Sixteen women and 13 male partners were engaged as "consultants" in a series of focus group discussions aimed at exploring their reactions and ideas about potentialtopics and approaches for the intervention. Each individual participated in three focus groups-two single-sex groups and a third that brought women and their male partners together. Focus group data extended our knowledge about the impact of relationship dynamics on safer sex negotiation and allowed us to design an intervention that is contextually specific and pragmatic. Target community members can provide critical input during the intervention development process and should berecognized as viable and meaningful collaborators in all phases of intervention research.
<162>Unique Identifier 11556933Authors Nallamothu BK. Saint S. Saha S. Fendrick AM. Kelley K. Ramsey SD.Institution Department of Internal Medicine, University of Michigan Medical School, Ann Arbor 48109-0022, USA. [email protected] Coronary artery bypass grafting in Native Americans: a higher risk of death compared to other ethnic groups?.Source Journal of General Internal Medicine. 16(8):554-9, 2001 Aug.Abstract BACKGROUND: While the efficacy and safety of coronary artery bypass grafting (CABG) has been established in several clinical trials, little is known about its outcomes in Native Americans. MEASUREMENTS AND MAIN RESULTS: We assessed clinical outcomes associated with CABG in 155 Native Americans using a national database of 18,061 patients from 25 nongovernmental, not-for-profit U.S. health care facilities.Patients were classified into five groups: 1) Native American, 2) white, 3) African American, 4) Hispanic, and 5) Asian. We evaluated for ethnic differences in in-hospital mortality and length of stay, and after adjusting for age, gender, surgical priority, case-mix severity, insurance status, and facility characteristics(volume, location, and teaching status). Overall, we found the adjusted risk for in-hospital death to be higher in Native Americans when compared to whites (odds ratio [OR], 3.8; 95% confidence interval [CI], 1.5 to 9.8), African Americans (OR, 3.4; 95% CI, 1.1 to 9.9), Hispanics (OR, 7.1; 95% CI, 2.5 to 20.3), and Asians (OR, 2.8; 95% CI, 1.1 to 7.0). No significant differences were found in length of stay after adjustment across ethnic groups. CONCLUSIONS: The risk of in-hospital death following CABG may be higher in Native Americans than in other ethnic groups. Given the small number of Native Americans in the database (n = 155), however, further research will be needed to confirm these findings.
<163>Unique Identifier 11555040Authors Kim-Godwin YS. Clarke PN. Barton L.Institution School of Nursing, University of North Carolina at Wilmington, North Carolina
Page 83

201-400.txt28403, USA. [email protected] A model for the delivery of culturally competent community care.Source Journal of Advanced Nursing. 35(6):918-25, 2001 Sep.Abstract AIM: To describe the proposed Culturally Competent Community Care (CCCC) model, and the process of development and testing of the model. BACKGROUND: Community health nurses are challenged to provide culturally competent care in all types of communities. However, existing models have not provided community nurses with specific guidelines, and none attempt to explain the effects of culturally competentcare on populations in community settings. Therefore, it is necessary to develop a model that is comprehensive in its description of the dimensions of culturally competent care in community-based settings and that also requires a focus on ethnic populations. The model is essential for reducing racial and ethnic health disparities. METHODS: Based on literature review and concept analysis, three constructs of the Culturally Competent Community Care Model were developed. Two of the constructs, the health care system and health outcomes, were developed based on a literature review. The main construct of the model, cultural competence, was developed after a concept analysis, following the development and testing of the Cultural Competence Scale (CCS). Interviews with eight community health nurses and asurvey by five community nurse experts were conducted in order to refine and confirmthe dimensions of cultural competence and its impact on health outcomes. CONCLUSIONS: The proposed dimensions of culturally competent care are caring, cultural sensitivity, cultural knowledge, and cultural skills. This model focuses onthe relationship between cultural competence and health outcomes for culturally diverse populations. The framework provides specific guidelines for community nursesin developing and assessing cultural competence and meeting the health needs of diverse communities.
<164>Unique Identifier 11548662Authors Howard K.Institution LAFAN (Los Angeles Family AIDS Network), USA.Title Multicultural and psychosocial aspects of HIV treatment failure.Source Focus: a Guide to AIDS Research. 16(7):1-4, 2001 Jun.
<165>Unique Identifier 11530155Authors Meegan ME. Conroy RM. Lengeny SO. Renhault K. Nyangole J.Title Effect on neonatal tetanus mortality after a culturally-based health promotion programme.[see comment].Source Lancet. 358(9282):640-1, 2001 Aug 25.Abstract The Maasai have high rates of death from neonatal tetanus, partly due to their custom of packing the umbilical stump with cow dung. We report on the effect of a simple health promotion programme, designed in consultation with the local communityand carried out by local women. After introduction of the programme in 1981, neonatal (<6 weeks of age) tetanus rates fell sharply, and by 1988 annual death rates had dropped to 0.75 (range 0-3) per 1000 births in the intervention areas compared with 82 (74-93) per 1000 in control areas.
Page 84

201-400.txt
<166>Unique Identifier 11509921Authors Alhaddad IA. Blum S. Heller EN. Beato MA. Bhalodkar NC. Keriaky GE. Brown EJJr.Institution Cardiology Division, Department of Medicine, Bronx Lebanon Hospital Center, AlbertEinstein College of Medicine, Bronx, NY, USA.Title Renal artery stenosis in minority patients undergoing diagnostic cardiac catheterization: prevalence and risk factors.Source Journal of Cardiovascular Pharmacology & Therapeutics. 6(2):147-53, 2001 Apr.Abstract BACKGROUND: Atherosclerotic renal artery stenosis (RAS) is a frequently overlookedclinical entity that can cause progressive renal failure and uncontrolled hypertension. Revascularization of a stenosed renal artery is associated with improved clinical outcomes including the prevention of renal failure. Thus, it is important to recognize all potential candidates for renal artery revascularization. In a general population referred for diagnostic cardiac catheterization, RAS of any severity was found in 30% of patients and significant stenosis (> or = 50% diameter narrowing) was found in 15% of patients. The number of minority groups is increasingin the US population, and RAS in this population is not well investigated. Our purpose was to determine the prevalence and risk factors associated with RAS in minority patients referred for diagnostic cardiac catheterization. METHODS: Abdominal aortography was performed in 171 consecutive minority patients referred for diagnostic cardiac catheterization (hispanics = 115, African Americans = 56). The association of clinical and angiographic variables with RAS was examined using univariate and multivariate logistic regression analyses. RESULTS: Renal artery stenosis of any severity was identified in 13.5% of patients (unilateral 7.7%, bilateral 5.8%). Significant RAS was found in 7.7% of patients (unilateral 4.8%, bilateral 2.9%). Independent predictors of RAS included age (mean +/-1SD, 68 +/-10 vs 57 +/-12 yr, P < 0.001, for patients with vs without RAS), coronary artery disease, and elevated serum creatinine levels (> 115 micromol/L). Race/ethnicity (hispanics vs African Americans), sex, smoking, congestive heart failure, diabetes mellitus, peripheral vascular disease, and hypertension were not independent predictors. CONCLUSIONS: Renal artery stenosis in minority patients undergoing diagnostic cardiac catheterization is less common than reported in white patients, is similar in hispanics and African Americans, and is similar in women and men. The clinical and angiographic features are helpful in predicting its presence.
<167>Unique Identifier 11506217Authors Quittan M. Wiesinger GF. Crevenna R. Nuhr MJ. Posch M. Hulsmann M. Muller D. Pacher R. Fialka-Moser V.Institution Department of Physical Medicine and Rehabilitation, University of Vienna, Vienna General Hospital, Austria.Title Cross-cultural adaptation of the Minnesota Living with Heart Failure Questionnairefor German-speaking patients.Source Journal of Rehabilitation Medicine. 33(4):182-6, 2001 Jul.Abstract We performed a cross-cultural adaptation of the "Minnesota Living with Heart Failure Questionnaire" (LHFQ) for use in German-speaking chronic heart failure patients. The instrument was translated and back translated, pre-tested and reviewedby a committee. The German version was tested in 114 patients with chronic heart
Page 85

201-400.txtfailure. Reliability was assessed by a test-retest procedure and Cronbach's coefficient alpha of internal consistency (0.94). To assess concurrent validity, we compared the LHFQ sum scores with the New York Heart Association classification rating (r = 0.53; p < 0.0001), the 6-minute walk (r = -0.39; p < 0.0001), the left ventricular ejection fraction (r = -0.24; p = 0.011) and big-endothelin (r = 0.27; p= 0.004). Construct validity on the LHFQ scores in comparison with the Medical Outcomes Study SF-36 Health Survey (MOS SF-36) was significant (-0.41 to -0.74; all p < 0.0001). The reliability and validity of the German version of the LHFQ was proved; the questionnaire can be recommended for use in future clinical trials.
<168>Unique Identifier 11504151Authors Huriwai T. Robertson PJ. Armstrong D. Kingi TP. Huata P.Institution National Centre for Treatment Development (Alcohol, Drugs & Addiction), Departmentof Psychological Medicine, Christchurch School of Medicine, New Zealand. [email protected] Whanaungatanga - a process in the treatment of Maori with alcohol- and drug-use related problems.Source Substance Use & Misuse. 36(8):1033-51, 2001 Jun.Abstract Maori, the indigenous people of New Zealand have advocated that culturally-based care requires goals and processes specifically defined within their ethnocultural context. Positive cultural identity and pride have been posited as integral to achieving wellbeing for Maori. A sample of Maori in treatment for alcohol- and drug-use associated problems was reported to believe that a sense of belonging to aniwi ("tribe") could contribute to the recovery process. Data relating to "tribal" affiliation, cultural self-identity and upbringing of that sample is presented. The key concepts of whanau ("family") and whanaungatanga ("relationships") in the treatment process for Maori are explored and the implications of their utility discussed. The findings highlight the complexity of providing treatment that is cognizant of ethnocultural factors.
<169>Unique Identifier 11504150Authors Robertson PJ. Futterman-Collier A. Sellman JD. Adamson SJ. Todd FC. Deering DE. Huriwai T.Institution National Centre for Treatment Development, (Alcohol, Drugs & Addiction), Department of Psychological Medicine, Christchurch School of Medicine and Health Sciences, New Zealand. [email protected] Clinician beliefs and practices related to increasing responsivity to the needs ofMaori with alcohol and drug problems.Source Substance Use & Misuse. 36(8):1015-32, 2001 Jun.Abstract Culturally responsive treatments are often cited as essential for successfully addressing substance use-associated problems in indigenous and other ethnic groups. However, there has been little investigation of the support for this assertion amongalcohol and drug-user treatment workers, or how it might translate into clinical practice. The current paper reports on the results of a survey of the New Zealand alcohol and drug-user treatment field, which canvassed these issues. Eighty-six percent of respondents advocated adjustment of clinical practice when working with Maori. Two key strategies were referral to specialist Maori groups or individuals
Page 86

201-400.txtand/or contacting/meeting with whanau (family). Comparisons were made between respondents who referred clients on and those who provided intervention themselves. Implications of results, limitations and future research are discussed.
<170>Unique Identifier 11499186Authors Twizer I. Sheiner E. Hallak M. Mazor M. Katz M. Shoham-Vardi I.Institution Departments of Obstetrics and Gynecology and of Epidemiology and Health Services Evaluation, Faculty of Health Sciences, Soroka University Medical Center, Ben-GurionUniversity of the Negev, Beer-Sheva, Israel.Title Lack of prenatal care in a traditional society. Is it an obstetric hazard?.Source Journal of Reproductive Medicine. 46(7):662-8, 2001 Jul.Abstract OBJECTIVE: To examine the association between lack of prenatal care (fewer than three visits at any prenatal care facility) and perinatal complications in the Bedouin parturient population where lack of prenatal care is not associated with absence of prenatal services, substance abuse or marital status. STUDY DESIGN: The study population consisted of all Bedouin women lacking prenatal care (n = 7,601) who gave birth between the years 1990-1997 in the Soroka University Medical Center. The analysis consisted of a comparison of labor and delivery outcomes in women without prenatal care to outcomes in women who had some prenatal care. RESULTS: During the years 1990-1997 there were 36,281 singleton deliveries to Bedouin women at our institution. Of those, 20.9% did not receive prenatal care. Mothers in the no-prenatal-care group tended to be in the extremes of their reproductive cycles (< 18 years, > 35 years) and were of higher parity (P < .001) than those receiving prenatal care. There were more deliveries prior to 32 weeks of gestation in the no-prenatal-care group (2.8%) in comparison to the prenatal care group (1.5%, P < .001) and fewer postterm deliveries (> 42 weeks, P < .01). The incidence of low birth weight (< 2,500 g) in the no-prenatal-care group was higher than in the prenatal-care group (11.2% vs. 8.4%, P < .001). Women who did not receive adequate prenatal care had statistically significantly higher rates of antepartum fetal death(OR = 1.8, 95% CI 1.4-2.3, P < .001), intrapartum fetal death (OR = 2.38, 95% CI 1.2-4.5, P < .03) and postpartum fetal death (OR = 1.60, 95% CI 1.2-2.1, P < .001). Multiple logistic regression models were used to analyze the independent contribution of lack of prenatal care to perinatal mortality and to very-low-birth-weight newborns. In both models lack of prenatal care was an independent contributing factor. CONCLUSION: Lack of prenatal care is an independentcontributor to perinatal mortality and low birth weight in a traditional society. Inlight of the high percentage of lack of prenatal care in Bedouin society, special attempts should be made to encourage women to use the available prenatal services.
<171>Unique Identifier 11495179Authors Hall GC.Institution Department of Psychology, The Pennsylvania State University, USA.Title Psychotherapy research with ethnic minorities: empirical, ethical, and conceptual issues. [Review] [80 refs]Source Journal of Consulting & Clinical Psychology. 69(3):502-10, 2001 Jun.Abstract There is an increasing demand for psychotherapy among ethnic minority populations.Yet, there is not adequate evidence that empirically supported therapies (ESTs) are
Page 87

201-400.txteffective with ethnic minorities. Ethical guidelines suggest that psychotherapies bemodified to become culturally appropriate for ethnic minority persons. Conceptual approaches have identified interdependence, spirituality, and discrimination as considerations for culturally sensitive therapy (CST). However, there is no more empirical support for the efficacy of CSTs than there is for the efficacy of ESTs with ethnic minority populations. The chasm between EST and CST research is a function of differences between methods and researchers in these 2 traditions. Specific recommendations for research collaboration between CST and EST researchers are offered. [References: 80]
<172>Unique Identifier 11467251Authors Landale NS. Oropesa RS.Institution Pennsylvania State University, USA. [email protected] Migration, social support and perinatal health: an origin-destination analysis of Puerto Rican women.Source Journal of Health & Social Behavior. 42(2):166-83, 2001 Jun.Abstract Using pooled origin-destination data from the Puerto Rican Maternal and Infant Health Study, we investigate linkages between migration, social support, and perinatal health. We document differences in social support between three groups of Puerto Rican women: non-migrant women in Puerto Rico, first-generation migrants to the U.S. mainland, and mainland-born women. The role of social support in producing differences in perinatal health outcomes between the groups is assessed. The analysis shows striking differences in social support between island and mainland women, but little systematic variation among mainland women by generation of U.S. residence. The lower level of social support available to mainland women is not reflected in the health outcomes examined, which do not generally worsen with migration to the United States (with the exception of maternal smoking). Nonetheless, we show that social support has important implications for stress, which in turn increases the risk of poor health behavior and compromised infant health.
<173>Unique Identifier 11456076Authors Kaplan CP. Napoles-Springer A. Stewart SL. Perez-Stable EJ.Institution Department of Medicine, Medical Effectiveness Research Center for Diverse Populations, University of California-San Francisco, 94143-0856, USA. [email protected] Smoking acquisition among adolescents and young Latinas: the role of socioenvironmental and personal factors.Source Addictive Behaviors. 26(4):531-50, 2001 Jul-Aug.Abstract This paper examined the effects of socioenvironmental and personal factors on two stages of the smoking continuum--onset of smoking and regular smoking--among a sample of 1411 Latina clients, ages 14-24, at two federally funded family planning clinics. The socioenvironmental factors included cultural indicators, smoking behavior of family and peers, and norms. The personal factors were risk-taking behaviors and intention to smoke in the future. Results showed that the indicators associated with experimentation were different than those linked with regular smoking. Socioenvironmental factors associated with the transition from never having
Page 88

201-400.txtsmoked to trying cigarettes included acculturation, as measured by language and familialism, and peer smoking behavior. Among the personal factors, risk-taking behavior (past use of drugs, alcohol, and general risk attitude) and smoking intentions were correlates of experimentation. The transition from experimenter to regular smoker was associated with peer smoking behavior (P< .05) in the socioenvironmental domain and drug use and intention to smoke in the future among the personal factors (both P values <.001). Age, years of education, marital status,norms, and parental smoking did not independently predict either of the smoking outcomes. Intention to smoke was the strongest predictor of experimentation (OR = 8.3, Cl 5.87-11.60) and regular smoking (OR= 19.9, CI 12.31-29.21) and could help identify those most likely to benefit from smoking prevention and cessation interventions.
<174>Unique Identifier 11455999Authors Levin S. Mayer-Davis EJ. Ainsworth BE. Addy CL. Wheeler FC.Institution Department of Epidemiology and Biostatistics, School of Public Health, University of South Carolina, Columbia, USA. [email protected] Behavioral and demographic correlates of diabetes, hypertension and overweight among the Catawba Indian Nation.Source Ethnicity & Disease. 11(2):241-50, 2001 Spring-Summer.Abstract OBJECTIVE: In 1998, the Catawba Diabetes and Health Survey (CDHS) was conducted among adult members of the Catawba Indian Nation living in the Carolinas to determine the prevalence of diabetes and other health conditions, and to assess the population's health-related behaviors. DESIGN: A population-based sample of adult members of the Catawba Indian Nation (N = 633) were surveyed by telephone or in person regarding health status and health-related behaviors. Logistic regression wasused to determine demographic and behavioral correlates of diabetes, hypertension, and overweight among the Catawba. RESULTS: Age-adjusted prevalence rates of self-reported diabetes, hypertension and overweight were 12.3%, 29.1%, and 63.8%, respectively. Older age was related to diabetes, hypertension, and overweight (P<.0001 each), and heavier weight status was related to diabetes (P = .026) and hypertension (P<.0001). Nearly 40% of the Catawba are physically inactive (29.5% men, 46.5% women). Physical inactivity was related to diabetes and hypertension among men only, and related to overweight among women only (P<.05 each). Current smoking was inversely related to overweight among men and women (P = .002). Dietary behavior was not associated with the health outcomes. CONCLUSION: Given the high rates of overweight and physical inactivity, reducing the rates of both may be very important for the health of the Catawba, considering their association with diabetesand hypertension.
<175>Unique Identifier 11433059Authors Hakim RB. Bye BV.Institution Health Care Financing Administration, Baltimore, Maryland, USA.Title Effectiveness of compliance with pediatric preventive care guidelines among Medicaid beneficiaries.Source Pediatrics. 108(1):90-7, 2001 Jul.Abstract OBJECTIVE: Because research has not confirmed a relationship between compliance
Page 89

201-400.txtwith health supervision in infancy and improved health outcomes, we examined the association between adherence to prevailing guidelines for periodic health supervision and adverse health outcome indicated by incidence of avoidable hospitalizations. METHODS: This was a historic cohort study of 308 131 children enrolled in Medicaid at birth in California, Georgia, and Michigan in 1990 using Medicaid records linked across 3 years. We used avoidable hospitalizations as indicators of health in a survival analysis. The analysis used variables that represented completeness and timeliness of well-child visits and immunizations usingAAP guidelines for health supervision as the gold standard. RESULTS: When the children in this cohort were up-to-date for age on their schedule of well-child visits, they were less likely to have an avoidable hospitalization (race, illness, and level of poverty adjusted hazard ratios 0.52 [95% confidence interval (CI): 0.50-0.55] in California, 0.54 [95% CI: 0.50-0.55] in Georgia, and 0.7 [95% CI: 0.69-0.79] in Michigan). Among children who were not up-to-date with well-child visits, a sporadic preventive care visit conferred a mild benefit. Immunizations andrace/ethnicity had no consistent relationship with incidence of avoidable hospitalizations. CONCLUSIONS: A series of well-child visits maintained during the first 2 years of life has a positive effect on health outcomes as indicated by a decrease in avoidable hospitalizations among poor and near-poor children, regardlessof race, level of poverty, or health status. National efforts to improve the qualityof child health services for young children should focus on increasing compliance with periodic preventive care for young children in addition to improving immunization levels.
<176>Unique Identifier 11422553Authors Whitehead D.Institution University of Plymouth, Institute of Health Studies, Veysey Building, Earl Richards Road-North, Exeter EX2 6AS, UK. [email protected] Health education, behavioural change and social psychology: nursing's contributionto health promotion?. [Review] [88 refs]Source Journal of Advanced Nursing. 34(6):822-32, 2001 Jun.Abstract AIMS: To critically review the complex processes that underpin the modification ofa client's health-related behaviour. This paper also seeks to contextualize the operational differences between health-educating and health-promoting activities - as a means of rationalizing current practice. BACKGROUND: In "health promotional" encounters, there is a plethora of evidence that suggests that nurses work predominantly within a "traditional" preventative framework of practice. The prevalence of a culturally inherent biomedical framework, governing most nursing practice, tends to reduce health-related client interventions to little more than one-off, reductionist information-giving exercises. The expectation on clients to respond to and subsequently modify their health behaviour, when presented with such information, is unrealistic in most cases. Nurses are often unaware of the extremelycomplex human phenomena associated with modifying health-related behaviours and the resultant change processes. In nursing-related health encounters, the planned or unplanned intervention and the subsequent outcomes are mostly viewed within a too simplistic and superficial context. DESIGN: A selective review of the relevant literature. CONCLUSION: Where many nurses believe themselves to be health promotionalists, the likelihood is that they are instead more likely to be traditional health educationalists. Not that this is the main problem, in itself--but if nursing is to progress on this issue, it must first become more effective in delivering its current health education initiatives. Armed with furtherknowledge and understanding of their practices, health educators are far more likelyto achieve a degree of success in their behavioural-change encounters as well as approach the intervention with a far more realistic expectation of outcome. Without this further understanding, it is argued that the integration of health educational
Page 90

201-400.txtinitiatives into nursing practice will generally do little or nothing to change the health status of clients. [References: 88]
<177>Unique Identifier 11421397Authors Torenbeek M. Caulfield B. Garrett M. Van Harten W.Institution Roessingh Research & Development, Enschede, The Netherlands.Title Current use of outcome measures for stroke and low back pain rehabilitation in five European countries: first results of the ACROSS project.Source International Journal of Rehabilitation Research. 24(2):95-101, 2001 Jun.Abstract Objectives were to obtain a view on the current use of outcome measures for strokeand low back pain rehabilitation in five European countries. A postal questionnaire,comparable for different cultural situations, was distributed in August 1998 to 581 rehabilitation facilities in Ireland, Germany, Italy, Austria and the Netherlands. Of these, 102 settings responded. In stroke rehabilitation the Barthel Index is the dominant outcome measure, followed by the Functional Independence Measure and the Frenchay Activities Index. Besides the Visual Analogue Scale, the most used outcome measures in low back pain rehabilitation were the Oswestry Pain Disability Questionnaire and the Roland Disability Questionnaire. Outcome measures are more frequently used in stroke than in low back pain rehabilitation. The purpose of use is mainly for the measurement of effectiveness, while a relation with quality management is seldom made. There appears to be little agreement on which outcome measures to use. Little attention was found to have been given to the assessment of handicap, quality of life and patient satisfaction.
<178>Unique Identifier 11417908Authors Nomura S. Hattori N. Sakakibara I. Fukuhara S.Institution First Department of Internal Medicine, Kansai Medical University, Moriguchi Osaka,Japan. [email protected] Effects of Saiko-ka-ryukotsu-borei-to in patients with hyperlipidemia.Source Phytomedicine. 8(3):165-73, 2001 May.Abstract We measured and compared levels of platelet-derived microparticles (PMPs), monocyte-derived microparticles (MMPs), CD62P on activated platelets, soluble E-selectin (sE-selectin), and anti-oxidized low density lipoprotein (LDL) antibody in hyperlipidemia patients and control subjects. Binding of anti-GPIIb/IIIa and anti-GPIb monoclonal antibodies to platelets was not significantly different betweenhyperlipidemia patients and controls. However, expression of CD62P on platelets and levels of PMPs were higher for hyperlipidemia patients than in controls, although the difference between groups in CD62P expression was not significant (PMPs: 534 +/-63 vs. 388 +/- 47, p < 0.05; CD62P: 9.1% +/- 1.45 vs. 7.3% +/- 1.15, N.S.). Althoughthere were no differences in expression of CD36 and CD40 by monocytes between the two groups, levels of MMPs were higher in hyperlipidemia patients than in controls (MMPs: 147 +/- 21 vs. 59 +/- 8, respectively, p < 0.01). Levels of anti-oxidized LDLantibody and sE-selectin were also higher in hyperlipidemia patients. We studied theeffects of Saiko-ka-ryukotsu-borei-to on levels of these factors in patients with elevated triglyceride levels. After Saiko-ka-ryukotsu-borei-to treatment, levels of CD62P, PMPs, sE-selectin, and anti-oxidized LDL antibody were reduced significantly.Levels of triglycerides, total cholesterol and MMPs also decreased, but the changes
Page 91
201-400.txtwere not significant. These findings suggest that Saiko-ka-ryukotsu-borei-to prevents the development of vascular complications in hyperlipidemia patients.
<179>Unique Identifier 11407456Authors Lange I. Ailinger RL.Institution Escuela de Enfermeria, Science Pontificia Universidad Catolica de Chile, Santiago.Title International nursing faculty exchange model: a Chile-USA case.Source International Nursing Review. 48(2):109-16, 2001 Jun.Abstract International faculty-exchange programmes can be cost-effective methods for faculty development and enhanced student learning. Despite the increasing interest in international nursing exchanges, the literature on faculty exchanges is limited. This article examines a case study of a successful international nursing faculty-exchange programme between a university in Chile and one in the United States of America (USA), based on a model for international faculty exchange. The model includes the components of pre-exchange planning, academic activities, socio-cultural events and evaluation of outcomes. Communication is at the centre of the model and ideally should be continuous, bilateral, flexible and technological. Examples from the case study illustrate teaching strategies and ongoing education offaculty. The article concludes with suggestions for successful international nursingfaculty exchanges.
<180>Unique Identifier 11388084Authors Reed SC. Andes S.Institution School for New Learning, Depaul University, 25 E. Jackson, Chicago, Illinois 60604, USA. [email protected] Supply and segregation of nursing home beds in Chicago communities.Source Ethnicity & Health. 6(1):35-40, 2001 Feb.Abstract OBJECTIVE: Previous research suggests that a shortage of nursing home beds in Latino communities and segregation within facilities in urban settings may contribute to low utilization patterns that both Latino and African American elders exhibit. In order to explore structural barriers to nursing home care for African American and Latino families, this study examines the supply and ethnoracial composition of nursing homes in Chicago communities. DESIGN: With data from the 1990US Census of Population and Illinois' 1994 Long-Term Care Facility Survey, regression was used to determine if Latino nursing home residents in Chicago follow neighborhood residential patterns in the same way that African American nursing homeresidents do. Next the availability of nursing home beds by ethnoracial community isexamined using analysis of variance. Finally, we present correlations between the racial/ethnic composition of Chicago's facilities, community demographics and facility characteristics that have been associated with quality outcomes. RESULTS: Both African American and Latino nursing home residents follow residential housing patterns, tending to reside in facilities located in their own communities. Latino communities have the fewest beds. However, Latinos appear to be more mobile in theirutilization of nursing facilities in other communities than either African Americansor whites and tend to reside in smaller homes with fewer Medicaid recipients. CONCLUSION: Health policy makers must actively address racial and ethnic differencesin access to long-term care or risk reinforcing the effects of poverty and
Page 92

201-400.txtsegregation. In order to ensure that Latino elders living alone are not going without needed care city leaders must promote a range of culturally sensitive alternatives to nursing home care within Latino communities while promoting geographic mobility for African Americans.
<181>Unique Identifier 11387731Authors Sanchez-Lacay JA. Lewis-Fernandez R. Goetz D. Blanco C. Salman E. Davies S. Liebowitz M.Institution Columbia University, Department of Psychiatry, New York, New York, USA.Title Open trial of nefazodone among Hispanics with major depression: efficacy, tolerability, and adherence issues.Source Depression & Anxiety. 13(3):118-24, 2001.Abstract The efficacy and tolerability of nefazodone in the treatment of major depression among Spanish-monolingual Hispanics was examined and compared to historical controlsamong English-speaking, predominantly non-Hispanic subjects. Fifty monolingual Hispanic outpatients with major depression and a HAM-D17 score > or = 18 were treated with nefazodone in a flexible-dose 8-week open-label protocol. Sixty-three percent of the intent-to-treat (ITT) sample with > or = 1 efficacy visit were considered responders according to CGI-I criteria, falling within the range of response rates (58-69%) reported in six prior nefazodone trials with non-Hispanic subjects. Significant improvement was found for the ITT and completer samples in HAM-D17, HAM-D28, and SCL-90 scores and in two measures of psychosocial functioning.Endpoint mean dose in the ITT sample was 379 mg/day (SD = 170), also within the range of previous trials (321-472 mg/day). Adverse effects were not elevated, with only dry mouth (8%) reported by > 6% of subjects. However, 42% of the sample droppedout of treatment before study termination, usually because of side effects or due tofamily or work difficulties, a higher rate than previously reported for nefazodone (21-33%). This open trial finds nefazodone to be an efficacious treatment for major depression among monolingual Hispanics, with comparable efficacy to previous controlled trials among non-Hispanic subjects. Double-blind studies are required to confirm this comparable efficacy. Mean endpoint doses and adverse effect rates similar to previous trials do not support the need for reduced doses of nefazodone among Hispanics. However, an elevated rate of treatment discontinuation threatens treatment efficacy among this population. Causes for this elevated rate require explanation, given the apparently unremarkable pattern of adverse effect reports.
<182>Unique Identifier 11384708Authors Mckee MD. Cunningham M. Jankowski KR. Zayas L.Institution Department of Family Medicine, Albert Einstein College of Medicine, Bronx, New York 10461, USA. [email protected] Health-related functional status in pregnancy: relationship to depression and social support in a multi-ethnic population.Source Obstetrics & Gynecology. 97(6):988-93, 2001 Jun.Abstract OBJECTIVE: To describe perceived well-being and functional status during uncomplicated late pregnancy among low-income minority women, and to examine the relationship of functional status to depression and social support. METHODS: Hispanic and black women with low-risk pregnancies completed an interview consisting
Page 93

201-400.txtof demographics, the Medical Outcomes Study Short Form 36 (SF-36), Beck Depression Inventory-II (BDI-II), and the Norbeck Social Support Questionnaire. RESULTS: Of the155 women who were eligible and asked to participate, 41 refused for a participationrate of 74%. Results of the SF-36 showed lowest perceived well-being in the vitalityand physical role dimensions. Depressive symptomatology was high, with a mean BDI score of 15 (standard deviation 8.6). Using a BDI score of 14 as the cutoff point, over half of the sample was categorized as having significant depressive symptoms. Significantly lower functional status was seen for depressed subjects in all subscales of the SF-36 compared with nondepressed subjects. Although functional status was negatively correlated with BDI score in all dimensions (r =.23-.69), correlation of SF-36 scores with social support was much weaker (r =.06-.24). CONCLUSION: Elevated levels of depressive symptomatology are strongly correlated with lowered health-related functioning and perceived well-being. Social support is not associated with increased physical or emotional well-being but is weakly associated with mental health as measured by the SF-36.
<183>Unique Identifier 11377436Authors Niklson IA. Reimitz PE.Institution Research and Development, NV Organon. [email protected] Baseline characteristics of major depressive disorder patients in clinical trials in Europe and United States: is there a transatlantic difference?.Source Journal of Psychiatric Research. 35(2):71-81, 2001 Mar-Apr.Abstract There is a widely spread belief that different patients are being recruited into antidepressant clinical trials conducted in Europe and the USA which is probably generated by the fact that recruitment strategies vary between the two continents. In order to get an insight into the patients' characteristics in clinical studies onboth continents, we compared the baseline characteristics of depressed patients in adatabase of a cancelled development program of an antidepressant (2220 patients, Intention-to-Treat group). For the evaluation of continental differences, we compared the elements of demographics, previous psychiatric history, DSM-III-R criteria, HAM-D and MADRS total scores and separate items and/or factors and CGI severity scores at baseline. USA patients had statistically significantly higher baseline values on height, weight and BMI. European patients showed statistically significantly higher baseline severity scores on HAM-D, MADRS and CGI. Furthermore, European patients had statistically significantly higher baseline scores on HAM-D factors I ('anxiety/somatization'), VI ('sleep disturbance'), and HAM-D Angst anxiety/agitation factor, whereas USA patients had a statistically significantly higher baseline value on the Bech depression factor and the HAM-D Angst retarded depression factor. European patients appear to have a more severe depressive episodewith more anxiety and melancholic features. Some of the statistically significant differences found may be the result of a large sample size and are probably without any clinical relevance when the absolute size of the difference is taken into account. Our opinion is that the differences found in our sample between European and USA populations are much smaller than is generally expected and not of a magnitude that would question the reliability of the results obtained in our global world-wide, antidepressant drug development program. If our findings were reproducible in other antidepressant databases it would indicate that data gathered in Europe and the USA within a global antidepressant drug development can be pooled.
<184>Unique Identifier 11371665Authors Osiri M. Deesomchok U. Tugwell P.
Page 94

201-400.txtInstitution Division of Rheumatology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.Title Evaluation of functional ability of Thai patients with rheumatoid arthritis by theuse of a Thai version of the Health Assessment Questionnaire.Source Rheumatology. 40(5):555-8, 2001 May.Abstract METHODS: The Health Assessment Questionnaire (HAQ) was translated into Thai and its validity and applicability were assessed in 22 Thai patients with active rheumatoid arthritis (RA) before and after 6 months of treatment with disease-modifying anti-rheumatic drugs (DMARDs). The activities in three subcategories of the Thai HAQ were modified, including Eating, Hygiene and ACTIVITIES: Two common activities in Thai people were incorporated into the items inthe Grip and Arising domains. RESULTS: Significant improvements in mean HAQ scores and other parameters were observed after DMARD therapy. Mean HAQ scores correlated significantly with tender joint count, patient global and physician global assessments, and grip strength. CONCLUSIONS: The Thai HAQ met validity requirements and can be used in the measurement of functional capacity of Thai RA patients.
<185>Unique Identifier 11371693Authors Sweat M. O'Donnell C. O'Donnell L.Institution Johns Hopkins University School of Hygiene and Public Health, Baltimore, MD 21205,USA. [email protected] Cost-effectiveness of a brief video-based HIV intervention for African American and Latino sexually transmitted disease clinic clients.Source AIDS. 15(6):781-7, 2001 Apr 13.Abstract BACKGROUND AND OBJECTIVES: Decisions about the dissemination of HIV interventions need to be informed by evidence of their cost-effectiveness in reducing negative health outcomes. Having previously shown the effectiveness of a single-session video-based group intervention (VOICES/VOCES) in reducing incidence of sexually transmitted diseases (STD) among male African American and Latino clients attending an urban STD clinic, this study estimates its cost-effectiveness in terms of diseaseaverted. METHODS: Cost-effectiveness was calculated using data on effectiveness froma randomized clinical trial of the VOICES/VOCES intervention along with updated dataon the costs of intervention from four replication sites. STD incidence and self-reported behavioral data were used to make estimates of reduction in HIV incidence among study participants. RESULTS: The average annual cost to provide the intervention to 10 000 STD clinic clients was estimated to be US$447 005, with a cost per client of US$43.30. This expenditure would result in an average of 27.69 HIV infections averted, with an average savings from averted medical costs of US$5 544 408. The number of quality adjusted life years saved averaged 387.61, with a cost per HIV infection averted of US$21 486. CONCLUSIONS: This brief behavioral intervention was found to be feasible and cost-saving when targeted to male STD clinic clients at high risk of contracting and transmitting infections, indicating that this strategy should be considered for inclusion in HIV prevention programming.
<186>Unique Identifier 11352407Authors Guendelman S. Malin C. Herr-Harthorn B. Vargas PN.Institution
Page 95

201-400.txt Division of Health Policy and Management, and the Maternal and Child Health Program, University of California, Berkeley 94720-7360, USA. [email protected] Orientations to motherhood and male partner support among women in Mexico and Mexican-origin women in the United States.Source Social Science & Medicine. 52(12):1805-13, 2001 Jun.Abstract Previous studies suggest that favorable pregnancy outcomes among Mexican immigrantwomen in the United States may be attributed to a protective sociocultural orientation, but few have explored the attitudes and values that shape Mexican women's perceptions of motherhood. This exploratory study examines orientation towards motherhood among Mexican and Mexican-origin women living in Mexico and the United States and their perceptions of their male partners' attitudes and roles. Focus groups were conducted with 60 pregnant low-income women in rural and urban communities in Mexico with high rates of migration to the US, among immigrant communities in rural and urban California and with US-born women of Mexican descent (Mexican Americans) in urban California. Notable differences were observed between women in Mexico and the US and between immigrant and Mexican American women in California as more women articulated life plans. Life plans seemed to reflect both processes of individuation and changing gender roles. While participants in Mexico largely abided by the conventional discourse on motherhood and domesticity, immigrants in California alternated between this ethos and the discourse of working mother, depending on financial resources. In contrast, Mexican American participantsassumed multiple roles. These differing orientations may be linked to other factors,including fertility control, the amount and type of partner support, and stress during pregnancy.
<187>Unique Identifier 11332414Authors Naylor CS. Porto M. Cohen B. Garite TJ.Institution Department of Obstetrics and Gynecology, University of California, Irvine Medical Center, Orange, USA. [email protected] Pregnancy outcome in Hispanic patients with unexplained positive triple marker screening for Down syndrome.Source Journal of Maternal-Fetal Medicine. 10(1):20-2, 2001 Feb.Abstract OBJECTIVE: The objective of this study was to compare pregnancy outcomes in Hispanic patients with a positive serum triple marker screen for Down syndrome and normal fetal karyotype with Hispanic women who had a negative triple marker screen. METHODS: This prospective investigation involved Hispanic gravidas who underwent maternal serum screening. A power analysis was performed to determine the sample size. Fifty women with false-positive screens for Down syndrome were matched with a control group of 100 women with a negative screen. Adverse pregnancy outcomes were compared between the two groups. RESULTS: An adverse pregnancy outcome occurred in 14% of the study group and in 13% of controls. There were no statistically significant differences between the two groups in the incidence of preterm labor (p > 0.5), pre-eclampsia (p > 0.1), intrauterine growth restriction (p > 0.5), or fetaldemise (p > 0.5). CONCLUSION: Hispanic patients with unexplained positive triple marker screen for Down syndrome do not appear to be at increased risk for adverse pregnancy outcomes.
<188>Unique Identifier 11326795
Page 96

201-400.txtAuthors Siega-Riz AM. Popkin BM.Institution Departments of Nutrition and Maternal and Child Health, University of North Carolina in Chapel Hill, USA. [email protected] Dietary trends among low socioeconomic status women of childbearing age in the United States from 1977 to 1996: a comparison among ethnic groups.Source Journal of the American Medical Womens Association. 56(2):44-8, 72, 2001 Spring.Abstract OBJECTIVE: To identify dietary trends among low socioeconomic status women of childbearing age from three ethnic groups from 1977 to 1996. METHODS: The sample consisted of 19- to 44-year-old women at 185% of poverty with 12 years of education or less (n = 4682) from three US Department of Agriculture surveys. The Revised DietQuality Index (DQI-R) and level of folate were the main outcomes measured. Changes in food consumption for several food groups were also examined. RESULTS: Diet quality significantly improved between 1977 and 1996 for Hispanics and non-Hispanic whites. All groups had significant decreases in saturated fat intake by 1996, but only Hispanic and non-Hispanic white women significantly decreased their total fat and cholesterol intakes. Fruit and vegetable intakes remained stable. Mean intakes of calcium, iron, and folate were below recommendations at every time point for all ethnic groups. All three groups decreased their intakes of butter, margarine, egg items, bacon, high-fat red meats, and low-fiber/high-fat breads and increased their intakes of high-fiber cereals, all of which are positive. These trends were balanced, however, by decreases in medium-fiber vegetables, soy, and legumes and increases in high-fat/high-fiber breads, high-fat desserts, high-fat salty snacks, and high-fat grain-based mixed dishes. CONCLUSIONS: This study highlights problem dietary habits that public health professionals need to address in order to reduce the prevalence of diet-related chronic diseases.
<189>Unique Identifier 11322752Authors Ruiz-Beltran M. Kamau JK.Institution Department of International Health, George Washington University, School of PublicHealth and Health Services, Washington, DC 20037, USA.Title The socio-economic and cultural impediments to well-being along the US-Mexico border. [Review] [10 refs]Source Journal of Community Health. 26(2):123-32, 2001 Apr.Abstract Among all of the underdeveloped and developing countries of the world, Mexico is the only nation that shares its borders with the United States. This unique link between the two nations has created one of the most multifaceted clusters in the world. Moreover, this relationship has sketched out the direction and the role of health services and economic development of the two countries. The cultural infrastructure of the region and the political force of this association affect and contribute to the development of the economies and to the outcomes of public health programs and initiatives on each side of the border. Culture as a barrier for integration faces many challenges. The disparities in terms of access to and utilization of health services that are observed along the border are enormous. Sometimes, such disparities exist between people from the same culture, same identical ethnic group, from the same racial background and in many cases from the same family. Lack of language skills, inadequate education and a poor understanding of values are not the principal impediments to well being. Instead, political agendas and a non-global commitment to health care are the causes for such discrepancies. The economy of the region possesses unusual financial characteristics. The Maquila industry with its cheap labor practices and the North
Page 97

201-400.txtAmerican free Trade Agreement (NAFTA's) two-way crossing of billions of dollars contribute to such characteristics. In addition, well-known drug smuggling activities and the daily crossing of thousands of documented and undocumented peoplecontribute to the unusual economic characteristics of this area. The health care development and the economic growth of both countries depend on mutual efforts. Eachnation can benefit if these efforts are directed at the development of binational partnerships, the enhancement of basic services in the region and by providing trans-boundary health coverage for all residents of the region regardless of linguistic, economic and/or migratory status. [References: 10]
<190>Unique Identifier 11320614Authors Shintani TT. Beckham S. Brown AC. O'Connor HK.Institution Preventive Health Department, Waianae Coast Comprehensive Health Center, 86-260 Farrington Hwy, Waianae, HI 96792, USA.Title The Hawaii Diet: ad libitum high carbohydrate, low fat multi-cultural diet for thereduction of chronic disease risk factors: obesity, hypertension, hypercholesterolemia, and hyperglycemia.Source Hawaii Medical Journal. 60(3):69-73, 2001 Mar.Abstract OBJECTIVE: The purpose of this study was to determine the health effects of a highcarbohydrate, low fat multi-cultural traditional diet, The Hawaii Diet, fed ad libitum to an adult population. METHODS: Twenty-two adults recruited from various cultural backgrounds in Hawaii were fed, without calorie or portion size restriction, the Hawaii Diet for 21 days. The Hawaii Diet, based on familiar traditional foods from different cultures, is high in complex carbohydrate (77% of calories), low in fat (12% of calories), and moderate in protein (11% of calories). Participants were encouraged to eat to satiety. RESULTS: There was a significant weight loss on The Hawaii Diet averaging 10.8 lbs (23.8 kg) (P < .0001). Blood pressure was decreased from an average of 136.0/82.7 mm Hg to 125.5/78.9 mm Hg yielding a significant decrease of 10.4 mm Hg for systolic (P < .01). Beginning diastolic levels were normal so decreases in these values were not significant. Average lipid values also decreased with total serum cholesterol being significantlyreduced from 205.3 to 156.9 mg/dl (P < .0001); LDL from 125.9 to 94.9 mg/dl (P < .001); and HDL from 38.3 to 31.3 mg/dl (P < .0005). Triglycerides (238.7 to 152.2 mg/dl) and the Chol:HDL ratio (5.8 to 5.2) improved at marginally significant levels(P < .08). There was also a significant reduction in blood glucose levels from 112.2to 91.5 mg/dL (P < .01). CONCLUSION: The Hawaii Diet consisting of high carbohydrate, low fat ethnic meals appears to have a beneficial influence on weight loss and in decreasing systolic blood pressure, total cholesterol, LDL, and blood glucose values. Marginal improvement occurred for triglyceride levels. There was also a significant drop in HDL levels, however, the Chol:HDL was ratio did not increase. Further studies of longer duration with a control group should be conducted to test the effectiveness of The Hawaii Diet in maintaining these health benefits over a longer period of time.
<191>Unique Identifier 11309220Authors Rodriguez MA. Sheldon WR. Bauer HM. Perez-Stable EJ.Institution Department of Family and Community Medicine, University of California, San Francisco, CA 94110, USA. [email protected] The factors associated with disclosure of intimate partner abuse to clinicians.
Page 98

201-400.txtSource Journal of Family Practice. 50(4):338-44, 2001 Apr.Abstract OBJECTIVE: Our goal was to identify the prevalence, determinants of, and barriers to clinician-patient communication about intimate partner abuse. STUDY DESIGN: We conducted telephone interviews with a random sample of ethnically diverse abused women. POPULATION: We included a total of 375 African American, Latina, and non-Latina white women aged 18 to 46 years with histories of intimate partner abuse who attended 1 of 3 primary care clinics in San Francisco, California, in 1997. OUTCOMES MEASURED: We measured the relevance and determinants of past communication with clinicians about abuse and barriers to communication. RESULTS: Forty-two percent (159) of the patients reported having communicated with a clinician about abuse. Significant independent predictors of communication were direct clinician questioning about abuse (odds ratio [OR]=4.6; 95% confidence interval [CI] 3.2-6.6),and African American ethnicity (OR=1.8; 95% CI, 1.1-2.9). Factors associated with lack of communication about abuse included immigrant status (OR=0.6; 95% CI, 0.3-1.0) and patient concerns about confidentiality (OR=0.7; 95% CI, 0.5-0.9). Barriers significantly associated with lack of communication were patients' perceptions that clinicians did not ask directly about abuse, beliefs that clinicians lack time and interest in discussing abuse, fears about involving police and courts, and concerns about confidentiality. CONCLUSIONS: Clinician inquiry appears to be one of the strongest determinants of communication with patients aboutpartner abuse. Other factors that need to be addressed include patient perceptions regarding clinicians' time and interest in discussing abuse, fear of police or courtinvolvement, and patient concerns about confidentiality.
<192>Unique Identifier 11308111Authors Callister LC.Institution Brigham Young University College of Nursing, Provo, UT 84602-5544, USA. [email protected] Culturally competent care of women and newborns: knowledge, attitude, and skills. [Review] [57 refs]Source JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing. 30(2):209-15, 2001Mar-Apr.Abstract In a variety of health care settings throughout the United States and Canada, nurses are caring for women and newborns from culturally diverse backgrounds. In thetechnologically complex and bureaucratic world of health care delivery, cultural considerations in provision of care often are overlooked and neglected. The purpose of this article is to define ways in which culturally competent nursing care can be implemented. Nursing education and clinical practice guidelines are clear on the importance of gaining cultural competence. Providing culturally competent care includes understanding the dimensions of culture; moving beyond the biophysical to amore holistic approach; and seeking to increase knowledge, change attitudes, and hone clinical skills. Building on the strengths of women rather than utilizing a deficit model of health care is an essential part of providing culturally competent care. The achievement of both measurable and "soft" outcomes related to the deliveryof culturally competent care can make a critical difference in the heath and well-being of women and newborns. [References: 57]
<193>Unique Identifier 11302292Authors Hojat M. Nasca TJ. Cohen MJ. Fields SK. Rattner SL. Griffiths M. Ibarra D.
Page 99

201-400.txtde Gonzalez AA. Torres-Ruiz A. Ibarra G. Garcia A.Institution Jefferson Longitudinal Study in the Center for Research in Medical Education and Health Care, Jefferson Medical College of Thomas Jefferson University, Philadelphia,Pennsylvania 19107-5083, USA.Title Attitudes toward physician-nurse collaboration: a cross-cultural study of male andfemale physicians and nurses in the United States and Mexico.Source Nursing Research. 50(2):123-8, 2001 Mar-Apr.Abstract BACKGROUND: Inter-professional collaboration between physicians and nurses, withinand between cultures, can help contain cost and insure better patient outcomes. Attitude toward such collaboration is a function of the roles prescribed in the culture that guide professional behavior. OBJECTIVES: The purpose of the study was to test three research hypotheses concerning attitudes toward physician-nurse collaboration across genders, disciplines, and cultures. METHOD: The Jefferson Scaleof Attitudes Toward Physician-Nurse Collaboration was administered to 639 physiciansand nurses in the United States (n = 267) and Mexico (n = 372). Attitude scores werecompared by gender (men, women), discipline (physicians, nurses), and culture (United States, Mexico) by using a three-way factorial analysis of variance design. RESULTS: Findings confirmed the first research hypothesis by demonstrating that bothphysicians and nurses in the United States would express more positive attitudes toward physician-nurse collaboration than their counterparts in Mexico. The second research hypothesis, positing that nurses as compared to physicians in both countries would express more positive attitudes toward physician-nurse collaboration, was also supported. The third research hypothesis that female physicians would express more positive attitudes toward physician-nurse collaboration than their male counterparts was not confirmed. CONCLUSIONS: Collaborative education for medical and nursing students, particularly in cultures with a hierarchical model of inter-professional relationship, is needed to promote positive attitudes toward complementary roles of physicians and nurses. Faculty preparation for collaboration is necessary in such cultures before implementing collaborative education.
<194>Unique Identifier 11300170Authors Marino R. Stuart GW. Wright FA. Minas IH. Klimidis S.Institution School of Health, The University of New England Armidale, NSW, Australia. [email protected] Acculturation and dental health among Vietnamese living in Melbourne, Australia.Source Community Dentistry & Oral Epidemiology. 29(2):107-19, 2001 Apr.Abstract OBJECTIVES: To describe the relationship between acculturation and oral health status, oral health knowledge and frequency of dental visits in subjects of Vietnamese background, 18 years or older, living in Melbourne, Australia. METHODS: Oral health status was measured using the DMFS index. Oral health knowledge was estimated by responses to six specific oral preventive measures: brushing, flossing,use of fluorides, diet, and dental visits. Dental visits was measured by the number of visits in the 12 months prior to the survey. Acculturation was measured along twodimensions, psychological and behavioural, using the Psychological-Behavioural Acculturation Scale. Data were analysed using multivariate analysis to identify the combined effect of eight predictors (age, gender, occupational status, education, reason for migration, proportion of life in the host country, behavioural acculturation and psychological acculturation) against the dependent variables. RESULTS: The analysis was conducted on a sample of 147 subjects and showed significant interactions between the acculturation variables and three outcome
Page 100

201-400.txtmeasures: dental caries, knowledge of preventive measures and dental visits. Resultsindicated that acculturation was an important intervening variable. Psychological acculturation was strongly related to the three oral health outcomes, although the effect of behavioural acculturation was also apparent regarding dental status. CONCLUSIONS: This study offers several insights for understanding the mechanisms by which acculturation impacts oral health status. Interventions that simplify the cultural influence of immigrant groups by focusing on socio-demographic differences and even immigration variables to define risk groups might not produce predicted changes in oral health status.
<195>Unique Identifier 11289467Authors Harris MI.Institution National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD 20892, USA. [email protected] Racial and ethnic differences in health care access and health outcomes for adultswith type 2 diabetes.Source Diabetes Care. 24(3):454-9, 2001 Mar.Abstract OBJECTIVE: To evaluate health care access and utilization and health status and outcomes for type 2 diabetic patients according to race and ethnicity and to determine whether health status is influenced by health care access and utilization.RESEARCH DESIGN AND METHODS: National samples of Caucasians, African-Americans, and Mexican-Americans were studied in the third National Health and Nutrition Examination Survey. Information on medical history and treatment of diabetes, healthcare access and utilization, and health status and outcomes was obtained by structured questionnaires and by clinical and laboratory assessments. RESULTS: Almost all patients in each race and ethnic group had one primary source of ambulatory medical care (92-97%), saw one physician at this source (83-92%), and hadat least semiannual physician visits (83-90%). Almost all patients > or = 65 years of age had health insurance (99-100%), and for those patients < 65 years of age, Caucasians (91%) and African-Americans (89%) had higher rates of coverage than Mexican-Americans (66%). Rates of treatment with insulin or oral agents (71-78%), eye examination in the previous year (61-70%), blood pressure check in the previous 6 months (83-89%), and the proportion of hypertension that was diagnosed (84-91%) were similar for each race and ethnic group. Lower proportions of African-Americans and Mexican-Americans self-monitored their blood glucose (insulin-treated, 27 vs. 44% of Caucasians), had their cholesterol checked (62-68 vs. 81%), and had their dyslipidemia diagnosed (45 vs. 58%). African-American and Mexican-American patients had a somewhat higher proportion than Caucasian patients, with HbA1c > or = 7% (58-66 vs. 55%), blood pressure > or = 140/90 mmHg among those with diagnosed hypertension (60-65 vs. 55%), and clinical proteinuria (11-14 vs. 5%). In contrast, they had better levels of total cholesterol (> or = 240 mg/dl) (28 -30 vs. 34%) and HDL cholesterol (> or = 45 mg/dl) (46 -59 vs. 38%), and African-American and Mexican-American men were less overweight than Caucasian men (BMI > or = 30) (34-37 vs. 44%), although the opposite was true for women. LDL cholesterol levels and the proportion of patients who smoked cigarettes or were hospitalized in the past year were similar among all three groups. In logistic regression analysis, there was little evidence that levels of blood glucose, blood pressure, lipids, or albuminuriawere associated with access to or utilization of health care or with socioeconomic status. CONCLUSIONS: There are some differences by race and ethnicity in health careaccess and utilization and in health status and outcomes for adults with type 2 diabetes. However, the magnitude of these differences pale in comparison with the suboptimal health status of all three race and ethnic groups relative to establishedtreatment goals. Health status does not appear to be influenced by access to health care.
Page 101

201-400.txt
<196>Unique Identifier 11274491Authors Drake RE. Essock SM. Shaner A. Carey KB. Minkoff K. Kola L. Lynde D. Osher FC. Clark RE. Rickards L.Institution New Hampshire--Dartmouth Psychiatric Research Center, Lebanon, New Hamphire 03766,USA. [email protected] Implementing dual diagnosis services for clients with severe mental illness. [Review] [87 refs]Source Psychiatric Services. 52(4):469-76, 2001 Apr.Abstract After 20 years of development and research, dual diagnosis services for clients with severe mental illness are emerging as an evidence-based practice. Effective dual diagnosis programs combine mental health and substance abuse interventions thatare tailored for the complex needs of clients with comorbid disorders. The authors describe the critical components of effective programs, which include a comprehensive, long-term, staged approach to recovery; assertive outreach; motivational interventions; provision of help to clients in acquiring skills and supports to manage both illnesses and to pursue functional goals; and cultural sensitivity and competence. Many state mental health systems are implementing dual diagnosis services, but high-quality services are rare. The authors provide an overview of the numerous barriers to implementation and describe implementation strategies to overcome the barriers. Current approaches to implementing dual diagnosis programs involve organizational and financing changes at the policy level,clarity of program mission with structural changes to support dual diagnosis services, training and supervision for clinicians, and dissemination of accurate information to consumers and families to support understanding, demand, and advocacy. [References: 87]
<197>Unique Identifier 11277477Authors D'Costa R. Ruygrok PN. Coverdale HA. Agnew TM. Gibbs HC. Reddy D. Haydock DA. Kerr AR. Whitlock RM.Institution Monash University, Melbourne.Title Outcome following heart transplantation in Maori and Polynesian patients: a comparison with European New Zealanders.Source New Zealand Medical Journal. 114(1125):44-6, 2001 Feb 9.Abstract AIM: To compare demographic, clinical and outcome data of Maori and Polynesian with New Zealand European heart transplant patients. METHODS: A retrospective analysis was made of data from the 104 patients who underwent heart transplantation at Green Lane Hospital over a period of twelve years, of whom 79 were European, 23 Maori/Polynesian, and two Asian. Clinical characteristics, blood group, HLA matchingand outcomes of recipients were compared. RESULTS: There was no significant difference in age and gender between the two groups. Maori and Polynesian patients were heavier, had a greater body mass index and were more likely to have rheumatic heart disease than their European counterparts. Maori/Polynesian patients were predominantly blood group A, whilst European patients were mainly group O. The waiting time for a donor heart was similar in both groups. There was no significant difference in number of rejection episodes and survival. CONCLUSIONS: Green Lane Hospital has the largest international experience of heart transplantation in Maori and Polynesian patients. Although there are some differences in clinical profile,
Page 102

201-400.txtoutcome in terms of rejection episodes and survival is similar in the two groups.
<198>Unique Identifier 11267406Authors Nair S. Thuluvath PJ.Institution Department of Medicine, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.Title Does race-matched liver transplantation offer any graft survival benefit?.Source Transplantation Proceedings. 33(1-2):1523-4, 2001 Feb-Mar.
<199>Unique Identifier 11267964Authors Bathe OF. Caldera H. Hamilton-Nelson K. Franceschi D. Sleeman D. Levi JU. Livingstone AS.Institution Department of Surgery, University of Miami, Miami, Florida. [email protected] Influence of Hispanic ethnicity on outcome after resection of carcinoma of the head of the pancreas.Source Cancer. 91(6):1177-84, 2001 Mar 15.Abstract BACKGROUND: Poor outcomes in Hispanic patients have been reported for tumors at a number of sites. The authors sought to determine whether a similar phenomenon occursin Hispanics after the resection of solid epithelial tumors of the head of the pancreas. METHODS: Between 1983-1995, 273 patients with noncystic epithelial carcinoma of the head of the pancreas were evaluated. Resection was accomplished in 104 patients (38%); these patients were the focus of the current retrospective review. Of the patients who underwent resection, 26 (25%) were Hispanic and 78 (75%)were non-Hispanic. RESULTS: Although Hispanic patients tended to present at a significantly younger age and their serum bilirubin level was significantly higher, no other differences in clinical characteristics were observed. After resection, Hispanic patients had a median survival of only 11.4 months, whereas the non-Hispanic group had a median survival of 21.7 months (P = 0.009). Hispanic ethnicity, as well as age > 74 years and jaundice at the time of presentation also were found to be significant prognostic factors on multivariate analysis. Hispanic patients did not present with more advanced disease and no delays in assessment by aphysician or in proceeding to surgery were observed. Furthermore, the rate of resection was the same in Hispanic patients and non-Hispanic patients. Long-term survival after palliative bypass was similarly worse in the Hispanic subgroup. CONCLUSIONS: Hispanic patients treated at the study center appeared to have a diminished survival after resection of a tumor of the head of the pancreas. No treatment-related factors were identified that could explain this discrepancy in outcome. Copyright 2001 American Cancer Society.
<200>Unique Identifier 11246064Authors Stewart S. Blue L. Capewell S. Horowitz JD. McMurray JJ.Institution Department of Cardiology, The Queen Elizabeth Hospital/University of Adelaide, Adelaide, Australia.
Page 103

201-400.txtTitle Poles apart, but are they the same? A comparative study of Australian and Scottishpatients with chronic heart failure.Source European Journal of Heart Failure. 3(2):249-55, 2001 Mar.Abstract This paper reports on an international comparison of the characteristics, treatment and health outcomes of chronic heart failure (CHF) patients discharged from acute hospital care in Australia and Scotland. The baseline characteristics andtreatment of 200 CHF patients recruited to a randomised study of a non-pharmacological intervention in Australia and 157 CHF patients concurrently recruited to a similar study in Scotland were compared. Subsequent health outcomes (including survival and readmission) within 3 months of discharge in those patients who received usual post-discharge care in Australia (n=100) and Scotland (n=75) werealso compared. Individuals in both countries were predominantly old and frail with significant comorbidity likely to complicate treatment. Similar proportions of Australian and Scottish patients were prescribed either a 'high' (20 vs. 18%) or medium (64 vs. 66%) dose of an angiotensin-converting enzyme inhibitor. Proportionately more Australian patients were prescribed a long-acting nitrate, digoxin and/or a beta-blocker. At 3 months post-discharge, 57 of the 100 (57%: 95% CI 47--67%) Australian and 37 of the 75 (49%: 95% CI 38--61%) Scottish patients assigned to 'usual care' remained event-free (NS). Similarly, 15 vs. 12% required > or =2 unplanned readmission (NS) and 16 vs. 19% of Australian and Scottish patients,respectively, died (NS). Australian and Scottish patients accumulated a median of 0.6 vs. 0.9 days, respectively, of hospitalisation/patient/month (NS). On multivariate analysis (including country of origin), unplanned readmission or death was independently correlated with severe renal impairment (adjusted odds ratio 4.4, P<0.05), a previous hospitalisation for CHF (2.3, P<0.05), longer index hospitalisation (2.7 for >10 days, P<0.05) and greater comorbidity (1.3 for each incremental unit of the Charlson Index, P=0.05). Health outcomes among predominantlyold and frail CHF patients appear to be independent of the health-care system in which the patient is managed and more likely to be dependent on the syndrome itself.
Page 104

401-600.txt<1>Unique Identifier 11238701Authors Hoffman RM. Gilliland FD. Eley JW. Harlan LC. Stephenson RA. Stanford JL. Albertson PC. Hamilton AS. Hunt WC. Potosky AL.Institution Medicine Service, Department of Veterans Affairs Medical Center, Albuquerque, NM 87108, USA. [email protected] Racial and ethnic differences in advanced-stage prostate cancer: the Prostate Cancer Outcomes Study.Source Journal of the National Cancer Institute. 93(5):388-95, 2001 Mar 7.Abstract BACKGROUND: African-Americans have twice the risk of non-Hispanic whites for presenting with advanced-stage prostate cancer. To investigate the reasons for this difference, we evaluated the association between race/ethnicity and advanced-stage prostate cancer, adjusting for demographic, socioeconomic, clinical, and pathologic factors. METHODS: A population-based cohort of 3173 men diagnosed with prostate cancer between October 1, 1994, and October 31, 1995, was analyzed. Medical record abstracts and self-administered survey questionnaires were used to obtain information regarding race/ethnicity, age, marital status, insurance status, educational level, household income, employment status, comorbidity, urinary function, prostate-specific antigen level, tumor grade, and clinical stage. The oddsratio (OR) for advanced-stage prostate cancer was estimated with weighted logistic regression analysis. All P: values were two-sided. RESULTS: Clinically advanced-stage prostate cancers were detected more frequently in African-Americans (12.3%) and Hispanics (10.5%) than in non-Hispanic whites (6.3%). Socioeconomic, clinical, and pathologic factors each accounted for about 15% of the increased relative risk. After adjusting for all covariates, the risk remained statistically significantly increased for African-Americans (OR = 2.26; 95% confidence interval [CI] = 1.43 to 3.58) but not for Hispanics (OR = 1.23; 95% CI = 0.73 to 2.08). CONCLUSION: Traditional socioeconomic, clinical, and pathologic factors accounted for the increased relative risk for presenting with advanced-stage prostate cancer in Hispanic but not in African-American men.
<2>Unique Identifier 11148584Authors Kagawa-Singer M.Institution Department of Community Health Sciences, University of California at Los Angeles School of Public Health and Asian American Studies, Los Angeles, California 90095-1772, USA. [email protected] From genes to social science: impact of the simplistic interpretation of race, ethnicity, and culture on cancer outcome.Source Cancer. 91(1 Suppl):226-32, 2001 Jan 1.
<3>Unique Identifier 11148586Authors Fouad MN. Partridge E. Wynn T. Green BL. Kohler C. Nagy S.Institution University of Alabama at Birmingham, Birmingham, Alabama 35294-4410, USA. [email protected]
Page 1

401-600.txt Statewide Tuskegee Alliance for clinical trials. A community coalition to enhance minority participation in medical research.Source Cancer. 91(1 Suppl):237-41, 2001 Jan 1.Abstract BACKGROUND: Cancer mortality rates for all sites are nearly 2.5 times greater for African-Americans compared with whites. In addition, there are data implying that cancer treatment outcomes for minorities are unfavorable compared with whites. Whether this is due to poor access to health care or a biologic property of malignancies occurring in specific populations remains to be determined. Because of these unknown factors, targeting minorities for clinical trials may contribute toward the reduction of the overall morbidity and mortality associated with specificcancers. METHODS: The current study describes the establishment of a genuine collaborative partnership between the targeted minority community and clinical investigators at the University of Alabama at Birmingham. This partnership was formed for the purpose of identifying strategies that would enhance the accrual and retention of minority participants into current and future cancer prevention and control trials. Focus groups and key informant interviews were conducted to ascertain the community's perception of participating in clinical trials. RESULTS: The majority of focus group participants were unclear regarding the nature of clinical trials. Participants indicated that they would participate in research studies if they received adequate information regarding the purpose and benefits of the study, and if the charge came from a pastor or physician. Barriers to participation included time commitments, family obligations, whether blood was involved, and past experiences. The majority of the participants indicated that their knowledge of the Tuskegee Syphilis Study did not influence their decision to participate in research. A major outcome of the conference was the formation of the Statewide Tuskegee Alliance Coalition. The planning coalition decided to continue their efforts to work with communities and promote cancer awareness among minorities. After the conference, the coalition conducted several meetings and in July 1998, 1 year after the conference, the coalition selected a chair, co-chair, and a formal name for the organized group. CONCLUSIONS: The planning, development, and implementation of this conference provided a valuable experience for researchersand community members. It was discovered that community involvement in the early phase of this project contributed to its success. Furthermore, the partnership that developed between researchers (academic institutions) and communities successfully provided an infrastructure that supported the interest of both groups. Copyright 2001 American Cancer Society.
<4>Unique Identifier 11189795Authors Philis-Tsimikas A. Walker C.Institution Project Dulce, Whittier Institute for Diabetes, La Jolla, California, USA.Title Improved care for diabetes in underserved populations.Source Journal of Ambulatory Care Management. 24(1):39-43, 2001 Jan.Abstract Diabetes mellitus (DM) is a common chronic health condition among the adult population in the United States. DM is more prevalent and complications higher in Latinos, possibly due to inadequate medical and self-care as well as inaccurate culture-bound beliefs. Project Dulce is a nurse-managed DM educational and treatmentprogram designed to measure the effect on clinical outcomes, adherence to American Diabetes Association and American Heart Association standards of care, and cultural beliefs in 210 high risk (HbA1c > 9.5%) and 346 lower risk (HbA1c < 9.5%) indigent Latinos with DM. METHODS: All patients were given a 12-week culturally sensitive educational program. Nurse manager/certified diabetes educators working together with primary care providers treated high-risk patients using protocols from Staged Diabetes Management. Physical exam and biochemical markers of DM were followed. Pre-
Page 2
401-600.txtand post-program questionnaires measured changes in diabetes knowledge, cultural beliefs practices, treatment satisfaction, and health locus of control. Chart reviews of Latinos with diabetes (n = 311) not enrolled in Project Dulce provided the case controls. RESULTS: After 1 year, the high-risk group showed significant improvements in HbA1c (11.5% to 8.3%, p < 0.0001), total cholesterol (219 to 181 mg/dL, p < 0.00001), SBP (129 to 122 mmHg, p < 0.03), and DBP (79 to 75 mmHg, p < 0.006). Pre- and post-test evaluations showed improved diabetes knowledge (p = .024), treatment satisfaction (p = .001) and internal locus of control (p = 0.04), and fewer inaccurate culture-bound beliefs (p = 0.001). Compliance was 100% in the high-risk group in obtaining HbAlc, lipids, urine microalbumin, and foot exams and 47% in obtaining eye exams, while the case controls had 28%, 46%, 31%, 14%, and 6% respectively. Mean TC and LDL values improved in Project Dulce patients compared to case controls (181 vs 221 Img/dL, p < 0.0001 and 99 vs 1241 mg/dL, p < 0.0004). CONCLUSION: Patients enrolled in Project Dulce had significantly improved clinical outcomes, adherence to standards of care, and culture bound beliefs. Nurse managed diabetes management programs that are culturally sensitive may decrease the incidence of complications of diabetes and improve health outcomes.
<5>Unique Identifier 12528721Authors Greiner KA.Title Patient-provider relations--understanding the social and cultural circumstances ofdifficult patients.Source Bioethics Forum. 16(3):7-12, 2000 Fall.Abstract Clinicians who have understanding and insight into the social and cultural background of their patients will be better prepared to foster the mutual respect required for effective chronic disease management. This paper will develop an argument linking respect in patient-physician relations to the social determinants of health.
<6>Unique Identifier 11982107Authors dela Cruz FA. Padilla GV. Agustin EO.Institution FNP Program, School of Nursing, Azusa Pacific University, Azusa, California, USA.Title Adapting a measure of acculturation for cross-cultural research. [Review] [40 refs]Source Journal of Transcultural Nursing. 11(3):191-8, 2000 Jul.Abstract Although Filipino Americans are projected to become the largest Asian American ethnic group in this millennium, no acculturation measure existed for this group. This article describes a systematic and replicable process used in adapting and modifying A Short Acculturation Scale for Hispanics (ASASH) for use with Filipino Americans. It depicts the multiple and iterative steps of translation and backtranslation to produce A Short Acculturation Scale for Filipino Americans (ASASFA) in English and in Tagalog--the Philippine national language. Also, it describes the methods undertaken for the measures to achieve linguistic and cross-cultural validity through content, technical, experiential, semantic, and conceptual equivalence. With the dearth of linguistically and culturally valid measures for immigrant populations, the adaptation of valid measures developed for other cultures remains a viable option. [References: 40]
Page 3

