Embed Size (px)
Citation preview

WHO/EHG/97.12.EDistr.: General
Original: English
Health and Environmentin Sustainable Development:
Five Years after the Earth Summit
EXECUTIVE SUMMARY
Programmes on Health and Environment
World Health Organization
Geneva
June 1997
i

iii
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Table of Contents
Page
Chapter 1 A New Perspective on Health .......................................................... 1
Chapter 2 Driving Forces Behind Current Health-and-Environment Trends...... 5
Chapter 3 Major Human Activities Affecting Environmental Quality ............... 9
Chapter 4 From Environmental Quality to Exposures and Risks....................... 15
Chapter 5 Health Conditions in an Environmental Context .............................. 23
Chapter 6 Integrated Policies, Strategies and Actions:Progress Since the Earth Summit ..................................................... 31
Chapter 7 Conclusions..................................................................................... 35
References ....................................................................................................... 37

The basic human need for a safe envi-ronment — one which provides cleanwater, and adequate food and shelter, andin which different people can live togeth-er in peace — is the same for all of us.
Five years have passed since the EarthSummit and numerous initiatives havebeen launched at local, national and glob-al level to highlight the need for health-and-environment action. So it is timelyto start the analysis of how we are doingas a community of peoples in terms ofmeeting this need, how development canprovide resources for health protection,but also how such development can threat-en health through degradation of natur-al resources. This analysis should high-light problems, but also give examples ofsolutions that will bring us closer tosustainable development. The dreams andaspirations of a healthy future for the nextgeneration can be accomplished only ifwe use our current knowledge wisely andtake action in solidarity.
Extract from the foreword ofDr Hiroshi Nakajima,Director-General, WHO.
HOW ARE WE DOING?
Human society is more able than everbefore to secure good health for eachcommunity. But the remarkable sus-tained improvement in human healthobserved in some societies has not beenrealized everywhere, as illustrated inTable 1.1. The contrast between manyof the “least developed countries”,where more than 20% of children diebefore they reach the age of 5, and typ-ical “developed countries”, where lessthan 1% of children will do so, indi-cates that we are far from doing as wellas we would like or in fact could.
FIVE YEARS SINCE THEEARTH SUMMIT
In response to the concern created bysuch disparity, the Earth Summit heldin Rio de Janeiro, Brazil, in June 1992heralded a new approach to nationaland international development and envi-ronment planning. In brief, the world’sleaders recognized the importance ofinvesting in improvements to people’shealth and their environment as a pre-requisite for sustainable development.Continuing commitment to securinghuman health and a healthy environ-ment is now widespread, as evidencedby a number of declarations and state-ments that have emanated from recentinternational conferences (Table 1.2).Indeed, a new perspective on “health”is clearly evolving whereby health is aconcern for almost every sector in soci-ety and not just the “health sector”.
ENVIRONMENTAL THREATSTO HUMAN HEALTH
Environmental threats to human healthare numerous. For ease of discussionand priority-setting, they can be divid-ed into “traditional hazards” associat-ed with lack of development, and “mod-ern hazards” associated with unsus-tainable development.
Traditional hazards related to poverty and“insufficient” development are wide-rang-ing and include: lack of access to safedrinking-water; inadequate basic sanita-tion in the household and the commu-nity; indoor air pollution from cookingand heating using coal or biomass fueland inadequate solid waste disposal.
Modern hazards are related to devel-opment that lacks health-and-envi-
1
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
CHAPTER 1
A New Perspective on Health

ronment safeguards, and to unsus-tainable consumption of naturalresources. They include: water pollu-tion from populated areas, industryand intensive agriculture; urban airpollution from motor cars, coal pow-er stations and industry; climate change;stratospheric ozone depletion and trans-boundary pollution.
The changing pattern of environmen-tal health hazards and associated healthrisks — moving from “traditional” to“modern” with time and economicdevelopment — is known as the “risktransition”.
A HEALTH-AND-ENVIRONMENTCAUSE–EFFECT FRAMEWORK
But although we can identify anddescribe individual environmentalhealth hazards, the relationship betweenhuman health and the environment ishighly complex. For instance, each ofthe traditional and modern hazardsis associated with a variety of aspectsof economic and social development,which complicates analysis of theirincidence and impact.
Thus it is useful to adopt a frameworkwithin which the different interactionsoperating between environmental healthhazards and the environment can beanalysed. A “health-and-environmentcause–effect framework” (Fig 1.3) has
been devised to view the develop-ment–environment–health relation-ship, to reveal and highlight importantinteractions, and to help pinpoint pos-sible entry points for public healthinterventions.
FINDING SOLUTIONS TOENVIRONMENTAL HEALTHPROBLEMS
As can be seen, action can be takenat each step in the framework (Fig1.3). Different levels of interventionare illustrated in Fig 1.4, which isbased on acute respiratory infections(ARI) in children. When quantified,the multiple-causation framework canbe a powerful guide to designing cost-effective and timely interventions.It also provides a means for examin-ing possible synergies among inter-ventions.
SUPPORTIVE ENVIRONMENTSFOR HEALTH
Too great a focus on environmentalhealth problems, however, can lead usto forget that the environment can alsobe “supportive” of health, exerting apositive influence in much the sameway as a healthy diet. A supportiveenvironment for health is free frommajor health hazards, satisfies the basicneeds of healthy living, and facilitatesequitable social interaction.
2
EXECUTIVE SUMMARY
Table 1.1
Infant mortality, child mortality, water supply and sanitation coverage, and GNP percapita in six countries
Infant mortality Child mortality*rate* (0-5 years, Access to safe Access to adequate
(0-1 years) cumulative) water** sanitation** GNP perCountry (per 1000) (per 1000) (% of population) (% of population) capita***(US$)
Sweden 5 6 100 100 24 740Chile 15 17 96 71 3 170Philippines 39 48 84 75 850Ghana 77 113 56 42 430Guinea-Bissau 135 207 57 20 240Afghanistan 159 251 10 8 (<200)+
+ estimate, data not available *1995 **1994 ***1993
Source: compiled from data in WHO. 1996a.
Table 1.2
Key elements of declarations andstatements of particular relevance tohuman health
Rio Declaration, Principle 1: “Human beings are at the centreof concerns for sustainable development. They are entitled toa healthy and productive life in harmony with nature.”
UNCEDRio de Janeiro, Brazil, 1992
“All countries should give priority to measures that improvethe quality of life and health by ensuring a safe and sanitaryliving environment for all population groups through measuresaimed at avoiding crowded housing conditions, reducing airpollution, ensuring access to clean water and sanitation,improving waste management, and increasing the safety ofthe workplace.”
International Conference on Population and DevelopmentCairo, Egypt, 1994
“In addressing inequalities in health status and unequal accessto health-care services between women and men, govern-ments and other actors should promote an active and visiblepolicy of mainstreaming a gender perspective in all policiesand programmes, so that…an analysis is made of the effectsfor women and men respectively.”
Fourth World Conference on Women Beijing, People's Republic of China, 1995
“… to sustain our global environment and improve thequality of living in our human settlements, we commit our-selves to sustainable patterns of production, consumption,transportation and settlements development; pollution pre-vention; respect for the carrying capacity of ecosystems; andthe preservation of opportunities for future generations. In thisconnection, we shall cooperate in a spirit of global partner-ship to conserve, protect and restore the health and integri-ty of the Earth's ecosystem.”
United Nations Conference on Human Settlements,HABITAT II
Istanbul, Turkey, 1996
“… a peaceful, stable and enabling political, social andeconomic environment is the essential foundation whichwill enable States to give adequate priority to food security,poverty eradication and sustainable agriculture, fisheries,forestry and rural development.”
World Food Summit Rome, Italy, 1996
“We decided to include this issue (i.e. health and environment)for the first time in our agenda to emphasize that the pro-tection of public health has been and remains a fundamen-tal objective of environmental policies.”
G7 meeting of Ministers of Environment(Canada, France, Germany, Italy, Japan, UK and USA)
Cabourg, France, 1996
Sources: UN, 1993; UN, 1995b; FAO, 1996a; UN, 1996b; UNCHS,1996a. Chairman’s summary of the Meeting of the Ministers ofthe Environment in Cabourg, France, 9–10 May, 1996.

3
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Effect
Exposure
State
Pressure
Drivingforce t
Well-being Morbidity Mortality
Externalexposure
Absorbeddose
Targetorgan dose
Naturalhazards
Resourceavailability
Pollutionlevels
Production Consumption Wasterelease
Populationgrowth
Economicdevelopment
Technology
Action
Fig. 1.3
Health and environment cause–effect framework
This diagram is a simplified abstraction of thecomplex cause–effect relationships operatingbetween driving forces, environmental pres-sures, envitonmental states, human exposures,health effects, and actions aimed at minimiz-ing these effects. The various boxes provideexamples of factors acting at each level. Arrowsmark the potential connections that exist betweenvarious causes and effects in environmentalhealth.
Sources: modified after Kjellström & Corvalán,1995 and Briggs, Corvalán & Nurminen, 1996.
Exposure
Effect
State
Pressure
Drivingforce
ARI
ts
Actio
n
Crowding Growth of slums
Dust particles,irritants
Chilling Infectious agents
Indoor airpollution
Indoor climate Poor housingquality
Availability andquality of food
Cookingemissions
Poverty Householdenergy policy
Housingpolicy
Agriculturalpolicy
VaccinationCase management
Landdegradation
Malnutrition
Fig. 1.4
Health and environment cause–effect framework for ARI in children
This framework, based on the model given in Fig. 1.3, provides examples of major cause–effect relationships affecting one spe-cific group of diseases: namely, acute respiratory infections (ARI). Additional linkages could take the form of education policyand the literacy rates of mothers, both of which could increase early detection and treatment of ARI in children.

4
EXECUTIVE SUMMARY
Creation of supportive environmentsfor health depends upon full partici-pation, however: not only in terms ofcontributory actions from all membersof society but also in terms of coop-erative action between sectors.
POWER AND PARTICIPATIONOF BOTH MEN AND WOMEN
Representation of women is particu-larly important in improving healthstatus, since women have key roles inall societies with respect to basic liv-ing conditions. Yet women remain large-ly underrepresented at most levels ofgovernment, especially in ministerialand other executive bodies. Morewomen in politics and decision-mak-ing positions would help to redefinepriorities, place new items on the agen-da, and provide new perspectives onmainstream political issues.
INTERSECTORAL ACTIONSFOR A HEALTHYENVIRONMENT
Along the same lines, an intersectoralapproach is the most effective meansof formulating environmental healthpolicy, since it can help to ensure thatpriorities are coherent and do not con-flict with those of individual sectors.Ministries of health and environmenthave key roles to play in such activi-
ty. Joint programmes involving theseand other ministries would enablemuch more to be achieved in envi-ronment and health. International agen-cies can also contribute much to envi-ronmental health policy development:through collaborative assessments, forexample.
HEALTH FOR ALL: THE WAYAHEAD
Action must follow policy. The WHOHealth-for-All Policy has provided aframework for translating the preven-tive health message of Agenda 21 (themajor document to emerge from theEarth Summit) into practical action tobe undertaken by the institutions andprofessionals of the health and othersectors. It is currently being updatedand renewed so that it meets the chal-lenges of the 21st Century effectively,and is able to light “the way ahead” forhealth-and-environment actions towardssustainable development.
“I would like to urge those whohave already achieved the bestindices to assist and cooperate ful-ly with the endeavours of thosewho are yet to attain the goal ofHealth for All”Mr S.I. Shervani, President of theWorld Health Assembly, 1997.

