Embed Size (px)
Citation preview

JOHN J CONLEY LECTURE ON ETHICS AND PHILOSOPHY
Health Care Reform: Ethical Foundations, Policy, and Law
Robert M Sade, MD, FACSmco
dcartnkhtso
tspswabggr
t
Health care system reform has enormous implications forthe future of American society and economic life. Since theearly days of the republic, 2 world views have vied fordetermination of this country’s political system: the view ofthe individual as sovereign vs government as sovereign. Asthey developed the foundations of our nation’s governance,the founders were heavily influenced by the Enlightenmentphilosophy of the late 17th and 18th centuries—the USConstitution sharply limited the power of central govern-ment to specific narrowly defined functions, and the eco-nomic system was largely laissez faire, that is, economicexchange was mostly free of government regulation andsecuring individual liberty was a high priority. This situa-tion has slowly reversed—the federal government origi-nally was narrowly limited, but now it dominates states andindividuals. The economic system has followed, lagging byseveral decades, so although it still retains some features oflaissez faire capitalism, federal and state regulation haveproduced a decidedly mixed economy.
Among economic sectors, health care has led the shifttoward government domination for decades. The shift ispropelled by the idea that there is a right to health care, aconcept that was first articulated by Franklin Delano Roos-evelt in his address to Congress in 1944, in which he spokeof a new set of basic rights, including “the right to adequatemedical care and the opportunity to achieve and enjoygood health.”1 The debate over whether such a right existshas been ongoing for decades, some claiming it does ex-ist,2,3 others that it does not.4,5 Although a right to healthcare has never been explicitly recognized in US law, theclosest approach is in the new health care reform law withits amendments, the Patient Protection and AffordableCare Act (ACA).6 Various ethical arguments have been
Disclosure Information: Nothing to disclose.Presented at the American College of Surgeons 97th Annual Clinical Con-gress, San Francisco, CA, October 2011.Supported by the South Carolina Clinical and Translational Research Insti-tute, Medical University of South Carolina’s Clinical and Translational Sci-ence Award Number UL1RR029882. The contents are solely the responsi-bility of the author and do not necessarily represent the official views of theNational Center for Research Resources or the National Institutes of Health.
Received February 28, 2012; Accepted March 6, 2012.From the Department of Surgery, the Institute of Human Values in HealthCare, and the Clinical Research Ethics Program, South Carolina Clinical andTranslational Research Institute, Medical University of South Carolina,Charleston, SC.Correspondence address: Robert M Sade, MD, FACS, Department of Sur-
gery, Medical University of South Carolina, 25 Courtenay Dr, Ashley RiverTower Suite 7028, MSC 295, Charleston, SC 29425. email: [email protected]286© 2012 by the American College of SurgeonsPublished by Elsevier Inc.
ade for and against establishment of a legal right to healthare in recent years—the current debate about the law restsn those ethical foundations.
To clarify competing ethical theories, I will describe 2istinct ideologies, by which I mean systems of more or lessoherent ideas, which bound the ends of a spectrum ofpproaches to health care reform. The ACA and most othereform proposals are admixtures of elements from the spec-rum’s boundary anchors that I refer to as “central plan-ing,” which relies on regulatory controls, and “free mar-et,” which favors minimal government involvement in theealth care system. Opposing ideas drive these 2 positions:hat health care is an entitlement that must be provided byociety and that obtaining health care is the responsibilityf individuals.
I will start by describing an approach to the ethicalhought that underlies free market systems, then do theame for central planning. I will go on to argue that centrallanning is fatally flawed and that free markets will deliverubstantial benefits for individuals and for society. Then Iill describe the implications of these ethical consider-
tions for the development of public policy, and will end byriefly describing health care system reforms that are wellrounded ethically and are likely to actually achieve theoals of increased access and cost control, namely, systemiceforms using market mechanisms.
ETHICS OF FREE MARKETSMoral justifications for limiting government interventionin markets have included the necessity for political systemsto be based on voluntary cooperation because generalagreement is lacking on any moral question,7 the presump-ion that the primary goal of society is to protect freedom,8
and the requirement for self-determination that is imposedby human nature.9,10 Based on the solidly grounded as-sumption that there is a human nature,11 I will present ajustification of free markets based on a particular under-standing of human nature and corollary natural rightstheory.
From human nature to natural rightsAs human beings, we interpret the world through percep-tions that are gained through our senses. We process per-ceptions into concepts and use our powers of reasoning tochoose alternative actions in dealing with the real-worldsituations we encounter every day. The basic difference
between human beings and other animals is that we makeISSN 1072-7515/12/$36.00http://dx.doi.org/10.1016/j.jamcollsurg.2012.03.019

aotGra
fmmfmejfspwhs
tpp
iddnihiawa
pdamisr
287Vol. 215, No. 2, August 2012 Sade Ethics of Health Care Reform
our way in the world by using our capacity to reason. Theuse of reason is volitional, however; that is, we have tochoose to think rationally. If we fail make that choice, thealternatives are to act on unprocessed emotional responsesor to respond blindly to the direction or command ofothers.10
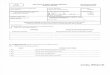
In order to survive and thrive, we have to pursue certaingoods or values that allow us to realize our potentials ashuman beings.12 The list of such goods fluctuates over timend with differing viewpoints, but Aristotle’s list will serveur purposes here (Fig. 1). Every human being needs all ofhese goods, but not in the equal proportions depicted aseneric in Figure 1, because genetic endowment and envi-
onmental influences contribute about equally to define uss unique individuals.
