Embed Size (px)
Citation preview
Health Assessment
Intro
• Nurses perform assessments regularly in nearly every health care setting
• ( )care- beginning of shift• Nursing home/home care- ( ) or
monthly
Assessment Techniques
• 5 basic assessment techniques– Inspection– ( )– Percussion– Auscultation– ( )
Inspection
• ( ) exam of body parts or areas• Important to know what is normal for age
before trying to determine abnormal• Watch all movements• Requires adequate ( )
Inspection
• Requires ( ) exposure of body parts• Inspect each area for:– Size, shape, color, symmetry, position, and
presence of abnormalities• Compare each side of body if possible• Ask the ( )
Palpation
• Uses sense of ( )• Detects resistance, resilience, roughness,
texture, temperature, and mobility• Can be done with ( )
Palpation
• Different parts of hand to detect specific characteristics– Back of hand is sensitive to ( )– Pads of fingertips detect changes in texture, size,
shape, consistency, and pulsation– Palm of hand is sensitive to ( )
Palpation
• Make sure patient is relaxed and comfortable• Ask patient to point out sensitive areas• Palpate tender areas ( )• Watch for ( ) signs of
discomfort• Consider the patient’s condition, the area, and
the reason for palpation
Palpation
• Light precedes deep• Light- apply pressure slowly and gently- ( )• Check tender areas further• Deeper- ( )
Percussion
• Tapping the body with ( )• Evaluates size, borders, and consistency of
body organs and discover fluid in body cavities• Identifies location, size, and density of
underlying structures • Character of sound depends on density of
underlying ( )
Auscultation
• Listening with a ( ) to sounds produced by body
• Listen in a quiet environment• Need to know normal sounds from each body
structure

Auscultation
• Need good hearing ( )• Good ( )• Knowledge of how to use stethoscope• Need to place directly on skin
Auscultation
• 4 characteristics of sound:– ( )- # of sound wave cycles
generated per second; higher the frequency the higher the pitch
– Loudness-amplitude of sound wave (loud or soft)– ( )- sounds of similar frequency
and loudness from different sources (ex: blowing, gurgling)
– Duration- length of time that sound lasts (short, medium, long)
Olfaction
• Sense of ( ) to detect abnormalities
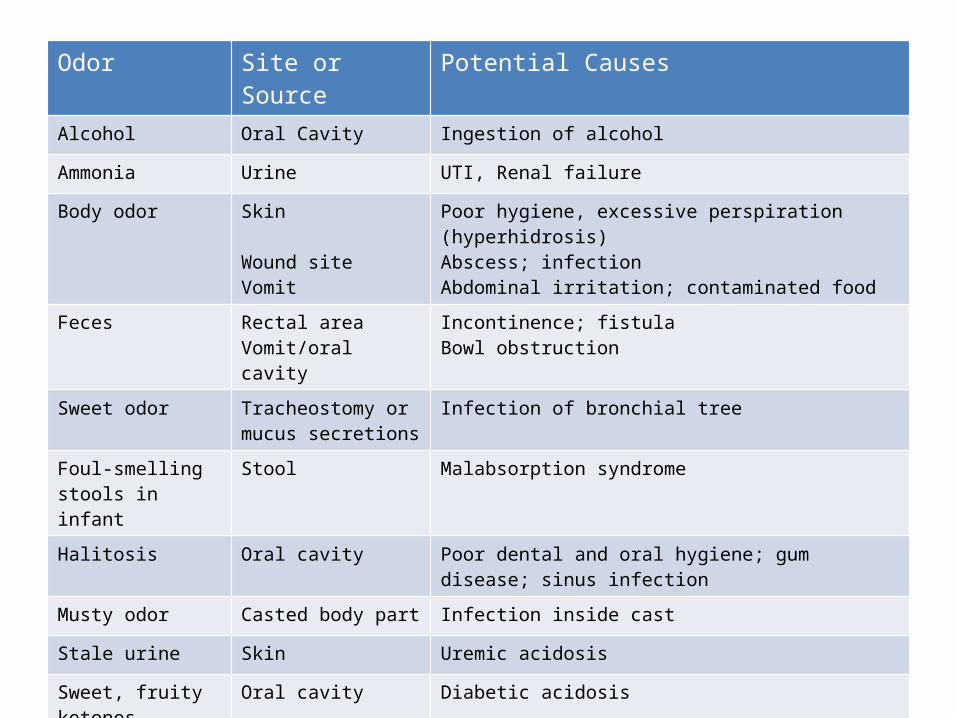
Odor Site or Source Potential CausesAlcohol Oral Cavity Ingestion of alcohol
Ammonia Urine UTI, Renal failure
Body odor Skin
Wound siteVomit
Poor hygiene, excessive perspiration (hyperhidrosis)Abscess; infectionAbdominal irritation; contaminated food
Feces Rectal areaVomit/oral cavity
Incontinence; fistulaBowl obstruction
Sweet odor Tracheostomy or mucus secretions
Infection of bronchial tree
Foul-smelling stools in infant
Stool Malabsorption syndrome
Halitosis Oral cavity Poor dental and oral hygiene; gum disease; sinus infection
Musty odor Casted body part Infection inside cast
Stale urine Skin Uremic acidosis
Sweet, fruity ketones Oral cavity Diabetic acidosis
Sweet, heavy, thick odor
Draining wound Pseudomonas infection
Preparation for Assessment
• Provide ( )– Close door and pull curtain– In home- examine in bedroom
• Promote ( )– Warm, comfortable temperature– Loose-fitting gown or pjs
Prep. For assessment
• Adequate ( )• Control of outside noises• Precautions to prevent interruptions• Place bed at ( ) level