THE DRIVING FORCESCONCEPT
Driving forces create the conditionsin which environmental health threatscan develop or be averted, as indi-cated in the health-and-environmentcause–effect framework (Fig. 1.3).These driving forces are often associ-ated simultaneously with a numberof health-and-environment issues, ashighlighted in Box 2.1. Governmentpolicies and programmes — which willvary according to the prevailing val-ue system — change the directionand/or magnitude of driving forcesand can therefore alleviate or exac-erbate a broad array of environmen-tal health threats.
Driving forces considered in our analy-sis are: population dynamics; urban-ization; poverty and inequity; techni-cal and scientific developments; con-sumption and production patterns, andeconomic development. Not consid-ered in our analysis, since it lies beyondthe scope of the book, but neverthe-less important, is the political system,or democratic governance, or lack there-of. Undemocratic societies are at highrisk of not achieving sustainable devel-opment, since they do not incorporateall the relevant stakeholders in deci-sion-making.
POPULATION DYNAMICS
Population driving forces have threebasic components: the total numberand geographical distribution of peo-ple, age-distribution, and changes tothese distributions caused by popula-tion movement. In its simplest form,increased population density leads tointensified human activities that if mis-
managed contribute to environmentaldamage and resource depletion, bothof which can have negative direct orindirect effects on human health.
At the same time, high fertility ratescoupled with decreasing mortality haveincreased the dependency ratio sig-nificantly in many developing coun-tries, helping to create ageing popu-lations. While a sign of successful pub-lic health policy and action, ageingpopulations bring with them a differ-ent set of disease prevention and health-care needs.
Population mobility is also causingshifts in the distribution, compositionand environmental impact of popula-tions. Population movement is seenespecially in relation to rural–urbanand rural–rural migration. Both areoften associated with economic entrap-ment, unemployment and hunger, allof which may drive populations to seeka better standard of living elsewhere.Population movement also occurs as aresult of warfare and environmentaldegradation. The rapid increase in theflow of refugees over the past decadeis illustrated in Figure 2.4.
URBANIZATION
Cities generate a large part of a nation’seconomic activity, and create poten-tial efficiencies not found elsewhere,as well as advantages in the deliveryof education, health and other socialservices. But given their concentrationof people and activities, and their greaterlevels of consumption and consumerism,and dependence on machines and tech-nologies, cities generate considerablewaste and pollution. Urban growthalso means greater dependence on
5
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
CHAPTER 2
Driving Forces Behind Current Health-and-Environment Trends

transport systems, generating yet fur-ther pollution, and risk of accidents.The resulting public health challengesare daunting, but with appropriate poli-cies and action programmes, health incities can be improved.
POVERTY AND INEQUITY
Poverty and inequity are two of themost important contributory factorsto poor environmental conditions andpoor health.
Poverty as reflected in global incomeinequity is actually increasing. In 1970,the richest 20% of humanity had rough-ly 30 times more income than the poor-est 20%. Today, the richest fifth receivemore than 60 times as much as thepoorest fifth. The net worth of theworld’s 358 richest people is larger
than the combined annual income ofthe poorest 45% of the world’s popu-lation (2300 thousand million people).
On a more general level, inequity isseen with respect to geographic area,gender and race/ethnicity (Box 2.5).
Poor local environmental conditionsprobably affect women more than anyother group — primarily by creatingadditional pressures and increasingwomen’s workload.
SCIENCE AND TECHNOLOGY
In the past three decades science andtechnology have been two of the mostdecisive driving forces for economicdevelopment, especially in developedcountries. They have played, and willcontinue to play, a significant role notonly in the search for new knowledgeand more efficient means of agricul-tural and industrial production, butalso in saving lives, improving health,improving environmental conditionsand promoting human development(Table 2.2). Technological developmentscan be polluting and wasteful, how-ever, and may create serious risks to environment and health. The preven-tion and reduction of such risks arethus key issues for sustainable devel-opment.
CONSUMPTION ANDPRODUCTION PATTERNS
Affluence, by most common defini-tions, means increased per capita con-sumption of food, goods and services.But increased consumption and pro-duction deplete natural resources andproduces waste, which can have severeeffects on the environment and humanhealth. Three of the most importantconsumption issues in terms of sus-tainability are: diet (particularly theconsumption of meat), consumptionof certain raw materials and persistentchemicals, and the consumption of fos-sil fuels and associated carbon dioxide(CO2) emissions.
Dietary composition and food con-sumption per capita are key driving
6
EXECUTIVE SUMMARY
Box 2.1
Elements of sustainable development
Value systems
Population growthPoverty and inequities
Technological developmentConsimption patterns
Economic developments
Trading patternsTechnology transfer
Financial flowsInternational agreements
Agriculture, industry,energy, construction,tourism, healthcare,
etc.
Land, forest,biodiversity, minerals,
atmosphere, fresh water,oceans,
etc.
Food, fuels,manufacturing,
transportation, housing,drinking-water, sanitation,
etc.
Meeting needsAlerting the living environment
Modifying risksChanging options for the future
Land degradation,waste dumps, air pollution,water pollution, workplace
hazards, ozone layerdepletion, climate change.
that impact
and produce
which influence
that determine
are driving forces are international influences
Sectoral developments in Natural Resource Use
Goods and services
Health and welfare ofcurrent and future generations by
Disservices
Sustainable development can be described in terms of theelements in this figure, interlinking in a logical manner: thedriving forces, intermediate elements and the eventual impactor effect on the health and welfare of current and future gen-erations.
Source: Mr Nitin Desai, Under-Secretary-General for PolicyCoordination and Sustainable Development, UN.
Asia 5.1 Europe 0.7Latin America 0.4North America 1.4
Oceania 0.1Africa 3.0
1985
Total 10.7 million
Asia 6.8Europe 0.8
Latin America 1.2
North America 1.4Oceania 0.1
Africa 4.6
1990
Total 14.9 million
Asia 7.9
Europe 6.5
Latin America 0.1North America 0.9
Oceania 0.1Africa 11.8
1995
Total 27.3 million
Fig. 2.4
Refugees and other persons ofconcern to UNHCR by region — 1985, 1990, 1995
Source: UNHCR, 1995.
7
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
forces because they heavily influenceagricultural use of land and water, withimpacts on environmental quality andhealth.
Consumption of raw materials canaffect health and environment if thoseraw materials are associated with greaterenvironmental health risks. Exampleshere include the toxic metals: lead,cadmium, mercury and chromium.Use of persistent organic pollutants(POPs) is also of great concern (Box2.8). It is the rich countries who con-sume the greatest proportions of theworld’s raw materials and the mostdangerous chemicals.
More insidiously, changes in the com-position of the atmosphere have result-ed from our unsustainable reliance onnatural resources in the quest for high-er living standards. Although not theonly factor at play, fossil fuel com-bustion for the generation of energyand for transportation is significant.Fossil fuel combustion is leading tohigher CO2 levels. CO2 is one of theprincipal greenhouse gases (GHGs).
ECONOMIC DEVELOPMENT
Overall life expectancy and other healthindicators have improved for thosebenefiting from economic develop-ment. Economic growth in itself is notsufficient, however, to reduce pover-ty. Furthermore, if economic devel-opment is misguided, poorly plannedor inadequately regulated, people’svulnerability to environmental healthhazards is increased.
In many countries an “environmen-tal health hazard transition” has occurredin tandem with economic development.That is, a shift from traditional haz-ards to modern hazards has beenobserved. In developing countries,though, this transition is ongoing, mean-ing that the modern hazards of indus-trial development become establishedbefore the traditional hazards of pover-ty have been significantly reduced.Some communities can therefore besaid to live in the “worst of both worlds”.
Box 2.5
Examples of inequity in health by socioeconomic group, geographical area,gender and race/ethnicity
By socioeconomic group
The life expectancy at birth of the most disadvantaged population group in Mexico is 20years less than that of its most affluent group.Adults in Saõ Paulo, Brazil, in the late 1980shad mortality rates that were two to three times higher if they worked in nonprofessionalrather than professional jobs. In Bolivia, most public spending on health goes towardscare for people belonging to the upper two income quintiles, although these groups alreadyhave the best health status. Disparities in health between rich and poor are also apparentwithin developed countries, although they are usually smaller; wealthy groups have the mostconcentrated medical attention, eat better, and can afford to live in environmentally cleanand disaster-free areas.
By geographical area
In Nigeria, the average life expectancy in one region, Borno, is only 40 years—18 years lessthan in the Bendel region.Although only 39% of the population of Côte d'lvoire lives in cities,at least 80% of the country's public health expenditure is directed towards urban areas. InLima, Peru, the infant mortality rate is 50 per 1000 live births, while in some rural areas itis as high as 150 per 1000.
By gender
A study in India showed that female infants were almost twice as likely to die by the ageof two as were males, and concluded that the most likely explanation was the differentbehaviour of families towards male and female children, not biological differences.Anotherreport concluded that the death of one out of every six female infants in India, Bangladeshand Pakistan was due to neglect and discrimination. Studies in Bangladesh found that boysunder 5 years of age were given 16% more food than girls the same age. Additionally, evi-dence is mounting that adolescent and adult women may not receive an appropriate pro-portion of available food within the family.
By race/ethnicity
In Guatemala, poverty and malnutrition during the 1980s was much higher among indige-nous children than among non-indigenous children. In 1990 in South Africa death rates fornon-white men were double those of white men, and more than four times as much mon-ey was spent on healthcare for whites than for blacks.
Sources: Batliwala, 1987; Das Gupta, 1987; Vogel, 1988; Chatterjee & Lambert, 1989; UNPF, 1989; Gittelsohn, 1991; UNDP,1991; Psacharaopoulos et al., 1993; UN, 1993; Unidad de Análises de Políticas Sociales, 1993; World Bank, 1993; Pan AmericanSanitary Bureau/UN-ELAC, 1994; UNDP, 1994; Yach & Harrison, 1995.

8
EXECUTIVE SUMMARY
THE FOUNDATIONS OFSUSTAINABILITY
These driving forces very much deter-mine whether a society is proceedingtowards or away from sustainability.Some of the trends that have evolvedsince the Earth Summit threaten sus-tainable development, especially thoseresulting in increased pressure on landand water resources, increased house-hold and hazardous waste, and increasedconflict between the economic imper-atives of a “globalizing” industry andthe health-and-environment protec-tion needs of people.
Box 2.8
Persistent organic pollutants
Considerable political attention has recently focused on persistent organic pollutants (POPs).POPs are organic compounds that have long half-lives in the environment and undergo slowphysical, chemical and biological degradation. They are able to pass through ecosystems becauseof their high vapour pressure and can travel great distances, both locally and globally. These char-acteristics mean that they may pose a special threat to the environment and human health. POPsinclude DDT, polychlorinated biphenyls, furans, chlordane, heptachlor, aldrin,dieldrin and endrin.
Many POPs are used in or arise from industry, agriculture and disease vector control. POPsmay also be created unintentionally, as by-products. Stockpiles of unwanted POPs are signifi-cant cause for concern.
POPs have high lipid solubility and therefore bioaccumulate in the fatty tissues of livingorganisms. They pose a special risk to human health and the environment since they mimic thefunction of steroid compounds such as hormones potentially leading to disruption of the endocrinesystem. Human exposure to POPs occurs via diet, occupation, accidents and the indoor envi-ronment, particularly in those developing countries where POPs are used in tropical agriculture.
It is widely accepted that the use of such substances cannot be considered sustainable.Increasingevidence of the long-range transport in the environment of these substances and the consequentthreats they pose to the whole globe, has prompted the international community to call for urgentglobal action to reduce and eliminate releases and emissions of these chemicals.
Among the twelve POPs under initial consideration for international action, DDT is the onlyinsecticide still in use for public health purposes. The use of DDT in public health programmes,notably for malaria control, has been the subject of much controversy for many years.Vector-bornediseases—malaria is one of the most significant—are major threats to human health, and socialand economic development. DDT has made a major contribution to the eradication, or virtual erad-ication of malaria from a number of countries and remains a most valuable tool, particularlysince the options for malaria control are limited. Use of DDT has declined, however, following devel-opment of vector resistance, reduction in its global production and adverse publicity.
Further options to minimize the use and impacts of POPs include Improving the availabilityof information and expertise on alternatives to POPs (through information exchange and educa-tion programmes) and guidance on the selection of replacements for POPs.This guidance shouldcover non-chemical as well as chemical alternatives, and include advice on the factors to be con-sidered in choosing alternatives.
Sources: IPCS, 1995a; IFCS, 1996.
“The quality of growth is as impor-tant as its quantity”Mr J.G. Speth, Administrator ofUNDP, 1996.
Table 2.2
Examples of new technologies which have positive health-and-environment impacts
Technology Positive impact on health and environmentImproved biomass stoves/burners Reduced indoor/outdoor air pollution
Greenhouse gas “neutral”*More efficient fuelwood use
Biogas stoves and lights Reduced indoor/outdoor air pollutionReduced dependence on power suppliesImproved recycling of organics**
Heat pump technology for space heating Negligible indoor/outdoor air pollutionNo greenhouse gas emissions
Photovoltaic energy conversion systems No indoor/outdoor air pollutionNo greenhouse gas emissionsReduced dependence on power supplies
Genetically improved crops Increased yieldsReduced dependence on pesticides
Catalytic converters and lead-free petrol Reduced air pollution from carsElectric vehicles Reduced emission of air pollutants along roadsHCFCs and HFCs as CFC alternatives Reduced stratospheric ozone depletionFibreglass cabling for telephone lines Vastly reduced use of copperLow water-use irrigations systems Reduced water use and waterloggingNew alloys and plastics in manufacturing industry Reduced wasteBiological pest control methods Reduced use of toxic chemicals
*The growing of biomass fuel (i.e. mostly trees) absorbs exact-ly the same amount of CO2 as is released in its combustion(i.e. it is neutral in terms of greenhouse gas emissions).
**Emissions produced during the production and completeburning of biogas are more oxidized and less harmful thanthose that would have been produced following the decay ofe.g. vegetable and plant waste, and organic household waste.