For example, athletic pursuits attract more attentionrom a professional athlete, such as Tom Brady, so it weighsore heavily than other goods. To achieve a thriving life, aovie leading lady, such as Angelina Jolie, would want to
ocus on achieving beauty, Albert Einstein on intellectualatters, Warren Buffet on creating wealth, and John Rob-
rts, Chief Justice of the US Supreme Court, on pursuingustice (Fig. 1). Each life contains all the goods needed tolourish, but every individual must spend time and re-ources differently in pursuing those goods, and, in light ofersonal talents and experiences, only he or she can knowhat is needed. The process of realizing one’s potential as auman being is highly individualized—there is no one-
Figure 1. Human goods: constituents of arealize the potentials for their own lives; sevperson has unique talents and abilities arisexperiences, and must use his or her persoachieve a flourishing life.
ize-fits-all decision making. To make choices appropriate
o one’s own life, the decision-making process has to berotected from interference by others. The idea of “rights”rovides such protection.I use the word rights in the sense of claim rights, which
mpose duties on others. Depending on the nature of theuty, claim rights may be positive or negative. A positiveuty requires that certain goods or actions be provided; aegative duty imposes on others the requirement not to
nterfere. So, if Smith has a right to have a house, someoneas the duty to provide him with a house—his entitlement
s a positive right. If Jones has a right to live in a house helready owns, everyone else has the duty not to interfereith his use of the house—his right of ownership is a neg-
tive right.The need for individuals to achieve the correct or best
ersonal balance of the goods we all seek requires a greateal of thought, judgment, and appropriate action thatre unique to each person. This need requires that othersust not interfere with their actions. In other words,
ndividuals have moral rights that are possessed in theame degree by everyone and are essentially negativeights of noninterference.10
Because such rights originate in human nature—who weare and what we are—they are “natural rights.” Naturalrights are universal—they belong to every human being,and they exist before any common or statutory law. In apolitical-legal context, laws govern societies, so they must
hing life. Everyone needs certain goods toare depicted in the generic pie graph. Eachom genetic composition and environmentaldgment in allocating time and resources to
flouriseraling frnal ju
be constructed on a foundation of natural rights and must

288 Sade Ethics of Health Care Reform J Am Coll Surg
apply uniformly and equally to all human beings, irrespec-tive of their individual circumstances.
From natural rights to the principleof noninterferenceBecause all human beings must pursue their unique formsof flourishing, no law can rightfully impose a preferredview of the requirements of a good life. At their roots, legalsystems have to maintain conditions that permit many dif-ferent approaches to the good life, so they must have thepower to prevent the initial use of force by one person orgroup against another. This requirement limits govern-ment to providing 3 services: military forces for nationaldefense, police for protecting people and property, andcourts to adjudicate violations of law and other disputes.Government interference with voluntary exchanges amongpeople and organizations is unjustified.
In the domain of economic action, the concrete expres-sion of the principle of noninterference is the free marketeconomy. This principle provides little guidance for deter-mining what is right or wrong or good or bad, and makesno judgments about whether people make good choices orbad choices, or whether they achieve their own good; it is ametanormative principle, which states, “No person mayinitiate force against another, nor use another for one’s ownpurposes without consent.”13
From ethical to political principlesThe idea of metanormative ethics provides the basis for alegal system that respects the right to liberty—that is, doesnot allow initiation of force against others, nor allow any-one to use others for their own purposes without consent.Most importantly, it is neutral toward differing views of thegood life. Normative and metanormative social theoriesunderlie the 2 basic forms of legal system (Fig. 2).
We clearly recognize the interference with human libertyby countries that are legally governed by the dictates ofreligious law, such as the Sharia of Islamic states, and bysecular ideologies that determine how citizens’ lives shouldbe lived, such as the People’s Republic of China, Myanmar,and other nations that impose secular norms of behaviorthrough laws based on their communist, socialist, or na-tionalist views.
We do not so easily recognize that the governments ofliberal democracies of North America and Western Europealso impose, to a significant extent, behavioral norms basedon secular beliefs of how their citizens should live theirlives. For example, welfare laws displace and ultimatelyreplace voluntary charity in the name of social justice, aparticular understanding of justice that makes dubious as-
sumptions about human values and virtues that everyoneshould or must accept, thereby substantially interferingwith individual self-determination.
Contemporary Western democracies are governedlargely under normative standards—those in power imposeby force of law limitations on what people can buy and selland to whom their earnings will be redistributed throughtaxation. In contrast, societies can be and have been orga-nized on the basis of metanorms, principles that say littleabout how lives should be lived, rather, that protect thepower of sovereign individuals to live their own lives with-out forceful interference by others.
The best example of a country founded on metanorma-tive political principles is the US. Our Declaration of In-dependence, says, “We hold these truths to be self-evident,that all men are created equal, that they are endowed bytheir Creator with certain unalienable rights, that amongthese are life, liberty and the pursuit of happiness. That tosecure these rights, governments are instituted among men,deriving their just powers from the consent of the gov-erned.”14 (Emphasis mine.)
