Embed Size (px)
Citation preview

* Correspondi
1876-1399/$ - se
http://dx.doi.org
Clinical Simulation in Nursing (2014) 10, e47-e52
www.elsevier.com/locate/ecsn
Featured Article
Health Care Educator Training in Simulation:A Survey and Web Site Development
Diana M. Taibi, PhD, RNa,*, Suzie Kardong-Edgren, PhD, RN, ANEF, CHSEbaAssistant Professor, Department of Biobehavioral Nursing and Health Systems, University of Washington, Seattle, WA98105, USAbResearch Associate Professor, Jody DeMeyer Endowed Chair in Nursing, Boise State University, Boise, ID 83725, USA
KEYWORDSsimulation training;needs survey;online training;online education;simulation
ng author: dmtaibi@uw.
e front matter � 2014 Int
/10.1016/j.ecns.2013.05.
AbstractBackground: Simulation is becoming ubiquitous in nursing education, but many educators do nothave the necessary training to use simulation effectively.Methods: This article describes a collaborative process by which our training initiative gathered dataon regional training needs of health care educators and designed in-person and online educationalresources to improve education for nurses and other health professions.Results: Our online survey showed that only 23% of the 66 respondents had used simulation in teach-ing. The training topics rated most helpful were teaching interprofessional communication, leading apostsimulation debriefing, and integrating simulation into course curricula. Based on this survey, wedeveloped and publicly disseminated four basic and three advanced online simulation courses that canbe taken by educators of nursing and other health professionals at no cost.Conclusions: Funds for faculty development in simulation are generally scarce. The InCITE simulationonline courses provide no-cost basic and reliable education in the use of simulation.
Cite this article:Taibi, D. M., & Kardong-Edgren, S. (2014, January). Health care educator training in simulation: A sur-vey and web site development. Clinical Simulation in Nursing, 10(1), e47-e52. http://dx.doi.org/10.1016/j.ecns.2013.05.013.
� 2014 International Nursing Association for Clinical Simulation and Learning. Published by ElsevierInc. All rights reserved.
Introduction
Simulation is becoming ubiquitous in nursing education. Infact, some evidence suggests that simulation might beuseful in the future for a majority of clinical learning(Jeffries, 2009). Harder (2009) suggests that the increasingaffordability of simulators in the late 1980s and the launchof a journal devoted solely to nursing simulation have
edu (D. M. Taibi).
ernational Nursing Association for Clinica
013
enhanced the diffusion of innovation and almost guaranteedthat simulation would become a major teaching strategy.Interest in simulation is increasing rapidly for a multitudeof reasons, including increasing restrictions placed onfaculty and students in clinical sites, lack of clinicalplacements, and fewer inpatients in the hospital and morerapid patient turnover. In addition, some nursing studentsnow seek out nursing education programs specifically basedon a program’s use of simulation.
National and regional surveys have provided evidenceon the trends and challenges facing simulation in nursing.
l Simulation and Learning. Published by Elsevier Inc. All rights reserved.

Simulation Survey and Web Site e48
The first large-scale survey of simulation adoption innursing was completed by Nehring and Lashley (2004),followed thereafter by smaller regional U.S. surveys(Adamson, 2010; Sole, Guimond, & Amidei, 2013). Thelargest study of simulation adoption and use in U.S.
Key Points� This article dissemi-nates a free onlineresource for simula-tion training foreducators.
� An entire section ofthe InCITE Websiteis devoted to interpro-fessional education.
� Teaching interpro-fessional education,debriefing, and curri-cular integration ofsimulation were iden-tified as high needtraining areas.
nursing education wasrecently published by theNational Council of StateBoards of Nursing. This sur-vey tracked and docu-mented current simulationuse in approximately 1,670U.S. nursing programs(Hayden, 2010; Kardong-Edgren, Willhaus, Bennett,& Hayden, 2012). Further-more, a 2012 internationalnursing simulation surveywas conducted by therecently formed Interna-tional Nursing SimulationOrganization (Gore, VanGele, Ravert, & Mabire,2012). Overall, these sur-veys show that nursing fac-
ulty and programs are interested in using simulation andare taking steps toward integrating simulation activitiesinto courses. However, many schools have been caughtoff guard by the simulation phenomenon and are nowscrambling to buy manikins with no budget for facultydevelopment and only ad hoc plans for curricular integra-tion. Adamson (2010) found most nursing programs under-budgeted for faculty development and curricularintegration, with these activities comprising only 1% to7% of the total simulation budget.