401-600.txt
<7>Unique Identifier 11982074Authors Liu HG. Moore JF.Institution University of Nevada, Reno, USA.Title Perinatal care: cultural and technical differences between China and the United States.Source Journal of Transcultural Nursing. 11(1):47-54, 2000 Jan.Abstract A comparison of perinatal care in the U.S. and China is presented. Perinatal care has made tremendous achievements in both countries since mid-century. However, the outcomes in the two cultures are different due to the different focus on caring concepts, the strengths of a nursing philosophy, and the emphasis on the nursing role in maternal care. Perinatal family in the U.S. will have advantages in perinatal education physical facilities, and a philosophy of care. North American women have greater access to early prenatal and continuing care, and less infant mortality. Chinese women have less access to qualified nursing services, higher infant mortality rates, and limited perinatal education. Overall, Chinese perinatal care is far behind that which is found in the U.S. This comparison analyzes the strengths and weaknesses in both cultures with a focus on change that will produce healthier and more consistent optimal outcomes.
<8>Unique Identifier 11935520Authors Parkman CA.Institution California State University, Sacramento, USA.Title Integrating CAM into traditional health care.Source Case Manager. 11(2):30-2, 2000 Mar-Apr.
<9>Unique Identifier 11908390Authors Vick VC. Harfst S.Institution Department of Periodontics, School of Dentistry, University of Louisville, Louisville, Kentucky, USA.Title The Oral Risk Assessment and Early Intervention System--a clinician's tool for integrating the bio/psycho/social risk into oral disease interventions.Source Compendium of Continuing Education in Dentistry. Supplement. (30):57-64; quiz 67,2000.Abstract An association between oral diseases and systemic diseases has been suspected for centuries. More recently, investigation has provided insight into the impact of psychologic factors, social value systems, beliefs about disease processes and predictive treatment outcomes. Historically, dentistry has focused primarily on the restoration of physical function rather than broader multifactorial issues that impact long-term health maintenance. Dental patients are a complex interaction of biologic susceptibilities, lifestyle behaviors, values, and disease risk variables,
Page 4

401-600.txtwhich require an interdisciplinary approach to provide optimal health care. This article provides information-processing tools to assist clinicians in developing appropriate patient interventions by employing on Oral Risk Assessment and Early Intervention System.
<10>Unique Identifier 11833976Authors Knight BG. Silverstein M. McCallum TJ. Fox LS.Institution Andrus Gerontology Center, University of Southern California, Los Angeles, 90089-0191, USA. [email protected] A sociocultural stress and coping model for mental health outcomes among African American caregivers in Southern California.Source Journals of Gerontology Series B-Psychological Sciences & Social Sciences. 55(3):P142-50, 2000 May.Abstract A sociocultural stress and coping model to explain emotional distress among caregivers of family members who have dementia across ethnic and cultural groups is presented and explored in a sample of 41 African American and 128 non-African American caregivers. In this sample, African American caregivers reported lower levels of burden but equal levels of depression and anxiety. In the structural equation model, previous reports that African Americans' lower appraisal of caregiving as burdensome resulted in lower levels of emotional distress were confirmed. However, in this model, this pathway was counterbalanced by a tendency ofAfrican American caregivers to use emotion-focused coping and, therefore, increase emotional distress. African American caregivers were also younger and in poorer health, factors which tend to increase both burden and emotional distress outcomes. As suggested by the sociocultural stress and coping model, the influences of ethnic group variables on stress and coping processes are complex and multidirectional.
<11>Unique Identifier 11558104Authors Mackay M. Hassan AM.Institution Birmingham Automotive Safety Centre, University of Birmingham, Birmingham, UK.Title Age and gender effects on injury outcome for restrained occupants in frontal crashes: a comparison of UK and US data bases.Source Annual Proceedings/Association for the Advancement of Automotive Medicine. 44:75-91, 2000.Abstract Field accident data from NASS/CDS in the US and CCIS in the UK are compared. The UK sample is deliberately weighted to conform to the same AIS proportions (within AIS 2-6) as the weighted NASS data so that crash severity distributions can be compared for various selected outcomes. Age and gender have a significant effect on the delta V distributions and median delta V values. These differences are documented both for overall AIS 2-6, 3-6, and 4-6, and also for body regions of the head, neck, chest, abdomen and upper and lower extremities. Anomalies between the two samples are profound which raises doubts about the recording of belt use in NASSand the calculation of delta V at lower crash severities.
<12>Unique Identifier
Page 5

401-600.txt 11449468Authors Paranjpe P. Patki P. Joshi N.Institution Medinova Diagnostic Services, 1319, Jungli Maharaj Road, Pune 411005, India.Title Efficacy of an indigenous formulation in patients with bleeding piles: a preliminary clinical study.Source Fitoterapia. 71(1):41-5, 2000 Feb.Abstract The results of the clinical assessment of a multiherbal indigenous formulation on 22 patients with bleeding piles are reported.
<13>Unique Identifier 11317592Authors Sebit MB. Chandiwana SK. Latif AS. Gomo E. Acuda SW. Makoni F. Vushe J.Institution Department of Psyhiatry, Faulty of Medicine, University of Zimbabwe, P O Box A 178, Avondale, Harare, Zimbabwe.Title Quality of life evaluation in patients with HIV-I infection: the impact of traditional medicine in Zimbabwe.Source Central African Journal of Medicine. 46(8):208-13, 2000 Aug.Abstract OBJECTIVES: To evaluate the impact of phytotherapy (traditional medicine) in persons with HIV infection and to assess the quality of life of those persons with respect to HIV disease progression, including sociodemographic characteristics. DESIGN: A community based open label non-intervention and uncontrolled cohort study.SETTING: Blair Research Institute Clinic. SUBJECTS: A total of 105 HIV infected persons at various stages of HIV infection. Seventy-nine percent were on phytotherapy (PT) and 21% on conventional medical care (CMC). MAIN OUTCOME MEASURES:(a) Assessment of quality of life of HIV infected persons on phytotherapy using the WHOQol instrument, and (b) assessment of quality of life of those persons in relation to the HIV disease progression using CD4 cell counts and viral load as measure of disease progression. METHODS: We interviewed 105 patients with various stages of HIV-I infection in a community based cohort study from June 1996 to May 1998, in Harare. The 96 (91.4%) asymptomatic and six (8.6%) symptomatic patients underwent regular physical examinations and had blood drawn for laboratory tests at the baseline afterwards at three month intervals over a period of two years. RESULTS: The mean (s.d.) age was 34.9 (7.3) years; 64.4% were women and 60.3% were married. In multi variate analyses, age was significantly correlated with the level of independence domains (p = 0.032), whereas, gender was significantly correlated with social relationships' domains (p = 0.034). The type of treatment received was significantly correlated with spiritual domains (p = 0.045). Proportions of scores on five domains measuring different aspects of quality of life for patients on phytotherapy were much lower than those on conventional therapy (p < 0.0001, for allvariables). CONCLUSION: Our data support the role of phytotherapy in improving the quality of life of HIV-I infected patients, yet its pharmacological basis is unknown. The WHOQol instrument is a good measure of quality of life for patients with HIV infection.
<14>Unique Identifier 11307227Authors Scott AA. Hatch JP. Rugh JD. Hoffman TJ. Rivera SM. Dolce C. Bays RA.Institution
Page 6

401-600.txt Department of Pediatrics, University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, Texas 78284-7792, USA. [email protected] Psychosocial predictors of satisfaction among orthognathic surgery patients.Source International Journal of Adult Orthodontics & Orthognathic Surgery. 15(1):7-15, 2000 Spring.Abstract This study assessed the usefulness of selected psychosocial tests and demographic measures in identifying satisfied versus dissatisfied patients who received orthognathic surgery. Data were collected prior to placement of orthodontic appliances, 1 to 2 weeks presurgery, and at 1 week, 8 weeks, 6 months, 12 months andand 2 years postsurgery. The Revised Symptom Checklist-90 (SCL-90-R) scales, the Eysenck Personality Inventory (EPI), the Sickness Impact Profile (SIP), and the OralHealth Status Questionnaire (OHSQ) were used as independent variables. Indicators from the Post-Surgical Patient Satisfaction Questionnaire (PSPSQ), which assesses patient satisfaction regarding psychosocial issues, oral functioning, and esthetics,served as a postsurgical dependent measure of patient satisfaction. Thirty-one male and 86 female subjects participated in the multisite randomized trial comparing rigid and wire fixation. Patient age was significantly correlated with patient satisfaction from 8 weeks postsurgery through 2 years postsurgery. Older patients appear to report greater postsurgical satisfaction in comparison to younger patients. The postsurgical OHSQ (esthetics subscale) and postsurgical PSPSQ (satisfaction) were significantly related at 8 weeks, 6 months, 12 months, and 2 years postsurgery. Additionally, PSPSQ (satisfaction) and postsurgical OHSQ (generaloral health scale) were correlated at 12 months. The EPI, SIP, and SCL-90-R were notsignificantly associated with postsurgical satisfaction when assessing the entire study sample. Postsurgical qualitative data from the PSPSQ indicated that 50% of thepatients reported positive outcomes in oral functioning. Sixty-five percent reportedesthetic improvements, and 37% reported neurosensory loss.
<15>Unique Identifier 11261051Authors Tonuma M. Winbolt M.Institution Melbourne Extended Care and Rehabilitation Service, PO Box 7000, Carlton South, Victoria 3053, Australia. [email protected] From rituals to reason: creating an environment that allows nurses to nurse.Source International Journal of Nursing Practice. 6(4):214-8, 2000 Aug.Abstract From rituals to reason is a description of the journey that one unit is taking to overturn traditional nursing culture and create an environment that will enable nurses to care for people. In our experience the reality of day-to-day nursing practice does not always correspond to the nursing rhetoric of individualised holistic nursing care for each person. We identified that traditional nursing culture, with a focus on task orientation, rigid hierarchical structures and resultant disempowerment of staff, is an impediment to delivery of patient-centered care. We introduced changes to management structures, care delivery models and staffbehaviours with the aim of overturning this traditional nursing culture. Changing clinical practice to focus on client outcomes and provide a relaxed and patient-centered environment was easier to achieve than staff empowerment and their full involvement in decision making and innovation.
<16>Unique Identifier 11224983
Page 7

401-600.txtAuthors Waldram JB.Institution Department of Psychology, University of Saskatchewan.Title The efficacy of traditional medicine: current theoretical and methodological issues. [Review] [79 refs]Source Medical Anthropology Quarterly. 14(4):603-25, 2000 Dec.Abstract The efficacy of traditional medicine is an issue that continues to vex medical anthropology. This article critically examines how the efficacy of traditional medicine has been conceived, operationalized, and studied and argues that a consensus remains elusive. Efficacy must be seen as fluid and shifting, the product of a negotiated, but not necessarily shared, understanding by those involved in the sickness episode, including physicians/healers, patients, and members of the community. Medical anthropology needs to return to the field to gather more data on indigenous understandings of efficacy to counteract the biases inherent in the utilization of biomedical understandings and methods characteristic of much previouswork. [References: 79]
<17>Unique Identifier 11272344Authors Korenbrot CC. Dudley RA. Greene JD.Institution Institute for Health Policy Studies, University of California San Francisco, USA. [email protected] Changes in births to foreign-born women after welfare and immigration policy reforms in California.Source Maternal & Child Health Journal. 4(4):241-50, 2000 Dec.Abstract OBJECTIVES: To determine whether passage of welfare and immigration policies was followed in California by changes in births to foreign-born women in California withrespect to total numbers, payer sources, prenatal care use, or health outcomes. METHODS: Comparison of births to foreign-born and US-born women from 1990 to 1997 using adjusted odds ratios generated with multivariate logistic regression. RESULTS:Policies passed in 1994 and 1996 were followed by decreases in adjusted odds of births to foreign-born women with prenatal Medicaid coverage, without a corresponding increase in uninsured foreign-born women. There was no decline in the use of prenatal care by foreign-born women, and no worsening of birth outcomes afterpassage of the reforms. Foreign-born women, however, remained more likely to have inadequate prenatal care than US-born women, and the improvement in outcomes that occurred for US-born women from 1994 to 1997 did not occur for foreign-born women. CONCLUSIONS: In spite of the fact that pregnant immigrant women remained eligible for Medicaid after passage of welfare and immigration policies in California, the volume of births to foreign-born women using Medicaid declined. The lack of a corresponding increase in births to uninsured foreign-born women appears to have prevented deterioration in the use of prenatal care or birth outcomes.
<18>Unique Identifier 11214095Authors Biritwum RB. Welbeck J. Barnish G.Institution Department of Community Health, Ghana Medical School, Korle Bu, Accra, Ghana. [email protected]
Page 8

401-600.txtTitle Incidence and management of malaria in two communities of different socio-economiclevel, in Accra, Ghana.Source Annals of Tropical Medicine & Parasitology. 94(8):771-8, 2000 Dec.Abstract Two adjacent communities of differing socio-economic levels were selected, in Accra, Ghana, for the study of the home management of malaria. The youngest child ineach selected household, each of which had a child aged < 5 years, was recruited forweekly follow-up, following informed consent. Malaria was the most common condition reported by the 'caregivers' (mothers of the subjects and others caring for the subjects) in each community, with 2.0 episodes of clinical malaria/child during the 9-month study. Most (89%) of the caregivers in the better-off community had been educated beyond primary-school level, but 55% of the caregivers in the poorer community had either received no formal education or only primary-school education. This difference was also reflected by the educational facilities provided to the children studied: 52% of the those in the better-off community attended nurseries, kindergartens or creches, compared with 8% of the children investigated in the poorer community. The proportion of caregivers who purchased drugs without prescription or used left-over drugs to treat clinical malaria in the children was higher in the poorer community (82% v. 53%), and a child from the poorer community was less likely to have been taken to a clinic or hospital to be treated for malariathan a child from the better-off community (27% v. 42%). During the follow-up periodtwo children died, one from each community. Treatment of malaria in young children is likely to be less effective in the poorer community, where a lack of economic access to health services was demonstrated.
<19>Unique Identifier 11189098Authors Kagawa-Singer M.Institution UCLA School of Public Health and Asian American Studies, Los Angeles, CA 90095-1772, USA. [email protected] Improving the validity and generalizability of studies with underserved U.S. populations expanding the research paradigm.Source Annals of Epidemiology. 10(8 Suppl):S92-103, 2000 Nov.Abstract The gap in cancer incidence and mortality between ethnic minority groups and European Americans in the U.S. is significant and growing. Compared with a drop in incidence and mortality rates in the U.S. since 1992, the rates for ethnic minority groups have increased or stayed the same. A major transformation in the predominantly deductive social and behavioral research paradigm in cancer is required to reduce these disparities in cancer outcomes and improve the quality of life for ethnic minority populations with cancer. This article highlights the fundamental changes that are required to transform the prevalent paradigm for socialand behavioral research in cancer care from a monocultural, Eurocentric framework toa multicultural one. Use of the expanded framework would enhance the scientific rigor, validity, generalizability, applicability, and acceptability of multiculturalbehavioral research. The strategies developed from such research would have a greater likelihood of success in providing optimal cancer care for underserved populations and reduce the disparities in cancer outcomes between U.S. ethnic minority populations and the white population. Examples from the cancer literature are used to illustrate each of the seven steps of the expanded paradigm.
<20>Unique Identifier 11194126
Page 9

401-600.txtAuthors Siegel C. Davis-Chambers E. Haugland G. Bank R. Aponte C. McCombs H.Institution Epidemiology & Health Services Research Laboratory, Nathan S. Kline Institute for Psychiatric Research, 140 Old Orangeburg Road, Building 35, Orangeburg, NY 10962, USA. [email protected] Performance measures of cultural competency in mental health organizations.Source Administration & Policy in Mental Health. 28(2):91-106, 2000 Nov.Abstract The authors utilized numerous documents created by advisory groups, expert panels and multicultural focus groups to develop performance measures for assessing the cultural competency of mental health systems. Competency was measured within three levels of organizational structure: administrative, provider network, and individualcaregiver. Indicators, measures and data sources for needs assessment, information exchange, services, human resources, plans and policies, and outcomes were identified. Procedures for selection and implementation of the most critical measures are suggested. The products of this project are broadly applicable to the concerns of all cultural groups.
<21>Unique Identifier 11151290Authors Brown SA. Harrist RB. Villagomez ET. Segura M. Barton SA. Hanis CL.Institution School of Nursing, University of Texas at Austin, 1700 Red River, Austin, TX 78701, USA. [email protected] Gender and treatment differences in knowledge, health beliefs, and metabolic control in Mexican Americans with type 2 diabetes.Source Diabetes Educator. 26(3):425-38, 2000 May-Jun.Abstract PURPOSE: The purpose of this project was to describe metabolic control, knowledge,and health beliefs of Mexican Americans with type 2 diabetes. METHODS: The study site was Starr County, Texas, a border community located on the Rio Grande River andbordering northern Mexico. Of the total sample of 360 persons, 252 agreed to participate in this intervention study and were randomized either to the treatment group or the control group that waited 1 year to begin the intervention. RESULTS: The majority of individuals were Spanish-speaking females with a mean age of 54 years and a mean diabetes duration of 8 years. For those treated with diet only, males exhibited higher fasting blood glucose levels than females. Gender effects were seen for cholesterol level, with females exhibiting higher levels than males. Males expressed stronger perceptions of control and social support for diet. Bivariate relationships were found between acculturation and diabetes knowledge. Thehealth belief subscales of control and impact on job together explained 16% of the variance in HbA1c values. CONCLUSIONS: Males and females held differing beliefs about ability to control their diabetes and degree of social support for diet. The impact of gender differences on ability to integrate diabetes self-care and on effectiveness of diabetes programs has not been determined but should be considered in future research.
<22>Unique Identifier 11147590Authors Roetzheim RG. Gonzalez EC. Ferrante JM. Pal N. Van Durme DJ. Krischer JP.Institution University of South Florida, Department of Family Medicine, Tampa 33612, USA.
Page 10

[email protected] Effects of health insurance and race on breast carcinoma treatments and outcomes.Source Cancer. 89(11):2202-13, 2000 Dec 1.Abstract BACKGROUND: The authors hypothesized that insurance payer and race would influencethe care and outcomes for patients with breast carcinoma. METHODS: The authors examined treatments and adjusted risk of death (through 1997) for all incident casesof breast carcinoma occurring in Florida in 1994 (n = 11,113) by using state tumor registry data. RESULTS: Patients lacking health insurance were less likely to receive breast-conserving surgery (BCS) compared with patients who had private health insurance. Among patients insured by Medicare, those belonging to a health maintenance organization (HMO) were more likely to receive BCS but less likely to receive radiation therapy after BCS. Non-Hispanic African Americans had higher mortality rates even when stage at diagnosis, insurance payer, and treatment modalities used were adjusted in multivariate models (adjusted risk ratio [RR], 1.35; 95% confidence interval [CI], 1.12-1.61; P = 0.001). Patients who had HMO insurance had similar survival rates compared with those with fee-for-service (FFS) insurance. Among non-Medicare patients, mortality rates were higher for patients whohad Medicaid insurance (RR, 1.58, 95% CI, 1.18-2.11; P = 0.002) and those who lackedhealth insurance (RR, 1.31; 95% CI, 1.03-1.68; P = 0.03) compared with patients who had commercial FFS insurance. There were no insurance-related differences in survival rates, however, once stage at diagnosis was controlled. CONCLUSIONS: As a result of later stage at diagnosis, patients with breast carcinoma who were uninsured, or insured by Medicaid, had higher mortality rates. Mortality rates were also higher among non-Hispanic African Americans, a finding that was not fully explained by differences in stage at diagnosis, treatment modalities used, or insurance payer.
<23>Unique Identifier 11138745Authors Ryan M. Twibell R. Brigham C. Bennett P.Institution School of Nursing, Ball State University, Muncie, Indiana 47306, USA.Title Learning to care for clients in their world, not mine.Source Journal of Nursing Education. 39(9):401-8, 2000 Dec.Abstract Current literature and trends support the need to incorporate concepts for culturally focused nursing care and experiences with diverse cultures into nursing curricula. The purposes of this qualitative research were to describe the phenomena of being immersed in a different culture and to generate a conceptual map depicting process and outcomes of the immersion experience. From analysis of stories told by practicing nurses (n=9) who had an immersion experience during a baccalaureate program, a dimensional matrix emerged. The core dimension was learning to care. Situational predetermining factors included educational setting, personal characteristics, and demographic factors. Characteristics of the immersion context were site conditions. Transitional factors included strategies for "learning to care" such as social support, coping responses, and openness to adapt communication patterns. Outcomes included personal and professional growth in values, communication, and nursing practice. The matrix can guide nurse educators in incorporating immersion experiences into nursing curricula.
<24>Unique Identifier 11125641Authors
Page 11
401-600.txt Sabo D.Institution D'Youville College, Buffalo, New York, USA. [email protected] Men's health studies: origins and trends.Source Journal of American College Health. 49(3):133-42, 2000 Nov.Abstract This article provides a brief outline of the development of men's health studies in the United States. Research on men's health is discussed within critical feministtheories that highlight the reciprocality of gender relations as well as power differences between men and women and among male subgroups. A relational theory of gender and health is used to identify both positive-gendered and negative-gendered health synergies that influence the health processes and outcomes of men and women. Several examples of gendered health synergies are presented to illustrate key concepts. Finally, some directions for future research and advocacy with reference to men's health are outlined.
<25>Unique Identifier 11115139Authors Gaffney KF.Institution George Mason University, College of Nursing and Health Science, Fairfax, VA 22030,USA. [email protected] Prenatal risk factors among foreign-born Central American women: a comparative study.Source Public Health Nursing. 17(6):415-22, 2000 Nov-Dec.Abstract The purpose of this study was to compare the incidence of empirically established prenatal risk factors for low birthweight (LBW) outcomes among two groups of low-income mothers: foreign-born Central American women and nonimmigrant, non-Hispanic women. Two hundred ninety-six women who were part of a larger study of maternal role sufficiency were included in the present study: 127 Central American women and 169 nonimmigrant, non-Hispanic women who identified themselves as Black (n= 59) or White (n = 110). Data were collected by public health nurses (PHNs) during home visits and by research nurses in prenatal health department clinics. Comparisons were made between the two groups in areas of demographic characteristics, prenatal health behaviors, and prenatal stressful life-events. Foreign-born Central American mothers were found to be less educated, more likely tobe living with their partners, less likely to engage in prenatal health risk behaviors, and less likely to identify stressors in their lives. The initiation of prenatal PHN services by the target group was similar to the comparison group. Theirrate of LBW deliveries did not reflect the protective effect often attributed to foreign-born Hispanic mothers. Findings are discussed in light of the paradox of LBWand Hispanic heritage. Recommendations for practice, clinical research, and public policy are also addressed.
<26>Unique Identifier 11128262Authors Oropesa RS. Landale NS. Inkley M. Gorman BK.Institution Department of Sociology & Population Research Institute, The Pennsylvania State University, University Park 16803, USA. [email protected] Prenatal care among Puerto Ricans on the United States mainland.
Page 12

401-600.txtSource Social Science & Medicine. 51(12):1723-39, 2000 Dec.Abstract Recent public health initiatives in the USA identify the improvement of maternal and infant health outcomes among ethnic minorities as a national priority. Prenatal care is emphasized in these initiatives as a crucial intervention for reducing the risks of adverse outcomes. We investigate the barriers to prenatal care and the adequacy of prenatal care among mainland Puerto Ricans using data from a follow-backsurvey of a representative sample of mothers. The results show that barriers to prenatal care and the adequacy of prenatal care cannot be reduced solely to financial problems or problems associated with migration. Rather, attention to the social and the psychological circumstances surrounding the pregnancy (e.g. pregnancywantedness) is required.
<27>Unique Identifier 11126225Authors Burke JP. Hazuda HP. Stern MP.Institution Department of Health Sciences Research, Mayo Clinic, Rochester, Minnesota 55905, USA. [email protected] Rising trend in obesity in Mexican Americans and non-Hispanic whites: is it due tocigarette smoking cessation?.Source International Journal of Obesity & Related Metabolic Disorders: Journal of the International Association for the Study of Obesity. 24(12):1689-94, 2000 Dec.Abstract OBJECTIVE: Several studies have examined the influence of smoking cessation on weight gain. However, to date no study has examined this association in Mexican Americans (MA). DESIGN: Using data collected from the San Antonio Heart Study, a population-based study of diabetes and cardiovascular disease, we examined the association between smoking cessation and weight gain in 1930 Mexican Americans and 1126 non-Hispanic whites (NHW). Smoking cessation was defined as self-reported smoking at baseline but not at follow-up. RESULTS: Although there was no significantethnic difference in the prevalence of smoking at baseline (27.2% in MA and 25.4% inNHW, P = 0.309), a greater proportion of MA smoked at follow-up compared to NHW (19.7% vs 16.5%, P = 0.037). However, there was no significant ethnic difference in the percentage of individuals who stopped smoking during the follow-up period. A two-fold greater percentage of MA quitters than NHW quitters became overweight or obese, defined as a body mass index greater than or equal to 25 kg/m2 (7.4% vs 3.1%). However, this difference did not quite reach statistical significance (P = 0.072). Using linear regression to predict change in weight or body mass index from baseline to follow-up, smoking cessation was predictive of either weight gain or BMIgain in both ethnic groups. However, smoking status accounted for only 1.0% of the variance in these outcomes, and the estimated risk of becoming overweight or obese attributable to smoking cessation was only 7.4% in MA and 3.1% in NHW. CONCLUSION: We conclude that there is an ethnic difference in the influence of smoking cessationon weight gain in MA and NHW. However, in both ethnic groups this effect is quite small and makes only a slight contribution to the overall increase in prevalence of obesity in this population.
<28>Unique Identifier 11126893Authors Elliot NL. Quinless FW. Parietti ES.Institution Department of Humanities and Social Sciences, New Jersey Institute of Technology, Cullimore Hall, Newark, NJ 07102-1982, USA. [email protected]
Page 13

401-600.txtTitle Assessment of a Newark neighborhood: process and outcomes.Source Journal of Community Health Nursing. 17(4):211-24, 2000 Winter.Abstract In 1996, the members of the St. Columba Collaboration conducted a grassroots neighborhood assessment of a Hispanic area in Newark, New Jersey. This assessment was undertaken during an era of significant political and policy change in New Jersey. As a community-driven and implemented effort, the processes, methods, and outcomes of this assessment provide lessons on community activism, political awareness, and strategic planning. Quantitative surveys were distributed to local residents as well as users of the various services provided through Collaboration programs. Ten qualitative focus groups were held among various Collaboration groups.A total of 471 surveys were returned from a door-to-door distribution and 295 surveys were returned from users of Collaboration programs. Findings from both the quantitative and qualitative components were surprisingly similar. It was striking to note that youth violence, domestic violence, crime, and lack of job skills surpassed poor housing and chronic health problems, including HIV/AIDS and drug and alcohol addiction, as the most noted neighborhood problems. Overwhelmingly, social, welfare, and environmental issues were identified as priority items in a neighborhood marked by extreme poverty, poor childhood immunization rates, high HIV/AIDS rates, and high incidence of childhood asthma. Focus group findings revealed that stressful daily life events and circumstances far overshadowed health and wellness concerns. Recommendations emanating from the St. Columba Neighborhood needs assessment included: (a) establishment of principled partnerships between the Collaboration and other regional entities to extend capacity to design and implementsolutions (e.g., partnerships with other higher education institutions, health care agencies); (b) development of strategic planning processes and procedures within theCollaboration; (c) establishment of collaborative partnerships with other Hispanic community-based organizations for political activism; and (d) reorganization of the Collaboration's internal structure and functions to capitalize on opportunities for change. Significant outcomes from this process, in evidence 4 years after the 1996 neighborhood assessment, include: (a) a successful grant application to study violence against Hispanic women, (b) a research program investigating the nature andextent of clinical depression among Hispanic women, (c) establishment of a teenage pregnancy program, (d) English classes for Hispanic women seeking language skills and eventual employment, and (e) partnership extended to the New Jersey Institute ofTechnology.
<29>Unique Identifier 11118931Authors Hessol NA. Fuentes-Afflick E.Institution Departments of Medicine, San Francisco, CA, USA. [email protected] The perinatal advantage of Mexican-origin Latina women.Source Annals of Epidemiology. 10(8):516-23, 2000 Nov.Abstract PURPOSE: To determine if there is a perinatal advantage for birth outcomes among Mexican-origin Latina (Latina) women compared to white non-Hispanic (white) women, after adjusting for maternal, paternal, and infant factors. METHODS: 1,439,583 births from the 1990-1993 California linked birth and infant death certificate data sets were analyzed for the risk of low birth weight infants and infant mortality. RESULTS: Latina women had a statistically higher unadjusted risk of low birth weightinfants and infant mortality compared to white women. After adjusting for potential confounders, Latina women had a similar risk of low birth weight infants and a lowerrisk of infant mortality relative to white women. In multivariate analyses, the mostsignificant risk factor for low infant birth weight was young gestational age (OR = 82.91 for gestational age 1-230 days and OR = 10.62 for gestational age 231-258
Page 14

401-600.txtdays) and the most significant risk factor for infant mortality was low birth weight(OR = 53.99 for infant birth weight <500 grams and OR = 9.27 for infant birth weight500-2499 grams). CONCLUSION: There was some evidence of a perinatal advantage for Latina women, when compared to white women and after adjusting for numerous potential confounders. To further reduce the risk of low birth weight infants and infant mortality, additional research is needed for etiologic clues beyond race/ethnicity and other traditional risk factors.
<30>Unique Identifier 11124735Authors Beaton DE. Bombardier C. Guillemin F. Ferraz MB.Institution Institute for Work and Health, Toronto ON, Canada. [email protected] Guidelines for the process of cross-cultural adaptation of self-report measures. [Review] [27 refs]Source Spine. 25(24):3186-91, 2000 Dec 15.
<31>Unique Identifier 11097657Authors Tsemberis S. Stefancic A.Institution [email protected] The role of an espiritista in the treatment of a homeless, mentally ill hispanic man.Source Psychiatric Services. 51(12):1572-4, 2000 Dec.Abstract This paper presents a case study from an emergency psychiatric outreach team that serves homeless and mentally ill persons in New York City. Mr. V was homeless and believed that he was possessed by evil spirits who were causing his physical and mental problems. He was hospitalized involuntarily twice for medical reasons, but herefused to cooperate in his treatment and returned to the streets after his first hospitalization. After one visit by a spiritual healer during his second hospitalization, Mr. V began to participate in his treatment. He was discharged to anursing home, and after three years he had not returned to the streets.
<32>Unique Identifier 11099121Authors Kuo M. Mohler B. Raudenbush SL. Earls FJ.Institution Harvard School of Public Health, Boston, MA 02120, USA. [email protected] Assessing exposure to violence using multiple informants: application of hierarchical linear model.Source Journal of Child Psychology & Psychiatry & Allied Disciplines. 41(8):1049-56, 2000 Nov.Abstract The present study assesses the effects of demographic risk factors on children's exposure to violence (ETV) and how these effects vary by informants. Data on exposure to violence of 9-, 12-, and 15-year-olds were collected from both child
Page 15

401-600.txtparticipants (N = 1880) and parents (N = 1776), as part of the assessment of the Project on Human Development in Chicago Neighborhoods (PHDCN). A two-level hierarchical linear model (HLM) with multivariate outcomes was employed to analyze information obtained from these two different groups of informants. The findings indicate that parents generally report less ETV than do their children and that associations of age, gender, and parent education with ETV are stronger in the self-reports than in the parent reports. The findings support a multivariate approach when information obtained from different sources is being integrated. The application of HLM allows an assessment of interactions between risk factors and informants and uses all available data, including data from one informant when data from the other informant is missing.
<33>Unique Identifier 11092163Authors Brach C. Fraser I.Title Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. [Review] [205 refs]Source Medical Care Research & Review. 57 Suppl 1:181-217, 2000.Abstract This article develops a conceptual model of cultural competency's potential to reduce racial and ethnic health disparities, using the cultural competency and disparities literature to lay the foundation for the model and inform assessments ofits validity. The authors identify nine major cultural competency techniques: interpreter services, recruitment and retention policies, training, coordinating with traditional healers, use of community health workers, culturally competent health promotion, including family/community members, immersion into another culture, and administrative and organizational accommodations. The conceptual model shows how these techniques could theoretically improve the ability of health systemsand their clinicians to deliver appropriate services to diverse populations, therebyimproving outcomes and reducing disparities. The authors conclude that while there is substantial research evidence to suggest that cultural competency should in fact work, health systems have little evidence about which cultural competency techniquesare effective and less evidence on when and how to implement them properly. [References: 205]
<34>Unique Identifier 11083308Authors Ostir GV. Uchida T.Institution Department of Preventive Medicine and Community Health, University of Texas Medical Branch, Galveston 77555-1143, USA.Title Logistic regression: a nontechnical review. [Review] [12 refs]Source American Journal of Physical Medicine & Rehabilitation. 79(6):565-72, 2000 Nov-Dec.Abstract Medical rehabilitation researchers are increasingly interested in investigating complex, multivariate problems. Logistic regression analysis is a statistical tool that may be useful in exploring the relationship between multiple explanatory factors and a categorical outcome. The purpose of this article is to describe logistic regression analysis in nontechnical terms. [References: 12]
<35>Page 16

401-600.txtUnique Identifier 11076989Authors Woodward A. Kawachi I.Institution Department of Public Health, Wellington School of Medicine, PO Box 7343 WellingtonSouth, New Zealand. [email protected] Why reduce health inequalities?.Source Journal of Epidemiology & Community Health. 54(12):923-9, 2000 Dec.Abstract It is well known that social, cultural and economic factors cause substantial inequalities in health. Should we strive to achieve a more even share of good health, beyond improving the average health status of the population? We examine four arguments for the reduction of health inequalities.1 Inequalities are unfair. Inequalities in health are undesirable to the extent that they are unfair, or unjust. Distinguishing between health inequalities and health inequities can be contentious. Our view is that inequalities become "unfair" when poor health is itself the consequence of an unjust distribution of the underlying social determinants of health (for example, unequal opportunities in education or employment).2 Inequalities affect everyone. Conditions that lead to marked health disparities are detrimental to all members of society. Some types of health inequalities have obvious spillover effects on the rest of society, for example, thespread of infectious diseases, the consequences of alcohol and drug misuse, or the occurrence of violence and crime.3 Inequalities are avoidable.Disparities in health are avoidable to the extent that they stem from identifiable policy options exercised by governments, such as tax policy, regulation of business and labour, welfare benefits and health care funding. It follows that health inequalities are, in principle, amenable to policy interventions. A government that cares about improving the health of the population ought therefore to incorporate considerationsof the health impact of alternative options in its policy setting process.3 Interventions to reduce health inequalities are cost effective.Public health programmes that reduce health inequalities can also be cost effective. The case can be made to give priority to such programmes (for example, improving access to cervical cancer screening in low income women) on efficiency grounds. On the other hand, few programmes designed to reduce health inequalities have been formally evaluated using cost effectiveness analysis.We conclude that fairness is likely to be the most influential argument in favour of acting to reduce disparities in health, but the concept of equity is contested and susceptible to different interpretations. There is persuasive evidence for some outcomes that reducing inequalities will diminish "spill over" effects on the health of society at large. In principle, you would expect that differences in health status that are not biologically determined are avoidable. However, the mechanisms giving rise to inequalities are still imperfectly understood, and evidence remains to be gathered on the effectiveness of interventions to reduce such inequalities.
<36>Unique Identifier 11076244Authors Roetzheim RG. Pal N. Gonzalez EC. Ferrante JM. Van Durme DJ. Krischer JP.Institution Department of Family Medicine, University of South Florida, Tampa 33612, USA.Title Effects of health insurance and race on colorectal cancer treatments and outcomes.Source American Journal of Public Health. 90(11):1746-54, 2000 Nov.Abstract OBJECTIVES: We hypothesized that health insurance payer and race might influence the care and outcomes of patients with colorectal cancer. METHODS: We examined treatments received for all incident cases of colorectal cancer occurring in Florida
Page 17

401-600.txtin 1994 (n = 9551), using state tumor registry data. We also estimated the adjusted risk of death (through 1997), using proportional hazards regression analysis controlling for other predictors of mortality. RESULTS: Treatments received by patients varied considerably according to their insurance payer. Among non-Medicare patients, those in the following groups had higher adjusted risks of death relative to commercial fee-for-service insurance: commercial HMO (risk ratio [RR] = 1.40; 95%confidence interval [CI] = 1.18, 1.67; P = .0001), Medicaid (RR = 1.44; 95% CI = 1.06, 1.97; P = .02), and uninsured (RR = 1.41; 95% CI = 1.12, 1.77; P = .003). Non-Hispanic African Americans had higher mortality rates (RR = 1.18; 95% CI = 1.01,1.37; P = .04) than non-Hispanic Whites. CONCLUSIONS: Patients with colorectal cancer who were uninsured or insured by Medicaid or commercial HMOs had higher mortality rates than patients with commercial fee-for-service insurance. Mortality was also higher among non-Hispanic African American patients.
<37>Unique Identifier 11071827Authors Bowen D. Raczynski J. George V. Feng Z. Fouad M.Institution Fred Hutchinson Cancer Research Center, Seattle, Washington 98109, USA. [email protected] The role of participation in the women's health trial: feasibility study in minority populations.Source Preventive Medicine. 31(5):474-80, 2000 Nov.Abstract BACKGROUND: This paper examines participation rates and the association between participation and study outcomes (% energy from fat) among participants in the Women's Health Trial: Feasibility Study in Minority Populations, a randomized clinical trial to determine if ethnically and socioeconomically diverse women could be recruited and make significant dietary changes. METHODS: Women (n = 2,208) were recruited from three clinical centers and randomized to either an intervention groupor a control group. Multiple measures were collected at 6 months. RESULTS: Participation rates for follow-up data collection activities were high (average participation 79%). Hispanics and lower educational groups participated significantly less (59% for Hispanics vs 86% for blacks and whites; 78% for lowest educational group vs 84% for highest educational group). Intervention participation significantly predicted change in percentage energy from fat (P < 0.001), accountingfor an additional 8% of variance after background variables were controlled for. CONCLUSIONS: These data suggest that intervention participation is positively related to dietary change, but they cannot rule out the possibility that other factors may influence both of these factors. Copyright 2000 American Health Foundation and Academic Press.
<38>Unique Identifier 11064297Authors Chang WC. Fu Y. Ohman EM. Gupta M. Morris A. Roth SN. Granger CB. Califf RM. Topol EJ. Mark DB. Armstrong PW.Institution University of Alberta, Edmonton, Canada.Title Temporal evolution in the management of acute ST elevation myocardial infarction: the seven-year GUSTO experience from canada and the united states. The North American GUSTO-I and GUSTO-III investigators.[see comment].Source Canadian Journal of Cardiology. 16(10):1231-9, 2000 Oct.Abstract
Page 18
401-600.txt BACKGROUND: Temporal changes in baseline characteristics, treatment and clinical outcomes of patients presenting with acute ST elevation myocardial infarction in Canada and the United States have not been examined comprehensively over time. OBJECTIVES: To evaluate baseline characteristics, process of care and clinical outcomes. Also, to explore whether earlier process-of-care differences between Canada and the United States had changed and, if so, whether they influenced clinical outcomes. PATIENTS AND Methods: A total of 13, 888 American and 3011 Canadian patients enrolled in 184 American and 38 Canadian hospitals that participated in both the Global Utilization of Streptokinase and Tissue Plasminogen Activator (alteplase) for Occluded Coronary Arteries (GUSTO-I) trial (1990 to 1993) and the Global Utilization of Strategies to Open Occluded Coronary Arteries (GUSTO-III) trial (1995 to 1997) were studied. Logistic regression was used to identify significant prognostic factors, to assess illness severity at hospital presentation and to classify trends between Canada and the United States. RESULTS: In both countries, illness severity on admission increased, door-to-needle time for thrombolysis was reduced, intensive care unit stay was shortened and hospital stay decreased from GUSTO-I to GUSTO-III. Whereas the administration of oral nitrates, calcium blockers and beta-blockers at discharge converged over time between countries, the disparity in the use of angiography and revascularization widened; the rise in American revascularization rate was most evident in patients without in-hospital ischemia. The 30-day and one-year mortality rates were comparable and declined nonsignificantly in both countries. CONCLUSIONS: Despite increased illness severity and varying medication and procedure rates, there was no increase over timein 30-day or one-year mortality; this remained comparable between countries throughout the seven-year observation period.
<39>Unique Identifier 11025937Authors Singer AT. Weinstein RS.Institution Department of Psychology, University of California, Berkeley 94720-1650, USA. [email protected] Differential parental treatment predicts achievement and self-perceptions in two cultural contexts.Source Journal of Family Psychology. 14(3):491-509, 2000 Sep.Abstract This study examined 148 Asian American and European American late adolescents' perceptions of differential affection and control by mothers and fathers as predictors of academic achievement and self-perceptions of intellectual ability and global self-worth. Overall, analyses generally confirmed the hypotheses that the more differentially favorable the treatment (more affection or less control) or the less differential treatment (above and beyond which sibling was favored) reported inthe home, the more positive late adolescents' outcomes. Perceptions of differential parental treatment predicted up to 13% of the variance in achievement and self-perceptions. Several findings were moderated by ethnicity or gender. Finally, and perhaps most importantly, perceptions of differential parental treatment predicted a significant and unique amount of variance in outcomes beyond that predicted by perceptions of absolute levels of affection and control.
<40>Unique Identifier 11025934Authors Gorman-Smith D. Tolan PH. Henry DB. Florsheim P.Institution Department of Psychiatry, University of Illinois at Chicago 60612, USA. [email protected]
Page 19

401-600.txtTitle Patterns of family functioning and adolescent outcomes among urban African American and Mexican American families.Source Journal of Family Psychology. 14(3):436-57, 2000 Sep.Abstract The relations of patterns of family functioning, prosocial behaviors, and internalizing and externalizing symptoms over time were evaluated among a sample of economically disadvantaged inner-city African American and Mexican American male adolescents. Ethnic group differences for configurations of family functioning over time, levels of prosocial and problem behaviors, and relations of family functioningto risk were found. Among both ethnic groups, exceptionally functioning families provided a protective effect against risk. Overall, African American youth had stronger attitudes toward school and higher educational aspirations than Mexican American youth. Unlike previous investigations, once socioeconomic status was controlled, no differences were found for either internalizing or externalizing problems between the 2 groups. The importance of considering socioeconomic status and community context when evaluating minority parenting and family functioning is discussed.
<41>Unique Identifier 11014742Authors Coll CG. Akerman A. Cicchetti D.Institution Education Department and Center for the Study of Human Development, Brown University, Providence, RI 02912, USA.Title Cultural influences on developmental processes and outcomes: implications for the study of development and psychopathology. [Review] [112 refs]Source Development & Psychopathology. 12(3):333-56, 2000 Summer.Abstract The purpose of this paper is to trace the role of culture as an explanatory construct in developmental processes and outcomes, and its implications in the understanding of developmental psychopathology. Literature reviews were conducted byhistorical period: 1930-1939, 1960-1969, and 1990-1999. The percentage of the total articles and chapters pertaining to cultural issues increased as a function of time.Both conceptual and methodological continuities and discontinuities were observed among the three periods. The preponderance of comparative studies using deficit models still remains, but more enlightened alternative conceptual models, within culture studies, and measures of cultural processes, are emerging. In contrast, although contextual influences are considered important in developmental psychopathology, the field lags in its empirical consideration of cultural influences. The need to seriously address these issues will increase as globalization and rapid cultural change become even more the norm than the exception. [References: 112]
<42>Unique Identifier 11011506Authors Finch BK. Kolody B. Vega WA.Institution Department of Sociology, Florida State University, Tallahassee 32306, USA. [email protected] Perceived discrimination and depression among Mexican-origin adults in California.Source Journal of Health & Social Behavior. 41(3):295-313, 2000 Sep.
Page 20
401-600.txtAbstract We contend that perceived discrimination has an independent effect on depression outcomes among adults of Mexican origin. Using a sample of 3,012 Mexican-origin respondents in Fresno, California in 1995/96 (ages 18-59) we investigate the direct and moderating connections between perceived discrimination, acculturative stress, and mental health (CES-D). We also investigate the social patterning of perceived discrimination. While more highly acculturated immigrant respondents were more likely to experience discrimination than their less acculturated counterparts, more highly acculturated U.S. born respondents were less likely to experience discrimination. Discrimination was directly related to depression, but this effect was moderated through nativity/country of residence, English-language acculturation,sex, and country of education variables. Moderate levels of legal status acculturative stress were especially depressive for native-born U.S. residents.
<43>Unique Identifier 10993608Authors Theuer CP.Institution Department of Surgery, University of California, Irvine, USA.Title Asian gastric cancer patients at a southern California comprehensive cancer centerare diagnosed with less advanced disease and have superior stage-stratified survival.Source American Surgeon. 66(9):821-6, 2000 Sep.Abstract The 5-year overall survival after curative gastrectomy for gastric cancer is markedly different in the West from that in the Far East. Japanese surgeons feel that extended lymphadenectomy contributes to this superior survival, although survival differences may reflect improved staging or less aggressive tumor biology. We analyzed consecutive cases of gastric adenocarcinoma diagnosed and treated at theUniversity of California, Irvine Medical Center from 1989 through 1998 to determine whether patients of Asian descent diagnosed with gastric cancer in Southern California have improved outcome. Fifty-two cases (36%) occurred in patients of Asian descent (39% Vietnamese, 31% Chinese, 13% Korean, 6% Filipino, and 2% Japanese). Only one Asian patient was born in the United States. Non-Asian patients (67% white, 30% Latino, and 3% black) were younger (59 years vs 64 years; P < 0.05) and more likely to have tumors of the gastroesophageal junction (33% vs 4%; P < 0.001). Asian patients were less likely to have distant metastases (24% vs 39%; P = 0.08), were more likely to undergo formal gastrectomy (71% vs 45%; P < 0.01), and were more likely to undergo a curative resection (40% vs 18%; P < 0.01). The overallsurvival of Asian patients at 3 years was significantly higher than the overall survival of non-Asians (39.4% vs 19.6%, P < 0.05). Asians with regional (node-positive) disease had superior survival (40.2% vs 14.8%, P < 0.05), which can be largely attributed to greater rates of resectability. We conclude that the clinical behavior of gastric cancer in Asians in Southern California differs from that in non-Asians. The increased proportion of resectable disease and improved survival of patients of Asian descent likely reflects less aggressive tumor biology.
<44>Unique Identifier 10980044Authors Stewart SM. Lee PW. Low LC. Cheng A. Yeung W. Huen KF. O'Donnell D.Institution Department of Community Health, The University of Hong Kong, Hong Kong, China. [email protected] Pathways from emotional adjustment to glycemic control in youths with diabetes in
Page 21

401-600.txtHong Kong.Source Journal of Pediatric Psychology. 25(6):393-402, 2000 Sep.Abstract OBJECTIVE: To examine factors that influence emotional adjustment, adherence to diabetic care, and glycemic control in Hong Kong youths with insulin-dependent diabetes mellitus (IDDM). METHODS: Seventy youths, their mothers, and matched controls provided information on health beliefs, authoritarian parenting style, parent-child conflict, emotional adjustment, and adherence to medical regimen. Glycosylated hemoglobin levels were obtained to measure glycemic control. RESULTS: Predictors explained 34% of the variance in emotional adjustment and 39% of the variance in glycemic control. The data supported a pathway from emotional adjustmentto self-efficacy to adherence behaviors to glycemic control. In contrast to Western culture and consistent with prediction, parenting style did not associate with negative outcomes, and even relatively low levels of parent-child conflict correlated negatively with emotional adjustment in this culture. CONCLUSIONS: Management of conflict and self-efficacy enhancing interactions are suggested interventions to enhance adherence to diabetic care in Hong Kong youths with IDDM.
<45>Unique Identifier 10982108Authors Patrick D. Chiang YP.Institution University of Washington, Seattle, USA.Title Postscript: the remaining questions.Source Medical Care. 38(9 Suppl):II209-10, 2000 Sep.
<46>Unique Identifier 10982107Authors Lohr KN.Institution Health Services and Policy Research Program, Research Triangle Institute, ResearchTriangle Park, North Carolina, USA. [email protected] Health outcomes methodology symposium: summary and recommendations. [Review] [27 refs]Source Medical Care. 38(9 Suppl):II194-208, 2000 Sep.Abstract BACKGROUND: Interest in the philosophy and techniques of the assessment of health outcomes has burgeoned, prompting research funding agencies and others to examine traditional and emerging methods for outcome measurement. OBJECTIVES: This report summarizes the presentations and discussions at and research recommendations stemming from an invitational symposium on health outcomes methodology convened in September 1999. RESEARCH DESIGN: The summary is based on the preliminary drafts of all formal reports and discussions, transcripts of all presentations and plenary discussions, and notes from breakout groups. RESULTS AND CONCLUSIONS: Existing health outcomes measures drawn from classic test theory and emerging approaches based on item response theory offer exciting opportunities for appreciably expanded applications in biomedical and health services research, clinical practice and decision making, and policy development. The major research agenda reflects the significance of this field of endeavor, its widening acceptance both at home and abroad, and its increasing applicability to many different patient and user communities. Of particular moment are the following: (1) refining and expanding of measurement techniques that rely on item response theory and making these approaches
Page 22

401-600.txtmore understandable to potential users; (2) improving measurement tools to make themmore culturally appropriate for diverse populations and more conceptually and psychometrically equivalent across such groups; (3) addressing longstanding issues in preference- and utility-based approaches, particularly in the elicitation of preference responses and scoring instruments; and (4) enhancing the ways in which data from outcomes measurement tools are calibrated against commonly understood clinical and lay metrics, are interpreted, and are made usable for different decision-makers. [References: 27]
<47>Unique Identifier 10982098Authors Wu AW.Institution Department of Health Policy and Management, School of Hygiene and Public Health, The Johns Hopkins University, Baltimore, Maryland, USA. [email protected] Quality-of-life assessment in clinical research: application in diverse populations.[comment].Source Medical Care. 38(9 Suppl):II130-5, 2000 Sep.
<48>Unique Identifier 10982096Authors Stewart AL. Napoles-Springer A.Institution University of California San Francisco, Institute for Health and Aging, 94143-0646, USA. [email protected] Health-related quality-of-life assessments in diverse population groups in the United States.[see comment]. [Review] [168 refs]Source Medical Care. 38(9 Suppl):II102-24, 2000 Sep.Abstract BACKGROUND: Effectiveness research needs to represent the increasing diversity of the United States. Health-related quality-of-life (HRQOL) measures are often included as secondary treatment outcomes. Because most HRQOL measures were developedin nonminority, well-educated samples, we must determine whether such measures are conceptually and psychometrically equivalent in diverse subgroups. Without equivalence, overall findings and observed group differences may contain measurementbias. OBJECTIVES: The objectives of this work were to discuss the nature of diversity, importance of ensuring the adequacy of HRQOL measures in diverse groups, methods for assessing comparability of HRQOL measures across groups, and methodological and analytical challenges. RESULTS: Integration of qualitative and quantitative methods is needed to achieve measurement adequacy in diverse groups. Little research explores conceptual equivalence across US subgroups; of the few studies of psychometric comparability, findings are inconsistent. Evidence is neededregarding whether current measures are comparable or need modifications to meet universality assumptions, and we need to determine the best methods for evaluating this. We recommend coordinated efforts to develop guidelines for assessing measurement adequacy across diverse subgroups, allocate resources for measurement studies in diverse populations, improve reporting of and access to measurement results by subgroups, and develop strategies for optimizing the universality of HRQOL measures and resolving inadequacies. CONCLUSIONS: We advocate culturally sensitive research that involves cultural subgroups throughout the research process.Because examining the cultural equivalence of HRQOL measures within the United States is somewhat new, we have a unique opportunity to shape the direction of this work through development and dissemination of appropriate methods. [References: 168]
Page 23

401-600.txt
<49>Unique Identifier 10974074Authors Gotay CC. Moinpour CM. Moody-Thomas S. Gritz ER. Albain KS. DeAntoni E. Hansen L. Ganz PA.Institution Cancer Research Center of Hawaii, University of Hawaii, Honolulu 96813, USA. [email protected] Behavioral science research in the cooperative group setting: the Southwest Oncology Group experience. [Review] [39 refs]Source Journal of the National Cancer Institute. 92(17):1381-7, 2000 Sep 6.
<50>Unique Identifier 10977019Authors Tabak AG. Tamas G. Zgibor J. Wilson R. Becker D. Kerenyi Z. Orchard TJ.Institution National Centre for Diabetes Care, Semmelweis University of Medicine, Budapest, Hungary.Title Targets and reality: a comparison of health care indicators in the U.S. (Pittsburgh Epidemiology of Diabetes Complications Study) and Hungary (DiabCare Hungary).Source Diabetes Care. 23(9):1284-9, 2000 Sep.Abstract OBJECTIVE: In the U.S., both primary care and specialist physicians share in the care of type 1 diabetic patients, often in an informal collaboration. In Hungary, however, type 1 diabetic patients are generally managed in special centralized diabetes units. These different treatment settings may lead to different health carepractices and outcomes. To determine if this is true, diabetes care indicators and complications were compared across representative study populations from the 2 countries. RESEARCH DESIGN AND METHODS: The Pittsburgh Epidemiology of Diabetes Complications Study (EDC) is a prospective cohort of childhood-onset type 1 diabeticpatients. DiabCare Hungary, a multicenter cross-sectional study, was developed for quality control purposes and provides a nationwide data set of diabetic patients. Weidentified 2 comparable populations (EDC, n = 416; DiabCare, n = 405) in terms of age (> or =14 years) and age at onset (<17 years). RESULTS: EDC patients were less likely to receive diabetes education (P<0.0001), see an ophthalmologist (P<0.0001), be treated by diabetologists (P<0.0001), or perform self-monitoring of blood glucose(P<0.0001). They were more likely to use conservative insulin regimens (i.e., 1-2 injections/day, P<0.0001) and have a higher glycated hemoglobin (P< 0.0001). DiabCare patients more often experienced severe hypoglycemia (P<0.01) and had a lower prevalence of proliferative retinopathy (P<0.0001), legal blindness (P<0.05), and albuminuria (> or =30 mg/day P<0.01). No significant differences in macrovascular complications were seen, although rates were generally low CONCLUSIONS: These data suggest that the 2 populations differ by their diabetes carepractices, degree of glycemic control, and microvascular complication status.
<51>Unique Identifier 10975163Authors Whaley AL.Institution
Page 24

401-600.txt Department of Social Psychiatry, New York State Psychiatric Institute, New York 10032, USA. [email protected] Sociocultural differences in the developmental consequences of the use of physicaldiscipline during childhood for African Americans. [Review] [24 refs]Source Cultural Diversity & Ethnic Minority Psychology. 6(1):5-12, 2000 Feb.Abstract Given the diverse cultures that can shape parenting behavior, some basic assumptions regarding the links between parenting styles and developmental outcomes may not be universal. Although a positive correlation between the use of physical discipline (i.e., spanking) and disruptive disorders in children is found in studiesof European American families, research on African American families has found a negative association or none at all. Moreover, a review of the literature indicates that the positive association between spanking and child behavior problems is bidirectional for White families, whereas it is the product of reverse causation (i.e., negative child behaviors result in spanking) in Black families. The implications of these sociocultural differences for parent training programs and thefamily study of disruptive behaviors are discussed. [References: 24]
<52>Unique Identifier 10971882Authors Nader T. Rothenberg S. Averbach R. Charles B. Fields JZ. Schneider RH.Institution Maharishi University of Management, Vlodrop, The Netherlands.Title Improvements in chronic diseases with a comprehensive natural medicine approach: areview and case series. [Review] [82 refs]Source Behavioral Medicine. 26(1):34-46, 2000 Spring.Abstract Approximately 40% of the US population report using complementary and alternative medicine, including Maharishi Vedic Medicine (MVM), a traditional, comprehensive system of natural medicine, for relief from chronic and other disorders. Although many reports suggest health benefits from individual MVM techniques, reports on integrated holistic approaches are rare. This case series, designed to investigate the effectiveness of an integrated, multimodality MVM program in an ideal clinical setting, describes the outcomes in four patients: one with sarcoidosis; one with Parkinson's disease; a third with renal hypertension; and a fourth with diabetes/essential hypertension/anxiety disorder. Standard symptom reports and objective markers of disease were evaluated before, during, and after the treatment period. Results suggested substantial improvements as indicated by reductions in major signs, symptoms, and use of conventional medications in the four patients during the 3-week in-residence treatment phase and continuing through the home follow-up program. [References: 82]
<53>Unique Identifier 11183584Authors Stone CE.Institution Rynne Marketing Group, Evanston, Illinois, USA.Title Cultural orientation: an emerging dimension of quality in women's health services.Source Quality Management in Health Care. 8(4):52-64, 2000 Summer.Abstract There are many efforts underway to document the differences in health status and
Page 25

401-600.txthealth services access of women in distinct cultural segments in the U.S. Along withthe measurable aspects of health status and utilization, each cultural segment carries its unique perspective on what constitutes "quality" in women's health services. These definitions of quality may reflect access, interactions, process, and outcomes. Health care providers that aspire to provide quality women's health care need to identify the distinct cultural segments in their own communities; document the gaps in women's health services; and develop programs that are specificto clinical needs and quality criteria of these populations.
<54>Unique Identifier 10969889Authors Burnett DM. Silver TM. Kolakowsky-Hayner SA. Cifu DX.Institution Department of Physical Medicine and Rehabilitation, Virginia Commonwealth University, Medical College of Virginia, Richmond 23298-0542, USA.Title Functional outcome for African Americans and Hispanics treated at a traumatic brain injury model systems centre.Source Brain Injury. 14(8):713-8, 2000 Aug.Abstract OBJECTIVE: To describe the demographics, incidence and functional outcome for African Americans and Hispanics treated at a traumatic brain injury (TBI) model systems centre. DESIGN: Retrospective data analysis of patients admitted to an acuteinpatient rehabilitation national TBI model systems centre. SETTING: A tertiary careuniversity medical centre participating in the NIDRR Traumatic Brain Injury Model Systems project. SUBJECTS: Eighty-seven patients with TBI admitted to a Model Systems acute intensive interdisciplinary rehabilitation setting between 1989-1999. Information was extracted from the National TBI Model Systems data base for demographics such as age, race, education, gender, marital and employment status, sponsorship, injury aetiology and severity. OUTCOME MEASURES: Functional outcome wasdetermined using the Functional Independence Measure (FIM), and the Disability Rating Scale (DRS) at the time of admission and discharge. RESULTS: Descriptive statistics were completed using SPSS. African American (94.3%) and Hispanic (5.7%) patients were injured most often as a result of motor vehicle accidents (48.8%). Males comprised 86.2% of this population, which had an average age of 34.5 years (SD= 13.1). On admission, average GCS score was 7.8 (SD = 3.6), average DRS was 13.5 (SD = 5.8), and average FIM total score was 49.8 (SD = 26.5). Average length of unconsciousness was 5.2 days (SD = 27.9), while average length of post-traumatic amnesia was 41.9 days (SD = 59.3). At the time of injury, 78.2% of the patients werenot married. The majority of patients (97.7%) had private residences and 88.5% returned to their original home. Most patients had at least a high school education or passed a high school equivalent exam (49.4%) and were employed (70.1%) at the time of injury. Only 7% of the patients had a history of prior TBI. With regard to substance use, only 34.2% of patients reported pre-morbid illicit drug use. However,50.5% met criteria for heavy or moderate alcohol use rates. Only 35.6% of patients reported a pre-morbid history of arrests, with the average number of arrests equal to 4.5 (SD = 10.2). Within this population, the number of drug or alcohol related arrests was 4.8 (SD = 13.5). CONCLUSIONS: Unmarried African American males, with an average age of 35 years, predominated at this institution. The primary mechanism of injury was motor vehicle accidents. The majority of patients had, at least, a high school education or passed an equivalency exam, were employed at the time of their injury and were discharged to their prior private residence. While half of the patients met criteria for moderate-to-heavy alcohol consumption, only one-third of the patients reported a history of pre-morbid illicit drug use. This descriptive analysis supports the need for further investigation of minority populations that sustain TBI and will enhance the accuracy of implications that minority status may have on functional outcome.
Page 26

401-600.txt<55>Unique Identifier 10968582Authors Chin JL.Institution CEO Services, Newton, Massachusetts, USA. [email protected] Culturally competent health care.[see comment].Source Public Health Reports. 115(1):25-33, 2000 Jan-Feb.
<56>Unique Identifier 10965389Authors Reyes O. Gillock KL. Kobus K. Sanchez B.Institution University of Illinois at Chicago, Department of Psychology 60607-7137, USA.Title A longitudinal examination of the transition into senior high school for adolescents from urban, low-income status, and predominantly minority backgrounds.Source American Journal of Community Psychology. 28(4):519-44, 2000 Aug.Abstract The current 6-year study investigates the impact of the elementary (K-8)-to-high school (9-12) transition on the school completion outcomes of 107 adolescents from urban, minority, low-income status backgrounds. Descriptive findings provide a longitudinal profile of students' enrollment status throughout high school. Studentswho had graduated or were Active in the school system at the end of the study evidenced more marked change in perceptions of social support following the transition to the ninth grade compared to Inactive students, dropouts, who evidencedlittle change. With respect to academic performance, while both groups evidenced declines following the transition and failed to recover sustained losses, Inactive students declined more sharply in grades and attendance. Findings are discussed in terms of the mixed support for the transitional life events perspective. In addition, study limitations and directions for future research are discussed, including variables that should be considered in research with the targeted group.
<57>Unique Identifier 10958877Authors Jackson R. Bimla Schwarz E. Freedman L. Darney P.Institution Center for Reproductive Health Research and Policy, University of California, San Francisco, USA. [email protected] Knowledge and willingness to use emergency contraception among low-income post-partum women.Source Contraception. 61(6):351-7, 2000 Jun.Abstract We performed a multivariate analysis to determine factors associated with knowledge and willingness to use emergency contraception in a consecutive sample of 371 post-partum women from an inner-city public hospital. Women were queried about previous contraceptive use, pregnancy history including abortions and unplanned pregnancies, and demographic characteristics. Outcomes included knowledge of emergency contraception and willingness to use it. Questionnaires were conducted in person, in English or Spanish.Of 371 women, 3% had used emergency contraception, 36%had heard of it, and 7% knew the correct timing for use. Two-thirds of the
Page 27
401-600.txtpopulation indicated a willingness to use emergency contraception in the future. Factors positively associated with knowledge included being a teenager or more than 30 years old, prior use of condoms, and history of an elective abortion. Being multiparous, monolingual Spanish-speaking, or Asian were negatively associated with knowledge. Willingness to use emergency contraception was positively associated withbeing multiparous and negatively associated with a higher income, moral or religiousobjections to the use of emergency contraception, a belief that it is unsafe or a perception that it is an abortificient. Knowledge about emergency contraception, especially correct timing, remains low. Multiparous women should receive increased education given their lack of knowledge but willingness to use emergency contraception. In order to increase the acceptability of emergency contraception, educational efforts must include accurate information about its mechanism of use andsafety.
<58>Unique Identifier 10954792Authors Nakamura Y. Mulliken JB. Belfer ML.Institution Department of Social Medicine, Harvard Medical School, Boston, MA 02115, USA.Title Cross-cultural understanding of aesthetic surgery: the male cosmetic surgery patient in japan and the USA.Source Aesthetic Plastic Surgery. 24(4):283-8, 2000 Jul-Aug.Abstract This review describes the historical development of aesthetic surgery in Japan andparallels with the development of the specialty in the United States. The focus is on the consequences of aesthetic surgery in the male patient when collaboration between mental health clinicians and surgeons lags. The cultural, social, and psychological issues raised are relevant to the diverse cultural groups now seeking aesthetic surgery in the United States. Case illustrations are a reminder to aesthetic surgeons of the potential need for more comprehensive evaluation in the group of male patients who may be at added risk for negative outcomes in terms of satisfaction.
<59>Unique Identifier 10938211Authors Elder JP. Campbell NR. Litrownik AJ. Ayala GX. Slymen DJ. Parra-Medina D. Lovato CY.Institution Graduate School of Public Health, San Diego State University, California, USA.Title Predictors of cigarette and alcohol susceptibility and use among Hispanic migrant adolescents.Source Preventive Medicine. 31(2 Pt 1):115-23, 2000 Aug.Abstract BACKGROUND: Little is known about interpersonal and broader sociocultural factors related to protection from or use of tobacco and alcohol among immigrant adolescents. This study presents the baseline predictors of tobacco and alcohol use and susceptibility to tobacco and alcohol among Hispanic migrant adolescents. METHODS: The sample consisted of 660 Hispanic adolescents (51% male) between the ages of 11 and 16 years enrolled in the Migrant Education Program through the CountyOffice of Education. Slightly more than 75% of the study sample was first generationHispanics and 79% preferred to speak Spanish. An interviewer-administered survey assessed the following information: standard demographic characteristics, modeling of cigarette smoking (including parental and peer smoking), attitudes (including
Page 28