Notice that the enumerated natural rights areunalienable—that is, they cannot be sold, given away, ortaken away—and that governments do not give us or createthese rights, they can only “secure” them because naturalrights are universal and are ours to from the start.
Nothing in the original US Constitution imposes on usa particular vision of the good life or proper living; rather,its protections enable us to choose how we live our ownlives and how we pursue our own happiness and that of ourfamilies and friends. This document is, in a word,
= Control of ac�vi�es by law/regula�on
= Freedom of ac�on
Norma�ve Metanorma�ve
China U.S.
Figure 2. Legal systems: control of an individual’s life activities.The locus of control of life activities can be internal (individualliberty) or external (coercive control by others). In highly regimentedsocial orders, such as the People’s Republic of China, one’s per-sonal choices are markedly restricted; in liberal social orders, suchas the US, the areas for unimpeded choice are much more numer-ous. In a metanormative social order, the only constraints on libertylie on the border, where one’s actions affect others.
metanormative.

ba
fsct
289Vol. 215, No. 2, August 2012 Sade Ethics of Health Care Reform
ETHICS OF CENTRAL PLANNINGDuring the lengthy debates in Congress that preceded thepassage of the ACA in March 2010, surprisingly little at-tention was paid to moral justification for collectivizinghealth care, but this was not always the case. The ethicssubgroup of President Clinton’s White House Task Forceon National Health Reform in 1993�1994 developed alist of principles and values that they described as “funda-mental national beliefs,” including, for example, universalaccess to health insurance, comprehensive benefits, equalbenefits, shared burdens, efficient management, and fairprocedures.15
Members of the ethics subgroup wrote a detailed analysisof the main ethical principles of the proposed law. Theysaid that equality is basic because health is a necessary con-dition for individuals to pursue their goals. Justice is foun-dational because it is a serious injustice when individualssuffer preventable loss of opportunity, pain and suffering,or loss of life for want of health care readily available tomost inhabitants of a country as wealthy as the US. Libertyis undermined when an individual is threatened by illnessor death. We are a single nation joined by community, theysaid, so there is a shared “concern and responsibility forone’s fellow members, especially those in need of help.”16
More recently, in 2007, the Ethical Force Program of theAmerican Medical Association found 3 core American val-ues underlying health care system reform: equality of op-portunity, justice, and compassion, which they justified ina manner similar to that of the earlier commentators.17
The principles and values these groups describe arebased on the assumption that broad agreement exists onwhat is meant by equality, justice, liberty, and compassion.This assumption is simply wrong—debate about what theymean is vigorous among philosophers and scholars in thesocial sciences and humanities. For current purposes,though, the important feature of these ethical principlesand values is that they are normative, that is, they imposeobligations or duties that require enforcement of rules,laws, and regulations to compel compliance.
Flaws of central planning ethicsAn important hidden assumption underlying the ethics ofcentral planning is that the promotion of human well beingis a legitimate concern of politics. There is a differencebetween recognizing that certain actions are desirable andmandating those actions by law. Legally compelling peopleto act for their own good requires justification, but philos-ophers and politicians who have advocated a central role forgovernment in the provision of health care have not pro-vided a convincing case. As I have argued, however, there isreason to doubt that a connection of desirable actions to
legal compulsion can be made rationally. pThis weakly grounded assumption has led to an unjus-tified insistence on normative, that is, prescriptive solu-tions to policy issues. Central planning disrupts nearly ev-ery aspect of self-directedness, thereby undermining thevery human flourishing the planners want to advance. Thearguments central planners offer to morally justify regulat-ing the lives of others are flawed. A few examples follow.
Liberty is lost to those who lack healthcare insuranceCentral planners claim that freedom is limited if healthinsurance is not available, so to protect liberty, everyone isentitled to health insurance.16 This idea fails to distinguishetween limitations imposed by facts of reality and thoserising from forceful interference by others.18 For example,
when I lived in Boston for the first half of my life, I couldchoose among several of the best health care facilities in theworld if I had a serious illness. I have lived in Charleston,SC, for the second half of my life. Charleston has excellenthospitals and physicians, but to obtain health care, mychoices are limited to a much narrower range than theywere in Boston. Despite these differences, I have beenequally free to choose among the available options in bothplaces—my liberty rights have not been infringed. Con-versely, the liberty rights of black Americans were violatedwhen they were prohibited by Jim Crow laws from usingcertain facilities, such as doctor’s offices, available only towhites, even though the law was on the side of segregation.Liberty rights are beyond the reach of positive law—theyare unalienable. Government has the power to constrainliberty, but not the right.4 The concept of liberty is notcomplicated. It means the unimpeded exercise of choiceamong available options, no matter how limited or expan-sive those options may be. Contrary to central planners,those who do not have health care insurance have not beendeprived of their liberty.9
A compassionate society must provide health careMany central planners have argued that benevolencegrounded in compassion is an important reason to have acentrally planned health care system. The American Med-ical Association’s Ethical Force Program says, “The tradi-tional value of compassion for the least fortunate among usdemands attention to the well-known effects of inadequateaccess to health care on individuals and families . . . A com-passionate society cannot tolerate such avoidable suffer-ing.”17 Society doesn’t have a brain and cannot think oreel—it is a metaphorical construct. Put simply, a compas-ionate society cannot exist—only thinking, feeling peoplean have compassion. But even if compassionate society isaken as a reality, the term still makes no sense. Coercing
eople into doing good deeds is not benevolence, yet gov-
clmatrt
tts
idehebi
mlga
pd
om
ig
uetufb
hlddi
admcasth
tWs
290 Sade Ethics of Health Care Reform J Am Coll Surg
ernment claims its health care programs exhibit benevo-lence while using its monopoly on the use of force to gen-erate the taxes that fund such programs.