Nursing faculty respond to simulation with varying levelsof enthusiasm. Many feel pressured to learn and adoptsimulation pedagogy with limited time and resources whilecontinuing to maintain the current curriculum (Jensen,Meyer, & Sternberger, 2009; Rothgeb, 2008). Jansen,Johnson, Larson, Berry, and Brenner (2009, p. e11) foundthat nursing faculty were reluctant to adopt simulationbecause of a lack of time, training, space, equipment, sched-uling, funding, and staffing and the inability to engage allstudents equally. Various approaches have been used toaddress such barriers to simulation. Some regions haveformed consortiums for sharing resources and educationalopportunities in simulation (Coleman et al., 2011; Jeffrieset al., 2013; Sportsman et al., 2009; Waxman & Telles,2009). Another approach to address faculty training needsis sharing resources and educating faculty through Websites. Organizations with Web sites disseminating simula-tion educational materials include that of the Quality andSafety in Nursing Education Consortium, the NationalLeague for Nursing Simulation Innovation ResourceCenter, and the California Simulation Alliance.
pp e47-
This article presents the efforts of the InterprofessionalCollaboration for Integrative Technologies in Education(InCITE) in assessing and addressing the need for trainingto increase the effective adoption of simulation in nursingand health care education. The first stage of this work wasdevelopment, distribution, and analysis of a needs assess-ment of five large western states (Washington, Wyoming,Alaska, Montana, and Idaho; the WWAMI region). Thesecond stage of the work was development of a large Website that houses free simulation education for educators ofnurses and other health professions. The purpose of thisarticle is to present our survey findings, which corroborateother recent reports of the persistent and pressing need forsimulation training (Adamson, 2010; Hayden, 2010;Howard, Englert, Kameg, & Perozzi, 2011) and to dissem-inate a free resource that could potentially meet this need.
Methods
Regional Needs Survey: Survey Design andDistribution
The purpose of InCITE is to address the technology trainingneeds of educators in the WWAMI region, an area thatgeographically covers one-fifth of the United States. Earlyin this process, we surveyed specific training needs onsimulation, clinical informatics, telehealth, and technology-enhanced learning (which encompasses distance learning,among other technologies); only simulation results arereported here. The questions on the Web-based surveywere developed by InCITE faculty and reviewed by keyInCITE personnel with experience in the areas of technol-ogy to be assessed. The survey was approved by theUniversity of Washington (UW) Human Subjects Boardand was administered online using the UW Catalyst surveytool. The full survey included a total of 63 items. Thisreport includes 18 items: 8 items pertaining to demographic,geographic, and professional information and 10 itemspertaining to simulation. Respondents rated various trainingtopics on a scale of 0 (not helpful) to 4 (very helpful).
We sought to recruit up to 300 survey respondents. Thesurvey stipulated that respondents must be directly orindirectly involved in clinical education in any healthprofession in an academic or clinical setting. This includedadministrators, lecturers, clinical instructors, laboratoryinstructors, course instructors, and clinical preceptors.The URL for the Web-based survey and an invitation toparticipate were distributed via listservs for college anduniversity faculty in the WWAMI region, as well aslistservs for the Council on Nursing Education in Wash-ington State. Particular effort was made to reach individualsworking in nonmetropolitan statistical areas (Ingram &Franco, 2012). According to this definition, a metropolitanstatistical area contains ‘‘at least one Census Bureau-defined urbanized area of 50,000 population or more’’
e52 � Clinical Simulation in Nursing � Volume 10 � Issue 1

Simulation Survey and Web Site e49
(Ingram & Franco, 2012, p. 3) and nonmetropolitanstatistical areas contain either an urban core of 10,000 to49,999 or no urban core. The URL for the survey andrequest for completion were also distributed to clinical sitesthroughout the WWAMI region by InCITE’s rural andclinical partners.