401-600.txtself-standards and anticipated outcomes), acculturation, communication with parents,amount of social support, and satisfaction with social support. RESULTS: Significantpredictors of susceptibility to tobacco and smoking status included age, gender, attitudes toward cigarettes (e.g., anticipated outcomes, self-standards), satisfaction with social support, and parent-child communication. Factors that were also significant predictors of susceptibility to alcohol and drinking status were age, attitudes toward drinking, satisfaction with social support, and level of parent-child communication. In addition, peer and household use of alcohol predictedadolescent outcomes. CONCLUSIONS: Based on these results it is suggested that tobacco and alcohol prevention efforts for first-generation Hispanic adolescents should target not only usual concerns (e.g., availability, peer pressure, modeling, expectancies), but also parent-child communication. Copyright 2000 American Health Foundation and Academic Press.
<60>Unique Identifier 10936632Authors Dodds S. Blaney NT. Nuehring EM. Blakley T. Lizzotte JM. Potter JE. O'Sullivan MJ.Institution Departments of Psychiatry and Behavioral Sciences, School of Medicine, University of Miami, Miami, FL 33101, USA.Title Integrating mental health services into primary care for HIV-infected pregnant andnon-pregnant women: Whole Life--a theoretically derived model for clinical care and outcomes assessment.Source General Hospital Psychiatry. 22(4):251-60, 2000 Jul-Aug.Abstract Poor women of color who are disproportionately both infected and affected by HIV/AIDS also face multiple lifestyle and psychosocial burdens that complicate effective delivery of health care, thereby contributing to their poorer prognosis. Addressing these factors within the context of HIV/AIDS primary care for women is the aim of Whole Life, a program to integrate mental health services into primary care for HIV-infected pregnant and non-pregnant women. Whole Life utilizes a theoretically derived clinical services model that provides data for both clinical care and patient outcomes research within the constraints of a clinical setting. During a woman's first two clinic visits, data are gathered in structured interviewswith standardized instruments-adapted for relevance to the population-that meet clinical and service needs, as well as measure components of the Whole Life model. Interviews are conducted by existing front-line staff who have been trained in usingthese instruments to gather information typically recorded in clinical notes. The implementation of Whole Life to date clearly demonstrates the feasibility of mental health-primary care services integration in a publicly funded HIV primary care clinic serving poor women of color.
<61>Unique Identifier 10977762Authors Hajat A. Lucas JB. Kington R.Title Health outcomes among Hispanic subgroups: data from the National Health Interview Survey, 1992-95.Source Advance Data. (310):1-14, 2000 Feb 25.Abstract BACKGROUND: Within the next 50 years, Hispanics will become the largest minority group in the United States. The largest Hispanic subgroups are those of Mexican, Cuban, and Puerto Rican descent. The Hispanic population is heterogeneous in terms
Page 29

401-600.txtof culture, history, socioeconomic status (SES) and health status. In this report, various health status measures are compared across Hispanic subgroups in the United States. METHODS: National Health Interview Survey (NHIS) data aggregated from 1992 through 1995 were analyzed. NHIS is one of the few national surveys that has a sufficiently large sample size to adequately compare the different subgroups. Data are presented for four Hispanic origin subgroups--Mexican, Cuban, Puerto Rican, and "other Hispanic" persons--for the Hispanic population as a whole and for the non-Hispanic white and non-Hispanic black populations. These groups are compared with respect to several health status outcomes, providing both age-adjusted and unadjusted estimates. RESULTS: The health indicators for Puerto Rican persons are significantly worse than for the other Hispanic origin subgroups. For example, about21% of Puerto Rican persons reported having an activity limitation, compared with about 15% of Cuban and Mexican persons and 14% of "other Hispanic" persons. In contrast, the health indicators of Cuban persons are often better than those of the other subgroups. For example, Cuban persons reported an average of 3 days per year lost from school or work, compared with about 6 days for Mexican and Puerto Rican persons and 7 days for "other Hispanic" persons. Mexican persons fare better than Puerto Rican persons on measures such as restricted activity days, bed disability days and hospitalizations. CONCLUSION: These data demonstrate clear differences in health status as well as indicators of socioeconomic status across Hispanic subgroups in the United States. Data on Hispanic subgroups facilitate the planning of public health services for various underserved populations.
<62>Unique Identifier 10929472Authors Flaskerud JH. Nyamathi AM.Institution UCLA's School of Nursing 90095-1702, USA.Title Collaborative inquiry with low-income Latina women.Source Journal of Health Care for the Poor & Underserved. 11(3):326-42, 2000 Aug.Abstract Collaborative inquiry is a form of research in which researchers and participants work collaboratively as partners. The purpose of this paper is to demonstrate the process of collaborative inquiry through an example of a longitudinal, community-based study conducted over a six-year period. The research program focusedon HIV education, counseling, and antibody testing with low-income Latina women attending a nutrition program for women, infants, and children (WIC) in Los Angeles.Collaborative, community-based inquiry emerges from the community and uses members of the targeted group to design the program, convey the message, act as advocates, evaluate the outcomes of the program, and disseminate research findings. The goal isempowerment and emancipation of both participants and researchers. Five areas in theconduct of community-based collaborative inquiry are demonstrated here: program design, implementation, evaluation, dissemination of the results of the program, andempowerment and emancipation.
<63>Unique Identifier 10920752Authors Dixon JM. Douglas RM. Eckersley RM.Institution National Centre for Epidemiology and Population Health, Australian National University, Canberra, ACT. [email protected] Making a difference to socioeconomic determinants of health in Australia: a research and development strategy.Source
Page 30

401-600.txt Medical Journal of Australia. 172(11):541-4, 2000 Jun 5.Abstract Disparities in health across the socioeconomic spectrum are now recognised worldwide and demand policy action. Pathways from social disadvantage to health outcomes are poorly understood, and reducing social disadvantage poses crosscutting political, moral and methodological issues. The Health Inequalities Research Collaboration, an initiative of the Commonwealth Department of Health and Aged Care,is establishing a research and development process to support departmental efforts to reduce health inequalities. The collaboration is building research networks in child development, community resources and primary healthcare. Policy action needs to extend beyond the health portfolio and the role of government. Broad strategies are required, as is research to fearlessly evaluate the health effects of governmentpolicy, economic activity and cultural change. The Canadian Institute for Advanced Research is a model for national research of the kind needed in Australia.
<64>Unique Identifier 10977465Authors de Lissovoy G. Ganoczy DA. Ray NF.Institution MEDTAP International, Inc, Bethesda, MD 20814, USA. [email protected] Relationship of hemoglobin A1c, age of diabetes diagnosis, and ethnicity to clinical outcomes and medical costs in a computer-simulated cohort of persons with type 2 diabetes.Source American Journal of Managed Care. 6(5):573-84, 2000 May.Abstract OBJECTIVE: To project the impact of maintaining long-term glycemic control (i.e., a sustained reduction in glycosylated hemoglobin (hemoglobin A1c [HbA1c]) on the lifetime incidence and direct medical costs of complications in persons with type 2 diabetes. STUDY DESIGN, PATIENTS, AND METHODS: Computer simulation of hypothetical patient cohorts using a published model developed by the National Institutes of Health. RESULTS: Across all HbA1c levels, Hispanics had the highest and whites had the lowest complication rates. With lower maintained HbA1c, the absolute decrease incomplication rates was greatest and the reduction in direct medical expenditures washighest among Hispanics (18% vs 15% for blacks and 12% for whites). Complication rates and costs were most dramatically reduced when lower levels of HbA1c were maintained among persons with a younger age at diagnosis. CONCLUSIONS: Maintaining long-term glycemic control reduces complication rates and costs for medical care forall ethnic groups regardless of age at diagnosis. Relatively greater benefit is achieved by interventions targeting Hispanics and younger, newly diagnosed persons.
<65>Unique Identifier 10910534Authors Smith GG. Celano M.Institution Cherokee Health Systems, Tazewell, Tennessee 37879, USA.Title Revenge of the mutant cockroach: culturally adapted storytelling in the treatment of a low-income African American boy.Source Cultural Diversity & Ethnic Minority Psychology. 6(2):220-7, 2000 May.Abstract A clinical case is presented in which a culturally adapted storytelling technique was used in child therapy with a socioeconomically disadvantaged African American boy. In this intervention, the child and therapist co-created a story by taking turns adding to the story during therapy sessions. The child's contributions to the
Page 31
401-600.txtstory were interpreted by taking into account his sociocultural context, and the therapist's responses were adapted to reflect relevant sociocultural factors. Advantages of storytelling techniques in child therapy are presented, and issues to consider when using these techniques with culturally diverse populations are discussed.
<66>Unique Identifier 10905417Authors Sagatun-Edwards I. Saylor C.Institution Administration of Justice Department, San Jose State University, CA 95192-0050, USA.Title Drug-exposed infant cases in juvenile court: risk factors and court outcomes.Source Child Abuse & Neglect. 24(7):925-37, 2000 Jul.Abstract OBJECTIVE: The purpose of this study was to determine which factors were significantly associated with court outcomes for drug exposed infants in dependency court. METHOD: A longitudinal study of 118 drug exposed infant social services and juvenile court files of petitioned cases through all court hearings, using chi-squares and logistic regressions data analysis. RESULTS: There was an overrepresentation of minority mothers who were poor, unemployed, undereducated, andsingle, with prior referrals to the dependency system and criminal records. The chi-square analysis suggested that variables such as ethnicity, past referrals, and criminal record were significantly associated with court outcomes for all hearings, with minority cases less likely to receive family maintenance orders, and more likely to have their children placed out of home. The regression analysis however showed a different pattern. Ethnicity and prior referrals disappeared as significantrisk factors altogether. Only at the initial dispositional hearing did a criminal record significantly influence court decisions. In subsequent hearings, mothers' compliance with court orders and attending court hearings became the significant factors associated with court outcomes. CONCLUSIONS: Mothers' behavior was more important for court outcomes than ethnicity, past referrals, and criminal record. Itis therefore imperative that mothers are motivated to successfully comply with courtorders by offering culturally appropriate services and facilitating attendance at court hearings.
<67>Unique Identifier 10897551Authors Wilson AH. Pittman K. Wold JL.Institution Department of Nursing, Clayton College and State University, Morrow, GA, USA. [email protected] Listening to the quiet voices of Hispanic migrant children about health.Source Journal of Pediatric Nursing. 15(3):137-47, 2000 Jun.Abstract There is a paucity of literature related to school-aged migrant children's perceptions of their own health. To best provide culturally competent care, more information is needed about migrant children's experiences. Focus-group methodology allowed the voices of migrant children to be heard by primary health care providers at a summer school program for children of migrant farm workers in south Georgia. Seventy-three children participated in 14 focus-group sessions. Six themes emerged from the data that were analyzed by using a qualitative software system. They are healthy behaviors, acculturation issues, environmental influences, health care
Page 32

401-600.txtactions, health behavior outcomes, and learning needs. Emerging patterns within eachtheme render insight about these migrant children. The findings suggest implicationsfor pediatric nurses related to culturally competent care.
<68>Unique Identifier 10898051Authors Rocco MV. Frankenfield DL. Frederick PR. Pugh J. McClellan WM. Owen WF.Institution Department of Internal Medicine, Section of Nephrology, Wake Forest University School of Medicine, Winston-Salem, North Carolina 27157-1053, USA. [email protected] Intermediate outcomes by race and ethnicity in peritoneal dialysis patients: results from the 1997 ESRD Core Indicators Project. National ESRD Core Indicators Workgroup.Source Peritoneal Dialysis International. 20(3):328-35, 2000 May-Jun.Abstract BACKGROUND: Hispanics are the fastest growing minority group in the United States,and approximately 10% of all end-stage renal disease (ESRD) patients are Hispanic. Few data are available, however, regarding dialysis adequacy and anemia management in Hispanic patients receiving peritoneal dialysis in the U.S. METHODS: Data from the Health Care Financing Administration (HCFA) ESRD Core Indicators Project were used to assess racial and ethnic differences in selected intermediate outcomes for peritoneal dialysis patients. RESULTS: Of the 1219 patients for whom data were available from the 1997 sample, 9% were Hispanic, 24% were non-Hispanic blacks, and 59% were non-Hispanic whites. Hispanics were more likely to have diabetes mellitus as a cause of ESRD compared to blacks or whites, and both Hispanics and blacks were younger than white patients (both p < 0.001). Although whites had higher weekly Kt/Vand creatinine clearance values compared to blacks or Hispanics (p < 0.05), blacks had been dialyzing longer (p < 0.01) and were more likely to be anuric compared to the other two groups (p < 0.001). Blacks had significantly lower mean hematocrit values (p < 0.001) and a greater proportion of patients who had a hematocrit level less than 28% (p < 0.05) compared to Hispanics or whites, despite receiving significantly larger weekly mean epoetin alfa doses (p < 0.05) and having significantly higher mean serum ferritin concentrations (p < 0.01). Multivariate logistic regression analysis revealed significant differences by race/ethnicity for experiencing a weekly Kt/V urea < 2.0 and hypertension, but not for other intermediate outcomes examined (weekly creatinine clearance < 60 L/week/1.73 m2, Hct< 30%, and serum albumin < 3.5/3.2 g/dL). CONCLUSION: Hispanics had adequacy values similar to blacks and anemia parameters similar to whites. Additional studies are needed to determine the etiologies of the differences in intermediate outcomes by racial and ethnic groupings in peritoneal dialysis patients.
<69>Unique Identifier 10893119Authors Strayhorn G.Institution University of North Carolina at Chapel Hill School of Medicine, USA.Title A pre-admission program for underrepresented minority and disadvantaged students: application, acceptance, graduation rates and timeliness of graduating from medical school.Source Academic Medicine. 75(4):355-61, 2000 Apr.Abstract PURPOSE: To determine whether students' performances in a pre-admission program predicted whether participants would (1) apply to medical school, (2) get accepted,
Page 33

401-600.txtand (3) graduate. METHOD: Using prospectively collected data from participants in the University of North Carolina at Chapel Hill's Medical Education Development Program (MEDP) and data from the Association of American Colleges Student and Applicant Information Management System, the author identified 371 underrepresented minority (URM) students who were full-time participants and completed the program between 1984 and 1989, prior to their acceptance into medical school. Logistic regression analysis was used to determine whether MEDP performance significantly predicted (after statistically controlling for traditional predictors of these outcomes) the proportions of URM participants who applied to medical school and wereaccepted, the timeliness of graduating, and the proportion graduating. Odds ratios with 95% confidence intervals were calculated to determine the associations between the independent and outcome variables. RESULTS: In separate logistic regression models, MEDP performance predicted the study's outcomes after statistically controlling for traditional predictors with 95% confidence intervals. CONCLUSIONS: Pre-admission programs with similar outcomes can improve the diversity of the physician workforce and the access to health care for underrepresented minority and economically disadvantaged populations.
<70>Unique Identifier 10890344Authors Sundquist J. Bayard-Burfield L. Johansson LM. Johansson SE.Institution Karolinska Institutet, Family Medicine Stockholm, Huddinge, Sweden.Title Impact of ethnicity, violence and acculturation on displaced migrants: psychological distress and psychosomatic complaints among refugees in Sweden.Source Journal of Nervous & Mental Disease. 188(6):357-65, 2000 Jun.Abstract This study uses data collected in 1996 by the Swedish National Board of Health andWelfare. By means of interviews with 1980 foreign-born immigrants, an attempt was made to determine the impact of a) migration status (country of birth/ethnicity), b)exposure to violence, c) Antonovsky's sense of coherence, d) acculturation status (knowledge of Swedish), e) sense of control over one's life, f) economic difficulties, and g) education, both on psychological distress (using General HealthQuestionnaire 12) and psychosomatic complaints (daytime fatigue, sleeping difficulties, and headache/migraine). Iranians and Chileans (age-adjusted) were at great risk for psychological distress as compared with Poles, whereas Turks and Kurds exhibited no such risk. When the independent factors were included in the model, the migration status effect decreased to insignificance (with the exception of Iranian men). A low sense of coherence, poor acculturation (men only), poor senseof control, and economic difficulties were strongly associated with the outcomes, generally accounting for a convincing link between migration status and psychological distress. Furthermore, a low sense of coherence, poor acculturation (men only), poor sense of control, and economic difficulties in exile seemed to be stronger risk factors for psychological distress in this group than exposure to violence before migration.
<71>Unique Identifier 10886472Authors Borowsky SJ. Rubenstein LV. Meredith LS. Camp P. Jackson-Triche M. Wells KB.Institution Center for Chronic Disease Outcomes Research, Veterans Affairs Medical Center, Minneapolis, MN 55417, USA. [email protected] Who is at risk of nondetection of mental health problems in primary care?.Source
Page 34

401-600.txt Journal of General Internal Medicine. 15(6):381-8, 2000 Jun.Abstract OBJECTIVE: To determine patient and provider characteristics associated with increased risk of nondetection of mental health problems by primary care physicians.DESIGN: Cross-sectional patient and physician surveys conducted as part of the Medical Outcomes Study. PARTICIPANTS: We studied 19,309 patients and 349 internists and family physicians. MEASUREMENTS AND MAIN RESULTS: We counted "detection" of a mental health problem whenever physicians reported, in a postvisit survey, that theythought the patient had a mental health problem or that they had counseled or referred the patient for mental health. Key independent variables included patient self-reported demographic characteristics, health-related quality of life (HRQOL), depression diagnoses according to the Diagnostic and Statistical Manual of Mental Disorders, and physician demographics and proclivity to provide counseling for depression. Logistic regression analysis, adjusted for HRQOL, revealed physicians were less likely to detect mental health problems in African Americans (odds ratio [OR], 0.63; 95% confidence interval [CI], 0.46 to 0.86), men (OR, 0.64; 95% CI, 0.54to 0.75), and patients younger than 35 years (OR, 0.61; 95% CI, 0.44 to 0.84), and more likely to detect them in patients with diabetes (OR, 1.4; 95% CI, 1.0 to 1.8) or hypertension (OR, 1.3; 95% CI, 1.1 to 1.6). In a model that included DSM-III diagnoses, odds of detection remained reduced for African Americans as well as for Hispanics (OR, 0.29; 95% CI, 0.11 to 0.71), and patients with more-severe DSM-III diagnoses were more likely to be detected. Physician proclivity toward providing counseling for depression influenced the likelihood of detection. CONCLUSIONS: Patients' race, gender, and coexisting medical conditions affected physician awareness of mental health problems. Strategies to improve detection of mental health problems among African Americans, Hispanics, and men should be explored and evaluated.
<72>Unique Identifier 10876468Authors Fletcher AB.Institution School of Nursing, University of Mississippi Medical Center, Jackson, USA.Title African American folk medicine: a form of alternative therapy. [Review] [15 refs]Source ABNF Journal. 11(1):18-20, 2000 Jan-Feb.Abstract Illness and healing are not discrete phenomena that can be isolated and consideredoutside their social, cultural and political contexts. When people develop a health problem and/or need, they secure relief by means of various options, all of which are social, cultural or political. As access to health care becomes increasingly difficult and Americans' lifestyles are becoming more fast pace, many people are literally going "back to nature" in their search for improved health and well being.As health care reform is forever changing and is being debated at the highest policylevels, many rural residents struggle with the distinctive features of their environment that can make obtaining good health care a challenge While many of theseresidents have long recognized self-care as a means of meeting this challenge, others have simply practiced self-care in the context of their cultural heritage. The purposes of this manuscript are (a) to identify some commonly used folk remedies, (b) to examine the relationships between health beliefs and the outcomes of these beliefs, and (c) educate healthcare professionals as to the importance of recognizing and accepting culturally diverse folk remedies. [References: 15]
<73>Unique Identifier 10876362Authors Akhtar S.
Page 35
401-600.txtInstitution Department of Management, City University of Hong Kong, Kowloon, Hong Kong. [email protected] Influences of cultural origin and sex on work values.Source Psychological Reports. 86(3 Pt 1):1037-49, 2000 Jun.Abstract This study examined the influences of cultural origin and sex on intrinsic, instrumental, and systemic work values using an individual level analysis. Data on importance of work outcomes were obtained from a stratified sample of 111 Hong Kong Chinese, British, and American managerial employees of a multinational media company. Analysis of variance showed that compared to Hong Kong Chinese, British andAmerican managerial employees scored significantly higher on intrinsic work values and lower on instrumental work values. Cultural origin did not significantly influence systemic work values. Sex differences in the three work values were also not significant. Implications for managerial practice are discussed.
<74>Unique Identifier 10867779Authors Ganguli M. Chandra V. Kamboh MI. Johnston JM. Dodge HH. Thelma BK. Juyal RC. Pandav R. Belle SH. DeKosky ST.Institution Western Psychiatric Institute and Clinic, 3811 O'Hara St, Pittsburgh, PA 15213-2593, USA. [email protected] Apolipoprotein E polymorphism and Alzheimer disease: The Indo-US Cross-National Dementia Study.[see comment].Source Archives of Neurology. 57(6):824-30, 2000 Jun.Abstract BACKGROUND: The APOE*E4 allele of the gene for apolipoprotein E (APOE) has been reported as a risk factor for Alzheimer disease (AD) to varying degrees in differentethnic groups. OBJECTIVE: To compare APOE*E4-AD epidemiological associations in India and the United States in a cross-national epidemiological study. DESIGN: Case-control design within 2 cohort studies, using standardized cognitive screening and clinical evaluation to identify AD and other dementias and polymerase chain reaction to identify APOE genotyping. PARTICIPANTS: Rural community samples, aged 55years or older (n=4450) in Ballabgarh, India, and 70 years or older (n=886) in the Monongahela Valley region of southwestern Pennsylvania. MAIN OUTCOME MEASURES: Criteria of the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer's Disease and Related Disorders Association for probable and possible AD and Clinical Dementia Rating (CDR) scale for dementia staging. RESULTS: Frequency of APOE*E4 was significantly lower (P<.001) in Ballabgarh vs the Monongahela Valley (0.07 vs 0.11). Frequency of probable or possible AD, with CDR ofat least 1.0, in the Indian vs US samples, was as follows: aged 55 to 69 years, 0.1%(Indian sample only); aged 70 to 79 years, 0.7% vs 3.1%; aged 80 years or older, 4.0% vs 15.7%. Among those aged 70 years or older, adjusted odds ratios (95% confidence interval) for AD among carriers of APOE*E4 vs noncarriers were 3.4 (1.2-9.3) and 2.3 (1.3-4.0) in the Indian and US samples, respectively, and not significantly different between cohorts (P=. 20). CONCLUSION: This first report of APOE*E4 and AD from the Indian subcontinent shows very low prevalence of AD in Ballabgarh, India, but association of APOE*E4 with AD at similar strength in Indian and US samples. Arch Neurol. 2000.
<75>Unique Identifier 10868612Authors
Page 36

401-600.txt O'Rourke KM. Redlinger TE. Waller DK.Institution Houston School of Public Health, University of Texas, El Paso 79902, USA.Title Declining levels of erythrocyte folate during the postpartum period among Hispanicwomen living on the Texas-Mexico border.Source Journal of Womens Health & Gender-Based Medicine. 9(4):397-403, 2000 May.Abstract Hispanic women have higher parity and shorter interbirth intervals than women of other ethnic groups. Thus, they are more likely to become pregnant relatively soon after giving birth, which may place these women at risk of low or deficient levels of specific nutrients. Folic acid is of particular concern because recent studies suggest that maternal use of folic acid supplements may be associated with better reproductive outcomes. The purpose of this study was to assess folic acid levels in postpartum Hispanic women. Using a cross-sectional design, we measured erythrocyte folate values for 188 low-income Hispanic women 1-12 months postpartum who were receiving services at the Women, Infants, and Children (WIC) clinics in El Paso, Texas. An interview was administered to collect information on diet, vitamin use, and method of infant feeding. Mean erythrocyte folate levels decreased from >1300 ng/ml during the first 4 months postpartum to a low of 1017 ng/ml by 12 months postpartum, for an overall decrease of approximately 23% (p = 0.004). Use of postpartum vitamin supplements was significantly associated with higher folate levels. However, only 35% of mothers used vitamins beyond 1 month postpartum. Study results suggest that these mothers may be at risk of developing low or deficient levels of folic acid during the postpartum period. Educational campaigns targeting these women as well as other groups of postpartum women should encourage them to comply with the U.S. Public Health Service recommendation that women of childbearingage consume 0.4 mg of folic acid daily.
<76>Unique Identifier 10861912Authors Harwood DG. Barker WW. Ownby RL. Bravo M. Aguero H. Duara R.Institution The Wien Center for Alzheimer's Disease and Memory Disorders, Mount Sinai Medical Center, Miami Beach, FL 33140, USA.Title Predictors of positive and negative appraisal among Cuban American caregivers of Alzheimer's disease patients.Source International Journal of Geriatric Psychiatry. 15(6):481-7, 2000 Jun.Abstract OBJECTIVE: This study investigated predictors of positive (satisfaction) and negative (burden) appraisal among Cuban American (CA) caregivers of Alzheimer's disease (AD) patients. DESIGN: Cross-sectional study of AD patients and their familycaregivers. SETTING: A university-affiliated outpatient memory disorders clinic. SUBJECTS: A convenience sample of 40 CA family caregivers of patients diagnosed withprobable or possible AD according to NINCDS-ADRDA diagnostic criteria. MEASURES: AD patients: Mini-Mental State Examination (MMSE), Blessed Dementia Scale (BDS) and theBehavioral Pathology in Alzheimer's Disease Rating Scale (BEHAVE-AD). Caregivers: Caregiving Burden Scale (CBS), Caregiving Satisfaction Scale (CSS), Perceived Emotional Support scale (PES) and the Short Form-36 Health Survey-General Health Index (GH). RESULTS: Appraised burden was predicted by increased patient behavioral pathology, female caregiver gender and lower levels of perceived emotional support. The association between older caregiver age and increased burden approached significance. Older caregiver age and higher levels of perceived social support wereshown to predict appraised satisfaction. Post-hoc analyses also indicated that length of residence in the United States, a measure of acculturation, was not associated with positive or negative appraisal. CONCLUSION: Appraised burden and satisfaction represent important outcomes of dementia care that show relations with
Page 37

401-600.txtdistinct factors among CA caregivers. It is clear that further research is warrantedin order to ascertain the relationship of ethnicity or culture to the process and psychological consequences of dementia caregiving. Continued investigations into predictors of caregiving satisfaction are also recommended. Copyright 2000 John Wiley & Sons, Ltd.
<77>Unique Identifier 10840885Authors Hasui C. Hayashi M. Tomoda A. Kohro M. Tanaka K. Dekio F. Kitamura T.Institution Department of Sociocultural and Environmental Research, National Institute of Mental Health, NCNP, Chiba, Japan.Title Patients' desire to participate in decision-making in psychiatry: a questionnaire survey in Japan.Source Psychological Reports. 86(2):389-99, 2000 Apr.Abstract Japanese national sentiment has been described as paternalistic, which has potentially wide-ranging implications for the manner in which psychiatric patients should participate in medical decision-making. To examine the extent and possible determinants of the desire to participate in medical decision-making among Japanese people, we distributed a packet of questionnaires to 747 (nonmedical) university students and 114 of their parents. The questionnaires included an imaginary case vignette of psychotic depression. The participants were asked whether they would want various types of medical information, i.e., diagnosis, aetiology, treatment, outcomes, medical charts, etc., disclosed to them were they in such a psychiatric condition. Also included was the 1995 Scale for Independent and Interdependent Construal of the Self by Kiuchi. More than half of the participants wanted all the types of medical information disclosed to them. Those participants who wanted to have all types of information disclosed to them (n = 413) as compared to those who did not want to know at least one type of information (n = 445), tended to be male and to have an educational background in psychiatry (9.7% vs 5.4%) as well as an assertive attitude as indicated by a higher score on Independence on the Scale for Independence and Interdependent Construal of the Self. These results suggest that the Japanese in this sample are more likely to want to make an autonomous contribution to the psychiatric decision-making process and that less desire for information can be predicted by some demographic and personality factors.
<78>Unique Identifier 10841294Authors Morehouse E. Tobler NS.Institution Student Assistance Services Corporation, Tarrytown, New York 10591, USA.Title Preventing and reducing substance use among institutionalized adolescents.Source Adolescence. 35(137):1-28, 2000 Spring.Abstract The Residential Student Assistance Program, serving high-risk, multiproblem, inner-city, primarily African-American and Latino youth, was evaluated for its ability to prevent and decrease alcohol and other drug use. Participants were drawn from several adolescent residential facilities: three foster care sites for abused, neglected, orphaned, or troubled adolescents, a nonsecure facility for adjudicated juvenile offenders, a treatment center for teens with severe psychiatric problems, and a locked county correctional facility. In addition, comparison groups were employed. A 5th-year outcome evaluation documented the program's effectiveness in
Page 38

401-600.txtboth preventing and reducing substance use among participants, with impact related to program dosage. Qualitative process data clarified and strengthened confidence inthe quantitative outcomes.
<79>Unique Identifier 10833676Authors Nyamathi AM. Stein JA. Swanson JM.Institution School of Nursing, University of California, Los Angeles 90095-1702, USA. [email protected] Personal, cognitive, behavioral, and demographic predictors of HIV testing and STDs in homeless women.Source Journal of Behavioral Medicine. 23(2):123-47, 2000 Apr.Abstract Using a multiracial sample of 621 homeless women, we tested a latent variable causal model of personal, cognitive, behavioral, and demographic predictors of two coping mediators and the outcome variables of HIV testing and return for test results and a recent STD infection. HIV testing and return were predicted by more social support, greater AIDS knowledge, greater perceived risk for AIDS, and more problem-focused coping strategies. Recent STDs were predicted by more AIDS knowledge, emotion-focused coping strategies, and risky sexual behavior and one measured variable, crack cocaine use. Emotion-focused coping strategies were predicted by drug use, less self-esteem, more social support, and greater perceived risk for AIDS. Hispanics reported less emotion-focused coping strategies than African-Americans. Predictors of problem-focused coping strategies included less drug use, more self-esteem, more social support, more AIDS knowledge, and less riskysexual behavior. African-Americans reported less problem-focused coping strategies than Latinas. Indirect effects on the outcomes mediated through coping styles are also reported. Theoretical and practical implications of results for community outreach are discussed.
<80>Unique Identifier 10829058Authors Rivera-Luna R. Cardenas-Cardos R. Leal-Leal C. Meza-Coria C.Title Leukemia in Mexican versus Mexican-American children.[comment].Source Journal of Clinical Oncology. 18(11):2349-51, 2000 Jun.
<81>Unique Identifier 10830735Authors Huan SY. Yang CH. Chen YC.Institution Department of Internal Medicine, National Taiwan University Hospital, Taipei.Title Arsenic trioxide therapy for relapsed acute promyelocytic leukemia: an useful salvage therapy. [Review] [72 refs]Source Leukemia & Lymphoma. 38(3-4):283-93, 2000 Jul.Abstract Arsenic trioxide (As2O3) was recently identified as a very potent agent against acute promyelocytic leukemia (APL). Intravenous infusion of 10 mg As2O3 daily for
Page 39

401-600.txtone to two months can induce significant complete remission (CR) of APL, and there is no cross drug-resistance between As2O3 and other antileukemic agents, including all-trans retinoic acid (ATRA). The CR rate of relapsed and/or refractory APL patients who received As2O3 treatment ranged from 52.3% to 93.3%. The median duration to CR ranged from 38 to 51 days, with accumulative As2O3 dosage of 340-430 mg. Although most adverse reactions of As2O3 treatment were tolerable, certain infrequent but severe toxicities related to As2O3 were observed, including renal failure, hepatic damage, cardiac arrhythmia and chronic neuromuscular degeneration, which should be monitored carefully. As2O3 can induce partial differentiation and subsequent apoptosis of APL cells through degradation of wild type PML and PML/RAR alpha chimeric proteins and possible anti-mitochondrial effects. Like the treatment of ATRA in APL, early relapses from As2O3 treatment within a few months were not infrequently seen, indicating that rapid emerging resistance to As2O3 can occur. Nevertheless, the PML/RAR alpha fusion protein was reported to disappear in some APLpatients who received As2O3, and who might earn long-survival. However, the follow-up is still too short to draw the conclusion. Intriguingly, it has been shownthat As2O3 can also induce apoptosis of other non-APL tumor cells with clinical achievable concentrations. However, the detailed molecular mechanisms are not yet fully understood. Further studies regarding to the pharmacological characters, clinical efficacies, toxicities, apoptogenic mechanisms, and spectrum of anti-tumor activity of As2O3 are warranted. [References: 72]
<82>Unique Identifier 10803449Authors Mastoor M. Iqbal U. Pinnow E. Lindsay J Jr.Institution Section of Cardiology, Washington Hospital Center, District of Columbia, USA.Title Ethnicity does not affect outcomes of coronary angioplasty.Source Clinical Cardiology. 23(5):379-82, 2000 May.Abstract BACKGROUND: Access to high quality medical care and especially to complex procedures may be adversely affected in members of a minority ethnic group or a lower socioeconomic class. For example, Caucasians undergo coronary artery bypass grafting (CABG) or percutaneous transluminal coronary interventions (PTCI) twice as frequently as African-Americans. Data exist to suggest that African-Americans deriveless benefit than Caucasians from CABG. HYPOTHESIS: We investigated the possibility that outcomes of catheter-based coronary angioplasty might also be less favorable inminority populations. METHODS: We analyzed in-hospital outcomes in 6,559 consecutivepatients who underwent PTCI in our laboratory. In 37 ethnicity was classified as "other," 5,203 (79.8%) were identified as Caucasians, 863 (13.2%), as African-Americans, and 456 (7.0%), as Hispanics. Twelve baseline clinical, angiographic, and procedural characteristics were entered into a computerized data base. Hospital complications were identified by trained quality assurance nurses. RESULTS: Substantial differences in baseline characteristics existed between the populations. Despite these differences, on univariate comparison of ethnicity and outcome, no differences between ethnic groups were found with a single exception. Mortality in Hispanics was higher than in the other two populations. (2.0 vs. 0.7 and 0.8%, respectively, p = 0.008). However, when this was adjusted for baseline characteristics, the difference was not significant. CONCLUSIONS: In contrast to previous studies suggesting less favorable outcomes of CABG in African-American patients, this analysis demonstrates an equal frequency of procedural success and rate of hospital complications for PTCI in that population, in Hispanics, and in Caucasians.
<83>Unique Identifier 10801066
Page 40

401-600.txtAuthors De La Rosa M. Vega R. Radisch MA.Institution Florida International University School of Social Work, Miami 33199, USA.Title The role of acculturation in the substance abuse behavior of African-American and Latino adolescents: advances, issues, and recommendations. [Review] [44 refs]Source Journal of Psychoactive Drugs. 32(1):33-42, 2000 Jan-Mar.Abstract This article provides a review of the literature on the acculturation of Latino and African-American adolescents to traditional European-American cultural values, and the effect on their substance abusing behaviors. The review includes a critical analysis of studies that examine the effects of acculturation on the mental health and well-being of Latino adolescents. Recent findings documenting the association between acculturation and substance abuse among Latino adolescents are discussed. The article also examines the dearth of research on the role of acculturation in thesubstance-abusing behaviors of African-American adolescents. The authors assert thatunderstanding the effects of acculturation on these behaviors could begin to explainwhy African-American adolescent substance abuse rates have been historically lower than those of European-American and Latino adolescents. Also included is an examination of research on the role of acculturation in treatment outcomes of Latinoand African-American adolescents. [References: 44]
<84>Unique Identifier 10793518Authors Zuvekas A. Wells BL. Lefkowitz B.Institution Center for Health Services Research and Policy, School of Public Health and HealthServices, George Washington University, Annandale, VA 22003, USA.Title Mexican American infant mortality rate: implications for public policy.Source Journal of Health Care for the Poor & Underserved. 11(2):243-57, 2000 May.Abstract Infants of Mexican American descent have lower infant mortality rates (IMRs) than do non-Hispanic blacks and non-Hispanic whites. Because IMR is used in allocation methods for primary health care resources, the result could be discrimination against Mexican American populations in the distribution of resources. This study examined the National Center for Health Statistics' infant birth and death records, as well as unpublished data from the Bureau of Primary Health Care. This study foundthat the low Mexican American IMRs are real and not simply a data anomaly and that inclusion of birth outcomes has a small and mixed effect on the designation of high-Hispanic areas as being medically underserved or short of primary health care professionals. The authors suggest inclusion of an additional high-Hispanic health indicator in the designation criteria for health resources.
<85>Unique Identifier 10793513Authors Cunningham WE. Mosen DM. Morales LS. Andersen RM. Shapiro MF. Hays RD.Institution Department of Health Services, School of Public Health, University of California, Los Angeles 90095, USA.Title Ethnic and racial differences in long-term survival from hospitalization for HIV infection.Source
Page 41
401-600.txt Journal of Health Care for the Poor & Underserved. 11(2):163-78, 2000 May.Abstract This prospective cohort study compares 200 hospitalized, HIV-infected patients (Hispanic, African American, and white) from May 1992 to October 1998 to assess mortality (versus survival) over 75 months of follow-up. The relative risk of six-year mortality for each ethnic group is compared using Cox proportional hazards models after controlling for sociodemographic and clinical characteristics, access to general medical care, and HIV-specific treatment. The median survival of Hispanics (15.5 months) was significantly (p < 0.05) shorter than that of whites (23.8); survival for African Americans (35.1) did not differ from whites. In multivariate analysis, the adjusted relative risk of six-year mortality for Hispanics compared with whites was 2.14 (95 percent confidence interval = 1.26-3.66). The poor outcomes of Hispanics was not explained by access to general care or by HIV-specific treatment.
<86>Unique Identifier 10791612Authors Jackson J. Kennedy BL. Mandel D. Carlson M. Cherry BJ. Fanchiang SP. Ding L. Zemke R. Azen SP. Labree L. Clark F.Institution University of Southern California, Los Angeles 90089-9003, USA.Title Derivation and pilot assessment of a health promotion program for Mandarin-speaking Chinese older adults.Source International Journal of Aging & Human Development. 50(2):127-49, 2000.Abstract As the percentage of older adults of diverse ethnicities increases in the United States, the call for culturally sensitive health care service strategies that targetthe special needs of older people grows. The present report describes methods used to adapt a health care program so that it would better meet the needs of a group of well, older Mandarin-speaking Chinese residents of Los Angeles. The specific qualitative research procedures that we used to adapt the treatment program are described, along with the particular adaptations that emerged. Additionally, outcomes from a randomized pilot experiment are presented that are consistent with the notion that the adapted program was effective in reducing health-related declines among older Mandarin-speaking men and women. The overall outcome of this project is in agreement with other reports in the health care literature that address the importance of providing culturally sensitive health care service for elders.
<87>Unique Identifier 10781779Authors Rivadeneyra R. Elderkin-Thompson V. Silver RC. Waitzkin H.Institution School of Social Ecology, University of California, Irvine, Irvine, California, USA.Title Patient centeredness in medical encounters requiring an interpreter.[see comment].Source American Journal of Medicine. 108(6):470-4, 2000 Apr 15.Abstract PURPOSE: Patient-centered interviewing is associated with greater patient satisfaction and better medical outcomes than traditional encounters, but actively seeking patients' views of their illnesses and encouraging patients to express expectations, thoughts, and feelings is difficult in encounters that require an interpreter. We sought to examine physicians' use of the patient-centered approach
Page 42

401-600.txtwith patients who required the assistance of an interpreter. SUBJECTS and METHODS: Across-sectional sample of patients was videorecorded during visits with physicians at a multi-ethnic, university-affiliated, primary care clinic. Nineteen medical encounters of Spanish-speaking patients who required an interpreter and 19 matched English-speaking encounters were coded for frequency that patients mentioned symptoms, feelings, expectations, and thoughts (collectively called "offers"). Physicians' responses were coded as ignoring, closed, open, or facilitative of further discussion. RESULTS: English-speaking patients made a mean (+/- SD) of 20 +/- 11 offers, compared with 7 +/- 4 for Spanish-speaking patients (P = 0.001). Spanish-speaking patients also were less likely to receive facilitation from their physicians and were more likely to have their comments ignored (P <0.005). English-speaking patients usually received an answer or acknowledgment to their questions even if the physicians did not encourage further discussion on the topic. CONCLUSION: Spanish-speaking patients are at a double disadvantage in encounters with English-speaking physicians: these patients make fewer comments, and the ones they do make are more likely to be ignored. The communication difficulties may result in lower adherence rates and poorer medical outcomes among Spanish-speaking patients.
<88>Unique Identifier 10783206Authors East MA. Peterson ED.Title Understanding racial differences in cardiovascular care and outcomes: issues for the new millennium.[comment].Source American Heart Journal. 139(5):764-6, 2000 May.
<89>Unique Identifier 10782870Authors Heilemann MV. Lee KA. Stinson J. Koshar JH. Goss G.Institution University of California, Los Angeles 90095-6919, USA.Title Acculturation and perinatal health outcomes among rural women of Mexican descent.Source Research in Nursing & Health. 23(2):118-25, 2000 Apr.Abstract Research has shown that health outcomes for urban women of Mexican descent are related to acculturation. The purpose of this research was to compare perinatal outcomes of 773 women of Mexican descent who gave birth in three rural northern California hospitals, in relation to acculturation measured three different ways: byplace of birth, by language spoken, and by the two factors combined as an Acculturation Index (AI). The prenatal and birth records of 773 Mexico-born or U.S.-born women of Mexican descent were reviewed. Results showed that language spoken was a less useful indicator of acculturation associated with perinatal complications than place of birth or the AI. The categorization of acculturation with the AI enhanced understanding of more specific groups of rural women and their particular health outcomes.
<90>Unique Identifier 10778043Authors Cunningham WE. Hays RD. Burton TM. Kington RS.Institution
Page 43

401-600.txt University of California, Los Angeles, USA.Title Health status measurement performance and health status differences by age, ethnicity, and gender: assessment in the medical outcomes study.Source Journal of Health Care for the Poor & Underserved. 11(1):58-76, 2000 Feb.Abstract The comparative measurement performance of self-reported health status instrumentsfor African American and Hispanic elderly has rarely been studied, despite evidence of their poor health status. This study examined psychometric performance and healthstatus differences by age, ethnicity, and gender among 10,569 ethnically diverse patients who completed the Short-Form General Health Survey in the Medical Outcomes Study (MOS). Hispanics and African Americans tended to have slightly lower measurement performance than other ethnic groups. Compared with whites, health status scores for African American and Hispanic women were slightly but significantly lower. The small differences in health status by ethnicity may be due to the MOS sampling strategy, which excluded low-socioeconomic status minorities with poor education and no regular medical care. The psychometric performance of MOShealth status measures should be examined in studies of ethnically diverse, community-dwelling, elderly populations who have poor access to care, poor education, and/or low socioeconomic status.
<91>Unique Identifier 10761813Authors Sadaniantz A. Gordon PC.Institution The Miriam Hospital, Brown University School of Medicine, Providence, Rhode Island02906, USA.Title Images in cardiology. Multiple ecchymotic lesions on the torso of a patient with unstable angina.Source Clinical Cardiology. 23(3):214-5, 2000 Mar.
<92>Unique Identifier 10757827Authors Staub L. Morgenstern LB.Institution T.L.L. Temple Foundation Stroke Project, Department of Neurology, University of Texas Medical School, Houston, TX 77030, USA.Title Stroke in Hispanic Americans. [Review] [34 refs]Source Neurologic Clinics. 18(2):291-307, 2000 May.Abstract The Hispanic American population is the fastest growing minority group with increasing representation among the older age strata. Current ethnic-specific cerebrovascular disease data regarding stroke outcomes and risk factor status revealsignificant differences compared with other race/ethnic groups. The authors discuss the literature on stroke incidence and mortality among Hispanic populations. Traditional risk factors, access to care and stroke mechanism differences are also discussed. Advances in Hispanic American specific stroke prevention and treatment efforts demand further investigation to better define Hispanic American stroke prevention and acute treatment strategies. [References: 34]
<93>Page 44

401-600.txtUnique Identifier 10755208Authors Mittal SR. Mathur A. Gokhroo R. Kaushik GG. Paldecha S.Title Effects of the Ayurvedic drug Cholesteronil on cardiovascular risk factors.Source Cardiovascular Drugs & Therapy. 14(1):95-6, 2000 Feb.
<94>Unique Identifier 10748987Authors Lewis SK. Oppenheimer VK.Institution Ohio State University, USA. [email protected] Educational assortative mating across marriage markets: non-Hispanic whites in theUnited States.Source Demography. 37(1):29-40, 2000 Feb.Abstract Whether local marriage market conditions shape marriage behavior is a central social demographic question. Most work on this subject, however, focuses on one typeof market condition--sex ratios--and on a single outcome--marital timing or sorting.We examine the impact of local marriage markets' educational composition on educational assortative mating and on how sorting varies with age. We estimate a discrete-time competing-risks model of educational sorting outcomes, using individual data from the NLSY and community descriptors aggregated from census microdata. Results show that residents of educationally less favorable marriage markets are more likely to marry down on education, and that (for women) their chance of doing so increases with age more than for residents of more favorable markets.
<95>Unique Identifier 10733064Authors Robbins MA. Elias PK. Elias MF.Title Low blood pressure and depression: comorbidity and competing outcomes.[comment].Source Journal of the American Geriatrics Society. 48(3):336-7, 2000 Mar.
<96>Unique Identifier 10673193Authors Homa DM. Mannino DM. Lara M.Institution Air Pollution and Respiratory Health Branch, Division of Environmental Hazards andHealth Effects, National Center for Environmental Health, Centers for Disease Control and Prevention, Atlanta, Georgia 30341, USA. [email protected] Asthma mortality in U.S. Hispanics of Mexican, Puerto Rican, and Cuban heritage, 1990-1995.Source American Journal of Respiratory & Critical Care Medicine. 161(2 Pt 1):504-9, 2000Feb.Abstract
Page 45

401-600.txt We used national vital statistics data for 1990 through 1995 to examine both national and regional age-adjusted asthma mortality rates for U.S. Hispanics of Mexican, Cuban, and Puerto Rican heritage, as well as for non-Hispanic whites and non-Hispanic blacks. Nationally, Puerto Ricans had an age-adjusted annual asthma mortality rate of 40.9 per million, followed by Cuban-Americans (15. 8 per million) and Mexican-Americans (9.2 per million). In comparison, non-Hispanic whites had an age-adjusted annual asthma mortality rate of 14.7 per million and non-Hispanic blacks had a rate of 38.1 per million. Age-adjusted asthma mortality for Puerto Ricans was highest in the Northeast (47.8 per million); this region accounted for 81% of all asthma deaths among Puerto Ricans in the United States. In the U.S., Puerto Ricans had the highest asthma mortality rates among Hispanics, followed by Cuban-Americans and Mexican-Americans. In addition, among Hispanic national groups, mortality rates were consistently higher in the Northeast than the Midwest, South, or West regions. These results further support that Hispanics do not represent a uniform, discrete group in terms of health outcomes, and that further public health research and interventions should take Hispanic national origin into account.
<97>Unique Identifier 10714744Authors Groff JY. Mullen PD. Byrd T. Shelton AJ. Lees E. Goode J.Institution The University of Texas-Houston Health Science Center Medical School, 77030, USA.Title Decision making, beliefs, and attitudes toward hysterectomy: a focus group study with medically underserved women in Texas.Source Journal of Womens Health & Gender-Based Medicine. 9 Suppl 2:S39-50, 2000.Abstract Variations in hysterectomy rates have been associated with assorted physician and patient characteristics, and the disproportionate rate of hysterectomies in African American women has been attributed to a higher prevalence of leiomyomas. The role ofwomen's beliefs and attitudes toward hysterectomy and participation in decision making for medical treatment has not been explored as a source of variance. The purposes of this qualitative study were to explore these constructs in a triethnic sample of women to understand beliefs, attitudes, and decision-making preferences among underserved women; to facilitate development of a quantitative survey; and to inform development of interventions to assist women with such medical decisions. Twenty-three focus groups were conducted with 148 women from community sites and public health clinics. Thirteen self-identified lesbians participated in three groups. Analysis of audiotaped transcripts yielded four main themes: perceived outcomes of hysterectomy, perceived views of men/partners, opinions about healthcareproviders, decision-making process. Across groups, the women expressed similar expectations from hysterectomy, differing only in the degree to which dimensions were emphasized. The women thought men perceived women with hysterectomy as less desirable for reasons unrelated to childbearing. Attitudes toward physicians were negative except among Hispanic women. All women expressed a strong desire to be involved in elective treatment decisions and would discuss their choice with important others. Implications for intervention development include enhancing women's skills and confidence to evaluate treatment options and to interact with physicians around treatment choices and creation of portable educational components for important others.
<98>Unique Identifier 10714741Authors Lewis CE. Groff JY. Herman CJ. McKeown RE. Wilcox LS.Institution Division of Preventive Medicine, School of Medicine, and the UAB Center for Health
Page 46

401-600.txtPromotion, University of Alabama at Birmingham, 35205, USA.Title Overview of women's decision making regarding elective hysterectomy, oophorectomy,and hormone replacement therapy. [Review] [96 refs]Source Journal of Womens Health & Gender-Based Medicine. 9 Suppl 2:S5-14, 2000.Abstract Over 600,000 hysterectomies are performed each year in the United States, the majority of which are to improve quality of life for perimenopausal women. Hysterectomy rates for common conditions differ between African American and white women, and African American women undergo surgery at a younger age for most diagnoses. Many hysterectomies are accompanied by elective oophorectomy, and hormonereplacement therapy (HRT) is commonly used, especially among women experiencing surgical menopause, despite questions about its long-term benefits and risks. Despite the high rates of hysterectomy in the United States, little is known about how women make decisions regarding this surgery and, in particular, how ethnic and cultural factors may influence these decisions. This article provides a review of what is currently known about the epidemiology of hysterectomy, oophorectomy, and HRT use and identifies gaps in knowledge about women's decision making, with a special focus on ethnic variations and cultural influences, issues addressed by the Ethnicity, Needs, and Decisions of Women (ENDOW) project. [References: 96]
<99>Unique Identifier 10714447Authors Huriwai T. Sellman JD. Sullivan P. Potiki TL.Institution National Centre for Treatment Development (Alcohol, Drugs & Addiction), Departmentof Psychological Medicine, Christchurch School of Medicine, New Zealand. [email protected] Optimal treatment for Maori with alcohol and drug-use-related problems: an investigation of cultural factors in treatment.Source Substance Use & Misuse. 35(3):281-300, 2000 Feb.Abstract There is an increasing emphasis on taking account of the diversity of social, psychological, and cultural factors in the assessment and treatment of alcohol and drug-use-related problems. In New Zealand the increasing use of customary Maori values, beliefs, and practices in the treatment of Maori with alcohol and drug-use-related problems has also been accompanied by the adaptation and integration of Western approaches to fit contemporary Maori sociocultural needs. This paper reports on an investigation of cultural factors and cultural identity in the alcohol and drug-user treatment of a clinical sample of Maori. The essential finding was a very high endorsement of the importance of cultural factors in treatment--irrespective of age, gender, mood, level of dependence, previous admissions, cultural connectedness, or whether they were treated in a Maori dedicated program or not. A significant number believed that a sense of belonging toan Iwi (tribe), identifying as a Maori and having pride in being Maori were also important in the recovery/healing process. The findings of this study support the need to investigate the relationship between specific "cultural factors" and other clinical components of effective treatment for Maori.
<100>Unique Identifier 10705354Authors Hunter CP.Institution Office of Research on Women's Health, National Institutes of Health, Bethesda,
Page 47

401-600.txtMaryland, USA.Title Epidemiology, stage at diagnosis, and tumor biology of breast carcinoma in multiracial and multiethnic populations. [Review] [37 refs]Source Cancer. 88(5 Suppl):1193-202, 2000 Mar 1.Abstract All women, regardless of their racial or ethnic origin or heritage, are at risk ofdeveloping breast cancer. Variations in breast carcinoma incidence rates among multicultural populations suggest that etiologic factors differ in their biologic expression and impact on disease outcome. Key among those factors that affect breastcarcinoma development are the roles of genetics and the environment, the reproductive experience and the effects of endogenous and exogenous hormones in women, the change in immune status and host vulnerability, and the biologic determinants of breast carcinoma. Cultural dynamics, sociodemographic differences, and behavioral characteristics across population subgroups modulate how biologic disease is expressed among different races and ethnic groups. These interactions contribute to the observed variations in breast carcinoma incidence, mortality, and survival. Stage, a measure of disease status, is used to assess prognosis, plan treatment, and evaluate outcome. Numerous studies have reported a more advanced stage of breast carcinoma at diagnosis in racial/ethnic subgroups, especially among women from African American, Hispanic, American Indian, and native Hawaiian cultures. Factors associated with advanced stage at diagnosis in multicultural populations range from changes in the basic biological characteristics at the molecular and cellular level, to more complex behavioral attributes unique to a particular multicultural population, to societal issues-such as access to care and socioeconomic conditions-all of which impact on the health measure called "stage at diagnosis." Rapid advancements in knowledge of cancer biology and of genetic markersand tumor products are providing new mechanisms for identifying etiologic pathways that can be utilized for better screening, detection, treatment and monitoring of disease. Further studies are needed that evaluate the biologic and molecular alterations in tumor development, progression, and response to therapy. Public health attention needs to be directed toward the societal influences that impact breast carcinoma development, as well as augmenting recognition of the need for culturally appropriate, broad-based behavioral changes at the community level. In addition, continued efforts are needed to ensure the inclusion of multicultural population subgroups and minority investigators in all aspects of research-basic, clinical and applied. Copyright 2000 American Cancer Society. [References: 37]
<101>Unique Identifier 10703030Authors Kieffer EC.Institution Department of Health Behavior and Health Education, Ann Arbor, MI 48109-2029, [email protected] Maternal obesity and glucose intolerance during pregnancy among Mexican-Americans.Source Paediatric and Perinatal Epidemiology. 14(1):14-9, 2000 Jan.Abstract Low birthweight is uncommon among Mexican-American infants, despite the substantial proportion of mothers who live in poverty. This apparent paradox has generated studies of factors protecting fetal growth, but may have masked other important health problems in the Mexican-American community. Obesity, impaired glucose tolerance and diabetes are common among Mexican-American women of childbearing age and during pregnancy. Prevalence of these conditions is two to fourtimes higher in Mexican-American than in non-Hispanic white women. As obesity and glucose intolerance during pregnancy are associated with fetal overgrowth and increased risk of subsequent obesity and type 2 diabetes in mother and child, the adequacy of birthweight as a measure of maternal and infant risk may be obscured in
Page 48

401-600.txtpopulations with a high prevalence of these conditions. Their possible contribution to the increasing incidence of obesity and type 2 diabetes in Mexican-American children, adolescents and young adults has not been examined. Appropriate preconception, prenatal and follow-up care may identify high-risk women, improve weight and metabolic status and reduce the severity and impact of diabetes and its complications. However, late or no prenatal care is common among Mexican-American women and the frequency of follow-up care is unknown. As low birthweight is a major public health indicator of maternal and neonatal health, perceived 'good birth outcomes' have reduced health policy, programme and research attention to Mexican-American mothers and infants. Studies of the impact of obesity and glucose intolerance during pregnancy on the birthweights of Mexican-American infants should be undertaken, along with systematic assessment of the subsequent health status and preventive health-care needs of women and children in this population.
<102>Unique Identifier 10701170Authors Guenter D. Esparza J. Macklin R.Institution Department of Family Medicine, McMaster University, Hamilton, Canada.Title Ethical considerations in international HIV vaccine trials: summary of a consultative process conducted by the Joint United Nations Programme on HIV/AIDS (UNAIDS).Source Journal of Medical Ethics. 26(1):37-43, 2000 Feb.Abstract Research that is initiated, designed or funded by sponsor agencies based in countries with relatively high social and economic development, and conducted in countries that are relatively less developed, gives rise to many important ethical challenges. Although clinical trials of HIV vaccines began ten years ago in the US and Europe, an increasing number of trials are now being conducted or planned in other countries, including several that are considered "developing" countries. Safeguarding the rights and welfare of individuals participating as research subjects in developing countries is a priority. In September, 1997, the Joint UnitedNations Programme on HIV/AIDS (UNAIDS) embarked on a process of international consultation; its purpose was further to define the important ethical issues and to formulate guidance that might facilitate the ethical design and conduct of HIV vaccine trials in international contexts. This paper summarises the major outcomes of the UNAIDS consultative process.
<103>Unique Identifier 10684743Authors Lawrence VA. Streiner D. Hazuda HP. Naylor R. Levine M. Gafni A.Institution Division of General Medicine at Audie L. Murphy Division, South Texas Veterans Health Care System, San Antonio, Texas 78284, USA.Title A cross-cultural consumer-based decision aid for screening mammography.Source Preventive Medicine. 30(3):200-8, 2000 Mar.Abstract BACKGROUND: "Women should have mammograms" is the usual perspective of educationalinterventions about screening. The perspective that "women should be informed" aboutpotential risks and benefits so they can make value- and evidence-integrated personal decisions has recently been advocated. However, this perspective has not previously been operationalized. We developed an evidence-based cross-cultural mammography decision aid (MDA), for European American and Mexican American women who
Page 49

401-600.txtare 50-70 years old, at average risk of breast cancer, of varying educational levels, and English- or Spanish-speaking. METHODS: MDA development included: (1) content development by a multidisciplinary team and lay women and (2) testing for validity and reliability. Four parts include: (1) introduction; (2) information about logistics (cost, time, discomfort) and risks (sequelae of false-positive or negative results; (3) probability of developing breast cancer; and (4) benefit of mammography regarding breast cancer outcomes (e.g., death and recurrence). We assessed reliability (stability of decisions with the same information) after 1-2 weeks. We assessed validity (comprehension of information) quantitatively (probabilities were changed to see whether preferences changed predictably) and qualitatively (focus groups, standardized probes for comprehension). Subjects were aconvenience sample of 49 European American (50-81 years old) and 54 Mexican American(49-89 years old) women from administrative staff at a medical school, the waiting room of an indigent primary care clinic, and a community center. RESULTS: Reliability was 100%. In quantitative validity testing, 22 of 28 women (89%) changedpreference as predicted with changed probabilities. Comprehension was confirmed qualitatively in all phases of testing with both Spanish and English versions. CONCLUSION: The decision aid is valid and reliable in English and Spanish for southwestern Mexican American and European American women at average risk of breast cancer, including those of low educational levels.
<104>Unique Identifier 10679533Authors Partridge MR.Title In what way may race, ethnicity or culture influence asthma outcomes?[see comment][comment].Source Thorax. 55(3):175-6, 2000 Mar.
<105>Unique Identifier 10673523Authors Pollock BH. DeBaun MR. Camitta BM. Shuster JJ. Ravindranath Y. Pullen DJ. Land VJ. Mahoney DH Jr. Lauer SJ. Murphy SB.Institution University of Florida, and Pediatric Oncology Group Statistical Office, Gainesville, FL, USA. [email protected] Racial differences in the survival of childhood B-precursor acute lymphoblastic leukemia: a Pediatric Oncology Group Study.[see comment].Source Journal of Clinical Oncology. 18(4):813-23, 2000 Feb.Abstract PURPOSE: We conducted a historic cohort study to test the hypothesis that, after adjustment for biologic factors, African-American (AA) children and Spanish surname (SS) children with newly diagnosed B-precursor acute lymphoblastic leukemia had lower survival than did comparable white children. PATIENTS AND METHODS: From 1981 to 1994, 4,061 white, 518 AA, and 507 SS children aged 1 to 20 years were treated onthree successive Pediatric Oncology Group multicenter randomized clinical trials. RESULTS: AA and SS patients were more likely to have adverse prognostic features at diagnosis and lower survival than were white patients. The 5-year cumulative survival rates were (probability +/- SE) 81.9% +/- 0.6%, 68.6% +/- 2.1%, and 74.9% +/- 2.0% for white, AA, and SS children, respectively. Adjusting for age, leukocyte count, sex, era of treatment, and leukemia blast cell ploidy, we found that AA children had a 42% excess mortality rate compared with white children (proportional hazards ratio [PHR] = 1.42; 95% confidence interval [CI], 1.12 to 1. 80), and SS children had a 33% excess mortality rate compared with white children (PHR = 1.33;
Page 50

401-600.txt95% CI, 1.19 to 1.49). CONCLUSION: Clinical presentation, tumor biology, and deviations from prescribed therapy did not explain the differences in survival and event-free survival that we observed, although differences seem to be diminishing over time with improvements in therapy. The disparity in outcome for AA and SS children is most likely related to variations in chemotherapeutic response to therapy and not to compliance. Further improvements in outcome may require individualized dosing based on specific pharmacogenetic profiles, especially for AA and SS children.
<106>Unique Identifier 10530367Authors Gruendemann BJ.Title International education--a kaleidoscopic view.[erratum appears in AORN J 1999 Dec;70(6):979].Source AORN Journal. 70(4):608-17, 1999 Oct.Abstract International travel presents opportunities for perioperative nurses to share their knowledge about surgical patient care and preventing the spread of infection. This article outlines the author's personal experiences with international travel, educational pursuits, and conferring with nurses, physicians, epidemiologists, hospital administrators, and medical product company representatives. It also discusses culture and values, teaching and learning, and accomplishments in settingswhere both financial and human resources are sparse, but outcomes are positive and meaningful.
<107>Unique Identifier 10526734Authors Harris MI.Institution National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland 20892, USA. [email protected] Racial and ethnic differences in health insurance coverage for adults with diabetes.Source Diabetes Care. 22(10):1679-82, 1999 Oct.Abstract OBJECTIVE: To evaluate the extent and types of health insurance coverage in a representative sample of adults with diabetes in the U.S. RESEARCH DESIGN AND METHODS: The Third National Health and Nutrition Examination Survey included national samples of non-Hispanic whites, non-Hispanic blacks, and Mexican-Americans aged > or = 20 years. Information on medical history and treatment of diabetes was obtained to determine subjects who had been diagnosed with diabetes by a physician before the survey (n = 1,503) and subjects without diagnosed diabetes (n = 17,319). Information on health insurance coverage was obtained via a structured questionnairefor 96% of participants. RESULTS: A total of 93% of all adults with diabetes had some form of health insurance. Of these subjects, 73% had private insurance, 48% hadMedicare coverage, 15% had Medicaid coverage, and 5% had Champus/Veterans Affairs coverage. Approximately 52% of adults with diabetes had multiple types of health insurance, and 54% had health care coverage through one or more government-sponsoredprograms. A greater proportion of non-Hispanic whites (91%) and non-Hispanic blacks (89%) than Mexican-Americans (66%) had health insurance among subjects aged 20-64 years. For those aged > or = 65 years, coverage was virtually 100% for all racial and ethnic groups. Non-Hispanic whites had the highest rate of coverage through private insurance (81%), with non-Hispanic blacks having an intermediate rate (56%)
Page 51
401-600.txtand Mexican-Americans having the lowest rate (45%). Rates of coverage were similar for adults with and without diabetes in each racial and ethnic group for any type ofinsurance and for private insurance. CONCLUSIONS: There are marked racial and ethnicdifferences in health insurance coverage for adults with diabetes, although these differences are similar to those for adults without diabetes. Whether these racial and ethnic disparities influence access to care, quality of care, or health outcomesfor people with diabetes remains to be determined.
<108>Unique Identifier 10526733Authors Benjamin EM. Schneider MS. Hinchey KT.Institution Clinical Practices Evaluation and Management, Baystate Medical Center, Springfield, MA 01199, USA. [email protected] Implementing practice guidelines for diabetes care using problem-based learning. Aprospective controlled trial using firm systems.Source Diabetes Care. 22(10):1672-8, 1999 Oct.Abstract OBJECTIVE: A controlled trial with 15-month follow-up was conducted in two outpatient clinics to study the effects of using the problem-based learning technique to implement a diabetes clinical practice guideline. RESEARCH DESIGN AND METHODS: A total of 144 patients with type 2 diabetes aged 25-65 years in two internal medicine outpatient clinics were enrolled in the study. African-Americans and Hispanics made up > 75% of the patients. Doctors and staff in one of the clinicswere trained in the use of a clinical practice guideline based on Staged Diabetes Management. A problem-based learning educational program was instituted to reach consensus on a stepped intensification scheme for glycemic control and to determine the standards of care used in the clinic. HbA1c was obtained at baseline and at 9 and 15 months after enrollment. RESULTS: At 9 months, there was a mean -0.90% within-subject change in HbA1c in the intervention group, with no significant changes in the control group. The 15-month mean within-subject change in HbA1c of -0.62% in the intervention group was also significant. Among intervention patients, those with the poorest glycemic control at baseline realized the greatest benefit inimprovement of HbA1c. The intervention group also exhibited significant changes in physician adherence with American Diabetes Association standards of care. CONCLUSIONS: Clinical practice guidelines are an effective way of improving the processes and outcomes of care for patients with diabetes. Problem-based learning isa useful strategy to gain physician support for clinical practice guidelines. More intensive interventions are needed to maintain treatment gains.
<109>Unique Identifier 10516355Authors Frankenfield DL. Rocco MV. Frederick PR. Pugh J. McClellan WM. Owen WF Jr.Institution Section of Nephrology, Health Care Financing Administration, Baltimore, MD 21244, USA. [email protected] Racial/ethnic analysis of selected intermediate outcomes for hemodialysis patients: results from the 1997 ESRD Core Indicators Project.[see comment].Source American Journal of Kidney Diseases. 34(4):721-30, 1999 Oct.Abstract Principal goals of the End-Stage Renal Disease (ESRD) Core Indicators Project are to improve the care provided to ESRD patients and to identify categorical variability in intermediate outcomes of dialysis care. The purpose of the current
Page 52