Truly charitable giving comes from individuals,churches, synagogues, foundations, and other private char-ities. They manifest compassion and benevolence becausethey donate freely.9 Government programs, to the contrary,ompel compliance of those who provide the funds. Theegislators, executives, and judges who constitute govern-
ent misuse their power when they force on their citizensparticular vision of the values and virtues that comprise
he good life, when instead they should be protecting theight of its citizens to develop their own virtues and pursueheir own values.
Compassion and benevolence are important virtues, buthey cannot be duties that entitle some to take the fruits ofhe productive time and effort of others, without their con-ent, to use for their own purposes.
Justice demands a fair share of goods and servicesfor allThe claim that justice requires everyone to receive a fairshare of goods and services is poorly grounded becausewidespread disagreement surrounds the meaning of theideas of justice and fairness.19 Two of the many understand-ngs of justice are justice as equality—all people equallyeserve basic goods and services, regardless of theirffort or accomplishments—and justice as reciprocity—ard-working, productive people deserve what they’vearned and it is unjust for those who are unproductive toenefit from the labor of others. Which of these approachess more consistent with our nation’s culture?
A Pew Foundation international poll asked which wasore important—that everyone be free to pursue their
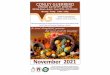
ife’s goals without interference from government, or thatovernment should play an active role in society to guar-ntee that no one is in need20 (Fig. 3). A significant major-
ity in the US—58%—favored freedom, the opposite of theresult in other developed countries and regions of theworld,21 in which the majority favored government sup-
ort. Since Colonial times, emphasis on individual free-om had been a persistent characteristic of our culture.
Health care exceptionalismPerhaps the most common argument in support of thecollectivization of health care is that the need for health careis categorically different from all other areas of human ac-tivity, even basic needs, such as food, clothing, and shel-ter.22 The idea of health care exceptionalism is based mostlyn moral intuitions—it just feels as though health care is
ore important than almost anything else—but moral rntuitions are, at best, an unreliable source of moraluidance.23
Two misunderstandings underlie the idea of health careexceptionalism: first, an unreasonably restrictive view ofwhat it means to be healthy and second, conflation ofhealth and health care.24 Many different activities contrib-
te to health, including the choice of a proper diet, routinexercise, and avoiding dangerous activities such as drinkingoo much alcohol or driving too fast. Less obvious contrib-tors to health are stress-reducing activities such as per-orming or listening to music and achieving an appropriatealance between work and play.For most people, health care is a minor component of
ealth. Achieving a proper balance of all the activities thatead to good health is highly individualized in light of in-ividual talents and abilities, so each person needs the free-om to determine how best to use personal time and lim-
ted resources to gain and maintain good health.If “health” were a positive right, that is, an entitlement,
s claimed by many central planners, then legislators have auty to enforce that right by ensuring access not only to theinor factor of health care, but to everything else that
ontributes to good health, such as properly chosen dietnd exercise facilities for maintenance of physical fitness. Ithould be clear that such a role for government is inconsis-ent with the notion of a free society, so if we believe that weave a free society, we cannot accept the idea of a positive
0
10
20
30
40
50
60
70
80
US Japan Canada W Europe E Europe
Figure 3. Pew Global Attitudes Project. This global survey asked thefollowing question: “What’s more important in (survey country) so-ciety – that everyone be free to pursue their life’s goals withoutinterference from the (state or government) OR that the (state orgovernment) play an active role in society so as to guarantee thatnobody is in need?” Responses in the US were different from thosein other developed countries and regions:21 a substantial majority inhe US favored freedom, unlike in Japan, Canada, East Europe, andest Europe (Australia and New Zealand were not included in theurvey).20 (Data derived from The Pew Research Center for the
People & the Press. Pew Global Attitudes Project 44-Nation MajorSurvey (2002). Question 34. 2002:T44.) Blue bar, freedom; red bar,government support; green bar, no answer.
ight to health or to health care.

yti(sei(
wfdf
291Vol. 215, No. 2, August 2012 Sade Ethics of Health Care Reform
THE POWER OF ECONOMIC FREEDOMThe idea that freedom to live their own lives is beneficial forindividuals and for society is supported by good empiricalevidence. The ethical principle of noninterference is re-alized economically in the form of free markets, which,in turn, are the clearest expression of economic freedom.Some of the best evidence for the power of liberty toadvance human welfare is found in the relations betweeneconomic freedom, economic growth, and humanhappiness.
Economic freedom in 141 countries has been analyzedusing 42 variables in 5 broad areas. National economiesgrow faster with increasing amounts of economic free-
Figure 4. Economic freedom and economic growth. Economicgrowth is linearly related to economic freedom.25 (Reprinted from:Gwartney J, Lawson R, Hall J. Economic Freedom of the World: 2011Annual Report. Vancouver, BC: Fraser Institute; 2011, withpermission.)