Results
Persons responding to the simulation questions were 66individuals from throughout the WWAMI region. Demo-graphics are presented in Table 1. The majority of therespondents were nurses (86%), and the age distribution of
Table 1 Respondent Characteristics
Variable Categories n (%)
Age <40 years old 4 (6.1)40-49 years old 12 (18.2)50-59 years old 30 (45.5)>60 years old 17 (25.8)Not reported 3 (4.5)
Ethnicity Latino 1 (1.5)Not Latino 65 (98.5)
Race American Indian-NativeAmerican
1 (1.5)
White 61 (97.0)Other 2 (3.0)Declined/Unknown 2 (3.0)
Profession* Nursing 60 (90.9)Other (chiropractic,dental hygiene)†
2 (3.0)
Not specified 5 (7.6)Teaching* Nursing: practical nursing
or associate’s degree19 (28.8)
Nursing: baccalaureate 38 (57.6)Nursing: master’s orpostmaster’s
34 (51.5)
Nursing: doctoral 7 (10.6)Medicine 2 (3.0)Staff education 2 (3.0)Other (audiology, pharmacy, dentalhygiene, public health)
3(4.5)
TeachingLocation*,‡
Metropolitan 51 (77.3)Nonmetropolitan 10 (15.2)State-wide teaching via distancewithin WWAMI
14 (21.2)
Teaching via distance tonon-WWAMI U.S. sites
9 (13.6)
Note.WWAMI ¼ Washington, Wyoming, Alaska, Montana, and Idaho.
* Respondents could select more than one answer option.† The respondent who reported certification as a chiropractor was
also a nurse.‡ Metropolitan ¼ metropolitan statistical area, contains ‘‘at least one
Census Bureauedefined urbanized area of 50,000 population or more.’’
Nonmetropolitan ¼ nonmetropolitan statistical areas, contain either
an urban core of 10,000 to 49,999 or no urban core (Ingram &
Franco, 2012, p. 3).
pp e47-
the sample reflected the demographics of this workforce;70%were over age 50 and 88%were over age 40. Themajor-ity of respondents identified ethnically as not Latino (n¼ 65)and racially as white (n ¼ 61). All respondents had at leastbaccalaureate level education. Most of the sample taught ina nursing program (n ¼ 63, ranging from associate degreeor diploma to PhD or DNP), with 52 individuals (79%)teaching at a practice-entry level (associate’s degree,diploma, or baccalaureate degree). Some respondents taughtin other fields, including medicine (n ¼ 2), clinical stafftraining (n ¼ 2), pharmacy (n ¼ 1), dental hygiene (n ¼ 1),public health (n ¼ 1), and audiology (n ¼ 1). Thirty-onerespondents (47%) taught in more than one program.
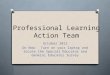
Among those interested in simulation, only 23% hadactually used this teaching method. Respondent ratings ofeach of the potential training areas are shown in Figure 1,which shows the helpfulness of potential training area insimulation as rated by all respondents. Figure 2 shows thehelpfulness of potential training needs in simulation asrated by nonmetropolitan respondents only. All trainingtopics were highly endorsed by the respondents as beinghelpful. The most highly endorsed (greatest percentage ofrespondents rating the item ‘‘helpful’’ or ‘‘very helpful’’)training need was teaching interprofessional communica-tion in a simulation (80%), followed by leading a postsimu-lation debriefing (70%) and integrating simulation intocourse curricula (66%). The lowest need was mechanicallyoperating a simulator (49%).
Ten (15%) respondents reported teaching in nonmetro-politan areas. None of the respondents taught in bothmetropolitan and nonmetropolitan areas. All topics weremore highly endorsed by nonmetropolitan than metropol-itan respondents (in fact, no respondents rated a topic ‘‘nothelpful’’). The most strongly endorsed topics were leadinga debriefing session and writing clinical simulationscenarios (both rated ‘‘helpful’’ or ‘‘very helpful’’ by90% of respondents). The least useful topic to nonmetro-politan educators was gaining support among faculty (50%rated ‘‘helpful’’ or ‘‘very helpful’’).
In summary, this regional survey assessed the self-reported simulation training needs of health care instructorsin the western United States. The survey showed that,despite widespread interest in simulation, less than onequarter of the respondents had actually used this teachingmethod. Results from the National Council of State Boardsof Nursing study (Hayden, 2010) indicated more widespreadusage and understanding of simulation; however, the ques-tionnaire in that study was mailed to deans and directors.This survey was sent to faculty via listservs and in-stateeducation links such as the Council on Nursing Educationin Washington State, reaching a different group of potentialresponders. In addition, the majority of responders in theHayden (2010) survey indicated that although they wereusing simulation, they had received no formal simulationtraining. Many users were trained exclusively by themanikin vendors. To address such training needs as those
e52 � Clinical Simulation in Nursing � Volume 10 � Issue 1

Figure 1 Simulation training needs rated by all metropolitan and nonmetropolitan respondents.
Simulation Survey and Web Site e50
found in our survey results and in the literature, the InCITESimulation Workgroup developed both online and in-personinstructor training, as described in the next section.