9
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
HOW DRIVING FORCES CREATEENVIRONMENTAL PRESSURE
The atmosphere, fertile soils, freshwa-ter resources, the oceans, and the ecosys-tems they support, play a key role inproviding humans with shelter, foodand safe water, and the capacity to recy-cle most wastes. However, the pressuresexerted by the driving forces are inmany instances increasing. They relateto household wastes, fresh water use,land use and agricultural development,industrialization and energy use.
HOUSEHOLD WASTES
Gaseous household wastes arise main-ly from heating and cooking. They con-tribute substantially to both outdoorand indoor air pollution. Liquid wastesare the by-products of domestic activ-ities; their disposal and treatment variesenormously by region. In Fig. 3.1 thevariability in rural and urban sanita-tion, for instance, can be seen for fourmajor regions. Of the unserved in devel-oping countries (2900 million), 80%live in rural areas.
Development efforts have been madeto improve provision of sanitation ser-vices by central and local governments,and household themselves. But popu-lation growth is outstripping these.Fig. 3.3 shows coverage projected to theyear 2000 for developing countries, byeach major region and in total.
In unserved areas faeces are recycled foruse in agriculture or deposited on landwithout prior destruction of pathogens.Not surprisingly, infectious diseases suchas diarrhoeal diseases, schistosomiasisand hepatitis are endemic, and some-times epidemic, in such areas.
Solid waste can also create environ-mental health problems. It consistsmainly of non-hazardous materialssuch as paper and plastic packagingmaterial, glass, food scraps and otherresidues. However, it generally alsocontains small quantities of hazardoussubstances such as paints, medicines,solvents, cleaning materials and bat-teries, leading to potential chemicalexposures. Production of householdand municipal solid waste continuesto increase worldwide, both in absoluteand per capita terms. Estimated typi-cal municipal waste production percapita increases with rising averageincome (Table 3.3). Encouragingly,however, industrial concerns in manydeveloped countries are realizing thatminimization of waste production canimprove efficiency and reduce costs.
FRESH WATER
For a large percentage of the world’spopulation, water supplies are nei-ther safe nor adequate. Currently,over 1000 million people do not haveaccess to an adequate supply of safewater for household consumption.Moreover, the world’s freshwaterresources are limited and unevenlydistributed over the global land mass.
Demand for water is neverthelessincreasing in several sectors — fordrinking-water (domestic needs), foodproduction (agriculture) and prod-uct manufacturing (industry). Wateruse figures differ significantly in termsof continent, region, country and area(Fig. 3.5) and type of use, but global-ly, total demand for water increasedby six times between 1900 and 1990,more than double the rate of popula-tion growth for the same period. Some
CHAPTER 3
Major Human Activities AffectingEnvironmental Quality

10
EXECUTIVE SUMMARY
water uses — such as irrigation foragriculture — are highly wasteful.Not surprisingly, water scarcity todayis increasingly becoming a problemof regional and even sub-continentalproportions. Evidently, it is particu-larly acute in dry zones, where com-petition between agricultural, indus-trial, domestic needs is often fierce.
Global freshwater resources are threat-ened not only by overexploitation, how-ever, but also by poor managementand ecological degradation. Untreatedsewage is discharged into rivers andlakes, industrial wastes are dumpedinto water bodies, and run-off fromagricultural fields treated with herbi-cides and pesticides is leading to watercontamination. Industrial development,the exponential growth of human set-tlements and the ever-increasing useof synthetic organic substances, arealso having serious adverse impactson freshwater bodies. Many surfaceand groundwaters are now contami-nated with nutrients, heavy metals andPOPs (see Box 2.8).
LAND USE AND AGRICULTURALDEVELOPMENT
Competition for land appears to beintensifying between sectors and pro-duction systems. Agriculture, in par-ticular, can be expected to becomean even more dominant form of landuse. Population increase and the finiteextent to which further land can beconverted to agricultural uses, meanthat per capita arable land availabili-ty is becoming an issue.
Agricultural production carries sever-al risks. Thus extension and intensi-fication of agricultural production sys-tems, together with fluctuation inthe supply of and demand for agri-cultural produce are causing shifts inthe environmental determinants of thehealth status of local communities.Some of these are masked or com-pounded by simultaneous demographicand socioeconomic shifts. Major envi-ronmental health risk factors of agri-cultural development are presented inTable 3.8.
Fig. 3.1
Sanitation coverage byregion — 1994
Fig. 3.3
Sanitation services coverage indeveloping countries
Source: WHO/UNICEF, 1996a.
Source: WHO/UNICEF, 1996a.
Urban served 44%
Ruralunserved
12%
UrbanUnserved 20%
Ruralunserved
17%UrbanUnserved20%
Urbanserved19%
Ruralserved16%
Urbanserved19%
Rural served 10%
Rural served 24%
Rural served 9%
81 million
473 million
Rural unserved 50%
707 million
Rural unserved 59%
3122 million
Western Asia
Urban served 54%Latin America and the Caribbean
Urban unserved 15%Africa
Urban unserved 12%Asia and the Pacific
2.602.87
3.31
1.47 1.51 1.57
404464
566
229 243 265
2.03 2.212.48
0.89 0.92 0.95
4755
65
136 177 239
304 296 285
25 26
32
0
1
2
3
4
5
0
200
400
600
800
1000
0
200
400
600
800
0
1
2
3
4
0
20
40
60
80
100
v
Popu
latio
n (1
000
mill
ion)
Popu
latio
n (1
000
mill
ion)
Popu
latio
n (m
illio
n)Po
pula
tion
(mill
ion)
Popu
latio
n (m
illio
n)
1990 1994 2000
1990 1994 2000
1990 1994 2000
1990 1994 2000
1990 1994 2000
West Asia
Asia and Pacific
Latin America and the Caribbean
Africa
All developing countries
Population served Population unserved

11
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
INDUSTRIALIZATION:IMPROVED PROSPECTS ANDADVERSE CONSEQUENCES
Industrialization is central to economicdevelopment and improved prospectsfor human well-being. But if properabatement technology is not used, indus-try becomes a major source of air, waterand soil pollution, hazardous wastes andnoise. Industrial workers are often athighest risk of health impacts.Furthermore, developed countries haveexacerbated the environmental prob-lems now being experienced by devel-oping countries through transfer of haz-ardous wastes, industries and technologies.
Major industrial impacts also arise fromsmall-scale industry. In developingcountries, small-scale industry con-tributes substantially to economic devel-opment, but can create problems forenvironment and health if environ-mental safeguards are not used.
If industrial development is to become
more environmentally sound, three tran-sitions must be completed. Firstly, envi-ronmental considerations must be incor-porated into all aspects of planning fornew industry. Secondly, techniques mustbe developed which more easily and flex-ibly control pollution within a legal frame-work which provides strong incentives,particularly economic incentives, to min-imize the release of pollutants and the pro-duction of waste, and which places greateremphasis on the “polluter pays” principle.Thirdly, producers of hazardous productsshould be required to be responsible forthose products “from cradle to grave”, i.e.from production to safe disposal.
ENERGY
Energy plays a critical role in basichuman survival. Too little energy —through its effects on nutrition and foodsafety, and on chilling — has importantimplications for health. Energy is alsocrucial to transportation and industri-al processes. However, production anduse of energy, if not properly controlled,
Table 3.3
Typical quantities of municipal wasteproduction per capita
Type of countryWaste generation(Kg/capita/day)
High-income countries 0.8 to 3.0Middle-income countries 0.5 to 0.9Low-income countries 0.3 to 0.6
Source: based on data from UNCHS, 1996b.
Table 3.8
Major environmental health risk factors of agricultural development
Agricultural development Direct environmental changes Secondary environmental Environmental healthissue changes risk factorsIrrigation development Hydrological changes Increased insect populations Introduction of new vector species
Waterlogging Increased densities Increased vector densitiesSalination Greater chemical inputs Changed vector population compositionIncreased water surfaces Prolonged transmission seasonIncreased relative humidity Chemical poisoning
Land-use changes Deforestation Changed composition of the Changed vector population compositionReduced biodiversity/habitat insect fauna Changed vector longevitySimplification
Cropping patterns High-yielding varieties Greater chemical inputs PoisoningShift from subsistence to cash crops Greater densities of insect Reduction of predator insectsAccelerated cropping cycle populations in favour of pest and vector speciesPlantation agriculture
Livestock management Changed in livestock densities and Changed densities of blood- Changed disease transmission potentialspacial distribution of livestock sucking insectsNew breeds of livestock
Mechanization Changes in livestock densities and Changed densities of blood- Changed disease transmission potentialLoss of ecological features sucking insectsAssociated with draught animals Reduced refuge areas for
predator insectsAir and water pollution
Chemical inputs Increased levels of pesticides, Chemical contamination Poisoningherbicides and/or fertilizer Eutrophication of water bodies Introduction of new vector species
Expansion of aquatic weeds Development of insecticide resistancein vector populations
Source: Bradley & Narayan 1987.

12
EXECUTIVE SUMMARY
may be accompanied by adverse health-and-environment impacts.
In developing countries, biomass accountsfor about one-third of all energy use,and in some of the least-developed coun-tries, for as much as two-thirds (Fig.3.10). Open fires impair indoor air qual-ity (Fig. 3.11), add to the risk of acci-dents and jeopardize food hygiene.
But the largest source of atmosphericpollution is the combustion of fossilfuels in power plants and by industries,in motor vehicles and by households.Huge quantities of sulphur and nitro-gen oxides, heavy metals, HCs, partic-ulates, CO, and other highly toxic pol-lutants are emitted. Associated majorhealth-and-environment effects include:• indoor and outdoor air pollution• emission of GHGs• contamination of water bodies and land
by atmospheric fallout of emissions• occupational health-and-safety risks.The rapid growth in the world motorvehicle fleet (Fig. 3.12) is also creatingserious air pollution problems in someparts of the world.
Clearly, the mix of technologies andfuels that are chosen today will haveconsiderable environmental implica-tions for tomorrow.
CONSIDERABLE THREATS TOENVIRONMENTAL QUALITYAND HEALTH
In summary, the adverse effects on theenvironment of human activities aremany and appear to be growing inintensity, at least in some parts of theworld, and affecting larger and larg-er areas. Current and future potential“pressures” on the environment havemajor implications for health.
Fig. 3.5
Per capita water use by continentfor 1995
Source: based on data from WRI, 1996.
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
0.0North
AmericaEurope Oceania Asia South
AmericaAfrica
Continent
Thou
sand
m3 p
er c
apita
Fig. 3.10
Number of people using different household fuels by region — 1990s
Source: based on data from Smith & Figuero, 1997.
0
200
400
600
800
1000
1200
SSA India China OAI LAC MEC FSE EMERegion
Popu
latio
n (m
illio
ns)
Biomass
Coal
Non-solid fuel
“Despite progress on several fronts,from a global perspective the envi-ronment has continued to degradeduring the last decade, and sig-nificant environmental problemsremain deeply embedded in thesocio-economic fabric of nations inall regions”UNEP Global Environment Outlook,1997a.

13
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Fig. 3.12
Growth of world motor vehicle fleet — 1930–1995
Source: based on data from AAMA, 1996
1930 1935 1940 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990 19950
100
200
300
400
500
600
700
Num
ber o
f veh
icle
s (m
illio
ns)
Year
Passengers cars
Commercial vehicles
Fig. 3.11
Emissions per meal for household cooking fuels
Source: adapted from Smith, 1991.
0
10
20
30
40
0.0
0.5
1.0
1.5
2.0
Dung Crop residues Wood Kerosene Gas
COper standard meal
Particulatesper standard meal
CO (g
ram
s) p
er m
eal
Particulates (grams) per m
eal