Figure 6. Economic freedom and literacy. Literacy is linearly relatedto economic freedom, and the greatest increase is among women.25
(Reprinted from: Gwartney J, Lawson R, Hall J. Economic Freedom ofthe World: 2011 Annual Report. Vancouver, BC: Fraser Institute;
2011, with permission.) Purple bar, women; blue bar, men.dom25 (Fig. 4). Life expectancy increases; it is about 20ears longer in countries with the most economic freedomhan in those with the least (Fig. 5). Literacy increases withncreasing economic freedom, especially among womenFig. 6). More economic freedom is associated with sub-tantially greater per-capita incomes (Fig. 7). Extreme pov-rty is inversely related to economic freedom—its lowestncidence is seen when economic freedom is greatestFig. 8).
Human happiness can be measured and is associatedith about 50% genetic variance.26 It is interesting, there-
ore, that a separate analysis using world economic freedomata along with several previously published instrumentsor measuring happiness, a nearly linear relationship was
Figure 7. Economic freedom and income per capita. Income percapita is linearly related to economic freedom.25 (Reprinted from:Gwartney J, Lawson R, Hall J. Economic Freedom of the World: 2011Annual Report. Vancouver, BC: Fraser Institute; 2011, with
Figure 5. Economic freedom and life expectancy. Life expectancy islinearly related to economic freedom.25 (Reprinted from: Gwartney J,Lawson R, Hall J. Economic Freedom of the World: 2011 AnnualReport. Vancouver, BC: Fraser Institute; 2011, with permission.)
permission.)

pt
s3l
RV
292 Sade Ethics of Health Care Reform J Am Coll Surg
found between economic freedom and human happiness27
(Fig. 9). If happiness can be taken as a measure of humanflourishing, then these data support the proposition thatfreedom is a key constituent of human flourishing.
IMPLICATIONS FOR HEALTH CARE REFORMLegislators do not have expertise in the wide range of prob-lems they are called on to repair, so they rely on groups ofexperts to develop policies addressing the problems. Thecritical difference between experts in the private sector andexperts in government is that governments have monopolypower that is ultimately backed by force, so governmentexperts do not face the competitive pressures that constrainthose in the private sector. In order to prosper, privateorganizations must satisfy the needs of their customers,because if they do not, customers can simply walk away andfind services elsewhere—not so for experts whose policiesare ultimately backed by law enforcement agencies.
Federal regulations have the force of law—they are re-ferred to as administrative law. As of 2009, the Code ofFederal Regulations contained 163,333 pages. In 2009alone, 3,503 new rules were added.28 Compliance withthese regulations costs the nation’s productive sectors morethan $1 thousand billion ($1 trillion) per year.29 The justi-fication for this crushing mountain of regulation is thatexternal controls are required to correct market failures, yetthose who argue for that need almost always fail to considerthe problem of government failures, of which our healthcare system is a good example.
Origins of our health care systemIn the late 19th century, most sick people were treated at
Figure 8. Economic freedom and poverty. Poverty is inversely re-ated to economic freedom.25 (Reprinted from: Gwartney J, Lawson, Hall J. Economic Freedom of the World: 2011 Annual Report.ancouver, BC: Fraser Institute; 2011, with permission.)
home and only the sickest went to hospitals. The increasing
use of hospitals in the early 20th century led to prepaymentlans, originally at Baylor University Hospital in 1929,hen Blue Cross and Blue Shield in the early 1930s.30
In the mid-1930s, Blue Cross gained exemption frominsurance regulations in exchange for charging lower ratesthan commercial insurance and insuring all comers. Soon,hospital services were reimbursed for their operating costsplus a percentage of the hospital’s capital, known as cost-plus reimbursement.31
Perversely, hospitals could prosper best not by the usu-ally effective method of decreasing their costs but by in-creasing their costs and expanding services and facilitiesunrelated to demand for them. Perverse incentives werealso firmly implanted in patients, who cared little about theprices that were paid on their behalf, because they paid onlya very small percentage out-of-pocket. The fundamentalproblem of our health care financing system today hasnever been properly addressed by previous attempts at re-form. The basic problem is this: because patients pay only10 cents out-of-pocket on every dollar spent for theirhealth care choices, they buy health care at a 90% discount,so, unlike their behavior in nearly all other areas of eco-nomic life, people are not prudent buyers of health carebecause they do not have the perception that they arespending their own money. Why buy a Kia when for only afew dollars more—a mere 10% of the actual pricedifference—you can be driving a Lexus? The perception ofhealth care at 90% discount is responsible for much of theuncontrolled inflation of health care costs of the last 50years. We were led into this situation a step at a time byfailures of government policy.
After the Blues solidly established prepayment for healthcare in the 1930s, wage and price controls during theWorld War II forced employers to attract workers they
Figure 9. Economic freedom and happiness. Happiness is linearlyrelated to economic freedom.27 (Reprinted from: Gropper DM, Law-on RA, Thorne JT. Economic freedom and happiness. Cato J 2011;1:237–255, with permission.)
needed by offering noncash benefits, specifically, health

wch
uaps(
e1ksccHcIMsT
293Vol. 215, No. 2, August 2012 Sade Ethics of Health Care Reform
insurance; the Internal Revenue Service ruled that healthinsurance was deductible when purchased by employers,but not deductible when purchased by individuals.32
Employer-based health insurance became an enormous taxdodge for both employers and employees. By 1947, theseinequities were solidly in place and positioned to lead ourhealth care system incrementally into its current state.