Simulation Resources
Our survey results indicated that basic skills such asdebriefing and simulation writing were of great interest tosurvey respondents. This made the development anddistribution of high-quality simulation education modulesimperative. Given that interprofessional education (IPE) wasthe most highly rated training need, an entire section of theInCITE Web site was devoted to IPE (http://collaborate.uw.edu/resources-and-publications/ipe-resources.html). Thissection of the Web site includes resources for botheducators and students. Furthermore, the InCITE Web siteincludes a comprehensive Simulation Team Training Toolkit(http://collaborate.uw.edu/educators-toolkit/interprofessional-simulation-team-training-faculty-toolkit/simulation-team-trainin) that includes all the informational resources neededfor planning, teaching, and evaluating an IPE training activity(Figure 3). The toolkit contains detailed and condensedguides for instructors and facilitators, an online videoexample of a real interprofessional student simulation, aTeamSTEPPS (Team Strategies and Tools to Enhance
Figure 2 Simulation training needs rated
pp e47-
Performance and Patient Safety, developed by the Depart-ment of Defense’s Patient Safety Program in collaborationwith the Agency for Healthcare Research and Quality)training lesson, evaluation forms for students and faculty,and a validated preepost assessment tool to assess the pro-gressive learning of students. The toolkit materials havebeen used for 3 years successfully in training activities bythe InCITE team, with student evaluations ranging from4.18 to 4.75 on a 1 to 5 scale (5 ¼ best).
The InCITE Simulation Workgroup also produced fourbasic and three advanced online courses on generalsimulation topics (Table 2). The materials were developedfor use by educators of various health professions acrossdifferent settings and program, ranging from communitycollege and baccalaureate education to graduate programsto postgraduate continuing education. These seven freecourses, ranging in length from 12 to 30 minutes, werewritten and posted to the University of Washington’s Centerfor Health Science Interprofessional Education, Researchand Practice’s Web site (http://collaborate.uw.edu). Themodules integrate hyperlinks that connect learners immedi-ately to simulation resources, such as articles, templates forplanning and debriefing, and ideas for staging simulations.To date, lessons in the basic 100 course series have beencompleted by up to 590 unique users and in the 200 series
by nonmetropolitan respondents only.
e52 � Clinical Simulation in Nursing � Volume 10 � Issue 1

Figure 3 A screenshot of the InCITE Simulation Team Training Toolkit for interprofessional education.
Simulation Survey and Web Site e51
by up to 240 users. Five free online courses in distancelearning and eight in clinical informatics were alsoproduced for the Web site. Since the launch of the Website in 2009, the courses have been taken by persons fromnine countries, across five continents. One nursing
Table 2 Open Access Simulation Courses Developed Based onSurvey Findings
Basic coursesSim 101 Introduction to clinical simulationSim 102 Pedagogical approaches in simulation for
developing critical thinkingSim 103 Designing and writing a simulation scenarioSim 104 Briefing and debriefing: the key to learning in
simulationAdvanced coursesSim 201 How to evaluate learning using simulationSim 202 Matching human patient simulators to clinical
learning outcomesSim 203 Bringing realism to simulation
pp e47-
program, Boise State University, is now using the onlinecourses as required training materials for faculty newto simulation and debriefing (R. Macy, personalcommunication).
Discussion
The growth of simulation and educational technologyappears to be continuing unabated, although funds forfaculty development are decreasing or nonexistent in manyplaces. Over the past 10 years, studies have reported a lackof adequate training as a barrier to effective adoption andimplementation of simulation (Adamson, 2010; Hayden,2010; Jansen et al., 2009). Our survey shows that, despitepersistent or increasing pressures to use simulation, facultyremain inadequately trained and simulation remains under-used. Our survey adds to prior findings by providing spe-cific information about topics on which faculty reportneeding training. Our findings may help others to prioritizetheir training activities.
e52 � Clinical Simulation in Nursing � Volume 10 � Issue 1

Simulation Survey and Web Site e52
Conclusions
Expert instruction in emerging educational technologieslike simulation at low or no cost, in a time of fiscalausterity, is highly desirable and in demand. The InCITEsimulation courses provide basic reliable education in theuse of simulation. The training meets the pressing need ofeducation for novices in simulation and also provides forskill development of those with simulation experience.These resources are available at no cost to aid instructors inclinical and academic settings to use simulation forimproving the effectiveness and efficiency of the trainingof health professionals.
Acknowledgments
This project was supported by funds from the HealthResources and Services Administration’s Faculty Develop-ment: Integrated Technology into Nursing Education andPractice initiative, grant number U1KHP09543.