401-600.txtanalysis is to extend our observations about the variability of intermediate outcomes of ESRD care among different racial and gender groups to a previously unreported group, Hispanic Americans. This group is a significant and growing minority segment of the ESRD population. A random sample of Medicare-eligible adult,in-center, hemodialysis patients was selected and stratified from an end-of-year ESRD patient census for 1996. Of the 6,858 patients in the final sample, 45% were non-Hispanic whites, 36% were non-Hispanic blacks, and 11% were Hispanic. Whites were older than blacks or Hispanics (P < 0.001). Hispanics were more likely to have diabetes mellitus as a primary diagnosis than either blacks or whites (P < 0.001). Even though they received longer hemodialysis times and were treated with high-flux hemodialyzers, blacks had significantly lower hemodialysis doses than white or Hispanic patients (P < 0.001). The intradialytic weight losses were greater for blacks (P < 0.05). The delivered hemodialysis dose was lower for blacks than for whites or Hispanics whether measured as a urea reduction ratio (URR) or as the Kt/V calculated by the second generation formula of Daugirdas (median 1. 32, 1.36, and 1.37, respectively, P < 0.001). Hispanics and whites had modestly higher hematocritsthan blacks (33.2, 33.2, and 33.0%, respectively, P < 0.01). There was no significant difference among groups in the weekly prescribed epoetin alfa dose ( approximately 172 units/kg/week). A significantly greater proportion of Hispanic patients had transferrin saturations >/=20% compared with the other two groups (P < 0.001). Logistic regression modeling revealed that whites were significantly more likely to have serum albumin <3. 5(BCG)/3.2(BCP) gm/dL (OR 1.4, p < 0.01); blacks were significantly more likely to have a delivered Kt/V < 1.2 (OR 1.4, P < 0.001) and hematocrit <30%, (OR 1.2; P < 0.05) and both blacks and Hispanics were significantly more likely to have a delivered URR < 65% (OR 1.5, P < 0.001 and 1.2, P < 0.05, respectively).
<110>Unique Identifier 10512559Authors Kristal AR. Shattuck AL. Patterson RE.Institution Cancer Prevention Research Program, Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, Washington 98109-1024, USA. [email protected] Differences in fat-related dietary patterns between black, Hispanic and White women: results from the Women's Health Trial Feasibility Study in Minority Populations.Source Public Health Nutrition. 2(3):253-62, 1999 Sep.Abstract OBJECTIVE: This report examines how sources of fat and patterns of fat-related dietary habits differed between black, Hispanic and white women participating in a randomized trial of a low-fat diet intervention. DESIGN: The intervention consisted of group sessions, which met weekly for 6 weeks, biweekly for 6 weeks and monthly for 9 months, and included didactic nutrition education and activities to provide motivation for sustained dietary change. Outcomes included total fat and fat from nine food groups from a food frequency questionnaire (FFQ), and a summary scale and five subscales that measure fat-related dietary habits. SETTING/SUBJECTS: Data are from 1702 post-menopausal women, recruited from clinical centres in Atlanta, Birmingham and Miami, with dietary assessments at baseline and 6 months post-randomization. RESULTS: Total fat intake was similar across race/ethnic groups at baseline, yet there were many differences in sources of fat and fat-related dietary habits. For example, blacks consumed less fat from dairy foods and more fat from meats than whites. Effects of the intervention on total fat intake or the summary fat-related dietary habits scale did not differ across race/ethnicity groups. There were, however, many differences in how the intervention affected sources of fat and fat-related dietary habits. For example, the intervention effect for added fats (e.g. butter and salad dressings) was -8.9 g for blacks and -12.0 g for whites (P<0.05). The intervention effect for adopting low-fat meat purchasing
Page 53
401-600.txtand preparation methods was larger for blacks than whites, and the intervention effect for replacing high-fat foods with fruits and vegetables was larger for Hispanics than whites. CONCLUSIONS: This study demonstrates that, if properly designed, a single nutrition intervention programme can work well even in groups with culturally diverse dietary patterns.
<111>Unique Identifier 10512335Authors Juarez G. Ferrell B. Borneman T.Institution City of Hope National Medical Center, Department of Nursing Research and Education, Duarte, California 91010, USA.Title Cultural considerations in education for cancer pain management.Source Journal of Cancer Education. 14(3):168-73, 1999 Fall.Abstract BACKGROUND: Ethnicity is an important factor not only in the incidence of cancer but also in relation to symptom management. Inadequate pain management at home has been demonstrated to result in associated physical symptoms as well as great distress to patients and family. METHODS: The study purpose was to evaluate a structure program to educate patients about cancer pain management. The City of Hopequality-of-life (QOL) tool was used to measure patient outcomes in the QOL domains of physical, psychological, social, and spiritual well-being. The Patient Pain Questionnaire was used to assess knowledge and beliefs about pain. RESULTS: A total of 369 patients were enrolled in the study. The three largest groups, Caucasians, Hispanics, and African Americans, were compared. There were several significant differences between groups; overall; Hispanics had the worst pain and QOL outcomes. CONCLUSIONS: The findings demonstrate significant differences among the three ethnicgroups, which indicates a continued need for cultural considerations in patient education.
<112>Unique Identifier 10509692Authors Youn G. Knight BG. Jeong HS. Benton D.Institution Department of Psychology, Chonnam National University, Kwangju, South Korea.Title Differences in familism values and caregiving outcomes among Korean, Korean American, and White American dementia caregivers.Source Psychology & Aging. 14(3):355-64, 1999 Sep.Abstract Recent theories have suggested that burden and distress among dementia caregivers may be higher in American culture, which emphasizes individualism, and lower in cultures with higher levels of familism. However, immigrants may experience higher levels of burden because of acculturation with attendant values, conflicts and stresses. Forty-four Korean caregivers and 32 Korean American caregivers were compared with 54 White American caregivers on sociodemographic variables, familism, burden, anxiety, and depression. Familism was highest in Korean caregivers and lowest in Whites, with Korean Americans in the middle. Koreans and Korean Americans reported higher levels of burden. Koreans showed higher levels of depression and of anxiety than White American caregivers, with Koreans and Korean Americans higher than Whites on anxiety. These results suggest a need for greater specificity in theories about familism values, with attention to the specific meaning of familism in different cultures.
Page 54

401-600.txt
<113>Unique Identifier 10493473Authors Lorig K. Gonzalez VM. Ritter P.Institution Stanford University School of Medicine, CA, USA.Title Community-based Spanish language arthritis education program: a randomized trial.Source Medical Care. 37(9):957-63, 1999 Sep.Abstract OBJECTIVES: To determine 4-month and 1-year health-related outcomes of a 6-week, lay-led, and community-based arthritis self-management program for Spanish-speaking participants and to determine the role of self-efficacy in predicting health status for this population. METHODS: Three hundred and thirty one subjects were randomized to the program or to a 4-month wait list control group. One hundred ninety eight subjects continued in a 1-year longitudinal study. Data were collected via mailed questionnaires with telephone follow up. RESULTS: At 4 months, treatment subjects, compared with controls, demonstrated positive changes in exercise, disability, pain,and self-efficacy (P < 0.05). At 1 year, compared with baseline, treatment subjects demonstrated improvements in exercise, general health, disability, pain, self-efficacy, and depression (P < 0.05). Baseline and 4-month changes in self-efficacy predicted health status at 1 year. CONCLUSIONS: Spanish-speaking participants of an arthritis self-management program demonstrate short- and long-term benefits (improved health behaviors, health status, and self-efficacy).
<114>Unique Identifier 10483028Authors Thumboo J. Fong KY. Chan SP. Leong KH. Feng PH. Thio ST. Boey ML.Institution Department of Rheumatology and Immunology, Tan Tock Seng Hospital, Singapore, Singapore.Title Validation of the medical outcomes study family and marital functioning measures in SLE patients in Singapore.Source Lupus. 8(7):514-20, 1999.Abstract OBJECTIVE: To validate the Medical Outcomes Study Family and Marital Functioning Measures (FMM and MFM) in a multi-ethnic, urban Asian population in Singapore. METHODS: English speaking Chinese, Malay or Indian SLE patients (n=120) completed a self-administered questionnaire containing the FFM and MFM at baseline, after 2 weeks and after 6 months. Lupus activity, disease-related damage and quality of lifewere assessed using the British Isles Lupus Assessment Group (BILAG), Systemic LupusInternational Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index and SF-36 Health Survey respectively. Scale psychometric properties were assessed through factor analysis, Cronbach's alpha, quantifying test-retest differences and known-groups construct validity. RESULTS: Factor analysis of scores obtained at baseline and after 6 months identified 3 factors corresponding to the FFM (1 factor) and the MFM (2 factors). Both scales showed acceptable internal consistency, with Cronbach's alpha of 0.95 for the FFM and 0.70 for the MFM. Mean (s.d.) test-retest differences were -0.31 (3.82) points for the FFM and -0.70 (4.26)points for the MFM. Eleven out of 13 a priori hypotheses relating both the FFM and MFM to demographic, disease and quality of life variables were confirmed, supportingthe construct validity of these scales. CONCLUSION: The FFM and MFM are valid and reliable measures of family and marital functioning in a multi-ethnic cohort of Asian SLE patients in Singapore.
Page 55

401-600.txt
<115>Unique Identifier 10477481Authors Richardson LD.Institution Department of Emergency Medicine, Box 1149, Mount Sinai School of Medicine, New York, NY 10029, USA.Title Patients' rights and professional responsibilities: the moral case for cultural competence.Source Mount Sinai Journal of Medicine. 66(4):267-70, 1999 Sep.Abstract A right to health care can be derived from basic ethical principles. The empiricalevidence revealing significant racial inequities in health status, access to health services, quality of care received and outcomes of health services is reviewed. The need for health care providers to acquire cultural competence in order to fulfill their professional responsibilities is discussed; the insight, knowledge and discipline required to function effectively in the context of cultural differences are described. The broader implications of cultural competence for institutional andpublic policy, research and professional education are outlined.
<116>Unique Identifier 10476544Authors Dedier J. Penson R. Williams W. Lynch T Jr.Institution Kenneth B. Schwartz Center, Massachusetts General Hospital, Hematology-Oncology Department, Boston 02114-2617, USA.Title Race, ethnicity, and the patient-caregiver relationship.Source Oncologist. 4(4):325-31, 1999.Abstract Shortly before his death in 1995, Kenneth B. Schwartz, a cancer patient at Massachusetts General Hospital (MGH), founded The Kenneth B. Schwartz Center at MGH.The Schwartz Center is a non-profit organization dedicated to supporting and advancing compassionate health care delivery, which provides hope to the patient, gives support to caregivers, and encourages the healing process. The center sponsorsthe Schwartz Center Rounds, a monthly multidisciplinary forum where caregivers reflect on important psychosocial issues faced by patients, their families, and their caregivers, and gain insight and support from fellow staff members. Racial discrimination is a pervasive problem with multiple damaging effects. It is naive tobelieve that medicine is somehow immune to race-based practices, but there is a growing literature detailing poorer disease-specific outcomes in minority populations for a range of illnesses. A recent study in the New England Journal of Medicine has implicated physician prejudice as a significant contributing factor. The March 1999 Schwartz Center Rounds sought to explore the influence of ethnic biason the patient-provider interaction and the quality of health care delivery. Using adifferent format with a current affairs video clip and an interactive panel discussion, participants were encouraged to identify the often subconscious racial prejudices which may undermine their relationships with patients. Staff members werechallenged to think creatively about how institutions and individuals might promote "cultural competence" and a more equitable health care environment.
<117>Unique Identifier 10469816
Page 56

401-600.txtAuthors Hediger ML. Overpeck MD. McGlynn A. Kuczmarski RJ. Maurer KR. Davis WW.Institution Division of Epidemiology, Statistics and Prevention Research, National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland 20892-7510, USA.Title Growth and fatness at three to six years of age of children born small- or large-for-gestational age.Source Pediatrics. 104(3):e33, 1999 Sep.Abstract OBJECTIVE: To compare young children 3 to 6 years of age who were born small-for-gestational age (SGA; <10th percentile for gestational age) or large-for-gestational age (LGA; >/=90th percentile) with those who were born appropriate-for-gestational age (10th-89th percentile) to determine whether there are differences in growth and fatness in early childhood associated with birth weight status. DESIGN AND METHODS: National sample of 3192 US-born non-Hispanic white, non-Hispanic black, and Mexican-American children 3 to 6 years of age (36-83 months) examined in the third National Health and Nutrition Examination Survey and for whom birth certificates were obtained. On the birth certificates, length of gestation from the mother's last menstrual period was examined for completeness, validity, and whether the pattern of missing (n = 141) and invalid data (n = 147) ongestation was random. Gestation was considered invalid when >44 weeks, or when at gestations of </=35 weeks, birth weight was inconsistent with gestation. To reclaim cases with missing or invalid data on gestation for analysis, a multiple imputation (MI) procedure was used. MI procedures are recommended when, as in this case, a critical covariate (length of gestation) is not missing at random, and complete-subject analysis may be biased. Using the results of the MI procedure, children were categorized, and growth outcome was assessed by birth weight-for-gestational age status. The growth outcomes considered in these analyses were body weight (kg), height (cm), head circumference (cm), mid-upper arm circumference (MUAC; cm), and triceps and subscapular skinfold thicknesses (mm). Theanthropometric outcomes first were transformed to approximate normal distributions and converted into z scores (standard deviation units [SDU]) to scale the data for comparison across ages. Outcomes at each age then were estimated using regression procedures. SUDAAN software that adjusts variance estimates to account for the sample design was used in analysis for prevalence estimates and to calculate regression coefficients (in SDU). RESULTS: Over these ages, children born SGA remained significantly shorter and weighed less (-0.70 to -0.60 SDU). Children born LGA remained taller and weighed more (0.40-0.60 SDU). For weight and height among LGA children, there was a divergence from the mean with age compared with those bornappropriate-for-gestational age (10th-89th percentile). Head circumference and MUAC followed these same patterns. The coefficients for MUAC show values for SGA childrenfairly consistently at about -0.50 SDU and children born LGA show increasing MUAC from +0.40 to +0.50 SDU from 36 to 83 months of age. As with weight, there is a trend toward increased MUAC coefficients with age. Measures of fatness (triceps and subscapular skinfolds), which are more prone to environmental influences, showed less association with birth weight-for-gestational age status. Only a single age group, the oldest (6 years of age) group showed a significant deficit in fatness forchildren born SGA. For children born LGA, there was an increase in fatness at both the triceps and subscapular sites after 3 years of age. CONCLUSION: These findings on a national sample of US-born non-Hispanic white, non-Hispanic black, and Mexican-American children show that children born SGA remain significantly shorter and lighter throughout early childhood and do not seem to catch up from 36 to 83 months of age. LGA infants remain longer and heavier through 83 months of age, but unlike children born SGA, children born LGA may be prone to an increasing accumulation of fat in early childhood. Thus, early childhood may be a particularly sensitive period in which there is increase in variation in levels of fatness associated with size at birth. These findings have implications for the evaluation of the growth of young children. The results indicate that intrauterine growth is associated with size in early childhood. (ABSTR
Page 57

401-600.txt
<118>Unique Identifier 10452198Authors Webb Y. Clifford PI. Graham P.Institution British Psychological Society's Centre for Outcomes, Research and Effectiveness, University College London, UK. [email protected] A simple method of evaluating patients' perceptions of their treatment and care.Source Bulletin of the Menninger Clinic. 63(3):401-12, 1999 Summer.Abstract Surveys of patient satisfaction have become commonplace in mental health services.However, questions about the appropriateness of "satisfaction" as a concept and its use as an approach to evaluating the quality of service provision remain as pertinent as ever. Although surveys of patients of mental health services routinely generate high levels of apparent satisfaction, noncompliance with treatment and medication continues to be a major difficulty in psychiatric care. To evaluate services properly, there is a need to access patients' dissatisfaction to determine whether it is a more valid indicator of quality of services and a better predictor of noncompliance. However, a method that is not time consuming and costly is also required. The authors introduce a new patient evaluation tool, "Your Treatment and Care," which requires patients to report on their direct experience of care according to a set of principles of good practice. The tool forms part of a broader package for obtaining patients' views of their own problems, need for care, quality of care received, and health and social outcomes. The authors also report the results of a survey using this tool. Responses of 75 patients of a psychiatric hospital in the United States are presented and compared with results from a similarsurvey in the United Kingdom. The comparisons show striking differences in patients'perceptions of quality of treatment and care, both within each population and acrossclinical contexts.
<119>Unique Identifier 10431934Authors Rini CK. Dunkel-Schetter C. Wadhwa PD. Sandman CA.Institution Department of Psychology, University of California, Los Angeles 90095, USA. [email protected] Psychological adaptation and birth outcomes: the role of personal resources, stress, and sociocultural context in pregnancy.Source Health Psychology. 18(4):333-45, 1999 Jul.Abstract Prenatal psychosocial predictors of infant birth weight and length of gestation were investigated in a prospective study of 120 Hispanic and 110 White pregnant women. Hypotheses specifying that personal resources (mastery, self-esteem, optimism), prenatal stress (state and pregnancy anxiety), and sociocultural factors (income, education, ethnicity) would have different effects on birth outcomes were tested using structural equation modeling. Results confirmed that women with stronger resources had higher birth weight babies (beta = .21), whereas those reporting more stress had shorter gestations (beta = -.20). Resources were also associated with lower stress (beta = -.67), being married, being White, having higher income and education, and giving birth for the first time. There was no evidence that resources buffered the effects of stress. The importance of personal resources in pregnancy is highlighted along with implications for understanding the etiology of adverse birth outcomes.
Page 58

401-600.txt
<120>Unique Identifier 10417598Authors Morales LS. Cunningham WE. Brown JA. Liu H. Hays RD.Institution University of California Los Angeles, School of Medicine, Division of General Internal Medicine and Health Services Research 90095-1736, USA.Title Are Latinos less satisfied with communication by health care providers?.Source Journal of General Internal Medicine. 14(7):409-17, 1999 Jul.Abstract OBJECTIVE: To examine associations of patient ratings of communication by health care providers with patient language (English vs Spanish) and ethnicity (Latino vs white). METHODS: A random sample of patients receiving medical care from a physiciangroup association concentrated on the West Coast was studied. A total of 7,093 English and Spanish language questionnaires were returned for an overall response rate of 59%. Five questions asking patients to rate communication by their health care providers were examined in this study. All five questions were administered with a 7-point response scale. MAIN RESULTS: We estimated the associations of satisfaction ratings with language (English vs Spanish) and ethnicity (white vs Latino) using ordinal logistic models, controlling for age and gender. Latinos responding in Spanish (Latino/Spanish) were significantly more dissatisfied comparedwith Latinos responding in English (Latino/English) and non-Latino whites respondingin English (white) when asked about: (1) the medical staff listened to what they say(29% vs 17% vs 13% rated this "very poor," "poor," or "fair"; p <.01); (2) answers to their questions (27% vs 16% vs 12%; p <.01); (3) explanations about prescribed medications (22% vs 19% vs 14%; p <.01); (4) explanations about medical procedures and test results (36% vs 21% vs 17%; p <.01); and (5) reassurance and support from their doctors and the office staff (37% vs 23% vs 18%; p <.01). CONCLUSION: This study documents that Latino/Spanish respondents are significantly more dissatisfied with provider communication than Latino/English and white respondents. These resultssuggest Spanish-speaking Latinos may be at increased risk of lower quality of care and poor health outcomes. Efforts to improve the quality of communication with Spanish-speaking Latino patients in outpatient health care settings are needed.
<121>Unique Identifier 10419221Authors Longshore D. Grills C. Annon K.Institution Drug Abuse Research Center, Neuropsychiatric Institute, University of California, Los Angeles, USA.Title Effects of a culturally congruent intervention on cognitive factors related to drug-use recovery.Source Substance Use & Misuse. 34(9):1223-41, 1999 Jul.Abstract This paper describes a culturally congruent intervention to promote recovery from illegal drug use among African Americans and reports initial outcomes. The intervention was based on the transtheoretical stages-of-change model and on techniques of focused dyadic counseling and motivational interviewing. Subjects wererandomly assigned to the culturally congruent intervention or to a control condition. Each condition featured a single counseling session during which drug-related and other needs were assessed and appropriate referrals offered. Posttest data indicated that subjects in the culturally congruent condition were more involved in the counseling session, more willing to self-disclose, more motivated to seek help for drug-use-associated problems, and higher on preparation
Page 59

401-600.txtfor change.
<122>Unique Identifier 10538187Authors DuBray W. Sanders A.Title Interactions between American Indian ethnicity and health care.Source Journal of Health & Social Policy. 10(4):67-84, 1999.Abstract Interventions in health care must be sensitive to the part that culture plays in treatment, recovery and healing of the American Indian patient. Cultural factors play an important part in how the family participates and copes with the intervention program. Interpreting communication and behavior from the perspective of the family's culture contributes to positive family-professional interaction. This paper addresses the most important cultural factors impinging on positive health care for American Indian families and addresses a process for assessment of cultural conflicts which may prevent positive outcomes in the delivery of health care to this population. In addition, this paper offers strategies throughout that can be used by health care professionals to assure culturally sensitive service delivery to American Indians.
<123>Unique Identifier 10401807Authors Kalister H. Newman RD. Read L. Walters C. Hrachovec J. Graham EA.Institution School of Pharmacy, University of Washington, and the Harborview Medical Center, Seattle 98118, USA.Title Pharmacy-based evaluation and treatment of minor illnesses in a culturally diversepediatric clinic.Source Archives of Pediatrics & Adolescent Medicine. 153(7):731-5, 1999 Jul.Abstract BACKGROUND: Among medically underserved immigrant parents, access to nonprescription medicines for home treatment of minor childhood illnesses may be limited by scarce financial resources or language barriers. OBJECTIVES: To design and implement a new clinical service for an urban ambulatory pediatric clinic with alarge immigrant population that allows pharmacists to evaluate and to treat childrenand adolescents aged 6 months to 19 years with minor acute illnesses and to provide bilingual patient education materials. METHODS: We developed protocols and encounterforms for pharmacist evaluation of 5 pediatric conditions: cough/cold, fever, diaperrash, vomiting/diarrhea, and head lice. We published bilingual patient education materials for these conditions in 8 commonly spoken languages. We assessed safety bythoroughly reviewing the medical records of all patients who returned within 1 week of a pharmacy encounter and by asking parents in a telephone survey to compare services received through the pharmacy and the acute care clinic for treatment of the common cold. RESULTS: During the first year of this pilot program, 191 patients were evaluated and treated, 145 (76%) for cough/cold. Seventy percent of the patients were immigrants. No unexpected or adverse outcomes were detected, although occasional deviations from established protocols were noted. Parent satisfaction with the pharmacy service was high, and similar to that received through the standard acute care clinic. Patients evaluated by pharmacists were more likely to beattended to promptly (< 15-minute wait) and were more likely to receive written information than patients evaluated by physicians for similar conditions. CONCLUSIONS: Pharmacist evaluation and treatment of minor pediatric illnesses seems to be both safe and well accepted. Further studies are needed to evaluate the
Page 60

401-600.txtcost-effectiveness of this service in diverse settings. In states that allow pharmacists to have prescriptive authority, pharmacy-based evaluation and treatment may improve access to care for children with minor illnesses.
<124>Unique Identifier 10381976Authors Armengol CG.Institution Counseling Psychology, Rehabilitation and Special Education Northeastern University Boston, Massachusetts 02115, USA.Title A multimodal support group with Hispanic traumatic brain injury survivors.Source Journal of Head Trauma Rehabilitation. 14(3):233-46, 1999 Jun.Abstract OBJECTIVES: (a) To design and pilot a culturally sensitive and neuropsychologically informed support group addressing barriers to emotional, social, and vocational adjustment among high-level functioning Hispanic/Latino TBI survivors. (b) To determine efficacy through outcome measures. INTERVENTION: Ten-week multimodal, culturally sensitive support group focusing on TBI sequelae education, relaxation techniques, coping skills development, behavioral goal settingand monitoring, and family participation. PARTICIPANTS: Six Spanish-speaking high-level functioning TBI survivors aged 20-42. SETTING: Outpatient neuropsychological assessment and treatment center. OUTCOME MEASURES: Beck Hopelessness Scale; Purpose in Life Test; Perceived Self-Regulatory Ability Inventory. RESULTS: Participants' sense of personal destiny and feelings of hopelessness improved, as evidenced by objective measures and self-report. A telephone interview a year later indicated that gains had been maintained, and most participants were vocationally active. CONCLUSIONS: Results underscore the importance of considering linguistic and ethnic factors in developing support groups.
<125>Unique Identifier 10374809Authors Small R. Rice PL. Yelland J. Lumley J.Institution Centre for the Study of Mothers' and Childrens' Health, School of Public Health, La Trobe University, Carlton, Victoria, Australia.Title Mothers in a new country: the role of culture and communication in Vietnamese, Turkish and Filipino women's experiences of giving birth in Australia.Source Women & Health. 28(3):77-101, 1999.Abstract There are few population based studies which explore the views immigrant women have of the maternity care they receive in their new homelands. Three hundred and eighteen Vietnamese, Turkish and Filipino women who gave birth in three major city hospitals in Melbourne, Australia were interviewed about their experiences of maternity care. Outcomes and experiences for women with different levels of English fluency were studied, as were women's needs and preferences for assistance with interpreting. Observance of traditional cultural practices surrounding birth and theimpact of not being able to observe such practices on women's experiences of care were also explored. Women in the study not fluent in English experienced problems incommunicating with their caregivers and these were reflected in less positive experiences of care. Women were less concerned that caregivers knew little about their cultural practices than they were about care they experienced as unkind, rushed, and unsupportive. Maternity care for immigrant women is only likely to
Page 61

401-600.txtimprove when barriers to effective communication are addressed and attention is paidto raising standards of care.
<126>Unique Identifier 10370354Authors Eichenberger RK. Shandera WX.Institution Department of Medicine, Baylor College of Medicine, Houston, Tex., USA.Title The public health care of Central Americans in Houston.Source Texas Medicine. 95(6):55-62, 1999 Jun.Abstract In recent years, Americans have witnessed a marked change in the source of immigrant groups. Current immigrants are more likely to be former residents of the less developed world (nations such as Guatemala, Nigeria, India, and Viet Nam) than were earlier immigrants. In urban Texas, the influx of peoples from Central America is particularly striking and is largely a consequence of homeland political and economic instability. The new immigrants tend to be young and sexually active. We analyzed utilization patterns of Central Americans at our district health care facilities over 18 months and compared results with those of our non-Central American health care recipients. The 30,000 annual visits by Central Americans accounted for 4% of all visits. Disproportionately large amounts of care were given for sexually transmitted diseases and obstetric problems; conversely, small amounts were given for chronic illnesses, infectious diseases, acquired immunodeficiency syndrome, mental health problems, and adverse fetal outcomes. Few exotic tropical diseases were recognized or treated.
<127>Unique Identifier 10358525Authors Mak JM. Clinton M.Institution University of Hong Kong. [email protected] Promoting a good death: an agenda for outcomes research--a review of the literature. [Review] [55 refs]Source Nursing Ethics: an International Journal for Health Care Professionals. 6(2):97-106, 1999 Mar.Abstract Outcomes research is topical in discussions about health-related research. Its emphasis on effectiveness creates an important opportunity for nurse researchers to strengthen the linkages between theory, outcomes research and nursing practice but, before care can be more effective, it is logical to establish patients' desired outcomes. A thorough review of the implications of this requirement for the care of hospice patients is needed, but is lacking in the literature. Therefore, the literature on a 'good death' is reviewed as a step towards assisting hospice patients to achieve what they regard as an acceptable death. The starting point is to define more clearly what it means to die a good death. The relationship between hospice care and achieving a good death is then examined. [References: 55]
<128>Unique Identifier 10354227Authors McNeese-Smith DK.
Page 62

401-600.txtInstitution Nursing Administration Graduate Program, School of Nursing, University of California, Los Angeles, 90095-6917, USA. [email protected] A content analysis of staff nurse descriptions of job satisfaction and dissatisfaction.Source Journal of Advanced Nursing. 29(6):1332-41, 1999 Jun.Abstract Job satisfaction of nurses has been studied, using quantitative methodology, but hospital staff nurse descriptions of the source of their job satisfaction and job dissatisfaction have rarely been examined. This study collected information from 30 staff nurses through semistructured, taped interviews. Using content analysis, interviews were coded and categories and themes were identified. Findings indicate that job satisfaction was derived from the following categories: patient care, environment, balanced workload, relations with coworkers, personal factors, salary and benefits, professionalism, cultural background of the nurse and career stage of the nurse. Themes related to patient care, the pace and variety in an acute care environment, relationships with coworkers and meeting personal and family needs werecited as particularly relevant to job satisfaction. Job dissatisfaction was primarily influenced by patient care, factors that interfere with the job and patient care, feeling overloaded, relations with coworkers, personal factors, organizational factors and the career stage of the nurse. Themes related to the following categories have the greatest influence on job dissatisfaction: feeling overloaded, factors that interfere with patient care, coworkers who do not provide good care and situations that feel unfair. The actual words of nurses were included to provide depth and substance to the categories and themes. A discussion was presented of the relationship of these findings to theory and to outcomes of quantitative research. These findings have implications for nursing practice, administration and education as the profession considers organizational and individual factors influencing nurses' feelings about their job and prepares for future nursing shortages.
<129>Unique Identifier 10335065Authors Chen ZY.Institution Department of Sociology, Texas A&M University, College Station 77843-4351, USA. [email protected] Ethnic similarities and differences in the association of emotional autonomy and adolescent outcomes: comparing Euro-American and Asian-American adolescents.Source Psychological Reports. 84(2):501-16, 1999 Apr.Abstract This study has conducted an ethnic comparison on the strength of the association between Individuation, a subscale from the Emotional Autonomy construct presented originally by Steinberg and Silverberg in 1986, and adolescent outcomes in terms of self-esteem and susceptibility to negative peer pressure. Consistent with what was expected, the association between Individuation and lowered self-esteem was more salient among 287 Asian-American adolescent boys than among 1,353 Euro-American adolescent boys. Contrary to what was hypothesized, the association between Individuation and susceptibility to negative peer pressure was more pronounced among1,573 Euro-American adolescent girls than among 292 Asian-American adolescent girls.
<130>Unique Identifier 10333907Authors
Page 63

401-600.txt Lipton RB. Drum M. Li S. Choi H.Institution Division of Epidemiology and Biostatistics, University of Illinois at Chicago, School of Public Health 60612, USA. [email protected] Social environment and year of birth influence type 1 diabetes risk for African-American and Latino children.Source Diabetes Care. 22(1):78-85, 1999 Jan.Abstract OBJECTIVE: Credible epidemiological data, primarily from European-origin populations, indicate that environmental factors play an important role in the incidence of type 1 diabetes. RESEARCH DESIGN AND METHODS: A population-based registry of incident cases of type 1 diabetes among African-American and Latino children in Chicago was used to explore the influence of individual and neighborhoodcharacteristics on diabetes risk. New cases of insulin-treated diabetes in African-American and Latino Chicagoans aged 0-17 years for 1985-1990 (n = 400) were assigned to one of 77 community areas based on street address. Census tables provided denominators, median household income, percentage of adults > or = 25 yearsold who had completed high school and college, and a crowding variable for each community area individual-level data were birth cohort, sex, and ethnicity. Outcomesin Poisson regression were sex-, ethnic-, and birth cohort-specific incidence rates.RESULTS: Significant univariate associations between diabetes risk and ethnicity, birth cohort, crowding, and the percentage of adults in each community area who had completed high school and college were observed. African-Americans had a relative risk (RR) of 1.42 (95% CI, 1.14-1.76) compared with Latinos. Risk varied significantly by birth cohort in both ethnic groups. For every 10% increase in the proportion of adults who completed college, the RR for diabetes increased by 25% (RR, 1.25 [95% CI, 1.09-1.44]). Social class variables were significant determinantsof risk for African Americans, but not for Latinos. CONCLUSIONS: The strong birth cohort and social class associations observed in this study implicate an infectious exposure linked with age.
<131>Unique Identifier 10327938Authors Braam A. Beekman AT. Deeg DJ. Smit JH. Van Tilburg W.Title Religiosity as a protective factor in depressive disorder.[comment].Source American Journal of Psychiatry. 156(5):809; author reply 810, 1999 May.
<132>Unique Identifier 10321347Authors Caplan AL.Title Wearing your organ transplant on your sleeve.Source Hastings Center Report. 29(2):52, 1999 Mar-Apr.
<133>Unique Identifier 10319211Authors Jordan JM.Institution Thurston Arthritis Research Center, University of North Carolina at Chapel Hill
Page 64

401-600.txt27599-7330, USA.Title Effect of race and ethnicity on outcomes in arthritis and rheumatic conditions. [Review] [48 refs]Source Current Opinion in Rheumatology. 11(2):98-103, 1999 Mar.Abstract Examination of racial and ethnic differences in outcome from arthritis and rheumatic conditions can provide important clues to cause. This article reviews literature dealing with ethnic differences in the outcomes of disability, pain and pain coping, psychological adjustment and dysfunction, quality of life, and work disability. Future studies that acknowledge the interactive effects of ethnicity andsocioeconomic, biologic, and sociocultural influences and that include growing segments of the population, such as Hispanics and Asians, can advance understanding of mechanisms behind racial and ethnic differences. Although ethnic comparisons of outcome across different studies can be helpful, comparability is enhanced when racial or ethnic groups are examined within the context of the same study with identical ascertainment of disease, measurement of risk factors and outcomes, and analytic strategy. [References: 48]
<134>Unique Identifier 10231998Authors Walter P.Institution Baruch College, City University of New York, USA.Title The doctrine of informed consent: a tale of two cultures and two legal traditions.[Review] [53 refs]Source Issues in Law & Medicine. 14(4):357-73, 1999 Spring.Abstract In this article, the author compares and contrasts the notion of informed consent in medical decision making in the Western legal system with the traditional Jewish biblical legal system. Walter critically examines the philosophical underpinnings ofdisease and medical healing in both legal systems, and describes the practical consequences that emanate from the different ideologies in terms of the individual'srights of choice of treatment. She explains that the Western system is predicated onnotions of individual autonomy and self determination. Patients therefore have the autonomous ability to select and direct their own medical therapy. By contrast, the traditional biblical system of law is based on the concept that the body does not belong to the individual. Instead, the body is given to man by God as a trust to respect and preserve. Therefore, the individual patients "has no absolute right to control his body and ... he has no real decision making power as to medical treatment choices." In the Jewish biblical tradition, consent is not necessary for obviously beneficial or obviously non-beneficial procedures; consent is only necessary in decisions with uncertain outcomes or when making choices between equal options. Patients are encouraged to seek the counsel of religious authorities and toconform to rabbinical interpretations of the traditional Jewish law. [References: 53]
<135>Unique Identifier 10224199Authors Wallace JM Jr.Institution University of Michigan, School of Social Work, Department of Sociology, and Institute for Social Research, Ann Arbor, Michigan, USA. [email protected]
Page 65

401-600.txt The social ecology of addiction: race, risk, and resilience. [Review] [41 refs]Source Pediatrics. 103(5 Pt 2):1122-7, 1999 May.Abstract OBJECTIVE: The purposes of this article are to inform pediatricians and other health professionals of key contextual risk factors that elevate black and Hispanic Americans' likelihood to use substances and to discuss selected protective mechanisms that may shield members of these populations against substance use. METHOD: The article selectively reviews the literature on the epidemiology, etiology, and consequences of alcohol and other drug use among white, black, and Hispanic adults and youth. RESULTS: The extant research suggests that historical andcontemporary racialized practices and ideologies influence racial/ethnic differencesin substance use outcomes, both directly and indirectly, through their influence on the communities in which people of different racial/ethnic groups are placed, through their influence on the structure and process of people's interpersonal relationships, and through the impact that they have on individuals' psychology and behavior. CONCLUSIONS: Although the emphasis of pediatricians' and many other helping professionals' work focuses on individuals and individual-level behaviors, these behaviors can only be properly examined, diagnosed, and treated when they are understood in light of the community and societal contexts in which they occur. [References: 41]
<136>Unique Identifier 10220642Authors Alexander M. Grumbach K. Remy L. Rowell R. Massie BM.Institution Medical Effectiveness Research Center for Diverse Populations, University of California, San Francisco, CA, USA.Title Congestive heart failure hospitalizations and survival in California: patterns according to race/ethnicity.Source American Heart Journal. 137(5):919-27, 1999 May.Abstract BACKGROUND: Congestive heart failure (CHF) disproportionately affects African Americans, but data are limited concerning CHF hospitalization patterns among Hispanic and Asian populations, the 2 fastest growing ethnic groups in the United States, and race/ethnic patterns of rehospitalization and survival among patients with CHF are unknown. We conducted a study to assess rates of CHF hospitalization, readmission, and survival among diverse populations in California. METHODS AND RESULTS: We used 2 study designs. First, we calculated the population-based incidence of CHF hospitalization in California in 1991. Next we conducted a retrospective cohort study that identified patients initially hospitalized for CHF in 1991 or 1992 and followed these patients for 12 months after their index hospitalization to determine their likelihood of rehospitalization or death. Data were analyzed with Cox proportional hazards models. African Americans had the highest rate of CHF hospitalization. Age-adjusted hospitalization rates were comparable among whites, Latinos, and Asian women and all lower than those in African American, whereas Asian men had the lowest rates. On adjusted analyses, African Americans were more likely than whites and Asians to be rehospitalized (relative risk 1.07; 95% confidence interval 1.04 to 1.10). However, they were less likely to die within the 12-month follow-up period (relative risk 0.86; 95% confidence interval 0.82 to 0.90). Whites, conversely, had the highest posthospitalization mortality rates. CONCLUSIONS: These findings demonstrate important racial-ethnic differences in CHF morbidity and mortality rates. The disparate findings of higher hospitalization and rehospitalization rates and lower mortality rates among African Americans than whites may represent differences in theunderlying pathophysiology of CHF in these groups or differences in access to quality care. Further studies are needed to explain these seemingly paradoxical outcomes.
Page 66

401-600.txt
<137>Unique Identifier 10218259Authors Winsler A. Diaz RM. Espinosa L. Rodriguez JL.Institution Department of Psychology, George Mason University, Fairfax, VA 22030-4444, USA. [email protected] When learning a second language does not mean losing the first: bilingual languagedevelopment in low-income, Spanish-speaking children attending bilingual preschool.Source Child Development. 70(2):349-62, 1999 Mar-Apr.Abstract This article discusses two investigations which explored the bilingual language development outcomes of comparable groups of low-income, Spanish-speaking, Mexican American children who either did or did not attended a bilingual (Spanish/English) preschool. Study 1 is a replication of a study by Rodriguez, Diaz, Duran, and Espinosa, involving a new sample of 26 children who attended bilingual preschool forone year and 20 control children who remained at home. Study 2 represents a 1-year, longitudinal follow-up of Rodriguez et al.'s, sample of children during and after the children spent another year at home or in the preschool. In both investigations,standardized, objective measures of three components of children's language proficiency (productive language, receptive language, and language complexity) in English and Spanish were obtained at the beginning and end of the academic year. Contrary to fears that have been expressed by some that early exposure to English would lead to children's native language loss, the results of both studies offered no evidence of Spanish proficiency loss for children attending bilingual preschool. Children who attended bilingual preschool, compared to those who remained at home, showed significant and parallel gains in Spanish language development as well as significant and greater increases in English language proficiency over time. Resultsare discussed in terms of the need for more systematic research to be conducted in this area to inform policy and practice in the early education and development of language-minority children.
<138>Unique Identifier 10202690Authors Shapiro J. Douglas K. de la Rocha O. Radecki S. Vu C. Dinh T.Institution Department of Family Medicine, University of California, Irvine, USA.Title Generational differences in psychosocial adaptation and predictors of psychological distress in a population of recent Vietnamese immigrants.Source Journal of Community Health. 24(2):95-113, 1999 Apr.Abstract While first-wave Vietnamese immigrants adapted well to life in the United States, subsequent immigrants have had greater adjustment difficulties, including more evidence of psychological distress. This study aimed to analyze psychosocial adaptation differences among three generations of recent Vietnamese immigrants, as well as to examine predictors of mental distress in the sample as a whole. A community sample of 184 recent Vietnamese immigrants, categorized as either elderly,middle-aged, or young adults, was assessed for levels of psychological distress, including depression, anxiety, and PTSD, as well as family conflict, dissatisfactionwith life in the U.S., acculturation and biculturalism, social support, coping, and premigratory stressors. Young Vietnamese adults were most acculturated, most bicultural, and reported themselves as healthiest and least depressed. They were most often working, least often on welfare, and had the highest family income.
Page 67

401-600.txtHowever, they also reported most dissatisfaction with their current lives in the U.S. and most family conflict. Regression analysis explaining approximately one-quarter of the variance in mental distress implicated current dissatisfaction with and lack of adjustment of life in the United States, as well as greater acculturation and increased family conflict. Although young adults scored significantly higher than other generations on most of the risk factors for psychological distress, they appeared to be buffered against poorer mental health outcomes by factors of generation and perceived positive overall well-being. In terms of testing a predictive model of psychological distress, this study found current adjustment factors significantly more important in determining mental healthoutcomes than premigratory stressors such as war-related traumas.
<139>Unique Identifier 10101613Authors Mulvaney FD. Brown LS Jr. Alterman AI. Sage RE. Cnaan A. Cacciola J. Rutherford M.Institution Center for Studies of Addiction, University of Pennsylvania School of Medicine, Philadelphia 19104, USA.Title Methadone-maintenance outcomes for Hispanic and African-American men and women.Source Drug & Alcohol Dependence. 54(1):11-8, 1999 Mar 1.Abstract Six-month methadone-maintenance response and outcome were examined for African-American and Hispanic men and women in a large urban sample. A consistent pattern of improvement was indicated for both races and genders on the addiction severity index (ASI). There were virtually no statistically significant differences in ASI outcomes between Hispanics and African-Americans and men and women using conventional analysis of variance (ANOVA) procedures. Results from an additional equivalence analysis, however, indicated that baseline to 6-month changes for the different groups were generally not similar enough to consider them equivalent. Urine toxicologies obtained during the 6-month treatment period were also not statistically equivalent by race and gender. Evaluating outcomes by gender and race are discussed, as are the implications of using equivalence tests when examining group differences.
<140>Unique Identifier 10081209Authors Rehm RS.Institution University of New Mexico, Health Sciences Center, Alberquerque 87131-1061, USA. [email protected] Religious faith in Mexican-American families dealing with chronic childhood illness.Source Image - the Journal of Nursing Scholarship. 31(1):33-8, 1999.Abstract PURPOSE: To explore Mexican-American family experiences with chronic childhood illness, from the perspective of parents, and report findings about the influence ofreligious faith on families' spiritual and secular responses to illness. Mexican-Americans are often characterized as religious, fatalistic, and passive, butfamilies' perceptions of the consequences of their daily faith and its meaning in the face of chronic childhood illness is not well understood. DESIGN: Descriptive. The sample included 25 parents from 19 families living with children with a variety of chronic conditions. Data were collected in 1995-1996. METHODS: Interpretive,
Page 68

401-600.txtusing symbolic interaction as the framework, and in-depth interviewing for data collection. FINDINGS: Parents professed a variety of beliefs and devotional practices. Six unifying dimensions of religious faith were related to parental caretaking and decision making for the family: (a) God determined the outcome of thechild's illness, (b) God and health care for the child were closely linked, (c) parents took an active role in facilitating God's will, (d) families had obligationsto God, (e) intercession with God by others was often sought by or offered to the family, and (f) faith encouraged optimism. CONCLUSIONS: Families were not fatalisticin the sense of feeling outcomes were predetermined and unalterable. Family members took spiritual and secular actions to assure the best possible familial and professional care for their child and sought to influence God's good will on behalf of the child and family.
<141>Unique Identifier 10063394Authors Mendoza FS. Fuentes-Afflick E.Institution Department of Pediatrics, Stanford University School of Medicine, Palo Alto, CA 94304, USA.Title Latino children's health and the family-community health promotion model.Source Western Journal of Medicine. 170(2):85-92, 1999 Feb.Abstract A majority of Latino children in the US live in poverty. However, unlike other poor children, Latino children do not seem to have a consistent association between poverty and poor health. Instead, many poor Latino children have unexpectedly good health outcomes. This has been labeled an epidemiologic paradox. This paper proposesa new model of health, the family-community health promotion model, to account for this paradox. The family-community health promotion model emphasizes the family-community milieu of the child, in contrast to traditional models of health. In addition, the family-community model expands the outcome measures from physical health to functional health status, and underscores the contribution of cultural factors to functional health outcomes. In this paper, we applied the family-community health promotion model to four health outcomes: low birthweight, infant mortality, chronic and acute illness, and perceived health status. The implications of this model for research and policy are discussed.
<142>Unique Identifier 10063393Authors Lara M. Morgenstern H. Duan N. Brook RH.Institution UCLA/RAND Program on Latino Children with Asthma, UCLA Department of Pediatrics, USA. [email protected] Elevated asthma morbidity in Puerto Rican children: a review of possible risk and prognostic factors.[see comment]. [Review] [63 refs]Source Western Journal of Medicine. 170(2):75-84, 1999 Feb.Abstract Latino children represent a significant proportion of all US children, and asthma is the most common chronic illness affecting them. Previous research has revealed surprising differences in health among Latino children with asthma of varying countries of family origin. For instance, Puerto Rican children have a higher prevalence of asthma than Mexican American or Cuban American children. In addition, there are important differences in family structure and socioeconomic status among these Latino populations: Cuban Americans have higher levels of education and family
Page 69

401-600.txtincome than Mexican-Americans and Puerto Ricans; mainland Puerto Rican children havethe highest proportion of households led by a single mother. Our review of past research documents differences in asthma outcomes among Latino children and identifies the possible genetic, environmental, and health care factors associated with these differences. Based on this review, we propose research studies designed to differentiate between mutable and immutable risk and prognostic factors. We also propose that the sociocultural milieus of Latino subgroups of different ethnic and geographic origin are associated with varying patterns of risk factors that in turn lead to different morbidity patterns. Our analysis provides a blue-print for future research, policy development, and the evaluation of multifactorial interventions involving the collaboration of multiple social sectors, such as health care, public health, education, and public and private agencies. [References: 63]
<143>Unique Identifier 9990439Authors Brooks D. Barth RP.Institution School of Social Welfare, University of California, Berkeley, USA.Title Adult transracial and inracial adoptees: effects of race, gender, adoptive family structure, and placement history on adjustment outcomes.Source American Journal of Orthopsychiatry. 69(1):87-99, 1999 Jan.Abstract Adjustment outcomes of 224 transracial and inracial adoptees were investigated using data collected over 17 years. Findings reveal an association between adoptees'outcomes and their race, gender, and adoptive family structure. Placement history was not significant. Implications for policy and practice are discussed, as are future directions for research.
<144>Unique Identifier 9988244Authors Fuentes-Afflick E. Hessol NA. Perez-Stable EJ.Institution Department of Pediatrics, Medical Effectiveness Research Center for Diverse Populations, Institute for Health Policy Studies, University of California, San Francisco 94110, USA. [email protected] Testing the epidemiologic paradox of low birth weight in Latinos.Source Archives of Pediatrics & Adolescent Medicine. 153(2):147-53, 1999 Feb.Abstract BACKGROUND: Rates of low-birth-weight (LBW) infants are similar between Latina andwhite women, an epidemiologic paradox. However, few studies have analyzed the relationship between ethnicity, Latino subgroup, confounding variables, and LBW. METHODS: We analyzed 395070 singleton livebirths to Latina and non-Latina white women in California during 1992. Multivariate logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the risks due to Latino ethnicity and Latino subgroup for very LBW (VLBW, 500-1499 g) and moderately LBW (MLBW, 1500-2499 g) outcomes. RESULTS: Latina and white women had similar unadjusted rates of VLBW (0.7% vs. 0.6%) and MLBW infants (3.7% vs. 3.4%). After adjusting for maternal age, education, birthplace, marital status, parity, tobacco use, use of prenatal care, infant sex, and gestational age, there was no difference in the odds of VLBW infants between Latina and white women (OR, 0.93 [95% CI, 0.81-1.071). Latina women had minimally elevated odds of MLBW infants (OR, 1.06 [95%CI, 1.01-1.11]) compared with white women. By Latino subgroup, there was no difference in the adjusted odds of VLBW infants among Central and South American,
Page 70

401-600.txtCuban, Mexican, Puerto Rican, and white women. The adjusted odds of MLBW infants were elevated among Central and South American (OR, 1.14 [95% CI, 1.05-1.25]) and Puerto Rican women (OR, 1.41 [95% CI, 1.12-1.78]), relative to white women. CONCLUSIONS: The epidemiologic paradox of LBW in Latinos is valid. New conceptual models are needed to identify Latina women who are at risk for adverse pregnancy outcomes.
<145>Unique Identifier 9926677Authors Ratliff SS.Institution Department of Human Resources, Children's Hospital, Columbus, OH, USA.Title Waterfalls and geysers: the development of diversity awareness at Children's Hospital.Source Journal of Nursing Care Quality. 13(3):36-46, 1999 Feb.Abstract The development of diversity awareness at Children's Hospital in Columbus, Ohio, has been a work in progress since the early 1980s. The interface of administration and individual initiatives ("waterfalls" and "geysers") has resulted in projects ranging from major international exchange programs to noontime Spanish language classes. This article recounts the journey from a parochial focus to a consciousnessof multiculturalism in virtually all aspects of hospital interaction.
<146>Unique Identifier 9893314Authors Mehl-Madrona LE.Institution Center for Complementary Medicine, University of Pittsburgh Medical Center, USA.Title Native American medicine in the treatment of chronic illness: developing an integrated program and evaluating its effectiveness.Source Alternative Therapies in Health & Medicine. 5(1):36-44, 1999 Jan.Abstract Traditional Native American healing practices are increasingly sought after by Native Americans as well as non-Natives. A series of meetings between traditional Native American healers and the author resulted in dialogues on the Native American worldview and biomedicine. Recommendations arose for how Native American treatment should proceed in the modern world and how to effectively introduce interested non-Natives to Native American healing practices. An approach for bridging cultures to facilitate the interaction of non-Natives with traditional healers was developed.A total of 116 patients were treated by the author in conjunction with traditional Native American healers. More than 80% of patients showed significant, persistent benefits from a time-intensive treatment program. A comparison group consisting of patients from the author's emergency room practice had significantly lower rates of improvement. An intensive program inspired by Native American practices lasting 7 to10 days can achieve both health benefits and improved cost-effectiveness in the treatment of chronic physical illness. The treatment philosophy underlying this approach is best described as a dynamic energy system. Within this theoretical framework, physical illness, which is viewed as simultaneously spiritual, mental, and physical, can be treated by counseling and ceremony. Due to the interaction and hierarchical nature of these levels, intervention at any one level affects the others.
Page 71
401-600.txt<147>Unique Identifier 9890362Authors O'Donnell L. Stueve A. San Doval A. Duran R. Atnafou R. Haber D. Johnson N. Murray H. Grant U. Juhn G. Tang J. Bass J. Piessens P.Institution Education Development Center, Inc., Newton, Massachusetts 02160, USA.Title Violence prevention and young adolescents' participation in community youth service.Source Journal of Adolescent Health. 24(1):28-37, 1999 Jan.Abstract PURPOSE: To examine whether participation in a school-sponsored community youth service program reduces self-reported violent behaviors among young urban adolescents. METHODS: A total of 972 seventh- and eighth-grade students at two large, urban, public middle schools were surveyed at baseline and at 6-month follow-up. One school was assigned to interventions and the other served as a control. All students at the intervention school received the Reach for Health classroom curriculum that included a 10-lesson unit focusing on violence prevention.In addition, approximately half the students were randomly assigned by classroom to participate in the Reach for Health Community Youth Service program (CYS). Under theguidance of teachers and community nurses, these students spent several hours each week providing service in local health care agencies. Regression analyses were used to assess the influence of treatment condition on violent behavior outcomes. RESULTS: Comparing students in the curriculum-only and curriculum-plus-CYS interventions to the control group, there is a statistically significant interaction(p < .03) among grade, CYS participation, and violence at follow-up. Eighth-grade CYS students reported significantly less violence at follow-up than students in the control school, taking into account baseline level of risk behavior, gender, ethnicity, and social desirability (p < .04). There was no significant difference between controls and students in the curriculum-only condition. Comparing students in the CYS intervention to the curriculum-only condition within the intervention school, the grade by intervention interaction again is significant (p < .05). Eighth-grade CYS students-who received the broadest CYS experience-reported less violence at follow-up than their curriculum-only counterparts. CONCLUSION: When delivered with sufficient intensity, school programs which couple community service with classroom health instruction can have a measurable impact on violent behaviors of a population of young adolescents at high risk for being both the perpetrators and victims of peer violence. Community service programs may be an effective supplement to curricular interventions and a valuable part of multicomponent violence prevention programs.
<148>Unique Identifier 12769095Authors Chin JL.Institution CEO Services, USA.Title Cultural competence and health care in Massachusetts: where are we? Where should we be?.Source Issue Brief (Massachusetts Health Policy Forum). (5):1-20, 1999 Jul 15.
<149>Unique Identifier 11951233Authors
Page 72

401-600.txt Beutter MB. Davidhizar R.Institution Home Health of Ancilla Health Care, Mishawaka, Indiana, USA.Title "A home care provider's challenge--caring for the hispanic client in the home". [Review] [38 refs]Source Journal of Practical Nursing. 49(3):26-33; quiz 34-7, 1999 Sep.Abstract It is important for home health care providers to keep in mind that clients from different cultures should be assessed and may vary according to 1) communication, 2)space, 3) time, 4) social organization, 5) environmental control, and 6) biological variations. Some variations, which have been evident by some Hispanic Americans havebeen discussed in this article. Careful assessment of the client and being aware of issues that differ between and within persons of a cultural group can enable the provider to provide culturally appropriate care. This will increase the likelihood of successful outcomes to health care interventions and optimal health for the client. [References: 38]
<150>Unique Identifier 11645874Authors Good MJ. Mwaikambo E. Amayo E. Machoki JM.Title Clinical realities and moral dilemmas: contrasting perspectives from academic medicine in Kenya, Tanzania, and America.Source Daedalus. 128(4):167-96, 1999 Fall.
<151>Unique Identifier 11081004Authors Escalante A. Cardiel MH. del Rincon I. Suarez-Mendoza AA.Institution Division of Clinical Immunology and Rheumatology, University of Texas Health Science Center at San Antonio 78284, USA.Title Cross-cultural equivalence of a brief helplessness scale for Spanish-speaking rheumatology patients in the United States.Source Arthritis Care & Research. 12(5):341-50, 1999 Oct.Abstract OBJECTIVE: To show evidence of the cross-cultural equivalence between the originalEnglish version of a 5-item scale for measuring helplessness and a translated Spanish version. METHODS: English and Spanish versions of the 5 items that constitute the helplessness factor of the Rheumatology Attitudes Index were tested in 3 separate groups of patients: 1) 20 bilingual rheumatology patients; 2) 100 consecutive English- and 50 consecutive Spanish-speaking monolingual rheumatology patients; and 3) 192 English- and 44 Spanish-speaking patients with rheumatoid arthritis who were consecutively enrolled in a cohort to study disease outcomes. English-Spanish concordance among bilingual subjects was measured using intraclass correlation coefficients (ICC). Internal consistency was measured by Cronbach's coefficient alpha. Associations between the helplessness scale and variables measured simultaneously in English- and Spanish-speaking patients were measured by correlation analysis. RESULTS: Agreement between the English and Spanish versions ofthe helplessness scale among bilingual subjects was excellent (ICC = 0.87), and internal consistency among monolingual subjects was acceptable (coefficient alpha = 0.73 in English and 0.87 in Spanish). The correlation between helplessness and most other measured variables was of similar size and direction in English as in Spanish
Page 73

401-600.txt(10-point pain scale r = -0.53 and -0.52; modified Health Assessment Questionnaire physical disability r = -0.45 and -0.43; self-assessed joint count r = 0.36 and 0.36; Medical Outcomes Study Short Form 36 [SF-36] physical function r = 0.37 and 0.39; SF-36 mental health r = 0.27 and 0.35; Center for Epidemiological Studies Depression scale r = -0.37 and -0.33, respectively). CONCLUSION: The evidence shown supports the cross-cultural equivalence between the original 5-item helplessness scale developed in English and our translated Spanish version.
<152>Unique Identifier 10981110Authors Betancourt JR. Carrillo JE. Green AR.Institution The New York Presbyterian Hospital, The Weill Medical College of Cornell University, Cornell Internal Medical Associates, 505 East 70th Street, HT-4, New York, NY 10021, USA.Title Hypertension in multicultural and minority populations: linking communication to compliance.Source Current Hypertension Reports. 1(6):482-8, 1999 Dec.Abstract Cardiovascular disease disproportionately affects minority populations, in part because of multiple sociocultural factors that directly affect compliance with antihypertensive medication regimens. Compliance is a complex health behavior determined by a variety of socioeconomic, individual, familial, and cultural factors. In general, provider-patient communication has been shown to be linked to patient satisfaction, compliance, and health outcomes. In multicultural and minoritypopulations, the issue of communication may play an even larger role because of linguistic and contextual barriers that preclude effective provider-patient communication. These factors may further limit compliance. The ESFT Model for Communication and Compliance is an individual, patient-based communication tool thatallows for screening for barriers to compliance and illustrates strategies for interventions that might improve outcomes for all hypertensive patients.
<153>Unique Identifier 10892418Authors Cervantes A. Keith L. Wyshak G.Institution Centro de Investigacion y docencia Economicas, A.C., Division de Economia, Lomas de Santa Fe, Mexico, D.F. [email protected] Adverse birth outcomes among native-born and immigrant women: replicating nationalevidence regarding Mexicans at the local level.Source Maternal & Child Health Journal. 3(2):99-109, 1999 Jun.Abstract OBJECTIVES: For almost two decades, the literature has consistently described an epidemiologic paradox relating to better birth outcomes among high-risk groups, particularly new immigrants from Mexico and Southeast Asia. We hypothesize that regardless of their sociodemographic profile, Mexican immigrants will exhibit lower rates of low birth weight and preterm deliveries than native-(U.S.) born women of Mexican origin, non-Hispanic White and Black women, and Puerto Rican Women. METHODS:We studied 57,324 live-born singleton infants born to residents in the city of Chicago in a linked data set of 1994 birth-death records. Multivariate logistic regression was used to analyze race/ethnicity differentials in two pregnancy outcomemeasures, low birth weight and preterm birth. RESULTS: Overall better birth outcome is related to maternal immigrant status regardless of race/ethnic groups. Immigrant
Page 74

401-600.txtMexican women had a significantly lower risk of both low birth weight [adjusted oddsratio (AOR): 0.78, 95% confidence interval (CI) 0.66-0.91] and preterm births (AOR: 0.75, 95% CI 0.65-0.86) and were at 28% and 33% lower risks of delivering a low birth weight infant or a premature infant, respectively, than non-Hispanic White women.
<154>Unique Identifier 10887459Authors Crump C. Lipsky S. Mueller BA.Institution University of Washington, School of Public Health and Community Medicine, Department of Epidemiology, Seattle, USA.Title Adverse birth outcomes among Mexican-Americans: are US-born women at greater risk than Mexico-born women?.Source Ethnicity & Health. 4(1-2):29-34, 1999 Feb-May.Abstract OBJECTIVE: We examined adverse birth outcomes among Mexican-Americans to determinethe effect of country of maternal birth, a measure of acculturation. DESIGN: We conducted a retrospective cohort analysis of birth outcomes among 4800 Mexico-born and 4800 US-born Mexican-American women using Washington State birth certificate data from 1989 to 1994. Length of residence at current address was used to help refine our measure of acculturation. RESULTS: US-born women had a slightly increasedrisk of preterm birth relative to Mexico-born women [relative risk (RR) 1.18, 95% confidence interval (CI) 1.04-1.33]. Among Mexico-born women, the risk of preterm birth increased with greater duration of current residence. CONCLUSIONS: US-born Mexican-American women had a slightly increased risk of preterm birth despite havingmore adequate prenatal care, more education, and higher socioeconomic indicators. This may be due to acculturation factors, such as earlier pregnancy, loss of social support systems, and increased smoking or alcohol use. Reducing this risk depends onrecognition among health care workers and policy-makers of the potential influence of acculturation on health in this population.
<155>Unique Identifier 10842504Authors De Wit ML. Embree BG. De Wit D.Institution Ontario Ministry of Community and Social Services, Toronto, Canada.Title Determinants of the risk and timing of alcohol and illicit drug use onset among natives and non-natives: similarities and differences in family attachment processes.Source Social Biology. 46(1-2):100-21, 1999 Spring-Summer.Abstract This study examines data from Native Ontario reserve residents (Embree, 1993) and a sample from the Ontario Health Survey Supplement (1990-91) in order to compare andcontrast the importance of family attributes such as parent-child attachment to Native and Non-native patterns of drug and alcohol use onset. Proportional Hazards modeling (Cox, 1972) was employed to identify factors associated with the risk and timing of onset of alcohol and illicit drugs for both cultural groups. For both Natives and Non-natives alike, and considering both drinking and drug use onset together, age cohort predominates as a risk factor, with youngest groups at greatestrisk, and especially in the case of drug use other than alcohol. For the model of drug use timing, age of alcohol use onset is the second best predictor for Natives, although its effect is still apparent, albeit weaker, in the case of Non-natives. As
Page 75

401-600.txtfor family characteristics, a number of factors emerge as determinants of risk and depend, in part, on the cultural group and the substance under consideration. Consistent with attachment theory's prediction about the universal applicability of the need for close parent-child relations (Bowlby, 1969), the findings for both Natives and Non-natives alike point to the salience of psychosocial attachment and other indicators of family functioning in affecting early onset drinking and drug use, behaviors well-recognized to lead to potentially adverse mental and physical health consequences as well as to negative social outcomes.
<156>Unique Identifier 10791358Authors Guendelman S. Buekens P. Blondel B. Kaminski M. Notzon FC. Masuy-Stroobant G.Institution Division of Health Policy and Management, School of Public Health, University of California, Berkeley 94720-7360, USA. [email protected] Birth outcomes of immigrant women in the United States, France, and Belgium.Source Maternal & Child Health Journal. 3(4):177-87, 1999 Dec.Abstract OBJECTIVES: To compare maternal characteristics and birth outcomes of Mexico-born and native-born mothers in the United States and those of North African mothers living in France and Belgium to French and Belgian nationals. METHODS: We examined information from single live birth certificates for 285,371 Mexico-born and 3,131,632 U.S.-born mothers (including 2,537,264 U.S.-born White mothers) in the United States, 4,623 North African and 103,345 Belgian mothers in Belgium, and a French national random sample consisting of 632 North African and 11,185 French mothers. The outcomes were mean birthweight, low birthweight, and preterm births. Differences between native/nationals and foreign-born mothers in each country were assessed in bivariate and multivariate analyses controlling for maternal risk factors. RESULTS: The adjusted odds for low birthweight were lower for immigrants than native/nationals by 32% in the United States, by 32% in Belgium, and by 30% in France. The adjusted odds for preterm births were lower for immigrants compared withnative/nationals by 11% in the United States and by 23% in Belgium. In France, the odds for preterm births were comparable for immigrants and naturalized mothers. Infants of immigrant mothers also had higher mean birthweights in all three countries. CONCLUSION: Despite their disadvantaged status, Mexico-born and North African-born women residing in the United States, France, and Belgium show good birth outcomes. These cannot be explained solely by traditional risk factors. Protective factors and selective migration may offer further clues.
<157>Unique Identifier 10732596Authors Clark C. Robinson TM.Institution Urban Education Leadership Doctoral Program, University of Cincinnati, Ohio, USA.Title Cultural diversity and transcultural nursing as they impact health care. [Review] [20 refs]Source Journal of National Black Nurses Association. 10(2):46-53, 1999 Fall-Winter.Abstract This article examines and critiques what can be broadly defined as "culturally sensitive nursing practice." The authors argue that both past and present research on culturally sensitive nursing practice, regardless of which branch of such practice it subscribes to (transcultural, cross-cultural, multicultural, intercultural, international, and so forth), is not sufficiently based in a
Page 76

401-600.txtsociopolitical context. As a result, there is not significant positive improvement in health care outcomes for patients from traditionally under-represented social membership groups (i.e., groups based on race, gender, socioeconomic class, etc.). Realizing sincere and affective culturally sensitive nursing practice is contingent upon the development and implementation of a comprehensive, sociopolitically conceptualized multicultural nursing education curriculum and pedagogy. [References:20]
<158>Unique Identifier 10693425Authors Flaskerud JH. Anderson N.Institution UCLA School of Nursing, USA.Title Disseminating the results of participant-focused research.Source Journal of Transcultural Nursing. 10(4):340-9, 1999 Oct.Abstract Participant-focused research (PFR) includes the "subjects" as full partners in theresearch process. As such, participants share in the products or outcomes of research. PFR goes beyond the traditional research approach of disseminating findings to other scientists and clinicians and includes participants and community residents in sharing the skills, knowledge, and resources of the study with the objective of empowering the participants. This article demonstrates the use of PFR in disseminating the results or products of study to the participants through two examples of long-term research projects conducted in Los Angeles. The first example is a community-based study of HIV prevention with low-income Latina women. The second example is an ethnographic study of health concerns and risks among adolescents in juvenile detention. These examples provide two approaches to dissemination of research findings and benefits to the participants and the community.
<159>Unique Identifier 10689990Authors Friedman AW. Alarcon GS. McGwin G Jr. Straaton KV. Roseman J. Goel N. Reveille JD.Institution Department of Medicine, University of Texas-Houston Medical School 77225, USA.Title Systemic lupus erythematosus in three ethnic groups. IV. Factors associated with self-reported functional outcome in a large cohort study. LUMINA Study Group. Lupus in Minority Populations, Nature versus Nurture.Source Arthritis Care & Research. 12(4):256-66, 1999 Aug.Abstract OBJECTIVE: To identify features of systemic lupus erythematosus (SLE) associated with poor functional outcome as measured by the 36-item Medical Outcomes Study ShortForm 36 Health Survey (SF-36). METHODS: Two hundred twenty-four patients with early SLE (70 Hispanic, 83 African American, and 71 white) enrolled in a longitudinal study of outcomes were evaluated at study entry. The 8 composite scales and 2 summary measures (physical and mental) of the SF-36 were the dependent variables. Independent variables--1) sociodemographic, 2) clinical features, 3) immunologic, 4)global scores, and 5) behavioral/cultural--were examined for each of the scales and summary measures and for each ethnic group. Significant variables in these analyses were then used to construct models to determine their association with each of the scales and the 2 summary measures for the entire population and the 3 ethnic groups.RESULTS: Self-reported physical and mental functioning were most consistently
Page 77