Those unsound policies led to a series of laws to attemptrepair of the damage they produced. Medicare and Medic-aid, in 1965, built on the deeply flawed, inflationary sys-tem already in place. The politically unpalatable but inev-itable massive increases in health care costs spawned byMedicare and Medicaid led to the Health MaintenanceOrganization Act of 1973; the National Health Planningand Resources Development Act of 1974; the Tax Equityand Fiscal Responsibility Act of 1982; the Health Insur-ance Portability and Accountability Act in 1994; the Medi-care Reform Act of 2004; and, most recently, the ACA (Fig.
Prepaid Health Insurance 1930sNWLB: HI exempt from wage controls 1940sIRS: HI deduc�ble for employers 1940s
M/M 1965
HMO 1973
NHPRD 1974
TEFRA 1982
HIPAA 1994
MRA 2004
ACA 2010
Figure 10. Successive laws for cost control. The foundation for ourmployer-based health insurance system was laid in the 1930s and940s by the development of prepayment for health insurance andey decisions by the NWLB and the IRS. Attempts were made by aeries of laws to control the resulting hyperinflation of health careosts; none provided more than temporary relief from health careost inflation.30,32 ACA, Patient Protection and Affordable Care Act;I, health insurance; HIPAA, Health Insurance Portability and Ac-ountability Act; HMO, Health Maintenance Organization Act; IRS,nternal Revenue Service; M/M, Medicare and Medicaid; MRA,edicare Reform Act; NHPRD, National Health Planning and Re-
ources Development Act; NWLB, National War Labor Board; TEFRA,ax Equity and Fiscal Responsibility Act.
10). All these expertly designed programs at the federal and t
state level have failed to achieve their main objective—costcontrol—while creating hundreds of thousands of pages offederal regulations and enormous amounts of mandatorypaperwork that increase the cost of health care, makinghealth insurance too expensive for millions of Americans.Worse, these programs have created a dangerously intrusivebureaucracy.
Friedrich von Hayek, a Nobel Laureate in economics,showed that prices in a free market are critically importantand arise from perceptions and preferences of a very largenumber of individuals. No expert or group of experts canpossibly acquire the price information needed to allocateresources correctly, so central planning by experts will even-tually fail.33
One of the leading economists of the 20th century, Lud-ig von Mises, argued that a centrally planned system
ould never succeed in the long run because the plannersave no way to allocate resources efficiently.34 Without the
price fluctuations driven by supply and demand in a freemarket, central planners cannot know where resources areneeded most, resulting inevitably in either shortages oroverproduction of some goods and services. The resultingproblems motivate laws and regulations attempting correc-tion, which lead to new unanticipated adverse conse-quences, attempted correction of the new problems, and soforth, in a downward spiral, which is precisely what we’veseen in our health care system (Fig. 10). Mises predictedthat a centrally planned economy ultimately will collapse, aprediction that proved prescient when the socialist econo-mies of Eastern Europe did in fact collapse in the late 1980sand 1990s.
The latest in the concatenation of policies attempting tocontrol costs of health care by fixing the failed policies ofthe past is the ACA. The ACA was passed and signed intolaw in great haste as the Democrats were about to lose theirsupermajority in the Senate, so, it suffers from prodigiouslength (2,700 pages), Gordian complexity, and numerousinternal contradictions that ensure it will be extensivelyrevised well into the future. We can still hope for substan-tial improvement.
Studies by the Congressional Budget Office and actuar-ies for the Centers for Medicare and Medicaid Servicesshow that the ACA’s goals of universal insurance coverageand reduced cost will not be achieved.35 The number of
ninsured will drop about in half by 2020, but will leavebout 23 million Americans still not covered (Fig. 11). Theroportion of the gross domestic product (GDP) con-umed by health care will actually be higher under the ACAFig. 12), and its cost from full implementation in 2014
hrough 2024 will be $2.7 trillion.
dTf
Cwk
Aia
294 Sade Ethics of Health Care Reform J Am Coll Surg
The centerpiece of the ACA, its insurance purchasemandate, has been found unconstitutional by 2 of the 3Circuit Courts of Appeals that have considered the issue,and the US Supreme Court has agreed to hear the case.36 A
ecision is expected by the end of this term, in June 2012.here appears to be a reasonable chance the ACA will be
ound to be unconstitutional in part or in whole.Whether or not the law is found to be unconstitutional,
ongress has the opportunity now to undo some of theorst aspects of the ACA by replacing them with free mar-et policies.
EFFECTIVE SYSTEMIC REFORMSThrough disregard of the principle of noninterference as itwas embodied in the original US Constitution, faulty pol-icies have reduced the financing of health care to a deplor-able state. It has taken more than 70 years to reach ourcurrent condition, so a relatively free market in health carecannot be achieved quickly. Markets are not perfect, norwill they repair all the problems the health care systemfaces. The point is, however, that government failures haveworse consequences than the market failures they aim tocorrect, and although markets are continuously self-correcting through what economist Joseph Schumpetercalled “creative destruction,”37 poorly conceived laws arerarely repealed—instead, they enter the spiral of legislativefixes that beget more failures and more losses of liberty, aswe have already seen.