15
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
THE HUMAN DIMENSION TOENVIRONMENTAL QUALITY
Pressures on the environment in theform of pollution emissions, resourcedepletion, land-use changes and oth-ers affect environmental quality (the“state” of the environment). Degradationof environmental quality can, in turn,lead to adverse human exposures andeventual health effects.
Air, water and food are the principalexposure routes of environmental healthhazards. Also heavily implicated arethe manner in which household wastesand sewage are handled, and the con-ditions in which people live and work.
AIR POLLUTION
When inhaled, air pollutants affect thelung and respiratory tract; they are alsotaken up by the blood and transport-ed throughout the body. And sinceair pollutants are deposited on soil andplants and in water, they can contributeto further human exposure if contam-inated food and water are ingested.
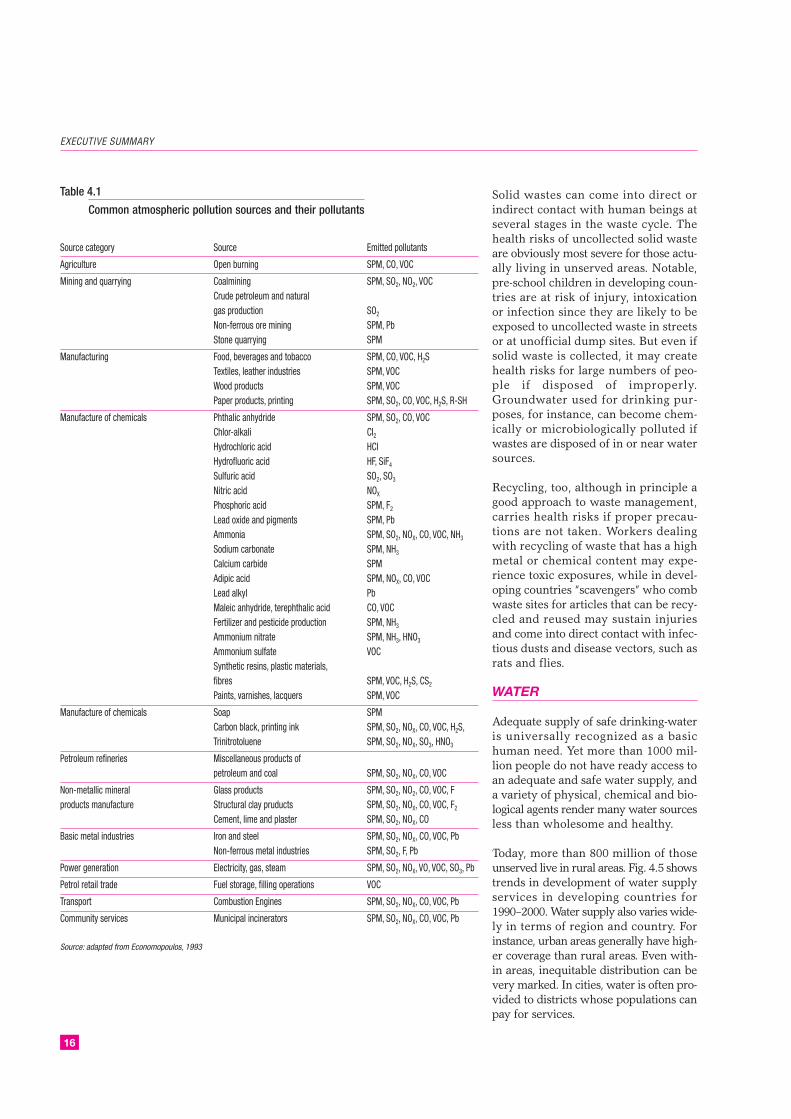
SPM and gaseous pollutants are emit-ted by a wide range of sources (Table4.1). In recent years, attention has shift-ed to that portion of SPM made upof particles that are so small that theycan penetrate deeply into the lung.Other health-damaging pollutantsinclude gaseous inorganic pollutantssuch as SO2, CO, and nitrogen diox-ide (NO2), as well as HCs, such as ben-zene and butadiene, other volatileorganic compounds (VOCs), and sec-ondary pollutants.
Indoor air pollution can be particularlyhazardous to health because it is released
in close proximity to people. The mostprominent source of indoor air pollu-tion in developing countries is house-hold use of biomass and coal for heat-ing and cooking, usually involving openfires or stoves without proper chim-neys.
A large number of studies in recentyears have shown remarkable consis-tency in the relationship observedbetween changes in daily ambient sus-pended particulate levels and changesin daily mortality. Two different meth-ods for estimating the total global mor-tality from suspended particulate airpollution exposures arrive at very sim-ilar total numbers (i.e. 3 million and2.7 million), with indoor air pollu-tion accounting for the vast majorityof total deaths (Fig. 4.4).
Other air pollutants of health concerninclude ozone (O3), environmentaltobacco smoke (ETS) and ionizing radi-ation. ETS is on the increase; in adultnon-smokers, chronic exposure to ETSincreases mortality from lung cancerby between 20% and 30%.
HOUSEHOLD WASTES
Poorly managed wastes — specifical-ly excreta, liquid and solid wastesfrom households and the communi-ty — represent a serious health threat.Waste from industries and agricul-ture can also cause serious healthrisks.
Human faeces are dangerous to humanhealth everywhere because of thepathogens they contain. Ingestion offaecal pathogens can cause diarrhoealdisease, cholera, intestinal worm infec-tions and typhoid fever.
CHAPTER 4
From Environmental Quality to Exposuresand Risks
16
EXECUTIVE SUMMARY
Table 4.1
Common atmospheric pollution sources and their pollutants
Source category Source Emitted pollutants
Agriculture Open burning SPM, CO, VOC
Mining and quarrying Coalmining SPM, SO2, NO2, VOCCrude petroleum and naturalgas production SO2
Non-ferrous ore mining SPM, PbStone quarrying SPM
Manufacturing Food, beverages and tobacco SPM, CO, VOC, H2STextiles, leather industries SPM, VOCWood products SPM, VOCPaper products, printing SPM, SO2, CO, VOC, H2S, R-SH
Manufacture of chemicals Phthalic anhydride SPM, SO2, CO, VOCChlor-alkali CI2Hydrochloric acid HCIHydrofluoric acid HF, SiF4
Sulfuric acid SO2, SO3
Nitric acid NOX
Phosphoric acid SPM, F2
Lead oxide and pigments SPM, PbAmmonia SPM, SO2, NOX, CO, VOC, NH3
Sodium carbonate SPM, NH3
Calcium carbide SPMAdipic acid SPM, NOX, CO, VOCLead alkyl PbMaleic anhydride, terephthalic acid CO, VOCFertilizer and pesticide production SPM, NH3
Ammonium nitrate SPM, NH3, HNO3
Ammonium sulfate VOCSynthetic resins, plastic materials,fibres SPM, VOC, H2S, CS2
Paints, varnishes, lacquers SPM, VOC
Manufacture of chemicals Soap SPMCarbon black, printing ink SPM, SO2, NOX, CO, VOC, H2S,Trinitrotoluene SPM, SO2, NOX, SO3, HNO3
Petroleum refineries Miscellaneous products ofpetroleum and coal SPM, SO2, NOX, CO, VOC
Non-metallic mineral Glass products SPM, SO2, NO2, CO, VOC, Fproducts manufacture Structural clay pruducts SPM, SO2, NOX, CO, VOC, F2
Cement, lime and plaster SPM, SO2, NOX, CO
Basic metal industries Iron and steel SPM, SO2, NOX, CO, VOC, PbNon-ferrous metal industries SPM, SO2, F, Pb
Power generation Electricity, gas, steam SPM, SO2, NOX, VO, VOC, SO3, Pb
Petrol retail trade Fuel storage, filling operations VOC
Transport Combustion Engines SPM, SO2, NOX, CO, VOC, Pb
Community services Municipal incinerators SPM, SO2, NOX, CO, VOC, Pb
Source: adapted from Economopoulos, 1993
Solid wastes can come into direct orindirect contact with human beings atseveral stages in the waste cycle. Thehealth risks of uncollected solid wasteare obviously most severe for those actu-ally living in unserved areas. Notable,pre-school children in developing coun-tries are at risk of injury, intoxicationor infection since they are likely to beexposed to uncollected waste in streetsor at unofficial dump sites. But even ifsolid waste is collected, it may createhealth risks for large numbers of peo-ple if disposed of improperly.Groundwater used for drinking pur-poses, for instance, can become chem-ically or microbiologically polluted ifwastes are disposed of in or near watersources.
Recycling, too, although in principle agood approach to waste management,carries health risks if proper precau-tions are not taken. Workers dealingwith recycling of waste that has a highmetal or chemical content may expe-rience toxic exposures, while in devel-oping countries “scavengers” who combwaste sites for articles that can be recy-cled and reused may sustain injuriesand come into direct contact with infec-tious dusts and disease vectors, such asrats and flies.
WATER
Adequate supply of safe drinking-wateris universally recognized as a basichuman need. Yet more than 1000 mil-lion people do not have ready access toan adequate and safe water supply, anda variety of physical, chemical and bio-logical agents render many water sourcesless than wholesome and healthy.
Today, more than 800 million of thoseunserved live in rural areas. Fig. 4.5 showstrends in development of water supplyservices in developing countries for1990–2000. Water supply also varies wide-ly in terms of region and country. Forinstance, urban areas generally have high-er coverage than rural areas. Even with-in areas, inequitable distribution can bevery marked. In cities, water is often pro-vided to districts whose populations canpay for services.

Water pollution, whether it involves sewage,nutrients, synthetic organics, acidificationor specific chemicals, has a direct bear-ing on human health . Sewage, in addi-tion to upsetting the ecological balance ofrivers and lakes, also carries microbialpathogens. Other nutrients contaminategroundwater sources with nitrates, withthe result that nitrate levels in drinking-water often exceed the safe levels rec-ommended by WHO. The most danger-ous can bioaccumulate in fish and shell-fish which, if consumed, may be haz-ardous to human health. Acidificationcontributes to high levels of heavy met-als in drinking-water where metals in soiland water distribution pipes are mobi-lized by acidified groundwater (Fig. 4.7).
Untreated sewage, industrial effluentsand agricultural waste are frequentlydischarged into inland waterways, lakesand coastal zones, endangering thehealth of those who use these waterbodies for recreational purposes suchas swimming, canoeing and wind-surfing. Recreational exposure to pol-luted waters can cause diarrhoea, res-piratory infections, skin irritation andother diseases, depending on the spe-cific pollutants involved.
Finally, the aquatic environment pro-vides an essential habitat for the mos-quito vectors and intermediate snailhosts of parasites that cause human
diseases. Accelerated development ofwater resources has led to habitat mod-ifications and ecological conditions thatfavour certain disease vectors. Healthissues linked to irrigation developmenthave become a particular focus of atten-tion, but increased transmission is alsolinked to the construction of dams andreservoirs, to changes in land-use pat-terns and to poor water managementin urban areas. The most importantwater-related vector-borne diseasesaffected by development projects inrecent decades include malaria, schis-tosomiasis, dengue fever, filariasis andJapanese encephalitis.
FOOD
Food is essential to a healthy life, but itcan also be a major route of exposurefor many pathogens and toxic chemi-cals. These contaminants may be intro-duced into food during cultivation, har-vesting, processing, storage, transportationand final preparation. Inspection andmonitoring of food quality are thereforenecessary to ensure food safety.
The increasing interdependency andcomplexity of our food supply meanthat even the best control systems arebecoming strained, however. Foodbornedisease is now a widespread and grow-ing threat to human health, and a majorcause of reduced economic produc-
17
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Fig. 4.4
Estimated global annual deaths due to indoor and outdoor pollution exposure
Source: Smith, 1996. Source: WHO/UNICEF, 1996a.
Developedcountries(urban)7%
Developingcountries
(urban)93%
Developingcountries
(rural)67%
Developingcountries
(urban)23%
Developedcountries(rural)1%
Developedcountries(urban)9%
Indoor exposures Outdoor exposures
Total deaths 2.8 million Total deaths 0.2 million
Fig. 4.5
Development of water supply servicesin developing countries 1990–2000
1.581.11
0.75
2.493.27
4.13
345381
447
288 326 384
1.13
0.63
0.23
1.802.50
3.23
94 97104
346 376 420
5671
90
16
10
7
0
1
2
3
4
5
0
200
400
600
800
1000
0
200
400
600
800
0
1
2
3
4
0
20
40
60
80
100
All developing countries
1990 1994 2000
1990 1994 2000
1990 1994 2000
1990 1994 2000
1990 1994 2000
Population served Population unserved
Africa
Latin America and the carribean
Asia and Pacific
West Asia
Popu
latio
n (1
000
mill
ion)
Popu
latio
n (m
illio
ns)
Popu
latio
n (m
illio
ns)
Popu
latio
n (1
000
mill
ion)
Popu
latio
n (m
illio
ns)

tivity. Health impacts range from mildindisposition to life-threatening illness.The people most affected are the poor,who are also vulnerable to lack of foodand undernutrition.
Biological and chemical agents in foodrepresent the two major types of food-borne hazard. Biological agents tendto pose acute hazards with incubationperiods of a few hours to several weeksbefore the onset of disease, whereaschemical hazards usually involve long-term, low-level exposures.
Many chemical hazards in food areproduced naturally by organisms inthe environment. Others are inherentcomponents of food itself. Yet otherpotentially hazardous chemicals areproduced during processing. Pollutantssuch as lead, cadmium and polychlo-rinated biphenyls (PCBs) in air, waterand soil can also lead to high levels oftoxic chemicals in food.
SOIL
Exposure to hazards in soil can occur,for instance, when farmers till agricul-tural soil, when children play in school-yards, or when dust from dry fields isblown into populated areas. Additionally,deposition of biological, chemical orradioactive hazards on or in soil canlead to indirect exposures following useof contaminated groundwater for drink-ing-water, or consumption of food grownon contaminated soil.
Direct contact with soil or soil dustthat has been contaminated withhelminth eggs is a major source ofexposure to intestinal worm infec-tion. Soil can also harbour many oth-er parasites and microbes, which cansurvive for long periods in spite oflarge variations in soil temperatureand humidity. Neonatal tetanus (NT)is a common example of an associ-ated disease. Tetanus spores infect
18
EXECUTIVE SUMMARY
Sensitive soilsPresent emissionsSensitive soilsand present emissions
Present problem areasPotential problem areas
Fig. 4.7
Global risk of surface water acidification
Source: UNEP, 1995b.