Preparing the Patient
• Allow patient to empty bowel or bladder• Use simple terms and thoroughly explain what
will be done, what they will feel, and what the patient can do
• Provide access to body parts while not exposing others
• Reduce ( )
Preparing Patient
• Help patient into position• Pace assessment according to patient’s
physical and ( ) tolerance• Encourage to ask questions and report
discomfort• Have a 3rd person of patient’s gender in room
during assessment of genitalia
Skill Guidelines
• Prioritize assessment based on patient’s presenting S/S
• Organize the exam- offer ( ) periods• Always identify using at least ( ) patient
identifiers other than room number• Follow standard precautions• Record quick notes to facilitate accurate
documentation; use appropriate terminology
General Survey
• Includes:– ( )– Height and weight- recent changes in weight– General behavior- emotional state– Appearance- hygiene, skin and body image
Assessment
• Note any acute distress• Review graphic sheet for previous V/S and
consider factors that may alter• Determine primary ( )• Identify normal height, weight and BMI– How much and how fast have they gained/lost
• Review past I&O records• Assess allergies- esp. ( )
Cultural Considerations
• Mexican American- eye behavior is important; always touch a child when examining him or her
• ( )- excessive eye contact or touch is offensive
• African-Americans- dialect requires careful communication to prevent interpretation errors
• American Indians- eye contact is considered disrespectful
General Survey Steps
1. Be sure to note verbal and nonverbal behaviors. Determine LOC and orientation
2. Obtain temp., pulse, respirations, and BP3. Observe gender, race, and age4. Always rephrase or ask a similar question if
unsure a patient understands5. If responses are inappropriate, ask short, to-
the-point questions that they should know

General Survey Steps
6. If unable to respond to questions of orientation, offer simple commands7. Assess affect and ( )8. Watch interaction with caregiver, children, or spouse. 9. Observe for signs of ( )
Signs Of Abuse-Child
• Blood on underclothing• Pain in genital area• Pain w/ ( )• Vaginal or penile discharge• Difficulty sitting or walking• Physical injury inconsistent with caregiver’s
account of how it occurred
Signs of Abuse- Female
• Injury or trauma inconsistent with reported cause
• Obvious injuries to face, neck, breasts, abdomen, and genitalia
Signs of Abuse-Older Adult
• Injury or trauma inconsistent w/ reported cause• Injuries in unusual locations (neck or genitalia)• Pattern injuries• Parallel injuries• Burns• Fractures• Poor hygiene• Poor nutrition
General Survey Steps
10. Assess ( ) (slumped, erect, bent). Note alignment of shoulders and hips. 11. Assess body movements. Purposeful? Tremors? Any body parts immobile? 12. Assess ( )
General Survey
13. Observe ( ) and grooming. – Observe color, distribution, quantity, thickness,
and texture of hair– Inspect condition of nails– Assess for body odor
General Survey
14. Inspect exposed skin and ask if patient has noticed any changes including:– Pruritus, oozing, bleeding– Change in appearance of moles, bumps, nodules– ( )
15. Inspect color of face, oral mucosa, lips, conjunctivae, sclera, palms of hands and nail beds
General Survey
16. Use ungloved fingertips to ( ) skin surfaces.– Use back of hand to palpate temp.– Assess skin turgor by grasping fold of skin on
sternum, forearm, or abdomen w/fingertips– Release skin fold and note ease and speed in
which in returns
General Survey
• 17. Inspect character of any secretions: note color, odor, amount, and consistency
• 18. Assess for pressure areas. If see any redness, place fingertip over area, apply gentle pressure and then release. ( )





