In the modern world, the surest way to solve problems is
Figure 11. Number of uninsured under the Patient Protection andffordable Care Act (ACA). Although the number of uninsured Amer-
cans will drop by more than half, 23 million will remain uninsuredfter the ACA has been fully implemented.35 (Reprinted from: Tanner
MG. Bad Medicine: A Guide to the Real Costs and Consequences ofthe New Health Care Law. Washington, DC: Cato Institute; 2011,with permission. Source: Letter from Douglas Elmendorf, director,Congressional Budget Office, to House Speaker Nancy Pelosi,March 20, 2010.)
to encourage innovation, which is stimulated by competi- h
tive forces that work most effectively in a free market. Gov-ernment can have an important role in health care by sup-porting market institutions and facilitating innovation,which is the engine for improvement of any system, as wein surgery know very well. Some specific policy ideas mayindicate some of the ways government can help repair de-cades of damage.
Free market reforms: a few suggestionsTo encourage innovation in health insurance, Congressshould reform the inequitable tax system so that individu-als get the same tax deduction as employers.31 Legislatorsshould increase innovation through competition by allow-ing purchase of health insurance across state lines, as ispossible for nearly everything else in this country.38 Theyshould repeal forced purchase of unwanted benefits, so-called mandated benefits, under many state laws.39 Whenthe innovation that comes from competition drives costsdown, health insurance will become affordable for a largenumber of those currently uninsured.40
To encourage innovation in the provision of care, legis-lators should deregulate the health care sector to furtherincrease healthy competition, such as doing away with cer-tificate of need laws.38 They can support development of
Figure 12. Estimated increases in national health expendituresunder the ACA. A major goal of the ACA is cost control. According tothe chief actuary of the Centers for Medicare and Medicaid Services,the proportion of GDP consumed by the health sector will be higherthan it would have been without the new law.35 (Reprinted from:Tanner MG. Bad Medicine: A Guide to the Real Costs and Conse-quences of the New Health Care Law. Washington, DC: Cato Insti-tute; 2011, with permission. Source: Richard S Foster, chief actu-ary, Centers for Medicare and Medicaid Services, “EstimatedFinancial Effects of the ‘Patient Protection and Affordable HealthCare Act,” as amended, April 22, 2010.) ACA, Affordable Care Act;GDP, Gross Domestic Product. Dotted line, current law; solid line,under ACA.
igh-quality, accurate outcomes data to help patients and

igciva
295Vol. 215, No. 2, August 2012 Sade Ethics of Health Care Reform
their advisors in making health care decisions, for example,through tax breaks for developers of sophisticated risk-adjusted databases.
Congress should reform Medicare by instituting a meanstest for Part A, so that ordinary workers do not have to payfor Warren Buffet’s health care.41 It should give participat-ng seniors vouchers that will work like food stamps in arocery store—participants will have the same range ofhoices in the health insurance market as every other Amer-can, thereby strengthening the market. The size of theoucher should be adjusted according to the health statusnd financial resources of the enrollee.42
Many other reforms can also help to move us away fromineffective, ultimately harmful central planning for healthcare, toward a more effective, beneficial, and morally ap-propriate market system. A national health care policyguided by the ethical principle of noninterference will freethe health care market from burdensome and expensiveregulation, allowing physicians and surgeons to keep ourprofessional activities fully focused on our proper objective,care of and caring for our patients.
REFERENCES
1. Roosevelt FD. State of the Union Message to Congress. January11, 1944. Available at: http://www.fdrlibrary.marist.edu/archives/address_text.html. Accessed February 10, 2012.
2. Peplau H. Is health care a right? Affirmative response. Image(IN); 1974;7:4–10.
3. Eberl JT, Kinney ED, Williams MJ. Foundation for a naturalright to health care. J Med Philos 2011;36:537–557.
4. Sade RM. Medical care as a right: A refutation. New Engl J Med1971;285:1288–1292.
5. Narveson J. The medical minimum: zero. J Med Philos 2011;36:558–571.
6. Patient Protection and Affordable Care Act (2010), U.S. Pub. L.No. 111�148 and supplement Pub. L. No. 111�152, HealthCare and Education Reconciliation Act. Available at: http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi?dbname�111_cong_public_laws&docid�f:publ148.111.pdf and http://www.gpo.gov/fdsys/pkg/PLAW-111publ152/pdf/PLAW-111publ152.pdf. Accessed February 18, 2012.
7. Engelhardt HT. The Foundations of Bioethics. New York: Ox-ford University Press; 1996.
8. Friedman M. Capitalism and Freedom. Chicago: The Univer-sity of Chicago Press; 1962:7–21.
9. Kelley D. A Life of One’s Own: Individual Rights and the Wel-fare State. Washington, DC: Cato Institute; 1998:63–96.
10. Rasmussen DB, Den Uyl DJ. Liberty and Nature: An Aristote-lian Defense of Liberal Order. LaSalle, IL: Open Court Publish-ing Company; 1991: 32–40 and 63–97.
11. Ridley M. The Rational Optimist: How Prosperity Evolves.New York: HarperCollins; 2010.
12. Den Uyl DJ. The Virtue of Prudence. New York: Peter Lang;
1991.13. Rasmussen DB, Den Uyl DJ. Norms of Liberty: A PerfectionistBasis for Non-Perfectionist Politics. University Park, PA: Penn-sylvania State University Press; 2005.