19
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
humans through direct contact withsoil or dirt; in developing countries,childbirth in impoverished conditionsoften leads to NT.
HOUSING
Housing is of central importance toquality of life. Ideally, it minimizes dis-ease and injury, and contributes muchto physical, mental and social well-being. The home environment shouldalso afford protection against the haz-ards to health arising from the physi-cal and social environment (Table 4.17).
Numerous factors in the home envi-ronment may influence health nega-tively, though. Lack of access to pipedwater or a nearby stand-pipe, and lackof sanitary facilities, are often consid-ered key indicators of “unhealthy” hous-ing, leading to high disease burdens, inboth urban and rural areas. Factors suchas high levels of noise, poor indoor airquality, inadequate refuse storage andcollection facilities, poor food storageand preparation facilities, temperatureextremes and high humidity, over-crowding, poor lighting, inadequate orinappropriate construction material,building defects and pests may alsoinfluence health significantly.
Crowded, cramped conditions, for instance,facilitate transmission of diseases includ-ing tuberculosis, influenza, meningitis,ARI, diarrhoeal diseases and measles.Some evidence suggests that women’shealth is more likely to be adversely affect-ed by crowding than that of men. If crowd-ing combines with poor-quality hous-ing materials, incidence of injuries andaccidents rises significantly.
THE WORKPLACE
In favourable circumstances, work con-tributes to good health and economicachievement. However, the work envi-ronment exposes many workers tohealth hazards that contribute to injuries,respiratory diseases, cancer, muscu-loskeletal disorders, reproductive dis-orders, allergies, cancer, CVD, mentaland neurological illnesses, psycholog-ical stress, eye damage and hearing
loss, as well as to communicable dis-eases.
Mechanical hazards, unshielded machin-ery, unsafe structures in the workplaceand dangerous tools are some of themost prevalent workplace hazards indeveloped and developing countriesalike. Approximately 30% of the work-force in developed countries andbetween 50% and 70% in developingcountries, may be exposed to a heavyphysical workload or ergonomicallypoor working conditions.
Exposure to some 200 biological agents,viruses, bacteria, parasites, fungi,moulds and organic dusts occurs inselected occupational environments.Physical factors in the workplace suchas noise, vibration, ionizing and non-ionizing radiation and microclimaticconditions can also affect health adverse-ly if not controlled. Occupational chem-ical exposures are another area ofincreasing concern. About 100 000 dif-ferent chemical products are in use inmodern work environments and thenumber is growing.
With economic development manycountries have experienced a shift fromthe hazards that characterized work inagriculture, mining and other prima-ry industries, to those that character-ize manufacturing industries or ser-vice industries. New occupational dis-ease problems have emerged and inci-dence of reported occupational diseasehas accordingly increased in certaindeveloped countries.
THE GLOBAL ENVIRONMENT
As a result of the combined action ofdriving forces at local and regional lev-els, environmental change is gradual-ly becoming “globalized”. Major exam-ples of global environmental changeinclude: climate change, stratospher-ic ozone depletion, transboundaryair and water pollution, acid precipi-tation, loss of biodiversity, desertifi-cation and deforestation.
Human-induced climate change is dueprimarily to accumulation of GHGs in
Table 4.17
Principles of healthy housing
Protection against communicablediseases through:
• safe water supply • sanitary excreta disposal • disposal of solid wastes • drainage of surface water • personal and domestic hygiene • safe food preparation• structural safeguards
Protection against injuries, poisoningsand chronic diseases through attention to:
• structural features and furnishings• indoor air pollution• chemical safety• use of the home as a workplace
Reduction of psychological and socialstress through:
• adequate living space, privacy and comfort• personal and family security• access to recreation and community amenities• protection against noise
Access to a supportive living environmentthrough provision of:
• security and emergency services• health and social services• access to cultural and other amenities
Protection of populations at special risk:
• women and children• displaced and mobile populations• the aged, ill and the disabled
Source: adapted from WHO 1989e.

20
EXECUTIVE SUMMARY
the atmosphere, resulting from activ-ities such as combustion of fossil fuels,large-scale deforestation and the rapidexpansion of irrigated agriculture. Bothdirect and indirect health impacts canbe expected to occur as a result ofclimate change (Fig. 4.9).
Although stratospheric ozone deple-tion and climate change are separatephenomena, they are linked by a num-ber of processes. For instance, sev-eral GHGs, especially CFCs, alsodestroy stratospheric ozone. The prin-cipal result of stratospheric ozone
depletion is that an increasing pro-portion of solar ultraviolet radiation(UVR) is reaching Earth’s surface.Higher UV exposure is expected toresult in a number of direct impactson human health, including an increasein the incidence of skin cancer (espe-cially non-melanoma skin cancers) inlight-skinned populations. It couldalso increase the incidence of eyelesions, such as cataracts, and lead tosuppression of the immune system.
Stratospheric ozone depletion was firstmeasured in the 1980s at Antarctica.It is now becoming significant in theArctic area too. An increasing extentof the northern hemisphere is becom-ing exposed (Fig. 4.12).
The transboundary movement of haz-ardous wastes and long-range transportof air pollution are two environmentalproblems of great international con-cern. There have been many instancesof hazardous waste being shipped todeveloping countries in order to takeadvantage of inadequate environmen-tal regulations and cheaper prices.
The main concern relating to long-range transport of air pollution isdeposition of harmful substances andreduced air quality in locations farremoved from the original sourcesof pollution. Acid deposition is aregional air pollution problem. Whileacidification of water bodies and soilsis largely an environmental threat,human health may also be affectedowing to the mobilization of heavymetals.
COMBINED EXPOSURESFROM A VARIETY OFSOURCES
Many environmental hazards — bethey chemical, biological or physical— occur in more than one environ-mental media or setting (e.g. air, water,housing, workplace). Their control,therefore, requires an understandingof the relative contribution made byeach medium or setting. This has ledto development of the total humanexposure concept.
Fig. 4.9
Possible major types of impact of climate change and stratospheric ozone depletionon human health
Mediating process Health outcomes
Direct
Exposures to thermal extremes ➤ Altered rates of heat- and cold-related illness and death
Altered frequency and/or intensity of other extreme ➤ Deaths, injuries, psychological disorders; damage to publicweather events health infrastructure
Temperature and weather changes
Indirect
Disturbances of ecological systems
Effects on range and activity of vectors and ➤ Changes in geographic ranges incidence of vector-infectious parasites borne diseases
Altered local ecology of waterborne and foodborne ➤ Changed incidence of diarrhoeal and other infectiousinfectious agents diseases
Altered food (especially crop) productivity, due to ➤ Malnutrition and hunger, and consequent impairment ofchanges in climate, weather events, and associated child growth and developmentpests and diseases
Sea level rise, with population displacement and ➤ Increased risk of infectious disease, psychological disordersdamage to infrastructure
Levels and biological impacts of air pollution, ➤ Asthma and allergic disorders; other acute and chronicincluding pollens and spores respiratory disorders and deaths
Social, economic and demographic dislocations due ➤ Wide range of public health consequences; mental healthto effects on economy, infrastructure and resource and nutritional impairment, infections diseases, civil strifesupply
Skin cancers, cataracts,and perhaps immune suppression;Stratospheric ozone depletion ➤ indirect impacts via impaired productivity and agricultural
and acquatic systems
Source: McMichael et al., 1996.
➤
➤

Of all the pollutants to which expo-sure occurs via multiple pathways, leadis probably the best known and moststudied. Although decreasing in manydeveloped countries, lead exposureremains a major public health issue,especially in cities and industrializedareas in developing countries.
HUMAN EXPOSURES ANDHEALTH RISK: MULTIPLECHALLENGES FOR HEALTHPROTECTION
Table 4.24 summarizes the multiplelinkages between the exposure situa-tions described in this chapter and themajor ill health conditions that theycan cause. Most of these health con-ditions are potentially related to sev-eral environmental exposure situations.
21
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Fig. 4.12
Ozone layer depletion around the North Pole; mean reduction of ozone levels(%) during the months of February and March during 1992–1997
Source: Bojkov et al. 1997.
Table 4.24
Potential relationships between exposure situations and health conditions
Exposure situations
Excreta and Polluted water or defienciesHealth conditions of concern Polluted air household wastes in water management Polluted food Unhealthy housing Global environmental change
Acute respiratory infections • •Diarrhoeal diseases • • • •Other infections • • • •Malaria and other
vector-borne diseases • • • •Injuries and poisonings • • • • •Mental health conditions •Cardiovascular diseases • •Cancer • • •Chronic respiratory diseases • •

23
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
ESTIMATING THE BURDEN OFDISEASE
One can also look at environmentalhealth problems from the viewpointof the burden of death, disease anddisability, and analyse the relativeimportance of the different environ-mental factors discussed earlier. Table5.1 shows two different estimates forthe total number of deaths for themajor causes of death for 1990–1993.Each of the two estimates involvesjudgements about the best sources ofmortality data, which explains the dif-ferences between the two columnsfor certain disease categories.
To clarify the relative importance ofdifferent causative factors, such analy-sis must take into account the age atwhich death occurs, or even better, thenumber of “years of life lost” (YLL).Furthermore, not all negative healthoutcomes are expressed only in termsof mortality. Morbidity and disabilityare important outcomes that ideallyshould also be considered when cal-culating disease burden.
The disability-adjusted life years (DALYs)concept is one approach which hasgenerated a comprehensive picture ofthe “burden of disease”, covering allmajor disease and injury categories.Estimates of disease burden basedon this approach are used in this booksince these estimates include all dis-eases of interest to this analysis andall regions of the world. Furthermore,the estimates relate to what is con-sidered “preventable”.
Each DALY indicates the loss of a yearof healthy life — that is, time lived witha disability or time lost through pre-
mature death. The number of DALYsin different regions provides a guideto the relative distribution of diseaseburden: the higher the DALYs, thegreater the burden. To calculate dis-ease burden in DALYs, data on pre-mature mortality and disability arecombined. The number of YLL areassessed as the difference betweenthe actual age at death and the age atwhich the person could have beenexpected to die, given the average ageof mortality of an advanced developedcountry (82.5 years for women and80 years for men). Next, the incidenceof disability due to disease or injuryis estimated on the basis of availableinformation pertaining to each com-munity. Different weights are assignedto different disability conditions, accord-ing to severity. Finally, discountingand age-weighting are incorporatedbecause this methodology assumesthat future years of life lost contributeless to the burden of disease than docurrent ones.
While most of the DALY burden is dueto premature death, the disability com-ponent is important for chronic ill-nesses which are present over manyyears. This is seen in Table 5.2 wherethe early death component of DALYs(i.e. years of life lost — YLL) is pre-sented along with the DALYs for select-ed causes.
Some diseases, such as ARI and diar-rhoeal diseases, are of particular impor-tance to children’s health. Thirty per-cent of the estimated number of deathsfor all diseases occur before 15 yearsof age (Table 5.3), but for ARI and diar-rhoeal diseases, the percentages are67% and 88% respectively. The childproportions of DALYs are even greater:
CHAPTER 5
Health Conditions in an EnvironmentalContext