401-600.txtassociated with abnormal illness-related behaviors, helplessness, fatigue, and pain at study entry. Helplessness was more strongly associated with functioning in the Hispanics than in the African American or white patients. Pain was strongly associated with physical but not mental health. The models were quite robust, accounting for 41% to 68% of the variance for the two summary measures. CONCLUSION: Patients' attitudes toward their disease, fatigue, and pain have greater impact on self-perceived functional levels, as measured by the SF-36, than do more objective measures of disease activity and damage such as the presence of specific autoantibodies and/or the occurrence of specific organ involvement. Interventions designed to improve outcome may need to include ethnic-specific as well as general strategies.
<160>Unique Identifier 10681898Authors Winkleby MA. Cubbin C. Ahn DK. Kraemer HC.Institution Stanford Center for Research in Disease Prevention, Stanford University School of Medicine, Palo Alto, California 94304-1825, USA. [email protected] Pathways by which SES and ethnicity influence cardiovascular disease risk factors.Source Annals of the New York Academy of Sciences. 896:191-209, 1999.Abstract Little is known about pathways by which socioeconomic status (SES) translates intoindividual differences in cardiovascular disease (CVD) risk factors. Because the socioeconomic structure is not the same for all ethnic subgroups, the pathways that lead to the development of CVD risk factors may vary by both SES and ethnicity. We used data from a large national survey to examine the independent associations of two indicators of SES (education and income) and ethnicity with six primary CVD riskfactors. We then used data on smoking that reflected a temporal sequence to examine the extent to which SES and ethnicity influenced smoking at three different time points, from smoking onset, to a serious quit attempt, to successful quitting. Theseanalyses provide an understanding of the relationships between SES, ethnicity, and CVD risk factors and suggest that if the timing, focus, and content of intervention programs take pathways into account they will result in more successful outcomes.
<161>Unique Identifier 10659384Authors Holcik J. Koupilova I.Institution Department of Social Medicine and Health Care Administration, Faculty of Medicine,Masaryk University, Brno, Czech Republic. [email protected] Defining and assessing health-related quality of life.Source Central European Journal of Public Health. 7(4):207-9, 1999 Nov.Abstract In recent years, there has been an increasing interest in quality of life assessment in clinical research and practice, as well as in public health and policyanalysis. Indicators of health-related quality of life are important not only for health professionals and their patients, but also for health administrators and health economists in health care planning and policy making. Most studies on the outcome of treatments and interventions now include some kind of a quality of life measure. This usually takes a form of an assessment of symptoms and physical functioning, measurement of psychological well-being, life satisfaction, or coping and adjustment. Numerous scales of psychological health, physical health status and physical functioning have been developed for use in the assessment of health
Page 78
401-600.txtoutcomes and a wide range of instruments for measurement of health-related quality of life is available. These fall into two broad categories of generic and disease-specific instruments. The selection of an instrument depends upon its measurement properties but also upon the specific context in which the instrument isgoing to be used. Adequate attention needs to be paid to the translation and validation of instruments for use across countries and cultural contexts.
<162>Unique Identifier 10643839Authors Handwerker WP.Institution Anthropology Department, University of Connecticut, Storrs 06269, USA.Title Cultural diversity, stress, and depression: working women in the Americas.Source Journal of Womens Health & Gender-Based Medicine. 8(10):1303-11, 1999 Dec.Abstract Social support lengthens life, and stressors induce morbidity early in life and death later. Social supports and stressors, however, particularly those embedded in daily social interactions, exhibit important forms of cultural variation not yet incorporated into stress measurements. This article reports a clinically useful measure of stress applicable to culturally diverse populations. Ninety working womenwith a wide range of ages, educational attainments, class backgrounds, and historical origins (Africa, northwest Europe, Hispanic, and Native Americans) provided cultural data on the meaning of stress. Consensus analysis, principal components analysis and Cronbach's alpha, and logistic regression document content validity of the stress scale items and the reliability and construct validity of thestress scale. The meaning of social supports (words or acts that imply respect, equality, or help or otherwise lead one to feel special and important) and stressors(words or acts that demean, imply inferiority, impede achievement, or otherwise leadone to feel bad about oneself) experienced in the course of daily social interactioncuts across cultural differences in other realms of life. Informants with a recent history of stress experienced a risk of depressive symptoms 85 times higher than informants without such a history. Standardized cultural research methods yield an instrument based on potential cultural universals that can facilitate clinical assessment and management of stress and health outcomes, such as depression, in culturally diverse populations.
<163>Unique Identifier 10624240Authors Mattson S. Rodriguez E.Institution College of Nursing, Arizona State University, Tempe, USA.Title Battering in pregnant Latinas.Source Issues in Mental Health Nursing. 20(4):405-22, 1999 Jul-Aug.Abstract Evidence suggests that abuse of women may be the most common form of family violence during the perinatal period. This battering is associated with adverse pregnancy outcomes and has physical, psychological, and social sequelae. Although some ethnic differences have been described in the occurrence of abuse, there is a paucity of research and culturally relevant prevention strategies and interventions to assist minority women. With both quantitative and qualitative methods, this studyexamined pregnant Latinas in three sites: urban Arizona, rural Arizona, and Mexico, to determine prevalence and type of abuse, level of acculturation, and self-esteem. Women were approached by a bilingual research assistant until 150 from each site
Page 79

401-600.txtagreed to participate. After informed consent was obtained, the questionnaires were administered in English or Spanish and read orally if the participant was unable to read. Focus groups with women recruited from each site by means of a return mail postcard provided qualitative information regarding their perceptions of battering, available resources, and how the Mexican culture influences this phenomenon. The women in the rural Arizona site reported the highest incidence of abuse and the highest levels of acculturation. Women in the focus groups discussed cultural reasons for violence and described helpful measures that could be offered to abused women.
<164>Unique Identifier 10621960Authors Barbarin OA.Institution South Africa Initiative Office, University of Michigan, Ann Arbor 48109-1285, [email protected] Social risks and psychological adjustment: a comparison of African American and South African children.Source Child Development. 70(6):1348-59, 1999 Nov-Dec.Abstract In the United States, race is highly associated with social risk factors such as poverty and family structure that may account by themselves for developmental outcomes often attributed to race alone. This cross-national study assesses the effects of social risks on adjustment of racially similar groups of 306 African American and 625 South African 6-year-olds. Poverty and gender were confirmed as risk factors but single female headship was not. Moreover, poverty and gender posed less risk for South African than for African American children. Poverty placed children at risk for immaturity, hyperactivity, and difficulty in peer relations. Boys were more likely to have behavior problems than were girls. African Americans exhibited higher rates of emotional symptoms but lower rates of bullying, destructiveness, and social rejection than did South Africans. African Americans, particularly the males, scored higher on the opposition and hyperactivity scales than did South Africans. Distinctive social contexts and cultural resources may account for differences in adjustment.
<165>Unique Identifier 10615165Authors Fresny CD. Stinghlamber B.Title [A new standardizing tool for all nurses. Interview by Bernadette Fabregas.]. [French]Source Soins; La Revue de Reference Infirmiere. (637):8-10, 1999 Jul-Aug.
<166>Unique Identifier 10600064Authors Balcazar H. Krull JL.Institution Department of Family Resources and Human Development, Arizona State University, Tempe 85287-2502, USA. [email protected] Determinants of birth-weight outcomes among Mexican-American women: examining
Page 80

401-600.txtconflicting results about acculturation.Source Ethnicity & Disease. 9(3):410-22, 1999 Autumn.Abstract In this article, we describe a comprehensive model for exploring the determinants of birth-weight outcomes among Mexican-American women from the Arizona Perinatal Acculturation Project. Data for this article came from a longitudinal study consisting of two phases. In phase one, a detailed prenatal survey was administered to 500 pregnant women. Phase two consisted of a postnatal survey administered to thewomen at least three months after they delivered (N = 269). Subjects who provided data were recruited from two health care agencies. Separate model building processeswere conducted for a continuous measure of birth weight, and a dichotomous indicatorof low-moderate birth weight (<2900 grams) using multiple linear and logistic regression analyses, respectively. The potential predictor variables for the models were divided into twelve predictor sets. The results showed that both final models included a combination of biological/behavioral factors, as well as protective sociocultural factor indicators. Acculturation status, one of the primary variables of interest in the study was found to be important for predicting birth weight and low-moderate birth weight. This result did not change when low birth weight (<2500 grams) infants were removed from the analyses. Low acculturation status was found tobe associated with better birth-weight outcomes than high acculturation status. Surprisingly, length of US residence had an opposite effect in predicting both birth-weight indicators when compared to acculturation status. These results suggestthat the relationships between acculturation and birth outcomes should be redefined to take into account the complexity of the phenomenon of acculturation in addition to the measurement of an array of family and sociocultural factors.
<167>Unique Identifier 10577563Authors Cohen MG. Granger CB. Ohman EM. Stebbins AL. Grinfeld LR. Cagide AM. ElizariMV. Betriu A. Kong DF. Topol EJ. Califf RM.Institution Duke Clinical Research Institute, Durham, North Carolina, USA. [email protected] Outcome of Hispanic patients treated with thrombolytic therapy for acute myocardial infarction: results from the GUSTO-I and III trials. Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries.Source Journal of the American College of Cardiology. 34(6):1729-37, 1999 Nov 15.Abstract OBJECTIVES: We sought to describe the differences in the process of care and clinical outcomes between Hispanics and non-Hispanics receiving thrombolytic therapyfor myocardial infarction (MI). BACKGROUND: Hispanics are the fastest growing and second largest minority in the U.S. but most cardiovascular disease data on Hispanics has been derived from retrospective studies and vital statistics. Despite their higher cardiovascular risk-factor profile, better outcomes after MI have been reported in Hispanics. METHODS: We studied the baseline characteristics, resource use and outcomes of 734 Hispanics and 27,054 non-Hispanics treated for MI in the GUSTO-I and -III trials. The primary end point of both trials was 30-day mortality. RESULTS: Hispanics were younger, shorter, lighter and more often diabetic and began thrombolysis 9 min later, compared with non-Hispanics. Measures of socioeconomic status (educational level, employment and health insurance) were lower among Hispanics. Fewer Hispanics than non-Hispanics underwent in-hospital angiography (70%vs. 74%, p = 0.013) or bypass surgery (11% vs. 13.5%, p = 0.04). Hispanics received more angiotensin-converting enzyme (ACE) inhibitors and less calcium-channel blockers, prophylactic lidocaine and inotropic agents. Mortality at 30 days and at one year did not differ significantly between Hispanics and non-Hispanics (6.4% vs. 6.7% and 9.0% vs. 9.7%, respectively). We noted no interactions between thrombolyticstrategy and Hispanic status on major outcomes (30-day death, stroke and major
Page 81

401-600.txtbleeding). CONCLUSIONS: The care of Hispanics with MI differed slightly from that ofnon-Hispanics. Nevertheless, these differences in care did not affect long-term outcomes.
<168>Unique Identifier 10575831Authors Jones ME. Bond ML.Institution Center for Hispanic Studies in Nursing and Health, University of Texas, Arlington School of Nursing, USA.Title Predictors of birth outcome among Hispanic immigrant women.Source Journal of Nursing Care Quality. 14(1):56-62, 1999 Oct.Abstract Eliminating racial and ethnic disparities in health is a major goal of Healthy People 2010. Health care providers and institutions can address the specialized cultural expectations and needs of Hispanic Americans by assessing acculturation status of the population, an intervening variable in patient compliance, and health outcomes. This article reports on maternal acculturation status and the relationshipto birth outcomes of 382 Hispanic pregnant women in the southwest United States. Themajority of these women were Mexican-oriented and had healthy pregnancies and healthy birth outcomes. Findings support the hypothesis that traditional Mexican cultural practices serve protective functions for the childbearing woman.
<169>Unique Identifier 10569437Authors Charlifue SW. Weitzenkamp DA. Whiteneck GG.Institution Research Department, Craig Hospital, Englewood, CO 80110, USA.Title Longitudinal outcomes in spinal cord injury: aging, secondary conditions, and well-being.Source Archives of Physical Medicine & Rehabilitation. 80(11):1429-34, 1999 Nov.Abstract OBJECTIVE: To specify the degree to which current age, duration of injury, and neurologic status affect the frequency of secondary health and psychosocial conditions in persons with long-term spinal cord injury (SCI), using both longitudinal and cross-sectional analysis techniques. DESIGN: Prospective longitudinal examination and data collection involving individuals with SCI studied initially at their 5th, 10th, and 15th anniversaries postinjury, and subsequently 5 years later at their 10th, 15th, and 20th anniversaries postinjury. SETTING: Five Regional Model Spinal Cord Injury Systems. PARTICIPANTS: The 439 individuals who meet the inclusion criteria for the National SCI Database and who are enrolled in a longitudinal study of secondary conditions and SCI. MAIN OUTCOME MEASURES: Physical and psychosocial status at various times postinjury. Results: There are different reports of various conditions when analyzing by neurologic groups, duration of injury, and age. Cross-sectional and longitudinal analyses also demonstrate different patterns of complications. CONCLUSIONS: The longitudinal method, like cross-sectional research, allows for identification of physical and psychosocial changes soon after they occur. Longitudinal research, however, also makes possible the development of predictive models for various long-term outcomes.
<170>Unique Identifier
Page 82

401-600.txt 10546722Authors Hopkins FW. MacKay AP. Koonin LM. Berg CJ. Irwin M. Atrash HK.Institution Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USA.Title Pregnancy-related mortality in Hispanic women in the United States.Source Obstetrics & Gynecology. 94(5 Pt 1):747-52, 1999 Nov.Abstract OBJECTIVE: To examine pregnancy-related mortality among Hispanic women in the United States. METHODS: We used data from the Centers for Disease Control and Prevention's ongoing Pregnancy Mortality Surveillance System to examine all reportedpregnancy-related deaths (deaths during or within 1 year of pregnancy that were caused by pregnancy, its complications, or treatment) in states that reported Hispanic origin for 1979-1992. The pregnancy-related mortality ratio was defined as the number of pregnancy-related deaths per 100,000 live births. RESULTS: For the 14-year period, the overall pregnancy-related mortality ratio was 10.3 deaths per 100,000 live births for Hispanic women, 6.0 for non-Hispanic white women, and 25.1 for black women. In Hispanic subgroups, the pregnancy-related mortality ratio was 9.7 for Mexican women and ranged from 7.8 for Cuban women to 13.4 for Puerto Rican women. Pregnancy-induced hypertension was the leading cause of pregnancy-related death for Hispanic women overall. CONCLUSION: Pregnancy-related mortality ratios forHispanic women were higher than those for non-Hispanic white women, but markedly lower than those for black women. The similarity in socioeconomic status between Hispanic and black women was not an indicator of similar health outcomes. Preventionof pregnancy-related deaths in Hispanic women should include investigation of medical and nonmedical factors and consider the heterogeneity of the Hispanic population.
<171>Unique Identifier 10536903Authors Vajkoczy P. Schurer L. Munch E. Schmiedek P.Institution Department of Neurosurgery, Klinikum Mannheim, University of Heidelberg, Germany. [email protected] Penetrating craniocerebral injuries in a civilian population in mid-Europe.Source Clinical Neurology & Neurosurgery. 101(3):175-81, 1999 Sep.Abstract Our current neurosurgical understanding of civilian penetrating craniocerebral injuries is based on US metropolitan series. It is unknown whether all principles applied to these patients are relevant in the Mid-European setting with its distinctepidemiology. The objective of this study was to characterize our patients with penetrating craniocerebral injuries, to analyze their outcome, and to identify relevant prognostic factors. Thirty-two patients with penetrating craniocerebral injuries were entered into the study. Patient evaluation comprised neurological, laboratory and radiographic analyses. Motivating factors were suicide (75%), assault(13%), and accident (9%). Initial GCS score, coagulopathy on admission, and radiographic extent of injury could be identified as outcome predictors (P < 0.001).An aggressive therapeutic approach to patients with GCS 3-7 reduced mortality when compared to a conservative management (67 vs. 91%). Due to major differences in epidemiology and outcome of our penetrating craniocerebral injury patients when compared to major US metropolitan series, current therapeutic strategies applied to this patient population in mid-Europe should be reconsidered. The results of our study justify an aggressive neurosurgical approach even in those patients that are thought to have a deleterious prognosis. Predictive variables identified in this
Page 83

401-600.txtstudy and a novel CT-grading algorithm may help in decision making.
<172>Unique Identifier 10531848Authors Brown SA. Hanis CL.Institution School of Nursing, University of Texas at Austin 78701, USA. [email protected] Culturally competent diabetes education for Mexican Americans: the Starr County Study.Source Diabetes Educator. 25(2):226-36, 1999 Mar-Apr.Abstract PURPOSE: Few culturally competent health programs have been designed for Mexican Americans, a group that bears a disproportionate burden of Type 2 diabetes. In StarrCounty, a Texas-Mexico border community, investigators designed and tested a culturally competent intervention aimed at improving the health of this target population. The purpose of this article is to describe the development process of this diabetes education and support group intervention. METHODS: The development stages were (1) community assessment, (2) intervention design, (3) selection or development of outcomes, (4) pilot testing, and (5) a randomized clinical investigation. RESULTS: Focus group participants identified knowledge deficits regarding diabetes and self-management strategies, and suggested characteristics of an effective intervention for Mexican Americans. Outcome measures included metaboliccontrol indicators, a newly developed knowledge instrument, and an existing health belief instrument. Preliminary analyses indicated that the intervention was successful in significantly improving metabolic control in the target population. CONCLUSIONS: Developing successful diabetes interventions for minority groups requires a number of stages, careful planning, assessment of cultural characteristics of the target population, and a systematic approach to implementation.
<173>Unique Identifier 10196934Authors Smith LS.Institution University of Alabama at Birmingham, USA.Title Cultural competence for nurses: canonical correlation of two culture scales.Source Journal of Cultural Diversity. 5(4):120-6, 1998 Winter.Abstract As the diversity of the US residential population increases, healthcare professionals need to recognize the importance of culturally competent care on health outcomes of individuals and communities. The purpose of this descriptive correlational pilot study (N = 51) was to describe the relationship among scores andsub-scores on scales measuring concepts of cultural competence. An additional purpose was to develop reliability and validity data on each of three culture scalesfor the population of hospital based registered nurses. Each of the scales had previously reported reliability and validity data but were administered to populations potentially different from southern-based, hospital-employed RNs. A large medical center located in Southeastern US was chosen as the study's site due to its diverse staff and client base. The Giger and Davidhizar Transcultural Assessment Model and Theory was the theoretical foundation for the study and Cultural Self-Efficacy Scale (CSES), Cultural Attitude Scale as developed by Bonaparte (1977, 1979) and modified by Rooda (1990, 1992) (CAS-Modified), and
Page 84

401-600.txtknowledge base questions (Rooda, 1990) were the chosen instruments. For this group of hospital based RNs, the reliability analysis--scale (Alpha) for the 58 item CSES was .9778. The reliability analysis (Alpha) for the 22 knowledge base questions was .6038 and .6412 for the 40 item CAS-M. Canonical correlation analysis was performed between a set of attitude variables and a set of self efficacy variables using SPSS (1995). Both sets of variables demonstrated statistically significant relationships (at an a priori alpha of .05) to each other (with an approximate Eta squared value for practical significance of .336), providing sufficient evidence to reject the non-relationship null hypothesis. For this sample and for these data, cultural self-efficacy toward Asian, Black, Hispanic clients, and self-efficacy regarding nursing skills when caring for diverse clients related to cultural attitudes and cultural self-efficacy. Nursing care, cultural health beliefs, and cultural health attitudes related to attitudes toward care of diverse clients. Both sets of variables related to each other as qualities of culturally competent nursing care.
<174>Unique Identifier 10093365Authors Mala TA. Gottlieb KL.Institution Southcentral (Tribal Health Care) Foundation, Anchorage, Alaska, USA.Title Designing a home health care system for Alaska Natives in Anchorage.Source International Journal of Circumpolar Health. 57 Suppl 1:675-8, 1998.Abstract PURPOSE: To design a health care program that allows Alaska Natives to receive culturally appropriate health services in their homes, thus avoiding the trauma of institutionalization and significantly increasing the quality of the patient's life during the course of the treated illness. METHOD: Utilizing the culturally appropriate sensitivity that is found within Tribal Health Corporations, Southcentral Foundation is designing a federally based community health care model to bring health support services into the patient's home. Health Aides and CommunityHealth Representatives play an important role in extending this model into an urban community setting. The cost of care is significantly reduced, as it is more cost-effective to keep patients in their own home environments rather than in institutions. RESULTS: Major outcomes for patients are increased cultural sensitivity to their needs, personal comfort, dignity, and care in their own home surroundings. Outcomes for the federal care system are significant savings and more efficient personalized health care.
<175>Unique Identifier 10093361Authors DeCourtney CA.Institution Bristol Bay Area Health Corporation, Dillingham, Alaska, USA.Title Alaska Native community assessment: health care services, knowledge of health issues, and health education.Source International Journal of Circumpolar Health. 57 Suppl 1:656-61, 1998.Abstract This project gathered information from 32 Alaska Native communities in Bristol Bay, located in southwestern Alaska, regarding use of health care services and knowledge of health care issues. It also educated residents about health care and their role in improving health status, enabling participants to feel that their involvement in planning health care services is important. In conjunction with the University of Washington Community Development Program and the Alaska Center for
Page 85

401-600.txtRural Health, a household survey was developed. A coordinator in each community was trained, and packets of surveys and health education materials were delivered to each household or post-office box. Completed surveys were returned, confidentially, to the village clinic. An English/Yup'ik cassette tape explaining the project was also available. Results were analyzed by the University of Washington. The findings were determined to be accurate with a 95% confidence level. Of surveys delivered to households, there was a 66% return rate and an overall return rate of 45%.
<176>Unique Identifier 10084352Authors Razali SM. Hasanah CI. Aminah K. Subramaniam M.Institution Department of Psychiatry, School of Medical Sciences, Universiti Sains Malaysia, Kubang Kerian Kelantan. [email protected] Religious--sociocultural psychotherapy in patients with anxiety and depression.Source Australian & New Zealand Journal of Psychiatry. 32(6):867-72, 1998 Dec.Abstract OBJECTIVE: To show the effectiveness of incorporating religious-sociocultural components in the management of patients with generalised anxiety disorders and major depression who have strong religious and cultural backgrounds as compared witha normal psychotherapeutic approach. METHODS: One hundred and three cases of anxietyand 100 cases of depression with strong religious and cultural backgrounds were randomly assigned to the study or control groups. Both groups received standard treatment for their respective illnesses. The study group was given additional religious-sociocultural psychotherapy. They were followed for 6 months and were assessed in a double-blind fashion using the Hamilton Anxiety Rating Scale or the Hamilton Depression Rating Scale. RESULTS: Patients receiving additional religious-sociocultural psychotherapy responded significantly faster than those who received standard treatment. However, the difference became non-significant at the end of 6 months. CONCLUSIONS: Incorporating a religious and sociocultural component in the treatment program rapidly improved anxiety and depressive symptoms in patients with strong religious and cultural backgrounds. The present study demonstrates a need for more sensitivity to religious-sociocultural issues in the field of mental health.
<177>Unique Identifier 10073197Authors Tervalon M. Murray-Garcia J.Title Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. [Review] [32 refs]Source Journal of Health Care for the Poor & Underserved. 9(2):117-25, 1998 May.Abstract Researchers and program developers in medical education presently face the challenge of implementing and evaluating curricula that teach medical students and house staff how to effectively and respectfully deliver health care to the increasingly diverse populations of the United States. Inherent in this challenge isclearly defining educational and training outcomes consistent with this imperative. The traditional notion of competence in clinical training as a detached mastery of atheoretically finite body of knowledge may not be appropriate for this area of physician education. Cultural humility is proposed as a more suitable goal in multicultural medical education. Cultural humility incorporates a lifelong commitment to self-evaluation and self-critique, to redressing the power imbalances in the patient-physician dynamic, and to developing mutually beneficial and
Page 86

401-600.txtnonpaternalistic clinical and advocacy partnerships with communities on behalf of individuals and defined populations. [References: 32]
<178>Unique Identifier 9987247Authors Smith LS.Institution Department of Nursing, State University of West Georgia, Carrollton, USA.Title Are we reaching the healthcare consumer?. [Review] [25 refs]Source Journal of Cultural Diversity. 5(2):48-52, 1998 Summer.Abstract With the diversity of our communities and waiting rooms increasing, can we continue to justify the lack of diversity among healthcare professionals? This article reports the demographic composition of the U.S. and compares those data withthe professional healthcare workforce. With a non-White population of nearly 25%, only 10% of RNs are non-White and about 12% of medical students are non-White. Four reasons are presented for increasing diversity among healthcare professionals. Thesefour include: improved culturally competent care, access to healthcare, healthcare outcomes and research, and provider access in high-need service areas. Healthcare organizations have gone on record as supporting increased diversity within high-skilled healthcare professions but without a commitment to increasing enrollments in professional healthcare programs, diversity goals will never be reached. [References: 25]
<179>Unique Identifier 10346658Authors Vazquez IM. Millen B. Bissett L. Levenson SM. Chipkin SR.Institution Section of Endocrinology, Nutrition and Diabetes, Boston Medical Center, Boston University School of Medicine, Massachusetts, USA.Title Buena Alimentacion, Buena Salud: a preventive nutrition intervention in Caribbean Latinos with type 2 diabetes.Source American Journal of Health Promotion. 13(2):116-9, 1998 Nov-Dec.Abstract A culturally sensitive 3-month intervention was provided to 18 Caribbean Latino men and women with non-insulin-dependent (type 2) diabetes mellitus. Compared to therandomly assigned control group, the intervention group showed statistically significant decreases in total calories, fat calories, percent of calories from fat,saturated fat calories, and percent of calories from saturated fat The intervention group showed increases in calories from carbohydrates and in the percent of caloriesfrom fiber.
<180>Unique Identifier 9891944Authors Shaila HP. Udupa SL. Udupa AL.Institution Dept. of Biochemistry, Kasturba Medical College, Manipal, India.Title Hypolipidemic activity of three indigenous drugs in experimentally induced atherosclerosis.
Page 87

401-600.txtSource International Journal of Cardiology. 67(2):119-24, 1998 Dec 1.Abstract The effect of orally administered indigenous drugs Terminalia arjuna, T. belerica and T. chebula were investigated on experimental atherosclerosis. Rabbits were fed acholesterol-rich diet to induce atherosclerosis. The three drugs were fed along withcholesterol. At the end of the experimental period the animals were killed and theirplasma and tissue lipid components estimated. Atherosclerotic lesions of the aorta were examined histologically. T. arjuna was found to be the most potent hypolipidemic agent and induced partial inhibition of rabbit atheroma. The results indicate that T. arjuna may play an anti-atherogenic role.
<181>Unique Identifier 9887714Authors Zollo JA.Institution Faculty of Nursing, University of South Australia.Title Reflective practice in nurse education: a step towards equity in education and health care.Source Collegian. 5(3):28-33, 1998 Jul.Abstract In the past, the Australian health care system, whose mainstream services are essentially monocultural, has not always successfully met the needs of clients from a variety of cultural groups. Entry of more young immigrant people into the essential health services is one strategy which may assist in bringing positive benefits to health care consumers from non-English speaking backgrounds (NESB). For NESB students, however, the tertiary education experience frequently produces inequities similar to those encountered by NESB consumers of health care, and failure rates of these students are often disproportionately high. This paper describes the process of reflective practice used to investigate the needs of NESB students enrolled in the first year of an undergraduate nursing degree, and the strategies subsequently initiated to improve educational outcomes for these students. In terms of academic success, outcomes for NESB students involved in the investigation were markedly improved in comparison to the previous year. More importantly, the project fostered reflection on teaching practices, and led to modifications which, although small, represented a positive step towards equity.
<182>Unique Identifier 9884992Authors Dressler WW. Balieiro MC. dos Santos JE.Institution Department of Anthropology, University of Alabama, Tuscaloosa, USA.Title Culture, socioeconomic status, and physical and mental health in Brazil.Source Medical Anthropology Quarterly. 12(4):424-46, 1998 Dec.Abstract The association of socioeconomic variables with poor health status has been widelyobserved, if not well understood, and cultural dimensions of socioeconomic differences have rarely been incorporated into research models. In this article, a cultural dimension of socioeconomic status is examined in a Brazilian city through the use of ethnographic and social survey techniques. It suggests that lifestyle, defined in terms of the relative ability to accumulate consumer goods and the adoption of associated behaviors, is an important component of socioeconomic differences. Further research using cultural consensus analysis, a structured
Page 88

401-600.txtethnographic technique that may be used to study shared cultural knowledge, demonstrates significant consensus regarding the definition of the successful lifestyle. Then, using that culturally defined model of the successful lifestyle as the central tendency, an individual-level measure of approximation to that lifestylewas developed for a representative sample of 250 persons. This culturally defined measure of lifestyle was inversely associated with arterial blood pressure (beta = -.216, p < .01), depressive symptoms (beta = -.236, p < .01), and globally perceivedstress (beta = -.358, p < .01); furthermore, it absorbed the explained variability in these outcomes that is associated with conventional socioeconomic variables (occupation, education, income). For arterial pressure, cultural consonance explained almost 10 percent of the differences in blood pressure between individuals; for the psychological outcome variables, cultural consonance explained between 10 percent and 20 percent of the differences between individuals. Finally, its statistical effects were independent of other socioeconomic, dietary, anthropometric, and psychosocial variables. These results suggest that an individual's approximation to the cultural ideal of lifestyle, his or her "cultural consonance," mediates the observed effects of socioeconomic variables on health status.
<183>Unique Identifier 9874323Authors Sorof JM. Hawkins EP. Brewer ED. Boydstun II. Kale AS. Powell DR.Institution Department of Pediatrics, Texas Children's Hospital, Baylor College of Medicine, Houston 77030-2399, USA.Title Age and ethnicity affect the risk and outcome of focal segmental glomerulosclerosis.Source Pediatric Nephrology. 12(9):764-8, 1998 Nov.Abstract In patients with proteinuria, African-American (AA) ethnicity is reported to be a risk factor for focal segmental glomerulosclereosis (FSGS) and its progression to end-stage renal disease (ESRD). We reviewed our single-center experience to determine the probability of FSGS and its progression to ESRD based on ethnicity andage at presentation in children with proteinuria with or without nephrotic syndrome.Proteinuria without systemic disease or acute glomerulonephritis was the presenting feature in 17% (236/1,403) of children in the renal patient database of Texas Children's Hospital, Baylor College of Medicine. Histopathological diagnoses were established in 107 of 236 patients (45%). FSGS was identified in 65 patients, accounting for 28% of all patients with proteinuria and 61% of patients who underwent renal biopsy. FSGS was more prevalent in AA (45%) than in non-AA patients (22%) (P=0.001), and AA patients with FSGS were older at presentation (12.7+/-4.4 years) than non-AA patients (5.6+/-4.6 years) (P<0.001). Among patients who underwent renal biopsy, increasing age at presentation increased the probability of having FSGS in AA but not non-AA patients (P=0.04). Five-year actuarial renal survival of FSGS was worse in AA (8%) than in non-AA patients (31%) (P=0.01). These data suggest an increased risk and worse outcome of FSGS in AA compared with non-AA children.
<184>Unique Identifier 9865892Authors Cloutterbuck JC. Cherry BS.Institution College of Nursing, University of Massachusetts, Boston 02125, USA.Title The Cloutterbuck Minimum Data Matrix: a teaching mechanism for the new millennium.
Page 89

401-600.txt[Review] [70 refs]Source Journal of Nursing Education. 37(9):385-93, 1998 Dec.Abstract The demands of the United States' rapidly changing health care system and society signal the need to design and implement health professions programs which prepare students for practice within a health care paradigm that will be very different fromthe one existing today and for work with an increasingly diverse and independent consumer population. The Cloutterbuck Minimum Data Matrix (CMDM) is a teaching mechanism designed to generate a comprehensive base of consumer information prerequisite to the indepth level of critical analysis and synthesis needed to produce quality health care outcomes in the 21st century. The CMDM assumes an interdisciplinary perspective and educates students to recognize and incorporate consumer diversity into strategies for care. [References: 70]
<185>Unique Identifier 9826838Authors Berman A. Manning MP. Peters E. Siegel BB. Yadao L.Institution Samuel Merritt College, Oakland, CA, USA.Title A template for cultural diversity workshops.Source Oncology Nursing Forum. 25(10):1711-8, 1998 Nov-Dec.Abstract PURPOSE/OBJECTIVES: To present a model for a series of workshops designed to improve the ability of oncology nurses to understand and fulfill culturally based needs of racially and ethnically diverse patients with cancer. DATA SOURCES: Published literature and author experience. DATA SYNTHESIS: Most nurses work with patients from a variety of ethnic or cultural backgrounds yet know little of how this affects patients' cancer experiences. Four workshops were presented that focused on the most common ethnic groups in the geographic area. A content template was developed that worked well to ensure complete topic coverage. CONCLUSIONS: Workshops were well-received. Nurses identified barriers to care and interventions that are appropriate for diverse patient populations. The follow-up survey indicatedthat some anticipated program outcomes may not be feasible if attendees do not regularly work with target populations. IMPLICATIONS FOR NURSING PRACTICE: The modelcan be modified for use in any geographic area. Such workshops should be repeated atregular intervals.
<186>Unique Identifier 9827851Authors Simmons D. Weblemoe T. Voyle J. Prichard A. Leakehe L. Gatland B.Institution South Auckland Division of Clinical Science, University of Auckland, Middlemore Hospital, New Zealand.Title Personal barriers to diabetes care: lessons from a multi-ethnic community in New Zealand.Source Diabetic Medicine. 15(11):958-64, 1998 Nov.Abstract The aim of this study was to identify and quantify barriers to diabetes care perceived by diabetic subjects from a multiethnic, urban community (mainly New Zealand Europeans, Maori, and Pacific Islanders). A qualitative survey including 57 diabetic subjects and health care providers from a diverse range of backgrounds was followed by a cross-sectional household survey. Barriers to care were quantified
Page 90

401-600.txtamong 1862 (2.1%) diabetic residents of a total surveyed population of 90477. Thirtybarriers to care categories were generated incorporating patient beliefs, internal and external physical barriers, educational, psycho-social and psychological barriers. In spite of major difference in culture, acculturation, and socio-economicstatus, the top 10 barriers were similar between the ethnic groups. The most important barriers were perceiving that the benefits of self-care were outweighed bythe disadvantages (20% Europeans, 20% Maori, 29% Pacific Islanders, 16% others, p<0.001), lack of community-based services (13% Europeans, 27% Maori, 25% Pacific Islanders, 11% others, p<0.001) and the limited range of services available (15% Europeans, 22% Maori, 20% Pacific Islanders, 14% others, p<0.05). It is postulated that definition of these barriers, with subsequent, systematic action to reduce their impact, in both patients and populations could result in an improvement in diabetes outcomes.
<187>Unique Identifier 9817473Authors Canto JG. Taylor HA Jr. Rogers WJ. Sanderson B. Hilbe J. Barron HV.Institution University of Alabama Medical Center, Birmingham, USA.Title Presenting characteristics, treatment patterns, and clinical outcomes of non-blackminorities in the National Registry of Myocardial Infarction 2.Source American Journal of Cardiology. 82(9):1013-8, 1998 Nov 1.Abstract Data from a national registry (cohort) of myocardial infarction, which has enrolled 275,046 patients from June 1994 to April 1996, were analyzed to compare thebaseline demographic and clinical characteristics, treatment patterns, and clinical outcomes among Hispanics, Asian-Pacific islanders, and native Americans with those of white Americans presenting to the hospital with acute myocardial infarction. Non-black minorities were younger, had a higher proportion of men, used the emergency medical services less frequently, and presented later to the hospital after the onset of symptoms (135 vs 122 minutes, p <0.001) than whites. Also, non-black minorities were less likely to receive beta-blocker therapy at discharge (crude odds ratio 0.86, confidence interval 0.82 to 0.90) than whites, but they weregenerally as likely to receive intravenous thrombolytic therapy (with the exception of Asian-Pacific islanders) and undergo both coronary arteriography and revascularization procedures as their white counterparts. There were no significant differences in hospital mortality for non-black minorities compared with whites.
<188>Unique Identifier 9811291Authors Flores G. Abreu M. Olivar MA. Kastner B.Institution Boston University School of Medicine, Department of Pediatrics, Boston Medical Center, MA 02118, USA. [email protected] Access barriers to health care for Latino children.Source Archives of Pediatrics & Adolescent Medicine. 152(11):1119-25, 1998 Nov.Abstract BACKGROUND: Latinos will soon be the largest minority group in the United States, but too little is known about major access barriers to health care for this group and whether these barriers result in adverse consequences. OBJECTIVE: To identify important access barriers to health care for Latino children, as cited by parents. DESIGN: Cross-sectional survey of parents of all 203 children coming to the pediatric Latino clinic at an innercity hospital. Questions focused on barriers to
Page 91
401-600.txthealth care experienced prior to receiving care at the Latino clinic. RESULTS: Parental ethnicity included Dominican (36%), Puerto Rican (34%), Central American (13%), and South American (11%). Only 42% of parents were American citizens, whereas36% had green cards, and 13% had no documentation. Eight percent of parents and 65% of the children were born in the United States. Parents rated their ability to speakEnglish as follows: very well/well, 27%; not very well, 46%; and not at all, 26%. The median annual household income was $11,000; 40% of parents never graduated from high school, and 49% headed single-parent households. Forty-three percent of the children were uninsured. A sick child was routinely brought to hospital clinics by 56% of parents, to the emergency department by 21%, and to neighborhood health centers by 21%. When asked to name the single greatest barrier to health care for their children, parents cited language problems (26%), long waiting time at the physician's office (15%), no medical insurance (13%), and difficulty paying medical bills (7%). When parents were asked if a particular barrier had ever caused them notto bring their children in, transportation was cited by 21%; not being able to afford health care, 18%; excessive waiting time in the clinic, 17%; no health insurance, 16%; and lack of cultural understanding by staff, 11%. Some parents who spoke little or no English reported that medical staff not speaking Spanish had led to adverse health consequences for their children, including poor medical care (8%),misdiagnosis (6%), and prescription of inappropriate medications (5%). Multivariate analyses of selected health outcomes using 7 independent variables showed that low family income was significantly associated with greater odds of a child's having suboptimal health status (odds ratio, 1.5; 95% confidence interval, 1.04-2.2) and anincreased number of physician visits in the past year (P<.04), but reduced odds (odds ratio, 0.6; 95% confidence interval, 0.4-0.9) of the child's being brought to the emergency department for a routine sick visit. Children whose parents had resided in the United States for fewer than 8 years were at reduced odds (odds ratio, 0.5; 95% confidence interval, 0.2-0.9) for having spent a day or more in bed for illness in the past year. CONCLUSIONS: Parents identified language problems, cultural differences, poverty, lack of health insurance, transportation difficulties, and long waiting times as the major access barriers to health care forLatino children. Language problems can result in adverse health consequences for some children, including poor medical care, misdiagnosis, and inappropriate medication and hospitalization. Low family income is an important independent risk factor among Latino children for suboptimal health and high utilization of health services.
<189>Unique Identifier 9811289Authors Fuentes-Afflick E. Hessol NA. Perez-Stable EJ.Institution Department of Pediatrics, Medical Effectiveness Research Center for Diverse Populations, Institute for Health Policy Studies, University of California, San Francisco 94110, USA. [email protected] Maternal birthplace, ethnicity, and low birth weight in California.Source Archives of Pediatrics & Adolescent Medicine. 152(11):1105-12, 1998 Nov.Abstract BACKGROUND: Although immigrants to the United States are usually ethnic minoritiesand socioeconomically disadvantaged, foreign-born women generally have lower rates of low birth weight infants than do US-born women. OBJECTIVE: To measure the relationship between maternal birthplace, ethnicity, and low birth weight infants. DESIGN: Retrospective cohort study of birth certificate data. SETTING: California, 1992. SUBJECTS: Singleton infants (n = 497 868) born to Asian, black, Latina, and white women. MAIN OUTCOME MEASURES: Very low birth weight (500-1499 g), moderately low birth weight (1500-2499 g), and normal birth weight (2500-4000 g, reference category). RESULTS: Foreign-born Latina women generally had less favorable maternal characteristics than US-born Latinas, yet foreign-born Latina women were less likelyto have moderately low birth weight infants (odds ratio, 0.91; 95% confidence
Page 92

401-600.txtinterval, 0.86-0.96) than US-born Latinas after adjusting for maternal age, education, marital status, parity, tobacco use, use of prenatal care, and gestational age. While foreign-born Asian women generally had a less favorable profile of maternal characteristics than US-born Asians, there was no statistically significant difference in the odds of very low birth weight or moderately low birth weight infants between foreign- and US-born Asian women. Foreign-born black women had more favorable maternal characteristics than US-born women, but there was no significant nativity difference in very low birth weight or moderately low birth weight between foreign- and US-born black women after adjusting for maternal and infant factors. CONCLUSIONS: The relationship between maternal birthplace and low birth weight varies by ethnicity. Further study is needed to understand the favorable pregnancy outcomes of foreign-born Latina women.
<190>Unique Identifier 9809707Authors Willke RJ. Glick HA. Polsky D. Schulman K.Institution Pharmacia & Upjohn, Inc., Kalamazoo, MI 49001-0199, USA. [email protected] Estimating country-specific cost-effectiveness from multinational clinical trials.Source Health Economics. 7(6):481-93, 1998 Sep.Abstract Because costs and outcomes of medical treatments may vary from country to country in important ways, decision makers are increasingly interested in having data based on their own country's health care situations. This paper proposes methods for estimating country-specific cost-effectiveness ratios from data available from multinational clinical trials. It examines how clinical and economic outcomes interact when estimating treatment effects on cost and proposes empirical methods for capturing these interactions and incorporating them when making country-specificestimates. We use data from a multinational phase III trial of tirilazad mesylate for the treatment of subarachnoid haemorrhage to illustrate these methods. Our findings suggest that it is possible for meaningful country-by-country differences to be found in such trial data. These differences can be useful in informing reimbursement, utilization, and other decisions taken at the country level.
<191>Unique Identifier 9786235Authors Khoshnood B. Lee KS. Wall S. Hsieh HL. Mittendorf R.Institution Department of Pediatrics, University of Chicago Children's Hospital, IL 60637, USA.Title Short interpregnancy intervals and the risk of adverse birth outcomes among five racial/ethnic groups in the United States.Source American Journal of Epidemiology. 148(8):798-805, 1998 Oct 15.Abstract The authors studied the effects and population-level impact of short (< or = 12 months) interpregnancy intervals on the risks for low (<2.5 kg) birth weight and preterm (<37 weeks) delivery of liveborn singleton infants to US African American, Mexican, Native American, non-Hispanic white, and Puerto Rican mothers (n = 4,841,418) from 1989 to 1991. Statistical analyses were done by using the Mantel-Haenszel correlation statistic chi-square test and logistic regression. The proportion of livebirths associated with < or =12-month interpregnancy intervals wasthe lowest among non-Hispanic whites (18.5%, 95% confidence interval 18.5-18.5) and
Page 93

401-600.txtthe highest among Native Americans (29.7%, 95% confidence interval 29.2-30.2). As compared with mothers with >12-month intervals, mothers with <6-month intervals had an approximately 50% to 80% increased risk of very low (<1.5 kg) birth weight delivery and a 30% to 90% increased risk of very preterm (<32 weeks) delivery. Logistic regression analyses showed that the adverse effects of short intervals werereduced by about 10% but remained for the most part significant after controlling for potential confounding by maternal age, education, parity, marital status, prenatal care, smoking, and previous preterm delivery.
<192>Unique Identifier 9782926Authors Barnes DM. Davis AJ. Moran T. Portillo CJ. Koenig BA.Institution University of Texas at Austin 78701, USA.Title Informed consent in a multicultural cancer patient population: implications for nursing practice.Source Nursing Ethics: an International Journal for Health Care Professionals. 5(5):412-23, 1998 Sep.Abstract Obtaining informed consent, an ethical obligation of nurses and other health care providers, occurs routinely when patients make health care decisions. The values underlying informed consent (promotion of patients' well-being and respect for theirself-determination) are embedded in the dominant American culture. Nurses who apply the USA's cultural values of informed consent when caring for patients who come fromother cultures encounter some ethical dilemmas. This descriptive study, conducted with Latino, Chinese and Anglo-American cancer patients in a large, public, west-coast clinic, describes constraints on the informed consent process in a multicultural setting, including language barriers, the clinical environment, control in decision making, and conflicting desired health outcomes for health care providers and patients, and suggests some implications for nursing practice.
<193>Unique Identifier 9780811Authors Stuchbery M. Matthey S. Barnett B.Institution Paediatric Mental Health Service, South West Sydney Health Service, Liverpool NSW,Australia.Title Postnatal depression and social supports in Vietnamese, Arabic and Anglo-Celtic mothers.Source Social Psychiatry & Psychiatric Epidemiology. 33(10):483-90, 1998 Oct.Abstract The significance of a western woman's social supports to postnatal depression is well documented. We examine which deficits in components of their social support network are associated with postnatal depression in women from a non-English-speaking background. The social support network and postnatal mood of 105 Anglo-Celtic, 113 Vietnamese and 98 Arabic women were assessed at 6 weeks postpartum. The role of social supports in determining scores on the Edinburgh Postnatal Depression Scale (EPDS) was analysed using multiple regressions. For Anglo-Celtic women, low postnatal mood was associated with perceived need for more emotional support from partners and mothers. For Vietnamese women, low postnatal mood was associated with poor quality of relationship with the partner and a perceived need for more practical help from him. For Arabic women, low postnatal mood was associated with perceived need for more emotional support from partners. We
Page 94

401-600.txtconclude that cultural factors mediate the relation between social supports and postnatal depression more likely to become clinically depressed (Lovestone and Kumar1993) and infants may have adverse cognitive, behavioural and emotional outcomes, which can be linked to the postnatal depression (Murray and Cooper 1996).Other Abstract Studies of mothers in industrialized societies have suggested that deficiencies inpersonal social support systems precede the development of postnatal depression. Thedeterminants of postpartum depression for non-English-speaking background mothers were investigated in a study of Anglo-Celtic, Vietnamese, and Arabic mothers recruited from antenatal clinics in South Western Sydney, Australia. 60% of Vietnamese and 43% of Arabic women had ben living in Australia for less than 3 years. The seven social support variables were wanting more practical support from one's partner or from another person; wanting more emotional support from one's mother, one's partner, or another person; and the quality of the relationship with one's partner and one's mother. In general, Vietnamese women reported a poorer quality of relationship with their partners than the two other groups, while Arabic women reported better quality relationships with their mothers. The associations between the support variables and scores on the Edinburgh Postnatal Depression Scale(EPDS) at 6 weeks postpartum were examined in three multiple linear regression analyses. For Anglo-Celtic mothers, two variables--wanting more emotional support from one's partner and from one's mother--accounted for 25% of the observed variancein EPDS scores. Poor quality of the relationship with one's partner and wanting morepractical support from one's partner explained 34% of the variance in EPDS scores for Vietnamese mothers. For Arabic mothers, wanting more emotional support from one's mother was the only significant predictor of the EPDS score and this accountedfor 5% of the variance. Overall, these findings indicate that cultural factors mediate the relation between social supports and postnatal depression.
<194>Unique Identifier 9779677Authors Waters RL. Adkins RH. Sie I. Cressy J.Institution Regional Spinal Injury Care System of Southern California, Injury Prevention Research Center, University of California, Los Angeles, USA.Title Postrehabilitation outcomes after spinal cord injury caused by firearms and motor vehicle crash among ethnically diverse groups.Source Archives of Physical Medicine & Rehabilitation. 79(10):1237-43, 1998 Oct.Abstract OBJECTIVES: To determine the differential effects of impairment, disability, etiology, and selected preinjury and social factors on medical complications, medical resources use, and handicap after rehabilitation for spinal cord injury (SCI). DESIGN: Survey including interview and medical record review. SETTING: Model SCI Care System centered at an urban, public medical center. PARTICIPANTS: A volunteer convenience sample of 164 men, ages 18 to 35yrs at injury, with SCI causedby firearms or motor vehicle crash. MAIN OUTCOME MEASURES: Mean numbers of documented complications, pressure sore episodes, nonroutine clinic visits, postrehabilitation hospitalization days per year, assessment by Functional Independence Measure (FIM), and total score on the Craig Handicap Assessment and Reporting Technique (CHART). RESULTS: Significant factors for postrehabilitation complications were discharge FIM (p < .001) and injury duration (p = .046); for pressure ulcer episodes, they were injury completeness (p < .001), drug abuse following injury (p = .005), and ethnicity (p = .043); for average annual nonroutineclinic visits, they were complications (p < .001), pressure ulcer episodes (p < .001), duration of injury (p = .001), and pain (p = .052); for hospitalization, theywere pressure ulcer episodes (p < .001) and complications (p = .043); for CHART scores, they were discharge FIM (p < .001), preinjury education (p < .001), hospitalization (p = .007), chronic pain (p = .01), longest time at one job (p = .02), completeness of injury (p = .042), and preinjury employment (p = .049).
Page 95

401-600.txtCONCLUSIONS: Disability is the most important factor in postrehabilitation outcomes for SCI, followed by injury completeness, which is also associated with multiple outcomes. Postinjury but not preinjury drug abuse is adversely associated with outcomes. Etiology and ethnicity are not important determinates of outcome.
<195>Unique Identifier 9777820Authors Milford EL.Title Organ transplantation--barriers, outcomes, and evolving policies.[comment].Source JAMA. 280(13):1184-5, 1998 Oct 7.
<196>Unique Identifier 9768384Authors Mishra SI. Chavez LR. Magana JR. Nava P. Burciaga Valdez R. Hubbell FA.Institution University of California, Department of Medicine, School of Social Ecology, USA. [email protected] Improving breast cancer control among Latinas: evaluation of a theory-based educational program.Source Health Education & Behavior. 25(5):653-70, 1998 Oct.Abstract The study evaluated a theory-based breast cancer control program specially developed for less acculturated Latinas. The authors used a quasi-experimental design with random assignment of Latinas into experimental (n = 51) or control (n = 37) groups that completed one pretest and two posttest surveys. The experimental group received the educational program, which was based on Bandura's self-efficacy theory and Freire's empowerment pedagogy. Outcome measures included knowledge, perceived self-efficacy, attitudes, breast self-examination (BSE) skills, and mammogram use. At posttest 1, controlling for pretest scores, the experimental groupwas significantly more likely than the control group to have more medically recognized knowledge (sum of square [SS] = 17.0, F = 6.58, p < .01), have less medically recognized knowledge (SS = 128.8, F = 39.24, p < .001), greater sense of perceived self-efficacy (SS = 316.5, F = 9.63, p < .01), and greater adeptness in the conduct of BSE (SS = 234.8, F = 153.33, p < .001). Cancer control programs designed for less acculturated women should use informal and interactive educationalmethods that incorporate skill-enhancing and empowering techniques.
<197>Unique Identifier 9768301Authors Suris AM. Trapp MC. DiClemente CC. Cousins J.Institution Department of Veteran Affairs, North Texas Health Care System, Dallas 75216, USA.Title Application of the transtheoretical model of behavior change for obesity in Mexican American women.Source Addictive Behaviors. 23(5):655-68, 1998 Sep-Oct.Abstract The prevalence, consequences, and resistance to treatment of obesity make it one of the most difficult psychological and medical problems in society today. The
Page 96

401-600.txtincidence of obesity is greater in Mexican Americans than in Caucasians. The purposeof this study was to apply the Transtheoretical Model of Behavior Change on a sampleof Mexican American women in weight-loss study. Questionnaires assessing the stages and processes of change were shortened, translated, and administered to subjects. Cluster analyses were conducted to determine the stage of change profiles, with fivedistinct profiles emerging. These profiles are consistent with those reported in previous research on smoking, psychotherapy, alcoholism, and overeating. Relationships among stages, processes, and profiles of change were examined and found to be consistent with previous research. This study supports the use of the Transtheoretical Model with Mexican American women who were enrolled in a behaviorally oriented weight-loss program. Results of the study are limited owing toa small sample size; however, it does provide a foundation to incorporate Hispanic populations in future studies pertaining to stages and processes of behavior change.
<198>Unique Identifier 9757754Authors Child J. Bierer M. Eagle K.Institution Mount Sinai School of Medicine, New York, NY, USA.Title Unexpected factors predict control of hypertension in a hospital-based homeless clinic.Source Mount Sinai Journal of Medicine. 65(4):304-7, 1998 Sep.Abstract BACKGROUND: Boston Health Care for the Homeless Program (BHCHP) physicians conducta primary care clinic twice a week at Massachusetts General Hospital (MGH). The MGH clinic is part of a city-wide network of BHCHP clinics providing primary care services to indigent patients. Despite this network, long term control of chronic illnesses such as hypertension (HTN) continues to challenge the clinic staff. METHODS: In an effort to better understand the factors obstructing long term treatment of chronic illness, we conducted a chart review of hypertensive patients seen over a three-year period (January 1991 to March 1994) at the MGH clinic. Frequency of visits, total number of visits and physicians' notes on concomitant diagnoses were analyzed for their correlation to control of hypertension. RESULTS: Overall control of hypertension was poor (42%). A greater proportion of patients with a diagnosis of psychiatric illness responded to treatment intended to lower their blood pressure below 140/90 mm Hg than those without such a diagnosis (odds ratio: 10.2). While there was no difference in the total number of clinic visits during the study period, those with a diagnosis of psychiatric illness had a lower average number of days between their first and third visits (52 days vs 108 p = 0.002). CONCLUSIONS: A greater proportion of patients with concomitant psychiatric diagnoses exhibited blood pressures < or = 140/90 mm Hg than patients without mentalillness. The increased frequency of visits at the onset of treatment may confer a positive effect on long term control of HTN among homeless patients attending outpatient hospital-based clinics.
<199>Unique Identifier 9753903Authors Jones ME. Bond ML. Cason CL.Institution University of Texas at Arlington, USA.Title Where does culture fit in outcomes management?. [Review] [39 refs]Source Journal of Nursing Care Quality. 13(1):41-51, 1998 Oct.Abstract
Page 97

401-600.txt The authors describe the concept of cultural competence and ways in which culture,a structure of care variable, is important to the delivery of culturally competent care. The role of culture in outcomes assessment and management is explored. The culture of the patient, the health care professional, and the organization is examined as it influences the potential to deliver culturally competent care. Strategies for developing a culturally competent work force are proposed with examples from ongoing projects in a large metroplex in the southwestern part of the United States. [References: 39]
<200>Unique Identifier 9741678Authors Deater-Deckard K. Dodge KA. Bates JE. Pettit GS.Institution Institute of Psychiatry, London. [email protected] Multiple risk factors in the development of externalizing behavior problems: groupand individual differences.Source Development & Psychopathology. 10(3):469-93, 1998 Summer.Abstract The aim of this study was to test whether individual risk factors as well as the number of risk factors (cumulative risk) predicted children's externalizing behaviors over middle childhood. A sample of 466 European American and 100 African American boys and girls from a broad range of socioeconomic levels was followed fromage 5 to 10 years. Twenty risk variables from four domains (child, sociocultural, parenting, and peer-related) were measured using in-home interviews at the beginningof the study, and annual assessments of externalizing behaviors were conducted. Consistent with past research, individual differences in externalizing behavior problems were stable over time and were related to individual risk factors as well as the number of risk factors present. Particular risks accounted for 36% to 45% of the variance, and the number of risks present (cumulative risk status) accounted for19% to 32% of the variance, in externalizing outcomes. Cumulative risk was related to subsequent externalizing even after initial levels of externalizing had been statistically controlled. All four domains of risk variables made significant uniquecontributions to this statistical prediction, and there were multiple clusters of risks that led to similar outcomes. There was also evidence that this prediction wasmoderated by ethnic group status, most of the prediction of externalizing being found for European American children. However, this moderation effect varied depending on the predictor and outcome variables included in the model.
Page 98

601-772.txt<1>Unique Identifier 9741678Authors Deater-Deckard K. Dodge KA. Bates JE. Pettit GS.Institution Institute of Psychiatry, London. [email protected] Multiple risk factors in the development of externalizing behavior problems: groupand individual differences.Source Development & Psychopathology. 10(3):469-93, 1998 Summer.Abstract The aim of this study was to test whether individual risk factors as well as the number of risk factors (cumulative risk) predicted children's externalizing behaviors over middle childhood. A sample of 466 European American and 100 African American boys and girls from a broad range of socioeconomic levels was followed fromage 5 to 10 years. Twenty risk variables from four domains (child, sociocultural, parenting, and peer-related) were measured using in-home interviews at the beginningof the study, and annual assessments of externalizing behaviors were conducted. Consistent with past research, individual differences in externalizing behavior problems were stable over time and were related to individual risk factors as well as the number of risk factors present. Particular risks accounted for 36% to 45% of the variance, and the number of risks present (cumulative risk status) accounted for19% to 32% of the variance, in externalizing outcomes. Cumulative risk was related to subsequent externalizing even after initial levels of externalizing had been statistically controlled. All four domains of risk variables made significant uniquecontributions to this statistical prediction, and there were multiple clusters of risks that led to similar outcomes. There was also evidence that this prediction wasmoderated by ethnic group status, most of the prediction of externalizing being found for European American children. However, this moderation effect varied depending on the predictor and outcome variables included in the model.
<2>Unique Identifier 10182529Authors Hutchins JJ.Institution Johns Hopkins Medicine, Baltimore, MD, USA.Title Bringing international patients to American hospitals: the Johns Hopkins perspective.Source Managed Care Quarterly. 6(3):22-7, 1998 Summer.Abstract American health care institutions are reaching out to the foreign market, assiduously cultivating patients from overseas. This innovative strategy, designed in part to help U.S. medical centers cope with cuts in federal funding, HMO pressures, and decreasing patient volumes, dovetails nicely with the current climateof global expansion in business and worldwide awareness of American medical expertise. This article describes the International Services Program at Johns Hopkins Hospital. The author and program director addresses its origins, implementation, outcomes, and the obstacles planners faced in launching a vigorous, international outreach initiative.
<3>Unique Identifier 9711457Authors Reichman NE. Kenney GM.
Page 1

601-772.txtInstitution Office of Population Research, Princeton University, NJ, USA.Title Prenatal care, birth outcomes and newborn hospitalization costs: patterns among Hispanics in New Jersey.Source Family Planning Perspectives. 30(4):182-7, 200, 1998 Jul-Aug.Abstract CONTEXT: With the influx of Latin American immigrants to the United States and therelatively high fertility of Hispanic women, the importance of understanding patterns of birth outcomes within the heterogeneous Hispanic community is growing. METHODS: Vital statistics data linked with hospital discharge files for single, liveborn infants delivered in New Jersey to state residents in 1989 and 1990 are used to examine the effects of maternal birthplace and Hispanic ethnicity on early initiation of prenatal care, low birth weight, infant mortality and newborn hospitalcosts. Multivariate analyses control for a range of demographic, economic, behavioral and medical factors. RESULTS: White women of Puerto Rican descent have a significantly higher risk than both non-Hispanic whites and other Hispanic whites ofhaving a low-birth-weight baby. However, their infants do not have an increased riskof mortality, and newborn hospitalization costs are not elevated for this group. Mexican-born white women begin prenatal care later than their U.S.-born counterparts, but do not have worse birth outcomes. The sharpest contrasts are not among Hispanics but between non-Hispanic black and non-Hispanic white women born in the same place. CONCLUSIONS: Ethnicity and birthplace affect prenatal care and birthoutcomes but are probably not as significant as racial differences. Poor outcomes without elevated newborn costs may indicate less access to high-quality neonatal care among some ethnic groups.Other Abstract Vital statistics data linked with hospital discharge files for single, live-born infants delivered in New Jersey (US) in 1989-90 were used to examine the effects of Hispanic ethnicity on prenatal care utilization, low birth weight, infant mortality,and newborn hospitalization costs. The findings indicate that disparities by race may be at least as important as variations in birthplace and ethnicity. Puerto RicanWhite women who gave birth in New Jersey were twice as likely, relative to their US-born non-Hispanic White counterparts, to have a low-birth-weight infant and to have an infant who died in the first year of life. In addition, their newborn hospitalization costs were 25% higher than those of US-born non-Hispanic White women. Women of Puerto Rican descent, regardless of whether they were born in the US, initiated prenatal care later than all other Whites, except the infants born in Mexico, and their infants had the highest rates of low birth weight and mortality among all Whites. Although the multivariate results indicated that ethnic Puerto Rican Black women begin prenatal care earlier and have better birth outcomes than non-Hispanic Blacks, the descriptive statistics showed that Puerto Rican Blacks and Whites have similar levels of prenatal care use and birth outcomes. Enhanced understanding of the sources of these racial disparities is important for the designof policies to improve birth outcomes. Poor outcomes without concomitant increases in hospitalization costs may be a sign of low access to high-quality neonatal care.
<4>Unique Identifier 9702272Authors Boozang KM.Institution Health Law & Policy Program, Seton Hall University School of Law, USA.Title Western medicine opens the door to alternative medicine. [Review] [165 refs]Source American Journal of Law & Medicine. 24(2-3):185-212, 1998.
<5>Page 2

601-772.txtUnique Identifier 9681286Authors Tumiel LM. Buck GM. Zayas LE. Jaen CR.Institution Department of Social and Preventive Medicine, School of Medicine and Biomedical Sciences, State University of New York at Buffalo, USA. [email protected] Unmasking adverse birth outcomes among Hispanic subgroups.Source Ethnicity & Disease. 8(2):209-17, 1998.Abstract The 1988 Upstate New York Live Birth Certificate was the first to record Hispanic ethnicity and country of origin. This registry was used to compare low birthweight and preterm delivery among non-Hispanic white, non-Hispanic black, and Hispanic infants. Risk of low birthweight and preterm delivery was assessed for Hispanics by country of origin. Unconditional backward elimination logistic regression analysis, controlling for confounders was used to assess risk of low birthweight and preterm delivery of Hispanic subgroups compared to non-Hispanic white and non-Hispanic blackmothers. The data showed that non-Hispanic black mothers are at greatest risk of lowbirthweight and preterm delivery. Hispanics as a group have rates similar to non-Hispanic white mothers, although risk of preterm delivery and low birthweight differs among Hispanic ethnic subgroups. This study supports the need to assess Hispanic subgroups separately rather than as a single entity.
<6>Unique Identifier 9672734Authors Mitchell P. Malak A. Small D.Institution Transcultural Mental Health Centre, Cumberland Hospital, Parramatta, New South Wales, Australia. [email protected] Bilingual professionals in community mental health services.Source Australian & New Zealand Journal of Psychiatry. 32(3):424-33, 1998 Jun.Abstract OBJECTIVE: This paper presents results from research that explored the roles of bilingual professionals in community mental health services in the Sydney metropolitan area of New South Wales. There were two main objectives to the research: (i) to identify and describe the roles of bilingual professionals that areimportant in improving the quality of community mental health services for clients from non-English-speaking backgrounds (NESB); and (ii) to identify and describe the factors that facilitate and inhibit the conduct of these roles. METHOD: Data collection involved indepth interviews with bilingual professionals and team leadersin community mental health services and various other community health services; andvarious staff responsible for policy and service development with regard to culturaldiversity. RESULTS: Bilingual mental health workers were found to have at least fourcritical roles. These were (i) direct clinical service provision to NESB clients; (ii) mental health promotion and community development; (iii) cultural consultancy; and (iv) service development. Respondents reported that the latter three roles were seriously underdeveloped compared to the clinical service provision role. CONCLUSIONS: It is critical that service managers implement strategies to make better use of the linguistic and cultural skills of bilingual professionals. In addition to their role in clinical service provision ways must be found to facilitate the community-focused, cultural consultancy and service development rolesof bilingual professionals employed in mental health services.
<7>Unique Identifier
Page 3

601-772.txt 9651636Authors Navarro AM. Senn KL. McNicholas LJ. Kaplan RM. Roppe B. Campo MC.Institution Department of Family and Preventive Medicine, University of California, San Diego,La Jolla 92093-0622, USA.Title Por La Vida model intervention enhances use of cancer screening tests among Latinas.Source American Journal of Preventive Medicine. 15(1):32-41, 1998 Jul.Abstract OBJECTIVE: To describe the short-term impact of the intervention known as Por La Vida (PLV) on cancer screening for Latinas in San Diego, California. METHODS: Thirty-six lay community workers (consejeras) were recruited and trained to conduct educational group sessions. Each consejera recruited approximately 14 peers from thecommunity to participate in the program. The consejeras were randomly assigned to either a twelve-week cancer screening intervention group or a control group in whichthey participated in an equally engaging program entitled "Community Living Skills."Pre- and post-intervention self-report information was obtained from project participants on the use of cancer screening examinations. Outcome measures were changes in the percentages of women who had breast and cervical cancer screening test within the past year before and after the intervention occurred. Experimental and control groups were compared using t-tests. Analyses were conducted using both consejeras and participants as the unit of analysis. RESULTS: The increase in the use of the cancer screening test was higher in the PLV cancer intervention group in comparison to women in the community living skills control group. CONCLUSIONS: Key to the PLV intervention model is the identification of natural helpers in the Latinocommunity and their subsequent training in intervention based on social learning theory using culturally appropriate educational materials. The model is an effectiveand viable approach for increasing the use of cancer screening tests in Latinas of low socioeconomic level and low level of acculturation.
<8>Unique Identifier 9642902Authors Miller KE. Sabo DF. Farrell MP. Barnes GM. Melnick MJ.Institution Department of Sociology, University at Buffalo, State University of New York 14260, USA. [email protected] Athletic participation and sexual behavior in adolescents: the different worlds ofboys and girls.Source Journal of Health & Social Behavior. 39(2):108-23, 1998 Jun.Abstract Using multivariate analysis of covariance to test hypotheses about the effects of sports and sexual behavior on a sample of 611 Western New York adolescents, this study concludes that athletic participation and gender interact to influence adolescent sexual outcomes. Female athletes report significantly lower rates of sexual activity than female nonathletes; male athletes report slightly (though not significantly) higher rates than male nonathletes. The gender-specific effect of sports on sexual behavior remains, net of the impacts of race, age, socioeconomic status, quality of family relations, and participation in other extracurricular activities. This paper introduces cultural resource theory to explain how athletic participation influences both traditional cultural scripts and exchange resources, which, in turn, condition the sexual bargaining process and its outcomes for adolescents.
<9>Page 4

601-772.txtUnique Identifier 9631160Authors Delfino RJ. Ferrini RL. Taylor TH. Howe S. Anton-Culver H.Institution Department of Medicine, University of California, College of Medicine, Irvine 92697-7550, USA.Title Demographic differences in prostate cancer incidence and stage: an examination of population diversity in California.Source American Journal of Preventive Medicine. 14(2):96-102, 1998 Feb.Abstract INTRODUCTION: Geographic and racial/ethnic variability in prostate cancer incidence rates and stage distribution may be partly attributed to differences in screening and early detection. METHODS: Using California Cancer Registry data we aimed to characterize variability in prostate cancer rates statewide and to examine differences in the stage at diagnosis of prostate cancer by racial/ethnic group statewide and by census tract per capita income in San Diego County. We calculated annual average (1988-1991) age-adjusted incidence rates per 100,000 (AAIR) of prostate cancer for 49,880 men over age 34 years. Racial/ethnic groups were comparedusing incidence rate ratios (IRR) (AAIR localized plus regional stages divided by AAIR distant stage). RESULTS: Statewide, Caucasians showed a higher IRR [6.16, 95% confidence interval (CI), 6.00-6.30] than did African Americans (2.34, 95% CI, 1.89-2.89), Hispanics (3.84, 95% CI, 3.63-4.05), or Asian/others (3.61, 95% CI, 1.80-7.22). Within San Diego County, Caucasians living in higher per capita income census tracts (> or = 65th percentile) had a significantly higher IRR (8.80, 95% CI 7.84-9.89) than did lower-income tracts (5.68, 95% CI, 5.13-6.30). CONCLUSION: Findings from the present and similar studies suggest that outcomes research is needed to determine the impact of these demographic differences on prostate cancer mortality and quality of life. This is particularly important given the current controversy regarding the treatment of clinically localized prostate cancers, increasingly found through early detection, which often involve difficult choices between aggressive therapies including prostatectomy or watchful waiting.
<10>Unique Identifier 9630128Authors Alonso J. Black C. Norregaard JC. Dunn E. Andersen TF. Espallargues M. Bernth-Petersen P. Anderson GF.Institution Health Services Research Unit, Institut Municipal d'Investigacio Medica, Barcelona, Spain.Title Cross-cultural differences in the reporting of global functional capacity: an example in cataract patients.Source Medical Care. 36(6):868-78, 1998 Jun.Abstract OBJECTIVES: Patient-based health status measures have an important role to play inthe assessment of health care outcomes. Among these measures, global assessments increasingly have been used, although the understanding of the performance of these indicators and the determinants of patients responses is underdeveloped. In this study, the performance of a single-item global indicator of visual function in cataract patients of four international settings was compared. METHODS: Visual acuity and ocular comorbidity was assessed by patients' ophthalmologist using Snellen-type charts in patients referred for a first cataract surgery in the United States, Manitoba (Canada), Denmark, and Barcelona (Spain). Patients also were interviewed by telephone and asked to report overall trouble with vision on a single-item indicator ("great deal," "moderate," "a little," "none") and to completethe Visual Functioning Index (VF-14), a scale of visual function ranging from 0
Page 5