14. The Declaration of Independence. Available at: http://www.ushistory.org/declaration/document/index.htm. Accessed Feb-ruary 18, 2012.
15. White House Domestic Policy Council. The President’s HealthSecurity Plan: The Clinton Blueprint New York: New YorkTimes Books 1993:11–13.
16. Brock DW, Daniels N. Ethical foundations of the Clinton ad-ministration’s proposed health care system. Jama 1994;271:1189–1196.
17. Levine MA, Wynia MK, Schyve PM, et al. Improving access tohealth care: a consensus ethical framework to guide proposals forreform. Hastings Cent Rep 2007;37:14–19.
18. Hayek FA. Constitution of Liberty. Chicago: Henry Regnery;1960:17.
19. DeGrazia D. Single payer meets managed competition: the casefor public funding and private delivery. Hastings Cent Rep2008;38:23–33.
20. The Pew Research Center for the People & the Press. PewGlobal Attitudes Project 44-Nation Major Survey (2002).Question 34. 2002:T44. Available at: http://pewglobal.org/files/pdf/185topline.pdf. Accessed February 20, 2012.
21. The United Nations Statistics Division. Composition of macrogeographical (continental) regions, geographical sub-regions,and selected economic and other groupings. Footnote c/. Avail-able at: http://unstats.un.org/unsd/methods/m49/m49regin.htm. Accessed February 27, 2012.
22. Daniels N. Just Health: Meeting Health Needs Fairly. New York:Cambridge University Press; 2007.
23. Hanson R. Why health is not special: errors in evolved bioethicsintuitions. Soc Philos Pol 2002:19:153–179.
24. Sade RM. A theory of health and disease: the objectivist-subjectivist dichotomy. J Med Philos 1995;20:513–525.
25. Gwartney J, Lawson R, Hall J. Economic Freedom of the World:2011 Annual Report. Vancouver, BC: Fraser Institute; 2011.Available at: http://www.freetheworld.com/2011/reports/world/EFW2011_complete.pdf. Accessed February 24, 2012.
26. Lykken D, Tellegen A. happiness is a stochastic phenomenon.Psychol Sci 1996;7:186–189.
27. Gropper DM, Lawson RA, Thorne JT. Economic freedom andhappiness. Cato J 2011;31:237–255.
28. Gattuso JL, Keen SA. Red Tape Rising: Regulation in theObama Era. Backgrounder No. 2394. Washington: HeritageFoundation. March 31, 2010, revised and updated April 8,2010. Available at: http://thf_media.s3.amazonaws.com/2010/pdf/bg_2394.pdf. Accessed February 20, 2012.
29. Crain WM.The impact of regulatory costs on small firms. Avail-able at: http://archive.sba.gov/advo/research/rs264tot.pdf. Ac-cessed February 20, 2012.
30. Sade RM. Foundational ethics of the health care system: themoral and practical superiority of free market reforms. J MedPhilos 2008;33:461–497.
31. Goodman JC, Musgrave GL. Patient Power: Solving America’sHealth Care Crisis. Washington, DC: Cato Institute; 1992.
32. Helms RB. Tax policy and the history of the health insuranceindustry. February 29, 2008. Available at: http://www.taxpolicycenter.org/tpccontent/healthconference_helms.pdf. AccessedFebruary 20, 2012.
33. Hayek FA. Individualism and Economic Order. Chicago: Uni-
versity of Chicago Press. 1948:77.
3
3
3
3
3
296 Sade Ethics of Health Care Reform J Am Coll Surg
34. von Mises L. Planned Chaos. New York: Foundation for Eco-nomic Education; 1947.
5. Tanner MG. Bad Medicine: A Guide to the Real Costs andConsequences of the New Health Care Law. Washington, DC:Cato Institute; 2011. Available at: http://www.cato.org/pubs/wtpapers/BadMedicineWP.pdf. Accessed February 24, 2012.
6. Liptak A. Justices to hear health care case as race heats up. NewYork Times. November 14, 2011:A1.
7. McCrawTK.Prophetof Innovation: JosephSchumpeter andCreativeDestruction. Cambridge: Harvard University Press; 2007.
8. Kling A. Crisis of Abundance: Rethinking How We Pay for
Health Care. Washington, DC: Cato Institute; 2006.9. Strayer J. Health Insurance Choice. NCPA Brief Analysis No.523. Dallas: National Center for Policy Analysis; 2005. Avail-able at: http://www.ncpa.org/pdfs/ba523.pdf. Accessed Febru-ary 20, 2012.
40. Herzlinger R. Who Killed Health Care? America’s $2 TrillionMedical Problem—and the Consumer-Driven Cure. New York:McGraw-Hill; 2007.
41. Cowen T. Means testing for Medicare. New York Times. July 20,2008.
42. Ryan P. A roadmap for America’s future: Medicare/Medicaid.Available at: http://www.roadmap.republicans.budget.house.
gov/Issues/Issue/?IssueID�8520. Accessed February 20, 2012.







![Conley s Motion[1]](https://img.dokumen.tips/doc/110x75/577d358a1a28ab3a6b90bbc2/conley-s-motion1.jpg)