References
Adamson, K. (2010). Integrating human patient simulation into associate
degree nursing curricula: Faculty experiences, barriers, and facilitators.
Clinical Simulation in Nursing, 6(3), e75-e81. http://dx.doi.org/10.
1016/j.ecsns.2009.06.002.
Coleman, P. A., Dufrene, C., Bonner, R. J., Martinez, J., Dawkins, V.,
Koch, M., & Norman, G. (2011). A regional partnership to promote
nursing instructor competence and confidence in simulation. Journal of
Professional Nursing, 27(6), e28-e32. http://dx.doi.org/10.1016/
j.profnurs.2011.09.003.
Gore, T., Van Gele, P., Ravert, P., & Mabire, C. (2012). A 2010 survey of
the INACSL membership about simulation use. Clinical Simulation in
Nursing, 8(4), e125-e133. http://dx.doi.org/10.1016/j.ecns.2012.01.002.
Harder, N. B. (2009). Evolution of simulation use in health care education.
Clinical Simulation in Nursing, 5(5), e169-e172. http://dx.doi.org/10.
1016/j.ecns.2009.04.092.
pp e47-
Hayden, J. (2010). Use of simulation in nursing education: National survey
results. Journal of Nursing Regulation, 1(3), 52-57.
Howard, V. M., Englert, N., Kameg, K., & Perozzi, K. (2011). Integration
of simulation across undergraduate curriculum: Student and faculty
perspectives. Clinical Simulation in Nursing, 7(1), e1-e10. http:
//dx.doi.org/10.1016/j.ecns.2009.10.004.
Ingram, D. D., & Franco, S. J. (2012). NCHS urban-rural classification
scheme for counties. Vital Health Statistics, 2(154). National Center
for Health Statistics. Retrieved June 18, 2013, from http://wonder.cdc.
gov/wonder/help/CMF/sr02_154.pdf
Jansen, D. A., Johnson, N., Larson, G., Berry, C., & Brenner, G. H.
(2009). Nursing faculty perceptions of obstacles to utilizing
manikin-based simulations and proposed solutions. Clinical
Simulation in Nursing, 5(1), e9-e16. http://dx.doi.org/10.1016/
j.ecns.2008.09.004.
Jeffries, P. R. (2009). Dreams for the future for clinical simulation. Nursing
Education Perspectives, 30(2), 71.
Jeffries, P. R., Battin, J., Franklin, M., Savage, R., Yowler, H., Sims, C.,.,
& Dorsey, L. (2013). Creating a professional development plan for
a simulation consortium. Clinical Simulation in Nursing, 6(9), e183-
e189. http://dx.doi.org/10.1016/j.ecns.2012.02.003.
Jensen, R., Meyer, L., & Sternberger, C. (2009). Three technological
enhancements in nursing education: Informatics instruction, personal
response systems, and human patient simulation. Nurse Education in
Practice, 9(2), 86-90.
Kardong-Edgren, S., Willhaus, J., Bennett, D., & Hayden, J. (2012).
Results of the National Council of State Boards of Nursing National
Simulation Survey: Part II. Clinical Simulation in Nursing, 8(4), e117-
e123. http://dx.doi.org/10.1016/j.ecns.2012.01.003.
Nehring, W. M., & Lashley, F. R. (2004). Current uses and opinions
regarding human patient simulators in nursing education. Nursing Edu-
cation Perspectives, 25(5), 244-248.
Rothgeb, M. K. (2008). Creating a nursing simulation laboratory:
A literature review. Journal of Nursing Education, 47(11), 489-494.
Sole, M. L., Guimond, M. E., & Amidei, C. (2013). An analysis of simu-
lation resources, needs, and plans in Florida. Clinical Simulation in
Nursing, 9(7), e265-e271. http://dx.doi.org/10.1016/j.ecns.2012.03.003.
Sportsman, S., Bolton, C., Bradshaw, P., Close, D., Lee, M., Townley, N.,
& Watson, M. N. (2009). A regional simulation center partnership:
Collaboration to improve staff and student competency. Journal of
Continuing Education in Nursing, 40(2), 67-73.
Waxman, K. T., & Telles, C. (2009). The use of Benner’s framework in
high-fidelity simulation faculty development: The Bay Area Simulation
Collaborative model. Clinical Simulation in Nursing, 5(6), e231-e235.
http://dx.doi.org/10.1016/j.ecns.2009.06.001.
e52 � Clinical Simulation in Nursing � Volume 10 � Issue 1