601-772.txt(worst function) to 100 (best level of function), along with other questions including the degree the patient was bothered by symptoms as measured by the Cataract Symptom Score (CSS). A total of 1,407 patients completed the clinical examination and the preoperative interview. RESULTS: Distribution of overall troublewith vision varied across the sites, with the proportion of patients reporting a great deal of trouble ranging from 21.7% to 37.9%. In all sites, patients reporting more trouble with vision tended to show a poorer age-adjusted and sex-adjusted visual acuity. The proportion of patients reporting great deal of trouble with vision was higher in the groups with worse visual acuity (P < 0.001). In multivariate analysis, after controlling for clinical and sociodemographic factors, the patients from Manitoba (OR = 0.32, 95% CI = 0.20, 0.51) and those from Barcelona(OR = 0.33, 95% CI = 0.20, 0.56) were less likely to report a great deal of trouble with their vision (P < 0.01) than the Danish and US patients. No such differences were found among the US patients from three sites. CONCLUSIONS: There is international variation in the self-reporting of global vision-related functional capacity that is not explained by clinical or sociodemographic factors, which may bebecause of cultural differences. International comparisons of patient-based health outcomes should not rely only on single-item indicators until there is convincing evidence of their cross-cultural equivalence.
<11>Unique Identifier 9615562Authors Brown ME. Bindman AB. Lurie N.Institution University of Minnesota, USA.Title Monitoring the consequences of uninsurance: a review of methodologies. [Review] [89 refs]Source Medical Care Research & Review. 55(2):177-210, 1998 Jun.Abstract The proportion of the United States population without health insurance continues to grow. How will this affect the health of the nation? Prior research suggests thatthe uninsured are at risk for poor health outcomes. They use fewer medical services and have higher mortality rates than do insured persons. The episodic nature of uninsurance and its prevalence among disadvantaged groups makes it difficult to ascertain the health effects of uninsurance. The goal of this review is to assist researchers and policy makers in choosing methodologies to assess the effects of uninsurance. It provides a compendium of methods that have been used to examine the health consequences of uninsurance, the populations in which these methods have beenused, and the strengths and weaknesses of different approaches. The review highlights the need for more longitudinal studies that focus on community-based samples of the uninsured. [References: 89]
<12>Unique Identifier 9600513Authors Heuser RR.Title Success with carotid stenting: a stroke of good luck or the wave of the future?[comment].Source Catheterization & Cardiovascular Diagnosis. 44(1):7-8, 1998 May.
<13>Unique Identifier 9598709
Page 6

601-772.txtAuthors Arroyo JA. Westerberg VS. Tonigan JS.Institution Department of Psychology, University of New Mexico at Albuquerque & Center on Alcoholism, Substance Abuse and Addictions, 87106, USA.Title Comparison of treatment utilization and outcome for Hispanics and non-Hispanic whites.Source Journal of Studies on Alcohol. 59(3):286-91, 1998 May.Abstract OBJECTIVE: To examine the use of formal alcohol treatment and Alcoholics Anonymous(AA) by Hispanics and non-Hispanic whites, and to compare ethnic groups on posttreatment functioning. METHOD: Data from a publicly funded substance abuse treatment center in New Mexico were used to investigate possible differences betweenHispanic (n = 46) and non-Hispanic white (n = 62) men (n = 76) and women (n = 32) onpercent days alcohol therapy and AA attendance for 6 months after study recruitment.RESULTS: Hispanic clients were more often male (80% vs 63%), had fewer years of education (mean = 11.6 vs 12.6) and were less likely to live alone (7% vs 29%) than were non-Hispanic white clients. The heavy drinking (drinks per drinking day mean = 16.7; standard drink units in prior 90 days mean = 941.00) and few abstinent days (mean = 0.44) that characterized both groups at intake improved over time with Hispanics engaging in more formal alcohol therapy sessions but attending fewer AA meetings than non-Hispanic whites over the course of 6 months of follow-up. Attendance at treatment and AA were separately associated with decreased intensity and quantity of alcohol use, but not abstinent days, for both ethnic groups. CONCLUSIONS: Hispanic and non-Hispanic white clients used somewhat different treatment strategies to deal with alcohol-related problems, these paths, however, ultimately resulted in similar posttreatment drinking outcomes (frequency, intensityand quantity of alcohol consumption).
<14>Unique Identifier 9595248Authors Ma J. Markides KS. Perkowski LP. Stroup-Benham CA. Lichtenstein M. Goodwin JS.Institution Gilead Sciences, Foster City, CA, USA.Title Impact of selected medical conditions on self-reported lower-extremity function inMexican-American elderly.Source Ethnicity & Disease. 8(1):52-9, 1998 Winter.Abstract OBJECTIVE: To examine the independent impact of common medical conditions on lower-extremity function in Mexican-American elderly. DESIGN: Cross-sectional study using a probability sample of non-institutionalized Mexican Americans aged 65 or older. SETTING: The five Southwestern states, Texas, New Mexico, Arizona, Colorado and California. PARTICIPANTS: All subjects were interviewed in person (n = 2,873) orby proxy (n = 177) in their homes during late 1993 and early 1994. MAIN OUTCOME MEASURES: Respondents were asked whether they could perform four activities related to lower-extremity function without help: walking across a small room, getting from a bed to a chair, walking up and down stairs, and walking half a mile. A summary measure of lower body disability created from these four items was regressed on seven common medical conditions plus five control variables using multiple logistic regression. RESULTS: Adjusted Odds Ratios (OR) suggested that impaired lower-extremity function was associated with previous diagnosis of hip fracture (OR = 4.28), stroke (OR = 3.47), lower extremity arthritis (OR = 2.60), heart attack (OR= 2.29), diabetes (OR = 2.03) and obesity (OR = 1.50). Impaired lower-extremity function was significantly associated with older age (75+ years old), gender (female) and marital status (unmarried). In addition, there was a linear increase in
Page 7

601-772.txtthe risk of function loss by number of medical conditions. CONCLUSIONS: It appears that Mexican-American elderly diagnosed with medical conditions, especially stroke and hip fracture, have a high risk for lower-extremity dysfunction. These findings have implications for efforts to prevent or reduce lower-extremity dysfunction, as well as for the provision of community-based long-term care services for Mexican-American elderly.
<15>Unique Identifier 9596068Authors Arocho R. McMillan CA.Institution Outcomes Research, Pfizer Pharmaceuticals, New York, New York 10017, USA.Title Discriminant and criterion validation of the US-Spanish version of the SF-36 Health Survey in a Cuban-American population with benign prostatic hyperplasia.Source Medical Care. 36(5):766-72, 1998 May.Abstract OBJECTIVES: The study tested the validity of the Medical Outcomes Study 36-Item Short-Form (SF-36) Health Survey (originally validated in the Mexican-American population) in a different Spanish subgroup to determine whether the Spanish versionis equally applicable to the Cuban-American population. METHODS: Individuals with and without benign prostatic hyperplasia served as the study sample. The SF-36 scores of 264 individuals with benign prostatic hyperplasia were compared with thoseof 273 individuals without benign prostatic hyperplasia to determine discriminant and criterion validity. These individuals were assigned to one of the following groups: non-Hispanic subjects, Cuban subjects who took the English version, and Cuban subjects who took the Spanish version. MANOVA with planned comparisons was used for this analysis. RESULTS: In all three culture/language groups, the quality-of-life scores of individuals without benign prostatic hyperplasia were significantly different than those of benign prostatic hyperplasia individuals. These results demonstrated that the English and Spanish versions can differentiate between individuals with and without benign prostatic hyperplasia. Moreover, the quality-of-life scores of Cuban subjects with and without benign prostatic hyperplasia who took the English version were statistically similar to those of their counterparts who took the Spanish version. CONCLUSIONS: The US-Spanish versionof the SF-36 appears to be valid when used to measure health status in Cuban-American subjects with benign prostatic hyperplasia. Further studies should beconducted to verify the validity of the US-Spanish version of the SF-36 for other health conditions.
<16>Unique Identifier 9596059Authors Handler A. Rosenberg D. Raube K. Kelley MA.Institution Maternal and Child Health Training Program of the University of Illinois School ofPublic Health Community Health Sciences Division, Chicago 60612, USA.Title Health care characteristics associated with women's satisfaction with prenatal care.Source Medical Care. 36(5):679-94, 1998 May.Abstract OBJECTIVES: The objective of this study was to explore the relation between prenatal care characteristics and satisfaction among Medicaid recipients. METHODS: African-American (n = 75) and Mexican-American (n = 26) nonadolescent primiparous pregnant women who had at least three prenatal care visits participated in a
Page 8

601-772.txt25-minute telephone survey that asked them about satisfaction with prenatal care (art of care, technical quality, physical environment, access, availability and efficacy); prenatal care characteristics (practitioner attributes, service availability, and features of the delivery of care); and, personal characteristics (sociodemographics, health status and behaviors, and pregnancy-related variables). Univariate and multivariable analyses were conducted to explore the relations between personal characteristics and satisfaction and between care characteristics and satisfaction. RESULTS: For the overall sample, the following prenatal care characteristics were associated with increased satisfaction: having procedures explained by the provider, short waiting times at the prenatal care site, the availability of ancillary services, and reporting that the prenatal care practitioner was male. When examining the data by ethnicity, whether the provider explained procedures was the most important determinant of satisfaction for both African-American and Mexican-American women. CONCLUSIONS: Knowledge of the care characteristics that impact low-income pregnant women's satisfaction can be utilizedto alter service delivery to increase use of prenatal care and ultimately to improveperinatal outcomes.
<17>Unique Identifier 9586343Authors Jarama SL. Reyst H. Rodriguez M. Belgrave FZ. Zea MC.Institution Department of Psychology, George Washington University, Washington, DC 20052, USA.Title Psychosocial adjustment among Central American immigrants with disabilities: an exploratory study.Source Cultural Diversity & Mental Health. 4(2):115-25, 1998.Abstract This is an exploratory study that investigated factors influencing the psychosocial adjustment of Central American immigrants with disabilities. The relationships between stress, and perception of disability severity and (a) depression and (b) anxiety were assessed. Furthermore, this study investigated whether social support moderated the impact of stress and severity of disability on depression and anxiety. Stress, severity of disability, and social support explaineda high percentage (54%) of the variance in depression. High levels of stress, increased perceptions of severity of disability, and low social support were associated with increased depression. The interactions between support and stress and between support and disability severity did not significantly add to the original model which predicted depression. Main effects were found for stress, disability severity, and the interaction between support and disability severity. Stress and social support significantly accounted for 31% of the variance in anxiety. Increased stress and decreased social support were associated with greater levels of anxiety. The interaction between support and stress did not significantly predict anxiety. Implications of the study in terms of future research and intervention programs targeting mental health outcomes for Latino immigrants with disabilities are discussed.
<18>Unique Identifier 9583421Authors Ihrig MM. Shalat SL. Baynes C.Institution Department of Veterinary Anatomy and Public Health, College of Veterinary Medicine, Texas A&M University, College Station, USA.Title A hospital-based case-control study of stillbirths and environmental exposure to arsenic using an atmospheric dispersion model linked to a geographical information
Page 9

601-772.txtsystem.Source Epidemiology. 9(3):290-4, 1998 May.Abstract Although adverse reproductive outcomes have been associated with arsenic exposure,the extent and severity of the effects of chronic inhalation of low levels of arsenic on reproduction are not known. We conducted a hospital-based case-control study of stillbirths in a central Texas community that included a facility with morethan a 60-year history of producing primarily arsenic-based agricultural products. We collected data on 119 cases and 267 controls randomly selected from healthy live-births at the same hospital and matched for year of birth. We abstracted medical and demographic data for the period January 1, 1983, to December 31, 1993, from hospital records and estimated socioeconomic status by median income from the 1990 Population and Housing Census data. We estimated arsenic exposure levels from airborne emission estimates and an atmospheric dispersion model and linked the results to a geographical information system (GIS) database. Exposure was linked by GIS to residential address at time of delivery. A conditional logistic regression model was fitted including maternal age, race/ethnicity, parity, income group, exposure as a categorical variable, and exposure-race/ethnicity interaction. The prevalence odds ratio observed for Hispanics in the high-exposure group (>100 ng perm3 arsenic) was 8.4, with a 95% confidence interval of 1.4-50.1.
<19>Unique Identifier 9579748Authors Hunt LM. Valenzuela MA. Pugh JA.Institution School of Nursing, University of Texas Health Science Center, San Antonio 78284-7947, USA.Title Porque me toco a mi? Mexican American diabetes patients' causal stories and their relationship to treatment behaviors.Source Social Science & Medicine. 46(8):959-69, 1998 Apr.Abstract This paper reports findings from an ethnographic study of self-care behaviors and illness concepts among Mexican-American non-insulin dependent diabetes mellitus (NIDDM) patients. Open-ended interviews were conducted with 49 NIDDM patients from two public hospital outpatient clinics in South Texas. They are self-identified Mexican-Americans who have had NIDDM for at least 1 yr, and have no major impairmentdue to NIDDM. Interviews focused on their concepts and experiences in managing theirillness and their self-care behaviors. Clinical assessment of their glucose control was also extracted from their medical records. The texts of patient interviews were content analyzed through building and refining thematic matrixes focusing on their causal explanations and treatment behaviors. We found patients' causal explanations of their illness often are driven by an effort to connect the illness in a direct and specific way to their personal history and their past experience with treatments. While most cite biomedically accepted causes such as heredity and diet, they elaborate these concepts into personally relevant constructs by citing Provoking Factors, such as behaviors or events. Their causal models are thus both specific to their personal history and consistent with their experiences with treatment success or failure. Based on these findings, we raise a critique of the Locus of Control Model of treatment behavior prevalent in the diabetes education literature. Our analysis suggests that a sense that one's own behavior is important to the disease onset may reflect patients' evaluation of their experience with treatment outcomes, rather than determining their level of activity in treatment.
<20>Unique Identifier 9576301
Page 10

601-772.txtAuthors Gilliland FD. Hunt WC. Key CR.Institution Department of Medicine, University of New Mexico Health Sciences Center, USA.Title Trends in the survival of American Indian, Hispanic, and Non-Hispanic white cancerpatients in New Mexico and Arizona, 1969-1994.Source Cancer. 82(9):1769-83, 1998 May 1.Abstract BACKGROUND: The burden of cancer mortality falls disproportionately on cancer patients belonging to ethnic minority groups. In the U.S., African American, Hispanic, and American Indian cancer patients are diagnosed at a more advanced stageand receive less appropriate treatment, resulting in poorer outcomes and higher mortality, than white cancer patients. The authors hypothesized that cancer control strategies based on earlier detection and more effective treatment may be most effective in increasing survival in groups with more advanced disease at diagnosis, less appropriate treatment, and lower survival. METHODS: Data collected by the New Mexico Tumor Registry, a member organization of the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute, afforded the authors anopportunity to investigate this hypothesis by studying trends in cancer survival forAmerican Indians, Hispanics, and non-Hispanic whites. The authors examined temporal trends and ethnic disparities in survival for in situ and invasive incident cancer cases at 25 sites diagnosed from 1969 through 1994 in New Mexico residents and in American Indians residing in Arizona. RESULTS: The distribution of stage became morefavorable and the percentage of patients receiving appropriate treatment increased for all three ethnic groups during the study period. Survival improved for patients with cancer at most sites in each ethnic group; however, because the increase in survival was greater for non-Hispanic whites than for American Indians or Hispanics,the number of sites associated with disparities in survival among non-Hispanic whites, American Indians, and Hispanics increased. Differences in the distribution of age, gender, stage at diagnosis, histologic grade, and treatment did not completely explain the improved survival or the ethnic disparities regarding survival. CONCLUSIONS: Increased cancer control efforts were associated with earlierdiagnosis, more patients receiving appropriate therapy, and improved survival for non-Hispanic whites, American Indians, and Hispanics. However, the improvement was greatest for non-Hispanic whites, and disparities in survival results for the different ethnic groups widened over the period of study. Cancer control strategies need to address the specific social, cultural, and biologic prognostic factors that affect different ethnic groups if disparities in outcomes are to be reduced.
<21>Unique Identifier 9572007Authors Sue S.Institution Department of Psychology, University of California, Davis 95616-8686, USA. [email protected] In search of cultural competence in psychotherapy and counseling.Source American Psychologist. 53(4):440-8, 1998 Apr.Abstract The characteristics involved in cultural competency in psychotherapy and counseling have been difficult to specify. This article describes attempts to study factors associated with cultural competency and addresses 3 questions. First, is ethnic match between therapists and clients associated with treatment outcomes? Second, do clients who use ethnic-specific services exhibit more favorable outcomes than those who use mainstream services? Third, is cognitive match between therapistsand clients a predictor of outcomes? The research suggests that match is important in psychotherapy. The cultural competency research has also generated some
Page 11
601-772.txtcontroversy, and lessons learned from the controversy are discussed. Finally, it is suggested that important and orthogonal ingredients in cultural competency are therapists' scientific mindedness, dynamic-sizing skills, and culture-specific expertise.
<22>Unique Identifier 9567580Authors Amodeo M. Robb N.Institution Boston University School of Social Work, USA.Title Evaluating outcomes in a substance abuse training program for Southeast Asian human service workers: problems in measuring change cross-culturally.Source Journal of Drug Education. 28(1):53-63, 1998.Abstract The following article describes the evaluation challenges faced in a cross-cultural substance abuse training program. Non-Southeast Asian instructors designed and taught courses for Cambodian and Vietnamese human service workers over a two-year period. Although cultural considerations were a central focus in the design of the program, instructors underestimated the difficulty of modifying standard questionnaires for use with Southeast Asian participants. As a consequence,the formal evaluation process had limited benefit but several insights were gleaned through alternative evaluation methods.
<23>Unique Identifier 9564212Authors Thompson M. Curry MA. Burton D.Institution Oregon Health Sciences University, Portland, USA.Title The effects of nursing case management on the utilization of prenatal care by Mexican-Americans in rural Oregon.Source Public Health Nursing. 15(2):82-90, 1998 Apr.Abstract This quasi-experimental, retrospective study used birth certificate and medical record data to evaluate the effectiveness of the Rural Oregon Minority Prenatal Program (ROMPP) in improving patterns of prenatal care utilization by rural-dwelling, low-income, Mexican-American women at risk of poor pregnancy outcomes. The ROMPP intervention provided nursing case management services and peer outreach to pregnant Mexican-American women in a rural Oregon community. The intervention group had more prenatal visits in months 2, 3, 4, 5, 6, and 7 than the comparison group (P < 0.05). The intervention group had a similar number of emergency room (ER) visits, but had more respiratory diagnoses and fewer urinary tract infections. ROMPP women had more inpatient admissions and longer lengths of stay. No differences were found in the initiation of prenatal care or the total number of prenatal care visits, nor in the timing of screening serum glucose tests. The intervention should be expanded to address the persistent attitudinal, financial, transportation and language barriers to adequate prenatal care. Nurses should increase their cultural competency and sharpen their clinical focus on advocacy, marketing, facilitation of relationships between community groups, and community organizing.
<24>Unique Identifier
Page 12
601-772.txt 9559016Authors Kaegi E.Institution National Cancer Institute of Canada, Toronto, Ont.Title Unconventional therapies for cancer: 1. Essiac. The Task Force on Alternative Therapies of the Canadian Breast Cancer Research Initiative. [Review] [27 refs]Source CMAJ Canadian Medical Association Journal. 158(7):897-902, 1998 Apr 7.Abstract Physicians and patients have been frustrated by the lack of reliable information on unconventional therapies. To help fill this gap in the area of breast cancer therapy, the Canadian Breast Cancer Research Initiative formed a task force to advise it on how best to promote research into unconventional therapies. As part of the work of the task force, a review of the available literature was carried out foreach of the following products: Essiac, green tea, Iscador, hydrazine sulfate, vitamins A, C and E, and 714-X. The first article in this series on unconventional therapies for cancer describes the methodology used to obtain and evaluate the information and provides a summary of the findings on Essiac. Subsequent articles will cover the other products. For most of the products reviewed, there has been some indication of possible benefit but no definitive evidence. Innovative and collaborative research needed to meet the information needs of growing numbers of patients and their physicians is now being sponsored by the Canadian Breast Cancer Research Initiative. Open communication between patients and physicians is also necessary for the maintenance of an appropriate therapeutic partnership and for the identification and control of side effects. The Ontario Division of the Canadian Cancer Society, a partner in the Canadian Breast Cancer Research Initiative, supported the preparation of a patient-information piece on unconventional therapiesto accompany the series. This item will assist patients who are considering such therapies and will promote open communication between patients and their physicians.[References: 27]
<25>Unique Identifier 9560060Authors Satish S. Stroup-Benham CA. Espino DV. Markides KS. Goodwin JS.Institution Department of Internal Medicine, The University of Texas Medical Branch, Galveston77555-0460, USA.Title Undertreatment of hypertension in older Mexican Americans.Source Journal of the American Geriatrics Society. 46(4):405-10, 1998 Apr.Abstract OBJECTIVE: To identify the prevalence of hypertension and factors associated with nontreatment and poor control of hypertension in Mexican Americans aged 65 years andolder. DESIGN: A population-based survey of older Mexican Americans conducted in 1993-1994. SETTING: Subjects residing in five Southwestern states: Texas, New Mexico, Colorado, Arizona, and California. PARTICIPANTS: An area probability sample of 3050 noninstitutionalized Mexican American men and women aged 65 and older took part in a 90-minute in-home interview, which included review of all medications taken and two sitting blood pressure measurements. OUTCOME MEASURES: Measured were previous diagnoses of hypertension, current medication for hypertension, and currentblood pressure RESULTS: Sixty-one percent of older Mexican-Americans were hypertensive, and 51% of those with hypertension were taking antihypertensive medications. Only 25% of hypertensive subjects (18% of males and 30% of females) were in good blood pressure control (i.e., systolic blood pressure < 140 mm Hg and diastolic blood pressure < 90 mm Hg). In multivariate analyses, factors associated with increased likelihood of treatment included female gender (OR = 1.9), history ofheart disease (OR = 2.4), possessing a regular source of health care (OR = 2.7), and
Page 13

601-772.txthaving seen a physician two or more times in the previous year (OR = 3.8). These were also independent predictors of good blood pressure control. CONCLUSION: Nontreatment of hypertension is still a major public health concern in older MexicanAmericans. We estimate that adequate blood pressure control in this population wouldprevent approximately 30,000 adverse cardiovascular events over 10 years, affecting approximately 6% of the entire Mexican American older population.
<26>Unique Identifier 9540024Authors Johnston PS. Feig PU. Coniff RF. Krol A. Davidson JA. Haffner SM.Institution Bayer Pharmaceuticals, West Haven, Connecticut, USA.Title Long-term titrated-dose alpha-glucosidase inhibition in non-insulin-requiring Hispanic NIDDM patients.Source Diabetes Care. 21(3):409-15, 1998 Mar.Abstract OBJECTIVE: To assess the long-term safety and effectiveness of a titrated dose of the alpha-glucosidase inhibitor miglitol (BAY m 1099) in Hispanic NIDDM patients. RESEARCH DESIGN AND METHODS: A 1-year double-blind randomized placebo-controlled study in which diet-treated or diet plus sulfonylurea-treated Hispanic NIDDM patients received either placebo (n = 131) or miglitol in doses of 50, 100, 150, 200mg t.i.d. (n = 254), up-titrated and down-titrated based on tolerability. Efficacy parameters included changes from baseline in HbA1c, fasting and 2-h postprandial plasma glucose and serum insulin, fasting serum lipids, and urinary albumin-to-creatinine ratio (ACR). Safety assessments consisted primarily of tabulation of adverse events and intercurrent illnesses, and of periodic laboratory determinations. RESULTS: Reductions from baseline in HbA1c levels at the 6-month (primary efficacy) endpoint were significantly greater by 0.83% in the miglitol group than in the placebo group. HbA1c reductions in the miglitol treatment group significantly exceeded those in the placebo group by 0.63, 0.73, and 0.92% at 3, 9, and 12 months of treatment, respectively. Reductions in 120-min postprandial glucoseand insulin levels were significantly greater in the miglitol group than in the placebo group at all postbaseline visits. There was little difference between treatments for changes in fasting insulin or lipid levels. Miglitol-associated reductions versus placebo in fasting plasma glucose (P = 0.0587 at 6 months) and in ACR (P = 0.0541 at 1-year) were nearly statistically significant. These efficacy results were not notably different between the 6-month endpoint, at which time the mean miglitol dose was 100 mg t.i.d., and the 1-year visit, when the mean miglitol dose was 149 mg t.i.d. Notable adverse events seen significantly more often in the miglitol group than in the placebo group were flatulence and diarrhea (or soft stools). The incidence of these gastrointestinal adverse events appeared to be dose dependent. CONCLUSIONS: Miglitol treatment of non-insulin-requiring Hispanic NIDDM patients at doses from 50 to 200 mg t.i.d. produced statistically and clinically significant reductions of HbA1c, primarily associated with reduction of glucose and insulin levels in the postprandial period, which were sustained over a year of treatment. Adverse events related to the drug's mechanism of action were common, butgenerally well tolerated. Doses above 100 mg t.i.d. were not associated with notablyenhanced efficacy in most patients.
<27>Unique Identifier 10177208Authors Millstead CM.Institution Bates County Memorial Hospital, Butler, MO 64730, USA.Title
Page 14

601-772.txt Chinese CLS sister school relationship.Source Clinical Laboratory Science. 11(1):13-7, 1998 Jan-Feb.Abstract OBJECTIVE: Establish a relationship with a Chinese CLS Program to foster cross-cultural diversity, provide for student and faculty cross-cultural exchange, scholarship, research, and improve the health care of both communities served by thecolleges. DESIGN: Information needed to develop agreement strategy was gathered by literature review, personal interviews, and direct observation in China. Based upon literature review an original list of items for discussion was developed. Discussions were held between administrators of both schools and the teaching hospital. The Chief Laboratory Technologist of the associated Chinese teaching hospital was interviewed to establish the extent of CLS students' experiences. A form for the interview was developed and the results were used during the negotiation of the final agreement. SETTING/PARTICIPANTS: A CLS faculty team member from the U.S. traveled to the Jingmen School of Nursing and Allied Medical Sciences,Jingmen City, China, Hubei Province, P.R. China to establish an agreement. Tours of six cities in China, the School, and Jingmen hospitals provided for a better understanding of the Chinese culture and the Chinese CLS program. RESULTS/CONCLUSION: Three major concerns for success of the relationship (language barriers, communication vehicles, and socialization issues) were determined and addressed in a final agreement. The components of the agreement may provide some insight for others considering such a collaborative venture. Outcomes will be more fully addressed when exchanges begin.
<28>Unique Identifier 9524810Authors Gorman-Smith D. Tolan P.Institution University of Illinois at Chicago, USA.Title The role of exposure to community violence and developmental problems among inner-city youth.Source Development & Psychopathology. 10(1):101-16, 1998 Winter.Abstract While research has well documented that urban youth are exposed to increasing rates of community violence, little is known about what increases risk for violence exposure, what protects children from exposure to violence, and what factors reduce the most negative outcomes associated with witnessing violence. This study expands on current research by evaluating the relations between exposure to violence, familyrelationship characteristics and parenting practices, and aggression and depression symptoms. Data were drawn from a sample of 245 African-American and Latino boys and their caregivers from economically disadvantaged inner-city neighborhoods in Chicago. Rates of exposure could not be predicted from family relationship and parenting characteristics, although there was a trend for discipline to be related. Exposure to community violence was related to increases in aggressive behavior and depression over a 1-year period even after controlling for previous status. Future studies should continue to evaluate the role of exposure to violence on the development of youth among different neighborhoods and communities. Implications forintervention and policy are discussed.
<29>Unique Identifier 9520963Authors Marcus AC. Kaplan CP. Crane LA. Berek JS. Bernstein G. Gunning JE. McClatchey MW.Institution
Page 15

601-772.txt AMC Cancer Research Center, Denver, CO 80214, USA.Title Reducing loss-to-follow-up among women with abnormal Pap smears. Results from a randomized trial testing an intensive follow-up protocol and economic incentives.Source Medical Care. 36(3):397-410, 1998 Mar.Abstract OBJECTIVES: This study evaluates the efficacy of two interventions designed to reduce loss-to-follow-up among women with abnormal Pap smears. METHODS: The two interventions were evaluated in two large public hospitals using a randomized 2 x 2 factorial design. One intervention involved an intensive follow-up protocol that relied on multiple attempts (mail and telephone) to contact the patient. The second intervention provided patients with economic vouchers to offset out-of-pocket expenses associated with the follow-up visits. Loss-to-follow-up was addressed by medical chart reviews and telephone interviews. RESULTS: The study population (n = 1453) was primarily Hispanic, married or otherwise living with a significant other, relatively young in age, and with no source of payment for health care. Overall, 30%of the total sample was loss-to-follow-up (i.e., no return visits). Among patients assigned to the control condition, loss-to-follow-up was 36.1% compared with 27.8% for the intensive follow-up condition, 28.8% for the voucher condition, and 29.0% for the intensive follow-up plus voucher condition. Both intervention conditions significantly improved follow-up rates. The odds ratio for intensive follow-up was 1.56 compared with 1.50 for the voucher intervention. The combined intervention condition (intensive follow-up x voucher program) did not have a significant effect after taking into account the main effects of the two interventions. Correlates of loss-to-follow-up included age (younger women had lower return rates), race/ethnicity (African American women had lower return rates), live-in relationship(women who were not married or living as married had lower return rates), and severity of the abnormal Pap smear (less severe abnormalities were associated with lower return rates). CONCLUSIONS: Both interventions were associated with moderate reductions in loss-to-follow-up in this underserved population. The implications of these findings are discussed relative to implementing cervical cancer control programs within state and local health departments.
<30>Unique Identifier 9500502Authors Cotch MF. Hillier SL. Gibbs RS. Eschenbach DA.Institution Division of Microbiology and Infectious Diseases, National Institute of Allergy and Infectious Diseases, Bethesda, Maryland, USA.Title Epidemiology and outcomes associated with moderate to heavy Candida colonization during pregnancy. Vaginal Infections and Prematurity Study Group.Source American Journal of Obstetrics & Gynecology. 178(2):374-80, 1998 Feb.Abstract OBJECTIVE: Our purpose was to determine the risk factors, physical findings, microflora, and pregnancy outcome among pregnant women with moderate to heavy vaginal growth of Candida albicans and other Candida species. STUDY DESIGN: A multicenter cohort of 13,914 women were enrolled between 23 and 26 weeks' gestation.Women completed a questionnaire, underwent a physical examination, and had genital specimens taken for culture. A subset of 1459 women were reexamined during the thirdtrimester. Pregnancy outcomes were recorded at delivery. RESULTS: The prevalence of moderate to heavy Candida colonization at midgestation was 10%. Colonized women, 83%of whom carried C. albicans, were more likely to be black or Hispanic, unmarried, a previous oral contraceptive user, and to manifest clinical signs indicative of Candida carriage. Candida colonization was positively associated with Trichomonas vaginalis, group B streptococci, and aerobic Lactobacillus and was not associated with adverse pregnancy outcome. CONCLUSION: These results suggest that Candida colonization is not associated with low birth weight or preterm delivery.
Page 16

601-772.txt
<31>Unique Identifier 9445324Authors Frey JL. Jahnke HK. Bulfinch EW.Institution Division of Neurology, Barrow Neurological Institute, Phoenix, Arizona, USA.Title Differences in stroke between white, Hispanic, and Native American patients: the Barrow Neurological Institute stroke database.[see comment][erratum appears in Stroke 1998 Jun;29(6):1257].Source Stroke. 29(1):29-33, 1998 Jan.Abstract BACKGROUND AND PURPOSE: Identification of specific features of stroke in minority populations should lead to more effectively focused treatment and prevention. METHODS: We examined 1290 white (WHI), 242 Hispanic (HIS), 83 Native American (NA), and 101 other stroke and transient ischemic attack (TIA) patients hospitalized at the Barrow Neurological Institute from 1990 through 1996. RESULTS: Chi-square analysis detected significant (P<.05) differences as follows: (1) Stroke types--lacunes more prevalent in NA than WHI and HIS (30% versus 16% and 15%); cardioembolic more prevalent in WHI than HIS (16% versus 9%, NA 14%); hemorrhages more prevalent in HIS than WHI and NA (48% versus 37% and 27%); (2) Risk factors--hypertension more prevalent in HIS than WHI (72% versus 66%; NA 71%); diabetes more prevalent in NA than HIS and WHI (62% versus 36% and 17%); cigarette smoking more prevalent in WHI than HIS and NA (61% versus 46% and 41%); cardiac disease more prevalent in WHI than HIS (34% versus 24%; NA 27%); heavier alcohol intake in NA than HIS than WHI (43% versus 24% versus 17%). There were no significant outcome differences between races for any stroke type. ANOVA detected significantly lower mean age at stroke onset in NA than HIS than WHI (56 versus 61 versus 69 years). CONCLUSIONS: There are significant differences in prevalence of risk factors and stroke types between WHI, HIS, and NA in our hospital-based population. Although the three races appear to respond to risk factors similarly, Hispanics may be especially susceptible to hemorrhage. Further evaluation of these observations in community-based studies will be important.
<32>Unique Identifier 11660501Authors Schmidt VH.Title The politics of justice and the paradox of justification.Source Social Justice Research. 11(1):3-19, 1998 Mar.
<33>Unique Identifier 11656755Authors Herdman R. Beauchamp TL. Potts JT.Title The Institute of Medicine's report on non-heart-beating organ transplantation.Source Kennedy Institute of Ethics Journal. 8(1):83-90, 1998 Mar.Abstract In December 1997, the Institute of Medicine (IOM) released a report on medical andethical issues in the procurement of non-heart-beating organ donors. This report hadbeen requested in May 1997 by the Department of Health and Human Services (DHHS). We
Page 17

601-772.txtwill here describe the genesis of the IOM report, the medical and moral concerns that led the DHHS to sponsor it, the process of producing it, and its conclusions. The analyses, findings, and recommendations of the report are also reviewed, in particular the central issues that led to suggestions for policy changes.
<34>Unique Identifier 10437607Authors Eun KY.Institution Dept. of Nursing, College of Medicine, Hanyang University.Title [A study on the relationship between women's health status and the experience of Sanhujori, the Korean traditional non-professional postpartal care]. [Korean]Source Taehan Kanho - Korean Nurse. 36(5):74-90, 1997 Nov-Dec.Abstract This descriptive study sought to define the relationship between women's health status and the experience of Sanhujori. Korean traditional non-professional postpartal care after delivery and abortion. A convenience sample of 308 women in 7 provinces in Korea including Seoul were studied from December, 1994 to December, 1996 for two years. Mean age of respondents was 50.5 years and mean number of children was 3. The rate of abortion was 91.5% and mean frequency was 2.2 times per woman. 82% of respondents did not have Sanhujori after abortion. The period and subjective evaluation of experience of Sanhujori after delivery were decreased according to the increment of the number of childbirth. The health status implies both subjective health status women perceived and physical symptom distress women are experiencing presently. The respondents expressed the physical symptom distress as painful one. 56.7% of respondents perceived unhealthy, such as sick and 99.6% complained more than one symptom. The factors related to health status were the first and third experience of Sanhujori after delivery, such as the period and subjective evaluation whether she did Sanhujori well or not; whether or not of Sanhujori after abortion and menopause; the number of child; and age, at the level of 1% or 5% of significance statistically. The factors related to the rate of physical symptom distress were only two: the first experience of Sanhujori after delivery, especially the subjective evaluation and whether women did Sanhujori afterabortion or not, at the level of 1% or 5% of significance statistically. In conclusion, this finding reconfirmed the possible relationship between women's health status and the experience of Sanhujori after delivery & abortion. It providesa challenge to the professional care givers to research further on the effects of Sanhujori on the health status, health recovery after abortion or delivery from the various aspects through the cross-sectional and longitudinal research for the refinement of the reality of Sanhujori not only as cultural phenomenon but as conceptual model for the appropriateness of intervention and qualty of care for desirable health outcomes. Besides, it is indispensable to refine and reestablish postpartal caring system by finding universal law through international & cross-cultural research on postpartal traditional care for women's life long health toward the 21C.
<35>Unique Identifier 9574146Authors Troidl H.Institution II. Lehrstuhl fur Chirurgie, Universitat zu Koln, Chirurgische Klinik Koln-Merheim.Title [Clinical research. Socioeconomic factors exemplified by endoscopic surgery]. [Review] [56 refs] [German]
Page 18

601-772.txtSource Langenbecks Archiv fur Chirurgie - Supplement - Kongressband. 114:300-22, 1997.
<36>Unique Identifier 9549993Authors Atchison KA. Gift HC.Institution Section of Public Health Dentistry, UCLA School of Dentistry 90095-1668, USA.Title Perceived oral health in a diverse sample.Source Advances in Dental Research. 11(2):272-80, 1997 May.Abstract Measures of perceived oral health represent subjective, individual perspective of one's health. One measure commonly used is the single-item perceived oral health rating: How would you rate your overall oral health? These analyses examine the associations among age, ethnicity, and perceived oral health within the context of acomprehensive battery of 21 predisposing, enabling, and need variables. The study ofcompares the adult data from three United States research locations of the International Collaborative Study of Oral Health Outcomes (ICS-II). Only social survey data were used for this analysis. The multiple regression model explains over30% of the variance in perceived oral health, with R squares ranging from 0.324 for Indian Health Service sites to 0.391 for San Antonio. The most important significantpredictors include ethnic group, education, perceived general health status, being edentulous or not having a partial denture, having no oral pain, fewer oral symptoms, and having one or more dental visits. The predictors of positive perceivedoral health for the diverse groups highlight interesting age and ethnic differences.The only universal predictor for the middle-aged adults was having fewer oral symptoms. For the older adults, being edentulous or not having a partial denture wasthe only universal predictor. The findings suggest that perceived oral health may bea useful outcome measure in dentistry because of its relation to predisposing sociodemographics and dental utilization.
<37>Unique Identifier 9549990Authors Davidson PL. Rams TE. Andersen RM.Institution Department of Health Services, School of Public Health, University of California, Los Angeles 90095, USA.Title Socio-behavioral determinants of oral hygiene practices among USA ethnic and age groups.Source Advances in Dental Research. 11(2):245-53, 1997 May.Abstract In this study, socio-behavioral determinants of oral hygiene practices were examined across several dentate ethnic and age groups. Oral hygiene scale scores were constructed from toothbrushing and dental floss frequencies self-reported by population-based samples of middle-aged (35-44 years) and older (65-74 years) dentate adults representing Baltimore African-American and White, San Antonio Hispanic and non-Hispanic White, and Navajo and Lakota Native American persons participating in the WHO International Collaborative Study of Oral Health Outcomes (ICS-II) survey. Female gender, education, certain oral health beliefs, household income, and the presence of a usual source of care were revealed with multivariate analysis to show a significant positive relationship with higher oral hygiene scale scores (indicating better personal oral hygiene practices). Other socio-behavioral variables exhibited a more varied, ethnic-specific pattern of association with oral
Page 19

601-772.txthygiene scale scores.
<38>Unique Identifier 9549988Authors Atchison KA. Davidson PL. Nakazono TT.Institution Section of Public Health Dentistry, School of Dentistry, University of California,Los Angeles 90095, USA.Title Predisposing, enabling, and need for dental treatment characteristics of ICS-II USA ethnically diverse groups.Source Advances in Dental Research. 11(2):223-34, 1997 May.Abstract Personal characteristics (predisposing, enabling, and need) are described for the population-based samples of adults interviewed in the International Collaborative Study of Oral Health Outcomes (ICS-II) USA research locations. Differences in samplecharacteristics are compared by ethnic group (African-American, Native American, Hispanic, and White) and age cohort (35-44 and 65-74 years old) by means of Bonferroni multiple-means tests and Student's t tests. Differences in the personal characteristics of these diverse comparison groups abound. Bivariate results indicated that White adults from both age cohorts had higher socioeconomic levels, more positive self-rated health status, and greater proportions of individuals with dental benefits. Lakota adults from both age cohorts reported lower self-rated health status and were most likely to report total tooth loss. Hispanic persons weresignificantly less likely to report a usual source of dental care or dental benefits. Need for dental treatment (oral pain and oral symptoms index) was generally higher amng Native American and Hispanic groups. It is critical that the differences highlighted between the among these groups be studied in appropriate strategies for improving the oral health of USA adults are to be determined.
<39>Unique Identifier 9549986Authors Reifel NM. Davidson PL. Rana H. Nakazono TT.Institution Indian Health Service, United States Public Health Service, Sacramento, CA, USA.Title ICS-II USA research locations: environmental, dental care delivery system, and population sociodemographic characteristics. [Review] [26 refs]Source Advances in Dental Research. 11(2):210-6, 1997 May.Abstract Secondary data sources are used to describe the ICS-II USA research locations in terms of external environment, dental care delivery system, and population sociodemographics. The Native American reservations located in Arizona, New Mexico, and South Dakota were rural, while the other research locations were primarily urban. Baltimore, Maryland, and the Native American communities had fluoridated water, but San Antonio did not. Dental services in Baltimore and San Antonio were predominantly financed by private sources, with a small public health component. Dental care services in Native American communities were largely Indian Health Services (IHS) financed by the US Government. Each geographical area exhibited diverse characteristics indicating unique challenges for the delivery of community and clinical dental services. [References: 26]
<40>Unique Identifier
Page 20
601-772.txt 9505018Authors Dwivedi S. Jauhari R.Institution Department of Medicine, University College of Medical Sciences, Delhi.Title Beneficial effects of Terminalia arjuna in coronary artery disease.Source Indian Heart Journal. 49(5):507-10, 1997 Sep-Oct.Abstract Effect of Terminalia arjuna on angina pectoris, congestive heart failure and left ventricular mass was studied in patients of myocardial infarction with angina and/orischaemic cardiomyopathy. Bark stem powder of T. arjuna, 500 mg 8 hourly was administered to 10 patients of postmyocardial infarction angina and two patients of ischaemic cardiomyopathy, in a dose of 500 mg 8 hourly postoperatively, for a periodof three months (Group A). These patients were also on conventional treatment comprising of nitrates, aspirin and/or calcium channel blockers. Twelve age-, sex-, body mass index- and ECG-matched patients of postmyocardial infarction angina receiving only conventional treatment served as controls (Group B). Significant reduction in anginal frequency was noted in both groups (3.5 +/- 1.98 to 1.08 + 1.08per day vs 3.10 + 0.72 to 1.17 + 0.84 per day). However, only Group A patients showed significant improvement in left ventricular ejection fraction (42.25 + 9.96 to 52.67 + 12.32% vs 51.83 + 5.99 to 49.83 + 2.52%) and reduction in left ventricular mass (159.18 + 51.11 to 127.47 + 52.40 gm/m2 vs 159.11 + 38.92 to 160.78+ 54.23 gm/m2) on echocardiography following three months of therapy. Both patients with ischaemic cardiomyopathy showed significant symptomatic relief in coronary heart failure from NYHA class III to NYHA class I. Prolonged administration of T. arjuna did not show any adverse effects on renal, hepatic and haematological parameters. The potential of T. arjuna to improve left ventricular ejection fractionand reduce left ventricular mass in coronary artery disease needs to be harnessed.
<41>Unique Identifier 9492974Authors Kagawa-Singer M. Wellisch DK. Durvasula R.Institution UCLA School of Public Health and Asian American Studies, Los Angeles, CA 90095-1772, USA. [email protected] Impact of breast cancer on Asian American and Anglo American women.Source Culture, Medicine & Psychiatry. 21(4):449-80, 1997 Dec.Abstract This pilot study constitutes the first exploration of the impact of breast cancer on Asian American women. Three hypotheses guided this study: (1) Asian American women would choose breast conserving therapy and breast reconstruction at a lower rate than the Anglo American women due to cultural differences in body image, (2) Asian American women with breast cancer would express psychological distress somatically and Anglo American women would express distress emotionally, and acculturation levels of the Asian American women would modify the expressions of distress such that women with high acculturation will express distress more emotionally and less acculturated women would express distress more somatically, and(3) Asian American women would seek assistance for psychosocial problems at a significantly lower rate than Anglo women. Ethnicity, age, and levels of acculturation were found to be significant variables that had to be considered simultaneously. The three hypotheses were only partially supported: (1) Asian American women chose breast conserving therapy and adjuvant therapy at a significantly lower rate than the Anglo American women, (2) Contrary to the hypothesis, somatization did not appear to be a dominant form of symptom presentation for Asian American women regardless of level of acculturation, and (3) Asian American women sought professional assistance for psychosocial problems at a
Page 21

601-772.txtsignificantly lower rate than Anglo women. Asian American women reported using different modes of help-seeking behavior for emotional concerns and receiving different sources of social support than the Anglo American women. Cultural interpretations of the findings are offered to explain the differences in the physical, emotional, and social responses to the breast cancer experience of Asian American women compared with the Anglo Americans, and notably between the Chinese- and Japanese Americans as well. The findings of this study warrant more refined exploration in order to improve the medical, psychological and social outcomes for Asian American women with breast cancer.
<42>Unique Identifier 9481237Authors Gonzalez-Calvo J. Gonzalez VM. Lorig K.Institution Women's Studies Program, California State University, Fresno 93740-0078, USA.Title Cultural diversity issues in the development of valid and reliable measures of health status.Source Arthritis Care & Research. 10(6):448-56, 1997 Dec.Abstract The development of instruments for use in culturally diverse settings and populations really involves much more than mere translation. Measurements must be tested for content validity and appropriate meaning among members of the group to bestudied. Attention to issues of validity, reliability, and cross-cultural differences will lead to effective assessment, culturally competent health care, andthe enhancement of the client/provider relationship. The concerns surrounding the use of quantitative measurement in diverse cultural groups are substantial. While the refinement of scales to meet the needs of various groups is a challenging task, such effort is essential to the diagnosis of disease, determination of health status, and the measurement of health outcomes in the diverse subgroups of this country's population.
<43>Unique Identifier 9472591Authors Voltz R. Akabayashi A. Reese C. Ohi G. Sass HM.Institution Department of Neurology, Klinikum Grosshadern, Munich.Title Organization and patients' perception of palliative care: a crosscultural comparison.Source Palliative Medicine. 11(5):351-7, 1997 Sep.Abstract The hospice model of care for patients with advanced diseases exists in almost allindustrialized countries. To date, there have been no international or crossculturalcomparisons of the organization and patient outcomes associated with hospice services in different parts of the world. This survey evaluated 159 patients in the USA, Germany and Japan. There were differences between countries in the time of first contact, who recommended palliative care first, the underlying diagnoses, the location of patients, and how consent for hospice care was obtained. Across all countries, there were similar levels of comfort and satisfaction with care. We conclude that the hospice philosophy addresses the basic needs of dying patients which are independent of cultural background, but may be adapted to very different cultures.
Page 22

601-772.txt<44>Unique Identifier 9470265Authors Morgan DL. Slade MD. Morgan CM.Institution School of Education, Flinders University of South Australia.Title Aboriginal philosophy and its impact on health care outcomes.Source Australian & New Zealand Journal of Public Health. 21(6):597-601, 1997 Oct.Abstract Philosophical perspective is an important factor influencing the health and healthcare outcomes of Aboriginal Australians. To date, the nature of the Aboriginal perspective and its differences from mainstream European thinking have been poorly understood. The negative impact that this has on the health and health care of Aboriginal people has been seriously neglected. We outline some of the important features of the philosophical perspective of Aboriginal Australians. We suggest waysin which the recognition of these views can inform changes in treatment settings andmethods that can contribute to improvements in the health care outcomes of Aboriginal Australians.
<45>Unique Identifier 9467706Authors English PB. Kharrazi M. Guendelman S.Institution Public Health Institute, Emeryville, CA 94608-2008, USA.Title Pregnancy outcomes and risk factors in Mexican Americans: the effect of language use and mother's birthplace.Source Ethnicity & Disease. 7(3):229-40, 1997 Autumn.Abstract Effects of acculturation have been thought to contribute adversely to poor reproductive health in Mexican immigrants, and a traditional Mexican orientation hasbeen hypothesized to be protective against poor birth outcomes. A population-based cross-sectional study of 4404 births of Mexico-born and U.S.-born Mexican-American women was conducted in California in 1992 to examine the effect of language use (as a proxy measure of acculturation) on reproductive outcomes. Utilizing birth certificates, supplemental questionnaires, and 1990 U.S. Census data, the study analyzed differences in the proportions of pregnancy risk factors, low birth weight infants, and preterm deliveries in six nativity/language subgroups. Compared to U.S.-born English-speakers, U.S.-born Spanish-speakers had a higher risk profile andMexico-born English-speakers had a lower risk profile for adverse pregnancy outcomes. After controlling for covariates, U.S.-born Spanish-speakers had the highest odds for low birth weight (OR = 1.98, 95% C.I. = 1.00, 3.93) and Mexico-bornEnglish-speakers had the lowest odds for preterm delivery (OR = 0.70, 95% C.I. = 0.35, 1.40) compared to U.S.-born English-speakers. These nativity/language differences in risk profiles and pregnancy outcomes suggest that Mexican Americans do not experience a simple negative mode of adaptation to U.S. society, but rather acomplex process of positive and negative acculturation, which may be dependent on socio-economic conditions or selection factors related to immigration.
<46>Unique Identifier 9451587Authors Bamberg R. Joiner CL.Title
Page 23

601-772.txt Strategic planning in a school of health related professions: organizational transformation for the future.Source Journal of Allied Health. 26(4):169-76, 1997 Fall.Abstract The School of Health Related Professions (SHRP) at The University of Alabama at Birmingham (UAB) has been in existence for over a quarter of a century. During this time, it expanded and grew to offering 34 individual programs at the time of its silver anniversary. A concerted strategic planning process over two years has resulted in the School pursuing major organizational transformations to better alignitself with the rest of the University's academic health center, to maximize its resources, and to refine its niche in academia. The strategic planning process used and major outcomes are described for the potential benefit of other schools of health related professions desiring to pursue introspection for future survival.
<47>Unique Identifier 9439937Authors Lavee Y. Ben-David A. Azaiza F.Institution Center for Research and Study of the Family, School of Social Work, University of Haifa, Mount Carmel, Israel.Title Israeli and Palestinian families in the peace process: sources of stress and response patterns.Source Family Process. 36(3):247-63, 1997 Sep.Abstract The Israeli-Palestinian peace process is characterized by its unknown outcomes andconsequences for the families involved. The purpose of this study was to identify family processes under conditions of prolonged uncertainty. Data were collected fromboth Israeli and Palestinian families in the West Bank by means of semi-structured interviews. Qualitative and quantitative analyses showed cross-cultural differences in the perception of the situation; different kinds of concerns and sources of stress; different coping responses; and differences in dyadic interaction patterns and intrafamily processes. The findings are discussed in social-contextual terms, particularly the ways in which political and cultural contexts shape the perception of the situation and family processes under prolonged stressful conditions.
<48>Unique Identifier 9437466Authors Fortinsky RH. Hazuda HP. Larson EB. Lindeman DA. Mullican CA. Tetzloff I. Wetle T.Institution Department of Medicine, Case Western Reserve University School of Medicine, Cleveland, Ohio 44106-6033, USA.Title Principles underlying selection of outcomes in Alzheimer disease research.Source Alzheimer Disease & Associated Disorders. 11 Suppl 6:184-5, 1997.
<49>Unique Identifier 9437460Authors Hazuda HP.Institution
Page 24

601-772.txt Department of Medicine, University of Texas, Health Science Center at San Antonio 78284-7873, USA.Title Minority issues in Alzheimer disease outcomes research.Source Alzheimer Disease & Associated Disorders. 11 Suppl 6:156-61, 1997.Abstract Taking account of cultural and linguistic variations among ethnic minority groups (the most rapidly growing segment of the U.S. elderly population) will have both conceptual and methodological impacts on Alzheimer disease outcomes research. At theconceptual level, researchers will need to evaluate whether the definition of Alzheimer disease, treatment approaches, and outcomes (anticipated and desired) central to their research are relevant or appropriate for the ethnic minorities in their target populations. The central methodological impact of cultural and linguistic diversity will be the need to use qualitative techniques as integral parts of the research process and to cross-culturally adapt English assessment instruments for use with ethnic minorities. More labor-intensive efforts will be required at all stages of the research process and, thus, higher costs will be incurred.
<50>Unique Identifier 9431287Authors Frisbie WP. Biegler M. de Turk P. Forbes D. Pullum SG.Institution Population Research Center, University of Texas at Austin 78712, USA.Title Racial and ethnic differences in determinants of intrauterine growth retardation and other compromised birth outcomes.Source American Journal of Public Health. 87(12):1977-83, 1997 Dec.Abstract OBJECTIVES: This study examined the extent of variation by race/ethnicity in the prevalence of adverse birth outcomes, whether differentials persisted after other risk factors were controlled for, and whether the direction and magnitude of relationships differed by type of outcome. METHODS: A revised system of measurement was used to estimate multinomial logistic models in a large, nationally representative US data set. RESULTS: Considerable racial/ethnic variation was found across birth outcome categories; differences persisted in the adjusted parameter estimates; and the effects of other risk factors on birth outcomes were similar as to direction, but varied somewhat in magnitude. The odds of compromised birth outcomes were much higher among African Americans than among Mexican Americans and non-Hispanic Whites. CONCLUSIONS: In addition to persistent racial inequality, we found strong adverse effects of both inadequate and "adequate-plus" prenatal care and smoking. Risk of intrauterine growth retardation was higher in the absence of medical insurance, and risk of all adverse birth outcomes was lower among mothers participating in the Special Supplemental Food Program for Women, Infants, and Children.
<51>Unique Identifier 9413309Authors Perez-Stable EJ. Napoles-Springer A. Miramontes JM.Institution Department of Medicine, University of California, San Francisco, USA.Title The effects of ethnicity and language on medical outcomes of patients with hypertension or diabetes.Source
Page 25

601-772.txt Medical Care. 35(12):1212-9, 1997 Dec.
<52>Unique Identifier 9399269Authors Kagawa-Singer M.Institution School of Public Health, University of California at Los Angeles, USA.Title Addressing issues for early detection and screening in ethnic populations. [Review] [49 refs]Source Oncology Nursing Forum. 24(10):1705-11, 1997 Nov-Dec.Abstract PURPOSE/OBJECTIVES: To describe how multicultural knowledge and skills are appliedin culturally competent practice to develop and deliver available, accessible, acceptable, and appropriate programs in early cancer detection and screening programs in ethnic communities. DATA SOURCES: Literature and clinical community practice reports. DATA SYNTHESIS: Successful community screening programs can be conducted within ethnic minority populations. Practitioners must tailor care based on salient cultural differences of the population of focus. Culturally based practice results in the (a) increased ability to think critically in community and individual assessments, (b) development of more accurate program plans and designs, and (c) increased likelihood that appropriate outcomes will be used in the evaluation of care. CONCLUSIONS: Greater cultural competence increases the accuracy of care and thereby its effectiveness, efficiency, and success in providing acceptable and optimal programs. IMPLICATIONS FOR NURSING PRACTICE: The first step in a cultural assessment is to know one's own beliefs and attitudes. The second step, conducted in parallel, requires knowledge about the groups that make up the patient and staff populations within the practice setting and then integrating thoseperspectives into practice. Practitioners then can begin the third step of negotiation of all stages of the project with members of the various communities on an equal basis that recognizes the expertise and integrity of all parties. [References: 49]
<53>Unique Identifier 9391943Authors Dyregrov A.Institution Center for Crisis Psychology, Bergen, Norway.Title The process in psychological debriefings.Source Journal of Traumatic Stress. 10(4):589-605, 1997 Oct.Abstract Critical Incident Stress Debriefings have become an intervention method used in various cultures, countries and groups following critical incidents. Although the structure of such meetings has been adequately described, utilization of the group processes involved has received less attention. A model, process debriefing (PD), based on experiences from Europe, is presented. Some differences between the currentCISD process in the United States and the Europe based model are outlined. Various factors that impact the process of debriefings are discussed with a special emphasison leadership, and implications of these group process variables for psychological debriefing are presented. It is emphasized that the continued exploration and discussion of process issues is critical to advance the understanding of the critical elements of debriefing.
Page 26

601-772.txt<54>Unique Identifier 9366864Authors Siega-Riz AM. Hobel CJ.Institution Department of Nutrition, University of North Carolina, Chapel Hill, USA.Title Predictors of poor maternal weight gain from baseline anthropometric, psychosocial, and demographic information in a Hispanic population.Source Journal of the American Dietetic Association. 97(11):1264-8, 1997 Nov.Abstract OBJECTIVE: To identify which baseline factors best predict poor maternal weight gain among Hispanics. SAMPLE: Pregnancy and outcome data collected prospectively from 4,791 Hispanic women attending public prenatal clinics in West Los Angeles, Calif, from 1983 through 1986. METHODS: Prepregnancy weight was categorized into weight status groups using body mass index (BMI). Poor total weight gain (based on amean gestational age at last measurement, which was at 35 weeks) was defined as lessthan 21 lb for women with BMI less than 26 and less than 10 lb for women with BMI of26 or greater. Analyses used Student's t test, chi 2, and multivariate regression techniques (linear and logistic). RESULTS: Poor total weight gain was identified in 29% of the women. For women who were underweight or normal weight before pregnancy, the only factor associated with increasing the risk of poor total weight gain was short stature (adjusted odds ratio [AOR] = 1.5, 95% confidence interval [CI] = 1.24,1.84). The following factors decreased the risk: being US born (AOR = 0.61, 95% CI =0.37, 1.00); being primiparous and under 29 years old (for < 20 years AOR = 0.69, 95% CI = 0.51, 0.92 and for 20 to 29 years AOR = 0.63, 95% CI = 0.49, 0.81); planning the pregnancy (AOR = 0.82, 95% CI = 0.67, 1.00); and having a close relative die during the pregnancy (AOR = 0.65, 95% CI = 0.44, 0.95). For obese and overweight women, physical abuse by the baby's father increased the risk (AOR = 3.19, 95% CI = 1.27, 8.01) of poor total weight gain, whereas receiving financial support from the baby's father decreased the risk (AOR = 0.59, 95% CI = 0.37, 0.95).APPLICATIONS/CONCLUSIONS: These baseline factors could aid in targeting nutrition and other social services earlier to pregnant Hispanic women. By strategically targeting pregnant women in greatest need of services, improvements in birth outcomes may be enhanced.
<55>Unique Identifier 9361869Authors Rosenheck R. Leda C. Frisman L. Gallup P.Institution Northeast Program Evaluation Center, V.A. Connecticut Healthcare System, West Haven, USA.Title Homeless mentally ill veterans: race, service use, and treatment outcomes.Source American Journal of Orthopsychiatry. 67(4):632-8, 1997 Oct.Abstract Comparisons of service use and treatment outcomes for 145 black and 236 white homeless veterans with mental disorders showed few differences. A greater improvement in psychiatric symptoms and alcohol problems among white than black veterans did not hold true when black veterans had participated in the residential treatment component of the program. The implications of the findings for the successful treatment of homeless black veterans are discussed.
<56>Unique Identifier 9379161
Page 27

601-772.txtAuthors Lieberman LS. Stoller EP. Burg MA.Institution Department of Anthropology, University of Florida, USA.Title Women's health care: cross-cultural encounters within the medical system.Source Journal of the Florida Medical Association. 84(6):364-73, 1997 Aug-Sep.Abstract Women, particularly minority women, have inadequate health care and treatment outcomes caused by a number of extrinsic and intrinsic factors. Salient external systems factors addressed in this article include the lack of health insurance and the inadequate organization and delivery of health care services, for example, difficult-to-reach clinic locations and limited hours of operation. The multiple family roles of women often necessitate alterations in adherence and treatment activities to fulfill competing time and resource demands. Furthermore, culturally widespread lay therapeutic activities, and more culturally limited ethnomedical practices, are routinely employed by patients, yet often are unknown or not acknowledged by physicians. Internal factors, that is, beliefs and attitudes and their behavioral outcomes, are described for African-American, Latino-American, Haitian-American, Asian-American and Native American patients. Suggestions are made for the enhancement of interethnic physician-patient communication. The medical encounter is the nexus for many factors that influence the quality of women's healthcare.
<57>Unique Identifier 9352167Authors Dressler WW. Balieiro MC. Dos Santos JE.Institution Department of Behavioral and Community Medicine, University of Alabama School of Medicine, Tuscaloosa 35487-0326, USA.Title The cultural construction of social support in Brazil: associations with health outcomes.Source Culture, Medicine & Psychiatry. 21(3):303-35, 1997 Sep.Abstract The association of social support and health outcomes has received considerable attention in recent years, but the cultural dimension of social support has not beenextensively investigated. In this paper, using data collected in a Brazilian city, we present results indicating that those individuals whose reported access to socialsupport more closely approximates an ideal cultural model of access to social support have lower blood pressure and report fewer depressive symptoms and lower levels of perceived stress. The cultural model of social support is derived using a combination of participant observation, semi-structured interviews, and the systematic ethnographic technique of cultural consensus modelling. These results arethen used to develop a measure of an individual's approximation to that model of social support in a survey of four diverse neighborhoods in the city (n = 250). We call this approximation to the ideal cultural model of social support "cultural consonance" in social support. The association of health outcomes with cultural consonance in social support is independent of individual differences in the reporting of social support, and of standard covariates. In the case of blood pressure and perceived stress, it is independent of diet, and other socioeconomic and psychosocial variables. The association with depressive symptoms is not independent of other psychosocial variables. The implications of these results are discussed with respect to research on cultural dimensions of the distribution of disease.
<58>Page 28

601-772.txtUnique Identifier 9351160Authors Bates MS. Rankin-Hill L. Sanchez-Ayendez M.Institution Division of Human Development, School of Education & Human Development, State University of New York at Binghamton 13902-6000, USA.Title The effects of the cultural context of health care on treatment of and response tochronic pain and illness.Source Social Science & Medicine. 45(9):1433-47, 1997 Nov.Abstract Qualitative data from two studies in Puerto Rico and New England are used to show how cultural values, standards and beliefs in different health care contexts affect (1) health care professionals' responses to patients' problems, (2) the relationships between providers and patients, and (3) the patients' responses to chronic pain and illness. Influencing elements in the care setting include the worldview of the relationship of mind and body in illness processes, the dominant values and standards regarding pain and illness behaviors and the degree of cooperation between the providers and other agencies the patient depends on for compensation, rehabilitation and health insurance. In the New England study, the biomedical world view of mind-body dualism was shared by providers and most patients, but this sharedbelief often contributed to substantial patient stress and alienation. In contrast, in the Puerto Rican study providers and patients often shared a view of mind-body integration in illness and valued treatments which addressed chronic pain as a biopsychosocial experience. In this setting, shared views and values contributed to more supportive patient-provider relationships, and patients thus experienced less treatment-related stress.
<59>Unique Identifier 9305515Authors Winblad B. Hill S. Beermann B. Post SG. Wimo A.Institution Department of Geriatric Medicine, Karolinska Institute, Huddinge Hospital, Sweden.Title Issues in the economic evaluation of treatment for dementia. Position paper from the International Working Group on Harmonization of Dementia Drug Guidelines.Source Alzheimer Disease & Associated Disorders. 11 Suppl 3:39-45, 1997.
<60>Unique Identifier 9305511Authors Post SG. Beerman B. Brodaty H. Gaines AW. Gauthier SG. Geldmacher DS. Hill S. Homma A. Rossor MN. Whitehouse PJ. Winblad B.Institution Center for Biomedical Ethics, School of Medicine, Case Western Reserve University,Cleveland, OH 44106, USA.Title Ethical issues in dementia drug development. Position paper from the InternationalWorking Group on Harmonization of Dementia Drug Guidelines.Source Alzheimer Disease & Associated Disorders. 11 Suppl 3:26-8, 1997.
<61>Unique Identifier
Page 29
601-772.txt 9294957Authors Di Domenico D. Bridges P. Sharifi R. Rubenstein M. Guinan P.Institution Department of Urology, University of Illinois, Chicago, USA.Title Survival of Mexican-American males with seminoma. [Review] [8 refs]Source Revista de Investigacion Clinica. 49(2):93-6, 1997 Mar-Apr.Abstract OBJECTIVE: The objective was to determine if ethnicity was a prognostic variable in survival outcomes for testicular seminoma. MATERIALS: Eighty-seven consecutive patients with a histologic diagnosis of seminoma treated at University of illinois Hospitals were evaluated. RESULTS: There were 52 (57%) white, 22 (24%) African-American, 16 (18%) Mexican-American and 1% Asian patients. Adjusted survivals for the life-table method were 84% and 80% for the whites and Africa-American patients and 69% for the Hispanic patients. The poorer outcome appeared to be related to stage at diagnosis. CONCLUSION: In this population with testicular seminoma Mexican-American patients appear to have a worse prognosis than other ethnic groups. These differences were associated to a delayed diagnosis probably due to cultural influences. [References: 8]
<62>Unique Identifier 9292862Authors Wilce JM.Institution Department of Anthropology, Northern Arizona University.Title Discourse, power, and the diagnosis of weakness: encountering practitioners in Bangladesh.Source Medical Anthropology Quarterly. 11(3):352-74, 1997 Sep.Abstract The author's experiences as a "patient" of nonbiomedical practitioners, and an examination of Bangladeshis encounters with practitioners (daktars [biomedical doctors], herbalists, exorcists, and diviners), reveal the interactive means by which the diagnosis of durbalata (weakness) is constructed. In the cases presented, facing power in the person of the practitioner means losing face. I argue that discursive phenomena above and below the lexical level are responsible. The phenomena described--(1) interruption or dismissal of the patient's words by practitioner and others present during the clinical encounter, (2) divinatory routines that assign the durbalata label to women, and (3) one patient's use of "creaky" voice quality in a strictly "popular sector" (domestic) encounter--are nonreferential but socially significant semiotic processes that operate, for the most part, beneath the level of discursive awareness. These encounters and their outcomes have more to do with social reproduction than with any unambiguously effective therapeutic outcome.
<63>Unique Identifier 10169888Authors Kuhn KM.Institution National Association for Home Care, USA.Title Improving maternal and child outcomes of hard-to-reach populations.Source Caring. 16(7):68-71, 1997 Jul.
Page 30