24
EXECUTIVE SUMMARY
48% for all diseases and more than90% for ARI and diarrhoeal diseases.
ACUTE RESPIRATORYINFECTIONS
ARI includes viral and bacterial infec-tions of the lungs and respiratory tract,the most severe and fatal being bac-terial pneumonia. Certain of the vac-cine-preventable infectious diseases(such as measles and whooping cough)can include severe symptoms affect-ing the respiratory tract and contributeto the global burden of these diseases.Pneumonia incidence is sufficientlyhigh to make it the biggest cause ofchildhood mortality. It is also the causeof death in many elderly people.Approximately 2.7 million of the esti-mated 11 million deaths that occurevery year in children under the ageof five year are due to pneumonia.The burden of disease due to ARIon a per capita basis is about 100 timeshigher in the least developed coun-tries than in the developed coun-tries (Fig. 5.1). Severe indoor air pol-lution from biomass burning for cook-ing and heating is an important con-tributory environmental factor, as ispoor housing.
In most developing countries, con-trol of pneumonia mortality relies onearly, effective case-management. Theeffectiveness of this approach is lim-ited, however, if the availability ofantibiotics, training of primary healthworkers and access to health facilitiesare poor. Efforts to reduce ARI inci-dence in children also depend uponthe reduction of indoor air pollutionexposures to biomass and coal smoke.
DIARRHOEAL DISEASES
The diarrhoeal diseases of main con-cern are cholera, typhoid fever, paraty-phoid fever, salmonella, shigella, gia-rdiasis, non-human Escherichia coliinfection, and a variety of other dis-eases caused by bacteria, parasites andviruses. Most of the global burden ofdiarrhoeal diseases occurs in childrenin developing countries; it is estimat-ed that approximately 90% of the diar-
Table 5.1
Estimated global number of deaths — 1990–1993
Disease A. Deaths (thousands) (%) B. Deaths (thousands) (%)
Cardiovascular diseases 14 327 28 9676 19
Cancer 6024 12 6013 12
Acute respiratory infections 4380 8.7 4110 8.1
Unintentional injuries 3233 6.4 2915 5.7
Diarrhoeal diseases 2946 5.8 3010 5.9
Chronic respiratory diseases 2935 5.8 2888 5.7
Perinatal conditions 2443 4.8 3180 6.2
Vaccine-preventable infections 1985 3.9 1677 3.3
Tuberculosis 1960 3.9 2709 5.3
Intentional injuries 1851 3.7 1082 2.1
Malaria 856 1.7 2000 3.9
Mental health conditions 700 1.4 – –
Other identified diseases 6827 13.5 3616 7.1
Unknown causes – – 8124 16
Total 50 467 100 51 000 100
Sources: A. deaths in 1990 according to Murray and Lopez, 1996b; B. deaths in 1993 according to WHO, 1995 a.
Table 5.2
Global YLL and DALYs for major health conditions — 1990
Disease YLL (thousands) (%) DALY (thousands) (%)
Infectious and vector-borne diseases
Acute respiratory infections 110 992 12 116 696 8.5
Diarrhoeal diseases 94 434 10 99 633 7.2
Vaccine-preventable infectious diseases 67 104 7.4 71 173 5.2
Tuberculosis 34 308 3.8 38 426 2.8
Malaria 28 038 3.1 31 706 2.3
Chronic diseases and injuries
Injuries and poisoning 132 519 15 208 647 15
Unintentional injury 84 536 9.3 152 188 11
Intentional injury 47 983 5.3 56 459 4.1
Mental health conditions 10 424 1.1 144 950 11
Cardiovascular diseases 116 325 13 133 236 9.7
Cancer 64 837 7.2 70 513 5.1
Chronic respiratory diseases 24 755 2.7 60 370 4.3
Total: all diseases and injuries 906 501 100 1 379 238 100
Sources: based on dat in Murray & Lopez, 1996b.

rhoeal disease burden is related to theenvironmental factors of poor sanita-tion and lack of access to clean waterand safe food (see Section 5.13).
VACCINE-PREVENTABLEINFECTIOUS DISEASES
The major vaccine-preventable diseases(measles, NT, poliomyelitis, diphtheriaand pertussis) account for nearly 15%of the total disease burden of the 0–4age group. Progress in immunizingthe world’s children has been rapid sincethe inception of the WHO ExpandedProgramme on Immunization in 1974.However, the transmission of these dis-eases — especially measles, tetanus andpoliomyelitis — is associated with poorliving conditions, crowding and otherenvironmental factors. Effective andsustainable elimination of these diseaseswill therefore require environmentalimprovements and immunization.
MALARIA, OTHER TROPICALVECTOR-BORNE DISEASES,AND NEWLY EMERGINGINFECTIOUS DISEASES
The environment plays a particularlyimportant role in determining the dis-tribution of vector-borne diseases. Inaddition to water and temperature, oth-er factors such as humidity, vegetationdensity, patterns of crop cultivationand housing may be critical to the sur-vival of the different species of dis-ease-carrying vector. All of these dis-eases are most serious in the poorestcountries, and among those living inthe most difficult and impoverishedconditions. They contribute to a viciouscircle of disease–poverty–disease andto the continued marginalization ofpeople living in disease-ridden areas.
Malaria is the only tropical vector-borne disease significant enough at theglobal level to feature in the DALY-esti-mated burden of diseases (Table 5.2).That said, other vector-borne diseasesare important in specific situations andshare similar environmental predis-positions with malaria (Table 5.4).
Globally, the malaria situation is seri-
ous and worsening. Around 90% ofthe malaria burden is estimated tooccur in Africa, south of the Sahara,almost all due to Plasmodium falciparum,the parasite species associated withthe most severe and fatal malaria. Infact, malaria is one of the most seri-ous health problems facing Africancountries and a major obstacle to theirsocial and economic development.Children under the age of five yearsand women in their first pregnancyare the most vulnerable. Approximatelyone million deaths among childrenunder 5 years of age can be attributedto malaria alone, or in combinationwith other diseases.
Of all the insects that transmit dis-ease, the mosquito represents by farthe greatest human health threat. Ittransmits not only malaria, but alsodengue, dengue haemorrhagic feverand lymphatic filariasis (Table 5.4).Diseases transmitted by other insectsinclude leishmaniasis (sandfly), Africantrypanosomiasis (tsetse fly), onchocer-ciasis (blackfly), and Chagas disease(triatomine bug). Schistosomiasis iscaused by infection with blood flukes,
25
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Table 5.3
Proportion of global burden deaths and diseases occurring in children underage 15 — 1990
Deaths, age 0–14 DALYs, age 0–14Disease (thousands) (%)* (thousands) (%)**
Acute respiratory infections 2918 67 105 077 90
Diarrhoeal diseases 2585 88 93 408 94
Perinatal conditions 2443 100 92 311 100
Vaccine-preventable infections 1897 96 69 147 97
Tuberculosis 139 7 5314 14
Malaria 699 82 27 151 86
Unintentional injuries 1065 33 74 620 49
Intentional injuries 258 14 10 415 18
Mental health conditions 96 14 11 000 8
Cardiovascular diseases 441 3 16 259 12
Cancer 163 3 6052 9
Chronic respiratory diseases 185 6 15 440 26
Total 15 073 30 655 112 48
** % of all deahs in this disease category** % of all DALYs in this disease category
Source: Murray & Lopez 1996b.
Fig. 5.1
Acute respiratory infections amongchildren aged 0–4 years, by region —DALYs per 1000 children (log scale)
Source: Murray & Lopez, 1996 b.
0 10 100 10001000 100 10
EME
FSE
LAC
SSA
Boys Girls

26
EXECUTIVE SUMMARY
whose larval stage develops in aquat-ic snails; the parasite penetrates theskin of anyone who comes into con-tact with infested water. Among thedriving forces and pressures consid-ered in earlier chapters, those of great-est relevance to these diseases arerapid and uncontrolled urbanization,poor housing and hygiene, water devel-opment schemes (including irrigationfor agriculture), and road construc-tion and mining activities.
During the past 20 years, at least 30new diseases have emerged to threat-en the health of hundreds of millionsof people. Environmental changes havecontributed in one way or another tothe appearance of most if not all ofthese. Human activity, such as the cut-ting down of forests or conversion ofgrasslands to agricultural lands, hascontributed to such change. In otherinstances, simple behavioural changeshave favoured the emergence of a dis-ease pathogen, for example, new andwidespread vector-breeding sites inurban environments have been cre-ated through careless disposal of foodand beverage containers, and motorvehicle tyres.
INJURIES AND POISONINGS
Injuries are one of the largest contribu-tors to YLL and disability at the globallevel (Table 5.2). They are of great impor-tance in developed and developing coun-tries alike, but the categories of injuryshift with development. Agriculturalinjuries, fires, drownings and war-relat-ed violence dominate at early stages ofeconomic development, while road-traf-fic accidents and industrial injuries appearto increase with economic development.Among unintentional injuries, road-traf-fic accidents are the sole category pro-jected to have increased by the year 2020.By contrast, intentional injuries are marked-ly on the rise.
From both an individual and a publichealth perspective, the burden of inten-tional injury has increased dramati-cally in the 20th Century, affecting notonly the well-being of those involved,but also the health services called onto provide care and treatment. Thegrowing problem of violence now alsothreatens family welfare, communitycohesion and the capacity of societiesto move towards better health and sus-tainable social development.
Table 5.4
The burden of some tropical and vector-borne diseases
People at risk People infected Number ofDisease (millions) (millions) Mortality Morbidity/disability countries affectedMalaria 2020 > 500 1.5–2.7 million 300–500 million clinical cases > 90Dracunculiasis 100 > 0.15 Exceptional High disability 18Chagas disease 100 18 > 45 000 3 milion 21Schistosomiasis 600 200 < 20 000 20 million 74Foodborne trematode
Infections 730 40 > 10 000 Liver disease or diarrhoea > 100Intestinal parasites 4000 3500 Helminths: 135 000 Helminths: 450 million > 100
Protozoa: 90 000 Protozoa: 48 million AllLymphatic filariasis 1100 120 Excess mortality among 44 million with chronic 73
those with elephantiasis disabilityOnchocerciasis 120 18 Excess mortality among 270 000 blind 34
the blindLeishmaniasis 350 12 Visceral: 75– 80 000 Visceral: very high 88
Cutaneous: very low Cutaneous: multiple lesionsDengue and dengue 2500–3000 > 10 20–30 000 Millions of cases > 100
Haemorrhagic feverSleeping sickness 55 > 0.3 20 000 > 300 000 cases: high disability 36
Note: Figures are provisional, subject to change as and when more current data become available. Some people may be infected with more than one disease. Figures have been rounded up.
Source: WHO, 1997h.

War-related injuries and injuries fromland mines are also of major concern.They represent not only a direct andavoidable injury burden, but also divertvaluable resources from other health-care needs and from investment inhealth services. The indirect effects ofwar on civilian populations are alsoserious and include disruption of watersupply systems and other environ-mental services.
MENTAL HEALTHCONDITIONS
Mental disorders comprise many con-ditions, ranging from mild anxiety anddepressive states to severe schizophreniaand dementia. The estimated globalprevalence of the main categories ofmental disorder is several hundred mil-lion cases. Mental disorders and oth-er psychological problems account foraround 10% of the total burden of dis-ease (Table 5.1). Those affected areusually more disabled in everyday lifethan persons with other common chron-ic conditions such as arthritis, backpain and diabetes. Of this burden, morethan one-third is accounted for byunipolar major depression. Globally,unipolar major depression is expectedto have become the number two con-tributor to DALYs after ischaemic heartdisease by 2020.
In considering the effects of environ-ment on mental health, chemical andphysical factors, that influence thebody’s nervous system, and psychosocialfactors that influence mental well-being, must be taken into account.
CARDIOVASCULAR DISEASES
As shown in Table 5.1, CVD tops thelist of global deaths. CVD encompassescoronary heart disease (CHD), otherdiseases of the heart and heart valves,stroke, and diseases affecting the bloodvessels. Its risk factors may be divid-ed into four categories: non-modifiablerisk factors (age, sex, race and familyhistory); modifiable physiological riskfactors (blood cholesterol, high bloodpressure, diabetes and obesity); behav-ioural risk factors (smoking, diet, alco-
hol, sedentary lifestyle); and environ-mental risk factors (air pollution, tem-perature, heavy metal exposures, infec-tious agents). Risk factors in the firstthree categories, especially diet andsmoking, contribute most to the totalCVD burden.
The very high indoor air pollution lev-els caused by the use of biomass andcoal for cooking and heating in hun-dreds of millions of households in devel-oping countries have been linked toincreased heart and lung disease mor-tality in exposed people. In particu-lar, CO can increase CVD through itsreduction of blood oxygen transport.Other components of indoor smokeinfluence CVD indirectly via their effectson the lungs.
Increasing evidence, much of it fromNorth America and Europe, suggeststhat CVD morbidity and mortality areassociated with outdoor air pollutionat relatively low levels (less than 100g/m3), especially airborne particles(PM10). A 10 g/m3 increase in PM10 lev-els has been estimated to be associat-ed with a 1% increase in cardiovas-cular mortality.
CANCER
Among the different cancer sites, can-cer of the trachea, bronchia or lungsis the leading cause of cancer death,accounting for more than 17.2 % ofdeaths in 1993, followed by stomachcancer, colon and rectum cancer, lip,oral cavity and pharynx cancer, livercancer, and female breast cancer.Collectively, cancer in these sitesaccounted for 57% of all cancers in1993.
About 5% of cancers could be due tooccupational exposures, 5% to virusesand other infectious agents (many ofwhich are due to environmental expo-sures) and 2% to air pollution. Manyof the associated exposures are pre-ventable. WHO, for instance, estimatesthat over 1.5 million (15%) of the newcancer cases occurring each year couldbe avoided by preventing infectiousdiseases associated with them.
27
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT

Helicobacter pylori is one example of aninfectious agent which can act as anenvironmental link with cancer.
Other environmental factors con-tributing to cancer risk include chem-ical exposures, food additives, radongas, other types of radiation and solarUVR. Additionally, tobacco smoking,diet and alcohol consumption interactwith each other and with environ-mental exposure, producing a highertotal combined risk than that producedby simply adding together the risks ofeach single factor.
CHRONIC RESPIRATORYDISEASES
Chronic respiratory diseases encom-pass a broad variety of human illnesssuch as: chronic obstructive lung dis-ease due to particulate air pollution;interstitial fibrotic lung disease due tosilica, beryllium, and asbestos expo-sure; upper airway irritation due toexposure to formaldehyde and othergases; asthma in workers exposed to
organic substances, and chronic res-piratory infections in people exposedto indoor smoke caused by combus-tion of biomass fuels (Table 5.12).
Infants in urban areas appear to beat increased risk of mortality due toambient (outdoor) air pollution andboth rural and urban children devel-op asthma and ARI at excess rates asa result of exposure to indoor and out-door air pollution. Additionally, hun-dreds of millions of adult women indeveloping countries are exposed toextremely high levels of airborne par-ticulates when cooking on stoves usingbiomass fuels.
In the workplace — especially in man-ufacturing, construction, and farming— adult men, and to a lesser extent,women, are occupationally exposed tofibrogenic dusts, irritant gases, and car-cinogenic agents.
Occupational chronic respiratory dis-eases are generally believed to consti-tute one-third of all occupational ill-nesses. As many as 50 million casesmay occur each year among the glob-al labour force. These diseases are ofgreat concern because they are wide-spread, debilitating, and affect peoplein the social and economic prime oftheir lives. They are also highly pre-ventable.
OTHER DISEASES
A number of other diseases and healthproblems are associated with expo-sures to environmental factors. Twospecific examples have been of con-cern in recent years: allergies and repro-ductive health problems. Allergic dis-eases mainly affect the respiratory sys-tem (asthma, hay fever, allergic rhini-tis), the skin (eczema) and the diges-tive system, and other parts of the bodyin the form of the autoimmune dis-eases. Growing motor vehicle air pol-lution makes it likely that asthma inci-dence will rise. Other environmentalexposures contributing to increasedasthma incidence include chemicalsin the workplace, indoor air pollutantsand certain food additives. Hand
28
EXECUTIVE SUMMARY
Table 5.12
Spectrum of environmental and occupational lung diseases
Exposure category Settings Populations at risk OutcomesAmbient air pollution Urban areas Infants, elderly Respiratory mortality
Industrial settings People with pre-existing Cardiovascular mortalityrespiratory diseases Chronic obstructive
lung diseaseAsthmaInfant respiratory mortality
Indoor air pollution Developed countries General population Lung cancerRadon-exposed areas Sick building syndromeOffice and commercial Asthmabuildings Solvent-related symptomsPrivate residences Legionnaire’s disease,
other infectious diseasesDeveloping countriesHome biomass fuel use Women, children Acute respiratory infectionfor cooking and heating Chronic obstructive lungRural > urban diseases
Lung cancerOccupational exposures Workplaces Men > women Lung cancer
Young and middle-aged MesotheliomaAsthmaChronic obstructivelung diseasePneumoconioses

eczemas are common in the generalpopulation, one estimate showing aprevalence of 10%.
Other health conditions that have beenlinked to environmental hazard expo-sures relate to reproduction, childbirthand the first days after a child is born.Living conditions and exposures toenvironmental hazards play importantroles with respect to the health ofthe mother and the newborn child, andother aspects of reproductive health.
Genetic damage has possibly the mostadverse basic effect on reproductionsince it may interfere with cell divisionand early development of the embryoand fetus. Experimental studies haveshown that ionizing radiation and cer-tain chemical compounds can causesuch damage. Other effects of envi-ronmental hazards on the fetus includeslow growth and low birth weight.
Infertility in both women and men hasbeen associated with exposure to envi-ronmental hazards. POPs and subse-quent disruption of endocrine func-tions have received much attention inthis respect (see Box 2.8) and in rela-tion to breast cancer. As these chem-icals accumulate in the environment,more and more people may be increas-ingly exposed.
ENVIRONMENTAL FACTORSAND THE GLOBAL BURDENOF DISEASE
In different ways and to differentdegrees each of the disease and dis-ability categories discussed above owetheir presence to one environmentalfactor or another. A summary portrayalof the environmental portion of theglobal burden of disease is given inTable 5.14. Applying these percentagesacross the diseases and conditions indi-cated leads to an estimate of the totalDALY burden that is associated withenvironmental factors. This is 320 mil-lion or 23% of the world’s total DALYburden.
In our analysis of the approximate envi-ronmental contribution of the health
conditions described in this chapter,we emphasize long-term sustainableprevention rather than curative mea-sures. We also assume that environ-mental preventive actions are takenfirst. The environmental fraction is con-sidered as the fraction of disease occur-rence that could be averted throughfeasible environmental interventionsbefore other interventions are applied.
The diseases or other types of poorhealth with the largest environmentalcontribution to disease burden (ARI,diarrhoeal diseases, malaria and unin-tentional injury) are also those whichparticularly affect children. Using thepercentage of all DALYs contributedby children under age 15 (Table 5.3),estimates of the “child component”of environmental DALYs can be made(Table 5.14). As seen in Table 5.14, thischild component adds up to 15% of allDALYs or about two-thirds of envi-ronmental DALYs. Taking action toreduce environmental DALYs couldthus make a major contribution to childhealth.
The impact of population growth andthe growth in the proportion of elder-
29
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
Table 5.14
Proportions of global DALYs associated with environmental exposures — 1990
EnvironmentalGlobal DALYs Environmental DALYs % of all DALYs(thousands) fraction (%) (thousands) (all age groups) (age 0–14 years)
Acute respiratory infections 116 696 60 70 017 5 4.5Diarrhoeal diseases 99 633 90 89 670 6.5 6.1Vaccine-preventable infections 71 173 10 7 117 0.5 0.49Tuberculosis 38 426 10 3 843 0.3 0.04Malaria 31 706 90 28 535 2.1 1.8injuries
unintentional 152 188 30 45 656 3.3 1.6intentional 56 459 N.E. N.E.
Mental health 144 950 10 14 495 1.1 0.08Cardiovascular diseases 133 236 10 13 324 1 0.12Cancer 70 513 25 17 628 1.3 0.11Chronic respiratory diseases 60 370 50 30 185 2.2 0.57Total these diseases 975 350 33 320 470 23 15.4Other diseases 403 888 N.E. N.E.Total all diseases 1 379 238 (23) (320 470)
N.E.: not estimated
Source: DALY data from Murray & Lopez, 1996b.

30
EXECUTIVE SUMMARY
ly age group on the relative importanceof different diseases and disabilities inrelation to the total disease burden, isexpected to be profound. New diseasepatterns are anticipated whereby non-communicable diseases come to theforefront in developing countries. Theassumed decline in infectious diseasesis based on the assumption that socioe-conomic development will decreasedisease incidence and severity, andthat research and development willmake available antibiotics that are effective against resistant strains ofmajor pathogens. But this assumptionmay be considered very optimistic inlight of the severe constraints outlinedin earlier chapters, such as increasedwaste production and pollution, waterscarcity, land limitation and global envi-
ronmental change. The potential detri-mental consequences of global envi-ronmental change on human healthworldwide makes it even more imper-ative that future scenarios be realisticand take potential lack of action toimprove environmental health and oth-er conditions explicitly into account.
“We increasingly understand thatthe health and well-being of ourfamilies depends upon a clean andhealthy environment. Nowhere isthis more true than in the case ofchildren, who are particularly vul-nerable to pollution”Declaration of the EnvironmentLeaders of the Eight IndustrialNations, 1997.

31
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
THE NEED FOR ANINTEGRATED FRAMEWORK
The problems facing the health sectortoday are increasingly complex, mul-tidisciplinary in nature, often ill-defined,and solutions to them uncertain. Thehealth sector cannot address these prob-lems on its own. New and innovativeapproaches are needed to integrate andoperationalize concepts of environ-mental sustainability, economic devel-opment and community developmentif human development is to be achieved.Wide-ranging reforms are also need-ed to more adequately deal with assess-ment and management of environ-mental health risks within a frame-work of sustainable development.
INTERNATIONAL INITIATIVES
UNCED asked the UN organizationsto play an active role in supportingcountries in sustainable developmentplanning and implementation of Agenda21 (UN, 1993). Many agencies are nowactive in health and environment anda number of collaborative activitieshave been strengthened or initiatedsince 1992, including those of the WaterSupply and Sanitation CollaborativeCouncil; the International Programmeon Chemical Safety, and the WHO,FAO and UNEP collaborative Panel ofExperts on Environmental Managementfor Vector Control (PEEM), whichaddresses vector-borne disease prob-lems that can result from waterresources development projects. Yetother activities, relating to occupationalhealth, have been developed by WHOand ILO, for example.
New initiatives include the creation ofthe Intergovernmental Forum on
Chemical Safety (IFCS) in 1994. TheForum is a non-institutional arrange-ment which provides an opportunityfor national governments, intergov-ernmental organizations and NGOs tomeet and consider issues associatedwith the assessment and managementof chemical risks.
The development of international con-ventions on key issues has proved tobe an important tool for securing inter-national cooperation on health-and-environment issues. At the EarthSummit such conventions on biodi-versity, deforestation and climate changewere discussed. Subsequently, theseand other international conventionson ozone-depleting chemicals, trans-boundary pollution and other key issueswere ratified by a number of countries.Agreements at the bilateral or multi-lateral level have also been instrumentalin reducing transboundary pollution.
A STRONGER HEALTH FOCUSIN NATIONAL PLANNING FORSUSTAINABLE DEVELOPMENT
Agenda 21 presented a golden oppor-tunity for health authorities to increasetheir influence on national planningand to reverse the trend of environ-mentally damaging and health-threat-ening development. Many countrieshave instituted new policy and plan-ning tools since the Earth Summit tomake environmental concerns a partof the planning process.
Measures to incorporate health-and-environment initiatives into nationalprogrammes have varied from coun-try to country, depending on planningmechanisms, the current status of sus-tainable development in the specific
CHAPTER 6
Integrated Policies, Strategies andActions: Progress Since the Earth Summit

country, and the way in which plan-ning responsibilities are divided. Thusdifferent approaches are being usedfor promoting health sector involve-ment in addressing health-and-envi-ronment issues. In some countries,health-and-environment plans havebeen prepared for inclusion in nation-al plans for sustainable development.In others, sectoral plans have beenreviewed and modified to includehealth-and-environment concerns.Many countries have established inter-sectoral committees for Agenda 21 fol-low-up. The health sector has beenable to exert significant influence,through these fora — which ofteninclude task forces and working groups
set up to address specific issues.Examples of country initiatives aregiven in Box 6.2.
A STRONGER HEALTH FOCUSIN LOCAL PLANNING FORSUSTAINABLE DEVELOPMENT
There is consensus that sustainabledevelopment can only occur at glob-al level if it first occurs at local level.One of UNCED’s most notable resultshas been the creation of a large num-ber of Local Agenda 21 initiatives, espe-cially in cities, but also in villages andeven on islands. Many of these featurehealth and health-related objectivesand activities.
Local Agenda 21 and related activitiesinclude, the WHO Healthy CitiesMovement, the Sustainable CitiesMovement (of UNCHS) and the ModelCommunities Programme of theInternational Council for LocalEnvironmental Initiatives. They all rec-ognize the fundamental importance andcentral role that communities can playin bringing about change. This impliesdecentralization. Indeed, a global trendtowards decentralized government ser-vices and greater emphasis on health-and-environment actions on the part ofNGOs and the community itself cannow be discerned. All these initiativesfocus on the development of partici-patory planning models.
RENEWING “HEALTH FOR ALL”
In 1977 the World Health Assemblydecided that the main social target ofgovernments and of WHO should bethe “attainment by all the people of theworld by the year 2000 of a level ofhealth that will permit them to leada socially and economically produc-tive life” — popularly known as “Healthfor All by the Year 2000». But beneathencouraging facts about decreasingmortality and increasing life expectan-cy, and many other unquestionableadvances, lie unacceptable disparitiesin health between rich and poor,between one population group andanother, between age groups, andbetween the sexes.
32
EXECUTIVE SUMMARY
Box 6.2
Country initiatives
In Jordan, an intersectoral working group was set up by the Ministry of Health and anational health-and-environment action plan prepared.
In Guatemala, a working team was established with representation from the HealthMinistry, planning and environment sectors, and a national plan for environmental healthand sustainable development produced, accompanied by an institutional analysis of nation-al sectors associated with health and the environment.
In Guinea-Bissau, a national inter-ministerial committee on health and the environ-ment was constituted to foster a national process of coordination among agencies, gov-ernment, and civil society, conducive to the integration of health-and-environment concernsinto overall national sustainable development planning. A national plan of action on healthand environment for sustainable development was produced.
In Iran, a draft strategy document on health and environment was developed, to beincorporated ultimately into a national strategy on sustainable development. The draft strat-egy included a situation analysis, and proposals for structural and institutional reform.
In Nepal, a health perspective was added to the draft Nepal Environmental Policy andAction Plan. Initially, it did not incorporate a public health component. Through the NepalEnvironmental Health Initiative, a comprehensive health-and-environment strategy wasdeveloped, and most of the resultant recommendations incorporated into the final EnvironmentalPolicy and Action Plan.
In the Philippines, collaboration was strengthened between health agencies and thePhilippine Council for Sustainable Development. The latter oversees implementation of activ-ities in support of commitments to sustainable development principles made at the EarthSummit. An Interagency Committee on Environmental Health organized by the Ministry ofHealth and the Council jointly sponsored at detailed analysis with case studies of the bestway of integrating health-and-environment issues into the development and implementa-tion of national plans for sustainable development.
Source: WHO, 1995I.