601-772.txtAbstract One county health department has created an innovative program to provide pre- andpostnatal health care to Hispanic women and children. This case study demonstrates the importance of finding new ways to meet the needs of a rapidly changing population, understanding different cultural beliefs, and establishing a level of trust to achieve positive outcomes within this hard-to-reach population.
<64>Unique Identifier 10169729Authors Behrendt WM. Klein WF.Institution BJC Health System, USA.Title The spirit of St. Louis. Merging organizational culture and decision making at BJCHealth System.Source Health Systems Review. 30(4):22-6, 1997 Jul-Aug.
<65>Unique Identifier 9280090Authors Patel D. Piotrowski ZH. Nelson M.Institution Columbus Cabrini Hospital and Northwestern University Medical School, Chicago, IL 60614, USA.Title Maternal and paternal risk factors and adverse neonatal outcomes among Hispanic subgroups in Illinois (1989 through 1993).Source Journal of Perinatology. 17(4):270-5, 1997 Jul-Aug.Abstract OBJECTIVES: The study purposes were to examine maternal and paternal high-risk factors and note associated differences in birth outcomes among Hispanic subgroups compared with white and black populations in Illinois. STUDY DESIGN: Computerized birth certificate data of 131,768 Hispanic singleton neonates (14.1% of all Illinoisbirths from 1989 through 1993) were compared among five Hispanic subgroups. Matched infant birth-death computerized files were obtained for neonatal and postneonatal mortality (1989 through 1992 birth cohorts) and separate fetal mortality tables werealso examined. RESULTS: Whereas Puerto Rican mothers had higher prevalence rates forvarious maternal risk factors and higher infant morbidity rates among the five Hispanic groups, infants of Cuban mothers had significantly higher fetal and infant mortality rates. CONCLUSIONS: Our study identified substantial differences during the prenatal period and in birth outcomes among the five Hispanic subgroups. Those differences may help us develop innovative targeted interventions.
<66>Unique Identifier 9274899Authors Haffner SM. Miettinen H.Institution Department of Medicine, University of Texas Health Science Center at San Antonio, 78284-7873, USA.Title Insulin resistance implications for type II diabetes mellitus and coronary heart disease.[see comment]. [Review] [106 refs]Source
Page 31

601-772.txt American Journal of Medicine. 103(2):152-62, 1997 Aug.Abstract PURPOSE: To review information on the implications of insulin resistance for type II diabetes mellitus (non-insulin-dependent diabetes mellitus) and coronary heart disease, and to derive guidance from this information for the management of these conditions. DATA SOURCES: A MEDLINE search of English-language articles published between 1985 and July 1996, and review of the bibliographies of articles obtained through the MEDLINE search and textbooks. STUDY SELECTION: Primary research articles, reviews and perspectives on the epidemiology of diabetes and cardiovascular diseases and on intervention outcomes in these diseases. DATA EXTRACTION: Study design and quality were assessed, with particular attention to methods, study population size and other characteristics. Conclusions of review articles and perspectives were analyzed critically. DATA SYNTHESIS: Type II diabetesis associated with a two- to fourfold excess of coronary heart disease, compared to nondiabetic populations. In most studies, glycemia and duration of clinical diabeteswere found to be only weak risk factors for coronary heart disease. Conventional coronary heart disease risk factors such as dyslipidemia and hypertension have been associated with coronary heart disease in type II diabetes subjects. Hyperinsulinemia and insulin resistance have been predictive of the development of type II diabetes and, in some studies, of coronary heart disease. CONCLUSION: Strategies to prevent the development of coronary heart disease in diabetic and possibly prediabetic subjects should emphasize a multifactorial approach, including:a) improved glycemic control; b) aggressive treatment of risk factors for coronary heart disease, including insulin resistance; c) primary prevention of NIDDM; and d) use of glucose lowering agents that improve insulin sensitivity and cardiovascular risk factors. [References: 106]
<67>Unique Identifier 9238997Authors Gordon C.Institution Kaiser Permanente Medical Center, Honolulu, HI, USA.Title The effect of cancer pain on quality of life in different ethnic groups: a literature review. [Review] [44 refs]Source Nurse Practitioner Forum. 8(1):5-13, 1997 Mar.Abstract Pain influences the quality of life (QOL) of the majority of people with cancer. The way that pain is perceived and the way it is dealt with is largely influenced bythe ethnocultural background of the individuals and families experiencing the pain. This article stresses the need for more research by advanced practice nurses (APN) into ethnocultural influences and the way these influences will affect the care we give and the outcomes of pain management. [References: 44]
<68>Unique Identifier 9232039Authors Fuentes-Afflick E. Lurie P.Institution Department of Pediatrics, School of Medicine, University of California, San Francisco, USA.Title Low birth weight and Latino ethnicity. Examining the epidemiologic paradox.Source Archives of Pediatrics & Adolescent Medicine. 151(7):665-74, 1997 Jul.Abstract OBJECTIVE: To assess the relation between Latino ethnicity, Latino subgroup, and
Page 32

601-772.txtlow birth weight (LBW). DATA SOURCES: From the MEDLINE computer data-base, we used the key words birth weight; infant, LBW; Latinos; Hispanic Americans; Cuban Americans; Mexican Americans; and Puerto Ricans to identify studies that analyzed LBW in Latinos. STUDY SELECTION: Thirty-two studies, published from 1982 to 1996, that analyzed US Latinos and whites or multiple Latino subgroups, that used the revised definition of LBW (< 2500 g), and had a large sample size (> 10,000) were selected. DATA EXTRACTION: Two reviewers extracted LBW rates and data on the relation between Institute of Medicine risk factors and LBW by maternal ethnicity and Latino subgroup. DATA SYNTHESIS: Low-birth-weight rates were similar for Latino (median, 6.2%) and white infants (median, 5.8%). By Latino subgroup, LBW rates were similar for Central/South American, Cuban, Mexican, and white infants. Puerto Rican infants had consistently higher LBW rates (median, 9.1%). Two risk factors-maternal birth-place and gestational weight gain-were identified as confounders of the relation between Latino ethnicity, Latino subgroup, and LBW. CONCLUSIONS: Low-birth-weight rates of Latinos and whites are similar, consistent with the "epidemiologic paradox" of unexpectedly favorable perinatal outcomes for Latinos. However, this paradoxical relation for all Latinos masks the notably elevated LBW risk among Puerto Ricans. Further study of LBW among Latinos, including cultural factors, is needed.
<69>Unique Identifier 9225175Authors Kittrell AP. Arjmand EM.Institution Department of Surgery (Otolaryngology), Southern Illinois University School of Medicine, Springfield 62794-1618, USA.Title The age of diagnosis of sensorineural hearing impairment in children.Source International Journal of Pediatric Otorhinolaryngology. 40(2-3):97-106, 1997 Jun 20.Abstract OBJECTIVE: To identify factors responsible for delays in diagnosis and treatment of pediatric sensorineural hearing impairment (SNHI), and to assess the thoroughnessof medical evaluation in these children. DESIGN: Retrospective analysis. SETTING: State-supported school for the deaf. PATIENTS AND OTHER PARTICIPANTS: 291 children with SNHI, the bast majority of whom are profoundly hearing impaired. Data were collected from the school's database, individual student records, and a parental questionnaire. MAIN OUTCOME MEASURES: (1) The age of diagnosis and treatment of SNHI; (2) actors leading to a delay in diagnosis; (3) current medical evaluations used to determine the etiology of SNHI; and (4) the level of parental satisfaction with the evaluation process. RESULTS: Many children with SNHI experience delays in diagnosis from the time of first suspicion of hearing loss. Children with a risk factor for SNHI are diagnosed no earlier than children without a risk factor. Caucasian children are diagnosed significantly earlier than either Black or Hispanicchildren, regardless of socioeconomic status. Inconsistent medical evaluation ensuesfollowing the diagnosis of SNHI, and parental satisfaction with this process is low.CONCLUSIONS: The average age of diagnosis of SNHI remains unacceptably high. There exists a need to enhance physician awareness of childhood deafness and to develop guidelines for the medical evaluation in cases of pediatric SNHI. Lastly, the importance of parental concern regarding a child's hearing or language development must be re-emphasized.
<70>Unique Identifier 9224331Authors Krongrad A. Perczek RE. Burke MA. Granville LJ. Lai H. Lai S.Institution
Page 33
601-772.txt Department of Urology, University of Miami School of Medicine, Florida, USA.Title Reliability of Spanish translations of select urological quality of life instruments.Source Journal of Urology. 158(2):493-6, 1997 Aug.Abstract PURPOSE: Many patients with urological disease do not speak English. In medical studies restricting patients to those who speak only English undermines efforts to understand disease because restrictions decrease efficiency of patient recruitment, and because language and culture are associated with variable outcomes. In Spanish speaking locations, such as South Florida, studies would suffer severe selection bias if patients were required to speak English. To allow grouping in future studiesof English and Spanish speaking patients we examined the English-Spanish reliabilityof select instruments that measure health related quality of life in patients with urological disease. MATERIALS AND METHODS: We assembled available Spanish versions and translated English versions of questions regarding satisfaction, the American Urological Association symptom index, the University of California, Los Angeles Prostate Cancer Index and a pain inventory. We then examined English-Spanish reliability by asking bilingual men 50 years old or older to complete English and Spanish versions at the same sitting. A convenience sample was recruited from outpatients and volunteers at the Miami Veterans Affairs Medical Center and population based subjects living in largely Hispanic Hialeah, Florida. Reliability estimates were calculated with kappa coefficients for categorical data and intraclass correlation coefficients for quantitative data. RESULTS: A total of 100 subjects a median of 59 years old completed the questionnaire, including 55 born in Puerto Rico or Cuba, while the remainder were born at various sites throughout the Americas and Spain. Reliability estimates showed that kappa = > 0.81 for almost all items. For 2 items relating to health and social interactions reliability was poor, and stratification showed that poor reliability was primarily a feature of subjects in good health who are theoretically socially active. CONCLUSIONS: Almost all items tested have excellent English-Spanish reliability in a mixed sample of bilingual men. Nonreliability of 2 items relating to health and social interactions probably originates from the effect of language on perception, and invalidates English and Spanish grouping of these items. Because the sample represents many dialects of Spanish, the translations tested may be transported to other cities. In studies thatuse these instruments investigators can reasonably group answers from English and Spanish speaking study subjects or study the effects of acculturation on quality of life.
<71>Unique Identifier 9220562Authors van de Wijngaart GF.Institution CVO, Utrecht University, The Netherlands.Title Drug problems among immigrants and refugees in The Netherlands and the Dutch health care and treatment system. [Review] [60 refs]Source Substance Use & Misuse. 32(7-8):909-38, 1997 Jun.Abstract Immigration from former colonies and the influx of refugees whose disadvantaged situation in society often leads to drug problems is described. The Dutch Governmentprovides for a wide variety of services for drug users which include programs for minorities like the Surinamese, Moluccan, Moroccan, and Turkish communities. However, they are either executed poorly or are based too much on "White" methods. An account of a survey about the current situation of Black Surinamese women in the Netherlands is given, and the situation of refugees in the Netherlands as it relatesto drug use is described. [References: 60]
Page 34

601-772.txt
<72>Unique Identifier 9211056Authors Zatzick DF. Johnson FA.Institution Robert Wood Johnson Clinical Scholars Program, University of California, San Francisco, USA.Title Alternative psychotherapeutic practice among middle class Americans: I: Case studies and follow-up.Source Culture, Medicine & Psychiatry. 21(1):53-88, 1997 Mar.Abstract Historically, alternative psychotherapeutic procedures have florished worldwide invarious inspirational, spiritualistic and shamanistic versions. However, few investigations have described these interventions in detail, or followed the clinical outcomes longitudinally. This present report is an ethnographic and clinical description of one particular American practitioner's alternative method asit is used with middle class clientele in several regions of the USA. Two case studies are presented in detail while nine individual cases are qualitatively reviewed with one month and one year treatment outcomes reported. A condensed ethnobiographical study of the practitioner's personal and professional life is included.
<73>Unique Identifier 9207338Authors Leplege A. Hunt S.Institution Institut National de la Sante et de la Recherche Medicale (INSERM), Unite 292, Hopital de Bicetre, Le Kremlin-Bicetre, France. [email protected] The problem of quality of life in medicine.[see comment].Source JAMA. 278(1):47-50, 1997 Jul 2.Abstract The use of the term "quality of life" to encompass the values and perceptions of patients has created doubt, confusion, and misunderstanding among practitioners, researchers, policymakers, and patients. The principal reason for this state of affairs is that a clear conceptual basis for quality-of-life measures is lacking. Inthis article, the current rationale for quality-of-life measurement in the health field is examined, and the drawbacks of the various models being used are outlined. Our suggestion is that quality of life as an outcome could be explored more clearly (ie, defined) if quality of life were replaced with a more easily handled notion such as that of "subjective health status." However, the idea that the patient's perspective is as valid as that of the clinician when it comes to evaluating outcomes has a great deal of legitimacy and should certainly not be abandoned.
<74>Unique Identifier 9203843Authors Goss GL. Lee K. Koshar J. Heilemann MS. Stinson J.Institution University of California, San Francisco, USA.Title More does not mean better: prenatal visits and pregnancy outcome in the Hispanic population.
Page 35

601-772.txtSource Public Health Nursing. 14(3):183-8, 1997 Jun.Abstract Early and consistent prenatal care (PNC) is thought to play an important role in the reduction of low birthweight (LBW) in the United States. It has been reported that LBW and delayed PNC are common to the Hispanic woman. In California, this cultural group comprises approximately 26% of the population, and much debate concerning health care reform has been targeted at this problem. A comparative studywas conducted in California to examine the number of prenatal visits and the outcomes of Mexico-born Hispanics and U.S.-born Hispanics. Obstetric and medical record review for 783 women was done. The results show that more prenatal visits didnot improve the outcome during pregnancy, labor, or the postpartum period. Because alarge portion of PNC is now delivered by the advanced practice nurse, implications for practice include exploring alternatives for the delivery of culturally relevant care, addressing the barriers to caring for this population, and finding alternativemodels of care that have the potential to produce positive outcomes.
<75>Unique Identifier 9200366Authors Bassuk EL. Weinreb LF. Dawson R. Perloff JN. Buckner JC.Institution Better Homes Fund, Newton, Massachusetts 02159, USA.Title Determinants of behavior in homeless and low-income housed preschool children.Source Pediatrics. 100(1):92-100, 1997 Jul.Abstract OBJECTIVES: To describe the characteristics of homeless and low-income preschool-aged children, and to identify family and environmental determinants of their behavior. METHODS: An unmatched case-control design was used to recruit a sample of sheltered homeless families and a comparison group of low-income housed families who were never homeless in Worcester, Massachusetts. Seventy-seven sheltered homeless and 90 low-income housed mothers with preschool-age children wereassessed using a comprehensive interview protocol. Information about mothers' housing, income, service use, par-enting practices, and children's father was obtained. Data about children's background, health, and life events were included. Standardized instruments were administered to assess mothers' mental health and their children's behavior. Comparisons of homeless and low-income housed families were used to describe the sample of 167 preschoolers. Multiple linear regression wasused to examine the association of various stressors, such as homelessness, and family factors with their behavior. RESULTS: Although homeless preschoolers were significantly more likely to have experienced stressful life events, undergone a care and protection investigation, and been placed in foster care when compared withlow income preschoolers, differences in adverse behaviors were minimal. Although homeless children scored higher than housed children on the internalizing, externalizing, and total problem score on the Child Behavior Checklist (CBCL) (52.5 vs 49.9, 54.8 vs 51.2, and 54.4 vs 51.1, respectively), approximately equal numbers of children from both groups scored in the clinical range. With regard to determinants of behavior, mothers' emotional status was one of the strongest independent predictors of negative behavioral outcomes on both subscales. Foster care placement and death of a child's friend were predictors of adverse internalizing behavioral outcomes on the CBCL. After controlling for housing status,parenting practices, child's age, child's history of physical abuse, and specific life stressors predicted adverse externalizing behavioral outcomes. For both subscales, housing status and behavior were only marginally associated in the multivariate model. CONCLUSIONS: Both homeless and low-income children experienced significant adversity in their lives, with homeless preschool children facing more stress. However, differences in behavior as measured by the CBCL were minimal. Mothers' emotional status, in addition to various stressors, strongly predict children's negative outcomes for both CBCL subscales. These findings emphasize the
Page 36

601-772.txtimportance of preventive family-oriented interventions that address the needs of preschoolers and their mothers.
<76>Unique Identifier 9193839Authors Hawkins BR. Chan P. Chan YT. Cheng IK. Cheung KO. Fenn J. Ho KK. Lai KN. Li CS. Lui SF. Opelz G. Tong MK.Institution Department of Pathology, University of Hong Kong, Hong Kong.Title Highly successful long-term outcome of kidney transplantation in Chinese recipients: an enhancing race effect?.Source Clinical Transplantation. 11(3):178-84, 1997 Jun.Abstract We report on 352 cadaveric kidney transplants and 294 living related transplants performed over a 25-yr period among the Chinese population of Hong Kong. There is a marked preference for transplanting male patients, especially from living donors, and we argue that this represents a cultural phenomenon within the Chinese population. The 10-yr graft survivals for related and cadaveric transplants are 86.2% and 67.4%, respectively. These figures are appreciably higher than corresponding figures in Caucasian populations. We show beneficial effects of using cyclosporin A, minimizing the cold ischemia time and avoiding very young and very old donors. There is a clear benefit of transplanting kidneys with zero or one mismatched HLA antigen against the recipient but no stepwise decrease in outcome as the number of mismatched antigens increases. There is close concordance between the outcome of living related grafts with zero, one, and two mismatched haplotypes against the recipient and no observable benefit of haplotype matching. We show that Chinese renal transplant recipients in other centers also have better long-term graft outcome than Caucasians, both for cadaveric and living related transplants. Wedraw attention to the existence of a detrimental "race effect" in other studies whenBlack recipients are compared with Caucasians and consider whether an enhancing raceeffect exists for Chinese or whether the better outcome reflects different underlying diseases in Chinese.
<77>Unique Identifier 9190781Authors Case-Smith J.Title Clinical interpretation of "The efficacy of an early prevention program facilitated by occupational therapists: a follow-up study".[comment].Source American Journal of Occupational Therapy. 51(4):252-5, 1997 Apr.
<78>Unique Identifier 9184507Authors Shiono PH. Rauh VA. Park M. Lederman SA. Zuskar D.Institution Center for the Future of Children, David and Lucile Packard Foundation, Los Altos,Calif 94022, USA.Title Ethnic differences in birthweight: the role of lifestyle and other factors.Source American Journal of Public Health. 87(5):787-93, 1997 May.
Page 37

601-772.txtAbstract OBJECTIVES: The purpose of this study was to expand the search for risk factors for low birthweight and to find new explanations for the ethnic-group disparities inbirth outcomes. METHODS: The subjects were 1150 pregnant women from six ethnic groups (African American, Chinese, Dominican, Puerto Rican, Mexican, and White) who received prenatal care at clinics in New York and Chicago between December 1987 and December 1989. Two interviews were conducted during the second and third trimesters of pregnancy. RESULTS: The study, after controlling for poverty and other birthweight correlates, showed that living in public housing and believing that chance plays a major role in determining one's health status were negatively associated with birthweight. Having a stable residence was positively related to birthweight. Material hardship, social adversity, perceived racial discrimination, physical abuse, anxiety, and depression were not associated with birthweight. CONCLUSIONS: The negative role of an impoverished living environment and feelings ofhelplessness, as well as the positive role of having a stable form of social support, suggest new directions for research on the causes of low birthweight and the ethnic disparities in US birth outcomes.
<79>Unique Identifier 9184495Authors Guralnik JM. Leveille SG.Institution Epidemiology, Demography and Biometry Program, National Institute on Aging, Bethesda, Md, USA.Title Race, ethnicity, and health outcomes--unraveling the mediating role of socioeconomic status.[comment].Source American Journal of Public Health. 87(5):728-30, 1997 May.
<80>Unique Identifier 9169158Authors Schiff M. Key CR. Gilliland FD. Becker TM.Institution Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque 87131, USA.Title Ethnic differences in uterine corpus cancer incidence and mortality in New Mexico's American Indians, hispanics and non-Hispanic whites.Source International Journal of Epidemiology. 26(2):249-55, 1997 Apr.Abstract BACKGROUND: Although ethnic and radical differences in uterine corpus cancer incidence and mortality have been reported worldwide, few published data have addressed the epidemiology of uterine cancer among US American Indians and Hispanics. METHODS: We reviewed uterine corpus cancer incidence and survival data from New Mexico's population-based cancer registry collected from 1969 to 1992, and examined State vital records data for uterine cancer deaths collected from 1958 to 1992, focusing on ethnic differences in occurrence and outcomes of uterine malignancies. RESULTS: Non-Hispanic white women had age-adjusted incidence rates that were substantially higher (20.8 per 100,000) than rates for Hispanics (10.3) and American Indians (6.0) over the 24-year period. Uterine cancer mortality rates were also higher for non-Hispanic whites and Hispanics than for American Indian women, although mortality rates were substantially lower than incidence rates. Five-year survival for uterine cancer was comparable among all groups for all stagescombined (87.3% for non-Hispanic whites, 81.4% for Hispanics, and 84.6% for AmericanIndians). CONCLUSIONS: Our population-based data show ethnic differences in uterine
Page 38

601-772.txtcorpus cancer incidence rates for non-Hispanic white women that were double those for Hispanics, and triple those for American Indian women. Ethnic differences in survival were comparable. Aetiologic studies are warranted to investigate the dramatic ethnic differences in occurrence of uterine cancer.
<81>Unique Identifier 9164425Authors Katerndahl DA. Realini JP.Institution University of Texas Health Science Center-San Antonio, Department of Family Practice 78284-7795, USA.Title Quality of life and panic-related work disability in subjects with infrequent panic and panic disorder.Source Journal of Clinical Psychiatry. 58(4):153-8, 1997 Apr.Abstract BACKGROUND: Panic disorder is associated with poor quality-of-life (QOL). However,little is known regarding the impact of panic disorder or infrequent panic on work-related disability. The purpose of this study was (1) to document QOL and panic-related work disability in subjects with panic disorder or infrequent panic, (2) to identify independent predictors of QOL and disability, and (3) to compare outcomes in subjects with panic disorder versus infrequent panic. METHOD: This cross-sectional community survey included 97 subjects with panic and matched controls. Subjects were screened for panic disorder or infrequent panic using the Structured Clinical Interview for DSM-III-R. The QOL questionnaire addressed life satisfaction as well as panic-related work disability. A structured interview assessed possible predictors of impaired QOL including comorbidity, illness attitudes and behaviors, coping style, family measures, and symptom perceptions. RESULTS: QOL was significantly (p < or = .001) poorer in subjects with panic than incontrols. Comorbid depression, social support, worry, and severity of chest pain predicted QOL. Although subjects with infrequent panic reported a lower QOL than controls, subjects with panic disorder had more panic-related disability and poorer QOL than those with infrequent panic. Predictors of work disability included panic frequency, illness attitudes, family dissatisfaction, and gender. CONCLUSION: Although both infrequent panic and panic disorder impact QOL and disability, panic disorder has a greater effect. Using predictors, patient education, provision of support, and focused therapy could potentially improve QOL and disability.
<82>Unique Identifier 9158907Authors Moisan PA. Sanders-Phillips K. Moisan PM.Institution Pacific Lodge Youth Services, Woodland Hills, CA 91364, USA.Title Ethnic differences in circumstances of abuse and symptoms of depression and anger among sexually abused black and Latino boys.Source Child Abuse & Neglect. 21(5):473-88, 1997 May.Abstract OBJECTIVE: The present study was designed to examine the extent to which ethnic differences in the circumstances of abuse would be related to psychological outcomesand whether the relationship of ethnicity to psychological outcomes would be independent of ethnic differences in the circumstances of abuse. METHOD: Ethnic difference in the circumstances of the abuse, depression, and anger, as measured by the Children's Depression Inventory and the State-Trait Anger Expression Inventory, were assessed in 60 Black and Latino sexually abused males aged 13 to 18 years.
Page 39

601-772.txtFactors related to levels of depression and anger in these two groups were also identified. RESULTS: Latino males were more likely to have been sexually abused by an extended family member, experienced more genital fondling and were exposed to more sexually abusive behaviors. Blacks were more likely to be abused by an immediate family member. Black males had higher anger scores than Latino males, but,there were no ethnic differences in depression scores. Both ethnicity and the relationship to the perpetrator were significantly related to scores on the State-Trait Anger Expression Inventory, however, ethnicity was also significantly related to anger scores irrespective of the relationship to the perpetrator. CONCLUSIONS: Ethnic differences in the circumstances of abuse were related to psychological outcome and the relationship of ethnicity to anger scores was independent of ethnic differences in the circumstances of abuse.
<83>Unique Identifier 9103570Authors Torrecillas L.Institution Oncology Service, Centro Medico de Especialidades 20 de Noviembre, ISSSTE, Mexico City, Mexico.Title Communication of the cancer diagnosis to Mexican patients. Attitudes of physiciansand patients.Source Annals of the New York Academy of Sciences. 809:188-96, 1997 Feb 20.
<84>Unique Identifier 9090803Authors Sellman JD. Huriwai TT. Ram RS. Deering DE.Institution Department of Psychological Medicine, Christchurch School of Medicine, New Zealand.Title Cultural linkage: treating Maori with alcohol and drug problems in dedicated Maoritreatment programs.Source Substance Use & Misuse. 32(4):415-24, 1997 Mar.Abstract Maori are the indigenous people of New Zealand and suffer more health problems, including alcohol and drug-related problems, per head of population compared with the Pakeha (non-Maori) population. An initiative to develop dedicated Maori alcohol and drug user treatment programs, which offer "cultural linkage," is currently beingundertaken. This initiative is based on the premise that addressing cultural needs makes alcohol and drug treatment more effective for Maori than mainstream programs which do not specifically address these special needs issues. As yet, there are no data from controlled studies which address this proposition. Key problems related tothe development of "cultural linkage" programs in New Zealand are identified and solutions suggested along with future direction for research in this area.
<85>Unique Identifier 9120176Authors Mickelson JK. Blum CM. Geraci JM.Institution Department of Medicine, Baylor College of Medicine, and the Veterans Affairs Medical Center, Houston, Texas 77030, USA.
Page 40

601-772.txtTitle Acute myocardial infarction: clinical characteristics, management and outcome in ametropolitan Veterans Affairs Medical Center teaching hospital.Source Journal of the American College of Cardiology. 29(5):915-25, 1997 Apr.Abstract OBJECTIVES: The influence of race and age on thrombolytic therapy, invasive cardiac procedures and outcomes was assessed in a Veterans Affairs teaching hospital. The influence of Q wave evolution on the use of invasive cardiac procedures and outcome was also assessed. BACKGROUND: It is not well known how earlyrevascularization procedures for acute myocardial infarction are delivered or influence survival in a Veterans Affairs patient population. METHODS: From October 1993 to October 1995, all patients with myocardial infarction were identified by elevated creatine kinase, MB fraction (CK-MB) and one of the following: chest pain or shortness of breath during the preceding 24 h or electrocardiographic (ECG) abnormalities. RESULTS: Racial groups were similar in terms of age, time to ECG, peak CK and length of hospital stay. Mortality increased with age (odds ratio [OR] 1.93, 95% confidence interval [CI] 1.33 to 2.81). A trend toward increased mortalityoccurred for race other than Caucasian. Patients meeting ECG criteria were given thrombolytic agents in 49% of cases, but age, comorbidity count and Hispanic race decreased the probability of thrombolytic use. Cardiac catheterization was performedmore often after thrombolytic agents (OR 1.85, 95% CI 0.97 to 3.54), but less often in African-Americans (OR 0.59, 95% CI 0.35 to 1.02), older patients (OR 0.39, 95% CI0.24 to 0.64) or patients with heart failure (OR 0.30, 95% CI 0.17 to 0.52). Patients evolving non-Q wave infarctions were older and had increased comorbidity counts and trends toward increased mortality. Angioplasty was chosen less for patients > or = 65 years old (p = 0.02); angioplasty and coronary artery bypass graft surgery were performed less in patients > or = 70 years old (p = 0.02). Patients treated invasively had lower mortality rates than those treated medically (p < 0.02). CONCLUSIONS: The use of thrombolytic agents and invasive treatment plansdeclined with age, and mortality increased with age. Trends toward increased mortality occurred with non-Q wave infarctions and race other than Caucasian.
<86>Unique Identifier 9084846Authors Franzini L. Williams AF. Franklin J. Singletary SE. Theriault RL.Institution Health Policy Institute, University of Texas School of Public Health, Houston 77030, USA.Title Effects of race and socioeconomic status on survival of 1,332 black, Hispanic, andwhite women with breast cancer.[see comment].Source Annals of Surgical Oncology. 4(2):111-8, 1997 Mar.Abstract BACKGROUND: A survival disadvantage for black women with breast cancer, which persists after controlling for stage of the disease, has been reported. This study investigates the effects of race and socioeconomic status (SES) on breast cancer survival after controlling for age, stage, histology, and type of treatment. METHODS: Kaplan-Meier and Cox proportional hazards models were used to analyze the interaction between race and SES in predicting survival in a sample of 163 black, 205 Hispanic and 964 white women with breast cancer treated at M.D. Anderson Cancer Center a (1987-1991). RESULTS: The results of univariate and multivariate analyses indicate that race was not a significant predictor of survival after adjusting for SES and other confounding factors such as demographic and disease characteristics. SES remained a significant predictor of survival after all adjustments were made. There was no evidence of differences in type of treatment by race or SES if adjustments were made for stage. CONCLUSIONS: These results suggest that institutional factors, such as access to treatment, do not explain survival differences by race or SES. Other factors associated with low SES, such as
Page 41

601-772.txtlife-style and behavior, may affect survival.
<87>Unique Identifier 9084844Authors Cady B.Title Effects of race and socioeconomic status on survival of women with breast cancer.[comment].Source Annals of Surgical Oncology. 4(2):102-3, 1997 Mar.
<88>Unique Identifier 9092081Authors Bausch RS. Serpe RT.Institution Department of Politics, Sociology, and Criminal Justice, Cameron University, Lawton, OK 73505, USA. [email protected] Negative outcomes of interethnic adoption of Mexican American children.Source Social Work. 42(2):136-43, 1997 Mar.Abstract This article identifies concerns about four possible negative outcomes of interethnic adoption involving Mexican American children and non-Mexican American parents. A sample of 861 Mexican Americans age 18 or older were asked whether they agreed or disagreed that four outcomes result from interethnic adoption: (1) The child may have an ethnic identity conflict, (2) the child may forget his or her Latino background, (3) the child's participation in Latino cultural events may be limited, and (4) the child may not acquire the skills to cope with racism. Respondents' agreement with the likelihood of these outcomes was associated with a belief in the importance of structural and cultural barriers preventing Latinos fromadopting; with higher levels of participation in Mexican American cultural events; and with income, education, and acculturation. However, agreement that the outcomes were likely did not necessarily reflect approval or disapproval of interethnic adoption. Suggestions are made for future research on Mexican American children adopted by non-Mexican American parents.
<89>Unique Identifier 9069019Authors DuPlessis HM. Bell R. Richards T.Institution RAND, Health Sciences Program, Santa Monica, California 90407-2138, USA.Title Adolescent pregnancy: understanding the impact of age and race on outcomes.Source Journal of Adolescent Health. 20(3):187-97, 1997 Mar.Abstract PURPOSE: To determine the independent effects of maternal age and race/ethnicity on poor pregnancy outcomes, with and without controlling for other factors. METHODS:Logistic regression analysis of 54,447 linked birth, fetal death, and infant death certificates in California from 1980-87. RESULTS: Women of young maternal age (10-13years) are approximately 2.5 times more likely to have a low birthweight infant and 3.4 times more likely to have a preterm birth than women of "prime" childbearing age. African-American women are 1.7 times more likely to have a low birthweight
Page 42
601-772.txtinfant, and 2 times more likely to have a preterm birth than their white and Hispanic counterparts. The association of infant death with maternal age and race/ethnicity is statistically significant in the unadjusted models, however, thoseassociations disappear completely when birthweight and gestational age are considered. Interactions between maternal age and race/ethnicity explained very little of the variability for any of the outcomes. CONCLUSIONS: Maternal age at delivery and race/ethnicity are independently and significantly associated with poorpregnancy outcomes such as low birthweight and premature births. However, young maternal age and race/ethnicity do not appear to interact in a manner that produces a differential effect on the birth outcomes assessed in this study. The incidence ofinfant mortality is unrelated to maternal age or race/ethnicity, after controlling for prematurity and low birthweight, underscoring the importance of intervention efforts aimed at their prevention.Other Abstract Logistic regression analysis of 54,447 linked birth, fetal death, and infant deathcertificates in California from 1980-87 revealed that maternal age at delivery and race/ethnicity are independently and significantly associated with poor pregnancy outcomes such as low birth weight (LBW) and premature delivery. Mothers 10-13 years of age were 2.5 times more likely to have a LBW infant and 3.4 times more likely to have a preterm birth than mothers 20-24 years old. Nearly 25% of the youngest mothers received no or late prenatal care compared with only 3-4% of mothers over 25years of age. The probability of a poor pregnancy outcome declined progressively with age among Blacks, Whites, and Hispanics. However, in each age group, Black mothers faced substantially higher probabilities of poor pregnancy outcomes than White or Hispanic women. Black women were 1.7 times more likely to have a LBW infantand 2 times more likely to have a preterm birth than their White or Hispanic counterparts. Associations of infant mortality with maternal age and race/ethnicity lost significance when birth weight and gestational age were controlled. All age andrace/ethnicity main effects were significant at the p 0.001 level. Interactions between maternal age and race/ethnicity explained very little of the variability forany of the outcomes.
<90>Unique Identifier 9118171Authors Frauenglass S. Routh DK. Pantin HM. Mason CA.Institution Department of Psychology, University of Miami, Coral Gables, FL 33124, USA.Title Family support decreases influence of deviant peers on Hispanic adolescents' substance use.Source Journal of Clinical Child Psychology. 26(1):15-23, 1997 Mar.Abstract Investigated the interplay of family support and peer modeling on adolescent alcohol, tobacco, and marijuana use and gang involvement within an ecosystemic model. The predominantly Hispanic sample of 236 eighth-grade students attended a public middle school in a high-density, impoverished Miami neighborhood, characterized by high rates of criminal activity, substance abuse, and other stressors, placing the adolescents at risk for negative developmental outcomes. The participants reported the level of perceived social support they received from family members and rates of drug use and gang, involvement for themselves and for peers. The results showed that family social support reduced the influence of deviant peers on some of the problem behaviors reported by these adolescents, specifically tobacco and marijuana use. Deviant peer modeling was strongly associated with levels of adolescent problem behavior for tobacco, alcohol and marijuana use and gang involvement.
<91>Unique Identifier
Page 43

601-772.txt 9055837Authors Alonso M. Val E. Rapaport MH.Title An open-label study of SSRI treatment in depressed hispanic and non-Hispanic women.Source Journal of Clinical Psychiatry. 58(1):31, 1997 Jan.
<92>Unique Identifier 10165099Authors Nevid JS. Javier RA.Institution St. John's University, Jamaica, NY 11439, USA.Title Preliminary investigation of a culturally specific smoking cessation intervention for Hispanic smokers.Source American Journal of Health Promotion. 11(3):198-207, 1997 Jan-Feb.Abstract PURPOSE: The purpose of this study was to compare a culturally specific, multicomponent behavioral smoking cessation program for Hispanic smokers with a low-intensity, enhanced self-help control condition. DESIGN: Participants who completed pretreatment assessment were randomly assigned to treatment conditions. Smoking status was evaluated at posttreatment, 6-month follow-up, and 12-month follow-up intervals. SETTING: The study was based in predominantly Hispanic neighborhoods in Queens, New York. PARTICIPANTS: Ninety-three Hispanic smokers participated: 48 men and 45 women. INTERVENTION: The multicomponent treatment involved a clinic-based group program that incorporated a culturally specific component consisting of videotaped presentations of culturally laden smoking-relatedvignettes. The self-help control program was enhanced by the use of an introductory group session and follow-up supportive telephone calls. MEASURES: Smoking outcomes were based on cotinine-validated abstinence and self-reported smoking rates. Predictors of abstinence were examined, including sociodemographic variables, smoking history, nicotine dependence, acculturation, partner interactions, reasons for quitting, self-efficacy, and linguistic competence. RESULTS: Significant group differences in cotinine-validated abstinence rates in favor of the multicomponent group were obtained, but only at posttreatment. With missing data included and codedfor nonabstinence, validated abstinence rates at posttreatment were 21% for the multicomponent group and 6% for the self-help group. At the 6-month follow-up, the rates were 13% for the multicomponent group and 9% for the self-help group. By the 12-month follow-up, the rates declined to 8% and 7% for the multicomponent and self-help groups, respectively. A dose-response relationship between attendance at group sessions and abstinence status was shown at posttreatment and 6-month follow-up intervals. CONCLUSIONS: The results of the present study failed to show any long-term benefit from use of a clinic-based, culturally specific multicomponentsmoking cessation intervention for Hispanic smokers relative to a minimal-contact, enhanced self-help control.
<93>Unique Identifier 9131892Authors Peele S.Institution Lindesmith Center, New York, NY 10106, USA.Title Utilizing culture and behaviour in epidemiological models of alcohol consumption and consequences for Western nations.
Page 44

601-772.txtSource Alcohol & Alcoholism. 32(1):51-64, 1997 Jan-Feb.Abstract Cultural differences in alcohol consumption are inescapable, but have been difficult to establish as predictor variables in epidemiological models. With respect to dependent variables, the behavioural outcomes of alcohol use have not been operationalized as successfully as the health outcomes. This study examined cultural differences in drinking by employing Levine's distinction between Temperance and non-Temperance cultures, along with other cultural, consumption, and policy predictor variables, among 21 Western countries. Dependent variables includedthe prevalence of Alcoholics Anonymous (AA) groups (as a measure of behavioural and social problems) and a range of alcohol consumption and health measures. Level of consumption was an important determinant of the health consequences of drinking among Western nations, but not so important in determining behavioural outcomes. Culture, on the other hand, is largely determinative of behavioural outcomes and also quite critical for some health outcomes. An inverse relationship between alcohol consumption and AA membership strongly indicated that consumption is modified by cultural styles in producing drinking behaviours. Temperance cultures, which are largely Protestant, have far more AA groups and higher rates of coronary heart disease mortality, but lower cirrhosis mortality. Overall mortality does not vary according to national alcohol consumption or cultural distinctions. The percentage of alcohol consumed as wine is a strong inverse predictor of mortality inthe 55-64 year age group, but the change in absolute national wine consumption is directly associated with overall all-age mortality. In conclusion, religious and cultural distinctions among Western nations strongly predict behavioural drinking problems and also enhance the prediction of death rates from diseases related to alcohol consumption. Social engineering techniques which attempt to modify well-established cultural drinking practices can have counter-productive results.
<94>Unique Identifier 12293212Authors Zhou M.Title Segmented assimilation: issues, controversies, and recent research on the new second generation.Source International Migration Review. 31(4):975-1,008, 1997 Winter.Abstract "The segmented assimilation theory offers a theoretical framework for understanding the process by which the new second generation--the children of contemporary immigrants--becomes incorporated into the system of stratification in the host society and the different outcomes of this process. This article examines the issues and controversies surrounding the development of the segmented assimilation theory and reviews the state of recent empirical research relevant to this theoretical approach. It also highlights main conclusions from recent research that bear on this theory and their implications for future studies." The geographical focus is on the United States. excerpt
<95>Unique Identifier 12293210Authors Rumbaut RG.Title Assimilation and its discontents: between rhetoric and reality.Source International Migration Review. 31(4):923-60, 1997 Winter.Abstract "It is in [the] conceptual interstices between theory, rhetoric, and reality that
Page 45

601-772.txtparadoxes (or at least what may appear as paradoxes) emerge. By focusing on paradoxes--on evidence that contradicts orthodox expectations and points instead to assimilation's discontents--the aim of this article is to test empirically the conception of assimilation as a linear process leading to improvements in immigrant outcomes over time and generation in the United States, to unmask underlying pre-theoretical ethnocentric pretensions, and to identify areas in need of conceptual, analytical and theoretical refinement. It is precisely through the examination of paradoxical cases--in effect, deviant case analyses--that fruitful reformulations can be stimulated, considered, and advanced." excerpt
<96>Unique Identifier 9395553Authors Wen SW. Goel V. Williams JI.Institution Institute for Clinical Evaluative Sciences in Ontario, University of Toronto, Canada.Title Utilization of health care services by immigrants and other ethnic/cultural groupsin Ontario.Source Ethnicity & Health. 1(1):99-109, 1996 Mar.Abstract OBJECTIVES: This study assesses the accessibility of health care services by immigrants and other ethnic/cultural groups in Ontario, using the 1990 Ontario Health Survey. METHODS: The population sample of 38,519 adults aged 16-64 is weighted to represent the entire non-institutionalized population of the province. Outcome measures were whether the study participants visited a general practitioner's office, a specialist's office, or a hospital's emergency department during the past 12 months. RESULTS: The results showed that while the percentages ofparticipants who ever visited a general practitioner's office during the past 12 months were slightly higher in immigrants and other ethnic/cultural groups, the rates of visits to the specialist's office were quite similar, and the rates of hospital emergency department's visits were often lower (except for aboriginals), than for Canadians. These differences in the utilization of health services across different immigrant and ethnic/cultural groups remained unchanged after controlling for health status (as measured by self-reported health problems) and age differences. However, because the sample sizes in some immigrant and ethnic/culturalgroups were small, many of the differences were not statistically significant. CONCLUSIONS: We conclude that while immigrants and other ethnic/cultural groups in Ontario usually had equal access to regular services (e.g., visits to general practitioner's office), they often had lower utilization of hospital emergency departments. However, general purpose surveys have limited utility in assessing reasons of health care utilization amongst different ethnic/cultural groups.
<97>Unique Identifier 9142668Authors Watters JK.Institution Institute for Health Policy Studies, University of California, San Francisco 94143-1304, USA.Title Impact of HIV risk and infection and the role of prevention services. [Review] [60refs]Source Journal of Substance Abuse Treatment. 13(5):375-85; discussion 439, 1996 Sep-Oct.Abstract Blood-borne infection associated with injection drug use is a significant cause of
Page 46
601-772.txtmorbidity and mortality. Over the last decade, HIV infection and its clinical sequelae have had a significant impact on research and interventions involving injecting drug users (IDUs) in the United States and elsewhere. Discussed are some of the major intervention options for reducing blood-borne infections in general andHIV in particular. The use of multiple interventions is considered within the community context in which both IDUs and service providers operate. Intervention options discussed include treatment for drug dependence; voluntary and confidential HIV testing and counseling; community health outreach; bleach distribution; and easy, legal access to needles and syringes through pharmacy sales and needle exchange programs. Many surveillance and evaluative studies have examined multiple intervention efforts that include all or some of these program components and suggest positive outcomes. However, these studies tend to be limited by experimentaldesigns that restrict attribution of causal inference. Examples of such programs in the United States and abroad are examined in terms of their potential for reducing HIV risk behaviors and averting new infections. The article concludes that diversityamong AIDS prevention programs, rapid deployment (at earlier stages of epidemics), and effective coordination (minimization of interagency conflicts) are important factors in successful AIDS prevention programming and attaining disease prevention objectives. [References: 60]
<98>Unique Identifier 9111806Authors Pearce CW. Hawkins JW. Carver-Chase D. Ebacher R. Matta S. Sullivan A. Vawter VJ. Vincent C. Windle KA.Institution Department of Nursing, University of Massachusetts Lowell, USA.Title Comprehensive interdisciplinary care: making a difference in pregnancy outcomes for Hispanic women.Source Public Health Nursing. 13(6):416-24, 1996 Dec.Abstract Hispanic women constitute one of the fastest growing and most diverse groups in the United States, representing many countries of origin and cultural practices. Thepurpose of this evaluation study, using an ex post facto design, was to examine well-being during pregnancy and pregnancy outcomes for a cohort of 113 Hispanic women receiving perinatal care at the clinic of a community hospital in an old industrial city in the Northeast. The received adequacy of prenatal care for the study sample women was very high. The low-birthweight rate was lower than for the study hospital, the study city, the state, and the entire United States. The resultsof this study demonstrate the favorable effects of a comprehensive, interdisciplinary, and culturally sensitive model of prenatal care on these women's well-being and birth outcomes. Findings also support the need for an outreach program targeted at hard-to-reach women in the inadequate, received-care group and women with later initiation of care.
<99>Unique Identifier 9119775Authors Wolff CB. Portis M.Institution Department of Biological Sciences, California State University-Chico 95929-0002, USA. [email protected] Smoking, acculturation, and pregnancy outcome among Mexican Americans.Source Health Care for Women International. 17(6):563-73, 1996 Nov-Dec.Abstract
Page 47

601-772.txt The authors present an evaluation of the role of acculturation in smoking practices and pregnancy outcome (N = 767 births) in a national sample of Mexican American women. Data employed are from the 1982-1984 Hispanic Health and Nutrition Examination Survey. The prevalence rates of smoking during pregnancy, low birth weight (< or = 2500 g), and preterm delivery (> or = 3 weeks prior to the expected date) are higher among more acculturated women compared with less acculturated women. Among the more acculturated women, the prevalence of smoking and poor birth outcomes did not increase linearly with increasing American orientation. Rather, women in the third quartile of acculturation scores, i.e., those with a moderate American orientation, experienced significantly poorer birth outcomes than women with either a stronger American orientation or a Mexican orientation. Women at this moderate level of acculturation appear to have the greatest need for public health services rather than women with the lowest level of acculturation (non-English speaking, lowest income) as a means of improving their pregnancy outcomes.
<100>Unique Identifier 9002000Authors Gray J. Puente S.Institution Midwest Latino Health Research, Training, and Policy Center, University of Illinois at Chicago, USA.Title Hispanic/Latino health outcomes research. Introduction to special issue. [Review] [23 refs]Source Journal of Medical Systems. 20(5):229-33, 1996 Oct.
<101>Unique Identifier 9001998Authors Sherraden MS. Barrera RE.Institution Department of Social Work and Research Associate, University of Missouri-St. Louis63121, USA.Title Prenatal care experiences and birth weight among Mexican immigrant women.Source Journal of Medical Systems. 20(5):329-50, 1996 Oct.Abstract National studies indicate that Mexican immigrant women tend to have more positive birth outcomes than other groups, despite receiving relatively low levels of medicalprenatal care. Our study-based on in-depth interviews with immigrant women who had recently given birth in Chicago-examines women's experiences seeking prenatal care. Qualitative findings contribute to understanding why many of these women received less than optimal care during pregnancy. The study also offers modest evidence that,despite overall positive birth outcomes and low levels of prenatal care, adequate prenatal care may make a difference in birth outcomes in this group. Suggestions aremade concerning ways to improve access to adequate care, paying particular attentionto the impact of migration and communication in prenatal care.
<102>Unique Identifier 9001997Authors Zambrana RE.Institution Center for Child Welfare, George Mason University, Fairfax, VA 22030, USA.
Page 48

601-772.txtTitle The role of Latino/Hispanic communities in health services research: strategies for a meaningful partnership. [Review] [21 refs]Source Journal of Medical Systems. 20(5):317-28, 1996 Oct.Abstract This paper critically assesses the important elements of the Latino/Hispanic community's participation in health services research and the known barriers to effective collaboration, and provides suggestions that may contribute toward a meaningful partnership among health care providers, researchers and the community. The discussion focuses on central strategies for community participation to help improve existing health care services' effectiveness, specifically for low-income Latino/Hispanic groups. It reviews current approaches for including communities in health care delivery and health services research and draws examples from the author's experiences of working with Latino/Hispanic communities for almost 20 years. The data implies that mutual benefits can be derived from forging alliances and meaningful partnerships between the health services research community and the Latino/Hispanic community. [References: 21]
<103>Unique Identifier 9001996Authors Davidson PL. Andersen RM. Marcus M. Atchison KA. Reifel N. Nakazono T. Rana H.Institution Department of Health Services, University of California, Los Angeles 900295-1772, USA.Title Indicators of oral health in diverse ethnic and age groups: findings from the International Collaborative Study of Oral Health Outcomes (ICS-II) USA research locations.Source Journal of Medical Systems. 20(5):295-316, 1996 Oct.Abstract Racial-ethnic group differences are assessed using a standardized set of oral health indicators, as well as various predisposing, enabling and need characteristics collected in the International Collaborative Study of Oral Health Outcomes (ICS-II) USA research locations. The unique data set contains comparable data on African-American, Native American, Hispanic, primarily Mexican-American, andWhite adults. Age group differences in oral health indicators are also compared in two adult age cohorts (35-44 and 65-74 years). Since data were collected from geographically diverse regions of the United States, differences in oral health indicators are considered within the context of different dental care delivery systems and external environments. Results indicate that the gap in oral health between Whites and ethnic minority groups is pervasive across research locations andage cohorts. Variation in regional dental care delivery systems and the varying effects of race-ethnicity and age cohort suggest that alternative health promotion strategies will be needed for improving oral health in diverse populations.
<104>Unique Identifier 9001995Authors Napoles-Springer A. Perez-Stable EJ. Washington E.Institution Department of Medicine, University of California, San Francisco 94143, USA.Title Risk factors for invasive cervical cancer in Latino women. [Review] [67 refs]Source Journal of Medical Systems. 20(5):277-93, 1996 Oct.
Page 49

601-772.txtAbstract Most invasive cervical cancer research in the United States has been conducted on non-Latino-White (NLW) and African-American women. Incidence, mortality, stage at diagnosis and survival indicators for invasive cervical cancer in Latino women in California are compared to NLW and African-American women. A model is presented which depicts structural, behavioral, genetic and biological risk factors for invasive cervical cancer. A literature review of risk factors and their association with invasive cervical cancer was conducted using MEDLINE and PsychINFO databases todetermine if ethnic differences in risk factors explain observed differences in morbidity and mortality. Latino women experience a significantly higher incidence and mortality associated with invasive cervical cancer than NLW women. The review ofrisk factors found that rate differences of cervical cancer screening, early detection and human papilloma virus (HPV) type-specific infection explain much of the disparity in disease burden. Further research must clarify if ethnic differencesexist in risk factors associated with ethnic variation in HPV-type prevalence in both cases and their sexual partners, in host immune responses, and multiparity. [References: 67]
<105>Unique Identifier 9001992Authors Giachello AL.Institution Midwest Latino Health Research, Training and Policy Center, Jane Addams College ofSocial Work, University of Illinois at Chicago, USA.Title Health outcomes research on Hispanics/Latinos. [Review] [41 refs]Source Journal of Medical Systems. 20(5):235-54, 1996 Oct.Abstract Outcomes research studies the impact of the health and medical interventions on the health status and quality of life of the population. This paper discusses some of the issues and challenges involved in conducting health and medical outcomes research on the Latino population in the U. S., and also provides some solutions or strategies to overcome some of the most common problems in studying this population.[References: 41]
<106>Unique Identifier 8993718Authors Suarez M. Raffaelli M. O'Leary A.Institution Department of Psychology, Rutgers University, New Brunswick, New Jersey 08903, USA.Title Use of folk healing practices by HIV-infected Hispanics living in the United States.Source AIDS Care. 8(6):683-90, 1996 Dec.Abstract In the absence of a medical cure for AIDS, HIV-infected individuals may seek alternative treatments that are consistent with cultural and social beliefs. This paper examines beliefs about, and use of, folk healing practices by HIV-infected Hispanics receiving care at an HIV/AIDS clinic in inner-city New Jersey. Anonymous individual interviews were conducted with 58 male and 18 female HIV-infected Hispanics aged 23-55, primarily of Puerto Rican origin (61%) or descent (29%). The majority of respondents believed in good and evil spirits (73.7%); among the 56 believers, 48% stated that the spirits had a causal role in their infection, either alone or in conjunction with the AIDS virus. Two thirds of the respondents engaged
Page 50

601-772.txtin folk healing (spiritualism and/or santeria). The main desired outcomes of folk healing included physical relief (44%), spiritual relief (40%), and protection from evil (26%). A number of respondents (n = 9) stated that they hoped to effect a cure by engaging in folk healing. These results indicate that health care professionals treating HIV-positive Hispanics should be aware of the prevalence of folk beliefs and alternative healing practices in this population.
<107>Unique Identifier 9081907Authors Nollert G. Reichart B.Institution Herzchirurgische Klinik, Universitat Munchen.Title [Quality assurance in heart surgery. General and personal concepts]. [German]Source Herz. 21(6):383-8, 1996 Dec.Abstract In the era of managed health care quality assurance has become more and more important. In cardiac surgery immense costs have to be justified. Some of the patients might be treated alternatively with drugs or by cardiological interventions. Additionally, the operative risk is still not neglectable in cases with substantial comorbidities and advanced age. Therefore in Germany, a nationwide quality assurance system was established in 1992 covering more than 90% of the casesin more than 90% of the centers. The goals of quality assurance have to address the needs of the patients, insurance companies, and surgeons, and thereby define the primary endpoints for analysis: mortality, quality of life, and therapy costs including reinterventions. A precondition for a sufficient quality assurance system is the isolation of quality relevant data by multivariate analysis and its documentation. Weighing the different factors allows a risk stratification in order to compare the results of various centers with different patient populations. For every center an expected mortality is calculated, and compared with the observed mortality. By taking the average mortality into account a risk adjusted mortality isderived for every center, which is independent from the patient population. An automated continuous follow-up of the patients is essential and allows assessment of30-day mortality, reinterventions and quality of life. In 1986, the German Society of Cardio-thoracic-surgery initiated the development of a multicentric method of quality assurance (Quadra). In 1992 the insurance companies agreed to cover the costs for the reduced documentation of 205 parameters for every patient undergoing CABG, valve surgery or repair of an aneurysm with the help of cardio-pulmonary bypass; a 30-day follow up is included. Isolation of risk factors has not been performed because the quality of the data was not considered valid due to incompletedocumentation and non-rigorous data control. For the first time in 1990, New York State Department of Health published data on risk adjusted mortality in CABG separate for every hospital. Due to a lawsuit brought on by the journal "Newsday" the department was forced to publish the results of every surgeon. Each clinic reports 41 different patient parameters, which are controlled for completeness and accuracy by an independent committee. The efficacy of this system has been proved bya 41% reduction in mortality from 1989 to 1992 mainly due to changes in patient management. Raw mortality rates to different hospitals in CABG were published by theadministration of the insurance companies in 1986 leading to misinterpretations by the public. In response, the Society of Thoracic Surgeons initiated a database to calculate risk adjusted data. Today, more than 50% of all US-American centers participate and more than 700,000 patients have been reported. The data is not controlled and the majority of participating hospitals are small community centers. We have developed a methodology of quality assurance which estimates the operative risks of an individual patient by calculating the survival curve of all patients with the same risk profile who have already been operated on in our center. An automated long-term follow-up at one and five years after surgery provides the data for the calculation. The development of an effective quality assurance in the US wasforced by media and insurance companies. Presentation of incorrect or misleading
Page 51

601-772.txtdata in Germany has already damaged the image of cardiac surgery and surgeons. Therefore, there are no alternatives to public presentation of risk-adjusted mortalities in order to regain trust. Fears of surgeons and hospitals with results below the average are serious and patients with a high mortality risk may be afraid of not being operated on, although the New York System shows that these fears have not become real...
<108>Unique Identifier 8982524Authors Rogut L. Newman LS. Cleary PD.Institution Patient-Centered Care Consortium, United Hospital Fund, New York, NY 10118, USA.Title Variability in patient experiences at 15 New York City hospitals.Source Bulletin of the New York Academy of Medicine. 73(2):314-34, 1996 Winter.Abstract To examine how patient experiences of the interpersonal aspects of quality of carevaried among a group of 15 New York City hospitals, and the extent to which hospitaland patient characteristics explained interhospital variability, a telephone survey was conducted with 3,423 randomly selected patients discharged from 15 New York Cityhospitals. Bivariate analysis, multiple linear regression, and least square means were used to assess the effects of 5 hospital characteristics and 15 patient characteristics on reports about problems with care. Outcome measures included patients' reported problems with selected aspects of care, patients' ratings of care, and patients' willingness to recommend the hospitals from which they had been discharged. The 15 hospitals varied widely in the rates at which patients reported problems with their care (10.7-21.7, mean = 14.8, p < 0.001). A multivariate model showed that patients in fair or poor health, those without a regular doctor, youngerpatients, and minorities other than black and Hispanic were more likely to report problems with aspects of their care. Medicaid volume was also a strong, significant predictor of problem scores. Patient reports can be used to measure differences in quality of interpersonal care among hospitals. Only some of these differences are explained by patient and hospital characteristics, indicating that other factors facilitate or inhibit the delivery of high-quality interpersonal care.
<109>Unique Identifier 8979722Authors Snowden LR.Institution School of Social Welfare, University of California at Berkeley, USA.Title Ethnic minority populations and mental health outcomes. [Review] [41 refs]Source New Directions for Mental Health Services. (71):79-87, 1996 Fall.Abstract This chapter presents a framework for evaluating outcomes from mental health intervention in ethnic minority populations, reviews existing outcomes research, anddescribes ways to increase the quantity and quality of minority outcomes research. [References: 41]
<110>Unique Identifier 8969728Authors Murphy JM. Ichinose C. Hicks RC. Kingdon D. Crist-Whitzel J. Jordan P.
Page 52

601-772.txtFeldman G. Jellinek MS.Institution Child Psychiatry, Service, Massachusetts General Hospital, Boston 02114, USA.Title Utility of the Pediatric Symptom Checklist as a psychosocial screen to meet the federal Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) standards: a pilot study.Source Journal of Pediatrics. 129(6):864-9, 1996 Dec.Abstract OBJECTIVE: To examine the usefulness of the Pediatric Symptom Checklist (PSC) as the psychosocial screening measure to meet federal Medicaid/Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) standards in a low-income Hispanic community. DESIGN AND SETTING: Three hundred seventy-nine children (aged 6 to 16 years) were screened with the PSC in a 10-month period during well child visits to three clinics in Ventura and San Mateo counties in California. The PSC was availablein English and Spanish and was administered both in written (paper-and-pencil) and oral formats. Follow-up services were provided for children identified as needing evaluation. RESULTS: The Cronbach alpha was high (r = 0.91) for the PSC in the wholesample and virtually identical for English, Spanish, oral, and written formats. All the PSC items were significantly associated with total score on the PSC in English, Spanish, oral, and written formats. Overall, the PSC identified 10.6% of the sample as at risk for psychosocial problems. Thirty-six children (9.5% of sample) were referred for mental health follow-up. Public health data from Ventura County showed a statistically significant increase in referrals for psychologic problems during the study period in two locations using the PSC: from 0.5% to 2.9% of the school-aged children seen. CONCLUSION: The PSC provides a feasible, well-accepted method for screening for psychosocial problems during EPSDT examinations of school-aged children. Psychosocial screening using a validated instrument such as the PSC, as well as increased efforts to refer positive screening results, track outcomes, and assess cost benefits should be essential requirements in capitated Medicaid approaches to caring for poor children.
<111>Unique Identifier 8968301Authors Clarvit SR. Schneier FR. Liebowitz MR.Institution Department of Psychiatry, College of Physicians and Surgeons, Columbia University,New York, USA.Title The offensive subtype of Taijin-kyofu-sho in New York City: the phenomenology and treatment of a social anxiety disorder.Source Journal of Clinical Psychiatry. 57(11):523-7, 1996 Nov.Abstract BACKGROUND: Taijin-kyofu-sho (TKS) is thought to be a common, culture-bound disorder of social anxiety in Japan and Korea. Its phenomenology has been noted to overlap with that of social phobia. The "offensive type" of TKS, which has no directparallel in Western classification, is characterized by a fear of offending others in social situations, which leads to social avoidance. There has been only one case of offensive-type TKS reported in the United States, and this case was not regarded as a variant of social phobia. METHOD: The phenomenology and treatment of six patients who presented to New York City anxiety disorders research clinic psychiatrists with the offensive type of TKS are described. Features of TKS are compared with those of social phobia, as described in Western countries. Treatment outcomes for four patients are discussed and compared with TKS treatment experience in Japan and Korea and with treatment outcome in social phobia. RESULTS: In this anxiety clinic sample, features of the offensive type of TKS showed much overlap with symptoms of social phobia. Only two of four treated patients in this TKS samplereceived adequate trials of medication known to be effective for social phobia, and
Page 53

601-772.txtone of the two improved significantly. CONCLUSION: The offensive type of TKS may notbe as culture-bound as previously thought. Further study is needed to determine whether such cases respond to medications and to cognitive-behavioral approaches that are effective for social phobia. How to classify the offensive type of TKS is uncertain, but social phobia should be considered in the differential diagnosis.
<112>Unique Identifier 9119514Authors Turkoglu C. Memis A. Payzin S. Akin M. Kultusay H. Akilli A. Can L. Altintig A.Institution Department of Cardiology and Radiology, Ege University School of Medicine, Izmir, Turkey.Title Takayasu arteritis in Turkey.Source International Journal of Cardiology. 54 Suppl:S135-6, 1996 Aug.Abstract Takayasu arteritis is a non-specific inflammatory process of unknown etiology affecting the aorta and its branches. A retrospective study was done in 14 patients diagnosed as Takayasu arteritis. Eleven patients were female and three were male. Ages ranged from 12 to 30 years. Seven patients had type I arteritis, three patientstype II arteritis, and four patients type III Takayasu arteritis. Successful angioplasty was performed in five cases.
<113>Unique Identifier 9119512Authors Jain S. Kumari S. Ganguly NK. Sharma BK.Institution Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.Title Current status of Takayasu arteritis in India.Source International Journal of Cardiology. 54 Suppl:S111-6, 1996 Aug.Abstract The clinical features of 106 patients of Takayasu arteritis (TA) seen over a period of 16 years are documented (65 females and 41 males). The mean age was 27.3 +/- 9.2 years. Hypertension was the commonest mode of presentation (51.3%) and was detected in 82 patients (77.4%) at the time of presentation. Vascular bruits were heard in 72 patients (67.9%) and 13 patients (12.3%) were in congestive heart failure. Aortography was performed in 95 patients. Based on the extent of involvement, Type I (branches of aortic arch) was seen in 7 (6.6%) patients, Type II(aortic arch, its branches and descending thoracic aorta) in 7 (6.6%) patients, TypeIII (descending thoracic aorta and abdominal aorta) in 4 (3.8%) patients, Type IV (abdominal aorta only) in 29 (27.3%) patients and Type V (aortic arch, descending thoracic aorta and abdominal aorta) in 59 (55.7%) patients. Therapeutic modalities included antihypertensive drug therapy in 81 patients, antitubercular drugs in 8 patients, steroids in 16 patients and cyclophosphamide in one patient. Response to steroids was satisfactory in 5 of these 16 patients while the lesions of vasculitis healed in the patient who was treated with cyclophosphamide. Surgical interventions included nephrectomy and autotransplantation of kidney in 3 patients each and revascularization in 4 patients and angioplasty in 4 patients. In the area of pathogenesis of this disease, a high activity of protein kinase C(PKC), an increasedintracellular calcium and inositol 1,4,5 triphosphate in both unstimulated and stimulated T cells of TA was observed. These findings suggest an activation of PKC-calcium pathway in TA.
Page 54

601-772.txt
<114>Unique Identifier 8957148Authors Caetano R. Schafer J.Institution Alcohol Research Group, Western Consortium for Public Health, Berkely, CA 94709, USA.Title DSM-IV alcohol dependence and drug abuse/dependence in a treatment sample of whites, blacks and Mexican Americans.Source Drug & Alcohol Dependence. 43(1-2):93-101, 1996 Dec 2.Abstract This paper examines the association between DSM-IV alcohol dependence, drug use and DSM-IV drug/abuse dependence in a sample of White (n = 256), Black (n = 263) andMexican American (n = 212) men consecutively admitted to five alcohol treatment programs in a Northern California county. Results show that drug use is higher amongBlacks and Mexican Americans than among Whites. About 35% of the Whites 43% of the Blacks and 35% of the Mexican Americans are both alcohol and drug dependent. Among alcohol dependent individuals, about 44% of the Whites, 72% of the blacks and 52% ofthe Mexican Americans report using at least one drug other than alcohol once a week or more in the 12 months previous to the interview. The drug most frequently used byWhites is marijuana, followed by cocaine and amphetamines. The drug most frequently used by Blacks and Mexican Americans is cocaine, followed by marijuana. Severity of drug dependence is inversely related to severity of alcohol dependence among Whites.Alcohol treatment programs for Whites, Blacks and Mexican Americans must offer assessment, treatment matching and relapse prevention that takes into consideration this high prevalence of drug use and dependence.
<115>Unique Identifier 8955702Authors Byrd TL. Mullen PD. Selwyn BJ. Lorimor R.Institution School of Public Health, University of Texas-Houston, El Paso 79902, USA. [email protected] Initiation of prenatal care by low-income Hispanic women in Houston.Source Public Health Reports. 111(6):536-40, 1996 Nov-Dec.Abstract OBJECTIVE: To understand why many Hispanic women begin prenatal care in the later stages of pregnancy. METHODS: The authors compared the demographic profile, insurance status, and health beliefs--including the perceived benefits of and barriers to initiating prenatal care--of low-income Hispanic women who initiated prenatal care at different times during pregnancy or received no prenatal care. RESULTS: A perception of many barriers to care was associated with later initiation of care and non-use of care. Perceiving more benefits of care for the baby was associated with earlier initiation of care, as was having an eligibility card for hospital district services. Several barriers to care were mentioned by women on open-ended questioning, including long waiting times, embarrassment the physical examination, and lack of transportation. CONCLUSIONS: Recommendations for practice included decreasing the number of visits for women at low risk for poor pregnancy outcomes while increasing the time spent with the provider at each visit, decreasingthe number of vaginal examinations for low risk women, increasing the use of midwives, training lay workers to do risk assessment, emphasizing specific messages about benefits to the baby, and increasing general health motivation to seek preventive care through community interventions.
Page 55

601-772.txt
<116>Unique Identifier 8945642Authors Cox C. Monk A.Institution Catholic University of America, Washington, D.C., USA.Title Strain among caregivers: comparing the experiences of African American and Hispanic caregivers of Alzheimer's relatives.Source International Journal of Aging & Human Development. 43(2):93-105, 1996.Abstract This study of the experiences of seventy-six Black and eighty-six Hispanic caregivers of Alzheimer's relatives sought to determine the factors characterizing the caregiving process and its outcomes, particularly personal and role strain, in each group. The findings reveal that Hispanics are more vulnerable to each type of strain and this may be partially attributed to their caring for more impaired relatives, their younger ages, and comparative lack of expressive supportive relationships. The mediating role played by culture and informal supports in the caregiving process is highlighted by the results as well as the need for the development of sensitive and appropriate interventions and supports.
<117>Unique Identifier 8939419Authors Frisbie WP. Forbes D. Pullum SG.Institution Population Research Center, University of Texas at Austin 78712, USA. [email protected] Compromised birth outcomes and infant mortality among racial and ethnic groups.[see comment].Source Demography. 33(4):469-81, 1996 Nov.Abstract Research based on hospital records demonstrates that many births classified as normal according to conventional demographic measurement are intrauterine growth-retarded (IUGR) when evaluated clinically; also, in addition to birth weight and gestational age, it is necessary to focus on a third dimension, maturity, in analyses of birth outcomes. Although clinical studies allow more precise classification, the small number of cases tends to result in unreliable estimates ofrates and in loss of generalizability. The fetal growth ratio, a measure recently shown to be a valid proxy for maturity, is used here to develop a classification system based on combinations of weight, gestational age, and maturity, which we apply in a comparative analysis of a large data set. The results show large differences in the distribution of compromised births across racial and ethnic groups, as well as significant race/ethnic differentials in the risk of infant mortality associated with adverse outcomes.
<118>Unique Identifier 8939416Authors Landale NS. Hauan SM.Institution Population Research Institute, Pennsylvania State University, University Park 16802, USA. [email protected]
Page 56

601-772.txtTitle Migration and premarital childbearing among Puerto Rican Women.Source Demography. 33(4):429-42, 1996 Nov.Abstract This paper examines the relationship between migration and premarital childbearingin a highly migratory Latino subgroup, Puerto Rican women. Using pooled origin-destination data from surveys conducted in Puerto Rico and in the New York metropolitan area, we find that first- and second-generation migrants to the U.S. mainland face substantially higher risks of conceiving and bearing a first child before marriage than do nonmigrants in Puerto Rico. This pattern is due largely to the relatively early transition to sexual activity among mainland women. Given the negative long-term consequences of premarital childbearing for women and their children, our findings call into question the assumption that migrants necessarily experience only positive outcomes as a result of the assimilation process.
<119>Unique Identifier 8935386Authors Trevino RP. Trevino FM. Medina R. Ramirez G. Ramirez RR.Institution Social and Health Research Center, San Antonio, TX 78210, USA.Title Health care access among Mexican Americans with different health insurance coverage.Source Journal of Health Care for the Poor & Underserved. 7(2):112-21, 1996 May.Abstract This study describes the rates of health care access among Mexican Americans with different health insurance coverage. An interview questionnaire was used to collect information regarding sociodemographics, perceived health status, health insurance coverage, and sources of health care from a random sample of 501 Mexican Americans from San Antonio, Texas. Health care access was determined more by having health insurance coverage than by health care needs. Poor Mexican Americans with health insurance had higher health care access rates than did poor Mexican Americans without health insurance. Health care access may improve health care outcomes, but more comprehensive community-based campaigns to promote health and better use of health services in underprivileged populations should be developed.
<120>Unique Identifier 8921483Authors Le LT. Kiely JL. Schoendorf KC.Institution Infant and Child Health Studies Branch, National Center for Health Statistics, Hyattsville, MD 20782, USA.Title Birthweight outcomes among Asian American and Pacific Islander subgroups in the United States.Source International Journal of Epidemiology. 25(5):973-9, 1996 Oct.Abstract BACKGROUND: Information on birth outcome among the Asian and Pacific Islander populations in the US is limited. This report examines the risks of moderately low (MLBW) and very low birthweight (VLBW) among six Asian subgroups (Chinese, Japanese,Fillipinos, Asian Indians, Koreans, Vietnamese) and three Pacific Islander subgroups(Hawaiians, Guamanians, Samoans) as compared with non-Hispanic whites. METHODS: Datafrom the 1992 US Natality File were used to calculate the percentage of MLBW and VLBW births among each Asian American and Pacific Islander subgroup. Logistic
Page 57

601-772.txtregression was used to calculate odds ratios (OR) after adjustment for maternal characteristics. RESULTS: VLBW OR ranged from 0.75 among Chinese to 1.59 among AsianIndians. MLBW OR ranged from 0.89 among Samoans to 2.12 among Asian Indians. Adjusted OR increased for most Asian American groups (e.g. VLBW OR = 1.89 for Asian Indians) and decreased among Pacific Islander subgroups, indicating relatively favourable risk characteristics for Asian Americans and unfavourable characteristicsfor Pacific Islanders. Risk of VLBW was not necessarily related to risk of MLBW. Forinstance, the VLBW OR among Japanese was 1.07, compared to an MLBW OR of 1.47. CONCLUSIONS: Marked heterogeneity in birthweight outcome was observed between Asian American and Pacific Islander subgroups. This heterogeneity was not related to traditional demographic risk factors. Additionally, risks of VLBW and MLBW were not always related. These findings suggests that the Asian American and Pacific Islanderpopulations should not be aggregated into a single category, and that traditional measures of risk and birth outcome may not be valid for those groups.
<121>Unique Identifier 8916617Authors Alvidrez J. Azocar F. Miranda J.Institution Department of Psychology, University of California, Berkeley, USA.Title Demystifying the concept of ethnicity for psychotherapy researchers. [Review] [50 refs]Source Journal of Consulting & Clinical Psychology. 64(5):903-8, 1996 Oct.Abstract At a time when ethnic minority populations are increasing in the United States, few psychotherapy studies are including minorities in their samples. To include ethnic minorities in psychotherapy studies, the complex construct of ethnicity must be carefully measured. In this article, practical advice is offered for conceptualizing, measuring, and interpreting ethnic factors in psychotherapy studies. Also discussed are identifying pathways from ethnicity to psychotherapy outcomes. Pathways that may influence ethnic differences in psychotherapy outcome include cultural factors, minority status, socioeconomic status, acculturation, and immigration experiences. [References: 50]
<122>Unique Identifier 8916613Authors Miranda J. Azocar F. Organista KC. Munoz RF. Lieberman A.Institution Department of Psychiatry, Georgetown University Medical Center, Washington, DC 20007-2197, USA.Title Recruiting and retaining low-income Latinos in psychotherapy research.Source Journal of Consulting & Clinical Psychology. 64(5):868-74, 1996 Oct.Abstract This article offers suggestions for recruiting and retaining low-income Latinos intreatment studies. Because Latinos underuse traditional mental health services, places such as medical centers or churches with large Latino constituents are suggested as useful alternative sources. To keep Latinos in research protocols, providing culturally sensitive treatments are necessary. Culturally sensitive treatments should incorporate families as part of recruitment efforts, particularly older men in the family. In addition, showing respect is an important aspect of traditional Latino culture that includes using formal titles and taking time to listen carefully. Finally, traditional Latinos tend to like interactions with othersthat are more warm and personal than is generally part of a research atmosphere.
Page 58

601-772.txt
<123>Unique Identifier 8916611Authors Norton IM. Manson SM.Institution University of Colorado Health Sciences Center, USA.Title Research in American Indian and Alaska Native communities: navigating the culturaluniverse of values and process.Source Journal of Consulting & Clinical Psychology. 64(5):856-60, 1996 Oct.Abstract The National Institutes of Health's guidelines for recruiting ethnic minorities and women into clinical research have raised numerous questions among investigators.Highlighted in this article are a number of important issues for those researchers seeking to include American Indians and Alaska Natives in their studies; that is, defining the population of American Indians and Alaska Natives for inclusion in a study, participation of the tribes in research and approval by the Institutional Review Board, issues of confidentiality and anonymity of individuals and tribes, identifying potential benefits to American Indian and Alaska Native communities, andthe importance of evaluating the scientific merit of a proposed study. Awareness anda commitment to ongoing education regarding these issues will enhance the quality and benefits of research among American Indian and Alaska Native people.
<124>Unique Identifier 8910122Authors Hochstenbach J. Donders R. Mulder T. Van Limbeek J. Schoonderwaldt H.Institution Department of Research and Development, St. Maartenskliniek, Nijmegen, The Netherlands.Title Long-term outcome after stroke: a disability-orientated approach.Source International Journal of Rehabilitation Research. 19(3):189-200, 1996 Sep.
<125>Unique Identifier 8909627Authors Hudley C. Friday J.Institution Graduate School of Education, University of California, Santa Barbara 93106, USA. [email protected] Attributional bias and reactive aggression.Source American Journal of Preventive Medicine. 12(5 Suppl):75-81, 1996 Sep-Oct.Abstract This article looks at a cognitive behavioral intervention designed to reduce minority youths' (Latino and African-American boys) levels of reactive peer-directedaggression. The BrainPower Program trains aggressive boys to recognize accidental causation in ambiguous interactions with peers. The objective of this research is toevaluate the effectiveness of this attribution retraining program in reducing levelsof reactive, peer-directed aggression. This research hypothesizes that aggressive young boys' tendency to attribute hostile intentions to others in ambiguous social interactions causes display of inappropriate, peer-directed aggression. A reduction
Page 59

601-772.txtin attributional bias should produce a decrease in reactive physical and verbal aggression directed toward peers. A 12-session, attributional intervention has been designed to reduce aggressive students' tendency to infer hostile intentions in peers following ambiguous peer provocations. The program trains boys to (1) accurately perceive and categorize the available social cues in interactions with peers, (2) attribute negative outcomes of ambiguous causality to accidental or uncontrollable causes, and (3) generate behaviors appropriate to these retrained attributions. African-American and Latino male elementary-school students (N = 384),in grades four-six, served as subjects in one of three groups: experimental attribution retraining program, attention training, and no-attention control group. Three broad categories of outcome data were collected: teacher and administrator reports of behavior, independent observations of behavior, and self-reports from participating students. Process measures to assess implementation fidelity include videotaped training sessions, observations of intervention sessions, student attendance records, and weekly team meetings. The baseline data indicated that students who were evenly distributed across the four sites were not significantly different on the baseline indicators: student cognitions, teacher perceptions of behavior, and student suspension rates. Substantial evidence has shown that aggressive boys tend to attribute hostile intentions to peers, often resulting in inappropriate retaliatory aggression. The BrainPower Program was designed to determine whether psychoeducational strategies in a school context are effective in reducing attributional bias and whether such reductions significantly reduce aggressive behavior.
<126>Unique Identifier 8909622Authors Ringwalt CL. Graham LA. Paschall MJ. Flewelling RL. Browne DC.Institution Research Triangle Institute, Research Triangle Park, NC 27709-2194, USA. CLR@RTIORGTitle Supporting Adolescents with Guidance and Employment (SAGE).Source American Journal of Preventive Medicine. 12(5 Suppl):31-8, 1996 Sep-Oct.Abstract Supporting Adolescents with Guidance and Employment (SAGE) is a multifaceted, community-based violence-prevention program. Its target is African-American male adolescents in Durham, North Carolina. Public health professionals, county government officials, and local businessmen collaborated in its development and implementation. The program is based on the paradigm of risk and protective factors,in which various risk factors for youth violence are buffered by modifiable, protective psychosocial processes. SAGE includes an eight-month African-American Rites of Passage program (adult mentoring, African-American culture and history lessons, and manhood and conflict-resolution training), a six-week summer employmentcomponent, and a 12-week entrepreneurial experience. Of the 260 youth recruited, 88 were randomly assigned to receive all three program components, 85 were assigned to the summer employment and entrepreneurial components only, and 87 were assigned to adelayed program or control condition. We compared these three groups' psychosocial and behavioral outcomes using survey data and archival records. Program implementation data include attendance records; mentor-youth activity logs pre- and postprogram focus group discussions; and telephone interviews with parents, program staff, and participants. The mean age of the adolescents recruited into the program was 14. Half reported receiving free lunches at school; half were not living with a father; and one quarter reported that their mothers had not completed high school. During the previous year, many had engaged in various violence-related behaviors, including fighting (49%) and carrying a gun (22%). Youths in each program condition were similar with respect to key demographic and behavioral characteristics. The keycomponents of the SAGE program represent increasingly popular but untested approaches. Preliminary results reveal that these youths are involved in violent behavior both as perpetrators and as victims.
Page 60

601-772.txt
<127>Unique Identifier 8909109Authors Albrecht SL. Miller MK.Institution College of Medicine, Department of Health Policy and Epidemology, University of Florida, Gainesville, USA.Title Hispanic subgroup differences in prenatal care.Source Social Biology. 43(1-2):38-58, 1996 Spring-Summer.Abstract Within SES categories in the United States, racial and ethnic minorities generallyfare less well on a variety of health-related indicators than do majority groups. Important differences exist within subgroups, however, and at present, these differences are poorly understood. In this paper we address Hispanic subgroup (CubanAmerican, Mexican American. Puerto Rican, and Central/South American) differences inutilization of prenatal care. Data from the 1986 and 1987 national Linked Birth/Infant Death files are used to assess patterns of prenatal care utilization across subgroups. Using Kotelchuck's Adequacy of Prenatal Care Utilization Index, wefind that when controlling for other factors, Cuban American and Puerto Rican women are more likely to obtain adequate care than are Hispanic women of Mexican or Central/South American origin. Other factors important in understanding utilization patterns include marital status, education level, birthplace, and region of the country. We conclude with a discussion of the relatively weak link between prenatal care and birth outcomes and identify important cultural factors that may be important in understanding why this relationship is not stronger.
<128>Unique Identifier 8908757Authors Watson EK. Firman DW. Baade PD. Ring I.Institution Epidemiology and Health Information Branch, Queensland Health, Brisbane.Title Telephone administration of the SF-36 health survey: validation studies and population norms for adults in Queensland.Source Australian & New Zealand Journal of Public Health. 20(4):359-63, 1996 Aug.Abstract The Rand Corporation medical outcomes short-form 36 health survey (SF-36) is a multidimensional measure of self-perceived general health status, which has been validated in adult populations in the United States and Great Britain, and, more recently, in an Australian population. The SF-36 is increasingly being used in health outcomes research internationally, mainly as a self-administered tool, and clearly has potential for use in Australia. This study aimed to assess the acceptability, reliability and validity of telephone administration of the instrument in the Queensland adult population, and to provide reliable population norms. We report the results of a telephone survey in which we interviewed 12,793 adults. It was the first large-scale, statewide application of the SF-36 in Australia. A response rate of 82 per cent was achieved, and the SF-36 satisfied psychometric criteria for reliability and construct validity. Population norms broken down by age and sex are provided. They will be important for the interpretation of future studies using the SF-36 in particular population or patientgroups.
<129>Page 61
601-772.txtUnique Identifier 10163577Authors Anderson RT. Aaronson NK. Bullinger M. McBee WL.Institution Department of Public Health Sciences, Bowman Gray School of Medicine, Winston-Salem, North Carolina, USA.Title A review of the progress towards developing health-related quality-of-life instruments for international clinical studies and outcomes research. [Review] [98 refs]Source Pharmacoeconomics. 10(4):336-55, 1996 Oct.Abstract This article reviews the international adaptation and use of generic health-related quality-of-life (HRQL) measures over the last several years. It focuses, as examples, on the Nottingham Health Profile (NHP), the Sickness Impact Profile (SIP), the Medical Outcomes Study Short-Form 36 Item Health Survey (MOS SF-36), the EuroQoL, Dartmouth Primary Care Cooperative Information Project (COOP) chart system, the European Organization for Research and Treatment of Cancer (EORTC)Quality of Life Questionnaire (QLQ) and the World Health Organization's WHOQOL. These instruments exemplify several different models for developing or adapting HRQLmeasures described in the literature, each model choosing unique approaches to the process of validation for cross-national use. There has been considerable scientificactivity in recent years aimed at advancing the capabilities for international HRQL assessments. Whereas prior adaptation work was focused exclusively on translation issues, recent work has begun to rely on common methodology for translation and validation of key measurement properties across language versions. Although the major HRQL measures reviewed have not yet reached the point at which there is sufficient evidence for measurement equivalence across different language versions, internationally coordinated projects are planned and under way for these instrumentsto advance and refine this capacity. Preliminary evidence suggests that there are few prominent differences between countries in ranking of health states that are representative of major HRQL dimensions, and in the levels of impact of illnesses onwell-being within those dimensions. Future studies should collect additional psychometric data to more fully quantify measurement equivalence among the various language versions in which each instrument is available. Additionally, more work is required to address cultural differences within nations or language groups. [References: 98]
<130>Unique Identifier 8904943Authors Marlatt GA.Institution Department of Psychology, University of Washington, Seattle 98195-1525, USA.Title Harm reduction: come as you are. [Review] [18 refs]Source Addictive Behaviors. 21(6):779-88, 1996 Nov-Dec.Abstract The purpose of this paper is to describe what harm reduction is, how it developed,how it works, and why it is becoming a major approach in the addictive behaviors field. Based on principles of public health, harm reduction offers a pragmatic yet compassionate set of strategies designed to reduce the harmful consequences of addictive behavior for both drug consumers and the communities in which they liver. To illustrate how harm reduction has been applied to both the prevention and treatment of addiction problems, highlights of a national conference on harm reduction are presented. The historical roots of harm reduction programs in Europe (Netherlands and the United Kingdom) are described. The paper concludes with a discussion of four basic assumptions central to harm reduction: (a) harm reduction
Page 62

601-772.txtis a public health alternative to the moral/criminal and disease models of drug use and addiction; (b) it recognizes abstinence as an ideal outcome but accepts alternatives that reduce harm; (c) it has emerged primarily as a "bottom-up" approach based on addict advocacy, rather than a "top-down" policy established by addiction professionals; and (d) it promotes low threshold access to services as an alternative to traditional high threshold approaches. [References: 18]
<131>Unique Identifier 8901382Authors Courtney ME. Barth RP. Berrick JD. Brooks D. Needell B. Park L.Institution School of Social Work, University of Wisconsin, Madison, USA.Title Race and child welfare services: past research and future directions. [Review] [68refs]Source Child Welfare. 75(2):99-137, 1996 Mar-Apr.Abstract A review of child welfare research suggests that children of color and their families experience poorer outcomes and receive fewer services than their Caucasian counterparts. The relationship between race and the outcomes of child welfare services is confounded, however, by the relationships among race and other contributors to poor child welfare outcomes. Child welfare researchers should take explicit account of race and ethnicity in designing and carrying out their studies. Service approaches intended to meet the special needs of children of color and theirfamilies should be developed and rigorously evaluated. [References: 68]
<132>Unique Identifier 8888461Authors Brown CM. Segal R.Institution College of Pharmacy, University of Texas at Austin 78712-1074, USA.Title The effects of health and treatment perceptions on the use of prescribed medication and home remedies among African American and white American hypertensives.Source Social Science & Medicine. 43(6):903-17, 1996 Sep.Abstract This study examines the relationships between health beliefs and the use of both prescribed medication and home remedies among a group of African American and White American hypertensives. Data were collected via telephone interviews with 300 individuals who had been medically diagnosed as having hypertension and had been prescribed at least one antihypertensive medication. Using the health belief model (HBM) as the theoretical framework, 4 primary hypotheses involving the perceptions of severity, susceptibility, benefits and costs of each treatment and compliance with prescribed mediation (Rx) and use of home remedies (HR) were tested. Multivariate logistic regression analyses indicated that age, costs of Rx and benefits of HR predicted compliance with Rx. The primary predictors of use of HR were ethnicity, poverty status, education, severity, benefits and costs of HR. The differences in predictor variables for each treatment behavior are discussed and speculations about the nature and importance of these differences are offered. Studyfindings support the suggestion that patient beliefs about their disease and their evaluations of treatment options should be considered when developing therapeutic plans and when monitoring patient outcomes.
Page 63

601-772.txt<133>Unique Identifier 8876896Authors Goh CR. Lee KS. Tan TC. Wang TL. Tan CH. Wong J. Ang PT. Chan ME. Clinch J. Olweny CL. Schipper H.Institution Hospice Care Association of Singapore.Title Measuring quality of life in different cultures: translation of the Functional Living Index for Cancer (FLIC) into Chinese and Malay in Singapore.Source Annals of the Academy of Medicine, Singapore. 25(3):323-34, 1996 May.Abstract Quality-of-life assessment has become an accepted method of evaluation in clinicalmedicine. The technique is based on a patient's self-assessment of physical, psychological, and social function, as well as the effects of distressing physical symptoms. The most important aspect of quality-of-life assessment is that it brings into focus a patient-centred view of health outcome, which is broader than the physiologic measures which predominate in Western medicine. Strategies for the development and use of assessment questionnaires have evolved over the past 15 years, and numerous questionnaires have been created. Most originate in Western societies, with English as the most common language of development. Adapting such questionnaires for use in other language and cultural settings is an imprecise practice. Language translation and equivalent cultural meaning must both be addressed. This paper reports on the language translation process and results for the Functional Living Index for Cancer (FLIC) as translated into Chinese and Malay in Singapore. We employed a step-wise process beginning with translation/back translation, followed by structured pilot field trials and population sampling. Taped versions of the questionnaire were devised to meet illiteracy problems in the sample population. Paired comparisons of the Chinese and Malay versions of individual questions with their English counterparts show good correlations and similar means most of the time. Factor analysis on a population sample of 246 (112 Chinese, 35 Malay and 98 English speaking) with cancers of minimal, extensive or palliative extent is convergent with that obtained on a North American population. However, a separate analysis of the Chinese questionnaires showed some differences in factor pattern. Specific language and cultural translation difficulties are discussed. Of note is the predicted significant decrease in total FLIC scores with extent of disease within each of the language preference populations, which providessome evidence for the validity for each language version in the Singapore culture(s). Thus, the FLIC translations into Malay and Chinese in Singapore can be considered for use in local trials, subject to ongoing evaluation.
<134>Unique Identifier 8876472Authors Jamerson K. DeQuattro V.Institution Department of Internal Medicine, Division of Hypertension, University of Michigan School of Medicine, Detroit, USA.Title The impact of ethnicity on response to antihypertensive therapy. [Review] [107 refs]Source American Journal of Medicine. 101(3A):22S-32S, 1996 Sep 30.Abstract The aim of this review is to assess the prevalence of complications and responses to various antihypertensive drug therapies in ethnic minority groups in the United States. In some instances, these comments are extended to responses of citizens in their countries of origin. The incidence of hypertension, mortality from hypertensive heart disease, stroke, and hypertensive renal disease are higher in
Page 64

601-772.txtAfrican Americans. Although some Hispanic Americans have a lesser risk for hypertension, they have a greater risk for other risk factors such as diabetes and dyslipidemia. There is a similar association between income and mortality for both African Americans and Hispanic Americans. When compared to European Americans and other ethnic minorities, African Americans respond less favorably to beta blockers and angiotensin-converting enzyme (ACE) inhibitors. Nevertheless, the observed response in African Americans to ACE inhibitors and beta blockers is clinically significant. The available literature indicates that Asian American responses to calcium antagonists seem to be more favorable than responses to ACE inhibitors and equivalent to their responses to diuretic and beta blocker therapy. Although there are few published studies of drug efficacy in Hispanic Americans, there appears to be no hierarchy in response to the various antihypertensive drug classes. Ethnicity is not an accurate criterion for predicting poor response to any class of antihypertensive therapy. Thus, there is little justification to use racial profiling as a criterion for the avoidance of selected drug classes because of presumed lack of efficacy. Observed differences in the incidence of hypertension andits poor outcomes have led some investigators to postulate that the etiology of hypertension in ethnic minority groups is intrinsically different from whites. Awareness of racial differences in hypertension outcomes evolved in the United States within a historical context that does not fully appreciate that race is oftena surrogate for many social and economic factors that influence health status and healthcare delivery. Poor outcomes in ethnic minority groups occur in many diseases,not only hypertension. The goal of ethnicity-related research should be to describe the diversity of disease expression in humans and to target at-risk groups for prevention and early intervention. The use of racial descriptors to explain genetic differences in ethnic groups should take a lesser priority. [References: 107]
<135>Unique Identifier 8873954Authors Pugh JA.Institution Mexican-American Medical Treatment Effectiveness Center, Department of Medicine, University of Texas Health Science Center at San Antonio, USA.Title Diabetic nephropathy and end-stage renal disease in Mexican Americans.Source Blood Purification. 14(4):286-92, 1996.Abstract Hispanics are the second largest minority group in the United States. Mexican Americans (MAs) are the largest subgroup at 14 million in 1990. MAs have a two- to threefold increased prevalence of non-insulin-dependent diabetes mellitus. Population-based studies of MAs with non-insulin-dependent diabetes have shown that these patients may be more likely than non-Hispanic whites to develop proteinuria and are more likely to develop end-stage renal disease. The reasons for this excess risk are yet to be completely elucidated, but may be due to worse glycemic control, worse blood pressure control when hypertension does occur, worse access to medical care, and/or genetics. When MAs are treated for diabetic end-stage renal disease, they have better survival. Much less data are available for other Hispanic subgroups. From a public health perspective, higher incidence and longer survival aswell as relatively young and rapidly growing population predict an increasing burdenfor MAs if prevention measures are not instituted soon.
<136>Unique Identifier 8866076Authors Lagattolla NR. Burnand KG. Ferrar D.Title Vena caval interruption in the prevention of pulmonary embolism.
Page 65

601-772.txtSource Cardiovascular Surgery. 4(4):438-40, 1996 Aug.
<137>Unique Identifier 9162296Authors Schiff M. Becker TM. Smith HO. Gilliland FD. Key CR.Institution Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque 87131-5286, USA.Title Ovarian cancer incidence and mortality in American Indian, Hispanic, and non-Hispanic white women in New Mexico.Source Cancer Epidemiology, Biomarkers & Prevention. 5(5):323-7, 1996 May.Abstract Although ethnic and racial differences in ovarian cancer incidence and mortality have been reported worldwide, few published data have addressed the epidemiology of ovarian cancer among U.S. American Indians and Hispanics. We reviewed ovarian cancerincidence and survival data from New Mexico's population-based cancer registry collected from 1969 to 1992, and examined state vital records data for ovarian cancer deaths collected from 1958 to 1992, focusing on ethnic differences in occurrence and outcomes of ovarian malignancies. Non-Hispanic white women had age-adjusted incidence rates that were slightly higher (13.3/100,000) than rates forAmerican Indians (11.4) and Hispanics (10.7) over the 24-year period. Ovarian cancermortality rates were also higher for non-Hispanic whites than for minority women. Neither incidence rates nor mortality rates for ovarian cancer improved over the span of the study period. In addition, the stage at diagnosis did not shift substantially over time for any of the ethnic groups studied, nor did the distribution of various histopathological types shift proportionately. Only slight improvement was observed in 5-year survival over the time period of the study, with greater gains among younger (50 years old or less) versus older women. Ethnic differences in ovarian cancer incidence and mortality were apparent in our population-based data. However, our analysis indicated no reduction in ovarian cancer incidence or mortality in our state over the past quarter century and only slight improvement in 5-year survival.
<138>Unique Identifier 8860062Authors Hayashi K. Walker AM.Institution Department of Population and International Health, Harvard School of Public Health, Boston, Massachusetts, USA.Title Japanese and American reports of randomized trials: differences in the reporting of adverse effects.Source Controlled Clinical Trials. 17(2):99-110, 1996 Apr.Abstract We sought to identify differences in the description of adverse drug experiences in reports of randomized clinical trials (RCTs) from the United States and Japan, using diclofenac and simvastatin as test drugs. Reports were identified in Medline (Index Medicus 1966-1990), EMBASE (Excerpta Medica 1974-1990), JAPICDOC (1979-1990),and JOIS-III (JMEDICINE 1980-1990). In each search keywords describing study design were paired with the drugs' generic names, chemical names, and development numbers. Twenty-seven U.S. reports (18 for diclofenac and 9 for simvastatin) and 22 Japanese reports (17 for diclofenac and 5 for simvastatin) identified in these four databaseswere selected for review. For each paper we identified the relation of the article
Page 66
601-772.txtto the data (preliminary, primary, and secondary reports, reviews), the means of identifying adverse reactions, the principal outcomes of the trials, and a variety of descriptive measures relating to study design, authorship, and elements of presentation. With few exceptions, Japanese reports were not indexed in English-language databases, and studies from the United States were not carried out in the Japanese databases. The Japanese literature consisted exclusively of primary reports of clinical trials, whereas the U.S. literature was dominated by review articles and secondary reports of data from trials not fully published elsewhere. Japanese reports contained more detail on adverse experiences but reported principally those attributed to the drugs by attending clinicians. U.S. reports by contrast offered little detail but tended to include all adverse experiences, whether or not clinically attributed to drugs. A preponderance of U.S. articles reported significant differences between drugs in safety or treatment efficacy, whereas only one third of the Japanese articles did so for the same agents. Reports from both countries offered few details of the methods used to gather information onadverse drug experiences, and as a result the reported absolute frequencies of such events are difficult to compare between trials or to generalize to other settings. In conclusion, the reporting of adverse reactions in clinical trials is inadequate in both the United States and Japanese literature. The shortcomings are complementary in that reports of U.S. trials contain insufficient detail and Japanese reports do not interpret or synthesize experience. Clinical research into drug safety in both countries could be improved through the adoption of simple standards of clarity and consistency in the monitoring and reporting of drug adverseeffects.
<139>Unique Identifier 8852227Authors Higgins PG. Burton M.Title New Mexico women with no prenatal care: reasons, outcomes, and nursing implications.Source Health Care for Women International. 17(3):255-69, 1996 May-Jun.Abstract A retrospective chart review was conducted to determine why women received no prenatal care during pregnancy and their subsequent maternal and neonatal outcomes. Five hundred and eighty medical records from 1990 through 1993 that were labeled as no care were reviewed. Actually, only 270 records had no care and of these, 92 had 156 recorded reasons as to why women did not receive prenatal care. These reasons were categorized into three types of barriers: attitudinal, sociodemographic, and system-related. The majority of the women were young, Hispanic, unmarried, between 20 and 29 years of age, and uninsured, and had one to three children. Overall, the women did not smoke cigarettes, drink alcohol, or use drugs during pregnancy. Overall, the women had good maternal and newborn outcomes. Results suggest a need toreevaluate the effect of prenatal care use on young Hispanic women.
<140>Unique Identifier 8851809Authors Posner SF. Marin G.Institution University of Southern California, Los Angeles, USA.Title Expectancies for driving under the influence of alcohol among Hispanics and non-Hispanic Whites.Source Substance Use & Misuse. 31(4):409-21, 1996 Mar.Abstract
Page 67

601-772.txt A random sample of 1418 (40.8% male) Hispanics and 501 (46.1% male) non-Hispanic Whites were surveyed about their behavioral expectations for driving under the influence of alcoholic beverages (DUI). Hispanics reported more often than Whites that the effects of DUI would be driving carelessly, being angry at other drivers, feeling nervous, losing the respect of friends, feeling guilty, feeling too tired todrive, and losing their self-respect. There were gender differences among Hispanics but not among Whites. Hispanic abstainers reported the likelihood of the various outcomes more frequently than drinkers although drinking status produced no statistically significant differences among non-Hispanic Whites.
<141>Unique Identifier 8851357Authors Greene GJ. Jensen C. Harper Jones D.Institution College of Social Work, Ohio State University, Columbus 43210, USA.Title A constructivist perspective on clinical social work practice with ethnically diverse clients.Source Social Work. 41(2):172-80, 1996 Mar.Abstract A person's reality and definition of self are socially constructed; ethnicity is integrally involved in this process. Clinical work is successful if the client constructs a self with a sense of positive self-esteem and empowerment. The profession views social workers' use of self as important in successful clinical work, especially with clients ethnically different from themselves. This article provides a framework adapted from a constructivist perspective for the clinician's skillful use of self in therapeutic discourse. The framework consists of five stances the clinician can use in transcending the discomfort he or she may experience in a cross-cultural clinical situation. Use of these stances facilitates clients' ethnic validation, which is essential to positive therapeutic outcomes. This article uses case examples to illustrate the use of the framework.
<142>Unique Identifier 8835283Authors Rehm J. Room R. Anderson P.Institution WHO Regional Office for Europe, Copenhagen, Denmark.Title WHO working group on population levels of alcohol consumption: Oslo, 14-16 December 1994.[erratum appears in Addiction 1996 Jun;91(6):896].Source Addiction. 91(2):275-83, 1996 Feb.Abstract Target 17 of the Health Policy for Europe calls for the health-damaging consumption of dependence-producing substances such as alcohol, tobacco and psychoactive substances to be significantly reduced in all Member States between theyear 1980 and the year 2000. With regard to alcohol, it is suggested that alcohol consumption be reduced by 25%, with particular attention to reducing harmful use. A question posed by a number of Member States is what is the level of per capita alcohol consumption of lowest risk to physical, psychological and social harm. A working group was convened to consider population levels of alcohol consumption withparticular reference to the Member States of the European Region of WHO. A basis forunderstanding population problem experience can be established through the interaction between individual risk and distribution of consumption levels within the population. The working group concluded that public health policy within the European Region should continue to advise decreases of per capita consumption. Even
Page 68

601-772.txtwhen taking into account coronary heart disease, it can be concluded at the population level, across all ranges of alcohol consumption found in almost all countries of Europe, that a reduction in consumption is linked to better health. However, public health policy concerning alcohol should not be based solely on mortality. All outcomes of drinking, that is mortality, morbidity, social and criminal consequences, as well as quality of life, should be considered. The existing data relating alcohol consumption to health originates from countries primarily with a cultural experience of consuming alcohol. In those countries, wherethere is a cultural or religious tradition of not consuming alcohol, there can be nopublic health grounds for recommending alcohol consumption.
<143>Unique Identifier 8830910Authors Parker VC. Sussman S. Crippens DL. Scholl D. Elder P.Institution Institute for Health Promotion and Disease Prevention Research, University of Southern California, Los Angeles, USA.Title Qualitative development of smoking prevention programming for minority youth.Source Addictive Behaviors. 21(4):521-5, 1996 Jul-Aug.Abstract Brief discussion groups were completed with 211 predominantly African American andLatino seventh graders to investigate reasons for adolescent smoking and perceived efficacious smoking prevention program strategies. Study data consisted of audiotaped group discussions, which were content-coded, and open-ended posttest responses. The results indicated that, through use of relatively nondirected methods, reasons for smoking and smoking prevention methods generated by African American and Latino youth were similar to those popularly endorsed by white youths in previous research. Perhaps, optimal program contents are similar across ethnic groups. Still, one may speculate that identification with and diffusion of prevention messages may be maximized if they demonstrate cultural relevancy.
<144>Unique Identifier 8830907Authors Marin G.Institution Department of Psychology, University of San Francisco, CA 94117-1080, USA.Title Expectancies for drinking and excessive drinking among Mexican Americans and non-Hispanic whites.Source Addictive Behaviors. 21(4):491-507, 1996 Jul-Aug.Abstract This study was designed to identify the expectancies held by Mexican Americans toward the drinking of alcoholic beverages as well as toward excessive drinking. Random samples of 534 Mexican American and 616 non-Hispanic White residents of San Jose, California and of San Antonio, Texas were interviewed over the telephone. Mexican Americans were found to have unique expectancies toward drinking of alcoholic beverages and toward excessive drinking that differed from those held by non-Hispanic Whites. In addition, Mexican Americans expected the various outcomes ingreater proportion than non-Hispanic Whites and the Mexican American respondents classified as high in acculturation tended to respond in a manner similar to that ofnon-Hispanic White respondents. Multivariate analyses of variance with common (across ethnic groups) factor scales with ethnicity, gender, and drinking status as independent variables showed main effects for drinking status and for ethnicity. Thegroup differences in expectancies identified here support the need for culturally
Page 69
601-772.txtappropriate interventions that target group-specific beliefs.
<145>Unique Identifier 8828313Authors Zaid A. Fullerton JT. Moore T.Title Factors affecting access to prenatal care for U.S./Mexico border-dwelling Hispanicwomen.Source Journal of Nurse-Midwifery. 41(4):277-84, 1996 Jul-Aug.Abstract A study of attitudes, beliefs, and behaviors about prenatal care was conducted among Hispanic women who resided on the U.S.-Mexico border. As part of a larger study that included chart reviews of 752 mothers and postpartum interviews of 587 ofthese women, the 118 women who elected to deliver in the university-affiliated teaching hospital, rather than any of four participating private hospitals, were reviewed separately. This study sought to determine whether the prenatal care behaviors and obstetric outcomes experienced by this subset of women would contribute to any particular adverse impact on the teaching hospital, such as the need for additional intervention services. The most common barriers to prenatal careidentified among women in the entire study were the same factors identified among women in the university hospital, including lack of financial means to pay for care,lack of information concerning where to obtain care, inadequate infrastructure of clinic services, sadness, and depression. Maternal and infant outcomes were generally favorable, even for women who did not receive any measure of prenatal care.
<146>Unique Identifier 8827936Authors Lewis MA. Lewis CE. Leake B. Monahan G. Rachelefsky G.Institution School of Nursing, University of California, Los Angeles 90095-6917, USA.Title Organizing the community to target poor Latino children with asthma.Source Journal of Asthma. 33(5):289-97, 1996.Abstract A community-university partnership to improve outcomes of care for poor Latino children (aged 6-14 years) with asthma in East Los Angeles was based on development of a community infrastructure. A family-centered educational program involved over 500 families. The Association of Latinos with Asthma and Allergy Symptoms (ALAAS) was formed. Parents report reductions in hospitalizations, emergency room, and acutecare visits. Survival of the infrastructure following the end of grant funds is unlikely unless other resources offset the costs of volunteerism among poor families. Block grants to community agencies from established fund-raising groups might reduce dependency-producing practices currently employed to "help" the poor.
<147>Unique Identifier 8826171Authors Gardner MO. Cliver SP. McNeal SF. Goldenberg RL.Title Ethnicity and sources of prenatal care: findings from a national survey.Source Birth. 23(2):84-7, 1996 Jun.
Page 70

601-772.txtAbstract BACKGROUND: Improving pregnancy outcomes for minorities is a major goal of health providers and policy makers. Since most strategies involve an intervention during pregnancy, it is important to know where minority women with various characteristicsreceive prenatal care and why. Our purpose was to evaluate services of prenatal carefor white, African-American, Mexican-American, and Puerto Rican women. METHODS: The National Maternal and Infant Health Survey (1988) was used to ascertain age, income,marital status, education level, and source of funding of the study population of 21,000 women, who were assigned to an ethnic group based on self-indentification in the survey. The sources of prenatal care were classified as private (private physician, nurse-midwife, health maintenance organization) or public (state or localhealth department, community health center, hospital-based clinic). RESULTS: When categorized by ethnic group alone, 78 percent of white women received private care compared with 51 percent of Mexican-American women, 44 percent of African-American women, and 37 percent of Puerto Rican women. Private health insurance was held by 78percent of white, 50 percent of African-American, 49 percent of Mexican-American, and 47 percent of Puerto Rican women. Of those with private insurance, 86, 62, 69, and 59 percent, respectively, received private care. Of white women with Medicaid funding, 52 percent received private care as opposed to a range of 20 to 42 percent for minority women. CONCLUSIONS: Substantial differences in sources of prenatal careexist between white and minority women and between different minority groups, suggesting that policy makers and health caregivers should tailor prenatal care intervention to the needs of specific minority populations.
<148>Unique Identifier 8975342Authors Bullinger M.Institution Abteilung fur Medizinische Psychologie, Universitat Hamburg.Title [Assessment of health related quality of life with the SF-36 Health Survey]. [German]Source Rehabilitation. 35(3):XVII-XXVII; quiz XXVII-XXIX, 1996 Aug.Abstract The SF-36 Health Survey is a generic instrument for assessment of the health-related quality of life of patients. Originally developed in the U.S. and used in the Medical Outcomes Study, the SF-36 is the empirically validated short form of outcome assessment instruments developed for this study. The SF-36 assesses 8 subscales of the health-related quality of life, or subjective health, which are conceptually subsumed in the areas of "physical" and "mental" health. On the basis of a translation of the instrument into the German language, the results of psychometric testing of the SF-36 in different populations of healthy and ill persons are described. In addition, the results of a norming study and the use of these data as age- and gender-specific reference information for clinical populations are demonstrated. In its German form as well, the SF-36 appears to be a psychometrically robust and practicable instrument for use in outcome evaluation in rehabilitative medicine.
<149>Unique Identifier 8790687Authors Kendall J.Institution Department of Mental Health Nursing, School of Nursing, Oregon Health Sciences University, Portland, USA.Title Creating a culturally responsive psychotherapeutic environment for African
Page 71

601-772.txtAmerican youths: a critical analysis. [Review] [43 refs]Source Advances in Nursing Science. 18(4):11-28, 1996 Jun.Abstract Psychotherapy has been used by psychiatric nurses in advanced practice since the 1950s. The majority of research and clinical literature on the processes and outcomes of psychotherapy as an intervention in treating mental health difficulties have involved primarily Euro-American populations with little emphasis on ethnic, cultural, or class distinctions. If the epistemic origins of psychotherapy and its emphasis on the "interior self" of emotions, thoughts, and perceptions are a holdover from 19th-century individualism, where does this leave African Americans, whose social and cultural experience is more embedded in communal activities of church, neighborhood, and family than that of Euro-Americans? This article critically examines the role of psychotherapeutic mental health care as an emancipatory action, seeking to create a more culturally responsive psychotherapeutic environment for African American youths. [References: 43]
<150>Unique Identifier 8784334Authors Bronner YL.Institution Department of Maternal and Child Health, School of Hygiene and Public Health, Johns Hopkins University, Baltimore, MD 21205, USA.Title Nutritional status outcomes for children: ethnic, cultural, and environmental contexts.[erratum appears in J Am Diet Assoc 1997 Jun;97(6):584]. [Review] [88 refs]Source Journal of the American Dietetic Association. 96(9):891-903, 1996 Sep.Abstract The objective of this literature review was to explore the relationship between nutritional status outcomes among ethnically diverse children and cultural and environmental contexts. Articles form the literature on anthropometric/body composition measure, diet, and physiologic outcomes among ethnically diverse children were identified through on-line literature searches and references from articles reviewed. These studies were critically reviewed and selected if they reported findings resulting from use of accepted methodologies. Explanations consistent with evaluation of results from the studies and reports were developed bysynthesis of the findings. Children from underserved, ethnically diverse population groups were at increased risk for obesity, increased serum lipid levels, and dietaryconsumption patterns that do not meet the Dietary Guidelines for Americans. More than 80% of all US children consume more than the recommended amount of total fat and saturated fat. These factors, which were noted during childhood, may track into adolescence, placing these children at increased risk for the early onset of chronicdiseases such as non-insulin-dependent diabetes mellitus, cardiovascular disease, hypertension, and some forms of cancer. Although federally funded food assistance programs are changing rapidly, currently they provide foods that, when eaten as recommended, exceed the Dietary Guidelines for these children. Future interventions to improve the health and nutritional status of our nation's children, especially those from underserved, ethnically diverse groups, should be culturally appropriate and implemented at the levels of individuals, families, and communities. [References: 88]
<151>Unique Identifier 8781005Authors Voorhees CC. Stillman FA. Swank RT. Heagerty PJ. Levine DM. Becker DM.Institution Center for Health Promotion, Johns Hopkins University School of Medicine,
Page 72

601-772.txtBaltimore, Maryland 21215, USA.Title Heart, body, and soul: impact of church-based smoking cessation interventions on readiness to quit.Source Preventive Medicine. 25(3):277-85, 1996 May-Jun.Abstract BACKGROUND: Given the relatively low spontaneous quit rates and poor treatment outcomes among African American smokers, this study was designed to evaluate the effects of a multimodal culturally relevant intervention for smoking behavior changecompared with a self-help strategy among urban African Americans in Baltimore churches. METHOD: This randomized controlled trial in urban African American churches used the stages of change model to compare the effectiveness of two interventions in moving smokers along a continuum toward smoking cessation. Twenty-two churches were randomly assigned to either an intensive culturally specific intervention or a minimal self-help intervention. Smokers were interviewed at baseline church health fairs and at a 1-year follow-up. Self-reported quitters atfollow-up were evaluated using saliva cotinine and exhaled carbon monoxide levels (CO). Stages of change were measured by applying a standardized stages of change instrument to individual interview response sequences. Analysis compared the two intervention groups at 1-year follow-up with baseline stages. Outcomes included quitrates and positive progress along the stages of change. RESULTS: Multiple logistic regression results, controlling for intrachurch correlation and demographic and baseline smoking characteristics, showed that the multimodal cultural intervention group was more likely to make positive progress along the stages of change continuum, compared with self-help intervention group (OR = 1.68; P = 0.04). Church denomination and intervention status interacted in the multivariate model; Baptists in the intensive intervention were three times (OR = 3.23; P = 0.010) more likely tomake progress than all the other denomination groups. CONCLUSION: The multimodal culturally relevant intervention was more likely than a self-help intervention to positively influence smoking behavior. This is the first community-based intervention study to report progress along the stages of change as a process-oriented measure of success. It is notable that a spiritually based model focusing on environmental sanctions was more likely than a standard church disseminated self-help intervention to positively influence smoking behavior in an urban African American population.
<152>Unique Identifier 8750424Authors Felts WM. Parrillo AV. Chenier T. Dunn P.Institution Department of Health Education School of Health and Human Performance, East Carolina University, Greenville, NC 27858-4353, USA.Title Adolescents' perceptions of relative weight and self-reported weight-loss activities: analysis of 1990 YRBS (Youth Risk behavior Survey) national data.Source Journal of Adolescent Health. 18(1):20-6, 1996 Jan.Abstract PURPOSE: The purpose of the study was to examine, among public high school students across the United States, perceptions of relative weight-loss and its relationship to physical activity levels, time spent viewing television, and effortsto lose weight. METHODS: Self-reported data from the 1990 Youth Risk Behavior Survey(YRBS) were used to analyze these relationships. The YRBS was developed and administered by the Division of Adolescent and School Health (DASH), Centers for Disease Control and Prevention (CDC), to assess important health behaviors which contribute significantly to adverse health outcomes among American youth. A total of10,870 black, Hispanic, and white respondents were included in this analysis. RESULTS: From this sample, 24.8% perceived themselves as being "too fat." Of that group, 76.4% were trying to lose weight. Females comprised 74.4% of those reporting
Page 73

601-772.txtthat they were "too fat" and trying to lose weight. Gender differences in weight perceptions were significant (p < .001), with females (34.6%) being more likely thanmales (14.4%) to report being "too fat." Whites (26.0%) reported being "too fat" more often than did Hispanics (23.9%) and blacks (17.2%) (p < .001). Skipping meals and exercise were the most commonly reported weight loss strategies. Hispanics were most likely to skip meals, followed by whites and blacks. Whites were more likely than the other groups to use exercise as a means of losing weight. Adolescents who perceived themselves as "too fat" reported fewer days of strenuous activity (p < .001), fewer hours of strenuous exercise in physical education class (p < .001), andmore hours spent viewing television on school days (p < .001) than others. CONCLUSIONS: One quarter of U.S. high school students perceive themselves as overweight; three-quarters of these students are trying to lose weight. Adolescents who perceive themselves as overweight are less physically active and spend more timeviewing television than those who do not perceive themselves as overweight.
<153>Unique Identifier 10159710Authors Sanders-Phillips K.Institution Department of Pediatrics, Charles R. Drew University of Medicine, Los Angeles, CA,USA.Title The ecology of urban violence: its relationship to health promotion behaviors in low-income black and Latino communities. [Review] [91 refs]Source American Journal of Health Promotion. 10(4):308-17, 1996 Mar-Apr.Abstract PURPOSE: The purpose of this review is to identify and examine relationships between exposure to violence and health promotion behaviors in low-income black and Latino groups. DESIGN: Based on computer surveys of the psychologic, public health, medical, and sociologic literature, approximately 90 previous studies of the impact of exposure to violence on psychologic functioning, perceptions of health and well-being, and health decisions and behavior were identified. This article reviews those studies that examine the relationships between experiences of violence and subsequent feelings of alienation, powerlessness, and hopelessness, and perceptions of health and well-being and studies that examine relationships between alienation, hopelessness, and powerlessness and health promotion behaviors. Studies of health promotion behavior that did not examine or address the impact of exposure to violence are not reviewed in this article. RESULTS: Violence affects low-income communities directly by contributing to rates of mortality, and indirectly by affecting health promotion behaviors. Exposure to violence can result in feelings ofpowerlessness, hopelessness, and alienation that significantly limit motivation, theextent of involvement, and persistence in overcoming barriers to health promotion behavior. CONCLUSIONS: Future researchers must consider the confounding effects of exposure to violence when investigating differences in health promotion behaviors for low-income black and Latino groups. Community empowerment programs that address the impact of violence and focus on developing control over life and health outcomesmay be needed to successfully address the effect of violence on health promotion behavior in low-income, black and Latino communities. [References: 91]
<154>Unique Identifier 8716428Authors Smith-Brew S. Yanai L.Title The organ donation process through a review of the literature. Part 2. [Review] [53 refs]Source
Page 74

601-772.txt Accident & Emergency Nursing. 4(2):97-102, 1996 Apr.Abstract Several studies have attempted to investigate the role of culture and race in organ donation and transplantation. These studies go beyond ones conducted out of mere interest. The researchers have found that there are indeed human leukocyte antigens that are specific to individual races and that affect transplantation outcomes (Milford et al 1987). Similarly, Weller et al (1987) have shown that graft and patient survivals were improved when donors and recipients are of the same race.[References: 53]
<155>Unique Identifier 8766389Authors Wang XT.Institution Psychology Department, University of South Dakota, Vermillion 57069, USA. [email protected] Domain-specific rationality in human choices: violations of utility axioms and social contexts.Source Cognition. 60(1):31-63, 1996 Jul.Abstract This study presents a domain-specific view of human decision rationality. It explores social and ecological domain-specific psychological mechanisms underlying choice biases and violations of utility axioms. Results from both the USA and China revealed a social group domain-specific choice pattern. The irrational preference reversal in a hypothetical life-death decision problem (a classical example of framing effects) was eliminated by providing a small group or family context in which most subjects favored a risky choice option regardless of the positive/negative framing of choice outcomes. The risk preference data also indicatethat the subjective scope of small group domain is larger for Chinese subjects, suggesting that human choice mechanisms are sensitive to culturally specific features of group living. A further experiment provided evidence that perceived fairness might be one major factor regulating the choice preferences found in small group (kith-and-kin) contexts. Finally, the violation of the stochastic dominance axiom of the rational theory of choice was predicted and tested. The violations werefound only when the "life-death" problem was presented in small group contexts; the strongest violation was found in a family context. These results suggest that human decisions and choices are regulated by domain-specific choice mechanisms designed tosolve evolutionary recurrent and adaptively important problems.
<156>Unique Identifier 8736683Authors Feldman T.Institution University of Chicago Hospital, IL 60637, USA.Title Rheumatic heart disease. [Review] [25 refs]Source Current Opinion in Cardiology. 11(2):126-30, 1996 Mar.Abstract Rheumatic heart disease seems in many ways emblematic of an older era in medicine,without any prospects of new development or change in the current era. Many new findings have come to light in the past few years regarding this illness, which has a relatively low prevalence in the United States. Not only have the diagnostic Jonescriteria for acute rheumatic fever changed, but substantial advances have been made in the use of penicillin prophylaxis for recurrent rheumatic attacks, the use of
Page 75

601-772.txtmitral valve repair or reconstruction for rheumatic mitral regurgitation, the management of rheumatic, aortic, and mitral valve disease, and the application of balloon commissurotomy for mitral stenosis. This review details some of these advances. [References: 25]
<157>Unique Identifier 8726488Authors Oquendo MA.Institution Columbia University, New York, New York, USA.Title Psychiatric evaluation and psychotherapy in the patient's second language.[see comment].Source Psychiatric Services. 47(6):614-8, 1996 Jun.Abstract Use of a patient's second language in psychiatric evaluation and treatment has a variety of effects. Patients frequently undergo psychiatric evaluation in their second language, yet competence in a second language varies depending on the phase of illness. Evaluation of bilingual patients should ideally be done in both their languages, preferably by a bilingual clinician or by a monolingual clinician with the help of an interpreter trained in mental health issues. Cultural nuances may be encoded in language in ways that are not readily conveyed in translation, even when the patient uses equivalent words in the second language. The monolingual clinician may clarify these nuances through consultation with a clinician who shares the patient's first language and culture or with an interpreter. In psychotherapy, patients may use a second language as a form of resistance, to avoid intense affect.Therapists may use language switching to overcome this resistance and to decrease emotional intensity, if necessary. Psychotherapy can also be affected by the attitudes toward speaking that are part of the patient's culture. Discussions with bilingual and bicultural consultants can elucidate these effects for the therapist who is unfamiliar with the patient's culture.
<158>Unique Identifier 8698983Authors Callister LC. Vehvilainen-Julkunen K. Lauri S.Title Cultural perceptions of childbirth: a cross-cultural comparison of childbearing women.Source Journal of Holistic Nursing. 14(1):66-78, 1996 Mar.Abstract The purpose of this comparative cross-cultural study was to describe the cultural/religious perception of the childbirth experiences of selected childbearingwomen. Finnish Lutheran women's beliefs and perceptions of childbirth were compared with those of Canadian Orthodox Jewish and American Mormon women. Methodological triangulation was achieved through semistructured, open-ended interviews and use of the Utah Test for the childbearing Year (UTCY). Canadian Orthodox Jewish women showed a significantly higher level of reliance on authority figures to ensure positive outcomes and significantly less active participation in childbirth care decisions. The Finnish Lutheran women showed less valuing of childbearing and childrearing, which may be related to a less active religious belief system and the view by Finnish women that motherhood is only one of a multiplicity of roles viewed as important. There is a need to understand and appreciate the cultural beliefs and values of childbearing women to facilitate more culturally sensitive and holistic nursing care.
Page 76

601-772.txt
<159>Unique Identifier 8727650Authors Smith KW. McGraw SA. Costa LA. McKinlay JB.Institution New England Research Institutes, Watertown, Massachusetts 02172, USA.Title A self-efficacy scale for HIV risk behaviors: development and evaluation.Source AIDS Education & Prevention. 8(2):97-105, 1996 Apr.Abstract To measure self-efficacy with respect to risk behaviors for HIV infection, a set of questionnaire items was developed regarding condom use, drug use with friends, and negotiations with potential sex partners. These items were tested with a sample of Latinos aged 14 to 22 years in two New England cities. A nine-item self-efficacy scale was found to have a high level of internal consistency (Cronbach's alpha = .77). Reliability coefficients were similar for men, women, and both English- and Spanish-speaking respondents. Strong associations with recent performance accomplishments, as specified in Bandura's social cognitive theory, support the construct validity of the scale.
<160>Unique Identifier 8706513Authors Reynolds AJ. Mavrogenes NA. Bezruczko N. Hagemann M.Institution School of Social Work, University of Wisconsin, Madison 53706, USA.Title Cognitive and family-support mediators of preschool effectiveness: a confirmatory analysis.Source Child Development. 67(3):1119-40, 1996 Jun.Abstract Investigated in this study were the mediators of the effects of preschool intervention on children's school achievement in sixth grade. A confirmatory structural model developed in a previous study of third graders was tested with 360 low-income, mostly black children who were available at the 3-year follow-up. The model incorporated cognitive readiness at kindergarten entry and parent involvement in school (rated by teachers and parents) as primary mediators of preschool effectiveness. In sixth grade (age 12), preschool participation at ages 3 or 4 was significantly associated with higher reading achievement, higher math achievement, and with lower incidence of grade retention. Cognitive readiness and parent involvement in school significantly mediated the estimated effects of preschool participation on school achievement and grade retention 7 years postprogram. Teacherratings of school adjustment, school mobility, and grade retention also contributed to the transmission of effects. This integrated model fit the data better than several alternative models, including those based on the cognitive-advantage and family-support hypotheses.
<161>Unique Identifier 8753154Authors Fenster A.Institution John Jay College of Criminal Justice, City University of New York, Dept. of Psychology, NY 10021, USA.Title
Page 77

601-772.txt Group therapy as an effective treatment modality for people of color. [Review] [42refs]Source International Journal of Group Psychotherapy. 46(3):399-416, 1996 Jul.Abstract The unique benefits for group therapy are examined with special emphasis on the treatment of blacks and Latinos. Because of racial prejudice, economic exploitation,and negative stereotypes, group forces have been especially detrimental to the personality development of people of color. The group therapist attempts to harness these powerful group forces and use them therapeutically, thus enabling people of color to relate better to others while retaining their own autonomy. Racial differences can intensely affect diagnosis, transference, countertransference, and the "real relationship." Distinctions between cultural and functional paranoia are particularly relevant in interracial groups. Implications for training group therapists are also explored. [References: 42]
<162>Unique Identifier 8740470Authors Radziszewska B. Richardson JL. Dent CW. Flay BR.Institution Prevention Research Branch, NICHD, NIH, Bethesda, Maryland 20892, USA.Title Parenting style and adolescent depressive symptoms, smoking, and academic achievement: ethnic, gender, and SES differences.Source Journal of Behavioral Medicine. 19(3):289-305, 1996 Jun.Abstract This paper examines whether the relationship between parenting style and adolescent depressive symptoms, smoking, and academic grades varies according to ethnicity, gender, and socioeconomic status. Four parenting styles are distinguished, based on patterns of parent-adolescent decision making: autocratic (parents decide), authoritative (joint process but parents decide), permissive (joint process but adolescent decides), and unengaged (adolescent decides). The sample included 3993 15-year-old White, Hispanic, African-American, and Asian adolescents. Results are generally consistent with previous findings: adolescents with authoritative parents had the best outcomes and those with unengaged parents were least well adjusted, while the permissive and the autocratic styles produced intermediate results. For the most part, this pattern held across ethnic and sociodemographic subgroups. There was one exception, suggesting that the relationship between parenting styles, especially the unengaged style, and depressive symptoms may vary according to gender and ethnicity. More research is needed to replicate and explain this pattern in terms of ecological factors, cultural norms, and socialization goals and practices.
<163>Unique Identifier 8728226Authors Nissenson AR.Institution Dialysis Program, UCLA School of Medicine 90095, USA.Title Health-care economics and peritoneal dialysis. [Review] [17 refs]Source Peritoneal Dialysis International. 16 Suppl 1:S373-7, 1996.Abstract There is no question that the next decade will see an enormous growth in the worldwide dialysis population. Increasingly, old and sick patients will be accepted on dialysis, and the worldwide dialysis population characteristics will approach
Page 78

601-772.txtthose now seen in the U.S. In addition, recent attention in the U.S. and elsewhere on the mortality of dialysis patients is already resulting in an improvement in thisregard, further expanding the future dialysis population. PD will continue to increase in use, particularly with continued worldwide economic pressures on dialysis providers. To the extent that the efficacy of this treatment can be improved, without eroding its economic benefits over HD, it should fare well in the future. If, on the other hand, expensive "adjustments" in the practice of PD are needed to assure reasonable medical outcomes, PD will likely fade in popularity. Thechallenge to those involved in PD--clinicians, scientists, companies--is to develop a PD system that optimizes patient medical and psychosocial outcomes, and minimizes costs. If this cannot be accomplished, PD is likely to be replaced by new dialytic systems in the future (e.g., daily, slow, home hemodialysis) that can succeed in these areas. [References: 17]
<164>Unique Identifier 8690690Authors Dreher GF. Cox TH Jr.Institution Department of Management, School of Business, Indiana University, Bloomington 47405, USA. [email protected] Race, gender, and opportunity: a study of compensation attainment and the establishment of mentoring relationships.Source Journal of Applied Psychology. 81(3):297-308, 1996 Jun.Abstract In this article, hypotheses concerned with how race, gender, and mentoring experiences account for compensation outcomes among master of business administration (MBA) program graduates are considered. African-American and HispanicMBAs were less likely than their White counterparts to establish mentoring relationships with White men. Women with MBAs were less likely than men with MBAs toform such relationships. Graduates who had been able to establish mentoring relationships with White men displayed an average annual compensation advantage of $16,840 over those with mentors displaying other demographic profiles. There were nocompensation differences between those who had established mentoring relationships with women or minority men and those who had not established a mentoring relationship.
<165>Unique Identifier 8730234Authors Caetano R. Schafer J.Institution Alcohol Research Group, Berkeley, California 94709, USA.Title DSM-IV alcohol dependence in a treatment sample of white, black, and Mexican-American men.Source Alcoholism: Clinical & Experimental Research. 20(2):384-90, 1996 Apr.Abstract This study examines the presentation, correlates, and factor structure of DSM-IV alcohol dependence among 256 White, 263 Black, and 212 Mexican-American men admittedconsecutively to five alcohol treatment programs in San Jose, CA. Interviews of approximately 1 hr were conducted in the programs' facilities by trained interviewers using a standardized questionnaire. The response rate was 87%. Results show that the proportion of Black respondents who are alcohol-dependent according tothe DSM-IV criteria is lower (63%) than the proportion of Whites (86%) and Mexican Americans (76%). However, the proportion of respondents reporting each criterion of
Page 79

601-772.txtdependence was similar across groups. The most powerful predictor of the number of dependence indicators reported by respondents was level of alcohol consumption, independent of ethnicity. A unidimensional model of dependence combining all seven indicators of DSM-IV alcohol dependence fit well across men in all three ethnic groups. These results indicate that both the presentation and factorial structure ofDSM-IV alcohol dependence were uniform across White, Black and Mexican-American men in treatment for alcohol problems.
<166>Unique Identifier 8667315Authors Watson MR.Title Diversity, dental public health practice, and the public's health.Source Journal of Public Health Dentistry. 56(1):3-4, 1996 Winter.
<167>Unique Identifier 8604766Authors Cobas JA. Balcazar H. Benin MB. Keith VM. Chong Y.Institution Department of Sociology and Hector Balcazar is with the Department of Family Resources and Human Development, Arizona State University, Tempe, AZ, 85287-2101, USA.Title Acculturation and low-birthweight infants among Latino women: a reanalysis of HHANES data with structural equation models.[see comment].Source American Journal of Public Health. 86(3):394-6, 1996 Mar.Abstract Previous studies have demonstrated that acculturation is associated with negative birth outcomes among mothers in numerous immigrant populations, including Latinas. This study used structural equation models to reanalyze data employed in the 1989 Scribner and Dwyer study on the effect of acculturation (measured through the Cuellar scale) on mothers' low-birthweight status. Data revealed that language components dominate the effects of acculturation on low-birthweight status. Acculturuation appears to affect low-birthweight status indirectly through smoking and dietary intake but not through parity. Acculturation has a persistent direct effect on low-birthweight status, suggesting that other intervening variables are operant.
<168>Unique Identifier 8604751Authors Scribner R.Title Paradox as paradigm--the health outcomes of Mexican Americans.[see comment][comment].Source American Journal of Public Health. 86(3):303-5, 1996 Mar.
<169>Unique Identifier 8551293Authors
Page 80

601-772.txt Stephane M. Hsu LK.Institution Department of Psychiatry, Tufts University School of Medicine, USA.Title Musical hallucinations: interplay of degenerative brain disease, psychosis, and culture in a Chinese woman.Source Journal of Nervous & Mental Disease. 184(1):59-61, 1996 Jan.
<170>Unique Identifier 8528732Authors Jacobson MA. Gundacker H. Hughes M. Fischl M. Volberding P.Institution Department of Medicine, University of California San Francisco, USA.Title Zidovudine side effects as reported by black, Hispanic, and white/non-Hispanic patients with early HIV disease: combined analysis of two multicenter placebo-controlled trials.Source Journal of Acquired Immune Deficiency Syndromes & Human Retrovirology. 11(1):45-52, 1996 Jan 1.Abstract The objective of this study was to determine whether HIV patients' subjective tolerance of zidovudine differs by racial or ethnic grouping by conducting a post hoc analysis of reported symptoms in two multicenter, placebo-controlled trials of zidovudine monotherapy for early HIV disease. Ratios of rates of developing new or worsening symptoms as reported by patients assigned to active drug or placebo were compared in groups of white/non-Hispanic, black, or Hispanic origin. Patients were included in the study if they had asymptomatic HIV disease and entry absolute CD4 lymphocyte counts below 500 cells/microL and were enrolled in National Institute of Allergy and Infectious Diseases AIDS Clinical Trials Group (ACTG) protocol 019 or had mild symptoms of HIV disease, were enrolled in ACTG protocol 016, met protocol eligibility criteria for the respective trial, and were categorized at entry as white/non-Hispanic (N = 1801), black (N = 195), or Hispanic (n = 214). The primary outcome measure was development of a new or worsening symptom of any severity. Amongpatients treated with zidovudine compared with placebo, the estimated risk for developing a new or worsening symptom was not significantly greater for blacks or Hispanics than for white/non-Hispanics for any of the most frequently reported symptoms (p > 0.05 after adjustment for the multiple comparisons performed). Our analysis of 195 black and 214 Hispanic patients did not reveal a significantly increased risk of subjective zidovudine intolerance compared with white/non-Hispanicsubjects. If there is an increased risk of such intolerance in minority groups compared with white/non-Hispanics, it is not likely to be clinically important.
<171>Unique Identifier 12321351Authors Leadbeater BJ.Title School outcomes for minority-group adolescent mothers at 28 to 36 months postpartum: a longitudinal follow-up.Source Journal of Research on Adolescence. 6(4):629-48, 1996.Other Abstract This study examines the educational status of 120 adolescent postpartum women in the US during 1987-88. Mothers were 14-19 years old at delivery. 53.1% were African American and 42.5% were Puerto Rican. All but 2 deliveries were first births. 71.7% lived with their own mothers. 64.6% came from families on welfare. The average
Page 81

601-772.txtnumber of years of completed schooling was 9.5. At 28-36 months postpartum the average age was 19.7 years, 52.4% lived with their mothers, 52.4% lived off their mother's public assistance, and 17.9% supported themselves. 7.9% were married. Interviews were conducted at 3-4 weeks, 6 months, 12 months, and 28-36 months postpartum. 94% had completed interviews by 12 months, and 71% had completed interviews by 28-36 months. 33% of mothers had attended school or graduated through the pregnancy and the last follow-up period. 19% who were not in school at the firstbirth returned or graduated by 28-36 months postpartum. 12% dropped out before the pregnancy and never returned; 36% dropped out during the pregnancy and never returned. Greater risk of delayed grade placement by 28-36 months was significantly associated with age at delivery and reports of stressful life events 1 year postpartum. Mothers who were more grade-delayed reported more depressive symptoms, more repeat pregnancies, and lower work plans. At 1 year postpartum, school returners reported significantly fewer stresses and more child care support than dropouts. 41% of the mothers had a new mate. 25.7% reported a close relationship with the baby's father. About 80% reported problems with the fathers such as drugs, promiscuity, jail, death, machismo, or physical abuse. Only 39% of attenders had a repeat pregnancy compared to 68% of returners, 93% of dropouts during pregnancy, and70% of dropouts before pregnancy. Only half of the mothers were likely to pursue educational and occupational goals.
<172>Unique Identifier 11645851Authors Pascalev A.Title Images of death and dying in the intensive care unit.Source Journal of Medical Humanities. 17(4):219-36, 1996 Winter.
<173>Unique Identifier 11660446Authors Young M. Klingle RS.Title Silent partners in medical care: a cross-cultural study of patient participation.Source Health Communication. 8(1):29-53, 1996.
Page 82