33
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
In 1995, therefore, the World HealthAssembly called for a reassessment ofthe Health-for-All Strategy, to culmi-nate in a Renewal Strategy. Varioustrends have made renewal necessary,including globalization of trade, trav-el and technology, urbanization andthe growth of megacities, wideninggaps between the rich and poor, chang-ing concepts of health, the rise of non-communicable diseases, environmen-tal threats, and expanded scientific andtechnical knowledge.
The new strategy will work on incor-porating forecasts of future trends indisease burden in policy-making andforward planning. More accurate esti-mation of future disease burdens willtherefore be needed. This in turn willdemand a more comprehensive under-standing of health determinants, includ-ing the complex interactions betweensocioeconomic, environmental, demo-graphic and macropolitical and healthsector determinants.

35
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT
At the time of the Earth Summit in1992 the WHO Commission on Healthand Environment presented an assess-ment of the relationship between healthand environment, in the context ofdevelopment. The report of theCommission was a major contributionto UNCED and brought health towardsthe top of the environment and devel-opment agenda.
The Rio Declaration’s first principleaffirms that human beings are entitledto a healthy life. Five years is a shorttime in which to report on progress insuch a complex field as health and envi-ronment, but the Special Session of theUN General Assembly review pre-sented an opportunity for reassess-ing the available information on health-and-environment linkages, and analysingthis information in the context of sus-tainable development.
The major health problems due to envi-ronmental hazards remain, but progresscan be seen in awareness raising, pol-icy and planning at various levels andconcrete action, particularly actionat the local level. Health indicatorsin some countries have improved main-ly due to economic development.However, the benefits of developmentare not distributed equitably andabsolute poverty is still on the increaseglobally.
It is the poor who are most vulnera-ble to health-and-environment hazards.Furthermore, it is becoming increas-ingly clear that the environmental fac-tors that most affect health are in turnlinked to underlying pressures on theenvironment. These pressures are deter-mined by driving forces such as pop-ulation growth, inequitable resource
distribution, consumption patterns,technological development and eco-nomic development. Since these pres-sures and subsequent health hazardsare associated with the activities ofseveral sectors, effective action to pro-tect health will require coordinationand collaboration between them.
Indeed, the 21st Century calls for anew health system which is partner-ship-oriented, population health-based,and proactive rather than reactive. Thehealth sector must serve as a guideto and be a partner in these actions sothat health concerns are representedappropriately at all stages of imple-mentation.
A number of major conclusions emergefrom the assessments made in thisbook. They are not listed here in orderof priority because each of them is ofmajor importance at global level andthe specific concerns at the local andnational levels vary.
• Environmental quality is animportant direct and indirectdeterminant of human health.Deteriorating environmental condi-tions are a major contributory fac-tor to poor health and poor qualityof life and hinder sustainable devel-opment.
• Major challenges to sustainabledevelopment are posed by mis-management of natural resources,excessive waste production and asso-ciated environmental conditions thataffect health.
• Impoverished populations livingin rural and peri-urban areas areat greatest risk from degraded
CHAPTER 7
Conclusions

environmental conditions. Thecumulative effects of inadequate andhazardous shelter, overcrowding,lack of water supply and sanitation,unsafe food, air and water pollution,and high accident rates, impact heav-ily on the health of these vulnera-ble groups.
• Poor environmental quality isdirectly responsible for around25% of all preventable ill-healthin the world today, with diarrhoealdiseases and ARI heading the list.Other diseases such as malaria, schis-tosomiasis, other vector-borne dis-eases, chronic respiratory diseasesand childhood infections are alsostrongly influenced by adverse envi-ronmental conditions, as are injuries.
• In today’s world, it is children’shealth that is most damaged bypoor environmental quality. Asmuch as two-thirds of all preventableill health due to environmental con-ditions occurs among children.
• Lack of basic sanitation, poorwater supply and poor food safe-ty contribute greatly to diarrhoealdisease mortality and morbidi-ty. Curative measures have broughtthe number of deaths from diarrhoealdiseases down, but action that dealswith the root causes of these dis-eases continues to be lacking.
• Air pollution figures prominent-ly as a contributor to a numberof diseases (ARI, chronic respira-tory diseases, CVD and cancer) andto a lowering of the quality of life ingeneral.
• The occurrence of the major vec-tor-borne diseases is closely relat-ed to naturally existing environ-mental conditions. In addition, the
incidence, severity and distributionof vector-borne diseases are affect-ed substantially by human activitiessuch as water and agricultural devel-opments and by urbanization.
• Hazardous chemicals and vari-ous forms of hazardous waste,including healthcare wastes, areincreasing health-and-environ-ment concerns. The lack of detailedquantitative information on the pro-duction and disposal of such waste,and the lack of information on theresulting health risks, severely ham-per efforts to control this problem.
• Global environmental change hasgreat implications for health, par-ticularly that of the poor.Marginalized population groups areagain at greatest risk, as their abili-ty to adapt is limited due to lack ofresources.
• There are some promising signs— not yet in terms of environmen-tal improvement, but rather in thenational development of policies andinfrastructure to address the prob-lems described here. However, thelack of financial and human resourcesis a major deterrent to progress.
• The health sector has an essen-tial advocacy role to play in high-lighting the links between health,environment, and sustainabledevelopment when future policiesare developed and actions planned.A much stronger partnership betweenthe health sector and other sectorsis required for successful reductionof health threats arising from poorenvironmental conditions. Renewalof the WHO Health-for-All Policyfor the 21st Century, which is cur-rently in progress, provides guidancefor the way ahead.
36
EXECUTIVE SUMMARY

References
AAMA (1996) World motor vehicle data 1996. Detroit, Michigan, AmericanAutomobile Manufactures Association.
Batliwala (1987) Women’s access to food. Indian journal of social work, 48(3):255–271.Bojkov RD et al. (1997) Proceedings of Ozone Symposium, Aquila, Italy, 1997.
Geneva, International Ozone Commission.Bradley DJ & Narayan R (1987) Epidemiological patterns associated with agri-
cultural activities in the tropics with special reference to vector-borne diseases. In: Effects of agricultural development on vector-borne dis-eases. Rome, FAO. (unpublished document AGL/MISC/12/87)
Briggs D, Corvalán C & Nurminen M, eds. (1996) Linkage methods for environ-ment and health analysis: general guidelines. Geneva, WHO (unpublisheddocument WHO/EHG/95.26).
Chatterjee & Lambert (1989) Women and nutrition: reflections from India andPakistan. Food and nutrition bulletin, 4:13–28.
Das Gupta M (1987) Selective discrimination against female children in ruralPunjab, India. Population and development review, 13(1):77–100.
Economopoulos AP (1993) Assessment of sources of air, water, and land pollu-tion: a guide to rapid source inventory techniques and their use in formu-lating environmental control strategies. Part one: rapid inventory techniquesin environmental pollution. Geneva, WHO (unpublished documentWHO/PEP/GETNET/93.1–A)
FAO (1996a) Rome declaration on world food security and world food summit planof action. World Food Summit, 13–17 November 1996. Rome, Food andAgriculture Organization of the United Nations (WFS/96/3)
Gittelsohn J (1991) Opening the box: intrahousehold food allocation in ruralNepal. Social science and medicine, 33(10):1141–1154.
IFCS (1996) Persistent organic pollutants: considerations for global action. IFCSExperts meeting on POPs: final report Geneva, IFCS. (unpublisheddocument IFCS/EXP. POPs/Report.1)
IPCS (1995a) Persistant organic pollutants: an assessment report on DDT-Aldrin-Dieldrin- Endrin-Chlordane-Heptachlor-Hexachlorobenzene-Mirex-Toxaphene,Polychlorinated biphenyls, dioxins and furans. Geneva, WHO (unpub-lished document PCS/95.38)
Kjellström T & Corvalán C (1995) Framework for the development of environ-mental health indicators. World health statistics quarterly, 48:144–154
McMichael AJ et al., eds (1996) Climate change and human health: an assessmentprepared by a Task Group on behalf of the World Health Organization, theWorld Meteorological Organization and the United Nations. Geneva, WHO(unpublished document WHO/EHG/96.7)
Murray CJL & Lopez AD, eds. (1996b) The global burden of disease: a compre-hensive assessment of mortality and disability from diseases, injuries, andrisk factors in 1990 and projected to 2020. Published by Harvard Schoolof Public Health on behalf of the WHO and the World Bank. Cambridge,Massachussets, Harvard University Press.
37
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT

Pan American Sanitary Bureau/UN–ECLAC (1994) Health, social equity and chang-ing production patterns in Latin America and the Caribbean. Documentsubmitted to the Twenty–fourth Pan American Sanitary Conference,Washington, DC, 26–30 September 1994. Cartagena.
Psacharaopoulos G et al. (1993) Poverty and income distribution in Latin America:the story of the 1980s. Washington, DC, The World Bank, Latin Americaand the Caribbean Technical Department, Regional Studies Program.(Report No. 27)
Smith KR (1991) Managing the risk transition. Toxicology and industrial health,7:319–327.
Smith KR (1996) Indoor air pollution in developing countries: growing evidenceof its role in the global disease burden. In Yoshizawa S et al., eds. (1996)Indoor air ‘96: proceedings of the 7th International Conference on IndoorAir Quality and Climate, Nagoya, Japan,21–26 July 1996. Tokyo, Japan,Institute of Public Health.
Smith KR & Figueroa M (1997) Global household use of solid fuels: a roughestimation. (in preparation)
UN (1993) Agenda 21: tThe United Nations programme of action from Rio. NewYork, UN.
UN (1995b) Report of the International Conference on Population and Development.Cairo, 5–13 September 1994. New York, UN. (document A/conf. 171/13/rev.1)
UN (1996b) The Beijing declaration and the platform for action. Fourth WorldConference on Women, Beijing, China, 4–15 September 1995. New York,UN Department of Public Information.
UNCHS (1996a) Report of the United Nations Conference on Human Settlements(HABITAT II), Istanbul, Turkey, 3–14 June 1996. New York, UN(A/CONF.165/14)
UNCHS (1996b) An urbanizing world: global report on human settlements, 1996.Oxford, Oxford University Press.
UNDP (1991) Human development report 1991. New York/Oxford, Oxford UniversityPress.
UNDP (1994) Human development report 1994. New York/Oxford, Oxford UniversityPress.
UNEP (1995b) Water quality of world river basins. Nairobi, UNEP (UNEPEnvironment Library No. 4)
UNHCR (1995) State of the world’s refugees: in search of solutions. Oxford, OxfordUniversity Press.
UNPF (1989) The state of the world population 1989. New York, United NationsPopulation Fund.
Unidad de Análises de Políticas Sociales (1993) Inversión en capital humano yfocalización del gasto social. La Paz, Bolivia, Ministry of HumanDevelopment.
Vogel RJ (1988 ) Cost recovery in the health care sector: selected country studies in WestAfrica.Washington DC, World Bank (World Bank Technical Paper No. 82)
WHO (1989e) Health principles of housing. Geneva, WHO. WHO (1995a) World health report 1995: bridging the gaps. Geneva, WHO.1995l) The healthy route to a sustainable world: health, environment and sustain-
able development. Geneva, WHO. (unpublished document WHO/EOS/95.21)WHO (1996a) World health report 1996: fighting disease, fostering development.
Geneva, WHO.WHO (1997h) CTD progress report. Geneva, WHO (unpublished document
CTD/PR/97.1)
38
EXECUTIVE SUMMARY

WHO/UNICEF (1996a) Water supply and sanitation sector monitoring report:sector status as of 31 December 1994. Geneva, WHO (unpublished doc-ument WHO/EOS/96.15)
WRI (1996) World resources report 1996–97: a guide to the global environment.Urbanization. New York, Oxford University Press (joint publicationwith UNDP, UNEP and the World Bank).
World Bank (1993) World development report 1993 : investing in health. NewYork/Oxford, Oxford University Press
Yach D & Harrison D (1995) Inequalities in health: determinants and status inSouth Africa. In: van der Walle K et al., eds. Health matters: public healthin North–South perspective. Health Policy Series, Part 9. Amsterdam,The Netherlands, Houten–Diegem.
39
HEALTH AND ENVIRONMENT IN SUSTAINABLE DEVELOPMENT





























